Multimodality therapy for a case of neuroendocrine tumor in the hilum with multiple hepatic metastases
|
|
|
- Stephen Benson
- 5 years ago
- Views:
Transcription
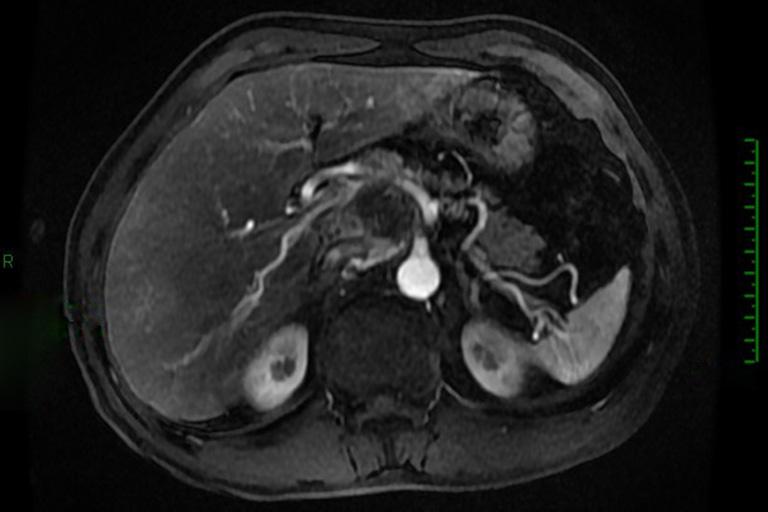
1 Case Report Multimodality therapy for a case of neuroendocrine tumor in the hilum with multiple hepatic metastases Yuan Li, Zhen Huang, Yefan Zhang, Hong Zhao Department of bdominal Surgery, Cancer Institute & Hospital, Chinese cademy of Medical Science and Peking Union Medical College, eijing , China Correspondence to: Hong Zhao. Department of bdominal Surgery, Cancer Institute & Hospital, Chinese cademy of Medical Science and Peking Union Medical College, eijing , China. pumczhaohong@126.com. bstract: This article reports a male mid-aged patient with a rare neuroendocrine tumor in hepatic hilum who finally received surgical treatment after multidisciplinary treatment (MDT). fter the condition was confirmed, the patient received sandostatin treatment based on MDT consultations and his family s willingness due to the high surgical risk. One year later, follow-up examinations showed stable disease (SD), and sandostatin was withdrawn due to economic consideration. One year after drug withdrawal, liver metastases were found. Sutent treatment was then applied after a second MDT consultation. Four months later, further examinations showed a partial response (PR). Finally, the patient received surgical treatment in the department of surgery. Keywords: Neuroendocrine tumor in hilar; hepatic metastases; multidisciplinary treatment (MDT) Received: 18 ugust 2016; ccepted: 09 October 2016; Published: 29 October doi: /tgh View this article at: rief disease history 45-year-old male patient was admitted to the department of surgery due to confirmed hilar neuroendocrine tumor for 30 months and liver metastasis for 4 months. The patient had a history of hypertension for over 10 years. In recent years his blood pressure remarkably increased and had become difficult to control. Physical examination showed a palpable mass in right upper abdomen. The mass was about 4-cm in diameter, with firm texture and moderate activity. The disease course is showed in Figure 1. uxiliary examination Positron emission tomography (PET)-CT (May 26, 2011) hilar tumor, with increased metabolism. malignancy was considered. SUVmax nodule was located deep in the right upper side of the neck, along with increase metabolism. malignancy was highly possible. iopsy was required (biopsy was performed on ugust 1, 2014, which showed that the lesion was inflammation). PET-CT images were showed in Figure 2. Contrast-enhanced CT (June 8, 2012) n irregular hilar mass extended towards the peritoneum and had poor borders with the caudate lobe of liver, left lobe of liver, and pancreatic head. It was adjacent to the inferior vena cava and the celiac trunk and sized 6.8 cm 5.6 cm, showing heterogeneous enhancement. The size was similar to that in previous imaging. CT images were showed in Figure 3. Contrast-enhanced CT (June 29, 2013) n irregular hilar mass sized 6.8 cm 5.6 cm, which was similar to that in previous imaging. In the right lobe of liver there were two new masses with blurred margins. The larger one had a longest diameter of 4.3 cm. Metastases were considered. CT images were showed in Figure 4. Translational Gastroenterology and Hepatology. ll rights reserved. tgh.amegroups.com




2 Page 2 of 9 Translational Gastroenterology and Hepatology, 2016 Puncture biopsy showed the presence of a G2 neuroendocrine tumor Sandostatin 20 mg im, once monthly Drug withdrawal due to economic consideration Sutent 37.5 mg Qd Detection of a hilar mass Feb, 2011 Jun, 2011 Jul, 2011 Jul, 2012 Jun, 2013 Dec, 2013 SRS: the somatostatin receptor was highly expressed in hilum and in right cervical lymph nodes PET-CT: a hilar mass sized 6.7 cm 5.6 cm with high metabolism; high metabolism was also detected in right cervical lymph nodes second examination showed that the hilar tumor had no obvious change CT: a hilar mass sized 6.8 cm 5.6 cm was found. two new tumors were seen in the right lobe of liver; the larger one was sized about 4.3 cm, and metastasis was considered MRI: a hilar mass sized 4.8 cm 4.0 cm was found; the two masses in the right lobe of liver persisted; the larger one had a longest diameter of 3.8 cm, which was smaller than before Figure 1 rief of disease course. Figure 2 Initial PET-CT scan. Figure 3 CT scan after sandostatin therapy for 1 year. Translational Gastroenterology and Hepatology. ll rights reserved. tgh.amegroups.com
 n irregular hilar mass sized 6.0 cm 4.9 cm, which was slightly smaller than that in previous imaging.")
 n irregular hilar mass sized 4.9 cm 4.9 cm, which was similar to that in previous imaging.")
 fusion mass in the hilar area and the head of pancreas. It was sized 4.0 cm 4.8 cm, with blurred margin and heterogeneous enhancement.")

3 Translational Gastroenterology and Hepatology, 2016 Page 3 of 9 Figure 4 CT scan after sandostatin withdrawal. Figure 5 CT scan after Sutent therapy for 1 month. Contrast-enhanced CT (ugust 22, 2013) n irregular hilar mass sized 6.0 cm 4.9 cm, which was slightly smaller than that in previous imaging. The two masses in the right lobe of liver persisted; the larger one had a longest diameter of 3.8 cm, which was also smaller than before. CT images were showed in Figure 5. Contrast-enhanced CT (October 29, 2013) n irregular hilar mass sized 4.9 cm 4.9 cm, which was similar to that in previous imaging. mong the two masses in the right lobe of liver, the larger one had a longest diameter of about 3.9 cm; although it more rounded than before, the degree of enhancement decreased. CT images were showed in Figure 6. MRI (December 11, 2013) fusion mass in the hilar area and the head of pancreas. It was sized 4.0 cm 4.8 cm, with blurred margin and heterogeneous enhancement. malignancy was considered. Multiple nodules and tumors were seen in the liver. The largest one was sized about 2.4 cm 3.4 cm, with blurred margin and circular enhancement. Multiple metastases were considered. MRI were showed in Figure 7. ased on the above findings, the following diagnoses were made: a hilar neuroendocrine tumor with multiple liver metastases; and, hypertension. s shown in the imaging, although there were liver metastases, the tumor was still believed to be resectable. The patient underwent surgical operation on January 6, Intraoperative exploration showed a hilar tumor sized 8.0 cm 10.0 cm. The main body of the tumor was located on the left side of the hepatoduodenal ligament, whereas part of the tumor passed through the back side of the hepatoduodenal ligament to reach the right side of common bile duct. The upper border of the tumor was closely attached to the liver surface, invading the inferior vena cava; its inferior margin surrounded the common hepatic artery; and, its left margin reached the left side of the left gastric vessel. Multiple liver metastases were seen. The largest one was located in hepatic segment VIII and at the border between segment VII and VIII, with a diameter of about 5 cm. Multiple nodules (about 0.5 cm in diameter) were observed on liver surface. Intraoperative photos were showed in Figure 8. No metastasis to other organ or Translational Gastroenterology and Hepatology. ll rights reserved. tgh.amegroups.com







4 Page 4 of 9 Translational Gastroenterology and Hepatology, 2016 Figure 6 CT scan after Sutent therapy for 3 months. C D E F Figure 7 MR scan after Sutent therapy for 4 months. Translational Gastroenterology and Hepatology. ll rights reserved. tgh.amegroups.com


5 Translational Gastroenterology and Hepatology, 2016 Page 5 of 9 Figure 8 Intraoperative photos. () Liver metastases; () a hilar tumor. abdominal and pelvic implantation metastasis was observed. The surgical procedure performed was resection of hilar tumor and multiple liver metastases. Compression of the tumor during the surgery caused the fluctuation of blood pressure, which ranged between 200/100 and 70/40 mmhg. The heart rate fluctuated between 130 and 70 beats/min. Pheochromocytoma was highly suspected. Noradrenaline was applied to maintain blood pressure before the transection of tumor vessels. The blood loss was 800 ml. Thus, 400 ml of red cell suspension and 200 ml of plasma were tranfused. fter the surgery, norepinephrine (NE) was pumped to increase blood pressure following initial volume expansion (IVE) and rehydration. The recovery was smooth. Post-operative pathology Pathological diagnosis: based on the morphology, immunohistochemical findings, and clinical manifestations, a diagnosis of malignant extra-adrenal paraganglioma was made. Some tumor cells showed mild degeneration, along with fibrosis, which was consistent with the features of mild postoperative changes. Tumor involvements included nodules in lesser sac, hepatic nodules in segment VI, small hepatic nodules in segment VI, small hepatic nodules in segment V, hepatic nodules in segment VIIII, mass at the border between segments VII and VIII, mass in the bare area of liver, and hepatic mass in segment VIII. No cancer was seen in the gallbladder tissues. Hematoxylin-eosin (HE) and immunohistochemistry (IHC) staining IHC showed: CD56(3+), chromogranin (2+), synaptophysin(2+), CK18( ), CK19( ), CK20( ), CK7( ), hepatocyte( ), CK8(2+), EM( ), GFP( ), S100[+(stroma)], and Ki-67(10%+). HE staining pictures were showed in Figures IHC staining pictures were showed in Figures 12,13. Case discussion Classification and nomenclature of paraganglioma In 1912, Pick recommended that intra-adrenal chromaffin tumors be called pheochromocytomas and that all extraadrenal chromaffin tumors be termed paragangliomas, which were also known as nonchromaffin paraganglioma or chemodectoma. Traditionally it was believed that paragangliomas accounted for only 10 15% of all pheochromocytomas. This proportion has risen in recent years to about 20%. s an extremely rare neuroendocrine tumor in soft tissues, paragangliomas belong to amine precursor uptake and decarboxylation (PUD) tumors. They arise from neural crest cells and can synthesize, store, and secret catecholamines (Cs), thus producing a variety of peptide neurohormones and chromaffin granules. In 2004, the Word Health Organization (WHO) defined the pheochromocytoma (or, adrenal paraganglioma) as tumors arising from C-producing adrenal medullary chromaffin cells. In contrast, tumors arising from sympathetic and parasympathetic ganglions were defined as extra-adrenal paragangliomas. It has been increasingly recognized that the pheochromocytoma specifically refers to adrenal pheochromocytoma, whereas the traditionally ectopic or extra-adrenal pheochromocytomas are collectively termed as paragangliomas. ased on the primary sites, the extra-adrenal pheochromocytomas can be further divided into four Translational Gastroenterology and Hepatology. ll rights reserved. tgh.amegroups.com




.")


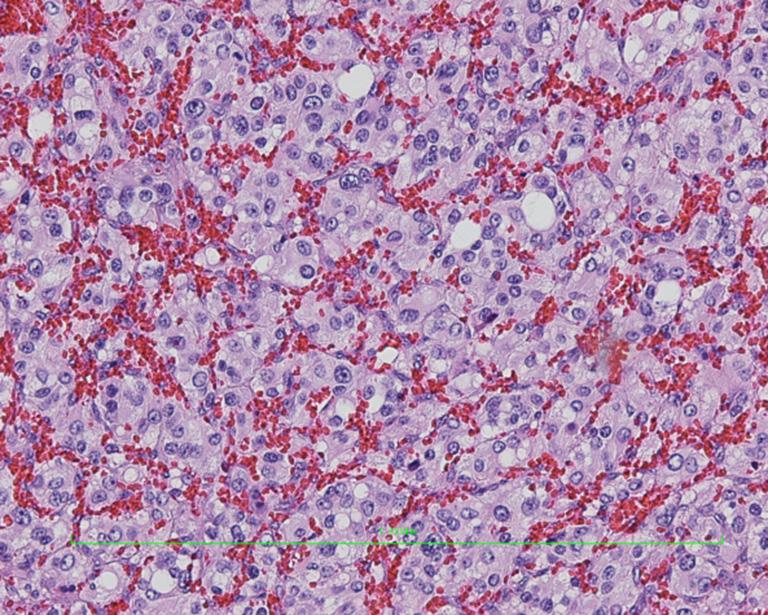
6 Translational Gastroenterology and Hepatology, 2016 Page 6 of 9 C D E F Figure 9 Hematoxylin-eosin (HE) staining images of hilar mass (40, 40, 100, 100, 100, 100 ). Figure 10 Hematoxylin-eosin (HE) staining images of liver metastases (40, 200 ). Translational Gastroenterology and Hepatology. ll rights reserved. tgh.amegroups.com
 staining of CD56(3+) (100 ) and Ki-67(10%+) (100 ).")
 arising")
; (II) type of vagus nerve: this type is distributed in the locations of peripheral vagus nerve; (III) Translational")
 visceral")
, mainly")
7 Translational Gastroenterology and Hepatology, 2016 Page 7 of 9 Figure 11 Hematoxylin-eosin (HE) staining images of nodules in lesser sac (100 ). Figure 13 Immunohistochemistry (IHC) staining of CD56(3+) (100 ) and Ki-67(10%+) (100 ). Figure 12 Immunohistochemistry (IHC) staining of Syn(2+) (100 ) and Cg(2+) (100 ). types: (I) arising from visceral arch: it is related with the development of visceral arch and is also known as chemodectoma (e.g., carotid chemodectoma or aortic body chemodectoma); (II) type of vagus nerve: this type is distributed in the locations of peripheral vagus nerve; (III) Translational Gastroenterology and Hepatology. ll rights reserved. arising from the aortic sympathetic ganglia: this type is mainly distributed in segmental ganglia in the neck, chest, abdomen, and retroperitoneum; and (IV) visceral type: this type is mainly related with vascular organs such as atria, atrial septum, urinary tract, and liver. Most extra-adrenal paragangliomas are located near the posterior abdominal wall and the abdominal aorta (from the upper abdomen till the bottom of the pelvis), mainly arising from the Zuckerkandl s body in this region. ased on the clinical manifestations and blood C level, paragangliomas can be divided into functional and non-functional types, among which the functional paragangliomas account for 10 20%, with the main manifestations including high blood pressure, heart palpitations, and elevated blood C levels. Differences benign and malignant paragangliomas Typically paragangliomas are rare and benign tumors, but about 10% cases may have malignant potential. It has been widely believed that paragangliomas are slowly growing tgh.amegroups.com
8 Page 8 of 9 Translational Gastroenterology and Hepatology, 2016 tumors with potentially or low-grade malignant behaviors. Some authors tried to predict the potential malignancy from a morphological perspective including tumor size, nuclear pleomorphism, mitotic figure, necrosis, and Ki-67 index, but with unsatisfactory results. Research has found that the pathological findings of a paraganglioma were not necessarily parallel with its biological behaviors. morphologically benign paraganglioma can also become metastatic. The histological feature alone is not sufficient to distinguish benign from malignant paragangliomas. The diagnosis of a malignant paraganglioma relies mainly on relapse and metastasis. Lymph node metastasis is the most reliable indicator for differentiation. The value of capsular and/or vascular invasion is limited. malignancy may be diagnosed if there is extensive capsular involvement or if the tumor invades the surrounding soft tissues. Malignant paraganglioma may spread to the lung, liver, kidney, brain, and lymph node via blood stream and/or lymphatic system. Liver metastases occurred in our current case. malignancy could be diagnosed according to its biological behaviors. lthough preoperative assessment showed that surgery in this patient might be difficult and risky, aggressive surgery should be carried out to remove the tumor. clinical manifestations of a chromaffin cell tumor, and OCT should be further applied in patients with negative IMG findings; (III) 18F-fluorodeoxyglucose positron emission tomography (PET): Literature has demonstrated that PET can successfully display and accurately locate pheochromocytomas. Treatment of paraganglioma Paraganglioma is not sensitive to radiotherapy or chemotherapy. Early or complete surgical resection remains the mainstream treatment for it. Even if the tumor has already become large or if there is a relapse, surgery should always be considered if the patient can tolerate it. It has been reported that the surgical resection could reach 75.5%. Resection of the tumors should be thorough and complete to prevent relapse and increase survival rate. For patients with suspected malignant paraganglioma, routine follow-up visits should be arranged after surgery; prophylactic radiotherapy may be applied if necessary. The paragangliomas usually have a good prognosis, with a 5-year survival rate of 33% and a 10-year survival rate of 25%. Special examinations for clinically suspicious pheochromocytoma or paraganglioma There is an estimated preoperative misdiagnosis rate of 100% for pheochromocytoma or paraganglioma. Further understanding and knowledge about this disease may facilitate the correct diagnosis of this disease. The following examinations may be applied for clinically suspicious pheochromocytoma or paraganglioma: (I) Iodine-131 metaiodobenzylguanidine ( 131 I-IMG): 131 I-IMG has a high affinity with chromaffin cell tissues. It can be used for both qualitative diagnosis and locating. It is more accurate than CT in locating multiple maligant, and/or metastatic pheochromocytoma. It is particularly valuable for non-functioning pheochromocytomas; (II) Octreotide (OCT) scan: somatostatin-receptor (SSTR) imaging using the radioactive-labeled OCT tracers can be useful for locating endocrine tumors and help to judge the efficacy of somatostatin treatment. While IMG is more valuable for adrenal pheochromocytoma, OCT is superior in diagnosing paraganglioma. They can complement each other. IMG is preferred for patients with Preoperative preparation for pheochromocytomas/ paragangliomas For functional pheochromocytomas/paragangliomas, adequate preoperative preparation is the key to the success of surgery. Without the routine administration of α-receptor blockers, the surgical mortality rate of pheochromocytomas patients can be as high as 24 50%; in contrast, the surgical mortality rate is below 3% after adequate preoperative preparation using drugs. The purpose of preoperative drug preparation include: (I) to block the effect of excessive C, maintain the normal blood pressure and heart rate/rhythm, and improve the function of the heart and other organs; (II) to correct hypovolemia; (III) to prevent the fluctuating blood pressure due to the massive release of C induced by surgery and anesthesia and reduce the occurrence of severe complications such as acute heart failure and pulmonary edema. Controlling high blood pressure (I) α-blockers (recommended): the most commonly used drug is the long-lasting non-selective α-blocker phenoxybenzamine (initial 5 10 mg bid; can be increased by mg every 2 3 days). If the paroxysmal symptoms are controlled, the blood Translational Gastroenterology and Hepatology. ll rights reserved. tgh.amegroups.com
9 Translational Gastroenterology and Hepatology, 2016 pressure is normal or slightly low, and/or there is postural hypotension or stuffy nose, the drug dose is appropriate (typically mg or 1 mg/kg daily, orally administered 3 4 times per day, with a daily dose not exceeding 2 mg/kg. lternately, α1-blockers can also be used. During the drug administration, increasing dietary salt intake may decrease the occurrence of orthostatic hypotension and facilitate volume expansion; (II) Calcium-channel blockers (recommended): calcium-channel blockers can block the entry of NE-mediated calcium ions into the vascular smooth muscle cells, thus achieving the control of blood pressure and arrhythmia. lso, they can prevent C-related coronary artery spasm and facilitate the improvement of cardiac function. They have comparable efficacy to α-blockers but do not cause orthostatic hypotension. Calcium-channel blockers are recommended to replace α-receptor blockers in the following three conditions: (I) lpha-receptor blocker monotherapy cannot satisfactorily control blood pressure and a combination with calcium-channel blockers can improve the therapeutic effectiveness and reduce the dose of α-receptor blockers; (II) The α-receptor blockers have severe side effects that cannot be tolerated by the patients; (III) The blood pressure is normal or only intermittently increased, replacing the α-receptor blockers with calcium-channel blockers can avoid hypotension or orthostatic hypotension. Controlling arrhythmias For C- or α-receptor blocker-mediated tachycardia (> /min) or supraventricular arrhythmias, β-receptor blockers may be added to control the heart rate below 90/min. However, the β-blockers must be used 2 3 days after α-blockers because β-blocker monotherapy may block the effects of adrenaline in activating β2 receptor and dilating vessels and thus induce fatal complications including hypertensive crisis, myocardial infarction, and pulmonary edema. Cardioselective β2 blockers such as atenolol and metoprolol are recommended. Treatment of hypertensive crisis Sodium nitroprusside, phentolamine, or nicardipine via Page 9 of 9 venous pump is recommended for the management of hypertensive crisis Duration of preoperative drug preparation n interval of at least days is recommended, and an interval of 4 6 weeks for patients with frequent attacks. The preoperative drug preparation is regarded as adequate in the following conditions: (I) The blood pressure is maintained at 120/80 mmhg, with a heart rate <80 90/min; (II) Without paroxysmal high blood pressure, heart palpitations, or sweating; (III) With increased body weight and hematocrit <45%; (IV) With mild nasal congestion, lost feeling of coldness in the extremities, experiencing warm feeling in the extremities, and/or ruddy nail bed (which suggests good microcirculation perfusion). Good communication between surgeon and anesthesiologists is required before surgery. In our current case, the fact that the tumor was functional was not considered before surgery, and the patient experienced fluctuations of heart rate and blood pressure during the surgery. Fortunately, the anesthesiologists dealt with the situation timely and properly, thus avoiding a perioperative death. cknowledgements None. Footnote Conflicts of Interest: The authors have no conflicts of interest to declare. Informed Consent: Written informed consent was obtained from the patient for publication of this manuscript and any accompanying images. doi: /tgh Cite this article as: Li Y, Huang Z, Zhang Y, Zhao H. Multimodality therapy for a case of neuroendocrine tumor in the hilum with multiple hepatic metastases. Transl Gastroenterol Hepatol 2016;1:81. Translational Gastroenterology and Hepatology. ll rights reserved. tgh.amegroups.com
Interventional therapy for rectal neuroendocrine tumor with liver metastases: report of one case
 Case Report Interventional therapy for rectal neuroendocrine tumor with liver metastases: report of one case Lingxiao Liu 1 *, Xu Han 2 *, Wenhui Lou 2 1 Department of Interventional Radiology, 2 Department
Case Report Interventional therapy for rectal neuroendocrine tumor with liver metastases: report of one case Lingxiao Liu 1 *, Xu Han 2 *, Wenhui Lou 2 1 Department of Interventional Radiology, 2 Department
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018
 Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Resection of postoperative liver metastasis from pancreatic neuroendocrine tumors: report of one case
 Case Report Resection of postoperative liver metastasis from pancreatic neuroendocrine tumors: report of one case Xiao Chen, Hu Ren, Yihebali Chi, Shun He, Zhen Huang, Xuhui Hu, Hong Zhao Department of
