PROBLEMS OF PROGNOSTICATION IN SOFT TISSUE TUMOURS. Christopher D.M. Fletcher Brigham and Women s Hospital and Harvard Medical School Boston, MA
|
|
|
- Ethan Dickerson
- 5 years ago
- Views:
Transcription
1 PROBLEMS OF PROGNOSTICATION IN SOFT TISSUE TUMOURS Christopher D.M. Fletcher Brigham and Women s Hospital and Harvard Medical School Boston, MA
2 Dr. Fletcher has no conflict of interest or disclosures to make.
3 PROGNOSTIC PROBLEMS Soft tissue sarcomas Soft tissue tumours with biologic continuum Tumours which rarely metastasise Benign tumours which exceptionally metastasise
4 VARIABLE BEHAVIOUR OF SOFT TISSUE SARCOMAS Usually metastasise, usually < 2 years Usually metastasise, maybe up to 20 years + 50% metastasise, usually < 5 years 20-30% metastasise, some predictable Rarely metastasise, unpredictable Some tumour-type specific Some types spread across spectrum
5 SOFT TISSUE SARCOMAS CLINICAL PROGNOSTIC FACTORS Stage Tumour size Depth Anatomic site Status of margins Disease-free interval Treatment response
6 SOFT TISSUE SARCOMAS PATHOLOGIC PROGNOSTIC FACTORS Diagnosis/histotype Histologic grade Tumour size Status of margins Vascular invasion Proliferative indices Molecular genetics
7
8 SOFT TISSUE SARCOMA PURPORTED REASONS FOR GRADING Prognostication Staging / planning management Avoids pathologists disagreement Copes with unclassified sarcomas Provides supposed objectivity
9 SOFT TISSUE SARCOMAS GENUINE REASONS FOR GRADING Prognostication Staging / planning management Clinical trials Comparisons of outcome data
10 SOFT TISSUE SARCOMAS HISTOLOGIC GRADING Histologic grade (however derived) is the single best prognostic indicator in some tumour types. Major staging systems (e.g. AJCC) use grade as a key parameter Modern oncologic practice attaches great importance to histologic grade Emphasis on grade, at least in part, paralleled the pre-eminence of MFH
11 POTENTIAL GRADES 1. Low Surgery alone 2. Low-to-intermediate 3. Intermediate Don t know 4. Intermediate-to-high 5. High Add chemo
12 SOFT TISSUE SARCOMAS POTENTIAL HISTOLOGIC COMPONENTS OF GRADE Cellularity Pleomorphism / anaplasia Necrosis Mitotic activity Character of margin Vascular invasion
13 SOFT TISSUE SARCOMAS PROBLEMS IN ASSESSING NECROSIS Macroscopic vs. microscopic Present vs. absent (EORTC) 15% (NCI) vs. 50% (French) Tumor necrosis vs. ischaemia/ infarction Treatment effect(s)
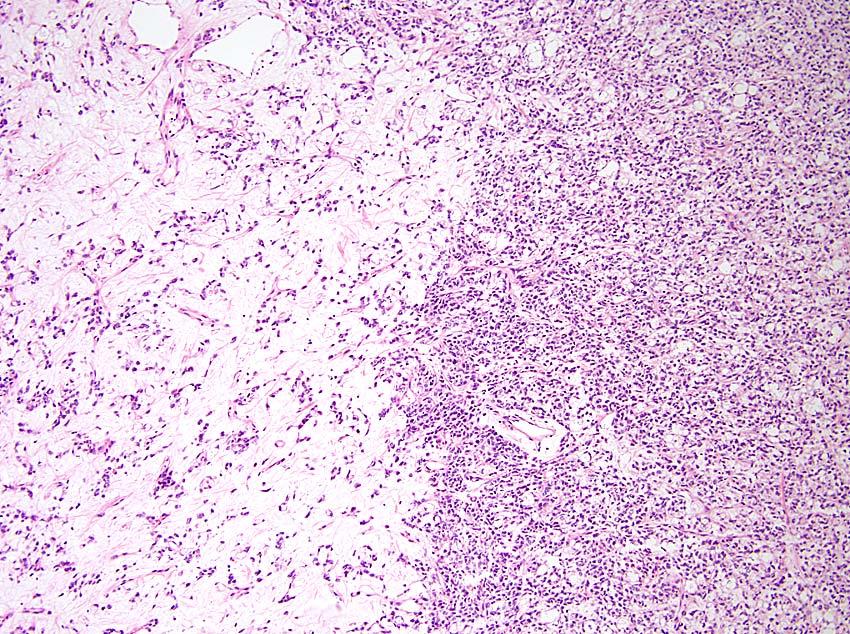
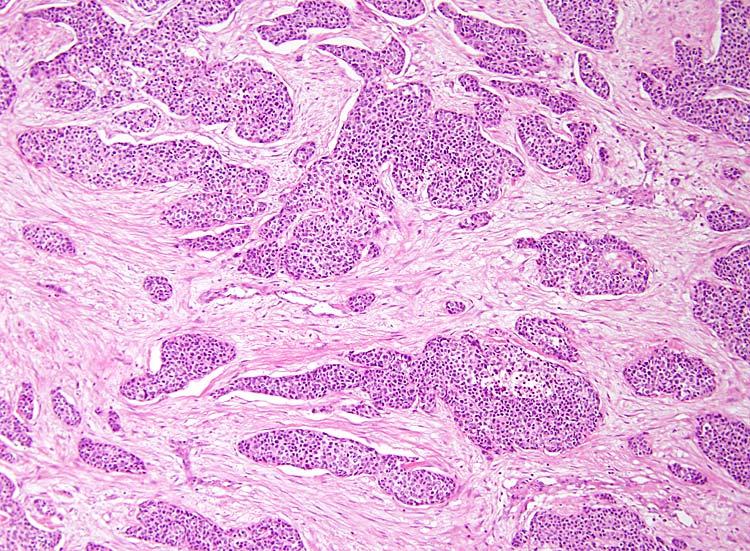
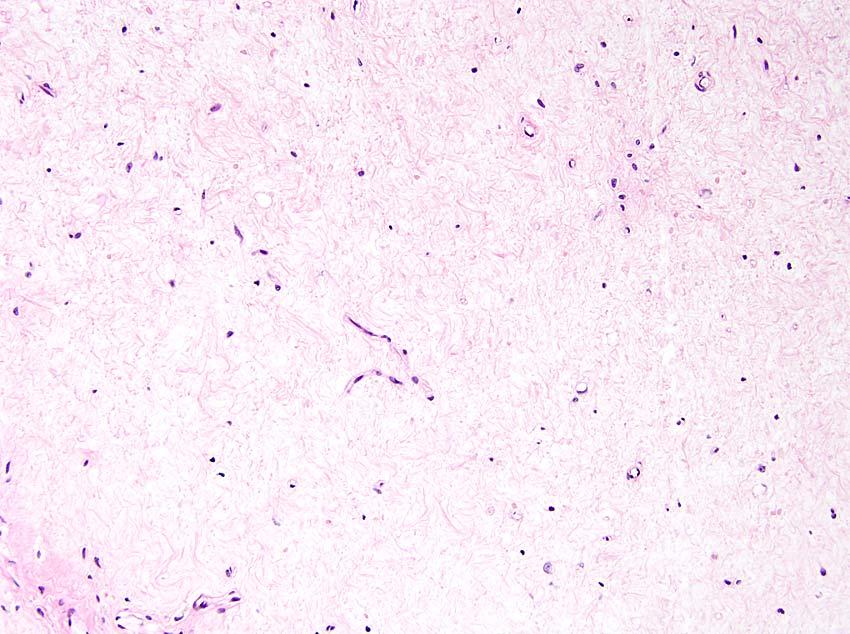
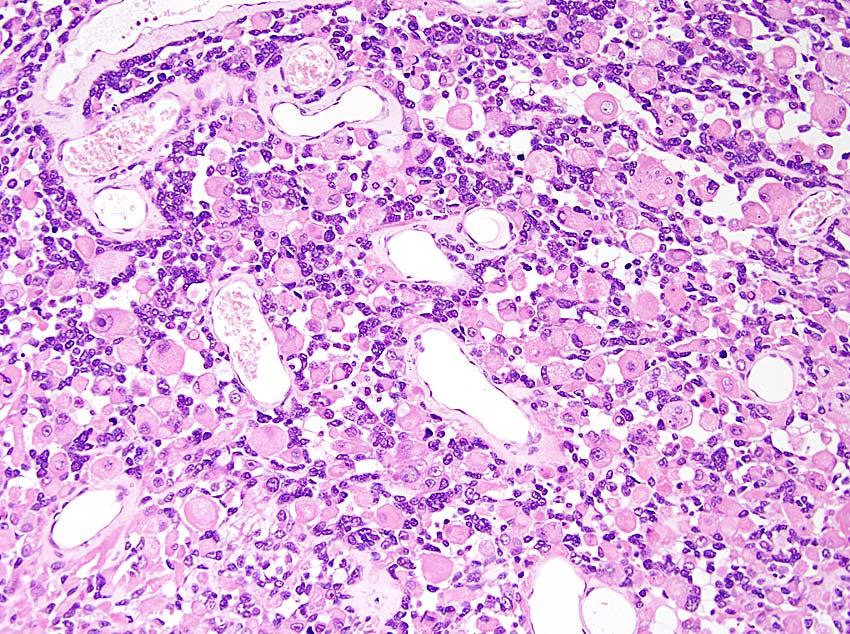
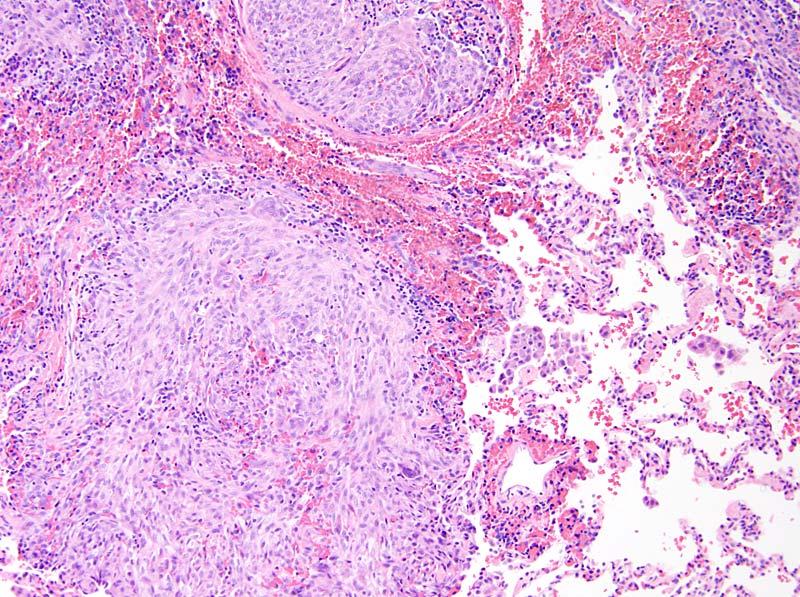
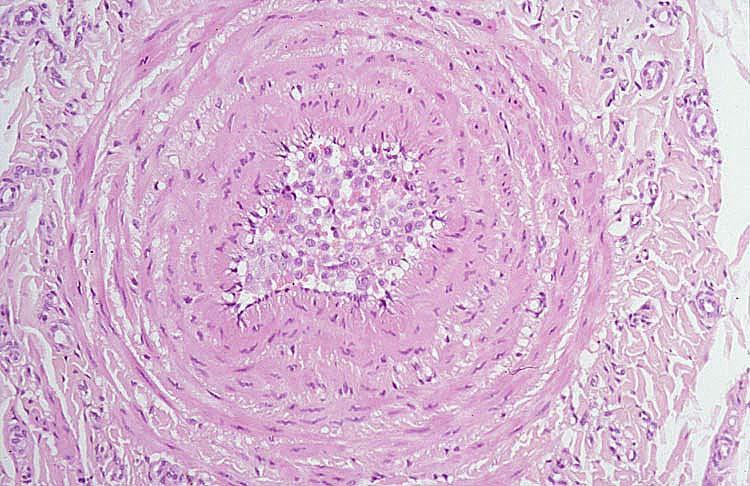
14 SOFT TISSUE TUMOURS MORPHOLOGY / OUTCOME MISMATCH Atypical fibroxanthoma Pleomorphic hyalinising angiectatic tumour Infantile fibrosarcoma Low-grade fibromyxoid sarcoma Rare benign lesions which metastasise Presumably relates to genetic hits / progression

15
16
17
18
19 SOFT TISSUE SARCOMAS Grading is heavily dependent upon the ability to accurately diagnose malignancy
20 SOFT TISSUE SARCOMAS KEY ELEMENTS IN CURRENTLY ACCEPTED GRADING SCHEMES Histotype / differentiation Mitoses Necrosis French (FNCLCC) & NCI systems best known and best validated French system is more discriminatory
21 Guillou et al. J Clin Oncol 1997; 15:
22 Guillou et al. J Clin Oncol 1997; 15:
23 HISTOLOGIC GRADING OF SOFT TISSUE SARCOMAS WHEN DOES IT WORK? In tumours which show a morphologic spectrum that correlates with outcome In the context of an accurate histologic diagnosis e.g. leiomyosarcoma, myxofibrosarcoma
24
25 TUMOUR TYPES IN WHICH FNCLCC SYSTEM DOES NOT WORK MPNST (?) Angiosarcoma Epithelioid sarcoma Clear cell sarcoma Extraskeletal myxoid chondrosarcoma Alveolar soft part sarcoma
26 SOFT TISSUE SARCOMAS TYPE-SPECIFIC GRADING PROBLEMS No differentiated tissue equivalent - synovial sarcoma - clear cell sarcoma - epithelioid sarcoma Usually low mitotic rate - high grade myxoid liposarcoma - alveolar soft part sarcoma - clear cell sarcoma Usually high mitotic rate - infantile fibrosarcoma (pseudosarcomatous lesions)
27
28
29
30
31 SOFT TISSUE SARCOMAS INTRINSIC PROBLEMS IN GRADING Determination of mitotic activity Determination of necrosis Sampling / regional variability Influence of histologic type Effect(s) of pre-op therapy Grade change in recurrence
32 In attempting to correlate structural grade and clinical course in the neurogenic sarcomas, it must be recognized that. histology may vary widely in different regions, that two adjacent tumor nodules may show two extremes of cellularity and that the structure of the recurrent tumors may be quite different from the primary growth. Stewart FW & Copeland MM, Am J Cancer 1931; 15:
33
34
35
36 Tumors of the soft tissues, Atlas of Tumor Pathology, 3 rd Series, RL Kempson et al, eds. Washington DC: AFIP 2001
37
38
39 SOFT TISSUE TUMOURS GRADING TRUISMS Grading on needle biopsies or FNA is often unreliable/may be misleading Grading on an incisional biopsy may be an underestimate Grading a pre-treated lesion most often is meaningless Provision of a grade without a diagnosis is often absurd
40 HISTOLOGIC GRADING OF SOFT TISSUE SARCOMAS PROBLEMS WITH MOST STUDIES To obtain statistically useful case numbers, histotypes are lumped together Only rare studies stratify by tumour type Any statistical analysis of large mixed series underestimates the importance of prognostic factors relevant in rare histotypes
41 HISTOLOGIC GRADING OF SOFT TISSUE SARCOMAS No reason to believe or expect that prognostic parameters would be same in all tumour types Grade - Myxofibrosarcoma Cellularity - Myxoid liposarcoma Size - Myxoid chondrosarcoma Location - Dedifferentiated liposarcoma Genotype - Alveolar rhabdomyosarcoma Clinical stage - Embryonal rhabdomyosarcoma Patient age - Alveolar soft part sarcoma
42 PROGNOSTICATION IN SOFT TISSUE SARCOMAS BROAD ISSUES Influence of histologic type very dependent on reproducibility Grading schemes don t work for some tumour types Type-specific influence of site (eg embryonal rhabdo, leiomyosarc) Prognostic factors change with time Specimen type (problem of needle bx) Use of preoperative therapy
43
44 LEIOMYOSARCOMA* INFLUENCE OF SITE ON PROGNOSIS Overall mortality SKIN 0 SUBCUT 20-30% INTRAMUSC ~ 50% RETROPERIT ~ 100% LARGE VESSEL % *Taking all grades together
45 DISEASE-SPECIFIC SURVIVAL FOR SOFT TISSUE SARCOMAS* 2 yrs 5 yrs 10yrs Day 0 88% 76% 67% Disease-free at 2 yrs 97% 90% 82% Disease-free at 5 yrs 99% 96% 92% *Localised / completely resected - J Clin Oncol 2002; 20:
46 PROGNOSTICATION IN SOFT TISSUE SARCOMAS INFLUENCE OF TIME At resectable locations, tumour size and histologic grade predict disease-free interval for first 3 years At resectable locations, status of margins is more important for patients disease free > 3 years At hard to resect locations, prognostic factors (size, grade, margins) remain unchanged over time
47 Kattan et al. J Clin Oncol 2002; 20:
48 MANAGEMENT OF SOFT TISSUE SARCOMAS A MODERN ONCOLOGIC PARADIGM Needle biopsy Grade and (maybe) diagnosis Neoadjuvant XRT or chemo Excision of undiagnosable altered / dead tissue Who knows what has been treated? How can one reliably predict behaviour?
49 Never mind grading how good are we at recognising a malignant lesion?
50 NON-VISCERAL SMOOTH MUSCLE TUMOURS CRITERIA FOR MALIGNANCY (1) RETROPERITONEUM Either more than minimal atypia or coagulative necrosis or > 10 mitoses / 50 HPF (females) (Insufficient data in males) DEEP SOFT TISSUE (LIMBS / TRUNK) Either more than minimal atypia or coagulative necrosis or > 1 mitosis / 50 HPF

51 ER
52 NON-VISCERAL SMOOTH MUSCLE TUMOURS CRITERIA FOR MALIGNANCY (2) SKIN If typically infiltrative growth pattern and confined to dermis, designate as atypical intradermal smooth muscle neoplasm SUBCUTIS Any mitotic activity - almost always accompanied by nuclear pleomorphism / atypia
53 NON-VISCERAL SMOOTH MUSCLE TUMOURS CRITERIA FOR MALIGNANCY (3) VULVA Three or more of the following: -> 5 cm - infiltrative margins - > 5 mitoses / 10 HPF - moderate or severe atypia SCROTUM Any mitotic activity
54 NON-VISCERAL SMOOTH MUSCLE TUMOURS CRITERIA FOR MALIGNANCY (4) Criteria ( rules ) continue to shift with time as more data are gathered Many studies plagued by inadequate follow-up data Individual cases with aberrant behaviour may have significant impact Need for pathologists to be aware of site-specific differences
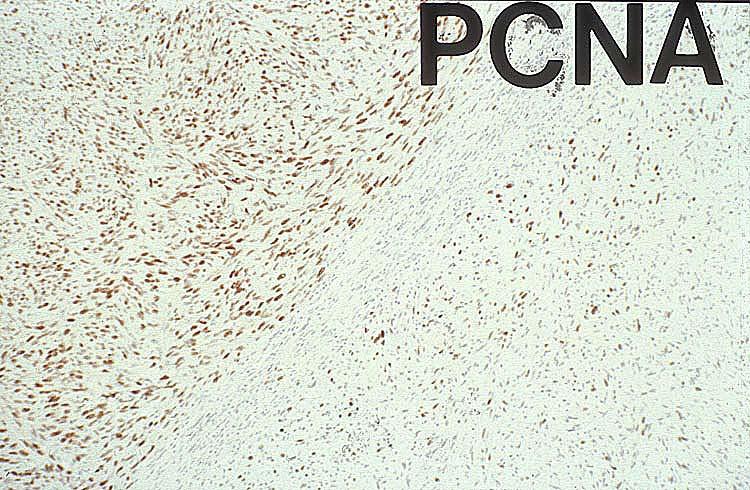
55 MEASURES OF PROLIFERATIVE ACTIVITY Mitotic activity Ki-67 / MIB-1 PCNA DNA polymerase α Cyclins / CDKs S-phase fraction (FCM) AgNORs BrdU / Thymidine labelling The cloak of objectivity.
56
57 SOFT TISSUE SARCOMAS FUSION GENES / BREAKPOINTS CLAIMED TO BE OF PROGNOSTIC VALUE Ewing s / PNET Synovial sarcoma Alveolar rhabdo EWSR1-FLI-1 fusion types SYT-SSX-1 vs. SYT-SSX-2 PAX3-FOXO1A vs. PAX7-FOXO1A Problems of reproducibility/large scale confirmation
58 PUTATIVE PROGNOSTIC RELEVANCE OF FUSION GENES IN EWING S / PNET Breakpoint location in FLI1 gene more important than translocation partner % Cases Med survival Type I EWS exon 7/FLI1 exon > 100 months Type II EWS exon 7/FLI1 exon Approx 2 yrs Now firmly disproved in large EORTC trial (J Clin Oncol 2010; 28: )
59 GENE EXPRESSION FOR PROGNOSIS - THE WAY FORWARD? (1) Large study by French Sarcoma Group 183 1º non-translocation-type sarcomas - validated in independent cohort of 127 cases Genomic profiling 3 groups - simple amplification type (DDLPS) (16%) - few alterations, whole arm / chromosome (23%) - high level of complexity (UPS/LMS) (61%) Genomic complexity histologic grade
60 GENE EXPRESSION FOR PROGNOSIS - THE WAY FORWARD? (2) Then selected genes reflecting (1) greatest CGH imbalance, (2) grade 3 vs 2, (3) chromosome instability final 67 gene set (CINSARC) 1) CINSARC better than FNCLCC grade 2) CINSARC also works in GIST, breast Ca, DLBCL Chibon et al, Nat Med 2010; 16: Needs independent validation
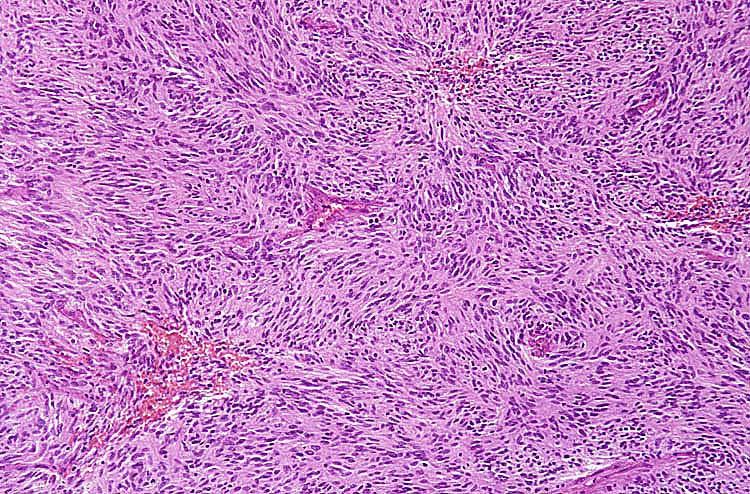
61 SOFT TISSUE TUMOURS WITH MORPHOLOGIC / BIOLOGIC CONTINUUM Smooth muscle tumours GIST Solitary fibrous tumour Ossifying fibromyxoid tumour
62
63
64
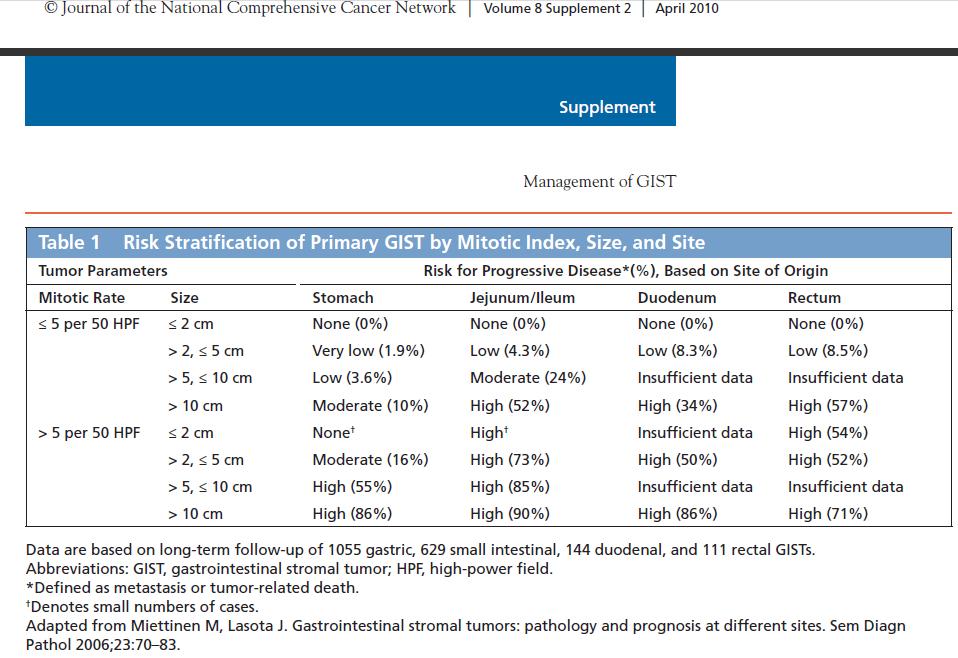
65 PROPOSED GUIDELINES FOR DEFINING RISK OF AGGRESSIVE BEHAVIOUR IN GISTs (NCI 2002) Size Mitotic Count Very low risk < 2 cm < 5 per 50 HPF Low risk 2-5 cm 5 per 50 HPF Intermediate risk 5 cm 5-10 cm > 5 cm 6-10 per 50 HPF 5 per 50 HPF > 5 per 50 HPF High risk > 10 cm > Any size Any mitotic rate > 10 per 50 HPF
66 GASTROINTESTINAL STROMAL TUMOURS PROGNOSTICATION (2002) Unpublished clinical data from large trials of Gleevec Approx. 10% of 1 tumours < 5 cm Approx. 10% of tumours < 5 mitoses / 50 HPF Approx. 15% of primaries were excised 5-10 yrs (or more) earlier
67
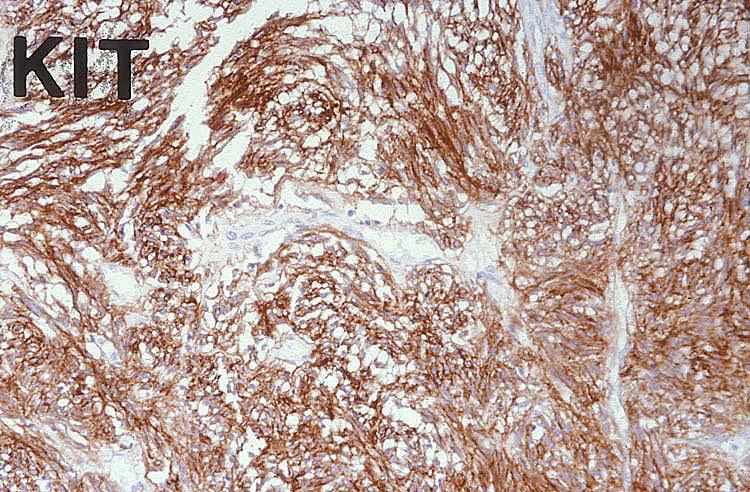
68 GASTROINTESTINAL STROMAL TUMOURS MUTATIONAL ANALYSIS Approx % have KIT mutations and 5-7% have PDGFRA mutations, irrespective of type/size % of cases Gleevec response KIT exon % KIT exon % KIT exon 13 < 5% Too few data KIT exon 17 < 5% Too few data PDGFRA ~ 6% Variable (exons 12/18) Tumors with PDGFRA mutations seem more indolent Tumours lacking either KIT or PDGFRA mutations still show 40-45% response but progress sooner Gleevec response, predicted by mutation type, correlates with survival (resistance due to 2 o mutations)
69
70
71
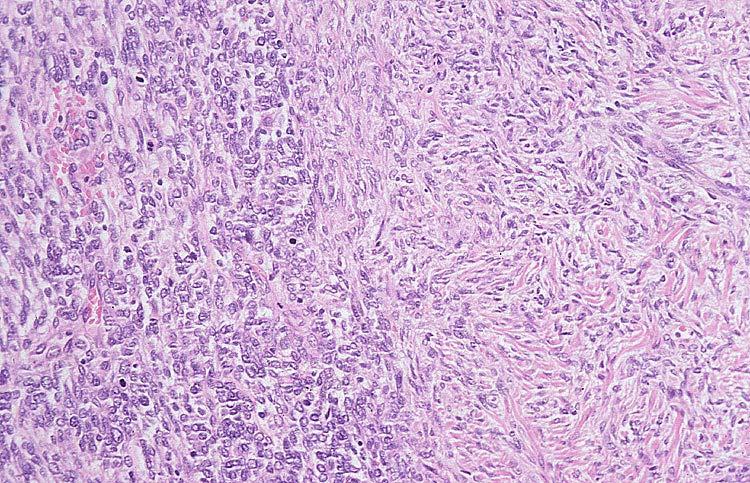
72 SOFT TISSUE TUMOURS WITH MORPHOLOGIC / BIOLOGIC CONTINUUM Sharp dichotomy is not possible (at present) Usual parameters are size and mitotic rate - but cut-offs not well defined To date, most objective parameters have provided no real improvement Morphologically benign lesions in these categories rarely metastasise May use risk assessment as alternative
73 SOFT TISSUE TUMOURS WHICH RARELY METASTASISE, GENERALLY IN THE ABSENCE OF MORPHOLOGIC CLUES Inflammatory myofibroblastic tumour Plexiform fibrohistiocytic tumour So-called angiomatoid MFH Retiform HE / Dabska tumour Others which we more readily accept as sarcoma (e.g. infantile fibrosarcoma)
74
75
76
77
78
79
80
81
82 BENIGN SOFT TISSUE TUMOURS WHICH EXCEPTIONALLY METASTASISE Cutaneous fibrous histiocytoma Diffuse-type giant cell tumour (Smooth muscle tumours) (GIST) Impact of/on pathologists perception

83
84
85
86
87
88
89
90 NOTABLE FEATURES OF METASTASISING CUTANEOUS FH Frequently preceded by repeated local recurrence Predilection to spread to lymph nodes and lung Metastases may be very delayed and may be indolent Metastases usually closely resemble the primary lesion Similar findings in diffuse-type GCT
91
92
93

94
95 CUTANEOUS FH / DERMATOFIBROMA CONSIDERATIONS History of local trauma Spontaneous regression Persistent growth Potential for recurrence Rarely reported metastasis Clonality
96 METASTASING BENIGN TUMOURS POTENTIAL RESPONSES Disbelieve Ignore Regard all histologically similar lesions as sarcomas Acknowledge unpredictability Work towards identification of reliable predictors -? genetic continuum
97 To accept an orthodoxy is always to inherit unresolved contradictions. George Orwell, 1948
98 World Health Organization Classification of Tumours of Soft Tissue BENIGN CATEGORY Most benign soft tissue tumours do not recur locally. Those that do recur do so in a non-destructive fashion and are almost always readily cured by complete local excision. Exceedingly rarely (almost certainly <1/50,000 cases, and probably even less than that), a morphologically benign lesion may give rise to distant metastases. This is entirely unpredictable on the basis of conventional histological examination and, to date, has been best documented in cutaneous benign fibrous histiocytoma.
99 PROGNOSTICATION IN SOFT TISSUE TUMOURS STEPS FORWARD (1) Acknowledgement of uncertainty Acknowledgement of biologic continuum Uncovering of molecular genetic steps
100 Autonomous local growth Local infiltration / invasion + angiogenesis Independent nodal growth Vascular invasion Independent growth in lung (or elsewhere) Local expansion and spread to other sites
101 PROGNOSTICATION IN SOFT TISSUE TUMOURS STEPS FORWARD (2) Larger multicentre collaborative studies Development of more objective approaches (where possible) Histotype-specific grading schemes (where possible) Increasing use of risk assessment
102 A man should never be ashamed to own that he has been wrong, which is but saying, in other words, that he is wiser today than he was yesterday. Jonathan Swift, 1711
Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON
 Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON Presentation outline Background and epidemiology of sarcomas Sarcoma classification Sarcoma
Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON Presentation outline Background and epidemiology of sarcomas Sarcoma classification Sarcoma
Update on Sarcomas of the Head and Neck. Kevin Harrington
 Update on Sarcomas of the Head and Neck Kevin Harrington Overview Classification and incidence of sarcomas Clinical presentation Challenges to treatment Management approaches Prognostic factors Radiation-induced
Update on Sarcomas of the Head and Neck Kevin Harrington Overview Classification and incidence of sarcomas Clinical presentation Challenges to treatment Management approaches Prognostic factors Radiation-induced
Prognostic Significance of Grading and Staging Systems using MIB-1 Score in Adult Patients with Soft Tissue Sarcoma of the Extremities and Trunk
 843 Prognostic Significance of Grading and Staging Systems using MIB-1 Score in Adult Patients with Soft Tissue Sarcoma of the Extremities and Trunk Tadashi Hasegawa, M.D. 1 Seiichiro Yamamoto, Ph.D. 2
843 Prognostic Significance of Grading and Staging Systems using MIB-1 Score in Adult Patients with Soft Tissue Sarcoma of the Extremities and Trunk Tadashi Hasegawa, M.D. 1 Seiichiro Yamamoto, Ph.D. 2
Scandinavian Sarcoma Group and Oncologic Center, Lund, Sweden. Centralized Registration of Sarcoma Patients in Scandinavia SSG VII:4
 Scandinavian Sarcoma Group and Oncologic Center, Lund, Sweden Centralized Registration of Sarcoma Patients in Scandinavia SSG VII:4 Modified April, 2009 Scandinavian Sarcoma Group & Oncologic Center, Lund,
Scandinavian Sarcoma Group and Oncologic Center, Lund, Sweden Centralized Registration of Sarcoma Patients in Scandinavia SSG VII:4 Modified April, 2009 Scandinavian Sarcoma Group & Oncologic Center, Lund,
Conceptual Evolution of Soft Tissue Tumors Classification
 Conceptual Evolution of Soft Tissue Tumors Classification Angelo P. Dei Tos M.D. Departments of Pathology & Oncology Treviso, Italy How WHO classification was reshaped Pathologists and Cytogeneticists
Conceptual Evolution of Soft Tissue Tumors Classification Angelo P. Dei Tos M.D. Departments of Pathology & Oncology Treviso, Italy How WHO classification was reshaped Pathologists and Cytogeneticists
5/10. Pathology Soft tissue tumors. Farah Bhani. Mohammed Alorjani
 5/10 Pathology Soft tissue tumors Mohammed Alorjani Farah Bhani Slides are included in this sheet. Objectives: Soft tissue tumors 1. Describe soft tissue tumors. 2. Understand the classification of soft
5/10 Pathology Soft tissue tumors Mohammed Alorjani Farah Bhani Slides are included in this sheet. Objectives: Soft tissue tumors 1. Describe soft tissue tumors. 2. Understand the classification of soft
Recommendations for Reporting Soft Tissue Sarcomas
 A J C P / REPORTING SOFT TISSUE SARCOMAS Recommendations for Reporting Soft Tissue Sarcomas Association of Directors of Anatomic and Surgical Pathology Key Words: Sarcoma; Soft tissue tumors Abstract The
A J C P / REPORTING SOFT TISSUE SARCOMAS Recommendations for Reporting Soft Tissue Sarcomas Association of Directors of Anatomic and Surgical Pathology Key Words: Sarcoma; Soft tissue tumors Abstract The
Update on Cutaneous Mesenchymal Tumors. Thomas Brenn
 Update on Cutaneous Mesenchymal Tumors Thomas Brenn Cutaneous Mesenchymal Tumours Wide morphological and biological spectrum Myofibroblastic, smooth muscle, neural, vascular, apidocytic, undifferentiated;
Update on Cutaneous Mesenchymal Tumors Thomas Brenn Cutaneous Mesenchymal Tumours Wide morphological and biological spectrum Myofibroblastic, smooth muscle, neural, vascular, apidocytic, undifferentiated;
Contents Part I Introduction 1 General Description 2 Natural History: Importance of Size, Site, Histopathology
 Contents Part I Introduction 1 General Description... 3 1.1 Introduction... 3 1.2 Incidence and Prevalence... 5 1.3 Predisposing and Genetic Factors... 8 References... 16 2 Natural History: Importance
Contents Part I Introduction 1 General Description... 3 1.1 Introduction... 3 1.2 Incidence and Prevalence... 5 1.3 Predisposing and Genetic Factors... 8 References... 16 2 Natural History: Importance
Disclosures. An update on ancillary techniques in the diagnosis of soft tissue tumors. Ancillary techniques. Introduction
 Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Soft Tissue Sarcoma. Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee
 Soft Tissue Sarcoma Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Soft Tissue Sarcoma Collective term for an unusual and diverse
Soft Tissue Sarcoma Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Soft Tissue Sarcoma Collective term for an unusual and diverse
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Classification (1) Classification (3) Classification (2) Spindle cell lesions. Spindle cell lesions of bladder (Mills et al.
 Classification (3) Classification (2) Spindle cell lesions. Spindle cell lesions of bladder (Mills et al.") Non-epithelial tumours and nonepithelial tumour-like lesions of the bladder Dr Jonathan H Shanks The Christie NHS Foundation Trust, Manchester, UK Classification (1) Myofibroblastic proliferations and
Non-epithelial tumours and nonepithelial tumour-like lesions of the bladder Dr Jonathan H Shanks The Christie NHS Foundation Trust, Manchester, UK Classification (1) Myofibroblastic proliferations and
Klinisch belang van chromosomale translocatie detectie in sarcomen
 Translocations in sarcomas Klinisch belang van chromosomale translocatie detectie in sarcomen Judith V.M.G. Bovée, M.D., Ph.D. Department of Pathology Leiden University Medical Center RNA binding DNA binding
Translocations in sarcomas Klinisch belang van chromosomale translocatie detectie in sarcomen Judith V.M.G. Bovée, M.D., Ph.D. Department of Pathology Leiden University Medical Center RNA binding DNA binding
WHO Classification of Soft Tissue Tumours
 WHO Classification of Soft Tissue Tumours This new WHO classification of soft tissue tumours, in line with other volumes in this new series, incorporates detailed clinical, histological and genetic data.
WHO Classification of Soft Tissue Tumours This new WHO classification of soft tissue tumours, in line with other volumes in this new series, incorporates detailed clinical, histological and genetic data.
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis
 Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Soft Tissue Sarcomas: Questions and Answers
 Soft Tissue Sarcomas: Questions and Answers 1. What is soft tissue? The term soft tissue refers to tissues that connect, support, or surround other structures and organs of the body. Soft tissue includes
Soft Tissue Sarcomas: Questions and Answers 1. What is soft tissue? The term soft tissue refers to tissues that connect, support, or surround other structures and organs of the body. Soft tissue includes
Molecular Diagnosis of Soft Tissue Tumors: Avoid Pitfalls
 Molecular Diagnosis of Soft Tissue Tumors: Avoid Pitfalls Cristina Antonescu, MD Department of Pathology Memorial Sloan-Kettering Cancer Center, New York Overview I. When should we rely on the help of
Molecular Diagnosis of Soft Tissue Tumors: Avoid Pitfalls Cristina Antonescu, MD Department of Pathology Memorial Sloan-Kettering Cancer Center, New York Overview I. When should we rely on the help of
Introduction to Musculoskeletal Tumors. James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon
 Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
USCAP COMPANION MEETING INTERNATIONAL SOCIETY OF BONE AND SOFT TISSUE PATHOLOGY DENVER, March 2 nd 2008
 1 USCAP COMPANION MEETING INTERNATIONAL SOCIETY OF BONE AND SOFT TISSUE PATHOLOGY DENVER, March 2 nd 2008 THE EVOLUTION OF SOFT TISSUE TUMOUR TAXONOMY: WHAT STILL NEEDS TO BE DONE? Christopher D.M. Fletcher,
1 USCAP COMPANION MEETING INTERNATIONAL SOCIETY OF BONE AND SOFT TISSUE PATHOLOGY DENVER, March 2 nd 2008 THE EVOLUTION OF SOFT TISSUE TUMOUR TAXONOMY: WHAT STILL NEEDS TO BE DONE? Christopher D.M. Fletcher,
Managing adult soft tissue sarcomas and gastrointestinal stromal tumours
 Managing adult soft tissue sarcomas and gastrointestinal stromal tumours Sarcomas and gastrointestinal stromal tumours include a wide variety of biologically diverse cancers, many of them very rare. Paolo
Managing adult soft tissue sarcomas and gastrointestinal stromal tumours Sarcomas and gastrointestinal stromal tumours include a wide variety of biologically diverse cancers, many of them very rare. Paolo
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Newer soft tissue entities
 Newer soft tissue entities Examples among fibroblastic tumors Turku, May 6, 2010 Markku Miettinen, M.D. AFIP, Washington, DC Fibroblastic neoplasms Solitary fibrous tumor /Hemangiopericytoma Low-grade
Newer soft tissue entities Examples among fibroblastic tumors Turku, May 6, 2010 Markku Miettinen, M.D. AFIP, Washington, DC Fibroblastic neoplasms Solitary fibrous tumor /Hemangiopericytoma Low-grade
3/27/2017. Disclosure of Relevant Financial Relationships
 Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
I sarcomi dei tessuti molli
 Novità e sequenze terapeutiche nelle neoplasie ginecologiche, melanoma e tumori rari: I sarcomi dei tessuti molli Giacomo G. Baldi Oncologia Medica Sandro Pitigliani Nuovo Ospedale S.Stefano Azienda USL
Novità e sequenze terapeutiche nelle neoplasie ginecologiche, melanoma e tumori rari: I sarcomi dei tessuti molli Giacomo G. Baldi Oncologia Medica Sandro Pitigliani Nuovo Ospedale S.Stefano Azienda USL
Protocol for the Examination of Specimens From Patients With Primary Malignant Tumors of the Heart
 Protocol for the Examination of Specimens From Patients With Primary Malignant Tumors of the Heart Protocol applies to primary malignant cardiac tumors. Hematolymphoid neoplasms are not included. No AJCC/UICC
Protocol for the Examination of Specimens From Patients With Primary Malignant Tumors of the Heart Protocol applies to primary malignant cardiac tumors. Hematolymphoid neoplasms are not included. No AJCC/UICC
Chapter 2 Natural History: Importance of Size, Site, and Histopathology
 Chapter 2 Natural History: Importance of Size, Site, and Histopathology Natural History The natural history of soft tissue sarcoma is highly in fl uenced by the site of the primary lesion, tumor histopathology,
Chapter 2 Natural History: Importance of Size, Site, and Histopathology Natural History The natural history of soft tissue sarcoma is highly in fl uenced by the site of the primary lesion, tumor histopathology,
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors
 The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
SMOOTH MUSCLE TUMOURS
 SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
Case Presentation. Gordon Callender M.D. Surgical Resident
 Case Presentation Gordon Callender M.D. Surgical Resident Retroperitoneal Sarcomas Sarcomas Heterogeneous group of rare tumors that arise predominantly from the embryonic mesoderm. Expected incidence for
Case Presentation Gordon Callender M.D. Surgical Resident Retroperitoneal Sarcomas Sarcomas Heterogeneous group of rare tumors that arise predominantly from the embryonic mesoderm. Expected incidence for
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Malcolm Mattes, MD Ajay Tejwani, MD, MPH New York Methodist Hospital
 Malcolm Mattes, MD Ajay Tejwani, MD, MPH New York Methodist Hospital 39 year old female patient who felt a mass in the right gluteal area. Slowly growing over the course of 2 3 months. The mass is associated
Malcolm Mattes, MD Ajay Tejwani, MD, MPH New York Methodist Hospital 39 year old female patient who felt a mass in the right gluteal area. Slowly growing over the course of 2 3 months. The mass is associated
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Overview of Genital Stromal Tumors
 An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine
An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine
* I have no disclosures or any
 Howard Rosenthal, M.D. Associate Professor of Orthopedic Surgery University of Kansas Sarcoma Center I have no disclosures or any conflicts related to the content of this presentation. Objectives 1. Describe
Howard Rosenthal, M.D. Associate Professor of Orthopedic Surgery University of Kansas Sarcoma Center I have no disclosures or any conflicts related to the content of this presentation. Objectives 1. Describe
HOW MAY THE CLASSIFICATION OF SOFT TISSUE TUMORS EVOLVE?
 Spanish Society of Pathology Zaragoza, May 2011 ARTHUR PURDY STOUT SYMPOSIUM HOW MAY THE CLASSIFICATION OF SOFT TISSUE TUMORS EVOLVE? Christopher D.M. Fletcher, M.D., FRCPath Brigham and Women s Hospital
Spanish Society of Pathology Zaragoza, May 2011 ARTHUR PURDY STOUT SYMPOSIUM HOW MAY THE CLASSIFICATION OF SOFT TISSUE TUMORS EVOLVE? Christopher D.M. Fletcher, M.D., FRCPath Brigham and Women s Hospital
G3.02 The malignant potential of the neoplasm should be recorded. CG3.02a
 G3.02 The malignant potential of the neoplasm should be recorded. CG3.02a Conventional adrenocortical neoplasm. Each of the below parameters is scored 0 when absent and 1 when present. 3 or more of these
G3.02 The malignant potential of the neoplasm should be recorded. CG3.02a Conventional adrenocortical neoplasm. Each of the below parameters is scored 0 when absent and 1 when present. 3 or more of these
Disclosures. An update on ancillary techniques in the diagnosis of soft tissue tumors. Ancillary techniques. Introduction
 Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
The Scandinavian Sarcoma Group annual report on extremity and trunk wall soft tissue and bone sarcomas
 The Scandinavian Sarcoma Group annual report on extremity and trunk wall soft tissue and bone sarcomas 2012-2016 1 The SSG annual report on extremity and trunk wall soft tissue and bone sarcomas. The Scandinavian
The Scandinavian Sarcoma Group annual report on extremity and trunk wall soft tissue and bone sarcomas 2012-2016 1 The SSG annual report on extremity and trunk wall soft tissue and bone sarcomas. The Scandinavian
La chemioterapia neoadiuvante nei sarcomi: novità e attuali indicazioni Lorenzo D Ambrosio, MD PhD Divisione di Oncologia Medica Istituto di Candiolo
 La chemioterapia neoadiuvante nei sarcomi: novità e attuali indicazioni Lorenzo D Ambrosio, MD PhD Divisione di Oncologia Medica Istituto di Candiolo Fondazione del Piemonte per l Oncologia. IRCCS 12 CONGRESSO
La chemioterapia neoadiuvante nei sarcomi: novità e attuali indicazioni Lorenzo D Ambrosio, MD PhD Divisione di Oncologia Medica Istituto di Candiolo Fondazione del Piemonte per l Oncologia. IRCCS 12 CONGRESSO
ACCME/Disclosures ALK FUSION-POSITIVE MESENCHYMAL TUMORS. Tumor types with ALK rearrangements. Anaplastic Lymphoma Kinase. Jason L.
 Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Multidisciplinary management of retroperitoneal sarcomas
 Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Slide Seminar Spanish Society of Pathology
 Slide Seminar Spanish Society of Pathology John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine 1921 Original
Slide Seminar Spanish Society of Pathology John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine 1921 Original
INDEX. in this web service Cambridge University Press
 actin 14 adamantinoma 202, 290 292, 297 adenocarcinoma 136 adipocytes in hibernoma 149, 150 in lipoblastoma 148 in lipoma 141, 142, 145 in liposarcoma 152 in myelolipoma 151 adrenal gland tumors see myelolipoma
actin 14 adamantinoma 202, 290 292, 297 adenocarcinoma 136 adipocytes in hibernoma 149, 150 in lipoblastoma 148 in lipoma 141, 142, 145 in liposarcoma 152 in myelolipoma 151 adrenal gland tumors see myelolipoma
Protocol for the Examination of Specimens From Patients With Soft Tissue Tumors
 Protocol for the Examination of Specimens From Patients With Soft Tissue Tumors Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Protocol for the Examination of Specimens From Patients With Soft Tissue Tumors Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Synovial Sarcoma. Dr. Michelle Ghert Dr. Rajiv Gandhi
 Synovial Sarcoma Dr. Michelle Ghert Dr. Rajiv Gandhi Synovial Sarcoma Young adult population (15-40yrs) 5-10% of all soft tissue sarcomas mainly found in the extremities 5 year survival only 60% at presentation;
Synovial Sarcoma Dr. Michelle Ghert Dr. Rajiv Gandhi Synovial Sarcoma Young adult population (15-40yrs) 5-10% of all soft tissue sarcomas mainly found in the extremities 5 year survival only 60% at presentation;
The Completeness of Soft Tissue Sarcoma Data in the National Cancer Data Repository
 The Completeness of Soft Tissue Sarcoma Data in the National Cancer Data Repository Tumours diagnosed between 2006 and 2008 West Midlands Cancer Intelligence Unit Completeness of cancer data 2008 Soft
The Completeness of Soft Tissue Sarcoma Data in the National Cancer Data Repository Tumours diagnosed between 2006 and 2008 West Midlands Cancer Intelligence Unit Completeness of cancer data 2008 Soft
Leiomyosarcoma of the inferior vena cava: 1 case. B. Bancel, A. Rode, C. Ducerf. Hôpital CROIX ROUSSE LYON. Case report
 Leiomyosarcoma of the inferior vena cava: 1 case B. Bancel, A. Rode, C. Ducerf Hôpital CROIX ROUSSE LYON Bucharest Nov 2011 Case report 34 yr-old woman, no antecedent Sept 2004: Abdominal upper right quadrant
Leiomyosarcoma of the inferior vena cava: 1 case B. Bancel, A. Rode, C. Ducerf Hôpital CROIX ROUSSE LYON Bucharest Nov 2011 Case report 34 yr-old woman, no antecedent Sept 2004: Abdominal upper right quadrant
Predictive biomarker profiling of > 1,900 sarcomas: Identification of potential novel treatment modalities
 Predictive biomarker profiling of > 1,900 sarcomas: Identification of potential novel treatment modalities Sujana Movva 1, Wenhsiang Wen 2, Wangjuh Chen 2, Sherri Z. Millis 2, Margaret von Mehren 1, Zoran
Predictive biomarker profiling of > 1,900 sarcomas: Identification of potential novel treatment modalities Sujana Movva 1, Wenhsiang Wen 2, Wangjuh Chen 2, Sherri Z. Millis 2, Margaret von Mehren 1, Zoran
Q&A. Fabulous Prizes. Collecting Cancer Data: Bone and Soft Tissue 1/10/113. NAACCR Webinar Series
 Collecting Cancer Data Bone & Soft Tissue NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data Bone & Soft Tissue NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Printed by Maria Chen on 3/11/2012 5:46:52 AM. For personal use only. Not approved for distribution. Copyright 2012 National Comprehensive Cancer
 , Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
, Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Research Article A Clinicopathological Analysis of Soft Tissue Sarcoma with Telangiectatic Changes
 Sarcoma Volume 2015, Article ID 740571, 5 pages http://dx.doi.org/10.1155/2015/740571 Research Article A Clinicopathological Analysis of Soft Tissue Sarcoma with Telangiectatic Changes Hiroshi Kobayashi,
Sarcoma Volume 2015, Article ID 740571, 5 pages http://dx.doi.org/10.1155/2015/740571 Research Article A Clinicopathological Analysis of Soft Tissue Sarcoma with Telangiectatic Changes Hiroshi Kobayashi,
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Molecular pathology in soft tissue tumors. Sylvia Höller Pathologie
 Molecular pathology in soft tissue tumors Sylvia Höller Pathologie When do we perform molecular testing? Morphology and IHC are not clearly fitting with an entity some translocations are entity specific
Molecular pathology in soft tissue tumors Sylvia Höller Pathologie When do we perform molecular testing? Morphology and IHC are not clearly fitting with an entity some translocations are entity specific
2010 Update. NAACCR Webinar Series 1 4/1/2010. Agenda. Access to 2010 Information. CSv2. Collecting Cancer Data: Soft Tissue Sarcoma
 NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Soft Tissue Sarcoma, Neuroendocrine Tumors (NET) and Gastrointestinal Stromal Tumors (GIST) Agenda Updates Soft Tissue Sarcoma Overview CSv2 MP/H
NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Soft Tissue Sarcoma, Neuroendocrine Tumors (NET) and Gastrointestinal Stromal Tumors (GIST) Agenda Updates Soft Tissue Sarcoma Overview CSv2 MP/H
Financial disclosures
 An update on immunohistochemical markers in mesenchymal neoplasms By Konstantinos Linos MD, FCAP, FASDP Assistant Professor of Pathology Geisel School of Medicine at Dartmouth Dartmouth-Hitchcock Medical
An update on immunohistochemical markers in mesenchymal neoplasms By Konstantinos Linos MD, FCAP, FASDP Assistant Professor of Pathology Geisel School of Medicine at Dartmouth Dartmouth-Hitchcock Medical
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Diagnostic problems in uterine smooth muscle tumors
 Diagnostic problems in uterine smooth muscle tumors Marina Kos Ljudevit Jurak Clinical Department of Pathology, Clinical Hospital Center Sestre milosrdnice, Zagreb Institute of Pathology, University of
Diagnostic problems in uterine smooth muscle tumors Marina Kos Ljudevit Jurak Clinical Department of Pathology, Clinical Hospital Center Sestre milosrdnice, Zagreb Institute of Pathology, University of
ESS: Pathologic Insights
 GEIS XVI INTERNATIONAL SYMPOSIUM Seville 4th October 2018 ESS: Pathologic Insights Sílvia Bagué The Royal Marsden Hospital London (United Kingdom) I have no conflicts of interest Endometrial stromal sarcoma
GEIS XVI INTERNATIONAL SYMPOSIUM Seville 4th October 2018 ESS: Pathologic Insights Sílvia Bagué The Royal Marsden Hospital London (United Kingdom) I have no conflicts of interest Endometrial stromal sarcoma
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Case Report Primary Small Bowel Liposarcoma (Atypical Lipomatous Tumour) with Myogenic Differentiation
 with Myogenic Differentiation") Sarcoma Volume 2010, Article ID 807981, 4 pages doi:10.1155/2010/807981 Case Report Primary Small Bowel Liposarcoma (Atypical Lipomatous Tumour) with Myogenic Differentiation J. Patel, R. Deb, W. Speake,
Sarcoma Volume 2010, Article ID 807981, 4 pages doi:10.1155/2010/807981 Case Report Primary Small Bowel Liposarcoma (Atypical Lipomatous Tumour) with Myogenic Differentiation J. Patel, R. Deb, W. Speake,
Rare Cancers. Andrew J. Wagner, MD, PhD Center for Sarcoma and Bone Oncology Dana-Farber Cancer Institute Sarcoma Patient Symposium October 15, 2017
 Rare Cancers Andrew J. Wagner, MD, PhD Center for Sarcoma and Bone Oncology Dana-Farber Cancer Institute Sarcoma Patient Symposium October 15, 2017 Why should we care about Rare Cancers? Raise your hand
Rare Cancers Andrew J. Wagner, MD, PhD Center for Sarcoma and Bone Oncology Dana-Farber Cancer Institute Sarcoma Patient Symposium October 15, 2017 Why should we care about Rare Cancers? Raise your hand
Molecular Genetics of Paediatric Tumours. Gino Somers MBBS, BMedSci, PhD, FRCPA Pathologist-in-Chief Hospital for Sick Children, Toronto, ON, CANADA
 Molecular Genetics of Paediatric Tumours Gino Somers MBBS, BMedSci, PhD, FRCPA Pathologist-in-Chief Hospital for Sick Children, Toronto, ON, CANADA Financial Disclosure NanoString - conference costs for
Molecular Genetics of Paediatric Tumours Gino Somers MBBS, BMedSci, PhD, FRCPA Pathologist-in-Chief Hospital for Sick Children, Toronto, ON, CANADA Financial Disclosure NanoString - conference costs for
A 25 year old female with a palpable mass in the right lower quadrant of her abdomen
 May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
Soft Tissue Sarcoma Early Detection, Diagnosis, and Staging
 Soft Tissue Sarcoma Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can
Soft Tissue Sarcoma Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can
Molecular pathology/genetics of sarcomas
 Molecular pathology/genetics of sarcomas Gunhild Mechtersheimer Institute of Pathology, University of Heidelberg Sarkomkonferenz: 17.03.2011 Berlin Characterization of soft tissue sarcomas / STS (~ 1%
Molecular pathology/genetics of sarcomas Gunhild Mechtersheimer Institute of Pathology, University of Heidelberg Sarkomkonferenz: 17.03.2011 Berlin Characterization of soft tissue sarcomas / STS (~ 1%
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Dystrophin Is a Tumor Suppressor in Human Cancers with Myogenic Programs
 SUPPLEMENTARY INFORMATION Dystrophin Is a Tumor Suppressor in Human Cancers with Myogenic Programs Yuexiang Wang 1, Adrian Marino-Enriquez 1, Richard R. Bennett 2, Meijun Zhu 1, Yiping Shen 3,4, Grant
SUPPLEMENTARY INFORMATION Dystrophin Is a Tumor Suppressor in Human Cancers with Myogenic Programs Yuexiang Wang 1, Adrian Marino-Enriquez 1, Richard R. Bennett 2, Meijun Zhu 1, Yiping Shen 3,4, Grant
Morphologically Benign Lesions of Soft Tissue and Bone Which Metastasize - What Can We Do?
 Andrew L. Folpe, MD Mayo Clinic, Rochester, MN ISBSTP Handout 2010 Morphologically Benign Lesions of Soft Tissue and Bone Which Metastasize - What Can We Do? Introduction Over the past several decades
Andrew L. Folpe, MD Mayo Clinic, Rochester, MN ISBSTP Handout 2010 Morphologically Benign Lesions of Soft Tissue and Bone Which Metastasize - What Can We Do? Introduction Over the past several decades
Prognostic Factors in Soft Tissue Sarcoma
 13 Prognostic Factors in Soft Tissue Sarcoma Luiz Eduardo Moreira Teixeira, Jose Carlos Vilela and Ivana Duval De Araujo Federal University of Minas Gerais Brazil 1. Introduction Soft tissue sarcoma (STS)
13 Prognostic Factors in Soft Tissue Sarcoma Luiz Eduardo Moreira Teixeira, Jose Carlos Vilela and Ivana Duval De Araujo Federal University of Minas Gerais Brazil 1. Introduction Soft tissue sarcoma (STS)
Neoplasia literally means "new growth.
 NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
Protocol for the Examination of Specimens from Patients with Tumors of Soft Tissue
 Protocol for the Examination of Specimens from Patients with Tumors of Soft Tissue Protocol applies to soft tissue tumors of intermediate (locally aggressive) and intermediate (rarely metastasizing) potential
Protocol for the Examination of Specimens from Patients with Tumors of Soft Tissue Protocol applies to soft tissue tumors of intermediate (locally aggressive) and intermediate (rarely metastasizing) potential
21/07/2017. Hobnail endothelial cells are not the same as epithelioid endothelial cells
 UPDATE IN CUTANEOUS VASCULAR S DERMATOPATHOLOGY SESSION BELFAST PATHOLOGY JUNE 21/2017 Dr E Calonje St John s Institute of Dermatology, London, United Kingdom THE FAMILY OF VASCULAR S WITH EPITHELIOID
UPDATE IN CUTANEOUS VASCULAR S DERMATOPATHOLOGY SESSION BELFAST PATHOLOGY JUNE 21/2017 Dr E Calonje St John s Institute of Dermatology, London, United Kingdom THE FAMILY OF VASCULAR S WITH EPITHELIOID
Disclosure of Relevant Financial Relationships
 Evening Specialty Conference - Genitourinary Pathology Case 2 Disclosure of Relevant Financial Relationships Sean R Williamson, MD Henry Ford Health System, Detroit, MI @Williamson_SR USCAP requires that
Evening Specialty Conference - Genitourinary Pathology Case 2 Disclosure of Relevant Financial Relationships Sean R Williamson, MD Henry Ford Health System, Detroit, MI @Williamson_SR USCAP requires that
Diagnostic Value of Immunohistochemistry in Soft Tissue Tumors
 Original Article DOI: 10.21276/APALM.1637 Diagnostic Value of Immunohistochemistry in Soft Tissue Tumors Sridevi. V*., Susruthan Muralitharan., and Thanka. J Dept of Pathology, SriMuthukumaran Medical
Original Article DOI: 10.21276/APALM.1637 Diagnostic Value of Immunohistochemistry in Soft Tissue Tumors Sridevi. V*., Susruthan Muralitharan., and Thanka. J Dept of Pathology, SriMuthukumaran Medical
Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology
 David M. Parham, MD Chief of Anatomic Pathology") Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology Tumors of skeletal muscle: Rhabdomyomas and rhabdomyosarcomas Embryonal muscle 2 3 4 5 6 7 8 Rhabdomyoma Benign
Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology Tumors of skeletal muscle: Rhabdomyomas and rhabdomyosarcomas Embryonal muscle 2 3 4 5 6 7 8 Rhabdomyoma Benign
Canine Mast Cell Tumors
 Canine Mast Cell Tumors By: Dr. Custead WVRC Introduction Mast cells Resident inflammatory cell of the skin, lungs, gastro- intestinal tract Reactions secondary to IgE binding Allergic reactions Granules
Canine Mast Cell Tumors By: Dr. Custead WVRC Introduction Mast cells Resident inflammatory cell of the skin, lungs, gastro- intestinal tract Reactions secondary to IgE binding Allergic reactions Granules
Case 8 Soft tissue swelling
 Case 8 Soft tissue swelling 26-year-old female presented with a swelling on the back of the left knee joint since the last 6 months and chronic pain in the calf and foot since the last 2 months. Pain in
Case 8 Soft tissue swelling 26-year-old female presented with a swelling on the back of the left knee joint since the last 6 months and chronic pain in the calf and foot since the last 2 months. Pain in
Diagnostic Approach to Soft Tissue Tumors
 SECTION 2 Diagnostic Approach to Soft Tissue Tumors Overview Biopsy and Resection of Soft Tissue Tumors 20 Clinical Approach Age- and Location-Based Approach to Diagnosis 24 Histologic Approach Pattern-Based
SECTION 2 Diagnostic Approach to Soft Tissue Tumors Overview Biopsy and Resection of Soft Tissue Tumors 20 Clinical Approach Age- and Location-Based Approach to Diagnosis 24 Histologic Approach Pattern-Based
category cm0. Category will ensure it T1 melanoma. 68 Retinoblastoma
 AJCC 8 th Edition Chapter 1 Principles of Cancer Staging: Node Status Not Required in Rare Circumstances Clinical Staging, cn Category For some cancer sites in which lymph node involvement is rare, patients
AJCC 8 th Edition Chapter 1 Principles of Cancer Staging: Node Status Not Required in Rare Circumstances Clinical Staging, cn Category For some cancer sites in which lymph node involvement is rare, patients
Slide seminar. Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana
 Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Financial disclosures
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
LAC + USC.
 Jeff McDavit,, M.D. LAC + USC mcdavit@usc.edu Clinical History 55 year old male with large, deep, non- tender left thigh mass. Seen at LAC+USC Med Ctr FNA clinic No h/o trauma or radiation Vimentin
Jeff McDavit,, M.D. LAC + USC mcdavit@usc.edu Clinical History 55 year old male with large, deep, non- tender left thigh mass. Seen at LAC+USC Med Ctr FNA clinic No h/o trauma or radiation Vimentin
Spindle Cell Lesions Of The Breast. Emad Rakha Professor of Breast Pathology and Consultant Pathologist
 Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Slide seminar: Soft tissue and bone pathology
 Slide seminar: Soft tissue and bone pathology Unusual tumors of bone and soft tissue or unusual presentations of common ones Gunhild Mechtersheimer Institute of Pathology, Heidelberg/DE (Sylvia Höller,
Slide seminar: Soft tissue and bone pathology Unusual tumors of bone and soft tissue or unusual presentations of common ones Gunhild Mechtersheimer Institute of Pathology, Heidelberg/DE (Sylvia Höller,
3/25/2019. Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates
 Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates") J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates Signs
J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates Signs
Grading of Bone Tumors
 Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Hsin-Nung Shih M.D. Soft Tissue Tumor
 Soft Tissue Tumor Hsin-Nung Shih M.D. PROFESSOR DIVISION OF JOINT RECONSTRUCTION DEPARTMENT OF ORTHOPEADIC CHANG GUNG MEMORIAL HOSPITAL CHANG GUNG UNIVERSITY,COLLEGE OF MEDICINE TAIWAN Soft Tissue Tumor
Soft Tissue Tumor Hsin-Nung Shih M.D. PROFESSOR DIVISION OF JOINT RECONSTRUCTION DEPARTMENT OF ORTHOPEADIC CHANG GUNG MEMORIAL HOSPITAL CHANG GUNG UNIVERSITY,COLLEGE OF MEDICINE TAIWAN Soft Tissue Tumor
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
Update On Lipomatous Tumors: Old Standbys and New Concepts
 Update On Lipomatous Tumors: Old Standbys and New Concepts John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine
Update On Lipomatous Tumors: Old Standbys and New Concepts John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
Table 1 Histiogenic Classification and Metastatic Potential of Canine Soft Tissue Sarcomas Tissue of Origin Benign Malignant Primary Sites
 Soft Tissue Sarcomas Incidence and Risk Factors Soft tissue sarcomas are a heterogeneous population of mesenchymal tumours representing 15% of skin and subcutaneous tumours in the dog and 7% in the cat.
Soft Tissue Sarcomas Incidence and Risk Factors Soft tissue sarcomas are a heterogeneous population of mesenchymal tumours representing 15% of skin and subcutaneous tumours in the dog and 7% in the cat.