Major Depression and Anxiety in Adolescents and Adults
|
|
|
- Barry Fox
- 5 years ago
- Views:
Transcription
1 Major Depression and Anxiety in Adolescents and Adults Miggie Greenberg, M.D. Associate Professor of Psychiatry St. Louis University School of Medicine *NO DISCLOSURES*
2 OBJECTIVES * Recognize Major Depressive D/O and Anxiety and to differentiate it from misery. * Understand basic pharmacological strategies for treating Depression and Anxiety * Understand secondary strategies for treating Depression and Anxiety * Recognize when to refer to a mental health professional
3
4 STEP 1 Clarify Diagnosis. Be sure you are dealing with a clinical depression rather than human misery.
5 STEP 2 If considering medication, think about: - Therapeutic Alliance - Side effects - Comorbid conditions - Family history of response to antidepressants - Cost In terms of efficacy: SSRI s= SNRI s= = bupropion= TCA s= MAOI s
6 STEP 3 Start SSRI or SNRI or SARI or bupropion or mirtazapine. SSRI s are usually the first choice SSRI s are usually the first choice It takes 4-8 weeks to see full effect of medication If there is NO improvement after a month, switch medication If there is partial improvement, increase the dose of the medication
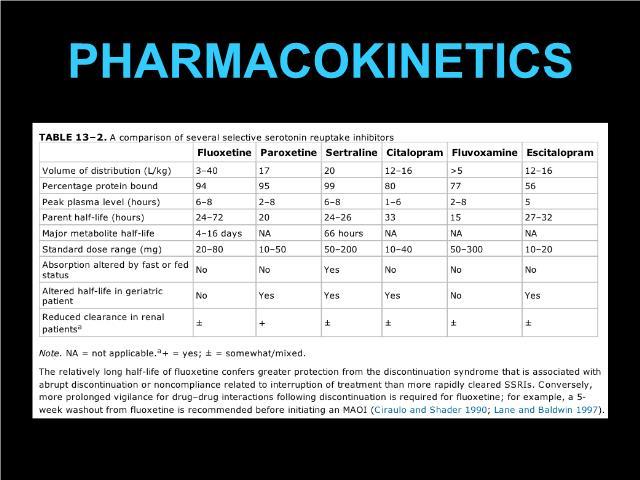
7 SSRI s Prozac / fluoxetine has the longest half life so if your pt is going to be unreliable about taking medication, it is a good choice. There is not much evidence that it is activating but that is still what is said. Paxil/ paroxetine has the shortest half life so pts will feel discontinuation symptoms quickly. It has more drug interactions than other SSRI s and after six months is more likely to contribute to weight gain.
8 SSRI s elexa/ citalopram: Few drug interactions and well tolerated by geriatric patients. May need to increase dose but not over 40 mg when there is a possibility of QTc prolongation. Has some antihistaminic effects. exapro-escitalopram: Similar to citalopram but does not have R enantiomer which causes antihistaminic effects so is the best tolerated SSRI
9 SSRI s oloft/ sertraline: Also has very few drug interactions and is easy to titrate slowly from a starting dose of 25 mg a day for very sensitive people. (Normal starting dose is 50 mg). Can titrate to 200 mg a day. It takes about 2 weeks to see effect of an increased dose. A poor response to one SSRI does not correlate to a poor response with a second SSRI so it is reasonable to switch SSRI s before switching families of medication
10
11
12 STEP 4 If the patient has a poor response to 2 SSRI s: Switch families of medication Or Augment with another medication
13
14 SNRI s Effexor / venlafaxine: Works as an SSRI until the dose is increased to 150 mg a day and then it is both a serotonin and norepinephrine reuptake inhibitor. Can raise blood pressure if HTN is already present. Needs to be discontinued at a VERY slow rate. Cymbalta/ duloxetine: May have less effect on blood pressure and be easier to discontinue. Helps with neuropathic pain but not all pain
15 NEWER ANTIDEPRESSANTS * Viibryd/ vilazadone (SPARI= serotonin partial agonist reuptake inhibitor) - Start at 10 mg for 7 days, can then increase to 20 mg. Max dose is 40 mg a day with or without food. - Main side effects can be nausea and vomiting and insomnia - If patients are taking a CYP3A4 inducer, vilazadone will be cleared more quickly and a higher dose will be required.
16 NEWER ANTIDEPRESSANTS * Trintellex/ vortioxetine: (also a SPARI) - Normal starting dose is 10 mg a day but can start at 5mg for patients who are very medication sensitive. - Aim for 20 mg a day as tolerated - Main side effects are nausea and vomiting and constipation - If taking CYP2D6 inhibitors such as bupropion or paroxetine, a lower dose of vortioxetine will be needed - If taking a CYP2D6 inducer like carbamazepine or phenytoin, a higher dose will be needed
17 NEWER ANTIDEPRESSANTS * Fetzima/ levomilnacipran : (an SNRI) - Start with 20 mg a day, with or without food for 2 days and then increase to 40 mg a day. - Main side effects are nausea and vomiting, constipation, diaphoresis, increased hear rate/ palpitations and erectile dysfunction. - Need a lower than average dose for patients also taking CYP3A4 inhibitors like anti-fungals
18

19
20
21 AUGEMENTATION STRATEGIES FOR ANTIDEPRESSANTS * Combine a non-ssri antidepressant with an SSRI * Add a low dose of a second generation antipsychotic suc as aripiprazole (Abilify) or risperidone (Risperdal) * Add lithium at 300 mg a day. After a few days increase to 300 mg bid. Should reach steady state in about 5 days. Level should be between 0.4 and 0.8 mg/dl * Mixed evidence on T3. Can add mcg/day of cytome
22 AUGEMENTATION STRATEGIES FOR ANTIDEPRESSANTS Add L-methylfolate. Approved by FDA as a medical food. Sold as Deplin. Need 15 mg a day for 30 days Omega 3 Fatty Acid 1.2 grams/ day for 8 weeks
23
24
25
26 LIGHT THERAPY * Some evidence that it is helpful for seasonal affective disorder * Bulb needs to be at least 10 thousand LUX * Light needs to be a table lamp rather than overhead light fixture. * Use at least 30 minutes a day
27 ECT * ECT remains the gold standard for treatment of depression. * Ultra- brief pulse width (0.3 msec) avoids memory problems * Anesthetic is used. Usually methohexitol or propofol. * A fall in EEG amplitude at the end of a seizure is the only predicto ECT outcome. ECT increases neuroplasticity through glutamate a MNDA receptors and produces neurogenesis in the hippocampu * Start with right lateral ECT but if not effective, can switch to bilat * Most patients need 6 12 treatments and they should be tapered rather than stopped abruptly
28 TMS Transcranial Magnetic Stimulation * Uses electrical energy in insulated coil on the scalp to induce a pulsed magnetic field of 1.5 Tesla through the cranium for 2-3 cm. Affects the neural circuitry * Approved by FDA in 2008 * Minimal side effects * After 6 week trial, 51% of patients had response and 25% had remission. John P. O Reardon, M.D. 2015
29 VNS Vagal Nerve Stimulation * A pulse generator is implanted in left chest wall and connected to leads attached to left vagal nerve. * Mild intermittent pulses are applied. When the pulse activates, the patient sounds hoarse if is speaking. * After 12 months, there is a divergence in response between placebo and VNS * This treatment is rarely reimbursed so is rare.
30 TREATING GENERALIZED ANXIETY AND PANIC Depression circuits and anxiety circuits are in overlapping parts of the brain so many of the treatments are the same Dr. Pollard has discussed non-medical strategies for treating anxiety When using medical strategies, the same steps are necessary as when coming up with medical interventions for depression
31 STEP 1: aluate for medical conditions that cause anxiet * Hyperthyroidism * COPD * Asthma * Pheochromocytoma * Coronary heart disease * Vitamin B deficiency * Lyme Disease * Attention Deficit Disorder * Large overlap of GI symptoms/ IBS and anxiety
32 STEP 2 If considering medication, think about: - Therapeutic Alliance - Side effects - Comorbid conditions - Family history of response to antidepressants - Cost In terms of efficacy: SSRI s= SNRI s= = bupropion= TCA s= MAOI s
33 STEP 3 * Start SSRI or SNRI. * SSRI s are usually the first choice. Use a smaller dose than fo depression so anxiety is not precipitated * It takes 12 weeks to see full effect of medication * If the is NO improvement after a month, switch medication * If there is partial improvement, increase the dose of the medication * Anxiety often needs higher doses of medication than depression does.
34 STEP 4 If the patient has a poor response to 2 SSRI s: Switch families of medication Or Augment with another medication
35 AUGMENTATION STRATEGIES * Benzodiazepines work on GABA receptors. They are often useful while an SSRI is getting started. Clonazepam is usually first line since it has the longest half-life. Alprazolam/ Xanax is the worst benzo to use. It has the shortest half-life so it is easier to develop tolerance and it works on a neurotransmitter that none of the other benzo s do so nothing ever feels as good. * Lorazepam is not metabolized by the liver so is the best benzo to use in patients who have liver damage.
36 AUGMENTATION STRATEGIES * Add bupirone/ buspar. Try a minimum of 30 mg for thirty day to judge response. This is a serotonin 1A partial antagonist. (azapirone) Try a minimum of 30 mg for thirty days to judge response. It only works as an adjunct and only for GAD. * alpha-delta Ca++ channel blockers ( gabapentin and pregabalin) * Beta blocker- work within min. * Antihistamines like hydroxyzine
37 SWITCHING STRATEGIES * Try other SSRI s and SNRI s * Try TCA s (tricyclic antidepressants) * Although MAOI s are effective, you will likely refer for that
38 When to Refer to Psychiatry * Comorbid conditions * Psychotic symptoms * Suicidal Ideation * Treatment resistance * The art of making a referral
Psychiatry curbside: Answers to a primary care doctor s top mental health questions
 Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Diagnosis & Management of Major Depression: A Review of What s Old and New. Cerrone Cohen, MD
 Diagnosis & Management of Major Depression: A Review of What s Old and New Cerrone Cohen, MD Why You re Treating So Much Mental Health 59% of Psychiatrists Are Over the Age of 55 AAMC 2014 Physician specialty
Diagnosis & Management of Major Depression: A Review of What s Old and New Cerrone Cohen, MD Why You re Treating So Much Mental Health 59% of Psychiatrists Are Over the Age of 55 AAMC 2014 Physician specialty
Quick Guide to Common Antidepressants-Adults
 Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
Treat mood, cognition, and behavioral disturbances associated with psychological disorders. Most are not used recreationally or abused
 Psychiatric Drugs Psychiatric Drugs Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally or abused Benzodiazepines
Psychiatric Drugs Psychiatric Drugs Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally or abused Benzodiazepines
PSYCHIATRIC DRUGS. Mr. D.Raju, M.pharm, Lecturer
 PSYCHIATRIC DRUGS Mr. D.Raju, M.pharm, Lecturer PSYCHIATRIC DRUGS Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally
PSYCHIATRIC DRUGS Mr. D.Raju, M.pharm, Lecturer PSYCHIATRIC DRUGS Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally
MEDICATION ALGORITHM FOR ANXIETY DISORDERS
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Children s Hospital Of Wisconsin
 Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Depression & Anxiety in Adolescents
 Depression & Anxiety in Adolescents Objectives 1) Review diagnosis of anxiety and depression in adolescents 2) Provide overview of evidence-based treatment options 3) Increase provider comfort level with
Depression & Anxiety in Adolescents Objectives 1) Review diagnosis of anxiety and depression in adolescents 2) Provide overview of evidence-based treatment options 3) Increase provider comfort level with
Psychiatric Medication Guide
 Psychiatric Medication Guide F O R : N E O N P R I M A R Y H E A L T H C A R E P R O V I D E R S B Y : M I C H E L L E R O M E R O, D O M A Y, 2 0 1 3 Anti-depressants TCA s & MAOI s (Tricyclic Antidepressants
Psychiatric Medication Guide F O R : N E O N P R I M A R Y H E A L T H C A R E P R O V I D E R S B Y : M I C H E L L E R O M E R O, D O M A Y, 2 0 1 3 Anti-depressants TCA s & MAOI s (Tricyclic Antidepressants
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment
 Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Medication for Anxiety and Depression. PJ Cowen Department of Psychiatry, University of Oxford
 Medication for Anxiety and Depression PJ Cowen Department of Psychiatry, University of Oxford Topics Medication for anxiety disorders Medication for first line depression treatment Medication for resistant
Medication for Anxiety and Depression PJ Cowen Department of Psychiatry, University of Oxford Topics Medication for anxiety disorders Medication for first line depression treatment Medication for resistant
Review of Psychotrophic Medications. (An approved North Carolina Division of Health Services Regulation Continuing Education Course)
") Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*
 DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*") COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
FROM MEDICATION TO MINDFULNESS: NEW INSIGHTS INTO THE WORLD OF ANXIETY
 13 th Pearl Leibovitch Clinical Day November 18th, 2014 Mounir H. Samy, MD, FRCP(C) Associate Professor of Psychiatry McGill University (ret.) FROM MEDICATION TO MINDFULNESS: NEW INSIGHTS INTO THE WORLD
13 th Pearl Leibovitch Clinical Day November 18th, 2014 Mounir H. Samy, MD, FRCP(C) Associate Professor of Psychiatry McGill University (ret.) FROM MEDICATION TO MINDFULNESS: NEW INSIGHTS INTO THE WORLD
8/15/17. Managing Psychiatric Conditions in Primary Care Beyond the Basics. Speaker s Biography. Situation
 Managing Psychiatric Conditions in Primary Care Beyond the Basics Source: US National Library of Medicine, Images from the History of Medicine Luis Berrios, DNP, MHA, ANP, PMHNP Internal Medicine & Primary
Managing Psychiatric Conditions in Primary Care Beyond the Basics Source: US National Library of Medicine, Images from the History of Medicine Luis Berrios, DNP, MHA, ANP, PMHNP Internal Medicine & Primary
Index. Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) b-adrenergic blockers
 b-adrenergic blockers") Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Practice Guideline for the Treatment of Patients With Major Depressive Disorder: American Psychiatric Association
 Practice Guideline for the Treatment of Patients With Major Depressive Disorder: American Psychiatric Association Our clinical advisor adds updated advice on electroconvulsive therapy, transcranial magnetic
Practice Guideline for the Treatment of Patients With Major Depressive Disorder: American Psychiatric Association Our clinical advisor adds updated advice on electroconvulsive therapy, transcranial magnetic
Psychiatric Illness. In the medical arena psychiatry is a fairly recent field A challenging field Numerous diagnosis
 Psychiatric Illness In the medical arena psychiatry is a fairly recent field A challenging field Numerous diagnosis 12,000,000 children infants through 18 y/o nation wide 5,000,000 suffer severely Serious
Psychiatric Illness In the medical arena psychiatry is a fairly recent field A challenging field Numerous diagnosis 12,000,000 children infants through 18 y/o nation wide 5,000,000 suffer severely Serious
Depression. University of Illinois at Chicago College of Nursing
 Depression University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Recognize depression, its symptoms and behaviors
Depression University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Recognize depression, its symptoms and behaviors
Objectives. Objectives. A practice review. 02-Nov-16 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS
 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
Medications Guide: Public Speaking And Social Anxiety
 AnxietyHub.org Dr. Cheryl Mathews Medications Guide: Public Speaking And Social Anxiety Copyright 2016 AnxietyHub Medications Specifically for Public Speaking and Social Anxiety This is not intended to
AnxietyHub.org Dr. Cheryl Mathews Medications Guide: Public Speaking And Social Anxiety Copyright 2016 AnxietyHub Medications Specifically for Public Speaking and Social Anxiety This is not intended to
Daniel Suzuki, MD Adjunct Clinical Associate Professor of Psychiatry, USC Keck School of Medicine Clinical Adjunct Professor/Faculty, Graduate School
 Daniel Suzuki, MD Adjunct Clinical Associate Professor of Psychiatry, USC Keck School of Medicine Clinical Adjunct Professor/Faculty, Graduate School of Psychology, Fuller Theological Seminary Medical
Daniel Suzuki, MD Adjunct Clinical Associate Professor of Psychiatry, USC Keck School of Medicine Clinical Adjunct Professor/Faculty, Graduate School of Psychology, Fuller Theological Seminary Medical
BRIEF ANTIDEPRESSANT OVERVIEW. Casey Gallimore, Pharm.D., M.S.
 BRIEF ANTIDEPRESSANT OVERVIEW Casey Gallimore, Pharm.D., M.S. Antidepressant Medication Classes First Generation Tricyclic Antidepressants (TCAs) Monoamine Oxidase Inhibitors (MAOIs) Second Generation
BRIEF ANTIDEPRESSANT OVERVIEW Casey Gallimore, Pharm.D., M.S. Antidepressant Medication Classes First Generation Tricyclic Antidepressants (TCAs) Monoamine Oxidase Inhibitors (MAOIs) Second Generation
Primary Care Psychopharmacology for Anxiety Disorders. Holly Ellison, RN, MSN, PMHNP-BC Board Certified Psychiatric Mental Health Nurse Practitioner
 Primary Care Psychopharmacology for Anxiety Disorders Holly Ellison, RN, MSN, PMHNP-BC Board Certified Psychiatric Mental Health Nurse Practitioner Prevalence of Any Anxiety Disorder Among U.S. Adults
Primary Care Psychopharmacology for Anxiety Disorders Holly Ellison, RN, MSN, PMHNP-BC Board Certified Psychiatric Mental Health Nurse Practitioner Prevalence of Any Anxiety Disorder Among U.S. Adults
A Brief Overview of Psychiatric Pharmacotherapy. Joel V. Oberstar, M.D. Chief Executive Officer
 A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
Mental Illness. Doreen L. Rasp, APN, FNP, PMHNP Advanced Behavioral Counseling
 Mental Illness Doreen L. Rasp, APN, FNP, PMHNP Advanced Behavioral Counseling Moodiness Changing Bodies Narcissism Self-Esteem Ignorant Naïve Insecure Self-Centered Independent Adolescence Disorders Affecting
Mental Illness Doreen L. Rasp, APN, FNP, PMHNP Advanced Behavioral Counseling Moodiness Changing Bodies Narcissism Self-Esteem Ignorant Naïve Insecure Self-Centered Independent Adolescence Disorders Affecting
Antidepressant Selection in Primary Care
 Antidepressant Selection in Primary Care R E B E C C A D. L E W I S, D O O O A S U M M E R C M E B R A N S O N, M O 1 5 A U G U S T 2 0 1 5 Objectives Understand the epidemiology of depression. Recognize
Antidepressant Selection in Primary Care R E B E C C A D. L E W I S, D O O O A S U M M E R C M E B R A N S O N, M O 1 5 A U G U S T 2 0 1 5 Objectives Understand the epidemiology of depression. Recognize
Common Antidepressant Medications for Adults
 (and Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac) Fluoxetine Weekly (Prozac Weekly) 20 in AM w/ food (10 mg in elderly or those w/ panic disorder) 20 40 40 (If age >60yo, max 20) 10 10
(and Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac) Fluoxetine Weekly (Prozac Weekly) 20 in AM w/ food (10 mg in elderly or those w/ panic disorder) 20 40 40 (If age >60yo, max 20) 10 10
Treatment of Major Depressive Disorder
 Treatment of Major Depressive Disorder Sarah Mullowney, MD PGY3 Psychiatry Resident, University of Utah Paula Gibbs, MD Medical Director of 5 West at UUMC Clerkship Director MS III Psychiatric Rotation
Treatment of Major Depressive Disorder Sarah Mullowney, MD PGY3 Psychiatry Resident, University of Utah Paula Gibbs, MD Medical Director of 5 West at UUMC Clerkship Director MS III Psychiatric Rotation
For: NEON Primary Healthcare Providers By: Michelle Romero, DO June 2013
 For: NEON Primary Healthcare Providers By: Michelle Romero, DO June 2013 This power point is only a guideline for recommendations in the treatment of psychiatric disorders. This is not comprehensive. Please
For: NEON Primary Healthcare Providers By: Michelle Romero, DO June 2013 This power point is only a guideline for recommendations in the treatment of psychiatric disorders. This is not comprehensive. Please
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Presenter Disclosure. Objectives 6/5/2017. Depression, Anxiety, PTSD: A Focus on Pharmacotherapy
 Depression, Anxiety, PTSD: A Focus on Pharmacotherapy Robert L Page II, Pharm.D., MSPH, FHFSA, FCCP, FAHA Professor of Clinical Pharmacy Clinical Specialist, Division of Cardiology University of Colorado
Depression, Anxiety, PTSD: A Focus on Pharmacotherapy Robert L Page II, Pharm.D., MSPH, FHFSA, FCCP, FAHA Professor of Clinical Pharmacy Clinical Specialist, Division of Cardiology University of Colorado
Antidepressant Medication Therapy in Primary Care July 25, 2013
 New York State Collaborative Care Initiative Antidepressant Medication Therapy in Primary Care July 25, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
New York State Collaborative Care Initiative Antidepressant Medication Therapy in Primary Care July 25, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Antidepressant Selection in Primary Care
 Antidepressant Selection in Primary Care Rebecca D. Lewis, DO OOA Summer CME Oklahoma City, OK 6 August 2017 Objectives Understand the epidemiology of depression. Recognize factors to help choose antidepressants.
Antidepressant Selection in Primary Care Rebecca D. Lewis, DO OOA Summer CME Oklahoma City, OK 6 August 2017 Objectives Understand the epidemiology of depression. Recognize factors to help choose antidepressants.
Antidepressant Medication Strategies We ve Come a Long Way or Have We? Who Writes Prescriptions for Psychotropic Medications. Biological Psychiatry
 Antidepressant Medication Strategies We ve Come a Long Way or Have We? Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free
Antidepressant Medication Strategies We ve Come a Long Way or Have We? Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free
Disclosures. Overview of Workshop. Objectives. Medical Care of Vulnerable and Underserved Populations: Advanced Cases in Anxiety and Depression
 Medical Care of Vulnerable and Underserved Populations: Advanced Cases in Anxiety and Depression Disclosures The speakers have no disclosures. Lisa Ochoa-Frongia, MD Christina Mangurian, MD, MAS L. Elizabeth
Medical Care of Vulnerable and Underserved Populations: Advanced Cases in Anxiety and Depression Disclosures The speakers have no disclosures. Lisa Ochoa-Frongia, MD Christina Mangurian, MD, MAS L. Elizabeth
Mood Disorders.
 Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Treatment of Anxiety (without benzos)
") Treatment of Anxiety (without benzos) Alison C. Lynch MD MS Clinical Professor Departments of Psychiatry and Family Medicine University of Iowa Health Care None Disclosures Overview/objectives Review common
Treatment of Anxiety (without benzos) Alison C. Lynch MD MS Clinical Professor Departments of Psychiatry and Family Medicine University of Iowa Health Care None Disclosures Overview/objectives Review common
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Anxiety Disorders.
 Anxiety Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Anxiety Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Adult Depression - Clinical Practice Guideline
 1 Adult Depression - Clinical Practice Guideline 05/2018 Diagnosis and Screening Diagnostic criteria o Please refer to Attachment A Screening o The United States Preventative Services Task Force (USPSTF)
1 Adult Depression - Clinical Practice Guideline 05/2018 Diagnosis and Screening Diagnostic criteria o Please refer to Attachment A Screening o The United States Preventative Services Task Force (USPSTF)
Psychiatry in Primary Care: What is the Role of Pharmacist?
 Psychiatry in Primary Care: What is the Role of Pharmacist? Benjamin Chavez, PharmD, BCPP, BCACP Clinical Associate Professor Director of Behavioral Health Pharmacy Services January 12, 2019 Disclosure
Psychiatry in Primary Care: What is the Role of Pharmacist? Benjamin Chavez, PharmD, BCPP, BCACP Clinical Associate Professor Director of Behavioral Health Pharmacy Services January 12, 2019 Disclosure
9/20/2011. Integrated Care for Depression & Anxiety: Psychotropic Medication Management for PCPs. Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Guide to Psychiatric Medications for Children and Adolescents
 Guide to Psychiatric Medications for Children and Adolescents by Glenn S. Hirsch, M.D. The following guide includes most of the medications used to treat child and adolescent mental disorders. It lists
Guide to Psychiatric Medications for Children and Adolescents by Glenn S. Hirsch, M.D. The following guide includes most of the medications used to treat child and adolescent mental disorders. It lists
Augmentation and Combination Strategies in Antidepressants treatment of Depression
 Augmentation and Combination Strategies in Antidepressants treatment of Depression Byung-Joo Ham, M.D. Department of Psychiatry Korea University College of Medicine Background The response rates reported
Augmentation and Combination Strategies in Antidepressants treatment of Depression Byung-Joo Ham, M.D. Department of Psychiatry Korea University College of Medicine Background The response rates reported
Clinical Update on Management of Depression and Anxiety in the Primary Care Setting. Objectives: Why Is This Important?
 Clinical Update on Management of Depression and Anxiety in the Primary Care Setting Kirstyn Kameg, DNP, PMHNP, BC University Professor PMHNP Program Coordinator Robert Morris University November 4, 2017
Clinical Update on Management of Depression and Anxiety in the Primary Care Setting Kirstyn Kameg, DNP, PMHNP, BC University Professor PMHNP Program Coordinator Robert Morris University November 4, 2017
Introduction to Drug Treatment
 Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
Prescribing Medications for Anxiety and Depression (without getting anxious and depressed)
") Prescribing Medications for Anxiety and Depression (without getting anxious and depressed) Stephen Warnick Jr., M.D. Assistant Professor Departments of Family Medicine and Psychiatry Disclosures None 2
Prescribing Medications for Anxiety and Depression (without getting anxious and depressed) Stephen Warnick Jr., M.D. Assistant Professor Departments of Family Medicine and Psychiatry Disclosures None 2
PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES
 PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES Table of Contents Print TABLE OF CONTENTS Drug Page Number Anafranil... 2 Asendin... 4 Celexa... 4 Cymbalta... 6 Desyrel... 8 Effexor...10 Elavil...14
PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES Table of Contents Print TABLE OF CONTENTS Drug Page Number Anafranil... 2 Asendin... 4 Celexa... 4 Cymbalta... 6 Desyrel... 8 Effexor...10 Elavil...14
Family Medicine Forum November 10, 2017 Montreal., Quebec. Jon Davine, CCFP, FRCP(C) Associate Professor, McMaster University
 Associate Professor, McMaster University") APPROACH TO DEPRESSION IN PRIMARY CARE Family Medicine Forum November 10, 2017 Montreal., Quebec. Jon Davine, CCFP, FRCP(C) Associate Professor, McMaster University DISCLOSURE Speaker/Presenter Disclosure
APPROACH TO DEPRESSION IN PRIMARY CARE Family Medicine Forum November 10, 2017 Montreal., Quebec. Jon Davine, CCFP, FRCP(C) Associate Professor, McMaster University DISCLOSURE Speaker/Presenter Disclosure
Treatment-resistant depression in primary care
 Treatment-resistant depression in primary care Interprofessional CME, October 2017 Brian J. Mickey, MD, PhD Associate Professor School of Medicine Department of Psychiatry Disclosures Speakers bureau:
Treatment-resistant depression in primary care Interprofessional CME, October 2017 Brian J. Mickey, MD, PhD Associate Professor School of Medicine Department of Psychiatry Disclosures Speakers bureau:
Mentoring Session: Participant Cases
 Handout for the Neuroscience Education Institute (NEI) online activity: Mentoring Session: Participant Cases The Case: 55-year-old patient with depression and anxiety The Question: What to do when antidepressants
Handout for the Neuroscience Education Institute (NEI) online activity: Mentoring Session: Participant Cases The Case: 55-year-old patient with depression and anxiety The Question: What to do when antidepressants
Psychiatry Curbside Top 10
 Psychiatry Curbside Top 10 April 27, 2018 Laurel Ralston, DO Staff Psychiatrist Director of Psych-Oncology, Taussig Cancer Institute Objectives Review current diagnostic and prescribing guidelines for
Psychiatry Curbside Top 10 April 27, 2018 Laurel Ralston, DO Staff Psychiatrist Director of Psych-Oncology, Taussig Cancer Institute Objectives Review current diagnostic and prescribing guidelines for
Cannabinoids and Mental Health
 Cannabinoids and Mental Health https://upload.wikimedia.org/wikipedia/commons Karen M. Lounsbury, PhD Professor of Pharmacology 802-656-3231, Karen.lounsbury@uvm.edu Objectives Describe the underlying
Cannabinoids and Mental Health https://upload.wikimedia.org/wikipedia/commons Karen M. Lounsbury, PhD Professor of Pharmacology 802-656-3231, Karen.lounsbury@uvm.edu Objectives Describe the underlying
Mixing and Matching: Layering Medications as Family Physicians
 Mixing and Matching: Layering Medications as Family Physicians Family Medicine Forum Vancouver, B.C. November 9-12, 2016. Jon Davine, CCFP, FRCP(C) McMaster University Objectives Discuss different examples
Mixing and Matching: Layering Medications as Family Physicians Family Medicine Forum Vancouver, B.C. November 9-12, 2016. Jon Davine, CCFP, FRCP(C) McMaster University Objectives Discuss different examples
Resistance is not futile: working with refractory depression and anxiety
 Resistance is not futile: working with refractory depression and anxiety Divulgation des conflits d intérêts Conseil consultatif ou comité analogue Essais cliniques ou études Honoraires ou autres revenus
Resistance is not futile: working with refractory depression and anxiety Divulgation des conflits d intérêts Conseil consultatif ou comité analogue Essais cliniques ou études Honoraires ou autres revenus
What s New in Depression in 2016? By: Phyliss Nicole Taylor, MD UF Health Jacksonville Psychiatry
 What s New in Depression in 2016? By: Phyliss Nicole Taylor, MD UF Health Jacksonville Psychiatry New Depression Screening Guidelines US Preventive Services Task Force (USPSTF) updated its 2009 recommendations
What s New in Depression in 2016? By: Phyliss Nicole Taylor, MD UF Health Jacksonville Psychiatry New Depression Screening Guidelines US Preventive Services Task Force (USPSTF) updated its 2009 recommendations
This initial discovery led to the creation of two classes of first generation antidepressants:
 Antidepressants - TCAs, MAOIs, SSRIs & SNRIs First generation antidepressants TCAs and MAOIs The discovery of antidepressants could be described as a lucky accident. During the 1950s, while carrying out
Antidepressants - TCAs, MAOIs, SSRIs & SNRIs First generation antidepressants TCAs and MAOIs The discovery of antidepressants could be described as a lucky accident. During the 1950s, while carrying out
Psychiatric Consultant Role in Collaborative Care Sept 12, 2013
 New York State Collaborative Care Initiative Psychiatric Consultant Role in Collaborative Care Sept 12, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
New York State Collaborative Care Initiative Psychiatric Consultant Role in Collaborative Care Sept 12, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
Study Guidelines for Quiz #1
 Annex to Section J Page 1 Study Guidelines for Quiz #1 Theory and Principles of Psychopharmacology, Classifications and Neurotransmitters, Anxiolytics/Antianxiety/Minor Tranquilizers, Stimulants, Nursing
Annex to Section J Page 1 Study Guidelines for Quiz #1 Theory and Principles of Psychopharmacology, Classifications and Neurotransmitters, Anxiolytics/Antianxiety/Minor Tranquilizers, Stimulants, Nursing
Psychiatric Medications. Positive and negative effects in the classroom
 Psychiatric Medications Positive and negative effects in the classroom Teaching the Medicated Child Beverly Bryant, M.D. Hattiesburg Clinic 9/17/14 Introduction According to the National Survey of Children
Psychiatric Medications Positive and negative effects in the classroom Teaching the Medicated Child Beverly Bryant, M.D. Hattiesburg Clinic 9/17/14 Introduction According to the National Survey of Children
Manual of Clinical Psychopharmacology
 Manual of Clinical Psychopharmacology Fourth Edition Alan F. Schatzberg, M.D. Kenneth T. Norris, Jr., Professor and Chairman, Department of Psychiatry and Behavioral Sciences, Stanford University School
Manual of Clinical Psychopharmacology Fourth Edition Alan F. Schatzberg, M.D. Kenneth T. Norris, Jr., Professor and Chairman, Department of Psychiatry and Behavioral Sciences, Stanford University School
Psychotropic Medications Archana Jhawar, PharmD, BCPP Clinical Faculty of UIC Pharmacy Practice Clinical Psychiatric Pharmacist Jesse Brown VA
 Psychotropic Medications Archana Jhawar, PharmD, BCPP Clinical Faculty of UIC Pharmacy Practice Clinical Psychiatric Pharmacist Jesse Brown VA Goals of Medications Use least number at lowest dose to get
Psychotropic Medications Archana Jhawar, PharmD, BCPP Clinical Faculty of UIC Pharmacy Practice Clinical Psychiatric Pharmacist Jesse Brown VA Goals of Medications Use least number at lowest dose to get
Psychobiology Handout
 Nsg 85A / Psychiatric Page 1 of 7 Psychobiology Handout STRUCTURE AND FUNCTION OF THE BRAIN Psychiatric illness and the treatment of psychiatric illness alter brain functioning. Some examples of this are
Nsg 85A / Psychiatric Page 1 of 7 Psychobiology Handout STRUCTURE AND FUNCTION OF THE BRAIN Psychiatric illness and the treatment of psychiatric illness alter brain functioning. Some examples of this are
Steps for Initiating Electroconvulsive Therapy Treatment
 Steps for Initiating Electroconvulsive Therapy Treatment PSYCHIATRISTS CAN REFER PATIENTS FOR ECT TREATMENT AT EL CAMINO HOSPITAL BY CALLING THE ECT NURSE COORDINATOR AT 650-962-5795. Once the referral
Steps for Initiating Electroconvulsive Therapy Treatment PSYCHIATRISTS CAN REFER PATIENTS FOR ECT TREATMENT AT EL CAMINO HOSPITAL BY CALLING THE ECT NURSE COORDINATOR AT 650-962-5795. Once the referral
Optimal Use of Antidepressants: Focusing on SNRI, NDRI and SSRE
 Optimal Use of Antidepressants: Focusing on SNRI, NDRI and SSRE Chan-Hyung Kim, MD Severance Mental Health Hospital Institute of Behavioral Science in Medicine Diagnostic Criteria Pyramid Etiologic Pathophysiologic
Optimal Use of Antidepressants: Focusing on SNRI, NDRI and SSRE Chan-Hyung Kim, MD Severance Mental Health Hospital Institute of Behavioral Science in Medicine Diagnostic Criteria Pyramid Etiologic Pathophysiologic
Disclosure Information
 Disclosure Information I have no financial relationships to disclose. I will discuss the off label use of several depression and anxiety medications in pediatric population Pediatric Depression & Anxiety
Disclosure Information I have no financial relationships to disclose. I will discuss the off label use of several depression and anxiety medications in pediatric population Pediatric Depression & Anxiety
Medications for Anxiety & Behavior in Williams Syndrome. Disclosure of Potential Conflicts. None 9/22/2016. Evaluation
 Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Pharmacotherapy of Anxiety Disorders (GAD, Panic, & SAD) Declaration of Interests
 Declaration of Interests") Pharmacotherapy of Anxiety Disorders (GAD, Panic, & SAD) University of Texas Health Science Center San Antonio Pharmacotherapy Education and Research Center (PERC) 7703 Floyd Curl Drive - MSC 6220 San
Pharmacotherapy of Anxiety Disorders (GAD, Panic, & SAD) University of Texas Health Science Center San Antonio Pharmacotherapy Education and Research Center (PERC) 7703 Floyd Curl Drive - MSC 6220 San
Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression
 Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression Michael D. Jibson, MD, PhD Professor of Psychiatry University of Michigan Major Depression #1 WHO cause of disability
Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression Michael D. Jibson, MD, PhD Professor of Psychiatry University of Michigan Major Depression #1 WHO cause of disability
Focusing on Depression in the Community. Kelly N. Gable, Pharm.D., BCPP Associate Professor SIUE School of Pharmacy
 Focusing on Depression in the Community Kelly N. Gable, Pharm.D., BCPP Associate Professor SIUE School of Pharmacy Disclosure and Conflict of Interest Dr. Gable declares no conflicts of interest, real
Focusing on Depression in the Community Kelly N. Gable, Pharm.D., BCPP Associate Professor SIUE School of Pharmacy Disclosure and Conflict of Interest Dr. Gable declares no conflicts of interest, real
Medications and Children Disorders
