Accelerated Partial Breast Irradiation. Dr Patricia Lillis MD, MHA,MSS Marshfield Clinic Radiation Oncology
|
|
|
- Dorothy Walton
- 5 years ago
- Views:
Transcription
1 Accelerated Partial Breast Irradiation Dr Patricia Lillis MD, MHA,MSS Marshfield Clinic Radiation Oncology
2 Outline 1. Rationale 2. Review of selected literature 3. Technical aspects 4. Selection criteria 5. Ongoing questions and trials
3 Early Investigations Charles H. Moore, 1867 (surgeon to the Middlesex Hospital, London). Cancer of the breast requires the careful extirpation of the entire organ; that the situation in which this operation is most likely to be incomplete is at the edge of the mamma near the sternum
4 Early Investigations William Halsted, (surgeon to the Johns Hopkins Hospital, Baltimore). Most of us have heard our teacher in surgery admit that they never cured a case of cancer of the breast Everyone knows how dreadful the end-results were before cleaning out the axilla became recognized as an essential part of the operation.
5 Early Investigations Sir Geoffrey Keynes, 1920s (St. Bartholomew Hospital, London). Interstitial radium implants of tumor bed and surrounding regions of the breast. treatment of choice for very advanced breast cancer.




6 Historical Perspective Interstitial Radium Brachytherapy for Breast Cancer, 1917 Radiotherapy for Breast Cancer, London Hospital, c. 1917
7 Breast Cancer: Critical Benchmark Studies NASBP (NEJM 2002: ) 20 year F/U shows lumpectomy + XRT 14% LRR lumpectomy alone 39.2% LRR Milan (Ann Oncol : ) Quadrantectomy + XRT 5.8% LRR Quadrantectomy alone 23.5% LRR
8 Meta-Analysis of Breast Cancer XRT Title: Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials Early Breast Cancer Trialists Collaborative Group (EBCTCG) Lancet 366: (2005)
9 Meta-Analysis of Breast Cancer XRT Meta-Analysis of 78 randomized controlled trials beginning by These trials included approximately 42,000 women and roughly ¾ were involved in XRT vs no XRT trials for either conservation therapy (intact breast) or post-mastectomy therapy. Trials separated into groups showing > or < 10% difference in LR.
10 From Lancet Meta-Analysis (N=42,000) XRT No XRT 5 year local recurrence: 7% 26% (conservation-intact breast) Post-Mastectomy (LN+) 6% 23% 15 year breast cancer mortality 30.5% 35.9% (intact breast) 15 year breast cancer mortality 54.7% 60.1% (post-mastectomy LN+) Overall all-cause reduction in mortality approx 4.4%! Similar proportional reductions in all groups
11 Techniques of APBI Interstitial implant brachytherapy Intra-Operative Radiotherapy External beam radiotherapy Intracavitary Brachytherapy
12 Breast Cancer: Critical Benchmark Studies NASBP (NEJM 2002: ) 20 year F/U shows lumpectomy + XRT 14% LRR lumpectomy alone 39.2% LRR Milan (Ann Oncol : ) Quadrantectomy + XRT 5.8% LRR Quadrantectomy alone 23.5% LRR
13 ASTRO APBI criteria Suitable Cautionary Age Diagnosis Invasive Ductal/DCIS Pure DCIS, EIS; 3cm tumor Tumor Size 2cm cm Surgical Margins Negative by at least 2mm Close ( 2mm) Nodal Status N 0 (i-, i+)

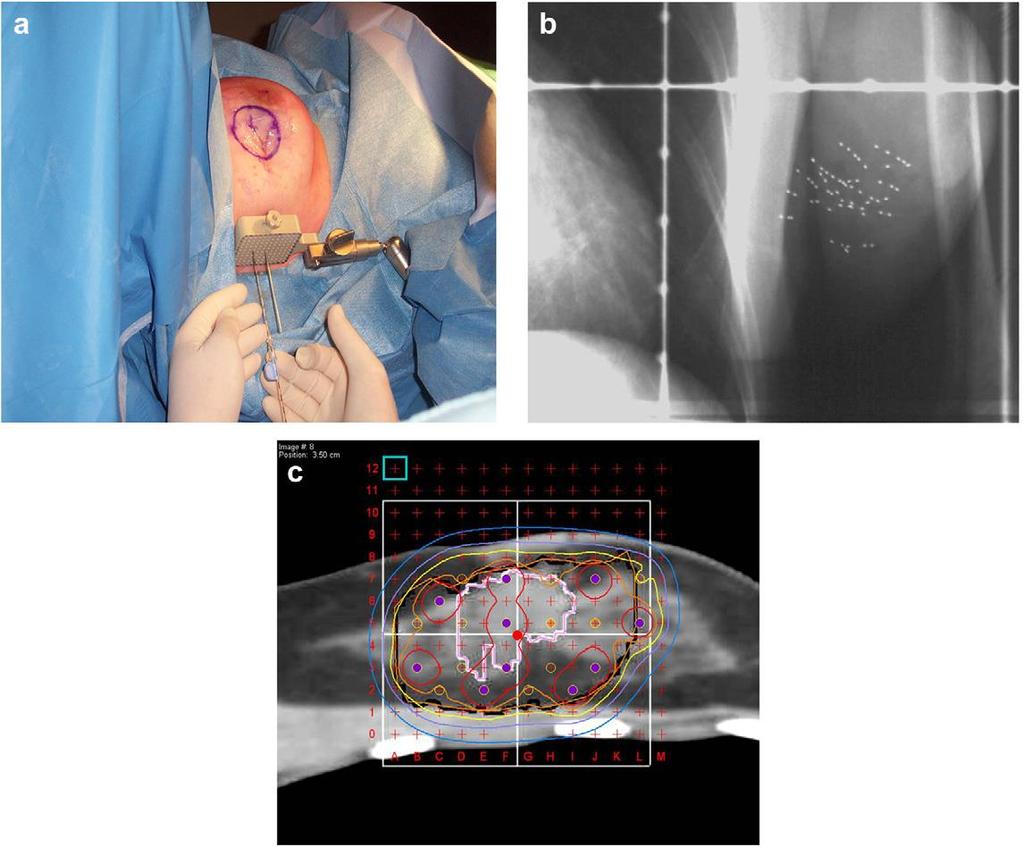
14 Multi-catheter interstitial brachytherapy

15 Method Open procedure Direct visualization of the lumpectomy cavity/clips Free hand method After catheter placement, wound closure and position secured

16 Closed cavity implant After the final pathology information to guide appropriate patient selection. Local anesthesia given min before the implantation. Virtual planning Simulator /CT based Appropriate number of catheters Number of catheter planes Optimal direction of placement.
17 Target volume Lumpectomy cavity plus a 2-cm margin Near chest wall and skin -1 to 1.5 cm Dose HDR-34 Gy/10# bid in 5 days LDR cgy/hr over 4.5 days Arthur et al. IJROBP 2003 vol 56, 681-9
18 Catheter implantation Free hand technique Template to ensure even needle spacing Using image guidance Ultrasound Fluoroscopy CT Scan

19
20 Design of the implant geometry Needles are implanted parallel and equidistance from each other (Paris system). In most cases inserted in a mediolateral direction. In very medially or laterally located tumor sites, needles should be implanted in a craniocaudal direction to enable separate target area from skin points. In some rare cases, the upper outer quadrant has to be implanted with needles orientated in a 45 angle to avoid overlap of source positions and skin

21 2 planes of needles are usually needed to cover the PTV. Single plane < 12 mm. Three planes are required in a large breast where the targeted breast tissue between pectoral fascia and skin is thicker than 30 mm. Five to nine needles spaced mm are usually required.

22 Reduction in skin dose Skin to source measuring bridge is used. If the superficial needles are too close to the skin, the templates are moved towards each other so that the overlying skin moves up and away from the needles. If this is not sufficient, templates with a smaller spacing between the needles are used, resulting in compression of the breast tissue and upward movement of the skin Some gauze is disposed between the templates and the skin of the thoracic wall at both sides of the implant to avoid skin necrosis secondary to continuous pressure of templates.
23 Advantages Has the longest follow-up. Better control and tailoring of radiation-dose delivery to variations in lumpectomy cavity, shape, or location within the breast. Limits toxicity to healthy tissue while delivering the maximum dose to atrisk tissue. Critical structures can be avoided by differential loading of the catheters
24 Limitations Considerable training and experience Appearance and patient acceptance of multiple catheter implants in the breast high skin dose: great care is required to ensure adequate source-toskin distance in patients treated with brachytherapy Therefore, may not be a viable treatment option for patients with superficial tumors or small breasts
25 results Njeh et al. Radiation Oncology 2010,5:90

26 n=258 pt1 pn0 grade 1 2, Age>40 WBI 130 PBI 128
, DCIS or invasive adenocarcinoma Node negative or with micrometastasis Margin 2 mm Accrual completed, Results")
27 Ongoing Trial (interstitial ) in Europe WBI (50 Gy/ 25#) +/- boost GEC-ESTRO n=1233 Interstitial brachytherapy 32 Gy in 8 fractions HDR, 30 Gy in 7 fractions HDR, 50 Gy LDR >40 years, Stages 0-II (T < 3 cm), DCIS or invasive adenocarcinoma Node negative or with micrometastasis Margin 2 mm Accrual completed, Results awaited
28 Intra-Operative Breast Irradiation
29 Intraoperative Radiation Therapy (IORT) for PBI TARGIT trial is comparing whole breast irradiation to IORT delivering a single dose of 20 Gy. Primary accrual is in Europe Using the Intrabeam Photon Radiosurgery System, 50 kv x- rays. Trial has enrolled 900 patients with target of 2200 patients.

30 Zeiss Intrabeam

 just published results of 590 pts treated with intra-op electron beam; 21 Gy single fraction. 3% breast fibrosis, 6/590 ipsilat.")
31 Intra-Operative Breast Irradiation London study using Intrabeam device (Photo Electron, now owned by Zeiss) Spherical applicators of different sizes 50 kv orthovoltage beam producing 5 Gy at 1 cm from application surface Clinical trial by Tobias et al. now underway; each site chooses its own entrance criteria. Other intra-op programs at MSK, etc. CCF used for boost only. Veronesi (Milan) just published results of 590 pts treated with intra-op electron beam; 21 Gy single fraction. 3% breast fibrosis, 6/590 ipsilat. recurrence after 2-year median f/u. [Ann. Surg 242:

32

33

34 Spherical Applicator 1.5-5cm with uniform surface dose Rate
35 Intracavitary Brachytherapy
36 Balloon based brachytherapy include: Mammosite Contura SAVI Axxent electronic brachytherapy

37 Mammosite brachytherapy system
38 structure Silicone balloon Double-lumen catheter (15 cm length and 6 mm in diameter) Inflation channel:- saline solution mixed with a small amount of contrast material to aid visualization. Source channel:- for passage of an Ir-192 high dose rate (HDR) brachytherapy source. Source channel runs centrally through the length of the balloon.


39 Post lumpectomy, the catheter is placed in the breast cavity either during the lumpectomy procedure or later through a closed technique balloon is inflated with ml of saline plus a small amount of contrast material, depending on the size of the lumpectomy cavity CT imaging to assess the adequate placement of the device An Ir-192 radioactive source, connected to a computer-controlled HDR remote after-loader delivers the prescription radiation dose



40 Quality of the implant Balloon Conformance: assessed by quantifying the volume of the PTV that is filled by air or seroma fluid. Less than 10% of the PTV should be composed of fluid or air. Large seroma Too much air


41 Minimum balloon-to-skin distance: for good cosmesis 5-7 mm is required Close to the skin


42 Symmetry Is essential for adequate dosimetry. A non-symmetrical implant can result in dose inhomogeneity in the surrounding tissues since the MSB device contains a single, central source channel that does not allow for shaping of the radiation isodose curves in the direction perpendicular to the central channel Asymmetrical
43 Dose 34 Gy over 10 fractions Minimum 6 hours between fractions D 90> 90% V150< 50cc V200< 20 cc Skin dose Max <145%
44 Limitations Not suitable in patients with small breast. Tumors located in the upper-inner quadrant. Irregular cavity. Requirement for skin-to-cavity distances too small superficial tumor
45 Njeh et al. Radiation Oncology 2010, 5:90 Results of mammosite
46 Contura MammoSite Multi-lumen (4 lumen) device
47 contura
48 Balloon based brachytherapy include: Mammosite Axxent electronic brachytherapy Contura

49 Axxent electronic brachytherapy Ballon is radiolucent :- No need of contrast Holes in the ballon Third port for drainage of seroma fluid or air surrounding the cavity.


50 Miniature X-ray source


51 Portable unit Digital touch-screen for the Physician and Physicist to input treatment data and monitor treatment progress. eb controller
52 Advantages Specifically shielded radiation room or an HDR afterloader unit are not required. This reduces costs and allows for portability of the system, which can lead to greater access for patients particularly in more remote or rural locations. Can be used intraoperatively
53 Electronic 50 Kv x-ray source Low energy spectrum that results in more rapid dose falloff with depth in tissue. Radiobiologic effect (RBE) for low-energy photons is higher on the order of This has currently not been taken into account in the prescribed dose for EBB, which uses the same prescription of 34.0 Gy in 10 fractions as used with 192Ir. Dose to structures proximal to the point(1 cm) is higher and the dose to structures beyond this point is lower with EBB Careful clinical evaluation is needed to determine the clinical impact of these factors with respect to late tissue affects and cosmesis.
54 In addition to a central lumen, the Contura balloon has four surrounding channels to accommodate the HDR source. Additional source positions allows increased dose flexibility compared with a single-catheter approach. Vacuum port to remove fluid or air around the lumpectomy cavity. Reduce the dose to normal tissues (chest wall and skin) better protection of organs at risk such as the heart and lungs. Possible to account for asymmetric balloon implant with respect to the central channel.
55 Hybrid brachytherapy devices Struts Adjusted Volume Implant (SAVI)
 HYBRID")
56 INTERSTITIAL BRACHYTHERAPY (VERSATILITY AND DOSIMETRIC CONFORMITY) BALLOON BRACHYTHERAPY (CONVENIENCE OF A SINGLE ENTRY DEVICE) HYBRID DEVICES

57 Strut Adjusted Volume Implant (SAVI)
58 Contains six outer expandable plastic tubes to displace the tissue Central catheter surrounded by six additional catheters that allow the passage of an HDR iridium-192 source The radiation source is not in direct contact with the breast tissue


59 CLEARPATH
60 Consists of a central strut Surrounded by 6, 8 or 10 peripheral struts Can be differentially loaded with HDR source Insertion done in collapsed form through an incision (freehand; USG guided) Then expanded to fit the cavity CT required (verification and planning)
61 EBRT (IMRT)
62 advantages Non-invasive (complications of surgery like seroma and infection can be avoided) Widespread availability Technically less demanding Treatment results with external beam may be more uniform between radiation oncologists Greater dose homogeneity
 to a total dose of 38.")
63 3.85 Gy twice daily (separated by at least 6 hours) to a total dose of 38.5 Gy delivered within 1 week

64 External beam radiotherapy 3D-CRT/ IMRT
65 planning CTV tumor bed on CT, including surgical clips plus 1 cm margin inside breast tissue PTV- CTV + 1 cm margin Prescribed dose 38.5 Gy in 10 # bid over 5-8 days/ minimum interfraction interval 6 hours The breast volume planning goals 0% to receive>107% <25% (up to 35% acceptable) to receive>95%, <50% (up to 60% acceptable) to receive >50% of the prescription dose Treated with 3-5 noncoplaner conformal fields 69

 Chemotherapy, if used, was")
66 Hypofrationated WBI (42.5 Gy/ 16#/22 days) 2128 patients 38.5 Gy/10#/5-8 days APBI >40 years, T < 3 cm, DCIS or invasive carcinoma, Node negative, Margin negative, No BRCA1 or 2 Large breasted patient :- 50 Gy/25# Boost allowed :- 10 Gy/5# (21%) Chemotherapy, if used, was completed before RT (15%)
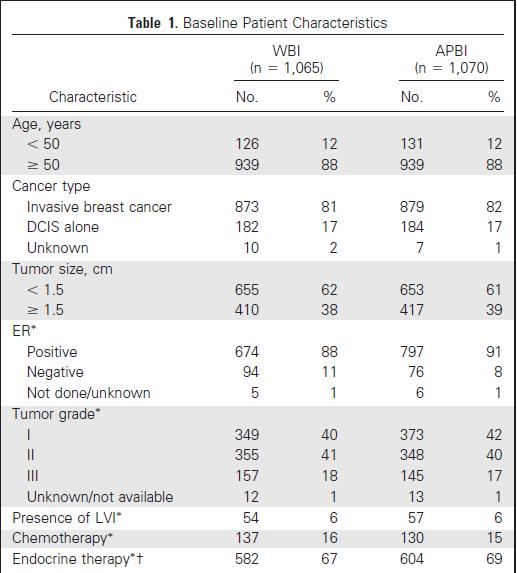
67 Patient Characteristics

68
69 Cosmetic Analysis By EORTC Cosmetic Rating System. At baseline, assessed by a trained nurse. Patient questionnaire Assessed by two panels of three radiation oncologists using the digital photographs on follow-up. The treated breast was compared with size and shape, location of the areola and nipple, appearance of the surgical scar, presence of telangiectasia, and global cosmetic score

70 Median follow-up- 36 months Cosmetic Outcome

71 NSABP B-39 trial
 51, 451 463520 patients")
 (50 Gy/ 25#/Boost 10")


72 5y European Journal of Cancer (2015) 51, patients n=1233 Conventional WBI (260) (50 Gy/ 25#/Boost 10 Gy ) APBI(260) 30 Gy/5# Nonconsecutive days >40 years T < 2.5cm LVI allowed DCIS allowed ALN positive allowed 5 year follow - up
73
74 ASTRO Recommendations Low risk - APBI outside the context of a clinical trial is an acceptable treatment option High-risk group- APBI is considered C/I Intermediate risk group- APBI is considered acceptable only in the context of prospective clinical trials.
75 Novel methods
76 Permanent breast seed implant Percutaneous insertion of radioactive seeds (palladium-103 ) under US guidance Use of LDR sources has the potential for improving the therapeutic ratio A preplan is generated with optimal seed position and spacing to deliver the prescribed dose of 90 Gy to cover the lumpectomy cavity with a 1.5- cm margin. Using a grid template 103Pd seeds are placed according to the preplan needle and seed distribution.
77
78 Current RTOG / NSABP Trial Phase III randomized comparison of whole breast vs. short-course partial breast XRT Stage 0, I, or II with T<3cm No more than 3 histologically positive nodes Post-surgical CT evaluations of lumpectomy cavity Defined ratios of partial-breast to whole-breast volumes Either interstitial catheters, Mammo Site, or 3D conformal (NOT IMRT) radiotherapy Twice daily for 10 fractions over 5-7 day No data available yet
79 CONCLUSIONS In about 5-8 years, the ongoing studies will hopefully answer the questions related to patient selection, long-term outcome, and toxicity of the different techniques. A modest reduction in initial treatment efficacy cannot be justified in patients with early breast cancer, who have an excellent prognosis with standard BCT including WBI. For now, patients should be carefully selected for APBI and closely followed with accurate documentation of outcomes
80 THANK YOU
ACCELERATED BREAST IRRADIATION EVOLVING PARADIGM FOR TREATMENT OF EARLY STAGE BREAST CANCER
 ACCELERATED BREAST IRRADIATION EVOLVING PARADIGM FOR TREATMENT OF EARLY STAGE BREAST CANCER KHANH NGUYEN, MD, MA DEPARTMENT OF RADIATION ONCOLOGY BAYHEALTH CANCER CENTER BREAST CANCER STATISTICS Most common
ACCELERATED BREAST IRRADIATION EVOLVING PARADIGM FOR TREATMENT OF EARLY STAGE BREAST CANCER KHANH NGUYEN, MD, MA DEPARTMENT OF RADIATION ONCOLOGY BAYHEALTH CANCER CENTER BREAST CANCER STATISTICS Most common
Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w
 Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w Quality assurance Classical implant systems w Manchester
Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w Quality assurance Classical implant systems w Manchester
Brachytherapy Planning and Quality Assurance
 Brachytherapy Planning and Quality Assurance Classical implant systems Most common clinical applications and modern dosimetry methods Quality assurance Classical implant systems Manchester (Paterson-Parker)
Brachytherapy Planning and Quality Assurance Classical implant systems Most common clinical applications and modern dosimetry methods Quality assurance Classical implant systems Manchester (Paterson-Parker)
New Technologies in Radiation Oncology. Catherine Park, MD, MPH Advocate Good Shepherd Hospital
 New Technologies in Radiation Oncology Catherine Park, MD, MPH Advocate Good Shepherd Hospital Breast Radiation Early Stage Breast Cancer Whole Breast Radiation Delivered to the whole breast Boost to the
New Technologies in Radiation Oncology Catherine Park, MD, MPH Advocate Good Shepherd Hospital Breast Radiation Early Stage Breast Cancer Whole Breast Radiation Delivered to the whole breast Boost to the
EARLY STAGE BREAST CANCER AND THE EMERGING ROLE OF IORT
 May 13, 2016 EARLY STAGE BREAST CANCER AND THE EMERGING ROLE OF IORT Presenter: Paul B. Fowler, MD Radiation Oncology, MGSH/MUMH 1 Objectives: 1. List treatment options for early stage breast cancer. 2.
May 13, 2016 EARLY STAGE BREAST CANCER AND THE EMERGING ROLE OF IORT Presenter: Paul B. Fowler, MD Radiation Oncology, MGSH/MUMH 1 Objectives: 1. List treatment options for early stage breast cancer. 2.
Partial Breast Irradiation using adaptive MRgRT
 Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Partial Breast Irradiation for Breast Conserving Therapy
 To Radiate or Not? Is APBI the Right Compromise Solution? Partial Breast Irradiation for Breast Conserving Therapy Julia White MD Professor, Radiation Oncology Agenda Role of radiotherapy in breast conservation
To Radiate or Not? Is APBI the Right Compromise Solution? Partial Breast Irradiation for Breast Conserving Therapy Julia White MD Professor, Radiation Oncology Agenda Role of radiotherapy in breast conservation
Current Status of Accelerated Partial Breast Irradiation. Julia White MD Professor, Radiation Oncology
 Current Status of Accelerated Partial Breast Irradiation Julia White MD Professor, Radiation Oncology I have no disclosures relative to the presented material Agenda ABPI Timeline APBI by Method Clinical
Current Status of Accelerated Partial Breast Irradiation Julia White MD Professor, Radiation Oncology I have no disclosures relative to the presented material Agenda ABPI Timeline APBI by Method Clinical
Breast Conservation Therapy
 May 18, 2018 Breast Conservation Therapy One Treatment No Longer Fits All Presenter: Paul B. Fowler, MD Radiation Oncology, MGSH/MUMH 1 Objectives: 1. Define stages of breast cancer that are candidates
May 18, 2018 Breast Conservation Therapy One Treatment No Longer Fits All Presenter: Paul B. Fowler, MD Radiation Oncology, MGSH/MUMH 1 Objectives: 1. Define stages of breast cancer that are candidates
Evaluation of three APBI techniques under NSABP B-39 guidelines
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 11, NUMBER 1, WINTER 2010 Evaluation of three APBI techniques under NSABP B-39 guidelines Daniel Scanderbeg, a Catheryn Yashar, Greg White, Roger Rice,
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 11, NUMBER 1, WINTER 2010 Evaluation of three APBI techniques under NSABP B-39 guidelines Daniel Scanderbeg, a Catheryn Yashar, Greg White, Roger Rice,
Why Choose Brachytherapy and Not External Beam RT or IORT?
 May 30 31, 2014 Miami Beach, FL USA Why Choose Brachytherapy and Not External Beam RT or IORT? Csaba Polgár, MD, PhD, MSc National Institute of Oncology Budapest, Hungary 1 Disclosure Csaba Polgár, MD,
May 30 31, 2014 Miami Beach, FL USA Why Choose Brachytherapy and Not External Beam RT or IORT? Csaba Polgár, MD, PhD, MSc National Institute of Oncology Budapest, Hungary 1 Disclosure Csaba Polgár, MD,
Intraoperative. Radiotherapy
 Intraoperative Radiotherapy ROBERTO ORECCHIA UNIVERSITY of MILAN & EUROPEAN INSTITUTE of ONCOLOGY & CNAO FOUNDATION Breast Cancer Brescia, 30th September 2011 IORT, very selective technique to intensify
Intraoperative Radiotherapy ROBERTO ORECCHIA UNIVERSITY of MILAN & EUROPEAN INSTITUTE of ONCOLOGY & CNAO FOUNDATION Breast Cancer Brescia, 30th September 2011 IORT, very selective technique to intensify
Brachytherapy: The precise answer for tackling breast cancer. Because life is for living
 Brachytherapy: The precise answer for tackling breast cancer Because life is for living Table of contents Executive summary 3 Introduction 4 Management of early stage breast cancer 5 Radiotherapy options
Brachytherapy: The precise answer for tackling breast cancer Because life is for living Table of contents Executive summary 3 Introduction 4 Management of early stage breast cancer 5 Radiotherapy options
Hypofractionated Radiotherapy for breast cancer: Updated evidence
 2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial
2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial
Carol Marquez, M.D. Department of Radiation Medicine OHSU
 Carol Marquez, M.D. Department of Radiation Medicine OHSU Describe partial breast irradiation (PBI) and discuss why it is being used. Detail methods of performing partial breast irradiation. Explain how
Carol Marquez, M.D. Department of Radiation Medicine OHSU Describe partial breast irradiation (PBI) and discuss why it is being used. Detail methods of performing partial breast irradiation. Explain how
Accelerated Partial Breast Irradiation
 Accelerated Partial Breast Irradiation OSCO/OU Stephenson Cancer Center Saturday, March 5, 2016 Robert Kuske, MD, FAACE Founder, Medical Director Arizona Breast Cancer Specialists Scottsdale, Arizona 1
Accelerated Partial Breast Irradiation OSCO/OU Stephenson Cancer Center Saturday, March 5, 2016 Robert Kuske, MD, FAACE Founder, Medical Director Arizona Breast Cancer Specialists Scottsdale, Arizona 1
Definitions. Brachytherapy in treatment of cancer. Implantation Techniques and Methods of Dose Specifications. Importance of Brachytherapy in GYN
 Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
RADIOTHERAPY IN BREAST CANCER :
 RADIOTHERAPY IN BREAST CANCER : PAST, PRESENT, FUTURE Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Cancer Institute Narayana Superspecialty Hospital Breast cancer is the classic paradigm
RADIOTHERAPY IN BREAST CANCER : PAST, PRESENT, FUTURE Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Cancer Institute Narayana Superspecialty Hospital Breast cancer is the classic paradigm
Objectives Intraoperative Radiation Therapy for Early Stage Breast Cancer
 Objectives Intraoperative Radiation Therapy for Early Stage Breast Cancer Cristina Lopez-Peñalver, MD, FACS October 11, 2014 Disclosures I have no relevant commercial relationships to disclose. Discuss
Objectives Intraoperative Radiation Therapy for Early Stage Breast Cancer Cristina Lopez-Peñalver, MD, FACS October 11, 2014 Disclosures I have no relevant commercial relationships to disclose. Discuss
Quality management for Breast Brachytherapy.
 Quality management for Breast Brachytherapy. DORIN TODOR, Ph.D. Medical College of Virginia Campus Department of Radiation Oncology New England AAPM Chapter 2012 Summer Meeting, Providence, RI Quality
Quality management for Breast Brachytherapy. DORIN TODOR, Ph.D. Medical College of Virginia Campus Department of Radiation Oncology New England AAPM Chapter 2012 Summer Meeting, Providence, RI Quality
Breast Brachytherapy: How to Allay Fears of Patients and Colleagues, and What Are Our Expectations for the Future?
 Breast Brachytherapy: How to Allay Fears of Patients and Colleagues, and What Are Our Expectations for the Future? Vratislav Strnad, MD, PhD, Prof. Department of Radiation Therapy University Hospital Erlangen
Breast Brachytherapy: How to Allay Fears of Patients and Colleagues, and What Are Our Expectations for the Future? Vratislav Strnad, MD, PhD, Prof. Department of Radiation Therapy University Hospital Erlangen
Accelerated Radiation Treatment for Early Stage Breast Cancer. update and perspective
 Accelerated Radiation Treatment for Early Stage Breast Cancer update and perspective School of Breast Oncology Atlanta, 11/2013 Douglas W. Arthur, M.D. Professor Traditional Whole Breast Irradiation WBI
Accelerated Radiation Treatment for Early Stage Breast Cancer update and perspective School of Breast Oncology Atlanta, 11/2013 Douglas W. Arthur, M.D. Professor Traditional Whole Breast Irradiation WBI
IORT What We ve Learned So Far
 IORT What We ve Learned So Far The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation
IORT What We ve Learned So Far The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Accelerated Breast Irradiation and Brachytherapy Boost Page 1 of 27 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Accelerated Breast Irradiation and Brachytherapy
Accelerated Breast Irradiation and Brachytherapy Boost Page 1 of 27 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Accelerated Breast Irradiation and Brachytherapy
NSABP PROTOCOL B-39B RTOG PROTOCOL 0413
 NSABP PROTOCOL B-39B RTOG PROTOCOL 0413 (A RANDOMIZED PHASE III STUDY OF CONVENTIONAL WHOLE BREAST IRRADIATION WBI) VERSUS PARTIAL BREAST IRRADIATION (PBI) FOR WOMEN WITH STAGE 0, I, OR II BREAST CANCER
NSABP PROTOCOL B-39B RTOG PROTOCOL 0413 (A RANDOMIZED PHASE III STUDY OF CONVENTIONAL WHOLE BREAST IRRADIATION WBI) VERSUS PARTIAL BREAST IRRADIATION (PBI) FOR WOMEN WITH STAGE 0, I, OR II BREAST CANCER
Técnicas y tipos de implantes intersticiales. Mauricio Cambeiro Oncología Radioterápica Clínica Universidad de Navarra
 Técnicas y tipos de implantes intersticiales Mauricio Cambeiro Oncología Radioterápica Clínica Universidad de Navarra Multi-catheter Breast Implant (MBI): 1. Brief MBI generalities & classification 2.
Técnicas y tipos de implantes intersticiales Mauricio Cambeiro Oncología Radioterápica Clínica Universidad de Navarra Multi-catheter Breast Implant (MBI): 1. Brief MBI generalities & classification 2.
Advances in Localized Breast Cancer
 Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Pavel ŠLAMPA, Jana RUZICKOVA, Barbora ONDROVA, Hana TICHA, Hana DOLEZELOVA
 Sole conformal perioperative interstitial brachytherapy of early stage breast carcinoma using high-dose rate afterloading: longer-term results and toxicity Received: 0.09.2007 Accepted: 7.02.2008 Subject:
Sole conformal perioperative interstitial brachytherapy of early stage breast carcinoma using high-dose rate afterloading: longer-term results and toxicity Received: 0.09.2007 Accepted: 7.02.2008 Subject:
MEDICAL POLICY MEDICAL POLICY DETAILS POLICY STATEMENT POLICY GUIDELINES. Page: 1 of 10
 Page: 1 of 10 MEDICAL POLICY MEDICAL POLICY DETAILS Medical Policy Title BRACHYTHERAPY AFTER BREAST-CONSERVING SURGERY, AS BOOST WITH WHOLE BREAST IRRADIATION OR ALONE AS ACCELERATED PARTIAL BREAST IRRADIATION
Page: 1 of 10 MEDICAL POLICY MEDICAL POLICY DETAILS Medical Policy Title BRACHYTHERAPY AFTER BREAST-CONSERVING SURGERY, AS BOOST WITH WHOLE BREAST IRRADIATION OR ALONE AS ACCELERATED PARTIAL BREAST IRRADIATION
Consensus Guideline on Accelerated Partial Breast Irradiation
 Consensus Guideline on Accelerated Partial Breast Irradiation Purpose: To outline the use of accelerated partial breast irradiation (APBI) for the treatment of breast cancer. Associated ASBS Guidelines
Consensus Guideline on Accelerated Partial Breast Irradiation Purpose: To outline the use of accelerated partial breast irradiation (APBI) for the treatment of breast cancer. Associated ASBS Guidelines
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Accelerated Breast Irradiation and Brachytherapy Boost Page 1 of 23 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Accelerated Breast Irradiation and Brachytherapy
Accelerated Breast Irradiation and Brachytherapy Boost Page 1 of 23 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Accelerated Breast Irradiation and Brachytherapy
Corporate Medical Policy
 Corporate Medical Policy Breast Brachytherapy for Accelerated Partial Breast Radiotherapy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: breast_brachytherapy_for_accelerated_partial_breast_radiotherapy
Corporate Medical Policy Breast Brachytherapy for Accelerated Partial Breast Radiotherapy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: breast_brachytherapy_for_accelerated_partial_breast_radiotherapy
Recent Advances in Breast Radiotherapy
 Recent Advances in Breast Radiotherapy Dr Anna Kirby Consultant Clinical Oncologist 2 The Royal Marsden Overview: Key innovations 1. 2D to 3D planning 2. Hypofractionation 3. Intensity modulated radiotherapy
Recent Advances in Breast Radiotherapy Dr Anna Kirby Consultant Clinical Oncologist 2 The Royal Marsden Overview: Key innovations 1. 2D to 3D planning 2. Hypofractionation 3. Intensity modulated radiotherapy
Treatment Planning for Breast Cancer: Contouring Targets. Julia White MD Professor
 Treatment Planning for Breast Cancer: Contouring Targets Julia White MD Professor Outline 1. RTOG Breast Cancer Atlas 2. Target development on Clinical Trials Whole Breast Irradiation 2-D Radiotherapy
Treatment Planning for Breast Cancer: Contouring Targets Julia White MD Professor Outline 1. RTOG Breast Cancer Atlas 2. Target development on Clinical Trials Whole Breast Irradiation 2-D Radiotherapy
Clinical outcomes of patients treated with accelerated partial breast irradiation with high-dose rate brachytherapy: Scripps Clinic experience
 Original Article Clinical outcomes of patients treated with accelerated partial breast irradiation with high-dose rate brachytherapy: Scripps Clinic experience Rachel Murray 1, Fantine Giap 2, Ray Lin
Original Article Clinical outcomes of patients treated with accelerated partial breast irradiation with high-dose rate brachytherapy: Scripps Clinic experience Rachel Murray 1, Fantine Giap 2, Ray Lin
By Rufus Mark, MD, Gail Lebovic, MD, Valerie Gorman, MD, Oscar Calvo, PhD. TABLE 1 EARLY STAGE BREAST CANCER RANDOMIZED TRIALS M vs.
 EVOLUTION OF BREAST CONSERVATION RADIATION TREATMENT TECHNIQUES IN BREAST CANCER : FROM 6 WEEKS TO 3 WEEKS TO 1 WEEK TO 1 DAY AND FROM WHOLE BREAST TO PARTIAL BREAST By Rufus Mark, MD, Gail Lebovic, MD,
EVOLUTION OF BREAST CONSERVATION RADIATION TREATMENT TECHNIQUES IN BREAST CANCER : FROM 6 WEEKS TO 3 WEEKS TO 1 WEEK TO 1 DAY AND FROM WHOLE BREAST TO PARTIAL BREAST By Rufus Mark, MD, Gail Lebovic, MD,
How ICD-10 Affects Radiation Oncology. Presented by, Lashelle Bolton CPC, COC, CPC-I, CPMA
 How ICD-10 Affects Radiation Oncology Presented by, Lashelle Bolton CPC, COC, CPC-I, CPMA ICD-10 ICD-10-CM has added new challenges to the radiation oncology specialty. Approximately 220 ICD-9-CM codes
How ICD-10 Affects Radiation Oncology Presented by, Lashelle Bolton CPC, COC, CPC-I, CPMA ICD-10 ICD-10-CM has added new challenges to the radiation oncology specialty. Approximately 220 ICD-9-CM codes
Accelerated Partial Breast Irradiation: Potential Roles Following Breast-Conserving Surgery
 APBI is a promising technique in selected patients with early-stage breast cancer, but further study is needed on outcome and toxicity associated with this approach. Nick Patten. Passing Light (detail).
APBI is a promising technique in selected patients with early-stage breast cancer, but further study is needed on outcome and toxicity associated with this approach. Nick Patten. Passing Light (detail).
MEDICAL POLICY. POLICY NUMBER: CATEGORY: Technology Assessment. Proprietary Information of Excellus Health Plan, Inc.
 MEDICAL POLICY SUBJECT: BRACHYTHERAPY AFTER BREAST- WHOLE BREAST OR ALONE PAGE: 1 OF: 8 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial
MEDICAL POLICY SUBJECT: BRACHYTHERAPY AFTER BREAST- WHOLE BREAST OR ALONE PAGE: 1 OF: 8 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial
Nitesh N. Paryani, M.D. First Radiation & Oncology Group Instructor of Radiation Oncology, Mayo Clinic Courtesy Professor, University of Florida
 Nitesh N. Paryani, M.D. First Radiation & Oncology Group Instructor of Radiation Oncology, Mayo Clinic Courtesy Professor, University of Florida I Invasive Breast Brachytherapy Non-invasive Image-guided
Nitesh N. Paryani, M.D. First Radiation & Oncology Group Instructor of Radiation Oncology, Mayo Clinic Courtesy Professor, University of Florida I Invasive Breast Brachytherapy Non-invasive Image-guided
Accelerated Partial Breast Irradiation (APBI)
") Accelerated Partial Breast Irradiation (APBI) Michael Zhang (MSIV), Matthew Spraker, MD, PhD (PGY3) Faculty Mentor: Janice Kim, MD University of Washington/Seattle Cancer Care Alliance Seattle, WA Case
Accelerated Partial Breast Irradiation (APBI) Michael Zhang (MSIV), Matthew Spraker, MD, PhD (PGY3) Faculty Mentor: Janice Kim, MD University of Washington/Seattle Cancer Care Alliance Seattle, WA Case
Breast Cancer Radiotherapy: Clinical challenges in 2011 from a European Perspective. Dr DA WHEATLEY CONSULTANT ONCOLOGIST ROYAL CORNWALL HOSPITAL
 Breast Cancer Radiotherapy: Clinical challenges in 2011 from a European Perspective Dr DA WHEATLEY CONSULTANT ONCOLOGIST ROYAL CORNWALL HOSPITAL Radiotherapy in Early Breast Cancer Why do we do it? Who
Breast Cancer Radiotherapy: Clinical challenges in 2011 from a European Perspective Dr DA WHEATLEY CONSULTANT ONCOLOGIST ROYAL CORNWALL HOSPITAL Radiotherapy in Early Breast Cancer Why do we do it? Who
Surgical Advances in the Treatment of Breast Cancer. Laura Kruper, MD, MSCE Chief, Breast Surgery
 Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Accelerated Radiation Treatment for Early Stage Breast Cancer. update and perspective
 Accelerated Radiation Treatment for Early Stage Breast Cancer update and perspective School of Breast Oncology Atlanta, 11/2012 Douglas W. Arthur, M.D. Professor Traditional Whole Breast Irradiation WBI
Accelerated Radiation Treatment for Early Stage Breast Cancer update and perspective School of Breast Oncology Atlanta, 11/2012 Douglas W. Arthur, M.D. Professor Traditional Whole Breast Irradiation WBI
Brachytherapy is better than external beam therapy for partial breast irradiation
 Brachytherapy is better than external beam therapy for partial breast irradiation For the proposition: Dorin Todor Virginia Commonwealth University, Richmond, VA AAPM 55 th Annual Meeting, Indianapolis,
Brachytherapy is better than external beam therapy for partial breast irradiation For the proposition: Dorin Todor Virginia Commonwealth University, Richmond, VA AAPM 55 th Annual Meeting, Indianapolis,
Protocol of Radiotherapy for Breast Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Breast Cancer Indication of radiotherapy Indications for Post-Mastectomy Radiotherapy (1) Axillary lymph node 4 positive (2) Axillary lymph node 1-3 positive:
107 年 12 月修訂 Protocol of Radiotherapy for Breast Cancer Indication of radiotherapy Indications for Post-Mastectomy Radiotherapy (1) Axillary lymph node 4 positive (2) Axillary lymph node 1-3 positive:
POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT VARIATIONS DISCLAIMER CODING INFORMATION REFERENCES POLICY HISTORY
 - Original Issue Date (Created): November 22, 2011 Most Recent Review Date (Revised): May 20, 2014 Effective Date: October 1, 2014 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS
- Original Issue Date (Created): November 22, 2011 Most Recent Review Date (Revised): May 20, 2014 Effective Date: October 1, 2014 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS
Accelerated Partial Breast Irradiation FACTS & MYTHS
 Accelerated Partial Breast Irradiation (APBI) Accelerated Partial Breast Irradiation FACTS & MYTHS V.Strnad Radiation options after breast conserving surgery Whole Breast Irradiation (EBRT) APBI technique
Accelerated Partial Breast Irradiation (APBI) Accelerated Partial Breast Irradiation FACTS & MYTHS V.Strnad Radiation options after breast conserving surgery Whole Breast Irradiation (EBRT) APBI technique
September 9, IORT Shows Promise in Early Use
 An actual intraoperative delivery; a Xoft unit is attached to a balloon ready for treatment. September 9, 2011 IORT Shows Promise in Early Use A look at techniques and appropriate uses for this emerging
An actual intraoperative delivery; a Xoft unit is attached to a balloon ready for treatment. September 9, 2011 IORT Shows Promise in Early Use A look at techniques and appropriate uses for this emerging
Principles of breast radiation therapy
 ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
Health technology description. Key points. Epidemiology. Clinical effectiveness
 In response to an enquiry from the Scottish Radiotherapy Advisory Group Number 35 May 2011 N The clinical and cost effectiveness of the use of brachytherapy to treat breast cancer Health technology description
In response to an enquiry from the Scottish Radiotherapy Advisory Group Number 35 May 2011 N The clinical and cost effectiveness of the use of brachytherapy to treat breast cancer Health technology description
Predicting Maximum Pacemaker/ICD Dose in SAVI HDR Brachytherapy
 Predicting Maximum Pacemaker/ICD Dose in SAVI HDR Brachytherapy Chaitanya Kalavagunta Ph.D. University of Maryland School of Medicine, Baltimore, Maryland. Background Aging population - Number of patients
Predicting Maximum Pacemaker/ICD Dose in SAVI HDR Brachytherapy Chaitanya Kalavagunta Ph.D. University of Maryland School of Medicine, Baltimore, Maryland. Background Aging population - Number of patients
Intra operative Intrabeam radiation for breast cancer
 Intra operative Intrabeam radiation for breast cancer Dr Gillian Campbell Radiation Oncologist May 2018 Disclaimer/Conflicts I am a radiation oncology consultant at Christchurch Hospital, Canterbury Breast
Intra operative Intrabeam radiation for breast cancer Dr Gillian Campbell Radiation Oncologist May 2018 Disclaimer/Conflicts I am a radiation oncology consultant at Christchurch Hospital, Canterbury Breast
Brachytherapy an Overview
 Brachytherapy an Overview Yakov Pipman, D Sc North Shore LIJ Health System Monterrey, Nov30-Dec1, 2007 Brachytherapy A procedure in therapeutic radiology that involves the irradiation of a target with
Brachytherapy an Overview Yakov Pipman, D Sc North Shore LIJ Health System Monterrey, Nov30-Dec1, 2007 Brachytherapy A procedure in therapeutic radiology that involves the irradiation of a target with
Surgery for Breast Cancer
 Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Accelerated Partial Breast Irradiation: A Review and Description of an Early North American Surgical Experience With the Intrabeam Delivery System
 A variety of techniques for accelerated partial breast irradiation are available. Photo courtesy of Lisa Scholder. Hidden Power, 24ʺ 28ʺ. Accelerated Partial Breast Irradiation: A Review and Description
A variety of techniques for accelerated partial breast irradiation are available. Photo courtesy of Lisa Scholder. Hidden Power, 24ʺ 28ʺ. Accelerated Partial Breast Irradiation: A Review and Description
Brachytherapy. What is brachytherapy and how is it used?
 Scan for mobile link. Brachytherapy Brachytherapy places radioactive sources inside the patient on a temporary or permanent basis to damage cancer cells DNA and destroy their ability to divide and grow.
Scan for mobile link. Brachytherapy Brachytherapy places radioactive sources inside the patient on a temporary or permanent basis to damage cancer cells DNA and destroy their ability to divide and grow.
Clinical Applications of Brachytherapy Radiobiology. Radiobiology is Essential
 Clinical Applications of Brachytherapy Radiobiology Dr Alexandra Stewart University of Surrey St Luke s Cancer Centre Guildford, England Radiobiology is Essential Knowledge of radiobiological principles
Clinical Applications of Brachytherapy Radiobiology Dr Alexandra Stewart University of Surrey St Luke s Cancer Centre Guildford, England Radiobiology is Essential Knowledge of radiobiological principles
COMMENTARY. Workshop on Partial Breast Irradiation: State of the Art and the Science, Bethesda, MD, December 8 10, 2002
 COMMENTARY Workshop on Partial Breast Irradiation: State of the Art and the Science, Bethesda, MD, December 8 10, 2002 P. Wallner, D. Arthur, H. Bartelink, J. Connolly, G. Edmundson, A. Giuliano, N. Goldstein,
COMMENTARY Workshop on Partial Breast Irradiation: State of the Art and the Science, Bethesda, MD, December 8 10, 2002 P. Wallner, D. Arthur, H. Bartelink, J. Connolly, G. Edmundson, A. Giuliano, N. Goldstein,
Comparison of two techniques of interstitial pulsed dose rate boost brachytherapy in conservative treatment of breast cancer
 Original article Original articles Comparison of two techniques of interstitial pulsed dose rate boost brachytherapy in conservative treatment of breast cancer Krystyna Serkies, MD, PhD 1, Zofia Tarnawska,
Original article Original articles Comparison of two techniques of interstitial pulsed dose rate boost brachytherapy in conservative treatment of breast cancer Krystyna Serkies, MD, PhD 1, Zofia Tarnawska,
doi: /j.ijrobp
 doi:10.1016/j.ijrobp.2009.12.047 Int. J. Radiation Oncology Biol. Phys., Vol. 79, No. 4, pp. 977 984, 2011 Copyright Ó 2011 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/$ see front matter
doi:10.1016/j.ijrobp.2009.12.047 Int. J. Radiation Oncology Biol. Phys., Vol. 79, No. 4, pp. 977 984, 2011 Copyright Ó 2011 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/$ see front matter
Breast Cancer. What is breast cancer?
 Scan for mobile link. Breast Cancer Breast cancer is a malignant tumor in or around breast tissue. It usually begins as a lump or calcium deposit that develops from abnormal cell growth. Most breast lumps
Scan for mobile link. Breast Cancer Breast cancer is a malignant tumor in or around breast tissue. It usually begins as a lump or calcium deposit that develops from abnormal cell growth. Most breast lumps
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Beam Direction RAO LAO. Pt supine. LL Treatment couch LPO RPO. WHA Consulting. Wilson Apollo
 Beam Direction AP RAO LAO Pt supine RL LL Treatment couch RPO LPO PA Wilson Apollo DELIVERY TECHNOLOGY & CODING Based on FORDS Manual Equipment Dose Delivery Method Modality Code Comments Zeiss Intrabeam
Beam Direction AP RAO LAO Pt supine RL LL Treatment couch RPO LPO PA Wilson Apollo DELIVERY TECHNOLOGY & CODING Based on FORDS Manual Equipment Dose Delivery Method Modality Code Comments Zeiss Intrabeam
Recent Advances in Breast Cancer Treatment
 Recent Advances in Breast Cancer Treatment Pornchai O-charoenrat MD, PhD, FRCST, FICS Professor Chief, Division of Head-Neck & Breast Surgery Department of Surgery, Siriraj Hospital, THAILAND Recent Advances
Recent Advances in Breast Cancer Treatment Pornchai O-charoenrat MD, PhD, FRCST, FICS Professor Chief, Division of Head-Neck & Breast Surgery Department of Surgery, Siriraj Hospital, THAILAND Recent Advances
Accelerated Partial Breast Irradiation and Hypofractionated Whole Breast Radiation
 Accelerated Partial Breast Irradiation and Hypofractionated Whole Breast Radiation Bryan P Rowe, MD 1 and Meena S Moran, MD 2 1. Resident; 2. Associate Professor, Department of Therapeutic Radiology, Yale
Accelerated Partial Breast Irradiation and Hypofractionated Whole Breast Radiation Bryan P Rowe, MD 1 and Meena S Moran, MD 2 1. Resident; 2. Associate Professor, Department of Therapeutic Radiology, Yale
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006
 Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Accurate Accurate boost or Simply Accuboost
 Accurate Accurate boost or Simply Accuboost Zoubir Ouhib MS DABR Lynn Cancer Institute of Boca Raton Community Hospital Disclosure: Advisory board Items to be discussed Big picture on management of Breast
Accurate Accurate boost or Simply Accuboost Zoubir Ouhib MS DABR Lynn Cancer Institute of Boca Raton Community Hospital Disclosure: Advisory board Items to be discussed Big picture on management of Breast
NIA MAGELLAN HEALTH RADIATION ONCOLOGY CODING STANDARD. Dosimetry Planning
 NIA MAGELLAN HEALTH RADIATION ONCOLOGY CODING STANDARD Dosimetry Planning CPT Codes: 77295, 77300, 77301, 77306, 77307, 77321, 77316, 77317, 77318, 77331, 77399 Original Date: April, 2011 Last Reviewed
NIA MAGELLAN HEALTH RADIATION ONCOLOGY CODING STANDARD Dosimetry Planning CPT Codes: 77295, 77300, 77301, 77306, 77307, 77321, 77316, 77317, 77318, 77331, 77399 Original Date: April, 2011 Last Reviewed
Patient Selection for APBI. C. Polgár National Institute ofoncology, Budapest, Hungary
 Patient Selection for APBI C. Polgár National Institute ofoncology, Budapest, Hungary Patient-, tumour- and treatment related factors affecting decision making in patient selection for APBI Patient age
Patient Selection for APBI C. Polgár National Institute ofoncology, Budapest, Hungary Patient-, tumour- and treatment related factors affecting decision making in patient selection for APBI Patient age
BREAST CANCER IOeRT RATIONALE
 BREAST CANCER IOeRT RATIONALE Approximately 80% of the breast tumor recurrences origins at the site of the original disease. These data suggest that the majority of breast tumor recurrences result from
BREAST CANCER IOeRT RATIONALE Approximately 80% of the breast tumor recurrences origins at the site of the original disease. These data suggest that the majority of breast tumor recurrences result from
Limitations. General Clinical Applications of Brachytherapy Physics. Learning Objectives. Conflicts of Interest. University of Wisconsin - Madison
 General Clinical Applications of Brachytherapy Physics Bruce Thomadsen Limitations Due to file size limitations for this handout, many of the figures have had to be removed. I apologize for the lack of
General Clinical Applications of Brachytherapy Physics Bruce Thomadsen Limitations Due to file size limitations for this handout, many of the figures have had to be removed. I apologize for the lack of
Radiotherapy Physics and Equipment
 Radiological Sciences Department Radiotherapy Physics and Equipment RAD 481 Lecture s Title: Introduction Dr. Mohammed EMAM Ph.D., Paris-Sud 11 University Vision :IMC aspires to be a leader in applied
Radiological Sciences Department Radiotherapy Physics and Equipment RAD 481 Lecture s Title: Introduction Dr. Mohammed EMAM Ph.D., Paris-Sud 11 University Vision :IMC aspires to be a leader in applied
The Case FOR Oncoplastic Surgery in Small Breasts. Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA
 The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
AccuBoost non invasive, real-time, image guided breast boosting
 AccuBoost non invasive, real-time, image guided breast boosting A new treatment option for the boost dose as part of the Whole Breast Irradiation treatment after breast cancer AccuBoost is a new system
AccuBoost non invasive, real-time, image guided breast boosting A new treatment option for the boost dose as part of the Whole Breast Irradiation treatment after breast cancer AccuBoost is a new system
 https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
Slide 1. Slide 2. Slide 3 History of Nurse Navigator
 Slide 1 The Nurse Navigators role in Early Stage Breast Cancer, and Development of Tailored Treatment Plan Laura Ochoa, RN, ANP-BC, Ph.D. Slide 2 Barnes Jewish Hospital at Washington University Slide 3
Slide 1 The Nurse Navigators role in Early Stage Breast Cancer, and Development of Tailored Treatment Plan Laura Ochoa, RN, ANP-BC, Ph.D. Slide 2 Barnes Jewish Hospital at Washington University Slide 3
3D Conformal Radiation Therapy for Mucinous Carcinoma of the Breast
 1 Angela Kempen February Case Study February 22, 2012 3D Conformal Radiation Therapy for Mucinous Carcinoma of the Breast History of Present Illness: JE is a 45 year-old Caucasian female who underwent
1 Angela Kempen February Case Study February 22, 2012 3D Conformal Radiation Therapy for Mucinous Carcinoma of the Breast History of Present Illness: JE is a 45 year-old Caucasian female who underwent
2015 Radiology Coding Survival Guide
 2015 Radiology Coding Survival Guide Chapter 31: Clinical Brachytherapy (77750-77799) Clinical brachytherapy involves applying radioelements into or around a treatment field. CPT guidelines clarify that
2015 Radiology Coding Survival Guide Chapter 31: Clinical Brachytherapy (77750-77799) Clinical brachytherapy involves applying radioelements into or around a treatment field. CPT guidelines clarify that
Chapter 9 Radiotherapy A New Approach to Risk- Adapted Selective Radiotherapy
 Chapter 9 Radiotherapy A New Approach to Risk- Adapted Selective Radiotherapy Csaba Polgár 9.1 Introduction During the last forty years, breast-conserving surgery (BCS) followed by whole breast irradiation
Chapter 9 Radiotherapy A New Approach to Risk- Adapted Selective Radiotherapy Csaba Polgár 9.1 Introduction During the last forty years, breast-conserving surgery (BCS) followed by whole breast irradiation
Breast Cancer. What is breast cancer?
 Scan for mobile link. Breast Cancer Breast cancer is a malignant tumor in or around breast tissue. It usually begins as a lump or calcium deposit that develops from abnormal cell growth. Most breast lumps
Scan for mobile link. Breast Cancer Breast cancer is a malignant tumor in or around breast tissue. It usually begins as a lump or calcium deposit that develops from abnormal cell growth. Most breast lumps
Intraoperative radiotherapy for breast cancer. Information for patients on IORT boost treatment
 Intraoperative radiotherapy for breast cancer Information for patients on IORT boost treatment 1 No reason for despair Patients go through a period of great anxiety and apprehension when breast cancer
Intraoperative radiotherapy for breast cancer Information for patients on IORT boost treatment 1 No reason for despair Patients go through a period of great anxiety and apprehension when breast cancer
How can surgeons help the Radiation Oncologists?
 How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
Who Should Know Radiation Oncology Coding?
 Why Should We Learn Radiation Oncology Coding? Terry Wu, Ph.D. Chief Physicist Radiation Oncology Department Willis-Knighton Cancer Center Who Should Know Radiation Oncology Coding? Radiation Oncologist
Why Should We Learn Radiation Oncology Coding? Terry Wu, Ph.D. Chief Physicist Radiation Oncology Department Willis-Knighton Cancer Center Who Should Know Radiation Oncology Coding? Radiation Oncologist
3D CONFORMATIONAL INTERSTITIAL BRACHYTHERAPY PLANNING FOR SOFT TISSUE SARCOMA
 3D CONFORMATIONAL INTERSTITIAL BRACHYTHERAPY PLANNING FOR SOFT TISSUE SARCOMA Alina TĂNASE 1,3, M. DUMITRACHE 2,3, O. FLOREA 1 1 Emergency Central Military Hospital Dr. Carol Davila Bucharest, Romania,
3D CONFORMATIONAL INTERSTITIAL BRACHYTHERAPY PLANNING FOR SOFT TISSUE SARCOMA Alina TĂNASE 1,3, M. DUMITRACHE 2,3, O. FLOREA 1 1 Emergency Central Military Hospital Dr. Carol Davila Bucharest, Romania,
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005 Advantages of inflatable multichannel endorectal applicator in the neo-adjuvant treatment of patients with locally advanced
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005 Advantages of inflatable multichannel endorectal applicator in the neo-adjuvant treatment of patients with locally advanced
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Trends in the Use of Implantable Accelerated Partial Breast Irradiation Therapy for Early Stage Breast Cancer in the United States
 Trends in the Use of Implantable Accelerated Partial Breast Irradiation Therapy for Early Stage Breast Cancer in the United States A THESIS SUBMITTED TO THE FACULTY OF THE GRADUATE SCHOOL OF THE UNIVERSITY
Trends in the Use of Implantable Accelerated Partial Breast Irradiation Therapy for Early Stage Breast Cancer in the United States A THESIS SUBMITTED TO THE FACULTY OF THE GRADUATE SCHOOL OF THE UNIVERSITY
Whole Breast Irradiation: Class vs. Hypofractionation
 Whole Breast Irradiation: Class vs. Hypofractionation Kyung Hwan Shin, MD, PhD. Dept. of Radiation Oncology, Seoul National University Hospital 2018. 4. 6. GBCC Treatment Trends of Early Breast Cancer
Whole Breast Irradiation: Class vs. Hypofractionation Kyung Hwan Shin, MD, PhD. Dept. of Radiation Oncology, Seoul National University Hospital 2018. 4. 6. GBCC Treatment Trends of Early Breast Cancer
Advances in Breast Cancer Diagnosis and Treatment. Heidi Memmel, MD FACS Surgical Director of Caldwell Breast Center September 26, 2015
 Advances in Breast Cancer Diagnosis and Treatment Heidi Memmel, MD FACS Surgical Director of Caldwell Breast Center September 26, 2015 Advances in Breast Cancer Diagnosis and Treatment Recommendations
Advances in Breast Cancer Diagnosis and Treatment Heidi Memmel, MD FACS Surgical Director of Caldwell Breast Center September 26, 2015 Advances in Breast Cancer Diagnosis and Treatment Recommendations
Electronics X-ray Sources for Brachytherapy
 Electronics X-ray Sources for Brachytherapy Mieczysław Słapa, Marek Traczyk, Marcin Talejko, Krzysztof Wincel, Barbara Zaręba The Andrzej Sołtan Institute for Nuclear Studies Department of Physics Applications
Electronics X-ray Sources for Brachytherapy Mieczysław Słapa, Marek Traczyk, Marcin Talejko, Krzysztof Wincel, Barbara Zaręba The Andrzej Sołtan Institute for Nuclear Studies Department of Physics Applications
FEE RULES RADIATION ONCOLOGY FEE SCHEDULE CONTENTS
 Tel: +27-21-9494060 Fax: +27-21-9494112 E-mail: leon.gouws@cancercare.co.za FEE RULES RADIATION ONCOLOGY FEE SCHEDULE CONTENTS 1. EXTERNAL BEAM RADIATION... 2 2. PLANNING OF TREATMENT... 2 3. DELIVERY
Tel: +27-21-9494060 Fax: +27-21-9494112 E-mail: leon.gouws@cancercare.co.za FEE RULES RADIATION ONCOLOGY FEE SCHEDULE CONTENTS 1. EXTERNAL BEAM RADIATION... 2 2. PLANNING OF TREATMENT... 2 3. DELIVERY
Dosimetric evaluation of multilumen intracavitary balloon applicator rotation in high-dose-rate brachytherapy for breast cancer
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 15, NUMBER 1, 2014 Dosimetric evaluation of multilumen intracavitary balloon applicator rotation in high-dose-rate brachytherapy for breast cancer Yongbok
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 15, NUMBER 1, 2014 Dosimetric evaluation of multilumen intracavitary balloon applicator rotation in high-dose-rate brachytherapy for breast cancer Yongbok
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
Accelerated partial breast irradiation: state of the art
 Accelerated partial breast irradiation: state of the art P.A. Coucke, N. Jansen, L. Jánváry, C. Louis, J. Vanderick, A. Rorive, J. Collignon, E. Lifrange, S. Maweja, G. Jerusalem Accelerated partial breast
Accelerated partial breast irradiation: state of the art P.A. Coucke, N. Jansen, L. Jánváry, C. Louis, J. Vanderick, A. Rorive, J. Collignon, E. Lifrange, S. Maweja, G. Jerusalem Accelerated partial breast
Radiation and DCIS. The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging
 Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
BRACHYTHERAPY IN HEAD & NECK CANCERS DR. GIRI G.V.
 BRACHYTHERAPY IN HEAD & NECK CANCERS DR. GIRI G.V. BASICS High dose to tumor = local control Spare normal structures i.e. salivary gland, mandible and muscles of mastication. Seed 100 Relative dose 10
BRACHYTHERAPY IN HEAD & NECK CANCERS DR. GIRI G.V. BASICS High dose to tumor = local control Spare normal structures i.e. salivary gland, mandible and muscles of mastication. Seed 100 Relative dose 10
Non-Invasive Brachytherapy of the Breast
 Non-Invasive Brachytherapy of the Breast New England AAPM Meeting February 15, 2006 Piran Sioshansi, Ph.D. Raymond Bricault Presentation Outline Breast radiotherapy facts and data Shortcomings in current
Non-Invasive Brachytherapy of the Breast New England AAPM Meeting February 15, 2006 Piran Sioshansi, Ph.D. Raymond Bricault Presentation Outline Breast radiotherapy facts and data Shortcomings in current