Deep discoveries: the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine
|
|
|
- Bartholomew Jacobs
- 6 years ago
- Views:
Transcription
 Canada Research Chair in Emergency Airway Diseases Department of Emergency")
1 Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta
2 Respiratory Conflicts Support for the studies reported in this talk: CIHR (ON); University of Alberta Hospital Foundation (AB); Canadian Assoc. of Emergency Physicians (CAEP); Department of Emergency Medicine, U of Alberta; The presenter is not a paid employee or consultant for any sponsor except the University of Alberta. Research funding and speakers fees for COPD- related topics from: GSK, AZ.
3 Outline Acute respiratory infections. Asthma, COPD, pneumonia (viral and bacterial) Evidence-based approaches: Antibiotics; Systemic corticosteroids; NIV. Emerging issues: Resistance, antibiotic duration and admission decisions. Summary.
4 Dyspnea how it should be treated!
5 Dyspnea sadly, this is how it is treated.
6 Case Presentation 31 year old male patient with history of asthma since age 8. Gradual deterioration X 3 days with exposure to dust; cough, SOB, and sputum x 3 days. Never smoked, no IN2B8 Ns; last admit ~ 12 years ago. O/E: short sentences; 1:2 = I: E; work of breathing; diffuse wheezing. Vitals: PR = 118/min (NSR) RR = 28/min T = 36.8 C SaO 2 = 94% Severity assessment? Differential Dx? Treatment?
7 Laboratory tests CBC: WBC = 19.4 (17 PMNs); Hgb = 145 Lytes - normal Urine normal. Spirometry: FEV 1 /FVC = 55% predicted; FEV 1 = 45% predicted improved with SABA.



8 Radiograph (not always needed)!
9 Pathophysiology - Asthma Definition: multi-factorial chronic respiratory disease, characterized by a history of intermittent symptoms (cough and/or wheeze and/or breathlessness) exacerbated by irritants (URTI). Pathophysiology of the acute episode: Primary: Airway inflammation; Secondary: Airway bronchospasm; Long-term:? Fixed airway obstruction. Acute treatment addresses primary inflammation and bronchodilators for reversible airway obstruction.
10 Asthma First line agents: Salbutamol + IB (MDI vs nebs) repeatedly; Systemic corticosteroids. Second line: MgSO 4 IV 2 grams over 20 minutes; ICS (variable doses). Final efforts: IM epinephrine (? allergy); NIV.
11 Asthma and infections Most infections i in acute asthma are viral. Antibiotics are not recommended as first line agents (but often used). Antibiotics are indicated d with signs of infection: fever, +ve sputum, new infiltrate on CXR. If failed aggressive anti-inflammatories, inflammatories, some pulmonary specialists suggest a trial of broad spectrum antibiotics after a week.
12 Case Presentation 80 year old male patient with emphysema. Gradual deterioration X 10 days cough, g, SOB, and sputum x 3 days. Ex-smoker X 1 year (60 pack years); Combivent (QID) + Theodur; Allergy: levo-something. O/E: tripod posture ;1:3=I:E; work of breathing; A/E to bases. Vitals: PR = 120/min (AF) RR = 40/min T = 37.9 C SaO 2 = 80% Severity assessment? Differential Dx? Treatment?
13 Radiograph
14 Pathophysiology - COPD Definition: chronic disease, mainly caused by tobacco exposure, characterized by a history of progressive symptoms (cough and/or wheeze and/or breathlessness). Pathophysiology of the acute episode: Primary: Airway infection; Secondary: Airway inflammation; Long-term: progressive decline in lung capacity. Acute treatment addresses primary infection and inflammation with underlying non-reversible airways.
15 ED COPD COPD exacerbations are common emergency department presentations. Exacerbations result in significant: Costs to the health care system; Impairments in quality of life for patients. Serious sequelae very common: Admissions to hospital; Airway support: NIV, IN2B8 ns; Death (fastest rising cause of CD death).
16 Classification of exacerbations Type 1 Increased dyspnea Increased sputum volume Increased sputum purulence Type 2 Two of the above Type 3 One of the above Anthonisen NR et al. Ann Intern Med 1987;106:
17 Bronchodilator choices Not as clear cut as asthma. Both salbutamol and IB are effective. Synergy: Not as effective. Side effects: More pronounced with salbutamol. Delivery: er MDI + spacer vs nebs in 2011.