 Mental Health Comprehensive Services Providing Family Stability and Developing Life Coping Skills Medications and Children Disorders Psychiatric medications can be an effective part of the treatment for
Mental Health Comprehensive Services Providing Family Stability and Developing Life Coping Skills Medications and Children Disorders Psychiatric medications can be an effective part of the treatment for
New Patient Questionnaire
 4 Embarcadero Center, Suite 1400, San Francisco, CA 94111 (415) 926-7774 phone; (415) 591-7760 office@sanfranciscopsych.com New Patient Questionnaire Thank you for trusting San Francisco Psychiatry with
4 Embarcadero Center, Suite 1400, San Francisco, CA 94111 (415) 926-7774 phone; (415) 591-7760 office@sanfranciscopsych.com New Patient Questionnaire Thank you for trusting San Francisco Psychiatry with
Effective Date: 5/28/2014 Version: 2.0 (Revised: 10/12/2015) Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017)
 Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017)") Protocol Title: Depression & Generalized Anxiety Disorder Effective Date: 5/28/2014 Version: 2.0 (Revised: 10/12/2015) Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017) Group
Protocol Title: Depression & Generalized Anxiety Disorder Effective Date: 5/28/2014 Version: 2.0 (Revised: 10/12/2015) Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017) Group
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
Joel V. Oberstar, M.D. 1
 Diagnosis and Treatment of Depressive Disorders in Children and Adolescents Joel V. Oberstar, M.D. CEO & Chief Medical Officer Adjunct Assistant Professor of Psychiatry University of Minnesota Medical
Diagnosis and Treatment of Depressive Disorders in Children and Adolescents Joel V. Oberstar, M.D. CEO & Chief Medical Officer Adjunct Assistant Professor of Psychiatry University of Minnesota Medical
Dr.Rahiminejad Roozbeh Hospital TUMS
 Dr.Rahiminejad Roozbeh Hospital TUMS Psychiatric disorders, particularly depression, anxiety and eating disorders, are prevalent in diabetes. Mental illness increases risk of diabetes and diabetic complications.
Dr.Rahiminejad Roozbeh Hospital TUMS Psychiatric disorders, particularly depression, anxiety and eating disorders, are prevalent in diabetes. Mental illness increases risk of diabetes and diabetic complications.
I have no conflicts. Objectives. Older Adult Depression: Diagnosis and Treatment. CDC & Elder Depression. Reminders. Major vs Minor Depression
 Older Adult Depression: Diagnosis and Treatment Objectives Describe prevalence, etiology & presentation of depression in the elderly Jody F Agins MSN, RNP, FNP/GNP-BC Collaborative Medical Provider Group
Older Adult Depression: Diagnosis and Treatment Objectives Describe prevalence, etiology & presentation of depression in the elderly Jody F Agins MSN, RNP, FNP/GNP-BC Collaborative Medical Provider Group
Pharmacological Treatment of Anxiety & Depressive Disorders
 Pharmacological Treatment of Anxiety & Depressive Disorders Dr Gary Jackson (MB BCh FRCPsych) Consultant Psychiatrist The Priory Hospital Chelmsford Wellesley Hospital Southend-on-Sea Medical Secretary:
Pharmacological Treatment of Anxiety & Depressive Disorders Dr Gary Jackson (MB BCh FRCPsych) Consultant Psychiatrist The Priory Hospital Chelmsford Wellesley Hospital Southend-on-Sea Medical Secretary:
Pharmacotherapy of depression
 Pharmacotherapy of depression Stuff you already know Stuff you probably know Stuff you possibly don t know Stuff you thought you knew but are mistaken about How long does it take for antidepressants
Pharmacotherapy of depression Stuff you already know Stuff you probably know Stuff you possibly don t know Stuff you thought you knew but are mistaken about How long does it take for antidepressants
Depressive Disorders A clinical overview. Dr. Scott Yarosh, Medical Director, Behavioral Health
 Depressive Disorders A clinical overview Dr. Scott Yarosh, Medical Director, Behavioral Health Depressive Disorders What is depression? Complex series of conditions Physical component Emotional component
Depressive Disorders A clinical overview Dr. Scott Yarosh, Medical Director, Behavioral Health Depressive Disorders What is depression? Complex series of conditions Physical component Emotional component
Depression: A Darker Shade of Blue. CareOregon Pharmacy
 Depression: A Darker Shade of Blue CareOregon Pharmacy Today s Agenda Welcome and Introduction 8:00 Clinical & In Real Life Aspects 8:05 Break 9:15 Medication Review 9:30 Questions 10:30 Closing 10:55
Depression: A Darker Shade of Blue CareOregon Pharmacy Today s Agenda Welcome and Introduction 8:00 Clinical & In Real Life Aspects 8:05 Break 9:15 Medication Review 9:30 Questions 10:30 Closing 10:55
ANTI-DEPRESSANT MEDICATIONS
 ANTI-DEPRESSANT MEDICATIONS This information is not intended to be a substitute for medical advice. It s purpose is solely informative. If your client or yourself are taking antidepressants, do not change
ANTI-DEPRESSANT MEDICATIONS This information is not intended to be a substitute for medical advice. It s purpose is solely informative. If your client or yourself are taking antidepressants, do not change
Pregnancy. General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition)
") Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Pharmacy Technician Objectives. Pharmacist Objectives. Pre-Test Question 2. Pre-Test Question 1 9/27/2016. Disclosure and Conflict of Interest
 Disclosure and Conflict of Interest Focusing on Depression in the Community Kelly N. Gable, Pharm.D., BCPP Associate Professor SIUE School of Pharmacy Dr. Gable declares no conflicts of interest, real
Disclosure and Conflict of Interest Focusing on Depression in the Community Kelly N. Gable, Pharm.D., BCPP Associate Professor SIUE School of Pharmacy Dr. Gable declares no conflicts of interest, real
Objectives. DSM-V Changes: Elimination of Multiaxial Diagnostic System
 Conflicts of Interest I have no conflicts to disclose. 2014 Updates to the Updates in Pharmacotherapy Webinar Psychiatry Updates for Pharmacotherapy Specialists Jacintha S. Cauffield, Pharm.D., BCPS Associate
Conflicts of Interest I have no conflicts to disclose. 2014 Updates to the Updates in Pharmacotherapy Webinar Psychiatry Updates for Pharmacotherapy Specialists Jacintha S. Cauffield, Pharm.D., BCPS Associate
BIOLOGICAL TREATMENT IN PSYCHIATRY. PTE ÁOK Dept.of Psychiatry Pécs
 BIOLOGICAL TREATMENT IN PSYCHIATRY PTE ÁOK Dept.of Psychiatry Pécs 1 SGA effects pharmacokinetic effect chemical strucrure Receptor block D2 5-HT2 α1 H-1 M Selectíve DA (D2D3) antagonists Benzamids Amisulpiride
BIOLOGICAL TREATMENT IN PSYCHIATRY PTE ÁOK Dept.of Psychiatry Pécs 1 SGA effects pharmacokinetic effect chemical strucrure Receptor block D2 5-HT2 α1 H-1 M Selectíve DA (D2D3) antagonists Benzamids Amisulpiride
Treatment of Depression in the Primary Care Office
 Treatment of Depression in the Primary Care Office Paul E.A. Glaser, MD, PhD Departments of Psychiatry, Pediatrics and Anatomy & Neurobiology University of Kentucky November 5, 2010 Disclosures of Potential
Treatment of Depression in the Primary Care Office Paul E.A. Glaser, MD, PhD Departments of Psychiatry, Pediatrics and Anatomy & Neurobiology University of Kentucky November 5, 2010 Disclosures of Potential
4/2/13 COMMON CLASSES OF MEDICATIONS. Child & Adolescent Behavioral Medicine & Medication Therapies. Behavioral Medicine & Medication Therapies
 Child & Adolescent Behavioral Medicine & Medication Therapies Brian J Cowles, PharmD Associate Professor of Pharmacy Practice Albany College of Pharmacy & Health Sciences; Vermont Campus Behavioral Medicine
Child & Adolescent Behavioral Medicine & Medication Therapies Brian J Cowles, PharmD Associate Professor of Pharmacy Practice Albany College of Pharmacy & Health Sciences; Vermont Campus Behavioral Medicine
PSYCHIATRIC MANAGEMENT IN PRIMARY CARE. Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust
 Mersey Care NHS Trust") PSYCHIATRIC MANAGEMENT IN PRIMARY CARE Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust Areas to cover Mood Disorders Anxiety Disorders Miscellaneous Conditions
PSYCHIATRIC MANAGEMENT IN PRIMARY CARE Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust Areas to cover Mood Disorders Anxiety Disorders Miscellaneous Conditions
Medication management of anxiety & depression. Dr Katie Simpson GP Mental health lead East Berks CCG
 Medication management of anxiety & depression Dr Katie impson GP Mental health lead East Berks CCG NICE guidelines for Anxiety tepped Care RIs and NRIs in Anxiety disorders RI ertraline Citalopram Fluoxetine
Medication management of anxiety & depression Dr Katie impson GP Mental health lead East Berks CCG NICE guidelines for Anxiety tepped Care RIs and NRIs in Anxiety disorders RI ertraline Citalopram Fluoxetine
Clinical Policy: Vilazodone (Viibryd) Reference Number: CP.PMN.145 Effective Date: Last Review Date: Line of Business: HIM, Medicaid
 Reference Number: CP.PMN.145 Effective Date: Last Review Date: Line of Business: HIM, Medicaid") Clinical Policy: (Viibryd) Reference Number: CP.PMN.145 Effective Date: 08.01.12 Last Review Date: 08.18 Line of Business: HIM, Medicaid Revision Log See Important Reminder at the end of this policy for
Clinical Policy: (Viibryd) Reference Number: CP.PMN.145 Effective Date: 08.01.12 Last Review Date: 08.18 Line of Business: HIM, Medicaid Revision Log See Important Reminder at the end of this policy for
Class Update: Second Generation Antidepressant Medications. Dossier received: Yes
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Managing Anxiety Disorder in Primary Care
 Saturday General Session Managing Anxiety Disorder in Primary Care Chris Ticknor, MD Private Practice, Psychiatry Adjunct Professor of Psychiatry UT Health Science Center at San Antonio San Antonio, Texas
Saturday General Session Managing Anxiety Disorder in Primary Care Chris Ticknor, MD Private Practice, Psychiatry Adjunct Professor of Psychiatry UT Health Science Center at San Antonio San Antonio, Texas
The Latest in Treating Depression and Anxiety in Primary Care
 The Latest in Treating Depression and Anxiety in Primary Care Wendy L. Wright MS, ANP-BC, FNP-BC, FAANP, FAAN, FNAP Adult/Family Nurse Practitioner Owner Wright & Associates Family Healthcare @ Amherst
The Latest in Treating Depression and Anxiety in Primary Care Wendy L. Wright MS, ANP-BC, FNP-BC, FAANP, FAAN, FNAP Adult/Family Nurse Practitioner Owner Wright & Associates Family Healthcare @ Amherst
Psychopharmacological Management of Depressive and Anxiety Disorders
 Psychopharmacological Management of Depressive and Anxiety Disorders Waseem Ahmed, M.D Medical Director: Population Health and Dallas County Correctional System Email: waseem.ahmed@phhs.org Tel: 214-653-2927
Psychopharmacological Management of Depressive and Anxiety Disorders Waseem Ahmed, M.D Medical Director: Population Health and Dallas County Correctional System Email: waseem.ahmed@phhs.org Tel: 214-653-2927
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
Management of SSRI Induced Sexual Dysfunction. Serotonin Reuptake Inhibitors*
 Management of SSRI Induced Sexual Dysfunction John J. Miller, M.D. Medical Director, Center for Health and WellBeing Exeter, NH Serotonin Reuptake Inhibitors* fluoxetine clomipramine sertraline paroxetine
Management of SSRI Induced Sexual Dysfunction John J. Miller, M.D. Medical Director, Center for Health and WellBeing Exeter, NH Serotonin Reuptake Inhibitors* fluoxetine clomipramine sertraline paroxetine