Case Report Resection of postoperative liver metastasis from pancreatic neuroendocrine tumors: report of one case Xiao Chen, Hu Ren, Yihebali Chi, Shun He, Zhen Huang, Xuhui Hu, Hong Zhao Department of
A rare case of retroperitoneal paraganglioma case report and literature review
 Case Report A rare case of retroperitoneal paraganglioma case report and literature review Peng Li, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital, Chinese Academy of Medical
Case Report A rare case of retroperitoneal paraganglioma case report and literature review Peng Li, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital, Chinese Academy of Medical
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Sporadic Pheochromocytoma. Bertil Hamberger Professor of Surgery Karolinska Institutet, Stockholm, Sweden
 Sporadic Pheochromocytoma Bertil Hamberger Professor of Surgery Karolinska Institutet, Stockholm, Sweden 1 Pheochromocytoma Anatomy, physiology and pathology Symptoms and diagnosis Plasma metanephrines
Sporadic Pheochromocytoma Bertil Hamberger Professor of Surgery Karolinska Institutet, Stockholm, Sweden 1 Pheochromocytoma Anatomy, physiology and pathology Symptoms and diagnosis Plasma metanephrines
Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case
 Case Report Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case Yang Wang, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital,
Case Report Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case Yang Wang, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital,
BONE METASTASIS OF MEDIASTINAL PARAGANGLIOMA: CASE REPORT
 BONE METASTASIS OF MEDIASTINAL PARAGANGLIOMA: CASE REPORT Dr. Abhinandan Gupta 1*, Kong Long 1, Prof. Huang Jing Bai 1, Dr. Deepikal Dhakal 1, Dr. Sunil Shrestha 1, Dr. Roshan Kumar Yadav 2 and Dr. Shashi
BONE METASTASIS OF MEDIASTINAL PARAGANGLIOMA: CASE REPORT Dr. Abhinandan Gupta 1*, Kong Long 1, Prof. Huang Jing Bai 1, Dr. Deepikal Dhakal 1, Dr. Sunil Shrestha 1, Dr. Roshan Kumar Yadav 2 and Dr. Shashi
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE
 ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
Robotic-assisted right inferior lobectomy
 Robotic Thoracic Surgery Column Page 1 of 6 Robotic-assisted right inferior lobectomy Shiguang Xu, Tong Wang, Wei Xu, Xingchi Liu, Bo Li, Shumin Wang Department of Thoracic Surgery, Northern Hospital,
Robotic Thoracic Surgery Column Page 1 of 6 Robotic-assisted right inferior lobectomy Shiguang Xu, Tong Wang, Wei Xu, Xingchi Liu, Bo Li, Shumin Wang Department of Thoracic Surgery, Northern Hospital,
Type 2 gastric neuroendocrine tumor: report of one case
 Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Wilms Tumor and Neuroblastoma
 Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
Accessory Glands of Digestive System
 Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
THE FACTS YOU NEED TO KNOW
 PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
A case of micturition syncope
 A case of micturition syncope Kimberly Bundick, PA-S S L I D E 1 Agenda Purpose Utilize case to illustrate classic finding of an interesting pathology Agenda Case study Epidemiology, etiology of disease
A case of micturition syncope Kimberly Bundick, PA-S S L I D E 1 Agenda Purpose Utilize case to illustrate classic finding of an interesting pathology Agenda Case study Epidemiology, etiology of disease
Robotic-assisted right upper lobectomy
 Robotic Thoracic Surgery Column Robotic-assisted right upper lobectomy Shiguang Xu, Tong Wang, Wei Xu, Xingchi Liu, Bo Li, Shumin Wang Department of Thoracic Surgery, Northern Hospital, Shenyang 110015,
Robotic Thoracic Surgery Column Robotic-assisted right upper lobectomy Shiguang Xu, Tong Wang, Wei Xu, Xingchi Liu, Bo Li, Shumin Wang Department of Thoracic Surgery, Northern Hospital, Shenyang 110015,
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Retroperitoneal Ganglioneuroma Encasing the Celiac and Superior Mesenteric Arteries
 Case Study TheScientificWorldJOURNAL (2004) 4, 974 977 ISSN 1537-744X; DOI 10.1100/tsw.2004.198 Retroperitoneal Ganglioneuroma Encasing the Celiac and Superior Mesenteric Arteries Justin K. Nelms, Eric
Case Study TheScientificWorldJOURNAL (2004) 4, 974 977 ISSN 1537-744X; DOI 10.1100/tsw.2004.198 Retroperitoneal Ganglioneuroma Encasing the Celiac and Superior Mesenteric Arteries Justin K. Nelms, Eric
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
PET IMAGING (POSITRON EMISSION TOMOGRAPY) FACT SHEET
 FACT SHEET") Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Superior mediastinal paraganglioma associated with von Hippel-Lindau syndrome: report of a case
 Takahashi et al. World Journal of Surgical Oncology 2014, 12:74 WORLD JOURNAL OF SURGICAL ONCOLOGY CASE REPORT Open Access Superior mediastinal paraganglioma associated with von Hippel-Lindau syndrome:
Takahashi et al. World Journal of Surgical Oncology 2014, 12:74 WORLD JOURNAL OF SURGICAL ONCOLOGY CASE REPORT Open Access Superior mediastinal paraganglioma associated with von Hippel-Lindau syndrome:
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
An Unexpected Cause of Hypoglycemia
 An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
Malignant extra-adrenal pancreatic paraganglioma: case report and literature review
 Al-Jiffry et al. BMC Cancer 2013, 13:486 CASE REPORT Open Access Malignant extra-adrenal pancreatic paraganglioma: case report and literature review Bilal O Al-Jiffry 1,2*, Yasir AlNemary 1, Samah H Khayat
Al-Jiffry et al. BMC Cancer 2013, 13:486 CASE REPORT Open Access Malignant extra-adrenal pancreatic paraganglioma: case report and literature review Bilal O Al-Jiffry 1,2*, Yasir AlNemary 1, Samah H Khayat
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
PHEOCHROMOCYTOMA. Anita Chiu, MD Kings County Hospital Center January 13, 2011
 PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
GUIDELINES FOR CANCER IMAGING Lung Cancer
 GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
To describe the liver. To list main structures in porta hepatis.
 GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
A fatal case of an adrenal gland melanoma with a mysterious primary lesion
 ISPUB.COM The Internet Journal of Urology Volume 6 Number 2 A fatal case of an adrenal gland melanoma with a mysterious primary lesion A Adam, M Engelbrecht, I van Heerden Citation A Adam, M Engelbrecht,
ISPUB.COM The Internet Journal of Urology Volume 6 Number 2 A fatal case of an adrenal gland melanoma with a mysterious primary lesion A Adam, M Engelbrecht, I van Heerden Citation A Adam, M Engelbrecht,
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Daniela Faivovich K., MS VII Universidad de Chile Gillian Lieberman, MD Harvard Medical School
 Daniela Faivovich K., MS VII Universidad de Chile Gillian Lieberman, MD Harvard Medical School May 21st, 2010 56 year old male patient History of hypertension, hyperlipidemia and insulin-resistance 2009:
Daniela Faivovich K., MS VII Universidad de Chile Gillian Lieberman, MD Harvard Medical School May 21st, 2010 56 year old male patient History of hypertension, hyperlipidemia and insulin-resistance 2009:
-12. -Renad Habahbeh. -Dr Mohammad mohtasib
 -12 -Renad Habahbeh - -Dr Mohammad mohtasib The Gallbladder -The gallbladder has a body, a fundus (a rounded end), a neck, Hartmann s pouch before the neck and a cystic duct that meets the common hepatic
-12 -Renad Habahbeh - -Dr Mohammad mohtasib The Gallbladder -The gallbladder has a body, a fundus (a rounded end), a neck, Hartmann s pouch before the neck and a cystic duct that meets the common hepatic
The Spleen. Dr Fahad Ullah
 The Spleen BY Dr Fahad Ullah Spleen The spleen is an largest lymphoid organ shaped like a shoe that lies relative to the 9th and 11th ribs and is located in the left hypochondrium. Thus, the spleen is
The Spleen BY Dr Fahad Ullah Spleen The spleen is an largest lymphoid organ shaped like a shoe that lies relative to the 9th and 11th ribs and is located in the left hypochondrium. Thus, the spleen is
Therefore MAP=CO x TPR = HR x SV x TPR
 Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Karim Said. 41 year old farmer. Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy
 Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Sectional Anatomy Quiz - III
 Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
1. Which of the following blood vessels has a thin elastic layer? A. Aorta. B. Pulmonary artery. C. Posterior vena cava. D. Mesenteric capillary.
 CIRCULATORY SYSTEM 1. Which of the following blood vessels has a thin elastic layer? A. Aorta. B. Pulmonary artery. C. Posterior vena cava. D. Mesenteric capillary. 2. Capillary beds are equipped with
CIRCULATORY SYSTEM 1. Which of the following blood vessels has a thin elastic layer? A. Aorta. B. Pulmonary artery. C. Posterior vena cava. D. Mesenteric capillary. 2. Capillary beds are equipped with
The posterior abdominal wall. Prof. Oluwadiya KS
 The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
Surface Anatomy. Location Shape Weight Role of Five Surfaces Borders Fissures Lobes Peritoneal Lig
 The Liver Functions Bile production and secretion Detoxification Storage of glycogen Protein synthesis Production of heparin and bile pigments Erythropoiesis (in fetus) Surface Anatomy Location Shape Weight
The Liver Functions Bile production and secretion Detoxification Storage of glycogen Protein synthesis Production of heparin and bile pigments Erythropoiesis (in fetus) Surface Anatomy Location Shape Weight
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
STAGING AND FOLLOW-UP STRATEGIES
 ATHENS 4-6 October 2018 European Society of Urogenital Radiology STAGING AND FOLLOW-UP STRATEGIES Ahmet Tuncay Turgut, MD Professor of Radiology Hacettepe University, Faculty of Medicine Ankara 2nd ESUR
ATHENS 4-6 October 2018 European Society of Urogenital Radiology STAGING AND FOLLOW-UP STRATEGIES Ahmet Tuncay Turgut, MD Professor of Radiology Hacettepe University, Faculty of Medicine Ankara 2nd ESUR
2. right heart = pulmonary pump takes blood to lungs to pick up oxygen and get rid of carbon dioxide
 A. location in thorax, in inferior mediastinum posterior to sternum medial to lungs superior to diaphragm anterior to vertebrae orientation - oblique apex points down and to the left 2/3 of mass on left
A. location in thorax, in inferior mediastinum posterior to sternum medial to lungs superior to diaphragm anterior to vertebrae orientation - oblique apex points down and to the left 2/3 of mass on left
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear
: CT, MRI, EUS, Nuclear") Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Evaluation of Thyroid Nodules
 Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Dr.Dafalla Ahmed Babiker Jazan University
 Dr.Dafalla Ahmed Babiker Jazan University Brain tumors are the second commonest malignancy in children Infratentorial tumors are more common As a general rule they do not metastasize out of the CNS, but
Dr.Dafalla Ahmed Babiker Jazan University Brain tumors are the second commonest malignancy in children Infratentorial tumors are more common As a general rule they do not metastasize out of the CNS, but
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
BY DR NOMAN ULLAH WAZIR
 BY DR NOMAN ULLAH WAZIR The stomach (from ancient Greek word stomachos, stoma means mouth) is a muscular, hollow and the most dilated part of the GIT. It starts from the point where esophagus ends. It
BY DR NOMAN ULLAH WAZIR The stomach (from ancient Greek word stomachos, stoma means mouth) is a muscular, hollow and the most dilated part of the GIT. It starts from the point where esophagus ends. It
Brain Tumors. What is a brain tumor?
 Scan for mobile link. Brain Tumors A brain tumor is a collection of abnormal cells that grows in or around the brain. It poses a risk to the healthy brain by either invading or destroying normal brain
Scan for mobile link. Brain Tumors A brain tumor is a collection of abnormal cells that grows in or around the brain. It poses a risk to the healthy brain by either invading or destroying normal brain
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Done by: Dina Sawadha & Mohammad Abukabeer
 Done by: Dina Sawadha & Mohammad Abukabeer The stomach *the stomach is a dilated part of the gastro intestinal tract, it's "J" shape. *the lower surface of the stomach ( the greater curvature ) reaches
Done by: Dina Sawadha & Mohammad Abukabeer The stomach *the stomach is a dilated part of the gastro intestinal tract, it's "J" shape. *the lower surface of the stomach ( the greater curvature ) reaches
Dr. Weyrich G07: Superior and Posterior Mediastina. Reading: 1. Gray s Anatomy for Students, chapter 3
 Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
PHENTOLAMINE MESYLATE INJECTION SANDOZ STANDARD 5 mg/ ml THERAPEUTIC CLASSIFICATION Alpha-adrenoreceptor Blocker
 PACKAGE INSERT Pr PHENTOLAMINE MESYLATE INJECTION SANDOZ STANDARD 5 mg/ ml THERAPEUTIC CLASSIFICATION Alpha-adrenoreceptor Blocker ACTIONS AND CLINICAL PHARMACOLOGY Phentolamine produces an alpha-adrenergic
PACKAGE INSERT Pr PHENTOLAMINE MESYLATE INJECTION SANDOZ STANDARD 5 mg/ ml THERAPEUTIC CLASSIFICATION Alpha-adrenoreceptor Blocker ACTIONS AND CLINICAL PHARMACOLOGY Phentolamine produces an alpha-adrenergic
Robotic-assisted left inferior lobectomy
 Robotic Thoracic Surgery Column Robotic-assisted left inferior lobectomy Shiguang Xu, Hao Meng, Tong Wang, Wei Xu, Xingchi Liu, Shumin Wang Department of Thoracic Surgery, Northern Hospital, Shenyang 110015,
Robotic Thoracic Surgery Column Robotic-assisted left inferior lobectomy Shiguang Xu, Hao Meng, Tong Wang, Wei Xu, Xingchi Liu, Shumin Wang Department of Thoracic Surgery, Northern Hospital, Shenyang 110015,
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Mediastinal Paraganglioma: a challenge to the echocardiographic
 Case - based learning from ESC Cardiologists of Tomorrow Look for the answer outside the heart Mediastinal Paraganglioma: a challenge to the echocardiographic 1 diagnosis and endovascular treatment 1 On
Case - based learning from ESC Cardiologists of Tomorrow Look for the answer outside the heart Mediastinal Paraganglioma: a challenge to the echocardiographic 1 diagnosis and endovascular treatment 1 On
Shadow because the air
 Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
Merkel Cell Carcinoma Case # 2
 DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Lecture 02 Anatomy of the LIVER
 Lecture 02 Anatomy of the LIVER BY Dr Farooq Khan Aurakzai Dated: 02.01.2018 Introduction to Liver Largest gland in the body. 2 nd largest organ of the body. Weight approximately 1500 gm, and is roughly
Lecture 02 Anatomy of the LIVER BY Dr Farooq Khan Aurakzai Dated: 02.01.2018 Introduction to Liver Largest gland in the body. 2 nd largest organ of the body. Weight approximately 1500 gm, and is roughly
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Community Case. Saeed Awan R5
 Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Malignant Paraganglioma of the Retroperitoneum with Lung Metastases: A 13-year Survivor After Radical Surgery
 Case Report Malignant Paraganglioma of the Retroperitoneum with Lung Metastases: A 13-year Survivor After Radical Surgery Hideo Matsui, 1,2 Shunji Ikeuchi, 3 Noboru Onoda 4 and Yutaka Tsutsumi, 5 1 Research
Case Report Malignant Paraganglioma of the Retroperitoneum with Lung Metastases: A 13-year Survivor After Radical Surgery Hideo Matsui, 1,2 Shunji Ikeuchi, 3 Noboru Onoda 4 and Yutaka Tsutsumi, 5 1 Research
Lesions of the pancreaticoduodenal groove, a pictorial review
 Lesions of the pancreaticoduodenal groove, a pictorial review Poster No.: C-2131 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Ni Mhurchu, L. Lavelle, I. Murphy, S. Skehan ; IE, Dublin/ IE Keywords:
Lesions of the pancreaticoduodenal groove, a pictorial review Poster No.: C-2131 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Ni Mhurchu, L. Lavelle, I. Murphy, S. Skehan ; IE, Dublin/ IE Keywords:
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Topics: Staging and treatment for pancreatic cancer. Staging systems for pancreatic cancer: Differences between the Japanese and UICC systems
 M. J Hep Kobari Bil Pancr and S. Surg Matsuno: (1998) Staging 5:121 127 system for pancreatic cancer 121 Topics: Staging and treatment for pancreatic cancer Staging systems for pancreatic cancer: Differences
M. J Hep Kobari Bil Pancr and S. Surg Matsuno: (1998) Staging 5:121 127 system for pancreatic cancer 121 Topics: Staging and treatment for pancreatic cancer Staging systems for pancreatic cancer: Differences
Esophageal Cancer Initially Thought to be Accompanied by a Solitary Metastasis to an Intrathoracic Paraaortic Lymph Node
 2012 66 5 417 421 Esophageal Cancer Initially Thought to be Accompanied by a Solitary Metastasis to an Intrathoracic Paraaortic Lymph Node a b* a a a a a a a b ʼ 418 Horio et al. Acta Med. Okayama Vol.
2012 66 5 417 421 Esophageal Cancer Initially Thought to be Accompanied by a Solitary Metastasis to an Intrathoracic Paraaortic Lymph Node a b* a a a a a a a b ʼ 418 Horio et al. Acta Med. Okayama Vol.
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Boot Camp Case Scenarios
 Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
10. Thick deposits of lipids on the walls of blood vessels, called, can lead to serious circulatory issues. A. aneurysm B. atherosclerosis C.
 Heart Student: 1. carry blood away from the heart. A. Arteries B. Veins C. Capillaries 2. What is the leading cause of heart attack and stroke in North America? A. alcohol B. smoking C. arteriosclerosis
Heart Student: 1. carry blood away from the heart. A. Arteries B. Veins C. Capillaries 2. What is the leading cause of heart attack and stroke in North America? A. alcohol B. smoking C. arteriosclerosis
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22
 Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Adrenal Medulla. Amelyn R. Rafael, M.D.
 Adrenal Medulla Amelyn R. Rafael, M.D. Adrenal Medulla Exodermal in origin Cells derived from the sympathogonia of the primitive neuroectoderm A sympathetic ganglion in which the post-ganglionic cells
Adrenal Medulla Amelyn R. Rafael, M.D. Adrenal Medulla Exodermal in origin Cells derived from the sympathogonia of the primitive neuroectoderm A sympathetic ganglion in which the post-ganglionic cells
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Circulatory System Review
 Circulatory System Review 1. Know the diagrams of the heart, internal and external. a) What is the pericardium? What is myocardium? What is the septum? b) Explain the 4 valves of the heart. What is their
Circulatory System Review 1. Know the diagrams of the heart, internal and external. a) What is the pericardium? What is myocardium? What is the septum? b) Explain the 4 valves of the heart. What is their
Gangliocytic Paraganglioma: Report of A Case
 2014 25 122-126 Gangliocytic Paraganglioma: Report of A Case Hsiu-Mei Su, Chi-Hung Chen, Jen-Chieh Huang, and Jeng-Shiann Shin Department of Gastroenterology, Chen-Chin General Hospital, Taichung, Taiwan
2014 25 122-126 Gangliocytic Paraganglioma: Report of A Case Hsiu-Mei Su, Chi-Hung Chen, Jen-Chieh Huang, and Jeng-Shiann Shin Department of Gastroenterology, Chen-Chin General Hospital, Taichung, Taiwan
5/26/16: CT scan of the abdomen showed a multinodular liver disease highly suspicious for metastasis and hydronephrosis of the right kidney.
 Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Fig Glossopharyngeal nerve transmits signals to medulla oblongata. Integrating center. Receptor. Baroreceptors sense increased blood pressure
 Fig. 5. Integrating center Glossopharyngeal nerve transmits signals to medulla oblongata Receptor 3 Vagus nerve transmits inhibitory signals to cardiac pacemaker Baroreceptors sense increased blood pressure
Fig. 5. Integrating center Glossopharyngeal nerve transmits signals to medulla oblongata Receptor 3 Vagus nerve transmits inhibitory signals to cardiac pacemaker Baroreceptors sense increased blood pressure
PDF created with pdffactory Pro trial version
 Neuroblastoma Tumor derived from neural crest cell that form the sympathetic ganglia&adrenal medulla. Causes *unknown. *familial neuroblastoma has been reported but is rare. * The incidence is 1:100,000
Neuroblastoma Tumor derived from neural crest cell that form the sympathetic ganglia&adrenal medulla. Causes *unknown. *familial neuroblastoma has been reported but is rare. * The incidence is 1:100,000
Evaluation of Liver Mass Lesions. American College of Gastroenterology 2013 Regional Postgraduate Course
 Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY
 THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
Pancreas and Biliary System
 Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Cardiovascular System B L O O D V E S S E L S 2
 Cardiovascular System B L O O D V E S S E L S 2 Blood Pressure Main factors influencing blood pressure: Cardiac output (CO) Peripheral resistance (PR) Blood volume Peripheral resistance is a major factor
Cardiovascular System B L O O D V E S S E L S 2 Blood Pressure Main factors influencing blood pressure: Cardiac output (CO) Peripheral resistance (PR) Blood volume Peripheral resistance is a major factor
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Case Report: Chondroid Syringoma of the Cheek
 Cronicon OPEN ACCESS Dina Amin 1 *, Abdullah Al-Gorashi 2 and Rahaf Y Al-Habbab 2 1 Assistant Consultant Al-Noor Specialist Hospital, Saudi Arabia, Clinical fellow University of Alabama, USA 2 Department
Cronicon OPEN ACCESS Dina Amin 1 *, Abdullah Al-Gorashi 2 and Rahaf Y Al-Habbab 2 1 Assistant Consultant Al-Noor Specialist Hospital, Saudi Arabia, Clinical fellow University of Alabama, USA 2 Department