18 Corticosteroids in Exacerbations of COPD
19 All evidence Systemic corticosteroids id vs placebo: Cochrane Review: high quality; Involving 11 trials and >1080 adult patients; Outcomes: Fewer treatment failures within 30 days (OR = 0.50; 95% CI: 0.36 to 0.69) NNT = 10. LOS (Hosp): -1.2 days (95% CI: -2.3 to -0.2); Caveat: S/Es(OR=23;95%CI:16to34) 2.3; ). Walters H, et al. Cochrane Database Syst Rev. 2009; 1:CD
20 Corticosteroids after discharge Emergency Department discharge Emergency Department Treatment R Prednisone 40 mg po OD X 10 days Combivent 2 puffs QID + antibiotics Placebo prednisone Combivent 2 puffs QID + antibiotics Visit: 1 PC1 2 Week: days 4 weeks Aaron S, et al NEJM 2003; 348:

21 Prednisone for Out-Patient Acute Exacerbation of COPD Aaron S, NEJM 2003:348
22 Summary NNT: 7! Other outcomes: congruent. Systemic corticosteroids are effective in the early treatment t tof acute severe COPDto prevent admission and the out-patient treatment of COPD to prevent relapse. S/E s are impressive, so selection must be appropriate.
23 Antibiotics in Exacerbations of COPD Who needs them and which ones do you use?
24 Effectiveness of Antibiotics in COPD Placebo Antibiotic % Success s Type 1 Type 2 Type 3 Anthonisen NR et al. Ann Intern Med 1987;106: Anthonisen NR et al. Ann Intern Med 1987;106:
25 All evidence Systemic antibiotics i vs placebo (Type II/I): SR: high quality; Involving 11 trials and >900 adult patients; Outcomes: Lower mortality (RR = 0.23; 95% CI: 0.1 to 0.5) NNT = 10. Fewer treatment failures (RR = 0.47; 95% CI: 0.4 to 0.6) NNT = 3. NB: not influenced by the antibiotic choice. Ram F, et al Cochrane Database Syst Rev. 2006; 2:CD004403
26 Canadian Guidelines O'Donnell D, et al. CRJ 2007; 14:5B-32B
27 Antibiotic Considerations Duration of treatment? 5 = 10 days
28 Summary Systematic ti review (21 studies; 10,698 pts). A short course of antibiotics (5 days) seems to be just as effective in achieving clinical and bacteriological cure rates as a longer course (7-10 days). Given the side effects of antibiotics and the elderly nature of COPD patients, it seems reasonable to reduce the duration of antibiotics in this patient population. Moussaoui RE, et al. Thorax 2008; 63:
29 Short (< 5 days) vs long (>7 days) Moussaoui RE, et al. Thorax 2008; 63:
30 Question NIV in Exacerbations of COPD

31 NIV

32 The evidence Design: 10 RCTs (> 750 patients). Population: Acute severe COPD. Interventions: NIV. Control: standard care. Outcomes: Death, intubation, LOS High quality methods for SRs Ram FSF, et al. CDSR. 2004, Issue 3.
33 NIV treatment failures Ram FSF, et al. CDSR. 2004, Issue 3.
34 NIV Mortality outcome Ram FSF, et al. CDSR. 2004, Issue 3.
35 NIV Intubation outcome Ram FSF, et al. CDSR. 2004, Issue 3.
36 Summary NIV reduces treatment failures, mortality and intubations in the ED. Complications associated with treatment (RR 0.38; 95% CI 0.24 to 0.60) and length of hospital stay (WMD days; 95% CI to -2.06) were lower with NIV.
37 Case #3 72 year old female with week history of dyspnea, Lives with demented husband. Ex-smoker 8 pack years. HTN, hyperlipidemia. Vitals: PR = 104/min (NSR) RR = 32/min T = 37.9 C SaO 2 = 83% Severity assessment? Differential Dx? Treatment?
38 Radiograph
39 Viral pneumonia The Id don t get no respect of pneumonia. Common cause of CAP (variable up to 32%). Predominant causal agents: Influenza, RSV, rhinovirus, H1N study identified #1 agent: coronavirus. Bacterial CAP on antibiotics often coinfected with viruses. Lieberman D, et al. Chest 2010; 138:
40 Investigations CXR: Recommended in all ED patients with suspected pneumonia. CBC/lytes/other labs: complex / severe cases: Microbiology: Blood: admitted patients with fever only; Sputum cultures: non-response?; PCR swabs for suspected viral CAP. Personalized tests (limited application): CRP, Procalcitonin, urinary antigens.
41 Radiography +ve CXR treat (look for abscess and pleural effusion [PSI]). False negative CXR can occur if severe dehydration or too early in course illness. A patient with negative CXR, signs and symptoms should be treated and followed closely. ED physicians (+vs /-ve CXR) treated the same, outcomes similar.
42 Assessment of Severity Prognosis is difficult to predict in moderatesevere CAP; some clinical prediction rule is better than gestalt. Pneumonia Severity Index (PSI): PSI is based on 20 variables that are used to derive a score; Enables patients to be stratified into five risk categories based on 30-day mortality. Alternatives: CURB - CTAS? - CRB65

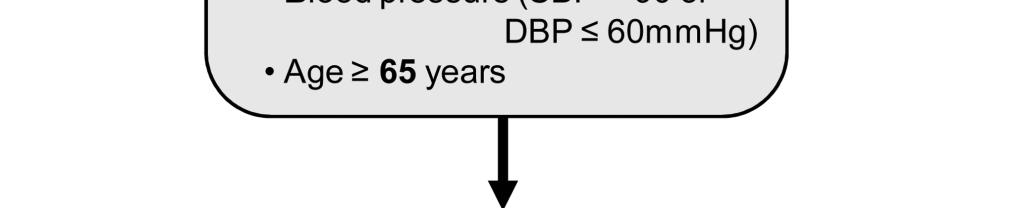
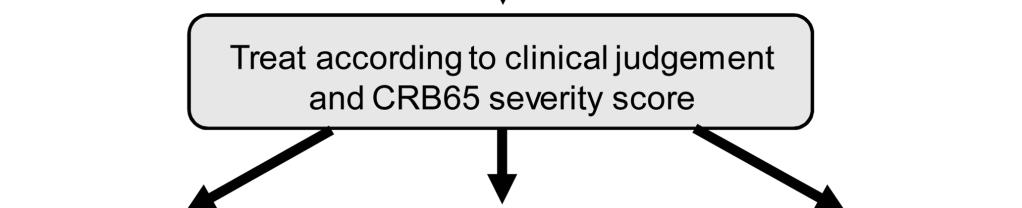
43 BTS Approach
44 Which should you use? SR of 40 studies and 81, day mortality patients (8.3% mortality) compared PSI, CURB-65 and CRB-65. Performance characteristics were similar across comparable cut-offs for low, intermediate and high risk for each score. CRB-65 had fewer low risk category pts. Chalmers JD, et al. Thorax. 2010;65:
45 Antibiotic Considerations I Empiric therapy?
46 Empiric antibiotic decisions IDSA (2007) - outpatients: First line: macrolide, doxycycline; Second line: respiratory fluoroquinolone. IDSA (2007) - inpatient: First line: respiratory fluoroquinolone; Second line: β-lactam plus macrolide. IDSA (2007) - ICU: First line: β-lactam plus azithromycin. Note: many recommendations are consensusbased.
47 Emerging Issues Corticosteroids, Antibiotic Resistance, and Performance Indicators.
48 Corticosteroids in pneumonia CDSR: 6 studies including 437 participants: i unable to make recommendations. Recent Lancet PICO-D: P: 304 pts with CAP admitted through ED; I: Dex 5 mg IV X 4 days + antibiotics; C: placebo + antibiotics; O: LOS; D: RCT. Results: 6.5 (dex) vs 7.8 (control) days. Chen Y, Li K, Pu H, et al.cdsr Mar 2011
:e139-e144.")
