Childhood Rage: Diagnosis and Treatment Strategies for Severe Mood Dysregulation - Part 2: Diagnosis and Treatment
|
|
|
- Buck Heath
- 5 years ago
- Views:
Transcription

1 Liberty University University Faculty Publications and Presentations Department for Counselor Education and Family Studies 2013 Childhood Rage: Diagnosis and Treatment Strategies for Severe Mood Dysregulation - Part 2: Diagnosis and Treatment Gary A. Sibcy Liberty University, gsibcy@liberty.edu John Kuhnley Liberty University, jkuhnley@liberty.edu Follow this and additional works at: Part of the Biological Psychology Commons, Child Psychology Commons, Counseling Psychology Commons, Developmental Psychology Commons, and the Mental and Social Health Commons Recommended Citation Sibcy, Gary A. and Kuhnley, John, "Childhood Rage: Diagnosis and Treatment Strategies for Severe Mood Dysregulation - Part 2: Diagnosis and Treatment" (2013). Faculty Publications and Presentations This Presentation is brought to you for free and open access by the Department for Counselor Education and Family Studies at DigitalCommons@Liberty University. It has been accepted for inclusion in Faculty Publications and Presentations by an authorized administrator of DigitalCommons@Liberty University. For more information, please contact scholarlycommunication@liberty.edu.
2 AACC 2013 Our Time is Now World Conference Pre Conference Workshop 043: Attachments and Neurobiology: Helping Children with Anxiety Disorders and Severe Mood Dysregulation* * DSM-5: Developmental Mood Dysregulation Disorder Gary Sibcy, Ph.D. and E. John Kuhnley, M.D.
3 Childhood Rage: Diagnosis and Treatment Strategies for Severe Mood Dysregulation Part 2: Diagnosis and Treatment E. John Kuhnley, MD Child & Adolescent Psychiatrist Lynchburg, Virginia
4 ODD ANX MDD Differential Diagnosis and Comorbidity ADHD BD DMDD * (SMD)
5 The most common diagnoses among patients with mood swings FREQUENCY DIAGNOSIS 39% ADHD 15% ODD with ADHD 15% ANXIETY D/O (GAD) 12% BIPOLAR DISORDER 10% SECONDARY MOOD DISORDER (eg. Fetal Alcohol Spectrum Disorder) 3% PDD, ASPERGER S Kowatch, et al, Current Psychiatry Vol. 10, No. 02 / February 2011

6 Rages--what are they and who has them? Conclusions: Psychiatrically hospitalized children with multiple rages have complex, chronic neuropsychiatric disorders and have failed prior conventional treatment. One third of children with rages had been given a bipolar diagnosis prior to admission. However, only 9% of children with rages were given that diagnosis after careful observation. Gabrielle A. Carlson, MD

7 Bipolar Disorder Not a 'Quick and Dirty' Diagnosis Although some children are being misdiagnosed as having BD, the opposite is also true. There are many children, he said, who have BD but whose conditions are misdiagnosed and treated inappropriately. "This is something we need to be aware of because bipolar seriously affects the normal development of a child and increases their risk of suicide, substance abuse, and psychosocial problems. Early recognition and appropriate treatment are most important. Boris Birmaher, MD
8 Disruptive Mood Dysregulation Disorder DSM-5 TM Diagnostic Criteria (F34.8) A. Severe recurrent temper outbursts manifested verbally (e.q., verbal rages) and/or behaviorally (e.q., physical aggression toward people or property) that are grossly out of proportion in intensity or duration to the situation or provocation. B. The temper outbursts are inconsistent with developmental level. C. The temper outbursts occur, on average, three or more times per week. D. The mood between temper outbursts is persistently irritable or angry most of the day, nearly every day, and is observable by others (e.q., parents, teachers, peers) APA
9 Disruptive Mood Dysregulation Disorder DSM-5 TM Diagnostic Criteria (F34.8) E. Criteria A-D have been present for 12 or more months. Throughout that time, the individual has not had a period lasting 3 or more consecutive months without all of the symptoms in Criteria A-D. F. Criteria A and D are present in at least two of three settings (i.e., at home, at school, with peers) and are severe in at least one of these. G. The diagnosis should not be made for the first time before age 6 years or after age 18 years. H. By history or observation, the age at onset of Criteria A-E is before 10 years. I. There has never been a distinct period lasting more than 1 day during which the full symptom criteria, except duration, for a manic or hypomanic episode have been met. Note: Developmentally appropriate mood elevation, such as occurs in the context of a highly positive event or its anticipation, should not be considered as a symptom of mania or hypomania APA
10 Disruptive Mood Dysregulation Disorder DSM-5 TM Diagnostic Criteria (F34.8) J. The behaviors do not occur exclusively during an episode of major depressive disorder and are not better explained by another mental disorder (e.g., autism spectrum disorder, posttraumatic stress disorder, separation anxiety disorder, persistent depressive disorder [dysthymia]). Note: This diagnosis cannot coexist with oppositional defiant disorder, intermittent explosive disorder, or bipolar disorder, though it can coexist with others, including major depressive disorder, attentiondeficit/hyperactivity disorder, conduct disorder, and substance use disorders. Individuals whose symptoms meet criteria for both disruptive mood dysregulation disorder and oppositional defiant disorder should only be given the diagnosis of disruptive mood dysregulation disorder. If an individual has ever experienced a manic or hypomanic episode, the diagnosis of disruptive mood dysregulation disorder should not be assigned. K. The symptoms are not attributable to the physiological effects of a substance or to another medical or neurological condition APA
11 Anxiety Disorders Excessive fear, worry, avoidance behavior Difficulty with transitions, unfamiliar circumstances Mood swings/outbursts during stressful periods when things don t proceed as they expect, tend to be short (5-10 minutes) Psychosomatic symptoms Restlessness is more likely practical, worrisome behavior, not the "driven," inquisitive, or overstimulated type Socially reticent, not disruptive, generally not impulsive or aggressive, often over inhibited ADHD-like Symptoms only during high anxiety state Difficulty sleeping common d/t excessive fear, worry, and psychosomatic symptoms Strong family history of anxiety disorders
12 Attention-Deficit/Hyperactivity Disorder Chronic symptoms of hyperactivity, distractibility, impulsivity, poor attentional skills, disorganization unrelated to mood; low frustration tolerance; present in 2 or more environments w/ onset before age 12 and strong family h/o ADHD Mood swings/outbursts are impulsive, reactive to frustration, brief, like hand-grenades Often difficulty falling asleep but then sleep well or sleepy/tired the next day; sometimes medication effect Busy minds, hyperactivity of thought Generally remorseful for negative behavior, including rage In ADHD, the aggression stems from an impulsive burst of anger when a goal is not achieved. Constant irritability is not a characteristic of ADHD.
13 Oppositional Defiant Disorder Daily (chronic) oppositionality, negativity, irritability & short (5-10 min.) mood swings or outbursts of anger (sometimes aggression) precipitated by not getting their way or being asked to do something they do not want to do Resists initiating demands, whereas ADHD children may initiate but cannot stay on task Lacks impulsive, disinhibited behavior Defiance primarily directed towards mother initially; able to cooperate & complete tasks requested by others Often associated with parental child management deficits or family dysfunction
14 Bipolar Disorder Episodic mood shifts, alternating between manic (Euphoric/ elated/ expansive/ high energy)(unrelated to substance use), depressive, and normal; You often may feel the energy output of a manic individual Sudden catastrophic meltdowns or affective storms, like a hurricane, not a hand grenade; may go on for hours, and even days, Rages may involve destruction of property or aggression toward a sibling, parent, or pet. Grandiose, boastful, belligerent, and delinquent youngster is suspect for BD Family history take carefully
15 Major Depression Depressed moods most days. Mad/cranky irritability found in depressive disorders; Depressed children had more severe irritability than depressed adolescents Impaired or excessive sleep Low energy and motivation Depression was the most common initial and most frequent episode for adolescents
16 Bipolar Disorder vs. ADHD Sleep (Decreased need vs. DFA then crash) Outbursts (hurricane vs. hand grenade) Elated or expansive mood in BD, not ADHD Mood energy vs. Motor activity Hypersexuality (BD>>ADHD) Racing vs. busy thoughts (BD>>ADHD) Episodic vs. Chronic/persistent
17 Individual Therapy (CBT, Mindfulness) Group Therapy Skill Development Attachment Parenting Behavioral Modification Medication Multimodal (Integrative) Treatment Family Therapy Psychosocial Psychoeducational Spiritual Counseling Environmental Accommodations Life style interventions (nutrition, exercise, sleep, etc.)
