SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]
|
|
|
- Roy Haynes
- 6 years ago
- Views:
Transcription
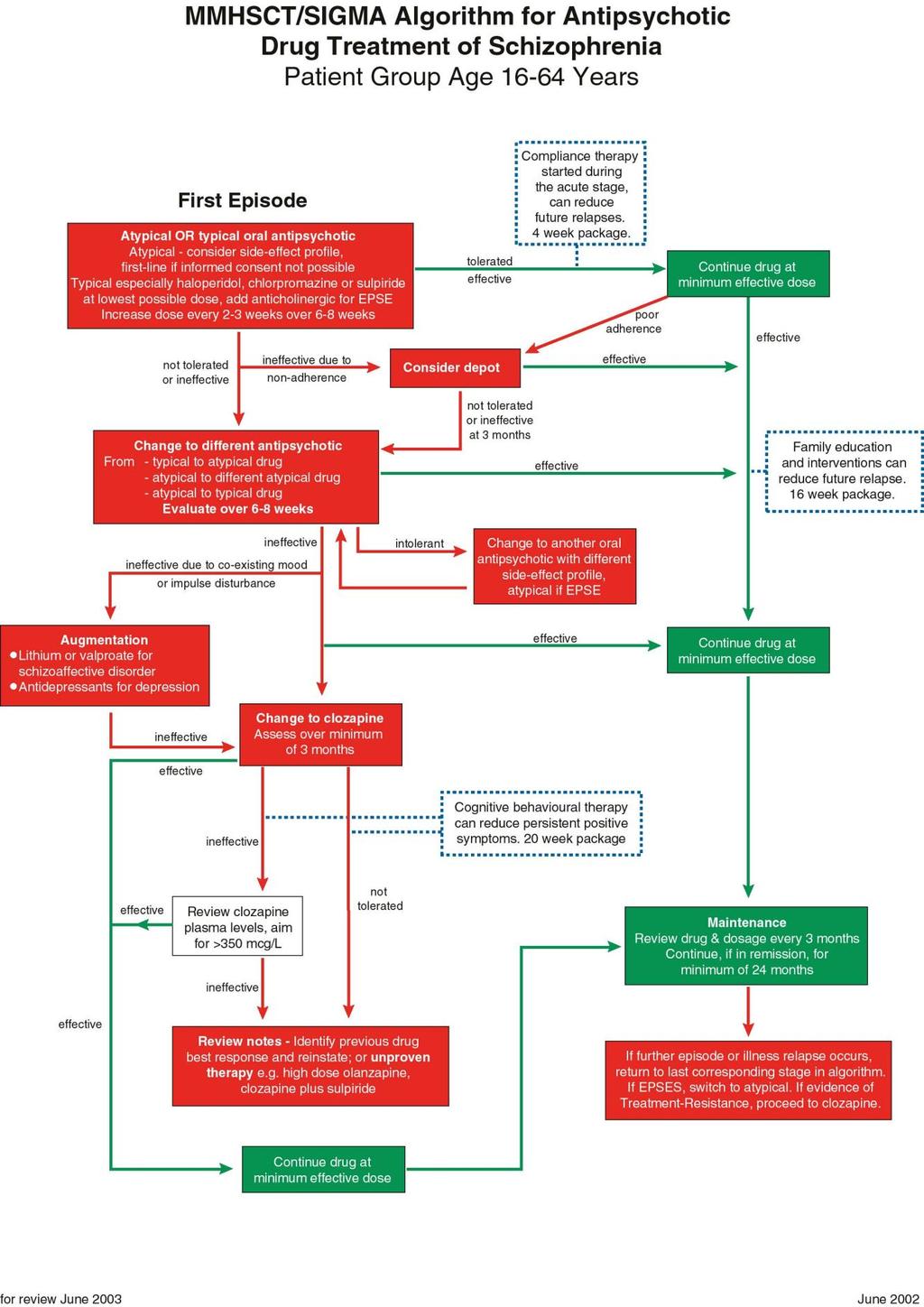
1 SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003
2 Rationale The SiGMA algorithm and corresponding guidelines for the antipsychotic treatment of schizophrenia and related disorders were developed out of the finding that across the twelve provider units of Greater Manchester, the use of, and expenditure on, clozapine and the other new atypical antipsychotic drugs varied greatly. There were no locally agreed standards or guidelines in place for the prescription of such drugs. Individual Trusts varied in whether they had current guidelines for the prescription of antipsychotic medication, the content of such guidelines, and the extent to which the guidelines were being followed by clinicians. The SiGMA guidelines have been adapted by the Manchester Mental Health and Social Care Trust Medicines Management Committee taking into account the NICE Guidelines Guidance on the use of newer (atypical) antipsychotic drugs for the treatment of schizophrenia. Scope The guidelines and accompanying algorithm offer a first-line choice of atypical or conventional antipsychotic treatment to be made in consultation with the patient, although the preferred treatment of choice would be an atypical antipsychotic. The algorithm avoids unnecessary delays in proceeding to clozapine, if appropriate and recognises evidence for psychological therapies in improving the outcome for patients with schizophrenia. Patient group: Primarily patients aged between years with schizophrenia or related functional disorders. For patients with these conditions who are elderly, lower doses than in younger adults should be considered and particular attention paid to side-effects.
3 SiGMA/ MMHSCT: Prescribing Antipsychotic Drugs in Schizophrenia Guidelines for use [compatible with NICE guidance] Prescribing policy: Pre-hospital treatment Agreed plan of action prior to contact with secondary care. Urgent assessment by secondary care needed. Treatment of a First Episode Choice of atypical or conventional antipsychotic choice made jointly by patient and clinician, although preferred treatment of choice would be an atypical antipsychotic 1. An atypical drug should be the treatment of choice when full discussion about choice of drug is not possible. Atypical Antipsychotic Drug Treatment The newer atypical drugs (amisulpride, olanzapine, quetiapine, risperidone, zotepine) are at least as effective first line agents as haloperidol and have less EPSEs. LE 1. The data for zotepine are not as secure as for other new atypicals. In diabetics and patients with risk factors for diabetes mellitus, receiving treatment with olanzapine, appropriate clinical and blood glucose monitoring should be conducted 2. Choice should be based on clinical considerations (efficacy, indications and likely side-effects) Sedation EPSE (haloperidol = +++) Increased prolactin Weight gain QTc prolongation Liquid Parenteral (IM) Preparation Amisulpride (+) (+) Yes No Olanzapine (+) Velotab Not licensed Quetiapine No No Risperidone + + (++ high Yes Yes 3 dose) Zotepine No No Key: - absent; (+)?absent or minor; + minor effect; ++ moderate effect; +++ severe effect 1 Situations in which typical antipsychotics favoured over atypical include: previous good efficacy and tolerability; need for parenteral antipsychotics in emergency treatment; intolerance of non-neurological side-effects; pregnancy 2 CSM Pharmacovigilance Report, April Separate guidance to be made available for usage
4 Suggested dosing schedules: Amisulpride Initial Dose At 14 days, if no response At days, if no response 400mg bd (100mg bd predom. negative Sx) 200mg bd (50mg bd predom. negative Sx) Olanzapine 10mg od 15mg od 20mg od Quetiapine 25mg bd day 1, 50mg bd day 2, 100mg bd day 3, 150mg bd day 4 300mg to 450mg/ day in divided doses 600mg bd max BNF dose(150mg bd predom. negative Sx) 500mg to 600mg/ day in divided doses, max 750mg/ day Risperidone 2mg od day 1, 4mg od day 2 6mg od 7mg od to recommended max 10mg od (BNF max 16mg od) Zotepine 25mg tds increasing at 4 days to 50mg tds 200mg to 300mg in three doses Max 300mg/ day When more than one atypical drug is considered appropriate choose the drug with the likely lowest purchase cost for that individual (see cost table below) Daily Dose 28 days hospital cost Basic NHS cost Haloperidol 10mg Risperidone 5mg Amisulpride 800mg Olanzapine 17.5mg Quetiapine 600mg Adapted from Oxford MH Guidelines Conventional Antipsychotic Drug Treatment Haloperidol, chlorpromazine or sulpiride are reasonable first line conventional treatments. Sedation EPSE Parenteral (IM) Preparation Haloperidol Yes Chlorpromazine Yes Sulpiride + + No Patients in a first episode are usually responsive to low doses, but are susceptible to EPSEs 4. Imaging studies show that drugs like haloperidol work when dopamine D2 receptor occupancy exceeds 60%. EPSEs emerge above 80% occupancy. Haloperidol 2 mg daily will give over 60% occupancy in most patients. Few first episode patients will need doses in excess of 6 mg haloperidol equivalents per day. 4 Extra-pyramidal side-effects
5 Suggested dosing schedules: Initial Dose At 14 days, if no response At days, if no response Haloperidol 1-2 mg bd 2-3 mg bd 3-5 mg bd Chlorpromazine mg bd mg bd mg bd Sulpiride 200 mg bd 400 mg bd 600 mg bd Psychotic symptom response can take days to begin. Haloperidol is a high potency drug 5. EPSEs are common, particularly acute dystonia, Parkinsonism and akathisia. There is a parenteral preparation. Chlorpromazine is more sedative. The recommendation for sulpiride recognises that it has a relative lack of EPSEs. Systematic review (of limited data) indicates that it is as effective as typical antipsychotics. Midpotency drugs such as chlorpromazine and sulpiride are probably preferable to haloperidol, in first episodes, due to the high incidence of EPSEs. LE1/ 2 For acutely agitated or disturbed patients, adding a sedative such as a short-acting benzodiazepine is better practice than using high dose antipsychotic treatment. Lorazepam 1-4mg orally or IM 6 hourly is recommended. For patients with anxiety symptoms, whilst the antipsychotic effects are awaited, diazepam 2-5 mg three times daily should be used. Neither drug should be continued on a regular basis for more than 2 weeks. LE 2 If EPSEs emerge, especially likely with the use of an initial conventional antipsychotic, one option is to add an adjunctive anticholinergic (such as procyclidine 5mg tds). The need for continuation should be reviewed every 3 months and withdrawal tried if no current EPSEs. At this point, the patient could equally be changed to a new atypical, bearing in mind that atypicals have their own side-effects e.g. weight gain. EPSEs in the first episode are known to be important causes of future non-compliance and their presence or absence should be monitored carefully, ideally using a valid side-effect rating scale. Similarly, akathisia responds poorly to anticholinergic drugs. Adding propranolol 30 mg daily or switching to an atypical drug should be considered. LE2 As needed (PRN) antipsychotic drug treatment should, if possible, be of the same medication as that given regularly, e.g. haloperidol up to 10 mg orally or IM up to 6 hourly. Initiating or changing an antipsychotic drug should be recorded in the case-notes, with reasons given for later reference. Record of progress including using simple rating scales for efficacy and tolerability at intervals is good practice in secondary care. All dosages should remain within those outlined within the BNF, following their recommendations for initiation and maintenance treatment. High dose prescribing is not advisable. Where undertaken, Royal College of Psychiatrists guidelines should be followed. The co-prescribing of two or more antipsychotic drugs at the same time, including atypical with typical drugs, apart from transitional periods, has no proven advantages in general 6. Disadvantages include increased side-effects and difficulty in calculating the total cumulative dose being taken. LE 1 5 Fewer milligrams needed for a clinical effect 6 But see later note under 4 th line treatment: Beyond clozapine
6 The following drugs should in general only be initiated by a psychiatrist: - Depot preparations Clozapine Second-stage treatment The new atypical drugs are less likely to cause EPSEs than haloperidol. Thus, they should be considered at this stage for patients receiving treatment with conventional antipsychotics who have unacceptable levels of EPSEs impairing quality of life or compliance. Also, they should be considered if first line conventional drugs have led to a poor clinical response after 6-8 weeks. There is little evidence that changing from one conventional to another if the first has not worked is worthwhile. LE 1 If an atypical has been used first line and led to unacceptable side-effects, choosing a drug with a different side-effect profile is advised. If there has been poor response there is a lack of evidence about the next step and it would be reasonable to choose a drug with different pharmacology. LE3 Resistant symptoms Clozapine is still the only drug whose efficacy has been shown to exceed all other antipsychotic drugs. It is prescribed for treatment-resistant schizophrenia and is effective in about 60% of patients. It is currently underused in clinical practice. LE1 Evidence of treatment-resistance is defined by NICE as the lack of satisfactory clinical improvement despite the sequential use of the recommended doses for 6-8 weeks of at least 2 antipsychotics, at least one of which should be an atypical. Recent trials of cognitive behavioural therapy (CBT) have shown improvements in patients with treatmentresistant schizophrenia. Its use alongside medication, including clozapine, can lead to improved quality of life and symptom outcomes. LE1 Beyond clozapine The use of sulpiride in addition to clozapine, in patients who are unresponsive to clozapine, has been tested in one small RCT. LE2 The addition of risperidone to clozapine may be effective in some cases. LE3 ECT has an effect on positive psychotic symptoms, but this lasts for 2-6 weeks only. LE2 Maintenance The minimum length of time a patient is maintained on antipsychotic drug treatment once in remission depends partly on the severity of past illness. Following a single first episode with a pre-treatment duration of illness of less than one month, a minimum maintenance period of 12 months is recommended. For a first episode with longer duration of untreated psychosis, or a second or later episode, a minimum of 2 years. The minimum effective dose should be used. Maintenance dosages below the lower limits of BNF ranges are associated with increased relapse, as are intermittent regimes. LE2 Depot typical antipsychotics are useful where adherence is intermittent, chaotic or unclear. They are not a solution for patients who explicitly do not wish to comply with any medication. They have a higher risk of EPSE than oral drugs, both conventional and atypical. Their pharmacokinetics mean that dose increases should not be more frequent than 8-weekly. They can continue to protect against relapse for several months after the drug is stopped. Depot atypical antipsychotics are now emerging and becoming licensed (e.g. risperidone Consta)
7 Acute relapse / Treatment of Further Episodes Advanced directives as to treatment choices in acute schizophrenic episodes should be developed where possible and documented in individuals care plans Assess likely reasons for relapse, including drug dose reduction, drug non-adherence, life stress, street drug abuse. Day-patient or inpatient admission may be needed. Review current antipsychotic drug and dosage. Where possible apply advanced directives and/ or make treatment choices jointly with individual based on informed discussion. If there has been good response to, and tolerance of, a specific typical drug previously, then this is the drug of choice. For patients experiencing further episodes or illness relapse with intolerable EPSE on conventional treatment, switch to treatment with an atypical agent. For patients with clear evidence of treatment resistance (i.e. 2 adequate trials of antipsychotic drugs) a decision could be made to proceed to treatment with clozapine. If relapse occurred off medication, including non-adherence, restart antipsychotic drug to which patient has responded previously. Choice of drug and dosage should be influenced first by a thorough review of past case-notes to evaluate past response, including side-effects, to individual drugs. Emergency Tranquillisation See separate MMHSCT Rapid Tranquillisation Guidelines Psychological interventions Family intervention therapy aims to educate the family about the illness and provide coping strategies. Systematic review has shown it to be effective in reducing relapse. LE 1 Compliance (concordance) therapy delivered in a package during treatment of an acute episode will enhance appropriate drug concordance and reduce future relapses. LE1 Cognitive behavioural therapy is effective in some patients with treatment-resistant positive symptoms (LE1) and probably accelerates remission in acute episodes (LE2) Distribution of Guidelines Copies to all clinicians who prescribe drugs All wards, home treatment services CMHTs These guidelines are intended to be evidence-based. They focus on pharmacological treatments. They reflect our interpretation of the best published evidence as of August 2002, but will change as new data emerge. Levels of evidence are cited as appropriate after statements in the glossary: LE1 is evidence based on systematic reviews or good quality randomised, controlled trials; LE2 is evidence based on good quality open trials or case control studies; LE3 is evidence based on uncontrolled trials or expert consensus only.
8
Mental Health Medicines Management Pilot. Community Pharmacy. High Dose Antipsychotic Screening, Education & Advice Service
 Mental Health Medicines Management Pilot Community Pharmacy High Dose Antipsychotic Screening, Education & Advice Service Approved Version 1 Date of First Issue Review Date Date of Issue Author / Contact
Mental Health Medicines Management Pilot Community Pharmacy High Dose Antipsychotic Screening, Education & Advice Service Approved Version 1 Date of First Issue Review Date Date of Issue Author / Contact
PORT, 2009 Spain, 2009 Malaysia, 2009 Singapore, 2009 BAP, 2011 WFSBP, 2012 SIGN, 2013 Harvard NICE RANZCP, 2016
 Appendix 3. Comparison of recommendations from clinical practice guidelines. Data extracted in relation to key health questions that are relevant to a clinician adopting an algorithmic approach to the
Appendix 3. Comparison of recommendations from clinical practice guidelines. Data extracted in relation to key health questions that are relevant to a clinician adopting an algorithmic approach to the
Antipsychotic Prescribing Audit:
 Antipsychotic Prescribing Audit: Measuring the impact of a prescribing intervention Audit Co-ordinator/ Author of Report: Supervisor: Professor Shôn W Lewis Table of Contents List of Tables... 3 List of
Antipsychotic Prescribing Audit: Measuring the impact of a prescribing intervention Audit Co-ordinator/ Author of Report: Supervisor: Professor Shôn W Lewis Table of Contents List of Tables... 3 List of
High Dose Antipsychotic Therapy (HDAT) guideline
 guideline") Document level: Trustwide (TW) Code: MP18 Issue number: 2 High Dose Antipsychotic Therapy (HDAT) guideline Lead executive Medical Director Author and contact number Lead Clinical Pharmacist 01625 663 857
Document level: Trustwide (TW) Code: MP18 Issue number: 2 High Dose Antipsychotic Therapy (HDAT) guideline Lead executive Medical Director Author and contact number Lead Clinical Pharmacist 01625 663 857
Document Title Antipsychotics Prescribing Guidelines for Schizophrenia
 Document Title Antipsychotics Prescribing Guidelines for Schizophrenia Document Description Document Type Prescribing Guidance Service Application Medicines Management Version 1.0 Policy Reference no.
Document Title Antipsychotics Prescribing Guidelines for Schizophrenia Document Description Document Type Prescribing Guidance Service Application Medicines Management Version 1.0 Policy Reference no.
Treatment of Schizophrenia Appendix Three Page 1 of 8
 Prescribing Guidelines Treatment of Schizophrenia Scope of this guidance This guidance aims to describe the pharmacological management of schizophrenia at a simple and intermediate level, with a brief
Prescribing Guidelines Treatment of Schizophrenia Scope of this guidance This guidance aims to describe the pharmacological management of schizophrenia at a simple and intermediate level, with a brief
MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES. MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) KEY ISSUES
 KEY ISSUES") MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) Medicines Management Services aim to ensure that (i) Service users receive their medicines
MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) Medicines Management Services aim to ensure that (i) Service users receive their medicines
Choosing and delivering ering interventions entions for
 Choosing and delivering ering interventions entions for psychosis and schizophrenia in adults bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to
Choosing and delivering ering interventions entions for psychosis and schizophrenia in adults bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to
High Dose Antipsychotic Medication Policy
 High Dose Antipsychotic Medication Policy Policy Title State previous title where relevant State if Policy New or Revised Policy Strand Org, HR, Clinical, H&S, Infection Control, Finance For clinical policies
High Dose Antipsychotic Medication Policy Policy Title State previous title where relevant State if Policy New or Revised Policy Strand Org, HR, Clinical, H&S, Infection Control, Finance For clinical policies
Clinical. High Dose Antipsychotic Prescribing Procedures. Document Control Summary. Contents
 Clinical High Dose Antipsychotic Prescribing Procedures Document Control Summary Status: Version: Author/Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation
Clinical High Dose Antipsychotic Prescribing Procedures Document Control Summary Status: Version: Author/Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation
PRESCRIBING GUIDELINES
 The Maudsley The South London and Maudsley NHS Foundation Trust & Oxleas NHS Foundation Trust PRESCRIBING GUIDELINES 10th Edition David Taylor Carol Paton Shitij Kapur informa healthcare Contents Authors
The Maudsley The South London and Maudsley NHS Foundation Trust & Oxleas NHS Foundation Trust PRESCRIBING GUIDELINES 10th Edition David Taylor Carol Paton Shitij Kapur informa healthcare Contents Authors
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Ongoing care for adults with psychosis or schizophrenia bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly
Ongoing care for adults with psychosis or schizophrenia bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly
HIGH DOSE ANTIPSYCHOTIC GUIDELINES (HDAT)
") HIGH DOSE ANTIPSYCHOTIC GUIDELINES (HDAT) Document Reference Version Number 2.00 High Dose Antipsychotic Guidelines (HDAT) G376 Author/Lead Job Title Jackie Stark Principal Pharmacist Clinical Services
HIGH DOSE ANTIPSYCHOTIC GUIDELINES (HDAT) Document Reference Version Number 2.00 High Dose Antipsychotic Guidelines (HDAT) G376 Author/Lead Job Title Jackie Stark Principal Pharmacist Clinical Services
Prescribing of high-dose and combined antipsychotics for patients on forensic wards.
 POMH-UK Topic 3 baseline May 2007 Prescribing of high-dose and combined antipsychotics for patients on forensic wards. Prepared by the Prescribing Observatory for Mental Health (POMH-UK) for member Healthcare
POMH-UK Topic 3 baseline May 2007 Prescribing of high-dose and combined antipsychotics for patients on forensic wards. Prepared by the Prescribing Observatory for Mental Health (POMH-UK) for member Healthcare
ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride (South Staffordshire Only)
") E099 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride (South Staffordshire Only) NOTE: Please complete details on P1 &3 Send one copy to GP, Patient and
E099 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride (South Staffordshire Only) NOTE: Please complete details on P1 &3 Send one copy to GP, Patient and
POLICY DOCUMENT. Pharmacy MMG/MPG. Approved By and Date Medicines Management roup March March 2016
 POLICY DOCUMENT Document Title High dose and combination antipsychotic guidance Reference Number n/a Policy Type Prescribing and Treatment Guideline Electronic File/Location Clinical Resources/Pharmacy/Prescribing
POLICY DOCUMENT Document Title High dose and combination antipsychotic guidance Reference Number n/a Policy Type Prescribing and Treatment Guideline Electronic File/Location Clinical Resources/Pharmacy/Prescribing
Formulary and Clinical Guideline Document Pharmacy Department Medicines Management Services
 Formulary and Clinical Guideline Document Pharmacy Department Medicines Management Services VIOLENCE, AGGRESSION OR SEVERE BEHAVIOURAL DISTURBANCE Introduction During an acute episode or illness, some
Formulary and Clinical Guideline Document Pharmacy Department Medicines Management Services VIOLENCE, AGGRESSION OR SEVERE BEHAVIOURAL DISTURBANCE Introduction During an acute episode or illness, some
SHARED CARE GUIDELINE
 SHARED CARE GUIDELINE Title: Prescribing and/ or Monitoring of Antipsychotics Scope: Pennine Care NHS Foundation Trust NHS Bury NHS Oldham NHS Heywood, Middleton and Rochdale NHS Stockport NHS Tameside
SHARED CARE GUIDELINE Title: Prescribing and/ or Monitoring of Antipsychotics Scope: Pennine Care NHS Foundation Trust NHS Bury NHS Oldham NHS Heywood, Middleton and Rochdale NHS Stockport NHS Tameside
The Deprescribing of Psychotropic Medication in Service Users (Patients) with Learning Disability
 with Learning Disability") The Deprescribing of Psychotropic Medication in Service Users (Patients) with Learning Disability Danielle Adams Principal Clinical Pharmacist Pharmacy and Medicines Optimisation Team HPFT July 2017 1
The Deprescribing of Psychotropic Medication in Service Users (Patients) with Learning Disability Danielle Adams Principal Clinical Pharmacist Pharmacy and Medicines Optimisation Team HPFT July 2017 1
ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride or Asenapine
 Ref No: E053 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride or Asenapine NOTE: Please complete details on P1 &3 Send one copy to GP, Patient and file
Ref No: E053 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride or Asenapine NOTE: Please complete details on P1 &3 Send one copy to GP, Patient and file
Olanzapine Long-Acting Injection (Zypadhera ) - Guidelines for Prescribing and Administration (Version 3 May 2015)
 - Guidelines for Prescribing and Administration (Version 3 May 2015)") 1. Key Points Olanzapine Long-Acting Injection (Zypadhera ) - Guidelines for Prescribing and Administration (Version 3 May 2015) 1.1 Olanzapine long acting injection (LAI) is indicated for the maintenance
1. Key Points Olanzapine Long-Acting Injection (Zypadhera ) - Guidelines for Prescribing and Administration (Version 3 May 2015) 1.1 Olanzapine long acting injection (LAI) is indicated for the maintenance
-Guidelines for the discontinuation of oral antipsychotics in patients with BPSD within the primary care setting Summary- Quetiapine
 -Guidelines for the discontinuation of oral antipsychotics in patients with BPSD within the primary care setting Summary- Quetiapine An independent report Time for action 1 by Professor Sube Banerjee looked
-Guidelines for the discontinuation of oral antipsychotics in patients with BPSD within the primary care setting Summary- Quetiapine An independent report Time for action 1 by Professor Sube Banerjee looked
Introduction to Drug Treatment
 Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
MMG012 GUIDELINES FOR THE USE OF HIGH DOSE ANTIPSYCHOTIC MEDICATION
 MMG012 GUIDELINES FOR THE USE OF HIGH DOSE ANTIPSYCHOTIC MEDICATION Page 1 of 16 Table of Contents Why we need this Policy... 3 What the Policy is trying to do... 3 Which stakeholders have been involved
MMG012 GUIDELINES FOR THE USE OF HIGH DOSE ANTIPSYCHOTIC MEDICATION Page 1 of 16 Table of Contents Why we need this Policy... 3 What the Policy is trying to do... 3 Which stakeholders have been involved
Preferred Prescribing Choices of Antipsychotic Drugs (APD) in Adults for Schizophrenia and Other Psychoses
 in Adults for Schizophrenia and Other Psychoses") Preferred Prescribing Choices of Antipsychotic Drugs (APD) in Adults for Schizophrenia and Other Psychoses HPFT Medicines Formulary lists the APDs that have been approved for use, however, it does not
Preferred Prescribing Choices of Antipsychotic Drugs (APD) in Adults for Schizophrenia and Other Psychoses HPFT Medicines Formulary lists the APDs that have been approved for use, however, it does not
Clinical guideline Published: 23 January 2013 nice.org.uk/guidance/cg155
 Psychosis and schizophrenia in children and young people: recognition and management Clinical guideline Published: 23 January 2013 nice.org.uk/guidance/cg155 NICE 2017. All rights reserved. Subject to
Psychosis and schizophrenia in children and young people: recognition and management Clinical guideline Published: 23 January 2013 nice.org.uk/guidance/cg155 NICE 2017. All rights reserved. Subject to
SECTION 9 : MANAGEMENT OF MOVEMENT DISORDERS AND EXTRAPYRAMIDAL SIDE EFFECTS
 SECTION 9 : MANAGEMENT OF MOVEMENT DISORDERS AND EXTRAPYRAMIDAL SIDE EFFECTS Formulary and Prescribing Guidelines 9.1 Introduction Movement disorders and extrapyramidal side effects can manifest in the
SECTION 9 : MANAGEMENT OF MOVEMENT DISORDERS AND EXTRAPYRAMIDAL SIDE EFFECTS Formulary and Prescribing Guidelines 9.1 Introduction Movement disorders and extrapyramidal side effects can manifest in the
Prescribing of high-dose and combination antipsychotics on adult acute and intensive care wards: Clinical introduction, methodology and glossary.
 POMH-UK Topic 1 report 1b Prescribing of high-dose and combination antipsychotics on adult : Clinical introduction, methodology and glossary. March 2007 Prepared by the Prescribing Observatory for Mental
POMH-UK Topic 1 report 1b Prescribing of high-dose and combination antipsychotics on adult : Clinical introduction, methodology and glossary. March 2007 Prepared by the Prescribing Observatory for Mental
S H A R E D P R E S C R I B I N G G U I D E L I N E
 S H A R E D P R E S C R I B I N G G U I D E L I N E Introduction This shared prescribing guideline for the second generation antipsychotic medications listed above has been developed with due consideration
S H A R E D P R E S C R I B I N G G U I D E L I N E Introduction This shared prescribing guideline for the second generation antipsychotic medications listed above has been developed with due consideration
Datix Ref:
 Title Document Details Shared Care Agreement: Antipsychotics (Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride or Asenapine) Trust Ref No 2081-38933 Local Ref (optional) Main points the document
Title Document Details Shared Care Agreement: Antipsychotics (Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride or Asenapine) Trust Ref No 2081-38933 Local Ref (optional) Main points the document
Rapid Tranquillisation for adolescent, adults and older people Medicines management team July 2014
 Rapid Tranquillisation for adolescent, adults and older people Medicines management team July 2014 A definition of rapid tranquillisation (RT) The use of medicines to quickly control extreme agitation,
Rapid Tranquillisation for adolescent, adults and older people Medicines management team July 2014 A definition of rapid tranquillisation (RT) The use of medicines to quickly control extreme agitation,
AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE
 AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE Topic AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE Scope 4.3.1 (a) Review question(s)
AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE Topic AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE Scope 4.3.1 (a) Review question(s)
Guidance on Consent to Treatment Documentation for Medication Patient s Detained under the Mental Health Act
 Guidance on Consent to Treatment Documentation for Medication Patient s Detained under the Mental Health Act This guidance is intended for Coventry and Warwickshire Partnership Trust staff to use when
Guidance on Consent to Treatment Documentation for Medication Patient s Detained under the Mental Health Act This guidance is intended for Coventry and Warwickshire Partnership Trust staff to use when
Psychotropic Drug Therapy in Adults with Learning Disability. Steve Wilkinson
 Psychotropic Drug Therapy in Adults with Learning Disability Steve Wilkinson Outline and Aims of the Session Drug use in learning disability Two distinct areas of drug therapy I. Treatment of common psychiatric
Psychotropic Drug Therapy in Adults with Learning Disability Steve Wilkinson Outline and Aims of the Session Drug use in learning disability Two distinct areas of drug therapy I. Treatment of common psychiatric
This shared care protocol covers when atypical antipsychotics are prescribed for the treatment of
 SHARED CARE PROTOCOL for ATYPICAL ANTIPSYCHOTICS SCOPE Greater Manchester West Mental health NHS Foundation Trust Bolton Primary Care Trust Salford Primary Care Trust Trafford Primary Care Trusts Issue
SHARED CARE PROTOCOL for ATYPICAL ANTIPSYCHOTICS SCOPE Greater Manchester West Mental health NHS Foundation Trust Bolton Primary Care Trust Salford Primary Care Trust Trafford Primary Care Trusts Issue
Treatment Options for Bipolar Disorder Contents
 Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Authorised by Greater Medicines Management Group
 SHARED CARE PROTOCOL for ATYPICAL ANTIPSYCHOTICS SCOPE Greater Manchester West Mental health NHS Foundation trust Bolton Primary Care Trust Salford Primary Care Trust Trafford Primary Care Trusts Issue
SHARED CARE PROTOCOL for ATYPICAL ANTIPSYCHOTICS SCOPE Greater Manchester West Mental health NHS Foundation trust Bolton Primary Care Trust Salford Primary Care Trust Trafford Primary Care Trusts Issue
ANTIPSYCHOTIC GUIDELINES
 ANTIPSYCHOTIC GUIDELINES TREATMENT OF SCHIZOPHRENIA AND PSYCHOSIS Page 1 of 44 Authors: Ms Diane Booth, Chief Pharmacist,. Mrs Kiran Hewitt, Lead Clinical Pharmacist, Berkshire Healthcare NHS Foundation
ANTIPSYCHOTIC GUIDELINES TREATMENT OF SCHIZOPHRENIA AND PSYCHOSIS Page 1 of 44 Authors: Ms Diane Booth, Chief Pharmacist,. Mrs Kiran Hewitt, Lead Clinical Pharmacist, Berkshire Healthcare NHS Foundation
Clinical guideline Published: 12 February 2014 nice.org.uk/guidance/cg178
 Psychosis and schizophrenia in adults: prevention ention and management Clinical guideline Published: 12 February 2014 nice.org.uk/guidance/cg178 NICE 2018. All rights reserved. Subject to Notice of rights
Psychosis and schizophrenia in adults: prevention ention and management Clinical guideline Published: 12 February 2014 nice.org.uk/guidance/cg178 NICE 2018. All rights reserved. Subject to Notice of rights
Schizophrenia: core interventions in the treatment and management of schizophrenia
 Schizophrenia: core interventions in the treatment and management of schizophrenia A guide for people with schizophrenia, their advocates and carers, and the public Information for the public (2 nd consultation)
Schizophrenia: core interventions in the treatment and management of schizophrenia A guide for people with schizophrenia, their advocates and carers, and the public Information for the public (2 nd consultation)
Introduction to psychotropic medications JAYNE CAMPBELL
 Introduction to psychotropic medications JAYNE CAMPBELL Introduction Psychotropic medications are prescription drugs that are commonly used to control some symptoms associated with many different types
Introduction to psychotropic medications JAYNE CAMPBELL Introduction Psychotropic medications are prescription drugs that are commonly used to control some symptoms associated with many different types
A systematic review of atypical antipsychotic drugs in schizophrenia. Atypical antipsychotic drugs in schizophrenia
 A systematic review of atypical antipsychotic drugs in schizophrenia Atypical antipsychotic drugs in schizophrenia A-M Bagnall 1 * S Gilbody 3 L Jones 1 L Davies 4 L Ginnelly 2 D Torgerson 2 R Lewis 1
A systematic review of atypical antipsychotic drugs in schizophrenia Atypical antipsychotic drugs in schizophrenia A-M Bagnall 1 * S Gilbody 3 L Jones 1 L Davies 4 L Ginnelly 2 D Torgerson 2 R Lewis 1
Management of Severe Agitation
 Management of Severe Agitation Key Points 1. The management of the severely agitated or violent patient embraces psychological, physical and pharmacological approaches. 2. Psychological methods focus on
Management of Severe Agitation Key Points 1. The management of the severely agitated or violent patient embraces psychological, physical and pharmacological approaches. 2. Psychological methods focus on
Guideline for use of Intramuscular Medication for Acutely Disturbed Behaviour in Mental Health and Associated Services
 NHS GGC Mental Health Service Guideline for use of Intramuscular Medication for Acutely Disturbed Behaviour in Mental Health and Associated Services Important Note: The Intranet version of this document
NHS GGC Mental Health Service Guideline for use of Intramuscular Medication for Acutely Disturbed Behaviour in Mental Health and Associated Services Important Note: The Intranet version of this document
Schizophrenia. Core interventions in the treatment and management of schizophrenia in adults in primary and secondary care
 Issue date: March 2009 Schizophrenia Core interventions in the treatment and management of schizophrenia in adults in primary and secondary care This is an update of NICE clinical guideline 1 NICE clinical
Issue date: March 2009 Schizophrenia Core interventions in the treatment and management of schizophrenia in adults in primary and secondary care This is an update of NICE clinical guideline 1 NICE clinical
The treatment of bipolar disorder in adults, children and adolescents
 DRAFT FOR CONSULTATION The treatment of bipolar disorder in adults, children and adolescents The paragraphs in the draft are numbered for the purposes of consultation. The final version will not contain
DRAFT FOR CONSULTATION The treatment of bipolar disorder in adults, children and adolescents The paragraphs in the draft are numbered for the purposes of consultation. The final version will not contain
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Psychosis and schizophrenia in children and young people: recognition and management 1.1 Short title Psychosis and schizophrenia
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Psychosis and schizophrenia in children and young people: recognition and management 1.1 Short title Psychosis and schizophrenia
NHS Grampian Guidance For Staff Working In The Mental Health Service For The Use Of High-Dose Antipsychotic Medication
 NHS Grampian Westholme Woodend Hospital Queens Road ABERDEEN AB15 6LS Date 20 th November 2014 Our Ref HDAT_MGPG/Nov14 Enquiries to Caroline Hind Extension 56088 Direct Line 01224 556088 Email caroline.hind2@nhs.net
NHS Grampian Westholme Woodend Hospital Queens Road ABERDEEN AB15 6LS Date 20 th November 2014 Our Ref HDAT_MGPG/Nov14 Enquiries to Caroline Hind Extension 56088 Direct Line 01224 556088 Email caroline.hind2@nhs.net
Psychopharmacological treatment of first episode psychosis
 Psychopharmacological treatment of first episode psychosis Matcheri S Keshavan MD First episode Psychosis Treatment Assistance Center (FEP-TAC), Harvard Medical School, Beth Israel Deaconess Medical Center
Psychopharmacological treatment of first episode psychosis Matcheri S Keshavan MD First episode Psychosis Treatment Assistance Center (FEP-TAC), Harvard Medical School, Beth Israel Deaconess Medical Center
ESSENTIAL SHARED CAR E AGREEMENT FOR
 E093 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, or Amisulpride for Behavioural indications in People with Learning Disability (LD) Referral Criteria In some
E093 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, or Amisulpride for Behavioural indications in People with Learning Disability (LD) Referral Criteria In some
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Step 3: GAD with marked functional impairment or that has not improved after step 2 interventionsentions bring together everything NICE says on a topic in an interactive flowchart. are interactive and
Step 3: GAD with marked functional impairment or that has not improved after step 2 interventionsentions bring together everything NICE says on a topic in an interactive flowchart. are interactive and
Measure #383 (NQF 1879): Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety
: Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety") Measure #383 (NQF 1879): Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety 2017 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Measure #383 (NQF 1879): Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety 2017 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
SHARED CARE GUIDELINE
 SHARED CARE GUIDELINE Title: Shared Care Guideline for the prescribing and monitoring of Antipsychotics for the treatment of Schizophrenia and psychotic symptoms in children and adolescents Scope: Pennine
SHARED CARE GUIDELINE Title: Shared Care Guideline for the prescribing and monitoring of Antipsychotics for the treatment of Schizophrenia and psychotic symptoms in children and adolescents Scope: Pennine
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
Managing Behavioural Problems in Patients with Learning Disabilities
 Managing Behavioural Problems in Patients with Learning Disabilities Some people with a learning disability display behaviour that challenges. Although such behaviour is a challenge to services, family
Managing Behavioural Problems in Patients with Learning Disabilities Some people with a learning disability display behaviour that challenges. Although such behaviour is a challenge to services, family
Appendix C - Summary form
 National Institute for Health and Clinical Excellence Appendix C - Summary form Single Techn Appraisal (STA) Agomelatine for the treatment of major depressive episodes Response to consultee and commentator
National Institute for Health and Clinical Excellence Appendix C - Summary form Single Techn Appraisal (STA) Agomelatine for the treatment of major depressive episodes Response to consultee and commentator
Formulary Item Restrictions and/or Advice Site availability
 Formulary Item Restrictions and/or Advice Site availability C&W CNWL Typical Antipsychotic drugs Chlorpromazine 25mg Chlorpromazine 50mg Chlorpromazine 100mg Chlorpromazine 25mg/5ml syrup Chlorpromazine
Formulary Item Restrictions and/or Advice Site availability C&W CNWL Typical Antipsychotic drugs Chlorpromazine 25mg Chlorpromazine 50mg Chlorpromazine 100mg Chlorpromazine 25mg/5ml syrup Chlorpromazine
Measure #383 (NQF 1879): Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety
: Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety") Measure #383 (NQF 1879): Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
Measure #383 (NQF 1879): Adherence to Antipsychotic Medications For Individuals with Schizophrenia National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
Schizophrenia in Greater Manchester: Audit
 S i G M A Schizophrenia in Greater Manchester: Audit SiGMA Schizophrenia in Greater Manchester: Audit Report 2011-2012 Audit Co-ordinator/ Author of Report: Project Lead Applicants: Darragh Downey, Karen
S i G M A Schizophrenia in Greater Manchester: Audit SiGMA Schizophrenia in Greater Manchester: Audit Report 2011-2012 Audit Co-ordinator/ Author of Report: Project Lead Applicants: Darragh Downey, Karen
Benzodiazepines and Hypnotics
 Benzodiazepines and Hypnotics Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date (when this version goes out of date):
Benzodiazepines and Hypnotics Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date (when this version goes out of date):
MENTAL HEALTH SERVICES 2010 MEDICATION
 MENTAL HEALTH SERVICES 2010 INTRODUCTION MEDICATION Under the Mental Health Act 2001 the Inspectorate carries out a review of mental health services in the state and furnishes a report on the quality of
MENTAL HEALTH SERVICES 2010 INTRODUCTION MEDICATION Under the Mental Health Act 2001 the Inspectorate carries out a review of mental health services in the state and furnishes a report on the quality of
Handout for the Neuroscience Education Institute (NEI) online activity: First-Episode Schizophrenia: Setting the Stage for Successful Outcomes
 online activity: First-Episode Schizophrenia: Setting the Stage for Successful Outcomes") Handout for the Neuroscience Education Institute (NEI) online activity: First-Episode Schizophrenia: Setting the Stage for Successful Outcomes Learning Objectives Initiate low-dose antipsychotic medication
Handout for the Neuroscience Education Institute (NEI) online activity: First-Episode Schizophrenia: Setting the Stage for Successful Outcomes Learning Objectives Initiate low-dose antipsychotic medication
Treatment of Schizophrenia
 Treatment of Schizophrenia Conduct comprehensive assessment and use measurement-based care as found in the Principles of Practice (review pages 4-7). Most importantly assess social support system (housing,
Treatment of Schizophrenia Conduct comprehensive assessment and use measurement-based care as found in the Principles of Practice (review pages 4-7). Most importantly assess social support system (housing,
Effects of Home Antipsychotic Reinitiation in ICU Patients with a History of Mental Illness
 Effects of Home Antipsychotic Reinitiation in ICU Patients with a History of Mental Illness Gary Sweet, PharmD PGY-1 Pharmacy Practice Resident St. John Medical Center, Tulsa, OK Conflict of Interest Nothing
Effects of Home Antipsychotic Reinitiation in ICU Patients with a History of Mental Illness Gary Sweet, PharmD PGY-1 Pharmacy Practice Resident St. John Medical Center, Tulsa, OK Conflict of Interest Nothing
Pregnancy. General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition)
") Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
This factsheet covers:
 Antipsychotics If you experience psychosis as part of your illness, you may be offered antipsychotic medication. Antipsychotics are generally used to treat psychosis, but are also used to treat bipolar
Antipsychotics If you experience psychosis as part of your illness, you may be offered antipsychotic medication. Antipsychotics are generally used to treat psychosis, but are also used to treat bipolar
Professor Tony Holland, Department of Psychiatry, University of Cambridge
 INFORMATION SHEET The Use of Medication for Challenging Behaviour Professor Tony Holland, Department of Psychiatry, University of Cambridge Introduction Challenging behaviours displayed by people with
INFORMATION SHEET The Use of Medication for Challenging Behaviour Professor Tony Holland, Department of Psychiatry, University of Cambridge Introduction Challenging behaviours displayed by people with
ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, or Amisulpride for Behavioural indications in DNLD
 Ref No: E050 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, or Amisulpride for Behavioural indications in DNLD Please complete the following details: Patient s name,
Ref No: E050 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, or Amisulpride for Behavioural indications in DNLD Please complete the following details: Patient s name,
Medication Audit Checklist- Antipsychotics - Atypical
 Medication Audit checklist Page 1 of 7 10-2018 Audit number: Client number: Ordering Provider: INDICATIONS 1) Disorders with psychotic symptoms (schizophrenia, schizoaffective disorder, manic disorders,
Medication Audit checklist Page 1 of 7 10-2018 Audit number: Client number: Ordering Provider: INDICATIONS 1) Disorders with psychotic symptoms (schizophrenia, schizoaffective disorder, manic disorders,
Schizophrenia: core interventions in the treatment and management of schizophrenia in adults in primary and secondary care (update)
") Schizophrenia: core interventions in the treatment and management of schizophrenia in adults in primary and secondary care (update) NICE guideline Draft for consultation, September 2008 If you wish to
Schizophrenia: core interventions in the treatment and management of schizophrenia in adults in primary and secondary care (update) NICE guideline Draft for consultation, September 2008 If you wish to
Assessment of physical monitoring following rapid tranquillisation. Stephen Dye
 Assessment of physical monitoring following rapid tranquillisation Stephen Dye Aims X Lecture on developments in RT Review of recent studies Discussion of specific medications Containment measures Definition
Assessment of physical monitoring following rapid tranquillisation Stephen Dye Aims X Lecture on developments in RT Review of recent studies Discussion of specific medications Containment measures Definition
Prescription of High Dose Antipsychotic Medication
 Subject (M1) Title Medicine Prescription of High Dose Antipsychotic Medication Manual Mental Health Procedure No M1-P-2-MH Department Pharmacy Distribution All Author Rae McKnight Review 4 Reviewer Jonathan
Subject (M1) Title Medicine Prescription of High Dose Antipsychotic Medication Manual Mental Health Procedure No M1-P-2-MH Department Pharmacy Distribution All Author Rae McKnight Review 4 Reviewer Jonathan
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
High Dose Antipsychotic Therapy (HDAT) guideline
 guideline") Document level: Trustwide (TW) Code: MP18 Issue number: 4 High Dose Antipsychotic Therapy (HDAT) guideline Lead executive Medical Director Authors details Michael Slater (Clinical Pharmacist, tel. 01625
Document level: Trustwide (TW) Code: MP18 Issue number: 4 High Dose Antipsychotic Therapy (HDAT) guideline Lead executive Medical Director Authors details Michael Slater (Clinical Pharmacist, tel. 01625
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Prescribing antipsychotics for children and adolescents
 POMH-UK Topic 10a baseline report Prescribing antipsychotics for children and adolescents September 2010 Prepared by the Prescribing Observatory for Mental Health-UK for Coventry and Warwickshire Partnership
POMH-UK Topic 10a baseline report Prescribing antipsychotics for children and adolescents September 2010 Prepared by the Prescribing Observatory for Mental Health-UK for Coventry and Warwickshire Partnership
Benzodiazepines: risks, benefits or dependence
 Benzodiazepines: risks, benefits or dependence A re-evaluation Council Report CR 59 January 1997 Royal College of Psychiatrists, London Due for review: January 2002 1 Contents A College Statement 3 Benefits
Benzodiazepines: risks, benefits or dependence A re-evaluation Council Report CR 59 January 1997 Royal College of Psychiatrists, London Due for review: January 2002 1 Contents A College Statement 3 Benefits
Technology appraisal guidance Published: 26 January 2011 nice.org.uk/guidance/ta213
 Aripiprazole for the treatment of schizophrenia in people aged 15 to 17 years Technology appraisal guidance Published: 26 January 2011 nice.org.uk/guidance/ta213 NICE 2018. All rights reserved. Subject
Aripiprazole for the treatment of schizophrenia in people aged 15 to 17 years Technology appraisal guidance Published: 26 January 2011 nice.org.uk/guidance/ta213 NICE 2018. All rights reserved. Subject
Guidance on the Use of Antipsychotic Long-acting Injections in North of England
 Guidance on the Use of Antipsychotic Long-acting Injections in North of England This guidance aims to inform and support prescribers within the three mental health service providers in the north of England
Guidance on the Use of Antipsychotic Long-acting Injections in North of England This guidance aims to inform and support prescribers within the three mental health service providers in the north of England
Dosing and Switching Strategies for Long-Acting Risperidone
 Clinical Guidelines: Dosing Long-Acting Risperidone Clinical Guidelines Dosing and Switching Strategies for Long-Acting Risperidone Stephen R. Marder, M.D.; Robert Conley, M.D.; Larry Ereshefsky, Pharm.D.,
Clinical Guidelines: Dosing Long-Acting Risperidone Clinical Guidelines Dosing and Switching Strategies for Long-Acting Risperidone Stephen R. Marder, M.D.; Robert Conley, M.D.; Larry Ereshefsky, Pharm.D.,
Guidelines for the use of Zuclopenthixol Acetate (Clopixol Acuphase ) injection. Version 1
 injection. Version 1") Guidelines for the use of Zuclopenthixol Acetate (Clopixol Acuphase ) injection Version 1 SUMMARY Guidelines for the use of Zuclopenthixol Acetate (Clopixol Acuphase ) injection POLICY CODE REPLACES POLICY
Guidelines for the use of Zuclopenthixol Acetate (Clopixol Acuphase ) injection Version 1 SUMMARY Guidelines for the use of Zuclopenthixol Acetate (Clopixol Acuphase ) injection POLICY CODE REPLACES POLICY
Mental Health Clinical Pathways Group. The Case for Change
 Mental Health Clinical Pathways Group The Case for Change Contents 1. Executive summary 2. Introduction 2.1. What is severe mental illness? 2.2. Findings of the Disability Rights Commission 3. Physical
Mental Health Clinical Pathways Group The Case for Change Contents 1. Executive summary 2. Introduction 2.1. What is severe mental illness? 2.2. Findings of the Disability Rights Commission 3. Physical
Antipsychotics. This factsheet covers -
 Antipsychotics If you experience psychosis as part of an illness, you may be offered antipsychotic medication. Antipsychotics are generally used to treat psychosis, but are also used to treat bipolar disorder
Antipsychotics If you experience psychosis as part of an illness, you may be offered antipsychotic medication. Antipsychotics are generally used to treat psychosis, but are also used to treat bipolar disorder
Psychotropic Strategies Handout Package
 Psychotropic Strategies Handout Package Psychotropic Strategies Learning Objectives Utilize all clinical information available Assess the patient s overall condition this is essential Basic Principles
Psychotropic Strategies Handout Package Psychotropic Strategies Learning Objectives Utilize all clinical information available Assess the patient s overall condition this is essential Basic Principles
THIOTHIXENE. THERAPEUTICS Brands Navane see index for additional brand names. Generic? Yes
 THIOTHIXENE THERAPEUTICS Brands Navane see index for additional brand names Generic? Yes Class Conventional antipsychotic (neuroleptic, thioxanthene, dopamine 2 antagonist) Commonly Prescribed for (bold
THIOTHIXENE THERAPEUTICS Brands Navane see index for additional brand names Generic? Yes Class Conventional antipsychotic (neuroleptic, thioxanthene, dopamine 2 antagonist) Commonly Prescribed for (bold
Method. NeuRA First versus second generation antipsychotics August 2016
 Introduction First generation typical are an older class of antipsychotic than second generation atypical. First generation are used primarily to treat positive symptoms including the experiences of perceptual
Introduction First generation typical are an older class of antipsychotic than second generation atypical. First generation are used primarily to treat positive symptoms including the experiences of perceptual
Psychopharmacology. Psychopharmacology. Hamish McAllister-Williams Reader in Clinical. Department of Psychiatry, RVI
 Regional Affective Disorders Service Psychopharmacology Northumberland, Tyne and Wear NHS Trust Hamish McAllister-Williams Reader in Clinical Psychopharmacology Department of Psychiatry, RVI Intro NOT
Regional Affective Disorders Service Psychopharmacology Northumberland, Tyne and Wear NHS Trust Hamish McAllister-Williams Reader in Clinical Psychopharmacology Department of Psychiatry, RVI Intro NOT
Clinical Guidelines for the Pharmacologic Treatment of Schizophrenia
 Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
DEMENTIA AND MEDICATION
 DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
Method. NeuRA Paliperidone August 2016
 Introduction Second generation antipsychotics (sometimes referred to as atypical antipsychotics) are a newer class of antipsychotic medication than first generation typical antipsychotics. Second generation
Introduction Second generation antipsychotics (sometimes referred to as atypical antipsychotics) are a newer class of antipsychotic medication than first generation typical antipsychotics. Second generation
Depression in adults: treatment and management
 1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
PROCEDURE REF NO SABP/EXECUTIVE BOARD/0017
 PROCEDURE REF NO SABP/EXECUTIVE BOARD/0017 NAME OF GUIDELINE REASON FOR GUIDELINE WHAT THE GUIDELINE WILL ACHIEVE? WHO NEEDS TO KNOW ABOUT IT? Medicines Guideline: Hypnotic Medication Compliance with NICE
PROCEDURE REF NO SABP/EXECUTIVE BOARD/0017 NAME OF GUIDELINE REASON FOR GUIDELINE WHAT THE GUIDELINE WILL ACHIEVE? WHO NEEDS TO KNOW ABOUT IT? Medicines Guideline: Hypnotic Medication Compliance with NICE
Minimising the Impact of Medication on Physical Health in Schizophrenia
 Minimising the Impact of Medication on Physical Health in Schizophrenia John Donoghue Liverpool Imagination is more important than knowledge Albert Einstein LIFESTYLE Making choices TREATMENT Worse Psychopathology,
Minimising the Impact of Medication on Physical Health in Schizophrenia John Donoghue Liverpool Imagination is more important than knowledge Albert Einstein LIFESTYLE Making choices TREATMENT Worse Psychopathology,
Document Title Pharmacological Management of Generalised Anxiety Disorder
 Document Title Pharmacological Management of Generalised Anxiety Disorder Document Description Document Type Policy Service Application Trust Wide Version 1.1 Policy Reference no. POL 201 Lead Author(s)
Document Title Pharmacological Management of Generalised Anxiety Disorder Document Description Document Type Policy Service Application Trust Wide Version 1.1 Policy Reference no. POL 201 Lead Author(s)
Hearts and Minds An ECG Update. Tuesday 18 th November The Met Hotel, Leeds
 Hearts and Minds An ECG Update Tuesday 18 th November The Met Hotel, Leeds Ashleigh Bradley Specialist Clinical Pharmacist for Mental Health and Lithium Clinic Airedale NHS Foundation Trust Introduction
Hearts and Minds An ECG Update Tuesday 18 th November The Met Hotel, Leeds Ashleigh Bradley Specialist Clinical Pharmacist for Mental Health and Lithium Clinic Airedale NHS Foundation Trust Introduction
First Steps: Considering Clozapine for your Patients
 First Steps: Considering Clozapine for your Patients The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental Health
First Steps: Considering Clozapine for your Patients The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental Health
Increasing post-operative delirium in cardiac surgery patients. Karen Kindness Hussein El-Shafei Lisa Lawman
 Increasing post-operative delirium in cardiac surgery patients. Karen Kindness Hussein El-Shafei Lisa Lawman Introduction why is it a problem? CTUs can expect to encounter pts with postoperative delirium/psychosis
Increasing post-operative delirium in cardiac surgery patients. Karen Kindness Hussein El-Shafei Lisa Lawman Introduction why is it a problem? CTUs can expect to encounter pts with postoperative delirium/psychosis
CHAPTER 3. Schizophrenia and Antipsychotic Treatment
 CHAPTER 3 Schizophrenia and Antipsychotic Treatment What is it? It is a severe, chronic, disabling brain disease Considered to have biological origins but exact unknown 1% of population affected Schizophrenia
CHAPTER 3 Schizophrenia and Antipsychotic Treatment What is it? It is a severe, chronic, disabling brain disease Considered to have biological origins but exact unknown 1% of population affected Schizophrenia