Supplementary Online Content
|
|
|
- Sibyl Maxwell
- 5 years ago
- Views:
Transcription
1 Supplementary Online Content Regan EA, Lynch DA, Curran-Everett D, et al; Genetic Epidemiology of COPD (COPDGene) Investigators. Clinical and radiologic disease in smokers with normal spirometry. Published online June 22, JAMA Intern Med. doi: /jamainternmed emethods. Detailed Methods efigure 1. Distribution of COPDGene Subjects by Age Group and GOLD Stages efigure 2. Current Smoking Declines in Older Age Groups efigure 3. Examples of CT Images in GOLD 0 Subjects etable 1. The COPDGene Cohort and Effect of Current Smoking etable 2. African American Subjects etable 3. Non-Hispanic White Subjects etable 4. Impairments in COPDGene Nonasthmatic Subjects etable NHANES Cohort Demographics etable 6. Predictors of Quality of Life by St George s Respiratory Score in COPDGene GOLD 0 Subjects This supplementary material has been provided by the authors to give readers additional information about their work.
2 emethods. Detailed Methods We used cross-sectional data from the initial COPDGene study visit ( ). The COPDGene study includes 10,300 subjects including self-described non-hispanic, White or African American subjects, age years, with at least a 10 pack-year smoking history; along with a comparison group of 108 never-smokers of a similar age range. IRB approval was obtained for the project at each clinical center and all participants provided written informed consent to participate. The details of the planned study design have been described previously 18. Smokers were enrolled based on smoking history and classified using GOLD spirometric criteria based on post-bronchodilator spirometry 17. Participants were recruited at 21 medical centers and their surrounding communities; never-smokers were recruited from a subset of 13 of these clinical centers. Recruitment strategies for non-copd smokers included outpatient clinics, word-of-mouth communication to friends and spouses of COPD subjects, advertisements, and outreach to community groups and churches. Clinical centers were instructed to not recruit non-copd subjects from pulmonary clinics. The never-smoker group was recruited to reflect a normal aging distribution for CT-based lung changes without any diagnosed lung disease and was permitted to have a variety of co-morbid conditions (n): BMI > 30 defined as obesity (34); cancer other than bronchogenic (8); coronary artery disease (CAD) (1); diabetes (10); and gastroesophageal reflux disease (GERD) (23). This report focuses on GOLD 0 subjects, defined as current and former smokers with normal post-bronchodilator FEV 1 /FVC ratio >0 7 and FEV 1 % predicted 80% (n = 4388 subjects). They were compared to: 1. never-smokers, 2. GOLD 1 subjects (FEV 1 /FVC ratio <0.7 & FEV 1 80% predicted) (n = 794 subjects) and 3. COPD cases GOLD 2-4 (n= 3690). Preserved Ratio Impaired Spirometry (PRISm) subjects 19,20 (FEV 1 /FVC ratio >0.7 & FEV 1 <80% predicted,) were not included in these analyses (n=1257).
3 Imaging Whole-lung volumetric CT images were acquired using multi-detector CT scanners at full inspiration and at the end of normal expiration. Detailed CT protocols for the COPDGene study have previously been published 15. Quantitative analysis of emphysema severity and gas trapping was performed on segmented images using Slicer software ( Percent emphysema was quantified as the percentage of lung volume with attenuation values <-950 Hounsfield Units (HU) on inspiratory images. Percent gas trapping was quantified as the percent of lung with attenuation values <- 856 HU on expiratory images. Segmental wall area percent (bronchial wall area as percentage of total bronchial area) was calculated using VIDA (VIDA Diagnostics, Coralville IA) software. Emphysema, gas trapping or airway wall measurements were not available in some subjects due to technical limitations. Spirometry and other data collected Each study subject had pre- and post-albuterol spirometry performed using a standardized protocol employing the EasyOne spirometer (ndd, Zurich, Switzerland). FEV 1 and FVC % predicted values were calculated according to the prediction equations by Hankinson et al. 16. Information collected from each subject included medications, medical history, St. George s Respiratory Questionnaire (SGRQ), American Thoracic Society (ATS) Respiratory Epidemiology Questionnaire, demographic information, height, weight, and oxygen saturation (on room air). A standardized 6-minute walk test was done on each subject according to ATS standards 17. Variable definitions Pack-years were calculated by taking the average number of cigarettes smoked per day divided by 20 and multiplied by the number of years smoked. Bronchodilator responsiveness (BDR) was considered positive if the subject had a 12% change in FEV 1 or FVC above pre-bronchodilator measurements and a
4 0.2L increase in FEV 1 or FVC. Chronic bronchitis was considered positive if the subject responded affirmatively to the questions: Do you cough like this on most days, for 3 consecutive months or more during the year? and Do you usually bring up phlegm on most days for 3 consecutive months or more during the year? for at least two years. The Modified Medical Research Council (MMRC) dyspnea score 18 was calculated based on the subject s response to five questions about dyspnea and ranged from no dyspnea 0, to mild -1, moderate - 2, severe -3 and very severe 4. A severe exacerbation was considered positive if the subject answered yes to the question, In the past year, have you been to the emergency room or hospitalized for lung problems?. Quality of life was assessed with a generic measure, the Medical Outcomes Study Short Form 36 version 2 (MOS SF-36 v2), and a disease-specific measure, the SGRQ 19. Coronary artery disease (CAD) was inferred from self-reports of any of the following: heart attack, coronary artery bypass graft surgery, coronary angioplasty, physician diagnosis of coronary artery disease, or angina. Gastro-Esophageal Reflux Disorder (GERD) was based on self-report of physician diagnosis. Visual Scoring of Chest CT scans CT scans were randomly selected for visual scoring in a subset of subjects (n=300 for GOLD 0 and 100 each for non-smokers and GOLD 1. The scans were read independently in a blinded fashion by up to five readers, and scans with divergent readings were re-read for a consensus score. The visual reading consisted of identifying the presence of emphysema and defining type (centrilobular, panlobular, mixed and paraseptal as present with or without another type), and also identifying definite airway thickening 20. Impairments in Smokers We defined seven characteristics of impairment to identify subjects in the GOLD 0 group who were negatively affected by smoking-related conditions. These were: chronic bronchitis, history of
5 respiratory exacerbations, dyspnea (MMRC score 2), quantitative emphysema score >5%, quantitative gas trapping score >20%, and SGRQ total score >25 (based on GOLD alternate to CAT classification for symptomatic disease 21 ), and six minute walk (6MW) distance <1150 feet (350 meters). Medication Use Respiratory medication use in the group was compared between subjects with and without any impairment by category (beta agonists, inhaled corticosteroids, and inhaled anti-cholinergics). National Health and Nutrition Examination Survey (NHANES) cohort We identified subjects from the NHANES dataset who were either: 1. neversmokers or 2. had similar smoking exposure to the COPDGene subjects (minimum of 10 pack years smoking). The selected NHANES subjects were those having recorded pre-bronchodilator spirometry values. Chest CT scans were not available for the NHANES group and therefore no assessment of emphysema, gas trapping or visual scoring could be done. The NHANES subjects were selected from a total of 20,686 enrolled subjects. To assess only NHANES subjects similar to COPDGene subjects, we excluded the following groups: subjects under age 45 and over age 80 (-14,421); Hispanic or mixed race subjects (-1997); never smokers with abnormal spirometry (-711); any subject with missing spirometry (-541); smokers whose spirometry was classified as PRISm 19,20 ; and smokers with <10 pack years of smoking history (-364). The final NHANES group for analysis was 2455 subjects. Statistical Analysis Analysis was done using JMP version 10 and SAS version 9.2 (both SAS, Cary, NC). Univariate comparisons were made using Chi Square and Fisher s exact test for dichotomous data; for continuous data, we used Student s t-test and Wilcoxon rank-sum test for normal and
6 non-normal data, respectively. An α <0.05 was considered significant. We estimated least square means for continuous variables after adjusting for age, gender, race and group in the basic description of the cohort in Table 1 as noted. We used multivariable regression to assess the factors predicting respiratory quality of life, as measured by the SGRQ Total score, among smokers with normal spirometry. Variables were selected for this model from univariate analyses showing significant differences between the study groups. Backwards stepwise selection was used to eliminate non-significant covariates from the model.
7 efigure 1. Distribution of COPDGene subjects by age group and GOLD stages. (Panel A. Non-smokers, Panel B. GOLD 0, Panel C. GOLD 1, Panel D. GOLD 2-4) Subjects were recruited as smokers with a minimum of 10 pack-years smoking and then classified by spirometry. No attempt was made to balance recruitment by age. Within the COPDGene cohort, younger age groups make up a greater proportion of subjects in the smokers with normal spirometry group that is the focus of this report.
8
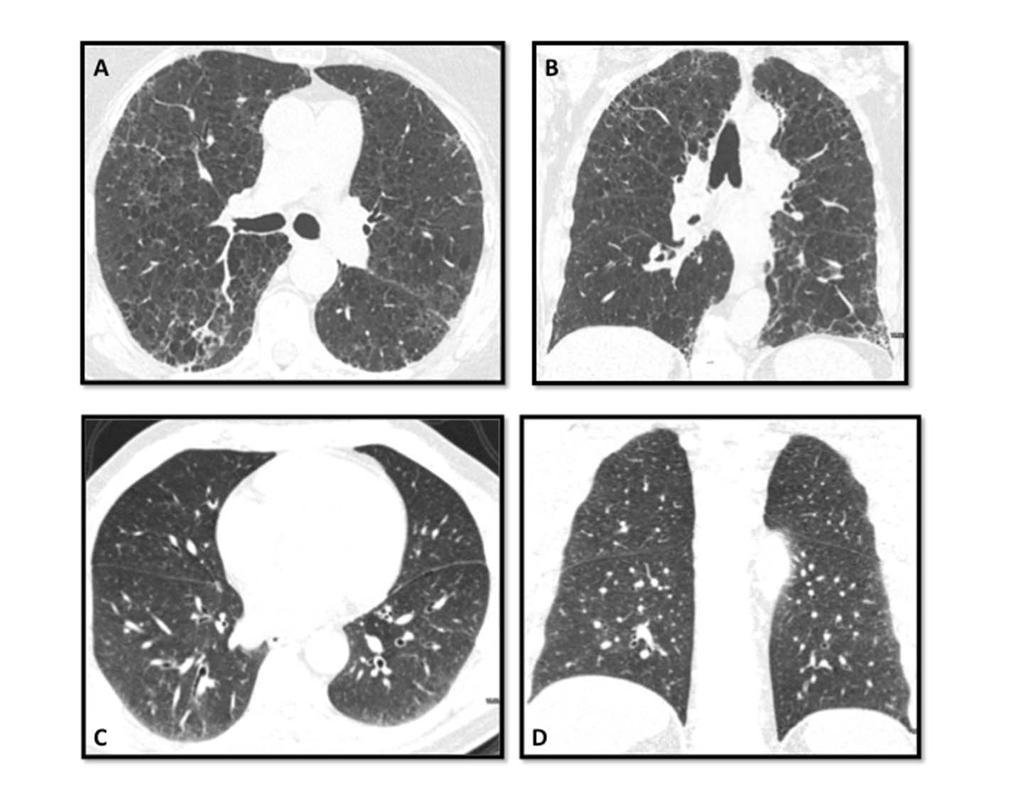
9 efigure 2. Examples of CT Images in GOLD 0 Subjects Panels A and B: Extensive emphysema in a former smoker. These axial and coronal CT images are from a 79 year old female non-hispanic white subject who is a former smoker with 53 pack years smoking history. She has significant dyspnea with MMRC score of 3 indicating shortness of breath with walking short distances, no history of chronic bronchitis or exacerbations and takes no respiratory medications. Six minute walk is reduced at 361 meters, BMI is 30, FEV 1 % Predicted = 100.2, FVC % predicted = 107.2, FEV 1 /FVC = 0.7. There is significant impairment in quality of life with SGRQ Total score of LAA% -950 is 9% suggesting mild emphysema, contrasting with the visual appearance of diffuse emphysema. Panels C and D: Airway disease in a current smoker. These axial and coronal CT images from a 60 year old African-American man and current smoker show definite airway disease on visual scoring. He has a six minute walk distance of 270 meters. Smoking exposure is 12.6 pack years. He denies chronic bronchitis symptoms, respiratory exacerbations or dyspnea. FEV 1 % predicted = 124%. MMRC= 0 SGRQ Total score is He is taking no respiratory medications. Airway Wall Area Percent at the segmental airway level is 63 8 (90 th percentile for GOLD 0 group) and at the sub-segmental airway level is 68.5 (98 th percentile for GOLD 0)

10 efigure 3 Current smoking declines in older age group
11 etable 1. The COPDGene Cohort and Effect of Current Smoking Never- Smoker GOLD 0 GOLD 1 Subjects GOLD 2-4 Current Smoker Former Smoker Current Smoker Former Smoker Current Smoker Former Smoker Number Age 62.1 (9.2) 53.4 (6.3) 61.6 (8.7)* 58 (8) 66.4 (7.9)* 58.7 (7.7) 66.6 (7.6)* Gender (% male) 31.5% 56.4 % 47.7 % * 59.4 % 55.3 % 57 % 54.5 % Race (% NHW) 92.6% 39.6 % 87.2 % * 65 % 93 % * 66 % 85 % * Pack Years (19.7) 35.6 (20.9)* 44.3 (23) 45.9 (26) 51 (26.7) 54.3 (28) Education (% some college or >) 91% 51.7 % 79 % * 60 % 78 % * 51.9 % 62.8 %* BMI 28.2 (5.1) 28.4 (5.8) 29.6 (5.7)* 26.2 (4.8) 28.2 (5.2)* 27.3 (6.2) 28.5 (6.3)* Obesity (BMI > 30) 31.5% 34 % 40 % * 17.8 % 30.2 % * 29 % 36 % * FEV 1 % predicted (13.8) 97.4 (11.7) 97.5 (11.3) 91 (8.8) 90.5 (9.2) 55.4 (16.6) 46.7 (18)* FVC % predicted (12.3) 97.3 (12.2) 95.5 (11.4)* 109 (12.5) 106 (12) 79.2 (16.4) 74.4 (17.6)* FEV 1 /FVC (0.05) 0.79 (0.05) 0.78 (0.05) * 0.65 (0.04) 0.64 (0.05) 0.54 (0.17) 0.47 (0.13)* Oxygen Saturation 97.0 (1.5) 96.8 (1.9) 97.3 (2.1) * 96.2 (2.6) 97.1 (1.8) * 95.5 (3.0) 94.1 (3.8)* Functional Measures Six Minute Walk (meters) (99.8) (106.7) (101.5)* (104.2) 464 (106.7) (117.7) 346 (60.9)* MMRC Dyspnea (% score 2) 3.7% 30 % 13.6 %* 23.5 % 20 % 71 % 60 % * SGRQ Total 3.8 (6.8) 20.9 (19 ) 11.2 (13.9)* 20.2 (19) 15.8 (16) 40.8 (23.1) 41.0 (21.1) SGRQ Impact 1.5 (3.9) 13.4 (17) 6.2 (11)* 13 (17) 9.5 (14) 30.5 (22.8) 26.7 (20.7) SGRQ Symptom 3.7 (7.1) 27 (23) 14.6 (18)* 30.9 (24) 20.6(20.8)* 51.2 (25.4) 42.4 (24.1)* SGRQ Activity 7.8 (14.1) 30.9 (27) 18 (21)* 27.5 (25) 24.3 (23) 53.3 (28) 59.9 (26.5)* Symptoms Chronic Bronchitis (% yes) % 6.2 % * 21.7 % 8.3 % * 39.6 % 20.3 % * Severe Exacerbation (% yes) % 2.8 % * 5.9 % 3.7 % NS 21.6 % 23.4 % Bronchodilator Responsiveness 4.6% 11 % 8.6 % 26.8 % 25 % NS 36.4 % 36.7 % Coronary Artery Disease 1% 5.4 % 10.7 %* 9.7 % 15.7 % 12.7% 19.0 %* Comorbidity Score 0.79 (0.95) 0.8 (1.0) 1.2 (1.1)* 0.87 (1.1) 1.35 (1.2)* 1.3 (1.2) 1.7 (1.3)* Imaging LAA % at -950 HU (Emphysema) 1.88 (2.4) 1.4 (1.9) 2.8 (3.1)* 3.8 (4.5) 7.0 (6.4)* 7.7 (9.6) 16.6 (13.4)* Proportion with Emphysema >5% 8.3% 5.1 % 18.1 % * 25.1 % 49.3 % * 42.3 % 74.4 % * LAA % at -856 HU on Exp. Scan (Gas Trapping) 10.2 (9.1) 9.9 (9.6) 12.5 ( 9.7)* 18.0 (12.5) 23.2 (11.3)* 31.0 (19.4) 44.6 (19.9)* Proportion with Gas Trapping > 20% 10.5% 12.7 % 17 % 36.9 % 59.9 % * 64.3 % 86.3 % * Wall Area % Segmental 58.4 (2.1) 60.5 (2.95) 59.4 (2.6)* 60.6 (2.9) 59.9 (2.6) 63.5 (3.2) 62.5 (2.9)* FRC by CT scan (liters) 2.6 (0.5) 2.8 (0.8) 2.7 (0.7)* 3.3 (0.9) 3.2 (0.8) 3.9 (1.2) 4.1 (1.3) TLC by CT scan (liters) 5.3 (1.2) 5.2 (1.3) 5.47 (1.3)* 6.0 (1.5) 6.1 (1.4) 5.9 (1.4) 6.1 (1.5) Mean (SD), BOLD = p<0.05 compared to current smoker within each Group, * = p<0.001 compared to the Nonsmoker group
12 etable 2. African American Subjects Non Smokers GOLD 0 GOLD 1 Subjects Current Smoker Former Smoker Current Smoker Former Smoker Number Age* 52.9 (5.2) 52.2 (5.2) 56.9 (8.6) 56 (7.2) 62.6 (11.3) Gender (% male) 25% 58.5% 49.1% 56.7% 34.8% Pack Years* (20) 34 (20.7) 41.7(25.5) 36.2(27.2) Education (% some college or >) % 69.6% 43.3% 62.4% BMI* 31.5(5.3) 28.7 (6) 30.8 (6.4) 27 (5.7) 29.5 (7) Obesity (BMI > 30) 50% 36.9% 51.8% 24.2% 26.1% FEV 1 % predicted* 108(13.8) 98.5(12.2) 98(11.9) 90.7 (8.6) 91.7(10.8) FVC % predicted* 99.1(10.2) 98.4(12.8) 97.3(12.7) 109.5(12.5) 113.4(14.8) FEV 1 /FVC* 0.87 (0.04) 0.8 (0.05) 0.8 (0.05) 0.65 (0.04) 0.63 (0.04) O 2 Saturation 98.6 (0.7) 97.5 (2) 97.5 (1.8) 97.5 (1.9) 96.4 (3) Functional Measures Six Minute Walk*(feet) 1386(225) 1372(351) 1379(348) (376) 1245(435) MMRC Dyspnea (% score 2) % 31.4% 33.0% 34.8% SGRQ Total* 8.1 (10.9) 21.7 (20.2) 19.8 (19) 21.5 (19.4) 25.5 (21.9) SGRQ Impact* (18) 12.4 ( (17.8) 18.1 (21.6) SGRQ Symptom* 7.3 (7.4) 25.7 (22.9) 22.2 (22.1) ) 28.7 (21.8) SGRQ Activity* 13.6 (18.4) 33.2 (28.6) 31.5 (27.5) 32(27.4) 36.8 (27.7) Symptoms Chronic Bronchitis (% yes) 0 13% 10.2% 13.4% 21.7% Severe Exacerbation (% yes) 0 6.0% 7.1% 5.1% 13% Bronchodilator Responsiveness % 12.7% 33.1% 31.8% * Mean (SD), Significantly different from non-smoker (p<0.05), Significantly different from current smoker (p<0.05) Significantly different from smoker control (p<0.05)
13 etable 3. Non-Hispanic White Subjects Non Smokers GOLD 0 GOLD 1 Subjects Current Smoker Former Smoker Current Smoker Former Smoker Number Age* 62.8 (9.1) 55.1 (7.2) 62.2 (8.5) 59.2 (8.3) 66.7 (7.6) Gender (% male) 32% 53.2% 47.4% 60.8% 56.7% Pack Years* (18.9) 34(20.7) 41.7(25.5) 36.2(27.2) Education (% some college or >) % 81.9% 69.2% 78.3% BMI* 28 (5.0) 28.7 (6) 29.4 (5.6) 27 (5.7) 28.1 (5.1) Obesity (BMI > 30) 30% 30.5% 30.5% 14.3% 38.8% FEV 1 % predicted* 102.9(13.8) 95.7(10.6) 97.5(11.2) 91.2(8.9) 90.4(9.1) FVC % predicted* 99.0(12.5) 95.7(11) 95.3(11.2) 108.3(12.5) 105.7(11.9) FEV 1 /FVC* 0.79 (0.05) 0.78(0.05) 0.78 (0.05) 0.65(0.04) 0.64 (0.05) O 2 Saturation 96.9 (1.5) 97.0(2.1) 96.7 (1.85) 96.9(1.7) 96.2 (2.6) Functional Measures Six Minute Walk*(feet) 1698(324) 1521(328) 1611(320) (308) 1543(336) MMRC Dyspnea (% score 2) 4% 22.7% 11.0% 18.2% 19.2% SGRQ Total* 3.4 (6.3) 12.3(15.7) 9.9 (12.5) 12.6(16.6) 15.1 (15.5) SGRQ Impact* 1.2 (3.3) 19.6(17.9) 5.3 (9.8) 19.5(18.5) 8.9 (12.9) SGRQ Symptom* 3.4 (7.0) 29.5(22.5) 13.5 (17.1) 32.9(24.4) 20.1 (20.6) SGRQ Activity* 7.3 (13.7) 27.3(24.7) 16.3 (19.6) 25.0(23.7) 23.4 (22.7) Symptoms Chronic Bronchitis (% yes) % 5.6% 26.2% 21.8% Severe Exacerbation (% yes) 0 4.4% 2.2% 6.3% 3.1% Bronchodilator Responsiveness 5% 9.6% 8.0% 23.3% 24.7% * Mean (SD), Significantly different from non-smoker (p<0.05) Significantly different from current smoker (p<0.05) Significantly different from smoker control (p<0.05)
14 etable 4. Impairments in in COPDGene non-asthmatic subjects Non-Smoker GOLD 0 GOLD 1 Individual Scores Chronic Bronchitis (by criteria) (12%) 104 (15%) History of Severe Exacerbation (3%) 27 (4%) SGRQ: Total >25 4 (4%) 887 (23%) 181 (26%) Six Min Walk < 1150 feet (350 m) 4 (4%) 577 (15%) 87(13%) MMRC Dyspnea Score 2 4 (4%) 802 (21%) 139 (20%) Emphysema > 5% 8 (8%) 394 (11%) 234 (35%) Gas Trapping >20% 10 (10%) 483 (15%) 276 (47%) N= 107 N= 3888 N= 687 Sums Any Impairment 25 (23%) 2052 (53%) 499 (73%) 6 Impairments Impairments Impairments Impairments Impairments Impairment No Impairment 82 (77%) 1836 (47%) 188 (27%) Number of Subjects (Percent)
15 etable NHANES Cohort Demographics Never Smokers GOLD 0 GOLD 1 GOLD 2-4 # Number Age 60.1 (10.0) 58.0 (9.2) 63.9 (9.4) 63.3 (9.7) Gender (% male) 41.1% 55.4% 73.4% 60.9% Race (% NHW) 70.6% 67.8% 76.7% 78.6% Pack Years (26.6) 37.7 (23.6) 50.3 (32.5) Current Smoking % N/A 48.8% 45.5% 60.5% Education (% some college or >) 60.0% 48.0% 42.9% 31.3% BMI 30.2 (6.6) 29.7 (6.6) 26.7 (5.0) 27.7 (6.5) FEV 1 % predicted (13.1) 99.0 (12.2) 93.0 (9.6) 63.6 (12.6) FVC % predicted (13.0) 98.8 (12.2) (11.8) 83.6 (13.2) FEV 1 /FVC 0.79 (0.05) 0.77 (0.05) 0.65 (0.04) 0.57(0.09) Chronic Bronchitis 2.3% 7.0% 6.4% 18.4% Obesity 44.6% 41.2% 22% 30.5% Any cancer 13.1% 14.4% 20.8% 22.0% CAD 5.7% 9.9% 12.1% 21.2% CHF 1.7% 4.2% 3.8% 6.6% Values are Mean (SD) except where percent is noted # GOLD 2= 247 subjects, GOLD 3= 47 subjects, GOLD 4 = 1 subject p<0.001 p<0.001 across groups
16 etable 6. Predictors of Quality of Life by St George s Respiratory Score in COPDGene GOLD 0 Subjects* Term Scaled Parameter Estimate P value R 2 = 0.65 Age <0.001 BMI 1.60 p=0.023 Current Smoker 1.37 <0.001 Pack years smoking 3.8 < Severe Exacerbations 2.99 <0.001 Has Chronic Bronchitis 4.64 <0.001 FEV 1 Percent Predicted p=0.087 Has history of "chest trouble flare-up" 3.03 <0.001 Has one or more diagnoses related to CAD Has history of Gastro-esophageal reflux disorder 1.27 <0.001 Six Minute Walk Distance (feet) <0.001 MMRC Dyspnea Score 17.9 <0.001 *Multiple Regression Model for SRGQ Total Score Race, Bronchodilator Responsiveness and Gender were tested and found non-significant in the model. Positive numbers indicate higher (worse) SGRQ Total Score for categorical variables. For continuous variables (age, six minute walk distance, pack years) a larger parameter estimate relates to the magnitude and direction (+/-) of the impact on SGRQ Total score.
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene
 Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
SGRQ Questionnaire assessing respiratory disease-specific quality of life. Questionnaire assessing general quality of life
 SUPPLEMENTARY MATERIAL e-table 1: Outcomes studied in present analysis. Outcome Abbreviation Definition Nature of data, direction indicating adverse effect (continuous only) Clinical outcomes- subjective
SUPPLEMENTARY MATERIAL e-table 1: Outcomes studied in present analysis. Outcome Abbreviation Definition Nature of data, direction indicating adverse effect (continuous only) Clinical outcomes- subjective
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Online Data Supplement. Prevalence of Chronic Obstructive Pulmonary Disease in Korea: Results of a Population-based Spirometry Survey
 Online Data Supplement Prevalence of Chronic Obstructive Pulmonary Disease in Korea: Results of a Population-based Spirometry Survey Dong Soon Kim, MD, Young Sam Kim MD, Kee Suk Chung MD, Jung Hyun Chang
Online Data Supplement Prevalence of Chronic Obstructive Pulmonary Disease in Korea: Results of a Population-based Spirometry Survey Dong Soon Kim, MD, Young Sam Kim MD, Kee Suk Chung MD, Jung Hyun Chang
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
This is a cross-sectional analysis of the National Health and Nutrition Examination
 SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
Supplementary Online Content
 Supplementary Online Content Deslée G, Mal H, Dutau H, et al; REVOLENS Study Group. Lung volume reduction coil treatment vs usual care in patients with severe emphysema: the REVOLENS randomized clinical
Supplementary Online Content Deslée G, Mal H, Dutau H, et al; REVOLENS Study Group. Lung volume reduction coil treatment vs usual care in patients with severe emphysema: the REVOLENS randomized clinical
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Woodruff PG, Barr RG, Bleecker E, et al. Clinical significance
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Woodruff PG, Barr RG, Bleecker E, et al. Clinical significance
Visual Assessment of CT Findings in Smokers With Nonobstructed Spirometric Abnormalities in The COPDGene Study
 88 Chronic Obstructive Pulmonary Diseases: Journal of the COPD Foundation Original Research. Visual Assessment of CT Findings in Smokers With Nonobstructed Spirometric Abnormalities in The COPDGene Study
88 Chronic Obstructive Pulmonary Diseases: Journal of the COPD Foundation Original Research. Visual Assessment of CT Findings in Smokers With Nonobstructed Spirometric Abnormalities in The COPDGene Study
9/22/2015 CONFLICT OF INTEREST OBJECTIVES. Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR
 Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org scerreta@copdfoundation.org CONFLICT OF INTEREST
Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org scerreta@copdfoundation.org CONFLICT OF INTEREST
Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR
 Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org scerreta@copdfoundation.org CONFLICT OF INTEREST
Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org scerreta@copdfoundation.org CONFLICT OF INTEREST
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
COMPARISON OF FEV1 REGARDLESS OF RATIO (FRR) WITH FORCED EXPIRATORY RATIO (FER) IN COPD; TO INCORPORATE PRESERVED RATIO IMPAIRED SPIROMETRY (PRISM)
 WITH FORCED EXPIRATORY RATIO (FER) IN COPD; TO INCORPORATE PRESERVED RATIO IMPAIRED SPIROMETRY (PRISM)") wjpmr, 2017,3(9), 03-07 SJIF Impact Factor: 4.103 WORLD JOURNAL OF PHARMACEUTICAL AND MEDICAL RESEARCH Research Article ISSN 2455-3301 WJPMR COMPARISON OF FEV1 REGARDLESS OF RATIO (FRR) WITH FORCED EXPIRATORY
wjpmr, 2017,3(9), 03-07 SJIF Impact Factor: 4.103 WORLD JOURNAL OF PHARMACEUTICAL AND MEDICAL RESEARCH Research Article ISSN 2455-3301 WJPMR COMPARISON OF FEV1 REGARDLESS OF RATIO (FRR) WITH FORCED EXPIRATORY
COPD in Korea. Division of Pulmonary, Allergy and Critical Care Medicine of Hallym University Medical Center Park Yong Bum
 COPD in Korea Division of Pulmonary, Allergy and Critical Care Medicine of Hallym University Medical Center Park Yong Bum Mortality Rate 1970-2002, USA JAMA,2005 Global Burden of Disease: COPD WHO & World
COPD in Korea Division of Pulmonary, Allergy and Critical Care Medicine of Hallym University Medical Center Park Yong Bum Mortality Rate 1970-2002, USA JAMA,2005 Global Burden of Disease: COPD WHO & World
Outline FEF Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications?
 Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
COPD-Related Musculoskeletal Disease. Jessica Bon Field, MD, MS 2017 Update in Internal Medicine October 20, 2017
 COPD-Related Musculoskeletal Disease Jessica Bon Field, MD, MS 2017 Update in Internal Medicine October 20, 2017 A 60-year old man with COPD comes into your office for a routine office visit. He is a former
COPD-Related Musculoskeletal Disease Jessica Bon Field, MD, MS 2017 Update in Internal Medicine October 20, 2017 A 60-year old man with COPD comes into your office for a routine office visit. He is a former
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Predictive Models of Emphysema Progression in HIV
 Predictive Models of Emphysema Progression in HIV Janice Leung, MD FRCPC A. Malagoli, A. Santoro, G. Besutti, G. Ligabue, D. Dai, J. Mayo, S. Lam, D. Sin, S. Man, G. Guaraldi COPD: An Emerging Comorbidity
Predictive Models of Emphysema Progression in HIV Janice Leung, MD FRCPC A. Malagoli, A. Santoro, G. Besutti, G. Ligabue, D. Dai, J. Mayo, S. Lam, D. Sin, S. Man, G. Guaraldi COPD: An Emerging Comorbidity
The Aging Lung. Sidney S. Braman MD FACP FCCP Professor of Medicine Brown University Providence RI
 The Aging Lung Sidney S. Braman MD FACP FCCP Professor of Medicine Brown University Providence RI Is the respiratory system of the elderly different when compared to younger age groups? Respiratory Changes
The Aging Lung Sidney S. Braman MD FACP FCCP Professor of Medicine Brown University Providence RI Is the respiratory system of the elderly different when compared to younger age groups? Respiratory Changes
Study No.: Title: Rationale: Phase: Study Period Study Design: Centres: Indication: Treatment: Objectives : Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
TORCH: Salmeterol and Fluticasone Propionate and Survival in COPD
 TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Hunninghake GM, Hatabu H, Okajima Y, et al. MUC5B promoter
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Hunninghake GM, Hatabu H, Okajima Y, et al. MUC5B promoter
Douglas W. Mapel MD, MPH, Melissa Roberts PhD
 Original Article Spirometry, the St. George s Respiratory Questionnaire, and other clinical measures as predictors of medical costs and COPD exacerbation events in a prospective cohort Douglas W. Mapel
Original Article Spirometry, the St. George s Respiratory Questionnaire, and other clinical measures as predictors of medical costs and COPD exacerbation events in a prospective cohort Douglas W. Mapel
PFT Interpretation and Reference Values
 PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university
 What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
Does the multidimensional grading system (BODE) correspond to differences in health status of patients with COPD?
 correspond to differences in health status of patients with COPD?") AUTHOR COPY ORIGINAL RESEARCH Does the multidimensional grading system (BODE) correspond to differences in health status of patients with COPD? Kian-Chung Ong 1 Suat-Jin Lu 1 Cindy Seok-Chin Soh 2 1 Department
AUTHOR COPY ORIGINAL RESEARCH Does the multidimensional grading system (BODE) correspond to differences in health status of patients with COPD? Kian-Chung Ong 1 Suat-Jin Lu 1 Cindy Seok-Chin Soh 2 1 Department
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology
 Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable
 THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
Decramer 2014 a &b [21]
![Decramer 2014 a &b [21]](/thumbs/90/101390504.jpg "Decramer 2014 a &b [21]") Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
COPD: early detection, screening and case-finding: what is the evidence? Prof. Jan-Willem Lammers, Md PhD Department of Respiratory Diseases
 COPD: early detection, screening and case-finding: what is the evidence? Prof. Jan-Willem Lammers, Md PhD Department of Respiratory Diseases «If you test one smoker with cough every day You will diagnose
COPD: early detection, screening and case-finding: what is the evidence? Prof. Jan-Willem Lammers, Md PhD Department of Respiratory Diseases «If you test one smoker with cough every day You will diagnose
UNDERSTANDING COPD MEDIA BACKGROUNDER
 UNDERSTANDING COPD MEDIA BACKGROUNDER What is COPD? Chronic Obstructive Pulmonary Disease (COPD) also called emphysema and/or chronic obstructive bronchitis* is a preventable lung disease caused by the
UNDERSTANDING COPD MEDIA BACKGROUNDER What is COPD? Chronic Obstructive Pulmonary Disease (COPD) also called emphysema and/or chronic obstructive bronchitis* is a preventable lung disease caused by the
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
abstract n engl j med 374;19 nejm.org May 12,
 The new england journal of medicine established in 1812 May 12, 2016 vol. 374 no. 19 Clinical Significance of Symptoms in Smokers with Preserved Pulmonary Function Prescott G. Woodruff, M.D., R. Graham
The new england journal of medicine established in 1812 May 12, 2016 vol. 374 no. 19 Clinical Significance of Symptoms in Smokers with Preserved Pulmonary Function Prescott G. Woodruff, M.D., R. Graham
APSR RESPIRATORY UPDATES
 APSR RESPIRATORY UPDATES Volume 4, Issue 7 Newsletter Date: July 2012 APSR EDUCATION PUBLICATION Inside this issue: Quantitative imaging of airways Small-Airway Obstruction and Emphysema in Chronic Obstructive
APSR RESPIRATORY UPDATES Volume 4, Issue 7 Newsletter Date: July 2012 APSR EDUCATION PUBLICATION Inside this issue: Quantitative imaging of airways Small-Airway Obstruction and Emphysema in Chronic Obstructive
Implications of the pulmonary artery to ascending aortic ratio in patients with relatively mild chronic obstructive pulmonary disease
 Original Article Implications of the pulmonary artery to ascending aortic ratio in patients with relatively mild chronic obstructive pulmonary disease Cho Rom Hahm 1, Myoung Nam Lim 2, Hee Yeong Kim 3,
Original Article Implications of the pulmonary artery to ascending aortic ratio in patients with relatively mild chronic obstructive pulmonary disease Cho Rom Hahm 1, Myoung Nam Lim 2, Hee Yeong Kim 3,
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Understanding the Basics of Spirometry It s not just about yelling blow
 Understanding the Basics of Spirometry It s not just about yelling blow Carl D. Mottram, RRT RPFT FAARC Technical Director - Pulmonary Function Labs and Rehabilitation Associate Professor of Medicine -
Understanding the Basics of Spirometry It s not just about yelling blow Carl D. Mottram, RRT RPFT FAARC Technical Director - Pulmonary Function Labs and Rehabilitation Associate Professor of Medicine -
Yuriy Feschenko, Liudmyla Iashyna, Ksenia Nazarenko and Svitlana Opimakh
 2018; 7(1): 74-78 ISSN (E): 2277-7695 ISSN (P): 2349-8242 NAAS Rating: 5.03 TPI 2018; 7(1): 74-78 2018 TPI www.thepharmajournal.com Received: 11-11-2017 Accepted: 12-12-2017 Yuriy Feschenko Liudmyla Iashyna
2018; 7(1): 74-78 ISSN (E): 2277-7695 ISSN (P): 2349-8242 NAAS Rating: 5.03 TPI 2018; 7(1): 74-78 2018 TPI www.thepharmajournal.com Received: 11-11-2017 Accepted: 12-12-2017 Yuriy Feschenko Liudmyla Iashyna
Occupational exposures are associated with worse morbidity in patients with COPD
 Occupational exposures are associated with worse morbidity in patients with COPD Laura M Paulin 1, Gregory B Diette 1,2, Paul D Blanc 3, Nirupama Putcha 1, Mark D Eisner 4, Richard E Kanner 5, Andrew J
Occupational exposures are associated with worse morbidity in patients with COPD Laura M Paulin 1, Gregory B Diette 1,2, Paul D Blanc 3, Nirupama Putcha 1, Mark D Eisner 4, Richard E Kanner 5, Andrew J
MEDICAL STUDENT INVOLVEMENT IN ASSESSING RESPIRATORY SYMPTOMS TO IMPROVE EARLY DETECTION OF LUNG DISEASE IN HIV PATIENTS.
 MEDICAL STUDENT INVOLVEMENT IN ASSESSING RESPIRATORY SYMPTOMS TO IMPROVE EARLY DETECTION OF LUNG DISEASE IN HIV PATIENTS Simone Neri Definition of COPD COPD, a common preventable and treatable disease,
MEDICAL STUDENT INVOLVEMENT IN ASSESSING RESPIRATORY SYMPTOMS TO IMPROVE EARLY DETECTION OF LUNG DISEASE IN HIV PATIENTS Simone Neri Definition of COPD COPD, a common preventable and treatable disease,
Interpreting pulmonary function tests: Recognize the pattern, and the diagnosis will follow
 REVIEW FEYROUZ AL-ASHKAR, MD Department of General Internal Medicine, The Cleveland Clinic REENA MEHRA, MD Department of Pulmonary and Critical Care Medicine, University Hospitals, Cleveland PETER J. MAZZONE,
REVIEW FEYROUZ AL-ASHKAR, MD Department of General Internal Medicine, The Cleveland Clinic REENA MEHRA, MD Department of Pulmonary and Critical Care Medicine, University Hospitals, Cleveland PETER J. MAZZONE,
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD: Genomic Biomarker Status and Challenge Scoring
 COPD: Genomic Biomarker Status and Challenge Scoring Julia Hoeng, PMI R&D Raquel Norel, IBM Research 3 rd October 2012 COPD: Genomic Biomarker Status Julia Hoeng, Ph.D. Philip Morris International, Research
COPD: Genomic Biomarker Status and Challenge Scoring Julia Hoeng, PMI R&D Raquel Norel, IBM Research 3 rd October 2012 COPD: Genomic Biomarker Status Julia Hoeng, Ph.D. Philip Morris International, Research
Association of low income with pulmonary disease progression in smokers with and without chronic obstructive pulmonary disease
 ORIGINAL ARTICLE COPD Association of low income with pulmonary disease progression in smokers with and without chronic obstructive pulmonary disease Katherine E. Lowe 1,BarryJ.Make 1, James D. Crapo 1,
ORIGINAL ARTICLE COPD Association of low income with pulmonary disease progression in smokers with and without chronic obstructive pulmonary disease Katherine E. Lowe 1,BarryJ.Make 1, James D. Crapo 1,
Combined pulmonary fibrosis and emphysema; prevalence and follow up among health-care personnel
 Combined pulmonary fibrosis and emphysema; prevalence and follow up among health-care personnel Poster No.: C-0698 Congress: ECR 2013 Type: Scientific Exhibit Authors: K. Chae, G. Jin, S. Chon, Y. Lee;
Combined pulmonary fibrosis and emphysema; prevalence and follow up among health-care personnel Poster No.: C-0698 Congress: ECR 2013 Type: Scientific Exhibit Authors: K. Chae, G. Jin, S. Chon, Y. Lee;
6- Lung Volumes and Pulmonary Function Tests
 6- Lung Volumes and Pulmonary Function Tests s (PFTs) are noninvasive diagnostic tests that provide measurable feedback about the function of the lungs. By assessing lung volumes, capacities, rates of
6- Lung Volumes and Pulmonary Function Tests s (PFTs) are noninvasive diagnostic tests that provide measurable feedback about the function of the lungs. By assessing lung volumes, capacities, rates of
C.S. HAWORTH 1, A. WANNER 2, J. FROEHLICH 3, T. O'NEAL 3, A. DAVIS 4, I. GONDA 3, A. O'DONNELL 5
 Inhaled Liposomal Ciprofloxacin in Patients With Non-Cystic Fibrosis Bronchiectasis and Chronic Pseudomonas aeruginosa: Results From Two Parallel Phase III Trials (ORBIT-3 and -4) C.S. HAWORTH 1, A. WANNER
Inhaled Liposomal Ciprofloxacin in Patients With Non-Cystic Fibrosis Bronchiectasis and Chronic Pseudomonas aeruginosa: Results From Two Parallel Phase III Trials (ORBIT-3 and -4) C.S. HAWORTH 1, A. WANNER
Office Based Spirometry
 Osteopathic Family Physician (2014)1, 14-18 Scott Klosterman, DO; Woodson Crenshaw, OMS4 Spartanburg Regional Family Medicine Residency Program; Edward Via College of Osteopathic Medicine - Virginia Campus
Osteopathic Family Physician (2014)1, 14-18 Scott Klosterman, DO; Woodson Crenshaw, OMS4 Spartanburg Regional Family Medicine Residency Program; Edward Via College of Osteopathic Medicine - Virginia Campus
Pulmonary Function Testing
 In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น
 รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE
 The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
SPIROMETRY TECHNIQUE. Jim Reid New Zealand
 Jim Reid New Zealand The Basics Jim Reid Spirometry measures airflow and lung volumes, and is the preferred lung function test in COPD. By measuring reversibility of obstruction, it is also diagnostic
Jim Reid New Zealand The Basics Jim Reid Spirometry measures airflow and lung volumes, and is the preferred lung function test in COPD. By measuring reversibility of obstruction, it is also diagnostic
Bode index as a predictor of severity in patients with chronic obstructive pulmonary disease.
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 5 Ver. VII (May. 2016), PP 93-100 www.iosrjournals.org Bode index as a predictor of severity
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 5 Ver. VII (May. 2016), PP 93-100 www.iosrjournals.org Bode index as a predictor of severity
SPIROMETRY. Marijke Currie (CRFS) Care Medical Ltd Phone: Copyright CARE Medical ltd
 Care Medical Ltd Phone: Copyright CARE Medical ltd") SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual can
SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual can
Michael S. Blaiss, MD
 Michael S. Blaiss, MD Clinical Professor of Pediatrics and Medicine Division of Clinical Immunology and Allergy University of Tennessee Health Science Center Memphis, Tennessee Speaker s Bureau: AstraZeneca,
Michael S. Blaiss, MD Clinical Professor of Pediatrics and Medicine Division of Clinical Immunology and Allergy University of Tennessee Health Science Center Memphis, Tennessee Speaker s Bureau: AstraZeneca,
Comparisons of health status scores with MRC grades in COPD: implications for the GOLD 2011 classification
 ORIGINAL ARTICLE COPD Comparisons of health status scores with MRC grades in COPD: implications for the GOLD 2011 classification Paul W. Jones 1, Lukasz Adamek 2, Gilbert Nadeau 2 and Norbert Banik 3 Affiliations:
ORIGINAL ARTICLE COPD Comparisons of health status scores with MRC grades in COPD: implications for the GOLD 2011 classification Paul W. Jones 1, Lukasz Adamek 2, Gilbert Nadeau 2 and Norbert Banik 3 Affiliations:
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data. The synopsis
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data. The synopsis
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD)
 Instructions for the Pulmonary Diagnosis Form (PLD)") Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
UMEC/VI vs. UMEC in subjects who responded to UMEC UMEC/VI vs. VI in subjects who responded to VI
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects
 Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC Benefits and Limitations of Pulmonary Function Testing Benefits
Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC Benefits and Limitations of Pulmonary Function Testing Benefits
Pulmonary Function Testing The Basics of Interpretation
 Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Lung function in HIV infected adolescents on antiretroviral therapy in Cape Town, South Africa
 Lung function in HIV infected adolescents on antiretroviral therapy in Cape Town, South Africa Leah Githinji, Di Gray, Landon Myer, Heather Zar MRC unit on Adolescent and Child Health Red Cross War Memorial
Lung function in HIV infected adolescents on antiretroviral therapy in Cape Town, South Africa Leah Githinji, Di Gray, Landon Myer, Heather Zar MRC unit on Adolescent and Child Health Red Cross War Memorial
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Center for Respiratory and Sleep Medicine COPD Chronic Disease Management Program
 Center for Respiratory and Sleep Medicine COPD Chronic Disease Management Program Cristina Ashworth, NP Khalil Diab,MD Center for Respiratory and Sleep Medicine Subgroup of Indiana Internal Medicine Consultants
Center for Respiratory and Sleep Medicine COPD Chronic Disease Management Program Cristina Ashworth, NP Khalil Diab,MD Center for Respiratory and Sleep Medicine Subgroup of Indiana Internal Medicine Consultants
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable: Secondary Outcome/Efficacy Variable(s): Statistical Methods:
: Statistical Methods:") The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Triennial Pulmonary Workshop 2012
 Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Productivity losses in chronic obstructive pulmonary disease a population-based survey.
 Online supplement to Productivity losses in chronic obstructive pulmonary disease a population-based survey. Running head: Productivity losses in COPD. Authors: Marta Erdal, Department of Thoracic Medicine,
Online supplement to Productivity losses in chronic obstructive pulmonary disease a population-based survey. Running head: Productivity losses in COPD. Authors: Marta Erdal, Department of Thoracic Medicine,
Spirometry Workshop for Primary Care Nurse Practitioners
 Spirometry Workshop for Primary Care Nurse Practitioners Catherine Casey S. Jones PhD, RN, AE-C, ANP-C Certified Adult Nurse Practitioner Texas Pulmonary & Critical Care Consultants P.A. and Adjunct Professor
Spirometry Workshop for Primary Care Nurse Practitioners Catherine Casey S. Jones PhD, RN, AE-C, ANP-C Certified Adult Nurse Practitioner Texas Pulmonary & Critical Care Consultants P.A. and Adjunct Professor
Gender Differences in the Severity of CT Emphysema in COPD*
 Original Research COPD Gender Differences in the Severity of CT Emphysema in COPD* Mark T. Dransfield, MD; George R. Washko, MD; Marilyn G. Foreman, MD, FCCP; Raul San Jose Estepar, PhD; John Reilly, MD,
Original Research COPD Gender Differences in the Severity of CT Emphysema in COPD* Mark T. Dransfield, MD; George R. Washko, MD; Marilyn G. Foreman, MD, FCCP; Raul San Jose Estepar, PhD; John Reilly, MD,
Coexistence of confirmed obstruction in spirometry and restriction in body plethysmography, e.g.: COPD + pulmonary fibrosis
 Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
ERS 2016 Congress Highlights Interstitial Lung Disease (ILD)
") ERS 216 Congress Highlights Interstitial Lung Disease (ILD) London, UK September 3 rd 7 th 216 The 26 th European Respiratory Society International Congress, (ERS) the largest respiratory meeting in the
ERS 216 Congress Highlights Interstitial Lung Disease (ILD) London, UK September 3 rd 7 th 216 The 26 th European Respiratory Society International Congress, (ERS) the largest respiratory meeting in the
Basic approach to PFT interpretation. Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic
 Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
GOLD UPDATE on COPD and the Importance of Accurate Dyspnea Evaluation
 GOLD UPDATE on COPD and the Importance of Accurate Dyspnea Evaluation George Anderson, PhD Sr. Medical Science Liaison MA-AZAP ML-4006-US-0212 Approved 11/16 Glob al Strategy for the Diagnosis, Management,
GOLD UPDATE on COPD and the Importance of Accurate Dyspnea Evaluation George Anderson, PhD Sr. Medical Science Liaison MA-AZAP ML-4006-US-0212 Approved 11/16 Glob al Strategy for the Diagnosis, Management,
Blood Eosinophils and Response to Maintenance COPD Treatment: Data from the FLAME Trial. Online Data Supplement
 Blood Eosinophils and Response to Maintenance COPD Treatment: Data from the FLAME Trial Nicolas Roche, Kenneth R. Chapman, Claus F. Vogelmeier, Felix JF Herth, Chau Thach, Robert Fogel, Petter Olsson,
Blood Eosinophils and Response to Maintenance COPD Treatment: Data from the FLAME Trial Nicolas Roche, Kenneth R. Chapman, Claus F. Vogelmeier, Felix JF Herth, Chau Thach, Robert Fogel, Petter Olsson,
Three s Company - The role of triple therapy in chronic obstructive pulmonary
 Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) October 26 th, 2018 Zahava Picado, PharmD PGY1 Pharmacy Resident Central Texas Veterans Healthcare System Zahava.Picado@va.gov
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) October 26 th, 2018 Zahava Picado, PharmD PGY1 Pharmacy Resident Central Texas Veterans Healthcare System Zahava.Picado@va.gov
ONLINE DATA SUPPLEMENT - ASTHMA INTERVENTION PROGRAM PREVENTS READMISSIONS IN HIGH HEALTHCARE UTILIZERS
 R2 (REVISED MANUSCRIPT BLUE 200208-877OC) ONLINE DATA SUPPLEMENT - ASTHMA INTERVENTION PROGRAM PREVENTS READMISSIONS IN HIGH HEALTHCARE UTILIZERS Mario Castro, M.D., M.P.H. Nina A. Zimmermann R.N. Sue
R2 (REVISED MANUSCRIPT BLUE 200208-877OC) ONLINE DATA SUPPLEMENT - ASTHMA INTERVENTION PROGRAM PREVENTS READMISSIONS IN HIGH HEALTHCARE UTILIZERS Mario Castro, M.D., M.P.H. Nina A. Zimmermann R.N. Sue
Content Indica c tion Lung v olumes e & Lung Indica c tions i n c paci c ties
 Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
Research in Real Life
 Research in Real Life Study 1: Exploratory study - identifying the benefits of pmdi versus Diskus for delivering fluticasone/salmeterol combination therapy in patients with chronic obstructive pulmonary
Research in Real Life Study 1: Exploratory study - identifying the benefits of pmdi versus Diskus for delivering fluticasone/salmeterol combination therapy in patients with chronic obstructive pulmonary
Genomewide Linkage of Forced Mid-Expiratory Flow in Chronic Obstructive Pulmonary Disease
 ONLINE DATA SUPPLEMENT Genomewide Linkage of Forced Mid-Expiratory Flow in Chronic Obstructive Pulmonary Disease Dawn L. DeMeo, M.D., M.P.H.,Juan C. Celedón, M.D., Dr.P.H., Christoph Lange, John J. Reilly,
ONLINE DATA SUPPLEMENT Genomewide Linkage of Forced Mid-Expiratory Flow in Chronic Obstructive Pulmonary Disease Dawn L. DeMeo, M.D., M.P.H.,Juan C. Celedón, M.D., Dr.P.H., Christoph Lange, John J. Reilly,
Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities
 Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities Jann Mortensen Final Phil meeting, 29 april 2004 Obstructive disease Definition Epidemiologi Mechanisms Natural history
Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities Jann Mortensen Final Phil meeting, 29 april 2004 Obstructive disease Definition Epidemiologi Mechanisms Natural history
AECOPD: Management and Prevention
 Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Yesterday we spoke of the increased airway resistance and its two examples: 1) emphysema, where we have destruction of the alveolar wall and thus reducing the area available for
بسم هللا الرحمن الرحيم Yesterday we spoke of the increased airway resistance and its two examples: 1) emphysema, where we have destruction of the alveolar wall and thus reducing the area available for
PULMONARY FUNCTION. VOLUMES AND CAPACITIES
 PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C
 MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
How to distinguish between uncontrolled and severe asthma
 How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct