Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research
|
|
|
- Benedict Miles
- 5 years ago
- Views:
Transcription
1 Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research




2 Concord Hospital




3 Woolcock Institute of Medical Research

4 Joe has asthma What the I get Short of breath Joe has COPD
5 Problems in the classification of airways disease New tools have defined different inflammatory profiles, some are common to asthma and COPD Disparity in clinical, physiologic, and pathologic markers within the spectrum of asthma, suggesting heterogeneity Spectrum of airways disease and a spectrum within types of airways disease Asthma and COPD are multidimensional diseases with generalised systemic aspects (COPD) or focal multisystem aspects (asthma) Marked heterogeneity in physiology, pathology, clinical presentation. Hence 1. Are the current diagnostic labels too simplistic? 2. Are different approaches to treatment required?
6 Why is it important to consider obstructive airways diseases beyond asthma and COPD? Patients with overlapping asthma and COPD are frequently excluded from clinical trials of treatments for either condition An accurate diagnosis is challenging in day to day practice, especially in older patients There is variability in bronchodilator responsiveness day to day and class to class in COPD, making not fully reversible difficult to define Identifying overlap or mixed disease opens up a more realistic spectrum of management issues and expectations, especially in people with irreversible AO people with AO and partial reversibility
7 The overlap syndrome of asthma and COPD Gibson & Simpson Thorax : Asthma = Episodic respiratory symptoms and variable airflow obstruction occurring spontaneously, with treatment or after provocation COPD = Incompletely reversible airflow obstruction Asthma and COPD are not mutually exclusive Overlap syndrome of Asthma and COPD = symptoms of increased variability of airflow and incompletely reversible airflow obstruction When a patient exhibits features of more than one condition, then they have an overlap syndrome
8 The overlap of airways diseases The ATS 1995 COPD guidelines defined asthma, chronic bronchitis, emphysema, COPD and airflow obstruction Identified 11 distinct syndromes Overlap between two or more conditions made up 6 of these 11 syndromes
9 Quantitative assessment of airway remodelling using high-resolution CT Nakano, Muller, King; Chest 2002 The relationship between emphysema (LAA, low attenuation areas) and airway wall thickness (WA%) in 94 COPD subjects and 20 smokers (quantitative CT scan analyses). The pattern (ie, phenotype) represented in the right lower quadrant of the graph is similar to the pattern found in patients with severe asthma that is incompletely reversible
10 Percentage of people with overlap syndrome related to increasing age Soriano JB et al Chest 2003;124:474 81

11 Airway Remodelling : what is affected? James A, Wenzel S. Clinical relevance of airway remodelling. Eur Respir J 2007;30:134
12 Cohort study of asthma followed to adulthood Sears et al. NEJM 2003;349:1414
13 Busselton Height adjusted FEV1 decline male female Subjects who have asthma and smoke have fastest rate of decline
14 Clinical phenotypes of asthma Haldar et al AJRCCM 2008; 178. pp Undertook cluster analysis in asthma subjects in primary care (n = 184) with predominantly mild to moderate disease Compared to a refractory asthma population managed in secondary care (n = 187) Compared differences in asthma outcomes - exacerbation frequency & change in ICS at 12m In a third population of 68 subjects with predominantly refractory asthma, RCT compared a strategy of minimizing eosinophilic inflammation (inflammation-guided strategy) with standard care Two clusters were common to both asthma populations early-onset atopic and obese, noneosinophilic Two clusters characterized by marked discordance between symptom expression and eosinophilic airway inflammation were specific to refractory asthma early-onset, symptom predominant late-onset, inflammation predominant
15 Clinical phenotypes of asthma Haldar et al AJRCCM 2008; 178. pp Inflammation-guided management was superior for both discordant subgroups a reduction in exacerbation frequency in the inflammationpredominant cluster (3.53 vs exac/pt/yr, P < 0.002) and A dose reduction of ICS in the symptom-predominant cluster (mean difference, 1829 mcg BDP eq/day (95% CI 307 3,349 mcg); P < 0.02 a symptom-led approach would be effective for concordant mild to moderate asthma in primary care for patients with early-onset atopic asthma = benign discordance between these domains is a prevalent characteristic of refractory asthma

16 Clinical phenotypes of asthma Haldar et al AJRCCM 2008; 178. pp
17 Distinct clinical phenotypes of airways disease defined by cluster analysis Weatherall et al Eur Respir J 2009; 34: A random population sample of yr-old adults underwent detailed investigation, including a clinical questionnaire, pulmonary function tests, nitric oxide measurements, blood tests and CT Cluster analysis was performed on the subgroup with a complete dataset (n=175) and current respiratory symptoms or obstructive spirometry Five clusters were identified Cluster 1: severe and markedly variable airflow obstruction with features of atopic asthma, chronic bronchitis and emphysema = an overlap syndrome Cluster 2: features of emphysema alone Cluster 3: atopic asthma with eosinophilic airways inflammation Cluster 4: mild airflow obstruction without other dominant phenotypic features Cluster 5: chronic bronchitis in non-smokers Overlap cluster had most severe disease : worse airflow obstruction, requirement for hospital admission, prescribed treatment and quality of life

18 Asthma and COPD The old approach to diagnosis and management
19 GOLD WORKSHOP REPORT 2010 Diagnosis of COPD A diagnosis of COPD should be considered in any patient who has chronic cough, sputum production or dyspnea, and/or a history of exposure to risk factors for the disease. The diagnosis should be confirmed by spirometry The presence of a post-bd FEV1/FVC< 0.7 and an FEV1<80% predicted confirms the presence of airflow limitation that is not fully reversible
20 Asthma diagnosis = symptoms + variable obstruction To establish the diagnosis of asthma, the clinician must determine that: Episodic symptoms of airflow obstruction are present. Airflow obstruction is at least partially reversible Working definition of asthma a disorder of the airways in which they are prone to narrowing too much and too easily in response to a wide variety of provoking stimuli, causing variable wheeze, chest tightness, cough and breathlessness.

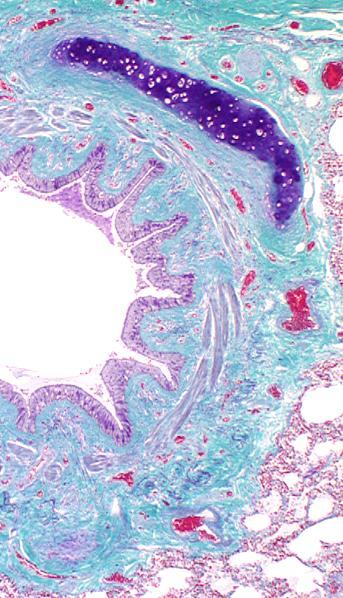
21 Asthmatic airway Non-asthmatic airway
22 Antecedents to Obstruction Several routes one outcome
23 FEV 1 % normal at age 20 Theoretical rates of lung function growth and decline Normal growth, peak and rate of decline Normal growth & peak, accelerated decline Normal growth, premature decline, normal rate Sub-maximal growth & peak, normal rate decline Age in years
24 Risk factors for sub maximal peak Intra-uterine ETS Early life RTI Early life ETS Early life biomass fuel smoke exposure Low birth weight Early life pneumonia malnutrition Socio-economic factors Under-treated asthma
25 Risk factors for accelerated rate of FEV1 decline Smoking Female AHR Age Chronic mucus hypersecretion Reversibility Atopy
26 Why (I believe) the distinction matters Predicting response to treatment Pulmonary rehab Preparation for future events Prognosis Public health initiatives prevention
27 Predicting response to treatment
28 Morning PEF, L/min FEV 1, % predicted b 2 -agonist use Nights/week 5 4 b 2 -agonist use 4 3 Night waking Morning PEF Clinic FEV
29 Rate ratio for death from asthma Low dose inhaled corticosteroids and the prevention of death from asthma Suissa, Ernst, Benayoun et al. NEJM 2000:343: % ICS canisters were BDP 50 mcg/puff No. canisters of ICS per year





30 Post-bronchodilator FEV1 Effect of fluticasone on FEV1 over 3 years * * * p<0.001 * * FP 1mg * Placebo Time (months) 32% reduction in absolute decline in FEV 1 Disease modifying effect Effect maintained over 3 years ISOLDE BMJ May 2000
31 PEF (L/min) Weeks from commencement of budesonide Morning pre - BD PEF Evening pre -BD PEF Post-BD PEF
32 Survival probability Exacerbations and Mortality Soler-Cataluna JJ, et al. Thorax 2005; 60: A p< B p=0.069 C p< n= Time (months) Prospective study in 304 male patients with stable COPD, recruited 1998 and followed for 5 years Group A: no exacerbations Group B: 1 2 exacerbations Group C: 3 exacerbations

 DEFINITION OF AN EXACERBATION")

33 40% 30% 20% 10% 0% ISOLDE results : COPD exacerbations Effect Greatest in Those With Lowest Lung Function (FEV 1 ) 35% 24% < FEV 1 (litres) DEFINITION OF AN EXACERBATION worsening of respiratory symptoms that required treatment with antibiotics, OCS or both; no objective symptom criteria Burge PS et al BMJ May 2000


34
35 ICS and risk of pneumonia Ernst et al. AJRCCM 2007;176:162
36 Rate per 10,000 Rate of patterns of comorbidity in newly diagnosed COPD in primary care Cataracts (0.90) Skin bruises (1.00) Glaucoma (1.29) Angina (1.67) Fractures (1.58) Respiratory infection (2.24) Myocardial infarction (1.75) Relative risk in COPD vs non-copd Osteoporosis (3.14) Pneumonia (16.00) Soriano et al 2005 Rate of medical events in UK General Practice Research Database 1998
37 Mortality in COPD : Role of co-morbidities Sin D et al ERJ 2006;28:1245 Estimated rate of 30d mortality post hospital D/C in patients with and without COPD National Hospital Discharge Survey, UK
38 Preparation for Future Events
39 Process and patterns of care in chronic disease Holman & Lorig BMJ 2000;320:526-7 Ambulatory care threshold Disease severity Medication Diagnosis Self management strategies Primary care threshold Self care threshold Effective self Mx controls progression and avoids crossing thresholds Progression of disease over time

40 Action Plans

41 ALF COPD Action Plan
42 Prognosis
43 Prognosis after ICU admission Seneff et al JAMA 1995/274:1852-7: Hospital & I year survival of patients admitted to ICU with acute exacerbations of COPD 362 admissions to ICU for COPD exacerbations Overall mortality 24% (12 months) Median survival 224 days Non-respiratory organ dysfunction was the major predictor of hospital mortality & 180 day mortality 167 patients aged > 65, mortality: 30% at D/C 41% at 90 days, 47% at 180 days, 59% at 1 year

44 A predictive model of hospitalisation and death from COPD Schembri et al Resp Med 2009;103:1461 Prospective observational study 3343 patients with FEV1 < 80% pred and FEV1/FVC < 70% from a clinical network in Tayside, Scotland Data collected during annual visits - spirometry, smoking history, MRC dyspnoea scale, BMI Main outcome measures were hospitalisations and death secondary to COPD Increasing age, low BMI, worsening MRC dyspnoea score, decreased FEV1, and prior respiratory or cardiovascular admission hospitalisation were predictors of poor outcome Influenza vaccination was protective
45
46 Prognostic issues for COPD patients need to be discussed Role of bacterial infection in exacerbations Planning for increased dependency Anticipate and manage co-morbidity Anticipating hospital admissions Review for LTOT Discuss choice for ventilatory support End of life decisions / Living will
47 Summary COPD and Asthma each have a spectrum of causes, manifestations and pathophysiologic stages Common clinical features in these diseases result in some indistinguishable features and overlap syndromes increase with age However, the natural history of each is different and prognosis is affected by pathology Asthma is predominantly an airways disease, while COPD is a mixed airways-parenchymal disease Patients are best served by Acknowledging the importance of symptoms and addressing these Respecting the differing pathologies and outlooks and tailoring treatment accordingly
48
Life-long asthma and its relationship to COPD. Stephen T Holgate School of Medicine University of Southampton
 Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
TORCH: Salmeterol and Fluticasone Propionate and Survival in COPD
 TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Bronchial Provocation Results: What Does It Mean?
 Bronchial Provocation Results: What Does It Mean? Greg King 1 Department of Respiratory Medicine, Royal North Shore Hospital, St Leonards 2065 2 Woolcock Institute of Medical Research and Sydney Medical
Bronchial Provocation Results: What Does It Mean? Greg King 1 Department of Respiratory Medicine, Royal North Shore Hospital, St Leonards 2065 2 Woolcock Institute of Medical Research and Sydney Medical
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Asma, BPCO ed Esercizio Fisico Ferrara, 6 e 7 Novembre Overlap asma BPCO. Dr. Marco Contoli
 Asma, BPCO ed Esercizio Fisico Ferrara, 6 e 7 Novembre 2015 Overlap asma BPCO Dr. Marco Contoli Sezione di Medicina Interna e Cardio-Respiratoria Dipartimento di Scienze Mediche Università di Ferrara (Sept.
Asma, BPCO ed Esercizio Fisico Ferrara, 6 e 7 Novembre 2015 Overlap asma BPCO Dr. Marco Contoli Sezione di Medicina Interna e Cardio-Respiratoria Dipartimento di Scienze Mediche Università di Ferrara (Sept.
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น
 รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
COPD or not COPD, that is the question.
 COPD or not COPD, that is the question. Asthma-COPD Overlap Syndrome: ACOS Do we really need this? Michelle Harkins Disclosure Slide Slide help - William Busse, MD Organizational Interests ATS, ACCP, ACP
COPD or not COPD, that is the question. Asthma-COPD Overlap Syndrome: ACOS Do we really need this? Michelle Harkins Disclosure Slide Slide help - William Busse, MD Organizational Interests ATS, ACCP, ACP
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university
 What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
This is a cross-sectional analysis of the National Health and Nutrition Examination
 SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
COPD: early detection, screening and case-finding: what is the evidence? Prof. Jan-Willem Lammers, Md PhD Department of Respiratory Diseases
 COPD: early detection, screening and case-finding: what is the evidence? Prof. Jan-Willem Lammers, Md PhD Department of Respiratory Diseases «If you test one smoker with cough every day You will diagnose
COPD: early detection, screening and case-finding: what is the evidence? Prof. Jan-Willem Lammers, Md PhD Department of Respiratory Diseases «If you test one smoker with cough every day You will diagnose
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013
 COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013 None Disclosures Definitions Asthma Asthma is a chronic inflammatory
COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013 None Disclosures Definitions Asthma Asthma is a chronic inflammatory
Potential risks of ICS use
 Potential risks of ICS use Randomised controlled trial Observational study Systematic review Pneumonia Tuberculosis Bone fracture Skin thinning/easy bruising Cataract Diabetes No effect on fracture risk
Potential risks of ICS use Randomised controlled trial Observational study Systematic review Pneumonia Tuberculosis Bone fracture Skin thinning/easy bruising Cataract Diabetes No effect on fracture risk
An Update in COPD John Hurst PhD FRCP
 An Update in COPD John Hurst PhD FRCP Reader in Respiratory Medicine / Honorary Consultant University College London / Royal Free London NHS Foundation Trust j.hurst@ucl.ac.uk What s new in COPD papers
An Update in COPD John Hurst PhD FRCP Reader in Respiratory Medicine / Honorary Consultant University College London / Royal Free London NHS Foundation Trust j.hurst@ucl.ac.uk What s new in COPD papers
Changing Landscapes in COPD New Zealand Respiratory Conference
 Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Turning Science into Real Life Roflumilast in Clinical Practice. Roland Buhl Pulmonary Department Mainz University Hospital
 Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
COPD and Asthma: Similarities and differences Prof. Peter Barnes
 and Asthma: Similarities and Differences and Asthma: 1 Imperial College Peter Barnes FRS, FMedSci, National Heart & Lung Institute Imperial College, London, UK p.j.barnes@imperial.ac.uk Royal Brompton
and Asthma: Similarities and Differences and Asthma: 1 Imperial College Peter Barnes FRS, FMedSci, National Heart & Lung Institute Imperial College, London, UK p.j.barnes@imperial.ac.uk Royal Brompton
Known Allergies: Shellfish. Symptoms: abdominal pain, nausea, diarrhea, or vomiting. congestion, trouble breathing, or wheezing.
 CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
American Thoracic Society (ATS) Perspective
 Perspective") National Surveillance System for Chronic Lung Disease (CLD): American Thoracic Society (ATS) Perspective Gerard J. Criner, M.D. Chronic Obstructive Pulmonary Disease (COPD) l Definition: Group of chronic
National Surveillance System for Chronic Lung Disease (CLD): American Thoracic Society (ATS) Perspective Gerard J. Criner, M.D. Chronic Obstructive Pulmonary Disease (COPD) l Definition: Group of chronic
COPD UPDATE ıdr Shitrit David ıhead of the Pulmonary Department ımeir Medical Center
 COPD UPDATE 2012 ıdr Shitrit David ıhead of the Pulmonary Department ımeir Medical Center Definition of COPD COPD is a preventable and treatable disease with some significant extra pulmonary effects that
COPD UPDATE 2012 ıdr Shitrit David ıhead of the Pulmonary Department ımeir Medical Center Definition of COPD COPD is a preventable and treatable disease with some significant extra pulmonary effects that
COPD GOLD Guidelines & Barnet inhaler choices. Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust
 COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
Referring for specialist respiratory input. Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL
 Referring for specialist respiratory input Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL Respiratory Specialist- who? GPSI Community Team Secondary Care Respiratory physician and
Referring for specialist respiratory input Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL Respiratory Specialist- who? GPSI Community Team Secondary Care Respiratory physician and
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Prof Neil Barnes. Respiratory and General Medicine London Chest Hospital and The Royal London Hospital
 Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD)
 Instructions for the Pulmonary Diagnosis Form (PLD)") Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Outline FEF Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications?
 Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
#1 cause of school absenteeism in children 13 million missed days annually
 Asthma Update 2013 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Pulmonary & Critical Care Medicine The Ohio State University Wexner Medical Center Disclosures None 2 Objectives Review burden
Asthma Update 2013 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Pulmonary & Critical Care Medicine The Ohio State University Wexner Medical Center Disclosures None 2 Objectives Review burden
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC
 KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC") Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
Asthma Phenotypes, Heterogeneity and Severity: The Basis of Asthma Management
 Asthma Phenotypes, Heterogeneity and Severity: The Basis of Asthma Management Eugene R. Bleecker, MD Professor and Director, Center for Genomics & Personalized Medicine Research Professor, Translational
Asthma Phenotypes, Heterogeneity and Severity: The Basis of Asthma Management Eugene R. Bleecker, MD Professor and Director, Center for Genomics & Personalized Medicine Research Professor, Translational
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Chronic Obstructive Pulmonary Disease (COPD) Measures Document
 Measures Document") Chronic Obstructive Pulmonary Disease (COPD) Measures Document COPD Version: 3 - covering patients discharged between 01/10/2017 and present. Programme Lead: Jo Higgins Clinical Lead: Dr Paul Albert Number
Chronic Obstructive Pulmonary Disease (COPD) Measures Document COPD Version: 3 - covering patients discharged between 01/10/2017 and present. Programme Lead: Jo Higgins Clinical Lead: Dr Paul Albert Number
Disclosures. Update on COPD & Asthma. Update on the Management of COPD. No Pharma Disclosures. NHLBI - Asthma Clinical Research Network
 Update on COPD & Asthma Michael C. Peters, M.D. MAS Division of Pulmonary & Critical Care Medicine Cardiovascular Research Institute University of California San Francisco UCSF Primary Care Medicine San
Update on COPD & Asthma Michael C. Peters, M.D. MAS Division of Pulmonary & Critical Care Medicine Cardiovascular Research Institute University of California San Francisco UCSF Primary Care Medicine San
Pathway diagrams Annex F
 Pathway diagrams Annex F Fig 1 Asthma: The patient journey Asthma is diagnosed Making the diagnosis of asthma Confirming the diagnosis may depend on history, response to treatment, measurement of airflow
Pathway diagrams Annex F Fig 1 Asthma: The patient journey Asthma is diagnosed Making the diagnosis of asthma Confirming the diagnosis may depend on history, response to treatment, measurement of airflow
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Using Patient Characteristics to Individualize and Improve Asthma Care
 Using Patient Characteristics to Individualize and Improve Asthma Care Leonard B. Bacharier, M.D. Associate Professor of Pediatrics Clinical Director, Division of Allergy, Immunology, & Pulmonary Medicine
Using Patient Characteristics to Individualize and Improve Asthma Care Leonard B. Bacharier, M.D. Associate Professor of Pediatrics Clinical Director, Division of Allergy, Immunology, & Pulmonary Medicine
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Choosing an inhaler for COPD made simple. Dr Simon Hart Castle Hill Hospital
 Choosing an inhaler for COPD made simple Dr Simon Hart Castle Hill Hospital 1 Declaration of interests I have received speaker fees, sponsorship to attend conferences, and funding for research from companies
Choosing an inhaler for COPD made simple Dr Simon Hart Castle Hill Hospital 1 Declaration of interests I have received speaker fees, sponsorship to attend conferences, and funding for research from companies
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD
 Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE
 The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
C hronic obstructive pulmonary disease (COPD) is one of
 is one of") 589 RESPIRATORY INFECTIONS Time course of recovery of health status following an infective exacerbation of chronic bronchitis S Spencer, P W Jones for the GLOBE Study Group... Thorax 2003;58:589 593 See
589 RESPIRATORY INFECTIONS Time course of recovery of health status following an infective exacerbation of chronic bronchitis S Spencer, P W Jones for the GLOBE Study Group... Thorax 2003;58:589 593 See
COPD: From Phenotypes to Endotypes. MeiLan K Han, M.D., M.S. Associate Professor of Medicine University of Michigan, Ann Arbor, MI
 COPD: From Phenotypes to Endotypes MeiLan K Han, M.D., M.S. Associate Professor of Medicine University of Michigan, Ann Arbor, MI Presenter Disclosures MeiLan K. Han Consulting Research support Novartis
COPD: From Phenotypes to Endotypes MeiLan K Han, M.D., M.S. Associate Professor of Medicine University of Michigan, Ann Arbor, MI Presenter Disclosures MeiLan K. Han Consulting Research support Novartis
Disclosures. Chronic Obstructive Pulmonary Disease. Chronic Obstructive Pulmonary Disease (COPD)
") Chronic Obstructive Pulmonary Disease May 14, 2016 Orlando, FL COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United States. Alarmingly, COPD recently became
Chronic Obstructive Pulmonary Disease May 14, 2016 Orlando, FL COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United States. Alarmingly, COPD recently became
THE COPD-ASTHMA OVERLAP SYNDROME
 THE COPD-ASTHMA OVERLAP SYNDROME NICOLA A. HANANIA, MD, MS, FRCP(C), FCCP, FACP ASSOCIATE PROFESSOR OF MEDICINE DIRECTOR OF ASTHMA & COPD CLINICAL RESEARCH CENTER BAYLOR COLLEGE OF MEDICINE HOUSTON, TX
THE COPD-ASTHMA OVERLAP SYNDROME NICOLA A. HANANIA, MD, MS, FRCP(C), FCCP, FACP ASSOCIATE PROFESSOR OF MEDICINE DIRECTOR OF ASTHMA & COPD CLINICAL RESEARCH CENTER BAYLOR COLLEGE OF MEDICINE HOUSTON, TX
Step-down approach in chronic stable asthma: A comparison of reducing dose Inhaled Formoterol/ Budesonide with maintaining Inhaled Budesonide.
 Step-down approach in chronic stable asthma: A comparison of reducing dose Inhaled Formoterol/ Budesonide with maintaining Inhaled Budesonide. By: DR MOHD SHAMSUL AMRI Supervisor: Associate Professor Dr
Step-down approach in chronic stable asthma: A comparison of reducing dose Inhaled Formoterol/ Budesonide with maintaining Inhaled Budesonide. By: DR MOHD SHAMSUL AMRI Supervisor: Associate Professor Dr
Research in Real Life
 Research in Real Life Study 1: Exploratory study - identifying the benefits of pmdi versus Diskus for delivering fluticasone/salmeterol combination therapy in patients with chronic obstructive pulmonary
Research in Real Life Study 1: Exploratory study - identifying the benefits of pmdi versus Diskus for delivering fluticasone/salmeterol combination therapy in patients with chronic obstructive pulmonary
Pharmacological Management of Obstructive Airways in Humans. Introduction to Scientific Research. Submitted: 12/4/08
 Pharmacological Management of Obstructive Airways in Humans Introduction to Scientific Research Submitted: 12/4/08 Introduction: Obstructive airways can be characterized as inflammation or structural changes
Pharmacological Management of Obstructive Airways in Humans Introduction to Scientific Research Submitted: 12/4/08 Introduction: Obstructive airways can be characterized as inflammation or structural changes
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease
 HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL
 DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
How to distinguish between uncontrolled and severe asthma
 How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
COPD: Preventable and Treatable. Lecture Outline. Diagnosis of COPD. COPD: Defining Terms
 COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Current Asthma Therapy: Little Need to Phenotype. Phenotypes of Severe Asthma. Cellular Phenotypes 12/7/2012
 Subbasement Membrane Thickness(µm) 12/7/212 Current Asthma Therapy: Little Need to Phenotype Phenotypes of Severe Asthma Most mild and to some degree moderate asthmatics respond well to currently available
Subbasement Membrane Thickness(µm) 12/7/212 Current Asthma Therapy: Little Need to Phenotype Phenotypes of Severe Asthma Most mild and to some degree moderate asthmatics respond well to currently available
How To Assess Severity and Prognosis
 How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
Asthma Tutorial. Trainer MRW. Consider the two scenarios, make an attempt at the questions, what guidance have you used?
 Registrar: LG PR RS Topic Asthma and COPD Asthma Tutorial Trainer MRW Date of Tutorial 18 th Jan 2007 Objectives of the tutorial How to diagnose What investigations and when Treatment guidelines QoF Criteria
Registrar: LG PR RS Topic Asthma and COPD Asthma Tutorial Trainer MRW Date of Tutorial 18 th Jan 2007 Objectives of the tutorial How to diagnose What investigations and when Treatment guidelines QoF Criteria
Chronic Obstructive Pulmonary Disease (COPD).
.") Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Epidemiology of COPD Prof. David M. Mannino, M.D.
 Epidemiology of COPD David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health College of Public Health University of Kentucky 1 Outline Definitions Severity Progression
Epidemiology of COPD David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health College of Public Health University of Kentucky 1 Outline Definitions Severity Progression
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
Supplementary Online Content
 Supplementary Online Content Regan EA, Lynch DA, Curran-Everett D, et al; Genetic Epidemiology of COPD (COPDGene) Investigators. Clinical and radiologic disease in smokers with normal spirometry. Published
Supplementary Online Content Regan EA, Lynch DA, Curran-Everett D, et al; Genetic Epidemiology of COPD (COPDGene) Investigators. Clinical and radiologic disease in smokers with normal spirometry. Published
Surveillance report Published: 6 April 2016 nice.org.uk. NICE All rights reserved.
 Surveillance report 2016 Chronic obstructive pulmonary disease in over 16s: diagnosis and management (2010) NICE guideline CG101 Surveillance report Published: 6 April 2016 nice.org.uk NICE 2016. All rights
Surveillance report 2016 Chronic obstructive pulmonary disease in over 16s: diagnosis and management (2010) NICE guideline CG101 Surveillance report Published: 6 April 2016 nice.org.uk NICE 2016. All rights
COPD: Genomic Biomarker Status and Challenge Scoring
 COPD: Genomic Biomarker Status and Challenge Scoring Julia Hoeng, PMI R&D Raquel Norel, IBM Research 3 rd October 2012 COPD: Genomic Biomarker Status Julia Hoeng, Ph.D. Philip Morris International, Research
COPD: Genomic Biomarker Status and Challenge Scoring Julia Hoeng, PMI R&D Raquel Norel, IBM Research 3 rd October 2012 COPD: Genomic Biomarker Status Julia Hoeng, Ph.D. Philip Morris International, Research
Management of Acute Exacerbations of COPD
 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD August 22, 2018 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD Expert Presenter: Catherine A. Meldrum PhD RN MS
MiCMRC Educational Webinar Management of Acute Exacerbations of COPD August 22, 2018 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD Expert Presenter: Catherine A. Meldrum PhD RN MS
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma Pathophysiology and Treatment. John R. Holcomb, M.D.
 Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Pharmacotherapy for COPD
 10/3/2017 Topics to be covered Pharmacotherapy for chronic treatment Pharmacotherapy for COPD Dr. W C Yu 3rd September 2017 Commonly used drugs Guidelines for their use Inhaled corticosteroids (ICS) in
10/3/2017 Topics to be covered Pharmacotherapy for chronic treatment Pharmacotherapy for COPD Dr. W C Yu 3rd September 2017 Commonly used drugs Guidelines for their use Inhaled corticosteroids (ICS) in
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma ASTHMA. Current Strategies for Asthma and COPD
 Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Around-COPD Verona (Italy), January Highlights
, January Highlights") Introduction Around-COPD Verona (Italy), January 18 2017 Highlights Prof. Dal Negro chairman of the symposium, opened the congress by highlighting the burden of COPD as a chronic invalidating disease affecting
Introduction Around-COPD Verona (Italy), January 18 2017 Highlights Prof. Dal Negro chairman of the symposium, opened the congress by highlighting the burden of COPD as a chronic invalidating disease affecting
Lecture 11: Clustering to discover disease subtypes and stages
 MACHINE LEARNING FOR HEALTHCARE 6.S897, HST.S53 Lecture 11: Clustering to discover disease subtypes and stages Prof. David Sontag MIT EECS, CSAIL, IMES Outline of today s class 1. Overview of clustering
MACHINE LEARNING FOR HEALTHCARE 6.S897, HST.S53 Lecture 11: Clustering to discover disease subtypes and stages Prof. David Sontag MIT EECS, CSAIL, IMES Outline of today s class 1. Overview of clustering
COPD exacerbation. Dr. med. Frank Rassouli
 Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
AECOPD: Management and Prevention
 Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Patient characteristics Intervention Comparison Length of followup
 ORAL MUCOLYTICS Ref ID: 2511 Bachh AA, Shah NN, Bhargava R et al. Effect oral N- in COPD - A randomised controlled trial. JK Practitioner. 2007; 14(1):12-16. Ref ID: 2511 RCT Single blind; unclear allocation
ORAL MUCOLYTICS Ref ID: 2511 Bachh AA, Shah NN, Bhargava R et al. Effect oral N- in COPD - A randomised controlled trial. JK Practitioner. 2007; 14(1):12-16. Ref ID: 2511 RCT Single blind; unclear allocation
INITIATING A COPD CLINIC: PROTOCOL & ASSESSMENT
 COPD Resource Pack Section 2A INITIATING A COPD CLINIC: PROTOCOL & ASSESSMENT In this section: 1. Initiating a COPD Clinic 2. Equipment for a COPD Clinic 3. Primary Care Chronic Obstructive Pulmonary Disease
COPD Resource Pack Section 2A INITIATING A COPD CLINIC: PROTOCOL & ASSESSMENT In this section: 1. Initiating a COPD Clinic 2. Equipment for a COPD Clinic 3. Primary Care Chronic Obstructive Pulmonary Disease
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
Sydney, AUSTRALIA Beijing, CHINA Hyderabad, INDIA Oxford, UK. Affiliated with
 Sydney, AUSTRALIA Beijing, CHINA Hyderabad, INDIA Oxford, UK Affiliated with COPD and Comorbidities Norbert Berend Professor Emeritus University of Sydney Head, Respiratory Research The George Institute
Sydney, AUSTRALIA Beijing, CHINA Hyderabad, INDIA Oxford, UK Affiliated with COPD and Comorbidities Norbert Berend Professor Emeritus University of Sydney Head, Respiratory Research The George Institute
Chronic obstructive pulmonary disease
 Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?