What would you think?
|
|
|
- Antony Henderson
- 5 years ago
- Views:
Transcription
1 What would you think?
2 Would you administer a medication to a patient if you were warned by the FDA that by giving it you have increased this resident s risk of death?
3 Strategies in Psychoactive Medication Management of Residents in Skilled Nursing Facilities Lou Czechowski RPh FASCP Senior Health First LLC A Consultant Pharmacist Service
4 FOR IMMEDIATE RELEASE June 16, 2008 FDA Requests Boxed Warnings on Older Class of Antipsychotic Drugs The U.S. Food and Drug Administration today exercised its new authority under the Food and Drug Administration Amendments Act of 2007 (FDAAA) to require manufacturers of "conventional" antipsychotic drugs to make safety-related changes to prescribing information, or labeling, to warn about an increased risk of death associated with the offlabel use of these drugs to treat behavioral problems in older people with dementia. In 2005, the FDA announced similar labeling changes for "atypical" antipsychotic drugs. At that time, Boxed Warnings, the FDA's strongest, were added. The Boxed Warning will now be added to an older class of drugs known as "conventional" antipsychotics. The warning for both classes of drugs will say that clinical studies indicate that antipsychotic drugs of both types are associated with an increased risk of death when used in elderly patients treated for dementia-related psychosis. "Thomas Laughren, M.D., director of the FDA's Division of Psychiatry Products in the Center for Drug Evaluation and Research. "The prescribing information for all antipsychotic drugs will be updated to describe the risk of death in elderly patients being treated for symptoms associated with dementia."
5 It s problems such as these that has lead to regulation of psychoactive medications in Long Term Care
6 CMS REGULATIONS Antidepressants, Sedative Hypnotics, Anxiolytics and Antipsychotics
7 Antidepressants antidepressants are prescribed for conditions other than depression, including: - Anxiety disorders - Post-traumatic stress disorder - Obsessive compulsive disorder - Insomnia - Neuropathic pain (ex. diabetic peripheral neuropathy) - Migraine headaches - Urinary incontinence
8 Gradual Dose Reduction (GDR) Requirements Duration - in accordance with pertinent literature-clinical practice guidelines. Antidepressants to manage behavior, stabilize mood, or treat a psychiatric disorder, during the first year in which a resident is admitted or after initiation GDR should be attempted during at least two separate quarters (with at least one month between the attempts), unless clinically contraindicated. After - first year, a GDR - attempted annually, unless clinically contraindicated. The GDR may be considered clinically contraindicated if: -The continued use is in accordance with relevant current standards of practice, and the physician has documented the clinical rationale for why any attempted dose GDR would be likely to impair the resident s function or cause psychiatric instability by exacerbating an underlying medical or psychiatric disorder; -OR - The resident s target symptoms returned or worsened after the most recent GDR within the care center and physician has documented the clinical rationale for why any additional attempted GDR at that time would be likely to impair the resident s function or cause psychiatric instability by exacerbating an underlying medical or psychiatric disorder.
9 Anxiolytics Indications 1. Use is for one of the following indications as defined in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Training Revision (DSM-IV TR) or subsequent editions: o Generalized Anxiety Disorder o Panic Disorder o Symptomatic anxiety that occurs in residents with another diagnosed psychiatric disorder (ex. depression, adjustment disorder) o Sleep disorders (refer to Sedative/Hypnotic requirements) o Acute alcohol/benzodiazepine withdrawal o Significant anxiety in response to a situational trigger o Delirium, dementia and other cognitive disorders with associated behaviors that: Are quantitatively and objectively documented Are persistent Are not due to preventable or correctable reasons Constitute clinically significant distress
10 Anxiolytics should only be used when: 2. Evidence exists that other possible reasons for the individual s distress have been considered; AND 3. Use of the anxiolytic results in maintenance or improvement in the resident's mental, physical or psychosocial well-being (ex. as reflected on the MDS or other assessment tools); OR 4. There are clinical situations that warrant the use of anxiolytics such as: a. A long-acting benzodiazepine is being used to withdraw the resident from a short-acting benzodiazepine. b. Used for neuromuscular syndromes (ex. cerebral palsy, tardive dyskinesia, restless leg syndrome, or seizure disorders) c. Symptom relief in end-of-life situations 5. These regulations pertain to short-acting and long-acting benzodiazepines, Buspar (Buspirone), and any antidepressants (except Wellbutrin [Bupropion]) used as an anxiolytic.
11 Anxiolytic (Anti-Anxiety Medication) regulations Brand Name Generic Name Daily Dose Thresholds (mg/day) Ativan Lorazepam 2 mg Dalmane Flurazepam 15mg Doral Quazepam 7.5mg Klonopin Clonazepam 1.5 mg Librium Chlordiazepoxide 20 mg ProSom Estazolam 0.5 mg Serax Oxazepam 30 mg Tranxene Clorazepate 15 mg Valium Diazepam 5 mg Xanax Alprazolam 0.75 mg The following medications are not appropriate for use as an anxiolytic Equanil, - Meprobamate Atarax, Vistaril, -Hydroxyzine Benadryl -Diphenhydramine
12 Anxiolytic Gradual Dose Reduction (GDR) Requirements During the first year in which a resident is admitted or after initiation Gradual Dose Reduction (GDR) should be attempted during at least two separate quarters (with at least one month between the attempts), unless clinically contraindicated. After the first year, a GDR should be attempted annually, unless clinically contraindicated. The GDR may be considered clinically contraindicated if: - The continued use is in accordance with relevant current standards of practice, and the physician has documented the clinical rationale for why any attempted dose reduction would be likely to impair the resident s function or cause psychiatric instability by exacerbating an underlying medical or psychiatric disorder; OR - The resident s target symptoms returned or worsened after the most recent GDR within the care center, and the physician has documented the clinical rationale for why any additional attempted dose reduction at that time would be likely to impair the resident s function or cause psychiatric instability by exacerbating an underlying medical or psychiatric disorder.
13 Sedative Hypnotics Before initiating medications to treat insomnia, other factors potentially causing insomnia should be evaluated, including, for example: - Environment, such as excessive heat, cold, or noise; lighting - Inadequate physical activity - Care center routines that may not accommodate residents individual needs (ex. time for sleep, awakening, toileting, medication treatments) - Provision of care in a manner that disrupts sleep - Caffeine or medications known to disrupt sleep - Pain and discomfort - Underlying conditions (secondary or co-morbid insomnia) such as psychiatric disorders (ex. depression), cardiopulmonary disorders (ex. COPD, CHF), urinary frequency, pain, obstructive sleep apnea, and restless leg syndrome It is expected that interventions (such as sleep hygiene approaches, individualizing the sleep and wake times to accommodate the person s wishes and prior customary routine, and maximizing treatment of any underlying conditions) are implemented to address the causative factor(s). The use of sedating medications for residents with diagnosed sleep apnea requires careful assessment, documented clinical rationale, and close monitoring.
14 Sedative Hypnotics These guidelines apply to any medication that is being used to treat insomnia. Initiation of medications to induce or maintain sleep should be preceded or accompanied by other interventions to try to improve sleep. All sleep medications should be used in accordance with approved product labeling (ex. timing and frequency of administration relative to anticipated waking time). The use of sedating medications for residents with diagnosed sleep apnea requires careful assessment, documented clinical rationale, and close monitoring. Exceptions: - Use of a single dose sedative for dental/medical procedures - During initiation of treatment for depression, pain or other co-morbid conditions, short-term use of a sedative/hypnotic may be necessary until symptoms improve or the underlying aggravating factor can be identified and/or effectively treated.
15 Ambien -Zolpidem 5mg Ambien CR- Zolpidem CR 6.25 mg Ativan - Lorazepam 1 mg Lunesta - Eszopiclone 1 mg ProSom - Estazolam 0.5 mg Restoril - Temazepam 15 mg Rozerem -Ramelteon 8 mg Atarax, Vistaril, etc. -Hydroxyzine 50 mg Dalmane Flurazepam- 15 Benadryl Diphenhydramine- 25 mg Doral Quazepam mg Halcion Triazolam mg Noctec, etc. - Chloral hydrate 500 mg
16 Sedative Hypnotic Gradual Dose Reduction (GDR) Requirements For as long as a resident remains on a sedative/hypnotic that is used routinely and beyond the manufacturer s recommendations for duration of use, required Gradual Dose Reduction (GDR) quarterly unless clinically contraindicated. Clinically contraindicated means: - The continued use is in accordance with relevant current standards of practice, and the physician has documented the clinical rationale for why any attempted dose reduction would be likely to impair the resident s function or cause psychiatric instability by exacerbating an underlying medical or psychiatric disorder, OR - The resident s target symptoms returned or worsened after the most recent attempt at tapering the dose within the care center, and the physician has documented the clinical rationale for why any additional attempted dose reduction at that time would be likely to impair the resident s function or cause psychiatric instability by exacerbating an underlying medical or psychiatric disorder.
