Respiratory Management in Pediatrics
|
|
|
- Nathan Andrews
- 6 years ago
- Views:
Transcription

1 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT
2 Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory distress and impending respiratory failure. Discuss management of respiratory distress and respiratory failure. Case Scenarios.

3 Children are not small adults Children are still growing in every way. Their bodies are different, they perceive things and communicate differently, and the long term implications of treatment are not the same.

4 Respiratory Emergencies Pediatric Respiratory Emergencies # 1 reason for pediatric hospital admissions. # 1 cause of death during the first year of life with the exception of congenital abnormalities.
5 Early Intervention is Critical Respiratory Distress Respiratory Failure/Shock Cardiopulmonary Failure Cardiopulmonary Arrest
6 Pediatric Cardiopulmonary Arrests Cardiac 10% Shock 10% Respiratory 80% Most pediatric cardiopulmonary arrests begin as respiratory failure or respiratory arrest. Decrease respiratory reserve + Increased O2 demand = Increased respiratory failure risk
7 Respiratory Emergencies in Pediatrics Airway Diseases Croup, epiglottitis, asthma, bronchiolitis, foreign body aspiration, bronchopulmonary dysplasia. Lung Tissue Diseases pneumonia, ARDS, aspiration, pulmonary contusion Non-respiratory causes CNS depression, musculoskeletal disorders, thoracic disorders or injuries, shock

8 Why are children more vulnerable? Obligate nose breathers until 6 months Large tongue Lymphoid tissue achieves adult size at 2 Large, anterior epiglottis Narrow subglottic region Fewer alveoli Smaller airways: Hagen-Pouiselle s Law Decreased cartilage in airways Increased chest wall compliance Increased metabolic rate, increased O2 consumption Typical oxygen consumption 6-8 ml/kg/min in a child vs. 3-4 ml/kg/min in adult
9 Pediatric Airway

10 Airway Resistance Full Term Newborn Airway 1mm of edema, the diameter will be 44% of normal. Adult Airway 1mm of edema, the diameter will be 81% of normal. Poiseuille s law If radius is halved, resistance increases 16fold Resistance increases 3x in an adult and 16x in an infant. R = 8 n l r4

11 Adult Airway VS. Pediatric Airway Adult Pediatric
12 The Licorice Airway Please bite a small piece off to top and bottom of your licorice. We will now perform a test on your airway. Breath in and out of the licorice for 30 seconds.
13 Airway Management Position Position Position
14 Airway Positioning Sniffing Position In the child older than 2 years Towel is placed under the head

15 Airway Position - Children <2yrs

16 Airway Position - Children <2yrs
17 Pediatric Respiratory Management Airway Breathing Circulation Without an A you will not get a B.
18 Airway Management A Open it correctly! Position the patient in the neutral, supine position. Use the head tilt, chin lift to open the airway and place the patient in a sniffing position. Use a shoulder role. If you can not open the airway: Reposition! Clear the airway by suctioning any secretions within the mouth or nose.
19 Airway Assessment OPEN and CLEAR Able to Maintain Unable to Maintain
20 Maintaining the Pediatric Airway Nasal Airway Oral Airway Bag Masking Intubation

21 Foreign Bodies ALWAYS consider a foreign body as a cause of Respiratory Distress. Usually will have a SUDDEN onset.
22 Signs of Respiratory Distress Tachypnea Tachycardia Grunting Stridor Head bobbing Flaring Inability to lie down Agitation Retractions Accessory muscles Wheezing Sweating Prolonged expiration Apnea Cyanosis
23 Signs of Impending Respiratory Failure Reduced air entry Severe work Irregular breathing or apnea Cyanosis despite Oxygen delivery Altered Level of Consciousness Diaphoresis
24 Respiratory Failure Respiratory Failure is the inability of the airway and lungs to meet the metabolic demands of the body. Hypoxic Respiratory Failure Inadequate oxygenation Can t Get Oxygen in Hypercarbic Respiratory Failure Inadequate ventilation Can t Get CO2 out

