Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
|
|
|
- Rudolph Chase
- 5 years ago
- Views:
Transcription




1 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep Institute AKL Dr Conroy Wong Respiratory Physician Clinical Head of Respiratory Medicine Middlemore Hospita Auckland Professor Innes Asher Professor and Chair of Paediatrics School of Medicine University of Auckland Auckland 8:30-10:30 WS #4: Respiratory Medicine 101 Forum 11:00-13:00 WS #11: Respiratory Medicine 101 Forum (Repeated)


2 Bronchiectasis update on current management Conroy Wong Respiratory Physician Middlemore Hospital and University of Auckland Auckland
3 Disclosures None
4 Bronchiectasis Etiology Burden of disease in NZ Investigation Treatment

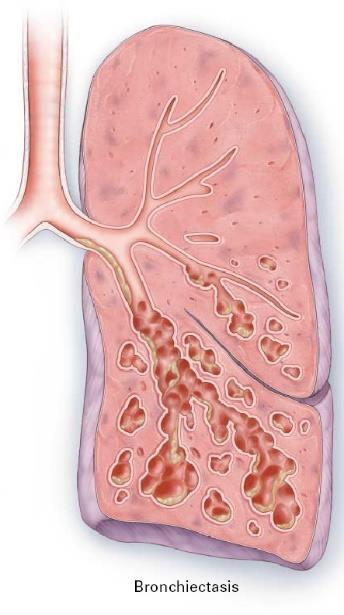

5 Bronchiectasis infection and inflammation Bronchos windpipe Ektasis - stretching N Engl J Med 2002
6 Bronchiectasis is a heterogeneous condition 56 studies 8216 pts Idiopathic 44.8% Post-infective 29.9% Immunodeficiency 5.0% COPD 3.9% Connective tissue dis. 3.8% ABPA 2.6% Ciliary dysfunction 2.5% Asthma 1.4% Inflammatory Bowel dis. 0.8% Others 5.3% Gao et al. Respirology 2016
7 49% of exacerbations are linked to viral infection Exacerbation 49% Coronavirus 39.2% Rhinovirus 24.6% Influenza 24.6% RSV 10.8% Stable 19% Gao et al. Chest 2015
8 Hospitalisations Pacific and Maori populations are disproportionately affected Hospital admissions Mean annual rate 25.7 per 100,000 Bimodal distribution children and elderly 9.1 fold higher for Pacific peoples, 4.9 fold higher for Maori Cost 2012/13 = $5.34 million Bibby et al. NZMJ 2015
9 Socioeconomic deprivation is a strong risk factor for the diagnosis of bronchiectasis Asthma and Respiratory Foundation report
10 Mortality in NZ is associated with ethnicity and socioeconomic deprivation Mortality rates 8.3 fold higher in Pacific peoples 4.7 fold higher in Maori Higher mortality if living in highly deprived areas Te Ao et al. World Bx meeting 2016
11 Factors associated with increased mortality Odds Ratio FEV1 <50% 5.19 Age >70y 4.98 Pseudomonas yes 2.37 Extent of disease >2 lobes 1.87 Dyspnoea mmrc Martinez-Garcia et al. Eur Respir J 2014
12 Pseudomonas aeruginosa colonisation increases morbidity and mortality FRIENDS cohort (Chalmers et al. ERS 2017) 8 European countries patients 5 year follow-up Radiological severity Dyspnea Quality of life Exacerbations (severe and moderate) Hospital admissions Mortality (HR 2.2) Confirm results of meta-analysis (3683 pts) (Finch et al. Ann ATS 2015)
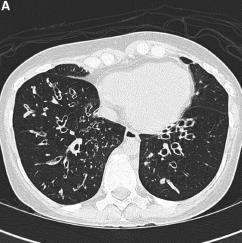
13 What tests should you do for a new patient? High resolution CT scan is the gold standard for diagnosis Recommended Minimum Bundle (ERS guideline. ERJ 2017) 1) Differential blood count 2) Serum immunoglobulins (total IgG, IgA and IgM) 3) Testing for allergic bronchopulmonary aspergillosis (ABPA) Aspergillus specific IgE and IgG, Total IgE Also Sputum culture (routine and mycobacterial) Pulmonary function tests Additional tests depending on specific clinical features
14 Current treatments for bronchiectasis in adults Main pillars of treatment Broad spectrum antibiotics for exacerbations Sputum clearance and physiotherapy Prevention of infections Influenza vaccination Pneumococcal vaccination Pulmonary rehabilitation 2017 ERS guidelines (strong recommendation)
15 Limited evidence base for treatments in bronchiectasis Prolonged antibiotics Pulmonary rehabilitation Nebulised antibiotics Physiotherapy Inhaled and oral steroids Long-acting bronchodilators Mannitol Hypertonic saline Influenza vaccine Pneumococcal vaccine Nebulised DNase Macrolides beneficial Beneficial Limited evidence Insufficient evidence Insufficient evidence Insufficient evidence Increased mucus clearance Insufficient evidence No trials No trials Harmful
16 How should we treat exacerbations? Consensus definition of exacerbation (Hill et al. Eur Respir J 2017) Deterioration in 3 or more key symptoms for at least 48 hours Cough Sputum volume and/or consistency Sputum purulence Breathlessness and/or exercise tolerance Fatigue and/or malaise Haemoptysis Antibiotics ERS guideline recommends 14 days of treatment (Eur Respir J 2017) Antibiotics include amoxycillin-clavulanic acid, roxithromycin, doxycycline, clindamycin.