18 The treatment of a child with impulsive or affective aggression The treatment of a child with impulsive or affective aggression may be successful in one-onone sessions or in group therapy. Principles include: anxiety management correction of cognitive distortions assertiveness training impulse control strategies stress reduction if applicable, therapy to address trauma. Bates 2006
19 Being Spiritual Protects People from Depression Those who rated their religious or spiritual beliefs as having high personal importance had one tenth of the risk of other participants for recurrence or new incidence of major depression over 10 years. Supporting religious or spiritual engagement by individuals with such inclinations may offer some protective value. Miller L et al. Religiosity and major depression in adults at high risk: A ten-year prospective study. Am J Psychiatry 2011 Aug 24
20 Stop the Pop: Soda Linked to Aggression, Inattention in Kids Deborah Brauser - Aug 22, Consumption of even 1 soft drink per day may be associated with increased negative behavior in young children, new research suggests. A cohort study of almost year-olds showed that those who drank 1 to 4 servings of soda per day had significantly higher aggressive measurement scores than their peers who drank no soda. In addition, those who consumed 2 or more servings had higher withdrawn behavior scores, and those who consumed 4 or more servings had higher attention problem scores.
21 TRAAY Recommendations Conduct a diagnostic interview. Assess current treatment effects. Begin with psychosocial and psychoeducational treatments. Treat the primary Axis I disorder with its first-line treatment. Use an atypical antipsychotic (not a typical antipsychotic) for the aggression. Use a conservative dosing strategy. Use crisis management techniques before emergency treatment of aggression.
22 TRAAY Recommendations Avoid using PRN medications to control behavior. Assess adverse effects routinely. Ensure an adequate trial before switching medications. After a failed trial of one atypical antipsychotic, try a second one. For a partial response, consider adding a mood stabilizer to the atypical antipsychotic. If non-response to polypharmacy, consider tapering one medication. If remission of symptoms for > 6 months, consider tapering the antipsychotics.
23 CONDITIONS ODD ADHD Anxiety Disorder Depression Bipolar Disorder Disruptive Mood Dysregulation Disorder Psychosis MEDICATIONS None Stimulants Antianxiety agents Antidepressants Mood Stabilizers α-2a agonists Antipsychotics Any medication option, or combination of medications, may apply to many of the conditions, or combinations of conditions.
24
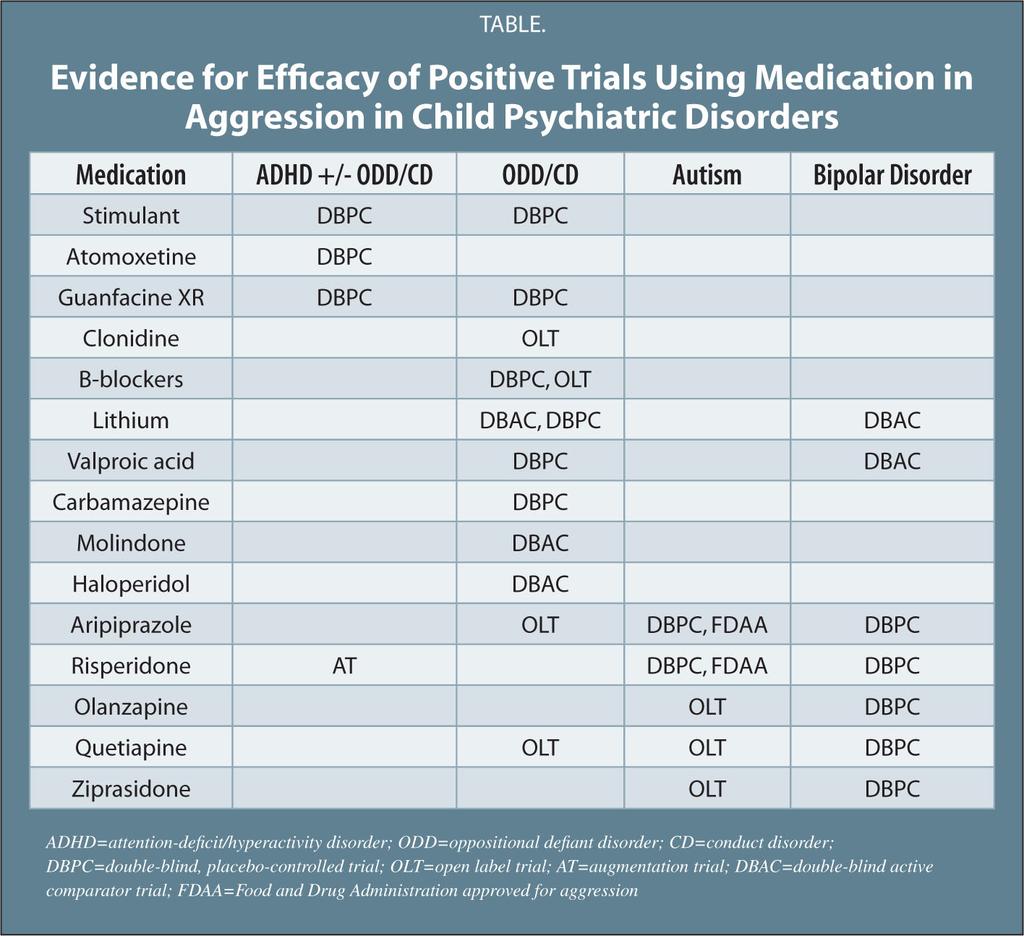
25 Evidence for Efficacy of Positive Trials Using Medications in Aggression in Child Psychiatric Disorders Medication ADHD +/- ODD/CD Stimulant (Ritalin, Concerta, Focalin, Metadate) (Adderall, Dexedrine, Vyvanse) Atomoxetine (Strattera) DBPC DBPC ODD/CD Autism Bipolar Disorder DBPC Guanfacine XR Intuniv) DBPC DBPC Clonidine (Kapvay) (DBPC) OLT B-Blockers (Inderal, Propranolol) DBPC,OLT Lithium DBAC,DBPC DBAC Valproic Acid (Depakote) DBPC DBAC Carbamazepine (Tegretol) DBPC ADHD = attention-deficit/hyperactivity disorder; ODD = oppositional defiant disorder; DBPC = double-blind, placebo-controlled trial; OLT = open label trial; AT = augmentation trial; DBAC = double-blind, active-comparator trial; FDAA = Food and Drug Administration approved for aggression Adelaide S. Robb, MD; Psychiatric Annals; April Volume 40 Issue 4:
26 Evidence for Efficacy of Positive Trials Using Medications in Aggression in Child Psychiatric Disorders Medication ADHD +/- ODD/CD Molindone (Moban) Haloperidol (Haldol) ODD/CD Autism Bipolar Disorder DBAC DBAC Aripiprazole (Abilify) OLT DBPC, FDAA DBPC Risperidone (Risperdal) AT DBPC, FDAA DBPC Olanzapine (Zyprexa) OLT DBPC Quetiapine (Seroquel) OLT OLT DBPC Ziprasidone (Geodon) OLT DBPC ADHD = attention-deficit/hyperactivity disorder; ODD = oppositional defiant disorder; DBPC = double-blind, placebo-controlled trial; OLT = open label trial; AT = augmentation trial; DBAC = double-blind, active-comparator trial; FDAA = Food and Drug Administration approved for aggression Adelaide S. Robb, MD; Psychiatric Annals; April Volume 40 Issue 4:
27 Child and Adolescent Bipolar Algorithm 2009
28 Diagnosis in Clinical Practice Start by allowing the patient to express concerns; ask questions to facilitate expression Obtain the patients (and collateral sources) accounts In Their Own Words rather than asking criteria they can endorse The clinical interview must elicit and elucidate the patient s experience and symptoms and thus lead us to diagnostic criteria; then the diagnostic criteria guide us to clarification/confirmation, rather than the diagnostic criteria guiding the interview
29 Severe Mood Dysregulation DSM-5: Disruptive Mood Dysregulation Disorder The distinction between severe mood dysregulation and bipolar disorder may have important treatment implications. If severe mood dysregulation is a pediatric bipolar disorder phenotype, then first-line treatment would include mood stabilizers and atypical antipsychotics, with stimulants and selective serotonin reuptake inhibitors (SSRIs) being relatively contraindicated. On the other hand, if severe mood dysregulation is more similar pathophysiologically to unipolar depressive and anxiety disorders, as well as to ADHD, then stimulants and SSRIs would be recommended. Given the relatively high side effect burden of atypical antipsychotics, coupled with the risks of using antidepressants or stimulants in bipolar disorder, this differentiation is important. Leibenluft, 2011
 following negative feedback were the same areas activated in healthy")
30 Ellen Leibenluft, M.D. The anterior cingulate cortex and medial frontal gyrus both hyperactivated in children with SMD (Severe Mood Dysregulation) following negative feedback were the same areas activated in healthy control children following positive feedback. It makes you think about cognitive training or therapies that could perhaps train children with SMD to pay greater attention to positive feedback and less attention to negative feedback, Liebenluft said.