25 Nasopharyngeal Airway Length: Nostril to Tragus Contraindications: Basilar skull fracture CSF leak Coagulopathy
26 Endotracheal tube as nasal airway A regular ETT can be cut and used as a nasal airway
27 Adjuncts: Oral Airway Wrong size: Too Long
28 Adjuncts: Oral Airway Wrong size: Too Short
29 Adjuncts: Oral Airway Correct size
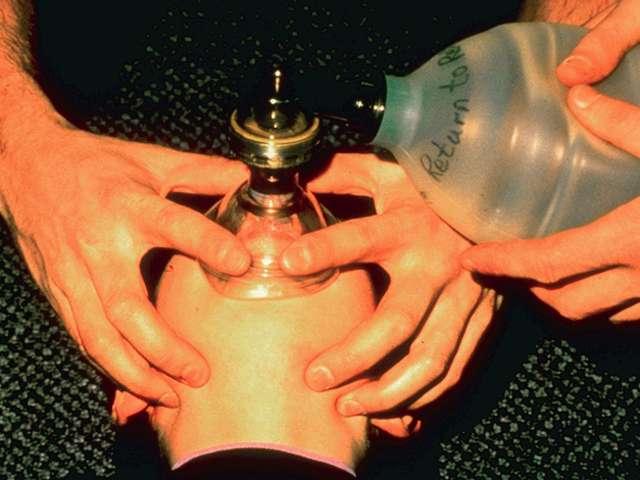
30 Bag Mask Ventilation
31 Intubation: Indications Failure to oxygenate Failure to remove CO 2 Increased WOB Cardiovascular failure Neuromuscular weakness CNS failure
32 Laryngoscope Blades Macintosh Miller

33 Airway Open? Able to maintain? Position and Assess? Bag/Mask? Intubation? Pediatric Airway with inflammation

34 A Closer Look Normal Pediatric Airway

35 A Closer Look Abnormal Pediatric Airway

36

37
38 ET Tube Sizing Age kg ETT Length (lip) Newborn mos yr yrs Children > 2 years: ETT size: (Age +16)/4 ETT depth (lip): Length of tube x 3 (Approximately)
39 Intubation Technique Better in younger children with a floppy epiglottis Straight Laryngoscope Blade used to pick up the epiglottis
40 Rapid Sequence Intubation When: Intubation is emergent and there is concern for aspiration Why: Obtain airway control rapidly and minimize aspiration risk How: All necessary intubation equipment and personnel Preoxygenate Rapidly acting sedative, analgesic and neuromuscular blocking agent are Presentation Template /15/2012
41 Rapid Sequence Intubation When: Intubation is emergent and there is concern for aspiration Why: Obtain airway control rapidly and minimize aspiration risk How: All necessary intubation equipment and personnel Preoxygenate Rapidly acting sedative, analgesic and neuromuscular blocking agent are Presentation Template /15/2012
42 Deterioration after Intubation Displaced tube Obstructed tube Pneumothorax Equipment

43 Respiratory Case Scenarios Let s manage some patients together
44 Case scenario 1 3 month old is admitted to the hospital with a runny nose, poor appetite, and frequent coughing. Classify patient

45 Scenario 1 Assessment
46 Scenario 1 Assessment Vitals H.R. = 136 R.R. = 60 WOB = Intercostal and subcostal retractions B.S. = Noisy breathing (crackles and wheezing) SpO2 on Room Air = 88% Diagnosis
47 Respiratory Syncytial Virus (RSV) RSV is a very common virus that infects half the children during their first year of life. Symptoms include wheezing, nasal congestion, rapid breathing, cough, irritability, retractions, poor feeding, sluggishness, and fever. Synagis is given as a prophalytic treatment to children with the highest risk for severe RSV.


48 RSV in the Airway Premature lung with RSV
49 Scenario 1 Treatment A Airway Management Secretion Management B Breathing * Suction before all feeds. Oxygen Therapy C Circulation Hydration Treat symptoms Prophylaxis (Synagis) SUCTION
50 The Nose Nose is responsible for 50% of total airway resistance at all ages Infant: blockage of nose = respiratory distress
51 Case Scenario 2 A 2 year old patient is admitted to the ED with lethargy, poor appetite for 3 days, fever, increasing respiratory distress. Classify Patient

52 Scenario 2 Assessment
53 Case Scenario 2 Vitals H.R. = 172 R.R. = 58 WOB = substernal retractions B.S. = rales, diminished bases SpO2 on Room Air = 80% Diagnosis
54 Scenario 2 Treatment A Airway Management Position child to Open Airway Clear Airway B Breathing Oxygen Therapy C Circulation Hydration
55 Case Scenario 2 30 minutes later: Vitals H.R. = 186 R.R. = 66 WOB = substernal and intercostal retractions B.S. = diminished SpO2 on 10 liter O2 mask = 90% X-ray = hyperinflation, right lower lobe atelectasis Cap gas results: ph = 7.26, CO2 = 75, O2 = 53

56 Case Scenario 2 Chest X-ray



57 What is plan B? L aryngeal M ask A irway

58 Needle Cricothyrotomy A quick fix, buys some time Used when you can t intubate or ventilate

59 King Airway Backup Airway Inserted Blind.
60 Case Scenario 3 7 year old child is brought to the Emergency Department with a chief complaint of SOB. Classify
61 Case Scenario 3 Vitals H.R. = 132 R.R. = 28 WOB = substernal and intercostal retractions B.S. = decreased SpO2 on Room Air = 87% Diagnosis
62 Asthma Statistics 23 million Americans currently have Asthma. Number of children who currently have Asthma: 7.0 million. Students with Asthma miss nearly 13 million school days every year due to illness.
63 Scenario 3 Treatment A Airway Management Oxygen Sitting Position, Position of Comfort B Breathing Albuterol 0.5 ml and more bronchodilators Steroids Encourage Coughing C Circulation Hydration

64 Special Populations Tracheotomies Stay CALM!!

65 Special Populations Cystic Fibrosis SUCTION, Position of Comfort, Cough SUCTION SUCTION
66 It is all about the ABC s Airway Breathing Circulation Recognize the signs of respiratory distress and use your ABC s.