17 Antipsychotics Indications An antipsychotic should only be used for the following conditions/diagnoses as documented in the resident s clinical record and meets the definition(s) in the Diagnostic & Statistical Manual of Mental Disorders, Fourth Edition, Training Revision (DSM-IV TR) or subsequent editions: - Schizophrenia - Schizo-affective disorder - Delusional Disorder - Mood Disorders (mania, bipolar disorder, depression with psychotic features, and treatment-refractory major depression) - Schizophreniform disorder - Psychosis NOS - Atypical psychosis - Brief psychotic disorder - Dementing illnesses with associated behavioral symptoms - Medical illnesses or delirium with manic or psychotic symptoms and/or treatmentrelated psychosis or mania (ex. Thyrotoxicosis, neoplasms, high dose steroids)
18 Antipsychotics Criteria Since diagnoses alone do not warrant the use of antipsychotics, the clinical condition must also meet at least one of the following criteria: 1. The symptoms due to mania or psychosis (such as: auditory, visual or other hallucinations; delusions [such as paranoia or grandiosity]) 2. The behavioral symptoms present a danger to the resident or others 3. The symptoms are significant enough that the resident is experiencing one or more of the following: a. inconsolable or persistent distress (ex. fear, continuous yelling, screaming, distress associated with end-of-life, or crying) b. a significant decline in function c. substantial difficulty receiving needed care (ex. not eating resulting in weight loss, fear and not bathing leading to skin breakdown or infection)
19 Antipsychotics Additional requirements Acute Psychiatric Situations - When an antipsychotic is initiated or used to treat an acute psychiatric emergency (i.e. recent or abrupt onset or exacerbation of symptoms) related to one or more of the allowable conditions/diagnoses listed above, that use must meet all of the following additional requirements: o The acute treatment is limited to 7 days or less o A clinical in conjunction with the interdisciplinary team must evaluate and document the situation within 7 days, to identify/address any contributing/underlying causes of the condition and verify the continued need of the antipsychotic o Pertinent non-pharmacological interventions must be attempted, unless contraindicated, and documented following the resolution of the acute psychiatric situation
20 Antipsychotics Enduring Psychiatric Situations - When an antipsychotic is used to treat an enduring (i.e. non-acute, chronic or prolonged) condition, the target behavior must be clearly and specifically identified, and monitored objectively and qualitatively, in order to ensure the behavioral symptoms are: o Not due to a medical condition or problem (ex. headache or joint pain, fluid or electrolyte imbalance, pneumonia, hypoxia, unrecognized hearing/visual impairment) that can be expected to improve or resolve as the underlying condition is treated; AND o Persistent or likely to reoccur without continued treatment; AND o Not sufficiently relieved by non-pharmacological interventions; AND o Not due to environmental stressors (ex. alteration in the resident s customary location or daily routine, unfamiliar care provider, hunger/thirst, excessive noise for that individual, inadequate or inappropriate staff response, physical barriers) that can be addressed to improve the psychotic symptoms or maintain safety; AND o Not due to psychological stressors (ex. loneliness, taunting, abuse), or anxiety/fear stemming from misunderstanding related to cognitive impairment (ex. the mistaken belief that this is not where he/she lives or inability to find his/her clothes/glasses) that can be expected to improve or resolve as the situation is addressed
21 Antipsychotics Exception: When an antipsychotic is used for behavioral disturbances related to Tourette s disorder, of for non-psychiatric indications such as movement disorders associated with Huntington s disease, hiccups, nausea/vomiting associated with cancer or cancer chemotherapy, or adjunctive therapy at end-of-life.
22 Antipsychotics Inadequate Indications Antipsychotics should not be used if the only indication is any of the following: 1. Wandering 2. Poor self-care 3. Restlessness 4. Impaired memory 5. Mild anxiety 6. Insomnia 7. Unsociability 8. Inattention or indifference to surroundings 9. Fidgeting 10. Nervousness 11. Uncooperativeness 12. Verbal expressions or behavior that are not due to the conditions listed under Indications and do not represent a danger to the resident or others.
23 Antipsychotics Doses for acute indications (ex. delirium) may differ from those used for long-term treatment, but should be the lowest possible to achieve the desired therapeutic effects. Brand name Generic name Daily Dose Thresholds (mg/day) used to manage behavioral symptoms related to dementing illnesses Clozaril- Clozapine 50 mg Compazine Prochlorperazine Not customarily used for the treatment of behavioral symptoms Haldol Haloperidol 2 mg Loxitane Loxapine 10 mg Mellaril Thioridazine 75 mg Moban Molindone 10 mg Navane Thiothixene 7 mg Prolixin Fluphenazine 4 mg Geodon Ziprasidone Not customarily used for the treatment of behavioral symptoms Risperdal Risperidone 2 mg Seroquel Quetiapine 150 mg Stelazine Trifluoperazine 8 mg Thorazine Chlorpromazine 75 mg Trilafon Perphenazine 8 mg Zyprexa Olanzapine 7.5 mg Abilify Aripiprazole 10 mg
24 Antipsychotic Gradual Dose Reduction (GDR) Requirements Within the first year in which a resident is admitted on an antipsychotic or after initiation Gradual Dose Reduction (GDR) must be attempted in two separate quarters (with at least one month between attempts), unless clinically contraindicated. After the first year, a GDR must be attempted annually, unless clinically contraindicated. For any resident receiving an antipsychotic to treat dementia-related behavioral symptoms, the GDR may be considered clinically contraindicated if: -The resident s target symptoms returned or worsened after the most recent attempt at a GDR within the care center; AND - The physician as documented the clinical rationale for why any additional attempted dose reduction at that time would be likely to impair the resident s function or increase distressed behavior.
25 Antipsychotics For any resident receiving an antipsychotic to treat a psychiatric disorder other than dementia-related behavioral symptoms, the GDR may be considered clinically contraindicated if: -The continued use is in accordance with relevant current standards of practice, and the physician has documented the clinical rationale for why any attempted dose reduction would be likely to impair the resident s function or cause psychiatric instability by exacerbating an underlying psychiatric disorder; OR - The resident s target symptoms returned or worsened after the most recent GDR attempt within the care center, and the physician has documented the clinical rationale for why any attempted dose reduction would be likely to impair the resident s function or cause psychiatric instability by exacerbating an underlying psychiatric disorder
26 Antipsychotics Monitoring/Adverse Consequences Residents are to be adequately monitored for antipsychotic adverse consequences, such as: - Anticholinergic effects - Akathisia - Neuroleptic Malignant Syndrome (NMS) - Cardiac arrhythmias - Death secondary to heart-related events (ex. heart failure, sudden death) - Falls - Lethargy - Increase in total cholesterol and triglycerides - Parkinsonism - Blood sugar elevation (including diabetes mellitus) - Orthostatic hypotension - Cerebrovascular event (ex. stroke, transient ischemic attack) in older residents with dementia - Tardive dyskinesia - Excessive sedation When antipsychotics are used without monitoring, they may be considered unnecessary medications because of inadequate monitoring.

27 Antipsychotics Monitoring

28 Antipsychotics Monitoring
29 Antipsychotics Monitoring Behavior Form Problems Often not seriously taken Lack of proper behaviors for monitoring suggested by CMS regulation of clinician Problem area often found by surveyors
30 Antipsychotics Monitoring Behavior forms benefits Quanitative assessment Identify trends (positive or negative) Comply with CMS regs
31 Antipsychotics Monitoring To improve compliance Have physician specify targeted behaviors (from regulations) 1. The symptoms due to mania or psychosis (such as: auditory, visual or other hallucinations; delusions [such as paranoia or grandiosity]) 2. The behavioral symptoms present a danger to the resident or others 3. The symptoms are significant enough that the resident is experiencing one or more of the following: a. inconsolable or persistent distress (ex. fear, continuous yelling, screaming, distress associated with end-of-life, or crying) b. a significant decline in function c. substantial difficulty receiving needed care (ex. not eating resulting in weight loss, fear and not bathing leading to skin breakdown or infection)
32 Antipsychotic Medications History Antipsychotics are a group of psychoactive drugs commonly but not exclusively used to treat psychosis which is typified by schizophrenia. A first generation of antipsychotics, known as typical antipsychotics, was discovered in the 1950s. Most of the drugs in the second generation, known as atypical antipsychotics, have more recently been developed, although the first atypical anti-psychotic, clozapine, was discovered in the 1950s, and introduced clinically in the 1970s. Both classes of medication tend to block receptors in the brain's dopamine pathways but antipsychotic drugs encompass a wide range of receptor targets. A number of side effects have been observed in relation to specific medications, including weight gain, agranulocytosis,, tardive dyskinesia, tardive akathisias, tardive psychoses and tardive dysphrenias. The development of new antipsychotics, and the relative efficacy of different ones, is an important ongoing field of research. Antipsychotic medication is not generally regarded as a good treatment, just the best available. The most appropriate drug for an individual patient requires careful consideration.