17 Additional points from Auckland Regional HealthPathways guideline for bronchiectasis Previous sputum bacteriology results should be used in guiding antibiotic choice. Obtain sputum for culture if possible prior to commencement of oral antibiotics. If no clinical improvement, modify the antibiotic once the pathogen is isolated and susceptibilities are available. If patient remains unwell, consider admission for intravenous antibiotics. Oral steroids are not recommended unless there is coexisting eosinophilic airway disease (e.g. asthma) Pseudomonas aeruginosa may be present as a colonising organism and does not necessarily need treatment if the patient is clinically stable. However, specific treatment should be considered if there are clinical features of acute infection.
18 ROBUST Study (RCT) limited benefit of LAMA Reduction Of exacerbations in Bronchiectasis USing Tiotropium 2.50 Exacerbation rates (per year) FEV Exacerbation rate 1.66 Baseline 6 months Tiotropium Placebo Tiotropium Placebo Rate ratio 0.96 p = 0.77 FEV 1 difference (Tiotropium placebo) 58 mls p = Wong et al. ERS 2017
19 Macrolides are effective in preventing exacerbations (azithromycin, erythromycin) Significant reduction in exacerbation frequency 43-62% reduction in rate Modest effects on lung function FEV1 20 ml (0.01) Improvement in quality of life SGRQ 5.4 u (p=0.02) Concerns about antimicrobial resistance Metaanalysis - Wu et al. Respirology 2014
20 Influenza and pneumococcal vaccination are recommended Annual influenza vaccine Efficacy in community ~ 60% Efficacy in hospitalised patients ~40% (SHIVERS study; Turner et al. Vaccine 2014) Pneumococcal vaccination NZ Immunisation Handbook 2017 Not funded for bronchiectasis 45% efficacy for vaccinetype pneumonia 75% efficacy for invasive disease Bonten et al. NEJM 2015 Naïve: 13-valent conjugate vaccine, then 23 valent vaccine at least 8 weeks later Previous 23-valent vaccine: give 13-valent vaccine 1 year later

21 Targeting treatable traits Chalmers et al. Lancet Resp Med 2018
22 Summary - Bronchiectasis Bronchiectasis is a heterogeneous condition Increasing burden of disease in NZ and worldwide Particularly for Pacific and Maori populations Treatment options are still limited but research activity increasing Antibiotics Physiotherapy and pulmonary rehabilitation Vaccination Macrolides
Bronchiectasis it s effects on the NZ population and what we can do to address this
 NZ Respiratory Conference - 2017 Bronchiectasis it s effects on the NZ population and what we can do to address this Conroy Wong Middlemore Hospital Auckland, NZ Bronchiectasis in NZ and new developments
NZ Respiratory Conference - 2017 Bronchiectasis it s effects on the NZ population and what we can do to address this Conroy Wong Middlemore Hospital Auckland, NZ Bronchiectasis in NZ and new developments
Bronchiectasis. What is bronchiectasis? What causes bronchiectasis?
 This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
NON-CF BRONCHIECTASIS IN ADULTS
 Séminaire de Pathologie Infectieuse Jeudi 25 juin 2008 Cliniques Universitaires UCL de Mont-Godinne, Yvoir NON-CF BRONCHIECTASIS IN ADULTS Dr Robert Wilson Royal Brompton Hospital, London, UK Aetiology
Séminaire de Pathologie Infectieuse Jeudi 25 juin 2008 Cliniques Universitaires UCL de Mont-Godinne, Yvoir NON-CF BRONCHIECTASIS IN ADULTS Dr Robert Wilson Royal Brompton Hospital, London, UK Aetiology
Bronchiectasis exacerbations; differences and management. Michael Loebinger Royal Brompton Imperial College
 Bronchiectasis exacerbations; differences and management Michael Loebinger Royal Brompton Imperial College Plan Bronchiectasis background and burden Exacerbation and Management Longer term Management Cases
Bronchiectasis exacerbations; differences and management Michael Loebinger Royal Brompton Imperial College Plan Bronchiectasis background and burden Exacerbation and Management Longer term Management Cases
CCLI. Bronchiectasis Treatment Antibiotics. Charles Haworth. Physician / Patient Conference, Georgetown University, May 2017
 Physician / Patient Conference, Georgetown University, May 2017 Bronchiectasis Treatment Antibiotics Charles Haworth CCLI Cambridge Centre for Lung Infection Disclosures Educational talks and / or consultancy
Physician / Patient Conference, Georgetown University, May 2017 Bronchiectasis Treatment Antibiotics Charles Haworth CCLI Cambridge Centre for Lung Infection Disclosures Educational talks and / or consultancy
Bronchiectasis Domiciliary treatment. Prof. Adam Hill Royal Infirmary and University of Edinburgh
 Bronchiectasis Domiciliary treatment Prof. Adam Hill Royal Infirmary and University of Edinburgh Plan of talk Background of bronchiectasis Who requires IV antibiotics Domiciliary treatment Results to date.
Bronchiectasis Domiciliary treatment Prof. Adam Hill Royal Infirmary and University of Edinburgh Plan of talk Background of bronchiectasis Who requires IV antibiotics Domiciliary treatment Results to date.
Professor Richard Beasley
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington 14:00-14:55 WS #111: Towards Precision Medicine in Asthma -Treatable Traits 15:05-16:00 WS #121:
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington 14:00-14:55 WS #111: Towards Precision Medicine in Asthma -Treatable Traits 15:05-16:00 WS #121:
COPD in primary care: reminder and update
 COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
How To Assess Severity and Prognosis
 How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
Conference Bronchiectasis A Growing Problem
 Conference 2015 Bronchiectasis A Growing Problem Bronchiectasis (in Children) What is it? Why such a concern in NZ? What to look out for? Management Positives? Just a note that the bar for diagnosis, referral
Conference 2015 Bronchiectasis A Growing Problem Bronchiectasis (in Children) What is it? Why such a concern in NZ? What to look out for? Management Positives? Just a note that the bar for diagnosis, referral
Update on bronchiectasis guidelines. James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK
 Update on bronchiectasis guidelines James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK University of Dundee Bronchiectasis guidelines 2017 2010 2006 2008 2015 2015 Currently valid guidelines
Update on bronchiectasis guidelines James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK University of Dundee Bronchiectasis guidelines 2017 2010 2006 2008 2015 2015 Currently valid guidelines
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Cystic Fibrosis Panel Applications (Dornase Alfa) Contents
 Contents") Cystic Fibrosis Panel Applications (Dornase Alfa) Contents Page 2-4: Entry and Stopping Criteria for Treatment with Dornase Alfa Page 5-9: Application and consent forms for a one month trail and long term
Cystic Fibrosis Panel Applications (Dornase Alfa) Contents Page 2-4: Entry and Stopping Criteria for Treatment with Dornase Alfa Page 5-9: Application and consent forms for a one month trail and long term
Surveillance report Published: 6 April 2016 nice.org.uk. NICE All rights reserved.
 Surveillance report 2016 Chronic obstructive pulmonary disease in over 16s: diagnosis and management (2010) NICE guideline CG101 Surveillance report Published: 6 April 2016 nice.org.uk NICE 2016. All rights
Surveillance report 2016 Chronic obstructive pulmonary disease in over 16s: diagnosis and management (2010) NICE guideline CG101 Surveillance report Published: 6 April 2016 nice.org.uk NICE 2016. All rights
Changing Landscapes in COPD New Zealand Respiratory Conference
 Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
COPD Treatable. Preventable.
 My COPD Action Plan Patient s Copy (Patient s Name) Date Canadian Respiratory COPD Treatable. Preventable. This is to tell me how I will take care of myself when I have a COPD flare-up. My goals are My
My COPD Action Plan Patient s Copy (Patient s Name) Date Canadian Respiratory COPD Treatable. Preventable. This is to tell me how I will take care of myself when I have a COPD flare-up. My goals are My
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Bronchiectasis. Introduction. Key points
 15 Bronchiectasis Introduction i Key points Patients with bronchiectasis typically have chronic airway infection, punctuated by acute exacerbations and accompanied by progressive airflow obstruction. Bronchiectasis
15 Bronchiectasis Introduction i Key points Patients with bronchiectasis typically have chronic airway infection, punctuated by acute exacerbations and accompanied by progressive airflow obstruction. Bronchiectasis
Dr Stephen Child. General Physician Auckland. 14:20-14:40 Secondary Care Perspective
 Dr Stephen Child General Physician Auckland 14:20-14:40 Secondary Care Perspective Wheeze Witchery Stephen Child MD, FRACP, FRCPC General Physician Respiratory Interest Director of Clinical Training Auckland
Dr Stephen Child General Physician Auckland 14:20-14:40 Secondary Care Perspective Wheeze Witchery Stephen Child MD, FRACP, FRCPC General Physician Respiratory Interest Director of Clinical Training Auckland
Management of bronchiectasis in adults
 STATE OF THE ART MANAGEMENT OF BRONCHIECTASIS IN ADULTS Management of bronchiectasis in adults James D. Chalmers 1, Stefano Aliberti 2 and Francesco Blasi 3 Affiliations: 1 Tayside Respiratory Research
STATE OF THE ART MANAGEMENT OF BRONCHIECTASIS IN ADULTS Management of bronchiectasis in adults James D. Chalmers 1, Stefano Aliberti 2 and Francesco Blasi 3 Affiliations: 1 Tayside Respiratory Research
Respiratory Subcommittee of PTAC Meeting held 4 March 2015
 Respiratory Subcommittee of PTAC Meeting held 4 March 2015 (minutes for web publishing) Respiratory Subcommittee minutes are published in accordance with the Terms of Reference for the Pharmacology and
Respiratory Subcommittee of PTAC Meeting held 4 March 2015 (minutes for web publishing) Respiratory Subcommittee minutes are published in accordance with the Terms of Reference for the Pharmacology and
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
NON-CYSTIC FIBROSIS BRONCHIECTASIS
 NON-CYSTIC FIBROSIS BRONCHIECTASIS MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the
NON-CYSTIC FIBROSIS BRONCHIECTASIS MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC
 KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC") Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Bronchiectasis. Grant Waterer. Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago
 Bronchiectasis Grant Waterer MBBS PhD MBA FRACP FCCP Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago Conflicts of Interest I have
Bronchiectasis Grant Waterer MBBS PhD MBA FRACP FCCP Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago Conflicts of Interest I have
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research
 Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013
 COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013 None Disclosures Definitions Asthma Asthma is a chronic inflammatory
COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013 None Disclosures Definitions Asthma Asthma is a chronic inflammatory
Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX
 Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX Pioneer of Respiratory Medicine 2016 marked 200th anniversary of his
Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX Pioneer of Respiratory Medicine 2016 marked 200th anniversary of his
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
The management of bronchiectasis in Europe
 The management of bronchiectasis in Europe Data from the European Bronchiectasis Registry James Chalmers University of Dundee, UK Presenter disclosures Clinical Trials AstraZeneca, Aradigm corporation,
The management of bronchiectasis in Europe Data from the European Bronchiectasis Registry James Chalmers University of Dundee, UK Presenter disclosures Clinical Trials AstraZeneca, Aradigm corporation,
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines
 Treatment Guidelines") Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Prophylactic antibiotic therapy for chronic obstructive pulmonary disease(copd)(review)
(review)") Cochrane Database of Systematic Reviews Prophylactic antibiotic therapy for chronic obstructive pulmonary disease(copd)(review) HerathSC,PooleP Herath SC, Poole P. Prophylactic antibiotic therapy for chronic
Cochrane Database of Systematic Reviews Prophylactic antibiotic therapy for chronic obstructive pulmonary disease(copd)(review) HerathSC,PooleP Herath SC, Poole P. Prophylactic antibiotic therapy for chronic
Chronic Obstructive Pulmonary Disease (COPD).
.") Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Prof Neil Barnes. Respiratory and General Medicine London Chest Hospital and The Royal London Hospital
 Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
COPD: From Phenotypes to Endotypes. MeiLan K Han, M.D., M.S. Associate Professor of Medicine University of Michigan, Ann Arbor, MI
 COPD: From Phenotypes to Endotypes MeiLan K Han, M.D., M.S. Associate Professor of Medicine University of Michigan, Ann Arbor, MI Presenter Disclosures MeiLan K. Han Consulting Research support Novartis
COPD: From Phenotypes to Endotypes MeiLan K Han, M.D., M.S. Associate Professor of Medicine University of Michigan, Ann Arbor, MI Presenter Disclosures MeiLan K. Han Consulting Research support Novartis
Bronchiectasis. Examples include: Viral infections (measles, adenovirus, influenza)
") Bronchiectasis What is Bronchiectasis? Bronchiectasis (pronounced bron-kee-ek'-tas-is) is a condition of the airways in the lungs. These airways (bronchial tubes) are tubelike structures that branch from
Bronchiectasis What is Bronchiectasis? Bronchiectasis (pronounced bron-kee-ek'-tas-is) is a condition of the airways in the lungs. These airways (bronchial tubes) are tubelike structures that branch from
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
AECOPD: Management and Prevention
 Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Bronchiectasis (non-cystic fibrosis), acute exacerbation: antimicrobial prescribing
, acute exacerbation: antimicrobial prescribing") National Institute for Health and Care Excellence Bronchiectasis (non-cystic fibrosis), acute exacerbation: antimicrobial prescribing Evidence review NICE guideline NG117 December 2018 Disclaimer The
National Institute for Health and Care Excellence Bronchiectasis (non-cystic fibrosis), acute exacerbation: antimicrobial prescribing Evidence review NICE guideline NG117 December 2018 Disclaimer The
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university
 What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
Modern Management of COPD.
 Modern Management of COPD. Associate Professor Robert Young BMedSc, MBChB, DPhil (Oxon), FRACP, FRCP Department of Medicine, Auckland City Hospital and University of Auckland, New Zealand 2 Sponsor Disclaimer
Modern Management of COPD. Associate Professor Robert Young BMedSc, MBChB, DPhil (Oxon), FRACP, FRCP Department of Medicine, Auckland City Hospital and University of Auckland, New Zealand 2 Sponsor Disclaimer
COPD EXACERBATIONS AND HOSPITAL ADMISSIONS HOW CAN WE PREVENT THEM? Wisia Wedzicha National Heart and Lung Institute, Imperial College London, UK
 COPD EXACERBATIONS AND HOSPITAL ADMISSIONS HOW CAN WE PREVENT THEM? Wisia Wedzicha National Heart and Lung Institute, Imperial College London, UK Presenter Disclosures Wisia Wedzicha All disclosures prior
COPD EXACERBATIONS AND HOSPITAL ADMISSIONS HOW CAN WE PREVENT THEM? Wisia Wedzicha National Heart and Lung Institute, Imperial College London, UK Presenter Disclosures Wisia Wedzicha All disclosures prior
COPD exacerbation. Dr. med. Frank Rassouli
 Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Turning Science into Real Life Roflumilast in Clinical Practice. Roland Buhl Pulmonary Department Mainz University Hospital
 Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Efficacy of Pseudomonas aeruginosa eradication regimens in bronchiectasis
 Efficacy of Pseudomonas aeruginosa eradication regimens in bronchiectasis Vallières, E., Tumelty, K., Tunney, M. M., Hannah, R., Hewitt, O., Elborn, J. S., & Downey, D. G. (2017). Efficacy of Pseudomonas
Efficacy of Pseudomonas aeruginosa eradication regimens in bronchiectasis Vallières, E., Tumelty, K., Tunney, M. M., Hannah, R., Hewitt, O., Elborn, J. S., & Downey, D. G. (2017). Efficacy of Pseudomonas
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease
 HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
Understanding the heterogeneity of the disease
 Symposium: Bronchiectasis in Europe: an update from the European Bronchiectasis Network (EMBARC) Understanding the heterogeneity of the disease Stefano Aliberti Health Science Department University of
Symposium: Bronchiectasis in Europe: an update from the European Bronchiectasis Network (EMBARC) Understanding the heterogeneity of the disease Stefano Aliberti Health Science Department University of
What is Cystic Fibrosis? CYSTIC FIBROSIS. Genetics of CF
 What is Cystic Fibrosis? CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Chronic, progressive and life limiting autosomal recessive genetic disease characterized by chronic
What is Cystic Fibrosis? CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Chronic, progressive and life limiting autosomal recessive genetic disease characterized by chronic
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
Disclosures. Update on COPD & Asthma. Update on the Management of COPD. No Pharma Disclosures. NHLBI - Asthma Clinical Research Network
 Update on COPD & Asthma Michael C. Peters, M.D. MAS Division of Pulmonary & Critical Care Medicine Cardiovascular Research Institute University of California San Francisco UCSF Primary Care Medicine San
Update on COPD & Asthma Michael C. Peters, M.D. MAS Division of Pulmonary & Critical Care Medicine Cardiovascular Research Institute University of California San Francisco UCSF Primary Care Medicine San
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
Life-long asthma and its relationship to COPD. Stephen T Holgate School of Medicine University of Southampton
 Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Using Recursive Logistic Regression to Develop a Patient-Reported Outcome in Non-Cystic Fibrosis Bronchiectasis
 Using Recursive Logistic Regression to Develop a Patient-Reported Outcome in Non-Cystic Fibrosis Bronchiectasis ORSNZ+NZSA Joint Conference, Christchurch, November 2015 Mark C. Wheldon 1,2 Alain C. Vandal
Using Recursive Logistic Regression to Develop a Patient-Reported Outcome in Non-Cystic Fibrosis Bronchiectasis ORSNZ+NZSA Joint Conference, Christchurch, November 2015 Mark C. Wheldon 1,2 Alain C. Vandal
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable
 THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
A Place For Airway Clearance Therapy In Today s Healthcare Environment
 A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
COPD: Preventable and Treatable. Lecture Outline. Diagnosis of COPD. COPD: Defining Terms
 COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
Potential risks of ICS use
 Potential risks of ICS use Randomised controlled trial Observational study Systematic review Pneumonia Tuberculosis Bone fracture Skin thinning/easy bruising Cataract Diabetes No effect on fracture risk
Potential risks of ICS use Randomised controlled trial Observational study Systematic review Pneumonia Tuberculosis Bone fracture Skin thinning/easy bruising Cataract Diabetes No effect on fracture risk
Recent advances in diagnosis and management of ABPA. Arindam SR(Pulmonary Medicine)
") Recent advances in diagnosis and management of ABPA Arindam SR(Pulmonary Medicine) Conventional diagnostic criteria for ABPA Primary Episodic bronchial obstruction (asthma) Peripheral blood eosinophilia
Recent advances in diagnosis and management of ABPA Arindam SR(Pulmonary Medicine) Conventional diagnostic criteria for ABPA Primary Episodic bronchial obstruction (asthma) Peripheral blood eosinophilia
BTS Guideline for non-cf Bronchiectasis
 ISSN 2040-2023 July 2010 BTS Guideline for non-cf Bronchiectasis A Quick Reference Guide British Thoracic Society www.brit-thoracic.org.uk BTS GUIDELINE FOR NON-CF BRONCHIECTASIS A QUICK REFERENCE GUIDE
ISSN 2040-2023 July 2010 BTS Guideline for non-cf Bronchiectasis A Quick Reference Guide British Thoracic Society www.brit-thoracic.org.uk BTS GUIDELINE FOR NON-CF BRONCHIECTASIS A QUICK REFERENCE GUIDE
COPD: Treatment Update Property of Presenter. Not for Reproduction. Barry Make, MD Professor of Medicine National Jewish Health
 COPD: Treatment Update Barry Make, MD Professor of Medicine National Jewish Health Disclosures Advisory board, consultant, multi-center trial, research funding, Data Safety Monitoring Board (DSMB), or
COPD: Treatment Update Barry Make, MD Professor of Medicine National Jewish Health Disclosures Advisory board, consultant, multi-center trial, research funding, Data Safety Monitoring Board (DSMB), or
Inhaled Antibiotics in Non-CF. Dr Michael Loebinger Host Defence Unit Royal Brompton Hospital London, United Kingdom
 Inhaled Antibiotics in Non-CF Dr Michael Loebinger Host Defence Unit Royal Brompton Hospital London, United Kingdom Advantages Increased drug concentrations locally Reduced systemic adverse effects Home
Inhaled Antibiotics in Non-CF Dr Michael Loebinger Host Defence Unit Royal Brompton Hospital London, United Kingdom Advantages Increased drug concentrations locally Reduced systemic adverse effects Home
Bronchiectasis: An Imaging Approach
 Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Assessing response to treatment of exacerbations of bronchiectasis in adults
 Eur Respir J 2009; 33: 312 317 DOI: 10.1183/09031936.00122508 CopyrightßERS Journals Ltd 2009 Assessing response to treatment of exacerbations of bronchiectasis in adults M.P. Murray, K. Turnbull, S. MacQuarrie
Eur Respir J 2009; 33: 312 317 DOI: 10.1183/09031936.00122508 CopyrightßERS Journals Ltd 2009 Assessing response to treatment of exacerbations of bronchiectasis in adults M.P. Murray, K. Turnbull, S. MacQuarrie
Pharmacotherapy for COPD
 10/3/2017 Topics to be covered Pharmacotherapy for chronic treatment Pharmacotherapy for COPD Dr. W C Yu 3rd September 2017 Commonly used drugs Guidelines for their use Inhaled corticosteroids (ICS) in
10/3/2017 Topics to be covered Pharmacotherapy for chronic treatment Pharmacotherapy for COPD Dr. W C Yu 3rd September 2017 Commonly used drugs Guidelines for their use Inhaled corticosteroids (ICS) in
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
C.S. HAWORTH 1, A. WANNER 2, J. FROEHLICH 3, T. O'NEAL 3, A. DAVIS 4, I. GONDA 3, A. O'DONNELL 5
 Inhaled Liposomal Ciprofloxacin in Patients With Non-Cystic Fibrosis Bronchiectasis and Chronic Pseudomonas aeruginosa: Results From Two Parallel Phase III Trials (ORBIT-3 and -4) C.S. HAWORTH 1, A. WANNER
Inhaled Liposomal Ciprofloxacin in Patients With Non-Cystic Fibrosis Bronchiectasis and Chronic Pseudomonas aeruginosa: Results From Two Parallel Phase III Trials (ORBIT-3 and -4) C.S. HAWORTH 1, A. WANNER
COPD Bronchiectasis Overlap Syndrome.
 COPD Bronchiectasis Overlap Syndrome. John R Hurst 1, J Stuart Elborn 2, and Anthony De Soyza 3 on Behalf of the BRONCH-UK Consortium (D Bilton, J Bradley, JS Brown, J Duckers, F Copeland, A Floto, J Foweraker,
COPD Bronchiectasis Overlap Syndrome. John R Hurst 1, J Stuart Elborn 2, and Anthony De Soyza 3 on Behalf of the BRONCH-UK Consortium (D Bilton, J Bradley, JS Brown, J Duckers, F Copeland, A Floto, J Foweraker,
Curriculum Vitae. Head of Public Wing HCU - RSCM. Head of ICU Sari Asih Ciledug Hospital
 Curriculum Vitae Name : Dr. Ceva W. Pitoyo,SpPD,K-P,KIC,FINASIM POB / DOB : Jakarta, March 8th 1968 Education : o General Practitioner : FKUI 1993 o Internist : FKUI 2002 o Pulmonology Consultant : PAPDI-UI
Curriculum Vitae Name : Dr. Ceva W. Pitoyo,SpPD,K-P,KIC,FINASIM POB / DOB : Jakarta, March 8th 1968 Education : o General Practitioner : FKUI 1993 o Internist : FKUI 2002 o Pulmonology Consultant : PAPDI-UI
Chronic productive cough: An approach to management
 Chronic productive cough: An approach to management Key Points Conditions most likely to cause chronic productive cough outlined. Epidemiology, clinical presentation, pathology and treatment of these conditions
Chronic productive cough: An approach to management Key Points Conditions most likely to cause chronic productive cough outlined. Epidemiology, clinical presentation, pathology and treatment of these conditions
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
UPDATE IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 UPDATE IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE Radhika Shah, MD Erlanger Health System University of Tennessee College of Medicine Chattanooga Respiratory, Critical Care, and Sleep medicine No disclosures
UPDATE IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE Radhika Shah, MD Erlanger Health System University of Tennessee College of Medicine Chattanooga Respiratory, Critical Care, and Sleep medicine No disclosures
COPD as a comorbidity of heart failure in elderly patients
 COPD as a comorbidity of heart failure in elderly patients Professor Mitja Lainscak, MD, PhD, FESC, FHFA Departments of Cardiology and Research&Education, General Hospital Celje Faculty of Medicine, University
COPD as a comorbidity of heart failure in elderly patients Professor Mitja Lainscak, MD, PhD, FESC, FHFA Departments of Cardiology and Research&Education, General Hospital Celje Faculty of Medicine, University
MCH-Immunization Conference. September 2012
 MCH-Immunization Conference September 2012 Rosalyn Singleton MD Arctic Investigations Program-CDC Alaska Native Tribal Health Consortium, Anchorage, AK DISCLAIMER: The results and conclusions presented
MCH-Immunization Conference September 2012 Rosalyn Singleton MD Arctic Investigations Program-CDC Alaska Native Tribal Health Consortium, Anchorage, AK DISCLAIMER: The results and conclusions presented
How do we define pneumonia?
 Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
A. Service Specifications
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No: 170050S Service Primary Ciliary Dyskinesia Management Service (adults) Commissioner Lead Provider Lead 1. Scope 1.1 Prescribed
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No: 170050S Service Primary Ciliary Dyskinesia Management Service (adults) Commissioner Lead Provider Lead 1. Scope 1.1 Prescribed
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Goyal V, Grimwood K, Byrnes CA, et al. Amoxicillin
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Goyal V, Grimwood K, Byrnes CA, et al. Amoxicillin
Managing adults with asthma in primary care: the four-stage consultation
 Respiratory conditions Managing adults with asthma in primary care: the four-stage consultation Key practice points: A four-stage consultation is recommended as a framework for managing patients with asthma
Respiratory conditions Managing adults with asthma in primary care: the four-stage consultation Key practice points: A four-stage consultation is recommended as a framework for managing patients with asthma
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
COPD Update. Muhammad Talha Khan MD. COPD Exacerbations. COPD Clinical Importance. COPD Pathophysiology. Overview/Objectives
 Overview/Objectives COPD Update Muhammad Talha Khan MD Pulmonologist St Croix Regional Medical Center, St Croix Falls, WI. Overview of COPD and disease impact Classification of COPD Severity Treatment
Overview/Objectives COPD Update Muhammad Talha Khan MD Pulmonologist St Croix Regional Medical Center, St Croix Falls, WI. Overview of COPD and disease impact Classification of COPD Severity Treatment
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic
 COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
Francesco Blasi Head Respiratory Medicine Section Cardio-Thoracic Department University of Milan, Italy
 COPD EXACERBATIONS Francesco Blasi Head Respiratory Medicine Section Cardio-Thoracic Department University of Milan, Italy COPD OUTCOMES Cazzola M et al. ERJ 2008 COPD AND CARDIOVASCULAR DISEASE Cumulative
COPD EXACERBATIONS Francesco Blasi Head Respiratory Medicine Section Cardio-Thoracic Department University of Milan, Italy COPD OUTCOMES Cazzola M et al. ERJ 2008 COPD AND CARDIOVASCULAR DISEASE Cumulative
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
pneumonia The management of community-acquired The prevalence of community-acquired pneumonia
 The management of community-acquired pneumonia Pneumonia is a significant cause of mortality in children and older people, particularly among Māori and Pacific Peoples. In New Zealand, Māori are six times
The management of community-acquired pneumonia Pneumonia is a significant cause of mortality in children and older people, particularly among Māori and Pacific Peoples. In New Zealand, Māori are six times
Rhinosinusitis. John Ramey, MD Joseph Russell, MD
 Rhinosinusitis John Ramey, MD Joseph Russell, MD Disclosure Statement RSFH as a continuing medical education provider, accredited by the South Carolina Medical Association, it is the policy of RSFH to
Rhinosinusitis John Ramey, MD Joseph Russell, MD Disclosure Statement RSFH as a continuing medical education provider, accredited by the South Carolina Medical Association, it is the policy of RSFH to
Around-COPD Verona (Italy), January Highlights
, January Highlights") Introduction Around-COPD Verona (Italy), January 18 2017 Highlights Prof. Dal Negro chairman of the symposium, opened the congress by highlighting the burden of COPD as a chronic invalidating disease affecting
Introduction Around-COPD Verona (Italy), January 18 2017 Highlights Prof. Dal Negro chairman of the symposium, opened the congress by highlighting the burden of COPD as a chronic invalidating disease affecting
PNEUMONIA. Introduction
 PNEUMONIA Introduction While most respiratory infections in children are acute upper respiratory infections, children presenting to hospital emergency departments commonly have lower tract respiratory
PNEUMONIA Introduction While most respiratory infections in children are acute upper respiratory infections, children presenting to hospital emergency departments commonly have lower tract respiratory
Airway Vista Background
 Airway Vista 2013 Chronic Obstructive Airway Diseases Symposium Asan Medical Center, Seoul, South Korea When Should Macrolide Antibiotics be Prescribed to Prevent COPD Exacerbations in Usual Clinical Practice?
Airway Vista 2013 Chronic Obstructive Airway Diseases Symposium Asan Medical Center, Seoul, South Korea When Should Macrolide Antibiotics be Prescribed to Prevent COPD Exacerbations in Usual Clinical Practice?
Update on Biologicals for ABPA and Asthma
 Update on Biologicals for ABPA and Asthma 5 th Advances Against Aspergillosis Istanbul 27 Jan 2012 Richard B. Moss MD Professor of Pediatrics Stanford University Palo Alto CA USA Disease of chronic airway
Update on Biologicals for ABPA and Asthma 5 th Advances Against Aspergillosis Istanbul 27 Jan 2012 Richard B. Moss MD Professor of Pediatrics Stanford University Palo Alto CA USA Disease of chronic airway