49 Representative Canadian Data Vanderkooi OG, et al. Can J ID Med Microbiol 2009;20(4):e139-e144.
50 Effect of Prior Antibiotic on S pneumoniae Resistance susceptib ble) Percent resistant t (or non No (or no known) antibiotic use Any prior antibiotic Prior use same class P enicillin Cefotaxime Erythromycin Tmp/Smx Quinolones Vanderkooi OG, CID 2005;40:
51 Performance indicators Increasing focus on how we do things. Proposed indicators can be gamed (Abx < 4 hours) and may not be evidence-based. ICES survey identified d KPIs for quality care in the ED. Respiratory (8): Asthma (4): % received CS in ED and at D/C; COPD (1): % received CS in ED and at D/C; CAP (3): time to antibiotic therapy. Schull M, et al. ICES (CJEM in press)
52 Antibiotic duration New paradigm: go hard and go home. Shorter courses of antibiotics may eradicate infection and decrease SAEs. Examples: AOM, UTI, etc. Overall evidence not as clear as COPD; however, out-patients don t need to be treated for as long as days.
53 Summary: Respiratory infections More expansive antibiotic i choices, although h the pipeline is drying up. Selective use of antibiotics (old is new); Empiric choices based on guidelines. Atypical and viral pathogens are increasingly common: Viral pneumonia (H1N1, influenza, etc); Management guidelines and local practice. Bacterial resistance stable 3 month queries.
54 Thanks for listening! Questions for Sam?
Antimicrobial Stewardship in Community Acquired Pneumonia
 Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
COPD exacerbation. Dr. med. Frank Rassouli
 Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma
 Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma Talk Outline Case Delivery of bronchodilators Meter-dose inhalers and spacers Continuous nebulization
Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma Talk Outline Case Delivery of bronchodilators Meter-dose inhalers and spacers Continuous nebulization
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
How do we define pneumonia?
 Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Pneumonia in the Hospitalized
 Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
Pneumonia 2017 OMAR PIRZADA
 Pneumonia 2017 OMAR PIRZADA Pneumonia Pneumonia is common 0.5-1% of adults per year, 5-12% presenting to GP with LRTi 22-42% will be admitted to hospital Symptoms and signs Case 1 26 year old man Sudden
Pneumonia 2017 OMAR PIRZADA Pneumonia Pneumonia is common 0.5-1% of adults per year, 5-12% presenting to GP with LRTi 22-42% will be admitted to hospital Symptoms and signs Case 1 26 year old man Sudden
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
CLAIRE NOWLAN & SAM SEARLE. Pneumonia in the nursing home
 CLAIRE NOWLAN & SAM SEARLE Pneumonia in the nursing home No disclosures or conflicts of interest PMHX: A. FIB. GERD MIXED DEMENTIA MMSE 16/30 HTN Mr. Hack 86 years old RAMIPRIL 4 MG OD PARIET 20MG OD DONEPEZIL
CLAIRE NOWLAN & SAM SEARLE Pneumonia in the nursing home No disclosures or conflicts of interest PMHX: A. FIB. GERD MIXED DEMENTIA MMSE 16/30 HTN Mr. Hack 86 years old RAMIPRIL 4 MG OD PARIET 20MG OD DONEPEZIL
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
CAP, HCAP, HAP, VAP. 1. In 1898, William Osler described community-acquired pneumonia as:
 1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
WORKSHOP. The Multiple Facets of CAP. Community acquired pneumonia (CAP) continues. Jennifer s Situation
 continues. Jennifer s Situation") Practical Pointers pointers For for Your your Practice practice The Multiple Facets of CAP Dr. George Fox, MD, MSc, FRCPC, FCCP Community acquired pneumonia (CAP) continues to be a significant health burden
Practical Pointers pointers For for Your your Practice practice The Multiple Facets of CAP Dr. George Fox, MD, MSc, FRCPC, FCCP Community acquired pneumonia (CAP) continues to be a significant health burden
COPD Treatable. Preventable.