31 Self-regulation refers to subject actions that indicate: Thinking: purposeful control of thoughts, Feeling: purposeful control of emotions, Doing: purposeful control of behaviors Actions related to the completion of tasks Academic Occupational Emotional self-regulation is normally implemented by a neural circuit comprising various prefrontal regions and subcortical limbic structures. Beauregard et al suggest that humans have the capacity to influence the electrochemical dynamics of their brains, by voluntarily changing the nature of the mind processes unfolding in the psychological space.
32 Summary Obtain careful clinical information in their own words from multiple sources Mood swings and rage do not equate to Bipolar Disorder (BD) and more likely stem from ADHD, ODD, Anxiety, and/or psychosocial circumstances in the world of the child, BUT must consider BD Treat the patient, not the Diagnosis, though diagnosis guides the treatment, and A multimodal integrative treatment approach must target the causes/impairments and adjust over time as the clinical picture develops
33 References Not all mood swings are bipolar disorder: How to evaluate children with mood lability; Robert A. Kowatch, MD, PhD ; Current Psychiatry Vol. 10, No. 02 / February 2011 Who Are the Children With Severe Mood Dysregulation, a.k.a. "Rages? Gabrielle A. Carlson, M.D., Journal of Child and Adolescent Psychopharmacology, 19.3 (July 2009): p281(8). Psychiatric Comorbidity, Family Dysfunction, and Social Impairment in Referred Youth With Oppositional Defiant Disorder, Ross W. Greene, Ph.D., Joseph Biederman, M.D., Stephanie Zerwas, B.A., Michael C. Monuteaux, B.A., Jennifer C. Goring, B.A., and Stephen V. Faraone, Ph.D., Am J Psychiatry 159: , July 2002 Severe Mood Dysregulation, Irritability, and the Diagnostic Boundaries of Bipolar Disorder in Youths, Ellen Leibenluft, M.D., Am J Psychiatry 2011; 168: Oppositional Defiant Disorder, W Douglas Tynan, PhD, emedicine.medscape.com,
RANZCP 2010 AUCKLAND, NEW ZEALAND
 RANZCP 2010 AUCKLAND, NEW ZEALAND Dr Veronica Stanganelli et al. RANZCP 2010 1 INTRODUCTION Bipolar disorder within young people has been debated for years. It is still controversial in DSM V (1), whether
RANZCP 2010 AUCKLAND, NEW ZEALAND Dr Veronica Stanganelli et al. RANZCP 2010 1 INTRODUCTION Bipolar disorder within young people has been debated for years. It is still controversial in DSM V (1), whether
Post Traumatic Stress Disorder (PTSD) versus Bipolar Disorder: Confusion in the face of chaos.
 versus Bipolar Disorder: Confusion in the face of chaos.") Post Traumatic Stress Disorder (PTSD) versus Bipolar Disorder: Confusion in the face of chaos. Randall Ricardi D.O. Child and Adolescent Psychiatry Phoenix Children s Hospital 6-24-17 10:50am Disclosures
Post Traumatic Stress Disorder (PTSD) versus Bipolar Disorder: Confusion in the face of chaos. Randall Ricardi D.O. Child and Adolescent Psychiatry Phoenix Children s Hospital 6-24-17 10:50am Disclosures
5/2/2017. By Pamela Pepper PMH, CNS, BC. DSM-5 Growth and Development
 By Pamela Pepper PMH, CNS, BC DSM-5 Growth and Development The idea that diagnosis is based on subjective criteria and that those criteria should fall neatly into a set of categories is not sustainable,
By Pamela Pepper PMH, CNS, BC DSM-5 Growth and Development The idea that diagnosis is based on subjective criteria and that those criteria should fall neatly into a set of categories is not sustainable,
Disruptive Mood Dysregulation Disorder
 Walden University ScholarWorks School of Counseling Publications College of Social and Behavioral Sciences 2015 Disruptive Mood Dysregulation Disorder Brandy L. Gilea Walden University Rachel M. O Neill
Walden University ScholarWorks School of Counseling Publications College of Social and Behavioral Sciences 2015 Disruptive Mood Dysregulation Disorder Brandy L. Gilea Walden University Rachel M. O Neill
Mood swings in young people
 Mood swings in young people Bipolar I & II Disorders are uncommon before puberty; Mood Dysregulation (MD) is very common before puberty Are they the same problem? What are the beginnings of bipolar? What
Mood swings in young people Bipolar I & II Disorders are uncommon before puberty; Mood Dysregulation (MD) is very common before puberty Are they the same problem? What are the beginnings of bipolar? What
Psychiatric Medications. Positive and negative effects in the classroom
 Psychiatric Medications Positive and negative effects in the classroom Teaching the Medicated Child Beverly Bryant, M.D. Hattiesburg Clinic 9/17/14 Introduction According to the National Survey of Children
Psychiatric Medications Positive and negative effects in the classroom Teaching the Medicated Child Beverly Bryant, M.D. Hattiesburg Clinic 9/17/14 Introduction According to the National Survey of Children
Explosive Youth: Common Brain Disorders. Juvenile Law Conference 2005 Larry Fisher, Ph.D. UHS Neurobehavioral Systems
 Explosive Youth: Common Brain Disorders Juvenile Law Conference 2005 Larry Fisher, Ph.D. UHS Neurobehavioral Systems For More Information Larry Fisher, Ph.D. Director of Neuropsychological Services UHS
Explosive Youth: Common Brain Disorders Juvenile Law Conference 2005 Larry Fisher, Ph.D. UHS Neurobehavioral Systems For More Information Larry Fisher, Ph.D. Director of Neuropsychological Services UHS
CHILD & ADOLESCENT PSYCHIATRY ALERTS, VOLUME XV, 2013 INDEX
 A acceptance and commitment therapy Posttraumatic Stress, 69 ADHD Adjunctive Fatty Acids, 5 Adjunctive Guanfacine Pharmacokinetics, 27 Amantadine, 21 Atomoxetine, 23 Cancer Risk, 31 CBT for Comorbid Anxiety,
A acceptance and commitment therapy Posttraumatic Stress, 69 ADHD Adjunctive Fatty Acids, 5 Adjunctive Guanfacine Pharmacokinetics, 27 Amantadine, 21 Atomoxetine, 23 Cancer Risk, 31 CBT for Comorbid Anxiety,
Chronic irritability in youth that may be misdiagnosed as bipolar disorder. Ellen Leibenluft, M.D.