33 The Term Antipsychotics are also referred to as neuroleptic drugs. ] The word neuroleptic is derived from Greek: "νεύρον" (originally meaning sinew but today referring to the nerves) and "λαμβάνω" (meaning take hold of). Thus, the word means taking hold of one's nerves. This term reflects the drugs' ability to make movement more difficult and sluggish, which clinicians previously believed indicated that a dose was high enough ] Antipsychotics are broadly divided into two groups, the typical or first-generation antipsychotics and the atypical or second-generation antipsychotics. There are also dopamine partial agonists, which are often categorized as atypicals.
34 Antipsychotic History The first antipsychotic was chlorpromazine, which was developed as a surgical anesthetic. It was first used on psychiatric patients because of its powerful calming effect; at the time it was regarded as a "chemical lobotomy". Lobotomy was used to treat many behavioral disorders, including psychosis, although its "effectiveness" was (from a modern viewpoint) due to its tendency to markedly reduce behavior of all types. However, chlorpromazine quickly proved to reduce the effects of psychosis in a more effective and specific manner than the extreme lobotomylike sedation it was known for.

35
36 All antipsychotic drugs tend to block D 2 receptors in the dopamine pathways of the brain. This means that dopamine released in these pathways has less effect. Excess release of dopamine in the mesolimbic pathway has been linked to psychotic experiences. It is the blockade of dopamine receptors in this pathway that is thought to control psychotic experiences.
37 The nigrostriatal pathway is a neural pathway that connects the substantia nigra with the striatum. It is one of the four major dopamine pathways in the brain, and is particularly involved in the production of movement, as part of a system called the basal ganglia motor loop. Loss of dopamine neurons in the substantia nigra is one of the main pathological features of Parkinson's disease, leading to a marked reduction in dopamine function in this pathway. The symptoms of the disease typically do not show themselves until 80-90% of dopamine function has been lost. This pathway is also implicated in producing tardive dyskinesia, one of the side-effects of antipsychotic drugs. These medications (particularly the older typical antipsychotics) block D 2 dopamine receptors in multiple pathways in the brain. The desired clinical effect of reducing psychotic symptoms is thought to be associated with blocking dopamine function in the mesolimbic pathway only. However, as many of these drugs are not selective, they block dopamine in all pathways. When this happens in the nigrostriatal pathway, similar movement problems to those found in Parkinson's disease can occur.
38 Geriatric Considerations Many elderly patients receive antipsychotic medications for inappropriate nonpsychotic behavior. Before initiating antipsychotic medication, the clinician should investigate any possible reversible cause; any stress or stress from any disease can cause acute confusion or worsening of baseline nonpsychotic behavior. Most commonly acute changes in behavior are due to increases in drug dose or addition of new drug to regimen; fluid electrolyte loss; infections; and changes in environment.
39 GERIATRIC CONSIDERATIONS In the treatment of agitated, demented, elderly patients, authors of meta-analysis of controlled trials of the response to the traditional antipsychotics (phenothiazines, butyrophenones) in controlling agitation have concluded that the use of neuroleptics results in a response rate of 18%. Clearly neuroleptic therapy for behavior control should be limited with frequent attempts to withdraw the agent given for behavior control. In light of significant risks and adverse effects in elderly population compared with limited data demonstrating efficacy in the treatment of dementia related psychosis, aggression, and agitation, An extensive risk:benefit analysis should be performed prior to use.
40 FDA FOR IMMEDIATE RELEASE June 16, 2008 FDA Requests Boxed Warnings on Older Class of Antipsychotic Drugs The U.S. Food and Drug Administration today exercised its new authority under the Food and Drug Administration Amendments Act of 2007 (FDAAA) to require manufacturers of "conventional" antipsychotic drugs to make safety-related changes to prescribing information, or labeling, to warn about an increased risk of death associated with the off-label use of these drugs to treat behavioral problems in older people with dementia. In 2005, the FDA announced similar labeling changes for "atypical" antipsychotic drugs. At that time, Boxed Warnings, the FDA's strongest, were added. The Boxed Warning will now be added to an older class of drugs known as "conventional" antipsychotics. The warning for both classes of drugs will say that clinical studies indicate that antipsychotic drugs of both types are associated with an increased risk of death when used in elderly patients treated for dementia-related psychosis. "Thomas Laughren, M.D., director of the FDA's Division of Psychiatry Products in the Center for Drug Evaluation and Research. "The prescribing information for all antipsychotic drugs will be updated to describe the risk of death in elderly patients being treated for symptoms associated with dementia."
41 The medications involved in this action are: Conventional Antipsychotic Drugs Atypical Antipsychotics Compazine (prochlorperazine) Abilify (aripiprazole) Haldol (haloperidol) Clozaril (clozapine) Loxitane (loxapine) FazaClo (clozapine) Mellaril (thioridazine) Geodon (ziprasidone) Moban (molindrone) Invega (paliperidone) Navane (thithixene) Risperdal (risperidone) Orap (pimozide) Seroquel (quetiapine) Prolixin (fluphenazine) Zyprexa (olanzapine) Stelazine (trifluoperazine) Symbyax (olanzapine and fluoxetine) Thorazine (chlorpromazine) Trilafon (perphenazine)
42 FDA Recently, two observational epidemiological studies were published that examined the risk of death in elderly patients with dementia who were treated with conventional antipsychotic drugs. The investigators compared the risk for death with use of an atypical antipsychotic versus either no antipsychotic or the use of a conventional antipsychotic. These studies have limitations that preclude reaching a definitive conclusion about comparative death rates for atypical and conventional antipsychotic drugs. Nevertheless, the FDA has concluded that these studies, along with the earlier evidence for atypical antipsychotic drugs, suggest that both classes of drugs should be considered to have an increased risk of death when used in elderly patients treated for dementiarelated psychosis.
43 Concerns Related to Antipsychotics Dementia: [U.S. Boxed Warning]: Elderly patients with dementia-related psychosis treated with antipsychotics dare at an increased risk of death compared to placebo. Most deaths appeared to be either cardiovascular (eg, heart failure, sudden death) or infectious (eg, pneumonia) in nature. Antipsychotics are not approved for the treatment of dementia-related psychosis. Seizures: Use with caution in patients at risk of seizures, including those with a history of seizures, head trauma, brain damage, alcoholism, or concurrent therapy with medications which may lower seizure threshold. Elderly patients may be at increased risk of seizures due to an increased prevalence of predisposing factors.
44 Implications of Black Box Warnings Thomas Laughren MD director of the FDA divisison of psychiatry products noted Not telling physicians to avoid use in dementia Meant to help families balance the risk of the medications against the benefit Evidence is poor supporting off label use of antipsychotics in treating dementia None of the medications have an dementia as an indication Lack of indication indicates lack of data
45 Implications of Black Box Warnings Yon Chen MD (University of Mass) published a study in Archives of Internal Medicine found more than 1/3 of nursing home residents who were prescribed an antipsychotic and no clinical indications for the drug (Journal of Archives of Internal Medicine )
46 Implications of Black Box warnings Increased risk of Citations during survey Increased risk of lawsuits
47 Decreasing Risk Extensive Risk/Benefit documentation regarding black box warnings by physician Risk of diabetes, Cardiovascular disease Benefits pharmacological benefit of medication provides significant improvement in behaviors that posed harm to resident or others. Risk/Benefit waiver for families Include black box warnings
48 ANTIPSYCHOTIC RISK / BENEFIT ACKNOWLEDGEMENT FORM Date: Resident / Room: Physician: Prescribed Antipsychotic Diagnosis: Because of the black-box warning in the prescribing information for antipsychotics when used in patients with dementia, a risk / benefit analysis is essential. Benefits Potential Risks Improved functional status Diabetes Control of distressing symptoms Myocardial Infarction Improved quality of life Stroke Death While the resident is prescribed an antipsychotic, members of the interdisciplinary care team will: Ensure lowest possible doses are utilized Review ongoing risk / benefit of continued use during interdisciplinary team meetings Attempt gradual dose reductions Monitor for side effects of the medication Please acknowledge that you have reviewed the risks vs. benefits of antipsychotic use in this resident.