 My COPD Action Plan Patient s Copy (Patient s Name) Date Canadian Respiratory COPD Treatable. Preventable. This is to tell me how I will take care of myself when I have a COPD flare-up. My goals are My
My COPD Action Plan Patient s Copy (Patient s Name) Date Canadian Respiratory COPD Treatable. Preventable. This is to tell me how I will take care of myself when I have a COPD flare-up. My goals are My
COPD in primary care: reminder and update
 COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA
 KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis. Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine
 Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Pediatric Respiratory Disease: A Model for the Future of Emergency Medicine Research
 Pediatric Respiratory Disease: A Model for the Future of Emergency Medicine Research Joseph J. Zorc, MD, MSCE Mark Fishman Professor, Department of Pediatrics Perelman School of Medicine, University of
Pediatric Respiratory Disease: A Model for the Future of Emergency Medicine Research Joseph J. Zorc, MD, MSCE Mark Fishman Professor, Department of Pediatrics Perelman School of Medicine, University of
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center
 Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Debating the use of inhaled corticosteroids in the treatment of COPD. COPD Epidemiology. A quick patient case. Risk Factors for COPD 1,2
 Debating the use of inhaled corticosteroids in the treatment of COPD Suzanne G. Bollmeier Pharm.D., BCPS, AE-C Associate Professor, St. Louis College of Pharmacy ACPE Guidelines on Non- Commercialism o
Debating the use of inhaled corticosteroids in the treatment of COPD Suzanne G. Bollmeier Pharm.D., BCPS, AE-C Associate Professor, St. Louis College of Pharmacy ACPE Guidelines on Non- Commercialism o
(cilia) that help sweep away fluids and/or particles International Journal of Pharmaceutical Sciences and Research 2055
 that help sweep away fluids and/or particles International Journal of Pharmaceutical Sciences and Research 2055") IJPSR (2014), Vol. 5, Issue 5 (Research Article) Received on 29 November, 2013; received in revised form, 21 February, 2014; accepted, 16 April, 2014; published 01 May, 2014 EVALUATION OF EFFICACY AND
IJPSR (2014), Vol. 5, Issue 5 (Research Article) Received on 29 November, 2013; received in revised form, 21 February, 2014; accepted, 16 April, 2014; published 01 May, 2014 EVALUATION OF EFFICACY AND
Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF
 Maximizing Care for Community- Acquired Pneumonia Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu 1. In 1898, William Osler described community-acquired
Maximizing Care for Community- Acquired Pneumonia Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu 1. In 1898, William Osler described community-acquired
What is New in COPD: Times Are Changing! Meredith Chiasson, MD, FRCPC April 6, 2018
 What is New in COPD: Times Are Changing! Meredith Chiasson, MD, FRCPC April 6, 2018 No disclosures Disclosures objectives How to diagnose & Assess severity Treatment: Pharmacologic Non-Pharmacologic Maintenance
What is New in COPD: Times Are Changing! Meredith Chiasson, MD, FRCPC April 6, 2018 No disclosures Disclosures objectives How to diagnose & Assess severity Treatment: Pharmacologic Non-Pharmacologic Maintenance
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF -- William Osler, M.D.
 Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu a. An ailment that often leads to suffocation and death. b. A friend of the aged. c. A common
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu a. An ailment that often leads to suffocation and death. b. A friend of the aged. c. A common
Upper...and Lower Respiratory Tract Infections
 Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Turning Science into Real Life Roflumilast in Clinical Practice. Roland Buhl Pulmonary Department Mainz University Hospital
 Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease
 HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic
 COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
Management of Acute Asthma Exacerbations in Children 2012 Update. Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch
 Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines
Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Disclosures. Case 1. Acute Bronchitis. Acute Bronchitis. Community-Acquired Pneumonia and other Respiratory Tract Infections. What do you recommend?
