Workshop II. How to manage highly active MS patients in practice?
|
|
|
- Bernard Abel Casey
- 5 years ago
- Views:
Transcription

1 Workshop II How to manage highly active MS patients in practice?
2 Gavin Giovannoni Department of Neurology Institute of Cell and Molecular Science Queen Mary University London & Barts and The London NHS Trust London, UK Declared receipt of compensation for participating on Advisory Boards in relation to clinical trial design, trial steering committees and data and safety monitoring committees from: Abbvie, Bayer-Schering Healthcare, Biogen-Idec, Eisai, Elan, Fiveprime, Genzyme, Genentech, GSK, GW Pharma, Ironwood, Merck, Novartis, Pfizer, Roche, Sanofi- Aventis, Synthon BV, Teva, UCB Pharma and Vertex Pharmaceuticals
3 Workshop II How to manage highly active MS patients in practice? Gavin Giovannoni Barts-MS Barts and The London School of Medicine and Dentistry Queen Mary University London
4 Learning objectives Describe the mechanisms of action of induction treatments Define the long-term benefit of induction based on the evidence currently available
5 Important questions for patients to consider before starting a DMT 1. What is MS? 2. Are you sure that you have MS? 3. What type of MS do you have? 4. What prognostic group do you fall into? 5. What is the risk of you not being treated with a DMT? 6. Do you have active MS? 7. Are you eligible for treatment with a DMT? 8. Do you understand the difference between the treatment strategies of maintenanceand-escalation and induction therapy? 9. Do you understand the concepts of treat-2-target or no evident disease activity (NEDA)? 10.What about pregnancy? 6 DMT, disease-modifying therapy; MS, multiple sclerosis
6 What prognostic group do you fall into? Good prognosis Young Female sex Unifocal onset Isolated sensory symptom (optic neuritis, sensory) Full recovery from attack Long interval to second relapse No disability after 5 years Normal MRI/low lesion load No Gd-enhancing, posterior fossa and spinal cord lesions No baseline brain atrophy Biomarkers ( ve OCBs, normal CSF neurofilament levels, high vd3 levels) CSF, cerebrospinal fluid; MRI, magnetic resonance imaging; OCB, oligoclonal band Poor prognosis Older age of onset Male sex Multifocal onset Efferent system affected (motor, cerebellar, bladder) Partial or no recovery from a relapse High relapse rate in first 2 years Disability after 5 years Abnormal MRI with large lesion load Gd-enhancing, posterior fossa and spinal cord lesions Baseline brain atrophy Biomarkers (OCBs, raised CSF neurofilament levels, low vd3 levels) Adapted from Miller DH, et al. Lancet Neurology 2005:4;281 8
7 What is active MS? Inactive MS: no relapses or MRI activity in the last 24 months 2001 Clinical Active MS: relapses in the last 12 or 24 months and/or MRI activity in the last 12 months 2009 Clinical and MRI 2014 Clinical or MRI



8 Am I eligible for treatment? Inactive MS: no relapses or MRI activity in the last 24 months 2001 Clinical Active MS: relapses in the last 12 or 24 months and/or MRI activity in the last 12 months Highly active MS: relapses in the last 12 months and MRI activity in the last 12 months Rapidly-evolving severe MS (RES); two disabling attacks in a 12-month period and MRI evidence of activity during this period 2009 Clinical and MRI Natalizumab Fingolimod Treatment No treatment 2014 Clinical or MRI

; two disabling attacks in a 12 month period and MRI evidence of activity during this period.")
9 Aim of treatment Inactive MS: no relapses or MRI activity in the last 24 months (NEDA) 2001 Clinical 2009 Clinical and MRI Active MS: relapses in the last 12 or 24 months and/or MRI activity in the last 12 months Highly active MS: relapses in the last 12 months and MRI activity in the last 12 months Rapidly-evolving severe MS (RES); two disabling attacks in a 12 month period and MRI evidence of activity during this period Clinical or MRI
10 Do you understand the difference between maintenance escalation and a pulsed immune reconstitution therapy (PIRT)? 3rd-line X 3rd-line y 1 st -line A 1st-line E 1 st -line B 1st-line D 2nd-line M 2nd-line N 1 st -line C
11 BARTS-MS T2T-NEDA algorithm Define the individual s MS Choose a therapeutic strategy Personalization: MS prognosis based on clinical and MRI indices Lifestyle and goals Shared goals for therapy Patient s preferences? Your choice? Only one licensed induction therapy at present Yes Maintenance-escalation Choose therapy A B C Initiate or Switch or Escalate Rx Rebaseline Monitoring Treatment failure? No Pulsed immune reconstitution therapy Choose therapy X Z Y Complete course / Re-treat Rebaseline Monitoring Yes Breakthrough disease Rebaselining: IFNβ, natalizumab, fingolimod, teriflunomide, Dimethyl fumarate, 3 6 months Glatiramer acetate, 9 months Alemtuzumab, 24 months Individual measures: Evidence of disease activity? Tolerability/safety? Adherence? Drug or inhibitory markers, e.g. NAbs? T2T, treat-to-target; IFNβ, interferon-beta; NAbs, neutralizing antibodies; Rx, treatment
12 Rebooting or reconstituting the immune system Genes Environment Multiple Sclerosis
13 What is PIRT? Pulsed immune reconstitution therapy (PIRT) is by definition given as a short course, i.e. intermittently and not continuously PIRT has the ability to induce long-term remission and in some cases the possibility of a cure Please note that a PIRT is not given continuously Additional courses of the therapy are only given if there is a recurrence of inflammatory activity* *Inflammatory activity in MS typically refers to clinical relapses and/or focal MRI activity (new T2 lesions and/or Gd-enhancing lesions) GD, gadolinium
14 What is maintenance therapy? Maintenance therapy is by definition given continuously, without an interruption in dosing Although it has the ability to induce long-term remission it cannot result in a cure Please note that maintenance therapy is given continuously A recurrence of, or ongoing, inflammatory activity* while on therapy is an indication of suboptimal response *Inflammatory activity in MS typically refers to clinical relapses and/or focal MRI activity (new T2 lesions and/or Gd-enhancing lesions)
15 Maintenance therapy vs PIRT Maintenance therapy Continuous treatment Low to very high efficacy Reversible Perceived to be lower risk Cumulative, or increased, risk with time Examples Laquinimod, GA, IFNβ, teriflunomide, BG12, fingolimod, natalizumab, daclizumab Breakthrough disease Suboptimal or failure to respond NEDA reliable metric for efficacy Rebound activity Highly likely Can be life-threatening Pregnancy No potential for a cure Rebound SPMS and progressive brain atrophy PIRT Short-courses or pulsed therapy High to very high efficacy Irreversible Perceived to be higher risk Frontloading of risk or reduced risk with time Examples Mitoxantrone, cladribine, alemtuzumab, anti-cd20 (?), HSCT-BMT Breakthrough disease Marker for retreatment NEDA unreliable to assess efficacy Rebound activity Less likely Unlikely to be life-threatening Pregnancy Potentially curative? year experiment The following may not be licensed for MS in your country: laquinimod, daclizumab, mitoxantrone, cladribine, anti-cd20 therapies, BMT. GA, glatiramer acetate; HSCT-BMT, hematopoietic stem cell transplantation bone marrow transplantation; IFNβ, interferon beta; SPMS, secondary progressive multiple sclerosis
16 Can we define a cure for MS? Survival analysis pulsed immune reconstitution therapy or PIRT No secondary progression MS is an autoimmune disease hypothesis REMISSION CURE Environ -ment Genes year experiment Multiple Sclerosis
17 Case study 1
18 25-year-old woman with RRMS 2011 Optic neuritis MRI+ve Patient case scenario provided by Professor Gavin Giovannoni
19 25-year-old woman with RRMS 2011 April 2015 May 2015 Optic neuritis MRI+ve Brain stem INO Spinal cord triparesis IV methylprednisolone IV methylprednisolone EDSS = 5.0 EDSS, Expanded Disability Status Scale; INO, internuclear ophthalmoplegia; IV, intravenous Patient case scenario provided by Professor Gavin Giovannoni
20 25-year-old woman with RRMS 2011 April 2015 May 2015 Optic neuritis MRI+ve Brain stem INO Spinal cord triparesis IV methylprednisolone IV methylprednisolone EDSS = 5.0 Natalizumab or Alemtuzumab? EDSS, Expanded Disability Status Scale; INO, internuclear ophthalmoplegia; IV, intravenous Patient case scenario provided by Professor Gavin Giovannoni
21 25-year-old woman with RRMS 2011 April 2015 May 2015 June 2015 Optic neuritis MRI+ve Brain stem INO Spinal cord triparesis JCV+ve (index = 1.6) IV methylprednisolone IV methylprednisolone EDSS = 5.0 Natalizumab or Alemtuzumab? EDSS, Expanded Disability Status Scale; INO, internuclear ophthalmoplegia; IV, intravenous; JCV, JC virus Patient case scenario provided by Professor Gavin Giovannoni

22 25-year-old woman with RRMS What would you do? Patient case scenario provided by Professor Gavin Giovannoni
23 25-year-old woman with RRMS 2011 April 2015 May 2015 June 2015 Sept 2015 Optic neuritis MRI+ve Brain stem INO IV methylprednisolone Spinal cord triparesis IV methylprednisolone JCV+ve (index = 1.6) Severe spinal cord relapse, paraparesis, loss B&B, pressure sore Anti-AQ4 ve IV methylprednisolone IV methylprednisolone 2 EDSS = 5.0 EDSS = Natalizumab or Alemtuzumab? Natalizumab or Alemtuzumab? Pressure sore Urinary catheter AQ4, Aquaporin-4; RRMS, relapsing-remitting multiple sclerosis Patient case scenario provided by Professor Gavin Giovannoni Haines JD, et al. Mt Sinai J Med 2011;78:231 43; Münzel EJ, et al. Drugs 2013;73:
24 25-year-old woman with RRMS 2011 April 2015 May 2015 June 2015 Sept 2015 Optic neuritis MRI+ve Brain stem INO IV methylprednisolone Spinal cord triparesis IV methylprednisolone JCV+ve (index = 1.6) Severe spinal cord relapse, paraparesis, loss B&B, pressure sore Anti-AQ4 ve IV methylprednisolone IV methylprednisolone 2 EDSS = 5.0 EDSS = Natalizumab or Alemtuzumab? Natalizumab or Alemtuzumab? Natalizumab Patient case scenario provided by Professor Gavin Giovannoni Haines JD, et al. Mt Sinai J Med 2011;78:231 43; Münzel EJ, et al. Drugs 2013;73:
25 Switching from natalizumab to alemtuzumab Option 1: Immediate switch (high risk if carry-over PML develops) Natalizumab Asymptomatic PML? LP-JCV DNA & MRI Alemtuzumab Option 2: Washout (intermediate risk; mainly related to rebound of MS disease activity) Natalizumab Asymptomatic PML?* LP-JCV DNA & MRI 3 6 MONTH WASHOUT * For this option the shorter the washout the more important the screen for asymptomatic PML ** PML screening and baseline MRI studies use different scans, hence the need for both Rebaseline MRI** Alemtuzumab Option 3: Bridging (low risk; mainly related to using a low efficacy bridging agent and using alemtuzumab after the bridging agent) Natalizumab Asymptomatic PML? LP-JCV DNA & MRI 6 12 MONTHS Oral bridging agent (Teriflunomide, DMF or Fingolimod) Rebaseline MRI Alemtuzumab DMF, dimethyl fumarate; LP, lumbar puncture; PML, progressive multifocal leukoencephalopathy
26 25-year-old woman with RRMS 2011 April 2015 May 2015 June 2015 Sept 2015 Optic neuritis MRI+ve Brain stem INO IV methylprednisolone Spinal cord triparesis IV methylprednisolone JCV+ve (index = 1.6) Severe spinal cord relapse, paraparesis, loss B&B, pressure sore Anti-AQ4 ve IV methylprednisolone IV methylprednisolone 2 EDSS = 5.0 EDSS = Natalizumab or Alemtuzumab? Natalizumab or Alemtuzumab? Natalizumab Feb 2016 Alemtuzumab EDSS = 6.0 Patient case scenario provided by Professor Gavin Giovannoni Haines JD, et al. Mt Sinai J Med 2011;78:231 43; Münzel EJ, et al. Drugs 2013;73:
27 Case study 2
28 38-year-old woman with RRMS Teacher
29 38-year-old woman with RRMS Glatiramer acetate 3 years (good adherence) Relapse with a mild left sensory loss Referred to me for a second opinion Teacher
30 38-year-old woman with RRMS Switched to interferon-beta (IM IFNbeta-1a; Mild persistent flu-like side-effects and lymphopenia 12/12 NAb screen negative Volunteers for new research programme, which included an MRI protocol Teacher IM, intramuscular
31 38-year-old woman with RRMS Forced to retire due to cognitive impairment and severe fatigue Developed depression and anxiety She becomes an expert patient Widely read Internet savvy Regular follower of Teacher
32 Unemployment Kobelt, et al. J Neurol Neurosurg Psychiatry 2006;77:918 26
33 38-year-old woman with RRMS
34 38-year-old woman with RRMS Teacher?



35 38-year-old woman with RRMS

36 38-year-old woman with RRMS Teacher What would you do if this was you? Would you risk the wrath of the NICE inspectors? NICE, National Institute for Health and Care Excellence
37 38-year-old woman with RRMS Teacher Natalizumab vs Fingolimod
38 Bermel RA, et al. Ann Neurol 2013;73:95 103
39 Predictors of long-term outcome in MSers treated with interferon beta-1a Treatment vs Natural history OR, odds ratio Bermel RA, et al. Ann Neurol 2013;73:95 103
40 Case study 3
41 EDSS 17-year-old girl, presents with myelitis Jun 2000 Myelitis Feb st -year university L-optic neuritis IFN-beta Jun 2000 IFN-beta
42 EDSS 17-year-old girl, presents with myelitis Jun 2000 Feb 2001 Myelitis 1 st -year university L-optic neuritis IFN-beta Jan 2002 Oct 2003 Clumsy left hand Pins & needles in legs Mar 2004 R-optic neuritis Dec 2007 Brainstem syndrome; diplopia and ataxia How are you going to manage her? Jun 2000 IFN-beta
43 EDSS 17-year-old girl, presents with myelitis Jun 2000 Feb 2001 Myelitis 1 st -year university L-optic neuritis IFN-beta Jan 2002 Oct 2003 Clumsy left hand Pins & needles in legs Mar 2004 R-optic neuritis Dec 2007 Brainstem syndrome; diplopia and ataxia Jan 2008 Cervical cord relapse weak L arm with pain 6.0 Jun 2000 IFN-beta
 Mild urinary frequency No depression, anxiety, fatigue IFN-beta Dec 2007 Brainstem syndrome;")
44 EDSS 17-year-old girl, presents with myelitis Jun 2000 Feb 2001 Myelitis 1 st -year university L-optic neuritis Jan 2002 Oct 2003 Clumsy left hand Pins & needles in legs Mar 2004 R-optic neuritis Feb 2008 to May 2014 Bladder dysfunction Depression, anxiety, fatigue NEDA (no evident disease activity) Mild urinary frequency No depression, anxiety, fatigue IFN-beta Dec 2007 Brainstem syndrome; diplopia and ataxia Jan 2008 Cervical cord relapse weak L arm with pain Reduced mobility Jan 2008 Natalizumab Fully mobile Residual deficits: Walking distance >500m Unable to run Exercise induces intermittent sensory symptoms in L arm Mild urinary frequency 6.0 Jun 2000 IFN-beta Natalizumab May 2014


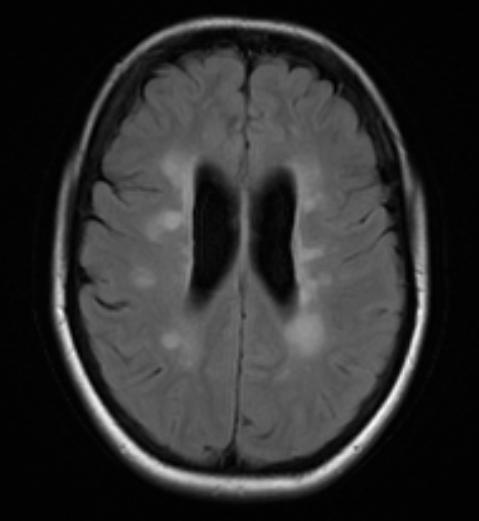
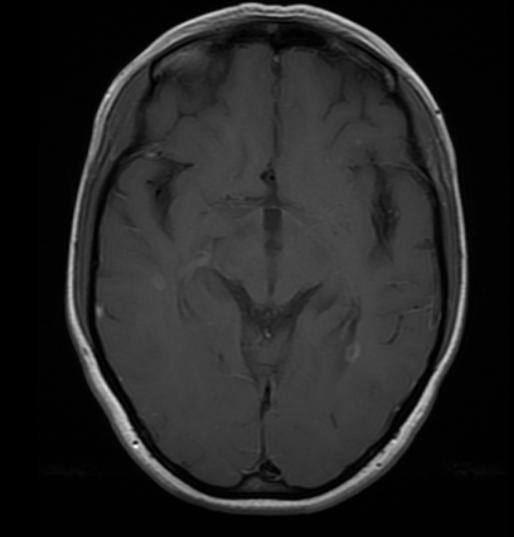
45 MRI progressive brain atrophy MRI progressive brain atrophy Dec 2007 Jul 2010 Jul 2013 Is this patient in long-term remission?
46 EDSS 17-year-old girl, presents with myelitis Jun 2000 Feb 2001 Myelitis 1 st -year university L-optic neuritis Jan 2002 Oct 2003 Clumsy left hand Pins & needles in legs Mar 2004 R-optic neuritis Feb 2008 to May 2014 Bladder dysfunction Depression, anxiety, fatigue NEDA (no evident disease activity) Mild urinary frequency No depression, anxiety, fatigue IFN-beta Dec 2007 Brainstem syndrome; diplopia and ataxia Jan 2008 Cervical cord relapse weak L arm with pain Reduced mobility Jan 2008 Natalizumab Fully mobile Residual deficits: Walking distance >500m Unable to run Exercise induces intermittent sensory symptoms in L arm Mild urinary frequency JCV positive - index Jun 2000 IFN-beta Natalizumab May 2014
47 Switching from natalizumab to alemtuzumab Option 1: Immediate switch (high risk if carry-over PML develops) Natalizumab Asymptomatic PML? LP-JCV DNA & MRI Alemtuzumab Option 2: Washout (intermediate risk; mainly related to rebound of MS disease activity) Natalizumab Asymptomatic PML?* LP-JCV DNA & MRI 3 6 MONTH WASHOUT * For this option the shorter the washout the more important the screen for asymptomatic PML ** PML screening and baseline MRI studies use different scans, hence the need for both Rebaseline MRI** Alemtuzumab Option 3: Bridging (low risk; mainly related to using a low efficacy bridging agent and using alemtuzumab after the bridging agent) Natalizumab Asymptomatic PML? LP-JCV DNA & MRI 6 12 MONTHS Oral bridging agent (Teriflunomide, DMF or Fingolimod) Rebaseline MRI Alemtuzumab Giovannoni et al. Pract Neurol Oct;16(5):




48 EDSS 17-year-old girl, presents with myelitis Jun-2000 Feb yr girl, myelitis 1 st -yr University L-optic neuritis Jan Clumsy left hand Oct-2003 Pins & needles in legs Feb-2008 to May-2014 NEDA (no evident disease activity) Bladder dysfunction Mild urinary frequency Feb-2001 IFN-beta Mar-2004 R-optic neuritis depression, anxiety and fatigue No depression,anxiety or fatigue Dec 2007 Brainstem syndrome; diplopia and ataxia Reduced mobility Fully mobile Jan 2008 Cervical cord relapse weak L arm with pain Jan-2008 Natalizumab Residual deficits: Walking distance >500m Unable to run Exercise induces intermittent sensory symptoms in L arm Mild urinary frequency 6.0 Jun-2000 IFN-beta Natalizumab May-2014
49 Switching from natalizumab to alemtuzumab Option 1: Immediate switch (high-risk if persistent lymphopenia occurs) Fingolimod Treat with alemtuzumab before lymphocyte counts normalize Alemtuzumab Option 2: Washout (intermediate risk; mainly related to rebound of MS disease activity) Fingolimod Only treat with alemtuzumab once lymphocyte counts normalize* 2 to 6 12 MONTH WASHOUT Alemtuzumab * What constitutes a normal level post-fingolimod needs to be defined; I would be reluctant to give alemtuzumab to anyone with a total lymphocyte count below Option 3: Bridging (low risk; mainly related to MS rebound as a result of using a low efficacy bridging agent after fingolimod) Fingolimod 3-12 MONTHS Bridging agent (IFN-beta, GA, teriflunomide or DMF) Only treat with alemtuzumab once lymphocyte counts normalize* * What constitutes a normal level in this situation needs to be defined; I would be reluctant to give alemtuzumab to anyone with a total lymphocyte count below Alemtuzumab Giovannoni et al. Pract Neurol Oct;16(5):

50 BartsMS blog
51 Natalizumab Continuous treatment (monthly infusions) Very high efficacy; high NEDA rates, significant proportion of subjects improve Prevents end-organ damage (reduced brain atrophy at year 2) Reversible treatment effect Infusion reactions uncommon No short-term generalized immunosuppression Reduced immune surveillance increases risk of CNS infections; in particular PML if JCV-seropositive Breakthrough disease Re-baseline at 3 6 months Neutralizing antibodies to natalizumab reduce efficacy and cause infusion reactions Suboptimal or failure to respond NEDA reliable metric for efficacy Rebound activity Pregnancy Highly likely, can be life threatening Not recommended, natalizumab crosses placenta and has transient effects in baby No secondary autoimmunity No obvious secondary malignancy risk Monitoring: yes, blood and liver function tests early on, anti-natalizumab antibodies, JCV serology and annual MRI No potential for a cure Rebound Alemtuzumab Short-course pulsed therapy (2 5 annual cycles of treatment) Very high efficacy; significant proportion of subjects improve Reported NEDA rates low, but not measured in correct epoch Prevents end-organ damage (reduced brain atrophy at year 2) Irreversible treatment effect Infusion reactions the norm Short-term generalised immunosuppression (8 12 weeks post infusion) Low risk of CNS and other infections after immune system reconstitution Breakthrough disease Re-baseline at 24 months Antibodies to alemtuzumab are transient and don t appear to inhibit activity of drug Marker for retreatment NEDA unreliable to assess efficacy Rebound activity Less likely, unlikely to be life-threatening Pregnancy Fine once immune system reconstituted Potential for autoantibodies to cross placenta, for example neonatal hyperthyroidism Secondary autoimmunity; ~50% of patients with long-term follow-up mainly thyroid related Potential, but undefined, secondary malignancy risk Monitoring: yes, monthly blood and urine tests for secondary autoimmunity and annual MRI Potentially curative Long-term remission established in about 50% of treated patients Ongoing year experiment, analogous to BMT
Per Soelberg Sørensen
 Per Soelberg Sørensen Danish Multiple Sclerosis Center Department of Neurology Rigshospitalet, University of Copenhagen Copenhagen, Denmark Declared receipt personal compensation for serving on scientific
Per Soelberg Sørensen Danish Multiple Sclerosis Center Department of Neurology Rigshospitalet, University of Copenhagen Copenhagen, Denmark Declared receipt personal compensation for serving on scientific
For HCPs Brain Health: Time Matters
 For HCPs Brain Health: Time Matters Gavin Giovannoni Barts and The London Disclosures Professor Giovannoni has received personal compensation for participating on Advisory Boards in relation to clinical
For HCPs Brain Health: Time Matters Gavin Giovannoni Barts and The London Disclosures Professor Giovannoni has received personal compensation for participating on Advisory Boards in relation to clinical
Benefit/Risk Strategies in Selecting Therapeutic Solutions for MS: HCP and Patient Viewpoints
 Benefit/Risk Strategies in Selecting Therapeutic Solutions for MS: HCP and Patient Viewpoints 1 Learning Objectives Review the benefit/risk strategies in selecting therapy for MS patients while assessing
Benefit/Risk Strategies in Selecting Therapeutic Solutions for MS: HCP and Patient Viewpoints 1 Learning Objectives Review the benefit/risk strategies in selecting therapy for MS patients while assessing
MS Trust Comments on the ACD
 MS Trust Comments on the ACD Name xxxxxxxxxxx Role other Other role xxxxxxxxxxxxxxxxxx Location England Conflict no Notes Comments on individual sections of the ACD: Section 1 The MS Trust maintains that
MS Trust Comments on the ACD Name xxxxxxxxxxx Role other Other role xxxxxxxxxxxxxxxxxx Location England Conflict no Notes Comments on individual sections of the ACD: Section 1 The MS Trust maintains that
MULTIPLE SCLEROSIS - REVIEW AND UPDATE
 MULTIPLE SCLEROSIS - REVIEW AND UPDATE Luka Vlahovic, MD Neuroimmunology/Multiple Sclerosis Creighton University Medical Center MS is primary demyelinating disease of the central nervous system. MS is
MULTIPLE SCLEROSIS - REVIEW AND UPDATE Luka Vlahovic, MD Neuroimmunology/Multiple Sclerosis Creighton University Medical Center MS is primary demyelinating disease of the central nervous system. MS is
CSF Axonal Injury Markers
 CSF Axonal Injury Markers Gavin Giovannoni Barts and The London Disclosures Professor Giovannoni has received personal compensation for participating on Advisory Boards in relation to clinical trial design,
CSF Axonal Injury Markers Gavin Giovannoni Barts and The London Disclosures Professor Giovannoni has received personal compensation for participating on Advisory Boards in relation to clinical trial design,
Progress in the field
 Progress in the field Eva Havrdová Charles University in Prague 1st Medical Faculty and General University Hospital Disclosures Dr. Havrdová has received consulting fees from Actelion, Biogen Idec, Merck,
Progress in the field Eva Havrdová Charles University in Prague 1st Medical Faculty and General University Hospital Disclosures Dr. Havrdová has received consulting fees from Actelion, Biogen Idec, Merck,
Life Long Brain Health and DMT Comparative Effectiveness
 Life Long Brain Health and DMT Comparative Effectiveness Timothy Vollmer, MD Professor of Neurology University of Colorado Denver Medical Director- RMMSC and Co-Director Rocky Mountain MS Center at CU
Life Long Brain Health and DMT Comparative Effectiveness Timothy Vollmer, MD Professor of Neurology University of Colorado Denver Medical Director- RMMSC and Co-Director Rocky Mountain MS Center at CU
Pediatric MS treatments: What do you start with, when do you switch?
 Pediatric MS treatments: What do you start with, when do you switch? Tim Lotze, M.D. Associate Professor of Pediatric Neurology Texas Children s Hospital Baylor College of Medicine Disclosures Clinical
Pediatric MS treatments: What do you start with, when do you switch? Tim Lotze, M.D. Associate Professor of Pediatric Neurology Texas Children s Hospital Baylor College of Medicine Disclosures Clinical
Hot Topics Multiple Sclerosis. Natalie Parks, MD, FRCPC Assistant Professor, Dalhousie University June 27, 2018
 Hot Topics Multiple Sclerosis Natalie Parks, MD, FRCPC Assistant Professor, Dalhousie University June 27, 2018 Disclosures Natalie Parks has received compensation from Biogen, EMD Serono, Roche, and Sanofi
Hot Topics Multiple Sclerosis Natalie Parks, MD, FRCPC Assistant Professor, Dalhousie University June 27, 2018 Disclosures Natalie Parks has received compensation from Biogen, EMD Serono, Roche, and Sanofi
Mitzi Joi Williams, MD Neurologist MS Center of Atlanta Atlanta, GA
 Mitzi Joi Williams, MD Neurologist MS Center of Atlanta Atlanta, GA Disclosures Consultant and Speaker Bureau member for Biogen-Idec, Pfizer, TEVA Neuroscience, Bayer, EMD Serrono, Questcor, Novartis,
Mitzi Joi Williams, MD Neurologist MS Center of Atlanta Atlanta, GA Disclosures Consultant and Speaker Bureau member for Biogen-Idec, Pfizer, TEVA Neuroscience, Bayer, EMD Serrono, Questcor, Novartis,
MS Academia: Multiple sclerosis advanced course
 13 September 2016 - London, UK MS Academia: Multiple sclerosis advanced course IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Robert J. Fox Assessment of treatment response IMPROVING
13 September 2016 - London, UK MS Academia: Multiple sclerosis advanced course IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Robert J. Fox Assessment of treatment response IMPROVING
Program Highlights. A multidisciplinary AAN working group identified areas for improvement in the diagnosis and management of patients with MS
 CasePerspectives: Illuminating Dark Pathways in Complex MS Cases Program Highlights Stephen Krieger, MD Associate Professor of Neurology Corinne Goldsmith Dickinson Center for MS Director, Neurology Residency
CasePerspectives: Illuminating Dark Pathways in Complex MS Cases Program Highlights Stephen Krieger, MD Associate Professor of Neurology Corinne Goldsmith Dickinson Center for MS Director, Neurology Residency
Advances in the Management of Multiple Sclerosis: A closer look at novel therapies. Disclosures
 Advances in the Management of Multiple Sclerosis: A closer look at novel therapies Lily Jung Henson, MD, MMM, FAAN Chief of Neurology Piedmont Healthcare, Atlanta, GA National Association of Managed Care
Advances in the Management of Multiple Sclerosis: A closer look at novel therapies Lily Jung Henson, MD, MMM, FAAN Chief of Neurology Piedmont Healthcare, Atlanta, GA National Association of Managed Care
MS Academia: Multiple sclerosis advanced course
 6 October 2015 - Barcelona, Spain MS Academia: Multiple sclerosis advanced course IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Mark S. Freedman University of Ottawa and the Ottawa
6 October 2015 - Barcelona, Spain MS Academia: Multiple sclerosis advanced course IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Mark S. Freedman University of Ottawa and the Ottawa
PATIENT INFORMATION: Patient Surname First Name Middle Initial Sex Date of Birth Alberta Personal Health Number M / F Year Month Day
 Applicant must be covered on an Alberta Government sponsored drug program. Page 1 of 6 PATIENT INFORMATION: Patient Surname First Name Middle Initial Sex Date of Birth Alberta Personal Health Number M
Applicant must be covered on an Alberta Government sponsored drug program. Page 1 of 6 PATIENT INFORMATION: Patient Surname First Name Middle Initial Sex Date of Birth Alberta Personal Health Number M
Progress in MS: Current and Emerging Therapies. Presented by: Dr. Kathryn Giles, MD MSc FRCPC Cambridge, Ontario, Canada
 Progress in MS: Current and Emerging Therapies Presented by: Dr. Kathryn Giles, MD MSc FRCPC Cambridge, Ontario, Canada Today s Discussion Natural History and Classification of MS Treating MS Management
Progress in MS: Current and Emerging Therapies Presented by: Dr. Kathryn Giles, MD MSc FRCPC Cambridge, Ontario, Canada Today s Discussion Natural History and Classification of MS Treating MS Management
Mellen Center Approaches: Natalizumab
 Cleveland Clinic Mellen Center for Multiple Sclerosis Treatment and Research 216.444.8600 Mellen Center Approaches: Natalizumab Who should be considered for Natalizumab therapy? In the phase II and phase
Cleveland Clinic Mellen Center for Multiple Sclerosis Treatment and Research 216.444.8600 Mellen Center Approaches: Natalizumab Who should be considered for Natalizumab therapy? In the phase II and phase
Local Natalizumab Treatment Protocol
 Local Natalizumab Treatment Protocol 1. New medicine name: Natalizumab 300mg concentrate for solution for infusion (Natalizumab ) 2. Licensed indication(s): Natalizumab is indicated for single disease
Local Natalizumab Treatment Protocol 1. New medicine name: Natalizumab 300mg concentrate for solution for infusion (Natalizumab ) 2. Licensed indication(s): Natalizumab is indicated for single disease
1996 vs 2013 MS Phenotype Descriptions of Progressive Disease
 Learning Objectives Upon completion, participants should be able to: Describe methods of distinguishing among RRMS, SPMS, and PPMS Incorporate available evidence about emerging and recently approved novel
Learning Objectives Upon completion, participants should be able to: Describe methods of distinguishing among RRMS, SPMS, and PPMS Incorporate available evidence about emerging and recently approved novel
Treatment Algorithm for Multiple Sclerosis Disease-modifying Therapies
 Treatment Algorithm for Multiple Sclerosis Disease-modifying Therapies NHS England Reference: 170079ALG Date Published: 4 September 2018 Gateway reference: 07603 Treatment Algorithm for Multiple Sclerosis
Treatment Algorithm for Multiple Sclerosis Disease-modifying Therapies NHS England Reference: 170079ALG Date Published: 4 September 2018 Gateway reference: 07603 Treatment Algorithm for Multiple Sclerosis
EAN Amsterdam June 23-27, 2017
 EAN 2017 Amsterdam June 23-27, 2017 MS Nowadays-new goals Giancarlo Comi Dept. of Neurology & Institute of Experimental Neurology Università Vita Salute S.Raffaele, Milano European Charcot Foundation Disclosure
EAN 2017 Amsterdam June 23-27, 2017 MS Nowadays-new goals Giancarlo Comi Dept. of Neurology & Institute of Experimental Neurology Università Vita Salute S.Raffaele, Milano European Charcot Foundation Disclosure
Evidence from bone marrow transplantation
 Evidence from bone marrow transplantation Gianluigi Mancardi Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, Ospedale Policlinico San Martino, University
Evidence from bone marrow transplantation Gianluigi Mancardi Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, Ospedale Policlinico San Martino, University
Switching from natalizumab to fingolimod: an observational study
 Acta Neurol Scand 2013: 128: e6 e10 DOI: 10.1111/ane.12082 Ó 2013 John Wiley & Sons A/S ACTA NEUROLOGICA SCANDINAVICA Clinical Commentary Switching from natalizumab to fingolimod: an observational study
Acta Neurol Scand 2013: 128: e6 e10 DOI: 10.1111/ane.12082 Ó 2013 John Wiley & Sons A/S ACTA NEUROLOGICA SCANDINAVICA Clinical Commentary Switching from natalizumab to fingolimod: an observational study
Update in Multiple Sclerosis
 Update in Multiple Sclerosis Kyle Smoot, MD Providence MS Center Portland, OR 1 Disclosures Research funds from Biogen. Consulting fees from Acorda, Biogen, EMDSerono, Genzyme, Novartis, and Teva. 2 Outline
Update in Multiple Sclerosis Kyle Smoot, MD Providence MS Center Portland, OR 1 Disclosures Research funds from Biogen. Consulting fees from Acorda, Biogen, EMDSerono, Genzyme, Novartis, and Teva. 2 Outline
Is it time to target no evident disease activity (NEDA) in multiple sclerosis?
 in multiple sclerosis?") Is it time to target no evident disease activity (NEDA) in multiple sclerosis? Giovannoni, G; Turner, B; Gnanapavan, S; Offiah, C; Schmierer, K; Marta, M Licensed with a Creative Commons Attribution Non-Commercial
Is it time to target no evident disease activity (NEDA) in multiple sclerosis? Giovannoni, G; Turner, B; Gnanapavan, S; Offiah, C; Schmierer, K; Marta, M Licensed with a Creative Commons Attribution Non-Commercial
The invisible facets of MS and everyday challenges clinician s perspective. Mar Tintore
 The invisible facets of MS and everyday challenges clinician s perspective Mar Tintore Centre d Esclerosi Múltiple de Catalunya (Cemcat). Department of Neurology/Neuroimmunology Hospital Universitari Vall
The invisible facets of MS and everyday challenges clinician s perspective Mar Tintore Centre d Esclerosi Múltiple de Catalunya (Cemcat). Department of Neurology/Neuroimmunology Hospital Universitari Vall
The Effects of Daclizumab High Yield Process (DAC HYP) on Patient Centered Functional Outcomes: Results From the DECIDE Study
 on Patient Centered Functional Outcomes: Results From the DECIDE Study") 2015 Annual Meeting of the Consortium of Multiple Sclerosis Centers May 27 30, 2015 Indianapolis, IN The Effects of Daclizumab High Yield Process () on Patient Centered Functional Outcomes: Results From
2015 Annual Meeting of the Consortium of Multiple Sclerosis Centers May 27 30, 2015 Indianapolis, IN The Effects of Daclizumab High Yield Process () on Patient Centered Functional Outcomes: Results From
Clinician s view of Benefit-Risk
 Clinician s view of Benefit-Risk Gordon Francis, MD Novartis, Clinical Development Clinician s View of Benefit-Risk: a need for reliable metrics A tale of 3 drugs Natalizumab MS Crohn s Disease Fingolimod
Clinician s view of Benefit-Risk Gordon Francis, MD Novartis, Clinical Development Clinician s View of Benefit-Risk: a need for reliable metrics A tale of 3 drugs Natalizumab MS Crohn s Disease Fingolimod
Consortium of Multiple Sclerosis Centers 2015 Abstract #3485
 Alemtuzumab (ALE) Improves Disability After Switch from Other Disease Modifying Therapies in a High Disability, Treatment Refractory Relapsing MS Cohort Consortium of Multiple Sclerosis Centers 2015 Abstract
Alemtuzumab (ALE) Improves Disability After Switch from Other Disease Modifying Therapies in a High Disability, Treatment Refractory Relapsing MS Cohort Consortium of Multiple Sclerosis Centers 2015 Abstract
Choices. Disease modifying treatments. Read me
 Choices Disease modifying treatments Read me Disease modifying treatments Disease modifying therapies (DMTs) are medications which modify the course of multiple sclerosis (MS) and are designed to reduce
Choices Disease modifying treatments Read me Disease modifying treatments Disease modifying therapies (DMTs) are medications which modify the course of multiple sclerosis (MS) and are designed to reduce
Carolyn Taylor, M.D. Swedish Neuroscience Center
 Carolyn Taylor, M.D. Swedish Neuroscience Center When should disease modifying therapy be discontinued in MS? Should we be using aggressive treatments earlier in the MS disease course and reserving the
Carolyn Taylor, M.D. Swedish Neuroscience Center When should disease modifying therapy be discontinued in MS? Should we be using aggressive treatments earlier in the MS disease course and reserving the
A Glimpse at Immunomodulators in MS
 A Glimpse at Immunomodulators in MS An Interview with Mark S. Freedman, HBSc, MSc, MD, CSPQ, FAAN, FRCPC Multiple Sclerosis Research Unit, University of Ottowa, Ottowa Canada Ottawa Hospital Research Institute,
A Glimpse at Immunomodulators in MS An Interview with Mark S. Freedman, HBSc, MSc, MD, CSPQ, FAAN, FRCPC Multiple Sclerosis Research Unit, University of Ottowa, Ottowa Canada Ottawa Hospital Research Institute,
Efficacy convenience of MS treatments. Xavier Montalban Department of Neurology-Neuroimmunology. ECF Baveno 2013
 Efficacy convenience of MS treatments Xavier Montalban Department of Neurology-Neuroimmunology ECF Baveno 2013 Disclaimer Dr. Montalban has received speaking honoraria and travel expenses for scientific
Efficacy convenience of MS treatments Xavier Montalban Department of Neurology-Neuroimmunology ECF Baveno 2013 Disclaimer Dr. Montalban has received speaking honoraria and travel expenses for scientific
Biologics and Beyond: Treatment of Multiple Sclerosis. Rita Jebrin, PharmD, BCPS
 Biologics and Beyond: Treatment of Multiple Sclerosis Rita Jebrin, PharmD, BCPS Disclosure Information Biologics and Beyond: Treatment of Multiple Sclerosis Rita Jebrin, PharmD, BCPS I have no financial
Biologics and Beyond: Treatment of Multiple Sclerosis Rita Jebrin, PharmD, BCPS Disclosure Information Biologics and Beyond: Treatment of Multiple Sclerosis Rita Jebrin, PharmD, BCPS I have no financial
European Commission Grants Approval for Mavenclad (Cladribine Tablets)
") Your Contact Friederike Segeberg +49 6151 72-6328 Investor Relations +49 6151 72-3321 August 25, 2017 European Commission Grants Approval for Mavenclad (Cladribine Tablets) First oral short-course treatment
Your Contact Friederike Segeberg +49 6151 72-6328 Investor Relations +49 6151 72-3321 August 25, 2017 European Commission Grants Approval for Mavenclad (Cladribine Tablets) First oral short-course treatment
MRI in Differential Diagnosis. CMSC, June 2, Jill Conway, MD, MA, MSCE
 MRI in Differential Diagnosis CMSC, June 2, 2016 Jill Conway, MD, MA, MSCE Director, Carolinas MS Center Clerkship Director, UNCSOM-Charlotte Campus Charlotte, NC Disclosures Speaking, consulting, and/or
MRI in Differential Diagnosis CMSC, June 2, 2016 Jill Conway, MD, MA, MSCE Director, Carolinas MS Center Clerkship Director, UNCSOM-Charlotte Campus Charlotte, NC Disclosures Speaking, consulting, and/or
MEDIA BACKGROUNDER. Multiple Sclerosis: A serious and unpredictable neurological disease
 MEDIA BACKGROUNDER Multiple Sclerosis: A serious and unpredictable neurological disease Multiple sclerosis (MS) is a complex chronic inflammatory disease of the central nervous system (CNS) that still
MEDIA BACKGROUNDER Multiple Sclerosis: A serious and unpredictable neurological disease Multiple sclerosis (MS) is a complex chronic inflammatory disease of the central nervous system (CNS) that still
Long-term effects of cladribine tablets on MRI activity outcomes in patients with relapsing remitting multiple sclerosis: the CLARITY Extension study
 753365TAN0010.1177/1756285617753365Therapeutic Advances in Neurological DisordersG Comi, S CooK research-article2018 Therapeutic Advances in Neurological Disorders Original Research Long-term effects of
753365TAN0010.1177/1756285617753365Therapeutic Advances in Neurological DisordersG Comi, S CooK research-article2018 Therapeutic Advances in Neurological Disorders Original Research Long-term effects of
Case Report PML-IRIS during Fingolimod Diagnosed after Natalizumab Discontinuation
 Case Reports in Neurological Medicine, Article ID 307872, 4 pages http://dx.doi.org/10.1155/2014/307872 Case Report PML-IRIS during Fingolimod Diagnosed after Natalizumab Discontinuation J. Killestein,
Case Reports in Neurological Medicine, Article ID 307872, 4 pages http://dx.doi.org/10.1155/2014/307872 Case Report PML-IRIS during Fingolimod Diagnosed after Natalizumab Discontinuation J. Killestein,
TREATING MULTIPLE SCLEROSIS The Current Disease Modifying Therapies Beverly Gilder, M.D. Blue Sky Neurology MS Center
 TREATING MULTIPLE SCLEROSIS 2018 The Current Disease Modifying Therapies Beverly Gilder, M.D. Blue Sky Neurology MS Center Welcome Thank you for joining us! Today you will learn about MS treatment choices
TREATING MULTIPLE SCLEROSIS 2018 The Current Disease Modifying Therapies Beverly Gilder, M.D. Blue Sky Neurology MS Center Welcome Thank you for joining us! Today you will learn about MS treatment choices
Multiple Sclerosis. Stanley L Cohan, MD, PhD Providence MS Center Providence Brain and Spine Institute
 Stanley L Cohan, MD, PhD Providence MS Center Providence Brain and Spine Institute 1 Stanley Cohan conflicts of interest Research Support: Biogen Idec, Novartis, Mallinkrodt, Genzyme, Sanofi-Aventis, Teva,
Stanley L Cohan, MD, PhD Providence MS Center Providence Brain and Spine Institute 1 Stanley Cohan conflicts of interest Research Support: Biogen Idec, Novartis, Mallinkrodt, Genzyme, Sanofi-Aventis, Teva,
Biothérapies et risques infectieux en. neurologie
 Biothérapies et risques infectieux en Lieu 14 Date neurologie Patrick Vermersch CHU de Lille XXIIe Journée Régionale de Pathologie Infectieuse Lille, 13 octobre 2015 Liens d intérêts Honoraires, Congrés,
Biothérapies et risques infectieux en Lieu 14 Date neurologie Patrick Vermersch CHU de Lille XXIIe Journée Régionale de Pathologie Infectieuse Lille, 13 octobre 2015 Liens d intérêts Honoraires, Congrés,
Treating MS. New medicines, strong evidence, better practice? September 2015
 Treating MS New medicines, strong evidence, better practice? September 2015 1 A Treatment Revolution for RRMS Over the past 20 years there has been a revolution in treatments for relapsing remitting MS
Treating MS New medicines, strong evidence, better practice? September 2015 1 A Treatment Revolution for RRMS Over the past 20 years there has been a revolution in treatments for relapsing remitting MS
What is Multiple Sclerosis? Gener al information
 What is Multiple Sclerosis? Gener al information Kim, diagnosed in 1986 What is MS? Multiple sclerosis (or MS) is a chronic, often disabling disease that attacks the central nervous system (brain and spinal
What is Multiple Sclerosis? Gener al information Kim, diagnosed in 1986 What is MS? Multiple sclerosis (or MS) is a chronic, often disabling disease that attacks the central nervous system (brain and spinal
Giancarlo Comi, M.D. On Behalf of the MS-LAQ-301 (ALLEGRO) Study Group. Assessment of oral laquinimod in preventing progression of Multiple Sclerosis
 Study Group. Assessment of oral laquinimod in preventing progression of Multiple Sclerosis") COMPARISON OF EARLY AND DELAYED ORAL LAQUINIMOD IN PATIENTS WITH RELAPSING- REMITTING MULTIPLE SCLEROSIS: EFFECTS ON DISABILITY PROGRESSION AT 36 MONTHS IN THE ALLEGRO TRIAL Giancarlo Comi, M.D. On Behalf
COMPARISON OF EARLY AND DELAYED ORAL LAQUINIMOD IN PATIENTS WITH RELAPSING- REMITTING MULTIPLE SCLEROSIS: EFFECTS ON DISABILITY PROGRESSION AT 36 MONTHS IN THE ALLEGRO TRIAL Giancarlo Comi, M.D. On Behalf
EMA confirms recommendations to minimise risk of brain infection PML with Tysabri
 25/04/2016 EMA/266665/2016 EMA confirms recommendations to minimise risk of brain infection PML with Tysabri More frequent MRI scans should be considered for patients at higher risk On 25 February 2016,
25/04/2016 EMA/266665/2016 EMA confirms recommendations to minimise risk of brain infection PML with Tysabri More frequent MRI scans should be considered for patients at higher risk On 25 February 2016,
Medication Policy Manual. Topic: Aubagio, teriflunomide Date of Origin: November 9, 2012
 Medication Policy Manual Policy No: dru283 Topic: Aubagio, teriflunomide Date of Origin: November 9, 2012 Committee Approval Date: December 16, 2016 Next Review Date: December 2017 Effective Date: January
Medication Policy Manual Policy No: dru283 Topic: Aubagio, teriflunomide Date of Origin: November 9, 2012 Committee Approval Date: December 16, 2016 Next Review Date: December 2017 Effective Date: January
Committee Approval Date: December 12, 2014 Next Review Date: December 2015
 Medication Policy Manual Policy No: dru283 Topic: Aubagio, teriflunomide Date of Origin: November 9, 2012 Committee Approval Date: December 12, 2014 Next Review Date: December 2015 Effective Date: January
Medication Policy Manual Policy No: dru283 Topic: Aubagio, teriflunomide Date of Origin: November 9, 2012 Committee Approval Date: December 12, 2014 Next Review Date: December 2015 Effective Date: January
2013 MS Phenotype Descriptions: Relapsing MS 1
 2013 MS Phenotype Descriptions: Relapsing MS 1 Disease-Modifying Therapies? which can be found in its entirety at. Clinically isolated syndrome (CIS) Not Active a Active a,b Relapsing-remitting disease
2013 MS Phenotype Descriptions: Relapsing MS 1 Disease-Modifying Therapies? which can be found in its entirety at. Clinically isolated syndrome (CIS) Not Active a Active a,b Relapsing-remitting disease
Activity presentations are considered intellectual property.
 Activity presentations are considered intellectual property. Activity presentations are considered intellectual property and are for viewing purposes only. No content should be copied or reproduced in
Activity presentations are considered intellectual property. Activity presentations are considered intellectual property and are for viewing purposes only. No content should be copied or reproduced in
Medication Policy Manual. Topic: Tecfidera, dimethyl fumarate Date of Origin: May 16, 2013
 Medication Policy Manual Policy No: dru299 Topic: Tecfidera, dimethyl fumarate Date of Origin: May 16, 2013 Committee Approval Date: December 16, 2016 Next Review Date: December 2017 Effective Date: January
Medication Policy Manual Policy No: dru299 Topic: Tecfidera, dimethyl fumarate Date of Origin: May 16, 2013 Committee Approval Date: December 16, 2016 Next Review Date: December 2017 Effective Date: January
Anisha Keshavan. Roland Henry, PhD. Proportion of Patients (%) Rituximab 2000mg (n=66) Placebo (n=35)
 Rituximab 2000mg (n=66) Placebo (n=35)") Two Faces of Multiple Sclerosis February 8, 217 5 T H A N N U A L R E C E N T A D V A N C E S I N N E U R O L O G Y B CELL THERAPY FOR MULTIPLE SCLEROSIS: A NEW DAY? Inflammation Relapsing MS Anisha Keshavan
Two Faces of Multiple Sclerosis February 8, 217 5 T H A N N U A L R E C E N T A D V A N C E S I N N E U R O L O G Y B CELL THERAPY FOR MULTIPLE SCLEROSIS: A NEW DAY? Inflammation Relapsing MS Anisha Keshavan
MULTIPLE SCLEROSIS Update
 MULTIPLE SCLEROSIS Update E. Torage Shivapour, M.D. Clinical Professor Department of Neurology University of Iowa Hospitals & Clinics Disclosures I do not have any disclosures. Multiple Sclerosis Most
MULTIPLE SCLEROSIS Update E. Torage Shivapour, M.D. Clinical Professor Department of Neurology University of Iowa Hospitals & Clinics Disclosures I do not have any disclosures. Multiple Sclerosis Most
Neuroimaging and Other Biomarkers. MRI for Diagnosis, Prognosis and Treatment Decisions in MS
 Neuroimaging and Other Biomarkers MRI for Diagnosis, Prognosis and Treatment Decisions in MS Eric Klawiter, MD MSc Massachusetts General Hospital May 30, 2014 Disclosures and Funding Disclosures: Consulting
Neuroimaging and Other Biomarkers MRI for Diagnosis, Prognosis and Treatment Decisions in MS Eric Klawiter, MD MSc Massachusetts General Hospital May 30, 2014 Disclosures and Funding Disclosures: Consulting
Demyelinating Diseases: Multiple Sclerosis January 10, 2018 Dr. Ostrow
 Demyelinating Diseases: Multiple Sclerosis January 10, 2018 Dr. Ostrow Reading: Robbins & Cotran, 9 th edition, pp 1283-1286 Robbins Basic Pathology, 9 th edition, 832-835 Overview: Grossly, myelin is
Demyelinating Diseases: Multiple Sclerosis January 10, 2018 Dr. Ostrow Reading: Robbins & Cotran, 9 th edition, pp 1283-1286 Robbins Basic Pathology, 9 th edition, 832-835 Overview: Grossly, myelin is
Autologous Hematopoietic Stem Cell Transplantation for the Treatment of Neuromyelitis Optica in Singapore
 Case Reports 26 Autologous Hematopoietic Stem Cell Transplantation for the Treatment of Neuromyelitis Optica in Singapore Koh Yeow Hoay, Pavanni Ratnagopal Abstract Introduction: Neuromyelitis optica (NMO)
Case Reports 26 Autologous Hematopoietic Stem Cell Transplantation for the Treatment of Neuromyelitis Optica in Singapore Koh Yeow Hoay, Pavanni Ratnagopal Abstract Introduction: Neuromyelitis optica (NMO)
Disclosures. Biogen Idec Novartis Acorda Genzyme Roche Pfizer
 Disclosures Biogen Idec Novartis Acorda Genzyme Roche Pfizer Erik V Burton, M.D. Department of Neurology Multiple Sclerosis Specialty Clinic UNM Health Science Center Albuquerque, NM LIVING WITH MULTIPLE
Disclosures Biogen Idec Novartis Acorda Genzyme Roche Pfizer Erik V Burton, M.D. Department of Neurology Multiple Sclerosis Specialty Clinic UNM Health Science Center Albuquerque, NM LIVING WITH MULTIPLE
Clinical and research application of MRI in diagnosis and monitoring of multiple sclerosis
 24-25 February 2016 - Siena, Italy Clinical and research application of MRI in diagnosis and monitoring of multiple sclerosis IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org What
24-25 February 2016 - Siena, Italy Clinical and research application of MRI in diagnosis and monitoring of multiple sclerosis IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org What
APPENDIX D SASKATCHEWAN MS DRUGS PROGRAM
 APPENDIX D SASKATCHEWAN MS DRUGS PROGRAM PROCEDURE FOR OBTAINING COVERAGE OF MS DRUGS UNDER THE DRUG PLAN Requests are initiated by a physician. The patient and physician complete the application form
APPENDIX D SASKATCHEWAN MS DRUGS PROGRAM PROCEDURE FOR OBTAINING COVERAGE OF MS DRUGS UNDER THE DRUG PLAN Requests are initiated by a physician. The patient and physician complete the application form
Helpful Information for evaluation of new neurological symptoms in patients receiving TYSABRI
 Helpful Information for evaluation of new neurological symptoms in patients receiving TYSABRI This information is provided as an educational resource for healthcare providers and should be considered current
Helpful Information for evaluation of new neurological symptoms in patients receiving TYSABRI This information is provided as an educational resource for healthcare providers and should be considered current
Updates to the Alberta Drug Benefit List. Effective August 1, 2018
 Updates to the Alberta Drug Benefit List Effective August 1, 2018 Inquiries should be directed to: Pharmacy Services Alberta Blue Cross 10009 108 Street NW Edmonton AB T5J 3C5 Telephone Number: (780) 498-8370
Updates to the Alberta Drug Benefit List Effective August 1, 2018 Inquiries should be directed to: Pharmacy Services Alberta Blue Cross 10009 108 Street NW Edmonton AB T5J 3C5 Telephone Number: (780) 498-8370
Before beginning this activity, please be sure to review the learning objectives and faculty disclosures.
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
MULTIPLE SCLEROSIS IN Managing the complexity of multiple sclerosis. Olga Ciccarelli and Alan Thompson
 MULTIPLE SCLEROSIS IN 2015 Managing the complexity of multiple sclerosis Olga Ciccarelli and Alan Thompson The application of imaging biomarkers has provided new insights into the mechanisms of damage
MULTIPLE SCLEROSIS IN 2015 Managing the complexity of multiple sclerosis Olga Ciccarelli and Alan Thompson The application of imaging biomarkers has provided new insights into the mechanisms of damage
Technology appraisal guidance Published: 6 December 2017 nice.org.uk/guidance/ta493
 Cladribine tablets for treating relapsing remitting multiple sclerosis Technology appraisal guidance Published: 6 December 2017 nice.org.uk/guidance/ta493 NICE 2018. All rights reserved. Subject to Notice
Cladribine tablets for treating relapsing remitting multiple sclerosis Technology appraisal guidance Published: 6 December 2017 nice.org.uk/guidance/ta493 NICE 2018. All rights reserved. Subject to Notice
Patient 1: 31-Year-Old Female. Fingolimod treatment
 Cell Counts (10 9 /L) Cell Count ( 10 9 /L) Cell Count ( 10 9 /L) Cell Count ( 10 9 /L) Cell Count ( 10 9 /L) Cell Count ( 10 9 /L) Lymphocyte Pharmacodynamics and Safety of Use in Patients Previously
Cell Counts (10 9 /L) Cell Count ( 10 9 /L) Cell Count ( 10 9 /L) Cell Count ( 10 9 /L) Cell Count ( 10 9 /L) Cell Count ( 10 9 /L) Lymphocyte Pharmacodynamics and Safety of Use in Patients Previously
The Impact of Multiple Sclerosis in the. James Bowen, MD Multiple Sclerosis Center
 The Impact of Multiple Sclerosis in the Pacific Northwest James Bowen, MD Multiple Sclerosis Center Swedish Neuroscience Institute Motor Symptoms of MS Weakness Spasticity - stiffness, brisk reflexes
The Impact of Multiple Sclerosis in the Pacific Northwest James Bowen, MD Multiple Sclerosis Center Swedish Neuroscience Institute Motor Symptoms of MS Weakness Spasticity - stiffness, brisk reflexes
Pharmacotherapy Update Multiple Sclerosis
 Pharmacotherapy Update Multiple Sclerosis Yolande Hanssens SIG Leader Medicine Information Hamad Medical Corporation Pharmacy Department - Clinical Service Unit Doha - Qatar Heidelberg/October 2017 Pharmacotherapy
Pharmacotherapy Update Multiple Sclerosis Yolande Hanssens SIG Leader Medicine Information Hamad Medical Corporation Pharmacy Department - Clinical Service Unit Doha - Qatar Heidelberg/October 2017 Pharmacotherapy
The TOUCH Program and Risk Management. Updated Safety Results From the Use of Natalizumab in Patients With Relapsing Multiple
 1 The TOUCH Program and Risk Management Plan for the Administration i ti of Natalizumab: Updated Safety Results From the Use of Natalizumab in Patients With Relapsing Multiple Sclerosis and Crohn s Disease
1 The TOUCH Program and Risk Management Plan for the Administration i ti of Natalizumab: Updated Safety Results From the Use of Natalizumab in Patients With Relapsing Multiple Sclerosis and Crohn s Disease
Neurology and Neurometabolic Unit Department of Neurological and Behavioral Sciences University of Siena Siena, Italy
 Nicola De Stefano Neurology and Neurometabolic Unit Department of Neurological and Behavioral Sciences University of Siena Siena, Italy Declared receipt of honoraria or consultation fees from Novartis,
Nicola De Stefano Neurology and Neurometabolic Unit Department of Neurological and Behavioral Sciences University of Siena Siena, Italy Declared receipt of honoraria or consultation fees from Novartis,
Disease-modifying therapies
 Updated May 2018. Please check nationalmssociety.org/dmt for the most current version of this publication. For some people, a diagnosis of multiple sclerosis (MS) is a relief, giving a name and a reason
Updated May 2018. Please check nationalmssociety.org/dmt for the most current version of this publication. For some people, a diagnosis of multiple sclerosis (MS) is a relief, giving a name and a reason
Le Hua, MD. Disclosures Teaching and Speaking: Teva Neurosciences, Genzyme, Novartis Advisory Board: Genzyme, EMD Serono
 Le Hua, MD Le Hua, MD, is a staff neurologist at Cleveland Clinic Lou Ruvo Center for Brain Health in Las Vegas, NV. She is involved in clinical trials assessing new therapies for the treatment of MS and
Le Hua, MD Le Hua, MD, is a staff neurologist at Cleveland Clinic Lou Ruvo Center for Brain Health in Las Vegas, NV. She is involved in clinical trials assessing new therapies for the treatment of MS and
Multiple Sclerosis (MS) Dr Oliver Lily Consultant Neurologist Leeds General Infirmary
 Dr Oliver Lily Consultant Neurologist Leeds General Infirmary") Multiple Sclerosis (MS) Dr Oliver Lily Consultant Neurologist Leeds General Infirmary Multiple sclerosis What is MS? What causes MS? Symptoms and signs of MS Making the diagnosis Investigations Treatments
Multiple Sclerosis (MS) Dr Oliver Lily Consultant Neurologist Leeds General Infirmary Multiple sclerosis What is MS? What causes MS? Symptoms and signs of MS Making the diagnosis Investigations Treatments
Expectation of a Rare Event. Laura Meyerson, Ph.D Midwest Biopharmaceutical Statistics Workshop Ball State University Muncie, IN
 Expectation of a Rare Event Laura Meyerson, Ph.D. 2011 Midwest Biopharmaceutical Statistics Workshop Ball State University Muncie, IN The Story Begins TYSABRI was approved in US for treatment of multiple
Expectation of a Rare Event Laura Meyerson, Ph.D. 2011 Midwest Biopharmaceutical Statistics Workshop Ball State University Muncie, IN The Story Begins TYSABRI was approved in US for treatment of multiple
Guideline for the use of beta-interferons in patients with multiple sclerosis a South African proposal
 GUIDELINE Guideline for the use of beta-interferons in patients with multiple sclerosis a South African proposal Multiple Sclerosis Advisory Committee of the Neurological Association of South Africa (NASA)
GUIDELINE Guideline for the use of beta-interferons in patients with multiple sclerosis a South African proposal Multiple Sclerosis Advisory Committee of the Neurological Association of South Africa (NASA)
Horizon Scanning Centre July Ocrelizumab for relapsing-remitting multiple sclerosis SUMMARY NIHR HSC ID: 3711
 Horizon Scanning Centre July 2014 Ocrelizumab for relapsing-remitting multiple sclerosis SUMMARY NIHR HSC ID: 3711 This briefing is based on information available at the time of research and a limited
Horizon Scanning Centre July 2014 Ocrelizumab for relapsing-remitting multiple sclerosis SUMMARY NIHR HSC ID: 3711 This briefing is based on information available at the time of research and a limited
Updates to the Alberta Human Services Drug Benefit Supplement
 Updates to the Alberta Human Services Drug Benefit Supplement Effective December 9, 2013 Inquiries should be directed to: Pharmacy Services Alberta Blue Cross 10009 108 Street NW Edmonton AB T5J 3C5 Telephone
Updates to the Alberta Human Services Drug Benefit Supplement Effective December 9, 2013 Inquiries should be directed to: Pharmacy Services Alberta Blue Cross 10009 108 Street NW Edmonton AB T5J 3C5 Telephone
Multiple Sclerosis , The Patient Education Institute, Inc. nr Last reviewed: 04/17/2017 1
 Multiple Sclerosis Introduction Multiple sclerosis, or MS, is a disease of the brain and spinal cord. Most patients with multiple sclerosis are able to lead a very functional life. However, MS causes a
Multiple Sclerosis Introduction Multiple sclerosis, or MS, is a disease of the brain and spinal cord. Most patients with multiple sclerosis are able to lead a very functional life. However, MS causes a
Novartis real-world data at AAN confirms benefit of Gilenya on four key measures of disease activity in relapsing MS
 Novartis International AG Novartis Global Communications CH-4002 Basel Switzerland http://www.novartis.com MEDIA RELEASE COMMUNIQUE AUX MEDIAS MEDIENMITTEILUNG Novartis real-world data at AAN confirms
Novartis International AG Novartis Global Communications CH-4002 Basel Switzerland http://www.novartis.com MEDIA RELEASE COMMUNIQUE AUX MEDIAS MEDIENMITTEILUNG Novartis real-world data at AAN confirms
Objectives. There Aren t Enough Hours in the Day
 There Aren t Enough Hours in the Day Medication monitoring and communication of results Objectives Review the types of testing being ordered on patients receiving therapies other than platforms Discuss
There Aren t Enough Hours in the Day Medication monitoring and communication of results Objectives Review the types of testing being ordered on patients receiving therapies other than platforms Discuss
MDWISE PRIOR AUTHORIZATION CRITERIA TYSABRI (natalizumab): 300mg/15mL single use vial
: 300mg/15mL single use vial") MDWISE PRIOR AUTHORIZATION CRITERIA TYSABRI (natalizumab): 300mg/15mL single use vial Formulary Status: Non-Formulary requiring prior authorization PA CRITERIA FOR INITIAL AUTHORIZATION FOR USE IN MULTIPLE
MDWISE PRIOR AUTHORIZATION CRITERIA TYSABRI (natalizumab): 300mg/15mL single use vial Formulary Status: Non-Formulary requiring prior authorization PA CRITERIA FOR INITIAL AUTHORIZATION FOR USE IN MULTIPLE
Natalizumab (Tysabri; Biogen Idec, Inc, Elan Pharmaceuticals,
 n report n Recommendations for the Selection, Treatment, and Management of Patients Utilizing Natalizumab Therapy for Multiple Sclerosis John Foley, MD Abstract Natalizumab is an integrin receptor antagonist
n report n Recommendations for the Selection, Treatment, and Management of Patients Utilizing Natalizumab Therapy for Multiple Sclerosis John Foley, MD Abstract Natalizumab is an integrin receptor antagonist
Shutting Down MS: New Insights on Induction, Escalation, Oral Agents, and Monitoring
 Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
Current Enrolling Clinical Trials
 ASSESS RRMS patients with active disease who are still able to walk. Mariko Kita MD Description of Study/Trial: A 12-month, randomized, rater- and dose-blinded study to compare the efficacy and safety
ASSESS RRMS patients with active disease who are still able to walk. Mariko Kita MD Description of Study/Trial: A 12-month, randomized, rater- and dose-blinded study to compare the efficacy and safety
NEUROLOGY UPDATE IV: MULTIPLE SCLEROSIS
 NEUROLOGY UPDATE IV: MULTIPLE SCLEROSIS Learning Objectives Daniel Harrison, MD University of Maryland School of Medicine Baltimore, MD Upon completion of this module, participants should be familiar with:
NEUROLOGY UPDATE IV: MULTIPLE SCLEROSIS Learning Objectives Daniel Harrison, MD University of Maryland School of Medicine Baltimore, MD Upon completion of this module, participants should be familiar with:
Disclosures 6/26/2015
 Salim Chahin, MD, MSCE Multiple Sclerosis division The University of Pennsylvania Disclosures I have no disclosure to report. This talk is based on published literature, survey of neurologists in Damascus,
Salim Chahin, MD, MSCE Multiple Sclerosis division The University of Pennsylvania Disclosures I have no disclosure to report. This talk is based on published literature, survey of neurologists in Damascus,
Cost-effectiveness of cladribine (Mavenclad ) for the
 for the") Cost-effectiveness of cladribine (Mavenclad ) for the treatment of adult patients with highly active relapsing multiple sclerosis (MS) as defined by clinical or imaging features The NCPE has issued a recommendation
Cost-effectiveness of cladribine (Mavenclad ) for the treatment of adult patients with highly active relapsing multiple sclerosis (MS) as defined by clinical or imaging features The NCPE has issued a recommendation
Class Update with New Drug Evaluation: Disease-Modifying Drugs for Multiple Sclerosis
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
CHAIR SUMMIT 7TH ANNUAL #CHAIR2014. Master Class for Neuroscience Professional Development. September 11 13, Westin Tampa Harbour Island
 #CHAIR2014 7TH ANNUAL CHAIR SUMMIT Master Class for Neuroscience Professional Development September 11 13, 2014 Westin Tampa Harbour Island Sponsored by #CHAIR2014 Use of MRI in Clinical Decision- Making
#CHAIR2014 7TH ANNUAL CHAIR SUMMIT Master Class for Neuroscience Professional Development September 11 13, 2014 Westin Tampa Harbour Island Sponsored by #CHAIR2014 Use of MRI in Clinical Decision- Making
HALT MS: Study Overview. Primary Endpoint. Previous Publication
 Five Year Outcomes of Halt MS: High Dose Immunosuppressive Therapy and Autologous Hematopoietic Cell Transplantation for Severe Relapsing Remitting Multiple Sclerosis James Bowen, MD Swedish Neuroscience
Five Year Outcomes of Halt MS: High Dose Immunosuppressive Therapy and Autologous Hematopoietic Cell Transplantation for Severe Relapsing Remitting Multiple Sclerosis James Bowen, MD Swedish Neuroscience
Technology appraisal guidance Published: 26 April 2017 nice.org.uk/guidance/ta441
 Daclizumab for treating relapsing remitting multiple sclerosis Technology appraisal guidance Published: 26 April 2017 nice.org.uk/guidance/ta441 NICE 2017. All rights reserved. Subject to Notice of rights
Daclizumab for treating relapsing remitting multiple sclerosis Technology appraisal guidance Published: 26 April 2017 nice.org.uk/guidance/ta441 NICE 2017. All rights reserved. Subject to Notice of rights
Education around PML risk and monitoring at NHNN Queen Square MS Centre
 Audit MS Masterclass, Sheffield, 31 st March 2017 Education around PML risk and monitoring at NHNN Queen Square MS Centre UCL Institute of Neurology Queen Square Multiple Sclerosis Centre National Hospital
Audit MS Masterclass, Sheffield, 31 st March 2017 Education around PML risk and monitoring at NHNN Queen Square MS Centre UCL Institute of Neurology Queen Square Multiple Sclerosis Centre National Hospital
Current and near-term impact of biomarkers for multiple sclerosis Gavin Giovannoni
 Current and near-term impact of biomarkers for multiple sclerosis Gavin Giovannoni Institute of Cell and Molecular Science Queen Mary's School of Medicine and Dentistry Barts and The London NHS Trust The
Current and near-term impact of biomarkers for multiple sclerosis Gavin Giovannoni Institute of Cell and Molecular Science Queen Mary's School of Medicine and Dentistry Barts and The London NHS Trust The
Page 1. Multiple Sclerosis. I have no conflicts of interest. Team Menstrual Cycles Waves to Wine for MS. Overview.
 Multiple Sclerosis New Developments Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts of interest Team Menstrual
Multiple Sclerosis New Developments Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts of interest Team Menstrual
Ocrevus. (ocrelizumab) New Product Slideshow
 New Product Slideshow") Ocrevus (ocrelizumab) New Product Slideshow Introduction Brand name: Ocrevus Generic name: Ocrelizumab Pharmacological class: CD20-directed cytolytic monoclonal antibody Strength and Formulation: 30mg/mL;
Ocrevus (ocrelizumab) New Product Slideshow Introduction Brand name: Ocrevus Generic name: Ocrelizumab Pharmacological class: CD20-directed cytolytic monoclonal antibody Strength and Formulation: 30mg/mL;
All relapsing multiple sclerosis patients should be managed at a specialist clinic- YES. Dr W J Brownlee FRACP 1. O Ciccarelli FRCP 1,2
 All relapsing multiple sclerosis patients should be managed at a specialist clinic- YES Dr W J Brownlee FRACP 1 O Ciccarelli FRCP 1,2 1 Queen Square Multiple Sclerosis Centre, Department of Neuroinflammation,
All relapsing multiple sclerosis patients should be managed at a specialist clinic- YES Dr W J Brownlee FRACP 1 O Ciccarelli FRCP 1,2 1 Queen Square Multiple Sclerosis Centre, Department of Neuroinflammation,
Multiple Sclerosis Update
 Multiple Sclerosis Update Amanda Stahnke, PharmD, BCACP University of Missouri-Kansas City School of Pharmacy Kansas City Veterans Affairs Honor Annex Kelsey Morris, PharmD University of Kansas Health-System
Multiple Sclerosis Update Amanda Stahnke, PharmD, BCACP University of Missouri-Kansas City School of Pharmacy Kansas City Veterans Affairs Honor Annex Kelsey Morris, PharmD University of Kansas Health-System
Real-World Effectiveness of Disease-Modifying Therapies in Korean Patients with Relapsing Multiple Sclerosis
 Open Access pissn 1738-6586 / eissn 2005-5013 / J Clin Neurol 2018 ORIGINAL ARTICLE Real-World Effectiveness of Disease-Modifying Therapies in Korean Patients with Relapsing Multiple Sclerosis Su-Hyun
Open Access pissn 1738-6586 / eissn 2005-5013 / J Clin Neurol 2018 ORIGINAL ARTICLE Real-World Effectiveness of Disease-Modifying Therapies in Korean Patients with Relapsing Multiple Sclerosis Su-Hyun
Do you or did you have any family members who have been diagnosed with MS? Yes No I Don t Know. Yes identical Yes not identical No
 The following survey will ask you questions about your family history of MS, your MS diagnosis and history, your symptoms, and your treatments. You may find it easier to fully answer these questions if
The following survey will ask you questions about your family history of MS, your MS diagnosis and history, your symptoms, and your treatments. You may find it easier to fully answer these questions if