Therapeutic drug monitoring in neuropsychopharmacology: does it hold its promises?
|
|
|
- Ginger Richardson
- 6 years ago
- Views:
Transcription

1 Therapeutic drug monitoring in neuropsychopharmacology: does it hold its promises? Prof. Dr. Christoph Hiemke Psychiatrische Klinik und Poliklinik Universität Mainz
2 Psychopharmacotherapy Psychiatric Patient Diagnosis Symptoms Severity of symptoms Patient s history Selection of medication including dose and/or other treatment options Theory Response Remission
3 Psychopharmacotherapy Step 1 Step 2 Step 3 Step 4 Step 5 Drug A monotherapy Drug B monotherapy Drug combination Other options: ECT Drugs from other classes Experimental methods Augmentation Augmentation Reality Continuation Continuation Continuation Continuation Continuation
4 Patient (male, age 29 years) Schizophrenia, psychotic symptoms Case Report First episode Olanzapine, quetiapine, venlafaxine (negative symptoms), insufficient response, relapse Next treatment: Ziprasidone plus quetiapine plus venlafaxine Suicide attempt, intoxication using venlafaxine Intensive care unit, discontinuation of antipsychotic medication Dept of Psychiatry Amisulpride 200 then 600 mg/day motor side effects Amisulpride 400 mg still side effects Clozapine 175 mg Clozapine 300 mg still negative symptoms Reboxetine, 4 mg Citalopram, 40 mg Improvement and stabilization 230 ng/ml 516 ng/ml 310 ng/ml 311 ng/ml 439 ng/ml 159 ng/ml 48 ng/ml

5 Arzneimittel und Metabolite Genotype Nutrition, smoking, comorbidity, age.. Psychiatric patient Pharmacodynamics Receptor Uptake Enzyme Ion channel e.t.c. Clinical effects Drug and metabolites Drug Arzneimittel- Metabolite und Muttersubstanz Pharmacokinetics Absorption Distribution Metabolism Phenotype Excretion C. Hiemke
6 Dose and blood level Citalopram (ng/ml) Citalopram Dose (mg/day)
7 Mean dose Mean plasma concentration (ng/ml) Dose and blood level 679 ± 229 mg/d 317 ± 270 ng/ml men women r = 0.32 r s = 0.37 P < (N = 179) Amisulpride dose (mg/day)
8 Blood and brain concentration r=0.953 P < Aravagiri et al., 1999

9 Dose and receptor binding Blood level and receptor binding
 Occupancy and Dose or Plasma Concentration of Paroxetine in 14 Healthy and Depressed Subjects Meyer et al.")
10 Dose and Uptake-binding Blood level and Uptake-binding Relationship Between Striatal Serotonin Transporter (5- HTT) Occupancy and Dose or Plasma Concentration of Paroxetine in 14 Healthy and Depressed Subjects Meyer et al., 2004
11 Plasma concentrations are highly variable between patients Plasma concentrations correlate well with brain concentrations Plasma concentrations correlate well with in vivo receptor binding Plasma concentrations reflect brain concentrations
12 Arzneimittel und Metabolite Genotype Nutrition, smoking, comorbidity, age.. Psychiatric patient Pharmacodynamics Receptor Uptake Enzyme Ion channel e.t.c. Clinical effects Drug and metabolites Drug Arzneimittel- Metabolite und Muttersubstanz Pharmacokinetics Absorption Distribution Metabolism Phenotype TDM Excretion C. Hiemke
13 Therapeutic Drug Monitoring Improves therapeutic efficacy Improves drug safety Reduces costs
14
15 Nonresponse Intoxication < >140 Åsberg et al. 1971
16 Promises Therapeutic Drug Monitoring Improves therapeutic efficacy? Improves drug safety? Reduces costs?
17 Cost effectiveness of TDM in psychiatry
18 Patients under amitriptyline/ nortriptyline US$ Costs Pharmacokinetic dosing 2100 Benefits Savings from fewer hospital days Savings from an earlier return to work Total savings 5322 Benefit/cost ratio 2,5 Simmons et al., 1985 TDM reduces direct and indirect costs
19 TDM of tricyclic antidepressants Extra costs per 1000 patients for additional managment Costs for 1000 drug determinations Savings by TDM USD USD USD Preskorn and Fast, 1991 TDM for antidepressants: efficacy, saftey, and cost effectiveness: J Clin Psychiatry 52:
20 TDM of new antidepressants Lundmark et al., (2001) Therapeutic drug monitoring of selective serotonin reuptake inhibitors influences clinical dosing strategies and reduces drug costs in depressed elderly patients. Acta Psychiatr. Scand. 101: depressed patients treated with citalopram, paroxetine or sertraline Drug costs before introduction of TDM: USD 71,071 Drug costs after introduction of TDM: USD 60,018 Analytical costs for TDM: USD 5,387 Savings after introduction of TDM: USD 5,666 TDM reduces drug costs
21 Medical impact of TDM in psychiatry
22 Therapeutic Drug Monitoring of Antidepressants Depressed patients Treament with a tricylic antidepressant Ther. effects: HAMD and CGI, weekly (day 0-70) Side effects: UKU TDM Blood level measurement Dose recommendation RANDOMIZATION No TDM No dose recommendation
23 TDM of tricyclic antidepressants Change in CGI score TDM no TDM 0 TDM no TDM Müller et al Change in HAMD score
24 TDM of tricyclic antidepressants plasma concentrations within optimal range plasma concentrations out of optimal range Day 7 Day 14 Day 21 Müller et al Change in HAMD score
25 . The results showed that combining TDM and clinical judgement during the early course of treatment provides a superior outcome in depression. However, the compliance of the psychiatrists in charge to recommendations provided together with serum levels was far from perfect. The results encourage further studies to optimize antidepressant pharmacotherapy when using TDM appropriately. Müller et al. 2003
26 Therapeutic Drug Monitoring of New Antidepressants Depressed patients Treament with an SSRI or venlafaxine Ther. effects: HAMD and CGI, weekly (day 0-70) Side effects: UKU TDM Blood level measurement Dose recommendation RANDOMIZATION No TDM No dose recommendation
27 Therapeutic Drug Monitoring of New Antidepressants
28 Therapeutic Drug Monitoring of New Antidepressants Ocurrence (% of patients)* Discontinuation of drugs with TDM: 9.1 without TDM: 17.9 Change of medication with TDM: 3.2 without TDM: 5.9 *n=219
29 Therapeutic Drug Monitoring of Venlafaxine R 2 = With TDM Without TDM R 2 = days Days of treatment HAMD % base line score reduction 17.8 days 24.2 days 33.9 days
30 TDM of antipsychotic drugs
31 TDM of amisulpride O N H C H 2 N O N H C H 2 N O-CH 3 C 2 H 5 O O-CH 3 C 2 H 5 H 2 NO 2 S C H 3 C H 2 S O NH 2 Sulpiride Amisulpride
32 Diagnoses TDM of amisulpride 80% SCHIZ (660mg) SAD (590 mg) AFFECT (480mg) ORGAN (500 mg) PERSDIS (800 mg) 6% 3% Müller et al. (2007) J Psychiatr Res 11% N=527
33 Mean daily dose Mean serum level Serum concentration (ng/ml) TDM of Amisulpride 679 ± 229 mg/d 317 ± 270 ng/ml Men Women r = 0.32 r s = 0.37 P < (N = 179) Amisulpride dose (mg/day)
34 TDM of amisulpride Patients with schizophrenia according to DSM IV Antipsychotic monotherapy with amisulpride N=378 Dose 594 ± 262 mg/day Mean trough plasma level 315 ± 277 ng/ml 50% range ng/ml Müller et al. (2005) J Psychiatr Res (e-pub ahead)
35 TDM of amisulpride Response 700 Mean daily dose [mg] 350 Trough plasma level [ng/ml] n.s. 0 Müller et al. (2007) J Psychiatr Res P = Non-Response (9%) At least slight response (91%) Median 248±291 ng/ml 316±253 ng/ml
36 TDM of amisulpride Side effects Mean daily dose [mg] Trough plasma level [ng/ml] n.s. 100 n.s. 50 P = No EPS (85%) At least mild EPS (15%) Median Müller et al. (2005) J Psychiatr Res
37 Müller et al. (2005) J Psychiatr Res (e-pub ahead)
38 Appropriateness of Therapeutic Drug Monitoring in Routine
39 Appropriateness of Therapeutic Drug Monitoring in Routine Δt BE Δt Lab Δt Reaction Dose Time Dose adaptiation Reporting of results Blood withdrawal Start of dosing Mann, Hiemke, Schmidt, Bates 2006
40 Appropriateness of Therapeutic Drug Monitoring in Routine ΔtBE Antidepressants Frequency >14 Days after change of dose Mann, Hiemke, Schmidt, Bates 2006
41 Zernig et al. 2004, Therapeutic Drug Monitoring *Retrospective analyses of 2nd requests (antipsychotic drugs) Pharmacokinetic Problems 41%, 0 to 3 days after 1. request 38%, on the day of dose change Clinical Problems 57%, no dose reduction in spite of too high blood levels dose change in spite of optimal level no dose increase in spite of too low blood levels
42 . The results showed that combining TDM and clinical judgement during the early course of treatment provides a superior outcome in depression. However, the compliance of the psychiatrists in charge to recommendations provided together with serum levels was far from perfect. The results encourage further studies to optimize antidepressant pharmacotherapy when using TDM appropriately. Müller et al. 2003

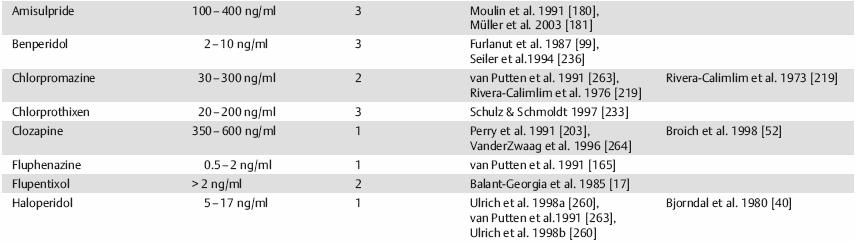
43 Lausanne 2004 Pharmacopsychiatry 37 (2004) AGNP-Guidelines: Therapeutic Drug Monitoring in Psychiatry
44


45
46 Specific Indications to Use TDM Comorbity Comorbity Renal Renal or or liver liver dysfunction dysfunction Suggested Suggested non-compliance non-compliance Risk Risk of of intoxication intoxication Aged Agedpatients >65 >65 y y Insufficient Insufficient response response Children Children adolescent adolescent TDM Side Side effects effects Distinct Distinct genotype genotype Drug Drug combinations combinations Relapse Relapse Relapse Relapse prevention prevention Suggested Suggested Drug Drug interaction interaction
47 Indications to use TDM Comorbity Comorbity Renal Renal or or liver liver dysfunction dysfunction Suggested Suggested non-compliance non-compliance Risk Risk of of intoxication intoxication Aged Agedpatients >65 >65 y y Insufficient Insufficient response response Children Children adolescent adolescent TDM Side Side effects effects Distinct Distinct genotype genotype Drug Drug combinations combinations Relapse Relapse Relapse Relapse prevention prevention Suggested Suggested Drug Drug interaction interaction
48 600 ng/ml Combination Clomipramine-Fluvoxamine-Oxybutynin Clomipramine Patient, female Age: 72 yrs Diagnosis: MDE CYP2D6-Status: EM Fluvoxamine + Oxybutynin /150 + Clomipramine 150 mg 125 mg 75 mg 37,5 mg 25 mg 50 mg / / /75 Norclomipramine /37, / / / /50

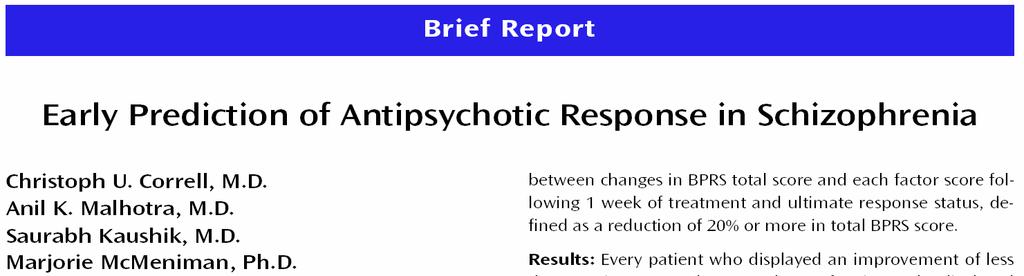
49 Indications to use TDM Comorbity Comorbity Renal Renal or or liver liver dysfunction dysfunction Suggested Suggested non-compliance non-compliance Risk Risk of of intoxication intoxication Aged Agedpatients >65 >65 y y Insufficient Insufficient response response Children Children adolescent adolescent TDM Side Side effects effects Distinct Distinct genotype genotype Drug Drug combinations combinations Relapse Relapse Relapse Relapse prevention prevention Suggested Suggested Drug Drug interaction interaction
50 Haro et al. (2006) J Clin Psychopharmacol 26:
51
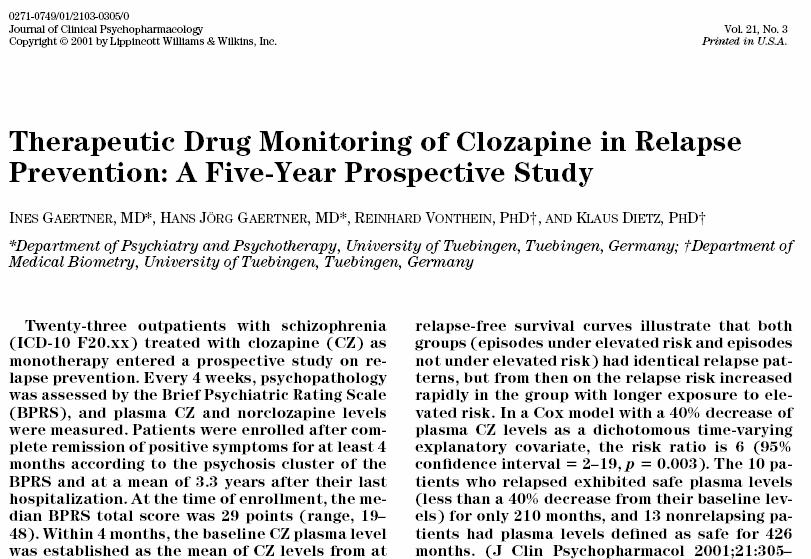
52 Cox analysis within the first two years, both groups exhibited identical relapse patterns: then 6fold risk > 12% of time on risk < 12% of time on risk Solid curve: elevated risk less than 12% of the whole observation period, dashed curve: elevated risk more than 12% of the whole observation period I. Gaertner et al., 2001
53 TDM and decision making
54 TDM and Clinical Decision Making TDM REQUEST Change of Medication Blood withdrawal under steady-state Trough levels Drug determination in blood serum or plasma Change of Dose within Serum level therapeutic range not within no Improvement yes Continuation of Drug Treatment
55 TDM in the future
56 ANTIPSYCHOTIC DRUG RESPONSE IN SCHIZOPHRENIA
57 ANTIPSYCHOTIC DRUG RESPONSE IN SCHIZOPHRENIA Improvement* >20% *BPRS total score 54 + fluphenazine 20 mg/day Number of patients Improvement* >20% Stable reponse Improvement* <20% Improvement* <20% + fluphenazine 20 mg/day 41 Week Week 4 Improvement* >20% Improvement* <20% Stable nonresponse C.U. Correll et al.: Early prediction of antipsychotic response in schizophrenia Am J Psychiatry 2003; 160:
58 ANTIPSYCHOTIC DRUG RESPONSE IN SCHIZOPHRENIA Improvement* >20% *BPRS total score 56 + fluphenazine 20 mg/day 37 % 63 % Improvement* >20% Stable reponse Improvement* <20% Number of patients 100 Nonresponse predicts nonresponse Improvement* <20% + fluphenazine 20 mg/day P< Week 1 0 % 100 % Week 4 Improvement* >20% Improvement* <20% Stable nonresponse C.U. Correll et al.: Early prediction of antipsychotic response in schizophrenia Am J Psychiatry 2003; 160:
59 ANTIPSYCHOTIC DRUG RESPONSE IN SCHIZOPHRENIA Nonresponse predicts nonresponse Relevant antipsychotic efficacy is unlikely to occur if it does not begin within the first weeks of treatment Objective symptom ratings may be a clinically useful, time-effective, and cost-effective method to guide early antipsychotic treatment decisions Correll et al. (2003) Am J Psychiatry 160:
60 TDM and Clinical Decision Making TDM REQUEST Change of Medication Blood withdrawal under steady-state Trough levels Drug determination in blood serum or plasma Change of Dose within Serum level therapeutic range not within Length of treatment > 2 weeks < 2 weeks Objective symptom rating Improvement <20% >20% Continuation of Drug Treatment
61 Therapeutic drug monitoring in neuropsychopharmacology: does it hold its promises? Pharmacology gives evidence that TDM is helpful for treatment optimization in neuropsychopharmacology since blood levels are highly variable blood levels reflect well brain concentrations blood levels correlate with receptor occupancy There are many distinct indications to use TDM not only suspected non-compliance Evidence is unclear for many antidepressant and antipsychotic drugs that TDM it is cost effective The appropriate use of TDM must be improved in the future considering the TDM guidelines
62 Thank you for your attention
Pharmacogenetic Testing in Psychiatry Jose de Leon, MD ( )
") Pharmacogenetic Testing in Psychiatry Jose de Leon, MD (12-01-15) Conflicts of Interest (See more details on conflict of interest in the first presentation Training Psychiatrists to Think like Pharmacologists
Pharmacogenetic Testing in Psychiatry Jose de Leon, MD (12-01-15) Conflicts of Interest (See more details on conflict of interest in the first presentation Training Psychiatrists to Think like Pharmacologists
Introduction to Drug Treatment
 Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
Risperidone Case 1: Drug-Drug Interactions
 Risperidone Case 1: Drug-Drug Interactions 1-14-16 de Leon & Bork (a resident) J Clin Psychiatry 1997;58:450-1 http://www.ncbi.nlm.nih.gov/pubmed/9375597 Jose de Leon, MD Educational Objectives At the
Risperidone Case 1: Drug-Drug Interactions 1-14-16 de Leon & Bork (a resident) J Clin Psychiatry 1997;58:450-1 http://www.ncbi.nlm.nih.gov/pubmed/9375597 Jose de Leon, MD Educational Objectives At the
Depression in Pregnancy
 TREATING THE MOTHER PROTECTING THE UNBORN A MOTHERISK Educational Program The content of this program reflects the expression of a consensus on emerging clinical and scientific advances as of the date
TREATING THE MOTHER PROTECTING THE UNBORN A MOTHERISK Educational Program The content of this program reflects the expression of a consensus on emerging clinical and scientific advances as of the date
They deserve personalized treatment
 Your patients are unique They deserve personalized treatment New laboratory service offered by STA 2 R is a panel of genetic tests that gives prescribers answers to the clinical questions below. The test
Your patients are unique They deserve personalized treatment New laboratory service offered by STA 2 R is a panel of genetic tests that gives prescribers answers to the clinical questions below. The test
Pharmacogenomics and Customized Therapies in Psychiatry
 Pharmacogenomics and Customized Therapies in Psychiatry Toshiyuki Someya,, MD, PhD Department of Psychiatry Niigata University Graduate School of Medical and Dental Sciences The efficacy and side effects
Pharmacogenomics and Customized Therapies in Psychiatry Toshiyuki Someya,, MD, PhD Department of Psychiatry Niigata University Graduate School of Medical and Dental Sciences The efficacy and side effects
CYP2D6: mirtazapine 2001/2002/2003
 CYP2D6: mirtazapine 2001/2002/200 Cl or = oral clearance,=c ss = steady state concentration, EM = extensive metaboliser, IM = intermediate metaboliser, MR = metabolic ratio, NS = non-significant, PM =
CYP2D6: mirtazapine 2001/2002/200 Cl or = oral clearance,=c ss = steady state concentration, EM = extensive metaboliser, IM = intermediate metaboliser, MR = metabolic ratio, NS = non-significant, PM =
Guidelines/Supporting Studies* FDA Label Information Additional Information/Commentsxc` Gene(s)/Level of evidence
/Level of evidence") Drug Gene(s)/Level of evidence Guidelines/Supporting Studies* FDA Label Information Additional Information/Commentsxc` Haloperidol CYP2D6 ( SLC6A5 ( 2D6: DPWG guidelines Reduce dose by 50% in PMs Aripiprazole
Drug Gene(s)/Level of evidence Guidelines/Supporting Studies* FDA Label Information Additional Information/Commentsxc` Haloperidol CYP2D6 ( SLC6A5 ( 2D6: DPWG guidelines Reduce dose by 50% in PMs Aripiprazole
KEY MESSAGES. It is often under-recognised and 30-50% of MDD cases in primary care and medical settings are not detected.
 KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
Psychopharmacology. Psychopharmacology. Hamish McAllister-Williams Reader in Clinical. Department of Psychiatry, RVI
 Regional Affective Disorders Service Psychopharmacology Northumberland, Tyne and Wear NHS Trust Hamish McAllister-Williams Reader in Clinical Psychopharmacology Department of Psychiatry, RVI Intro NOT
Regional Affective Disorders Service Psychopharmacology Northumberland, Tyne and Wear NHS Trust Hamish McAllister-Williams Reader in Clinical Psychopharmacology Department of Psychiatry, RVI Intro NOT
Mental Health DNA Insight WHITE PAPER
 Mental Health DNA Insight WHITE PAPER JULY 2016 Mental Health DNA Insight / White Paper Mental Health DNA Insight Pathway Genomics Mental Health DNA Insight test is aimed to help psychiatrists, neurologists,
Mental Health DNA Insight WHITE PAPER JULY 2016 Mental Health DNA Insight / White Paper Mental Health DNA Insight Pathway Genomics Mental Health DNA Insight test is aimed to help psychiatrists, neurologists,
Antidepressants (Tricyclic Antidepressants, Selective Serotonin Reuptake Inhibitors) in children 6-12 years of age with depressive episode/disorder
 in children 6-12 years of age with depressive episode/disorder") updated 2012 Antidepressants (Tricyclic Antidepressants, Selective Serotonin Reuptake Inhibitors) in children 6-12 years of age with depressive episode/disorder Q10: Are antidepressants (Tricyclic antidepressants
updated 2012 Antidepressants (Tricyclic Antidepressants, Selective Serotonin Reuptake Inhibitors) in children 6-12 years of age with depressive episode/disorder Q10: Are antidepressants (Tricyclic antidepressants
Clinical Guideline for the Management of Bipolar Disorder in Adults
 Clinical Guideline for the Management of Bipolar Disorder in Adults Goal: To improve the quality of life of adults with bipolar disorder Identification and Treatment of Bipolar Disorder Criteria for Diagnosis:
Clinical Guideline for the Management of Bipolar Disorder in Adults Goal: To improve the quality of life of adults with bipolar disorder Identification and Treatment of Bipolar Disorder Criteria for Diagnosis:
TREATING MAJOR DEPRESSIVE DISORDER
 TREATING MAJOR DEPRESSIVE DISORDER A Quick Reference Guide Based on Practice Guideline for the Treatment of Patients With Major Depressive Disorder, Second Edition, originally published in April 2000.
TREATING MAJOR DEPRESSIVE DISORDER A Quick Reference Guide Based on Practice Guideline for the Treatment of Patients With Major Depressive Disorder, Second Edition, originally published in April 2000.
Clozapine Case 1 The Relevance of CYP Jose de Leon, MD
 Clozapine Case 1 The Relevance of CYP 12-18-15 Jose de Leon, MD 1. Clozapine Case 1 J Clin Psychiatry 1996;57:175-176 http://www.ncbi.nlm.nih.gov/pubmed/8601555 Educational Objectives At the conclusion
Clozapine Case 1 The Relevance of CYP 12-18-15 Jose de Leon, MD 1. Clozapine Case 1 J Clin Psychiatry 1996;57:175-176 http://www.ncbi.nlm.nih.gov/pubmed/8601555 Educational Objectives At the conclusion
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Pharmacological treatment of anxiety disorders where is
 Pharmacological treatment of anxiety disorders where is the room for improvement? David S Baldwin, Professor of Psychiatry BAP Masterclass, 15 th April 2011 dsb1@soton.ac.uk Declaration of interests (last
Pharmacological treatment of anxiety disorders where is the room for improvement? David S Baldwin, Professor of Psychiatry BAP Masterclass, 15 th April 2011 dsb1@soton.ac.uk Declaration of interests (last
Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A
 Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A Faculty/Presenter Disclosures Faculty: Mike Allan Salary: College
Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A Faculty/Presenter Disclosures Faculty: Mike Allan Salary: College
Clozapine Case 6: Half-Life Jose de Leon, MD
 Clozapine Case 6: Half-Life 1-16-16 Jose de Leon, MD 6. Clozapine Case 6 J Clin Psychopharmacol 1996;16:193-4. http://www.ncbi.nlm.nih.gov/pubmed/8690839 Educational Objectives At the conclusion of this
Clozapine Case 6: Half-Life 1-16-16 Jose de Leon, MD 6. Clozapine Case 6 J Clin Psychopharmacol 1996;16:193-4. http://www.ncbi.nlm.nih.gov/pubmed/8690839 Educational Objectives At the conclusion of this
Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A
 Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A Faculty/Presenter Disclosures Faculty: Mike Allan Salary: College
Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A Faculty/Presenter Disclosures Faculty: Mike Allan Salary: College
Mood Disorders.
 Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Antidepressants. Dr Malek Zihlif
 Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
Pharmacogenomics of Medications for Pain and Major Depression: Promise and Peril
 Pharmacogenomics of Medications for Pain and Major Depression: Promise and Peril Geoffrey C. Wall, PharmD, FCCP, BCPS, CGP Professor of Clinical Sciences Drake University College of Pharmacy and Health
Pharmacogenomics of Medications for Pain and Major Depression: Promise and Peril Geoffrey C. Wall, PharmD, FCCP, BCPS, CGP Professor of Clinical Sciences Drake University College of Pharmacy and Health
The Pharmacological Management of Bipolar Disorder: An Update
 Psychobiology Research Group The Pharmacological Management of Bipolar Disorder: An Update R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon.
Psychobiology Research Group The Pharmacological Management of Bipolar Disorder: An Update R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon.
Clinical Perspective on Conducting TRD Studies. Hans Eriksson, M.D., Ph.D., M.B.A. Chief Medical Specialist, H. Lundbeck A/S Valby, Denmark
 Clinical Perspective on Conducting TRD Studies Hans Eriksson, M.D., Ph.D., M.B.A. Chief Medical Specialist, H. Lundbeck A/S Valby, Denmark Overview of Presentation Treatment-Resistant Depression (TRD)
Clinical Perspective on Conducting TRD Studies Hans Eriksson, M.D., Ph.D., M.B.A. Chief Medical Specialist, H. Lundbeck A/S Valby, Denmark Overview of Presentation Treatment-Resistant Depression (TRD)
The AGNP-TDM Expert Group Consensus Guidelines: Therapeutic Drug Monitoring in Psychiatry
 P. Baumann 1 C. Hiemke 2 S. Ulrich 3 G. Eckermann 4 I. Gaertner 5 M. Gerlach 6 H.-J. Kuss 7 G. Laux 8 B. Müller-Oerlinghausen 9 M. L. Rao 10 P. Riederer 11 G. Zernig 12 The AGNP-TDM Expert Group Consensus
P. Baumann 1 C. Hiemke 2 S. Ulrich 3 G. Eckermann 4 I. Gaertner 5 M. Gerlach 6 H.-J. Kuss 7 G. Laux 8 B. Müller-Oerlinghausen 9 M. L. Rao 10 P. Riederer 11 G. Zernig 12 The AGNP-TDM Expert Group Consensus
Antipsychotics. Something Old, Something New, Something Used to Treat the Blues
 Antipsychotics Something Old, Something New, Something Used to Treat the Blues Objectives To provide an overview of the key differences between first and second generation agents To an overview the newer
Antipsychotics Something Old, Something New, Something Used to Treat the Blues Objectives To provide an overview of the key differences between first and second generation agents To an overview the newer
Treatment of Schizophrenia
 Treatment of Schizophrenia Conduct comprehensive assessment and use measurement-based care as found in the Principles of Practice (review pages 4-7). Most importantly assess social support system (housing,
Treatment of Schizophrenia Conduct comprehensive assessment and use measurement-based care as found in the Principles of Practice (review pages 4-7). Most importantly assess social support system (housing,
Florida Best Practice Medication Guidelines Principles of Practice for Adults
 http://flmedicaidbh.fmhi.usf.edu Florida Best Practice Medication Guidelines Principles of Practice for Adults 1. Goal of the Guidelines Persistent gaps exist in the quality of mental health care delivered
http://flmedicaidbh.fmhi.usf.edu Florida Best Practice Medication Guidelines Principles of Practice for Adults 1. Goal of the Guidelines Persistent gaps exist in the quality of mental health care delivered
Psychiatry curbside: Answers to a primary care doctor s top mental health questions
 Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Guidelines MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD)
") MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
Two decades of clinical pharmacogenetic testing - Where do we stand?
 Two decades of clinical pharmacogenetic testing - Where do we stand? Marja-Liisa Dahl, MD PhD, Professor Dept of Clinical Pharmacology Karolinska University Hospital/Karolinska Institutet Stockholm, Sweden
Two decades of clinical pharmacogenetic testing - Where do we stand? Marja-Liisa Dahl, MD PhD, Professor Dept of Clinical Pharmacology Karolinska University Hospital/Karolinska Institutet Stockholm, Sweden
DISEASES AND DISORDERS
 DISEASES AND DISORDERS 13. The mood (affective) disorders 99 14. The psychotic disorders: schizophrenia 105 15. The anxiety and somatoform disorders 111 16. Dementia and delirium 117 17. Alcohol and substance-related
DISEASES AND DISORDERS 13. The mood (affective) disorders 99 14. The psychotic disorders: schizophrenia 105 15. The anxiety and somatoform disorders 111 16. Dementia and delirium 117 17. Alcohol and substance-related
Augmentation and Combination Strategies in Antidepressants treatment of Depression
 Augmentation and Combination Strategies in Antidepressants treatment of Depression Byung-Joo Ham, M.D. Department of Psychiatry Korea University College of Medicine Background The response rates reported
Augmentation and Combination Strategies in Antidepressants treatment of Depression Byung-Joo Ham, M.D. Department of Psychiatry Korea University College of Medicine Background The response rates reported
Class Update: Oral Antipsychotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Efficacy and Acceptability of Pharmacological Treatments for Post- Stroke Depression: A Bayesian Network Meta-Analysis
 Efficacy and Acceptability of Pharmacological Treatments for Post- Stroke Depression: A Bayesian Network Meta-Analysis Presenter: Miss Deng Tutor: Prof. Liu Ming Department of Neurology West China Hospital
Efficacy and Acceptability of Pharmacological Treatments for Post- Stroke Depression: A Bayesian Network Meta-Analysis Presenter: Miss Deng Tutor: Prof. Liu Ming Department of Neurology West China Hospital
Pharmacological Managment of Treatment Resistant Schizophrenia. Jean-Marie Batail - France 21 st July 2015
 Pharmacological Managment of Treatment Resistant Schizophrenia Jean-Marie Batail - France 21 st July 2015 Introduction A chronic and debilitating illness - Lifetime prevalence of around 0,7%. - Beginning
Pharmacological Managment of Treatment Resistant Schizophrenia Jean-Marie Batail - France 21 st July 2015 Introduction A chronic and debilitating illness - Lifetime prevalence of around 0,7%. - Beginning
Guidelines on Choice and Selection of Antidepressants for the Management of Depression
 Guidelines on Choice and Selection of Antidepressants for the Management of Depression 1. Introduction This guidance should be considered as part of a stepped care approach in the management of depressive
Guidelines on Choice and Selection of Antidepressants for the Management of Depression 1. Introduction This guidance should be considered as part of a stepped care approach in the management of depressive
Medications for Anxiety & Behavior in Williams Syndrome. Disclosure of Potential Conflicts. None 9/22/2016. Evaluation
 Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Medication management of anxiety & depression. Dr Katie Simpson GP Mental health lead East Berks CCG
 Medication management of anxiety & depression Dr Katie impson GP Mental health lead East Berks CCG NICE guidelines for Anxiety tepped Care RIs and NRIs in Anxiety disorders RI ertraline Citalopram Fluoxetine
Medication management of anxiety & depression Dr Katie impson GP Mental health lead East Berks CCG NICE guidelines for Anxiety tepped Care RIs and NRIs in Anxiety disorders RI ertraline Citalopram Fluoxetine
Scottish Medicines Consortium
 Scottish Medicines Consortium escitalopram, 5mg, 10mg, and 20mg tablets and 10mg/ml oral drops (Cipralex) No. (406/07) Lundbeck Ltd 7 September 2007 The Scottish Medicines Consortium has completed its
Scottish Medicines Consortium escitalopram, 5mg, 10mg, and 20mg tablets and 10mg/ml oral drops (Cipralex) No. (406/07) Lundbeck Ltd 7 September 2007 The Scottish Medicines Consortium has completed its
Guidelines on Choice and Selection of Antidepressants for the Management of Depression
 Working in partnership: Hertfordshire Partnership University NHS Foundation Trust East and North Hertfordshire Clinical Commissioning Group Herts Valleys Clinical Commissioning Group Guidelines on Choice
Working in partnership: Hertfordshire Partnership University NHS Foundation Trust East and North Hertfordshire Clinical Commissioning Group Herts Valleys Clinical Commissioning Group Guidelines on Choice
Mixing and Matching: Layering Medications as Family Physicians
 Mixing and Matching: Layering Medications as Family Physicians Family Medicine Forum Vancouver, B.C. November 9-12, 2016. Jon Davine, CCFP, FRCP(C) McMaster University Objectives Discuss different examples
Mixing and Matching: Layering Medications as Family Physicians Family Medicine Forum Vancouver, B.C. November 9-12, 2016. Jon Davine, CCFP, FRCP(C) McMaster University Objectives Discuss different examples
Diagnosis & Management of Major Depression: A Review of What s Old and New. Cerrone Cohen, MD
 Diagnosis & Management of Major Depression: A Review of What s Old and New Cerrone Cohen, MD Why You re Treating So Much Mental Health 59% of Psychiatrists Are Over the Age of 55 AAMC 2014 Physician specialty
Diagnosis & Management of Major Depression: A Review of What s Old and New Cerrone Cohen, MD Why You re Treating So Much Mental Health 59% of Psychiatrists Are Over the Age of 55 AAMC 2014 Physician specialty
Mr. E, age 37, has a 20-year history
 Antipsychotics for obsessive-compulsive disorder: Weighing risks vs benefits Taylor Modesitt, PharmD, Traci Turner, PharmD, BCPP, Lindsay Honaker, DO, Todd Jamrose, DO, Elizabeth Cunningham, DO, and Christopher
Antipsychotics for obsessive-compulsive disorder: Weighing risks vs benefits Taylor Modesitt, PharmD, Traci Turner, PharmD, BCPP, Lindsay Honaker, DO, Todd Jamrose, DO, Elizabeth Cunningham, DO, and Christopher
Pharmacogenetics of antidepressants and antipsychotics: the contribution of allelic variations to the phenotype of drug response
 (2004) 9, 442 473 & 2004 Nature Publishing Group All rights reserved 1359-4184/04 $25.00 www.nature.com/mp FEATURE REVIEW Pharmacogenetics of antidepressants and antipsychotics: the contribution of allelic
(2004) 9, 442 473 & 2004 Nature Publishing Group All rights reserved 1359-4184/04 $25.00 www.nature.com/mp FEATURE REVIEW Pharmacogenetics of antidepressants and antipsychotics: the contribution of allelic
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment
 Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
ETHNICITY AND PSYCHOTROPIC RESPONSE
 Ethnic Differences in Drug Metabolism ETHNICITY AND PSYCHOTROPIC RESPONSE Bridging Cultures: Improving Evaluation & Treatment of Cognitive 8 March 28 Keh-Ming Lin, M.D., M.P.H. Professor Emeritus of Psychiatry,
Ethnic Differences in Drug Metabolism ETHNICITY AND PSYCHOTROPIC RESPONSE Bridging Cultures: Improving Evaluation & Treatment of Cognitive 8 March 28 Keh-Ming Lin, M.D., M.P.H. Professor Emeritus of Psychiatry,
PRODUCT INFORMATION TEVATIAPINE XR (quetiapine fumarate)
") PRODUCT INFORMATION TEVATIAPINE XR (quetiapine fumarate) NAME OF THE MEDICINE Active ingredient: Quetiapine fumarate Chemical Name: Bis[2-(2-[4-(dibenzo[b,f][1,4]-thiazepin-11-yl)piperazin-1-yl] ethoxy)
PRODUCT INFORMATION TEVATIAPINE XR (quetiapine fumarate) NAME OF THE MEDICINE Active ingredient: Quetiapine fumarate Chemical Name: Bis[2-(2-[4-(dibenzo[b,f][1,4]-thiazepin-11-yl)piperazin-1-yl] ethoxy)
SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]
![SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]](/thumbs/80/80440271.jpg "SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]") SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003 Rationale The SiGMA algorithm
SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003 Rationale The SiGMA algorithm
Clinically Relevant Interactions between Newer Antidepressants and Second-Generation Antipsychotics
 University of Kentucky UKnowledge Psychiatry Faculty Publications Psychiatry 5-2014 Clinically Relevant Interactions between Newer Antidepressants and Second-Generation Antipsychotics Edoardo Spina University
University of Kentucky UKnowledge Psychiatry Faculty Publications Psychiatry 5-2014 Clinically Relevant Interactions between Newer Antidepressants and Second-Generation Antipsychotics Edoardo Spina University
Update on neurochemistry: Decision-making for Clinicians
 Update on neurochemistry: Decision-making for Clinicians Pierre Blier, MD, Ph.D Professor, Psychiatry and Cellular & Molecular Medicine University of Ottawa Endowed Chair and Director Mood Disorders Research
Update on neurochemistry: Decision-making for Clinicians Pierre Blier, MD, Ph.D Professor, Psychiatry and Cellular & Molecular Medicine University of Ottawa Endowed Chair and Director Mood Disorders Research
Volume 4; Number 5 May 2010
 Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
Treating treatment resistant depression
 Treating treatment resistant depression These slides are the intellectual property of Ian Anderson and must not be reproduced Ian Anderson Neuroscience and Psychiatry Unit University of Manchester and
Treating treatment resistant depression These slides are the intellectual property of Ian Anderson and must not be reproduced Ian Anderson Neuroscience and Psychiatry Unit University of Manchester and
Quetiapine Case 1 Warfarin Jose de Leon, MD
 Quetiapine Case 1 Warfarin 1-23-16 Jose de Leon, MD 1. Quetiapine Case 1 J Clin Psychopharm 1999;19:382-3 http://www.ncbi.nlm.nih.gov/pubmed/10440472 Educational Objectives At the conclusion of this presentation,
Quetiapine Case 1 Warfarin 1-23-16 Jose de Leon, MD 1. Quetiapine Case 1 J Clin Psychopharm 1999;19:382-3 http://www.ncbi.nlm.nih.gov/pubmed/10440472 Educational Objectives At the conclusion of this presentation,
I received help from Bosch Health Care
 John Kasckow, MD, PhD VA Pittsburgh Health Care System Western Psychiatric Institute and Clinic, UPMC VA Pittsburgh Health Care System I received help from Bosch Health Care 1 Diagnoses of Interest Early
John Kasckow, MD, PhD VA Pittsburgh Health Care System Western Psychiatric Institute and Clinic, UPMC VA Pittsburgh Health Care System I received help from Bosch Health Care 1 Diagnoses of Interest Early
Dr.Rahiminejad Roozbeh Hospital TUMS
 Dr.Rahiminejad Roozbeh Hospital TUMS Psychiatric disorders, particularly depression, anxiety and eating disorders, are prevalent in diabetes. Mental illness increases risk of diabetes and diabetic complications.
Dr.Rahiminejad Roozbeh Hospital TUMS Psychiatric disorders, particularly depression, anxiety and eating disorders, are prevalent in diabetes. Mental illness increases risk of diabetes and diabetic complications.
PEER REVIEW HISTORY ARTICLE DETAILS VERSION 1 - REVIEW
 PEER REVIEW HISTORY BMJ Open publishes all reviews undertaken for accepted manuscripts. Reviewers are asked to complete a checklist review form (see an example) and are provided with free text boxes to
PEER REVIEW HISTORY BMJ Open publishes all reviews undertaken for accepted manuscripts. Reviewers are asked to complete a checklist review form (see an example) and are provided with free text boxes to
UnitedHealthcare Community (UHCCP) Louisiana Clinical Program Guidelines Record Supplemental Tool
 Louisiana Clinical Program Guidelines Record Supplemental Tool") December-18 UnitedHealthcare Community (UHCCP) Louisiana Clinical Program Guidelines Record Supplemental Tool Facility Name: Primary Dx: Member Gender: Member Age: Reviewer Name: Date of Facility Review:
December-18 UnitedHealthcare Community (UHCCP) Louisiana Clinical Program Guidelines Record Supplemental Tool Facility Name: Primary Dx: Member Gender: Member Age: Reviewer Name: Date of Facility Review:
Index. Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) b-adrenergic blockers
 b-adrenergic blockers") Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
POLYPHARMACY : FOR AND AGAINST NZMA GP CONFERENCE 2012 PSYCHOPHARMACOLOGY SERIES. Guna Kanniah Waikato Hospital
 POLYPHARMACY : FOR AND AGAINST NZMA GP CONFERENCE 212 PSYCHOPHARMACOLOGY SERIES Guna Kanniah Waikato Hospital POLYPHARMACY FIVE REASONS FOR POLYPHARMACY 1. To treat a concomitant disorder 2. To treat an
POLYPHARMACY : FOR AND AGAINST NZMA GP CONFERENCE 212 PSYCHOPHARMACOLOGY SERIES Guna Kanniah Waikato Hospital POLYPHARMACY FIVE REASONS FOR POLYPHARMACY 1. To treat a concomitant disorder 2. To treat an
Objectives. Objectives. A practice review. 02-Nov-16 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS
 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
PORT, 2009 Spain, 2009 Malaysia, 2009 Singapore, 2009 BAP, 2011 WFSBP, 2012 SIGN, 2013 Harvard NICE RANZCP, 2016
 Appendix 3. Comparison of recommendations from clinical practice guidelines. Data extracted in relation to key health questions that are relevant to a clinician adopting an algorithmic approach to the
Appendix 3. Comparison of recommendations from clinical practice guidelines. Data extracted in relation to key health questions that are relevant to a clinician adopting an algorithmic approach to the
FL Medicaid Drug Therapy Management Program for Behavioral Health Monitoring for Safety and Quality
 FL Medicaid Drug Therapy Management Program for Behavioral Health Monitoring for Safety and Quality April 23, 2014 Pensacola, FL Presentation Objectives To briefly describe the program and how its components
FL Medicaid Drug Therapy Management Program for Behavioral Health Monitoring for Safety and Quality April 23, 2014 Pensacola, FL Presentation Objectives To briefly describe the program and how its components
Your footnote
 MANIA Your footnote Your footnote Cipriani A, Barbui C, Salanti G et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis. The Lancet 2011;
MANIA Your footnote Your footnote Cipriani A, Barbui C, Salanti G et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis. The Lancet 2011;
Antidepressant Treatment of Depression
 Antidepressant Treatment of Depression PLEASE REFER TO INTEGRATED CARE PATHWAY FOR INFORMATION RELATING TO THE OVERALL MANAGEMENT OF DEPRESSION SSRI s are first choice agents because they are as effective
Antidepressant Treatment of Depression PLEASE REFER TO INTEGRATED CARE PATHWAY FOR INFORMATION RELATING TO THE OVERALL MANAGEMENT OF DEPRESSION SSRI s are first choice agents because they are as effective
Department of Psychiatry & Behavioral Sciences. University of Texas Medical Branch
 Depression in Childhood: Advances and Controversies in Treatment Karen Dineen Wagner, MD, PhD Marie B. Gale Centennial Professor & Vice Chair Department of Psychiatry & Behavioral Sciences Director, Division
Depression in Childhood: Advances and Controversies in Treatment Karen Dineen Wagner, MD, PhD Marie B. Gale Centennial Professor & Vice Chair Department of Psychiatry & Behavioral Sciences Director, Division
Source of effectiveness data The effectiveness evidence was derived from published studies and from experts' opinions.
 Analisis coste-efectividad de olanzapina frente a haloperidol en el tratamiento de la esquizofrenia en Espana [Cost effectiveness analysis of olanzapine versus haloperidol in the treatment of schizophrenia
Analisis coste-efectividad de olanzapina frente a haloperidol en el tratamiento de la esquizofrenia en Espana [Cost effectiveness analysis of olanzapine versus haloperidol in the treatment of schizophrenia
QUEPINE XR PRODUCT INFORMATION. Name of the medicine. Description. Pharmacology
 QUEPINE XR PRODUCT INFORMATION Name of the medicine Quetiapine fumarate. The chemical name is Bis[2-(2-[4-(dibenzo[b,f][1,4]-thiazepin-11-yl)piperazin- 1-yl] ethoxy) ethanol] fumarate. Its structural formula
QUEPINE XR PRODUCT INFORMATION Name of the medicine Quetiapine fumarate. The chemical name is Bis[2-(2-[4-(dibenzo[b,f][1,4]-thiazepin-11-yl)piperazin- 1-yl] ethoxy) ethanol] fumarate. Its structural formula
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
Quetiapine Case 2 Therapeutic Drug Monitoring Jose de Leon, MD
 Quetiapine Case 2 Therapeutic Drug Monitoring 1-27-16 Jose de Leon, MD 2. Quetiapine Case Therapeutic Drug Monitoring (unpublished) Educational Objectives At the conclusion of this presentation, the participant
Quetiapine Case 2 Therapeutic Drug Monitoring 1-27-16 Jose de Leon, MD 2. Quetiapine Case Therapeutic Drug Monitoring (unpublished) Educational Objectives At the conclusion of this presentation, the participant
Treatment-resistant depression in primary care
 Treatment-resistant depression in primary care Interprofessional CME, October 2017 Brian J. Mickey, MD, PhD Associate Professor School of Medicine Department of Psychiatry Disclosures Speakers bureau:
Treatment-resistant depression in primary care Interprofessional CME, October 2017 Brian J. Mickey, MD, PhD Associate Professor School of Medicine Department of Psychiatry Disclosures Speakers bureau:
5 COMMON QUESTIONS WHEN TREATING DEPRESSION
 5 COMMON QUESTIONS WHEN TREATING DEPRESSION Do Antidepressants Increase the Possibility of Suicide? Will I Accidentally Induce Mania if I Prescribe an SSRI? Are Depression Medications Safe and Effective
5 COMMON QUESTIONS WHEN TREATING DEPRESSION Do Antidepressants Increase the Possibility of Suicide? Will I Accidentally Induce Mania if I Prescribe an SSRI? Are Depression Medications Safe and Effective
Optimal Use of Antidepressants: Focusing on SNRI, NDRI and SSRE
 Optimal Use of Antidepressants: Focusing on SNRI, NDRI and SSRE Chan-Hyung Kim, MD Severance Mental Health Hospital Institute of Behavioral Science in Medicine Diagnostic Criteria Pyramid Etiologic Pathophysiologic
Optimal Use of Antidepressants: Focusing on SNRI, NDRI and SSRE Chan-Hyung Kim, MD Severance Mental Health Hospital Institute of Behavioral Science in Medicine Diagnostic Criteria Pyramid Etiologic Pathophysiologic
Canterbury District Health Board Endocrine Test Centre Protocols. Date Signature Next review Sign when read
 0855 Prolactin Series test ASY-855.1: Associated documents Prolactin Series Test Patient information sheet Prolactin series sample request form 0 ASY-855.2: Distribution of Documents Copy No Number Location
0855 Prolactin Series test ASY-855.1: Associated documents Prolactin Series Test Patient information sheet Prolactin series sample request form 0 ASY-855.2: Distribution of Documents Copy No Number Location
Antidepressant Medication Strategies We ve Come a Long Way or Have We? Who Writes Prescriptions for Psychotropic Medications. Biological Psychiatry
 Antidepressant Medication Strategies We ve Come a Long Way or Have We? Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free
Antidepressant Medication Strategies We ve Come a Long Way or Have We? Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free
ALAMEDA COUNTY BEHAVIORAL HEALTH CARE SERVICES MEDICATION FORMULARY
 ANTIDEPRESSANTS Serotonin Selective Reuptake Inhibitors citalopram 10, 20, 40 mg, 10 mg/5cc $ 0.40 No escitalopram 10, 20 mg $ 2.60 Yes fluoxetine 10, 20 mg, 20 mg/5 ml $ 0.40 Yes fluvoxamine 25, 50, 100
ANTIDEPRESSANTS Serotonin Selective Reuptake Inhibitors citalopram 10, 20, 40 mg, 10 mg/5cc $ 0.40 No escitalopram 10, 20 mg $ 2.60 Yes fluoxetine 10, 20 mg, 20 mg/5 ml $ 0.40 Yes fluvoxamine 25, 50, 100
Perinatal Mental Health: Prescribing Guidance for Trust Prescribers and GPs
 Perinatal Mental Health: Prescribing Guidance for Trust Prescribers and GPs (Version 3 January 2015) Principal Author: Dr Jenny Cooke Consultant Psychiatrist, Brighton & Hove Perinatal Mental Health Service
Perinatal Mental Health: Prescribing Guidance for Trust Prescribers and GPs (Version 3 January 2015) Principal Author: Dr Jenny Cooke Consultant Psychiatrist, Brighton & Hove Perinatal Mental Health Service
Common Antidepressant Medications for Adults
 (and Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac) Fluoxetine Weekly (Prozac Weekly) 20 in AM w/ food (10 mg in elderly or those w/ panic disorder) 20 40 40 (If age >60yo, max 20) 10 10
(and Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac) Fluoxetine Weekly (Prozac Weekly) 20 in AM w/ food (10 mg in elderly or those w/ panic disorder) 20 40 40 (If age >60yo, max 20) 10 10
HEDIS BEHAVIORAL HEALTH RESOURCE GUIDE
 HEDIS BEHAVIORAL HEALTH RESOURCE GUIDE What is HEDIS? 3 HEDIS Reference Guide for Behavioral Health 4 Behavioral Health HEDIS Measures 13 WHAT IS HEDIS? HEDIS (Healthcare Effectiveness Data and Information
HEDIS BEHAVIORAL HEALTH RESOURCE GUIDE What is HEDIS? 3 HEDIS Reference Guide for Behavioral Health 4 Behavioral Health HEDIS Measures 13 WHAT IS HEDIS? HEDIS (Healthcare Effectiveness Data and Information
1 1 Evidence-based pharmacotherapy of major depressive disorder. Michael J. Ostacher, Jeffrey Huffman, Roy Perlis, and Andrew A.
 1 1 Evidence-based pharmacotherapy of major depressive disorder Michael J. Ostacher, Jeffrey Huffman, Roy Perlis, and Andrew A. Nierenberg Massachusetts General Hospital and Harvard University, Boston,
1 1 Evidence-based pharmacotherapy of major depressive disorder Michael J. Ostacher, Jeffrey Huffman, Roy Perlis, and Andrew A. Nierenberg Massachusetts General Hospital and Harvard University, Boston,
Manual of Clinical Psychopharmacology
 Manual of Clinical Psychopharmacology Fourth Edition Alan F. Schatzberg, M.D. Kenneth T. Norris, Jr., Professor and Chairman, Department of Psychiatry and Behavioral Sciences, Stanford University School
Manual of Clinical Psychopharmacology Fourth Edition Alan F. Schatzberg, M.D. Kenneth T. Norris, Jr., Professor and Chairman, Department of Psychiatry and Behavioral Sciences, Stanford University School
CME. Pharmacotherapy of Depression in Older Adults. Introduction. Major Depression
 CME Pharmacotherapy of Depression in Older Adults This CME learning activity is available at www.geriatricsandaging.ca/cme_page.htm. Participating physicians are entitled to one () MAINPRO-M credit by
CME Pharmacotherapy of Depression in Older Adults This CME learning activity is available at www.geriatricsandaging.ca/cme_page.htm. Participating physicians are entitled to one () MAINPRO-M credit by
Children s Hospital Of Wisconsin
 Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Index. Bulimia, 13 Bupropion, 12, 51 Buspirone, 81
 Index A α-adrenergic blockade, 55 Ablative neurosurgery, 83 Activity scheduling, 61 Acupuncture, 64, 69 71 Alcohol, 7, 13 Alprazolam, 50 Amfebutamone, 52 Amitriptyline, 34 Anhedonia, 13, 17, 18 Anterior
Index A α-adrenergic blockade, 55 Ablative neurosurgery, 83 Activity scheduling, 61 Acupuncture, 64, 69 71 Alcohol, 7, 13 Alprazolam, 50 Amfebutamone, 52 Amitriptyline, 34 Anhedonia, 13, 17, 18 Anterior
Evidence-Based, Pharmacological Treatment Guideline for Depression in Korea, Revised Edition
 SPECIAL ARTICLE Psychiatry & Psychology http://dx.doi.org/10.3346/jkms.2014.29.4.468 J Korean Med Sci 2014; 29: 468-484 -Based, Pharmacological Treatment Guideline for Depression in Korea, Revised Edition
SPECIAL ARTICLE Psychiatry & Psychology http://dx.doi.org/10.3346/jkms.2014.29.4.468 J Korean Med Sci 2014; 29: 468-484 -Based, Pharmacological Treatment Guideline for Depression in Korea, Revised Edition
Guilt Suicidality. Depression Co-Occurs with Medical Illness The rate of major depression among those with medical illness is significant.
 1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
Effective Health Care Program
 Comparative Effectiveness Review Number 43 Effective Health Care Program Off-Label Use of Atypical Antipsychotics: An Update Executive Summary Background Antipsychotics medications are approved by the
Comparative Effectiveness Review Number 43 Effective Health Care Program Off-Label Use of Atypical Antipsychotics: An Update Executive Summary Background Antipsychotics medications are approved by the
Depression. University of Illinois at Chicago College of Nursing
 Depression University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Recognize depression, its symptoms and behaviors
Depression University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Recognize depression, its symptoms and behaviors
PSYCHIATRIC MANAGEMENT IN PRIMARY CARE. Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust
 Mersey Care NHS Trust") PSYCHIATRIC MANAGEMENT IN PRIMARY CARE Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust Areas to cover Mood Disorders Anxiety Disorders Miscellaneous Conditions
PSYCHIATRIC MANAGEMENT IN PRIMARY CARE Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust Areas to cover Mood Disorders Anxiety Disorders Miscellaneous Conditions
Role of Clozapine in Treatment-Resistant Schizophrenia
 Disease Management and Treatment Strategies Elkis H, Meltzer HY (eds): Therapy-Resistant Schizophrenia. Adv Biol Psychiatry. Basel, Karger, 2010, vol 26, pp 114 128 Role of Clozapine in Treatment-Resistant
Disease Management and Treatment Strategies Elkis H, Meltzer HY (eds): Therapy-Resistant Schizophrenia. Adv Biol Psychiatry. Basel, Karger, 2010, vol 26, pp 114 128 Role of Clozapine in Treatment-Resistant
Comorbid Conditions and Antipsychotic Use in Patients with Depression
 Comorbid Conditions and Antipsychotic Use in Patients with Depression Thomas W. Heinrich, MD Professor of Psychiatry and Family Medicine Director, Division of Consultation-Liaison Psychiatry Medical College
Comorbid Conditions and Antipsychotic Use in Patients with Depression Thomas W. Heinrich, MD Professor of Psychiatry and Family Medicine Director, Division of Consultation-Liaison Psychiatry Medical College
Pharmacological treatment for obsessive compulsive disorder
 Freeston M H, Ladouceur R, Gagnon F et al. Cognitive-behavioral treatment of obsessive thoughts: a controlled study. J Consult Clin Psychol 997; 65: 405 3. Meyer V. Modification of expectations in cases
Freeston M H, Ladouceur R, Gagnon F et al. Cognitive-behavioral treatment of obsessive thoughts: a controlled study. J Consult Clin Psychol 997; 65: 405 3. Meyer V. Modification of expectations in cases
How to treat depression with medication: Some rules of thumb
 How to treat depression with medication: Some rules of thumb R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon. Consultant Psychiatrist Regional
How to treat depression with medication: Some rules of thumb R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon. Consultant Psychiatrist Regional
APO-QUETIAPINE XR. quetiapine fumarate PRODUCT INFORMATION
 APO-QUETIAPINE XR quetiapine fumarate PRODUCT INFORMATION NAME OF THE MEDICINE Quetiapine fumarate Chemical Name: Bis[2-(2-[4-(dibenzo[b,f][1,4]-thiazepin-11-yl)piperazin-1-yl] ethoxy) ethanol] fumarate.
APO-QUETIAPINE XR quetiapine fumarate PRODUCT INFORMATION NAME OF THE MEDICINE Quetiapine fumarate Chemical Name: Bis[2-(2-[4-(dibenzo[b,f][1,4]-thiazepin-11-yl)piperazin-1-yl] ethoxy) ethanol] fumarate.
Effective Health Care
 Number 7 Effective Health Care Comparative Effectiveness of Second- Generation Antidepressants in the Pharmacologic Treatment of Adult Depression Executive Summary Background Depressive disorders such
Number 7 Effective Health Care Comparative Effectiveness of Second- Generation Antidepressants in the Pharmacologic Treatment of Adult Depression Executive Summary Background Depressive disorders such
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 in children and young people: recognition, detection, risk profiling and NICE Pathways bring together everything NICE says on a topic in an interactive flowchart. NICE Pathways are interactive and designed
in children and young people: recognition, detection, risk profiling and NICE Pathways bring together everything NICE says on a topic in an interactive flowchart. NICE Pathways are interactive and designed
MEDICATION ALGORITHM FOR ANXIETY DISORDERS
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
PRESCRIBING GUIDELINES
 The Maudsley The South London and Maudsley NHS Foundation Trust & Oxleas NHS Foundation Trust PRESCRIBING GUIDELINES 10th Edition David Taylor Carol Paton Shitij Kapur informa healthcare Contents Authors
The Maudsley The South London and Maudsley NHS Foundation Trust & Oxleas NHS Foundation Trust PRESCRIBING GUIDELINES 10th Edition David Taylor Carol Paton Shitij Kapur informa healthcare Contents Authors
for anxious and avoidant behaviors.
 Summary of the Literature on the Treatment of Anxiety Disorders in Children and Adolescents Sucheta D. Connolly, M.D.* Non-OCD anxiety disorders in youth are common and disabling, with 12-month prevalence
Summary of the Literature on the Treatment of Anxiety Disorders in Children and Adolescents Sucheta D. Connolly, M.D.* Non-OCD anxiety disorders in youth are common and disabling, with 12-month prevalence