MLO. Edition 1, Medications for Listed Organisations (SI 449 OF 2015)
|
|
|
- Charles Robinson
- 5 years ago
- Views:
Transcription



1 MLO Edition 1, 2016 Medications for Listed Organisations (SI 449 OF 2015)
2 CLINICAL PRACTICE GUIDELINES - SI 449 OF 2015, EDITION 1 Published by: Pre-Hospital Emergency Care Council Abbey Moat House, Abbey Street, Naas, Co Kildare, W91 NN9V, Ireland Phone: (0) Fax: (0) info@phecc.ie Web: ISBN Pre-Hospital Emergency Care Council 2016 Permission is hereby granted to redistribute this document, in whole or part, for educational, non-commercial purposes providing that the content is not altered and that the Pre-Hospital Emergency Care Council (PHECC) is appropriately credited for the work. Written permission from PHECC is required for all other uses. Please contact the author: b.power@phecc.ie 1
3 CLINICAL PRACTICE GUIDELINES - SI 449 OF 2015, EDITION 1 Table of Contents ACKNOWLEDGEMENTS... 3 INTRODUCTION... 4 IMPLEMENTATION AND USE OF CLINICAL PRACTICE GUIDELINES... 5 CLINICAL PRACTICE GUIDELINES KEY/CODES EXPLANATION... 6 Epinephrine (auto injector adult)... 7 Epinephrine (auto injector paediatric)... 8 Naloxone (adult)... 9 Salbutamol Glucagon (adult) Glucagon (paediatric) Glyceryl Trinitrate (GTN) Nitrous Oxide and Oxygen Appendix 1 - Medication Formulary Index of Medication Formulary Aspirin Epinephrine (Adrenaline) Auto injector Glucagon Glucose gel Glyceryl trinitrate (GTN) Naloxone Nitrous Oxide 50% and Oxygen 50% (Entonox ) Salbutamol
4 ACKNOWLEDGEMENTS The process of developing CPGs has been long and detailed. The quality of the finished product is due to the painstaking work of many people, who through their expertise and review of the literature, ensured a world-class publication. PROJECT LEADER & EDITOR Mr Brian Power, Programme Development Officer, PHECC. INITIAL CLINICAL REVIEW Ms Pauline Dempsey, Programme Development Officer, PHECC. Ms Jacqueline Egan, Programme Development Officer, PHECC. MEDICAL ADVISORY COMMITTEE Dr Mick Molloy, (Chair) Consultant in Emergency Medicine Dr Niamh Collins, (Vice Chair) Consultant in Emergency Medicine, Connolly Hospital Blanchardstown Prof Gerard Bury, Professor of General Practice, University College Dublin Dr Seamus Clarke, General Practitioner, representing the Irish College of General Practitioners Dr Jack Collins, Emergency Medical Technician, Representative from the PHECC register Prof Stephen Cusack, Consultant in Emergency Medicine, Cork University Hospital A/Prof Conor Deasy, Consultant in Emergency Medicine, Cork University Hospital, Deputy Medical Director HSE National Ambulance Service Mr Michael Dineen, Paramedic, Vice Chair of Council Mr David Hennelly, Advanced Paramedic, Clinical Development Manager, National Ambulance Service Mr Macartan Hughes, Advanced Paramedic, Head of Education & Competency Assurance, HSE National Ambulance Service Mr Eoghan Connolly, Advanced Paramedic, representative from the Irish College of Paramedics Mr Thomas Keane, Paramedic, Member of Council Mr Shane Knox, Education Manager, National Ambulance Service College Col Gerard Kerr, Director, the Defence Forces Medical Corps Mr Declan Lonergan, Advanced Paramedic, Education & Competency Assurance Manager, HSE National Ambulance Service Mr Seamus McAllister, Divisional Training Officer, rthern Ireland Ambulance Service Dr David McManus, Medical Director, rthern Ireland Ambulance Service Dr David Menzies, Consultant in Emergency Medicine, Clinical Lead, Emergency Medical Science, University College Dublin Mr Shane Mooney, Advanced Paramedic, Chair of Quality and Safety Committee Mr Joseph Mooney, Emergency Medical Technician, Representative from the PHECC register Mr David O Connor, Advanced Paramedic, representative from the PHECC register Dr Peter O Connor, Consultant in Emergency Medicine, Medical Advisor Dublin Fire Brigade Mr Cathal O Donnell, Consultant in Emergency Medicine, Medical Director, HSE National Ambulance Service Mr Kenneth O Dwyer, Advanced Paramedic, representative from the PHECC register Mr Martin O Reilly, Advanced Paramedic, District Officer Dublin Fire Brigade Mr Rory Prevett, Paramedic, representative from the PHECC register Dr Neil Reddy, Medical Director, Code Blue Mr Derek Rooney, Paramedic, representative from the PHECC register Ms Valerie Small, Advanced Nurse Practitioner, Chair of Education and Standards Committee. Dr Sean Walsh, Consultant in Paediatric Emergency Medicine, Our Lady s Hospital for Sick Children, Crumlin 3

5 INTRODUCTION The purpose of these clinical practice guidelines (CPGs) is to provide safe guide-lines to non-medical persons when administering specified prescription-only medications, without a prescription, to a person for the purpose of saving life or reducing severe distress in emergency situations. The non-medical person wil be an individual appointed by a listed organisation where that individual has completed an approved course of training regarding the administration of such medications and the management of any adverse reaction. Dr Mick Molloy, Chair, Medical Advisory Committee. 4
6 IMPLEMENTATION The CPGs herein may be implemented provided: 1 The non-medical person maintains current certification on the medication(s) as outlined in PHECC s Education & Training Standard. 2 The non-medical person is authorised, by listed organisation on whose behalf he/she is acting, to implement the specific CPG. 3 The medications are listed on the tenth schedule. Medication dose The medication dose specified on the relevant CPGs shall be the definitive dose in relation to non-medical person s administration of the specified medication(s). The onus rests on the non-medical person to ensure that he/she is using the latest version of CPGs which are available on the PHECC website Definitions Adult Paediatric patient A patient of 16 years or greater A patient less than 16 years Documentation Completing patient documentation is paramount in the interest of patient safety and the risk management process. The Ambulatory Care Report (ACR) must be completed to meet these requirements. 5
7 CODES Clinical Practice Guidelines for Listed Organisations Codes explanation 1/2/3.4.1 Version 2, 07/11 1/2/3.x.y Version 2, mm/yyyy Sequence step CPG numbering system 1/2/3 = clinical levels to which the CPG pertains x = section in CPG manual, y = CPG number in sequence mm/yyyy = month/year CPG published A sequence (skill) to be performed Start from Mandatory sequence step A clinical condition that may precipitate entry into the specific CPG A mandatory sequence (skill) to be performed Ring ambulance control 112 /999 A decision process The responder must follow one route Request an AED from local area Instructions An instruction box for information Request AED Consider treatment options Reassess Given the clinical presentation consider the treatment option specified Reassess the patient following intervention Special instructions Special authorisation Special instructions Which the Responder must follow Special authorisation This authorises the responder to perform an intervention under specified conditions Medication, dose & route Medication, dose & route A medication which may be administered by a CFR or higher clinical level The medication name, dose and route is specified A medication which may be administered by an EFR or higher clinical level The medication name, dose and route is specified Go to xxx CPG A direction to go to a specific CPG following a decision process te: only go to the CPGs that pertain to your clinical level 6
8 Version 1, 02/2016 Listed Organisations and Epinephrine (auto injector adult) Exposure to a known allergen for the patient reinforces the diagnosis of anaphylaxis Be aware that: Skin or mouth/ tongue changes alone are not a sign of an anaphylactic reaction There may also be vomiting, abdominal pain or incontinence Anaphylaxis suspected 112/ 999 Anaphylaxis is a life threatening condition identified by the following criteria: Sudden onset and rapid progression of symptoms Airway swelling Breathing difficulty Swollen eyes Red, blotchy skin Airway, Breathing or Circulation problem Lie flat with legs raised Allergic reaction diagnosed or prescribed Epinephrine autoinjector previously Signs of anaphylaxis present Signs of Anaphylaxis Rapid onset Exposed to trigger ABC compromised Epinephrine 300 mcg IM Auto injection Reassess Patient Improves after 5 minutes Epinephrine 300 mcg IM Auto injection Monitor vital signs Maintain care until handover to appropriate Practitioner Special Authorisation: You are authorised to administer Epinephrine (auto injector) IM following successful completion of the training module, provided you are acting on behalf of an organisation listed with the HPRA as specified in SI 449 of 2015 Reference: Immunisation Guidelines for Ireland 2008 RCPI, ILCOR Guidelines 2015 SI 449 of
9 Version 1, 02/2016 Listed Organisations and Epinephrine (auto injector paediatric) Exposure to a known allergen for the patient reinforces the diagnosis of anaphylaxis Be aware that: Skin or mouth/ tongue changes alone are not a sign of an anaphylactic reaction There may also be vomiting, abdominal pain or incontinence Anaphylaxis suspected 112/ 999 Anaphylaxis is a life threatening condition identified by the following criteria: Sudden onset and rapid progression of symptoms Airway swelling Breathing difficulty Swollen eyes Red, blotchy skin Airway, Breathing or Circulation problem Lie flat with legs raised Allergic reaction diagnosed or prescribed Epinephrine autoinjector previously Signs of anaphylaxis present Signs of Anaphylaxis Rapid onset Exposed to trigger ABC compromised Epinephrine IM 6 mts to < 10 yrs 0.15 mg (auto injector) 10 yrs 0.3 mg (auto injector) Reassess Patient Improves after 5 minutes Epinephrine IM 6 mts to < 10 yrs 0.15 mg (auto injector) 10 yrs 0.3 mg (auto injector) Monitor vital signs Maintain care until handover to appropriate Practitioner Special Authorisation: You are authorised to administer Epinephrine (auto injector) IM following successful completion of the training module, provided you are acting on behalf of an organisation listed with the HPRA as specified in SI 449 of 2015 Reference: Immunisation Guidelines for Ireland 2008 RCPI, ILCOR Guidelines 2015 SI 449 of
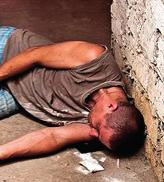
10 1.3.6 Version 1, 02/2016 Listed Organisations and Naloxone (adult) Suspected opioid overdose and unresponsive Clinical indication of opioid overdose 1. Reduced level of consciousness 2. Inadequate breathing 3. Pin point pupil size Get someone to call 112/ 999 or call yourself Confirmation 4. Drug paraphernalia present 5. Bystander history Scene safety Be careful of sharps Shout for help Breathing abnormally or gasping Request AED Breathing abnormally may include; breathing Breathing very slowly Intermittent gasping Inject Naloxone 0.4 mg (IM) into the thigh muscle Place patient in the Recovery Position Pulse present Ventilate using pocket mask (1 breath/ 6 sec) Commence CPR Switch on AED Follow instructions from AED and Ambulance Call Taker Maintain care until handover to appropriate practitioner Continue CPR until an appropriate Practitioner takes over or patient starts to move Special Authorisation: You are authorised to administer Naloxone IM, following successful completion of the training module, provided you are acting on behalf of an organisation listed with the HPRA as specified in SI 449 of 2015 Do not touch open wounds or blood without disposable gloves Reference: SI 449 of 2015, ILCOR Guidelines
11 1.3.4 Version 1, 02/2016 Listed Organisations and Salbutamol Unable to speak normally with a history of asthma All asthma incidents are treated as an emergency until proven otherwise Life threatening asthma Able to self manage 112/ 999 Life threatening asthma; Inability to complete sentences in one breath Respiratory rate > 25 or < 10/ min Heart rate > 110/ min and any one of the following; Feeble respiratory effort Exhaustion Confusion Unresponsive Blueish colour (cyanosis) Encourage patient to administer Salbutamol Asthma diagnosed or prescribed Salbutamol previously Salbutamol, 1 puff, (0.1 mg) metered aerosol During an asthma attack; Do use a spacer device if one is available Do listen to what the patient is saying they may have had attacks before. Don't put your arm around the patient or lie them down - this will restrict their breathing. Don't worry about giving too much Salbutamol, during an asthma attack extra puffs of medication are safe. Repeat up to 11 times if no improvement Reassess Refer patient to GP Breathlessness resolves within 10 minutes 112/ 999 Maintain care until handover to appropriate Practitioner Special Authorisation: You are authorised to administer Salbutamol inhaler, following successful completion of the training module, provided you are acting on behalf of an organisation listed with the HPRA as specified in SI 449 of 2015 Reference: Management of an Acute Asthma Attack in Adults, Clinical Guideline. 14, National Clinical Effectiveness Committee, 2015, Emergency Asthma Guidelines, British Thoracic Society, 2008, British Guidelines on the Management of Asthma, a national clinical guideline, ILCOR Guidelines 2015, Asthma Society of Ireland, SI 449 of
12 Version 1, 02/2016 Listed Organisations and Glucagon (adult) Known diabetic with rapid onset confusion or altered levels of consciousness Check blood glucose (if glucometer available) 112/ 999 Alert and able to swallow Recovery position Blood glucose < 4 mmol/l Or suspected low blood sugar Diabetes diagnosed or prescribed Glucagon previously Glucagon, 1 mg IM Reassess Sweetened drink and/ or Glucose gel, g buccal Alert and able to swallow Allow 5 minutes to elapse following administration of sweetened drink or Glucose gel Reassess Alert and orientated Advise a carbohydrate meal (sandwich) Maintain care until handover to appropriate Practitioner Special Authorisation: You are authorised to administer Glucagon IM, following successful completion of the training module, provided you are acting on behalf of an organisation listed with the HPRA as specified in SI 449 of 2015 Glucagon will not be effective when administered to under nourished persons Reference: Mohun J, 2003, First Aid Manual 8 th Edition, Irish Red Cross & Order of Malta Ambulance Corps SI 449 of
13 Version 1, 02/2016 Listed Organisations and Glucagon (paediatric) Known diabetic with rapid onset confusion or altered levels of consciousness Check blood glucose (if glucometer available) 112/ 999 Alert and able to swallow Recovery position Blood glucose < 4 mmol/l Or suspected low blood sugar Diabetes diagnosed or prescribed Glucagon previously Glucagon 8 years 0.5 mg IM > 8 years 1 mg IM Reassess Sweetened drink and/ or Glucose gel 8 years 5-10 g Buccal > 8 years g Buccal Alert and able to swallow Allow 5 minutes to elapse following administration of sweetened drink or Glucose gel Reassess Alert and orientated Advise a carbohydrate meal (sandwich) Maintain care until handover to appropriate Practitioner Special Authorisation: You are authorised to administer Glucagon IM, following successful completion of the training module, provided you are acting on behalf of an organisation listed with the HPRA as specified in SI 449 of 2015 Glucagon will not be effective when administered to under nourished persons Reference: Mohun J, 2003, First Aid Manual 8 th Edition, Irish Red Cross & Order of Malta Ambulance Corps SI 449 of
14 Version 1, 02/2016 Listed Organisations and Glyceryl Trinitrate (GTN) Patient with chest pain and known angina history 112/ 999 Chest pain ongoing Angina diagnosed or prescribed GTN previously Place patient in a sitting position Glyceryl Trinitrate 0.4 mg SL Assist patient to administer Maintain care until handover to appropiate Practitioner Special Authorisation: You are authorised to administer Glyceryl Trinitrate SL, following successful completion of the training module, provided you are acting on behalf of an organisation listed with the HPRA as specified in SI 449 of 2015 Reference: ILCOR Guidelines 2015 SI 449 of
15 3.2.6 Version 1, 02/2016 Listed Organisations and Nitrous Oxide & Oxygen Pain Consider non pharmacological pain management techniques Splinting Physiological support Heat or cold therapy Positioning Analogue Pain Scale 0 = no pain..10 = unbearable Pain assessment If severe pain Request ALS Moderate to severe pain Pharmacology intervention required Nitrous Oxide & Oxygen, inh Adequate Relief of pain Request ALS Package patient for transport Go back to originating CPG Decisions to give analgesia must be based on clinical assessment and not directly on a linear scale Special Authorisation: You are authorised to administer Nitrous oxide & oxygen gas, following successful completion of the training module, provided you are acting on behalf of an organisation listed with the HPRA as specified in SI 449 of 2015 and operating in a remote or hostile environment. Reference: Park, C. L., et al. (2010). "Prehospital analgesia: systematic review of evidence." J R Army Med Corps 156(4 Suppl 1): SI 449 of
16 Appendix 1 Medication Formulary FOR This Medication Formulary is published by the Pre-Hospital Emergency Care Council (PHECC). It supports material to non-medical persons operating on behalf of listed organisations while administering medications permitted under Medicinal Products Tenth Schedule (SI 449 of 2015). This is a summary document only and non-medical persons are advised to consult with official publications to obtain more detailed information about the medications if required. The Medication Formulary for listed organisations is a subset of the PHECC Medication Formulary for Practitioners published by Council. The CPGs herein may be implemented provided: 1. The non-medical person maintains current certification on the specific medication(s) as outlined in PHECC s Education & Training Standard. 2. The non-medical person is authorised, by the listed organisation on whose behalf he/she is acting, to implement the specific CPG. 3. The medications are listed on the tenth schedule. Medication dose Every effort has been made to ensure accuracy of the medication doses herein. The medication dose specified on the relevant CPGs shall be the definitive dose in relation to non-medical person s administration of the specified medication(s). The onus rests on the non-medical person to ensure that he/she is using the latest version of CPGs which are available on the PHECC website Definitions: Adult: a patient of 16 years or greater. Paediatric patient: a patient less than 16 years. The dose for paediatric patients may never exceed the adult dose. 15

17 APPENDIx 1 MEDICATION FORMULARy ClINICAl level: Medication Class Descriptions Aspirin Platelet aggregation inhibitor. Anti-inflammatory agent and an inhibitor of blood clotting function. Useful agent in the treatment of various cardiovascular diseases such as heart attack. Presentation 300 mg tablet. Administration Indications (reason for administration) ContraIndications (reasons for not administrating) orally - dissolved in water, or to be chewed - if not dissolvable form. (CPG: 1/2/3.4.10). Cardiac chest pain or suspected heart attack. Active ulcer. Bleeding disorder (e.g. haemophilia). Known severe adverse reaction. Patients < 16 years old. Usual Dosages Adult: Paediatric: 300 mg tablet. Contraindicated. Pharmacology/Action Prevents the clotting action of the platelets in the blood. This reduces clot formation during a heart attack. Side effects (anticipated but unwanted effects that may occur) Abdominal pain and discomfort. Wheezing. Stomach and intestinal haemorrhage. Long-term effects Generally mild and infrequent but incidence of stomach or intestinal irritation with slight blood loss, increased clotting time, chest wheeze and skin reaction in hypersensitive patients. Additional information Aspirin 300 mg is indicated for cardiac chest pain even if patient is on blood thining medication or is already on aspirin. If the patient has swallowed an aspirin (enteric coated) tablet without chewing it, or dissolving in water, administer 300 mg Po as the patient should be regarded as not having taken any aspirin. 16
18 APPENDIx 1 MEDICATION FORMULARy ClINICAl level: Medications for listed organisations Medication Class Descriptions Presentation Administration Indications (reason for administration) Contra-Indications (reasons for not administrating) Usual Dosages Epinephrine (Adrenaline) Auto injector Sympathetic agonist. Naturally occurring hormone. It is a potent stimulant. Pre-filled Auto injector. Intramuscular (IM). (CPG: , ). Severe anaphylaxis. ne Known. Adult: 0.3 mg (Auto injector). Repeat once after 5 minutes if no improvement. Paediatric: 6 months < 10 years; 0.15 mg (Auto injector). 10 years; 0.3 mg (Auto injector). Repeat once after 5 minutes if no improvement. Pharmacology/Action Reversal of swelling in the throat & chest wheeze in anaphylaxis. Blocks the effects of histamine. Side effects (anticipated but unwanted effects that may occur) Palpitations. Increased blood pressure. Chest pain. Additional Information 17
19 APPENDIx 1 MEDICATION FORMULARy ClINICAl level: Medications for listed organisations Medication Class Descriptions Presentation Administration Indications (reason for administration) Contra-Indications (reasons for not administrating) Usual Dosages Glucagon Hormone and Antihypoglycaemic. Glucagon is a protein produced in the pancreas. It is used to increase the blood glucose level in cases of low blood sugar. 1 mg vial powder and solution for disolving the powder. Intramuscular (IM). (CPG: , ) low blood sugar in patients unable to take oral glucose with a blood glucose level < 4 mmol/l. Known severe adverse reaction. Adult: 1 mg IM. Paediatric: 8 years 0.5 mg IM. > 8 years 1 mg IM. Pharmacology/Action Increases glucose in the blood by mobilising sugar stored in the liver. Side effects (anticipated but unwanted effects that may occur) Rare, may cause low blood pressure, dizziness, headache, nausea & vomiting. Additional Information May be ineffective in patients with low stored sugar e.g. prior use in previous 24 hours or poorly nourished people. Store in refrigerator. Protect from light. 18
20 APPENDIx 1 MEDICATION FORMULARy ClINICAl level: Medications for listed organisations Medication Class Descriptions Presentation Administration Indications (reason for administration) Contra-Indications (reasons for not administrating) Usual Dosages Glucose gel Antihypoglycaemic. Synthetic glucose paste. Glucose gel in a tube or sachet. Buccal administration: Administer gel to the inside of the patient s cheek and gently massage the outside of the cheek. (CPG: , ) low blood sugar. Blood sugar < 4 mmol/l. Known diabetic with confusion or altered levels of consciousness. Known severe adverse reaction. Adult: g buccal. Repeat as required. Paediatric: 8 years; 5 10 g buccal. > 8 years: g buccal. Repeat as required. Pharmacology/Action Side effects (anticipated but unwanted effects that may occur) Increases blood glucose levels. May cause vomiting in patients under the age of five if administered too quickly. Additional Information Proceed with caution for patients with: - airway difficulties. - reduced level of consciousness. 19
21 APPENDIx 1 MEDICATION FORMULARy ClINICAl level: Medications for listed organisations Medication Class Descriptions Presentation Administration Indications (reason for administration) Contra-Indications (reasons for not administrating) Usual Dosages Glyceryl trinitrate (GTN) Nitrate. Special preparation of Glyceryl trinitrate in an aerosol form that delivers precisely 0.4 mg of Glyceryl trinitrate per spray. Aerosol spray: metered dose 0.4 mg. Sublingual (Sl) under the tongue: Hold the pump spray vertically with the valve head uppermost. Place as close to the mouth as possible and spray under the tongue. The mouth should be closed after each dose. (CPG: ) Angina. Suspected heart attack or angina. Assist patient with administration. Viagra or similar medication used within previous 24 hours. Known severe adverse reaction. Adult: 0.4 mg Sublingual (under the tongue). Paediatric: t indicated. Pharmacology/Action Side effects (anticipated but unwanted effects that may occur) Releases nitric oxide which acts to dilate blood vessels. Dilates coronary arteries particularly if in spasm increasing blood flow to the heart muscle. Reduces blood pressure. Headache. Temporary low blood pressure. Flushing. Dizziness. Additional Information If the pump is new or it has not been used for a week or more the first spray should be released into the air. 20
22 APPENDIx 1 MEDICATION FORMULARy ClINICAl level: Medications for listed organisations Medication Class Descriptions Presentation Administration Naloxone Narcotic antagonist. Effective in management and reversal of overdoses caused by narcotics or synthetic narcotic agents. Pre-loaded syringe. Intramuscular (IM). (CPG: 1.3.6). Indications (reason for administration) Contra-Indications (reasons for not administrating) Usual Dosages Inadequate breathing and/or altered level of consciousness following known or suspected narcotic overdose. Known severe adverse reaction. Adult: 0.4 mg IM. Paediatric: t indicated. Pharmacology/Action Narcotic antagonist Reverse the respiratory depression and analgesic effect of narcotics. Side effects (anticipated but unwanted effects that may occur) Acute reversal of narcotic effect ranging from nausea & vomiting to agitation and seizures. Additional Information Rapid reversal will precipitate acute withdrawal syndrome. Prepare to deal with aggressive patients. 21

23 APPENDIx 1 MEDICATION FORMULARy ClINICAl level: Medication Class Descriptions Medications for listed organisations Nitrous oxide 50% and oxygen 50% (Entonox ) Analgesic. Potent analgesic gas contains a mixture of both nitrous oxide and oxygen. Presentation Cylinder, coloured blue with white and blue triangles on cylinder shoulders. Medical gas: 50% Nitrous oxide & 50% oxygen. Administration Indications (reason for administration) Contra-Indications (reasons for not administrating) Usual Dosages Pharmacology/Action Side effects (anticipated but unwanted effects that may occur) Additional Information Self administered. Inhalation by demand valve with face-mask or mouthpiece. (CPG: 3.2.6) Pain Relief. Altered level of consciousness. Chest Injury/Pneumothorax. Shock. Recent scuba dive. Decompression sickness. Intestinal obstruction. Inhalation Injury. Carbon monoxide (Co) poisoning. Known severe adverse reaction. Adult: Self-administered until pain relieved. Paediatric: Self-administered until pain relieved. Analgesic agent gas: - CNS depressant. - Pain relief. Disinhibition. Decreased level of consciousness. light headedness. Do not use if patient unable to understand instructions. In cold temperatures, warm cylinder and invert to ensure mix of gases. Brand name: Entonox. Has an addictive property. Caution when using Entonox for greater than one hour as risk of Sickle Cell Crisis. 22
24 APPENDIx 1 MEDICATION FORMULARy ClINICAl level: Medications for listed organisations Medication Class Descriptions Presentation Administration Indications (reason for administration) Salbutamol Sympathetic agonist. Stimulant that mimics the effects of beta-2 adrenergic receptors. Aerosol inhaler: metered dose 0.1 mg. Inhalation via aerosol inhaler. (CPG: 1.3.4). Acute asthmatic attack. Contra-Indications (reasons for not administrating) Usual Dosages Known severe adverse reaction. Adult: 0.1 mg metered aerosol spray. Repeat up to 11 sprays. Paediatric: 0.1 mg metered aerosol spray. Repeat up to 11 sprays. Pharmacology/Action Side effects (anticipated but unwanted effects that may occur) Dilates muscle in airways. Increased heart rate. Tremors. Additional Information It is more efficient to use a volumizer (spacer) in conjunction with an aerosol inhaler when administering Salbutamol. 23
25 Published by: Pre-Hospital Emergency Care Council Abbey Moat House, Abbey Street, Naas, Co. Kildare, W91 NN9V Ireland Phone: (0) Fax: (0) info@phecc.ie Web: Medications for Listed Organisations (SI 449 OF 2015)
Guidelines - Edition 2, 2017
 Clinical Practice Guidelines - Edition 2, 2017 Medications for Listed Organisations (SI 449 of 2015) PHECC Clinical Practice Guidelines First Edition, 2016 Second Edition, 2017 Published by: Pre-Hospital
Clinical Practice Guidelines - Edition 2, 2017 Medications for Listed Organisations (SI 449 of 2015) PHECC Clinical Practice Guidelines First Edition, 2016 Second Edition, 2017 Published by: Pre-Hospital
Platelet aggregation inhibitor. Cardiac chest pain or suspected Myocardial Infarction.
 s Aspirin Platelet aggregation inhibitor. Anti-inflammatory agent and an inhibitor of platelet function. Useful agent in the treatment of various thromboembolic diseases such as acute myocardial infarction.
s Aspirin Platelet aggregation inhibitor. Anti-inflammatory agent and an inhibitor of platelet function. Useful agent in the treatment of various thromboembolic diseases such as acute myocardial infarction.
APPENDIX 1 - MEDICATION FORMULARY
 The medication formulary is published by the Pre-Hospital Emergency Care Council (PHECC) to enable pre-hospital emergency care Responders to be competent in the use of medications permitted under Clinical
The medication formulary is published by the Pre-Hospital Emergency Care Council (PHECC) to enable pre-hospital emergency care Responders to be competent in the use of medications permitted under Clinical
The dose for paediatric patients may never exceed the adult dose.
 The medication formulary is published by the Pre-Hospital Emergency Care Council (PHECC) to support Emergency First Responders to be competent in the use of medications permitted under Clinical Practice
The medication formulary is published by the Pre-Hospital Emergency Care Council (PHECC) to support Emergency First Responders to be competent in the use of medications permitted under Clinical Practice
Clinical Practice Guidelines Edition (Updated February 2018)
") The Formulary is published by the Pre-Hospital Emergency Care Council (PHECC) to support Emergency First Responders to be competent in the use of medications permitted under Clinical Practice Guidelines
The Formulary is published by the Pre-Hospital Emergency Care Council (PHECC) to support Emergency First Responders to be competent in the use of medications permitted under Clinical Practice Guidelines
APPENDIX 1 - MEDICATION FORMULARY
 The Formulary is published by the Pre-Hospital Emergency Care Council (PHECC) to enable pre-hospital emergency care Practitioners to be competent in the use of medications permitted under SI 512 of 2008
The Formulary is published by the Pre-Hospital Emergency Care Council (PHECC) to enable pre-hospital emergency care Practitioners to be competent in the use of medications permitted under SI 512 of 2008
Drug Profiles Professional Responder
 Entonox Classification Medical Gas Entonox (50% oxygen 50% nitrous oxide) Effects Potent analgesic, weak anesthetic Onset Rapid Peak Immediate Indications Relief of moderate to severe pain Cardiac-related
Entonox Classification Medical Gas Entonox (50% oxygen 50% nitrous oxide) Effects Potent analgesic, weak anesthetic Onset Rapid Peak Immediate Indications Relief of moderate to severe pain Cardiac-related
Clinical Key Performance Indicators (KPIs)
") Clinical Key Performance Indicators (KPIs) Mission Statement The Pre-Hospital Emergency Care Council protects the public by independently specifying, reviewing, maintaining and monitoring standards of
Clinical Key Performance Indicators (KPIs) Mission Statement The Pre-Hospital Emergency Care Council protects the public by independently specifying, reviewing, maintaining and monitoring standards of
Chapter 7. Principles of Pharmacology
 Chapter 7 Principles of Pharmacology Introduction Administering medications is a serious business. Medications may alleviate pain and improve patient s well-being. Used inappropriately, may cause harm
Chapter 7 Principles of Pharmacology Introduction Administering medications is a serious business. Medications may alleviate pain and improve patient s well-being. Used inappropriately, may cause harm
Medical Emergencies and Current Management in Dentistry. Prof. Mark Greenwood Newcastle University
 Medical Emergencies and Current Management in Dentistry Prof. Mark Greenwood Newcastle University Lancaster 1.02.12 PREVENTION! Attitude and environment Usually a clue in the history PREVENTION! Attitude
Medical Emergencies and Current Management in Dentistry Prof. Mark Greenwood Newcastle University Lancaster 1.02.12 PREVENTION! Attitude and environment Usually a clue in the history PREVENTION! Attitude
EMT OPTIONAL SKILL. Cell Phones and Pagers. Epinephrine Auto-injector. Course Outline 9/2017
 EMT OPTIONAL SKILL Epinephrine Auto-injector Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and
EMT OPTIONAL SKILL Epinephrine Auto-injector Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and
Appendix (i) The ABCDE approach to the sick patient
 The ABCDE approach to the sick patient") Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Statutory Instrument. S.I. No. 510 of Medicinal Products (Prescription and Control of Supply) (Amendment) Regulations 2005
 (Amendment) Regulations 2005") Statutory Instrument S.I. No. 510 of 2005 Medicinal Products (Prescription and Control of Supply) (Amendment) Regulations 2005 PUBLISHED BY THE STATIONERY OFFICE, DUBLIN To be purchased directly from the
Statutory Instrument S.I. No. 510 of 2005 Medicinal Products (Prescription and Control of Supply) (Amendment) Regulations 2005 PUBLISHED BY THE STATIONERY OFFICE, DUBLIN To be purchased directly from the
Management of ANAPHYLAXIS in the School Setting. Updated September 2010
 Management of ANAPHYLAXIS in the School Setting Updated September 2010 What is an Allergy? Allergies occur when the immune system becomes unusually sensitive and over reacts to common substance that are
Management of ANAPHYLAXIS in the School Setting Updated September 2010 What is an Allergy? Allergies occur when the immune system becomes unusually sensitive and over reacts to common substance that are
The dose for paediatric patients may never exceed the adult dose.
 The Formulary is published by the Pre-Hospital Emergency Care Council (PHECC) to enable pre-hospital emergency care practitioners to be competent in the use of medications permitted under the Medicinal
The Formulary is published by the Pre-Hospital Emergency Care Council (PHECC) to enable pre-hospital emergency care practitioners to be competent in the use of medications permitted under the Medicinal
MEDICAL EMERGENCIES (PART 1) IDENTIFYING AT RISK PATIENTS AND IDENTIFYING THE CONTENTS OF THE EMERGENCY DRUG KIT
 IDENTIFYING AT RISK PATIENTS AND IDENTIFYING THE CONTENTS OF THE EMERGENCY DRUG KIT") MEDICAL EMERGENCIES (PART 1) IDENTIFYING AT RISK PATIENTS AND IDENTIFYING THE CONTENTS OF THE EMERGENCY DRUG KIT Aims To explain the categories of patients that may be considered as being at risk during
MEDICAL EMERGENCIES (PART 1) IDENTIFYING AT RISK PATIENTS AND IDENTIFYING THE CONTENTS OF THE EMERGENCY DRUG KIT Aims To explain the categories of patients that may be considered as being at risk during
Managing Illness 8/9/2010 1
 Managing Illness 1 Fainting Caused by a temporary drop in blood pressure thus causing a reduction in oxygen to the brain. Insufficient oxygen causes casualty to black out and fall. Consciousness normally
Managing Illness 1 Fainting Caused by a temporary drop in blood pressure thus causing a reduction in oxygen to the brain. Insufficient oxygen causes casualty to black out and fall. Consciousness normally
General Pharmacology. Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 16: General Pharmacology. Case History.
 Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 16: General Pharmacology Chapter 16 General Pharmacology Slide 1 Case History You arrive at the home of a patient with chest pain.
Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 16: General Pharmacology Chapter 16 General Pharmacology Slide 1 Case History You arrive at the home of a patient with chest pain.
PATIENT INFORMATION. C ardiac Diseases. Anti-anginal Agents (I) Nitrates
 Nitrates") PATIENT INFORMATION Medicine To Treat: C ardiac Diseases Anti-anginal Agents (I) Nitrates ABOUT YOUR MEDICINE Your doctor has just prescribed for you a nitrate, e.g. Isosorbide dinitrate (Isobin, Isordil,
PATIENT INFORMATION Medicine To Treat: C ardiac Diseases Anti-anginal Agents (I) Nitrates ABOUT YOUR MEDICINE Your doctor has just prescribed for you a nitrate, e.g. Isosorbide dinitrate (Isobin, Isordil,
Chapter 11 - Principles of Pharmacology
 1 2 3 4 5 6 7 8 9 Chapter 11 Principles of Pharmacology National EMS Education Standard Competencies (1 of 5) Pharmacology Applies fundamental knowledge of the medications that the EMT may assist/administer
1 2 3 4 5 6 7 8 9 Chapter 11 Principles of Pharmacology National EMS Education Standard Competencies (1 of 5) Pharmacology Applies fundamental knowledge of the medications that the EMT may assist/administer
Management of medical emergencies for the dental team
 Management of medical emergencies for the dental team Update November 2006 In July 2006, the UK Resuscitation Council published a document entitled Medical emergencies and resuscitation standards for clinical
Management of medical emergencies for the dental team Update November 2006 In July 2006, the UK Resuscitation Council published a document entitled Medical emergencies and resuscitation standards for clinical
Anaphylaxis: Treatment in the Community
 : Treatment in the Community is likely if a patient who, within minutes of exposure to a trigger (allergen), develops a sudden illness with rapidly progressing skin changes and life-threatening airway
: Treatment in the Community is likely if a patient who, within minutes of exposure to a trigger (allergen), develops a sudden illness with rapidly progressing skin changes and life-threatening airway
Core Subject Part 4. Identify the principles of approaching the sick patient.
 The Role of The Dental Care Professional During a Medical Emergency: General Dental Council Standards and The Management of The Collapsed Patient Using the ABCDE Approach Aims: Core Subject Part 4 To provide
The Role of The Dental Care Professional During a Medical Emergency: General Dental Council Standards and The Management of The Collapsed Patient Using the ABCDE Approach Aims: Core Subject Part 4 To provide
Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off.
 1 2 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. 3 4 5 6 Course Outline Introduction
1 2 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. 3 4 5 6 Course Outline Introduction
Recognize Anaphylaxis Symptoms
 Recognize Anaphylaxis Symptoms File: JHCD-F1 Recognize the Common Anaphylaxis Symptoms Sudden difficulty breathing, wheezing Hives, generalized flushing, itching, or redness of the skin, Swelling of the
Recognize Anaphylaxis Symptoms File: JHCD-F1 Recognize the Common Anaphylaxis Symptoms Sudden difficulty breathing, wheezing Hives, generalized flushing, itching, or redness of the skin, Swelling of the
Anaphylaxis Independent Learning Package
 Anaphylaxis Independent Learning Package What is Anaphyalxis? Anaphylaxis is a very severe allergic reaction, usually to a substance to which an individual has previously shown sensitivity. It is for this
Anaphylaxis Independent Learning Package What is Anaphyalxis? Anaphylaxis is a very severe allergic reaction, usually to a substance to which an individual has previously shown sensitivity. It is for this
Naloxone Intranasal EMT OPTIONAL SKILL. Cell Phones and Pagers. Course Outline 09/2017
 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and Overview
EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and Overview
ANAPHYLAXIS AND EPIPEN ADMINISTRATION
 ANAPHYLAXIS AND EPIPEN ADMINISTRATION EpiPen Administration This program has been designed for the school staff member who will administer an EpiPen in the event that a student has a life-threatening allergic
ANAPHYLAXIS AND EPIPEN ADMINISTRATION EpiPen Administration This program has been designed for the school staff member who will administer an EpiPen in the event that a student has a life-threatening allergic
Developed By Name Signature Date
 Patient Group Direction 2155 version 2.0 Administration / Supply of Inhaled Salbutamol in Asthma by Registered Practitioners employed by Torbay and South Devon NHS Foundation Trust Date of Introduction:
Patient Group Direction 2155 version 2.0 Administration / Supply of Inhaled Salbutamol in Asthma by Registered Practitioners employed by Torbay and South Devon NHS Foundation Trust Date of Introduction:
patient group direction
 SALBUTAMOL v01 1/12 SALBUTAMOL PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
SALBUTAMOL v01 1/12 SALBUTAMOL PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
Medical First Responder Program Protocols
 Medical Scene Safety Protocol Verify Scene Safety with Police or Dispatch UNKWN Scene Safe? Enter Continue to Appropriate Protocol Possible to Make Safe Make Safe Then Continue Exit Area and Stage Outside
Medical Scene Safety Protocol Verify Scene Safety with Police or Dispatch UNKWN Scene Safe? Enter Continue to Appropriate Protocol Possible to Make Safe Make Safe Then Continue Exit Area and Stage Outside
MEDICAL KIT - ALGORITHMS
 MEDICAL KIT - ALGORITHMS Page 2 : BRONCHOSPASM / ASTHMA Page 3 : TENSION PNEUMOTHORAX Page 4 : Page 5 : Page 6 : CONGESTIVE HEART FAILURE/ PULMONARY EDEMA ANAPHYLACTIC SHOCK / ALLERGIC REACTION ANGINA
MEDICAL KIT - ALGORITHMS Page 2 : BRONCHOSPASM / ASTHMA Page 3 : TENSION PNEUMOTHORAX Page 4 : Page 5 : Page 6 : CONGESTIVE HEART FAILURE/ PULMONARY EDEMA ANAPHYLACTIC SHOCK / ALLERGIC REACTION ANGINA
Primary Care practice clinics within the Edmonton Southside Primary Care Network.
 Allergy/Immunotherapy Injections Last Review: November 2016 Intervention(s) and/or Procedure: Administration of allergen injections throughout immunotherapy treatment. Immunotherapy for allergic disease
Allergy/Immunotherapy Injections Last Review: November 2016 Intervention(s) and/or Procedure: Administration of allergen injections throughout immunotherapy treatment. Immunotherapy for allergic disease
REQUIREMENTS FOR DEVELOPING AN INDIVIDUALIZED HEALTHCARE PLAN FOR STUDENTS WITH FOOD AND LIFE THREATENING ALLERGIES
 REQUIREMENTS FOR DEVELOPING AN INDIVIDUALIZED HEALTHCARE PLAN FOR STUDENTS WITH FOOD AND LIFE THREATENING ALLERGIES Parent/ Guardian: Notify the appropriate school personnel of all student allergies and
REQUIREMENTS FOR DEVELOPING AN INDIVIDUALIZED HEALTHCARE PLAN FOR STUDENTS WITH FOOD AND LIFE THREATENING ALLERGIES Parent/ Guardian: Notify the appropriate school personnel of all student allergies and
ADMINISTRATIVE REQUIREMENT MANUAL EFFECTIVE DATE
 PURPOSE: I. To establish the minimum requirements for a first responder training course in first aid, which all first responders must take, in order to meet the requirements of M.G.L. c. 111, 201 and 105
PURPOSE: I. To establish the minimum requirements for a first responder training course in first aid, which all first responders must take, in order to meet the requirements of M.G.L. c. 111, 201 and 105
Asthma Policy. Mrs Freame and Mrs Cicco are Asthma Lead Professionals at Bromham Primary School and have attended training in April 2017.
 Asthma Policy Reviewed: May 2018 Date of next review: May 2021 For parents and school staff Statement of intent Bromham CofE Primary School welcomes children with asthma and tries to create a safe environment
Asthma Policy Reviewed: May 2018 Date of next review: May 2021 For parents and school staff Statement of intent Bromham CofE Primary School welcomes children with asthma and tries to create a safe environment
Chapter 21. Objectives. Objectives 01/09/2013. Anaphylactic Reactions
 Chapter 21 s Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced in this
Chapter 21 s Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced in this
Chapter 7. National EMS Education Standard Competencies (1 of 5) National EMS Education Standard Competencies (2 of 5) Principles of Pharmacology
 National EMS Education Standard Competencies (2 of 5) Principles of Pharmacology") Chapter 7 Principles of Pharmacology National EMS Education Standard Competencies (1 of 5) Pharmacology Applies fundamental knowledge of the medications that the EMT may assist/administer to a patient
Chapter 7 Principles of Pharmacology National EMS Education Standard Competencies (1 of 5) Pharmacology Applies fundamental knowledge of the medications that the EMT may assist/administer to a patient
MEDICAL EMERGENCIES IN THE DENTAL PRACTICE
 CARDIFF UNIVERSITY PRIFYSGOL CAERDYDD DENTAL POSTGRADUATE SECTION MEDICAL EMERGENCIES IN THE DENTAL PRACTICE FLOWCHARTS ANAPHYLAXIS History suggests Anaphylactic reaction? SIGNS and SYMPTOMS SUGGESTS Anaphylactic
CARDIFF UNIVERSITY PRIFYSGOL CAERDYDD DENTAL POSTGRADUATE SECTION MEDICAL EMERGENCIES IN THE DENTAL PRACTICE FLOWCHARTS ANAPHYLAXIS History suggests Anaphylactic reaction? SIGNS and SYMPTOMS SUGGESTS Anaphylactic
Managing Medical Emergencies in a Dental Practice
 Managing Medical Emergencies in a Dental Practice To download a copy of this handout, or for further information please visit www.backtolife.co.uk/resources Back to Life Ltd, Milton Heath House, Westcott
Managing Medical Emergencies in a Dental Practice To download a copy of this handout, or for further information please visit www.backtolife.co.uk/resources Back to Life Ltd, Milton Heath House, Westcott
Anaphylaxis: treatment in the community
 : treatment in the community Item Type Guideline Authors Health Service Executive Citation Health Service Executive. : treatment in the community. Dublin: Health Service Executive;. 5p. Publisher Health
: treatment in the community Item Type Guideline Authors Health Service Executive Citation Health Service Executive. : treatment in the community. Dublin: Health Service Executive;. 5p. Publisher Health
ACTION PLAN FOR. Difficult/noisy breathing Swelling of tongue Swelling/tightness in throat Wheeze or persistent cough ACTION FOR ANAPHYLAXIS
 www.allergy.org.au Name: Date of birth: Photo Confirmed allergens: Family/emergency contact name(s): ACTION PLAN FOR Anaphylaxis SIGNS OF MILD TO MODERATE ALLERGIC REACTION Swelling of lips, face, eyes
www.allergy.org.au Name: Date of birth: Photo Confirmed allergens: Family/emergency contact name(s): ACTION PLAN FOR Anaphylaxis SIGNS OF MILD TO MODERATE ALLERGIC REACTION Swelling of lips, face, eyes
TREATMENT OF ANAPHYLACTIC REACTION WITH EPINEPHRINE
 TREATMENT OF ANAPHYLACTIC REACTION WITH EPINEPHRINE FILE: JGCDC Background: The Bibb County School System recognizes the growing concern with severe life-threatening allergic reactions to food items, latex,
TREATMENT OF ANAPHYLACTIC REACTION WITH EPINEPHRINE FILE: JGCDC Background: The Bibb County School System recognizes the growing concern with severe life-threatening allergic reactions to food items, latex,
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 22.1 Define key terms introduced in this chapter. Slides 10, 14, 19, 37, 39 22.2 Differentiate between the signs and symptoms of an allergic reaction
Introduction to Emergency Medical Care 1 OBJECTIVES 22.1 Define key terms introduced in this chapter. Slides 10, 14, 19, 37, 39 22.2 Differentiate between the signs and symptoms of an allergic reaction
SAN JOAQUIN COUNTY EMERGENCY MEDICAL SERVICES AGENCY. Administration of Epinephrine Auto-Injector Training
 SAN JOAQUIN COUNTY EMERGENCY MEDICAL SERVICES AGENCY Administration of Epinephrine Auto-Injector Training Disclaimer: Authorization - EMT Optional Skills Only authorized Emergency Medical Technicians (EMT)
SAN JOAQUIN COUNTY EMERGENCY MEDICAL SERVICES AGENCY Administration of Epinephrine Auto-Injector Training Disclaimer: Authorization - EMT Optional Skills Only authorized Emergency Medical Technicians (EMT)
Allergy to: NOTE: Do not depend on antihistamines or inhalers (bronchodilators) to treat a severe reaction. USE EPINEPHRINE.
 to treat a severe reaction. USE EPINEPHRINE.") Name: D.O.B.: Allergy to: PLACE PICTURE HERE Weight: lbs. Asthma: [ ] Yes (higher risk for a severe reaction) [ ] No NOTE: Do not depend on antihistamines or inhalers (bronchodilators) to treat a severe
Name: D.O.B.: Allergy to: PLACE PICTURE HERE Weight: lbs. Asthma: [ ] Yes (higher risk for a severe reaction) [ ] No NOTE: Do not depend on antihistamines or inhalers (bronchodilators) to treat a severe
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Naloxone HCI 4 mg/0.1. nostril. Repeat after 3 minutes if minimal or no
 THE SOUTH CAROLINA BOARD OF MEDICAL EXAMINERS AND THE SOUTH CAROLINA BOARD OF PHARMACY S JOINT PROTOCOL TO INITIATE DISPENSING OF NALOXONE HCI WITHOUT A PRESCRIPTION This joint protocol authorizes any
THE SOUTH CAROLINA BOARD OF MEDICAL EXAMINERS AND THE SOUTH CAROLINA BOARD OF PHARMACY S JOINT PROTOCOL TO INITIATE DISPENSING OF NALOXONE HCI WITHOUT A PRESCRIPTION This joint protocol authorizes any
Anaphylaxis Emergency Plan (individual)
") Appendix D Anaphylaxis Emergency Plan (individual) Recommendation In schools and other child care settings, each child at risk of anaphylaxis should have an Anaphylaxis Emergency Plan. (See following page.)
Appendix D Anaphylaxis Emergency Plan (individual) Recommendation In schools and other child care settings, each child at risk of anaphylaxis should have an Anaphylaxis Emergency Plan. (See following page.)
Westchester Regional BASIC LIFE SUPPORT SPECIAL PROCEDURE PROTOCOLS APPROVED APRIL 2002 / UPDATE JUNE 2004 WESTCHESTER REGIONAL EMS COUNCIL
 Westchester Regional BASIC LIFE SUPPORT SPECIAL PROCEDURE PROTOCOLS APPROVED APRIL 2002 / UPDATE JUNE 2004 WESTCHESTER REGIONAL EMS COUNCIL TABLE OF CONTENTS SECTION PAGE Introduction BLS Special Procedure
Westchester Regional BASIC LIFE SUPPORT SPECIAL PROCEDURE PROTOCOLS APPROVED APRIL 2002 / UPDATE JUNE 2004 WESTCHESTER REGIONAL EMS COUNCIL TABLE OF CONTENTS SECTION PAGE Introduction BLS Special Procedure
Epinephrine Intramuscular (IM) Injection Administration EMT Optional Scope Highlights
 Injection Administration EMT Optional Scope Highlights") Epinephrine Intramuscular (IM) Injection Administration EMT Optional Scope Highlights Nor-Cal EMS February 2018 version 1 Special Thank You To Seattle / King County EMS NY State Department of Health, Check
Epinephrine Intramuscular (IM) Injection Administration EMT Optional Scope Highlights Nor-Cal EMS February 2018 version 1 Special Thank You To Seattle / King County EMS NY State Department of Health, Check
NEW ZEALAND CONSUMER MEDICINE INFORMATION. Salbutamol (as sulfate) 100 micrograms per actuation inhalation aerosol
 100 micrograms per actuation inhalation aerosol") NEW ZEALAND CONSUMER MEDICINE INFORMATION RESPIGEN TM Salbutamol (as sulfate) 100 micrograms per actuation inhalation aerosol Read all of this leaflet carefully before you start using this medicine. Keep
NEW ZEALAND CONSUMER MEDICINE INFORMATION RESPIGEN TM Salbutamol (as sulfate) 100 micrograms per actuation inhalation aerosol Read all of this leaflet carefully before you start using this medicine. Keep
Emergency First Response (EFR) Skills Assessment Sheets V4 June 2017
 Skills Assessment Sheets V4 June 2017") Emergency First Response () Skills Assessment Sheets V4 June 2017 Airway management & ventilation Airway management & ventilation Trauma jaw thrust 1 Hand positions 2 Perform jaw thrust / mouth open 3
Emergency First Response () Skills Assessment Sheets V4 June 2017 Airway management & ventilation Airway management & ventilation Trauma jaw thrust 1 Hand positions 2 Perform jaw thrust / mouth open 3
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Pharmacy Services PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable DOCUMENT # INITIAL EFFECTIVE DATE REVISION
TITLE SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Pharmacy Services PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable DOCUMENT # INITIAL EFFECTIVE DATE REVISION
Managing the Medically Compromised Patient in General Dental Practice Risk Assessment
 Managing the Medically Compromised Patient in General Dental Practice Risk Assessment Core subject Aim: To provide an outline of the risk factors that should be considered in order to provide the safe
Managing the Medically Compromised Patient in General Dental Practice Risk Assessment Core subject Aim: To provide an outline of the risk factors that should be considered in order to provide the safe
Intermediate Medications. Epinephrine cardiac Epinephrine anaphylaxis Dextrose Atropine Narcan Thiamine Albuterol
 Intermediate Medications Epinephrine cardiac Epinephrine anaphylaxis Dextrose Atropine Narcan Thiamine Albuterol Needle Handling Precautions Minimize the tasks performed in a moving ambulance Balance the
Intermediate Medications Epinephrine cardiac Epinephrine anaphylaxis Dextrose Atropine Narcan Thiamine Albuterol Needle Handling Precautions Minimize the tasks performed in a moving ambulance Balance the
P26. Mount. Medicine Policy. Date Written: August 2016 Date of Review: August 2017 WLLP
 Medicine Policy Date Written: August 2016 Date of Review: August 2017 St Mary s College Preparatory School The Mount Medicine Policy (This policy includes EYFS Reception, KS1 and KS2) This policy has been
Medicine Policy Date Written: August 2016 Date of Review: August 2017 St Mary s College Preparatory School The Mount Medicine Policy (This policy includes EYFS Reception, KS1 and KS2) This policy has been
CHAPTER 9. Shock National Safety Council
 CHAPTER 9 Shock Shock Dangerous condition: Not enough oxygen-rich blood reaching vital organs, such as brain and heart Caused by anything that significantly reduces blood flow Life-threatening emergency
CHAPTER 9 Shock Shock Dangerous condition: Not enough oxygen-rich blood reaching vital organs, such as brain and heart Caused by anything that significantly reduces blood flow Life-threatening emergency
Nitrolingual Pumpspray
 Glyceryl Trinitrate Consumer Medicine Information What is in this leaflet This leaflet answers some common questions about Nitrolingual It does not contain all the available information. It does not take
Glyceryl Trinitrate Consumer Medicine Information What is in this leaflet This leaflet answers some common questions about Nitrolingual It does not contain all the available information. It does not take
Policy for the Treatment of Anaphylaxis in Adults and Children
 Policy for the Treatment of Anaphylaxis in Adults and Children June 2008 Policy Title: Policy for the Treatment of Anaphylaxis in Adults or Children Policy Reference Number: PrimCare08/17 Implementation
Policy for the Treatment of Anaphylaxis in Adults and Children June 2008 Policy Title: Policy for the Treatment of Anaphylaxis in Adults or Children Policy Reference Number: PrimCare08/17 Implementation
Oxfordshire Asthma Guidelines. for use in schools and other child care settings
 Oxfordshire Asthma Guidelines for use in schools and other child care settings This document is underpinned by the principles of the United Nations Convention on the rights of the child, in particular
Oxfordshire Asthma Guidelines for use in schools and other child care settings This document is underpinned by the principles of the United Nations Convention on the rights of the child, in particular
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
CLINICAL PROTOCOL FOR THE MEDICAL EMERGENCY TREATMENT OF DENTAL PATIENTS
 CLINICAL PROTOCOL FOR THE MEDICAL EMERGENCY TREATMENT OF DENTAL PATIENTS INTRODUCTION Medical emergency treatments are based on current best practice. (See references) This protocol should be kept in a
CLINICAL PROTOCOL FOR THE MEDICAL EMERGENCY TREATMENT OF DENTAL PATIENTS INTRODUCTION Medical emergency treatments are based on current best practice. (See references) This protocol should be kept in a
Allergy to: NOTE: Do not depend on antihistamines or inhalers (bronchodilators) to treat a severe reaction. USE EPINEPHRINE.
 to treat a severe reaction. USE EPINEPHRINE.") Name: D.O.B.: Allergy to: PLACE PICTURE HERE Weight: lbs. Asthma: [ ] Yes (higher risk for a severe reaction) [ ] No NOTE: Do not depend on antihistamines or inhalers (bronchodilators) to treat a severe
Name: D.O.B.: Allergy to: PLACE PICTURE HERE Weight: lbs. Asthma: [ ] Yes (higher risk for a severe reaction) [ ] No NOTE: Do not depend on antihistamines or inhalers (bronchodilators) to treat a severe
MEDICAL CONDITIONS INFORMATION + QUIZ
 MEDICAL CONDITIONS INFORMATION + QUIZ Information to help answer questions Medical conditions include such pre-existing conditions as asthma, epilepsy and diabetes, severe allergic reactions. For an outdoor
MEDICAL CONDITIONS INFORMATION + QUIZ Information to help answer questions Medical conditions include such pre-existing conditions as asthma, epilepsy and diabetes, severe allergic reactions. For an outdoor
The administration of epinephrine for severe anaphylactic type allergic reactions. Training for Quebec first aiders 2012-MAJ-3
 The administration of epinephrine for severe anaphylactic type allergic reactions Training for Quebec first aiders 2012-MAJ-3 2 Objectives Understand the causes and mechanisms of anaphylaxis Know the symptoms
The administration of epinephrine for severe anaphylactic type allergic reactions Training for Quebec first aiders 2012-MAJ-3 2 Objectives Understand the causes and mechanisms of anaphylaxis Know the symptoms
Allergic Reactions and Envenomations. Chapter 16
 Allergic Reactions and Envenomations Chapter 16 Allergic Reactions Allergic reaction Exaggerated immune response to any substance Histamines and leukotrienes Chemicals released by the immune system Anaphylaxis
Allergic Reactions and Envenomations Chapter 16 Allergic Reactions Allergic reaction Exaggerated immune response to any substance Histamines and leukotrienes Chemicals released by the immune system Anaphylaxis
ANAPHYLAXIS POLICY & PROCEDURES
 PHOENIX P-12 COMMUNITY COLLEGE ANAPHYLAXIS POLICY & PROCEDURES Policy Statement Anaphylaxis is a severe, rapidly progressive allergic reaction that involves various areas of the body simultaneously and
PHOENIX P-12 COMMUNITY COLLEGE ANAPHYLAXIS POLICY & PROCEDURES Policy Statement Anaphylaxis is a severe, rapidly progressive allergic reaction that involves various areas of the body simultaneously and
Using an Inhaler and Nebulizer
 Using an Inhaler and Nebulizer Introduction An inhaler is a handheld device that is used to deliver medication directly to your airways. A nebulizer is an electric or battery powered machine that turns
Using an Inhaler and Nebulizer Introduction An inhaler is a handheld device that is used to deliver medication directly to your airways. A nebulizer is an electric or battery powered machine that turns
QI. Read the following questions and choose the most correct answer (20 Marks):
:") Question One: QI. Read the following questions and choose the most correct answer (20 Marks): 1- Some people are very allergic to some drugs like penicillin. This condition is called: a) Septic shock.
Question One: QI. Read the following questions and choose the most correct answer (20 Marks): 1- Some people are very allergic to some drugs like penicillin. This condition is called: a) Septic shock.
Epinephrine Auto Injector Self-Administration Authorization Packet for Anaphylaxis (A new packet must be completed yearly)
") Epinephrine Auto Injector Self-Administration Authorization Packet for Anaphylaxis (A new packet must be completed yearly) Packet Contents: 1. Anaphylaxis Medication Self-Administration Form (requires
Epinephrine Auto Injector Self-Administration Authorization Packet for Anaphylaxis (A new packet must be completed yearly) Packet Contents: 1. Anaphylaxis Medication Self-Administration Form (requires
all about your heart...
 For a healthy heart If you smoke, stop smoking. Eat lots of fruit and vegetables and less fat. Be more active every day. Be a healthy weight. Relax take time out for yourself. Local contact: For more information
For a healthy heart If you smoke, stop smoking. Eat lots of fruit and vegetables and less fat. Be more active every day. Be a healthy weight. Relax take time out for yourself. Local contact: For more information
Individual Health Care Plan-Diabetes
 Individual Health Care Plan-Diabetes Effective Date: School Year: 20 to 20 This plan should be completed by the student s diabetes care aide/health clerk and parents/guardians. It should be reviewed with
Individual Health Care Plan-Diabetes Effective Date: School Year: 20 to 20 This plan should be completed by the student s diabetes care aide/health clerk and parents/guardians. It should be reviewed with
Should a pupil show signs of a mild- moderate allergic reaction:
 Guidelines for pupils with a severe allergy who carry an auto- injector JEXT EPI-PEN EMERADE When in school pupils are expected to carry their auto-injector at all times. A pupil with a severe allergy
Guidelines for pupils with a severe allergy who carry an auto- injector JEXT EPI-PEN EMERADE When in school pupils are expected to carry their auto-injector at all times. A pupil with a severe allergy
PROCEDURE FOR MANAGING AN ANAPHYLACTIC EMERGENCY
 MULTIDISCIPLINARY PROCEDURE PROCEDURE FOR MANAGING AN ANAPHYLACTIC EMERGENCY First Issued June 2011 Issue Version Four Purpose of Issue/Description of Change Planned Review Date To promote safe and consistent
MULTIDISCIPLINARY PROCEDURE PROCEDURE FOR MANAGING AN ANAPHYLACTIC EMERGENCY First Issued June 2011 Issue Version Four Purpose of Issue/Description of Change Planned Review Date To promote safe and consistent
WHAT IS ATHEROSCLEROSIS?
 ATHEROSCLEROSIS WHAT IS ATHEROSCLEROSIS? Atherosclerosis is a narrowing of the arteries that can significantly reduce the blood supply to vital organs such as the heart, brain and intestines. In atherosclerosis,
ATHEROSCLEROSIS WHAT IS ATHEROSCLEROSIS? Atherosclerosis is a narrowing of the arteries that can significantly reduce the blood supply to vital organs such as the heart, brain and intestines. In atherosclerosis,
Medicines Policy including EYFS (Including Asthma and Anaphylaxis Guidelines) St Aubyn's School
 St Aubyn's School") Policy Owner Jacquie Smith RGN. OHN. Cert. Approving Body Board of Governors Date Approved November 2017 Effective Date November 2017 Review date November 2018 Medicines Policy including EYFS (Including
Policy Owner Jacquie Smith RGN. OHN. Cert. Approving Body Board of Governors Date Approved November 2017 Effective Date November 2017 Review date November 2018 Medicines Policy including EYFS (Including
PERRYSBURG EXEMPTED VILLAGE SCHOOL DISTRICT
 5330 F1/page 1 of 5 PERRYSBURG EXEMPTED VILLAGE SCHOOL DISTRICT MEDICATION IN SCHOOL Before the student will be permitted to take medication during school hours or to use a self-administer medication and
5330 F1/page 1 of 5 PERRYSBURG EXEMPTED VILLAGE SCHOOL DISTRICT MEDICATION IN SCHOOL Before the student will be permitted to take medication during school hours or to use a self-administer medication and
Naloxone Standardized Procedures Illinois Departments of DFPR, DPH & DHS Opioid Antagonist Initiative
 Naloxone Standardized Procedures Illinois Departments of DFPR, DPH & DHS Opioid Antagonist Initiative Background: In September 2015, Illinois passed a new law, PA99-0480, expanding access to the opioid
Naloxone Standardized Procedures Illinois Departments of DFPR, DPH & DHS Opioid Antagonist Initiative Background: In September 2015, Illinois passed a new law, PA99-0480, expanding access to the opioid
Pre-Hospital Emergency Care and Scope of Practice
 Pre-Hospital Emergency Care and Scope of Practice EMT Paramedic Advanced Paramedic 1 Introduction The Pre-Hospital Emergency Care Council (PHECC) is an independent statutory body whose functions include
Pre-Hospital Emergency Care and Scope of Practice EMT Paramedic Advanced Paramedic 1 Introduction The Pre-Hospital Emergency Care Council (PHECC) is an independent statutory body whose functions include
Competency Log Professional Responder Courses
 Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
ASTHMA TOOLKIT. Document creation date: August Version: 1 Amended. Date of review: September Review frequency Biennial
 ASTHMA TOOLKIT Document creation date: August 2014 Version: 1 Amended Date of review: September 2017 Review frequency Biennial Author: Liz Darke Health and Safety Officer Page 1 of 8 What is asthma? Asthma
ASTHMA TOOLKIT Document creation date: August 2014 Version: 1 Amended Date of review: September 2017 Review frequency Biennial Author: Liz Darke Health and Safety Officer Page 1 of 8 What is asthma? Asthma
School District No. 40 Medical Alert Form
 Medical Alert Form Student s Full Name: Birthdate: Wears Medic Alert ID First Parent/Legal Guardian Same address as child Yes No Full Name: Relationship: Home Phone: Work Phone: Cell Phone Email: Second
Medical Alert Form Student s Full Name: Birthdate: Wears Medic Alert ID First Parent/Legal Guardian Same address as child Yes No Full Name: Relationship: Home Phone: Work Phone: Cell Phone Email: Second
2.5 Circulatory Emergencies. Congestive Heart Failure. Cardiovascular Disease (CVD) Health Services: Unit 2 Circulatory System
 Health Services: Unit 2 Circulatory System") 2.5 Circulatory Emergencies In Canada, thousands of people die every year from heart disease and stroke; half of these deaths occur before the patient reaches the hospital. The three major factors contributing
2.5 Circulatory Emergencies In Canada, thousands of people die every year from heart disease and stroke; half of these deaths occur before the patient reaches the hospital. The three major factors contributing
Holiday Program BOOKING FORM
 Holiday Program BOOKING FORM January 2016 PRICES EFFECTIVE FROM 1 JANUARY 2016 RISK MANAGEMENT ASSESSMENT IS AVAILABLE AT OUR WEB SITE www.bathurstgoldfields.com.au Please return by email: info@bathurstgoldfields.com.au
Holiday Program BOOKING FORM January 2016 PRICES EFFECTIVE FROM 1 JANUARY 2016 RISK MANAGEMENT ASSESSMENT IS AVAILABLE AT OUR WEB SITE www.bathurstgoldfields.com.au Please return by email: info@bathurstgoldfields.com.au
Cardiovascular Emergencies. Chapter 12
 Cardiovascular Emergencies Chapter 12 Cardiovascular Emergencies Cardiovascular disease (CVD) claimed 931,108 lives in the US during 2001. 2,551 per day Almost two people per minute! CVD accounts for 38.5%
Cardiovascular Emergencies Chapter 12 Cardiovascular Emergencies Cardiovascular disease (CVD) claimed 931,108 lives in the US during 2001. 2,551 per day Almost two people per minute! CVD accounts for 38.5%
Ask your doctor if you have any. has been prescribed for you. There is no evidence that LYCINATE is addictive or habit forming. Before you take it
 LYCINATE TABLETS glyceryl trinitrate Consumer Medicine Information (CMI) What is in this leaflet This leaflet answers some common questions about LYCINATE. It does not contain all of the available information.
LYCINATE TABLETS glyceryl trinitrate Consumer Medicine Information (CMI) What is in this leaflet This leaflet answers some common questions about LYCINATE. It does not contain all of the available information.
TO BE COMPLETED BY LICENSED HEALTH CARE PROFESSIONAL
 PART I OFFICE OF CATHOLIC SCHOOLS DIOCESE OF ARLINGTON DIABETES MEDICAL MANAGEMENT PLAN Page 1 of 5 TO BE COMPLETED BY PARENT OR GUARDIAN Student School Date of Birth Date of Diagnosis Grade/ Teacher Physical
PART I OFFICE OF CATHOLIC SCHOOLS DIOCESE OF ARLINGTON DIABETES MEDICAL MANAGEMENT PLAN Page 1 of 5 TO BE COMPLETED BY PARENT OR GUARDIAN Student School Date of Birth Date of Diagnosis Grade/ Teacher Physical
P26. Mount. Medicine Policy. Date Written: August 2016 Date of Review: August 2017 WLLP
 Medicine Policy Date Written: August 2016 Date of Review: August 2017 St Mary s College Preparatory School The Mount Medicine Policy (This policy includes EYFS Reception, KS1 and KS2) This policy has been
Medicine Policy Date Written: August 2016 Date of Review: August 2017 St Mary s College Preparatory School The Mount Medicine Policy (This policy includes EYFS Reception, KS1 and KS2) This policy has been
Allergy Awareness & EpiPen Administration
 Allergy Awareness & EpiPen Administration 2017-18 Common Allergens in Children! Shellfish! Milk! Egg! Peanut! Tree Nuts! Fish! Soy! Latex! Insect Stings! Exercise What is an allergy? * An allergy is an
Allergy Awareness & EpiPen Administration 2017-18 Common Allergens in Children! Shellfish! Milk! Egg! Peanut! Tree Nuts! Fish! Soy! Latex! Insect Stings! Exercise What is an allergy? * An allergy is an
Asthma With a Slight Chance of Anaphylaxis
 Asthma With a Slight Chance of Anaphylaxis An Update for Alberta Oral Health Professionals Sept 25/13 Presented by Val Olson CRE Community Pediatric Asthma Service Air passes through the: Nose or mouth
Asthma With a Slight Chance of Anaphylaxis An Update for Alberta Oral Health Professionals Sept 25/13 Presented by Val Olson CRE Community Pediatric Asthma Service Air passes through the: Nose or mouth
Commonwealth of Massachusetts Department of Early Education and Care
 Commonwealth of Massachusetts Department of Early Education and Care MEDICATION CONSENT FORM 606 CMR 7.11(2)(b) Name of child: Name of medication: Please one of the following: Prescription: Oral/Non-Prescription:
Commonwealth of Massachusetts Department of Early Education and Care MEDICATION CONSENT FORM 606 CMR 7.11(2)(b) Name of child: Name of medication: Please one of the following: Prescription: Oral/Non-Prescription:
Anaphylaxis/Latex Allergy
 Children s Acute Transport Service CATS Clinical Guideline Anaphylaxis/Latex Allergy Document Control Information Author D Lutman Author Position Consultant Document Owner E Polke Document Owner Position
Children s Acute Transport Service CATS Clinical Guideline Anaphylaxis/Latex Allergy Document Control Information Author D Lutman Author Position Consultant Document Owner E Polke Document Owner Position
Respiratory Emergencies. Chapter 11
 Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
PGD5717. Director of Quality & Clinical Performance. Therèsa Moyes
 PGD5717 Patient Group Direction Administration of Nicotine Lozenges 4mg, Sublingual Tablets 2mg or Mouth Spray By Registered Nurses employed as by South Staffordshire & Shropshire Healthcare Foundation
PGD5717 Patient Group Direction Administration of Nicotine Lozenges 4mg, Sublingual Tablets 2mg or Mouth Spray By Registered Nurses employed as by South Staffordshire & Shropshire Healthcare Foundation
NASSAU REGIONAL EMERGENCY MEDICAL ADVISORY COMMITTEE
 NASSAU REGIONAL EMERGENCY MEDICAL ADVISORY COMMITTEE 2201 Hempstead Turnpike, Bin 78 Phone: 516-542-0025 East Meadow, NY 11554-1859 FAX: 516-542-0049 Website: www.nassauems.org To: All Emergency Medical
NASSAU REGIONAL EMERGENCY MEDICAL ADVISORY COMMITTEE 2201 Hempstead Turnpike, Bin 78 Phone: 516-542-0025 East Meadow, NY 11554-1859 FAX: 516-542-0049 Website: www.nassauems.org To: All Emergency Medical
Asthma Basic Facts. Staying safe and well with asthma. For people with asthma and their carers.
 Asthma Basic Facts Staying safe and well with asthma. For people with asthma and their carers. Asthma App Contact your local Asthma Foundation asthmaaustralia.org.au Breathing Breathing is how we get air
Asthma Basic Facts Staying safe and well with asthma. For people with asthma and their carers. Asthma App Contact your local Asthma Foundation asthmaaustralia.org.au Breathing Breathing is how we get air
MANAGING COMMON PRESENTATIONS OF ALLERGY IN PRIMARY CARE. Helen Bourne Consultant Immunologist
 MANAGING COMMON PRESENTATIONS OF ALLERGY IN PRIMARY CARE Helen Bourne Consultant Immunologist AIMS Presentation of Allergic Disease in Adults Rhinitis/ Rhinoconjuctivitis Urticaria and Angioedema Food
MANAGING COMMON PRESENTATIONS OF ALLERGY IN PRIMARY CARE Helen Bourne Consultant Immunologist AIMS Presentation of Allergic Disease in Adults Rhinitis/ Rhinoconjuctivitis Urticaria and Angioedema Food
PATIENT GROUP DIRECTION (PGD)
") PATIENT GROUP DIRECTION (PGD) SUPPLY OF NALOXONE HYDROCHLORIDE INJECTION BY REGISTERED NURSES TO CLIENTS BEING RELEASED FROM HMP FORD Version Number: 01HMP Patient Group Direction originally drawn up by:
PATIENT GROUP DIRECTION (PGD) SUPPLY OF NALOXONE HYDROCHLORIDE INJECTION BY REGISTERED NURSES TO CLIENTS BEING RELEASED FROM HMP FORD Version Number: 01HMP Patient Group Direction originally drawn up by:
Developed By Name Signature Date
 Patient Group Direction 2156 version 2.0 Administration of Ipratropium 250mcg/ml Nebuliser Solution in Acute Asthma by Registered Practitioners employed by Torbay and South Devon NHS Foundation Date of
Patient Group Direction 2156 version 2.0 Administration of Ipratropium 250mcg/ml Nebuliser Solution in Acute Asthma by Registered Practitioners employed by Torbay and South Devon NHS Foundation Date of