 Chronic irritability in youth that may be misdiagnosed as bipolar disorder Ellen Leibenluft, M.D. Chief, Section on Bipolar Spectrum Disorders Emotion and Development Branch National Institute of Mental
Chronic irritability in youth that may be misdiagnosed as bipolar disorder Ellen Leibenluft, M.D. Chief, Section on Bipolar Spectrum Disorders Emotion and Development Branch National Institute of Mental
CASE 5 - Toy & Klamen CASE FILES: Psychiatry
 CASE 5 - Toy & Klamen CASE FILES: Psychiatry A 14-year-old boy is brought to the emergency department after being found in the basement of his home by his parents during the middle of a school day. The
CASE 5 - Toy & Klamen CASE FILES: Psychiatry A 14-year-old boy is brought to the emergency department after being found in the basement of his home by his parents during the middle of a school day. The
BIPOLAR DISORDER AND ADHD IN CHILDREN
 BIPOLAR DISORDER AND ADHD IN CHILDREN BIPOLAR I DISORDER IS BEING DIAGNOSED WITH INCREASING FREQUENCY (INTENSITY) IN PRE-PUBERTAL CHIDREN WITH THE CAVEAT (WARNING / STIPULATION) THAT CLASSIC MANIC EPISODES
BIPOLAR DISORDER AND ADHD IN CHILDREN BIPOLAR I DISORDER IS BEING DIAGNOSED WITH INCREASING FREQUENCY (INTENSITY) IN PRE-PUBERTAL CHIDREN WITH THE CAVEAT (WARNING / STIPULATION) THAT CLASSIC MANIC EPISODES
Pediatric Bipolar Disorder and ADHD
 Pediatric Bipolar Disorder and ADHD Janet Wozniak, M.D. Director, Pediatric Bipolar Disorder Research Program Associate Professor Psychiatry Massachusetts General Hospital Harvard Medical School Disclosures
Pediatric Bipolar Disorder and ADHD Janet Wozniak, M.D. Director, Pediatric Bipolar Disorder Research Program Associate Professor Psychiatry Massachusetts General Hospital Harvard Medical School Disclosures
6/22/2012. Co-morbidity - when two or more conditions occur together. The two conditions may or may not be causally related.
 Autism Spectrum Disorders and Co-existing Mental Health Issues By Dr. Karen Berkman Objective To present an overview of common psychiatric conditions that occur in persons with autism spectrum disorders
Autism Spectrum Disorders and Co-existing Mental Health Issues By Dr. Karen Berkman Objective To present an overview of common psychiatric conditions that occur in persons with autism spectrum disorders
Perspective Truth on ADHD & Medications. Thomas L. Matthews, M.D. Associate Dean of Student Affairs Professor of Psychiatry
 Perspective Truth on ADHD & Medications Thomas L. Matthews, M.D. Associate Dean of Student Affairs Professor of Psychiatry Disclosures National Institute of Health ADHD and Aggression Study Co- Investigator
Perspective Truth on ADHD & Medications Thomas L. Matthews, M.D. Associate Dean of Student Affairs Professor of Psychiatry Disclosures National Institute of Health ADHD and Aggression Study Co- Investigator
Behavioral Health. Behavioral Health. Prescribing Guidelines
 Behavioral Health Behavioral Health Prescribing Guidelines Attention Deficit/Hyperactivity Disorder (ADHD) Start with a first line medication, either from the methylphenidate or dextroamphetamine-amphetamine
Behavioral Health Behavioral Health Prescribing Guidelines Attention Deficit/Hyperactivity Disorder (ADHD) Start with a first line medication, either from the methylphenidate or dextroamphetamine-amphetamine
Child & Adolescent Psychiatry (a brief overview)
") Child & Adolescent Psychiatry (a brief overview) Lance Feldman, MD, FAPA, MBA, BSN Vice Chair Clinical Affairs, Department of Psychiatry Affiliate Clinical Assistant Professor, University of South Carolina
Child & Adolescent Psychiatry (a brief overview) Lance Feldman, MD, FAPA, MBA, BSN Vice Chair Clinical Affairs, Department of Psychiatry Affiliate Clinical Assistant Professor, University of South Carolina
Pediatric Psychopharmacology
 Pediatric Psychopharmacology General issues to consider. Pharmacokinetic differences Availability of Clinical Data Psychiatric Disorders can be common in childhood. Early intervention may prevent disorders
Pediatric Psychopharmacology General issues to consider. Pharmacokinetic differences Availability of Clinical Data Psychiatric Disorders can be common in childhood. Early intervention may prevent disorders
Treating Disruptive Behavior Disorders in Children and Teens. A Review of the Research for Parents and Caregivers
 Treating Disruptive Behavior Disorders in Children and Teens A Review of the Research for Parents and Caregivers e Is This Information Right for Me? This information is for you if: A health care professional*
Treating Disruptive Behavior Disorders in Children and Teens A Review of the Research for Parents and Caregivers e Is This Information Right for Me? This information is for you if: A health care professional*
Disruptive mood dysregulation disorder (DMDD) a
 a") Disruptive mood dysregulation disorder: A better understanding Recognizing key differences in DMDD can help distinguish it from similar pediatric disorders Disruptive mood dysregulation disorder (DMDD)
Disruptive mood dysregulation disorder: A better understanding Recognizing key differences in DMDD can help distinguish it from similar pediatric disorders Disruptive mood dysregulation disorder (DMDD)
Pediatric Bipolar Disorder: Advances in Diagnosis and Research
 Pediatric Bipolar Disorder: Advances in Diagnosis and Research Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric Bipolar Disorder Research Program Harvard Medical School Massachusetts
Pediatric Bipolar Disorder: Advances in Diagnosis and Research Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric Bipolar Disorder Research Program Harvard Medical School Massachusetts
7/9/2013. Psychiatric medication treatment in children and adolescents: The good, the bad and the ugly. What ADHD is
 Psychiatric medication treatment in children and adolescents: The good, the bad and the ugly Gabrielle A. Carlson, MD Professor of Psychiatry and Pediatrics Director, Child and Adolescent Psychiatry Stony
Psychiatric medication treatment in children and adolescents: The good, the bad and the ugly Gabrielle A. Carlson, MD Professor of Psychiatry and Pediatrics Director, Child and Adolescent Psychiatry Stony
Psychopharmacology for Treatment of ADHD and ADHD with other co-existing psychiatric condition
 Psychopharmacology for Treatment of ADHD and ADHD with other co-existing psychiatric condition Presented by Cat Dang, D.O Medical Director - Insightful Minds, Inc. Objectives Evaluation process Pharmacology
Psychopharmacology for Treatment of ADHD and ADHD with other co-existing psychiatric condition Presented by Cat Dang, D.O Medical Director - Insightful Minds, Inc. Objectives Evaluation process Pharmacology
Comprehensive Quick Reference Handout on Pediatric Bipolar Disorder By Jessica Tomasula
 Comprehensive Quick Reference Handout on Pediatric Bipolar Disorder By Jessica Tomasula Official Name Bipolar Disorder; also referred to as Manic Depression Definitions (DSM-IV-TR, 2000) Bipolar I Disorder
Comprehensive Quick Reference Handout on Pediatric Bipolar Disorder By Jessica Tomasula Official Name Bipolar Disorder; also referred to as Manic Depression Definitions (DSM-IV-TR, 2000) Bipolar I Disorder
ADHD and. Shaw Wendi Fortuchang, M.D. Board certified in Child & Adolescent, Adult, and Forensic Psychiatry
 ADHD and Beyond Shaw Wendi Fortuchang, M.D. Board certified in Child & Adolescent, Adult, and Forensic Psychiatry Overview Use of medications in children How do medications work in the brain? Risperdal?
ADHD and Beyond Shaw Wendi Fortuchang, M.D. Board certified in Child & Adolescent, Adult, and Forensic Psychiatry Overview Use of medications in children How do medications work in the brain? Risperdal?
Treatment of Bipolar Disorder in Youth
 Treatment of Bipolar Disorder in Youth Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric Bipolar Disorder Research Program Harvard Medical School Massachusetts General Hospital
Treatment of Bipolar Disorder in Youth Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric Bipolar Disorder Research Program Harvard Medical School Massachusetts General Hospital
MOOD DISORDERS 101: A primer for recognizing and intervening with children with DMDD JULIE T. STECK, PH.D., HSPP CRG/CHILDREN S RESOURCE GROUP
 MOOD DISORDERS 101: A primer for recognizing and intervening with children with DMDD JULIE T. STECK, PH.D., HSPP CRG/CHILDREN S RESOURCE GROUP OBJECTIVES Participants will develop an understanding of Disruptive
MOOD DISORDERS 101: A primer for recognizing and intervening with children with DMDD JULIE T. STECK, PH.D., HSPP CRG/CHILDREN S RESOURCE GROUP OBJECTIVES Participants will develop an understanding of Disruptive
Ask The Shrink: ADHD
 Ask The Shrink: ADHD Theodore A. Petti, MD Professor of Psychiatry Division of Child and Adolescent Psychiatry Robert Wood Johnson Medical School PPC Hub Psychiatrist Hackensack Meridian Hubs @ Saint Peter'
Ask The Shrink: ADHD Theodore A. Petti, MD Professor of Psychiatry Division of Child and Adolescent Psychiatry Robert Wood Johnson Medical School PPC Hub Psychiatrist Hackensack Meridian Hubs @ Saint Peter'
Humberto Nagera M.D. Director, The Carter-Jenkins Center Psychoanalyst, Children, Adolescents and Adults Professor of Psychiatry at USF Professor
 The Carter Jenkins Center presents 1 Humberto Nagera M.D. Director, The Carter-Jenkins Center Psychoanalyst, Children, Adolescents and Adults Professor of Psychiatry at USF Professor Emeritus of Psychiatry
The Carter Jenkins Center presents 1 Humberto Nagera M.D. Director, The Carter-Jenkins Center Psychoanalyst, Children, Adolescents and Adults Professor of Psychiatry at USF Professor Emeritus of Psychiatry
4/2/13 COMMON CLASSES OF MEDICATIONS. Child & Adolescent Behavioral Medicine & Medication Therapies. Behavioral Medicine & Medication Therapies
 Child & Adolescent Behavioral Medicine & Medication Therapies Brian J Cowles, PharmD Associate Professor of Pharmacy Practice Albany College of Pharmacy & Health Sciences; Vermont Campus Behavioral Medicine
Child & Adolescent Behavioral Medicine & Medication Therapies Brian J Cowles, PharmD Associate Professor of Pharmacy Practice Albany College of Pharmacy & Health Sciences; Vermont Campus Behavioral Medicine
Psychiatric medication treatment in children and adolescents:
 Psychiatric medication treatment in children and adolescents: The good, the bad and the ugly Gabrielle A. Carlson, MD Professor of Psychiatry and Pediatrics Director, Child and Adolescent Psychiatry Stony
Psychiatric medication treatment in children and adolescents: The good, the bad and the ugly Gabrielle A. Carlson, MD Professor of Psychiatry and Pediatrics Director, Child and Adolescent Psychiatry Stony
4/29/2015. Dr. Carman Gill Wednesday, April 29th
 Dr. Carman Gill Wednesday, April 29th 1 Impacted diagnoses Major changes and rationale Special considerations Implications for counselors A sustained condition of prolonged emotional dejection, sadness,
Dr. Carman Gill Wednesday, April 29th 1 Impacted diagnoses Major changes and rationale Special considerations Implications for counselors A sustained condition of prolonged emotional dejection, sadness,
What are the most common signs of ADHD? And what are the most common medication interventions?
 What are the most common signs of ADHD? And what are the most common medication interventions? Bennett Gertz, MD, FAAP Developmental Behavioral Pediatrician Children s Developmental Health Services Albertina
What are the most common signs of ADHD? And what are the most common medication interventions? Bennett Gertz, MD, FAAP Developmental Behavioral Pediatrician Children s Developmental Health Services Albertina
Severe Mood Dysregulation in Children and Adolescents Research Findings Support Diagnostic Validity of Pediatric Bipolar Disorder
 Severe Mood Dysregulation in Children and Adolescents Research Findings Support Diagnostic Validity of Pediatric Bipolar Disorder Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric
Severe Mood Dysregulation in Children and Adolescents Research Findings Support Diagnostic Validity of Pediatric Bipolar Disorder Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric
2013 Virtual AD/HD Conference 1
 Medication for & Coexisting Conditions Part 2 Dr. Kenny Handelman Child, Adolescent & Adult Psychiatrist Halton Healthcare Adjunct Professor of Psychiatry, University of Western Ontario www.drkenny.com
Medication for & Coexisting Conditions Part 2 Dr. Kenny Handelman Child, Adolescent & Adult Psychiatrist Halton Healthcare Adjunct Professor of Psychiatry, University of Western Ontario www.drkenny.com
Current. A bad boy s behavior problems CASES THAT TEST YOUR SKILLS
 Two weeks after changing medications, a hyperactive 11-year-old becomes manic and attempts suicide. Is the new regimen or an undiagnosed mental disorder to blame? A. Kenneth Fuller, MD Chief of psychiatry
Two weeks after changing medications, a hyperactive 11-year-old becomes manic and attempts suicide. Is the new regimen or an undiagnosed mental disorder to blame? A. Kenneth Fuller, MD Chief of psychiatry
Brief Notes on the Mental Health of Children and Adolescents
 Brief Notes on the Mental Health of Children and Adolescents The future of our country depends on the mental health and strength of our young people. However, many children have mental health problems
Brief Notes on the Mental Health of Children and Adolescents The future of our country depends on the mental health and strength of our young people. However, many children have mental health problems
Ohio Psychotropic Medication Quality Improvement Collaborative. Minds Matter. Toolkit. for You and Your Family. This is the property of
 Minds Matter Ohio Psychotropic Medication Quality Improvement Collaborative Minds Matter Toolkit for You and Your Family This is the property of About Minds Matter Minds Matter is a project to help teens,
Minds Matter Ohio Psychotropic Medication Quality Improvement Collaborative Minds Matter Toolkit for You and Your Family This is the property of About Minds Matter Minds Matter is a project to help teens,
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine June 10-12, 2011
 Adelaide Robb, MD Associate Professor Psychiatry and Pediatrics Source Advisory Board Disclosure Speaker s Bureau Bristol Myers Squibb Yes Yes Yes Epocrates Research Contract Royalties Yes Stock Janssen
Adelaide Robb, MD Associate Professor Psychiatry and Pediatrics Source Advisory Board Disclosure Speaker s Bureau Bristol Myers Squibb Yes Yes Yes Epocrates Research Contract Royalties Yes Stock Janssen
RCHC Case Presentation
 Michael Kennedy, MFT Division Director RCHC Case Presentation Starring Melissa Ladrech as Susan and Michael Kozart as Dr. Keigh The following case is presented in three video installments. After each installment,
Michael Kennedy, MFT Division Director RCHC Case Presentation Starring Melissa Ladrech as Susan and Michael Kozart as Dr. Keigh The following case is presented in three video installments. After each installment,
Attention Deficit Hyperactivity Disorder State of the Art. Christopher Okiishi, MD
 Attention Deficit Hyperactivity Disorder State of the Art Christopher Okiishi, MD What is ADHD? Three subtypes: Inattentive (under diagnosed, esp. in girls) Hyperactive Impulsive Combined Impairments must
Attention Deficit Hyperactivity Disorder State of the Art Christopher Okiishi, MD What is ADHD? Three subtypes: Inattentive (under diagnosed, esp. in girls) Hyperactive Impulsive Combined Impairments must
Pediatric Behavior Problems: ODD and DMDD. Stanley Brewer, DO Pediatrics Assistant Professor (Clinical) Psychiatry Adjunct Instructor
 Psychiatry Adjunct Instructor") Pediatric Behavior Problems: ODD and DMDD Stanley Brewer, DO Pediatrics Assistant Professor (Clinical) Psychiatry Adjunct Instructor Acting out: What to call it Externalizing disorders Oppositional Defiant
Pediatric Behavior Problems: ODD and DMDD Stanley Brewer, DO Pediatrics Assistant Professor (Clinical) Psychiatry Adjunct Instructor Acting out: What to call it Externalizing disorders Oppositional Defiant
Aggression (Severe) in Children under Age 6
 in Children under Age 6") Aggression (Severe) in Children under Age 6 Level 0 Comprehensive diagnostic assessments. Refer to Principles of Practice on page 6. Evaluate and treat comorbid conditions (i.e. medical, other psychiatric
Aggression (Severe) in Children under Age 6 Level 0 Comprehensive diagnostic assessments. Refer to Principles of Practice on page 6. Evaluate and treat comorbid conditions (i.e. medical, other psychiatric
Big Lots Behavioral Health. Prescribing Guidelines for Behavioral Health
 Big Lots Behavioral Health Prescribing Guidelines for Behavioral Health Prescribing for Behavioral Health This document was developed by Nationwide Children s Hospital in conjunction with Partners For
Big Lots Behavioral Health Prescribing Guidelines for Behavioral Health Prescribing for Behavioral Health This document was developed by Nationwide Children s Hospital in conjunction with Partners For
Piecing the Puzzle Together: Pharmacologic Approaches to Behavioral Management in Autism Spectrum Disorder
 Piecing the Puzzle Together: Pharmacologic Approaches to Behavioral Management in Autism Spectrum Disorder Hannah Sauer, PharmD PGY1 Pediatric Pharmacy Resident Mayo Clinic 2015 MFMER slide-1 Objectives
Piecing the Puzzle Together: Pharmacologic Approaches to Behavioral Management in Autism Spectrum Disorder Hannah Sauer, PharmD PGY1 Pediatric Pharmacy Resident Mayo Clinic 2015 MFMER slide-1 Objectives
Presented by Bevan Gibson Southern IL Professional Development Center -Part of the Illinois Community College Board Service Center Network
 Bipolar Disorder: What It Means to You and Your Classroom Presented by Bevan Gibson Southern IL Professional Development Center -Part of the Illinois Community College Board Service Center Network Introduction
Bipolar Disorder: What It Means to You and Your Classroom Presented by Bevan Gibson Southern IL Professional Development Center -Part of the Illinois Community College Board Service Center Network Introduction
Medically Accepted Indications for Pediatric Use of Psychotropic Medications by
 Key: White Background: Medically Accepted Indication Yellow Backgroun: Medically Accepted Indication Status Not Ascertained Orange Background: Pediatric Indication cited, but not supported Red Background:
Key: White Background: Medically Accepted Indication Yellow Backgroun: Medically Accepted Indication Status Not Ascertained Orange Background: Pediatric Indication cited, but not supported Red Background:
Medications for Anxiety & Behavior in Williams Syndrome. Disclosure of Potential Conflicts. None 9/22/2016. Evaluation
 Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
CHILD & ADOLESCENT PSYCHIATRY ALERTS, VOLUME XIV, 2012 INDEX
 A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder,
 Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder, Journal of the Academy of Child and Adolescent Psychiatry, 1997 Primary Authors: Jon McClellan MD
Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder, Journal of the Academy of Child and Adolescent Psychiatry, 1997 Primary Authors: Jon McClellan MD
9/29/2011 TRENDS IN MENTAL DISORDERS. Trends in Child & Adolescent Mental Health: What to look for and what to do about it. Autism Spectrum Disorders
 Trends in Child & Adolescent Mental Health: What to look for and what to do about it. Jason J. Washburn, Ph.D., ABPP Director, Center for Evidence-Based Practice TRENDS IN MENTAL DISORDERS Autism Spectrum
Trends in Child & Adolescent Mental Health: What to look for and what to do about it. Jason J. Washburn, Ph.D., ABPP Director, Center for Evidence-Based Practice TRENDS IN MENTAL DISORDERS Autism Spectrum
1. What is a clinical disorder? [provide the detailed definition you learned in class]
![1. What is a clinical disorder? [provide the detailed definition you learned in class]](/thumbs/77/76431275.jpg "1. What is a clinical disorder? [provide the detailed definition you learned in class]") 1. What is a clinical disorder? [provide the detailed definition you learned in class] A constellation of symptoms that significantly impairs an individual s ability to function, and is characterized by
1. What is a clinical disorder? [provide the detailed definition you learned in class] A constellation of symptoms that significantly impairs an individual s ability to function, and is characterized by
Criteria for Child Psychiatrist on the Use of Selected Psychotropic Medications in Children & Adolescents
 Criteria for Child Psychiatrist on the Use of Selected Psychotropic Medications in Children & Adolescents DRUG NAME INDICATIONS / ACCEPTABLE USES PRIOR STIMULANT/ADHD DRUGS Daytrana (methylphenidate) ADHD
Criteria for Child Psychiatrist on the Use of Selected Psychotropic Medications in Children & Adolescents DRUG NAME INDICATIONS / ACCEPTABLE USES PRIOR STIMULANT/ADHD DRUGS Daytrana (methylphenidate) ADHD
Trends in Child & Adolescent Mental Health: What to look for and what to do about it.
 Trends in Child & Adolescent Mental Health: What to look for and what to do about it. Jason J. Washburn, Ph.D., ABPP Director, Center for Evidence-Based Practice TRENDS IN MENTAL DISORDERS 1 Autism Spectrum
Trends in Child & Adolescent Mental Health: What to look for and what to do about it. Jason J. Washburn, Ph.D., ABPP Director, Center for Evidence-Based Practice TRENDS IN MENTAL DISORDERS 1 Autism Spectrum
Affective Disorders.
 Affective Disorders http://www.bristol.ac.uk/medicalschool/hippocrates/psychethics/ Affective Disorders Depression Mania / Hypomania Bipolar mood disorder Recurrent depression Persistent mood disorders
Affective Disorders http://www.bristol.ac.uk/medicalschool/hippocrates/psychethics/ Affective Disorders Depression Mania / Hypomania Bipolar mood disorder Recurrent depression Persistent mood disorders
Kelly E. Williams, Pharm.D. PGY2 Psychiatric Pharmacy Resident April 16,2009
 Kelly E. Williams, Pharm.D. PGY2 Psychiatric Pharmacy Resident April 16,2009 List the antipsychotics most often prescribed Compare and contrast the use and adverse effects experienced in the pediatric
Kelly E. Williams, Pharm.D. PGY2 Psychiatric Pharmacy Resident April 16,2009 List the antipsychotics most often prescribed Compare and contrast the use and adverse effects experienced in the pediatric
Review of Psychotrophic Medications. (An approved North Carolina Division of Health Services Regulation Continuing Education Course)
") Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
J. Indian Assoc. Child Adolesc. Ment. Health 2012; 8(1):1-5. Editorial
:1-5. Editorial") 1 J. Indian Assoc. Child Adolesc. Ment. Health 2012; 8(1):1-5 Editorial Controversies in Paediatric Bipolar Disorder Vivek Agarwal 1, Sivakumar T 2 1.Editor JIACAM & Associate Professor, Department of
1 J. Indian Assoc. Child Adolesc. Ment. Health 2012; 8(1):1-5 Editorial Controversies in Paediatric Bipolar Disorder Vivek Agarwal 1, Sivakumar T 2 1.Editor JIACAM & Associate Professor, Department of
The New DSM- 5: A Clinical Discussion Through A Developmental Lens. Marit E. Appeldoorn, MSW, LICSW
 The New DSM- 5: A Clinical Discussion Through A Developmental Lens Marit E. Appeldoorn, MSW, LICSW 612-412- 1159 mappeldoornlicsw@gmail.com Introductions and My (Not- So- Bad) Dilemma What We Already Know
The New DSM- 5: A Clinical Discussion Through A Developmental Lens Marit E. Appeldoorn, MSW, LICSW 612-412- 1159 mappeldoornlicsw@gmail.com Introductions and My (Not- So- Bad) Dilemma What We Already Know
Understanding the Use of Psychotherapy and Psychotropic Medications for Oppositional Defiance and Conduct Disorders. Prof.
 Understanding the Use of Psychotherapy and Psychotropic Medications for Oppositional Defiance and Conduct s Prof. Daniel Kaplin College of Staten Island One of the new chapters in the Diagnostic and Statistical
Understanding the Use of Psychotherapy and Psychotropic Medications for Oppositional Defiance and Conduct s Prof. Daniel Kaplin College of Staten Island One of the new chapters in the Diagnostic and Statistical
III. Anxiety Disorders Supplement
 K-SADS-PL A. Screen Interview B. Supplements I. Disorders Supplement II. Psychotic Disorders Supplement III. Anxiety Disorders Supplement IV. Disorders Supplement V. Substance Disorders Supplement Advanced
K-SADS-PL A. Screen Interview B. Supplements I. Disorders Supplement II. Psychotic Disorders Supplement III. Anxiety Disorders Supplement IV. Disorders Supplement V. Substance Disorders Supplement Advanced
Attention deficit hyperactivity disorder (ADHD), Conduct disorder biological treatments
, Conduct disorder biological treatments") Attention deficit hyperactivity disorder (ADHD), Conduct disorder biological treatments Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal
Attention deficit hyperactivity disorder (ADHD), Conduct disorder biological treatments Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal
Mood Disorders Workshop Dr Andrew Howie / Dr Tony Fernando Psychological Medicine Faculty of Medical and Health Sciences University of Auckland
 Mood Disorders Workshop 2010 Dr Andrew Howie / Dr Tony Fernando Psychological Medicine Faculty of Medical and Health Sciences University of Auckland Goals To learn about the clinical presentation of mood
Mood Disorders Workshop 2010 Dr Andrew Howie / Dr Tony Fernando Psychological Medicine Faculty of Medical and Health Sciences University of Auckland Goals To learn about the clinical presentation of mood
Depressive and Bipolar Disorders
 Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Bipolar disorder and severe irritability in youth: Diagnosis and treatment. Ellen Leibenluft, M.D.
 Bipolar disorder and severe irritability in youth: Diagnosis and treatment Ellen Leibenluft, M.D. Chief, Section on Bipolar Spectrum Disorders Emotion and Development Branch National Institute of Mental
Bipolar disorder and severe irritability in youth: Diagnosis and treatment Ellen Leibenluft, M.D. Chief, Section on Bipolar Spectrum Disorders Emotion and Development Branch National Institute of Mental
Attention Deficit Hyperactivity Disorder (ADHD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Conduct comprehensive assessment and provide psychoeducation about ADHD, including clearly defined treatment expectations. Consider co-morbid developmental language disorder,
in Children under Age 6 Level 0 Conduct comprehensive assessment and provide psychoeducation about ADHD, including clearly defined treatment expectations. Consider co-morbid developmental language disorder,
Child and Adolescent Psychopharmacology Made Simple (2nd edition)
") Child and Adolescent Psychopharmacology Made Simple (2nd edition) Questions from chapter 1 1) It is likely that the majority of emotional suffering experienced by youngsters is related to a) genetics b)
Child and Adolescent Psychopharmacology Made Simple (2nd edition) Questions from chapter 1 1) It is likely that the majority of emotional suffering experienced by youngsters is related to a) genetics b)
Differentiating MDD vs. Bipolar Depression In Youth
 Differentiating MDD vs. Bipolar Depression In Youth Mai Uchida, M.D. Staff Physician Clinical and Research Programs in Pediatric Psychopharmacology Massachusetts General Hospital Disclosures Neither I
Differentiating MDD vs. Bipolar Depression In Youth Mai Uchida, M.D. Staff Physician Clinical and Research Programs in Pediatric Psychopharmacology Massachusetts General Hospital Disclosures Neither I
To Give or not to Give Medication: That is the Question
 To Give or not to Give Medication: That is the Question Charmi Patel Rao, MD September 14, 2018 Introduction Board Certified Child & Adolescent Psychiatrist Clinical expertise in ECMH and Developmental
To Give or not to Give Medication: That is the Question Charmi Patel Rao, MD September 14, 2018 Introduction Board Certified Child & Adolescent Psychiatrist Clinical expertise in ECMH and Developmental
Prevalence of Comorbidity and Pattern Drug Use among Children with Attention-deficit hyperactivity disorder: A Single Center in Thailand
 The 25th Federation Of Asian Pharmaceutical Association (FAPA) Congress 2014 Kota Kinabalu, Sabah, Malaysia 9th - 12th October, 2014 Prevalence of Comorbidity and Pattern Drug Use among Children with Attention-deficit
The 25th Federation Of Asian Pharmaceutical Association (FAPA) Congress 2014 Kota Kinabalu, Sabah, Malaysia 9th - 12th October, 2014 Prevalence of Comorbidity and Pattern Drug Use among Children with Attention-deficit
Impact of Psychotropics in School
 Impact of Psychotropics in School H O W T O C O O R D I N A T E C A R E A C R O S S S E T T I N G S W I L L I A M P U G A, M D C H I L D A N D A D O L E S C E N T P S Y C H I A T R I S T Age of onset
Impact of Psychotropics in School H O W T O C O O R D I N A T E C A R E A C R O S S S E T T I N G S W I L L I A M P U G A, M D C H I L D A N D A D O L E S C E N T P S Y C H I A T R I S T Age of onset
Evidence-Based Pharmacotherapy. Emily Harris, MD, MPH, FAAP Cincinnati Children s Hospital Medical Center
 Evidence-Based Pharmacotherapy Emily Harris, MD, MPH, FAAP Cincinnati Children s Hospital Medical Center CME Disclosure I have no personal financial relationships in any commercial interest related to
Evidence-Based Pharmacotherapy Emily Harris, MD, MPH, FAAP Cincinnati Children s Hospital Medical Center CME Disclosure I have no personal financial relationships in any commercial interest related to
Mental Illness. Doreen L. Rasp, APN, FNP, PMHNP Advanced Behavioral Counseling
 Mental Illness Doreen L. Rasp, APN, FNP, PMHNP Advanced Behavioral Counseling Moodiness Changing Bodies Narcissism Self-Esteem Ignorant Naïve Insecure Self-Centered Independent Adolescence Disorders Affecting
Mental Illness Doreen L. Rasp, APN, FNP, PMHNP Advanced Behavioral Counseling Moodiness Changing Bodies Narcissism Self-Esteem Ignorant Naïve Insecure Self-Centered Independent Adolescence Disorders Affecting
WORKING WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER (ADHD) OPPOSITIONAL DEFIANT DISORDER CONDUCT DISORDER
 OPPOSITIONAL DEFIANT DISORDER CONDUCT DISORDER") COURSES ARTICLE - THERAPYTOOLS.US WORKING WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER (ADHD) OPPOSITIONAL DEFIANT DISORDER CONDUCT DISORDER WORKING WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER (ADHD)
COURSES ARTICLE - THERAPYTOOLS.US WORKING WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER (ADHD) OPPOSITIONAL DEFIANT DISORDER CONDUCT DISORDER WORKING WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER (ADHD)
ADHD Explanation 5: Medications used in ADHD
 ADHD Explanation 5: Medications The aim of treatment is efficient functioning and achieving goals in life It is most important to find the dose of medications that works best As children grow they may
ADHD Explanation 5: Medications The aim of treatment is efficient functioning and achieving goals in life It is most important to find the dose of medications that works best As children grow they may
Pediatric Bipolar Disorder
 Pediatric Bipolar Disorder Jason J. Washburn, Ph.D., ABPP 1 Overview of Talk Bipolar Disorder Understanding Differences between Adults & Children Diagnosis of Pediatric Bipolar Disorder Treatment of Pediatric
Pediatric Bipolar Disorder Jason J. Washburn, Ph.D., ABPP 1 Overview of Talk Bipolar Disorder Understanding Differences between Adults & Children Diagnosis of Pediatric Bipolar Disorder Treatment of Pediatric
Introductory discussion
 Billina R. Shaw, MD Assistant Professor University of Maryland School of Medicine Department of Psychiatry Division of Child and Adolescent Psychiatry Introductory discussion Prescribing trends in foster
Billina R. Shaw, MD Assistant Professor University of Maryland School of Medicine Department of Psychiatry Division of Child and Adolescent Psychiatry Introductory discussion Prescribing trends in foster
The Mental Health and Wellbeing of Children and Adolescents who are affected by Autism and Related Disorders
 The Mental Health and Wellbeing of Children and Adolescents who are affected by Autism and Related Disorders Charles Cartwright, M.D Director: YAI Autism Center March 2013 Autism Spectrum Defined by the
The Mental Health and Wellbeing of Children and Adolescents who are affected by Autism and Related Disorders Charles Cartwright, M.D Director: YAI Autism Center March 2013 Autism Spectrum Defined by the
Index. Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) b-adrenergic blockers
 b-adrenergic blockers") Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Differentiating Unipolar vs Bipolar Depression in Children
 Differentiating Unipolar vs Bipolar Depression in Children Mai Uchida, M.D. Director, Center for Early Identification and Prevention of Pediatric Depression Massachusetts General Hospital Assistant Professor
Differentiating Unipolar vs Bipolar Depression in Children Mai Uchida, M.D. Director, Center for Early Identification and Prevention of Pediatric Depression Massachusetts General Hospital Assistant Professor
Judges Reference Table for the March 2016 Psychotropic Medication Utilization Parameters for Foster Children
 Judges Reference Table for the Psychotropic Medication Utilization Parameters for Foster Children Stimulants for treatment of ADHD Preschool (Ages 3-5 years) Child (Ages 6-12 years) Adolescent (Ages 13-17
Judges Reference Table for the Psychotropic Medication Utilization Parameters for Foster Children Stimulants for treatment of ADHD Preschool (Ages 3-5 years) Child (Ages 6-12 years) Adolescent (Ages 13-17
Tools that make a difference in mental health symptoms of autistic spectrum children Sumru Bilge-Johnson M.D. Program Director of Child Psychiatry
 Tools that make a difference in mental health symptoms of autistic spectrum children Sumru Bilge-Johnson M.D. Program Director of Child Psychiatry Fellowship Associate Professor, Child Psychiatry NEOMED
Tools that make a difference in mental health symptoms of autistic spectrum children Sumru Bilge-Johnson M.D. Program Director of Child Psychiatry Fellowship Associate Professor, Child Psychiatry NEOMED
HealthyPlace s Introductory Guide to Bipolar Disorder. By Natasha Tracy
 HealthyPlace s Introductory Guide to Bipolar Disorder By Natasha Tracy 1 Index Introduction Chapter One Bipolar Disorder Basics Chapter Two Bipolar Disorder Diagnosis Chapter Three Treatment of Bipolar
HealthyPlace s Introductory Guide to Bipolar Disorder By Natasha Tracy 1 Index Introduction Chapter One Bipolar Disorder Basics Chapter Two Bipolar Disorder Diagnosis Chapter Three Treatment of Bipolar
Mental Health & Your Teen Tools, Strategies & Resources
 3 rd Annual 22q11DS Family Conference Mental Health & Your Teen Tools, Strategies & Resources Dr. Claire De Souza Child & Adolescent Psychiatrist Medical Director, Consultation-Liaison Psychiatry Program
3 rd Annual 22q11DS Family Conference Mental Health & Your Teen Tools, Strategies & Resources Dr. Claire De Souza Child & Adolescent Psychiatrist Medical Director, Consultation-Liaison Psychiatry Program
SECTION 1. Children and Adolescents with Depressive Disorder: Summary of Findings. from the Literature and Clinical Consultation in Ontario
 SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
Practical Psychopharmacology for More Complex Mental Health Presentations
 MINISTRY OF CHILDREN AND YOUTH SERVICES Practical Psychopharmacology for More Complex Mental Health Presentations Part 1: Stimulants Dr. Ajit Ninan & Joel Lamoure 1 Practical Psychopharmacology for More
MINISTRY OF CHILDREN AND YOUTH SERVICES Practical Psychopharmacology for More Complex Mental Health Presentations Part 1: Stimulants Dr. Ajit Ninan & Joel Lamoure 1 Practical Psychopharmacology for More
CONTROVERSIES AND NEW DIRECTIONS
 BIPOLAR Introduction DISORDER IN CHILDHOOD AND EARLY ADOLESCENCE Introduction MELISSA P. D ELBELLO, DAVID AXELSON, and BARBARA GELLER CONTROVERSIES AND NEW DIRECTIONS Although the existence and diagnostic
BIPOLAR Introduction DISORDER IN CHILDHOOD AND EARLY ADOLESCENCE Introduction MELISSA P. D ELBELLO, DAVID AXELSON, and BARBARA GELLER CONTROVERSIES AND NEW DIRECTIONS Although the existence and diagnostic
Schedule FDA & literature based indications
 Psychotropic Medication List Recommended dosages are intended to serve only as a guide for children. Recommended doses are literature based. Clinicians should consult package insert of medications for
Psychotropic Medication List Recommended dosages are intended to serve only as a guide for children. Recommended doses are literature based. Clinicians should consult package insert of medications for
Depression in Adolescents PREMA MANJUNATH, MD CHILD AND ADOLESCENT PSYCHIATRIST
 Depression in Adolescents PREMA MANJUNATH, MD CHILD AND ADOLESCENT PSYCHIATRIST Francis Bacon Children sweeten labors, but they make misfortunes bitter. They increase the cares of life, but they mitigate
Depression in Adolescents PREMA MANJUNATH, MD CHILD AND ADOLESCENT PSYCHIATRIST Francis Bacon Children sweeten labors, but they make misfortunes bitter. They increase the cares of life, but they mitigate
A Brief Overview of Psychiatric Pharmacotherapy. Joel V. Oberstar, M.D. Chief Executive Officer
 A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
Advocating for people with mental health needs and developmental disability GLOSSARY
 Advocating for people with mental health needs and developmental disability GLOSSARY Accrued deficits: The delays or lack of development in emotional, social, academic, or behavioral skills that a child
Advocating for people with mental health needs and developmental disability GLOSSARY Accrued deficits: The delays or lack of development in emotional, social, academic, or behavioral skills that a child
Handout for the Neuroscience Education Institute (NEI) online activity: Juvenile Bipolar Disorder: Further Complicated by Comorbidity
 online activity: Juvenile Bipolar Disorder: Further Complicated by Comorbidity") Handout for the Neuroscience Education Institute (NEI) online activity: Juvenile Bipolar Disorder: Further Complicated by Comorbidity Learning Objectives Utilize evidence-based strategies to accurately
Handout for the Neuroscience Education Institute (NEI) online activity: Juvenile Bipolar Disorder: Further Complicated by Comorbidity Learning Objectives Utilize evidence-based strategies to accurately
Bipolar Disorder. Other Organic Diagnoses. Assessment/Diagnosis of Bipolar Disorder 2/6/2018 1
 Bipolar Disorder 2/6/2018 1 Assessment/Diagnosis of Bipolar Disorder Complicated; mimicking other disorders and has comorbidity (presents with other disorders) Half of bipolar children have relatives with
Bipolar Disorder 2/6/2018 1 Assessment/Diagnosis of Bipolar Disorder Complicated; mimicking other disorders and has comorbidity (presents with other disorders) Half of bipolar children have relatives with
11/11/2018. The ABCs of Medication Management for Autism Spectrum Disorder. ABC Logging (FBA) First. ABC Logging HOW TO COMPLEMENT BEHAVIORAL THERAPY
 First. ABC Logging HOW TO COMPLEMENT BEHAVIORAL THERAPY") The ABCs of Medication Management for Autism Spectrum Disorder OR HOW TO COMPLEMENT BEHAVIORAL THERAPY ABC Logging (FBA) First We need to know what, when, where and why behaviors happen. Antecedent: What
The ABCs of Medication Management for Autism Spectrum Disorder OR HOW TO COMPLEMENT BEHAVIORAL THERAPY ABC Logging (FBA) First We need to know what, when, where and why behaviors happen. Antecedent: What
EDUCATING THE EDUCATORS
 EDUCATING THE EDUCATORS A Professional Development Program of NAMI Massachusetts Newburyport School District May 7, 2015 Copyrighted and Developed by NAMI NJ GREAT Teachers are the Product of Nurture and
EDUCATING THE EDUCATORS A Professional Development Program of NAMI Massachusetts Newburyport School District May 7, 2015 Copyrighted and Developed by NAMI NJ GREAT Teachers are the Product of Nurture and
Mood Disorders for Care Coordinators
 Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
managing complicated ADHD in primary care
 managing complicated ADHD in primary care Nhung T. Tran, MD, FAAP vtran@sw.org Developmental-Behavioral Pediatrics Scott & White Healthcare Section of Child Development Associate Professor Texas A&M Health
managing complicated ADHD in primary care Nhung T. Tran, MD, FAAP vtran@sw.org Developmental-Behavioral Pediatrics Scott & White Healthcare Section of Child Development Associate Professor Texas A&M Health
Medications and Children Disorders
 Mental Health Comprehensive Services Providing Family Stability and Developing Life Coping Skills Medications and Children Disorders Psychiatric medications can be an effective part of the treatment for
Mental Health Comprehensive Services Providing Family Stability and Developing Life Coping Skills Medications and Children Disorders Psychiatric medications can be an effective part of the treatment for
475 Child & Adolescent Psychopharmacology p.1
 475 Child & Adolescent Psychopharmacology p.1 Introduction? #s of prescriptions for psychoactive meds have increased x2-3 in last 10 years? Ability to diagnose psychiatric disorders in children/adolescents
475 Child & Adolescent Psychopharmacology p.1 Introduction? #s of prescriptions for psychoactive meds have increased x2-3 in last 10 years? Ability to diagnose psychiatric disorders in children/adolescents