WADA STATEMENT ON THE SALBUTAMOL THRESHOLD/DECISION LIMIT
|
|
|
- Gavin Todd
- 5 years ago
- Views:
Transcription
1 NOTE: AS REFERENCED IN WADA'S MEDIA RELEASE OF 11 JULY 2018, ON 15 MAY, WADA PROVIDED THE FOLLOWING NOTE TO UCI ON THE SALBUTAMOL REGIME, ADDRESSING THE SUBSTANCE OF MR. FROOME S QUESTIONS. WADA STATEMENT ON THE SALBUTAMOL THRESHOLD/DECISION LIMIT 1. HISTORICAL BACKGROUND 1.1 The List Pre-World Anti-Doping Code 15 MAY 2018 Before January 2004, the International Olympic Committee (IOC) was responsible for establishing the antidoping rules on behalf of the international sport movement. The IOC List of Prohibited Substances and Prohibited Methods (IOC List) was an annex to the Olympic Movement Anti-Doping Code (OMAC). According to WADA s records, salbutamol was included in the IOC List as a prohibited stimulant in 1991, with the anabolic properties of salbutamol being acknowledged in the 1994 IOC List. In the final IOC List in 2003, salbutamol was prohibited in Section A, subsection b (Stimulants), which indicated that Prohibited substances in class A.b include the following examples with both their L- and D- isomers : formoterol***, salbutamol***, salmeterol*** and terbutaline*** and related substances. This List also included a footnote in the section B, Anabolic Agents, which clarified ***permitted by inhaler only to prevent and/or treat asthma and exercise induced asthma. Written declaration of asthma and/or exercise-induced asthma by a respiratory or team physician is necessary to the relevant medical authority. In addition, salbutamol was also prohibited in Section C.2 as Other anabolic agents and a footnote read that For salbutamol, a concentration in urine greater than 1000 nanograms per milliliter of non-sulphated salbutamol constitutes a doping violation. In this regard, section IV of the 2003 IOC List entitled Summary of urinary concentrations above which a doping violation has occurred indicated Salbutamol (as anabolic agent) > 1,000 nanograms/milliliter. On the basis of the above, even before 1 January 2004, when the World Anti-Doping Code (WADC) and its related International Standards, including the International Standard for the List of Prohibited Substances and Methods (Prohibited List), came into force, salbutamol was prohibited for urinary concentrations higher than 1,000 ng/ml (i.e. 1 µg/ml), and its use required the athlete to provide an explanation of their respiratory medical condition to the sport authorities. The IOC threshold of 1,000 ng/ml was established as a conservative cut-off to distinguish between inhaled (permitted) and oral (prohibited) administration of salbutamol 1. It was derived from routine doping 1 The introduction of the 1,000 ng/ml threshold to distinguish oral from inhaled use of salbutamol reflected findings from numerous animal and human studies, which showed anabolic properties of β2-agonists when administered by systemic routes but not following the intake of therapeutic dosages by inhalation. In this regard, in humans, oral salbutamol increased performance and affected metabolism and selected anabolic hormones during submaximal cycling to exhaustion (Collomp et al., 2000 a & b; van Baak et al, 2000) and augmented strength in resistance training
2 control analytical data, which the IOC had compiled over many years, the published salbutamol excretion studies available at the time (see below), as well as a number of cases that the IOC Medical Commission had reviewed when in charge of the anti-doping rules. By the early 2000s, the Barcelona anti-doping laboratory published two excretion studies (Ventura et al., 2000; Berges et al., 2000) conducted with asthmatic and non-asthmatic volunteers, who had been exposed to 200, 400 or 1600 µg of inhaled salbutamol and 4, 16 or 20 mg of oral salbutamol. No volunteer using inhaled salbutamol in those studies exceeded 1,000 ng/ml in urine when non-sulfated (Ventura et al, 2000) or free enantiomeric salbutamol (Berges et al, 2000) were measured by gas chromatographymass spectrometry (GC-MS) (Ventura et al, 2000) or high performance liquid chromatography mass spectrometry (HPLC-MS) (Berges et al, 2000). On the basis of the results of these studies, the research teams recommended establishing a urinary threshold at 500 ng/ml of non-sulfated or free racemic salbutamol to distinguish oral from inhaled use. In addition, Berges et al proposed determining the ratio of S(+) to R(-) free salbutamol enantiomers, and to use a discriminant function when urinary concentrations were higher than 500 ng/ml to distinguish between routes of administration. Consequently, in 1999, the IOC introduced a threshold of 500 ng/ml of salbutamol to distinguish between inhaled and oral administration and a year later, in April 2000, this threshold was increased to 1,000 ng/ml, which was considered a conservative level (Fitch, 2006). Therefore, by 2001, under the applicable IOC rules, any case with urinary concentrations higher than the 1,000 ng/ml threshold was considered an anti-doping rule violation. In 2004, a case report published by Schweizer et al. from the Lausanne laboratory claimed that an athlete had surpassed the 1,000 ng/ml threshold value and recommended a review of this value. After further discussion between WADA and the authors, it was noted that there had not been a strict control of the dose intake during the study; moreover, assuming that the athlete had inhaled 900 µg of salbutamol in 5 hours, this was clearly not in accordance with medical guidelines for the treatment of asthma. 1.2 Evolution of the rules for β2-agonists and more specifically salbutamol under the WADC Prohibited List As of 1 January 2004, when the WADC and its associated International Standards came into force, WADA became responsible for the harmonization of anti-doping policies worldwide. During the initial stages, (Martineau et al., 1992; Caruso et al, 1995). During that period, studies done in animal models showed, for example, that systemic salbutamol induced skeletal muscle hypertrophy and increased muscle mass (Carter & Lynch, 1994; Cepero et al., 1998 & 2000) and antagonized cachexia (Carbo et al., 1997). Following the adoption of the WADC and the publication of the Prohibited List by WADA, a number of other studies continued to show the performance enhancing effects of oral salbutamol, including, for example, resistance exercise and maximal anaerobic power (Caruso et al, 2005 & 2008; Le Panse et al., 2005, 2006 & 2007; Collomp et al., 2005; Hostrup et al., 2016).
3 WADA had to ensure continuity in anti-doping practice and incorporated many of the rules included in the OMAC, in particular for the prohibited substances and methods, to avoid major disruptions in doping control and confusion for its stakeholders. More specifically for salbutamol, the WADA List Expert Group (LiEG), supported by the WADA Health, Medical and Research Committee (HMRC) and by the WADA Executive Committee, agreed to maintain the prohibition of salbutamol when measured in excess of a urinary threshold concentration of 1,000 ng/ml (the Threshold ). Accordingly, in the 2004 Prohibited List, under section S6 (Beta2 agonists), it was stipulated that All beta2 agonists including their D- and L-isomers are prohibited except that formoterol, salbutamol, salmeterol and terbutaline are permitted by inhalation only to prevent and/or treat asthma and exercise-induced asthma/bronchoconstriction. A medical notification in accordance with section 8 of the International Standard for Therapeutic Use Exemptions is required. Section S6 continued with the following paragraph: Despite the granting of a TUE, when the laboratory has reported a concentration of salbutamol (free plus glucuronide) greater than 1,000ng/mL, this will be considered as an adverse analytical finding unless the athlete proves that the abnormal result was the consequence of the therapeutic use of inhaled salbutamol. On the basis of the foregoing, the WADA approach to the regulation of salbutamol allowed athletes who exceeded the urinary threshold of 1,000 ng/ml to demonstrate that the result had resulted from inhaled, therapeutic use. Other than changing β2-agonists from category S6 to S3 in January 2005, which was a purely administrative change, from 2005 to 2009 there were no major changes and only minor adjustments to the wording of the β2-agonists section of the Prohibited List, including for salbutamol. As time passed, it was observed by WADA that many salbutamol prescriptions, received as part of Therapeutic Use Exemption (TUE) applications, were labeled as needed or as required, with no maximum daily dose indicated. To address this situation, WADA introduced the notion of the maximum inhaled daily therapeutic dose of salbutamol that athletes could take, in line with the manufacturer s recommendations, in the 2010 Prohibited List 2. By taking this approach, athletes could use inhaled salbutamol without a TUE; however, it limited such use to approved therapeutic doses, thus minimizing the risk of overdosing and surpassing the urinary threshold. 3 The maximum daily dose was based on the salbutamol manufacturer s recommendation for a therapeutic regime by inhalation and as described in reference pharmacopeias (e.g. see MIMS Ireland, 2004; Compendium of Pharmaceuticals and Specialties 2005; Martindale 2011). It was introduced to address 2 Section S3. β2-agonists of the 2010 Prohibited List indicated: All beta-2 agonists (including both optical isomers where relevant) are prohibited except salbutamol (maximum 1600 micrograms per 24 hours) and salmeterol by inhalation which require a declaration of Use in accordance with the International Standard for Therapeutic Use Exemptions. 3 However, the principle of a urinary threshold concentration for salbutamol was strictly maintained in the 2010 Prohibited List: The presence of salbutamol in urine in excess of 1,000 ng/ml is presumed not to be an intended therapeutic use of the substance and will be considered as an Adverse Analytical Finding unless the Athlete proves through a controlled pharmacokinetic study, that the abnormal result was the consequence of the use of a therapeutic dose (maximum 1600 micrograms over 24 hours) of inhaled salbutamol.
4 the problem of athletes using inhaled salbutamol in excessive doses after being prescribed an as needed or as required regimen of salbutamol. In addition, the possibility of a controlled excretion study had been introduced for the first time in the 2009 Prohibited List, acknowledging de facto the inter-individual variability in the excretion of salbutamol observed in recent research studies. The clarification of the origin of the 1600 g/day maximum daily dose for inhaled salbutamol was introduced in the 2011 Prohibited List with the reference in the core text to in accordance with the manufacturers recommended therapeutic regime. In other words, not only was there a maximum of 1600 g/day but this dose was to be taken in accordance with the therapeutic regime (e.g. not as a single dose). Subsequently, from 2012 to 2016, the wording for salbutamol in section S3 of the Prohibited List remained unchanged, with the exception of minor cosmetic adjustments. In 2017, the number of examples of β2-agonists in the Prohibited List was expanded to specifically mention the names of other substances that fell within this non-exhaustive category (i.e., higenamine). Also, for salbutamol in particular, it was specified that the maximum daily dose of 1600 micrograms over 24 hours was not to exceed 800 micrograms every 12 hours. This rule was introduced to be more in line with good medical practice in terms of therapeutic use of salbutamol (GINA; Parsons et al 2013), as well as to address observations from recent studies indicating that the inhalation of salbutamol in high dosages, over a short period of time, could lead, in some cases, to urinary concentrations in excess of the Decision Limit of 1,200 ng/ml 4 (Dickinson et al, 2014; Haase et al., 2016). In 2018, a more precise requirement for the maximum allowed daily dose of salbutamol was included in the Prohibited List that is currently in force. It reads: salbutamol, maximum 1600 micrograms over 24 hours in divided doses not to exceed 800 micrograms over 12 hours starting from any dose. For both the 2017 and 2018 Prohibited Lists, explanations were provided in the respective Summary of Modifications, which accompanied the publication of each of the Prohibited Lists, in order to better inform and guide the sports community on the appropriate use of salbutamol to avoid excessive dosing and potential adverse analytical findings (AAFs; Summary of Modifications, 2017 and 2018). In parallel to reviewing the Prohibited List on an annual basis, from the outset, WADA specifically reviewed the thresholds of the relevant substances with the aim of refining and consolidating the applicable values as required. This was particularly the case for β2-agonists and more specifically for salbutamol as early as , when WADA started to commission research teams to generate original data on salbutamol excretion. 1.3 Consolidation of the salbutamol threshold over the years As indicated above, the IOC rules on salbutamol prescribed that any finding for a urinary concentration of salbutamol higher than 1,000 ng/ml was considered as an anti-doping rule violation. However, as also mentioned, it was very clear in the context of use of salbutamol that many athletes were prescribed 4 The concept of Decision Limit is explained in section 3.2 below.
5 salbutamol as needed or as required, as reported on their TUE applications. Such use was not in line with good medical practice for treatment of asthma (e.g. GINA Guidelines) and created a significant risk of overexposure to salbutamol. As a result, it was possible for athletes to surpass the anti-doping analytical threshold when excessive doses of inhaled salbutamol were used, even if the athlete was following a legitimate physician s prescription. As early as September 2003, shortly before WADA became responsible for establishing the Prohibited List, WADA undertook a review of the relevance of the 1,000 ng/ml threshold and commissioned, under its research program, excretion studies with the support of Prof McKenzie s research team. Two studies were conducted with inhaled single doses of salbutamol of 200, 400 and 800 g (Sporer et al. 2008a and 2008b). Even though the administration was by a one-off single dose and not spread over several hours, none of the volunteers exceeded the 1,000 ng/ml threshold in those studies. In addition, in 2006, Pichon and colleagues published an article with volunteers exposed to 200 g, 3 times/day over three days in order to distinguish the results of a preventive treatment for exerciseinduced asthma from doping practices. Based upon the low excreted salbutamol concentrations, the conclusion of the study was that the urinary salbutamol threshold should be lowered to 250 ng/ml. In the following years, WADA continued to support studies on inhaled and oral use of salbutamol and its effect on athletic performance, as well as to further explore the relationship between inhaled doses and urinary excretion of this β2-agonist. Several WADA-sponsored studies were conducted by the group of V. Backer in Copenhagen from 2008 to today, aiming at better defining the relationship between various regimens of β2-agonists and the pharmacokinetics of their urinary excretion. In these studies by Backer, doses of 800 g 4 x 200 g and 1 x 800 g), 1600 g 4 x 400 g) 8 mg 40 x 200 g of inhaled salbutamol were administered to asthmatic or non-asthmatic volunteers or noncompeting athletes in various sports (Mareck et al ; Elers et al. 2010, Elers et al. 2011; Elers et al., 2012a). All the studies concluded that urinary concentrations of salbutamol were below the Decision Limit. The Decision Limit was only breached in one study designed to administer inhaled salbutamol equivalent to an oral dose (40 x 200 g = 8 mg) (Elers et al., 2012b), which was consistent with concentrations found following oral administration of 8 mg (Pichon et al., 2006; Mareck et al ; Elers et al. 2010; Hostrup et al., 2014). As a world-renowned expert in the field, Prof. Vibeke Backer was invited to present and discuss the results of her research studies at the April 2013 meeting of the LiEG. In parallel to WADA s sponsored studies on salbutamol excretion, a study of Elers and colleagues published in 2010 (Elers et al., 2010) exposed volunteers to 800 g of inhaled salbutamol and concluded that the results support that a limit of 1,000 ng/ml is sufficiently high to secure a low risk false positive but noted that 50% false negative were observed with oral administration of 8 mg salbutamol. Other studies observed that the Decision Limit meant that a number of samples would be considered as negative following oral (prohibited) administration of salbutamol (Ventura et al., 2000; Mareck et al., 2011; Elers et al., 2012a; Hostrup et al, 2014). Correction of some of the diluted samples for the urinary specific gravity
6 (SG) of 1.020, as suggested by the authors, would render the concentrations of salbutamol above the Decision Limit and flag these samples as AAFs following the prohibited administration of salbutamol. (Hostrup et al., 2014). In recent years, WADA has continued its efforts to explore the conditions influencing salbutamol excretion by commissioning additional studies with different research teams. In particular, salbutamol administration studies conducted by the groups of Backer and Dickinson investigated the effect of exercise, hot environment and dehydration, as factors that could affect the excretion of salbutamol in urine (Dickinson et al, 2014 a; Dickinson et al., 2014 b; Haase et al., 2016). In these studies, single doses of 800 g or 1600 g inhaled salbutamol were administered, and the analysis of salbutamol excreted in urine confirmed the high inter-individual variability of salbutamol urinary excretion and revealed that when high doses of 1600 g were administered in one intake (and in combination with exercise and dehydration), some individuals could temporarily exceed the Decision Limit (0 out of 7 in Dickinson et al., 2014b; 16 of 30 in Dickinson et al., 2014a; and 17 of 117 (with correction for SG) in Haase et al., 2016). Despite these results, the authors considered that the limits established by WADA were adequate to distinguish inhaled use of salbutamol in therapeutic doses from over-dosing by inhalation or oral administration of salbutamol (Dickinson et al 2014 a & b). At about the same time, another study was published by Pillard and colleagues (Pillard et al., 2015), in which inhaled salbutamol was administered for four (without exercise) and five (with exercise) consecutive days at 200 g every 6 h three times per day (total daily dose 600 g) following GINA and ATS guidelines. The study recommended lowering the salbutamol threshold to 507 ng/ml and correcting the urinary concentrations for the SG of the urine sample. The most recent studies conducted under the WADA research program, in particular by the groups of Backer and Jacobson (ongoing and unpublished studies), were primarily aimed at studying the pharmacokinetics of several β2-agonists when administered by inhalation alone or in combination, as well as to evaluate the measuring of enantiomeric salbutamol as a means to distinguish oral from inhaled administration. In Jacobson s study, following the administration of acute or chronic high doses (800 g or 1600 g) of inhaled salbutamol, some samples appear to have exceeded the Decision Limit. However, the exact conditions in which such situations occurred remain unclear (clarifications are currently being sought from the investigator). In the Backer study, following a unique dose of 1600 g inhaled salbutamol (alone or in combination with other β2-agonists), 6 out of 37 samples exceeded the Decision Limit and this number was reduced to 4 when concentrations were corrected for SG. No sample exceeded the Decision Limit 6 h after administration. However, as noted by Backer, it can be expected that many of the samples that exceeded the Decision Limit in that study would not have done so under the current rule that prohibits exceeding 800 g of inhaled salbutamol over 12 hours. 1.4 Measurement of salbutamol urinary concentration Salbutamol is excreted in urine as a combination of unchanged (parent compound) and phase-ii metabolites (mainly as the sulfated metabolite). The relative proportion of the different molecular forms depends on dosage and route of administration, as well as on the genetics of the individual, as judged by
7 the observed inter-individual variability in salbutamol excretion. Due to the first-pass metabolism in the gastrointestinal tract, the proportion of sulfated salbutamol excreted in urine is higher (~ 50%) after oral administration (Morgan et al., 1986; Hussey, Donn and Powell, 1991). Salbutamol is not metabolized extensively in the lungs (Hindle and Chrystyn, 1992); therefore, following inhalation, salbutamol is mainly excreted as the parent compound, while the glucuronidated metabolite may be excreted in much lower proportions (Mareck et al., 2011). However, a significant fraction (up to 60-70%) of inhaled salbutamol may be swallowed (depending on user experience, delivery device, etc.), which would lead to an increased proportion of the sulfated metabolite excreted in urine. In doping control, measurement of urinary concentrations of salbutamol is based upon the determination of the free (unchanged) and glucuroconjugated fractions of salbutamol. Historically, the analysis has been done by gas chromatography-mass spectrometry (GC-MS), following the pre-treatment (hydrolysis) of the sample using an enzyme (glucuronidase) in order to excise the glucuronide moiety of the minor phase-ii metabolite. As a result, non-sulfated salbutamol content, including the unchanged parent compound and the free salbutamol released from the glucuroconjugated metabolite, is quantified. As mentioned in sections 1.1 and 1.2 above, the IOC, pre-wada 1,000 ng/ml threshold for salbutamol had been determined based on the measurement of non-sulfated salbutamol by GC-MS. WADA continued to apply this approach, and these target analytes were also analyzed in the later excretion studies described in paragraph 1.3 above, which have been used to monitor the WADA-established Decision Limit for salbutamol. Nevertheless, the relevance of the sulfate fraction has been indirectly explored through a few studies using chiral analysis (Berges et al., 2000, and two WADA-sponsored studies (Fiacco et al., 2012 and Jacobson-unpublished results). In this regard, the R(-) enantiomer undergoes a higher rate of sulfation after oral intake, therefore the non-metabolized S(+) enantiomer would be excreted in a greater proportion than the non-metabolized R(-) (Boulton et al 1996; Walle et al., 1993). Results from Fiacco s study confirmed the initial results by Berges et al. in 2000 on the feasibility of the chiral analysis; however, it concluded that the ratios of the non-metabolized or metabolized (sulfated fraction) salbutamol enantiomers would not have a marked benefit to distinguish permitted and prohibited administrations of salbutamol, since it strongly depended on the percentage of the inhaled dose that is swallowed. In the study by Jacobson, analysis of chiral ratios only provided a modest increase in diagnostic performance over existing approaches. 2. CONCEPT OF THE CONTROLLED EXCRETION STUDY It is important to note that, starting from the first WADA Prohibited List in 2004, the Threshold of 1,000 ng/ml was no longer considered as a strict Threshold because, unlike for some other threshold substances (e.g. hgh, pseudoephedrine), surpassing the Threshold did not automatically lead to the assertion of the
8 finding as an AAF 5. It was considered by WADA from the outset that the 1,000 ng/ml is a reasonable value to allow appropriate medical use of inhaled salbutamol by the vast majority of asthmatic athletes while deterring the risk of abuse of salbutamol by inhalation in excessive doses or by systemic routes of administration. In other words, in a situation where there is overlap in the urinary concentrations of salbutamol following its use by allowed or prohibited routes of administration, WADA s objective was to define a Threshold, which would permit the therapeutic use of inhaled salbutamol while serving as a means to deter the abuse of this substance by prohibited, performance-enhancing routes of administration. Numerous studies have revealed the high variability in salbutamol urinary excretion between individuals. As known for some other substances, it appears that some individuals would have a stronger propensity than others to excrete higher concentrations of free salbutamol when exposed to a similar regime of administration of this substance. To account for the possibility of different metabolizers, even if rare, the Prohibited List allows athletes to request a controlled excretion study when salbutamol urinary concentrations exceed the Decision Limit of 1200 ng/ml. This offers the athlete the possibility to demonstrate that his/her unusual personal metabolism leads to a higher excretion of salbutamol (i.e. above the Decision Limit) even when salbutamol is taken by inhalation following an appropriate therapeutic regime. It is important to note than any athlete with a urinary concentration higher than the Decision Limit for salbutamol can request a controlled excretion study. The study can be conducted in a WADA-accredited laboratory that has the capability to handle the protocol of such a study. Controlled excretion studies will aim at reproducing the conditions of intake of salbutamol (e.g. doses, frequency, time intervals) as well as any other reasonable known (i.e. demonstrable) conditions or circumstances that could reasonably have caused the salbutamol AAF. 3. INTEGRATION OF THE MEASUREMENT UNCERTAINTY 3.1 Compliance decisions for Threshold Substances: Thresholds, Measurement Uncertainties and Decision Limits The standards of Laboratory performance of the WADA-accredited laboratories are defined in the WADA International Standard for Laboratories (ISL) and its associated Technical Documents (TDs). These sets of rules aim to harmonize the production of valid test results and evidentiary data and the reporting of analytical findings. 5 The 2004 Prohibited List indicated, in section S6. Beta-2 Agonists: Despite the granting of a TUE, when the Laboratory has reported a concentration of salbutamol (free plus glucuronide) greater than 1000 ng/ml, this will be considered as an adverse analytical finding unless the athlete proves that the abnormal result was the consequence of the therapeutic use of inhaled salbutamol.
9 Prohibited Threshold Substances are substances, included in the Prohibited List, for which an AAF can be reported only if they are detected in a concentration that is in excess of a defined Threshold value. Therefore, the confirmatory analyses for the presence of prohibited Threshold Substances requires the application of fully quantitative tests, which produce analytical results with sufficient accuracy and statistical confidence to allow unequivocal application of anti-doping regulatory compliance decisions. Such specific compliance decision rules are currently established in the WADA TD on Decision Limits (TDDL), which is based on the application of GUM (Guide to the Expression of Uncertainty in Measurement) principles described in the EURACHEM/CITAC Guide on Use of Uncertainty Information in Compliance Assessment 6. In this context, it is important to understand the difference between a Threshold and a Decision Limit, explain the role of the uncertainty of the measurement in the calculation of the Decision Limit, and describe how these concepts have been historically applied in the anti-doping testing field. Several empirical approaches may be used for establishing the Threshold for prohibited Threshold Substances, depending on the origin of the substance (exogenous or endogenously produced by the body) and whether it is prohibited at all times or only in-competition. Thus, for salbutamol (an exogenous β2- agonist prohibited at all times, except if taken by inhalation in a dose not exceeding 800 µg every 12 hours), the Threshold was established by the IOC prior to the first Prohibited List and WADC coming into force in 2004 (as described above in section 1.1). The Threshold, set at a concentration value of 1,000 ng/ml (of parent compound plus its glucuroconjugated form) allows, to a great extent, differentiating permitted use by inhalation from abuse at supratherapeutic inhaled doses or administration by prohibited routes (e.g. oral). This Threshold was further verified by controlled excretion studies, in which the drug was administered to healthy individuals in permitted, inhaled therapeutic doses (see, in particular, section 1.3 above). In order to report an AAF for a Threshold Substance, the result of the analysis shall demonstrate that the concentration of the Threshold Substance in the sample exceeds the Threshold with a certain level of statistical confidence (at least 95%). In this regard, two different approaches have been historically applied by WADA when defining compliance decision rules for Threshold Substances. 3.2 Rule applied until 1 September 2010 The ISL v 6.0 from Jan 2009 (and similar previous versions of the ISL) established, in Article that The mean value of the results of three Aliquots for the A Sample finding for Threshold Substances minus the value of the measurement uncertainty determined by the Laboratory [underwritten for emphasis] must exceed the relevant Threshold. 6 EURACHEM/CITAC Guide. Use of uncertainty information in compliance assessment. First edition. Ellison SRL, Williams A (Eds) (2007). uncertainty_2007_v1.pdf
10 This compliance rule to determine an AAF for Threshold Substances can be mathematically expressed as: where: y - U95% > T y: mean concentration of the substance obtained from measuring 3 Aliquots of the A Sample (i.e. the measurement result); U95%: the expanded uncertainty of the measurement result 7 ; T: the threshold for the substance (e.g. 1,0 µg/ml for Salbutamol) The expression of the measurement result y and its expanded uncertainty U as y ± U95% defines an interval within which the true value of the target analyte in the sample is believed to lie with a 95% level of confidence. Therefore, if y - U95% is higher than the Threshold, then it can be concluded that the measurement result y exceeds the Threshold with at least 95% statistical confidence, and therefore such result shall be reported as an AAF. However, this approach, while scientifically and methodologically correct, had an important drawback for anti-doping applications. In the early stages after the introduction of the WADA External Quality Assessment (EQAS) program, it became evident that the differences between Laboratories in the estimation of the MU for Threshold Substances were considerable. It was clear that guidance was required to estimate the MU of the measurement and to decide with reasonable certainty when the Threshold was exceeded to declare an AAF. In other words, whereas there was a clearly defined Threshold for each Threshold Substance, compliance decisions could vary between Laboratories based on their different estimates of the MU: while in one Laboratory a given result expressed as y - U95% may have constituted an AAF, in a second Laboratory, with a higher MU estimate, this same measurement result would have been reported as negative. This created a perception of unfairness and confusion amongst athletes and other WADA stakeholders. 3.3 Rule applied from 1 September 2010 On 1 September 2010, the first version of the WADA TD on Decision Limits for the Confirmatory Quantification of Threshold Substances (TD2010DL) became effective. The scope of the document was to 7 The Measurement Uncertainty (MU), expressed either as the combined standard uncertainty uc or the expanded uncertainty U95% (which defines an approximate 95% confidence range in which the true value of the measurement result is expected to be found, and is obtained by multiplying the uc by a coverage factor k = 2) defines the quality or fitness-for-purpose of a measurement. It provides an objective basis for demonstrating the equivalence of results obtained by different laboratories and for the assessment of conformity with a threshold value. The estimation and use of the MU associated with results obtained by a quantitative procedure is a requirement that the anti-doping laboratories must fulfill as part of their quality assurance measures (in compliance with ISO/IEC accreditation as well as with the ISL). It serves to establish the necessary confidence in the validity of the measurement results, and ensure that they provide analytical data of the expected quality.
11 harmonize the rules for the reporting of AAFs for Threshold Substances and described the use of MU information in the establishment of Decision Limits. In principle, the same compliance decision rule still applied (i.e. that the concentration of the Threshold Substance in the sample had to exceed the Threshold with at least 95% statistical confidence). However, in order to ensure harmonization of the application of this rule across all WADA-accredited Laboratories, the concepts of Decision Limits and Maximum Acceptable Combined Standard Uncertainty (u c Max) were introduced. The u c Max for each Threshold Substance constitutes the minimum requirement to be achieved by a Laboratory for their MU (as estimated at levels close to the Threshold concentration during method validation) when reporting a result for the determination of a Threshold Substance. Whatever approach is applied by the Laboratories to estimate the MU, their estimated uc value at levels close to the Threshold shall not be higher than the uc-max specified in the TD DL. Since the uc at levels close to the Threshold shall not be higher than the uc-max, the reporting of the Laboratory s uc serves to demonstrate that the Laboratory performs the analytical procedure to determine the Threshold Substance according to the technical specifications of assay accuracy and precision. For determination of the u c-max, as defined in the TD DL, WADA relies on data obtained from its EQAS program. It is considered that these types of data include contributions from all relevant sources of uncertainty and provide a conservative overall estimate of u c, which is suitable for the intended purpose of establishing a Decision Limit above which an AAF shall be reported. Thus, the (robust) standard deviation (inter-laboratory precision, sr) of the participant Laboratories results obtained from the analysis of representative samples in the EQAS can be used as a conservative estimate of the uc associated with an individual result. The Decision Limit defines the value for the measurement result, obtained from testing an individual sample using a fit-for-purpose quantitative procedure, above which it can be concluded that the true value for the substance in the sample exceeds the Threshold with a statistical confidence of at least 95%. For calculating the Decision Limit, a guard zone (g) is added to the value of the Threshold established for a particular prohibited Threshold Substance. This guard zone takes into account the analytical uncertainty in the reported value when the method is applied to samples that contain the analyte at or near the Threshold level. Since the critical determination is whether a value measured has exceeded the established Threshold with a confidence level of at least 95%, the value of the guard band is calculated by multiplying the uc-max for a result at levels close to the Threshold (as defined from EQAS data and specified in the TD DL), by an applicable coverage factor k. For a one-tailed normal distribution 8 with a 8 Note that, in this case, a one-tailed (i.e. one-sided) distribution is applied (which defines the coverage factor k at 1.645) since the important element is to determine whether the result is higher than the Threshold with 95% confidence. In other words, the only values that need be considered are those lying on one side (i.e. higher than) of the Threshold value. In the first approach, a coverage factor k of 2 is used to determine the U95%, since in this case a two-tailed (i.e. 2-sided) distribution is needed to determine the interval (on both sides of the measured value) where the true value is expected to be found.
12 95% coverage range, this coverage factor would correspond to Furthermore, the calculated value of the Decision Limit (i.e. calculated as T plus u c Max) is rounded up to 2 significant figures. This compliance decision rule to determine an AAF for Threshold Substances can be mathematically expressed as: where: y > DL, i.e. y > T uc-max y: mean concentration of the substance obtained from measuring 3 Aliquots of the A Sample (i.e. the measurement result); uc-max : maximum allowed uncertainty at levels close to the threshold, as determined by WADA from data obtained from Laboratory analysis of representative EQAS samples T: the threshold for the substance. Applying this formula to the determination of salbutamol, considering the T = 1,000 ng/ml and a u c-max of 100 ng/ml (i.e. 10% of the T), results in a value of 1,160 ng/ml, which after rounding up to 2 significant figures produces a Decision Limit at 1,200 ng/ml. Therefore, any sample with a urinary concentration of salbutamol higher than 1,200 ng/ml is considered to have exceeded the Threshold with a statistical confidence of at least 95%, and shall be reported as an AAF for salbutamol. This approach, while methodologically equivalent to the first approach applied before 1 September 2010, ensured a better harmonization of the reporting of results by Laboratories through: 1- The definition of a unique Decision Limit for each Threshold Substance, to be applied by all Laboratories; and 2- The establishment of a maximum acceptable value of the MU, ensuring the accuracy and precision of Laboratory quantitative determinations to the levels expected to conclude an AAF with at least 95% confidence when the measured value of the Threshold Substance in the sample exceeds the Decision Limit. This compliance decision rule, initially set out in the TD2010DL, was later included in the revised ISL v 7.0 from January 2012, which established in Article that For Threshold Substances, Adverse Analytical Finding or Atypical Finding decisions for the A Sample finding shall be based on the mean of the measured analytical values (e.g. concentrations) of three Aliquots which shall exceed the value of the relevant Decision Limit. In conclusion, in order to include a robust Decision Limit for several quantitative analyses in the field of anti-doping, the laboratory experts proposed a harmonized approach in line with international guidelines which led to a systematic application of a requisite 95% of confidence applied to the established thresholds of all quantitative analysis in anti-doping. For the specific case of salbutamol, this interval of confidence applied the Threshold of 1,000 ng/ml and established a Decision Limit at 1,200 ng/ml. In routine practice, any urinary concentration of salbutamol below the Decision Limit of 1,200 ng/ml is not considered an AAF and therefore not reported by WADA accredited laboratories as such. Conversely, any
13 urinary concentration of salbutamol above the Decision Limit of 1,200 ng/ml shall be reported by antidoping laboratories as an AAF. 4. SPECIFIC GRAVITY The measurement of SG is a means to take into account the concentration of the athlete s urine samples and indirectly reflects the hydration status of the athlete at the time of the sample collection. Historically, SG correction was applied for the quantitative analysis of endogenous threshold substances when values of SG were higher than (which is considered to be the reference SG value for a normally hydrated athlete). This approach benefited athletes, since concentrations would only be corrected in cases of concentrated urine (therefore resulting in a lower adjusted concentration), while the same correction was not applied to diluted urine (which would result in higher adjusted concentrations). The LabEG recently decided to propose a systematic correction of concentrations for all threshold substances (endogenous and exogenous, including salbutamol) when SG is higher than This decision was introduced in the TD2018DL, which was approved by the WADA Executive Committee in November 2017 with a deadline for implementation (i.e. effective date) on 1 March CONCLUSIONS The Threshold of 1,000 ng/ml for salbutamol was adopted from the IOC rules in place before 1 January 2004 to distinguish permitted therapeutic inhaled use of salbutamol from abuse by excessive inhalation or oral administration. However, one important change that WADA made from the outset was that exceeding the urinary threshold concentration was no longer automatically considered as an anti-doping rule violation. This change reflected the possibility that certain athletes could, albeit rarely, exceed the Threshold in view of their particular metabolism of salbutamol (in particular, when no maximum allowed dose had been set yet and medical prescriptions often referred to use as needed ). The Threshold value of 1,000 ng/ml has been constantly reviewed and confirmed as appropriate over the years by multiple research studies conducted by different investigators, many of which had been commissioned by WADA. It is well acknowledged that due to inter-individual variability in the excretion of salbutamol, the Threshold at 1,000 ng/ml and Decision Limit at 1,200 ng/ml are not hard values, which could be used to unequivocally determine an anti-doping rule violation, as can be the case for other threshold substances. One of the primary purposes of this soft Threshold is to distinguish between systemic use (where there is evidence of anabolic effects) and therapeutic use by inhalation. Studies have consistently revealed that the vast majority of athletes taking salbutamol within the maximum allowed therapeutic inhaled dose will not exceed the Decision Limit. In contrast, it has been demonstrated that a proportion of athletes taking salbutamol by prohibited systemic routes will excrete salbutamol in urine at concentrations below the Decision Limit; this has resulted over the years in numerous calls for the Decision Limit to be reduced.
14 In conclusion, the Threshold/Decision Limit for salbutamol does not purport categorically to distinguish between two mutually exclusive options such as doping and not doping. Rather, this Decision Limit has been established at a reasonable level to allow the use of inhaled salbutamol therapeutically by athletes without the need to apply for a TUE and with a minimal risk of producing an AAF. At the same time, this Decision Limit acts as an adequate detector and deterrent of the abuse of salbutamol for performance enhancement purposes. After years of research, monitoring and verification of the salbutamol system since the IOC model, various generations of WADA s LiEG members have considered the Threshold of 1,000 ng/ml and later the Decision Limit of 1,200 ng/ml to be at an appropriate level to achieve this dual purpose. It is important to understand that this balancing act is, to some extent, a qualitative exercise integrating the specific anti-doping expertise of the specialists that are called upon to make this determination, in particular the LiEG, but also the HMRC experts and, ultimately, the members of the WADA Executive Committee as representatives of the sport and government interests in the fight against doping in sport. For analytical results exceeding the Decision Limit, the possibility of conducting a controlled excretion study, simulating as much as reasonably practicable the known conditions on the day of the positive doping test, is a step accessible to all athletes. This allows the athlete to demonstrate that he/she has a rare metabolism that can lead to excreting salbutamol in urine at or around the reported level in excess of the Decision Limit further to an inhaled dose within the prescribed maximum. If so demonstrated, the AAF would be nullified. For more than 15 years since the inception of the WADC and the Prohibited List, the Threshold of salbutamol has remained unchanged at 1,000 ng/ml. However, the anti-doping rules defining the permitted therapeutic use of inhaled salbutamol have significantly evolved over this time: from the simple application of the Threshold at 1,000 ng/ml to determine an anti-doping rule violation, to a system which: i) includes the analytical measurement uncertainty to define a compliance Decision Limit at 1,200 ng/ml; ii) provides athletes with the opportunity to overturn the AAF through a controlled pharmacokinetic study; and iii) requires the correction of urinary salbutamol concentrations for SG (for concentrated urines) to determine an adverse analytical finding for salbutamol. The evolution of the rules established by the anti-doping regulatory bodies to allow the therapeutic use of inhaled salbutamol has also been significant: from no dose limitation and a considerable risk of excessive intake when athletes were prescribed use of inhaled salbutamol as needed or as required, to a prescribed maximum daily dose as recommended by the manufacturer (i.e g inhaled salbutamol daily), to the more recent requirement not to exceed 800 g of inhaled salbutamol over any 12 hour period in fractionated doses.
15 Anti-doping experts consider that the rules currently in force, including the possibility for athletes to request a controlled excretion study in case of an adverse analytical finding for salbutamol, are fair and balanced. Such rules support good medical practice for the therapeutic use of inhaled salbutamol, and represent at the same time a strong deterrent factor to prevent its abuse for doping purposes. 6. CONSULTATION AND PEER REVIEW The Threshold for salbutamol was in place before WADA became responsible for the world anti-doping program. Indeed, it was adopted (albeit with refinements) from the IOC at a time when Code Article (on the presumed validity of analytical methods or decision limits approved by WADA following consultation with the relevant scientific community and being subject to peer review) did not even exist in the WADC. However, it is WADA s firm opinion that the Threshold/Decision Limit for salbutamol has been subject to significant consultation and peer review with the scientific community over the years. 9 The Threshold implemented by the IOC was based on a recommendation from the IOC Medical Commission, which took into account the studies published in the scientific literature and anti-doping data available at the time. Based on its own review of the existing literature, the WADA LiEG and the HMRC adopted this Threshold (although softened it by removing the automatic consequence of doping, if exceeded). Over the years and as set out above, WADA has continuously commissioned a significant amount of research projects, resulting in peer-reviewed and published studies, to ascertain the correlation between the salbutamol administration regime (dose, frequency and mode of administration), the corresponding urinary concentration levels and the potential for performance enhancement. On each occasion, WADA and its committees (in particular the List and the Laboratory Expert Groups) discussed and reviewed the results of the research with the investigators and concluded that the Threshold was adequate. Indeed, none of the research teams has ever recommended that the Decision Limit be increased; rather, it has been proposed on numerous occasions that the level be lowered, as it was not sufficiently sensitive for systematically detecting systemic use of salbutamol. The scientists that have conducted these studies and been involved in those discussions include some of the world s most renowned specialists in the field, such as D. McKenzie and V. Backer. In addition, the various List and Laboratory Expert Groups, and HMRC that have reviewed and refined the salbutamol system over the years (always confirming the basic Threshold of 1,000 ng/ml) have comprised more than 110 scientists from around the world with particular expertise in anti-doping, pharmacology and sports physiology. In particular, the List Expert Groups have included several experts on β2-agonists (see section 8 below) and analytical science. 9 According to the Cambridge Dictionary, peer review is defined as the process of someone reading, checking, and giving his or her opinion about something that has been written by another scientist or expert working in the same subject area.
16 Each year, the modified Prohibited List drafted by the LiEG for the following calendar year, together with explanations of any modifications to the current version of the List, are circulated to WADA stakeholders for comments pursuant to Article 4.1 of the WADC. The WADA stakeholders, such as International Federations and National Anti-Doping Organizations, have medical commissions composed of scientists with expertise in different fields, including anti-doping science. Comments received from the stakeholders are considered by the LiEG, and the new Prohibited List is further reviewed and approved by the HMRC before it is recommended for adoption to the WADA Executive Committee. In short, therefore, the Threshold for salbutamol has been subject to ongoing monitoring and refinement in a process that has been public and transparent for WADA s stakeholders; in particular, it has been debated and approved by different generations of the WADA LiEG, which itself has taken into account the evolving body of peer-reviewed and published literature, the recommendations from (and discussions with) research teams that have been commissioned by WADA and also the comments received from WADA s stakeholders. Similarly, the Decision Limit has been the subject of review by the Laboratory Expert Group, and has been ratified in various versions of the TDDL. Like any other TD, the TDDL has also been circulated to the stakeholders for review, including all the ADOs and their experts in the field of analytical science, before being approved by the WADA Executive Committee. The Decision Limit, despite being in place for eight years, has never been subject to challenge to WADA s knowledge. The current version of the salbutamol system, which inter alia (i) accounts for analytical measurement uncertainty, (ii) provides for adjustment based on the SG of concentrated samples, (iii) gives specific indications on the maximum allowed inhaled doses and (iv) affords athletes the opportunity to conduct a controlled study in order to seek to overturn an adverse analytical finding, is as balanced and fair to athletes as it has ever been.
17 7. REFERENCES - Berges et al., (2000) Clin Chem. 46: Boulton et al., (1996) Br J Clin Pharm. 41 :35 - Carbo et al (1997) Cancer Lett. 115:113 - Carter & Lynch (1994) Metabolism. 43: Caruso et al (1995) Med. Sci Sports Exerc 27: Caruso et al, (2005) J Strength Cond Res. 19: Caruso et al, (2008) J Strength Cond Res. 22: Cepero et al (1998) J Pharm Pharmacol. 50: Cepero et al, (2000) Comp Biochem Physiol C Toxicol Pharmacol. 126:45. - Collomp et al (2000a) Int J Sports Med 21: Collomp et al (2000b) J Appl Physiol 89: Collomp et al., (2005) Int J Sports Med. 26: Compendium of Pharmaceuticals and Specialties (2005) Canadian Pharmacists Association. - Dickinson et al, (2014a) Clin J Sport Med :482 - Dickinson et al., (2014b) J Sport Sci Med, 13:271 - Elers et al., (2010) Med Sci Sports Exerc 42:244 - Elers et al., (2011) Int J Sport Med 32:574 - Elers et al., (2012a) Clin J Sport Med 22: Elers et al., (2012b) Scan J Sport Med 22 :232 - EURACHEM/CITAC Guide. Use of uncertainty information in compliance assessment. First edition. Ellison SRL,Williams A (Eds) (2007). - Fiacco et al, (2012) Proceedings of the Manfred-Donike-Workshop 20 ; 30th Cologne Workshop on Dope Analysis p Fitch (2006) Clin Rev Allergy Immunol. 31(2-3):259 - GINA Guidelines- - Haase et al., (2016) Drug Test Anal. 8:613 - Hindle and Chrystyn, (1192) Br J Clin Pharmacol 34:311 - Hostrup et al., (2014) Drug Test Anal. 6: Hostrup et al., (2016) Scand J Med Sci Sports. 26:8 - Le Panse et al., (2005) Int J Sports Med. 26:518 - Le Panse et al., (2006) Br J Sports Med 40:627 - Le Panse et al., (2007) Br J Sports Med. 41: Martindale, 2011 Edition, Pharmaceutical Press, London. - Mareck et al., (2011) Drug Test Analysis, 3: Martineau et al., (1992) Clin Sci (Lond) 83: MIMS Ireland, (2004), pp Parsons et al., (2013) Am J Respir Crit Care Med 187: Pichon et al., (2006) Int J Sports Med. 27:187.
18 - Pillard et al., (2015) Resp Res 16: Schweitzer et al (2004) Clin J Sport Med.14:31 - Sporer et al., (2008a) Med Sci Sports Exerc. 40: Sporer et al., (2008b) Clin J Sport Med. 18:282 - Summary of Modifications, Prohibited List - Van Baak et al., (2000) Med. Sci. Sports Exerc., 32: Ventura et al, (2000) Ther Drug Monit.22: Walle et al., (1993) Drug Metab Dispos 21:76

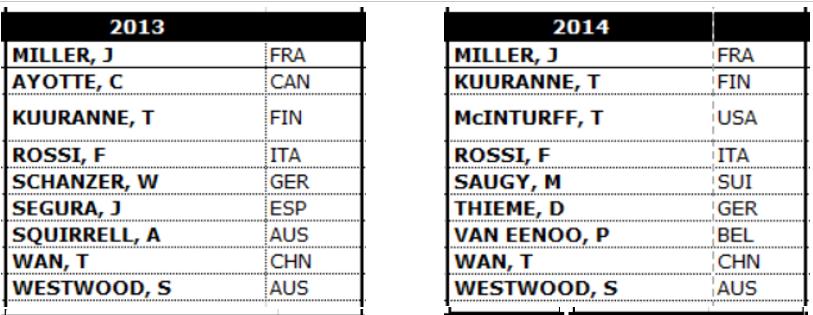
19 8.0 COMPOSITION OF WADA SCIENTIFIC COMMITTEES 8.1 COMPOSITION OF WADA HEALTH, MEDICAL AND RESEARCH COMMITTEES ( )
20
21
22
23

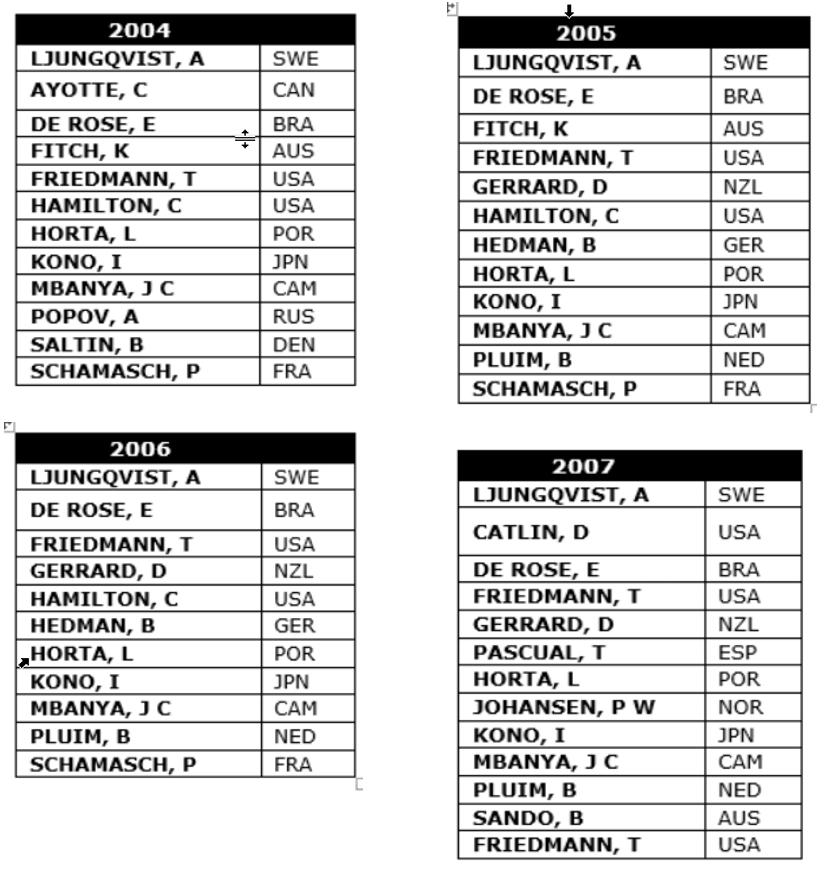
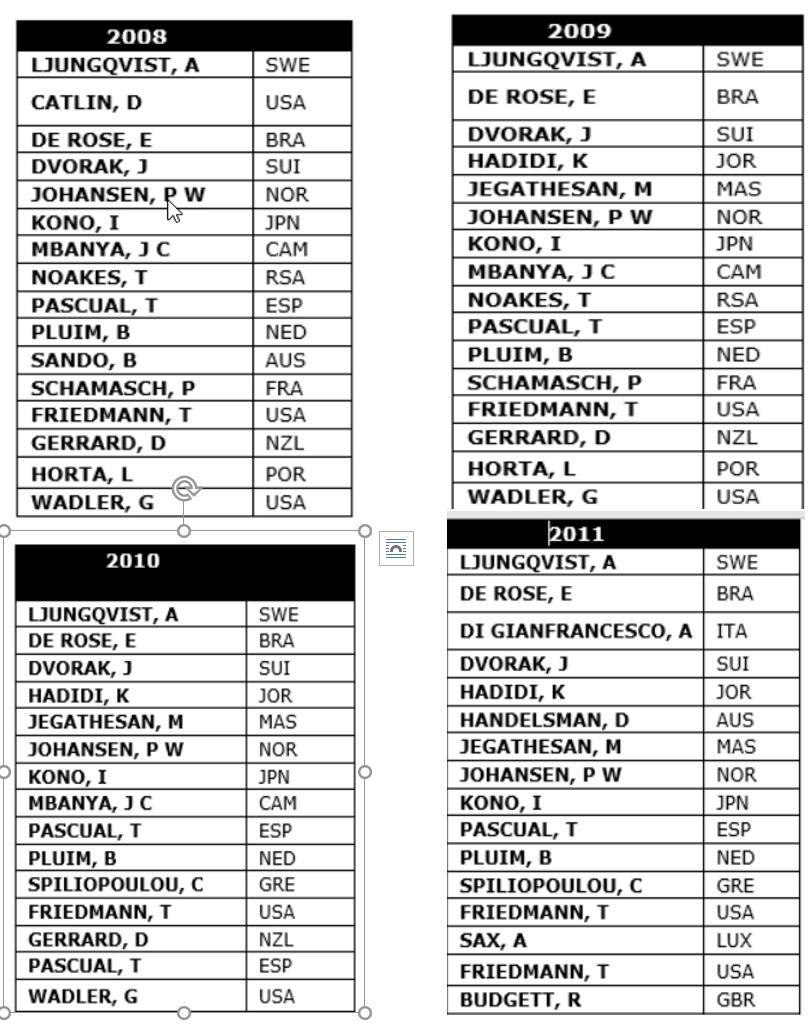
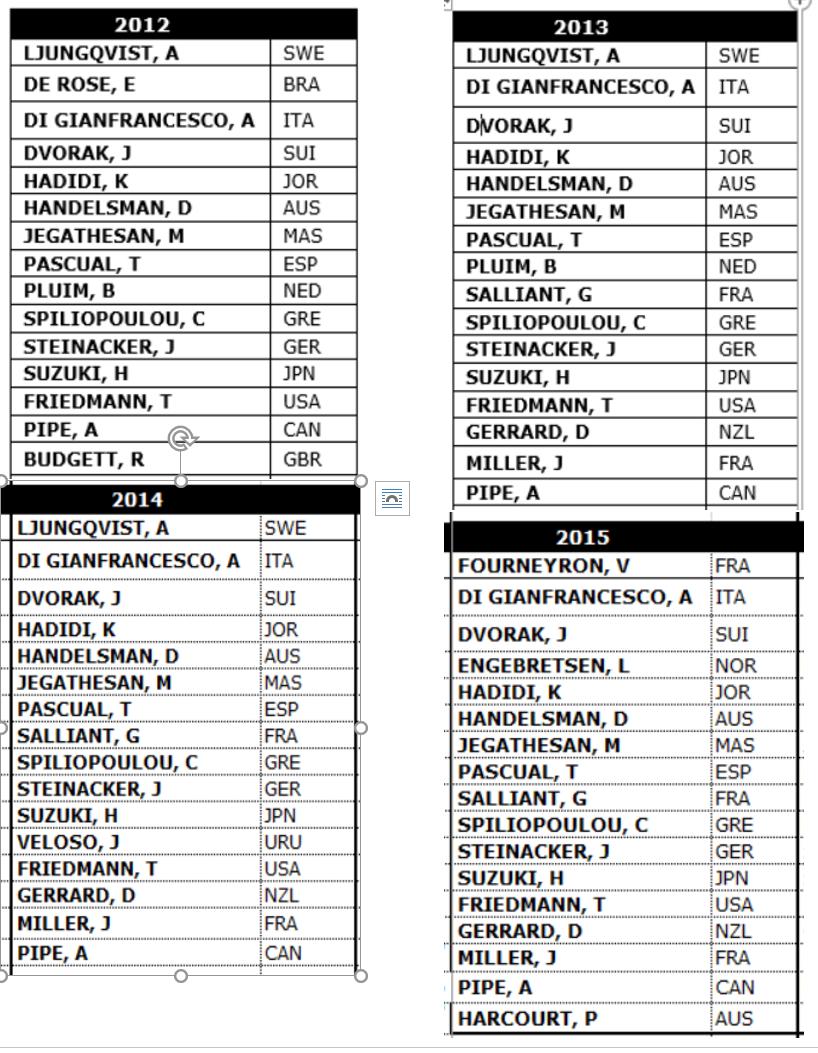
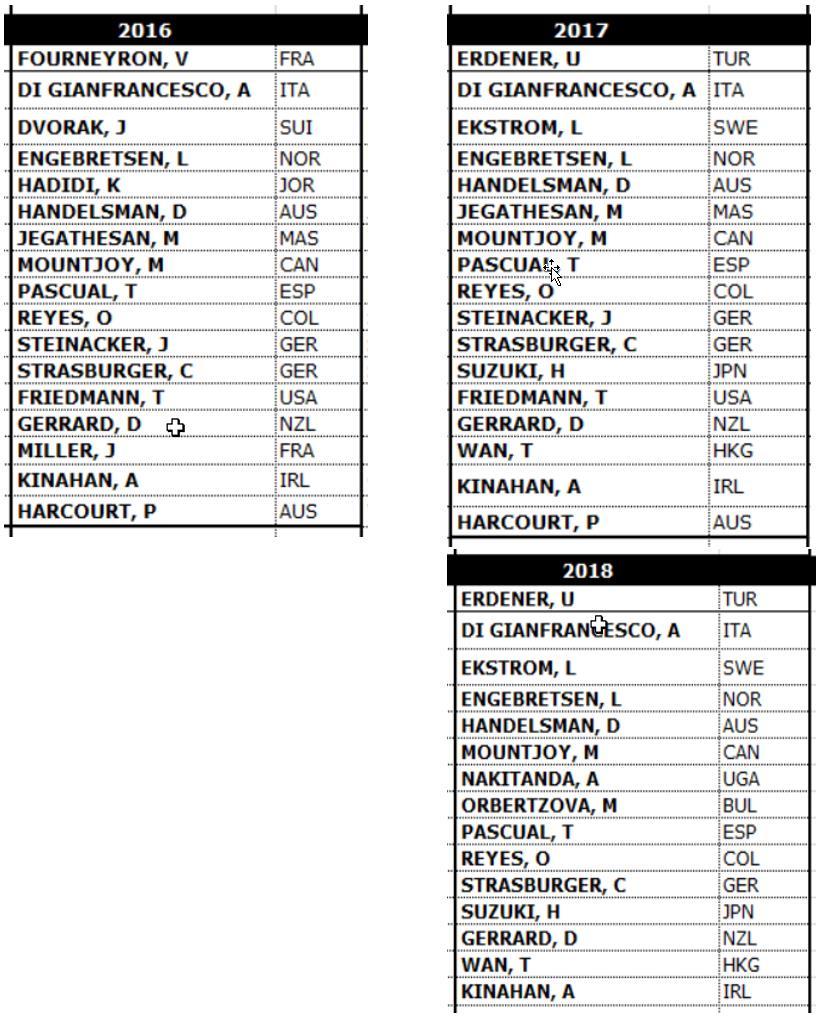
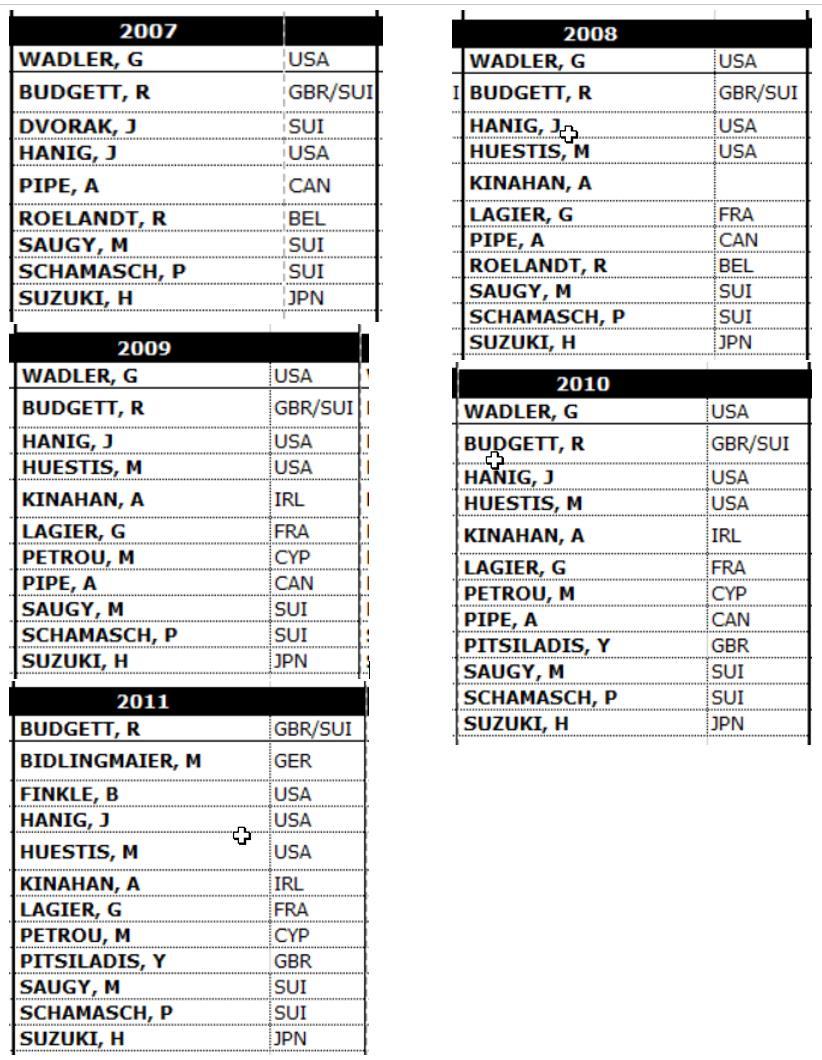
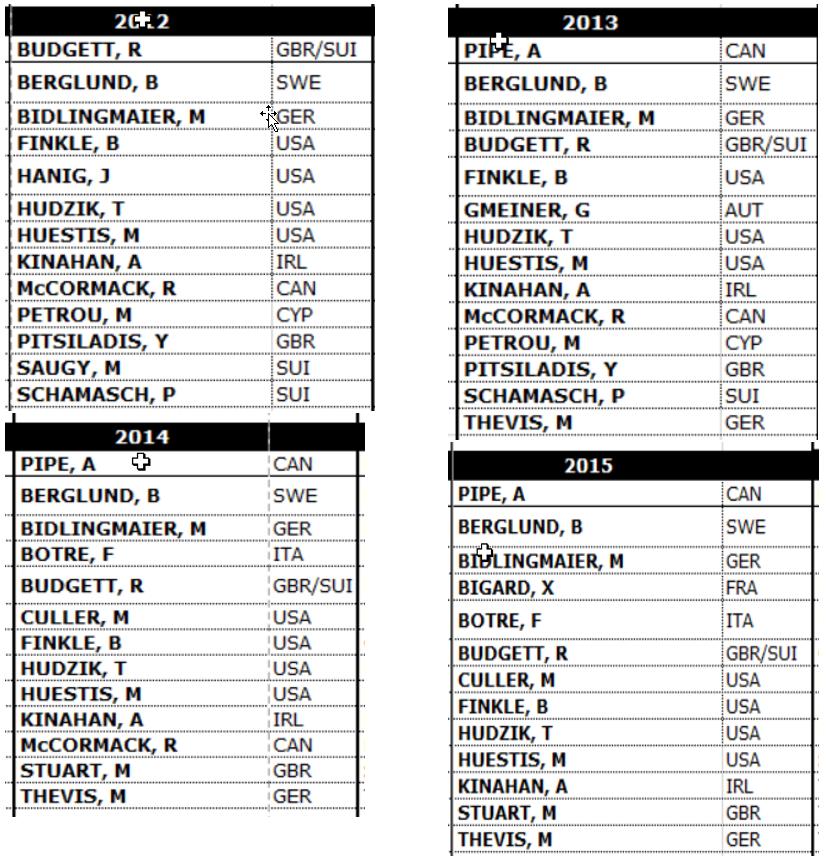
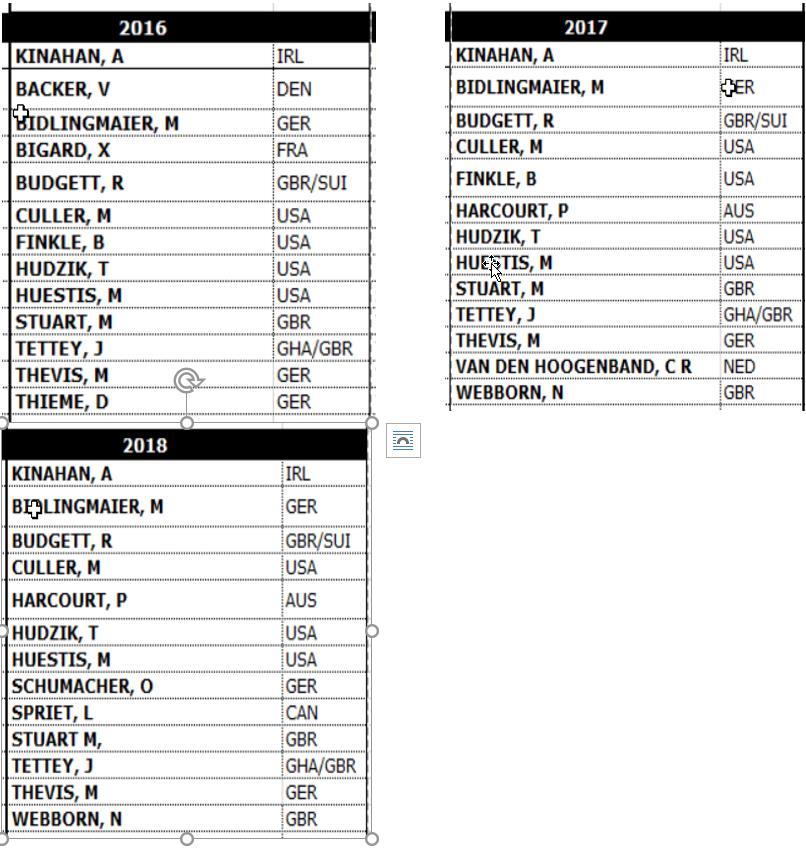
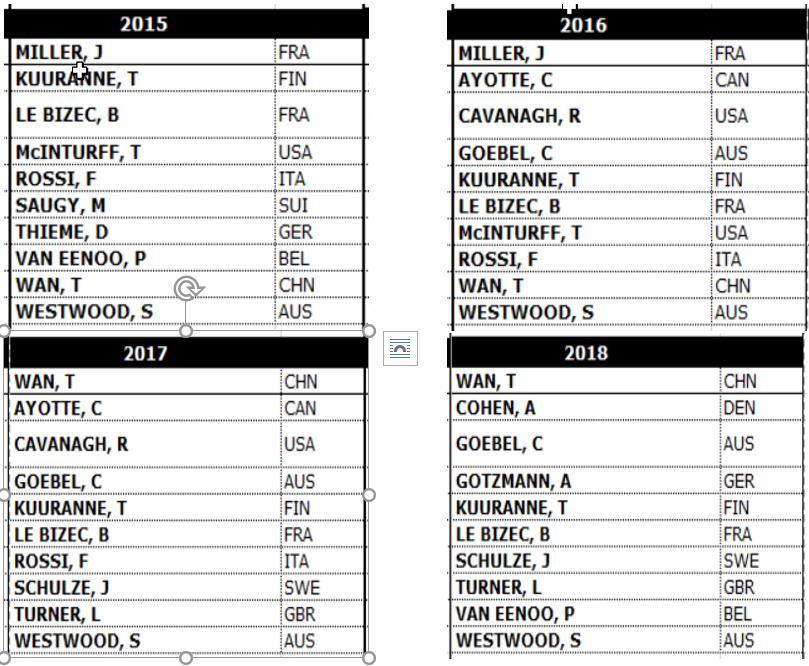
24 8.2 COMPOSITION OF LIST EXPERT GROUPS ( )
25
26
27

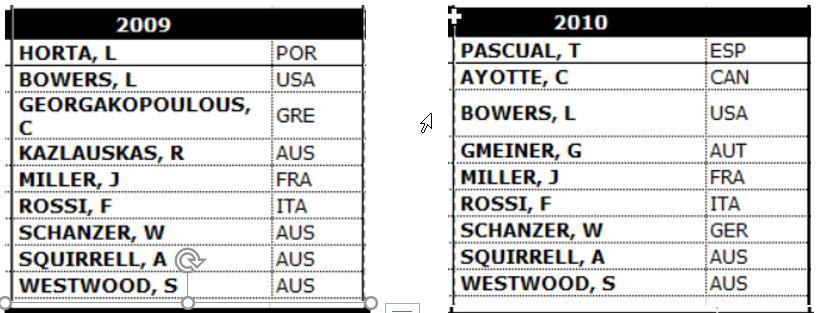
28 8.3 COMPOSITIONS OF LABORATORY EXPERT GROUPS ( )

29

30
31
2009 Prohibited List
 September 20 th, 2008 2009 Prohibited List Summary of Major Modifications and Clarifications INTRODUCTORY PARAGRAPH Article 4.2.2 of the 2009 Code states: For purposes of the application of Article 10
September 20 th, 2008 2009 Prohibited List Summary of Major Modifications and Clarifications INTRODUCTORY PARAGRAPH Article 4.2.2 of the 2009 Code states: For purposes of the application of Article 10
WADA Technical Document TD2017MRPL
 MINIMUM REQUIRED PERFORMANCE LEVELS FOR DETECTION AND IDENTIFICATION OF NON-THRESHOLD SUBSTANCES In order to ensure that all WADA-accredited Laboratories can report the presence of Prohibited Substances,
MINIMUM REQUIRED PERFORMANCE LEVELS FOR DETECTION AND IDENTIFICATION OF NON-THRESHOLD SUBSTANCES In order to ensure that all WADA-accredited Laboratories can report the presence of Prohibited Substances,
2012 Prohibited List
 2012 Prohibited List and Explanatory Notes INTRODUCTION Members of the Anti-Doping Community should be aware that careful consideration has been given to all of the thoughtful comments that have been provided
2012 Prohibited List and Explanatory Notes INTRODUCTION Members of the Anti-Doping Community should be aware that careful consideration has been given to all of the thoughtful comments that have been provided
DOPING RISK MANAGEMENT
 DOPING RISK MANAGEMENT REQUIREMENTS ON ATHLETES At all times, you should educate your athletes to minimize the risk of an accidental infraction: 1. Education! 2. Ensure all medications and products do
DOPING RISK MANAGEMENT REQUIREMENTS ON ATHLETES At all times, you should educate your athletes to minimize the risk of an accidental infraction: 1. Education! 2. Ensure all medications and products do
Therapeutic Use Exemption (TUE) Policy
 Policy") Therapeutic Use Exemption (TUE) Policy Following an amendment to the Irish Anti-Doping Rules by Sport Ireland on 6th April 2010, Sport Ireland has established a Therapeutic Use Exemption (TUE) Policy based
Therapeutic Use Exemption (TUE) Policy Following an amendment to the Irish Anti-Doping Rules by Sport Ireland on 6th April 2010, Sport Ireland has established a Therapeutic Use Exemption (TUE) Policy based
IN THE MATTER OF THE INTERNATIONAL MIXED MARTIAL ARTS FEDERATION ANTI DOPING PROCEEDINGS CONCERNING BREACH OF ARTICLE 2.1 BETWEEN:
 IN THE MATTER OF THE INTERNATIONAL MIXED MARTIAL ARTS FEDERATION ANTI DOPING PROCEEDINGS CONCERNING BREACH OF ARTICLE 2.1 BETWEEN: THE INTERNATIONAL MIXED MARTIAL ARTS FEDERATION --AND-- JAMIE HERRINGTON
IN THE MATTER OF THE INTERNATIONAL MIXED MARTIAL ARTS FEDERATION ANTI DOPING PROCEEDINGS CONCERNING BREACH OF ARTICLE 2.1 BETWEEN: THE INTERNATIONAL MIXED MARTIAL ARTS FEDERATION --AND-- JAMIE HERRINGTON
BACKGROUND + GENERAL COMMENTS
 Response on behalf of Sobi (Swedish Orphan Biovitrum AB) to the European Commission s Public Consultation on a Commission Notice on the Application of Articles 3, 5 and 7 of Regulation (EC) No. 141/2000
Response on behalf of Sobi (Swedish Orphan Biovitrum AB) to the European Commission s Public Consultation on a Commission Notice on the Application of Articles 3, 5 and 7 of Regulation (EC) No. 141/2000
NOTE FOR GUIDANCE ON TOXICOKINETICS: THE ASSESSMENT OF SYSTEMIC EXPOSURE IN TOXICITY STUDIES S3A
 INTERNATIONAL CONFERENCE ON HARMONISATION OF TECHNICAL REQUIREMENTS FOR REGISTRATION OF PHARMACEUTICALS FOR HUMAN USE ICH HARMONISED TRIPARTITE GUIDELINE NOTE FOR GUIDANCE ON TOXICOKINETICS: THE ASSESSMENT
INTERNATIONAL CONFERENCE ON HARMONISATION OF TECHNICAL REQUIREMENTS FOR REGISTRATION OF PHARMACEUTICALS FOR HUMAN USE ICH HARMONISED TRIPARTITE GUIDELINE NOTE FOR GUIDANCE ON TOXICOKINETICS: THE ASSESSMENT
Therapeutic Use Exemption (TUE) Policy
 Policy") Therapeutic Use Exemption (TUE) Policy Following an amendment to the Irish Anti-Doping Rules by the Council on 6th April 2010, the Irish Sports Council has established a Therapeutic Use Exemption (TUE)
Therapeutic Use Exemption (TUE) Policy Following an amendment to the Irish Anti-Doping Rules by the Council on 6th April 2010, the Irish Sports Council has established a Therapeutic Use Exemption (TUE)
EUROPEAN COMMISSION HEALTH AND FOOD SAFETY DIRECTORATE-GENERAL. PHARMACEUTICAL COMMITTEE 21 October 2015
 EUROPEAN COMMISSION HEALTH AND FOOD SAFETY DIRECTORATE-GENERAL Health systems and products Medicinal products authorisations, European Medicines Agency PHARM 689 PHARMACEUTICAL COMMITTEE 21 October 2015
EUROPEAN COMMISSION HEALTH AND FOOD SAFETY DIRECTORATE-GENERAL Health systems and products Medicinal products authorisations, European Medicines Agency PHARM 689 PHARMACEUTICAL COMMITTEE 21 October 2015
COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP)
") The European Medicines Agency Pre-authorisation Evaluation of Medicines for Human Use London, 15 December 2005 EMEA/357981/2005 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON PROCEDURES
The European Medicines Agency Pre-authorisation Evaluation of Medicines for Human Use London, 15 December 2005 EMEA/357981/2005 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON PROCEDURES
Cigarettes Determination of tobacco specific nitrosamines in mainstream cigarette smoke Method using LC-MS/MS
 INTERNATIONAL STANDARD ISO 19290 First edition 2016-12-01 Cigarettes Determination of tobacco specific nitrosamines in mainstream cigarette smoke Method using LC-MS/MS Cigarettes Dosage des nitrosamines
INTERNATIONAL STANDARD ISO 19290 First edition 2016-12-01 Cigarettes Determination of tobacco specific nitrosamines in mainstream cigarette smoke Method using LC-MS/MS Cigarettes Dosage des nitrosamines
C 178/2 Official Journal of the European Union
 C 178/2 Official Journal of the European Union 29.7.2003 Communication from the Commission on Regulation (EC) No 141/2000 of the European Parliament and of the Council on orphan medicinal products (2003/C
C 178/2 Official Journal of the European Union 29.7.2003 Communication from the Commission on Regulation (EC) No 141/2000 of the European Parliament and of the Council on orphan medicinal products (2003/C
JANUARY Guide to the WADA Prohibited List and Therapeutic Use Exemptions
 JANUARY 2018 Guide to the WADA Prohibited List and Therapeutic Use Exemptions Contents The WADA Prohibited List 3 Therapeutic Use Exemptions (TUEs) 5 Requirements for asthma TUEs 9 2 The WADA Prohibited
JANUARY 2018 Guide to the WADA Prohibited List and Therapeutic Use Exemptions Contents The WADA Prohibited List 3 Therapeutic Use Exemptions (TUEs) 5 Requirements for asthma TUEs 9 2 The WADA Prohibited
Sterilization of health care products Radiation. Part 3: Guidance on dosimetric aspects of development, validation and routine control
 Provläsningsexemplar / Preview INTERNATIONAL STANDARD ISO 11137-3 Second edition 2017-06 Sterilization of health care products Radiation Part 3: Guidance on dosimetric aspects of development, validation
Provläsningsexemplar / Preview INTERNATIONAL STANDARD ISO 11137-3 Second edition 2017-06 Sterilization of health care products Radiation Part 3: Guidance on dosimetric aspects of development, validation
ISA 540, Auditing Accounting Estimates, Including Fair Value Accounting Estimates, and Related Disclosures Issues and Task Force Recommendations
 Agenda Item 1-A ISA 540, Auditing Accounting Estimates, Including Fair Value Accounting Estimates, and Related Disclosures Issues and Task Force Recommendations Introduction 1. Since the September 2016
Agenda Item 1-A ISA 540, Auditing Accounting Estimates, Including Fair Value Accounting Estimates, and Related Disclosures Issues and Task Force Recommendations Introduction 1. Since the September 2016
IAASB Main Agenda (March 2005) Page Agenda Item. DRAFT EXPLANATORY MEMORANDUM ISA 701 and ISA 702 Exposure Drafts February 2005
 Page Agenda Item. DRAFT EXPLANATORY MEMORANDUM ISA 701 and ISA 702 Exposure Drafts February 2005") IAASB Main Agenda (March 2005) Page 2005 579 Agenda Item 13-F DRAFT EXPLANATORY MEMORANDUM ISA 701 and ISA 702 Exposure Drafts February 2005 Introduction This memorandum provides some background to, and
IAASB Main Agenda (March 2005) Page 2005 579 Agenda Item 13-F DRAFT EXPLANATORY MEMORANDUM ISA 701 and ISA 702 Exposure Drafts February 2005 Introduction This memorandum provides some background to, and
FIH CODE OF CONDUCT, FIH ANTI-DOPING RULES, FIH IMAGE RIGHTS POLICY AND FIH ANTI-CORRUPTION REGULATIONS
 Notes: FIH CODE OF CONDUCT, FIH ANTI-DOPING RULES, FIH IMAGE RIGHTS POLICY AND FIH ANTI-CORRUPTION REGULATIONS ACKNOWLEDGMENT AND AGREEMENT 1. No Participant may participate in an FIH world level event
Notes: FIH CODE OF CONDUCT, FIH ANTI-DOPING RULES, FIH IMAGE RIGHTS POLICY AND FIH ANTI-CORRUPTION REGULATIONS ACKNOWLEDGMENT AND AGREEMENT 1. No Participant may participate in an FIH world level event
DRAFT (Final) Concept Paper On choosing appropriate estimands and defining sensitivity analyses in confirmatory clinical trials
 Concept Paper On choosing appropriate estimands and defining sensitivity analyses in confirmatory clinical trials") DRAFT (Final) Concept Paper On choosing appropriate estimands and defining sensitivity analyses in confirmatory clinical trials EFSPI Comments Page General Priority (H/M/L) Comment The concept to develop
DRAFT (Final) Concept Paper On choosing appropriate estimands and defining sensitivity analyses in confirmatory clinical trials EFSPI Comments Page General Priority (H/M/L) Comment The concept to develop
DRAFT GUIDANCE DOCUMENT Comparative Bioavailability Standards: Formulations Used for Systemic Effects
 1 2 3 DRAFT GUIDANCE DOCUMENT Comparative Bioavailability Standards: Formulations Used for Systemic Effects 4 This guidance document is being distributed for comment purposes only. 5 6 Published by authority
1 2 3 DRAFT GUIDANCE DOCUMENT Comparative Bioavailability Standards: Formulations Used for Systemic Effects 4 This guidance document is being distributed for comment purposes only. 5 6 Published by authority
DIRECTIVE 2004/24/EC OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL. of 31 March 2004
 30.4.2004 Official Journal of the European Union L 136/85 DIRECTIVE 2004/24/EC OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL of 31 March 2004 amending, as regards traditional herbal medicinal products,
30.4.2004 Official Journal of the European Union L 136/85 DIRECTIVE 2004/24/EC OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL of 31 March 2004 amending, as regards traditional herbal medicinal products,
The 2018 Prohibited List will be effective 1 January As usual there are some changes.
 TO: PSA ATHLETES and MEMBER NATIONS WADA PROHIBITED LIST 2018 The 2018 Prohibited List will be effective 1 January 2018. As usual there are some changes. Below is a synopsis of the major modifications.
TO: PSA ATHLETES and MEMBER NATIONS WADA PROHIBITED LIST 2018 The 2018 Prohibited List will be effective 1 January 2018. As usual there are some changes. Below is a synopsis of the major modifications.
ISPM No. 28 PHYTOSANITARY TREATMENTS FOR REGULATED PESTS (2007)
") ISPM No. 28 INTERNATIONAL STANDARDS FOR PHYTOSANITARY MEASURES ISPM No. 28 PHYTOSANITARY TREATMENTS FOR REGULATED PESTS (2007) Produced by the Secretariat of the International Plant Protection Convention
ISPM No. 28 INTERNATIONAL STANDARDS FOR PHYTOSANITARY MEASURES ISPM No. 28 PHYTOSANITARY TREATMENTS FOR REGULATED PESTS (2007) Produced by the Secretariat of the International Plant Protection Convention
ARE CURRENT SPORT REGULATIONS FAIR TO ALLERGIC ATHLETES?
 ARE CURRENT SPORT REGULATIONS FAIR TO ALLERGIC ATHLETES? Sergio Bonini Second University of Naples & Institute of Neurobiology and Molecular Medicine, Italian National Research Council (INMM-CNR), Rome,
ARE CURRENT SPORT REGULATIONS FAIR TO ALLERGIC ATHLETES? Sergio Bonini Second University of Naples & Institute of Neurobiology and Molecular Medicine, Italian National Research Council (INMM-CNR), Rome,
International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use
 Final Concept Paper E9(R1): Addendum to Statistical Principles for Clinical Trials on Choosing Appropriate Estimands and Defining Sensitivity Analyses in Clinical Trials dated 22 October 2014 Endorsed
Final Concept Paper E9(R1): Addendum to Statistical Principles for Clinical Trials on Choosing Appropriate Estimands and Defining Sensitivity Analyses in Clinical Trials dated 22 October 2014 Endorsed
**This form MUST accompany a TUE Application for a Beta-2 Agonist if submitted to USADA**
 **This form MUST accompany a TUE Application for a Beta-2 Agonist if submitted to USADA** PHYSICIAN- You must select one of the Objective Tests in the Table below and report the result. Please take note
**This form MUST accompany a TUE Application for a Beta-2 Agonist if submitted to USADA** PHYSICIAN- You must select one of the Objective Tests in the Table below and report the result. Please take note
LAB5 EDITION 2 NOVEMBER 2012
 2007 LAB5 EDITION 2 NOVEMBER 2012 Reporting Calibration Results JH CONTENTS SECTION PAGE 1 Introduction 2 2 UKAS calibration accreditation symbol 3 3 General guidance for the presentation of calibration
2007 LAB5 EDITION 2 NOVEMBER 2012 Reporting Calibration Results JH CONTENTS SECTION PAGE 1 Introduction 2 2 UKAS calibration accreditation symbol 3 3 General guidance for the presentation of calibration
By to: Dear Mr. Howman and members of WADA s Prohibited List Expert Group,
 By e-mail to: violet.maziar@wada-ama.org, david.howman@wada-ama.org Regarding: Capelle aan den IJssel, 27 June 2011 Dear Mr. Howman and members of WADA s Prohibited List Expert Group, Thank you very much
By e-mail to: violet.maziar@wada-ama.org, david.howman@wada-ama.org Regarding: Capelle aan den IJssel, 27 June 2011 Dear Mr. Howman and members of WADA s Prohibited List Expert Group, Thank you very much
Issue Paper: Monitoring a Rights based Approach: Key Issues and Suggested Approaches
 Issue Paper: Monitoring a Rights based Approach: Key Issues and Suggested Approaches Defining the Issue This paper explores issues and approaches relevant to the assessment of the application of a rights
Issue Paper: Monitoring a Rights based Approach: Key Issues and Suggested Approaches Defining the Issue This paper explores issues and approaches relevant to the assessment of the application of a rights
Working Document prepared by the Commission services - does not prejudice the Commission's final decision 3/2/2014 COMMISSION STAFF WORKING DOCUMENT
 COMMISSION STAFF WORKING DOCUMENT on certain requirements for FSMPs [Supporting Document for the Expert Group meeting of 7 February 2014] Introduction Following the discussions in the Expert Group meeting
COMMISSION STAFF WORKING DOCUMENT on certain requirements for FSMPs [Supporting Document for the Expert Group meeting of 7 February 2014] Introduction Following the discussions in the Expert Group meeting
Psychotherapists and Counsellors Professional Liaison Group (PLG) 30 September 2010
 30 September 2010") Psychotherapists and Counsellors Professional Liaison Group (PLG) 30 September 2010 Information for organisations invited to present to meetings of the Psychotherapists and Counsellors Professional Liaison
Psychotherapists and Counsellors Professional Liaison Group (PLG) 30 September 2010 Information for organisations invited to present to meetings of the Psychotherapists and Counsellors Professional Liaison
INTERNATIONAL STANDARD ON ASSURANCE ENGAGEMENTS 3000 ASSURANCE ENGAGEMENTS OTHER THAN AUDITS OR REVIEWS OF HISTORICAL FINANCIAL INFORMATION CONTENTS
 INTERNATIONAL STANDARD ON ASSURANCE ENGAGEMENTS 3000 ASSURANCE ENGAGEMENTS OTHER THAN AUDITS OR REVIEWS OF HISTORICAL FINANCIAL INFORMATION (Effective for assurance reports dated on or after January 1,
INTERNATIONAL STANDARD ON ASSURANCE ENGAGEMENTS 3000 ASSURANCE ENGAGEMENTS OTHER THAN AUDITS OR REVIEWS OF HISTORICAL FINANCIAL INFORMATION (Effective for assurance reports dated on or after January 1,
TUE PHYSICIAN GUIDELINES Medical Information to Support the Decisions of TUE Committees Asthma ASTHMA
 1. Medical Condition ASTHMA is a syndrome of the respiratory airways manifested by recurrent episodic symptoms. It is associated with variable airway obstruction that is reversible either spontaneously
1. Medical Condition ASTHMA is a syndrome of the respiratory airways manifested by recurrent episodic symptoms. It is associated with variable airway obstruction that is reversible either spontaneously
15 May 2017 Exposure Draft. Response Due Date 23 June Exposure Draft
 15 May 2017 Exposure Draft Response Due Date 23 June 2017 Exposure Draft Proposed Application Material Relating to: (a) Professional Skepticism Linkage with the Fundamental Principles; and (b) Professional
15 May 2017 Exposure Draft Response Due Date 23 June 2017 Exposure Draft Proposed Application Material Relating to: (a) Professional Skepticism Linkage with the Fundamental Principles; and (b) Professional
INTERNATIONAL STANDARD ON AUDITING (NEW ZEALAND) 530
 530") Issued 07/11 INTERNATIONAL STANDARD ON AUDITING (NEW ZEALAND) 530 Audit Sampling (ISA (NZ) 530) Issued July 2011 Effective for audits of historical financial statements for periods beginning on or after
Issued 07/11 INTERNATIONAL STANDARD ON AUDITING (NEW ZEALAND) 530 Audit Sampling (ISA (NZ) 530) Issued July 2011 Effective for audits of historical financial statements for periods beginning on or after
WADA Technical Document TD2017CG/LH
 REPORTING & MANAGEMENT of URINARY HUMAN CHORIONIC GONADOTROPHIN (hcg) and LUTEINIZING HORMONE (LH) FINDINGS IN MALE ATHLETES The purpose of this Technical Document is to ensure a harmonized approach in
REPORTING & MANAGEMENT of URINARY HUMAN CHORIONIC GONADOTROPHIN (hcg) and LUTEINIZING HORMONE (LH) FINDINGS IN MALE ATHLETES The purpose of this Technical Document is to ensure a harmonized approach in
IMPORTANT DISCLAIMER. Note
 yn EUROPEAN COMMISSION HEALTH AND CONSUMERS DIRECTORATE-GENERAL June 2012 DRAFT GUIDANCE DOCUMENT FOR COMPETENT AUTHORITIES FOR THE CONTROL OF COMPLIANCE WITH EU LEGISLATION ON: Regulation (EU) No 1169/2011
yn EUROPEAN COMMISSION HEALTH AND CONSUMERS DIRECTORATE-GENERAL June 2012 DRAFT GUIDANCE DOCUMENT FOR COMPETENT AUTHORITIES FOR THE CONTROL OF COMPLIANCE WITH EU LEGISLATION ON: Regulation (EU) No 1169/2011
on the approximation of the laws of the Member States concerning food additives authorized for use in foodstuffs intended for human consumption
 11. 2. 89 Official Journal of the European Communities No L 40/ 27 COUNCIL DIRECTIVE of 21 December 1988 on the approximation of the laws of the Member States concerning food additives authorized for use
11. 2. 89 Official Journal of the European Communities No L 40/ 27 COUNCIL DIRECTIVE of 21 December 1988 on the approximation of the laws of the Member States concerning food additives authorized for use
5.I.1. GENERAL PRACTITIONER ANNOUNCEMENT OF CREDENTIALS IN NON-SPECIALTY INTEREST AREAS
 Report of the Council on Ethics, Bylaws and Judicial Affairs on Advisory Opinion 5.I.1. GENERAL PRACTITIONER ANNOUNCEMENT OF CREDENTIALS IN NON-SPECIALTY INTEREST AREAS Ethical Advertising under ADA Code:
Report of the Council on Ethics, Bylaws and Judicial Affairs on Advisory Opinion 5.I.1. GENERAL PRACTITIONER ANNOUNCEMENT OF CREDENTIALS IN NON-SPECIALTY INTEREST AREAS Ethical Advertising under ADA Code:
ISO 5495 INTERNATIONAL STANDARD. Sensory analysis Methodology Paired comparison test. Analyse sensorielle Méthodologie Essai de comparaison par paires
 INTERNATIONAL STANDARD ISO 5495 Third edition 2005-11-15 Sensory analysis Methodology Paired comparison test Analyse sensorielle Méthodologie Essai de comparaison par paires Reference number ISO 2005 Provläsningsexemplar
INTERNATIONAL STANDARD ISO 5495 Third edition 2005-11-15 Sensory analysis Methodology Paired comparison test Analyse sensorielle Méthodologie Essai de comparaison par paires Reference number ISO 2005 Provläsningsexemplar
March 12, Medical Marijuana Preliminary Consultation Online Survey Report and Analysis. Introduction:
 March 12, 2014 Medical Marijuana Preliminary Consultation Online Survey Report and Analysis Introduction: The College s current Medical Marijuana policy is under review. As part of this review, the College
March 12, 2014 Medical Marijuana Preliminary Consultation Online Survey Report and Analysis Introduction: The College s current Medical Marijuana policy is under review. As part of this review, the College
Scope of Practice for the Diagnostic Ultrasound Professional
 Scope of Practice for the Diagnostic Ultrasound Professional Copyright 1993-2000 Society of Diagnostic Medical Sonographers, Dallas, Texas USA: All Rights Reserved Worldwide. Organizations which endorse
Scope of Practice for the Diagnostic Ultrasound Professional Copyright 1993-2000 Society of Diagnostic Medical Sonographers, Dallas, Texas USA: All Rights Reserved Worldwide. Organizations which endorse
in the ICH Regions Table of Content Annexes to Guideline and 3. Why is Q4B necessary? Q4B Annexes? for Human Use
 Frequently Asked Questions Q4B: Evaluation and Recommendation of Pharmacopoeial Texts for Use in the ICH Regions The Q4B Expert Working Group developed a set of frequently asked questions to help users
Frequently Asked Questions Q4B: Evaluation and Recommendation of Pharmacopoeial Texts for Use in the ICH Regions The Q4B Expert Working Group developed a set of frequently asked questions to help users
College of American Pathologists
 College of American Pathologists Comments to the Food and Drug Administration on the draft guidance In Vitro Companion Diagnostics Devices October 12, 2011 College of American Pathologists 1350 I Street,
College of American Pathologists Comments to the Food and Drug Administration on the draft guidance In Vitro Companion Diagnostics Devices October 12, 2011 College of American Pathologists 1350 I Street,
Guidance for Industry DRAFT GUIDANCE. This guidance document is being distributed for comment purposes only.
 Compounded Drug Products That Are Essentially Copies of a Commercially Available Drug Product Under Section 503A of the Federal Food, Drug, and Cosmetic Act Guidance for Industry DRAFT GUIDANCE This guidance
Compounded Drug Products That Are Essentially Copies of a Commercially Available Drug Product Under Section 503A of the Federal Food, Drug, and Cosmetic Act Guidance for Industry DRAFT GUIDANCE This guidance
TUEC Guidelines Medical Information to Support the Decisions of TUE Committees Asthma ASTHMA
 1. Medical Condition ASTHMA is a syndrome of the respiratory airways manifested by recurrent episodic symptoms. It is associated with variable airway obstruction that is reversible either spontaneously
1. Medical Condition ASTHMA is a syndrome of the respiratory airways manifested by recurrent episodic symptoms. It is associated with variable airway obstruction that is reversible either spontaneously
General Chapter/Section: <232> Elemental Impurities - Limits Expert Committee(s): General Chapters Chemical Analysis No.
: General Chapters Chemical Analysis No.") General Chapter/Section: Elemental Impurities - Limits Expert Committee(s): General Chapters Chemical Analysis No. of Commenters: 18 Editorial changes suggested by commenters have been reviewed by
General Chapter/Section: Elemental Impurities - Limits Expert Committee(s): General Chapters Chemical Analysis No. of Commenters: 18 Editorial changes suggested by commenters have been reviewed by
Chapter III PROTECTION AND PROMOTION OF THE RIDER S HEALTH
 MEMORANDUM 20 February 2019 PART 13 MEDICAL RULES Rules amendments applying on 01.03.2019 update on DATE Chapter III PROTECTION AND PROMOTION OF THE RIDER S HEALTH [ ] 6 In-Competition Prohibition of tramadol
MEMORANDUM 20 February 2019 PART 13 MEDICAL RULES Rules amendments applying on 01.03.2019 update on DATE Chapter III PROTECTION AND PROMOTION OF THE RIDER S HEALTH [ ] 6 In-Competition Prohibition of tramadol
Questions and Answers on Candidates for Substitution
 Questions and Answers on Candidates for Substitution Rev. 1, January 2015 Background The European Commission is required by Regulation (EC) No 1107/2009 ( the Regulation ) to establish a list of substances
Questions and Answers on Candidates for Substitution Rev. 1, January 2015 Background The European Commission is required by Regulation (EC) No 1107/2009 ( the Regulation ) to establish a list of substances
COUNCIL OF THE EUROPEAN UNION. Brussels, 7 September 2009 (OR. en) 11261/09 Interinstitutional File: 2008/0002 (COD) DENLEG 51 CODEC 893
 11261/09 Interinstitutional File: 2008/0002 (COD) DENLEG 51 CODEC 893") COUNCIL OF THE EUROPEAN UNION Brussels, 7 September 2009 (OR. en) 11261/09 Interinstitutional File: 2008/0002 (COD) DLEG 51 CODEC 893 LEGISLATIVE ACTS AND OTHER INSTRUMTS Subject: Common Position with
COUNCIL OF THE EUROPEAN UNION Brussels, 7 September 2009 (OR. en) 11261/09 Interinstitutional File: 2008/0002 (COD) DLEG 51 CODEC 893 LEGISLATIVE ACTS AND OTHER INSTRUMTS Subject: Common Position with
Payment Policy: Urine Specimen Validity Testing Reference Number: CC.PP.056 Product Types: ALL Effective Date: 11/01/2017 Last Review Date:
 Payment Policy: Reference Number: CC.PP.056 Product Types: ALL Effective Date: 11/01/2017 Last Review Date: Coding Implications Revision Log See Important Reminder at the end of this policy for important
Payment Policy: Reference Number: CC.PP.056 Product Types: ALL Effective Date: 11/01/2017 Last Review Date: Coding Implications Revision Log See Important Reminder at the end of this policy for important
European Commission request to the European Food Safety Authority for scientific advice on:
 European Commission request to the European Food Safety Authority for scientific advice on: the Community list of permitted health claims pursuant article 13 of Regulation 1924/2006 on nutrition and health
European Commission request to the European Food Safety Authority for scientific advice on: the Community list of permitted health claims pursuant article 13 of Regulation 1924/2006 on nutrition and health
Payment Policy Drug Testing EFFECTIVE DATE: POLICY LAST UPDATED:
 Payment Policy Drug Testing EFFECTIVE DATE: 05 23 2013 POLICY LAST UPDATED: 06 05 2018 OVERVIEW This policy documents the criteria and documentation requirements for immunoassay (IA) testing (also called
Payment Policy Drug Testing EFFECTIVE DATE: 05 23 2013 POLICY LAST UPDATED: 06 05 2018 OVERVIEW This policy documents the criteria and documentation requirements for immunoassay (IA) testing (also called
Therapeutic Use Exemption (TUE) Checklist and Application
 Checklist and Application") Therapeutic Use Exemption (TUE) Checklist and Application Attention Deficit Disorder (ADD) and Attention Deficit and Hyperactivity Disorder (ADHD) Step 1: Read all about Therapeutic Use Exemptions (TUE)
Therapeutic Use Exemption (TUE) Checklist and Application Attention Deficit Disorder (ADD) and Attention Deficit and Hyperactivity Disorder (ADHD) Step 1: Read all about Therapeutic Use Exemptions (TUE)
COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP)
") European Medicines Agency London, 26 July 2006 Doc. Ref. EMEA/186279/2006 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON LEGAL STATUS FOR THE SUPPLY TO THE PATIENT OF CENTRALLY AUTHORISED
European Medicines Agency London, 26 July 2006 Doc. Ref. EMEA/186279/2006 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON LEGAL STATUS FOR THE SUPPLY TO THE PATIENT OF CENTRALLY AUTHORISED
Drug Free Workplace and Employee Drug and Alcohol Testing
 Drug Free Workplace and Employee Drug and Alcohol Testing Contents Definitions... 2 General Provisions... 3 Legal Drugs... 3 Responsibilities of Albuquerque Public Schools Employees... 3 Testing for Drugs
Drug Free Workplace and Employee Drug and Alcohol Testing Contents Definitions... 2 General Provisions... 3 Legal Drugs... 3 Responsibilities of Albuquerque Public Schools Employees... 3 Testing for Drugs
IAASB Exposure Draft, Proposed ISAE 3000 (Revised), Assurance Engagements Other Than Audits or Reviews of Historical Financial Information
, Assurance Engagements Other Than Audits or Reviews of Historical Financial Information") Tel +44 (0) 20 7694 8871 Fax +44 (0) 20 7694 8429 8 Salisbury Square DX 38050 Blackfriars London EC4Y 8BB sylvia.smith@kpmgifrg.com United Kingdom Technical Director International Auditing and Assurance
Tel +44 (0) 20 7694 8871 Fax +44 (0) 20 7694 8429 8 Salisbury Square DX 38050 Blackfriars London EC4Y 8BB sylvia.smith@kpmgifrg.com United Kingdom Technical Director International Auditing and Assurance
ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ TUE APPLICATION CHECKLIST POST INFECTIOUS COUGH
 ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ USADA can grant a Therapeutic Use Exemption (TUE) in compliance with the World Anti- Doping Agency International Standard for TUEs. The TUE application process
ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ USADA can grant a Therapeutic Use Exemption (TUE) in compliance with the World Anti- Doping Agency International Standard for TUEs. The TUE application process
International Standard for Athlete Evaluation. July 2015
 International Standard for Athlete Evaluation July 2015 International Paralympic Committee Adenauerallee 212-214 Tel. +49 228 2097-200 www.paralympic.org 53113 Bonn, Germany Fax +49 228 2097-209 info@paralympic.org
International Standard for Athlete Evaluation July 2015 International Paralympic Committee Adenauerallee 212-214 Tel. +49 228 2097-200 www.paralympic.org 53113 Bonn, Germany Fax +49 228 2097-209 info@paralympic.org
Athlete Support Personnel Anti-Doping Guidance Document
 Athlete Support Personnel Anti-Doping Guidance Document Contents Who are Athlete Support Personnel 4 WADA & UKAD 5 Anti-Doping Rule Violations 6 Checking Medications 7-8 Therapeutic Use Exemption (TUEs)
Athlete Support Personnel Anti-Doping Guidance Document Contents Who are Athlete Support Personnel 4 WADA & UKAD 5 Anti-Doping Rule Violations 6 Checking Medications 7-8 Therapeutic Use Exemption (TUEs)
on the advertising of medicinal products for human use
 30. 4. 92 Official Journal of the European Communities No L 113 / 13 COUNCIL DIRECTIVE 92/28/EEC of 31 March 1992 on the advertising of medicinal products for human use THE COUNCIL OF THE EUROPEAN COMMUNITIES,
30. 4. 92 Official Journal of the European Communities No L 113 / 13 COUNCIL DIRECTIVE 92/28/EEC of 31 March 1992 on the advertising of medicinal products for human use THE COUNCIL OF THE EUROPEAN COMMUNITIES,
KEY DIFFERENCES BETWEEN THE NEW MEDICAL DEVICE AND THE OTC REGULATIONS IN EUROPE
 RNI Conseil 2017 Tous droits réservés Toute reproduction interdite sans l'autorisation de l'auteur. KEY DIFFERENCES BETWEEN THE NEW MEDICAL DEVICE AND THE OTC REGULATIONS IN EUROPE Anne Laure TARDY, PhD
RNI Conseil 2017 Tous droits réservés Toute reproduction interdite sans l'autorisation de l'auteur. KEY DIFFERENCES BETWEEN THE NEW MEDICAL DEVICE AND THE OTC REGULATIONS IN EUROPE Anne Laure TARDY, PhD
Use of Standards in Substantial Equivalence Determinations
 Guidance for Industry and for FDA Staff Use of Standards in Substantial Equivalence Determinations Document issued on: March 12, 2000 U.S. Department Of Health And Human Services Food and Drug Administration
Guidance for Industry and for FDA Staff Use of Standards in Substantial Equivalence Determinations Document issued on: March 12, 2000 U.S. Department Of Health And Human Services Food and Drug Administration
European public MRL assessment report (EPMAR)
") 22 August 2014 EMA/CVMP/751522/2013 Committee for Medicinal Products for Veterinary Use European public MRL assessment report (EPMAR) Closantel (bovine and ovine milk) after the provisional maximum residue
22 August 2014 EMA/CVMP/751522/2013 Committee for Medicinal Products for Veterinary Use European public MRL assessment report (EPMAR) Closantel (bovine and ovine milk) after the provisional maximum residue
AGREEMENT ON COMMON PRINCIPLES AND RULES OF CIRCULATION OF MEDICINAL PRODUCTS WITHIN THE EURASIAN ECONOMIC UNION. (Moscow, 23 December 2014)
") AGREEMENT ON COMMON PRINCIPLES AND RULES OF CIRCULATION OF MEDICINAL PRODUCTS WITHIN THE EURASIAN ECONOMIC UNION (Moscow, 23 December 2014) Member States of the Eurasian Economic Union, hereinafter referred
AGREEMENT ON COMMON PRINCIPLES AND RULES OF CIRCULATION OF MEDICINAL PRODUCTS WITHIN THE EURASIAN ECONOMIC UNION (Moscow, 23 December 2014) Member States of the Eurasian Economic Union, hereinafter referred
Guide to Professional Conduct and Ethics for Registered Medical Practitioners. Relationships between doctors and industry Frequently Asked Questions
 Guide to Professional Conduct and Ethics for Registered Medical Practitioners Relationships between doctors and industry Frequently Asked Questions Partnership Practice Performance Relationships between
Guide to Professional Conduct and Ethics for Registered Medical Practitioners Relationships between doctors and industry Frequently Asked Questions Partnership Practice Performance Relationships between
Access to electronic communications services for disabled customers
 Access to electronic communications services for disabled customers Statement Publication date: 12 March 2014 Contents Section Page 1 Summary 1 2 Introduction 2 3 Access to and pricing of the relay service
Access to electronic communications services for disabled customers Statement Publication date: 12 March 2014 Contents Section Page 1 Summary 1 2 Introduction 2 3 Access to and pricing of the relay service
Residual Solvents: FDA/ Regulatory Perspective
 Rosa Motta Compliance Officer Residual Solvents: FDA/ Regulatory Perspective PDA/USP Residual Solvents Conference January 18-19, 2007 1 Outline Laws and regulations governing the compliance requirements
Rosa Motta Compliance Officer Residual Solvents: FDA/ Regulatory Perspective PDA/USP Residual Solvents Conference January 18-19, 2007 1 Outline Laws and regulations governing the compliance requirements
Panel: Mr Quentin Byrne-Sutton (Switzerland), President; Mr Martin Schimke (Germany); Mr Jean- Jacques Bertrand (France)
, President; Mr Martin Schimke (Germany); Mr Jean- Jacques Bertrand (France)") Tribunal Arbitral du Sport Court of Arbitration for Sport Arbitration CAS 2008/A/1668 World Anti-Doping Agency (WADA) v. National Olympic Committee & Sports Confederation of Denmark & Dansk Boldspil-Union
Tribunal Arbitral du Sport Court of Arbitration for Sport Arbitration CAS 2008/A/1668 World Anti-Doping Agency (WADA) v. National Olympic Committee & Sports Confederation of Denmark & Dansk Boldspil-Union
Trainer Assessment Report Guidelines (TARG) 2019 Approved : December Contents
 2019 Approved : December Contents") Contents TARG1 TARG2 TARG3 TARG4 TARG5 TARG6 TARG7 to 11 TARG12 Before Completing this Report Applicants Declaration (no guidelines) Eligibility of Trainer Trainer s Details (no guidelines) Trainer s Qualifications
Contents TARG1 TARG2 TARG3 TARG4 TARG5 TARG6 TARG7 to 11 TARG12 Before Completing this Report Applicants Declaration (no guidelines) Eligibility of Trainer Trainer s Details (no guidelines) Trainer s Qualifications
COMPENDIUM OF MONOGRAPHS NATURAL HEALTH PRODUCTS DIRECTORATE
 COMPENDIUM OF MONOGRAPHS NATURAL HEALTH PRODUCTS DIRECTORATE June 13 2013 Version 3.0 i FOREWORD Guidance documents are meant to provide assistance to industry and health care practitioners on how to comply
COMPENDIUM OF MONOGRAPHS NATURAL HEALTH PRODUCTS DIRECTORATE June 13 2013 Version 3.0 i FOREWORD Guidance documents are meant to provide assistance to industry and health care practitioners on how to comply
ASTRAZENECA v GLAXOSMITHKLINE
 CASE AUTH/1986/4/07 ASTRAZENECA v GLAXOSMITHKLINE Symbicort and Seretide cost comparisons AstraZeneca complained about cost comparisons made by GlaxoSmithKline between AstraZeneca s Symbicort (budesonide/formoterol)
CASE AUTH/1986/4/07 ASTRAZENECA v GLAXOSMITHKLINE Symbicort and Seretide cost comparisons AstraZeneca complained about cost comparisons made by GlaxoSmithKline between AstraZeneca s Symbicort (budesonide/formoterol)
HUMA RESOURCES POLICY
 HUMA RESOURCES POLICY Title: Drug Free Workplace Policy No: 3.08 Originator: Human Resources Page: 1 of 7 Purpose To provide written notification to employees that Children s Medical Center of Dallas (Children
HUMA RESOURCES POLICY Title: Drug Free Workplace Policy No: 3.08 Originator: Human Resources Page: 1 of 7 Purpose To provide written notification to employees that Children s Medical Center of Dallas (Children
Guide to Interchangeable Medicines
 Guide to Interchangeable Medicines AUT-G0115-6 01 JUNE 2018 This guide does not purport to be an interpretation of law and/or regulations and is for guidance purposes only. CONTENTS 1 BACKGROUND 3 1.1
Guide to Interchangeable Medicines AUT-G0115-6 01 JUNE 2018 This guide does not purport to be an interpretation of law and/or regulations and is for guidance purposes only. CONTENTS 1 BACKGROUND 3 1.1
Discussion of Changes in the Draft Preamble
 Discussion of Changes in the Draft Preamble Prepared by the staff of the IARC Monographs programme 31 August 2005 This paper describes the major changes that appear in the draft Preamble that will be reviewed
Discussion of Changes in the Draft Preamble Prepared by the staff of the IARC Monographs programme 31 August 2005 This paper describes the major changes that appear in the draft Preamble that will be reviewed
COMMISSION DELEGATED REGULATION (EU).../... of XXX
.../... of XXX") EUROPEAN COMMISSION Brussels, XXX SANTE/10355/2015 (POOL/E4/2015/10355/10355-EN. doc) [...1(2015) XXX draft COMMISSION DELEGATED REGULATION (EU).../... of XXX supplementmg Regulation (EU) No 609/2013 of
EUROPEAN COMMISSION Brussels, XXX SANTE/10355/2015 (POOL/E4/2015/10355/10355-EN. doc) [...1(2015) XXX draft COMMISSION DELEGATED REGULATION (EU).../... of XXX supplementmg Regulation (EU) No 609/2013 of
EUR-Lex L EN. Council Directive 93/74/EEC of 13 September 1993 on feedingstuffs intended for particular nutritional purposes
 Page 1 of 5 Avis juridique important 31993L0074 Council Directive 93/74/EEC of 13 September 1993 on feedingstuffs intended for particular nutritional purposes Official Journal L 237, 22/09/1993 P. 0023-0027
Page 1 of 5 Avis juridique important 31993L0074 Council Directive 93/74/EEC of 13 September 1993 on feedingstuffs intended for particular nutritional purposes Official Journal L 237, 22/09/1993 P. 0023-0027
Submitted to the House Energy and Commerce Committee. Federal Efforts to Combat the Opioid Crisis
 STATEMENT FOR THE RECORD Submitted to the House Energy and Commerce Committee Federal Efforts to Combat the Opioid Crisis October 25, 2017 America s Health Insurance Plans 601 Pennsylvania Avenue, NW Suite
STATEMENT FOR THE RECORD Submitted to the House Energy and Commerce Committee Federal Efforts to Combat the Opioid Crisis October 25, 2017 America s Health Insurance Plans 601 Pennsylvania Avenue, NW Suite
Agenda Item 14 CX/FFP 12/32/14
 E Agenda Item 14 CX/FFP 12/32/14 JOINT FAO/WHO FOOD STANDARDS PROGRAMME CODEX COMMITTEE ON FISH AND FISHERY PRODUCTS Thirty-Second Session Bali, Indonesia 1 5 October 2012 DISCUSSION PAPER HISTAMINE Prepared
E Agenda Item 14 CX/FFP 12/32/14 JOINT FAO/WHO FOOD STANDARDS PROGRAMME CODEX COMMITTEE ON FISH AND FISHERY PRODUCTS Thirty-Second Session Bali, Indonesia 1 5 October 2012 DISCUSSION PAPER HISTAMINE Prepared
Panel: Malcom Holmes (Australia), Sole Arbitrator. Handball Doping (salbutamol) Extenuating circumstances
, Sole Arbitrator. Handball Doping (salbutamol) Extenuating circumstances") Tribunal Arbitral du Sport Court of Arbitration for Sport Arbitration CAS (Oceania registry) A3, A4 / 99; Australian Olympic Committee (AOC) and Australian Handball Federation (AHF)/ A., Panel: Malcom
Tribunal Arbitral du Sport Court of Arbitration for Sport Arbitration CAS (Oceania registry) A3, A4 / 99; Australian Olympic Committee (AOC) and Australian Handball Federation (AHF)/ A., Panel: Malcom
COMMISSION OF THE EUROPEAN COMMUNITIES REPORT FROM THE COMMISSION TO THE COUNCIL AND THE EUROPEAN PARLIAMENT
 EN EN EN COMMISSION OF THE EUROPEAN COMMUNITIES Brussels, 5.12.2008 COM(2008) 824 final REPORT FROM THE COMMISSION TO THE COUNCIL AND THE EUROPEAN PARLIAMENT on the use of substances other than vitamins
EN EN EN COMMISSION OF THE EUROPEAN COMMUNITIES Brussels, 5.12.2008 COM(2008) 824 final REPORT FROM THE COMMISSION TO THE COUNCIL AND THE EUROPEAN PARLIAMENT on the use of substances other than vitamins
Annex I. Scientific conclusions and grounds for refusal presented by the European Medicines Agency
 Annex I Scientific conclusions and grounds for refusal presented by the European Medicines Agency Scientific conclusions and grounds for refusal presented by the European Medicines Agency Overall summary
Annex I Scientific conclusions and grounds for refusal presented by the European Medicines Agency Scientific conclusions and grounds for refusal presented by the European Medicines Agency Overall summary
Professional Development: proposals for assuring the continuing fitness to practise of osteopaths. draft Peer Discussion Review Guidelines
 5 Continuing Professional Development: proposals for assuring the continuing fitness to practise of osteopaths draft Peer Discussion Review Guidelines February January 2015 2 draft Peer Discussion Review
5 Continuing Professional Development: proposals for assuring the continuing fitness to practise of osteopaths draft Peer Discussion Review Guidelines February January 2015 2 draft Peer Discussion Review
BEFORE THE SPORTS TRIBUNAL ST 10/16 OF NEW ZEALAND
 BEFORE THE SPORTS TRIBUNAL ST 10/16 OF NEW ZEALAND BETWEEN DRUG FREE SPORT NEW ZEALAND Applicant AND CLAYTON LEWIS Respondent AND NEW ZEALAND FOOTBALL Interested Party DECISION OF SPORTS TRIBUNAL 27 July
BEFORE THE SPORTS TRIBUNAL ST 10/16 OF NEW ZEALAND BETWEEN DRUG FREE SPORT NEW ZEALAND Applicant AND CLAYTON LEWIS Respondent AND NEW ZEALAND FOOTBALL Interested Party DECISION OF SPORTS TRIBUNAL 27 July
Identifying New Cannabis Use with Urine Creatinine- Normalized THCCOOH Concentrations and Time Intervals Between Specimen Collections *
 Identifying New Cannabis Use with Urine Creatinine- Normalized THCCOOH Concentrations and Time Intervals Between Specimen Collections * Michael L. Smith 1, Allan J. Barnes 2, and Marilyn A. Huestis 2,
Identifying New Cannabis Use with Urine Creatinine- Normalized THCCOOH Concentrations and Time Intervals Between Specimen Collections * Michael L. Smith 1, Allan J. Barnes 2, and Marilyn A. Huestis 2,
Comparability and quality of experimental data under different quality systems. S. Caroli Istituto Superiore di Sanità Rome
 Comparability and quality of experimental data under different quality systems S. Caroli Istituto Superiore di Sanità Rome Programme of this presentation Part I. Background information Part II. Key aspects
Comparability and quality of experimental data under different quality systems S. Caroli Istituto Superiore di Sanità Rome Programme of this presentation Part I. Background information Part II. Key aspects
The EU PIP - a step in Pediatric Drug Development. Thomas Severin Bonn,
 The EU PIP - a step in Pediatric Drug Development Thomas Severin Bonn, 13.01.2009 Agenda Implications for Industry Company Preparation Time of PIP Submission Content of the PIP The PIP Process and first
The EU PIP - a step in Pediatric Drug Development Thomas Severin Bonn, 13.01.2009 Agenda Implications for Industry Company Preparation Time of PIP Submission Content of the PIP The PIP Process and first
Re: National Bioengineered Food Disclosure Standard; Proposed Rule; Request for Comments, 83 Fed. Reg (May 4, 2018), Docket No.
, Docket No.") VIA ELECTRONIC SUBMISSION July 3, 2018 Dockets Management Staff (HFA-305) Food and Drug Administration 5630 Fishers Lane, Rm. 1061 Rockville, MD 20852 Re: National Bioengineered Food Disclosure Standard;
VIA ELECTRONIC SUBMISSION July 3, 2018 Dockets Management Staff (HFA-305) Food and Drug Administration 5630 Fishers Lane, Rm. 1061 Rockville, MD 20852 Re: National Bioengineered Food Disclosure Standard;
WADA Technical Document TD2018CG/LH
 REPORTING & MANAGEMENT of URINARY HUMAN CHORIONIC GONADOTROPHIN (hcg) and LUTEINIZING HORMONE (LH) FINDINGS IN MALE ATHLETES The purpose of this Technical Document is to ensure a harmonized approach in
REPORTING & MANAGEMENT of URINARY HUMAN CHORIONIC GONADOTROPHIN (hcg) and LUTEINIZING HORMONE (LH) FINDINGS IN MALE ATHLETES The purpose of this Technical Document is to ensure a harmonized approach in
trends bulletin ecstasy and related drug Key findings
 april 2010 Author: Dr. Matthew Dunn & Ms Johanna Thomas, National Drug and Alcohol Research Centre, University of New South Wales. Suggested citation: Dunn, M. & Thomas, J.O. (2010). Attitudes toward,
april 2010 Author: Dr. Matthew Dunn & Ms Johanna Thomas, National Drug and Alcohol Research Centre, University of New South Wales. Suggested citation: Dunn, M. & Thomas, J.O. (2010). Attitudes toward,
COMMISSION REGULATION (EU)
") 11.3.2011 Official Journal of the European Union L 64/15 COMMISSION REGULATION (EU) No 234/2011 of 10 March 2011 implementing Regulation (EC) No 1331/2008 of the European Parliament and of the Council
11.3.2011 Official Journal of the European Union L 64/15 COMMISSION REGULATION (EU) No 234/2011 of 10 March 2011 implementing Regulation (EC) No 1331/2008 of the European Parliament and of the Council
The Nutrition (Amendment) (EU Exit) Regulations 2018
 (EU Exit) Regulations 2018") The Nutrition (Amendment) (EU Exit) Regulations 2018 A public consultation Contents Introduction... 3 Why we are consulting... 4 Nutrition and Health Claims... 6 Proposals... 6 Vitamins, minerals, and
The Nutrition (Amendment) (EU Exit) Regulations 2018 A public consultation Contents Introduction... 3 Why we are consulting... 4 Nutrition and Health Claims... 6 Proposals... 6 Vitamins, minerals, and
Official Journal of the European Union. (Non-legislative acts) REGULATIONS
 REGULATIONS") 21.2.2015 L 50/1 II (Non-legislative acts) REGULATIONS COMMISSION REGULATION (EU) 2015/282 of 20 February 2015 amending Annexes VIII, IX and X to Regulation (EC) No 1907/2006 of the European Parliament
21.2.2015 L 50/1 II (Non-legislative acts) REGULATIONS COMMISSION REGULATION (EU) 2015/282 of 20 February 2015 amending Annexes VIII, IX and X to Regulation (EC) No 1907/2006 of the European Parliament
Overview of USP General Chapters <476> and <1086> Prescription/Non-Prescription Stakeholder Forum October 19, 2017
 Overview of USP General Chapters and Prescription/Non-Prescription Stakeholder Forum October 19, 2017 Introduction Periodic review of existing general chapters Typically an approximately 5
Overview of USP General Chapters and Prescription/Non-Prescription Stakeholder Forum October 19, 2017 Introduction Periodic review of existing general chapters Typically an approximately 5
This document is meant purely as a documentation tool and the institutions do not assume any liability for its contents
 1997R0258 EN 07.08.2009 004.001 1 This document is meant purely as a documentation tool and the institutions do not assume any liability for its contents B REGULATION (EC) No 258/97 OF THE EUROPEAN PARLIAMENT
1997R0258 EN 07.08.2009 004.001 1 This document is meant purely as a documentation tool and the institutions do not assume any liability for its contents B REGULATION (EC) No 258/97 OF THE EUROPEAN PARLIAMENT
Food additives. FAO guidelines on the structure and content of the document called "Chemical and Technical Assessment (CTA)" Rome, February 2003
 Rome, February 2003") FAO Joint Secretariat to JECFA Joint FAO/WHO Expert Committee on Food Additives Food additives FAO guidelines on the structure and content of the document called "Chemical and Technical Assessment (CTA)"
FAO Joint Secretariat to JECFA Joint FAO/WHO Expert Committee on Food Additives Food additives FAO guidelines on the structure and content of the document called "Chemical and Technical Assessment (CTA)"
ISO INTERNATIONAL STANDARD
 INTERNATIONAL STANDARD ISO 15197 First edition 2003-05-01 In vitro diagnostic test systems Requirements for blood-glucose monitoring systems for self-testing in managing diabetes mellitus Systèmes d'essais
INTERNATIONAL STANDARD ISO 15197 First edition 2003-05-01 In vitro diagnostic test systems Requirements for blood-glucose monitoring systems for self-testing in managing diabetes mellitus Systèmes d'essais
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
codex alimentarius commission
 codex alimentarius commission FOOD AND AGRICULTURE WORLD HEALTH ORGANIZATION ORGANIZATION OF THE UNITED NATIONS JOINT OFFICE: Via delle Terme di Caracalla 00100 Rome Tel.: 39.06.57051 Telex: 625825-625853
codex alimentarius commission FOOD AND AGRICULTURE WORLD HEALTH ORGANIZATION ORGANIZATION OF THE UNITED NATIONS JOINT OFFICE: Via delle Terme di Caracalla 00100 Rome Tel.: 39.06.57051 Telex: 625825-625853
Testing Railway Safety Critical Workers for Drugs and Alcohol
 Rail Industry Standard RIS-8070-TOM Issue One Date December 2016 Critical Workers for Drugs and Alcohol Synopsis This document sets out common requirements for drugs and alcohol testing of staff carrying
Rail Industry Standard RIS-8070-TOM Issue One Date December 2016 Critical Workers for Drugs and Alcohol Synopsis This document sets out common requirements for drugs and alcohol testing of staff carrying