49 Strategies Decreasing antipsychotic use Ensure that Consultant Pharmacist Notes include review of antipsychotic medications Ensure that Physicians review CRPh notes thoroughly Psychoactive Committees Need to have a understanding of medications as well as regulation
50 Decreasing Antipsychotic Use Education Often staff is the most common reason that medications are initiated Need to rule out physical condition as underlying cause/contribution to exacerbation to behaviors CMS regs require this
51 Decreasing Antipsychotic Use CMS Regulations Not due to a medical condition or problem (ex. headache or joint pain, fluid or electrolyte imbalance, pneumonia, hypoxia, unrecognized hearing/visual impairment) that can be expected to improve or resolve as the underlying condition is treated; AND o Persistent or likely to reoccur without continued treatment; AND o Not sufficiently relieved by non-pharmacological interventions; AND o Not due to environmental stressors (ex. alteration in the resident s customary location or daily routine, unfamiliar care provider, hunger/thirst, excessive noise for that individual, inadequate or inappropriate staff response, physical barriers) that can be addressed to improve the psychotic symptoms or maintain safety; AND o Not due to psychological stressors (ex. loneliness, taunting, abuse), or anxiety/fear stemming from misunderstanding related to cognitive impairment (ex. the mistaken belief that this is not where he/she lives or inability to find his/her clothes/glasses) that can be expected to improve or resolve as the situation is addressed
52 Decreasing Antipsychotic Use Suggest new orders be written with a review (e.g. Quetiapine 50mg q hs x 2 weeks then review) To observe for change in physical condition UTI, URI, pain related to physical condition Resolve in behaviors may be related to physical condition and interpreted as positive medication response
53 Decreasing Antipsychotic Use Have Consultant Pharmacist perform medication review to see if new onset behaviors related to medication(s) Oxybutynin, Phenytoin dosage etc.. Rule out Hypo/Hyperthyroidism, anemia, change in renal function (affect medication clearance, e.g. Digoxin etc)
54 Psychoactive Rounds Medical Director, Consultant Pharmacist, Nursing other members of interdisciplinary team. Began in 2006 as an interdisciplinary meeting lasting 3-4 hours a month reviewing all residents Rounding began in 2008 with Medical Director, Consultant Pharmacist and representive member from the unit
55 Psychoactive Rounds Rounding last 1-2 hours monthly Improved psychoactive monitoring Use of behavioral forms was taken seriously by staff Point person (usually RN) was established to carry out recommendations from the rounding team Included, contacting psychiatry, updating behavior forms and any pertinent issues
56
57
58

59
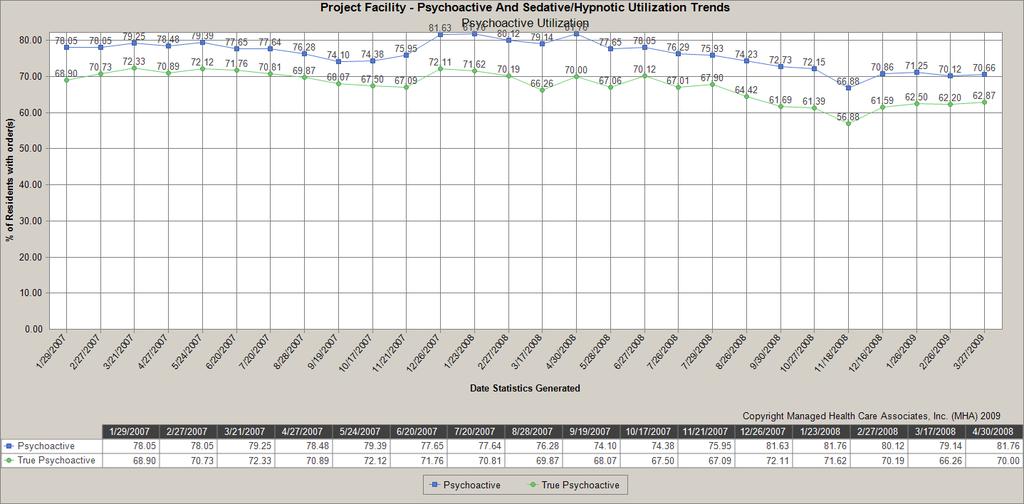
60 Outcomes Decreased psychoactive medication use Established relationship between CRPh, physicians as well as staff Increased compliance with behavioral monitoring forms
61 Consultant Pharmacy Service The Office of the Inspector General (OIG) published an annual notice soliciting proposals and recommendations for developing new and modifying existing safe harbor provisions under the Federal anti-kickback statute (section 1128B(b) of the Social Security Act), as well as developing new OIG Special Fraud Alerts. Public comments must be delivered by no later than 5 p.m. on March 1, 2010.
62 NEWS! The Office of the Inspector General (OIG) published an annual notice soliciting proposals and recommendations for developing new and modifying existing safe harbor provisions under the Federal anti-kickback statute (section 1128B(b) of the Social Security Act), as well as developing new OIG Special Fraud Alerts. Public comments must be delivered by no later than 5 p.m. on March 1, 2010.
63 NEWS! At the same time, the United States announced the unsealing of its Complaint against two large nursing home chains, Mariner Health Care, Inc. SavaSeniorCare Administrative Services, LLC, both of Atlanta, Georgia, and their principals, Leonard Grunstein, Murray Forman and Rubin Schron.
64 NEWS! The Government contends that Omnicare offered its consultant pharmacist services to nursing homes at below cost and below fair market value in order to induce the homes to refer their patients to Omnicare for dispensing pharmacy services.
65 American Society of Consultant Pharmacists Because of the potential for conflicts of interest, or the appearance of conflicts of interest, the American Society of Consultant Pharmacists recommends that consultant pharmacists who serve long-term care facilities should be independent of the longterm care pharmacy that provides medications to residents of the facility - Feb 2010
Objectives. Antipsychotics 7/25/2016. LeadingAge Florida 53rd Annual Convention & Exposition
 Reducing the Use of Antipsychotics in Long Term Care Communities Alan W. Obringer RPh, CPh, CGP Executive Director Senior Care Pharmacy Objectives Recognize the clinical evidence for the need to change
Reducing the Use of Antipsychotics in Long Term Care Communities Alan W. Obringer RPh, CPh, CGP Executive Director Senior Care Pharmacy Objectives Recognize the clinical evidence for the need to change
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist. HMS Training Webinar January 27, 2017
 Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan Pretest 1. Appropriate target symptoms for emergency room medication treatment
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan Pretest 1. Appropriate target symptoms for emergency room medication treatment
The Basics of Psychoactive/Psychotropic Medications Tina Sanchez, RN, SMQT New Mexico Department of Health Division of Health Improvement State
 The Basics of Psychoactive/Psychotropic Medications Tina Sanchez, RN, SMQT New Mexico Department of Health Division of Health Improvement State RAI/MDS Coordinator Objectives Upon completion of this training,
The Basics of Psychoactive/Psychotropic Medications Tina Sanchez, RN, SMQT New Mexico Department of Health Division of Health Improvement State RAI/MDS Coordinator Objectives Upon completion of this training,
Psychotropic Medication Use in Dementia
 Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
9/11/2012. Clare I. Hays, MD, CMD
 Clare I. Hays, MD, CMD Review regulatory background for current CMS emphasis on antipsychotics Understand the risks and (limited) benefits of antipsychotic medications Review non-pharmacologic management
Clare I. Hays, MD, CMD Review regulatory background for current CMS emphasis on antipsychotics Understand the risks and (limited) benefits of antipsychotic medications Review non-pharmacologic management
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
Psychotropic Medication. Including Role of Gradual Dose Reductions
 Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
12/17/2012. Unnecessary Drugs
 Nursing Home Social Work Webinar Series December 19, 2012 Dr. Robin P. Bonifas, PhD, MSW Arizona State University School of Social Work Importance of familiarity with psychotropic medication regulations.
Nursing Home Social Work Webinar Series December 19, 2012 Dr. Robin P. Bonifas, PhD, MSW Arizona State University School of Social Work Importance of familiarity with psychotropic medication regulations.
Antipsychotic Medication
 Antipsychotic Medication Mary Knutson, RN 3-7-12 Mosby items and derived items 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 1 Clinical Uses of Antipsychotics Short-term: in severe depression and
Antipsychotic Medication Mary Knutson, RN 3-7-12 Mosby items and derived items 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 1 Clinical Uses of Antipsychotics Short-term: in severe depression and
Integrating INTERACT into Interim Pharmacist Reviews
 Integrating INTERACT into Interim Pharmacist Reviews Chad R. Worz, Pharm.D. President, Medication Managers, LLC Adjunct Assistant Professor of Pharmacy Practice, University of Cincinnati, College of Pharmacy
Integrating INTERACT into Interim Pharmacist Reviews Chad R. Worz, Pharm.D. President, Medication Managers, LLC Adjunct Assistant Professor of Pharmacy Practice, University of Cincinnati, College of Pharmacy
Appendix: Psychotropic Medication Reference Tables
 Appendix: Psychotropic Medication Reference Tables How to Use these Tables These reference tables are designed to provide clinic staff with specific medication related criteria for the Polypharmacy, Cardiometabolic
Appendix: Psychotropic Medication Reference Tables How to Use these Tables These reference tables are designed to provide clinic staff with specific medication related criteria for the Polypharmacy, Cardiometabolic
Use of Psychotropic Medications in Older Adults with Dementia!