 Community-Acquired Pneumonia and other Respiratory Tract Infections none Disclosures Joel T. Katz, M.D. Associate Professor of Medicine Division of Infectious Diseases Brigham and Women s Hospital Case
Community-Acquired Pneumonia and other Respiratory Tract Infections none Disclosures Joel T. Katz, M.D. Associate Professor of Medicine Division of Infectious Diseases Brigham and Women s Hospital Case
Paediatric Wheeze and pneumonia. RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa
 Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
COPD: Preventable and Treatable. Lecture Outline. Diagnosis of COPD. COPD: Defining Terms
 COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN. Dr Lại Lê Hưng Respiratory Department
 TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN Dr Lại Lê Hưng Respiratory Department Literature review current through: Feb 2013. This topic last updated: Aug 14, 2012 INTRODUCTION Wheezing
TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN Dr Lại Lê Hưng Respiratory Department Literature review current through: Feb 2013. This topic last updated: Aug 14, 2012 INTRODUCTION Wheezing
Current Approaches to Asthma & COPD
 10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
Pulmonary and Critical Care Year in Review
 Pulmonary and Critical Care Year in Review Heath E Latham, MD Assistant Professor University of Kansas Dept of Internal Medicine Division of Pulmonary and Critical Care None Disclosure Lung Cancer Screening
Pulmonary and Critical Care Year in Review Heath E Latham, MD Assistant Professor University of Kansas Dept of Internal Medicine Division of Pulmonary and Critical Care None Disclosure Lung Cancer Screening
TORCH: Salmeterol and Fluticasone Propionate and Survival in COPD
 TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Acute Respiratory Infection. Dr Anthony Gibson
 Acute Respiratory Infection Dr Anthony Gibson Range of Conditions Upper tract Common Cold coryza Sore Throat- Pharyngitis Sinusitis Epiglottitis Range of Conditions Lower Acute Bronchitis Acute Exacerbation
Acute Respiratory Infection Dr Anthony Gibson Range of Conditions Upper tract Common Cold coryza Sore Throat- Pharyngitis Sinusitis Epiglottitis Range of Conditions Lower Acute Bronchitis Acute Exacerbation
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
CLINICAL PATHWAY. Acute Medicine. Chronic Obstructive Pulmonary Disease
 CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
Pulmonary Predicaments in Primary Care Peter F. Bidey, DO
 Pulmonary Predicaments in Primary Care Peter F. Bidey, DO Pulmonary Predicaments in Primary Care Peter F. Bidey, D.O. Clinical Instructor -Family Medicine Philadelphia College of Osteopathic Medicine
Pulmonary Predicaments in Primary Care Peter F. Bidey, DO Pulmonary Predicaments in Primary Care Peter F. Bidey, D.O. Clinical Instructor -Family Medicine Philadelphia College of Osteopathic Medicine
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
Fraser Health pandemic preparedness
 Fraser Health pandemic preparedness DRAFT Last revised: April 2006 General Management of Patients in Acute Care Facilities During an Influenza Pandemic 1. OVERVIEW GENERAL MANAGEMENT OF PATIENTS IN ACUTE
Fraser Health pandemic preparedness DRAFT Last revised: April 2006 General Management of Patients in Acute Care Facilities During an Influenza Pandemic 1. OVERVIEW GENERAL MANAGEMENT OF PATIENTS IN ACUTE
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT
 Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
AECOPD: Management and Prevention
 Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Known Allergies: Shellfish. Symptoms: abdominal pain, nausea, diarrhea, or vomiting. congestion, trouble breathing, or wheezing.
 CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
Management of Acute Exacerbations
 15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
Background. Background. Background 3/14/2014. Conflict of Interest Statement:
 Platform Presentations Comparison of zolpidem to other drugs associated with falls in hospitalized patients Ed Rainville, MSPharm. Conflict of Interest Statement: The speaker has no conflict of interest
Platform Presentations Comparison of zolpidem to other drugs associated with falls in hospitalized patients Ed Rainville, MSPharm. Conflict of Interest Statement: The speaker has no conflict of interest
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Patient characteristics Intervention Comparison Length of followup
 ORAL MUCOLYTICS Ref ID: 2511 Bachh AA, Shah NN, Bhargava R et al. Effect oral N- in COPD - A randomised controlled trial. JK Practitioner. 2007; 14(1):12-16. Ref ID: 2511 RCT Single blind; unclear allocation
ORAL MUCOLYTICS Ref ID: 2511 Bachh AA, Shah NN, Bhargava R et al. Effect oral N- in COPD - A randomised controlled trial. JK Practitioner. 2007; 14(1):12-16. Ref ID: 2511 RCT Single blind; unclear allocation
Chronic obstructive pulmonary disease
 Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Getting Smart About: Upper Respiratory Infections
 Getting Smart About: Upper Respiratory Infections Daniel Z. Uslan, MD Assistant Clinical Professor Director, Antimicrobial Stewardship Program UCLA Health System Disclosures None relevant to the topic
Getting Smart About: Upper Respiratory Infections Daniel Z. Uslan, MD Assistant Clinical Professor Director, Antimicrobial Stewardship Program UCLA Health System Disclosures None relevant to the topic
Predicting, Preventing and Managing Asthma Exacerbations. Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa
 Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Over the last several years various national and
 Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC
 KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC") Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Pharmacotherapy for COPD
 10/3/2017 Topics to be covered Pharmacotherapy for chronic treatment Pharmacotherapy for COPD Dr. W C Yu 3rd September 2017 Commonly used drugs Guidelines for their use Inhaled corticosteroids (ICS) in
10/3/2017 Topics to be covered Pharmacotherapy for chronic treatment Pharmacotherapy for COPD Dr. W C Yu 3rd September 2017 Commonly used drugs Guidelines for their use Inhaled corticosteroids (ICS) in
I have no perceived conflicts of interest or commercial relationships to disclose.
 ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
Guidelines/Guidance/CAP/ Hospitalized Child. PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014
 Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Community-Acquired Pneumonia. Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital. Nothing to disclose.
 Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Nothing to disclose. Community-Acquired Pneumonia Talk will focus on adults Guideline
Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Nothing to disclose. Community-Acquired Pneumonia Talk will focus on adults Guideline
Management of wheeze in pre-school children. Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne
 Management of wheeze in pre-school children Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne General Practitioner encounters for asthma Asthma in Australia, 2003 Emergency
Management of wheeze in pre-school children Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne General Practitioner encounters for asthma Asthma in Australia, 2003 Emergency
Management of Dyspnea and Cough in Lung Cancer
 Management of Dyspnea and Cough in Lung Cancer Dr. Chris Ogaranko Lung Cancer Educational Event November 2013 Presenter Disclosure Faculty: Dr. Chris Ogaranko Relationships with commercial interests: Grants/Research
Management of Dyspnea and Cough in Lung Cancer Dr. Chris Ogaranko Lung Cancer Educational Event November 2013 Presenter Disclosure Faculty: Dr. Chris Ogaranko Relationships with commercial interests: Grants/Research
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Guidelines. 14 Nov Marc Bonten
 Guidelines 14 Nov 2014 Marc Bonten Treatment of Community-Acquired Pneumonia SWAB/ NVALT guideline 2011, replaced SWAB guideline 2005 Empirical treatment must cover the most likely causative pathogen.
Guidelines 14 Nov 2014 Marc Bonten Treatment of Community-Acquired Pneumonia SWAB/ NVALT guideline 2011, replaced SWAB guideline 2005 Empirical treatment must cover the most likely causative pathogen.
Bronchial Provocation Results: What Does It Mean?
 Bronchial Provocation Results: What Does It Mean? Greg King 1 Department of Respiratory Medicine, Royal North Shore Hospital, St Leonards 2065 2 Woolcock Institute of Medical Research and Sydney Medical
Bronchial Provocation Results: What Does It Mean? Greg King 1 Department of Respiratory Medicine, Royal North Shore Hospital, St Leonards 2065 2 Woolcock Institute of Medical Research and Sydney Medical
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research
 Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Outline FEF Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications?
 Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Online Data Supplement. Prevalence of Chronic Obstructive Pulmonary Disease in Korea: Results of a Population-based Spirometry Survey
 Online Data Supplement Prevalence of Chronic Obstructive Pulmonary Disease in Korea: Results of a Population-based Spirometry Survey Dong Soon Kim, MD, Young Sam Kim MD, Kee Suk Chung MD, Jung Hyun Chang
Online Data Supplement Prevalence of Chronic Obstructive Pulmonary Disease in Korea: Results of a Population-based Spirometry Survey Dong Soon Kim, MD, Young Sam Kim MD, Kee Suk Chung MD, Jung Hyun Chang
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017
 Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Antibiotic Therapy in Preventing Exacerbations of Severe Chronic Obstructive Pulmonary Disease
 University of North Dakota UND Scholarly Commons Physician Assistant Scholarly Project Papers Department of Physician Studies 2018 Antibiotic Therapy in Preventing Exacerbations of Severe Chronic Obstructive
University of North Dakota UND Scholarly Commons Physician Assistant Scholarly Project Papers Department of Physician Studies 2018 Antibiotic Therapy in Preventing Exacerbations of Severe Chronic Obstructive
COPD exacerbation. Chiara Maruggi, PGY2
 COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise