Running head: ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 1
|
|
|
- Brendan Summers
- 6 years ago
- Views:
Transcription
1 Running head: ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 1 Antipsychotic Medication-Associated Weight Gain: Development of an Evidence-Based Management Algorithm and Practice Guideline for Primary Care Providers Tracy E. Thornett University of Hawaii at Hilo-School of Nursing June 11, 2015 Committee Chair: Alice Davis Committee Member: Cecilia Mukai
2 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 2 Abstract Obesity is a growing public health concern. Although people from all walks of life are affected by obesity, rates of this chronic disease are especially high among individuals with mental illness. Of particular concern are patients who take antipsychotic medications, as weight gain is a well-established side effect of many of these drugs. This practice inquiry project investigated the problem of antipsychotic medication-associated weight gain by applying the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) methodology to develop a preliminary evidence-based practice guideline and algorithm for use by primary care providers. As part of the project, an interdisciplinary panel of key stakeholders evaluated the proposed guideline for both quality and applicability. The results of this evaluation are discussed with future revision and expansion of the guideline in mind. Additionally, implications for advanced nursing practice are examined and strategies for promoting safe, effective, patientcentered, and equitable health care are suggested.
3 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 3 Table of Contents Chapter Problem Statement Support for the Problem..7 Project Purpose...8 Objectives and Aims Chapter 2.10 Review of Literature Theoretical and Conceptual Foundation Chapter Project Design...31 Facilities and Resources.31 Study Population and Setting Key Questions Interventions.. 32 Comparison...33 Outcomes...33 Evidence Search Strategy.33 Data Extraction and Quality Assessment..34 Data Synthesis and Analysis 34 Evaluation..35 Human Subjects and Ethics...36 Chapter Part 1: Systematic Review and Clinical Practice Guideline.37
4 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 4 Part 2: Guideline Evaluation Chapter Purpose, Aims, and Objectives..44 The Guideline. 45 Project Facilitators.46 Project Barriers..46 Project Limitations Plan for Revision...48 Chapter Relevance to Advanced Nursing Practice..49 Contributions to Practice Future Projects...53 References 54 Appendices 87 Appendix A: List of Second-Generation Antipsychotics Appendix B: Summary of GRADE Approach to Rating Importance of Outcomes...88 Appendix C: Summary of GRADE Approach to Rating Quality. 89 Appendix D: Risk of Bias Summaries..90 Appendix E: Forest Plots According to Interventions and Outcomes.. 92 Appendix F: Summary of the Determinants of Strength of Recommendations...96 Appendix G: Summary of AGREE II Instrument Questions Appendix H: Consent Form for Guideline Evaluators...98 Appendix I: Institutional Review Board Approval Letter....99
5 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 5 Appendix J: Summary of Database Findings..100 Appendix K: Characteristics of Excluded Studies..103 Appendix L: Characteristics of Included Studies Appendix M: Summary of AGREE II Evaluation Data.126 Appendix N: Permissions to Reproduce Copyrighted Materials Appendix O: Clinical Practice Guideline...146
6 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 6 Chapter 1: Statement of the Problem Obesity is a growing social and public health concern in the United States and globally. The Centers for Disease Control and Prevention (CDC) report that as of 2010, more than onethird (35.7%) of U.S. adults were obese and this rate has increased since 1988 in adults of all income and education levels. Furthermore, it is reported that in the same year 17% of children between the ages of 2 and 19 years were obese, which is triple the rate observed in 1980 (CDC, 2013). These findings suggest that the rates of obesity will continue to increase. As such, the rising prevalence of obesity has prompted calls from researchers, journalists, policy makers, corporations, healthcare professionals, and independent organizations to advocate for increased efforts to both manage and prevent obesity. Although there is significant concern about the prevalence of obesity in the general population, obesity rates are alarmingly high among individuals diagnosed with a mental illness. For example, the prevalence rate of obesity in patients with schizophrenia is estimated to be 1.5 to 4 times higher than that of the general population (Mukundan, Faulkner, Cohn, & Remington, 2010; Reynolds & Kirk, 2010). Similarly, the prevalence of metabolic syndrome (a combination of risk factors including central adiposity, elevated triglycerides, decreased HDL cholesterol, hypertension, and glucose intolerance) among schizophrenics is approximately 40%, or twice that of the general population (Maayan & Correll, 2010; Reynolds & Kirk, 2010). Of particular concern is a subpopulation of adults who take antipsychotic medications. In fact, weight gain is an established, predictable side effect of second-generation antipsychotic (SGA) medications (Usher, Park, & Foster, 2013), with as many as three-quarters of patients receiving an antipsychotic medication experiencing a baseline weight increase of more than 7% (Wu et al., 2008). Weight gain, as a side effect, poses a special problem in this population, not only in
7 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 7 regard to medication adherence, but also because obesity is associated with numerous medical, psychological, social, and economic consequences. Given the increased prevalence of obesity among individuals diagnosed with mental illness, along with their elevated vulnerability to medication-induced weight gain, one important area of inquiry for successful weight management in this population is the identification of effective interventions which are specific to antipsychotic-associated weight gain. This project investigated antipsychotic-associated weight gain within the context of the obesity epidemic and examined potential solutions for preventing and/or intervening to reduce this side effect. Effective solutions for antipsychotic-associated weight gain will help to promote medication adherence among the mentally ill, prevent relapse, improve physical health and related quality of life, and ultimately, improve treatment outcomes for this vulnerable population. Problem Statement Growing concerns about the prevalence and consequences of obesity require clinicians to tailor obesity prevention and treatment strategies to known causes of weight gain. SGAs have weight gain as an established common side effect. This medication side effect poses a special problem for patients with mental illness, who already experience significant health disparities and substantial barriers to medication adherence. Support for the Problem Adults diagnosed with severe mental illness (SMI) experience substantial health disparities compared to the overall population. For example, up to 60% of patients with SMI are obese (White, Elmore, Luthin, & Cates, 2013), compared to approximately 36% of the overall U.S. population (CDC, 2013). Additionally, adults with SMI have higher rates of conditions such as dyslipidemias, metabolic syndrome, hypertension, and type 2 diabetes mellitus, which
8 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 8 ultimately result in shorter life spans and increased mortality (White, et al., 2013). Unfortunately, many of the medications used to treat SMI (particularly SGAs) have adverse effects that include problematic metabolic changes and associated weight gain. These medication effects compound the already significant health disparities experienced by individuals with SMI. Given these challenges, there is a need for clear guidelines that help to address the physical consequences of antipsychotic therapy, particularly those related to weight gain. Project Purpose The purpose of this project was to develop evidence-based practice recommendations for the management of antipsychotic-associated weight gain in adults. In order to develop such practice recommendations, research questions were designed that focus on the elements of the clinical problem that are of the greatest interest and concern. A standard method was used to design effective research questions, namely, the PICO approach. PICO stands for Population, Intervention, Comparison, and Outcomes. Additionally, a time element (Time) may be added to the question by the researcher to add greater precision (Moran, 2014). The following PICO questions were used to guide the literature review in order to generate practice recommendations based upon the best possible evidence: 1. In adults taking second-generation antipsychotic medication (P), how does medication switching (I) compare to standard care (C) for decreasing weight (O)? 2. In adults taking second-generation antipsychotic medication (P), how do pharmacological interventions (I) compare to standard care (C) for decreasing weight (O)?
9 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 9 3. In adults taking second-generation antipsychotic medication (P), how do behavioral interventions (I) compare to standard care (C) for decreasing weight (O)? Objectives and Aims There were two primary aims of this project. The first aim was to improve the care and treatment of adults with SMI by effectively addressing population-specific physical health concerns by developing evidence-based recommendations that will assist primary care providers in the management of antipsychotic-associated weight gain. Objectives for achieving this aim included: 1. Conduct a structured literature review investigating interventions for managing antipsychotic-associated weight gain. 2. Analyze the literature to both grade and compare interventions. 3. Determine best practice recommendations for the management of weight gain in adults taking antipsychotic medications. The second aim of the project was to promote the translation of new knowledge into health care practice by achieving the following objectives: 4. Synthesize findings into an evidence-based algorithm and guideline for managing antipsychotic-associated weight gain in the primary care setting. 5. Discuss the relevance of medication-associated weight gain to advanced nursing practice. 6. Suggest strategies for advanced nursing practice that promote the Institute of Medicine s (IOM) aims for quality care, specifically those relating to the safe, effective, and equitable care of patients.
10 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 10 Chapter 2: Project Description Review of Literature The review of literature begins with a general overview of obesity and a synopsis of the current state of knowledge regarding the causes of obesity. It then follows with an overview of antipsychotics, a discussion of the current knowledge surrounding antipsychotic-associated weight gain and proposed mechanisms of action, a review of the consequences of weight gain, and a summary of recent trends in antipsychotic prescribing. Finally, the section concludes with a description of the current interventions used in the management of antipsychotic-associated weight gain, along with specific examples to illustrate each intervention strategy. Prevalence and Costs of Overweight and Obesity The CDC reports that as of 2010, more than one-third (35.7%) of U.S. adults were obese and that this rate has increased since 1988 in adults of all income and education levels. Furthermore, they report that 17% of children between the ages of 2 and 19 years were obese and that this is triple the rate observed in 1980 (CDC, 2013). Medical expenditures related to obesity were estimated to be $75 billion in 2003 (Donohoe, 2008). Others have suggested that obesity accounts for 6 to 7 percent of overall healthcare expenditures and costs as much as $100 billion annually in the United States (Tai- Seale & Chandler, 2003). More recently, the CDC estimated the cost of obesity in the U.S in 2008 was $147 billion. Furthermore, the CDC determined that medical costs for obese individuals were $1,429 higher than for people of normal weight (CDC, 2013). Obesity Knowledge Obesity is defined by a standard medical text as a state of excess adipose tissue mass, (Flier & Maratos-Flier, 2008, p. 462). While this is often equated with increased body weight,
11 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 11 there are clear problems with this approach, as evidenced by muscular athletes who may weigh more, but are also very lean. Furthermore, because human weights exist on a continuum, the authors of the same text concede that designating a line between lean or obese is somewhat arbitrary, (p. 462). The authors point out that the Body Mass Index (BMI), which is equal to weight divided by height squared in kg/m 2, is the most commonly used method to define obesity. They admit, however, that BMI is still not a direct measure of adiposity and further acknowledge that while obesity is associated with a number of clinically relevant problems (such as insulin resistance, diabetes, hypertension, and hyperlipidemia), the underlying mechanism for this association has still not been identified. Despite these limitations, BMI is still the most ubiquitous measure of obesity in the research literature, and as such, discussion about obesity must be confined to this primary parameter. Within these guidelines, overweight is medically defined as a BMI between 25 and 30, while obesity is defined as a BMI greater than 30 (Flier & Maratos-Flier, 2008). Obesity causes. The causes of obesity are complex and multifactorial. Generally, obesity is attributed to an overall positive energy balance, with individuals consuming too much food (increased caloric intake) and engaging in too little physical exercise (decreased caloric expenditure). In other words, too many calories in, plus too few calories out, equals weight gain. While there is little doubt about the physics of this energy balance axiom, several mechanisms contribute both to the behaviors that promote obesity, and to the biological mechanisms that affect the storage and metabolism of fat. Factors known to affect the behaviors associated with obesity include chronic stress (McEwen, 2008), mental illness (Taylor et al., 2012), low socioeconomic status (Ernsberger & Koletsky, 1999), low educational attainment (Befort, Nazir, & Perri, 2012; Braveman, Cubbin,
12 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 12 Egerter, Williams & Pamuk, 2010; Roskam, et al., 2010), social and cultural norms (Williams, Crockett, Harrison, & Thomas, 2012), the built environment, such as sidewalks and neighborhood parks (Wen & Kowaleski-Jones, 2012), geographic residency, such as urban or rural location (Befort et al., 2012; Tai-Seale & Chandler, 2003), food marketing (Williams et al., 2012), food availability (Larson, Story, & Nelson, 2009), food insecurity (Pan, Sherry, Njai, & Blanck, 2012), and lifestyle preferences. Factors known to affect the biological storage and metabolism of fat include chronic stress (McEwen, 2008), genetics and epigenetics (Speakman & O'Rahilly, 2012), the environment in utero (Lillycrop & Burdge, 2011), medical disorders (CDC, 2013), injury (Selassie, Snipe, Focht & Welldaregay, 2013), gut microbes (Jumpertz et al., 2011; Ley, Turnbaugh, Klein, & Gordon, 2006; Lomangino, 2006; Ridaura, et al., 2013), environmental chemicals (Grün & Blumberg, 2009; Thayer, Heindel, Bucher & Gallo, 2012), and medications (Grün & Blumberg, 2009). In particular, numerous studies have demonstrated that antipsychotic medications promote significant weight gain leading to obesity (Maayan & Correll, 2010; Mukundan et al., 2010; Reynolds & Kirk, 2010). Overview of Antipsychotics Introduced in the 1950 s, chlorpromazine was recognized as being the first medication to effectively treat the psychotic symptoms of schizophrenia, such as hallucinations and delusions. Numerous antipsychotics were subsequently developed which have similar mechanisms of action, however, all of these medications were (and still are) commonly associated with the adverse effects of elevated prolactin and extrapyramidal symptoms (EPS) such as Parkinsonism and tardive dyskinesia. Additionally, these first-generation medications were limited in their efficacy for treating the full range of symptoms in schizophrenia. In the 1970 s, clozapine was
13 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 13 developed as the first atypical antipsychotic, otherwise known a second-generation antipsychotic (SGA). These SGAs showed greater efficacy in reducing psychotic symptoms and markedly reduced risk for neurological side effects. Unfortunately, most of these SGAs have their own adverse effects, including metabolic changes such as glucose intolerance and hyperlipidemia, as well as substantial medication-induced weight gain (Ballon, Pajvani, Freyberg, Leibel, & Lieberman, 2014; Lett et al., 2011). Despite these effects, SGAs are now considered the standard-of-care in schizophrenia, due to their improved tolerability over first-generation antipsychotics. Additionally, SGAs are now increasingly being used as adjunctive therapies for mood disorders such as depression and bipolar disorder (Ballon et al., 2014; Maayan & Correll, 2010). Antipsychotics and Weight gain As noted previously, SGAs are currently the primary treatment for schizophrenia (Mukundan et al., 2010) and are often used as an adjunct treatment in many other psychiatric disorders (Maayan & Correll, 2010). Unfortunately, this class of drugs also has well-known side effects that include weight gain and metabolic disturbance (Maayan & Correll, 2010; Mukundan et al., 2010; Reynolds & Kirk, 2010). It appears, however, that the magnitude of weight gain varies according to specific drugs, with some medications having greater risk potential than others (De Hert, 2012; Maayan & Correll, 2010; Mukundan et al., 2010; Usher, Park, Foster, & Buettner, 2012). For example, one recent meta-analysis concluded that nearly every antipsychotic had some degree of associated weight gain after only 10 weeks of treatment. The greatest weight increase was seen with olanzapine and clozapine, which increased body weight by 9 to 10 lbs (4-4.5 kg) on average after only 10 weeks of treatment (Mukundan et al., 2010). Another study demonstrated that there are relative differences in antipsychotic-associated weight
14 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 14 gain in the first 10 weeks of treatment for SGAs with the following findings: Clozapine, 4.45 kg; Olanzapine, 4.15 kg; Risperidone, 2.10 kg; and Ziprasidone, 0.04 kg (Usher et al., 2012). Furthermore, this adverse effect is quite common, with one study demonstrating marked weight gain of at least 7% body weight after one year of treatment in 86% of patients taking olanzapine, 65% of patients taking quetiapine, and 63% of patients taking amisulpride (Maayan & Correll, 2010). Another study demonstrated that this effect is even greater in adolescents, with 90.5% of patients gaining >7% of their baseline body weight after taking olanzapine for only 12 weeks (Maayan & Correll, 2010). Overall, weight gain is estimated to affect between 15%-72% of patients taking antipsychotics (De Hert, 2012). In addition to concerns about weight gain, one study reported that patients taking antipsychotics had a quadrupled incidence of diabetes and a doubled incidence of hypertension compared to those in control groups (Lett et al., 2011). Both of these conditions are known to be associated with obesity, and it is not entirely clear whether this increased incidence is due to obesity, the stress associated with having a severe mental illness, or to the use of the antipsychotic medications themselves. Finally, another recent meta-analysis investigating newer antipsychotic agents (including asenapine, iloperidone, lurasidone, and paliperidone) was unable to reach any strong conclusions regarding the metabolic effects of these newer medications, but results suggest that lurasidone has the lowest weight gain potential of the group (De Hert, 2012). These newer SGAs have yet to be integrated into the current knowledge of antipsychoticassociated weight gain. Mechanisms of Antipsychotic-Associated Weight Gain In contrast to first generation antipsychotics which are more specific to and have greater affinity for D2 receptors, SGAs have a strong affinity for 5-HT2 receptors as well as affinities for
15 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 15 dopaminergic, muscarinic, histaminergic, and adrenergic receptors. In particular, increased risk of metabolic abnormalities has been associated with the 5-HT2c- and H1 blocking activity of second-generation antipsychotics (Lett et al., 2011; Reynolds & Kirk, 2010). Despite these associations, the physiologic mechanism of antipsychotic-induced weight gain is not well understood and is most likely due to a myriad of factors including appetite stimulation, direct impairment of metabolic regulation, alteration of insulin sensitivity, and sedation leading to decreased physical activity (Maayan & Correll, 2010; Wu et al., 2008). In addition, genetics may be one of the strongest risk factors influencing antipsychotic-associated weight gain, as demonstrated by recent twin and sibling studies. These studies conclude that 60-80% of antipsychotic-induced weight gain is contributed by genetic factors (Gebhardt et al., 2010; Lett et al., 2011). Lett et al. (2011) note, however, that heritable causes of antipsychotic-associated weight gain are likely to be polygenic, with approximately 60 important genes related to antipsychotic-induced weight gain currently being investigated, especially the genes HTR2C and DRD2. Gene variants with susceptibility to antipsychotic influence include pathways involving intracellular signaling via G-protein coupled receptors, intercellular synaptic signaling, appetite regulators (such as leptin, neuropeptide Y, pro-melanin-concentrating hormone, ghrelin, and endocannabinoids), lipid metabolism, and proinflammatory cytokines (such as tumor necrosis factor alpha). These are among the many mechanisms being investigated with the potential to explain the pathophysiology of antipsychotic-associated weight gain. Finally, it has also been hypothesized that since most SGAs are metabolized by CYP450 enzymes, gene polymorphisms resulting in poor CYP450 activity may also be a mechanism for associated weight gain (Lett et al., 2011; Reynolds & Kirk, 2010). Lett et al. (2011) concede, however, that there remains a paucity of evidence to support these various theories at this time, and assert that antipsychotic-
16 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 16 associated weight gain is likely due to the combined contribution of several risk alleles as well as other environmental, behavioral, and epigenetic factors traditionally associated with obesity. Obesity-Associated Complications & Diseases Obesity has been linked with overall increased morbidity and mortality. Many studies report that obesity is associated with 2 times the risk of all-cause mortality, coronary heart disease, stroke, type II diabetes, and metabolic syndrome (Lett et al., 2011; Mukundan et al., 2010). Furthermore, it is associated with an increased risk of some cancers, musculoskeletal problems, and negative psychological consequences (Mukundan et al., 2010). These health risks are compounded by the observation from several studies that people with severe mental illness die up to 25 to 30 years sooner than the general population, with cardiovascular disease cited as the leading cause of death (Maayan & Correll, 2010; Wu et al., 2008). Ultimately, the risk of mortality in patients with schizophrenia is estimated to be 2.5 times higher than age-matched people in the general population (Maayan & Correll, 2010). With obesity as a major risk factor for additional morbidity and mortality, weight gain associated with the treatment of psychosis is emerging as a significant clinical, social, and economic concern. Ultimately, both the health and cost concerns associated with obesity compel clinicians to carefully consider the seriousness of antipsychotic-associated weight gain. Stigma of Obesity Stigma is defined as the negative attitudes, beliefs, perceptions, and behaviors associated with a mark of disgrace related to a particular circumstance, quality, or person (Abate, 2001). In the current sociocultural environment, the stigma of obesity induces significant mental health effects such as chronic stress, low self-esteem, and negative self concept (Xiao, Baker, & Oyewumi, 2012). Furthermore, obesity-related stigma often results in obese individuals having
17 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 17 reduced access to social resources known to promote health such as positive interpersonal relationships, education, gainful employment, and access to healthcare (Puhl & Heuer, 2009). Finally, the stigmatization of weight gain and obesity is considered a major factor in patient nonadherence to their medication regimen, especially among the mentally ill (Lett et al, 2011). Ultimately, the stigma-related effects of obesity add to the burden of health disparities already experienced by individuals with mental illness. Weight Gain and Treatment Non-adherence Medication-associated weight gain is not only associated with increased health risks, but is also linked with decreased quality of life and poor treatment adherence in individuals diagnosed with mental illness (Correll, Lencz, & Malhotra, 2011). For example, one study reported a significant association between subjective distress from weight gain and medication non-adherence in people with schizophrenia (Weiden, Mackell, & McDonnell, 2004). Furthermore, Lett et al. (2011) assert that weight gain is a leading factor in patient noncompliance with their prescribed medication regimen, particularly in response to the social stigmatization of weight gain and obesity. Trends in Antipsychotic Prescribing Although SGAs have well-established metabolic side effects, such as weight gain, their use continues to increase. In fact, antipsychotics are now among the most commonly prescribed, and most costly, medications being used in the United States today (Olfson, Blanco, Liu, Wang, & Correll, 2012). In recent years, the percentage of visits to primary care providers that included a prescription for antipsychotics increased significantly faster than the corresponding percentage of visits to psychiatrists (Olfson, Kroenke, Wang, & Blanco, 2014). According to Olfson et al. (2012), among antipsychotic medication visits for adults, the most commonly prescribed drugs
18 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 18 were quetiapine (32.6%) followed by risperidone (16.9%), olanzapine (15.2%), and aripiprazole (13.8%). More recently, aripiprazole was recently listed as the 14 th most prescribed medication (ahead of all other SGAs) in the United States and had the highest sales of any prescription medication, at $7.2 billion during the period between July 2013 and June 2014 (Brooks, 2014). Although SGAs were initially approved for schizophrenia, they are now used for several other conditions including psychoses, bipolar disorder, delirium, depression, personality disorders, dementia, and autism (Alexander, Gallagher, Mascola, Moloney, & Stafford, 2011). Many of these conditions are treated with SGAs as off-label, meaning that they have not yet been approved by the Federal Drug Administration for such purposes. Management Approaches to Antipsychotic-Associated Weight Gain Various strategies have previously been identified to address antipsychotic-associated weight gain. Mayaan and Correll (2010), in an article reviewing research related to antipsychotic-related weight gain, have described three primary approaches for management: switching medication, pharmacological augmentation, and behavioral intervention. Additionally, other researchers have suggested that the initial selection of medication with the lowest weightgain potential is prudent (White et al., 2013). The following section provides additional information about each of these management options. Medication selection. Selecting the appropriate medication at the start of treatment is an important initial strategy in preventing weight gain. For patients who are already overweight or obese, or who have expressed concerns about the possibility of gaining weight, the provider must choose a medication with the lowest potential for medication-associated weight gain (White, et al., 2013). As described previously, the greatest weight increases have been observed with olanzapine and clozapine (Mukundan et al., 2010), while ziprasidone and aripiprazole are
19 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 19 associated with the least weight gain (Lett et al., 2008). Additionally, there is some evidence that ziprasidone and aripiprazole may provide protection against weight gain (Reynolds & Kirk, 2010). Evidence regarding newer SGAs (such as asenapine, iloperidone, lurasidone, and paliperidone) is still limited, however, recent findings suggest that lurasidone may have the lowest weight-gain potential of these (De Hert, 2012). Switching medications. Studies have shown that switching between atypical antipsychotics can result in significant weight changes. For example, one study reports that patients switched to olanzapine gained weight, while those who switched to risperidone lost weight (Mukundan et al., 2010). When using the switching strategy to manage weight gain, however, it is important for the provider to first establish a clear connection between the antipsychotic exposure and the weight gain (White, et al., 2013). A consensus statement on this issue recommends that if a stable patient on a second-generation antipsychotic gains 5% of his or her initial weight at any time during therapy, one should consider switching the medication, (Mukundan et al., 2010, p. 6). Other considerations for switching medications include whether there is: a new onset of another health risk condition (hyperlipidemia, diabetes, etc.), nonadherence to the medication regimen due to weight gain, and/or abuse of other medications in order to offset the weight gain (White, et al., 2013). When a decision is made to switch antipsychotic medications because of the weight effects, several methods have been suggested for making the transition (Mukundan et al., 2010): 1. Cross-tapering gradually titrating up the new medication while tapering off the older medication. 2. Starting the new medication at the therapeutic dose while tapering off the older one. 3. Stopping the older medication abruptly while gradually increasing the new one.
20 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN Starting the new drug at therapeutic dose and stopping the old one abruptly. Slow cross-tapering is generally considered the safest approach to medication switching at this time (Maayan & Correll, 2010; Mukundan et al., 2010). Additionally, rapid switching may worsen outcomes (such as early termination of treatment), particularly when switching to aripiprazole or risperdone (Maayan & Correll, 2010). Although related reviews are limited by a relatively small number of studies on this topic, findings indicate that switching medications to an antipsychotic with the least potential for weight gain is both a pragmatic and effective approach to addressing this problem. It is cautioned, however, that medication switching be implemented with careful consideration, particularly in regard to concerns about psychiatric symptom exacerbation leading to relapse and an increased risk of discontinuing treatment (Mukundan et al., 2010). Pharmacologic augmentation. Studies investigating pharmacologic interventions to mitigate antipsychotic-associated weight gain report promising results for the use of adjunct medications. It is generally recommended, however, that adjunctive medications be started only after non-pharmacological strategies such a lifestyle changes and other behavioral interventions have failed to produce sustained weight loss (White, et al., 2013). Medications currently showing promise for mitigating the effects of antipsychotic-associated weight gain include amantadine, metformin, nizatidine, and topiramate (Maayan, Vakhrusheva, & Correll, 2010; White, et al., 2013). Other medications with positive findings include reboxetine, sibutramine, and dexfenfluramine, however, these are not available in the United States at this time (White, et al., 2013). Of all the adjunctive medications identified, metformin and topiramate show the most promise for reducing antipsychotic-associated weight gain (White, et al., 2013). According to
21 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 21 one related meta-analysis, patients experienced an average weight change of kg versus placebo over a mean time period of 3 weeks using various adjunct medications. In particular, metformin was identified as the most superior to placebo with an average decrease of 2.94 kg. Other agents superior to placebo included fenfluramine (-2.60 kg), sibutramine (-2.56 kg), topiramate (-2.52 kg), and reboxetine (-1.90 kg). In a major limitation to the findings of the review, however, the results of the studies were found to be rather heterogeneous. This suggests that there were likely significant differences across the various studies and individual agents. Furthermore, even in the studies demonstrating the most profound weight loss, subjects lost only part (and not all) of the weight they had gained during treatment. Additionally, as previously mentioned, reboxetine, sibutramine, and dexfenfluramine are not currently available in the United States. Finally, although metformin outperformed other agents, there is still not enough evidence to support its regular use as an adjunctive medication to prevent weight gain in patients taking antipsychotic medications (Maayan, Vakhrusheva, & Correll, 2010) and the use of topiramate is associated with several other adverse effects and risks including sedation, memory problems, acute myopia, metabolic acidosis, nephrolithiasis, paresthesias, and increased suicidality (White, et al., 2013). At this time, there may be too few randomized controlled trials testing adjunct medications for antipsychotic-associated weight gain to support clinical practice guidelines. Furthermore, there are no head-to-head studies of these pharmacologic interventions to demonstrate clear superiority of certain medications over others (Faulkner, Cohn, & Remington, 2007; Maayan & Correll, 2010; Maayan et al., 2010). Finally, current studies conflict about whether pharmacological intervention is superior to behavioral intervention in preventing and treating antipsychotic-associated weight gain (Maayan & Correll, 2010).