67 Questions?

68 Thank You!!!
The Pediatric Patient. Morgen Bernius, MD NCEMS Conference February 24, 2007
 The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
Common Pediatric Respiratory Illness and Emergencies
 Common Pediatric Respiratory Illness and Emergencies Rob Cloutier, MD Assistant Professor Emergency Medicine & Pediatrics Oregon Health & Science University Overview Review key differences between pediatric
Common Pediatric Respiratory Illness and Emergencies Rob Cloutier, MD Assistant Professor Emergency Medicine & Pediatrics Oregon Health & Science University Overview Review key differences between pediatric
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Your Virtual Health Partner. Respiratory Distress in the Pediatric Patient: Think quick and calmly
 Your Virtual Health Partner Respiratory Distress in the Pediatric Patient: Think quick and calmly Are kids really so different? You be the judge Children are not small adults Children are still growing
Your Virtual Health Partner Respiratory Distress in the Pediatric Patient: Think quick and calmly Are kids really so different? You be the judge Children are not small adults Children are still growing
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Transporting Children With Serious Respiratory Illness: A Presentation For Non-Specialty Teams
 Transporting Children With Serious Respiratory Illness: A Presentation For Non-Specialty Teams Laurie Gehrke, R.N., BSN, CPEN, CEN, CMTE Pediatric Transport Team Blank Children s Hospital Des Moines, Iowa
Transporting Children With Serious Respiratory Illness: A Presentation For Non-Specialty Teams Laurie Gehrke, R.N., BSN, CPEN, CEN, CMTE Pediatric Transport Team Blank Children s Hospital Des Moines, Iowa
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
PEDIATRIC RESPIRATORY ILLNESS MADE SIMPLE
 Copyright 2012 Joel Berezow, MD and The Pediatrics for Emergency Physicians Network All rights reserved. Duplication in whole or in part, or electronic transmission in any form, is prohibited THE PEDIATRICS
Copyright 2012 Joel Berezow, MD and The Pediatrics for Emergency Physicians Network All rights reserved. Duplication in whole or in part, or electronic transmission in any form, is prohibited THE PEDIATRICS
Airway and Ventilation. Emergency Medical Response
 Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Anatomy Review. Anatomy Review. Respiratory Emergencies CHAPTER 16
 CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review 1 Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons
CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review 1 Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons
Respiratory Emergencies
 CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons for
CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons for
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
Respiratory Emergencies. Chapter 11
 Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Respiratory Distress/Failure - General
 Respiratory Distress/Failure - General Criteria: Dyspnea WITHOUT a clear etiology O 2 V/S and SpO 2 (with and without Oxygen therapy if possible) Blood glucose analysis: if less than 80 mg/dl, refer to
Respiratory Distress/Failure - General Criteria: Dyspnea WITHOUT a clear etiology O 2 V/S and SpO 2 (with and without Oxygen therapy if possible) Blood glucose analysis: if less than 80 mg/dl, refer to
Pediatric Bronchiolitis. Janie Robles, PharmD, AE-C Assistant Professor of Pharmacy Practice Pediatrics School of Pharmacy TTUHSC Lubbock, Texas
 This PowerPoint file is a supplement to the video presentation. Some of the educational content of this program is not available solely through the PowerPoint file. Participants should use all materials
This PowerPoint file is a supplement to the video presentation. Some of the educational content of this program is not available solely through the PowerPoint file. Participants should use all materials
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Paediatric Resuscitation. EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009
 Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Firefighter Pre-Hospital Care Program Recruit Presentation. Respiratory Emergencies
 Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
BRONCHIOLITIS PEDIATRIC
 DEFINITION Bronchiolitis is typically defined as the first episode of wheezing in infants < 24 months of age. It is a viral illness of the lower respiratory tract that causes tachypnea, bronchospasm, and
DEFINITION Bronchiolitis is typically defined as the first episode of wheezing in infants < 24 months of age. It is a viral illness of the lower respiratory tract that causes tachypnea, bronchospasm, and
Respiratory Emergencies. Lesson Goal. Lesson Objectives 9/10/2012
 Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
Discuss the benefits for developing an outpatient bronchiolitis clinic.
 Diana L Mark, RRT Pediatric Clinical Specialist Respiratory Care Wesley Medical Center Discuss the benefits for developing an outpatient bronchiolitis clinic. 1 Definition Inflammation of the bronchioles
Diana L Mark, RRT Pediatric Clinical Specialist Respiratory Care Wesley Medical Center Discuss the benefits for developing an outpatient bronchiolitis clinic. 1 Definition Inflammation of the bronchioles
Chapter 16. Objectives. Objectives. Respiratory Emergencies
 Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
AIRWAY & HEART ANOTOMY
 Objectives I CAN T BREATH Respiratory Emergencies Review of anatomical structures related to heart & lungs Differentiate differences between adult and pediatric airways Identify the need for airway assistance
Objectives I CAN T BREATH Respiratory Emergencies Review of anatomical structures related to heart & lungs Differentiate differences between adult and pediatric airways Identify the need for airway assistance
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
BRONCHIOLITIS. See also the PSNZ guideline - Wheeze & Chest Infections in infants under 1 year (www.paediatrics.org.nz)
") Definition What is Bronchiolitis? Assessment Management Flow Chart Admission Guidelines Investigations Management Use of Bronchodilators Other treatments Discharge Planning Bronchiolitis & Asthma References
Definition What is Bronchiolitis? Assessment Management Flow Chart Admission Guidelines Investigations Management Use of Bronchodilators Other treatments Discharge Planning Bronchiolitis & Asthma References
PALS Pulseless Arrest Algorithm.
 PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
Simulation 01: Two Year-Old Child in Respiratory Distress (Croup)
") Simulation 01: Two Year-Old Child in Respiratory Distress (Croup) Flow Chart Opening Scenario 2 year-old child in respiratory distress - assess Section 1 Type: IG audible stridor with insp + exp wheezing;
Simulation 01: Two Year-Old Child in Respiratory Distress (Croup) Flow Chart Opening Scenario 2 year-old child in respiratory distress - assess Section 1 Type: IG audible stridor with insp + exp wheezing;
PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department
 PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department Overview Roles of the EMS in Pediatric Care Growth and Development Assessment Airway Adjuncts and Intravenous Access
PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department Overview Roles of the EMS in Pediatric Care Growth and Development Assessment Airway Adjuncts and Intravenous Access
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Protocol Update 2019
 Protocol Update 2019 There have been several questions revolving around protocol updates and how they are to be conducted. As many of you are aware there is a protocol submission process in the appendix
Protocol Update 2019 There have been several questions revolving around protocol updates and how they are to be conducted. As many of you are aware there is a protocol submission process in the appendix
Airway Management. Teeradej Kuptanon, MD
 Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Pulmonary
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
Chapter 13. Respiratory Emergencies
 Chapter 13 Respiratory Emergencies Introduction Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine. Even for physician in
Chapter 13 Respiratory Emergencies Introduction Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine. Even for physician in
Pediatric Respiratory Distress. Dr. Karen Forward Dr. Mike Peddle
 Pediatric Respiratory Distress Dr. Karen Forward Dr. Mike Peddle Objectives Discuss epidemiology & causes of respiratory distress in pediatric patients Identify differences between the pediatric and adult
Pediatric Respiratory Distress Dr. Karen Forward Dr. Mike Peddle Objectives Discuss epidemiology & causes of respiratory distress in pediatric patients Identify differences between the pediatric and adult
Chapter 19 - Respiratory_Emergencies
 Introduction to Emergency Medical Care 1 OBJECTIVES 19.1 Define key terms introduced in this chapter. Slides 14 15, 41, 54 19.2 Describe the anatomy and physiology of respiration. Slides 13 15 19.3 Differentiate
Introduction to Emergency Medical Care 1 OBJECTIVES 19.1 Define key terms introduced in this chapter. Slides 14 15, 41, 54 19.2 Describe the anatomy and physiology of respiration. Slides 13 15 19.3 Differentiate
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Pediatric Assessment Triangle
 Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
SUMPh N. Testemitanu Radiology and Medical imaging department PEDIATRIC IMAGING. M. Crivceanschii, assistant professor
 SUMPh N. Testemitanu Radiology and Medical imaging department PEDIATRIC IMAGING M. Crivceanschii, assistant professor GOALS AND OBJECTIVES to be aware of the role of modern diagnostic imaging modalities
SUMPh N. Testemitanu Radiology and Medical imaging department PEDIATRIC IMAGING M. Crivceanschii, assistant professor GOALS AND OBJECTIVES to be aware of the role of modern diagnostic imaging modalities
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Pediatric Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Pediatric Revised: 11/2013 (10 questions from this outline in the blue section) Emergency Medical
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Pediatric Revised: 11/2013 (10 questions from this outline in the blue section) Emergency Medical
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis. Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine
 Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Objectives. Objectives 10/12/2011. Case Study: Initial Assessment of the Critically Ill Child. By Rebecca Saul, MSN, CRNP
 Case Study: Initial Assessment of the Critically Ill Child By Rebecca Saul, MSN, CRNP Objectives Define the anatomic variations between children and adults Recognize and implement exam techniques useful
Case Study: Initial Assessment of the Critically Ill Child By Rebecca Saul, MSN, CRNP Objectives Define the anatomic variations between children and adults Recognize and implement exam techniques useful
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
CHILDREN S SERVICES. Patient information Leaflet BRONCHIOLITIS
 CHILDREN S SERVICES Patient information Leaflet BRONCHIOLITIS Sept 2014 INTRODUCTION This leaflet aims to help you understand bronchiolitis, how to make your child comfortable and when to contact for emergency
CHILDREN S SERVICES Patient information Leaflet BRONCHIOLITIS Sept 2014 INTRODUCTION This leaflet aims to help you understand bronchiolitis, how to make your child comfortable and when to contact for emergency
Review. 1. How does a child s anatomy differ from an adult s anatomy?
 Chapter 32 Review Review 1. How does a child s anatomy differ from an adult s anatomy? A. The child s trachea is more rigid B. The tongue is proportionately smaller C. The epiglottis is less floppy in
Chapter 32 Review Review 1. How does a child s anatomy differ from an adult s anatomy? A. The child s trachea is more rigid B. The tongue is proportionately smaller C. The epiglottis is less floppy in
Pediatric Emergencies. Lesson Goal. Lesson Objectives 9/10/2012
 Pediatric Emergencies Lesson Goal Explain special characteristics of infants and children to become both comfortable & efficient in treating pediatric emergencies Lesson Objectives Identify physical &
Pediatric Emergencies Lesson Goal Explain special characteristics of infants and children to become both comfortable & efficient in treating pediatric emergencies Lesson Objectives Identify physical &
Guidelines and Best Practices for High Flow Nasal Cannula (HFNC) Pediatric Pocket Guide
 Pediatric Pocket Guide") Guidelines Best Practices for High Flow Nasal Cannula (HFNC) Pediatric Pocket Guide Patient Selection Diagnoses Patient presents with one or more of the following signs or symptoms of respiratory distress:
Guidelines Best Practices for High Flow Nasal Cannula (HFNC) Pediatric Pocket Guide Patient Selection Diagnoses Patient presents with one or more of the following signs or symptoms of respiratory distress:
Management of Bronchiolitis in Infants
 Co-issued by Paediatric Medicine and the Division of Paediatric Emergency Medicine. 1.0 Introduction Bronchiolitis is an acute inflammatory disease of the lower respiratory tract, resulting from obstruction
Co-issued by Paediatric Medicine and the Division of Paediatric Emergency Medicine. 1.0 Introduction Bronchiolitis is an acute inflammatory disease of the lower respiratory tract, resulting from obstruction
Condensed version.
 I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
Simulation 1: Two Year-Old Child in Respiratory Distress
 Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
BPD. Neonatal/Pediatric Cardiopulmonary Care. Disease. Bronchopulmonary Dysplasia. Baby Jane
 1 Neonatal/Pediatric Cardiopulmonary Care Disease 2 Bronchopulmonary Dysplasia 3 is a 33-day-old prematurely born girl who weighs 1420 g. At birth, her estimated gestational age was 28 weeks. Her initial
1 Neonatal/Pediatric Cardiopulmonary Care Disease 2 Bronchopulmonary Dysplasia 3 is a 33-day-old prematurely born girl who weighs 1420 g. At birth, her estimated gestational age was 28 weeks. Her initial
Bayfield-Ashland Counties EMS Council Pediatric Protocol PP-001 PREHOSPITAL CARE GUIDELINE
 INTRODUCTION: Pediatric emergencies may present a daunting challenge to prehospital care providers for a variety of reasons including: 1. The historical scarceness of primary training materials about the
INTRODUCTION: Pediatric emergencies may present a daunting challenge to prehospital care providers for a variety of reasons including: 1. The historical scarceness of primary training materials about the
Dr. (Kate) Katherine Miller GUELPH ON 121 RESPIRATORY DISTRESS IN THE NEWBORN
 Katherine Miller GUELPH ON 121 RESPIRATORY DISTRESS IN THE NEWBORN") Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. (Kate) Katherine Miller GUELPH ON 121 RESPIRATORY DISTRESS
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. (Kate) Katherine Miller GUELPH ON 121 RESPIRATORY DISTRESS
Training. Continuous Positive Airway Pressure (CPAP)
") Training The training module will follow the national standard curriculum as it relates to the application and use of CPAP. The proposed curriculum will closely resemble the following algorithm utilizing
Training The training module will follow the national standard curriculum as it relates to the application and use of CPAP. The proposed curriculum will closely resemble the following algorithm utilizing
Management of Respiratory Issues in the School Setting. Pediatric Indicators of High Risk 8/7/2015. Facts about Pediatric Respiratory Failure
 Management of Respiratory Issues in the School Setting Toni B. Vento, MS, RN, NCSN Supervisor of Health Services Medford Public Schools Pediatric Indicators of High Risk Anatomic features of the immature
Management of Respiratory Issues in the School Setting Toni B. Vento, MS, RN, NCSN Supervisor of Health Services Medford Public Schools Pediatric Indicators of High Risk Anatomic features of the immature
Appendix (i) The ABCDE approach to the sick patient
 The ABCDE approach to the sick patient") Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
PEDIATRIC RESPIRATORY SYNCYTIAL VIRUS (RSV) ALL THAT WHEEZES IS NOT ASTHMA
 ALL THAT WHEEZES IS NOT ASTHMA") PEDIATRIC RESPIRATORY SYNCYTIAL VIRUS (RSV) ALL THAT WHEEZES IS NOT ASTHMA Season changes here in Ohio can send the census numbers in our local P.I.C.U. s, N.I.C.U. s and Emergency Rooms through the roof.
PEDIATRIC RESPIRATORY SYNCYTIAL VIRUS (RSV) ALL THAT WHEEZES IS NOT ASTHMA Season changes here in Ohio can send the census numbers in our local P.I.C.U. s, N.I.C.U. s and Emergency Rooms through the roof.
STRIDOR. Respiratory system. Lecture
 STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
PROFESSIONAL NURSING SERVICES, INC York Road Cockeysville, MD (410)
") PROFESSIONAL NURSING SERVICES, INC. 10615 York Road Cockeysville, MD 21030 (410) 683-9770 www.pnsnursing.com Aspiration and Airway Precautions Guideline Purpose: All medical personnel will assess for signs
PROFESSIONAL NURSING SERVICES, INC. 10615 York Road Cockeysville, MD 21030 (410) 683-9770 www.pnsnursing.com Aspiration and Airway Precautions Guideline Purpose: All medical personnel will assess for signs
Advanced Airway Management
 CHAPTER 37 Advanced Airway Management Airway Anatomy and Physiology Review Respiratory System: The Airway Respiratory System (Supine) Physiology: Factors of Adequate Breathing Functioning brainstem Open
CHAPTER 37 Advanced Airway Management Airway Anatomy and Physiology Review Respiratory System: The Airway Respiratory System (Supine) Physiology: Factors of Adequate Breathing Functioning brainstem Open
Overview. The Respiratory System. Chapter 18. Respiratory Emergencies 9/11/2012
 Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Airway and Breathing
 Airway and Breathing ETAT Module 2 Adapted from Emergency Triage Assessment and Treatment (ETAT): Manual for Participants, World Health Organization, 2005 Learning Objectives Accurately determine whether
Airway and Breathing ETAT Module 2 Adapted from Emergency Triage Assessment and Treatment (ETAT): Manual for Participants, World Health Organization, 2005 Learning Objectives Accurately determine whether
yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management
 yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management Overview: Managing a patient s airway may be necessitated due to upper or lower airway obstruction, inadequate
yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management Overview: Managing a patient s airway may be necessitated due to upper or lower airway obstruction, inadequate
Chapter 10. Objectives. Objectives 01/09/2013. Airway Management, Artificial Ventilation, and Oxygenation
 Chapter 10 Airway Management, Artificial Ventilation, and Oxygenation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Chapter 10 Airway Management, Artificial Ventilation, and Oxygenation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Phases of Respiration. Chapter 18: The Respiratory System. Structures of the Respiratory System. Structures of the Respiratory System
 Phases of Respiration Chapter 18: The Respiratory System Respiration Process of obtaining oxygen from environment and delivering it to cells Phases of Respiration 1. Pulmonary ventilation between air and
Phases of Respiration Chapter 18: The Respiratory System Respiration Process of obtaining oxygen from environment and delivering it to cells Phases of Respiration 1. Pulmonary ventilation between air and
INTUBATION/RSI. PURPOSE: A. To facilitate secure, definitive control of the airway by endotracheal intubation in an expeditious and safe manner
 Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Pediatric Airway and Respiratory Emergencies. Objectives 30/01/2009
 Objectives Pediatric Airway and Respiratory Emergencies Patrick Mahar, MD Review the anatomical differences between adult and pediatric airways Recognize different causes of respiratory comprise in pediatric
Objectives Pediatric Airway and Respiratory Emergencies Patrick Mahar, MD Review the anatomical differences between adult and pediatric airways Recognize different causes of respiratory comprise in pediatric
A Trust Guideline for the Management of. Bronchiolitis in Infants and Children under the age of 24 months
 A Clinical Guideline recommended Children s Assessment Unit (CAU), Buxton Ward, For use in: Children s Day Ward, Jenny Lind Out-patients Department, Accident and Emergency Department By: Medical and Nursing
A Clinical Guideline recommended Children s Assessment Unit (CAU), Buxton Ward, For use in: Children s Day Ward, Jenny Lind Out-patients Department, Accident and Emergency Department By: Medical and Nursing
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Basic Airway Management
 Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
ENDOTRACHEAL INTUBATION POLICY
 POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
Airway Management. DFMRT Casualty Care Examination Course. Revision notes for. January Les Gordon
 Airway Management Revision notes for DFMRT Casualty Care Examination Course January 2013 Les Gordon Indicating special information in Revision Notes presentations New information since Casualty Care in
Airway Management Revision notes for DFMRT Casualty Care Examination Course January 2013 Les Gordon Indicating special information in Revision Notes presentations New information since Casualty Care in
February EMS Training: Pulmonary Emergencies. Used with permission of Silver Cross EMS System
 February EMS Training: Pulmonary Emergencies Used with permission of Silver Cross EMS System Goals Review airway anatomy and physiology for adults and pediatrics Review issues and techniques in airway
February EMS Training: Pulmonary Emergencies Used with permission of Silver Cross EMS System Goals Review airway anatomy and physiology for adults and pediatrics Review issues and techniques in airway
Respiratory System Anatomy Respiratory system: all the structures that contribute to
 1 2 3 4 5 6 7 8 Chapter 15 Respiratory Emergencies Respiratory Distress Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine.
1 2 3 4 5 6 7 8 Chapter 15 Respiratory Emergencies Respiratory Distress Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine.
Airway Management Adult
 Airway Management Adult Goals: Provide effective oxygenation and ventilation; recognize and alleviate respiratory distress or failure; provide necessary interventions quickly and safely to patients who
Airway Management Adult Goals: Provide effective oxygenation and ventilation; recognize and alleviate respiratory distress or failure; provide necessary interventions quickly and safely to patients who
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway.
 PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
TOWN OF FAIRFIELD HEALTH DEPARTMENT PUBLIC HEALTH NURSING
 TOWN OF FAIRFIELD HEALTH DEPARTMENT PUBLIC HEALTH NURSING PROGRAM: School Health APPROVED BY: Board of Health POLICY: Nebulizer Therapy DATE: 5-10-93 PROCEDURE: a) Nebulizer Therapy With Non-oxygenated
TOWN OF FAIRFIELD HEALTH DEPARTMENT PUBLIC HEALTH NURSING PROGRAM: School Health APPROVED BY: Board of Health POLICY: Nebulizer Therapy DATE: 5-10-93 PROCEDURE: a) Nebulizer Therapy With Non-oxygenated
Respiratory Failure in the Pediatric Patient
 Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize