Management of Acute Asthma Exacerbations in Children 2012 Update. Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch
|
|
|
- Kristian Chambers
- 5 years ago
- Views:
Transcription


1 Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch

2 Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines Presentation Prof Tex Kissoon, CritSat Congress, Cape Town 2008
3 Definition: ATS / ERS 2009 Severe asthma exacerbations: Events that require urgent attention on the part of the patient and physician to prevent a serious outcome, such as hospitalisation or death. The occurrence of either an asthma related hospitalisation or visit to the ED or an urgent care facility, leading to treatment with systemic (oral, IM or IV) CS or use of CS for at least 3 days. Forno Curr Opin Pulm Med 2012;18:63 9; Reddel ATS/ERS Task Force, AJRCCM 2009;180:59 99
4 Moderate asthma exacerbations: The occurrence of at least one of the following events for at least 2 days (without the need for systemic CS): deterioration in symptoms, deterioration in lung function, and/or increased rescue bronchodilator use ED visits not requiring CS classified as moderate disease exacerbations Mild asthma exacerbation: just outside normal range of variation for individual patient; difficult to distinguish from transient loss of asthma control Forno Curr Opin Pulm Med 2012;18:63 9 Reddel ATS/ERS Task Force, AJRCCM 2009;180:59 99
5 Severe asthma exacerbations Occur in patients with all degrees of asthma severity Even patients thought to have mild, easy totreat asthma can experience severe exacerbations, sometimes even fatal 1 severe exacerbation per patient with mild asthma per year Almost all develop over 5 7 days rather than acute catastrophic events; gradual increase in sx and deterioration in lung function Most resolve over 7 10 days after Rx initiated O'Byrne JACI 2011
6 Environmental factors associated with asthma exacerbations Upper respiratory tract infections Human rhinovirus infection Interaction with sensitisation & allergen exposure Passive smoke exposure Gene environment interactions O'Byrne JACI 2011


7 Objective Evaluation Respiratory rate Retraction Ability to speak Ability to feed Peak flow O 2 saturation
8 Danger Signs in Acute Asthma Rising pulse rate Pulsus paradoxus Agitation, restlessness or consciousness Silent chest on auscultation Chest pain Cyanosis Peak flow < 50% predicted Rising PaCO 2

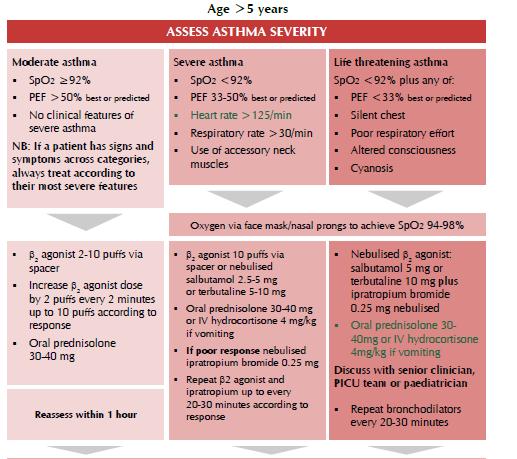
9 Assessment of severity
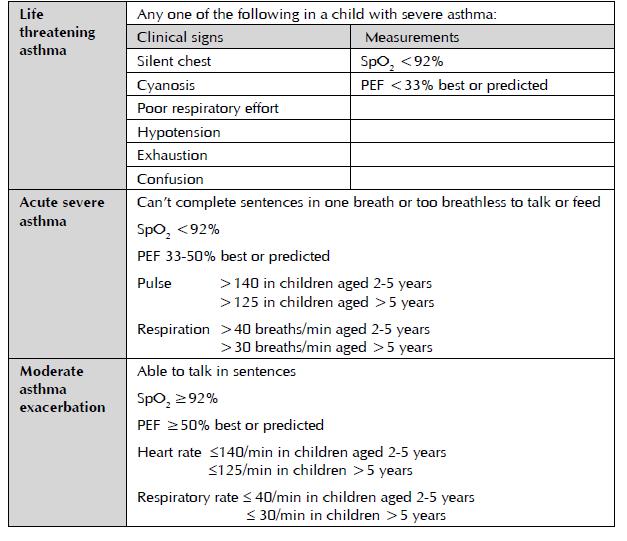
10
11 Oxygen Administer in all cases if unable to monitor saturations Oxygen levels in patients with acute asthma should be maintained at SpO % Oxygen saturation should be measured by pulse oximeters in adults and children. Pulse oximeters should therefore be available in both primary and secondary care settings If SpO 2 <92% in air after initial bronchodilators, admit to hospital
12 How would you treat? β2 agonist? Delivered how? One or more? Ipratropium? One or more? How frequently? Steroids? When? Route? Which steroid? Dose? If he doesn t improve, then what? Continue same therapy? Other options? Tex Kissoon, CritSat Congress 2008
 Repeated β2 agonist aerosols")

13 The Golden Hour MDI with spacer (unless hypoxic) Repeated β2 agonist aerosols Repeated ipratropium aerosols Early oral steroid Tex Kissoon, CritSat Congress 2008
14 MDI & Spacer vs Nebuliser Mild asthma: MDI/spacer better Schuh J Pediatr 1999 Cochrane Review Cates CJ 2006, updated RCTs ED & community Settings 2295 children > 2 years & 614 adults 6 RCTs inpatients with acute asthma 213 children & 28 adults MDI spacer outcomes at least equivalent to nebulisers Spacers may have some advantages for children in acute asthma (shorter LOS, lower pulse rate) Home made spacers no different from commercially produced spacers Zar Lancet 1999, Rodriguez Martinez Cochrane Review 2008

15 Initial treatment β2 agonist aerosols 1
16 β2 agonist aerosols 2 Inhaled β2 agonists are first line treatment for acute asthma 2 4 puffs of salbutamol 100 mcg repeated every minutes depending on response Single puffs, one at a time, inhaled separately with 5 tidal breaths If hourly doses of bronchodilators required for > 4 6 hours, switch to nebulised bronchodilators
17 β2 agonist aerosols 2 Life threatening asthma (SpO 2 <92%): give frequent doses of nebulised bronchodilators driven by oxygen (2.5 5 mg salbutamol) Repeat doses every minutes
18 β2 agonist x 3 over 60 minutes Continuous vs. Intermittent Nebulisation Camargo CA Cochrane Review 2003, updated to RCTs, 461 patients total Hospital admission: those with severe airway obstruction benefitted most Small but statistically significant improvement in pulmonary function tests No difference in side effects BTS: no difference, but old references
19 Anticholinergic therapy for acute asthma in children Inhaled anticholinergic as single agent bronchodilators less efficacious than β2 agonists Inhaled anticholinergic less efficacious than inhaled anticholinergic combined with β2 agonists Six studies, unclear quality Teoh Cochrane review April 2011, published 2012
20 Ipratropium x 3 over 60 minutes Combined inhaled anticholinergics and β2 agonists for initial treatment of acute asthma in children (18 months to 17 years) Plotnick Cochrane Review 2000, published 2008 Single dose 5 RCTs, 453 patients Small difference in PFTs, no difference in admissions Multiple doses 7 RCTs, 1045 patients Greater improvement in PFTs NNT 12.5; if severe acute attack, NNT 7 Multiple doses preferred to single dose; use in schoolage children with severe exacerbations Safe, improves lung function
21 Early Steroids Early ED treatment of acute asthma with systemic corticosteroids (CS)(< 60 minutes) Rowe BH Cochrane Review 2001 RCTs, IV/IM or oral CS vs placebo 12 RCTs, 863 patients Significant reduction in hospital admission Benefits greatest with more severe asthma 3 RCTs using oral steroids in children Good response, reduced admission

22 Summary: Golden Hour Strong Evidence MDI with spacer Repeated β2 agonists Repeated ipratropium bromide Early oral steroids Tex Kissoon, CritSat Congress 2008
23 What next? Observe response Good response: not tachypnoeic, minimal wheezing, no retraction, able to speak & feed, PEF 80% predicted/best If good response, observe x 1 hour Discharge with written action plan and followup appointment
24 Poor response what now? Incomplete / poor response: Tachypnoeic Persistent wheezing Retraction present Impaired speech or feeding PEF 79% predicted or personal best Admit to hospital Continue oxygen, nebulised SABA+IB, oral corticosteroids
25 Additional therapy? What about? Intravenous β2 agonist? Intravenous magnesium sulphate? Intravenous theophylline? Adrenaline? Tex Kissoon, CritSat Congress 2008
26 Intravenous β2 Agonists IV salbutamol as once off dose 15 mcg/kg over 10 minutes in children with acute asthma in ED IV + nebulised salbutamol vs nebulised salbutamol only 29 children, severe symptoms Discharged 10 hrs earlier Browne Lancet 1997 IV+nebulised salbutamol vs nebulised salbutamol + ipratropium 55 children, severe symptoms Discharged 28 hrs earlier Browne Pediatr Crit Care Med 2002
27 Intravenous β2 Agonists IV β2 agonists for acute asthma in ED 15 RCTs, 584 patients Travers AA Cochrane Review 2000, published 2012 IV selective or non selective β2 agonists vs placebo, inhaled β2 agonists or other standard of care Adults & children IV β2 agonists conferred no advantage over comparator regimens
28 Intravenous Magnesium Sulphate Magnesium sulphate for treating exacerbations of acute asthma in ED Bota G Cochrane Review trials (5 adult, 2 paediatric), 665 patients Non significant improvements in PEF except in patients with severe acute asthma Hospital admissions reduced only in severe group Probably provides additional benefit (less hospitalization) in severe acute asthma in children Cheuk DKL A meta analysis on intravenous magnesium sulphate for treating acute asthma. Arch Dis Child 2005
29 Aminophylline Narrow therapeutic index Potentially severe side effects Cardiac arrhythmias Hypotension Convulsions Only used for severely ill children in ICU with cardiac monitoring & measurement of serum levels
30 Intravenous Aminophylline IV aminophylline for acute severe asthma in children >2 years receiving inhaled bronchodilators Mitra Cochrane Review 2007, published 2009 Inpatients, severe asthma 7 RCTs, 380 children Improved lung function by 6 hrs No difference in LOS, no of nebs; unable to assess PICU admission or MV More vomiting IV salbutamol bolus vs aminophylline infusion in children with severe asthma Roberts Thorax 2003 Inpatients, severe, nonresponsive to Rx RCT, 54 children IV salbutamol bolus vs aminophylline bolus + infusion No difference in clinical score in first 2 hours However shorter LOS in aminophylline group
31 Inhaled magnesium sulphate MgSO 4 + ß 2 agonists vs ß 2 agonists alone; Outcome admission to hospital Six RCTs, 296 patients. 4 studies MgSO 4 + ß 2 agonists vs ß 2 agonists alone; 2 studies MgSO 4 vs ß 2 agonists alone Improved pulmonary function; trend towards benefit in hospital admission Blitz M, et al. Inhaled magnesium sulfate in the treatment of acute asthma. Cochrane Review 2005, edited & published Tex Kissoon, CritSat Congress 2008
32 Adrenaline Given subcutaneously (0.01 ml/kg of 1:1000 solution) Only if no nebuliser or p MDI available OR If patient moribund and unable to benefit from inhaled therapy
33 Leukotriene receptor antagonists Oral montelukast as add on therapy: decrease symptoms, hospitalisation, steroid use Harmanci Ann Allergy Asthma Immunol 2006 Robertson AJRCCM 2007; Nelson Pediatr Emerg Care 2008 Capsomidis Arch Dis Child 2010 IV montelukast added to standard care in adults improved FEV 1 Ramsay Thorax 2011 Oral LTA + usual care in children (3 trials, 194 children): no difference IV LTA (1 trial, 276 children): decreased hospital admission, no difference FEV 1 Watts Cochrane review 2012
34 Respiratory failure
35 Features suggesting impending respiratory failure in children with acute asthma Disturbance in level of consciousness Inability to speak in sentences Inability to feed properly Severely decreased or absent breath sounds ( silent chest ) Central cyanosis very late sign Normal pco 2 on arterial blood gas
36 Indications for admission to ICU Poor response to maximal pharmacologic therapy in ward / emergency room Cyanosis and hypoxaemia (PaO 2 < 8kPa) unrelieved by O 2 PaCO 2 > 4.5kPa PEFR < 30% predicted or best Minimal chest movement, silent chest Severe retraction Deteriorating mental status, lethargy or agitation Cardio respiratory arrest
37 ICU management of acute severe asthma Oxygen Continuous nebulised SABA; add ipratropium 4 hourly IV corticosteroids IV magnesium sulphate IV salbutamol and/or aminophylline infusions Intubation and ventilation Inhaled anaesthetic gas, ketamine
38 Acute asthma: unproven therapies Routine antibiotics Graham V Cochrane Review 2001 Physiotherapy Mucolytics Antihistamines Heliox Rodrigo GJ Cochrane Review 2006
39 Other considerations

40 PEF

41 Chest X ray

42 Arterial blood gases NB: initial response to acute asthma is to lower pco 2, so if pco2 is within normal limits, the child is already in impending respiratory failure
43

44
45 Summary: Rx acute asthma First line therapy Supplemental Oxygen (maintain SpO %) Inhaled ß2 agonist (pmdi spacer) Steroids ± Inhaled ipratropium bromide
46 Summary: Rx acute asthma 2 Second line therapy Add inhaled ipratropium bromide IV ß2 agonist IV magnesium sulphate IV aminophylline
Supplementary Medications during asthma attack. Prof. Dr Finn Rasmussen PhD. DrMedSc. Near East University Hospital North Cyprus
 Supplementary Medications during asthma attack Prof. Dr Finn Rasmussen PhD. DrMedSc. Near East University Hospital North Cyprus Conflicts of Interest None Definition of Asthma Airway narrowing that is
Supplementary Medications during asthma attack Prof. Dr Finn Rasmussen PhD. DrMedSc. Near East University Hospital North Cyprus Conflicts of Interest None Definition of Asthma Airway narrowing that is
Management of acute asthma in children in emergency department. Moderate asthma
 152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
Predicting, Preventing and Managing Asthma Exacerbations. Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa
 Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
PEDIATRIC ACUTE ASTHMA SCORE (P.A.A.S.) GUIDELINES. >97% 94% to 96% 91%-93% <90% Moderate to severe expiratory wheeze
 GUIDELINES. >97% 94% to 96% 91%-93% <90% Moderate to severe expiratory wheeze") Inclusion: Children experiencing acute asthma exacerbation 24 months to 18 years of age with a diagnosis of asthma Patients with a previous history of asthma (Consider differential diagnosis for infants
Inclusion: Children experiencing acute asthma exacerbation 24 months to 18 years of age with a diagnosis of asthma Patients with a previous history of asthma (Consider differential diagnosis for infants
Exacerbations. Ronald Dahl, Aarhus University Hospital, Denmark
 1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
Management of acute severe asthma in adults in general practice. Moderate asthma Acute severe asthma Life-threatening asthma INITIAL ASSESSMENT
 British guideline on the management of asthma Annex 2 Management of acute severe asthma in adults in general practice Many deaths from asthma are preventable. Delay can be fatal. Factors leading to poor
British guideline on the management of asthma Annex 2 Management of acute severe asthma in adults in general practice Many deaths from asthma are preventable. Delay can be fatal. Factors leading to poor
Nguyen Tien Dung A/Prof. PhD. MD Head of Pediatric Department - Bach Mai Hospital
 Nguyen Tien Dung A/Prof. PhD. MD Head of Pediatric Department - Bach Mai Hospital A girl patient 11 years old admitted to Bach mai Hospital at 4h15, 12nd November because of difficult breathing She has
Nguyen Tien Dung A/Prof. PhD. MD Head of Pediatric Department - Bach Mai Hospital A girl patient 11 years old admitted to Bach mai Hospital at 4h15, 12nd November because of difficult breathing She has
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
AT TRIAGE. Alberta Acute Childhood Asthma Pathway: Evidence based* recommendations For Emergency / Urgent Care
 1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
Recurrent wheezing illnesses 24.9% Similar to Australia Above global averages
 Prof Mike South Department of General Medicine Royal Children s Hospital Melbourne Australia www.mikesouth.org.au Asthma is very common in Australia Approx 25% children have recurrent wheezing illnesses
Prof Mike South Department of General Medicine Royal Children s Hospital Melbourne Australia www.mikesouth.org.au Asthma is very common in Australia Approx 25% children have recurrent wheezing illnesses
 β 2004 2004 o β β β β 2004 β β β β β β β β β 2004 2004 2004 2004 2004 β 2004 2004 2004 2004 β β 2004 β β β β β β β 2004 β β β β β β 2004 β β β β STEP 5: CONTINUOUS OR FREQUENT USE OF ORAL
β 2004 2004 o β β β β 2004 β β β β β β β β β 2004 2004 2004 2004 2004 β 2004 2004 2004 2004 β β 2004 β β β β β β β 2004 β β β β β β 2004 β β β β STEP 5: CONTINUOUS OR FREQUENT USE OF ORAL
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
Medicine Dr. Kawa Lecture 4 - Treatment of asthma :
 Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
10/6/2014. Tommy s Story: An Overview of Asthma Mangement. Disclosure. Objectives for this talk.
 Tommy s Story: An Overview of Asthma Mangement Clifton C. Lee, MD, FAAP, FHM Associate Professor of Pediatrics Chief, Pediatric Hospital Medicine Children s Hospital of Richmond at VCU Disclosure Obviously,
Tommy s Story: An Overview of Asthma Mangement Clifton C. Lee, MD, FAAP, FHM Associate Professor of Pediatrics Chief, Pediatric Hospital Medicine Children s Hospital of Richmond at VCU Disclosure Obviously,
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Title Protocol for the Management of Asthma
 Document Control Title Protocol for the Management of Asthma Author Author s job title Professional Lead, Minor Injuries Unit Directorate Emergency Services, Logistics and Resilience Department Version
Document Control Title Protocol for the Management of Asthma Author Author s job title Professional Lead, Minor Injuries Unit Directorate Emergency Services, Logistics and Resilience Department Version
Emergency Asthma Care
 Emergency Asthma Care Contents Introduction 3 Why good emergency asthma care is important 4 Access to emergency asthma care 5 How to improve emergency asthma care 6 Developing emergency asthma treatment
Emergency Asthma Care Contents Introduction 3 Why good emergency asthma care is important 4 Access to emergency asthma care 5 How to improve emergency asthma care 6 Developing emergency asthma treatment
Asthma Care in the Emergency Department Clinical Practice Guideline
 Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Asthma/wheeze management plan
 Asthma/wheeze management plan Name of Patient Date of Birth NHS Number GP surgery Telephone Next appointment Children s Assessment unit/ward telephone Out of hours call 111 Open access Y/N Until date Some
Asthma/wheeze management plan Name of Patient Date of Birth NHS Number GP surgery Telephone Next appointment Children s Assessment unit/ward telephone Out of hours call 111 Open access Y/N Until date Some
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
(PLACE PATIENT LABEL HERE) Date: Time: Assessment nurse: Sign: STOP!
 Date: Time: Assessment nurse: Sign: STOP!") ASTHMA BEST CARE BUNDLE P A T H W A Y ADULT ASTHMA Date: Time: Assessment nurse: Sign: INCLUSION CRITERIA Known asthmatic Shortness of breath and / or wheeze EXCLUSION CRITERIA Chronic lung disease other
ASTHMA BEST CARE BUNDLE P A T H W A Y ADULT ASTHMA Date: Time: Assessment nurse: Sign: INCLUSION CRITERIA Known asthmatic Shortness of breath and / or wheeze EXCLUSION CRITERIA Chronic lung disease other
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
Asthma Exacerbation Management in Children. Kong-Sang Wan, MD,PhD 温港生醫師 台北市聯合醫院仁愛院區小兒科
 Asthma Exacerbation Management in Children Kong-Sang Wan, MD,PhD 温港生醫師 台北市聯合醫院仁愛院區小兒科 Hypocapnia & respiratory alkalosis due to increase resp. rate Symptom classification Severe persistent - day: continue
Asthma Exacerbation Management in Children Kong-Sang Wan, MD,PhD 温港生醫師 台北市聯合醫院仁愛院區小兒科 Hypocapnia & respiratory alkalosis due to increase resp. rate Symptom classification Severe persistent - day: continue
Children & Young People s Directorate Paediatric-Neonatal Guidelines Checklist & Version Control Sheet
 1 Children & Young People s Directorate Paediatric-Neonatal Guidelines Checklist & Version Control Sheet 1 Name of Guideline / Policy/ Procedure MANAGEMENT OF ACUTE PAEDIATRIC ASTHMA Purpose of Procedure/
1 Children & Young People s Directorate Paediatric-Neonatal Guidelines Checklist & Version Control Sheet 1 Name of Guideline / Policy/ Procedure MANAGEMENT OF ACUTE PAEDIATRIC ASTHMA Purpose of Procedure/
Bronchospasm & SOB. Kim Kilmurray Senior Clinical Teaching Fellow
 Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma
 Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma Talk Outline Case Delivery of bronchodilators Meter-dose inhalers and spacers Continuous nebulization
Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma Talk Outline Case Delivery of bronchodilators Meter-dose inhalers and spacers Continuous nebulization
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
LRI Children s Hospital
 LRI Children s Hospital Asthma Management in Children On-going Care after Admission to Ward Staff relevant to: Medical & Nursing staff providing asthma management care to Children within UHL Children s
LRI Children s Hospital Asthma Management in Children On-going Care after Admission to Ward Staff relevant to: Medical & Nursing staff providing asthma management care to Children within UHL Children s
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
Asthma. chapter 7. Overview
 chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
Emergency Department Protocol Initiative
 Emergency Department Protocol Initiative ACUTE ASTHMA MANAGEMENT TOOLKIT March 2006 Provincial Emergency Services Project PHYSICIAN ORDER TEMPLATE FOR CTAS LEVEL 1 ASTHMA ADULT PEDIATRIC Date: Site: Arrival
Emergency Department Protocol Initiative ACUTE ASTHMA MANAGEMENT TOOLKIT March 2006 Provincial Emergency Services Project PHYSICIAN ORDER TEMPLATE FOR CTAS LEVEL 1 ASTHMA ADULT PEDIATRIC Date: Site: Arrival
patient group direction
 SALBUTAMOL v01 1/12 SALBUTAMOL PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
SALBUTAMOL v01 1/12 SALBUTAMOL PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
Asthma and COPD in the ICU
 Asthma and COPD in the ICU Prescott Woodruff, MD, MPH Assistant Professor Medicine in Residence Pulmonary and Critical Care Medicine, Department of Medicine Acute Exacerbations of Asthma Asthma exacerbations
Asthma and COPD in the ICU Prescott Woodruff, MD, MPH Assistant Professor Medicine in Residence Pulmonary and Critical Care Medicine, Department of Medicine Acute Exacerbations of Asthma Asthma exacerbations
Clinical guideline for acute wheeze & asthma in children 5 years and over Hospital care
 Clinical guideline for acute wheeze & asthma in children years and over Hospital care Airedale NHS Trust Bradford Teaching Hospitals NHS Foundation Trust NHS Bradford and Airedale DOB: A&E/Hospital : Weight:
Clinical guideline for acute wheeze & asthma in children years and over Hospital care Airedale NHS Trust Bradford Teaching Hospitals NHS Foundation Trust NHS Bradford and Airedale DOB: A&E/Hospital : Weight:
1. What is delayed sequence intubation? Can it be used for severe Asthma exacerbation? 2. What about pregnancy and Asthma is so important?
 Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
GUIDELINES LET S TALK ABOUT THE ASTHMA ...MADE MORE PRACTICAL GUIDELINES FOR PRACTICE...
 LET S TALK ABOUT THE ASTHMA GUIDELINES GUIDELINES FOR PRACTICE......MADE MORE PRACTICAL NICE quality standard QOF asthma indicators BTS/SIGN guidelines Provided as a service to medicine by Teva UK Limited.
LET S TALK ABOUT THE ASTHMA GUIDELINES GUIDELINES FOR PRACTICE......MADE MORE PRACTICAL NICE quality standard QOF asthma indicators BTS/SIGN guidelines Provided as a service to medicine by Teva UK Limited.
ACUTE ASTHMA (WARD) Paediatrics > Scenario 5
 Paediatrics > Scenario 5") ACUTE ASTHMA (WARD) MODULE: BREATHING TARGET: ALL PAEDIATRIC TRAINEES; ED NURSING STAFF BACKGROUND: Acute asthma is a common presentation in the Emergency Department, and many of these children are admitted
ACUTE ASTHMA (WARD) MODULE: BREATHING TARGET: ALL PAEDIATRIC TRAINEES; ED NURSING STAFF BACKGROUND: Acute asthma is a common presentation in the Emergency Department, and many of these children are admitted
Practical Approach to Managing Paediatric Asthma
 Practical Approach to Managing Paediatric Asthma Dr Andrew Tai FRACP, PhD Paediatric Respiratory and Sleep Specialist Women's and Children's Hospital, Adelaide Approaching the patient Check the diagnosis
Practical Approach to Managing Paediatric Asthma Dr Andrew Tai FRACP, PhD Paediatric Respiratory and Sleep Specialist Women's and Children's Hospital, Adelaide Approaching the patient Check the diagnosis
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Type: Clinical Guideline Register No: Status: Public MANAGEMENT OF ACUTE ASTHMA IN CHILDREN MORE THAN 2 YEARS IN HOSPITAL
 MANAGEMENT OF ACUTE ASTHMA IN CHILDREN MORE THAN 2 YEARS IN HOSPITAL Type: Clinical Guideline Register No: 09055 Status: Public Developed in Response to: Best practice CQC Fundamental Standard: 9, 12,
MANAGEMENT OF ACUTE ASTHMA IN CHILDREN MORE THAN 2 YEARS IN HOSPITAL Type: Clinical Guideline Register No: 09055 Status: Public Developed in Response to: Best practice CQC Fundamental Standard: 9, 12,
control in the lowest dose providing adequate Maintain high dose ICS Use daily steroid tablet dose Consider trials of: Increasing ICS up to
 Summary of management in adults sthma - suspected dult asthma - diagnosed Diagnosis and ssessment Evaluation: assess symptoms, measure lung function, check inhaler technique and adherence adjust dose update
Summary of management in adults sthma - suspected dult asthma - diagnosed Diagnosis and ssessment Evaluation: assess symptoms, measure lung function, check inhaler technique and adherence adjust dose update
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis. Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine
 Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Acute NIV in COPD and what happens next. Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital
 Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Knowledge Translation and Emergency Medicine. Eddy Lang Jeremy Grimshaw Michael Brown
 Knowledge Translation and Emergency Medicine Eddy Lang Jeremy Grimshaw Michael Brown Knowledge Translation The exchange, synthesis and application of research evidence within a complex system of relationships
Knowledge Translation and Emergency Medicine Eddy Lang Jeremy Grimshaw Michael Brown Knowledge Translation The exchange, synthesis and application of research evidence within a complex system of relationships
The Acute & Maintenance Treatment of Asthma via Aerosolized Medications
 The Acute & Maintenance Treatment of Asthma via Aerosolized Medications Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Associate Professor and Chairman Department of Respiratory Therapy Objectives Define Asthma.
The Acute & Maintenance Treatment of Asthma via Aerosolized Medications Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Associate Professor and Chairman Department of Respiratory Therapy Objectives Define Asthma.
Management of wheeze in pre-school children. Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne
 Management of wheeze in pre-school children Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne General Practitioner encounters for asthma Asthma in Australia, 2003 Emergency
Management of wheeze in pre-school children Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne General Practitioner encounters for asthma Asthma in Australia, 2003 Emergency
INPATIENT ASTHMA CARE PROTOCOL
 INPATIENT ASTHMA CARE PROTOCOL When ordered by a physician, an eligible child 2 years of age or older who is admitted to the General Pediatric Inpatient Unit at the Children s Hospital of Georgia with
INPATIENT ASTHMA CARE PROTOCOL When ordered by a physician, an eligible child 2 years of age or older who is admitted to the General Pediatric Inpatient Unit at the Children s Hospital of Georgia with
Episode 79 Pediatric Asthma
 Reliable Validated Measures of Pediatric Asthma Episode 79 Pediatric Asthma With Dr. Dennis Scolnik & Dr. Sanjay Mehta Prepared by Dr. Anton Helman, April 2016 Pediatric Asthma Severity Indicators life-threatening
Reliable Validated Measures of Pediatric Asthma Episode 79 Pediatric Asthma With Dr. Dennis Scolnik & Dr. Sanjay Mehta Prepared by Dr. Anton Helman, April 2016 Pediatric Asthma Severity Indicators life-threatening
GUIDE LINE SUMMARY THE DIAGNOSIS AND TREATMENT OF ADULT ASTHMA BEST PRACTICE EV I DENCE-BASED KEY MESSAGES. Diagnosis.
 THE DIAGSIS AND TREATMENT OF ADULT ASTHMA The purpose of the guideline is to provide an evidence-based summary of the diagnostic management and treatment options available for asthma in the adult population
THE DIAGSIS AND TREATMENT OF ADULT ASTHMA The purpose of the guideline is to provide an evidence-based summary of the diagnostic management and treatment options available for asthma in the adult population
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Advanced Pediatric Emergency Medicine Assembly
 (+)Charles Macias, MD, FACEP Associate Professor of, Section of Emergency Medicine, Baylor College of Medicine; Director, Evidence Based Outcomes Center and Center for Clinical Effectiveness, Baylor College
(+)Charles Macias, MD, FACEP Associate Professor of, Section of Emergency Medicine, Baylor College of Medicine; Director, Evidence Based Outcomes Center and Center for Clinical Effectiveness, Baylor College
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
MANAGEMENT OF AN ACUTE EPISODE OF ASTHMA IN CHILDREN
 MANAGEMENT OF AN ACUTE EPISODE OF ASTHMA IN CHILDREN Dr. Ebor Jacob 1, Dr. Manivachagan 2, Dr. Amith Balachandran 3 1 Professor, 2 Associate Professor, Paediatric ICU, Christian Medical College, Vellore.
MANAGEMENT OF AN ACUTE EPISODE OF ASTHMA IN CHILDREN Dr. Ebor Jacob 1, Dr. Manivachagan 2, Dr. Amith Balachandran 3 1 Professor, 2 Associate Professor, Paediatric ICU, Christian Medical College, Vellore.
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
ACUTE ASTHMA (PAEDIATRIC)
") ACUTE ASTHMA (PAEDIATRIC) MODULE: BREATHING TARGET: ALL PAEDIATRIC TRAINEES; ED TRAINEES BACKGROUND: Acute asthma is a common presentation to the Emergency Department. Every 17 minutes a child is admitted
ACUTE ASTHMA (PAEDIATRIC) MODULE: BREATHING TARGET: ALL PAEDIATRIC TRAINEES; ED TRAINEES BACKGROUND: Acute asthma is a common presentation to the Emergency Department. Every 17 minutes a child is admitted
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Efficacy of Nebulised Ipratropium in Acute Bronchial Asthma
 ORIGINAL ARTICLE JIACM 2002; 3(4): 353-59 Efficacy of Nebulised Ipratropium in Acute Bronchial Asthma Praveen Aggarwal*, Onkar Singh**, Jyoti P Wali***, Rohini Handa*, Sada N Dwivedi****, Ashutosh Biswas*****,
ORIGINAL ARTICLE JIACM 2002; 3(4): 353-59 Efficacy of Nebulised Ipratropium in Acute Bronchial Asthma Praveen Aggarwal*, Onkar Singh**, Jyoti P Wali***, Rohini Handa*, Sada N Dwivedi****, Ashutosh Biswas*****,
DATE: 09 December 2009 CONTEXT AND POLICY ISSUES:
 TITLE: Tiotropium Compared with Ipratropium for Patients with Moderate to Severe Chronic Obstructive Pulmonary Disease: A Review of the Clinical Effectiveness DATE: 09 December 2009 CONTEXT AND POLICY
TITLE: Tiotropium Compared with Ipratropium for Patients with Moderate to Severe Chronic Obstructive Pulmonary Disease: A Review of the Clinical Effectiveness DATE: 09 December 2009 CONTEXT AND POLICY
Treatment of Acute Asthma Exacerbations in Adults in the Primary Care or Urgent Care Setting Clinical Practice Guideline MedStar Health.
 Treatment of Acute Asthma Exacerbations in Adults in the Primary Care or Urgent Care Setting Clinical Practice Guideline MedStar Health Background: These guidelines are provided to assist physicians and
Treatment of Acute Asthma Exacerbations in Adults in the Primary Care or Urgent Care Setting Clinical Practice Guideline MedStar Health Background: These guidelines are provided to assist physicians and
PAEDIATRIC RESPIRATORY FAILURE. Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre
 PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
Sample. Affix patient label within this box.
 Instructions for completing orders Complete pages 1-3 for General Inpatient Orders. All pathway compatible orders (indicated by ) within the General Inpatient Orders will be followed automatically. Optional
Instructions for completing orders Complete pages 1-3 for General Inpatient Orders. All pathway compatible orders (indicated by ) within the General Inpatient Orders will be followed automatically. Optional
ASTHMA (SEE BTS GUIDELINES NEXT PAGE)
") ASTHMA (SEE BTS GUIDELINES NEXT PAGE) RESPIRATORY Signs of Severe asthma Unable to speak in sentences? Peak flow < 50% predicted or best? Respiratory Rate >25/min? Pulse>110/min? Sa0 2
ASTHMA (SEE BTS GUIDELINES NEXT PAGE) RESPIRATORY Signs of Severe asthma Unable to speak in sentences? Peak flow < 50% predicted or best? Respiratory Rate >25/min? Pulse>110/min? Sa0 2
Acute Asthma in the Emergency Room
 Acute Asthma in the Emergency Room José A. Castro-Rodríguez, MD, PhD Escuela de Medicina Pontificia Universidad Católica de Chile Potential ConConflict of Interest: In the last three years, I received
Acute Asthma in the Emergency Room José A. Castro-Rodríguez, MD, PhD Escuela de Medicina Pontificia Universidad Católica de Chile Potential ConConflict of Interest: In the last three years, I received
Allwin Mercer Dr Andrew Zurek
 Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Sample. Affix patient label within this box.
 Instructions for completing orders: Determine PRAM Clinical Score as per the Alberta Acute Childhood Asthma Pathway for Emergent/Urgent Care and select orders based on PRAM Score. Custom orders can be
Instructions for completing orders: Determine PRAM Clinical Score as per the Alberta Acute Childhood Asthma Pathway for Emergent/Urgent Care and select orders based on PRAM Score. Custom orders can be
The Office of Evidence Based Practice, 2011 Center of Clinical Effectiveness. Importance. Quality. No of studies
 Question 6: In the child with asthma exacerbation in the ED should magnesium sulfate IV be used prevent hospitalization, decrease time in the ED, and improve pulmonary function? GRADEprofiler Table: Rowe
Question 6: In the child with asthma exacerbation in the ED should magnesium sulfate IV be used prevent hospitalization, decrease time in the ED, and improve pulmonary function? GRADEprofiler Table: Rowe
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
Asthma Guidelines and Pharmacological Treatment. Dr James Wilkinson
 Asthma Guidelines and Pharmacological Treatment Dr James Wilkinson Asthma is a common disease in the UK 5.4 million people in the UK are currently receiving treatment for asthma: 4.3 million adults (1
Asthma Guidelines and Pharmacological Treatment Dr James Wilkinson Asthma is a common disease in the UK 5.4 million people in the UK are currently receiving treatment for asthma: 4.3 million adults (1
REVIEW AMINOPHYLLINE. Background
 REVIEW AMINOPHYLLINE Background The current 13 th edition of the WHO Model Essential Medicines List (dated April 2003) includes aminophylline on the Complementary List. The listing is as shown below (together
REVIEW AMINOPHYLLINE Background The current 13 th edition of the WHO Model Essential Medicines List (dated April 2003) includes aminophylline on the Complementary List. The listing is as shown below (together
SCVMC RESPIRATORY CARE PROCEDURE
 Page 1 of 8 Rev. - 11/99, 11/05, 4/11 R-NC - 08/99,08/00, 04/03,10/08,04/09, 07/11, 6/12 B7180-43 OBJECTIVE Continuous Nebulization allows for continuous, controlled drug delivery to the lung, avoiding
Page 1 of 8 Rev. - 11/99, 11/05, 4/11 R-NC - 08/99,08/00, 04/03,10/08,04/09, 07/11, 6/12 B7180-43 OBJECTIVE Continuous Nebulization allows for continuous, controlled drug delivery to the lung, avoiding
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma
 with asthma") Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Acute Asthma in Adults and Children
 Guideline for The Management of Administered by the Alberta Medical Association Acute Asthma in Adults and Children This guideline has been adapted from the CAEP guidelines for Acute Asthma Management
Guideline for The Management of Administered by the Alberta Medical Association Acute Asthma in Adults and Children This guideline has been adapted from the CAEP guidelines for Acute Asthma Management
EXACERBATIONS IN ADULTS WHEN TO REFER
 06 Bronchial Asthma Contributors: Dr Chong Phui Nah Dr Tang Wern Ee PRESENTATION AND DIAGNOSIS CLASSIFICATION OF ASTHMA BY LEVEL OF CONTROL ASSESSMENT OF ASTHMA CONTROL USING THE ASTHMA CONTROL TEST ASTHMA
06 Bronchial Asthma Contributors: Dr Chong Phui Nah Dr Tang Wern Ee PRESENTATION AND DIAGNOSIS CLASSIFICATION OF ASTHMA BY LEVEL OF CONTROL ASSESSMENT OF ASTHMA CONTROL USING THE ASTHMA CONTROL TEST ASTHMA
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
In 2005, the prevalence of asthma in the. Management of Acute Asthma Exacerbations
 Management of Acute Asthma Exacerbations SUSAN M. POLLART, MD, MS; REBEKAH M. COMPTON, MSN, FNP-C; and KURTIS S. ELWARD, MD, MPH University of Virginia Health System, Charlottesville, Virginia Asthma exacerbations
Management of Acute Asthma Exacerbations SUSAN M. POLLART, MD, MS; REBEKAH M. COMPTON, MSN, FNP-C; and KURTIS S. ELWARD, MD, MPH University of Virginia Health System, Charlottesville, Virginia Asthma exacerbations
Evaluation of the Use of High-Dose Inhaled Corticosteroids for the Treatment of Acute Asthma
 11 Inhaled Corticosteroids for Asthma Attacks ORIGINAL ARTICLE RAMR 2016;1:11-16 ISSN 1852-236X Evaluation of the Use of High-Dose Inhaled Corticosteroids for the Treatment of Acute Asthma Correspondence:
11 Inhaled Corticosteroids for Asthma Attacks ORIGINAL ARTICLE RAMR 2016;1:11-16 ISSN 1852-236X Evaluation of the Use of High-Dose Inhaled Corticosteroids for the Treatment of Acute Asthma Correspondence:
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Pediatric Respiratory Disease: A Model for the Future of Emergency Medicine Research
 Pediatric Respiratory Disease: A Model for the Future of Emergency Medicine Research Joseph J. Zorc, MD, MSCE Mark Fishman Professor, Department of Pediatrics Perelman School of Medicine, University of
Pediatric Respiratory Disease: A Model for the Future of Emergency Medicine Research Joseph J. Zorc, MD, MSCE Mark Fishman Professor, Department of Pediatrics Perelman School of Medicine, University of
Medical Emergencies at Moderate and High Altitude
 Medical Emergencies at Moderate and High Altitude Annalisa Cogo Clinica Pneumologica e Centro Studi Biomedici Applicati allo Sport Università di Ferrara Payer Hutte, Ortler Mountain Environment Barometric
Medical Emergencies at Moderate and High Altitude Annalisa Cogo Clinica Pneumologica e Centro Studi Biomedici Applicati allo Sport Università di Ferrara Payer Hutte, Ortler Mountain Environment Barometric
Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom
 Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom 2 BEYOND SYMPTOMS ADDRESSING FUTURE RISK IN ASTHMA South GP CME 2013,
Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom 2 BEYOND SYMPTOMS ADDRESSING FUTURE RISK IN ASTHMA South GP CME 2013,
An Audit on Hospital Management of Bronchial Asthma
 An Audit on Hospital Management of Bronchial Asthma Pages with reference to book, From 298 To 300 Javaid A. Khan, Shehryar Saghir, Ghazala Tabassum, S. Fayyaz Husain ( Department of Medicine, The Aga Khan
An Audit on Hospital Management of Bronchial Asthma Pages with reference to book, From 298 To 300 Javaid A. Khan, Shehryar Saghir, Ghazala Tabassum, S. Fayyaz Husain ( Department of Medicine, The Aga Khan
+ Asthma and Athletics
 + Asthma and Athletics Shaylon Rettig, MD, MBA Champion Sports Medicine + Financial Disclosure Dr. Shaylon Rettig has no relevant financial relationships with commercial interests to disclose. + Asthma
+ Asthma and Athletics Shaylon Rettig, MD, MBA Champion Sports Medicine + Financial Disclosure Dr. Shaylon Rettig has no relevant financial relationships with commercial interests to disclose. + Asthma
Decramer 2014 a &b [21]
![Decramer 2014 a &b [21]](/thumbs/90/101390504.jpg "Decramer 2014 a &b [21]") Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
BRONCHIOLITIS. See also the PSNZ guideline - Wheeze & Chest Infections in infants under 1 year (www.paediatrics.org.nz)
") Definition What is Bronchiolitis? Assessment Management Flow Chart Admission Guidelines Investigations Management Use of Bronchodilators Other treatments Discharge Planning Bronchiolitis & Asthma References
Definition What is Bronchiolitis? Assessment Management Flow Chart Admission Guidelines Investigations Management Use of Bronchodilators Other treatments Discharge Planning Bronchiolitis & Asthma References
INTERNAL ONLY STANDING ORDER EMERGENCY DEPARTMENTS SALBUTAMOL SULFATE Administration by Accredited Emergency Nurses for symptom relief of asthma
 POLICY STATEMENT This order may only be activated under the specific circumstances set out in the section Indications and provided there are no contraindications present. The administering nurse must be
POLICY STATEMENT This order may only be activated under the specific circumstances set out in the section Indications and provided there are no contraindications present. The administering nurse must be
Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma (Review)
 versus nebulisers for beta-agonist treatment of acute asthma (Review)") EVIDENCE-BASED CHILD HEALTH: A COCHRANE REVIEW JOURNAL Evid.-Based Child Health 1: 948 1017 (2006) Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/ebch.67 Holding chambers
EVIDENCE-BASED CHILD HEALTH: A COCHRANE REVIEW JOURNAL Evid.-Based Child Health 1: 948 1017 (2006) Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/ebch.67 Holding chambers
Air or oxygen as driving gas for nebulised salbutamol
 Archives of Disease in Childhood, 1988, 63, 9-94 Air or oxygen as driving gas for nebulised salbutamol J G A GLEESON, S GREEN, AND J F PRICE Paediatric Respiratory Laboratory, Department of Thoracic Medicine,
Archives of Disease in Childhood, 1988, 63, 9-94 Air or oxygen as driving gas for nebulised salbutamol J G A GLEESON, S GREEN, AND J F PRICE Paediatric Respiratory Laboratory, Department of Thoracic Medicine,
Asthma is global health problem in children,
 Paediatrica Indonesiana VOLUME 52 July NUMBER 4 Original Article Efficacy of salbutamol-ipratropium bromide nebulization compared to salbutamol alone in children with mild to moderate asthma attacks Matahari
Paediatrica Indonesiana VOLUME 52 July NUMBER 4 Original Article Efficacy of salbutamol-ipratropium bromide nebulization compared to salbutamol alone in children with mild to moderate asthma attacks Matahari
Over the last several years various national and
 Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Inhaled short-acting bronchodilators for managing emergency childhood asthma: an overview of reviews
 Allergy REVIEW ARTICLE Inhaled short-acting bronchodilators for managing emergency childhood asthma: an overview of reviews M. Pollock 1, I. P. Sinha 2, L. Hartling 1, B. H. Rowe 3, S. Schreiber 1 & R.
Allergy REVIEW ARTICLE Inhaled short-acting bronchodilators for managing emergency childhood asthma: an overview of reviews M. Pollock 1, I. P. Sinha 2, L. Hartling 1, B. H. Rowe 3, S. Schreiber 1 & R.
What s new in Asthma? Dr Alexandra Nanzer-Kelly Consultant Respiratory Physician Royal Brompton and Harefield Hospitals
 What s new in Asthma? Dr Alexandra Nanzer-Kelly Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Asthma is an inflammatory disease Relaxed smooth muscles Air trapped in alveoli Tightened
What s new in Asthma? Dr Alexandra Nanzer-Kelly Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Asthma is an inflammatory disease Relaxed smooth muscles Air trapped in alveoli Tightened