22 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 22 Behavioral interventions. Behavioral intervention is often considered the first line treatment in non-medication-related weight gain. In a meta-analysis of behavioral interventions designed to reduce antipsychotic-associated weight gain, the authors report that nutritional counseling was as effective as cognitive behavioral therapy, and both were superior to treatment as usual (Maayan et al., 2010, p. 1521). Furthermore, similar studies have found no significant difference in prevention versus intervention, and individual versus group interventions (Maayan & Correll, 2010). In contrast, not all studies demonstrate the effectiveness of behavioral interventions for preventing weight gain. For example, one randomized controlled trial of nurseled weight management and exercise intervention for people taking second-generation antipsychotics showed no significant difference between the intervention group compared to those in the control group (Usher et al., 2012). Combination approach. As yet, only a single study has examined the effectiveness of a combined approach to antipsychotic-associated weight gain (Maayan & Correll, 2010). This study investigated the efficacy of metformin and found that the use of this drug in conjunction with lifestyle interventions was more effective than either metformin or lifestyle intervention used alone (Wu, et al., 2008). Since then, multiple trials are currently underway to test this approach further (Maayan & Correll, 2010). In general, however, most obesity management programs assume that a combination approach will yield better results than single interventions alone. Need for Guideline A recent search of clinical practice guideline resources, such as the Agency for Healthcare Research and Quality (AHRQ) National Guideline Clearinghouse and UpToDate (an evidence-based clinical decision support system), reveals that no formal guidelines exists to
23 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 23 specifically address antipsychotic-associated weight gain. Although there are several review articles summarizing the evidence for interventions to manage antipsychotic-associated weight gain, none provide a simple, clear format for clinicians to use in everyday practice. Final Summary of Literature Review Obesity is a growing social and public health concern, with raising rates of obesity across all ages and demographics. The increasing prevalence of obesity means that healthcare providers will be caring for a greater proportion of obese individuals. At the same time that obesity prevalence is rising, so too is the use of antipsychotics which have been linked with significant metabolic changes and weight gain. Medication-associated weight gain in the treatment of mental illness, particularly in regard to the use of SGAs, is a serious concern for a multitude of reasons including medical, psychological, social, and economic. In addition, adherence to medication regimens is threatened by this very common side effect, putting psychiatric patients at serious risk for relapse. While research investigating ways to manage SGA-associated weight gain is ongoing, no clear guideline yet exists that reflects the current state of knowledge regarding this issue. Theoretical and Conceptual Foundation The development of clinical practice recommendations begins with a clear concept and explicit framework for translating research into evidence-based practice. This section provides a summary of the concepts and theoretical framework used to inform the project s design and implementation. The ACE Star Model of Knowledge Transformation (Stevens, 2013) is used to link concepts for translation of evidence into practice. The GRADE theoretical framework will be used to both inform project design and as a method to analyze and synthesize the evidence regarding the effectiveness of interventions designed to manage SGA-associated weight gain.

24 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 24 Concepts Map and Definitions The ACE Star Model of Knowledge Transformation was developed as a conceptual model to simplify the approach of translating health care research into evidence-based clinical practice. The model is a five-point star (Figure 1) that depicts the critical steps for moving research findings into practice interventions (Stevens, 2013). Stevens (2013) asserts that it is inefficient for clinicians to search through volumes of research articles in order to make safe and effective practice decisions while caring for patients. Rather, clinical decision-making is best supported by evidence-based recommendations, which are summarized in the form of clinical practice guidelines. The five points of the star are further described below. Figure 1. The ACE Star Model of Knowledge Transformation, copyrighted material (Stevens, 2012). Reproduced with expressed permission. Discovery research. According to Stevens (2004), discovery research is the knowledge generating stage. This represents the traditional field of scientific inquiry, using defined research methodologies to understand and describe natural and social phenomena. The products of this
25 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 25 stage may be referred to as primary research studies and includes the full spectrum of research designs, from randomized control trials to qualitative studies. Evidence summary. Stevens (2004) describes evidence summary as the synthesis of research knowledge into a single statement that meaningfully conveys the state of science regarding a topic. Evidence summaries are also part of knowledge generation, as they create new knowledge from the combination of studies. Stevens identifies several advantages to evidence summaries such as the reduction of large volumes of information into a manageable form, enhanced generalizability, identification of consistencies and inconsistencies across studies, increased statistical power for assessing cause and effect, reduction in bias, integration of existing information, increased efficiency in time between research findings and clinical practice implementation, and establishment of a basis for continuous update with new evidence as it emerges. Translation into guidelines. According to the ACE Star Model, the translation of evidence into guidelines requires two stages: translation of evidence into practice recommendations and integration into practice. The goal of translation is to produce a useful summary of evidence in the form of recommendations that address time, cost, and care standards (Stevens, 2004). Practice integration. The step of practice integration involves changing both individual and organizational practices to reflect the most current evidence. This change can be achieved through both formal and informal processes, and involves the factors that address rate of adoption and the sustainability of the changes (Stevens, 2004). Process, outcome evaluation. The final stage in the ACE Star Model is the evaluation of the impact evidence-based practice has upon various outcomes including patient health,
26 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 26 patient and provider satisfaction, efficacy, efficiency, cost, and health status impact (Stevens, 2004). Related Terms Guidelines. Guidelines are described by the World Health Organization (WHO, 2012) as recommendations intended to assist providers and recipients of health care and other stakeholders to make informed decisions, (p. 1). Additionally, these recommendations must be generated by a process that is objective, comprehensive, free of bias, meets a public health need, and is clear enough for others to see how the recommendation has been developed, by whom, and on what basis. Stevens (2004) states that well-developed clinical practice guidelines describe the benefits, harms, and costs of various decision options. Furthermore, strong guidelines are developed systematically using a process that is described explicitly and can, therefore, be reproduced. Finally, evidence-based clinical practice guidelines clearly identify the strength of the evidence in relation to each practice recommendation (Stevens, 2004). Evidence-based practice. Many definitions of evidence-based practice exist, however, all include themes of applying the most current research to clinical practice decisions. The website for the Agency for Healthcare Research and Quality (AHRQ, n.d.) defines evidencebased practice as: Applying the best available research results (evidence) when making decisions about health care. Health care professionals who perform evidence-based practice use research evidence along with clinical expertise and patient preferences. Systematic reviews (summaries of health care research results) provide information that aids in the process of evidence-based practice.

27 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 27 Hierarchy of evidence. When reviewing evidence to make practice recommendations, researchers and clinicians rank evidence to reflect the type of studies that can provide the best findings for clinical practice. In general, these hierarchies are presented as pyramids depicting the best types of evidence at the peak. Systematic reviews and meta-analyses are considered the gold standard of evidence, with Cochrane Systematic Reviews among the most widely recognized and respected (Fitzpatrick, 2007). Figure 2 depicts a suggested evidence hierarchy based upon these premises (University of Washington, 2011). Figure 2. Hierarchy of evidence. The highest levels on the pyramid are considered the best evidence for clinical practice (University of Washington, 2011). Reproduced with permission. Theoretical Framework The GRADE (Grades of Recommendation, Assessment, Development, and Evaluation) system is a framework used in the development of guidelines in healthcare. It was created and refined by an international working group of health professionals, researchers, and guideline
28 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 28 developers with the purpose of designing an optimal system for rating quality of evidence and determining the strength of recommendations for clinical practice guidelines (Guyatt, 2011). GRADE is now used by many health-related organizations including the WHO, CDC, AHRQ, American College of Physicians, Cochrane Collaboration, UpToDate, and over 60 other major organizations (Schunemann, Ahmed, & Morgan, 2011). Researchers promoting the use of GRADE have identified how the methodology itself is embedded in a larger theoretical framework (Figure 3) that outlines an ideal process for guideline development. Figure 3 depicts the relationships between the formulation of PICO questions, the creation of evidence profiles for quality assessment, and the translation of these findings into practice recommendations for clinical guidelines (Schunemann, et al., 2011).
 identifies several advantages of using the GRADE framework and quality assessment methodology including: Provides explicit and comprehensive")
29 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 29 Figure 3: The GRADE framework for guideline development (Schunemann, et al., 2011). Reproduced with permission. The Insitute for Clinical Systems Improvement (2015) identifies several advantages of using the GRADE framework and quality assessment methodology including: Provides explicit and comprehensive criteria for downgrading and upgrading quality of evidence ratings Clearly separates quality of evidence and strength of recommendations with a transparent process of moving from evidence evaluation to recommendation Provides clear, pragmatic interpretations of strong versus weak recommendations for use by clinicians, patients, and policy-makers
30 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 30 Includes an explicit acknowledgement of values and preferences In the GRADE process, evidence is gathered according to the PICO question, with systematic reviews utilized first. Additional literature may be reviewed (using randomized control trials, observational studies, etc.) and included to enhance the overall quality of evidence.
31 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 31 Chapter 3: Project Design and Evaluation Plan The purpose of this project was to develop evidence-based practice recommendations for the management of antipsychotic-associated weight gain in adults. The following section describes the overall design of the project, the implementation of the project, and the method for evaluation upon completion of the evidence-based algorithm and guideline for managing antipsychotic-associated weight gain in the primary care setting. Project Design The project design was informed by the GRADE approach to guideline development. Key elements of the GRADE approach include the formulation of PICO questions, the creation of evidence profiles for quality assessment, and the translation of these findings into practice recommendations (Schunemann, et al., 2011). Additionally, project evaluation is an important component of the project, with evaluation measures also informing the overall project design. Facilities and Resources Minimal facilities and resources were needed for project implementation, as this project relied primarily upon electronic sources of data. Furthermore, management and analysis of data was conducted using free and/or already available software. These software programs included EndNote for storing and managing articles, ReviewManager5 (RevMan5) for meta-analysis of study data and generation of risk of bias summaries, and GRADEpro (McMaster University, 2014) for data analysis, synthesis, and display. Additional materials (in the form of paper, pens, staples, etc.) were also needed for both project implementation and evaluation, however, such expenses were minimal and the cost of these were borne entirely by the researcher.
32 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 32 Study Population and Setting The population studied in this project included adults between the ages of 18 and 65 years who were receiving treatment with SGAs (see Appendix A for a list of SGAs). Trials included were those conducted in settings generalizable to the U.S. primary care system, feasible for conducting in the primary care setting, eligible for referral from primary care, or conducted in commercial settings (e.g., Weight Watchers). Trials conducted in hospitals, institutionalized settings, school-based programs, occupational settings, churches, and other settings deemed not generalizable to the primary care setting were excluded. Key Questions 1. In adults taking second-generation antipsychotic medication (P), how does medication switching (I) compare to standard care (C) for decreasing weight (O)? 2. In adults taking second-generation antipsychotic medication (P), how do pharmacological interventions (I) compare to standard care (C) for decreasing weight (O)? 3. In adults taking second-generation antipsychotic medication (P), how do behavioral interventions (I) compare to standard care (C) for decreasing weight (O)? Interventions Only interventions that focused upon weight loss were included and these were further limited to the following intervention strategies: switching medications between SGAs, pharmacotherapies used as adjunctive medications, and behavioral interventions. Combination interventions (such as pharmacotherapy plus behavioral interventions) were excluded with the assumption that combination therapies are generally considered more effective than single
33 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 33 interventions alone. Interventions that did not focus primarily on weight or that did not report weight-related outcomes were also be excluded. Comparison All interventions were compared to standard care. In this project, standard care refers to patients who continue their usual antipsychotic medication without any other specific interventions to reduce weight gain. Outcomes The primary outcome for consideration was weight loss as measured by standard instruments such as standing scales. Secondary outcomes included global state, adverse effects, serious adverse effects, and discontinuation of treatment. Serious adverse effects included serious treatment-related harms such as death, medical issue requiring hospitalization, and psychiatric issue requiring hospitalization. Outcomes reported more than 12 months after the start of the intervention were included when available. Outcomes related to treatment-related harms had no minimum follow up requirement. Outcomes were prioritized according to the GRADE method (Appendix B) prior to initiation of the study. Evidence Search Strategy The evidence search was conducted using relevant electronic databases such as the Cochrane Database of Systematic Reviews, MEDLINE (PubMed), CINAHL, and Web of Science. Additionally, websites hosting clinical practice guidelines (such as AHRQ) were searched for any updates related to antipsychotic medications and weight gain. Searches were supplemented by reviewing reference lists from other relevant publications. Search terms included antipsychotic*, obes*, switching, intervention*, topiramate, metformin, behav*, and systematic review. Only studies conducted between February 28, 2005 and February 28, 2015
34 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 34 were considered. Additionally, only studies available in English and obtainable as full-text using the University of Hawaii at Hilo journal subscriptions were used. Only interventions focused upon weight loss were considered and limited to the following intervention strategies: switching medications, adjunct medications, and behavioral interventions. Combination interventions (such as adjunct medication plus behavioral intervention) were excluded with the assumption that combination therapies are generally considered more effective than single interventions alone. Interventions that did not focus primarily upon weight or did not report weight-related outcomes were excluded. Interventions focused upon dietary and physical activity changes were also excluded, as these are considered standard care for weight management. Studies of child, adolescent, and inpatient populations were excluded as the guideline was focused upon adults in the outpatient setting. Data Extraction and Quality Assessment Potentially relevant studies were identified for each review question and search result titles and abstracts were screened according to the inclusion and exclusion criteria. Those papers identified for inclusion were then obtained in full text and further reviewed against the inclusion and exclusion criteria. The studies were then classified according to a hierarchy of evidence, utilizing systematic reviews first and then high-quality randomized-controlled trials. Evidence quality was assessed according to the GRADE criteria (Appendix C). Data Synthesis and Analysis Evidence for medication switching, pharmacological augmentation, and behavioral interventions were separately synthesized and displayed as evidence summaries using the GRADEpro software. Data from randomized controlled trials were entered into the RevMan5 software according to the outcomes of interest. Furthermore, the individual studies were
35 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 35 evaluated for risk of bias and a risk of bias summary was generated for each of the interventions (Appendix D). Pooled data was then depicted in forest plots for each intervention and according to the outcomes of interest (Appendix E). This pooled data was then exported to the GRADEpro software to generate evidence tables (Appendix O, pp ) and summary of findings tables (Appendix O, pp ). These summaries included GRADE ratings for each intervention described, according to the quality assessment domains included in the GRADEpro software. Recommendations for clinical practice were then developed according to the GRADE standards (Appendix F) and utilizing the Guideline Development Tables included in the GRADEpro software. Evidence-to-decision tables generated by the GRADEpro software are displayed in Appendix O (pp ). Recommendations were then organized in the form of a guideline (Appendix O), along with a proposed management algorithm (Appendix O, p. 181) that reflects the study findings and other sources of evidence-based practice. Evaluation The final product of the project (the practice guideline) was evaluated by a small panel of interdisciplinary experts and stakeholders. Invited participants included experts from academia, behavioral health, primary care, and family members of patients affected by antipsychoticassociated weight gain. Participants were recruited via networking by the researcher through personal and professional contacts. The AGREE II (Appraisal of Guidelines for Research and Evaluation II) instrument was used by panel members to evaluate the practice guideline produced by the project. The AGREE II instrument is a standardized method to assess the quality of guidelines. It is a generic instrument that can be applied to guidelines in any disease and any step in the healthcare continuum (i.e. prevention, management, public health). Key domains measured by the AGREE II instrument include: scope and purpose, stakeholder
36 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 36 involvement, rigor of development, clarity of presentation, applicability, and editorial independence. Additionally, the AGREE II instrument includes a rating of the overall quality of the guideline and whether the guideline would be recommended for use in practice. The statements used for assessments in each domain are listed in Appendix G. Finally, the AGREE II developers recommend that an evaluation panel contain no less than 2 people and preferably greater than 4 evaluators to increase the reliability of the assessment (AGREE Next Steps Consortium, 2009). For this project, invitations were sent to 11 prospective participant evaluators. For those that returned consents, a digital or paper copy of the guideline was distributed to the evaluators and a link to an on-line survey containing the AGREE II questions was sent via . Once the AGREE II evaluations were collected, descriptive statistics were generated summarizing the ratings (by domain, question, and overall score). Additionally, the written comments offered by the evaluators were summarized by describing the major themes identified. Ethics and Human Subjects Protection The research project proposal was submitted to the Institutional Review Board (IRB) of the University of Hawaii as an exempt application, as the project did not involve experimentation with human participants. For evaluators of the guideline, a consent form (Appendix H) was used to ensure their rights and responsibilities as participants in a research project. This consent, along with the project application was approved by the IRB on March 5, 2015 (Appendix I). Copies of the consents have been kept on a digital file by the author. The identities of the participants were not required for submission of the evaluation responses.
37 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 37 Chapter 4: Results The following section describes the objective results of the project in two parts. The first part refers to the results of the systematic review and the final synthesis of the evidence, the clinical practice guideline. The second part of this section describes the feedback from the evaluators of the guideline, using both descriptive statistics and summaries of the comments according to the major themes identified. Part 1: Systematic Review and Clinical Practice Guideline As described in the project design, a systematic search was conducted using 4 electronic databases using series of key search terms for each intervention. After applying the inclusion and exclusion criteria, 21 articles were included in the evidence review, including 12 systematic reviews and 9 high-quality randomized controlled trials. Appendix O (pp ) provides flow diagrams of the article selection according to each review question. Note that the number of systematic reviews cited in the flow diagrams is greater than the 21 articles stated here. This discrepancy results from systematic reviews that included more than one intervention type in their analysis, and were therefore, listed more than once in the article selection process. Tables of database findings are included in Appendix J and tables of excluded studies are included in Appendix K. Initially, it was hoped that data from the systematic reviews could be used to generate summary of findings tables and evidence summaries directly. Given the narrow scope of the PICO questions, however, randomized controlled trials were extracted from these systematic reviews and the data were collected for meta-analyses according to each intervention. Pooled data was summarized using forest plots (Appendix E) according to the following outcomes of interest:
38 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN Weight change 2. Global state 3. Adverse effects 4. Serious adverse effects 5. Discontinuation of treatment The findings were then validated by comparing pooled data to the outcomes of similar meta-analyses reported in the systematic reviews identified in the evidence search. Additionally, each study included in the meta-analyses and summary of findings tables were critically appraised using a risk of bias tool embedded in the RevMan5 software. A summary of the risk of bias assessments for each of the included studied can be found in Appendix D and a description of all included studies can be found in Appendix L. Once the studies were appraised and the data were pooled, the results were exported to the GRADEpro software. This software includes another quality of evidence rating tool, which allows the reviewer to grade evidence according to the outcomes of interest. Additionally, outcomes were rated according to the GRADE methodology outlined in Appendix B. Evidence tables were then generated for each intervention (Appendix O, pp ) following the GRADE criteria embedded in the software. Furthermore, these evidence tables were then used to generate summary of findings tables (Appendix O, pp ), a recommended format for presenting the findings of systematic reviews. Synthesis of the evidence into a clinical practice guideline was facilitated by the GRADEpro software s evidence-to-decision guideline development template. Key questions were addressed by reviewing the evidence from the systematic review and by referencing additional articles related to patient preferences, medication side-effects, resource utilization,
39 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 39 incremental costs, and feasibility of implementing recommendations. From these evidence-todecision tables (Appendix O, pp ), a guideline was written following the web-based format utilized by AHRQ s National Guideline Clearinghouse (AHRQ, 2015). Additionally, an algorithm (Appendix O, p. 181) was developed to synthesize the recommendations included in the guideline. The full guideline, along with supporting documentation, is found in Appendix O. Part 2: Guideline Evaluation As described in the project design, participants were recruited to evaluate the clinical practice guideline in Appendix O. Eleven potential evaluators were identified and a recruitment flyer and consent were sent by to each prospective participant by . In response, nine people returned signed consents to the principle investigator. For those consenting to participate, either a digital or paper copy of the guideline was provided according to evaluator preference. Additionally, each evaluator received an with a hyperlink to a web-based survey containing the AGREE II questions. Included with each question in the web-based survey were AGREE II user manual instructions to provide clarity. For each survey question/statement, participants were asked to rate their answer on a 7-point Likert scale (1-strongly disagree to 7 strongly agree). Additionally, a comment box was provided for each question to allow for optional evaluator feedback. Of the nine participants, seven completed the on-line survey. Data was collected on May 5, 2015 for the evaluator responses and a summary is provided in Appendix M. The following section provides a description of the evaluators, along with a summary of the responses from each of the six domains from AGREE II survey, and a final summary of the overall evaluation of the guideline according to the responses of the participants.
40 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 40 Evaluators. Seven people participated in the guideline evaluation. Among these were two academics/professors (one specializing in pharmacy and the other in neuroscience), one advance practice nurse, two physicians (one primary care physician and one psychiatrist), one psychologist, and one family member of a patient affected by antipsychotic-associated weight gain. Additionally, the family member is also a registered nurse working in acute behavioral health. Of the these stakeholders, two identified their clinical specialty as academic/research, four as behavioral/mental health, one as primary care, two as pharmacology, and one as other. Scope and purpose. In general, the majority of evaluators (85.7%) rated the guideline 6 or higher in the various aspects of this domain. Strengths identified in the comments include that the objectives were clear and concise, and the health questions were straight-forward and relevant. Limitations identified by evaluators included a need to address the health risks associated with obesity such as metabolic dysfunction, diabetes, and cardiovascular disease. Additionally, some evaluators noted that the target population was too generalized and the diagnoses were not specific enough. Stakeholder involvement. The results for this domain were mixed, with evaluators somewhat divided in two of the three questions/statements. For example, only 66.7% of evaluators agreed or strongly agreed (rated 5 or higher) that the views and preferences of the target population (patients, public, etc.) had been sought. The remaining participants (33.3%) rated this question as a 4 or neutral. Evaluators commented that more information regarding patient perspectives should be provided, particularly in regard to what patients believe is (or is not) effective in weight management. Likewise, only 57.1% of participants strongly agreed that the guideline development group (i.e. evaluators) included individuals from all relevant professional groups. Suggestions for professionals to involve in the guideline evaluation
41 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 41 included registered dieticians, social workers, and staff in forensic settings such as prisons and probation offices. Evaluators were more unified, however, in their response to the AGREE II statement regarding the target users of the guideline, with 85.7% of participants strongly agreeing that target users were clearly defined. Comments from this section indicate, however, that the target user group could have been expanded, such as to patients in the long-term care setting. Rigor of development. Responses in this domain were mostly favorable, with one major exception: a procedure for updating the guideline. Reviewers were mixed in their response to this statement, noting that they could not find information to answer the question. Indeed, the only mention of an update for the guideline, was in reference to modifications that might be made after feedback from the evaluations. In other areas, however, the majority of evaluators agreed or strongly agreed that systematic methods were used to search for evidence (71.4%), that the criteria for selecting the evidence was clearly described (85.7%), that the strengths and limitations of the body of evidence were clearly described (100%), that the methods for formulating the recommendations were clearly described (100%), that the health benefits, side effects, and risks have been considered in formulating the recommendations (71.5%), that there was an explicit link between the recommendations and the supporting evidence (100%), and that the guideline has been externally reviewed by experts prior to its publication (100%). Strengths identified in the comments include that the review was thorough, with excellent data sources and categorization. Limitations offered in the comments included a lack of explanation for the exclusion of FDA approved obesity management medications, the lack of adequate long-term follow up in the included studies, concern about whether sufficient attention was given to the side-effects of adjunct medications, a need for further discussion of co-morbidities, and the need
42 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 42 for additional information regarding the emerging knowledge of the role of genetics in the development of obesity. Clarity of presentation. The reviewers were unified in their reporting regarding the clarity of the guideline presentation. On all questions/statements for this domain, evaluators agreed or strongly agreed that the recommendations were specific and unambiguous (100%), that the different management options were clearly presented (100%), and that key recommendations were easily identifiable (100%). Limitations offered in the comments included the need for specific dosages, the need for guidance with managing complications and co-morbidities, and the concern about the limited scope of the guideline (which only targets weight gain). Applicability. The evaluators were largely unified in their response regarding the applicability of the guideline. The majority (83.3%) agreed or strongly agreed that the guideline described facilitators and barriers to its application, however, the comments indicated that this area could have been expanded with extra attention given to patient acceptance of the risks involved, patient adherence to recommendations, and reimbursement issues related to off label use of medications and referral to specialists. Additionally, 100% of respondents agreed or strongly agreed that the guideline provided advice and/or tools on how the recommendations could be put into practice. In particular, comments noted that the algorithm was easy to follow and put into practice. One commenter suggested, however, that an additional test (Hemoglobin A1c) be included in the assessment and monitoring. In regard to resource implications for applying the recommendations, the majority (83.3%) agreed or strongly agreed that these had been considered in the guideline. Commenters noted, however, that this section could have been expanded to include reimbursement issues and availability of specialists. Finally, 100% of
43 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 43 evaluators agreed or strongly agreed that the guideline presented monitoring and/or auditing criteria. Editorial independence. Questions in this domain were difficult for respondents to answer, as issues regarding editorial independence (such as funding and competing interests) were not explicitly addressed in the guideline. For the current draft of the guideline, no funding was provided to the author and the competing interests of the guideline evaluators were not surveyed. Overall guideline assessment. The guideline received favorable overall ratings, with 14.3% of evaluators rating it as a 5, 57.1% of evaluators rating it as a 6, and 28.6% of evaluators rating it as a 7. Additionally, 50% of respondents would recommend the guideline for use without any modifications and 50% would recommend it with some modifications. One evaluator did not answer this question. Evaluators who offered comments in this section noted a desire for more literature regarding the use of metformin before supporting the recommendations and suggested that perhaps cognitive-behavioral therapy should play a more dominant role in the algorithm. Other comments were consistent with those offered in the previous domains.
44 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 44 Chapter 5: Recommendations and Conclusions The following section describes how the results of the project are linked with project s purpose and how the aims and objectives were achieved. Furthermore, the guideline developed from the project is discussed from the author s perspective, in light of the evaluation results. Additionally, facilitators and barriers to the project are reviewed and limitations to the project are discussed. Purpose, Aims, and Objectives The purpose of this project was to develop evidence-based practice recommendations for the management of antipsychotic-associated weight gain in adults. This was accomplished by using a structured methodology to develop a clinical practice guideline targeting this problem. The purpose of the project was supported by two primary aims. The first aim was to improve the care and treatment of adults with SMI by effectively addressing their population-specific physical health concerns through the development of evidence-based recommendations designed to assist primary care providers in the management of antipsychotic-associated weight gain. Objectives for achieving this aim included: 1. Conduct a structured literature review investigating interventions for managing antipsychotic-associated weight gain. 2. Analyze the literature to both grade and compare interventions. 3. Determine best practice recommendations for the management of weight gain in adults taking antipsychotic medications. Each of the above objectives were achieved using the methods described in chapter 3. Briefly, these methods included: a systematic review of the literature according to the PICO questions created, identification of studies meeting the inclusion and exclusion criteria, meta-
45 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 45 analysis of the data from the highest quality evidence available for each intervention strategy and according to the identified outcomes, quality assessment of the included studies, prioritization of the outcomes, quality assessment of the evidence according to the outcomes, synthesis of the evidence in summary of findings tables, analysis and comparison of the interventions according to the quality of the evidence, and formulation of recommendations using a structured evidenceto-decision framework. The second aim of the project was to promote the translation of new knowledge into health care practice by achieving the following objectives: 4. Synthesize findings into an evidence-based algorithm and guideline for managing antipsychotic-associated weight gain in the primary care setting. 5. Discuss the relevance of medication-associated weight gain to advanced nursing practice. 6. Suggest strategies for advanced nursing practice that promote the IOM s aims for quality care, specifically those relating to the safe, effective, and equitable care of patients. Only one of the above objectives has thus far been addressed, which is the synthesis of the project findings into an evidence-based algorithm and guideline. The product of this objective is included in Appendix O. As for the objectives numbered five and six, these are discussed in the last chapter of this manuscript. The Guideline The product of this project, the clinical practice guideline (Appendix O), was favorably received by a diverse panel of stakeholders with clinical expertise in family practice, advanced nursing practice, psychiatry, psychology, pharmacology, and neuroscience. Although some of
46 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 46 the domains measured by the AGREE II instrument were more weakly rated than others, the guideline currently provides a sound foundation for establishing best-practices in the management of antipsychotic-associated weight gain in adults. Previously, peer-reviewed articles have offered clinical practice advice for this problem (Alvarez-Jimenez, Hetrick, Gonzalez-Blanch, Gleeson, & McGorry, 2008; Bonfioli, Berti, Goss, Muraro, & Burti, 2012; Buckley & Correll, 2008; Fiedorowicz, Miller, Bishop, Calarge, Ellingrod, & Hayes, 2012; Hasnain, Vieweg, & Hollett, 2012; Maayan & Correll, 2010; Mizuno, et al., 2014), but to date, none has offered a comprehensive guideline for providers. This guideline developed during this project helps to fill this need. Additionally, the external review of the guideline using a structured evaluation completed by key stakeholders, helps to strengthen its validity for future use in practice. Project Facilitators The successful completion of this project was facilitated by: Free access to an extensive body of evidence made easily available through electronic databases and the internet Availability of free software for analyzing and synthesizing data Availability of free web-based tutorials for using the software and applying the GRADE methodology Easy dissemination of guideline and evaluation instrument using and webbased surveys Willingness of stakeholders to take the time to evaluate the guideline Project Barriers Barriers to the successful completion of this project included:
47 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 47 Time constraints An overwhelming body of evidence that required the scope of inquiry to be substantially narrowed Lack of technical skill required for using related software and appropriately applying the GRADE methodology Lack of a guideline development group at the outset Lack of cost-analysis data for the interventions recommended in the guideline Project Limitations There were several limitations to this project, but most important among them, was the fact that the guideline was developed with only one researcher/author. In nearly all systematic reviews, articles are critiqued against inclusion and exclusion criteria by at least two authors. This helps to reduce both the risk of bias and error in article selection. The same is true with evaluating the quality of studies included in the evidence summaries. Although the GRADE approach offers structured, specific guidance for assessing risk of bias and the quality of evidence, ultimately, these decisions remain part of the subjective purview of the assessors. Likewise, according to the GRADE methodology, guidelines panels (comprised of multiple individuals with diverse expertise) should be involved in formulating the guideline recommendations before development. Recommendations are typically negotiated among panel members through discussion, reflection, and debate that considers the quality of evidence, the balance of benefits and harms, the values and preferences of stakeholders (including patients), and the anticipated resources needed (costs). Although some of these elements were addressed by having the guideline externally reviewed and evaluated, multiple people should have been involved in all phases of the guideline development; from formulating the PICO questions to
48 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 48 conducting the systematic review, and from assessing the quality of evidence to making recommendations. Other limitations of the project include the narrow scope of the guideline, the lack of long-term follow up for the interventions, the limited number of studies included in the metaanalyses, and the lack of data regarding patient preferences and cost-effectiveness of interventions. There are many reasons for these limitation, but most significantly, is the fact the project was conducted by a sole individual. Sole authorship required a narrow scope, to make the project manageable. This narrow scope then limited the number of studies for meta-analysis, again, to make the project more manageable. As for the lack of long-term follow up for interventions, this gap in the literature is a concern of many authors of systematic reviews examining the problem of antipsychotic-associated weight gain and calls have been made for longer term studies. Likewise, the lack of studies examining patient preferences and the costeffectiveness of proposed interventions represent significant gaps in the literature. Further studies examining these issues will help with the development of a more comprehensive and patient-centered guideline in the future. Plan for Revision Given the limitations of this project, a prudent plan for revision of the guideline includes additional inquiry into patient perspectives regarding antipsychotic medications, medicationassociated weight gain, barriers to treatment adherence, and prioritization of treatment outcomes. Additionally, the guideline would clearly benefit from greater participation by key stakeholders and a more explicit explanation for the exclusion of medications and treatments targeting at obesity in the general population. These changes must be implemented before the guideline can be submitted for dissemination to providers and patients.
49 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 49 Chapter 6: Implications for Practice The following section provides a discussion regarding the project s contributions to practice and identifies research possibilities for future projects. Furthermore, objectives five and six of the project are addressed by describing the project s relevance of antipsychotic medication-associated weight gain to advanced nursing practice and suggesting strategies for promoting the Institute of Medicine s aims for quality care, specifically those relating to safe, effective, patient-centered, and equitable care. Relevance to Advanced Nursing Practice The use of SGAs for a wide spectrum of conditions continues to increase (Alexander, et al., 2011; Olfson, et al., 2014). As these medications become more commonly prescribed, it is prudent for advance practice nurses to be aware of the significant metabolic effects SGAs can have upon the patients taking them. Likewise, the advance practice nurse must be familiar with the recommended metabolic monitoring parameters for patients receiving SGAs, as well as informed about the most effective interventions for addressing adverse effects such as glucose dysregulation, insulin resistance, dyslipidemia, and weight gain. Additionally, as obesity rates continue to increase, advanced practice nurses must learn to tailor weight loss interventions to probable causes that are specific to the individual patient, such as the weight-gain effect associated with many psychotropic medications. Contributions to Practice The major contribution to practice achieved by this project is the establishment of a clinical practice guideline for managing antipsychotic-associated weight gain. As noted previously, although several articles exist that provide clinical practice advice for this problem, to date, none have comprehensively summarized the evidence-based interventions into a single
50 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 50 guideline. The development of this guideline provides clinicians with evidence-based tools that are specifically targeted at this known, predictable cause of obesity. These tools are meant to both complement and support more universal approaches to weight management, and are explicitly designed to address the population-specific health concerns of individuals with mental illness, particularly those taking antipsychotic medications. Furthermore, the guideline is designed to promote the IOM quality care aims for safety, effectiveness, patient-centeredness, and equity. Safety. The IOM calls upon the healthcare system, and related professionals, to provide treatment that does not result in additional harm or injury to patients (Berwick, 2002). In the case of SGAs, while these medications have a positive impact upon a wide range of psychiatric symptoms, they are also associated with significant metabolic changes that can have long-lasting negative physical and social effects upon patients. This project helps to both raise awareness of the adverse effects of SGAs and provide needed tools for clinicians to intervene early, ideally limiting the negative impact these medications may have upon patients. Additionally, the project s use of the GRADE methodology helps to promote greater recognition of evidence summaries, which clinicians can use to more efficiently translate the latest scientific knowledge into everyday clinical practice. Such evidence summaries provide a standardized format to assist clinicians with quickly evaluating the safety outcomes of treatment interventions across multiple studies. To advance the IOM s quality care aim of safety, healthcare professionals should use evidence summaries regularly to assess key outcomes, particularly when weighing the risks and benefits of treatment options with patients. Effectiveness. The IOM asserts that the healthcare system should only provide services and interventions that are based upon scientific knowledge (Berwick, 2002). In the context of
51 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 51 obesity, interventions must be targeted at the underlying cause of weight gain in order to be effective. This project identified evidence-based strategies for managing weight gain caused by antipsychotic medications by creating evidence summaries using the GRADE methodology. This GRADE approach was specifically designed to translate scientific knowledge into clinical practice, by providing researchers and clinicians with a standardized system for both rating the quality of evidence and determining the strength of clinical practice recommendations. To advance the IOM s quality care aim of effectiveness, healthcare professionals should use evidence summaries to assess the outcomes of interventions. Likewise, researchers and guideline developers should use the GRADE methodology to ensure high-quality, transparent, and evidence-based clinical practice recommendations. Patient-centeredness. In a paradigm shift for understanding the patient-provider relationship, the IOM calls on healthcare professionals to honor and respect a patient s culture, social context, specific needs, and individual choices (Berwick, 2002). In regard to SGAs and weight gain, this project addressed the social and physical impact of this medication side effect by seeking out evidence-based interventions to address the problem. Too often, patients are blamed for weight gain and obesity, resulting in stigmatization and poorer quality of care (Puhl & Heuer, 2009). This project helps clinicians focus upon the specific needs of patients, by raising awareness about the problem of medication-associated weight gain and providing evidence-based solutions. Furthermore, the unique health challenges of individuals with mental illness are targeted, namely, the much higher rates of obesity in this population. Likewise, medication adherence is a known problem for individuals diagnosed with mental illness, with weight gain identified as a significant reason for not taking the prescribed psychotropic medications (Correll, et al., 2011; Lett, et al., 2011; Mukundan et al., 2010; Weiden, et al., 2004).
52 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 52 In order to meet the IOM quality care aim of effectiveness, providers should consider patient concerns about weight gain when selecting medications. Likewise, developers of clinical practice guidelines should seek out patient values and preferences at the outset (and throughout) the guideline development process, while also encouraging greater patient participation in guideline development. Equity. The IOM, recognizing the problem of growing health disparities, calls upon healthcare professionals to provide care that does not vary in quality due to personal characteristics and tasks the healthcare system with closing gaps in health status experienced by vulnerable populations (Berwick, 2002). This project focused upon reducing the health disparities experienced by individuals with mental illness by developing a guideline targeted at population-specific health care needs. The aims and objectives of this project were driven by the observation that obesity rates among individuals with mental illness are markedly higher than the general population (De Hert, et al., 2011). By providing evidence-based solutions for antipsychotic-associated weight gain, this project helps to promote medication adherence, improve physical health and related quality of life, and ultimately, reduce morbidity and mortality for patients with mental illness. Healthcare professionals can support the IOM quality care aim of equity by learning more about health disparities and seeking out ways to uncover, challenge, and change the implicit and explicit biases (we all have) that are associated with the physical and social characteristics of vulnerable populations. For researchers, healthcare policy makers, and guideline developers, consider health disparities as a starting point for clinical practice problems.
53 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 53 Future Projects There are many future research possibilities related to this project. In particular, additional research is needed regarding the long-term impact of antipsychotic-associated weight gain upon the overall quality of life, physical health, and treatment adherence patterns of patients affected by this problem. Likewise, additional studies comparing the various interventions for managing antipsychotic-associated weight gain (particularly studies with long-term follow up) are needed to help clarify the safest and most effective treatments. Finally, there is a paucity of costanalysis research for interventions targeted at managing antipsychotic-associated weight gain. Such information would be valuable to both practitioners and policy-makers as organizations strive for greater efficiency in healthcare spending. Additional research in all of these areas will help healthcare professionals promote the IOM s aims for patient care that is safe, effective, patient-centered, and equitable.
54 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 54 References Abate, F. (2001). The new Oxford American dictionary. New York: Oxford University Press. Afshar, H., Roohafza, H., Mousavi, G., Golchin, S., Toghianifar, N., Sadeghi, M., & Talaei, M. (2009). Topiramate add-on treatment in schizophrenia: a randomised, double-blind, placebo-controlled clinical trial. Journal Of Psychopharmacology (Oxford, England), 23(2), doi: / Agency for Healthcare Research and Quality. (2015). National Guideline Clearinghouse. Retrieved from Agency for Healthcare Research and Quality. (n.d.). Glossary of Terms. Retrieved from Agius, M., Davis, A., Gilhooley, M., Chapman, S., & Zaman, R. (2010). What do large scale studies of medication in schizophrenia add to our management strategies? Psychiatria Danubina, 22(2), AGREE Next Steps Consortium. (2009). The AGREE II Instrument [Electronic version]. Retrieved from Alexander, G. C., Gallagher, S. A., Mascola, A., Moloney, R. M., & Stafford, R. S. (2011). Increasing off-label use of antipsychotic medications in the United States, Pharmacoepidemiology and Drug Safety, 20(2), doi: /pds.2082 Alvarez-Jimenez, M., Hetrick, S. E., Gonzalez-Blanch, C., Gleeson, J. F., & McGorry, P. D. (2008). Non-pharmacological management of anti psychotic-induced weight gain: systematic review and meta-analysis of randomised controlled trials. British Journal of Psychiatry, 193(2), doi: /bjp.bp
55 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 55 American Diabetes Association. (2004). American Association for Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care, 27(2), Andersen, T. H., Bech, P., & Larsen, N. E. (2005). Switching patients from olanzapine or risperidone to a combination treatment using perphenazine plus buspirone: evaluation of antipsychotic efficacy and side-effects, including extrapyramidal effects and weight loss. Nordic Journal Of Psychiatry, 59(3), Andrews, J. C., Schünemann, H. J., Oxman, A. D., Pottie, K., Meerpohl, J. J., Coello, P. A.,... & Guyatt, G. (2013). GRADE guidelines: 15. Going from evidence to recommendation determinants of a recommendation's direction and strength. Journal of clinical epidemiology, 66(7), Arnoldy, R., Curtis, J., & Samaras, K. (2014). The effects of antipsychotic switching on diabetes in chronic schizophrenia. Diabetic Medicine: A Journal Of The British Diabetic Association, 31(3), e16-e19. doi: /dme Attux, C., Martini, L. C., Elkis, H., Tamai, S., Freirias, A., Camargo, M.,... Bressan, R. A. (2013). A 6-month randomized controlled trial to test the efficacy of a lifestyle intervention for weight gain management in schizophrenia. BMC Psychiatry, 13, doi: / X Baker, A., Kay-Lambkin, F. J., Richmond, R., Filia, S., Castle, D., Williams, J., & Lewin, T. J. (2011). Study protocol: a randomised controlled trial investigating the effect of a healthy lifestyle intervention for people with severe mental disorders. BMC Public Health, 11(1), doi: /
56 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 56 Ballon, J. S., Pajvani, U., Freyberg, Z., Leibel, R. L., & Lieberman, J. A. (2014). Molecular pathophysiology of metabolic effects of antipsychotic medications. Trends Endocrinol Metab, 25(11), doi: /j.tem Balshem, H., Helfand, M., Schunemann, H. J., Oxman, A. D., Kunz, R., Brozek, J.,... Guyatt, G. H. (2011). GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol, 64(4), doi: /j.jclinepi Baptista, T., ElFakih, Y., Uzcategui, E., Sandia, I., Talamo, E., de Baptista, E. A., & Beaulieu, S. (2008). Pharmacological management of atypical antipsychotic-induced weight gain. CNS Drugs, 22(6), Baptista, T., Martínez, J., Lacruz, A., Rangel, N., Beaulieu, S., Serrano, A.,... Hernández, L. (2006). Metformin for prevention of weight gain and insulin resistance with olanzapine: a double-blind placebo-controlled trial. Canadian Journal Of Psychiatry. Revue Canadienne De Psychiatrie, 51(3), Baptista, T., Rangel, N., Fernández, V., Carrizo, E., El Fakih, Y., Uzcátegui, E.,... de Baptista, E. A. (2007). Metformin as an adjunctive treatment to control body weight and metabolic dysfunction during olanzapine administration: A multicentric, double-blind, placebocontrolled trial. Schizophrenia research, 93(1 3), doi: Barnes, T. R. E., Paton, C., Hancock, E., Cavanagh, M. R., Taylor, D., & Lelliott, P. (2008). Screening for the metabolic syndrome in community psychiatric patients prescribed antipsychotics: a quality improvement programme. Acta Psychiatrica Scandinavica, 118(1), doi: /j x Befort, C., Nazir, N., & Perri, M. (2012). Prevalence of obesity among adults from rural and
57 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 57 urban areas of the United States: findings from NHANES ( ). The Journal Of Rural Health: Official Journal Of The American Rural Health Association And The National Rural Health Care Association, 28(4), doi: /j x Berner, M. M., Hagen, M., & Kriston, L. (2007). Management of sexual dysfunction due to antipsychotic drug therapy. Cochrane Database of Systematic Reviews(1). doi: / CD pub2 Berwick, D. M. (2002). A user s manual for the IOM s Quality Chasm report. Health affairs, 21(3), Bhuvaneswar, C. G., Baldessarini, R. J., Harsh, V. L., & Alpert, J. E. (2009). Adverse Endocrine and Metabolic Effects of Psychotropic Drugs Selective Clinical Review. CNS Drugs, 23(12), Björkhem-Bergman, L., Asplund, A. B., & Lindh, J. D. (2011). Metformin for weight reduction in non-diabetic patients on antipsychotic drugs: a systematic review and meta-analysis. Journal of Psychopharmacology, 25(3), Blouin, M., Binet, M., Bouchard, R.-H., Roy, M.-A., Després, J.-P., & Alméras, N. (2009). Improvement of metabolic risk profile under second-generation antipsychotics: a pilot intervention study. Canadian Journal Of Psychiatry. Revue Canadienne De Psychiatrie, 54(4), Bobo, W. V., & Shelton, R. C. (2010). Efficacy, safety and tolerability of Symbyax (R) for acute-phase management of treatment-resistant depression. Expert Review of Neurotherapeutics, 10(5), doi: /ern Bonfioli, E., Berti, L., Goss, C., Muraro, F., & Burti, L. (2012). Health promotion lifestyle
58 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 58 interventions for weight management in psychosis: a systematic review and meta-analysis of randomised controlled trials. BMC Psychiatry, 12. doi: / x Braveman, P. A., Cubbin, C., Egerter, S., Williams, D. R., & Pamuk, E. (2010). Socioeconomic disparities in health in the United States: What the patterns tell us. American Journal Of Public Health, 100(S1), S186-S196. doi: /ajph Brooks, M. (2014). Top 100 most prescribed, top-selling drugs. Medscape. Retrieved from Brouwers, M. C., Kho, M. E., Browman, G. P., Burgers, J. S., Cluzeau, F., Feder, G.,... Hanna, S. E. (2010). AGREE II: advancing guideline development, reporting and evaluation in health care. Canadian Medical Association Journal, 182(18), E839-E842. Brown, S., & Mitchell, C. (2012). Predictors of death from natural causes in schizophrenia: 10- year follow-up of a community cohort. Social Psychiatry And Psychiatric Epidemiology, 47(6), doi: /s Brufani, C., Fintini, D., Nobili, V., Patera, P. I., Cappa, M., & Brufani, M. (2011). Use of metformin in pediatric age. Pediatric Diabetes, 12(6), doi: /j x Buchanan, R. W., Kreyenbuhl, J., Kelly, D. L., Noel, J. M., Boggs, D. L., Fischer, B. A.,... Keller, W. (2010). The 2009 Schizophrenia PORT Psychopharmacological Treatment Recommendations and Summary Statements. Schizophrenia Bulletin, 36(1), doi: /schbul/sbp116 Buckley, P. F. (2008). Factors that influence treatment success in schizophrenia. Journal of Clinical Psychiatry, 69, Buckley, P. F., & Correll, C. U. (2008). Strategies for dosing and switching antipsychotics for
59 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 59 optimal clinical management. J Clin Psychiatry, 69 Suppl 1, Bushe, C. J., Bradley, A. J., Doshi, S., & Karagianis, J. (2009). Changes in weight and metabolic parameters during treatment with antipsychotics and metformin: do the data inform as to potential guideline development? A systematic review of clinical studies. International Journal of Clinical Practice, 63(12), doi: /j x Carrizo, E., Fernández, V., Connell, L., Sandia, I., Prieto, D., Mogollón, J.,... Baptista, T. (2009). Extended release metformin for metabolic control assistance during prolonged clozapine administration: A 14 week, double-blind, parallel group, placebo-controlled study. Schizophrenia research, 113(1), doi: Cassano, G. B., Fagiolini, A., Lattanzi, L., Monteleone, P., Niolu, C., Sacchetti, E.,... Vita, A. (2007). Aripiprazole in the treatment of schizophrenia - A consensus report produced by schizophrenia experts in Italy. Clinical Drug Investigation, 27(1), doi: / Caulderwood, K. (2014). Maker of America's best-selling drug to lose billions as 'patent cliff' approaches Retrieved April 12, 2014, from Cefalu, W. T. (2012). Steps toward the meaningful translation of prevention strategies for type 2 diabetes. Diabetes Care, 35(4), Centers for Disease Control and Prevention. (2013). Obesity and overweight. Retrieved from Chawla, B., & Luxton-Andrew, H. (2008). Long-term weight loss observed with olanzapine orally disintegrating tablets in overweight patients with chronic schizophrenia. A 1 year
60 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 60 open-label, prospective trial. Human Psychopharmacology, 23(3), doi: /hup.921 Chen, C.-K., Chen, Y.-C., & Huang, Y.-S. (2009). Effects of a 10-week weight control program on obese patients with schizophrenia or schizoaffective disorder: a 12-month follow up. Psychiatry And Clinical Neurosciences, 63(1), doi: /j x Chen, Y., Bobo, W. V., Watts, K., Jayathilake, K., Tang, T., & Meltzer, H. Y. (2012). Comparative effectiveness of switching antipsychotic drug treatment to aripiprazole or ziprasidone for improving metabolic profile and atherogenic dyslipidemia: a 12-month, prospective, open-label study. Journal of Psychopharmacology, 26(9), doi: / Cimo, A., Stergiopoulos, E., Cheng, C., Bonato, S., & Dewa, C. S. (2012). Effective lifestyle interventions to improve type II diabetes self-management for those with schizophrenia or schizoaffective disorder: a systematic review. BMC Psychiatry, 12. doi: / x Citrome, L. (2007). The effectiveness criterion: Balancing efficacy against the risks of weight gain. Journal of Clinical Psychiatry, 68, Citrome, L. (2009). Using oral ziprasidone effectively: the food effect and dose-response. Advances in Therapy, 26(8), doi: /s Citrome, L. (2012). Lurasidone in Schizophrenia: New Information About Dosage and Place in Therapy. Advances in Therapy, 29(10), doi: /s Citrome, L., Blonde, L., & Damatarca, C. (2005). Metabolic issues in patients with severe mental illness. Southern Medical Journal, 98(7), doi:
61 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN /01.smj Citrome, L., Kalsekar, I., Baker, R. A., & Hebden, T. (2014). A review of real-world data on the effects of aripiprazole on weight and metabolic outcomes in adults. Current Medical Research and Opinion, 30(8), doi: / Citrome, L., & Vreeland, B. (2008). Schizophrenia, obesity, and antipsychotic medications: What can we do? Postgraduate Medicine, 120(2), doi: /pgm Cohn, T. A., & Sernyak, M. J. (2006). Metabolic monitoring for patients treated with antipsychotic medications. Canadian Journal of Psychiatry-Revue Canadienne De Psychiatrie, 51(8), Consumer Reports. (2012). The oral diabetes drugs treating type 2 diabetes: Comparing effectiveness, safety, and price. FINAL-Feb09.pdf Correll, C. U. (2010). Switching and combining antipsychotics. Cns Spectrums, 15(4), Correll, C. U., Lencz, T., & Malhotra, A. K. (2011). Antipsychotic drugs and obesity. Trends in Molecular Medicine, 17(2), doi: /j.molmed Correll, C. U., Sheridan, E. M., & DelBello, M. P. (2010). Antipsychotic and mood stabilizer efficacy and tolerability in pediatric and adult patients with bipolar I mania: a comparative analysis of acute, randomized, placebo-controlled trials. Bipolar Disorders, 12(2), doi: /j x Cousins, D. A., & Young, A. H. (2007). The armamentarium of treatments for bipolar disorder: a review of the literature. International Journal of Neuropsychopharmacology, 10(3), doi: /s
62 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 62 Cousins, D. A., & Young, A. H. (2007). The armamentarium of treatments for bipolar disorder: a review of the literature. International Journal of Neuropsychopharmacology, 10(3), doi: /s Croft, B., & Parish, S. L. (2013). Care Integration in the Patient Protection and Affordable Care Act: Implications for Behavioral Health. Administration and policy in mental health, 40(4), /s doi: /s Croxtall, J. D. (2012). Aripiprazole: A review of its use in the management of schizophrenia in adults. CNS Drugs, 26(2), Curtis, J., Newall, H., Myles, N., Shiers, D., & Samaras, K. (2012). Considering metformin in cardiometabolic protection in psychosis. Acta Psychiatrica Scandinavica, 126(4), doi: /j x De Fazio, P., Girardi, P., Maina, G., Mauri, M. C., Mauri, M., Monteleone, P.,... Rossi, A. (2010). Aripiprazole in Acute Mania and Long-Term Treatment of Bipolar Disorder A Critical Review by an Italian Working Group. Clinical Drug Investigation, 30(12), De Hert, M. Y. (2012). Body Weight and Metabolic Adverse Effects of Asenapine, Iloperidone, Lurasidone and Paliperidone in the Treatment of Schizophrenia and Bipolar Disorder. CNS Drugs, 26(9), De Hert, M., Correll, C. U., Bobes, J., Cetkovich-Bakmas, M., Cohen, D., Asai, I.,... Ndetei, D. M. (2011). Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry, 10(1), De Hert, M., Vancampfort, D., Correll, C. U., Mercken, V., Peuskens, J., Sweers, K.,... Mitchell, A. J. (2011). Guidelines for screening and monitoring of cardiometabolic risk in
63 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 63 schizophrenia: systematic evaluation. British Journal of Psychiatry, 199(2), doi: /bjp.bp Dell'Osso, B., & Ketter, T. A. (2013). Use of adjunctive stimulants in adult bipolar depression. International Journal of Neuropsychopharmacology, 16(1), doi: /s Diabetes Prevention Program Research Group. (2012). The 10-year cost-effectiveness of lifestyle intervention or metformin for diabetes prevention: an intent-to-treat analysis of the DPP/DPPOS. Diabetes Care, 35(4), doi: /dc DiBonaventura, M., Gabriel, S., Dupclay, L., Gupta, S., & Kim, E. (2012). A patient perspective of the impact of medication side effects on adherence: results of a cross-sectional nationwide survey of patients with schizophrenia. BMC Psychiatry, 12(1), 20. Dold, M., Li, C., Tardy, M., Khorsand, V., Gillies, D., & Leucht, S. (2012). Benzodiazepines for schizophrenia. Cochrane Database of Systematic Reviews, (11). doi: / cd pub2 Donohoe, M. (2008). Weighty matters: Public health aspects of the obesity epidemic; Part V-- treatments and public health approaches to combating the problem. Medscape Nurses. Retrieved from Edlinger, M., Baumgartner, S., Eltanaihi-Furtmuller, N., Hummer, M., & Fleischhacker, W. W. (2005). Switching between second-generation antipsychotics - Why and how? CNS Drugs, 19(1), doi: / Edwards, N. C., Pesa, J., Meletiche, D. M., Engelhart, L., Thompson, A. K., Sherr, J., & Dirani, R. (2008). One-year clinical and economic consequences of oral atypical antipsychotics
64 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 64 in the treatment of schizophrenia. Current Medical Research and Opinion, 24(12), doi: / Edwards, N. C., Pesa, J., Meletiche, D. M., Engelhart, L., Thompson, A. K., Sherr, J., & Dirani, R. (2008). One-year clinical and economic consequences of oral atypical antipsychotics in the treatment of schizophrenia. Current Medical Research and Opinion, 24(12), doi: / Ehret, M., Goethe, J., Lanosa, M., & Coleman, C. I. (2010). The effect of metformin on anthropometrics and insulin resistance in patients receiving atypical antipsychotic agents: a meta-analysis. J Clin Psychiatry, 71(10), doi: /JCP.09m05274yel Ellinger, L. K., Ipema, H. J., & Stachnik, J. M. (2010). Efficacy of metformin and topiramate in prevention and treatment of second-generation antipsychotic-induced weight gain. The Annals Of Pharmacotherapy, 44(4), doi: /aph.1M550 Essock, S. M., Covell, N. H., Davis, S. M., T Scott Stroup, M., Rosenheck, R. A., & Lieberman, J. A. (2006). Effectiveness of switching antipsychotic medications. The American journal of psychiatry, 163(12), Evans, S., Newton, R., & Higgins, S. (2005). Nutritional intervention to prevent weight gain in patients commenced on olanzapine: a randomized controlled trial. The Australian And New Zealand Journal Of Psychiatry, 39(6), Fagiolini, A., Forgione, R. N., Morana, B., Maccari, M., Goracci, A., Bossini, L.,... Casamassima, F. (2013). Asenapine for the treatment of manic and mixed episodes associated with bipolar I disorder: from clinical research to clinical practice. Expert Opinion on Pharmacotherapy, 14(4), doi: / Faulkner, G., & Cohn, T. A. (2006). Pharmacologic and nonpharmacologic strategies for weight
65 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 65 gain and metabolic disturbance in patients treated with antipsychotic medications. Canadian Journal of Psychiatry-Revue Canadienne De Psychiatrie, 51(8), Faulkner, G., Cohn, T., & Remington, G. (2007). Interventions to reduce weight gain in schizophrenia. Schizophrenia Bulletin, 33(3), doi: /schbul/sbm022 Fernandez-San-Martin, M. I., Martin-Lopez, L. M., Masa-Font, R., Olona-Tabuena, N., Roman, Y., Martin-Royo, J.,... Flores-Mateo, G. (2014). The effectiveness of lifestyle interventions to reduce cardiovascular risk in patients with severe mental disorders: metaanalysis of intervention studies. Community mental health journal, 50(1), doi: /s Fiedorowicz, J. G., Miller, D. D., Bishop, J. R., Calarge, C. A., Ellingrod, V. L., & Haynes, W. G. (2012). Systematic Review and Meta-analysis of Pharmacological Interventions for Weight Gain from Antipsychotics and Mood Stabilizers. Current psychiatry reviews, 8(1), doi: / Fitzpatrick, J. (2007). Finding the research for evidence-based practice: part two -- selecting credible evidence. Nursing Times, 103(18), Flier, J. S., & Maratos-Flier, E. (2008). Biology of Obesity. In A. S. Fauci (Ed.), Harrison's principles of internal medicine (17th ed., pp ). New York: McGraw- Hill Medical. Gabriele, J. M., Dubbert, P. M., & Reeves, R. R. (2009). Efficacy of behavioural interventions in managing atypical antipsychotic weight gain. Obesity Reviews, 10(4), doi: /j X x Gallego, J. A., Nielsen, J., De Hert, M., Kane, J. M., & Correll, C. U. (2012). Safety and tolerability of antipsychotic polypharmacy. Expert Opinion on Drug Safety, 11(4), 527-
66 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN doi: / Ganguli, R., Brar, J. S., Mahmoud, R., Berry, S. A., & Pandina, G. J. (2008). Assessment of strategies for switching patients from olanzapine to risperidone: a randomized, openlabel, rater-blinded study. BMC Medicine, 6, doi: / Gebhardt, S., Theisen, F., Haberhausen, M., Heinzel-Gutenbrunner, M., Wehmeier, P., Krieg, J., &... Hebebrand, J. (2010). Body weight gain induced by atypical antipsychotics: an extension of the monocygotic twin and sib pair study. Journal Of Clinical Pharmacy & Therapeutics, 35(2), doi: /j x Generali, J. A., & Cada, D. J. (2014). Topiramate: Antipsychotic-Induced Weight Gain. Hospital Pharmacy, 49(4), doi: /hpj Gierisch, J. M., Nieuwsma, J. A., Bradford, D. W., Wilder, C. M., Mann-Wrobel, M. C., McBroom, A. J.,... Williams, J. W., Jr. (2014). Pharmacologic and Behavioral Interventions to Improve Cardiovascular Risk Factors in Adults With Serious Mental Illness: A Systematic Review and Meta-Analysis. Journal of Clinical Psychiatry, 75(5), E424-E440. doi: /JCP.13r08558 Godleski, L. S., Goldsmith, L. J., Vieweg, W. V. R., Zettwoch, N., Stikovac, D., & Lewis, S. (2005). Switching depot antipsychotic drug responders to oral olanzapine. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 29(1), doi: /j.pnpbp Gopal, S., Gassmann-Mayer, C., Palumbo, J., Samtani, M. N., Shiwach, R., & Alphs, L. (2010). Practical guidance for dosing and switching paliperidone palmitate treatment in patients with schizophrenia. Current Medical Research and Opinion, 26(2), doi: /
67 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 67 Grande, I., Bernardo, M., Bobes, J., Saiz-Ruiz, J., Álamo, C., & Vieta, E. (2014). Antipsychotic switching in bipolar disorders: a systematic review. International Journal of Neuropsychopharmacology, 17(3), Greenberg, W. M., & Citrome, L. (2007). Ziprasidone for schizophrenia and bipolar disorder: A review of the clinical trials. Cns Drug Reviews, 13(2), doi: /j x Group, D. P. P. R. (2012). Long-term safety, tolerability, and weight loss associated with metformin in the Diabetes Prevention Program Outcomes Study. Diabetes Care, 35(4), Grün, F., & Blumberg, B. (2009). Endocrine disrupters as obesogens. Molecular & Cellular Endocrinology, 304(1/2), doi: /j.mce Guyatt, G. H., Oxman, A. D., Kunz, R., Atkins, D., Brozek, J., Vist, G.,... Schunemann, H. J. (2011). GRADE guidelines: 2. Framing the question and deciding on important outcomes. J Clin Epidemiol, 64(4), doi: /j.jclinepi Ha, E., Yim, S. V., Jung, K. H., Yoon, S. H., Zheng, L. T., Kim, M. J.,... Kim, J. W. (2006). Topiramate stimulates glucose transport through AMP-activated protein kinase-mediated pathway in L6 skeletal muscle cells. The Pharmacogenomics Journal, 6(5), Hall, E., & Burt, V. K. (2012). Male fertility: psychiatric considerations. Fertility and Sterility, 97(2), doi: /j.fertnstert Happell, B., Davies, C., & Scott, D. (2012). Health behaviour interventions to improve physical health in individuals diagnosed with a mental illness: A systematic review. International Journal Of Mental Health Nursing, 21(3), Hasan, A., Falkai, P., Wobrock, T., Lieberman, J., Glenthoj, B., Gattaz, W. F.,... Möller, H.-J.
68 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 68 (2013). World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of schizophrenia, part 2: update 2012 on the long-term treatment of schizophrenia and management of antipsychotic-induced side effects. World Journal of Biological Psychiatry, 14(1), Hasnain, M., Fredrickson, S. K., & Vieweg, W. V. R. (2011). Metformin for obesity and glucose dysregulation in patients with schizophrenia receiving antipsychotic drugs. Journal of Psychopharmacology, 25(6), doi: / Hasnain, M., & Vieweg, W. V. R. (2013). Weight considerations in psychotropic drug prescribing and switching. Postgraduate Medicine, 125(5), doi: /pgm Hasnain, M., Vieweg, W. V. R., & Hollett, B. (2012). Weight gain and glucose dysregulation with second-generation antipsychotics and antidepressants: A review for primary care physicians. Postgraduate Medicine, 124(4), doi: /pgm Hawley, C., Turner, M., Latif, M. A., Curtis, V., Saleem, P. T., & Wilton, K. (2010). Switching stable patients with schizophrenia from depot and oral antipsychotics to long-acting injectable risperidone: reasons for switching and safety. Human Psychopharmacology, 25(1), doi: /hup.1085 Hellerstein, D. J., Almeida, G., Devlin, M. J., Mendelsohn, N., Helfand, S., Dragatsi, D.,... Capitelli, L. (2007). Assessing obesity and other related health problems of mentally ill Hispanic patients in an urban outpatient setting. The Psychiatric Quarterly, 78(3), Hester, E. K., & Thrower, M. R. (2005). Current options in the management of olanzapineassociated weight gain. Annals of Pharmacotherapy, 39(2), doi:
69 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN /aph.1D423 Higashi, K., Medic, G., Littlewood, K. J., Diez, T., Granström, O., & De Hert, M. (2013). Medication adherence in schizophrenia: factors influencing adherence and consequences of nonadherence, a systematic literature review. Therapeutic Advances in Psychopharmacology, 3(4), doi: / Hjorth, P., Davidsen, A. S., Kilian, R., & Skrubbeltrang, C. (2014). A systematic review of controlled interventions to reduce overweight and obesity in people with schizophrenia. Acta Psychiatrica Scandinavica, 130(4), doi: /acps Holland, K. (2014). The cost of epilepsy medications. Retrieved April 12, 2015, from Hong, J., Novick, D., Brugnoli, R., Karagianis, J., Dossenbach, M., & Haro, J. M. (2012). Clinical consequences of switching from olanzapine to risperidone and vice versa in outpatients with schizophrenia: 36-month results from the Worldwide Schizophrenia Outpatients Health Outcomes (W-SOHO) study. BMC Psychiatry, 12, doi: / X Institute for Clinical Systems Improvement. (2015). Reviewing evidence using GRADE. Retrieved from Ishitobi, M., Kosaka, H., Takahashi, T., Yatuga, C., Asano, M., Tanaka, Y.,... Wada, Y. (2013). Effectiveness and tolerability of switching to aripiprazole From risperidone in subjects with autism spectrum disorders: A prospective open-label study. Clinical Neuropharmacology, 36(5), doi: /WNF.0b013e3182a31ec0 Johnstone, R., Nicol, K., Donaghy, M., & Lawrie, S. (2009). Barriers to uptake of physical
70 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 70 activity in community-based patients with schizophrenia. Journal of Mental Health, 18(6), doi: / Jumpertz, R., Le, D., Turnbaugh, P., Trinidad, C., Bogardus, C., Gordon, J., & Krakoff, J. (2011). Energy-balance studies reveal associations between gut microbes, caloric load, and nutrient absorption in humans. The American Journal Of Clinical Nutrition, 94(1), doi: /ajcn Kantrowitz, J. T., & Citrome, L. (2008). Olanzapine: review of safety Expert Opinion on Drug Safety, 7(6), doi: / Karagianis, J., Hoffmann, V. P., Arranz, B., Treue, T., Maguire, G. A., de Haan, L., & Chawla, B. (2008). Orally disintegrating olanzapine and potential differences in treatmentemergent weight gain. Human Psychopharmacology-Clinical and Experimental, 23(4), doi: /hup.933 Khazaal, Y., Fresard, E., Rabia, S., Chatton, A., Rothen, S., Pomini, V.,... Zullino, D. (2007). Cognitive behavioural therapy for weight gain associated with antipsychotic drugs. Schizophrenia research, 91(1), Kim, S.-W., Shin, I.-S., Kim, J.-M., Bae, K.-Y., Yang, S.-J., & Yoon, J.-S. (2010). Effectiveness of switching From aripiprazole to ziprasidone in patients with schizophrenia. Clinical Neuropharmacology, 33(3), doi: /WNF.0b013e3181d52b85 Kim, S.-W., Shin, I.-S., Kim, J.-M., Lee, S.-H., Lee, Y.-H., Yang, S.-J., & Yoon, J.-S. (2009). Effects of switching to long-acting injectable risperidone from oral atypical antipsychotics on cognitive function in patients with schizophrenia. Human Psychopharmacology, 24(7), doi: /hup.1057 Ko, Y.-H., Joe, S.-H., Jung, I.-K., & Kim, S.-H. (2005). Topiramate as an adjuvant treatment
71 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 71 with atypical antipsychotics in schizophrenic patients experiencing weight gain. Clinical Neuropharmacology, 28(4), Kramer, C., Leitao, C., Pinto, L., Canani, L., Azevedo, M., & Gross, J. (2011). Efficacy and safety of topiramate on weight loss: a meta analysis of randomized controlled trials. Obesity Reviews, 12(5), e338-e347. Kwon, J. S., Choi, J.-S., Bahk, W.-M., Yoon, K. C., Hyung, K. C., Chul, S. Y.,... Geun, O. C. (2006). Weight management program for treatment-emergent weight gain in olanzapinetreated patients with schizophrenia or schizoaffective disorder: A 12-week randomized controlled clinical trial. J Clin Psychiatry, 67(4), Lachin, J. M., Christophi, C. A., Edelstein, S. L., Ehrmann, D. A., Hamman, R. F., Kahn, S. E.,... Nathan, D. M. (2007). Factors associated with diabetes onset during metformin versus placebo therapy in the diabetes prevention program. Diabetes, 56(4), Larson, N. I., Story, M. T., & Nelson, M. C. (2009). Neighborhood Environments: Disparities in Access to Healthy Foods in the U.S. American Journal Of Preventive Medicine, 36(1), doi: /j.amepre Lee, H.-B., Yoon, B.-H., Kwon, Y.-J., Woo, Y. S., Lee, J.-G., Kim, M.-D., & Bahk, W.-M. (2013). The efficacy and safety of switching to ziprasidone from olanzapine in patients with bipolar I disorder: an 8-week, multicenter, open-label study. Clinical Drug Investigation, 33(10), doi: /s y Lee, Y. J., & Jeong, J. H. (2011). A systematic review of metformin to limit weight-gain with atypical antipsychotics. Journal Of Clinical Pharmacy And Therapeutics, 36(5), doi: /j Lett, T. A. P., Wallace, T. J. M., Chowdhury, N. I., Tiwari, A. K., Kennedy, J. L., &
72 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 72 Müller, D. J. (2011). Pharmacogenetics of antipsychotic-induced weight gain: review and clinical implications. Molecular psychiatry, 17(3), Leucht, S., Cipriani, A., Spineli, L., Mavridis, D., Örey, D., Richter, F.,... Geddes, J. R. (2013). Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. The Lancet, 382(9896), Levri, K. M., Slaymaker, E., Last, A., Yeh, J., Ference, J., D'Amico, F., & Wilson, S. A. (2005). Metformin as treatment for overweight and obese adults: a systematic review. Annals Of Family Medicine, 3(5), Ley, R., Turnbaugh, P., Klein, S., & Gordon, J. (2006). Microbial ecology: human gut microbes associated with obesity. Nature, 444(7122), Liauw, S. S., & McIntyre, R. S. (2010). Atypical antipsychotic tolerability and switching strategies in bipolar disorder. Expert Opinion on Pharmacotherapy, 11(17), doi: / Lillycrop, K. A., & Burdge, G. C. (2011). Epigenetic changes in early life and future risk of obesity. International Journal Of Obesity, 35(1), doi: /ijo Lin, C.-C., Bai, Y.-M., Wang, Y.-C., Chen, T.-T., Lai, I.-C., Chen, J.-Y.,... Liou, Y.-J. (2009). Improved body weight and metabolic outcomes in overweight or obese psychiatric patients switched to amisulpride from other atypical antipsychotics. J Clin Psychopharmacol, 29(6), Lin, Y.-H., Liu, C.-Y., & Hsiao, M.-C. (2005). Management of atypical antipsychotic-induced weight gain in schizophrenic patients with topiramate. Psychiatry And Clinical Neurosciences, 59(5), Lomangino, K. (2006). Gut microbes seen as potential obesity risk factor. Nutrition &
73 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 73 The M.D, 32(8), 7-8. Lu, Z., Hu, J., Chen, C.-K., Lan, T.-H., Diokno, G. L., Jr., Lee, B. Y.,... Ang, Q. (2007). Effectiveness and safety of olanzapine in the treatment of schizophrenia among Asian patients switching from conventional antipsychotics. Progress in Neuro- Psychopharmacology & Biological Psychiatry, 31(1), doi: /j.pnpbp Maayan, L., & Correll, C. U. (2010). Management of antipsychotic-related weight gain. Expert Review of Neurotherapeutics, 10(7), doi: /ern Maayan, L., Vakhrusheva, J., & Correll, C. U. (2010). Effectiveness of medications used to attenuate antipsychotic-related weight gain and metabolic abnormalities: a systematic review and meta-analysis. Neuropsychopharmacology, 35(7), Mahmood, S., Booker, I., Huang, J., & Coleman, C. I. (2013). Effect of topiramate on weight gain in patients receiving atypical antipsychotic agents. J Clin Psychopharmacol, 33(1), doi: /JCP.0b013e31827cb2b7 Martinez-Ortega, J., Funes-Godoy, S., Diaz-Atienza, F., Gutierrez-Rojas, L., Perez-Costillas, L., & Gurpegui, M. (2013). Weight gain and increase of body mass index among children and adolescents treated with antipsychotics: a critical review. European Child & Adolescent Psychiatry, 22(8), doi: /s McCloughen, A., & Foster, K. (2011). Weight gain associated with taking psychotropic medication: An integrative review. International Journal Of Mental Health Nursing, 20(3), McCreadie, R. G., Kelly, C., Connolly, M., Williams, S., Baxter, G., Lean, M., & Paterson, J. R. (2005). Dietary improvement in people with schizophrenia: Randomised controlled trial.
74 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 74 The British Journal of Psychiatry, 187(4), McElroy, S. L., Frye, M. A., Altshuler, L. L., Suppes, T., Hellemann, G., Black, D.,... Keck, P. E., Jr. (2007). A 24-week, randomized, controlled trial of adjunctive sibutramine versus topiramate in the treatment of weight gain in overweight or obese patients with bipolar disorders. Bipolar Disorders, 9(4), McEwen, B. S. (2008). Central effects of stress hormones in health and disease: Understanding the protective and damaging effects of stress and stress mediators. European Journal Of Pharmacology, 583(2/3), doi: /j.ejphar McIntyre, R. S., Alsuwaidan, M., Goldstein, B. I., Taylor, V. H., Schaffer, A., Beaulieu, S., & Kemp, D. E. (2012). The Canadian Network for Mood and Anxiety Treatments (CANWAT) task force recommendations for the management of patients with mood disorders and comorbid metabolic disorders. Annals of Clinical Psychiatry, 24(1), McKibbin, C. L., Patterson, T. L., Norman, G., Patrick, K., Jin, H., Roesch, S.,... Jeste, D. V. (2006). A lifestyle intervention for older schizophrenia patients with diabetes mellitus: A randomized controlled trial. Schizophrenia research, 86(1 3), doi: McMaster University. (2014). GRADEpro. [Computer program on Version [2015]. Mechanic, D. (2014). More people than ever before are receiving behavioral health care in the United States, but gaps and challenges remain. Health Aff (Millwood), 33(8), doi: /hlthaff Medved, V., Jovanovic, N., & Knapic, V. P. (2009). THE COMORBIDITY OF DIABETES
75 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 75 MELLITUS AND PSYCHIATRIC DISORDERS. Psychiatria Danubina, 21(4), Meyer, J. M., Pandina, G., Bossie, C. A., Turkoz, I., & Greenspan, A. (2005). Effects of switching from olanzapine to risperidone on the prevalence of the metabolic syndrome in overweight or obese patients with schizophrenia or schizoaffective disorder: analysis of a multicenter, rater-blinded, open-label study. Clinical therapeutics, 27(12), Mizuno, Y., Suzuki, T., Nakagawa, A., Yoshida, K., Mimura, M., Fleischhacker, W. W., & Uchida, H. (2014). Pharmacological strategies to counteract antipsychotic-induced weight gain and metabolic adverse effects in schizophrenia: a systematic review and meta-analysis. Schizophrenia Bulletin, sbu030. Montes, J. M., Rodriguez, J. L., Balbo, E., Sopelana, P., Martin, E., Soto, J. A.,... Villardaga, I. (2007). Improvement in antipsychotic-related metabolic disturbances in patients with schizophrenia switched to ziprasidone. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 31(2), doi: /j.pnpbp Moran, K. (2014). The doctor of nursing practice scholarly project: A framework for success. Burlington, Mass.: Jones & Bartlett Learning. Mukundan, A., Faulkner, G., Cohn, T., & Remington, G. (2010). Antipsychotic switching for people with schizophrenia who have neuroleptic-induced weight or metabolic problems. In The Cochrane Collaboration & A. Mukundan (Eds.), Cochrane Database of Systematic Reviews. Chichester, UK: John Wiley & Sons, Ltd. Retrieved from Narula, P. K., Rehan, H. S., Unni, K. E. S., & Gupta, N. (2010). Topiramate for prevention of olanzapine associated weight gain and metabolic dysfunction in schizophrenia: A double-
76 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 76 blind, placebo-controlled trial. Schizophrenia research, 118(1 3), doi: Newall, H., Myles, N., Ward, P. B., Samaras, K., Shiers, D., & Curtis, J. (2012). Efficacy of metformin for prevention of weight gain in psychiatric populations: a review. International clinical psychopharmacology, 27(2), Newcomer, J. W., Campos, J. A., Marcus, R. N., Breder, C., Berman, R. M., Kerselaers, W.,... McQuade, R. D. (2008). A multicenter, randomized, double-blind study of the effects of aripiprazole in overweight subjects with schizophrenia or schizoaffective disorder switched from olanzapine. Journal of Clinical Psychiatry, 69(7), Newcomer, J. W., Weiden, P. J., & Buchanan, R. W. (2013). Switching antipsychotic medications to reduce adverse event burden in schizophrenia: Establishing evidencebased practice. Journal of Clinical Psychiatry, 74(11), doi: /JCP.12028ah1 Nyhuis, A. W., Faries, D. E., Ascher-Svanum, H., Stauffer, V. L., & Kinon, B. J. (2010). Predictors of switching antipsychotic medications in the treatment of schizophrenia. BMC Psychiatry, 10, doi: / X Ohlsen, R. I., Peacock, G., & Smith, S. (2005). Developing a service to monitor and improve physical health in people with serious mental illness. Journal Of Psychiatric And Mental Health Nursing, 12(5), Olfson, M., Blanco, C., Liu, S., Wang, S., & Correll, C. U. (2012). National trends in the officebased treatment of children, adolescents, and adults with antipsychotics. Archives Of General Psychiatry, 69(12), doi: /archgenpsychiatry Olfson, M., Kroenke, K., Wang, S., & Blanco, C. (2014). Trends in office-based mental health
77 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 77 care provided by psychiatrists and primary care physicians. The Journal Of Clinical Psychiatry, 75(3), doi: /jcp.13m08834 Pae, C.-U., Serretti, A., Chiesa, A., Mandelli, L., Lee, C., Lee, C.,... Paik, I.-H. (2009). Immediate versus gradual suspension of previous treatments during switch to aripiprazole: results of a randomized, open label study. European Neuropsychopharmacology, 19(8), Pan, L., Sherry, B., Njai, R., & Blanck, H. M. (2012). Food insecurity is associated with obesity among US adults in 12 states. Journal Of The Academy Of Nutrition & Dietetics, 112(9), doi: /j.jand Pani, L., Villagran, J. M., Kontaxakis, V. P., & Alptekin, K. (2008). Practical issues with amisulpride in the management of patients with schizophrenia. Clinical Drug Investigation, 28(8), Pearsall, R., Smith, D. J., Pelosi, A., & Geddes, J. (2014). Exercise therapy in adults with serious mental illness: a systematic review and meta-analysis. BMC Psychiatry, 14. doi: / x Porsdal, V., Beal, C., Kleivenes, O. K., Martinsen, E. W., Lindström, E., Nilsson, H., & Svanborg, P. (2010). The Scandinavian Solutions for Wellness study - a two-arm observational study on the effectiveness of lifestyle intervention on subjective well-being and weight among persons with psychiatric disorders. BMC Psychiatry, 10, doi: / X Poulin, M. J., Chaput, J. P., Simard, V., Vincent, P., Bernier, J., Gauthier, Y.,... Tremblay, A. (2007). Management of antipsychotic-induced weight gain: prospective naturalistic study of the effectiveness of a supervised exercise programme. Australian & New Zealand
78 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 78 Journal of Psychiatry, 41(12), Praharaj, S. K., & Sharma, P. S. V. N. (2012). Amantadine for olanzapine-induced weight gain: a systematic review and meta-analysis of randomized placebo-controlled trials. Therapeutic Advances in Psychopharmacology, 2(4), doi: / Puhl, R. M., & Heuer, C. A. (2009). The stigma of obesity: A review and update. Obesity, 17(5), Purnell, T. S., Joy, S., Little, E., Bridges, J. F. P., & Maruthur, N. (2014). Patient preferences for noninsulin diabetes medications: a systematic review. Diabetes Care, 37(7), doi: /dc Rege, S. (2008). Antipsychotic induced weight gain in schizophrenia: mechanisms and management. Australian and New Zealand Journal of Psychiatry, 42(5), doi: / Ren-Rong Wu, M. D., Jing-Ping Zhao, M. D., Xiao-Feng Guo, M. D., Yi-Qun He, M. D., Mao-Sheng Fang, M. D., Wen-Bin Guo, M. D.,... Le-Hua Li, M. D. (2008). Metformin addition attenuates olanzapine-induced weight gain in drug-naive first-episode schizophrenia patients: A double-blind, placebo-controlled study. American Journal of Psychiatry, 165(3), doi: doi: /appi.ajp Reynolds, G. P., & Kirk, S. L. (2010). Metabolic side effects of antipsychotic drug treatment pharmacological mechanisms. Pharmacology & Therapeutics, 125(1), doi: /j.pharmthera Review Manager (RevMan5) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
79 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 79 Ried, L. D., Renner, B. T., McConkey, J. R., Bengtson, M. A., & Lopez, L. M. (2006). Increased cardiovascular risk with second-generation antipsychotic agent switches. Journal of the American Pharmacists Association, 46(4), doi: / Roberts, S. H., & Bailey, J. E. (2011). Incentives and barriers to lifestyle interventions for people with severe mental illness: a narrative synthesis of quantitative, qualitative and mixed methods studies. Journal Of Advanced Nursing, 67(4), doi: /j x Roerig, J. L. S. K. J. M. J. E. (2011). Atypical antipsychotic-induced weight gain. CNS Drugs, 25(12), Roffeei, S. N., Reynolds, G. P., Zainal, N. Z., Said, M. A., Hatim, A., Aida, S. A., & Mohamed, Z. (2014). Association of ADRA2A and MTHFR gene polymorphisms with weight loss following antipsychotic switching to aripiprazole or ziprasidone. Human Psychopharmacology, 29(1), doi: /hup.2366 Rosa, F., Schreiner, A., Thomas, P., & Sherif, T. (2012). Switching patients with stable schizophrenia or schizoaffective disorder from olanzapine to risperidone long-acting injectable. Clinical Drug Investigation, 32(4), doi: / Rosenheck, R. A., Davis, S., Covell, N., Essock, S., Swartz, M., Stroup, S.,... Lieberman, J. (2009). Does switching to a new antipsychotic improve outcomes?: Data from the CATIE trial. Schizophrenia research, 107(1), Roskam, A., Kunst, A., Van Oyen, H., Demarest, S., Klumbiene, J., Regidor, E., &... Mackenbach, J. (2010). Comparative appraisal of educational inequalities in overweight and obesity among adults in 19 European countries. International Journal Of
80 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 80 Epidemiology, 39(2), doi: /ije/dyp329 Rossi, A., Bagalà, A., Del Curatolo, V., Scapati, F., Bernareggi, M. M., & Giustra, M. G. (2009). Remission in schizophrenia: one-year Italian prospective study of risperidone long-acting injectable (RLAI) in patients with schizophrenia or schizoaffective disorder. Human Psychopharmacology, 24(7), doi: /hup.1067 Rummel-Kluge, C., Komossa, K., Schwarz, S., Hunger, H., Schmid, F., Lobos, C. A.,... Leucht, S. (2010). Head-to-head comparisons of metabolic side effects of second generation antipsychotics in the treatment of schizophrenia: a systematic review and meta-analysis. Schizophrenia research, 123(2), Samtani, M. N., Gopal, S., Gassmann-Mayer, C., Alphs, L., & Palumbo, J. M. (2011). Dosing and switching strategies for paliperidone palmitate based on population pharmacokinetic modelling and clinical trial data. CNS Drugs, 25(10), Schorr, S. G., Slooff, C. J., Postema, R., Van Oven, W., Schilthuis, M., Bruggeman, R., & Taxis, K. (2008). A 12-month follow-up study of treating overweight schizophrenic patients with aripiprazole. Acta Psychiatrica Scandinavica, 118(3), doi: /j x Schunemann, H., Ahmed, F., & Morgan, R. (2011). Guideline development using GRADE. Centers for Disease Control and Prevention. Retrieved from Seeman, M. V. (2008). Prevention inherent in services for women with schizophrenia. Canadian Journal Of Psychiatry. Revue Canadienne De Psychiatrie, 53(5), Selassie, A., Snipe, L., Focht, K. L., & Welldaregay, W. (2013). Baseline prevalence of heart diseases, hypertension, diabetes, and obesity in persons with acute traumatic spinal cord
81 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 81 injury: Potential threats in the recovery trajectory. Topics In Spinal Cord Injury Rehabilitation, 19(3), doi: /sci Sendt, K.-V., Tracy, D. K., & Bhattacharyya, S. (2015). A systematic review of factors influencing adherence to antipsychotic medication in schizophrenia-spectrum disorders. Psychiatry research, 225(1), Sharma, E., Rao, N. P., & Venkatasubramanian, G. (2014). Association between antipsychoticinduced metabolic side-effects and clinical improvement: a review on the Evidence for "metabolic threshold". Asian J Psychiatr, 8, doi: /j.ajp Shin, L., Bregman, H., Frazier, J., & Noyes, N. (2008). An overview of obesity in children with psychiatric disorders taking atypical antipsychotics. Harvard Review Of Psychiatry, 16(2), doi: / Shrivastava, A., & Johnston, M. E. (2010). Weight-gain in psychiatric treatment: Risks, implications, and strategies for prevention and management. Mens Sana Monographs, 8(1), doi: / Speakman, J., & O'Rahilly, S. (2012). Fat: an evolving issue. Disease Models & Mechanisms, 5(5), Stevens, K. R. (2004). ACE Star Model of EBP: Knowledge Transformation. Academic Center for Evidence-based Practice. The University of Texas Health Science Center at San Antonio. Retrieved from Stevens, K. R. (2012). ACE Star Model of EBP: Knowledge Transformation. Academic Center for Evidence-Based Practice. The University of Texas Health Science Center San Antonio. Stevens, K. R. (2013) The impact of evidence-based practice in nursing and the next big ideas.
82 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 82 Online Journal Of Issues In Nursing, 18(2), 1. doi: /ojin.vol18no02man04 Stroup, T. S., McEvoy, J. P., Ring, K. D., Hamer, R. H., LaVange, L. M., Swartz, M. S.,... Schizophrenia Trials, N. (2011). A randomized trial examining the effectiveness of switching from olanzapine, quetiapine, or risperidone to aripiprazole to reduce metabolic risk: comparison of antipsychotics for metabolic problems (CAMP). The American journal of psychiatry, 168(9), doi: /appi.ajp Suttajit, S., Srisurapanont, M., Maneeton, N., & Maneeton, B. (2014). Quetiapine for acute bipolar depression: a systematic review and meta-analysis. Drug Design Development and Therapy, 8, doi: /dddt.s63779 Suzuki, Y., Sugai, T., Fukui, N., Watanabe, J., Ono, S., Tsuneyama, N.,... Someya, T. (2012). Quetiapine-induced insulin resistance after switching from blonanserin despite a loss in both bodyweight and waist circumference. Psychiatry And Clinical Neurosciences, 66(6), doi: /j x Tai-Seale, T., & Chandler, C. (2003) Nutrition and overweight concerns in rural areas: A literature review. Rural Healthy People 2010: A Companion Document to Healthy People Volume 2. Texas A&M University System Health Science Center, School of Rural Public Health, Southwest Rural Health Research Center, College Station, TX. Takeuchi, H., Uchida, H., Suzuki, T., Watanabe, K., & Kashima, H. (2010). Changes in metabolic parameters following a switch to aripiprazole in Japanese patients with schizophrenia: One-year follow-up study. Psychiatry And Clinical Neurosciences, 64(1), doi: /j x Tanaka, K., Morinobu, S., Ichimura, M., Asakawa, A., Inui, A., Hosoda, H.,... Yamawaki, S. (2008). Decreased levels of ghrelin, cortisol, and fasting blood sugar, but not n-
83 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 83 octanoylated ghrelin, in Japanese schizophrenic inpatients treated with olanzapine. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 32(6), doi: /j.pnpbp Taylor, V. H., Mclntyre, R. S., Remington, G., Levitan, R. D., Stonehocker, B., & Sharma, A. M. (2012). Beyond pharmacotherapy: Understanding the links between obesity and chronic mental illness. Canadian Journal Of Psychiatry, 57(1), Thayer, K. A., Heindel, J. J., Bucher, J. R., & Gallo, M. A. (2012). Role of environmental chemicals in diabetes and obesity: A national toxicology program workshop review. Environmental Health Perspectives, 120(6), doi: /ehp University of Washington. (2011). Evidence-based practice tools. University of Washington Health Sciences Library. Retrieved from Usher, K., Park, T., & Foster, K. (2013). The experience of weight gain as a result of taking second-generation antipsychotic medications: the mental health consumer perspective. Journal Of Psychiatric & Mental Health Nursing, 20(9), doi: /jpm Usher, K., Park, T., Foster, K., & Buettner, P. (2012). A randomized controlled trial undertaken to test a nurse-led weight management and exercise intervention designed for people with serious mental illness who take second generation antipsychotics. Journal of Advanced Nursing, n/a n/a. doi: /jan Vandyk, A. D., & Baker, C. (2012). Qualitative descriptive study exploring schizophrenia and the everyday effect of medication-induced weight gain. International Journal Of Mental Health Nursing, 21(4), doi: /j x Verhaeghe, N., De Maeseneer, J., Maes, L., Van Heeringen, C., & Annemans, L. (2011).
84 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 84 Effectiveness and cost-effectiveness of lifestyle interventions on physical activity and eating habits in persons with severe mental disorders: A systematic review. International Journal of Behavioral Nutrition and Physical Activity, 8. doi: / Verma, S., Subramaniam, M., Abdin, E., Sim, K., Su, A., Lee, N., & Chong, S. A. (2010). Safety and efficacy of long-acting injectable risperidone in patients with schizophrenia spectrum disorders: a 6-month open-label trial in Asian patients. Human Psychopharmacology, 25(3), doi: /hup.1104 Vieweg, W. V. R., Sood, A. B., Pandurangi, A., & Silverman, J. J. (2005). Newer antipsychotic drugs and obesity in children and adolescents. How should we assess drug-associated weight gain? Acta Psychiatrica Scandinavica, 111(3), doi: /j x Wang, M., Tong, J.-h., Zhu, G., Liang, G.-m., Yan, H.-f., & Wang, X.-z. (2012). Metformin for treatment of antipsychotic-induced weight gain: A randomized, placebo-controlled study. Schizophrenia research, 138(1), doi: Wang, S.-M., Han, C., Lee, S.-J., Patkar, A. A., Masand, P. S., & Pae, C.-U. (2014). Schizophrenia relapse and the clinical usefulness of once-monthly aripiprazole depot injection. Neuropsychiatric Disease and Treatment, 10, doi: /ndt Weber, M., Gutierrez, A. M., & Mohammadi, M. (2009). The risks and benefits of switching antipsychotics: a case study approach. Perspectives In Psychiatric Care, 45(1), doi: /j x Weber, M., & Wyne, K. (2006). A cognitive/behavioral group intervention for weight loss in
85 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 85 patients treated with atypical antipsychotics. Schizophrenia research, 83(1), doi: Wehmeier, P. M., Kluge, M., Schneider, E., Schacht, A., Wagner, T., & Schreiber, W. (2007). Quality of life and subjective well-being during treatment with antipsychotics in outpatients with schizophrenia. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 31(3), doi: /j.pnpbp Weiden, P. J. (2007). Switching antipsychotics as a treatment strategy for antipsychotic-induced weight gain and dyslipidemia. Journal of Clinical Psychiatry, 68, Weiden, P. J., Mackell, J. A., & McDonnell, D. D. (2004). Obesity as a risk factor for antipsychotic noncompliance. Schizophrenia research, 66(1), Weiden, P. J., Newcomer, J. W., Loebel, A. D., Yang, R., & Lebovitz, H. E. (2008). Long-term changes in weight and plasma lipids during maintenance treatment with ziprasidone. Neuropsychopharmacology, 33(5), Weiden, P. J., Preskorn, S. H., Fahnestock, P. A., Carpenter, D., Ross, R., & Docherty, J. P. (2007). Translating the psychopharmacology of antipsychotics to individualized treatment for severe mental illness: A roadmap. Journal of Clinical Psychiatry, 68, Wen, M., & Kowaleski-Jones, L. (2012). The built environment and risk of obesity in the United States: Racial-ethnic disparities. Health & Place, 18(6), doi: /j.healthplace Williams, J., Crockett, D., Harrison, R., & Thomas, K. (2012). The role of food culture and marketing activity in health disparities. Preventive Medicine, 55(5), doi: /j.ypmed White, W., Elmore, L., Luthin, D. R., & Cates, M. E. (2013). Psychotropic-induced weight gain:
86 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 86 A review of management strategies. Consultant ( ), 53(3), World Health Organization. (2012). WHO Handbook for guideline development. Retrieved from Wu, R., Zhao, J.-P., Jin, H., Shao, P., Fang, M.-S., Guo, X.-F., Li, L.-H. (2008). Lifestyle intervention and metformin for treatment of antipsychotic-induced weight gain. JAMA: the journal of the American Medical Association, 299(2), Xiao, S., Baker, C., & Oyewumi, L. K. (2012). Psychosocial processes influencing weight management among persons newly prescribed atypical antipsychotic medications. Journal of Psychiatric and Mental Health Nursing, 19(3), doi: /j Yarborough, B. J. H., Leo, M. C., Stumbo, S., Perrin, N. A., & Green, C. A. (2013). STRIDE: a randomized trial of a lifestyle intervention to promote weight loss among individuals taking antipsychotic medications. BMC Psychiatry, 13, doi: / X Ye, W., Fujikoshi, S., Nakahara, N., Takahashi, M., Ascher-Svanum, H., & Ohmori, T. (2012). Improved outcomes following a switch to olanzapine treatment from risperidone treatment in a 1-year naturalistic study of schizophrenia patients in Japan. Psychiatry And Clinical Neurosciences, 66(4), doi: /j x Yearwood, E. L., McCulloch, M. R., Tucker, M. L., & Riley, J. B. (2011). Care of the patient with Prader-Willi syndrome. MEDSURG Nursing, 20(3), Young, S. L., Taylor, M., & Lawrie, S. M. (2014). First do no harm. A systematic review of the prevalence and management of antipsychotic adverse effects. Journal of Psychopharmacology,
87 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 87 Appendix A List of Second-Generation Antipsychotics Aripiprazole Asenapine Clozapine Iloperidone Lurasidone Olanzapine Paliperidone Quetiapine Risperidone Ziprasidone
88 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 88 Appendix B Summary of GRADE method for rating importance of study outcomes (Guyatt, et al., 2011). Reproduced with permission.
89 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 89 Appendix C Summary of the GRADE approach to rating quality of evidence (Balshem et al., 2011). Initial Rating of Quality of Evidence HIGH Randomized Trials LOW Observational Studies Criteria for Rating Evidence HIGHER Large Effect +1 Large +2 Very large Dose Response +1 Evidence of a gradient Residual Confounding +1 Would reduce demonstrated effect +1 Would suggest a spurious effect if no effect was observed Criteria for Rating Evidence LOWER Risk of Bias -1 Serious -2 Very serious Inconsistency -1 Serious -2 Very serious Indirectness -1 Serious -2 Very serious Imprecision -1 Serious -2 Very serious Publication Bias -1 Likely -2 Very likely Significance of Overall Quality of Evidence Quality Level Symbol Definition HIGH We are very confident that the true effect lies close to that of the estimate of the effect MODERATE We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different LOW Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect VERY LOW We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect
90 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 90 Appendix D Risk of Bias Summaries Figure D1: Risk of bias summary for medication switching studies.
91 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 91 Figure D2: Risk of bias summary for adjunct medication studies. Figure D3: Risk of bias summary for cognitive behavioral studies.
92 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 92 Appendix E Forest Plots According to Intervention and Outcomes Figure E1: Forest plot comparison: Medication switching, outcome weight loss. Figure E2: Forest plot comparison: Medication switching, outcome global state. Figure E3: Forest plot comparison: Medication switching, outcome any adverse effect. Figure E4: Forest plot comparison: Medication switching, outcome serious adverse effect. Figure E5: Forest plot comparison: Medication switching, outcome discontinuation of treatment.
93 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 93 Figure E6: Forest plot comparison: Adjunct medication, outcome weight loss. Figure E7: Forest plot comparison: Adjunct medication, outcome global state. Figure E8: Forest plot comparison: Adjunct medication, outcome adverse effects (no data).
94 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 94 Figure E9: Forest plot comparison: Adjunct medication, outcome serious adverse effects. Figure E10: Forest plot comparison: Adjunct medication, outcome discontinuation of treatment. Figure E11: Forest plot comparison: Cognitive behavioral therapy, outcome weight loss.
95 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 95 Figure E11: Forest plot comparison: Cognitive behavioral therapy, outcome discontinuation of treatment.
96 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 96 Appendix F Summary of the Determinants of the Strength of Recommendations Based Upon the GRADE Approach (Andrews, et al., 2013). Determinants Quality of Evidence Balance of Benefits & Harms Values and Preferences Resource Allocation (Costs) Explanation Higher quality evidence supports a strong recommendation, lower quality evidence more likely to warrant a weak recommendation Greater benefit than harm supports a strong recommendation, while smaller or more uncertain benefit more likely to warrant a weak recommendation Greater variability in values and preferences more likely to warrant a weak recommendation Higher cost of intervention more likely to warrant a weak recommendation

97 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 97 Appendix G AGREE II Instrument Questions

98 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 98 Appendix H Consent Form for Guideline Evaluators.
99 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 99 Appendix I Institutional Review Board Approval Letter
100 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 100 Appendix J Summary of Database Findings Table J1: Database Findings Medication Switching Database Key Words Results Cochrane Library Antipsychotic* 148 Search limits: -Cochrane reviews -Between MEDLINE (EBSCO) Search limits: -Full text -Between All adult -English language CINAHL (EBSCO) Search limits: -Full text -Between All adult -English language Web of Science Search limits: -Between English language Antipsychotic* AND weight* Antipsychotic* AND weight* AND switching Antipsychotic* Antipsychotic* AND weight* Antipsychotic* AND weight* AND switching Antipsychotic* Antipsychotic* AND weight* Antipsychotic* AND weight* AND switching Antipsychotic* Antipsychotic* AND weight* Antipsychotic* AND weight* AND switching Refine: Science & technology only Refine: Review Refine: English Refine: Web of Science Core Collection (Excludes MEDLINE and Biological Abstracts) , ,454 7,
101 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 101 Table J2: Database Findings Adjunct Medications Database Key Words Results Cochrane Library Antipsychotic* 170 Search limits: -Reviews -Between MEDLINE (EBSCO) Search limits: -Full text -Between All adult 19+ years -English language CINAHL (EBSCO) Search limits: -Full text -Between All adult -English language Web of Science Search limits: -Between English language Antipsychotic* AND obes* Antipsychotic* Antipsychotic* AND obes* Antipsychotic* AND obes* AND intervention* Antipsychotic* AND obes* AND metformin Antipsychotic* AND obes* AND topiramate Antipsychotic* Antipsychotic* AND obes* Antipsychotic* AND obes* AND intervention* Antipsychotic* Antipsychotic* AND obes* Antipsychotic* AND obes* AND intervention* Antipsychotic* AND obes* AND intervention* AND systematic review 5 2, ,592 1,
102 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 102 Table J3: Database Findings Behavioral Interventions Database Key Words Results Cochrane Library Antipsychotic* 170 Search limits: -Reviews -Between MEDLINE (EBSCO) Search limits: -Full text -Between All adult 19+ years -English language CINAHL (EBSCO) Search limits: -Full text -Between All adult -English language Web of Science Search limits: -Between English language Antipsychotic* AND obes* Antipsychotic* Antipsychotic* AND obes* Antipsychotic* AND obes* AND intervention* Antipsychotic* AND obes* AND intervention* AND behav* Antipsychotic* Antipsychotic* AND obes* Antipsychotic* AND obes* AND intervention* Antipsychotic* Antipsychotic* AND obes* Antipsychotic* AND obes* AND intervention* Antipsychotic* AND obes* AND intervention* AND behav* Antipsychotic* AND obes* AND intervention* AND behav* AND systematic review 5 2, ,656 1,
103 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 103 Appendix K Characteristics of Excluded Studies Table K1: Characteristics of Excluded Studies Medication Switching Study Characteristics Reason for exclusion Aguis 2010 Type: Review Sample: 5 major studies involving antipsychotics No mention of weight in relation to medication switching Andersen 2005 Arnoldy 2013 Type: pilot study, non-randomized Sample: 6 adults with schizophrenia spectrum diagnoses who had experienced significant weight gain after long-term treatment with olanzapine and/or risperidone Intervention: Switch to perphenazine plus buspirone Type: case study Sample: 56 year-old male with schizophrenia Intervention: switched from clozapine to aripiprazole Non-randomized; Very small sample; Switch to conventional antipsychotic plus a non-antipsychotic medication; Average 10 kg weight loss Lowest level of evidence Berner 2007 Type: Systematic Review No mention of switching to reduce weight gain Bhuvaneswar 2009 Bobo 2010 Buchanan 2010 Type: Narrative review Topic: Adverse endocrine and metabolic effects of psychotropic drugs Type: Review Intervention: olanzapine-fluoxetine combination (Symbyax) Type: Expert consensus statement Topic: Treatment recommendations for schizophrenia No usable data; Saved for general overview Focus on adding antipsychotic to antidepressants for treatment resistant depression No usable data; Saved for general overview Buckley 2008 Pending ILLiad request No full text available Buckley 2008 Type: Narrative review Topic: Strategies for switching antipsychotics No usable data; Some references extracted for further review Cassano 2007 Type: Review Topic: Aripiprazole in schizophrenia No specific data regarding weight change when switching to aripiprazole
104 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 104 Chawla 2008 Type: Prospective, non-controlled cohort study Sample: 26 patients taking standard oral olanzapine Intervention: switch to orally disintegrating tablets No control group; Olanzapine known cause of weight gain Citrome 2007 ILLiad request submitted No full text available Citrome 2008 ILLiad request submitted No full text available Citrome 2009 Type: Article Intervention: Switch to ziprasidone No specific numbers provided regarding weight loss and switch to ziprasidone Citrome 2012 Type: Narrative Review Limited data on weight loss as a result of switching Citrome 2012 Citrome 2014 Citrome 2014 Cohn 2007 Type: Review article Topic: lurasidone Type: systematic review Sample: 22 articles Intervention: aripiprazole Type: Systematic Review of observational/naturalistic studies and open-label studies Topic: effects of aripiprazole on weight and metabolic outcomes Type: Review Topic: Metabolic monitoring in patients taking antipsychotics No usable data; No switching studies included No medication switching mentioned Observational, openlabel, noncontrolled; No usable data; Selected citations reviewed for further use Mostly focused on monitoring, not intervention; Saved for overview Correll 2010 No abstract available No full text available Cousins 2007 Type: Review No mention of Topic: Treatments for bipolar disorder switching to reduce Croxtall 2008 De Fazio 2010 Type: review Sample: Adults with schizophrenia Intervention: taking or switched to aripiprazole Type: Review article Topic: aripiprazole weight gain Only includes one study of medication switching to aripiprazole and effect on weight (Newcomer, 2008); Newcomer 2008 already included in Cochrane Review (Mukundan, 2010) No usable data; No mention of switching to reduce weight gain
105 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 105 Dell Osso 2013 Dold 2012 Edlinger 2005 Edwards 2008 Essock 2006 Fabiolini 2013 Faulkner 2006 Gallego 2012 Ganguli 2008 Type: Review Sample: Unknown Type: systematic review Sample: 34 studies with 2657 participants Intervention: randomized controlled trials comparing benzodiazepines (as monotherapy or as adjunctive agent) with antipsychotic drugs or placebo for the pharmacological management of schizophrenia and/or schizophrenia-like psychoses Type: Review article Topic: Switching second-generation antipsychotics Type: Review of clinical trials Topic: Clinical outcomes and cost analysis Type: Secondary analysis of randomized controlled trial Sample: Data from Clinical Antipsychotic Trial of Intervention Effectiveness (CATIE) Intervention: switching versus staying on antipsychotic monotherapies Type: Review Sample: Unknown Type: Narrative review Topic: Strategies for management of weight gain in patients taking antipsychotic medication Type: Systematic Review Topic: Safety of antipsychotic polypharmacy Type: randomized, open-label Sample: 123 adult patients taking olanzapine Intervention: switch to risperidone No mention of medication switching Does not specifically address weight loss; Does not switch between antipsychotics No usable data; All studies referenced older than 2005; None of the studies have weight as a primary outcome No mention of switching to reduce weight gain No outcome measures regarding weight change No full text available; Switching and weight loss not mentioned as inquiry for the review No usable data; Saved for general overview No mention of medication switching; No usable data Studied effect of switching method, therefore short duration, only 6 weeks; No significant weight change observed Gierisch 2014 ILLiad request submitted No full text available
106 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 106 Godleski 2005 Type: Open-label, nonrandomized Sample: 13 patients taking depot antipsychotic Intervention: switched to oral olanzapine No mention of switching to reduce weight gain; Olanzapine known cause of weight gain Gopal 2010 Type: Expert Review of clinical trials Focus only on longacting injectable paliperidone; no mention of weight Greenberg 2007 Type: Review No full text available Topic: ziprasidone Hasnain 2011 Type: Narrative Review Focused on adjunct medications; Saved for adjunct evidence summary Hasnain 2012 Type: Literature review Topic: weight gain and antipsychotics and antidepressants No usable data; Used for overview of problem Hasnain 2013 ILLiad request submitted No full text available Hawley 2010 Type: open-label, non-randomized Sample: 182 adults taking antipsychotics Intervention: switch to long-acting injectable risperidone Non-randomized; Majority of patients switching from conventional antipsychotic to atypical antipsychotic Hester 2005 ILLiad request submitted No full text available Hong 2012 Ishitobi 2013 Kantrowitz 2008 Karagianis 2008 Type: Observational study Sample: 17,000 outpatients with schizophrenia taking olanzapine or risperidone Intervention: switch to olanzapine or risperidone Type: prospective, open-label Sample: 9 male patients with autism spectrum disorders Type: Review Topic: Efficacy and safety of olanzapine Type: Narrative Review of case series Topic: Olanzapine standard tablets versus orally disintegrating tablets Observational; Olanzapine known cause of weight gain Includes children and adolescents No mention of switching to reduce weight gain; Olanzapine known cause of weight gain No usable data; Olanzapine known cause of weight gain
107 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 107 Kim 2009 Type: open-label, non-randomized Sample: 36 adults with schizophrenia taking conventional antipsychotics Intervention: switch to long-acting injectable risperidone Non-randomized; Patients switched from conventional antipsychotic to atypical antipsychotic; Significant weight gain after switch Kim 2010 ILLiad request submitted No full text available Lee 2013 Type: Prospective, open-label, noncontrolled Sample: 56 patients with bipolar disorder taking olanzapine Intervention: switch to ziprasidone No control group Liauw 2010 ILLiad request submitted No full text available Lin 2009 Type: prospective cohort study, nonrandomized Sample: 46 inpatient adults with schizophrenia, taking an SGA, with BMI >27 kg/m 2 Intervention: switch to amisulpride Not randomized, inpatient setting Lu 2007 Type: Prospective, observational Sample: 1267 outpatients with schizophrenia taking conventional antipsychotics Intervention: switch to olanzapine Switch from conventional antipsychotics; Olanzapine known cause of weight gain Martinez-Ortega 2013 Type: Review Sample: 127 reports Includes children and adolescents Medved 2009 Type: Article Focused on diabetes and psychiatric disorders; No mention of medication switching Meyer 2005 Montes 2007 Newcomer 2013 Type: Post-hoc analysis, open-label, non-randomized Sample: 121 patients with metabolic syndrome taking olanzapine Intervention: switch to risperidone Type: Observational, open-label Sample: 84 outpatients with schizophrenia or schizoaffective disorder experiencing some type of metabolic disturbance related to antipsychotic use Intervention: switch to ziprasidone Type: Literature review Topic: Switching antipsychotic medication Post-hoc, nonrandomized, no control group Observational No usable data; Some references extracted for further review
108 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 108 Nyhuis 2010 Type: post-hoc analysis of RCT Sample: 664 adults taking antipsychotics Intervention: Open-label switching between first generation antipsychotic, olanzapine, and risperidone Type: Randomized, open-label trial Sample: 175 patients (inpatient and outpatient) with schizophrenia considering switch due to inefficacy or intolerability Intervention: switch to aripiprazole using one of three different switching approaches Reports predictors of medication switching, not outcomes from switching Pae 2009 Outcome measures include BMI but not weight specifically; No usable data; No control group; Designed to test tolerability of switching method rather than switch effect upon weight Pani 2008 Type: Review article No usable data; No Topic: amisulpride reference to studies using switch to reduce weight gain Rege 2008 Type: Narrative review No usable data; Saved Topic: mechanisms and management of for general overview; antipsychotic induced weight gain Many duplicate studies in references Ried 2006 ILLiad request submitted No full text available Roffeei 2014 Rosa 2012 Rosenheck 2009 Type: Head-to-head controlled comparison Sample: 115 patients with schizophrenia with 1 year of metabolic abnormalities associated with antipsychotic use Intervention: switch to ziprasidone or aripiprazole Type: Prospective, non-randomized trial Sample: 96 adults with non-acute psychotic disorders taking olanzapine Intervention: switch to long-acting injectable risperidone Type: Secondary analysis of randomized controlled trial Sample: Data from Clinical Antipsychotic Trial of Intervention Effectiveness (CATIE) Intervention: switching versus staying on antipsychotic monotherapies No control group; Useful for comparing effects of ziprasidone or aripiprazole, but because no control, low quality evidence for switching strategy in general Non-random, no control group Outcome measures regarding weight do not include usable data; Switching was not explicitly intended to address weight gain
109 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 109 Rossi 2009 Type: open-label, non-randomized Sample: 347 adults with schizophrenia or schizoaffective disorder taking antipsychotics Intervention: switch to long-acting injectable risperidone Non-randomized; No information about type of antipsychotics taken prior to switch; No significant weight gain after switch Samtani 2011 Type: Narrative Review No mention of weight in regard to medication switching Schorr 2008 Suttajit 2014 Suzuki 2012 Takeuchi 2010 Tanaka 2008 Verma 2010 Type: Non-controlled cohort study Sample: 53 overweight patients with schizophrenia taking antipsychotics Intervention: switch to aripiprazole Type: Systematic review Sample: 11 RCTs Type: case study Sample: 19 year-old female with schizophrenia Intervention: switched from blonanserin to quetiapine Type: Observational Sample: 32 patients with schizophrenia taking antipsychotics Intervention: switch to aripiprazole Type: Clinical trail Topic: Metabolic effects of olanzapine Type: open-label trial Sample: 25 adults with schizophrenia spectrum disorders taking antipsychotics Intervention: switch to long-acting injectable risperidone No control group Includes children and adolescents; No switching mentioned Lowest level of evidence; blonanserin not available in the United States Observational study, no control group, no randomization No mention of switching to reduce weight gain; Olanzapine known cause of weight gain Weight loss was not the purpose of switching; Weight gain a significant outcome; Half of participants dropped out Wang 2014 Type: Review of three studies? Unclear Abstract does not mention switching; No full text available Weber 2009 Type: fictional case study Fictional case study Wehmeier 2007 Type: Prospective study Topic: Quality of life for outpatients with schizophrenia taking antipsychotics No mention of switching to reduce weight gain Weiden 2007 ILLiad request submitted No full text available
110 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 110 Weiden 2008 Ye 2012 Type: randomized cross-titration methods, no control group Sample: 185 outpatient adults taking risperidone, olanzapine, or conventional antipsychotic Intervention: switch to ziprasidone using varying cross-tapering methods Type: Naturalistic/observational study Sample: 258 patients with schizophrenia taking risperidone Intervention: switch to olanzapine No control group Observational; Olanzapine known cause of weight gain Table K2: Characteristics of Excluded Studies Adjunct Medication Study Characteristics Reason for exclusion Attux 2013 Type: RCT Sample: 160 adults taking SGAs Intervention: Lifestyle interventions No mention of medication for weight loss Baker 2011 Baptista 2006 Barnes 2008 Blouin 2009 Bonfioli 2012 Brown 2012 Type: Study protocol Sample: Adults with severe mental illness taking antipsychotic medication and current smoker Intervention: Lifestyle intervention Type: RCT Sample: 40 adults taking olanzapine Intervention: Metformin Type: quality improvement study Sample: adults taking antipsychotics Intervention: screening for metabolic syndrome Type: nonrandomized pilot study Sample: 16 adults taking SGAs Intervention: Lifestyle (diet & exercise) Type: Systematic Review Topic: Non-pharmacological interventions for weight management in psychosis Type: Retrospective study Sample: 95 adults with schizophrenia No intervention Study protocol; Focused on lifestyle interventions; No mention of medication for weight loss Reported in later review Focus on quality improvement screening program Focus on lifestyle interventions; No mention of medication for weight loss Focus on lifestyle interventions; No mention of medication for weight loss Focus on predictors of death from natural causes; No mention of medication for weight loss Involves children Brufani 2001 Type: Review article Topic: metformin in children Chen 2009 Type: Nonrandomized clinical Focus on lifestyle
111 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 111 Cimo 2012 Correll 2010 intervention study Sample: 33 adults taking SGAs with BMI >25 Intervention: Lifestyle mixed with behavioral Type: Systematic Review Topic: Lifestyle interventions to improve type II diabetes in patients with schizophrenia or schizoaffective disorder Type: Comparative review Topic: mood stabilizers and antipsychotics interventions; No mention of medication for weight loss Focus on lifestyle interventions; No mention of medication for weight loss Includes pediatric patients Curtis 2012 Type: Discussion paper Opinion piece DeHert 2011 Type: Evaluation of guidelines Topic: Screening and monitoring of cardiometabolic risk in schizophrenia Evans 2005 Fernandez 2014 Ha 2006 Type: RCT Sample: 51 adults taking olanzapine Intervention: nutritional Type: Systematic Review Topic: Lifestyle interventions to reduce cardiovascular risk in patients with severe mental disorders Type: Article Topic: Mechanism of action for topiramate on body weight Type: Systematic Review Topic: Male fertility and psychiatric considerations Focus on screening and monitoring; No mention of medication for weight loss Focus on nutritional interventions; No mention of medication for weight loss Focus on lifestyle interventions; No mention of medication for weight loss No new clinical data regarding efficacy for reducing body weight Hall 2012 Not relevant; No mention of medication for weight loss Haw 2012 Study of adolescents Includes adolescents Hellerstein 2007 Hjorth 2014 Johnstone 2009 Lin 2005 Type: Observational study Sample: charts of 105 adults at a community mental health center Type: Systematic Review Topic: Interventions to reduce overweight and obesity in schizophrenia Type: Qualitative study Topic: Barriers to physical activity in schizophrenia Type: case series Topic: 3 adults taking SGAs No intervention Medication interventions excluded; Saved for behavioral search Qualitative study; No intervention; No mention of medication for weight loss Case series; low level of evidence
112 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 112 McElroy 2007 McIntyre 2012 Ohlsen 2005 Pearsall 2014 Porsdal 2010 Intervention: topiramate Type: Comparative study, RCT Sample: 46 outpatients with bipolar taking antipsychotics or mood stabilizers Intervention: topiramate vs. sibutramine Type: Literature Review Topic: Evidence-Based Practice Recommendations for management of mood disorders with comorbid metabolic disorders Type: Nonrandomized Sample: adults with severe mental illness taking antipsychotics Intervention: lifestyle intervention Type: Systematic Review Topic: Exercise for patients with mental illness Type: Observational study Sample: 363 adults attending psychiatric clinics Intervention: Lifestyle intervention Includes mood stabilizers Does not specifically address antipsychotic medications and weight gain Focus on lifestyle interventions; No mention of medication for weight loss Focus on lifestyle interventions; No mention of medication for weight loss Focus on lifestyle interventions; No mention of medication for weight loss Roberts 2011 Type: Narrative Review Focus on lifestyle interventions; No mention of medication for weight loss Seeman 2008 Shin 2008 Usher 2013 Vandyk 2012 Verhaeghe 2011 Type: Perspective article Intervention: Preventative services for women with schizophrenia Type: Review article Topic: obesity in children taking SGAs Type: RCT Sample: 101 adults taking SGAs Intervention: Lifestyle interventions Type: Qualitative study Sample: 18 patients with schizophrenia and medication-induced weight gain No intervention Type: Systematic Review Topic: Lifestyle interventions in persons with severe mental disorders Focus on preventative health interventions; No mention of medication for weight loss Involves children No mention of medication for weight loss Qualitative study; No intervention; No mention of medication for weight loss Focus on lifestyle interventions; No mention of medication
113 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 113 Vieweg 2005 Yarborough 2013 Yearwood 2001 Type: review Sample: 21 articles Intervention: antipsychotic medications in children and adolescents Type: Study protocol Sample: Adults taking antipsychotic medication Intervention: Lifestyle interventions Type: Practice article Topic: Prader-Willli Syndrome for weight loss Limited to children and adolescents; No mention of medication for weight loss Study protocol; Focused on lifestyle interventions; No mention of medication for weight loss Not relevant; No mention of medication for weight loss
114 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 114 Appendix L Characteristics of Included Studies Characteristics of Included Studies Medication Switching Table L1: Characteristics of Included Study by Newcomer (2008) Methods Allocation: Randomized Blindness: Double Duration: 16 weeks Setting: Multi-site, multinational, outpatient Participants Diagnosis: Schizophrenia or schizoaffective disorder N = 173 Age: Between years, mean~39 years (SD 10) BMI: >27kg/m 2 Sex: 111 males and 62 females History: mg olanzapine 1-24 months prior to screening, clinically stable, weight gain prior to olanzapine verified Excluded: other axis 1 disorder, Type I or II diabetes mellitus, women who were pregnant, breastfeeding, or unwilling/unable to use acceptable form of contraception during the entire study period, any clinically significant neurological abnormality (i.e. epilepsy, Parkinson s disease), stroke, TIA, increased risk of suicide, psychoactive substance or alcohol dependence (except for caffeine and nicotine), increase in symptoms requiring hospitalization or change in antipsychotic therapy, weight loss >10% of total body weight 3 months before screening, received ECT 3 months prior, received aripiprazole or other investigational agent 4 weeks prior, previously failed a course of aripiprazole 10 mg per day for 4 weeks, abnormal vital signs, ECG, or laboratory tests Interventions 1. Switch to aripiprazole monotherapy (mean dose 16 mg per day), N = Continue olanzapine monotherapy (mean dose 15.9 mg per day), N = 85 Outcomes Weight (kg), BMI, waist circumference, fasting lipid levels, fasting plasma glucose, fasting insulin, fasting C-peptide, Clinical Global Impressions- Severity of Illness (CGI-S) scores, adverse effects, and significant adverse effects Notes Risk of Bias Assessment Bias Author s judgment Support for judgment Randomization (selection Unclear Risk bias) Quote: evenly randomly assigned Comment: May indicate alternate allocation (considered quasi-random and insufficient) or could simply refer to even distribution of participants (88 received intervention, 85 in control group)
115 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 115 Allocation concealment (selection bias) Blinding of participants and personnel (performance bias) Blinding of outcome assessment (detection bias) Incomplete outcome data (attrition bias) Selective reporting (reporting bias) Unclear Risk Low Risk Low Risk Low Risk Low Risk Not described Quote: double-blind study Comments: Methods not described, but unlikely to impact outcomes such as weight, physiologic measures Quote: double-blind study Comments: Methods not described, but unlikely to impact outcomes such as weight, physiologic measures Reports rates of attrition and gives reasons (i.e. due to adverse effects) when able; Attrition rates due to adverse effects similar between groups; Intervention group with higher number of attrition overall, but consistent with studies showing that switching groups discontinue treatment earlier than those continuing medication Baseline measures reflective of outcome measures; Data sufficient for metaanalysis Other bias Unclear Risk Some authors employed by interested pharmaceutical company Table L2: Characteristics of Included Study by Stroup (2011) Methods Allocation: Random Blindness: Double Duration: 24 weeks Setting: Multi-site, outpatient, United States Participants Diagnosis: Schizophrenia or schizoaffective disorder N = 215 Age: Mean~41 years (SD 11.1) BMI: >27kg/m 2 Sex: 137 males and 78 females History: Patients clinically stable on olanzapine, quetiapine, or risperidone and who were at increased risk of cardiovascular disease as evidenced by BMI 27 and dyslipidemia. Patients on qualifying medication for at least 3 months prior to enrollment and had desire to improve their metabolic risk profile Interventions 1. Titrated switch to aripiprazole (between 5-30 mg daily), N = Continue current therapy: olanzapine (5-20 mg daily), quetiapine ( mg daily), or risperidone (1-16 mg daily), N = 106 Outcomes Weight, lipids, global state, adverse effects, serious adverse effects,
116 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 116 discontinuation of treatment Notes Risk of Bias Assessment Bias Author s judgment Support for judgment Randomization (selection bias) Allocation concealment (selection bias) Blinding of participants and personnel (performance bias) Blinding of outcome assessment (detection bias) Incomplete outcome data (attrition bias) Selective reporting (reporting bias) High Risk Quote: randomly assigned on a 1:1 basis Comment: Indicate alternate allocation (considered quasi-random and insufficient) Unclear Risk High Risk Low Risk Low Risk Low Risk Not described Quote: "Participants and their physicians were aware of the medication assignment Comment: Unlikely to impact physiologic outcomes such as weight Raters of outcomes were "blinded to treatment" Reports rates of attrition and gives reasons (i.e. due to adverse effects) when able; Attrition rates due to adverse effects similar between groups; Intervention group with higher number of attrition overall, but consistent with studies showing that switching groups discontinue treatment earlier than those continuing medication Baseline measures reflective of outcome measures; Data sufficient for metaanalysis Other bias Low Risk The study appears to be free of other sources of bias Characteristics of Included Studies Adjunct Medication Table L3: Characteristics of Included Study by Afshar (2009) Methods Allocation: randomized Blindness: double-blind, placebo-controlled Duration: 8 weeks Setting: outpatient, Iran Participants Diagnosis: schizophrenia N = 32 Age: Between years, mean~38 years (SD±5.1) Sex: 20 males and 12 females History: Patients who had poor clinical outcome in spite of long-term
117 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 117 Interventions Outcomes treatment with several types of antipsychotics who were currently receiving treatment with clozapine at a maximum dose of 100 mg/day for the previous 2 months. No significant difference in baseline measurements between treatment and control groups. 3. Addition of topiramate starting at 25 mg/day and increasing to 300 mg/day by titrating up 25 mg/day every 3 to 4 days according to individual tolerability, N = Continue clozapine monotherapy plus placebo, N = 16 Weight (kg), BMI, Positive and Negative Syndrome Scale (PANSS), tolerability of treatment, adverse effects, and significant adverse effects Notes Risk of Bias Assessment Bias Author s judgment Support for judgment Randomization (selection bias) Allocation concealment (selection bias) Blinding of participants and personnel (performance bias) Blinding of outcome assessment (detection bias) Incomplete outcome data (attrition bias) Low risk Low risk Low risk Low risk Low risk Quote: "Patients were randomly assigned to one of two groups using random number generator software." Quote: "The researcher who allocated patients to one of the two group had no role in the treatment plan or filling the questionnaires, and the psychiatrist responsible for the treatment of patients and filling PANSS was not informed about patients' medication. Follow-up was conducted using patient's code." Quote: "Placebo tablets were made...with the same appearance as topiramate Quote: "The psychiatrist responsible for the treatment of patients and filling PANSS was not informed about patients' medication."tablets." All patients completed the study; Outcome data reflects baseline measurement data, but not all outcomes had specific information included in the article, rather these were listed and described as "had insignificant differences in two groups at the beginning and end of the study." Selective reporting (reporting bias) Unclear risk Not all outcomes had specific information included in the article, rather these were listed and described as "had insignificant differences in two groups at the beginning and end of the study." Other bias Low risk No evidence of other bias detected
118 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 118 Table L4: Characteristics of Included Study by Baptista (2007) Methods Allocation: Random Blindness: Double Duration: 12 weeks Setting: Multi-site, inpatient and outpatient, Venezuela Participants Diagnosis: Schizophrenia or bipolar disorder, taking olanzapine N = 80 Age: Reported by sex and group type, means between 42.4 years and 46.2 years, with varying SDs by group BMI in placebo group: ~26.18 kg/m 2 (SD 5.7) BMI in experimental group: ~25.0 kg/m 2 (SD 4.9) Sex: 42 males and 30 females History: Patients older than 18 years, free of hormone replacement therapy, no chronic disease besides mental disorder, and with normal physical and laboratory tests (liver, kidney, thyroid, and fasting glucose) before starting olanzapine. Olanzapine treatment for at least 4 months and with desire to lose weight or prevent weight gain. Interventions 3. Continue current therapy plus metformin, N = Continue current therapy plus placebo, N = 36 Outcomes Weight, waist circumference, fasting glucose, HbA1c, insulin, lipids, leptin, c-reactive protein, fibrinogen, cortisol, growth hormone, global state, adverse effects, serious adverse effects, discontinuation of treatment Notes Risk of Bias Assessment Bias Author s judgment Support for judgment Randomization (selection Low Risk bias) Allocation concealment (selection bias) Blinding of participants and personnel (performance bias) Blinding of outcome assessment (detection bias) Incomplete outcome data (attrition bias) Low Risk Low Risk Low Risk Low Risk Quote: "Subjects were randomly assigned through a computer-based program." Quote: "The study coordinator was the only team's member to know the individual treatment." Quote: "The study coordinator was the only team's member to know the individual treatment." Quote: "identical placebo pills" Quote: "The study coordinator was the only team's member to know the individual treatment." Quote: "Seven subjects abandoned the study by change in residence and one patient relapsed and required combined antipsychotic treatment." Selective reporting Low Risk Outcome data reflective of baseline data (reporting bias) collected and intent of the study Other bias Low Risk No evidence of other bias detected
119 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 119 Table L5: Study by Carrizo (2009) Methods Allocation: Random Blindness: Double Duration: 14 weeks Setting: Single site, outpatient, Venezuela Participants Diagnosis: Schizophrenia, receiving clozapine > 3 months N = 61 Age in placebo group: Mean~39.6 years (SD 9.7) Age in experimental group: Mean~38.3 years (SD 9.7) BMI in placebo group: >27.4 kg/m 2 (SD 5.7) BMI in experimental group: >28.7 kg/m 2 (SD 5.3) Sex: Not reported History: Patients primarily with schizophrenia receiving treatment with clozapine for >3 consecutive months, older than 18 years, free of hormone replacement therapy, and with normal physical and laboratory test (kidney, thyroid, and liver). Also, no symptoms of type II diabetes. No significant differences between groups at baseline. Interventions 1. Add extended release metformin mg PO daily, N = Continue current therapy, N = 30 Outcomes Weight, lipids, insulin, glucose, leptin, cortisol, blood pressure, waist circumference, HbA1c, global state, adverse effects, serious adverse effects, discontinuation of treatment Notes Risk of Bias Assessment Bias Author s judgment Support for judgment Randomization (selection bias) Low Risk Quote: "Patients were randomly assigned by a computer program" Allocation concealment Low Risk Quote: "Only the study coordinator (selection bias) Blinding of participants and personnel (performance bias) Blinding of outcome assessment (detection bias) Incomplete outcome data (attrition bias) Low Risk Low Risk Unclear Risk knew the treatment assignment" Quote: "Metformin or placebo in identical pills. Both treatments were daily provided with the last meal in a double-blined protocol. Only the study coordinator knew the treatment assignment." Quote: "Only the study coordinator knew the treatment assignment." One psychiatrist conducted both initial and follow-up assessments. Quote: "All the placebo subjects completed the study. Seven out of 31 metformin-treated patients abandoned the protocol before the first follow-up
120 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 120 visit at week 7. One woman became pregnant, and the other dropouts had a severe mental disorder at baseline and manifested vague and unstable side effects that even the caregivers could not explain. None of these patients complained of gastrointestinal discomfort." Selective reporting (reporting bias) Low Risk Outcome data reflective of baseline data collected and intent of the study Other bias Low Risk No evidence of other bias detected Table L5: Characteristics of Included Study by Narula (2010) Methods Allocation: Random Blindness: Double Duration: 12 weeks Setting: Single site, majority outpatient, India Participants Diagnosis: Schizophrenia, first episode, drug naïve N = 77 (72 randomly assigned) Age in placebo group: Mean~31 years (SD 10.1) Age in experimental group: Mean~31.2 years (SD 9.7) BMI in placebo group: ~20.2 kg/m 2 (SD 3.92) BMI in experimental group: ~20.56 kg/m 2 (SD 3.85) Sex: 44 males and 23 females History: Patients attending psychiatry clinic at tertiary care hospital in New Delhi, India with first-episode schizophrenia. Drug naïve and between the ages of years. Excluded if any other neuropsychiatric illness, on any other medications known to influence weight, any substance abuse diagnosis in the past 3 months, pregnancy, lactation, or not using adequate contraception. Interventions 1. Olanzapine 5-20 mg PO daily, N = Olanzapine 5-20 mg PO daily plus topiramate mg PO daily:, N = 33 Outcomes Weight, lipids, fasting glucose, insulin, insulin resistance, leptin, blood pressure, global state, adverse effects, serious adverse effects, discontinuation of treatment Notes Risk of Bias Assessment Bias Author s judgment Support for judgment Randomization (selection bias) Allocation concealment (selection bias) Blinding of participants and personnel (performance bias) Unclear Risk Unclear Risk Low Risk Randomization method not described Allocation concealment not described Described as "double-blind" but blinding methods are not explicitly described
121 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 121 Blinding of outcome assessment (detection bias) Incomplete outcome data (attrition bias) Low Risk Low Risk Described as "double-blind" but blinding methods are not explicitly described Exclusion and attrition information provided for all participants not included in study Selective reporting (reporting bias) Low Risk Outcome data reflective of baseline data collected and intent of the study Other bias Low Risk No evidence of other bias detected Table L6: Characteristics of Included Study by Wu (2008) Methods Allocation: Random Blindness: Double Duration: 12 weeks Setting: Single site, outpatient, China Participants Diagnosis: Schizophrenia, first episode N = 128 Age: Mean~26.3 years (SD 0.8) BMI: ~24.5 kg/m 2 Sex: 64 males and 64 females History: Patients aged 18 to 45 years with first psychotic episode of schizophrenia taking only 1 antipsychotic medication of clozapine, olanzapine, risperidone, or sulpiride for over 3 months with no more than a 25% increase in dosage. Also have gained more than 10% of pre-drug body weight within the first year of treatment and have been seen in the outpatient clinic at least once in previous 12 months. Excluded if liver or renal dysfunction, cardiovascular disease, diabetes mellitus, pregnant or lactating, physical condition limiting ability to perform lifestyle modifications, other psychiatric diagnosis, or history of substance abuse. Interventions 1. Continue current therapy plus placebo, N = Continue current therapy plus placebo plus lifestyle intervention, N = Continue current therapy plus metformin 750 mg PO daily (divided into 3 doses, with meals), N = Continue current therapy plus metformin 750 mg PO daily (divided into 3 doses, with meals) plus lifestyle intervention, N = 32 Outcomes Weight, waist circumference, fasting glucose, insulin, global state, adverse effects, serious adverse effects, discontinuation of treatment Notes Risk of Bias Assessment Bias Author s judgment Support for judgment Randomization (selection bias) Low Risk Quote: "Participants were randomized through a computergenerated table in blocks of 8 to
122 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 122 ensure approximately equal numbers of participants in each group." Allocation concealment (selection bias) Low Risk Quote: "To ensure concealment of the treatment assignment, randomization was conducted independently of the investigators by a research pharmacist at a separate facility and medication was provided in coded containers of identical-appearing capsules of metformin or placebo supplied by the manufacturer." Blinding of participants and personnel (performance bias) Low Risk Quote: "To ensure concealment of the treatment assignment, randomization was conducted independently of the investigators by a research pharmacist at a separate facility and medication was provided in coded containers of identical-appearing capsules of metformin or placebo supplied by the manufacturer." Blinding of outcome assessment (detection bias) Low Risk Quote: "The research nurses who performed all assessments were blinded to the treatments that the patients were receiving and were not involved in implementing any aspects of the intervention." Incomplete outcome data (attrition bias) Low Risk Exclusion and attrition information provided for all participants not included in study Selective reporting (reporting bias) Low Risk Outcome data reflective of baseline data collected and intent of the study Other bias Low Risk No evidence of other bias detected Characteristics of Included Studies Behavioral Interventions Table L7: Characteristics of Included Study by Attux (2013) Methods Allocation: Random Blindness: Single Duration: 12 weeks Setting: Multi-site, outpatient, Brazil Participants Diagnosis: Schizophrenia, being treated with antipsychotic N = 160 Age in standard care group: Mean~38.3 years (SD 10.7) Age in intervention group: Mean~36.2 years (SD 9.9) BMI in standard care group: ~29.9 kg/m 2 (SD 5.2)
123 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 123 Interventions Outcomes BMI in intervention group: ~29.1 kg/m 2 (SD 4.7) Sex: 96 males and 64 females History: Patients between 18 to 65 years old, with schizophrenia, using any antipsychotic in the past 3 months, and clinically stable. Also had motivation to lose weight or had concern about weight gain. Excluded if presence of diabetes mellitus, history of eating disorder or substance abuse, and taking or planning to take any weightreducing medications. 3. Standard care (i.e. regular visits to psychiatrist and psychosocial interventions), N = Lifestyle Wellness Program (one hour weekly sessions combining behavioral interventions and psychoeducation), N = 81 Weight, waist circumference, blood pressure, glucose, lipids, insulin, global state, multiple secondary outcomes, discontinuation of treatment Notes Risk of Bias Assessment Bias Author s judgment Support for judgment Randomization (selection bias) Allocation concealment (selection bias) Blinding of participants and personnel (performance bias) Blinding of outcome assessment (detection bias) Incomplete outcome data (attrition bias) Unclear Risk Unclear Risk Low Risk Low Risk Low Risk Quote: "Randomly allocated" No description of randomization method Quote: "Randomly allocated" No description of allocation concealment Quote: "Blind investigators applied the following instruments..." Unable to blind participants to intervention Quote: "Blind investigators applied the following instruments..." All exclusions and attrition data provided for first 3 months, no attrition information provided for 6-month follow-up, but data for this group was not included Selective reporting Unclear Risk 6-month outcome data not reported, but (reporting bias) explained by authors Other bias Low Risk No evidence of other bias detected Table L8: Characteristics of Included Study by Khazaal (2007) Methods Allocation: Random Blindness: Unclear Duration: 12 weeks of intervention, 24 week follow up Setting: Single site, outpatient, Switzerland Participants Diagnosis: Taking an antipsychotic
124 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 124 N = 61 Age in standard care group: Mean~38.3 years (SD 10.4) Age in intervention group: Mean~43 years (SD 9.8) BMI in standard care group: ~28.7 kg/m 2 (SD 4.3) BMI in intervention group: ~32.4 kg/m 2 (SD 5.0) Sex: 28 males and 33 females History: Patients between 18 to 65 years, taking an antipsychotic for at least 2 months, and with a reported weight gain of >2 kg over 6 months of antipsychotic treatment. Excluded if diagnosis of anorexia, bulimia nervosa, opiate, alcohol, or cocaine dependence, mental retardation, or diabetes mellitus. Interventions 1. Standard care (Brief Nutritional Education), N = Cognitive-behavioral therapy on eating and weightrelated cognitions, N = 31 Outcomes Weight, eating and weight-related cognitions, binge eating symptomatology Notes Risk of Bias Assessment Bias Author s judgment Support for judgment Randomization (selection bias) Unclear Risk Quote: "Eligible patients were randomly allocated to one of the two treatments" No description of randomization method Allocation concealment (selection bias) Unclear Risk No description of allocation concealment Blinding of participants and personnel (performance Unclear Risk No description of blinding of participants or personnel bias) Blinding of outcome assessment (detection bias) Unclear Risk No description of blinding of outcome assessment Incomplete outcome data (attrition bias) Unclear Risk Attrition rates reported but not explained Selective reporting (reporting bias) Low Risk Outcome data reflects baseline data and intent of study Other bias Low Risk No evidence of other bias detected Table L9: Characteristics of Included Study by Weber (2006) Methods Allocation: Random Blindness: Unclear Duration: 16 weeks Setting: Single site, outpatient, United States Participants Diagnosis: Schizophrenia or schizoaffective disorder N = 17 Age: Between 18 and 65 years old, no mean reported BMI: 25 kg/m 2, Mean = 33 kg/m 2
125 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 125 Interventions Outcomes Sex: 5 males and 12 females History: Patients taking only one oral atypical antipsychotic and with a BMI 25 kg/m 2. Excluded if acutely psychotic, in need of immediate detoxification, or alcohol dependent. 1. Treatment as usual (scheduled appointments at public mental health clinic), N = 7 2. Cognitive/behavioral intervention (1-hour structured group sessions once per week), N = 8 Weight, weight-to-hip ratio, fasting glucose, discontinuation of treatment Notes Risk of Bias Assessment Bias Author s judgment Support for judgment Randomization (selection bias) Allocation concealment (selection bias) Blinding of participants and personnel (performance bias) Blinding of outcome assessment (detection bias) Unclear Risk Unclear Risk Unclear Risk Low Risk Quote: "were randomized" No description of randomization method No description of allocation concealment Quote: "Placebo controlled," Control group "continued to receive care as usual at the clinic." Not exactly clear how this is a "placebo," an unrelated group intervention would have been more appropriate. Quote: "All measurements were completed by one Graduate Research Assistant who was blind to the randomization." Incomplete outcome data (attrition bias) Low Risk Attrition rates reported with explanations given Selective reporting (reporting bias) Low Risk Outcome data reflects baseline data and intent of study Other bias Low Risk No evidence of other bias detected


126 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 126 Appendix M Summary of AGREE II Evaluation Data from Google Forms
127 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 127
128 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 128

129 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 129
130 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 130

131 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 131
132 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 132
133 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 133
134 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 134
135 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 135
136 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 136
137 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 137
138 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 138
139 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 139
140 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 140
141 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 141
142 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 142 Appendix N Permissions to Reproduce Copyrighted Materials Figure N1: Permission to reproduce ACE Star Model of Evidence-Based Practice image (Stevens, 2012).
143 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 143 Figure N2: Permission to reproduce Hierarchy of Evidence image (University of Washington, 2011).
144 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 144 Figure N3: Permission to reproduce the GRADE framework for guideline development (Schunemann, et al., 2011).
145 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 145 Figure N4: Permission to reproduce the Summary of GRADE method for rating importance of study outcomes (Guyatt, et al., 2011).
146 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 146 Guideline Title Appendix O Clinical Practice Guideline Guideline Information Management of medication-associated weight gain in adults taking antipsychotics. Bibliographic Source N/A Guideline Status This is a provisional release of the guideline. It is still under development while pending review by experts and revision according to feedback. FDA Warning/Regulatory Alert Adjunct medications suggested for the management of antipsychotic-associated weight gain have not been approved by the FDA for this purpose. Disease/Condition(s) Scope Weight gain caused by antipsychotic medication Guideline Category Evaluation Management Prevention Treatment Clinical Specialty Family Practice General Practice Mental Health Care Primary Care Psychiatry Intended Users
147 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 147 Advance Practice Nurses Health Care Providers Hospitals Nurses Patients Pharmacists Physician Assistants Physicians Psychologists/Non-physician Behavioral Health Clinicians Guideline Objective(s) To offer evidence-based practice advice on the management of weight gain in adults taking antipsychotic medications. Target Population Adults taking atypical antipsychotic medications who are concerned about weight gain or who have experienced >5% increase in body weight since starting antipsychotic therapy. Interventions and Practices Considered 1. Screening and evaluation of individuals for antipsychotic-associated weight gain 2. Management and prevention options for antipsychotic-associate weight gain in adults Major Outcomes Considered Change in weight (primary outcome) Global state Adverse events Serious adverse events Discontinuation of treatment Methods Used to Collect/Select the Evidence Methodology Hand-searches of Published Literature (Primary and Secondary Sources) Searches of Electronic Databases Description of Methods Used to Collect/Select the Evidence
148 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 148 Review questions were developed using a PICO framework (patient, intervention, comparison, and outcome). A total of 3 review questions were identified: 1. In adults taking antipsychotic medication (P), how does medication switching (I) compare to standard care (C) for decreasing weight (O)? 2. In adults taking antipsychotic medication (P), how do pharmacological interventions (I) compare to standard care (C) for decreasing weight (O)? 3. In adults taking antipsychotic medication (P), how do behavioral interventions (I) compare to standard care (C) for decreasing weight (O)? The evidence search was conducted using electronic databases such as the Cochrane Database of Systematic Reviews, MEDLINE (PubMed), CINAHL, and Web of Science. Additionally, websites hosting clinical practice guidelines were searched for any updates related to antipsychotic medications and weight gain. Searches were supplemented by reviewing the reference lists from other relevant publications. Search terms included antipsychotic*, obes*, switching, intervention*, topiramate, metformin, behav*, and systematic review. Only studies conducted between February 28, 2005 and February 28, 2015 were considered. Additionally, only studies available in English and obtainable as full-text using the University of Hawaii at Hilo journal subscriptions were used. Only interventions focused upon weight loss were considered and limited to the following intervention strategies: switching medications, adjunct medications, and behavioral interventions. Combination interventions (such as adjunct medication plus behavioral intervention) were excluded with the assumption that combination therapies are generally considered more effective than single interventions alone. Interventions that did not focus primarily upon weight or did not report weight-related outcomes were excluded. Interventions focused upon dietary and physical activity changes were also excluded, as these are considered standard care for weight management. Studies of child, adolescent, and inpatient populations were excluded as this guideline is focused upon adults in the outpatient setting. Potentially relevant studies were identified for each review question and search result titles and abstracts were screened according to the inclusion and exclusion criteria. Those papers identified for inclusion were then obtained in full text and further reviewed against the inclusion and exclusion criteria. The studies were then classified according to a hierarchy of evidence, utilizing systematic reviews first and then high-quality randomized-controlled trials. Number of Source Documents 21 articles were included in the evidence review, including 12 systematic reviews and 9 high quality randomized controlled trials. Refer to Appendix A for a flow diagram of article selection according to each review question. Note that the number of systematic reviews cited in the flow diagrams is greater than the number listed here. This discrepancy is a result of systematic reviews that included more than one intervention type in their analysis, and were therefore, listed more than once in the article selection process.
149 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 149 Methods Used to Assess the Quality and Strength of the Evidence The quality and strength of included studies were rated according to the Grading of Recommendations Assessment, Development, and Evaluation criteria (see scheme given below). Rating Scheme for the Strength of the Evidence Overall Quality of Outcome Evidence according to Grading of Recommendations Assessment, Development, and Evaluation (GRADE). Level High quality Moderate quality Low quality Very low quality Description We are very confident that the true effect lies close to that of the estimate of the effect We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of effect We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect Methods Used to Analyze the Evidence Meta-Analysis Review of Published Meta-Analyses Systematic Review with Evidence Tables Description of the Methods Used to Analyze the Evidence Included studies were critically appraised using the GRADE risk of bias assessment criteria. Key information was then extracted regarding each study s methods, PICO factors, and results. Where possible, meta-analyses were conducted to combine the results of the studies for each review question according to the outcomes of interest. This was done using Cochrane Review Manager (RevMan5) software. Pooled risk ratios were calculated for binary outcomes. Pooled measures of central tendency (means) and variation (standard deviation) were calculated for continuous outcomes. For interpretation of binary outcome results, differences in the absolute event rate were calculated using software developed by the GRADE working group (GRADEpro) using data reported in the control group of included studies. For interpretation of continuous data, mean ranges for control groups were manually entered and the anticipated absolute effects for each intervention were calculated by GRADEpro according to the data from the meta-analyses. The quality of evidence for each outcome in each intervention was assessed using the GRADE quality assessment criteria. Evidence profiles were then generated for each review question (see Appendix B) and summaries of findings were created (see Appendix C). The GRADE Guideline Development Tool (GDT) was then
150 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 150 used to make specific recommendations regarding each review question, using an evidence-to-decision table (see Appendix D). Methods Used to Formulate Recommendations Author determination GRADE evidence-to-decision tables (Appendix D) Description of Methods Used to Formulate the Recommendation Recommendations were formulated using the GRADE Guideline Development Tool after reviewing: -The evidence summaries for each review question -Findings from similar systematic reviews -Expert consensus statements regarding antipsychotic medications and obesity. -Cost-analyses of interventions (when available) -Studies of patient outcome and intervention preferences (when available) Rating Scheme for the Strength of the Recommendation The wording of recommendations conforms to the standards set by the GRADE Guideline Development Tool, whereby a strong recommendation uses the words we recommend and a weak recommendation uses the words we suggest. Cost Analysis The literature was searched for economic data regarding each of the interventions reviewed. Unfortunately, there was limited evidence available for determining the costeffectiveness of the interventions included. When possible, cost information was included the guideline development tables (Appendix D). Method of Guideline Validation External Peer Review Description of Method of Guideline Validation A draft of the guideline was reviewed by an interdisciplinary panel of key stakeholders including: -Advance Practice Nurses -Family members of patients affected -Family Practice Physicians -Other Healthcare Professionals/Experts -Primary Care Providers -Psychiatrists Participating reviewers used the AGREE II (Appraisal of Guidelines for Research and
151 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 151 Evaluation II) instrument to assess the quality and applicability of the guideline. Major Recommendations Generic Principles of Care Recommendations All adults taking antipsychotic medication should have their weight routinely checked at the start of therapy and at regular intervals thereafter. Weight should be evaluated in relation to height by calculating the patient s Body Mass Index (BMI) to screen for overweight or obesity. Define the degree of overweight or obesity in adults according to the following table: Classification BMI (kg/m 2 ) Healthy weight Overweight Obesity I Obesity II Obesity III 40 or more Interpret BMI with caution by considering individual differences in muscularity, fitness level, age, gender, racial/ethnic group, and comorbidities. Offer lifestyle interventions for weight management according to the patient s risk and preferences, following standard obesity management guidelines for the general adult population. Specific Principles of Care Weight gain and associated metabolic dysfunction are now recognized as significant problems primarily associated with the newer (second-generation or atypical) antipsychotic medications (Leucht et al., 2013). Prevalence rates of antipsychotic-associated weight gain are between 15% to 72% (De Hert et al., 2011), with some medications having much greater weight-gain liability than others (Leucht et al., 2013). Additionally, several studies report that psychotropic medication-associated weight gain is distressing to patients (McCloughen & Foster, 2011) and may represent an important barrier to medication adherence (DiBonaventura, Gabriel, Dupclay, Gupta, & Kim, 2012; Weiden, Mackell, & McDonnell, 2004). Furthermore, individuals with severe mental illness experience significant physical health disparities, with markedly higher rates of obesity, as well as increased morbidity and mortality overall (De Hert et al., 2011). Recommendation #1: Medication Switching
152 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 152 We recommend switching antipsychotic medication for patients who have experienced >5% body weight increase since the initiation of therapy, if the patient is willing to consider switching and has a relapse prevention and safety plan in place. Justification Systematic reviews report that an elective switch from antipsychotics with high weightgain liability to those with low weight-gain potential can improve weight outcomes with minimal risk of psychiatric deterioration (Grande et al., 2014; John W. Newcomer, Weiden, & Buchanan, 2013). With any medication switch, however, the potential for relapse exists and patients, in collaboration with the healthcare team, should have plan in place to ensure safety. Subgroup Considerations A systematic review of medication adherence in schizophrenia reports that lack of insight, medication beliefs, and substance abuse are key drivers of medication nonadherence (Higashi et al., 2013). These factors require careful assessment by the treatment team for patients considering medication switching. Risks of medication nonadherence include increased risk of relapse, hospitalization, and suicide (Higashi et al., 2013). Additionally, expert authors assert that patients with long-term (several years) exposure to an antipsychotic with high weight-gain liability are less likely to benefit from medication switching, whereas patients with relatively short-term exposure are more likely to benefit (Hasnain, Vieweg, & Hollett, 2012). Implementation Consideration Systematic reviews do not report any significant differences in outcomes associated with the medication switching strategy (i.e. abrupt stop/start versus cross-tapering) in patients taking antipsychotics (Mukundan, Faulkner, Cohn, & Remington, 2010; John W. Newcomer et al., 2013). In general, however, a cross-tapering strategy (where the current medication is gradually reduced while a new medication is gradually increased) is believed by many to reduce the risk of adverse effects and discontinuation of treatment (Buckley & Correll, 2008; John W. Newcomer et al., 2013). Medication should be switched from those with high weight-gain liability to those with lower weight-gain potential. The following list of antipsychotics (including both first- and secondgeneration antipsychotics) is ordered from highest weight-gain potential (olanzapine) to lowest weight potential (haloperidol) according to a recent meta-analysis (Leucht et al., 2013): olanzipine (highest weight-gain potential) zotepine clozapine iloperidone
153 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 153 Definitions chlorpromazine sertindole quetiapine risperidone paliperidone asenapine amisulpride aripiprazole lurasidone ziprasidone haloperidol (lowest weight-gain potential) Relapse prevention and safety plan There are many forms that a relapse prevention plan can take, but in general, they are written statements that include collaboratively identified warning signs of relapse (i.e. difficulty sleeping, decreased tolerability of auditory hallucinations) and are specific to the individual client. For each symptom, coping skills are identified that have been helpful to the patient in the past. In addition to coping skills, an action plan is included that usually involves contacting the prescriber for urgent follow-up. A safety plan should also be included, in case of further escalation of symptoms. A safety plan includes written instructions that direct the patient toward a mental health telephone crisis line and/or the nearest emergency department, should he or she begin to experience suicidal and/or homicidal thoughts, or other thoughts of self-harm. Recommendation #2: Adjunct Medications We suggest offering adjunct medications (metformin or topiramate) for patients taking antipsychotics who have experienced >5% body weight increase since initiation of therapy, particularly those patients who are reluctant to switch to an antipsychotic with lower weight-gain potential and for whom lifestyle interventions have been (or are likely to be) unsuccessful. Adjunct medication should be offered in conjunction with lifestyle modification for maximum weight loss benefit. Justification Antipsychotic-associated weight gain is most pronounced during the first 12 weeks of treatment and early intervention has been shown to substantially reduce and/or reverse weight gain while also preventing related metabolic effects (Newall et al., 2012). Systematic reviews evaluating the efficacy of metformin for antipsychoticassociated weight gain consistently report clinically significant weight loss with low rates of adverse effects (Fiedorowicz et al., 2012; Hasnain, Fredrickson, & Vieweg, 2011;
154 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 154 Mizuno et al., 2014; Newall et al., 2012). Systematic reviews regarding topiramate also report significant weight loss, however, there is much greater variability in the incidence and severity of adverse effects (Generali & Cada, 2014; Mahmood, Booker, Huang, & Coleman, 2013). Appendix A provides a summary of findings for the outcomes related to using adjunct medications for this problem. Additionally, studies consistently report that adjunct medications for managing antipsychotic-associated weight gain show the most benefit when combined with lifestyle interventions (Hasnain et al., 2011). Subgroup Considerations Studies assessing adjunct pharmacotherapy in antipsychotic-associated weight gain include patients primarily taking olanzapine and clozapine (Mizuno et al., 2014). This finding suggests greater effect for patients taking these medications, and lesser effect for patients taking antipsychotics with lower weight-gain liability. Additionally, older patients with long-term exposure to antipsychotic-induced weight gain benefit less from metformin, than younger newly-exposed patients (Hasnain et al., 2012). This finding suggests that the best candidates for metformin adjunct therapy are those that are younger and have a shorter history of antipsychotic use. In terms of adverse effects, metformin is associated with the rare occurrence of lactic acidosis, primarily in patients with renal insufficiency and has also been recently associated with the generation of amyloid-beta proteins, involved in the development of Alzheimer's disease. These findings suggest that metformin should be used cautiously in elderly patients and those with renal impairment and/or cognitive decline (Björkhem-Bergman, Asplund, & Lindh, 2011). In studies of topiramate, reduction in general psychopathologic symptoms were reported in patient's with schizophrenia (Mahmood et al., 2013). This suggests that patients with schizophrenia may achieve additional benefit from topiramate, beyond the medication's weight loss effect. Implementation Considerations The FDA has not yet approved metformin for medication-associated weight gain. The use of metformin for this purpose would be considered "off-label." The FDA has approved topiramate (in combination with phentermine, under the brand name Qsymia) for general weight loss. For metformin, gastrointestinal symptoms (nausea, diarrhea, and bloating) are the most common side effects (up to 30%). These symptoms can be avoided with gradual dose increases and administration with food. Additionally, metformin is not reported to have any significant drug-drug interactions, including with antipsychotic medications (Newall et al., 2012). Topiramate is associated with a number of side effects including paresthesia, hypoesthesia, changes in taste, cognitive impairment, and acute glaucoma (rare). These side effects must be discussed with patients considering topiramate as an adjunctive therapy (Ellinger, Ipema, & Stachnik, 2010; Kramer et al., 2011). The incidence of side effects is reported as greater at higher doses, although these appear to diminish over the course of treatment (Ko, Joe, Jung, & Kim, 2005). In regard to its weight loss effect, studies of topiramate report that longer duration of treatment and higher doses are associated with greater weight loss (Ko et al., 2005; Kramer et al., 2011).
155 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 155 Recommendation #3: Cognitive-Behavioral Therapy We suggest offering cognitive-behavioral therapy to all patients taking antipsychotic medications who may be concerned about weight gain as a side effect, have more than 1 risk factor for obesity, or have already experienced weight gain. Justification Systematic reviews of behavioral interventions for reducing antipsychotic-associated weight gain report that these interventions, in combination with lifestyle changes, produce modest weight reduction (Alvarez-Jimenez, Hetrick, Gonzalez-Blanch, Gleeson, & McGorry, 2008; Faulkner, Cohn, & Remington, 2007). Additionally, behavioral interventions appear to help patients prevent weight gain when initiated early in the course of antipsychotic therapy (Alvarez-Jimenez et al., 2008; Gabriele, Dubbert, & Reeves, 2009). The cost-effectiveness of this approach, however, is not certain, nor is it's relative superiority compared to more traditional educational interventions for nutrition and physical activity (Alvarez-Jimenez et al., 2008). Subgroup Considerations There were no significant subgroup differences noted in the literature. One systematic review reports that there were similar effects between groups with chronic illness and first-episode psychosis (Bonfioli, Berti, Goss, Muraro, & Burti, 2012). Implementation Considerations Group interventions appear to be as effective as individual interventions for preventing weight gain and promoting weight loss (Alvarez-Jimenez et al., 2008), providing a more cost-effective option for patients and payers. Longer length of intervention and followup appears to produce greater weight loss (Gabriele et al., 2009). Monitoring and Evaluation A consensus statement on antipsychotic drugs and obesity recommends weight monitoring at 4, 8, and 12 weeks after initiating or changing antipsychotic therapy, and every 3 months thereafter (American Diabetes Association, 2004). Clinical Algorithm See Appendix E for larger image.
156 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 156 Figure 1: Clinical algorithm for the management of antipsychotic-associated weight gain. Refer to Appendices C and D. Potential Benefits Evidence Supporting the Recommendations Benefits/Harms of Implementing Guideline Recommendations Appropriate identification, assessment, and management of antipsychotic-associated weight gain. Refer to in Appendix D for further information regarding the balance of benefits and harms for each intervention. Potential Harms Risk of relapse, hospitalization, and suicide with medication switching. Side effects of adjunct medications used.
157 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 157 Unclear cost-effectiveness of cognitive-behavioral therapy for weight loss. Qualifying Statements This guideline represents the views of one author after careful evaluation of the evidence for interventions to manage antipsychotic-associated weight gain. The recommendations reflect the best evidence at the time of publication and continued research may result in new knowledge that generates different recommendations. The guideline does not replace the individual responsibility of healthcare professionals to make clinical decisions based upon the circumstances of the individual patient, the context of care, and the product information for any of the medications suggested. Implementation of this guideline is at the sole discretion of the healthcare professional, in collaboration with the patient and the treatment team. Treatment and care should be tailored to the individual needs and preferences of patients. Decisions about treatment should be patient-directed with supportive guidance from the healthcare professional. Appropriate information must be provided to the patient regarding the potential benefits and harms of each intervention option, before treatment decisions are made. The guideline recommends some medications for indications that have not been approved by the FDA, but only if there was good evidence to support their use. The decision to use such medications is the sole responsibility of the medication prescriber. Description of the Implementation Strategy Implementation of the Guideline An implementation strategy is pending external peer review. Implementation Tools Clinical Algorithm Mobile Device Resources Institute of Medicine (IOM) National Healthcare Quality Report Categories IOM Care Need Getting Better Living with Illness
158 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 158 IOM Domain Staying Healthy Effectiveness Equity Patient-centeredness Safety Identifying Information and Availability Pending peer review and evaluation of the guideline.
159 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 159 Appendix A: Summary of Article Selection Summary of Article Selection Medication Switching Figure 2: Stages of article selection for systematic review of medication switching. Summary of Article Selection Adjunct Medication Figure 3: Stages of article selection for systematic review of adjunct medication.
160 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 160 Summary of Article Selection Cognitive-Behavioral Therapy Figure 4: Stages of article selection for systematic review of cognitive-behavioral therapy.
, Stroup et al.")
161 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 161 Evidence Profile Medication Switching Appendix B: Evidence Profile Tables Included studies: John W Newcomer et al. (2008), Stroup et al. (2011)
, Baptista et al. (2007), Carrizo et al. (2009), Narula, Rehan, Unni, and Gupta (2010), Wu, Zhao, Jin, and et al.")
162 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 162 Evidence Profile Adjunct Medication Included studies: Afshar et al. (2009), Baptista et al. (2007), Carrizo et al. (2009), Narula, Rehan, Unni, and Gupta (2010), Wu, Zhao, Jin, and et al. (2008)
, Khazaal et al.")
163 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 163 Evidence Profile Cognitive-Behavioral Therapy Included studies: Attux et al. (2013), Khazaal et al. (2007), Weber and Wyne (2006)
, Stroup et al.")
164 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 164 Appendix C: Summary of Findings Summary of Findings Medication Switching Included studies: John W Newcomer et al. (2008), Stroup et al. (2011)
, Baptista et al. (2007), Carrizo et al. (2009), Narula et al.")
165 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 165 Summary of Findings Adjunct Medication Included studies: Afshar et al. (2009), Baptista et al. (2007), Carrizo et al. (2009), Narula et al. (2010), Wu et al. (2008)
, Khazaal et al.")
166 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 166 Summary of Findings Cognitive-Behavioral Therapy Included studies: Attux et al. (2013), Khazaal et al. (2007), Weber and Wyne (2006)

167 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 167 Appendix D: Evidence to Decision Tables Evidence to Decision Table Medication Switching
168 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 168
169 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 169

170 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 170

171 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 171 Evidence to Decision Table Adjunct Medication
172 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 172
173 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 173
174 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 174

175 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 175

176 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 176 Evidence to Decision Table Cognitive-Behavioral Therapy
177 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 177
178 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 178
179 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 179
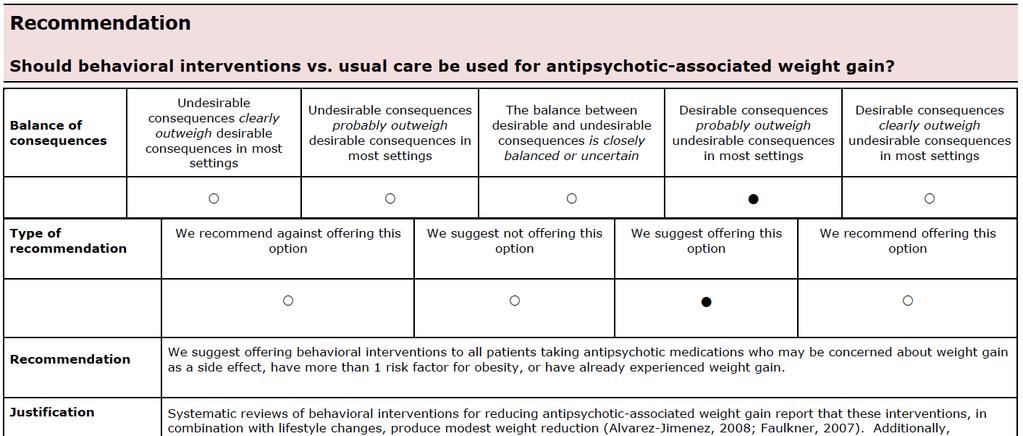
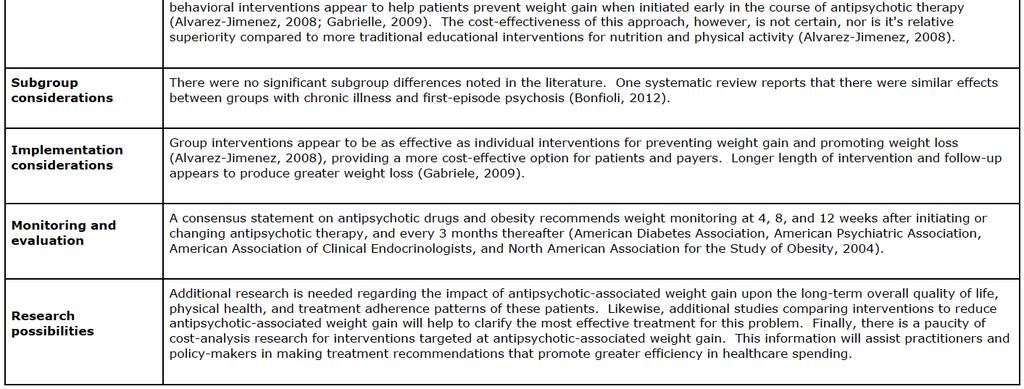
180 ANTIPSYCHOTIC MEDICATION-ASSOCIATED WEIGHT GAIN 180
Meccanismi fisiopatologici e trattamento dei disturbi metabolici in soggetti affetti da disturbo mentale grave
 Meccanismi fisiopatologici e trattamento dei disturbi metabolici in soggetti affetti da disturbo mentale grave Francesco Bartoli, MD, PhD Università degli Studi di Milano Bicocca Ospedale San Gerardo di
Meccanismi fisiopatologici e trattamento dei disturbi metabolici in soggetti affetti da disturbo mentale grave Francesco Bartoli, MD, PhD Università degli Studi di Milano Bicocca Ospedale San Gerardo di
Metabolic Monitoring, Schizophrenia Spectrum Illnesses, & Second Generation Antipsychotics
 Metabolic Monitoring, Schizophrenia Spectrum Illnesses, & Second Generation Antipsychotics National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental
Metabolic Monitoring, Schizophrenia Spectrum Illnesses, & Second Generation Antipsychotics National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental
Promoting and Monitoring Evidenced-Based Antipsychotic Prescribing Practices in Children and Adolescents: Florida Medicaid Initiatives
 Promoting and Monitoring Evidenced-Based Antipsychotic Prescribing Practices in Children and Adolescents: Florida Medicaid Initiatives Mary Elizabeth Jones, Pharm BSc, RPh Senior Pharmacist AHCA Pharmacy
Promoting and Monitoring Evidenced-Based Antipsychotic Prescribing Practices in Children and Adolescents: Florida Medicaid Initiatives Mary Elizabeth Jones, Pharm BSc, RPh Senior Pharmacist AHCA Pharmacy
Class Update: Oral Antipsychotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Antipsychotics. Something Old, Something New, Something Used to Treat the Blues
 Antipsychotics Something Old, Something New, Something Used to Treat the Blues Objectives To provide an overview of the key differences between first and second generation agents To an overview the newer
Antipsychotics Something Old, Something New, Something Used to Treat the Blues Objectives To provide an overview of the key differences between first and second generation agents To an overview the newer
Pharmacotherapy of psychosis and schizophrenia in youth
 Pharmacotherapy of psychosis and schizophrenia in youth Benedetto Vitiello Pavia, 2 December 2017 Disclosure Benedetto Vitiello, M.D. Professor of Child and Adolescent Neuropsychiatry University of Turin,
Pharmacotherapy of psychosis and schizophrenia in youth Benedetto Vitiello Pavia, 2 December 2017 Disclosure Benedetto Vitiello, M.D. Professor of Child and Adolescent Neuropsychiatry University of Turin,
Minimising the Impact of Medication on Physical Health in Schizophrenia
 Minimising the Impact of Medication on Physical Health in Schizophrenia John Donoghue Liverpool Imagination is more important than knowledge Albert Einstein LIFESTYLE Making choices TREATMENT Worse Psychopathology,
Minimising the Impact of Medication on Physical Health in Schizophrenia John Donoghue Liverpool Imagination is more important than knowledge Albert Einstein LIFESTYLE Making choices TREATMENT Worse Psychopathology,
FL Medicaid Drug Therapy Management Program for Behavioral Health Monitoring for Safety and Quality
 FL Medicaid Drug Therapy Management Program for Behavioral Health Monitoring for Safety and Quality April 23, 2014 Pensacola, FL Presentation Objectives To briefly describe the program and how its components
FL Medicaid Drug Therapy Management Program for Behavioral Health Monitoring for Safety and Quality April 23, 2014 Pensacola, FL Presentation Objectives To briefly describe the program and how its components
EARLY ONSET SCHIZOPHRENIA
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences EARLY ONSET SCHIZOPHRENIA JON MCCLELLAN CHILD STUDY AND TREATMENT CENTER GENERAL DISCLOSURES The University of Washington
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences EARLY ONSET SCHIZOPHRENIA JON MCCLELLAN CHILD STUDY AND TREATMENT CENTER GENERAL DISCLOSURES The University of Washington
Network Meta-Analyses of Antipsychotics for Schizophrenia: Clinical Implications
 Network Meta-Analyses of Antipsychotics for Schizophrenia: Clinical Implications JOHN M. DAVIS, MD Professor of Psychiatry University of Illinois at Chicago Chicago, Illinois and STEFAN LEUCHT, MD Klinik
Network Meta-Analyses of Antipsychotics for Schizophrenia: Clinical Implications JOHN M. DAVIS, MD Professor of Psychiatry University of Illinois at Chicago Chicago, Illinois and STEFAN LEUCHT, MD Klinik
PORT, 2009 Spain, 2009 Malaysia, 2009 Singapore, 2009 BAP, 2011 WFSBP, 2012 SIGN, 2013 Harvard NICE RANZCP, 2016
 Appendix 3. Comparison of recommendations from clinical practice guidelines. Data extracted in relation to key health questions that are relevant to a clinician adopting an algorithmic approach to the
Appendix 3. Comparison of recommendations from clinical practice guidelines. Data extracted in relation to key health questions that are relevant to a clinician adopting an algorithmic approach to the
Hearts and Minds An ECG Update. Tuesday 18 th November The Met Hotel, Leeds
 Hearts and Minds An ECG Update Tuesday 18 th November The Met Hotel, Leeds Ashleigh Bradley Specialist Clinical Pharmacist for Mental Health and Lithium Clinic Airedale NHS Foundation Trust Introduction
Hearts and Minds An ECG Update Tuesday 18 th November The Met Hotel, Leeds Ashleigh Bradley Specialist Clinical Pharmacist for Mental Health and Lithium Clinic Airedale NHS Foundation Trust Introduction
Is Lurasidone more safe and effective in the treatment ofschizoaffective disorder and schizophrenia than other commonanti-psychotic medications?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2015 Is Lurasidone more safe and effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2015 Is Lurasidone more safe and effective
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Psychosis and schizophrenia in children and young people: recognition and management 1.1 Short title Psychosis and schizophrenia
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Psychosis and schizophrenia in children and young people: recognition and management 1.1 Short title Psychosis and schizophrenia
Michael J. Bailey, M.D. OptumHealth Public Sector
 Michael J. Bailey, M.D. OptumHealth Public Sector LIHP Quality Charter To ensure the quality of care delivered to enrollees in San Diego County Assistance Programs, such as County Medical Services (CMS)
Michael J. Bailey, M.D. OptumHealth Public Sector LIHP Quality Charter To ensure the quality of care delivered to enrollees in San Diego County Assistance Programs, such as County Medical Services (CMS)
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
Psychotropic Medication. Including Role of Gradual Dose Reductions
 Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]
![SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]](/thumbs/80/80440271.jpg "SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]") SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003 Rationale The SiGMA algorithm
SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003 Rationale The SiGMA algorithm
SCHIZOPHRENIA. For Primary Care Providers. Project ECHO LA Adult Psychiatry ECHO June 25, 2014
 SCHIZOPHRENIA For Primary Care Providers Project ECHO LA Adult Psychiatry ECHO June 25, 2014 Curley L. Bonds, MD Medical Director Didi Hirsch Mental Health Services SCHIZOPHRENIA The most common psychotic
SCHIZOPHRENIA For Primary Care Providers Project ECHO LA Adult Psychiatry ECHO June 25, 2014 Curley L. Bonds, MD Medical Director Didi Hirsch Mental Health Services SCHIZOPHRENIA The most common psychotic
Abbreviated Class Review: Long-Acting Injectable Antipsychotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Abbreviated Class Review: Long-Acting Injectable Antipsychotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
The Brain and the Body: Medical Comorbidities in Psychiatric Illness. Kate Miley, CNP Psychiatric Nurse Practitioner, HCMC Adult Psychiatry Clinic
 The Brain and the Body: Medical Comorbidities in Psychiatric Illness Kate Miley, CNP Psychiatric Nurse Practitioner, HCMC Adult Psychiatry Clinic The Problem: Health Disparities in SMI Life expectancy
The Brain and the Body: Medical Comorbidities in Psychiatric Illness Kate Miley, CNP Psychiatric Nurse Practitioner, HCMC Adult Psychiatry Clinic The Problem: Health Disparities in SMI Life expectancy
Method. NeuRA Paliperidone August 2016
 Introduction Second generation antipsychotics (sometimes referred to as atypical antipsychotics) are a newer class of antipsychotic medication than first generation typical antipsychotics. Second generation
Introduction Second generation antipsychotics (sometimes referred to as atypical antipsychotics) are a newer class of antipsychotic medication than first generation typical antipsychotics. Second generation
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist. HMS Training Webinar January 27, 2017
 Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia
 Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
MEDICAL ASSISTANCE HANDBOOK PRIOR AUTHORIZATION OF PHARMACEUTICAL SERVICES. I. Requirements for Prior Authorization of Antipsychotics
 MEDICAL ASSISTANCE HBOOK PRI AUTHIZATION OF PHARMACEUTICAL SERVICES I. Requirements for Prior Authorization of Antipsychotics A. Prescriptions That Require Prior Authorization Prescriptions for Antipsychotics
MEDICAL ASSISTANCE HBOOK PRI AUTHIZATION OF PHARMACEUTICAL SERVICES I. Requirements for Prior Authorization of Antipsychotics A. Prescriptions That Require Prior Authorization Prescriptions for Antipsychotics
PRIMARY CARE MANAGEMENT OF OBESITY
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences PRIMARY CARE MANAGEMENT OF OBESITY LYDIA CHWASTIAK MD, MPH ASSOCIATE PROFESSOR UNIVERSITY OF WASHINGTON DEPARTMENT
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences PRIMARY CARE MANAGEMENT OF OBESITY LYDIA CHWASTIAK MD, MPH ASSOCIATE PROFESSOR UNIVERSITY OF WASHINGTON DEPARTMENT
More than We Bargained For: Metabolic Side Effects of Antipsychotic Medications
 More than We Bargained For: Metabolic Side Effects of Antipsychotic Medications Michael D. Jibson, MD, PhD Professor of Psychiatry University of Michigan Disclosure In the past 12 months I have received
More than We Bargained For: Metabolic Side Effects of Antipsychotic Medications Michael D. Jibson, MD, PhD Professor of Psychiatry University of Michigan Disclosure In the past 12 months I have received
Schizophrenia and bipolar disorders are lifelong
 THE STANDARD OF CARE IN TREATING PSYCHIATRIC DISORDERS Peter J. Weiden, MD,* and David G. Daniel, MD ABSTRACT In recent years, several guidelines and algorithms have appeared to help clinicians address
THE STANDARD OF CARE IN TREATING PSYCHIATRIC DISORDERS Peter J. Weiden, MD,* and David G. Daniel, MD ABSTRACT In recent years, several guidelines and algorithms have appeared to help clinicians address
Atypical Antipsychotic Use for the Behavioural and Psychological Symptoms of Dementia in the Elderly
 Overall Comprehensive Research Plan: Atypical Antipsychotic Use for the Behavioural and Psychological Symptoms of Dementia in the Elderly October 9, 2014 30 Bond Street, Toronto ON, M5B 1W8 www.odprn.ca
Overall Comprehensive Research Plan: Atypical Antipsychotic Use for the Behavioural and Psychological Symptoms of Dementia in the Elderly October 9, 2014 30 Bond Street, Toronto ON, M5B 1W8 www.odprn.ca
Introduction. Objectives. Psychotropic Medications & Cardiometabolic Risk
 Psychotropic Medications & Cardiometabolic Risk Sam Ellis, PharmD, BCPS, CDE Associate Professor University of Colorado School of Pharmacy Introduction Second GenerationAntipsychotics (SGA) first FDA approved
Psychotropic Medications & Cardiometabolic Risk Sam Ellis, PharmD, BCPS, CDE Associate Professor University of Colorado School of Pharmacy Introduction Second GenerationAntipsychotics (SGA) first FDA approved
Choosing Wisely Psychiatry s Top Priorities for Appropriate Primary Care
 Choosing Wisely Psychiatry s Top Priorities for Appropriate Primary Care JASON BEAMAN D.O., M.S., FAPA ASSISTANT CLINICAL PROFESSOR CHAIR, DEPARTMENT OF PSYCHIATRY AND BEHAVIORAL SCIENCES OKLAHOMA STATE
Choosing Wisely Psychiatry s Top Priorities for Appropriate Primary Care JASON BEAMAN D.O., M.S., FAPA ASSISTANT CLINICAL PROFESSOR CHAIR, DEPARTMENT OF PSYCHIATRY AND BEHAVIORAL SCIENCES OKLAHOMA STATE
Re: Safety data on Zyprexa (olanzapine) and Symbyax (olanzapine and fluoxetine HCl capsules) Hyperglycemia, Weight Gain, and Hyperlipidemia
 and Symbyax (olanzapine and fluoxetine HCl capsules) Hyperglycemia, Weight Gain, and Hyperlipidemia") www.lilly.com Eli Lilly and Company Lilly Corporate Center Indianapolis, Indiana 46285 U.S.A. Phone 317 276 2000 October 5, 2007 Re: Safety data on Zyprexa (olanzapine) and Symbyax (olanzapine and fluoxetine
www.lilly.com Eli Lilly and Company Lilly Corporate Center Indianapolis, Indiana 46285 U.S.A. Phone 317 276 2000 October 5, 2007 Re: Safety data on Zyprexa (olanzapine) and Symbyax (olanzapine and fluoxetine
I received help from Bosch Health Care
 John Kasckow, MD, PhD VA Pittsburgh Health Care System Western Psychiatric Institute and Clinic, UPMC VA Pittsburgh Health Care System I received help from Bosch Health Care 1 Diagnoses of Interest Early
John Kasckow, MD, PhD VA Pittsburgh Health Care System Western Psychiatric Institute and Clinic, UPMC VA Pittsburgh Health Care System I received help from Bosch Health Care 1 Diagnoses of Interest Early
Treatment of Schizophrenia
 Treatment of Schizophrenia Conduct comprehensive assessment and use measurement-based care as found in the Principles of Practice (review pages 4-7). Most importantly assess social support system (housing,
Treatment of Schizophrenia Conduct comprehensive assessment and use measurement-based care as found in the Principles of Practice (review pages 4-7). Most importantly assess social support system (housing,
Antipsychotic Prior Authorization Request
 Antipsychotic Prior Authorization Request Commonwealth of Massachusetts MassHealth Drug Utilization Review Program P.O. Box 2586, Worcester, MA 01613-2586 Fax: 1-877-208-7428 Phone: 1-800-745-7318 MassHealth
Antipsychotic Prior Authorization Request Commonwealth of Massachusetts MassHealth Drug Utilization Review Program P.O. Box 2586, Worcester, MA 01613-2586 Fax: 1-877-208-7428 Phone: 1-800-745-7318 MassHealth
Objectives. Pre Discussion Question #2. Disparity in Care Demographics
 Objectives Implementation of a pharmacist driven metabolic monitoring protocol for second generation antipsychotics (SGAs) Jonathan Willett, PharmD PGY 1 Pharmacy Practice Resident Chickasaw Nation March
Objectives Implementation of a pharmacist driven metabolic monitoring protocol for second generation antipsychotics (SGAs) Jonathan Willett, PharmD PGY 1 Pharmacy Practice Resident Chickasaw Nation March
Preferred Practice Guidelines Bipolar Disorder in Children and Adolescents
 BadgerCare Plus Preferred Practice Guidelines Bipolar Disorder in Children and Adolescents These Guidelines are based in part on the following: American Academy of Child and Adolescent Psychiatry s Practice
BadgerCare Plus Preferred Practice Guidelines Bipolar Disorder in Children and Adolescents These Guidelines are based in part on the following: American Academy of Child and Adolescent Psychiatry s Practice
AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE
 AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE Topic AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE Scope 4.3.1 (a) Review question(s)
AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE Topic AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE Scope 4.3.1 (a) Review question(s)
Antipsychotic-Related Risk for Weight Gain and Metabolic Abnormalities During Development Christoph U. Correll, MD
 Antipsychotic-Related Risk for Weight Gain and Metabolic Abnormalities During Development Christoph U. Correll, MD Professor of Psychiatry and Molecular Medicine Hofstra North Shore - LIJ School of Medicine
Antipsychotic-Related Risk for Weight Gain and Metabolic Abnormalities During Development Christoph U. Correll, MD Professor of Psychiatry and Molecular Medicine Hofstra North Shore - LIJ School of Medicine
Role of Clozapine in Treatment-Resistant Schizophrenia
 Disease Management and Treatment Strategies Elkis H, Meltzer HY (eds): Therapy-Resistant Schizophrenia. Adv Biol Psychiatry. Basel, Karger, 2010, vol 26, pp 114 128 Role of Clozapine in Treatment-Resistant
Disease Management and Treatment Strategies Elkis H, Meltzer HY (eds): Therapy-Resistant Schizophrenia. Adv Biol Psychiatry. Basel, Karger, 2010, vol 26, pp 114 128 Role of Clozapine in Treatment-Resistant
Comparative incidence of metabolic syndrome in patients with schizophrenia. being treated with second generation antipsychotics vs.
 Comparative incidence of metabolic syndrome in patients with schizophrenia being treated with second generation antipsychotics vs. first generation antipsychotics: A Systematic Review of Literature By
Comparative incidence of metabolic syndrome in patients with schizophrenia being treated with second generation antipsychotics vs. first generation antipsychotics: A Systematic Review of Literature By
Platforms for Performance: Clinical Dashboards to Improve Quality and Safety 2011 Midyear Clinical Meeting
 Improving Mental Health Outcomes in Veterans Through Dashboard Technology Learning Objectives 1. Describe VA Academic Detailing 2. Show how an increase in metabolic monitoring and a decrease in off-label
Improving Mental Health Outcomes in Veterans Through Dashboard Technology Learning Objectives 1. Describe VA Academic Detailing 2. Show how an increase in metabolic monitoring and a decrease in off-label
Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD
 Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD Define BPSD and review the spectrum of associated symptoms Review pharmacologic and non-pharmacologic treatments for BPSD Evaluate
Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD Define BPSD and review the spectrum of associated symptoms Review pharmacologic and non-pharmacologic treatments for BPSD Evaluate
Literature Scan: Parenteral Antipsychotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Age 18 years and older BMI 18.5 and < 25 kg/m 2
 Quality ID #128 (NQF 0421): Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up Plan National Quality Strategy Domain: Community/Population Health 2018 OPTIONS F INDIVIDUAL MEASURES:
Quality ID #128 (NQF 0421): Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up Plan National Quality Strategy Domain: Community/Population Health 2018 OPTIONS F INDIVIDUAL MEASURES:
Epidemiology of Psychosis
 Epidemiology of Psychosis Chris Gale Otago Registrar Training Group Feb 2011. Methodologies used. Population surveys. General population. High risk populations. Screener and re-interview. Case records
Epidemiology of Psychosis Chris Gale Otago Registrar Training Group Feb 2011. Methodologies used. Population surveys. General population. High risk populations. Screener and re-interview. Case records
National Academy of Science July 17-18, 2018 Washington DC Larry Alphs, MD, PhD RESTRICTION OF TREATMENT QUALITY IN PRAGMATIC CLINICAL TRIALS
 National Academy of Science July 17-18, 2018 Washington DC Larry Alphs, MD, PhD RESTRICTION OF TREATMENT QUALITY IN PRAGMATIC CLINICAL TRIALS Key Points for RWE in Randomized Clinical Trials What is the
National Academy of Science July 17-18, 2018 Washington DC Larry Alphs, MD, PhD RESTRICTION OF TREATMENT QUALITY IN PRAGMATIC CLINICAL TRIALS Key Points for RWE in Randomized Clinical Trials What is the
RECOMMENDATIONS FOR GROWTH MONITORING, PREVENTION AND MANAGEMENT OF OVERWEIGHT AND OBESITY IN CHILDREN AND YOUTH IN PRIMARY HEALTH CARE 2015
 Slide 2 Use of deck RECOMMENDATIONS FOR GROWTH MONITORING, PREVENTION AND MANAGEMENT OF OVERWEIGHT AND OBESITY IN CHILDREN AND YOUTH IN PRIMARY HEALTH CARE 2015 These slides are made available publicly
Slide 2 Use of deck RECOMMENDATIONS FOR GROWTH MONITORING, PREVENTION AND MANAGEMENT OF OVERWEIGHT AND OBESITY IN CHILDREN AND YOUTH IN PRIMARY HEALTH CARE 2015 These slides are made available publicly
Medication Audit Checklist- Antipsychotics - Atypical
 Medication Audit checklist Page 1 of 7 10-2018 Audit number: Client number: Ordering Provider: INDICATIONS 1) Disorders with psychotic symptoms (schizophrenia, schizoaffective disorder, manic disorders,
Medication Audit checklist Page 1 of 7 10-2018 Audit number: Client number: Ordering Provider: INDICATIONS 1) Disorders with psychotic symptoms (schizophrenia, schizoaffective disorder, manic disorders,
Cardiometabolic Side Effects of Risperidone in Children with Autism
 Cardiometabolic Side Effects of Risperidone in Children with Autism Susan J. Boorin, MSN, PMHNP-BC PhD Candidate Yale School of Nursing 1 This speaker has no conflicts of interest to disclose. 2 Boorin
Cardiometabolic Side Effects of Risperidone in Children with Autism Susan J. Boorin, MSN, PMHNP-BC PhD Candidate Yale School of Nursing 1 This speaker has no conflicts of interest to disclose. 2 Boorin
February 7-9, 2019 The Westin Fort Lauderdale Florida. Provided by
 February 7-9, 2019 The Westin Fort Lauderdale Florida Provided by Addressing Your Greatest Concerns in Schizophrenia Management: From Suicide to Relapse Prevention and the Role of LAIs John Lauriello,
February 7-9, 2019 The Westin Fort Lauderdale Florida Provided by Addressing Your Greatest Concerns in Schizophrenia Management: From Suicide to Relapse Prevention and the Role of LAIs John Lauriello,
ANTIPSYCHOTIC POLYPHARMACY
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences ANTIPSYCHOTIC POLYPHARMACY RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UWMC GENERAL DISCLOSURES The University
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences ANTIPSYCHOTIC POLYPHARMACY RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UWMC GENERAL DISCLOSURES The University
Age 18 years and older BMI 18.5 and < 25 kg/m 2
 Quality ID #128 (NQF 0421): Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up Plan National Quality Strategy Domain: Community/Population Health 2018 OPTIONS F INDIVIDUAL MEASURES:
Quality ID #128 (NQF 0421): Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up Plan National Quality Strategy Domain: Community/Population Health 2018 OPTIONS F INDIVIDUAL MEASURES:
Use of Psychotherapeutic Medications in Children and Adolescents with ASD and ID
 Use of Psychotherapeutic Medications in Children and Adolescents with ASD and ID Although not considered first line treatment in children with ASD and ID, depending on the severity of symptoms, some medications
Use of Psychotherapeutic Medications in Children and Adolescents with ASD and ID Although not considered first line treatment in children with ASD and ID, depending on the severity of symptoms, some medications
Current Non-Preferred Agents
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Type of intervention Secondary prevention and treatment. Economic study type Cost-effectiveness analysis.
 Modelling the treated course of schizophrenia: development of a discrete event simulation model Heeg B M, Buskens E, Knapp M, van Aalst G, Dries P J, de Haan L, van Hout B A Record Status This is a critical
Modelling the treated course of schizophrenia: development of a discrete event simulation model Heeg B M, Buskens E, Knapp M, van Aalst G, Dries P J, de Haan L, van Hout B A Record Status This is a critical
Aggression (Severe) in Children under Age 6
 in Children under Age 6") Aggression (Severe) in Children under Age 6 Level 0 Comprehensive diagnostic assessments. Refer to Principles of Practice on page 6. Evaluate and treat comorbid conditions (i.e. medical, other psychiatric
Aggression (Severe) in Children under Age 6 Level 0 Comprehensive diagnostic assessments. Refer to Principles of Practice on page 6. Evaluate and treat comorbid conditions (i.e. medical, other psychiatric
In recent years, reports of diabetes, diabetic
 A REVIEW OF METABOLIC ISSUES IN ATYPICAL ANTIPSYCHOTIC TREATMENT John W. Newcomer, MD, * and Henry A. Nasrallah, MD ABSTRACT Reports of diabetes, diabetic ketoacidosis, hyperglycemia, and dyslipidemias
A REVIEW OF METABOLIC ISSUES IN ATYPICAL ANTIPSYCHOTIC TREATMENT John W. Newcomer, MD, * and Henry A. Nasrallah, MD ABSTRACT Reports of diabetes, diabetic ketoacidosis, hyperglycemia, and dyslipidemias
Measure #383 (NQF 1879): Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety
: Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety") Measure #383 (NQF 1879): Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
Measure #383 (NQF 1879): Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
SP.236 / ESG.SP236 Exploring Pharmacology Spring 2009
 MIT OpenCourseWare http://ocw.mit.edu SP.236 / ESG.SP236 Exploring Pharmacology Spring 2009 For information about citing these materials or our Terms of Use, visit: http://ocw.mit.edu/terms. Atypical (2
MIT OpenCourseWare http://ocw.mit.edu SP.236 / ESG.SP236 Exploring Pharmacology Spring 2009 For information about citing these materials or our Terms of Use, visit: http://ocw.mit.edu/terms. Atypical (2
Table of Contents. 1.0 Policy Statement...1
 Division of Medical Assistance General Clinical Policy No. A-6 Table of Contents 1.0 Policy Statement...1 2.0 Policy Guidelines...1 2.1 Eligible Recipients...1 2.1.1 General Provisions...1 2.1.2 EPSDT
Division of Medical Assistance General Clinical Policy No. A-6 Table of Contents 1.0 Policy Statement...1 2.0 Policy Guidelines...1 2.1 Eligible Recipients...1 2.1.1 General Provisions...1 2.1.2 EPSDT
Recent Advances in the Antipsychotic Treatment of People with schizophrenia. Robert W. Buchanan, M.D.
 Recent Advances in the Antipsychotic Treatment of People with schizophrenia Robert W. Buchanan, M.D. Antipsychotic medications are the primary class of drugs used in the pharmacological treatment of schizophrenia.
Recent Advances in the Antipsychotic Treatment of People with schizophrenia Robert W. Buchanan, M.D. Antipsychotic medications are the primary class of drugs used in the pharmacological treatment of schizophrenia.
ESSENTIAL SHARED CAR E AGREEMENT FOR
 E093 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, or Amisulpride for Behavioural indications in People with Learning Disability (LD) Referral Criteria In some
E093 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, or Amisulpride for Behavioural indications in People with Learning Disability (LD) Referral Criteria In some
What Team Members Other Than Prescribers Need To Know About Antipsychotics
 What Team Members Other Than Prescribers Need To Know About Antipsychotics The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State
What Team Members Other Than Prescribers Need To Know About Antipsychotics The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State
Quality Standards. Schizophrenia Care in the Community for Adults. October 2017
 Quality Standards Schizophrenia Care in the Community for Adults October 2017 Summary This quality standard addresses care for adults aged 18 years and older with a primary diagnosis of schizophrenia (including
Quality Standards Schizophrenia Care in the Community for Adults October 2017 Summary This quality standard addresses care for adults aged 18 years and older with a primary diagnosis of schizophrenia (including
Disclosure. Speaker Bureaus. Grant Support. Pfizer Forest Norvartis. Pan American Health Organization/WHO NIA HRSA
 Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
-Guidelines for the discontinuation of oral antipsychotics in patients with BPSD within the primary care setting Summary- Quetiapine
 -Guidelines for the discontinuation of oral antipsychotics in patients with BPSD within the primary care setting Summary- Quetiapine An independent report Time for action 1 by Professor Sube Banerjee looked
-Guidelines for the discontinuation of oral antipsychotics in patients with BPSD within the primary care setting Summary- Quetiapine An independent report Time for action 1 by Professor Sube Banerjee looked
Epidemiology of Psychosis
 Epidemiology of Psychosis Chris Gale Otago Registrar Training Group Feb 2011. Methodologies used. Population surveys. General population. High risk populations. Screener and re-interview. Case records
Epidemiology of Psychosis Chris Gale Otago Registrar Training Group Feb 2011. Methodologies used. Population surveys. General population. High risk populations. Screener and re-interview. Case records
BLONANSERIN. THERAPEUTICS Brands Lonasen see index for additional brand names
 BLONANSERIN THERAPEUTICS Brands Lonasen see index for additional brand names Generic? No Class Atypical antipsychotic (serotonin dopamine antagonist; second-generation antipsychotic; also a potential mood
BLONANSERIN THERAPEUTICS Brands Lonasen see index for additional brand names Generic? No Class Atypical antipsychotic (serotonin dopamine antagonist; second-generation antipsychotic; also a potential mood
Clinical Guidelines for the Pharmacologic Treatment of Schizophrenia
 Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Expert Committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report
 Expert Committee s Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report (1) Overview material Release Date December 2007 Status Available in
Expert Committee s Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report (1) Overview material Release Date December 2007 Status Available in
Illinois CHIPRA Medical Home Project Baseline Results
 Illinois CHIPRA Medical Home Project Baseline Results On the National Committee for Quality Assurance Patient Centered Medical Home Self-Assessment June 25, 2012 Prepared by MetroPoint Research & Evaluation,
Illinois CHIPRA Medical Home Project Baseline Results On the National Committee for Quality Assurance Patient Centered Medical Home Self-Assessment June 25, 2012 Prepared by MetroPoint Research & Evaluation,
Slide 1. Slide 2. Slide 3. About this module. About this module. Antipsychotics: The Essentials Module 5 A Primer on Selected Antipsychotics
 Slide 1 Antipsychotics: The Essentials Module 5 A Primer on Selected Antipsychotics Flavio Guzmán, MD Slide 2 About this module 13 antipsychotics will be studied 3 first generation antipsychotics 10 second
Slide 1 Antipsychotics: The Essentials Module 5 A Primer on Selected Antipsychotics Flavio Guzmán, MD Slide 2 About this module 13 antipsychotics will be studied 3 first generation antipsychotics 10 second
Chapter 161 Antipsychotics
 Chapter 161 Antipsychotics Episode Overview Extrapyramidal syndromes are a common complication of antipsychotic medications. First line treatment is benztropine or diphenhydramine. Lorazepam is used in
Chapter 161 Antipsychotics Episode Overview Extrapyramidal syndromes are a common complication of antipsychotic medications. First line treatment is benztropine or diphenhydramine. Lorazepam is used in
ASENAPINE. THERAPEUTICS Brands SAPHRIS see index for additional brand names
 ASENAPINE THERAPEUTICS Brands SAPHRIS see index for additional brand names Generic? No Class Neuroscience-based Nomenclature: dopamine, serotonin, norepinephrine receptor antagonist (DSN-RAn) Atypical
ASENAPINE THERAPEUTICS Brands SAPHRIS see index for additional brand names Generic? No Class Neuroscience-based Nomenclature: dopamine, serotonin, norepinephrine receptor antagonist (DSN-RAn) Atypical
Out with the Old In with the New: Novel, Neuroscience-Based Re-Classification of Psychiatric Medications
 Program Outline Out with the Old In with the New: Novel, Neuroscience-Based Re-Classification of Psychiatric Medications Rajiv Tandon, MD Professor of Psychiatry University of Florida College of Medicine
Program Outline Out with the Old In with the New: Novel, Neuroscience-Based Re-Classification of Psychiatric Medications Rajiv Tandon, MD Professor of Psychiatry University of Florida College of Medicine
COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP)
") European Medicines Agency London, 15 November 2007 Doc. Ref. EMEA/CHMP/EWP/517497/2007 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON CLINICAL EVALUATION OF MEDICINAL PRODUCTS USED
European Medicines Agency London, 15 November 2007 Doc. Ref. EMEA/CHMP/EWP/517497/2007 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON CLINICAL EVALUATION OF MEDICINAL PRODUCTS USED
UNDERSTANDING AND MANAGING METABOLIC SYNDROME IN PSYCHIATRY Dr Sanil Rege MBBS, MRCPsych, FRANZCP Consultation-Liaison Psychiatry PaRK MHS, Western
 UNDERSTANDING AND MANAGING METABOLIC SYNDROME IN PSYCHIATRY Dr Sanil Rege MBBS, MRCPsych, FRANZCP Consultation-Liaison Psychiatry PaRK MHS, Western Australia Talks Facilitator of the CTF Exam Prep Course
UNDERSTANDING AND MANAGING METABOLIC SYNDROME IN PSYCHIATRY Dr Sanil Rege MBBS, MRCPsych, FRANZCP Consultation-Liaison Psychiatry PaRK MHS, Western Australia Talks Facilitator of the CTF Exam Prep Course
Elements for a Public Summary
 VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Schizophrenia Schizophrenia is a mental illness with a number of symptoms, including confused or unclear thinking and speech,
VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Schizophrenia Schizophrenia is a mental illness with a number of symptoms, including confused or unclear thinking and speech,
Executive Summary. Context. Guideline Origins
 Executive Summary Context In America today, tobacco stands out as the agent most responsible for avoidable illness and death. Millions of Americans consume this toxin on a daily basis. Its use brings premature
Executive Summary Context In America today, tobacco stands out as the agent most responsible for avoidable illness and death. Millions of Americans consume this toxin on a daily basis. Its use brings premature
CHCS. Multimorbidity Pattern Analyses and Clinical Opportunities: Dementia. Center for Health Care Strategies, Inc. FACES OF MEDICAID DATA SERIES
 CHCS Center for Health Care Strategies, Inc. FACES OF MEDICAID DATA SERIES Multimorbidity Pattern Analyses and Clinical Opportunities: Dementia December 2010 Cynthia Boyd, MD, MPH* Bruce Leff, MD* Carlos
CHCS Center for Health Care Strategies, Inc. FACES OF MEDICAID DATA SERIES Multimorbidity Pattern Analyses and Clinical Opportunities: Dementia December 2010 Cynthia Boyd, MD, MPH* Bruce Leff, MD* Carlos
Client Report Screening Program Results For: Missouri Western State University October 28, 2013
 Client Report For: Missouri Western State University October 28, 2013 Executive Summary PROGRAM OVERVIEW From 1/1/2013-9/30/2013, Missouri Western State University participants participated in a screening
Client Report For: Missouri Western State University October 28, 2013 Executive Summary PROGRAM OVERVIEW From 1/1/2013-9/30/2013, Missouri Western State University participants participated in a screening
Practical Psychopharmacology for More Complex Mental Health Presentations
 MINISTRY OF CHILDREN AND YOUTH SERVICES Practical Psychopharmacology for More Complex Mental Health Presentations Part 2: Antipsychotics & Mood Stabilizers Dr. Ajit Ninan & Joel Lamoure 1 : Who are we?
MINISTRY OF CHILDREN AND YOUTH SERVICES Practical Psychopharmacology for More Complex Mental Health Presentations Part 2: Antipsychotics & Mood Stabilizers Dr. Ajit Ninan & Joel Lamoure 1 : Who are we?
SYNOPSIS. Risperidone-R064766: Clinical Study Report RIS-USA-232 (FOR NATIONAL AUTHORITY USE ONLY)
") SYNOPSIS Protocol No.: RIS-USA-232 Title of Study: Efficacy and Safety of a Flexible Dose of Risperidone Versus Placebo in the Treatment of Psychosis of Alzheimer's Disease Principal Investigator: M.D.
SYNOPSIS Protocol No.: RIS-USA-232 Title of Study: Efficacy and Safety of a Flexible Dose of Risperidone Versus Placebo in the Treatment of Psychosis of Alzheimer's Disease Principal Investigator: M.D.
Antipsychotics: The Essentials. Module 5: A Primer on Selected Antipsychotics
 Antipsychotics: The Essentials Module 5: A Primer on Selected Antipsychotics Slide 1 Recently approved antipsychotics Iloperidone (Fanapt) - 2009 Asenapine (Saphris, Sycrest) - 2009 Lurasidone (Latuda)
Antipsychotics: The Essentials Module 5: A Primer on Selected Antipsychotics Slide 1 Recently approved antipsychotics Iloperidone (Fanapt) - 2009 Asenapine (Saphris, Sycrest) - 2009 Lurasidone (Latuda)
SYNOPSIS. Clinical Study Report CN138002: Addendum 1. Individual Study Table Referring to the Dossier
 Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Abilify Name of Active Ingredient: aripiprazole Individual Study Table Referring to the Dossier (For National Authority Use Only)
Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Abilify Name of Active Ingredient: aripiprazole Individual Study Table Referring to the Dossier (For National Authority Use Only)
Collaborating, Co-managing and Facilitating Metabolic Improvement in Patients with Severe Mental Illness (SMI)
") Collaborating, Co-managing and Facilitating Metabolic Improvement in Patients with Severe Mental Illness (SMI) 14 th Canadian Collaborative Mental Health Care Conference Montréal, Québec June 28, 2013
Collaborating, Co-managing and Facilitating Metabolic Improvement in Patients with Severe Mental Illness (SMI) 14 th Canadian Collaborative Mental Health Care Conference Montréal, Québec June 28, 2013
Clinical Policy: Olanzapine Long-Acting Injection (Zyprexa Relprevv) Reference Number: CP.PHAR.292 Effective Date: Last Review Date: 08.
 Reference Number: CP.PHAR.292 Effective Date: Last Review Date: 08.") Clinical Policy: (Zyprexa Relprevv) Reference Number: CP.PHAR.292 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid See Important Reminder at the end of this policy for important
Clinical Policy: (Zyprexa Relprevv) Reference Number: CP.PHAR.292 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid See Important Reminder at the end of this policy for important
First Episode Schizophrenia
 First Episode Schizophrenia Abigail Donovan, M.D. Assistant Professor of Psychiatry, Harvard Medical School Director, First Episode and Early Psychosis Program MGH Schizophrenia Program Massachusetts General
First Episode Schizophrenia Abigail Donovan, M.D. Assistant Professor of Psychiatry, Harvard Medical School Director, First Episode and Early Psychosis Program MGH Schizophrenia Program Massachusetts General
Mental Health Medicines Management Pilot. Community Pharmacy. High Dose Antipsychotic Screening, Education & Advice Service
 Mental Health Medicines Management Pilot Community Pharmacy High Dose Antipsychotic Screening, Education & Advice Service Approved Version 1 Date of First Issue Review Date Date of Issue Author / Contact
Mental Health Medicines Management Pilot Community Pharmacy High Dose Antipsychotic Screening, Education & Advice Service Approved Version 1 Date of First Issue Review Date Date of Issue Author / Contact
Severe Mental Illness and Diabetes. Charlie Place
 Severe Mental Illness and Diabetes Charlie Place Intro Me Community Mental Health Nurse Case manager for Assertive Outreach Team in Leeds Severe Mental Illness (SMI) usually diagnosis of schizophrenia
Severe Mental Illness and Diabetes Charlie Place Intro Me Community Mental Health Nurse Case manager for Assertive Outreach Team in Leeds Severe Mental Illness (SMI) usually diagnosis of schizophrenia
THIOTHIXENE. THERAPEUTICS Brands Navane see index for additional brand names. Generic? Yes
 THIOTHIXENE THERAPEUTICS Brands Navane see index for additional brand names Generic? Yes Class Conventional antipsychotic (neuroleptic, thioxanthene, dopamine 2 antagonist) Commonly Prescribed for (bold
THIOTHIXENE THERAPEUTICS Brands Navane see index for additional brand names Generic? Yes Class Conventional antipsychotic (neuroleptic, thioxanthene, dopamine 2 antagonist) Commonly Prescribed for (bold
Measure #383 (NQF 1879): Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety
: Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety") Measure #383 (NQF 1879): Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety 2017 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Measure #383 (NQF 1879): Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety 2017 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
SFHPT02 Develop a formulation and treatment plan with the client in cognitive and behavioural therapy
 Develop a formulation and treatment plan with the client in cognitive Overview This standard shows how the cognitive and behavioural therapist works collaboratively with the client to help them understand
Develop a formulation and treatment plan with the client in cognitive Overview This standard shows how the cognitive and behavioural therapist works collaboratively with the client to help them understand
Pharmacy Medical Necessity Guidelines: Atypical Antipsychotic Medications. Effective: February 20, 2017
 Pharmacy Medical Necessity Guidelines: Effective: February 20, 2017 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy (RX) or Medical (MED)
Pharmacy Medical Necessity Guidelines: Effective: February 20, 2017 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy (RX) or Medical (MED)
LURASIDONE. THERAPEUTICS Brands LATUDA see index for additional brand names
 LURASIDONE THERAPEUTICS Brands LATUDA see index for additional brand names Generic? No Class Neuroscience-based Nomenclature: dopamine, serotonin receptor antagonist (DS-RAn) Atypical antipsychotic (serotonin-dopamine
LURASIDONE THERAPEUTICS Brands LATUDA see index for additional brand names Generic? No Class Neuroscience-based Nomenclature: dopamine, serotonin receptor antagonist (DS-RAn) Atypical antipsychotic (serotonin-dopamine
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: HIM.PA.59 Effective Date: 12/14 Last Review Date: 08/17 Line of Business: Health Insurance Marketplace Coding Implications Revision Log See Important Reminder at the
Clinical Policy: Reference Number: HIM.PA.59 Effective Date: 12/14 Last Review Date: 08/17 Line of Business: Health Insurance Marketplace Coding Implications Revision Log See Important Reminder at the
Policy Evaluation: Low Dose Quetiapine Safety Edit
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University 500 Summer Street NE, E35, Salem, Oregon 97301 1079 Phone 503 947 5220 Fax 503
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University 500 Summer Street NE, E35, Salem, Oregon 97301 1079 Phone 503 947 5220 Fax 503
Mr. E, age 37, has a 20-year history
 Antipsychotics for obsessive-compulsive disorder: Weighing risks vs benefits Taylor Modesitt, PharmD, Traci Turner, PharmD, BCPP, Lindsay Honaker, DO, Todd Jamrose, DO, Elizabeth Cunningham, DO, and Christopher
Antipsychotics for obsessive-compulsive disorder: Weighing risks vs benefits Taylor Modesitt, PharmD, Traci Turner, PharmD, BCPP, Lindsay Honaker, DO, Todd Jamrose, DO, Elizabeth Cunningham, DO, and Christopher