 Use of Psychotropic Medications in Older Adults with Dementia! Deepa Pattani, PharmD, RPh Owner: PrevInteract Health Deepa.Pattani@PrevInteract.com 972-372-9775 About Me Deepa Pattani, PharmD, RPh with
Use of Psychotropic Medications in Older Adults with Dementia! Deepa Pattani, PharmD, RPh Owner: PrevInteract Health Deepa.Pattani@PrevInteract.com 972-372-9775 About Me Deepa Pattani, PharmD, RPh with
SEDATIVE-HYPNOTIC AGENTS
 SEDATIVE-HYPNOTIC AGENTS Documentation A. FDA approved indications 1. Insomnia 2. Sedation for an agitated patient in an inpatient setting Documentation B. Non-FDA approved, commonly used indications 1.
SEDATIVE-HYPNOTIC AGENTS Documentation A. FDA approved indications 1. Insomnia 2. Sedation for an agitated patient in an inpatient setting Documentation B. Non-FDA approved, commonly used indications 1.
MO Medicaid Foster Care Drugs FY10-FY14
 MO Medicaid Foster Care Drugs FY10-FY14 Medicaid (MO HealthNet) Cost of Drugs given to Missouri Foster Care Children by combinations of Age, Gender, Drug Class and Fiscal Year [Raw Data Provided by Missouri
MO Medicaid Foster Care Drugs FY10-FY14 Medicaid (MO HealthNet) Cost of Drugs given to Missouri Foster Care Children by combinations of Age, Gender, Drug Class and Fiscal Year [Raw Data Provided by Missouri
Psychiatric Illness. In the medical arena psychiatry is a fairly recent field A challenging field Numerous diagnosis
 Psychiatric Illness In the medical arena psychiatry is a fairly recent field A challenging field Numerous diagnosis 12,000,000 children infants through 18 y/o nation wide 5,000,000 suffer severely Serious
Psychiatric Illness In the medical arena psychiatry is a fairly recent field A challenging field Numerous diagnosis 12,000,000 children infants through 18 y/o nation wide 5,000,000 suffer severely Serious
Dementia Care Principles
 New CMS Surveyor Guidance: Care & Services for a Resident with Dementia Cat Selman, BS www.thehealthcarecommunicators.com 2015 The Healthcare Communicators, Inc. All rights reserved. Dementia Care Principles
New CMS Surveyor Guidance: Care & Services for a Resident with Dementia Cat Selman, BS www.thehealthcarecommunicators.com 2015 The Healthcare Communicators, Inc. All rights reserved. Dementia Care Principles
Medications and Children Disorders
 Mental Health Comprehensive Services Providing Family Stability and Developing Life Coping Skills Medications and Children Disorders Psychiatric medications can be an effective part of the treatment for
Mental Health Comprehensive Services Providing Family Stability and Developing Life Coping Skills Medications and Children Disorders Psychiatric medications can be an effective part of the treatment for
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Invega Sustenna, Invega Trinza) Reference Number: CP.PHAR.291 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid See Important Reminder at the end of this policy
Clinical Policy: (Invega Sustenna, Invega Trinza) Reference Number: CP.PHAR.291 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid See Important Reminder at the end of this policy
Clinical Policy: Olanzapine Long-Acting Injection (Zyprexa Relprevv) Reference Number: CP.PHAR.292 Effective Date: Last Review Date: 08.
 Reference Number: CP.PHAR.292 Effective Date: Last Review Date: 08.") Clinical Policy: (Zyprexa Relprevv) Reference Number: CP.PHAR.292 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid See Important Reminder at the end of this policy for important
Clinical Policy: (Zyprexa Relprevv) Reference Number: CP.PHAR.292 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid See Important Reminder at the end of this policy for important
Chapter 17. Psychoses. Classifications of Psychoses. Schizophrenia. Factors Attributed to Development of Psychoses
 Chapter 17 Psychoses Drugs for Psychoses Delusions Hallucinations Illusions Paranoia Upper Saddle River, New Jersey 07458 All rights reserved. Classifications of Psychoses Acute episode Chronic episode
Chapter 17 Psychoses Drugs for Psychoses Delusions Hallucinations Illusions Paranoia Upper Saddle River, New Jersey 07458 All rights reserved. Classifications of Psychoses Acute episode Chronic episode
Guide to Psychiatric Medications for Children and Adolescents
 Guide to Psychiatric Medications for Children and Adolescents by Glenn S. Hirsch, M.D. The following guide includes most of the medications used to treat child and adolescent mental disorders. It lists
Guide to Psychiatric Medications for Children and Adolescents by Glenn S. Hirsch, M.D. The following guide includes most of the medications used to treat child and adolescent mental disorders. It lists
HOSPITAL BASED INPATIENT PSYCHIATRIC SERVICES (HBIPS) MEASURE SET
 MEASURE SET") HOSPITAL BASED INPATIENT PSYCHIATRIC SERVICES (HBIPS) MEASURE SET Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: February, 2013 Most recently revised: December 2018 The Psychiatric Measure Set CMS
HOSPITAL BASED INPATIENT PSYCHIATRIC SERVICES (HBIPS) MEASURE SET Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: February, 2013 Most recently revised: December 2018 The Psychiatric Measure Set CMS
Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD
 Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD Define BPSD and review the spectrum of associated symptoms Review pharmacologic and non-pharmacologic treatments for BPSD Evaluate
Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD Define BPSD and review the spectrum of associated symptoms Review pharmacologic and non-pharmacologic treatments for BPSD Evaluate
What Team Members Other Than Prescribers Need To Know About Antipsychotics
 What Team Members Other Than Prescribers Need To Know About Antipsychotics The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State
What Team Members Other Than Prescribers Need To Know About Antipsychotics The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State
Insomnia: Updates in Medical Management. Michael Newnam M.D.
 Insomnia: Updates in Medical Management Michael Newnam M.D. Sleep Neurobiology Delicate balance of excitatory and inhibitory neurotransmitters that control the switch between wakefulness and sleep Circadian
Insomnia: Updates in Medical Management Michael Newnam M.D. Sleep Neurobiology Delicate balance of excitatory and inhibitory neurotransmitters that control the switch between wakefulness and sleep Circadian
Friend or Foe? Review of the Regulations & Benefits: Risk Profiles of the Benzodiazepines
 Friend or Foe? Review of the Regulations & Benefits: Risk Profiles of the Benzodiazepines Program Learning Objectives At the conclusion of the activity, participants should be able to: Have a basic understanding
Friend or Foe? Review of the Regulations & Benefits: Risk Profiles of the Benzodiazepines Program Learning Objectives At the conclusion of the activity, participants should be able to: Have a basic understanding
Anxiolytic and Hypnotic drugs
 Anxiolytic and Hypnotic drugs Anxiolytic and Hypnotic drugs Anxiety is unpleasant state of tension and fear that seems to arise from unknown source. The symptoms of severe anxiety are similar to those
Anxiolytic and Hypnotic drugs Anxiolytic and Hypnotic drugs Anxiety is unpleasant state of tension and fear that seems to arise from unknown source. The symptoms of severe anxiety are similar to those
How did we get here? 1876 Methylene Blue. Insecticide 1935 Du Pont Anthelmintic. Garrett McCann, RPh
 Polypharmacy, Adverse Effects, and the Importance of Tapering Medications for People with Intellectual and Developmental Disabilities Garrett McCann, RPh How did we get here? 1876 Methylene Blue Insecticide
Polypharmacy, Adverse Effects, and the Importance of Tapering Medications for People with Intellectual and Developmental Disabilities Garrett McCann, RPh How did we get here? 1876 Methylene Blue Insecticide
Making Sense of the Long Term Care Mega Rule: Unnecessary Drugs & Psychotropics. Session Objectives. January 2018
 Making Sense of the Long Term Care Mega Rule: Unnecessary Drugs & Psychotropics Bridget McCrate Protus, PharmD, MLIS, BCGP, CDP Director of Drug Information Optum Hospice Pharmacy Services Session Objectives
Making Sense of the Long Term Care Mega Rule: Unnecessary Drugs & Psychotropics Bridget McCrate Protus, PharmD, MLIS, BCGP, CDP Director of Drug Information Optum Hospice Pharmacy Services Session Objectives
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Abilify Maintena, Aristada, Aristada Initio) Reference Number: CP.PHAR.290 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid Coding Implications Revision Log
Clinical Policy: (Abilify Maintena, Aristada, Aristada Initio) Reference Number: CP.PHAR.290 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid Coding Implications Revision Log
Chapter 161 Antipsychotics
 Chapter 161 Antipsychotics Episode Overview Extrapyramidal syndromes are a common complication of antipsychotic medications. First line treatment is benztropine or diphenhydramine. Lorazepam is used in
Chapter 161 Antipsychotics Episode Overview Extrapyramidal syndromes are a common complication of antipsychotic medications. First line treatment is benztropine or diphenhydramine. Lorazepam is used in
Delirium, Dementia, and Amnestic Disorders. Dr.Al-Azzam 1
 Delirium, Dementia, and Amnestic Disorders Dr.Al-Azzam 1 Introduction Disorders in which a clinically significant deficit in cognition or memory exists The number of people with these disorders is growing
Delirium, Dementia, and Amnestic Disorders Dr.Al-Azzam 1 Introduction Disorders in which a clinically significant deficit in cognition or memory exists The number of people with these disorders is growing
Treat mood, cognition, and behavioral disturbances associated with psychological disorders. Most are not used recreationally or abused
 Psychiatric Drugs Psychiatric Drugs Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally or abused Benzodiazepines
Psychiatric Drugs Psychiatric Drugs Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally or abused Benzodiazepines
Overview and Update on Current Psychopharmacological Medications, Including New Medications in Clinical Trials
 SPEAKER NOTES Overview and Update on Current Psychopharmacological Medications, Including New Medications in Clinical Trials Summarized by Thomas T. Thomas New psychotropic medications are coming on the
SPEAKER NOTES Overview and Update on Current Psychopharmacological Medications, Including New Medications in Clinical Trials Summarized by Thomas T. Thomas New psychotropic medications are coming on the
Review of Psychotrophic Medications. (An approved North Carolina Division of Health Services Regulation Continuing Education Course)
") Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
Safe and Effective Medication Approaches for Anxiety and Insomnia
 Safe and Effective Medication Approaches for Anxiety and Insomnia Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free monthly
Safe and Effective Medication Approaches for Anxiety and Insomnia Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free monthly
Psychotropic Medications Archana Jhawar, PharmD, BCPP Clinical Faculty of UIC Pharmacy Practice Clinical Psychiatric Pharmacist Jesse Brown VA
 Psychotropic Medications Archana Jhawar, PharmD, BCPP Clinical Faculty of UIC Pharmacy Practice Clinical Psychiatric Pharmacist Jesse Brown VA Goals of Medications Use least number at lowest dose to get
Psychotropic Medications Archana Jhawar, PharmD, BCPP Clinical Faculty of UIC Pharmacy Practice Clinical Psychiatric Pharmacist Jesse Brown VA Goals of Medications Use least number at lowest dose to get
PSYCHIATRIC DRUGS. Mr. D.Raju, M.pharm, Lecturer
 PSYCHIATRIC DRUGS Mr. D.Raju, M.pharm, Lecturer PSYCHIATRIC DRUGS Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally
PSYCHIATRIC DRUGS Mr. D.Raju, M.pharm, Lecturer PSYCHIATRIC DRUGS Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally
Antipsychotics and stroke risk
 Integrating Sentinel into Routine Regulatory Drug Review: A Snapshot of the First Year Antipsychotics and stroke risk Lockwood G. Taylor, PhD, MPH Division of Epidemiology II Office of Pharmacovigilance
Integrating Sentinel into Routine Regulatory Drug Review: A Snapshot of the First Year Antipsychotics and stroke risk Lockwood G. Taylor, PhD, MPH Division of Epidemiology II Office of Pharmacovigilance
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
11/1/2010. Psychology 472 Pharmacology of Psychoactive Drugs. Listen to the audio lecture while viewing these slides
 Treatment for Anxiety Disorders Benzodiazepines and Other Anxiolytics Psychology 472 Pharmacology of Psychoactive Drugs Listen to the audio lecture while viewing these slides Ethanol Barbiturates and related
Treatment for Anxiety Disorders Benzodiazepines and Other Anxiolytics Psychology 472 Pharmacology of Psychoactive Drugs Listen to the audio lecture while viewing these slides Ethanol Barbiturates and related
Management of Delirium in Hospice Patients
 Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Plante Moran Clinical Group
 Handouts Prepared By: Jane Belt, MS, RN, RAC-MT Plante Moran Clinical Group jane.belt@ 2 Plante Moran Clinical Group 2013 1 Objectives Delineate the key requirements in F329 Unnecessary Medications Describe
Handouts Prepared By: Jane Belt, MS, RN, RAC-MT Plante Moran Clinical Group jane.belt@ 2 Plante Moran Clinical Group 2013 1 Objectives Delineate the key requirements in F329 Unnecessary Medications Describe
Objectives. Epidemiology. Diagnosis 3/27/2013. Identify positive and negative symptoms used for diagnosis of schizophrenia
 Objectives Identify positive and negative symptoms used for diagnosis of schizophrenia Mohamed Sallout, Pharm D. Pharmacist Resident St. Luke s Magic Valley Regional Medical Center List medications used
Objectives Identify positive and negative symptoms used for diagnosis of schizophrenia Mohamed Sallout, Pharm D. Pharmacist Resident St. Luke s Magic Valley Regional Medical Center List medications used
Treat Schizophrenia Schizoaffective disorder Bipolar disorder Psychotic depression Off-label uses Insomnia Tics Delirium Stuttering
 Robert M. Millay RN MSN Ed Professor, Napa Valley College Psychiatric Technician Programs Copyright 2015, 2011, 2007, 2003, 1999, 1995, 1991 by Mosby, an imprint of Elsevier Inc. Treat Schizophrenia Schizoaffective
Robert M. Millay RN MSN Ed Professor, Napa Valley College Psychiatric Technician Programs Copyright 2015, 2011, 2007, 2003, 1999, 1995, 1991 by Mosby, an imprint of Elsevier Inc. Treat Schizophrenia Schizoaffective
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Antipsychotic Use in the Elderly
 Antipsychotic Use in the Elderly Presented by: Fatima M. Ali, PharmD, RPh, BCPS Clinical Consultant Pharmacist MediSystem Pharmacy, Kingston Originally Prepared by: Nicole Tisi BScPhm, RPh ACPR Disclosure
Antipsychotic Use in the Elderly Presented by: Fatima M. Ali, PharmD, RPh, BCPS Clinical Consultant Pharmacist MediSystem Pharmacy, Kingston Originally Prepared by: Nicole Tisi BScPhm, RPh ACPR Disclosure
Policy Evaluation: Low Dose Quetiapine Safety Edit
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University 500 Summer Street NE, E35, Salem, Oregon 97301 1079 Phone 503 947 5220 Fax 503
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University 500 Summer Street NE, E35, Salem, Oregon 97301 1079 Phone 503 947 5220 Fax 503
IMPORTANT NOTICE. Changes to dispensing of some Behavioral Health Medications for DC Healthcare Alliance members
 IMPORTANT NOTICE Changes to dispensing of some Behavioral Health Medications for DC Healthcare Alliance members These changes apply only to members covered under the DC Healthcare Alliance program Alliance
IMPORTANT NOTICE Changes to dispensing of some Behavioral Health Medications for DC Healthcare Alliance members These changes apply only to members covered under the DC Healthcare Alliance program Alliance
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults
 Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
A Brief Overview of Psychiatric Pharmacotherapy. Joel V. Oberstar, M.D. Chief Executive Officer
 A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
ANTIPSYCHOTICS AGENTS CONVENTIONAL
 ANTIPSYCHOTICS AGENTS CONVENTIONAL Documentation A. FDA approved indications 1. Psychotic Disorder (Haloperidol, Thiothixene) 2. Schizophrenia 3. Bipolar Disorder, Manic (Chlorpromazine) 4. Severe Behavioral
ANTIPSYCHOTICS AGENTS CONVENTIONAL Documentation A. FDA approved indications 1. Psychotic Disorder (Haloperidol, Thiothixene) 2. Schizophrenia 3. Bipolar Disorder, Manic (Chlorpromazine) 4. Severe Behavioral
Antipsychotics Prior Authorization Criteria for Louisiana Fee for Service and MCO Medicaid Recipients
 Antipsychotics Prior Authorization Criteria for Louisiana Fee for Service and MCO Medicaid Recipients Preferred Agents (Oral) a Amitriptyline/Perphenazine (Generic) Aripiprazole Tablet (Generic) b Chlorpromazine
Antipsychotics Prior Authorization Criteria for Louisiana Fee for Service and MCO Medicaid Recipients Preferred Agents (Oral) a Amitriptyline/Perphenazine (Generic) Aripiprazole Tablet (Generic) b Chlorpromazine
PROBLEM: PSYCHOSIS GOALS APPROACHES
 PROBLEM: PSYCHOSIS GOALS APPROACHES Behavior (only one is required to be monitored, per Title XXII): A. new admission: currently assessing for behaviors. 1. 2. Atypical psychosis Bipolar, mania Brief psychotic
PROBLEM: PSYCHOSIS GOALS APPROACHES Behavior (only one is required to be monitored, per Title XXII): A. new admission: currently assessing for behaviors. 1. 2. Atypical psychosis Bipolar, mania Brief psychotic
Kelly E. Williams, Pharm.D. PGY2 Psychiatric Pharmacy Resident April 16,2009
 Kelly E. Williams, Pharm.D. PGY2 Psychiatric Pharmacy Resident April 16,2009 List the antipsychotics most often prescribed Compare and contrast the use and adverse effects experienced in the pediatric
Kelly E. Williams, Pharm.D. PGY2 Psychiatric Pharmacy Resident April 16,2009 List the antipsychotics most often prescribed Compare and contrast the use and adverse effects experienced in the pediatric
Schizophrenia Pharmacology UNIVERSITY OF HAWAI I HILO PRE -NURSING PROGRAM
 Schizophrenia Pharmacology UNIVERSITY OF HAWAI I HILO PRE -NURSING PROGRAM NURS 203 GENERAL PHARMACOLOGY DANITA NARCISO PHARM D Learning Objectives Understand the result of dopamine binding to D2 receptors
Schizophrenia Pharmacology UNIVERSITY OF HAWAI I HILO PRE -NURSING PROGRAM NURS 203 GENERAL PHARMACOLOGY DANITA NARCISO PHARM D Learning Objectives Understand the result of dopamine binding to D2 receptors
APPENDIX E COMMONLY PRESCRIBED MEDICATIONS BY CATEGORY BY BRAND (GENERIC)
") APPENDIX E COMMONLY PRESCRIBED MEDICATIONS BY CATEGORY BY BRAND (GENERIC) Revised June 2005 Page E-1 Prescribed Medications by Category by Brand This is not an all-inclusive list ANTIPSYCHOTICS ANTIDEPRESSANTS
APPENDIX E COMMONLY PRESCRIBED MEDICATIONS BY CATEGORY BY BRAND (GENERIC) Revised June 2005 Page E-1 Prescribed Medications by Category by Brand This is not an all-inclusive list ANTIPSYCHOTICS ANTIDEPRESSANTS
ANTIPSYCHOTICS/ NEUROLEPTICS
 Pharmacological Interventions Tutorial Antipsychotic medications First Generation (Typicals) Includes phenothiazines, thioxanthenes, butyrophenones ANTIPSYCHOTICS/ NEUROLEPTICS Second Generation (Atypicals)
Pharmacological Interventions Tutorial Antipsychotic medications First Generation (Typicals) Includes phenothiazines, thioxanthenes, butyrophenones ANTIPSYCHOTICS/ NEUROLEPTICS Second Generation (Atypicals)
An algorithm for medication in the treatment of Complex PTSD
 An algorithm for medication in the treatment of Complex PTSD Andreas Laddis, M.D. aladdis@gmail.com ESTD Conference Bern November 10, 2017 The purpose for the presentation Algorithm for medication: My
An algorithm for medication in the treatment of Complex PTSD Andreas Laddis, M.D. aladdis@gmail.com ESTD Conference Bern November 10, 2017 The purpose for the presentation Algorithm for medication: My
Antipsychotics. Neuroleptics/ Major Tranquilizers. Hiwa K. Saaed, PhD Pharmacology & Toxicology /5/18 1
 Antipsychotics Neuroleptics/ Major Tranquilizers Hiwa K. Saaed, PhD Pharmacology & Toxicology hiwa.saaed@univsul.edu.iq 2018-2019 12/5/18 1 Learning objectives Pharmacy students should: be familiar with
Antipsychotics Neuroleptics/ Major Tranquilizers Hiwa K. Saaed, PhD Pharmacology & Toxicology hiwa.saaed@univsul.edu.iq 2018-2019 12/5/18 1 Learning objectives Pharmacy students should: be familiar with
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*
 DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*") COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
Richard Heidenfelder M.D. Child, Adolescent and Adult Psychiatry 447 9th Ave San Diego, CA
 *We are not accepting any New Patients who are currently taking any controlled pain medications *We are *Note: not completion accepting of the any following New Patients paperwork who and Initial are Screening
*We are not accepting any New Patients who are currently taking any controlled pain medications *We are *Note: not completion accepting of the any following New Patients paperwork who and Initial are Screening
PSYCHIATRY INTAKE FORM
 Please complete all information on this form. PSYCHIATRY INTAKE FORM Name Date Date of Birth Primary Care Physician Current Therapist/Counselor What are the problem(s) for which you are seeking help? 1.
Please complete all information on this form. PSYCHIATRY INTAKE FORM Name Date Date of Birth Primary Care Physician Current Therapist/Counselor What are the problem(s) for which you are seeking help? 1.
Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation. Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project
 Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project This project is funded through a grant from the Pew Charitable
Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project This project is funded through a grant from the Pew Charitable
2/12/2016. Drugs and Dementia in the Hospice Patient. Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources
 Drugs and Dementia in the Hospice Patient Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources 1 Drug Therapy: Targeted at Symptoms Cognitive: Impaired abstract thinking Impaired
Drugs and Dementia in the Hospice Patient Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources 1 Drug Therapy: Targeted at Symptoms Cognitive: Impaired abstract thinking Impaired
#55 PRESCRIBING AND MONITORING PSYCHI RIC MEDICATIONS
 - '_ ADMINISTRA TIVE/FISCAUCLINICAL/PHF POLICY AND PROCEDURES COUNTY OF SANTA BARBARA ALCOHOL, DRUG AND MENTAL HEAL TH SERVICES Section - QUALITY ASSURANCE Effective: 12/1/09 Policy- Director's Approval
- '_ ADMINISTRA TIVE/FISCAUCLINICAL/PHF POLICY AND PROCEDURES COUNTY OF SANTA BARBARA ALCOHOL, DRUG AND MENTAL HEAL TH SERVICES Section - QUALITY ASSURANCE Effective: 12/1/09 Policy- Director's Approval
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Soma (carisoprodol), Soma Compound (carisoprodol and aspirin), Soma Compound w/ Codeine (carisoprodol and aspirin and codeine)
, Soma Compound (carisoprodol and aspirin), Soma Compound w/ Codeine (carisoprodol and aspirin and codeine)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.75.07 Subject: Soma Page: 1 of 7 Last Review Date: September 15, 2017 Soma Description Soma (carisoprodol),
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.75.07 Subject: Soma Page: 1 of 7 Last Review Date: September 15, 2017 Soma Description Soma (carisoprodol),
NorthSTAR. Pharmacy Manual
 NorthSTAR Pharmacy Manual Revised October, 2008 Table of I. Introduction II. III. IV. Antidepressants New Generation Antipsychotic Medications Mood Stabilizers V. ADHD Medications VI. Anxiolytics and Sedative-Hypnotics
NorthSTAR Pharmacy Manual Revised October, 2008 Table of I. Introduction II. III. IV. Antidepressants New Generation Antipsychotic Medications Mood Stabilizers V. ADHD Medications VI. Anxiolytics and Sedative-Hypnotics
Soma (carisoprodol), Soma Compound (carisoprodol and aspirin), Soma Compound w/ Codeine (carisoprodol and aspirin and codeine)
, Soma Compound (carisoprodol and aspirin), Soma Compound w/ Codeine (carisoprodol and aspirin and codeine)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.75.07 Subject: Page: 1 of 7 Last Review Date: September 15, 2016 Description (carisoprodol), Compound
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.75.07 Subject: Page: 1 of 7 Last Review Date: September 15, 2016 Description (carisoprodol), Compound
Judges Reference Table for the March 2016 Psychotropic Medication Utilization Parameters for Foster Children
 Judges Reference Table for the Psychotropic Medication Utilization Parameters for Foster Children Stimulants for treatment of ADHD Preschool (Ages 3-5 years) Child (Ages 6-12 years) Adolescent (Ages 13-17
Judges Reference Table for the Psychotropic Medication Utilization Parameters for Foster Children Stimulants for treatment of ADHD Preschool (Ages 3-5 years) Child (Ages 6-12 years) Adolescent (Ages 13-17
Dosing & Administration
 Dosing & Administration REAL LIFE. REAL RESULTS. INDICATION INVEGA SUSTENNA (paliperidone palmitate) is indicated for the treatment of: Schizophrenia. Schizoaffective disorder as monotherapy and as an
Dosing & Administration REAL LIFE. REAL RESULTS. INDICATION INVEGA SUSTENNA (paliperidone palmitate) is indicated for the treatment of: Schizophrenia. Schizoaffective disorder as monotherapy and as an
Using Benzodiazepines in Primary Care
 Using Benzodiazepines in Primary Care Spencer A. Tighe MD, FRCPC Saturday, Feb. 16, 2008 Overview Historical context Drug information Indications Side effects Abuse vs. physical dependence Clinical practice
Using Benzodiazepines in Primary Care Spencer A. Tighe MD, FRCPC Saturday, Feb. 16, 2008 Overview Historical context Drug information Indications Side effects Abuse vs. physical dependence Clinical practice
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Schizophrenia and Related Psychotic Disorders
 and Related Psychotic Disorders Anand K. Pandurangi, MD Professor & Chair, Div. of Inpatient Psychiatry Director, Program VCU Medical Center 1 Kraeplin 1896 Dementia Praecox. Single, Homogenous Disorder
and Related Psychotic Disorders Anand K. Pandurangi, MD Professor & Chair, Div. of Inpatient Psychiatry Director, Program VCU Medical Center 1 Kraeplin 1896 Dementia Praecox. Single, Homogenous Disorder
COMBATTING THE EXCESSIVE AND ILLEGAL USE OF PSYCHOTROPIC DRUGS ON PEOPLE WITH DEMENTIA IN NURSING FACILITIES
 COMBATTING THE EXCESSIVE AND ILLEGAL USE OF PSYCHOTROPIC DRUGS ON PEOPLE WITH DEMENTIA IN NURSING FACILITIES Kelly Bagby and Iris Gonzalez kbagby@aarp.org (202) 434-2103 igonzalez@aarp.org (202) 434-6289
COMBATTING THE EXCESSIVE AND ILLEGAL USE OF PSYCHOTROPIC DRUGS ON PEOPLE WITH DEMENTIA IN NURSING FACILITIES Kelly Bagby and Iris Gonzalez kbagby@aarp.org (202) 434-2103 igonzalez@aarp.org (202) 434-6289
Antidepressants. Dr Malek Zihlif
 Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
Participating Hospital Certification Form
 Participating Hospital Certification Form ATTENTION: this Certification Form is only applicable for Free Trial Product Units of ABILIFY MAINTENA (aripiprazole). Instructions: The Authorized Representative
Participating Hospital Certification Form ATTENTION: this Certification Form is only applicable for Free Trial Product Units of ABILIFY MAINTENA (aripiprazole). Instructions: The Authorized Representative
Seniors Health Strategic Clinical Network Restraint as a Last Resort
 Seniors Health Strategic Clinical Network Restraint as a Last Resort Elder Friendly Care 2018 Alberta Health Services, Seniors Health Strategic Clinical Network Disclaimer, Copyright and Creative Commons
Seniors Health Strategic Clinical Network Restraint as a Last Resort Elder Friendly Care 2018 Alberta Health Services, Seniors Health Strategic Clinical Network Disclaimer, Copyright and Creative Commons
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Pharmacy Medical Necessity Guidelines: Antipsychotic Medications
 Pharmacy Medical Necessity Guidelines: Antipsychotic Medications Effective: July. 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy
Pharmacy Medical Necessity Guidelines: Antipsychotic Medications Effective: July. 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy
Ativan and geodon compatibility
 P ford residence southampton, ny Ativan and geodon compatibility In this case, a patient developed severe hypotension (66/30 mm Hg) after receiving intramuscular olanzapine and intramuscular lorazepam
P ford residence southampton, ny Ativan and geodon compatibility In this case, a patient developed severe hypotension (66/30 mm Hg) after receiving intramuscular olanzapine and intramuscular lorazepam
Antipsychotic use in Dementia care. Jabbar Fazeli, MD
 Antipsychotic use in Dementia care Jabbar Fazeli, MD www.mainegeriatrics.com What changed in 2012? NY times- May 9, 2011!! Antipsychotic Drugs Called Hazardous for the Elderly - referencing the OIG audit
Antipsychotic use in Dementia care Jabbar Fazeli, MD www.mainegeriatrics.com What changed in 2012? NY times- May 9, 2011!! Antipsychotic Drugs Called Hazardous for the Elderly - referencing the OIG audit
Switching antipsychotics: Basing practice on pharmacology & pharmacokinetics
 Switching antipsychotics: Basing practice on pharmacology & pharmacokinetics John Donoghue Liverpool L imagination est plus important que le savoir Albert Einstein Switching Antipsychotics: Objectives
Switching antipsychotics: Basing practice on pharmacology & pharmacokinetics John Donoghue Liverpool L imagination est plus important que le savoir Albert Einstein Switching Antipsychotics: Objectives
Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia
 Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia Tiffany D. Long, MS4 UNC School of Medicine MD Candidate Class of 2018 Disclaimers A portion of this project is/was supported
Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia Tiffany D. Long, MS4 UNC School of Medicine MD Candidate Class of 2018 Disclaimers A portion of this project is/was supported
Study Guidelines for Quiz #1
 Annex to Section J Page 1 Study Guidelines for Quiz #1 Theory and Principles of Psychopharmacology, Classifications and Neurotransmitters, Anxiolytics/Antianxiety/Minor Tranquilizers, Stimulants, Nursing
Annex to Section J Page 1 Study Guidelines for Quiz #1 Theory and Principles of Psychopharmacology, Classifications and Neurotransmitters, Anxiolytics/Antianxiety/Minor Tranquilizers, Stimulants, Nursing
First-Generation Versus Second-Generation Antipsychotics in Adults: Comparative Effectiveness
 1 First-Generation Versus Second-Generation Antipsychotics in Adults: Comparative Effectiveness This continuing education monograph examines the results of a comparative effectiveness review to compare
1 First-Generation Versus Second-Generation Antipsychotics in Adults: Comparative Effectiveness This continuing education monograph examines the results of a comparative effectiveness review to compare
Pharmacological Help for a Good Night s s Sleep. Thomas Owens, MD
 Pharmacological Help for a Good Night s s Sleep Thomas Owens, MD Objectives 1. Define insomnia and characterize the symptoms and array of causes. 2. Describe traditional and new pharmacologic approaches
Pharmacological Help for a Good Night s s Sleep Thomas Owens, MD Objectives 1. Define insomnia and characterize the symptoms and array of causes. 2. Describe traditional and new pharmacologic approaches
Antipsychotics Detect, Select, Effect (P.I.E.C.E.S. 6 th Ed)
") Antipsychotics Detect, Select, Effect (P.I.E.C.E.S. 6 th Ed) CLeAR Webinar February 14, 2014 Paula Diaz (Pharm) Carol Ward MD Carol Ward Tertiary Mental Health IHA Hillside Centre (Acute Tertiary Mental
Antipsychotics Detect, Select, Effect (P.I.E.C.E.S. 6 th Ed) CLeAR Webinar February 14, 2014 Paula Diaz (Pharm) Carol Ward MD Carol Ward Tertiary Mental Health IHA Hillside Centre (Acute Tertiary Mental
Psychosis and Agitation in Dementia
 Psychosis and Agitation in Dementia Dilip V. Jeste, MD Estelle & Edgar Levi Chair in Aging, Director, Stein Institute for Research on Aging, Distinguished Professor of Psychiatry & Neurosciences, University
Psychosis and Agitation in Dementia Dilip V. Jeste, MD Estelle & Edgar Levi Chair in Aging, Director, Stein Institute for Research on Aging, Distinguished Professor of Psychiatry & Neurosciences, University
Nursing Process Focus: Patients Receiving Chlorpromazine (Thorazine)
") Nursing Process Focus: Patients Receiving Chlorpromazine (Thorazine) Potential Nursing Diagnoses Ineffective Therapeutic Regimen Management Risk for Activity Intolerance, related to side effect of drug
Nursing Process Focus: Patients Receiving Chlorpromazine (Thorazine) Potential Nursing Diagnoses Ineffective Therapeutic Regimen Management Risk for Activity Intolerance, related to side effect of drug
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Treatment of Schizophrenia
 Treatment of Schizophrenia Conduct comprehensive assessment and use measurement-based care as found in the Principles of Practice (review pages 4-7). Most importantly assess social support system (housing,
Treatment of Schizophrenia Conduct comprehensive assessment and use measurement-based care as found in the Principles of Practice (review pages 4-7). Most importantly assess social support system (housing,
Medication Audit Checklist- Antipsychotics - Atypical
 Medication Audit checklist Page 1 of 7 10-2018 Audit number: Client number: Ordering Provider: INDICATIONS 1) Disorders with psychotic symptoms (schizophrenia, schizoaffective disorder, manic disorders,
Medication Audit checklist Page 1 of 7 10-2018 Audit number: Client number: Ordering Provider: INDICATIONS 1) Disorders with psychotic symptoms (schizophrenia, schizoaffective disorder, manic disorders,
MEDICATION ALGORITHM FOR ANXIETY DISORDERS
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Antipsychotic Medications Age and Step Therapy
 Market DC *- Florida Healthy Kids Antipsychotic Medications Age and Step Therapy Override(s) Approval Duration Prior Authorization 1 year Quantity Limit *Virginia Medicaid See State Specific Mandates *Indiana
Market DC *- Florida Healthy Kids Antipsychotic Medications Age and Step Therapy Override(s) Approval Duration Prior Authorization 1 year Quantity Limit *Virginia Medicaid See State Specific Mandates *Indiana
Medication Treatment of Cognitive and Behavioral Symptoms in Dementia
 Medication Treatment of Cognitive and Behavioral Symptoms in Dementia Cary J. Kohlenberg, M.D. Medical Director, IPC Research and Independent Psychiatric Consultants Environmental interventions directly
Medication Treatment of Cognitive and Behavioral Symptoms in Dementia Cary J. Kohlenberg, M.D. Medical Director, IPC Research and Independent Psychiatric Consultants Environmental interventions directly
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Vraylar) Reference Number: CP.PMN.91 Effective Date: 11.16.16 Last Review Date: 02.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Vraylar) Reference Number: CP.PMN.91 Effective Date: 11.16.16 Last Review Date: 02.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy