Nuevas alternativas en el manejo de TNE avanzados
|
|
|
- Loreen Webster
- 5 years ago
- Views:
Transcription

1 Nuevas alternativas en el manejo de TNE avanzados Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Coordinación científica: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla, Santander Organizado por: Fundación para el progreso de la oncología en Cantabria
2 Treatments Classification/Guidelines PROGRESS IN THE LAND OF NENS / AJCC/UICC TNM classification GI/pNET / ENETS guidelines including TC/AC Karzinoide coined by Oberndofer 1 WHO classification Carcinoids 3 WHO classification NET and NEC 6 ENETS guidelines 4 ; TNM staging 5,7 NANETS guidelines 8 ESMO guidelines 22, 27 WHO classification Lung NET/carcinoids 35 WHO classification GEP- NENs / / / / STZ pnet 36 OCT SC CS 25, STZ combination: survival benefit pnet 2 LAN symptom control 24 OCT LAR carcinoid tumors 23,26, /11 PROMID OCT LAR: antitumor activity 9,31 RADIANT-3 EVE in pnet 11,12,32,33 Sunitinib phase 3 pnet 13,31,34 CLARINET LAN GEP NET 16,17,29 ELECT LAN: symptom control 27 RADIANT-4 EVE NF GI and lung NET 15, TELESTAR telotristat etiprate CS 20 NDA filed 3/30/16 US Approv al US/EU Approv al EU Approv al RADIANT-2 EVE + OCT, LAR in mnet w/cs 14 NETTER Lu-Dotatate midgut NET 18
3 Frilling A, et al Lancet Oncol 2014
4 ADVANCED NENS THERAPEUTIC ALGORITHM Unresectable NENs Si-NET pannet LUNG NET NEN G3 G1 G2 G1 G2 G1 G2 NETG3 NECG3 Octreotide (PROMID) Everolimus RADIANT-4 Chemotherapy Lanreotide (CLARINET) Somatostatin Analogues Somatostatin Analogues? Everolimus RADIANT-3 & RADIANT-4 Chemotherapy Targeted agents? PRRT NETTER-1 Interferon Sunitinib Chemotherapy
 12 24 36 48 72 96 Study visits (weeks)")
5 PROMID AND CLARINET STUDIES Screening period Treatment period weeks* CT scan 1 CT scan 2 Lanreotide Autogel 120 mg s.c. every 28 days Randomization 1:1 Placebo s.c. every 28 days 1 (baseline) Study visits (weeks)
6 RADIANT PROGRAM RAD001 IN NEUROENDOCRINE TUMORS RADIANT-1 Phase II Pancreatic NETs Everolimus w/wo Octreotide LAR E E+O ORR 9.6% PFS 9.7m ORR 4.4% PFS 16.7m RADIANT-2 Phase III Non- Pancreatic NETs Octreotide LAR + Everolimus vs Octreotide LAR + placebo 16.4 vs 11.3m HR 0.77 P=0.026 (one sided) RADIANT-3 Phase III Pancreatic NETs Everolimus vs Placebo 11 vs 4.6m HR 0.35 P<0.001 RADIANT-4 Phase III GI & Lung NETs Everolimus vs Placebo 11 vs 3.9m HR 0.48 P<
7 RADIANT-4 STUDY DESIGN Patients with welldifferentiated (G1/G2), advanced, progressive, nonfunctional NET of lung or GI origin (N=302) Absence of active or any history of carcinoid syndrome Pathologically confirmed advanced disease Radiologic disease progression in 6 months R A N D O M I Z E 2:1 Everolimus 10 mg/day N=205 Placebo N=97 Treated until PD, intolerable AE, or consent withdrawal Endpoints: Primary: PFS (central) Key Secondary: OS Secondary: ORR, DCR, safety, HRQoL (FACT-G), WHO PS, NSE/CgA, PK Stratified by: Prior SSA treatment (yes vs. no) Tumor origin (stratum A vs. B)* WHO PS (0 vs. 1) *Based on prognostic level, grouped as: Stratum A (better prognosis) appendix, caecum, jejunum, ileum, duodenum, and NET of unknown primary. Stratum B (worst prognosis) lung, stomach, rectum, and colon except caecum. Crossover to open-label everolimus after progression in the placebo arm was not allowed prior to the primary analysis. Yao JC, et al. Lancet 2016
8 Probability of Progression-free Survival (%) PRIMARY ENDPOINT: PFS BY CENTRAL REVIEW 52% reduction in the relative risk of progression or death with everolimus vs placebo HR = 0.48 (95% CI, ); P < No.of patients still at risk Censoring Times Everolimus (n/n = 113/205) Placebo (n/n = 65/97) Kaplan Meier medians Everolimus: 11.0 months (95% CI, ) Placebo: 3.9 months (95% CI, ) Months Everolimus Placebo P-value is obtained from the stratified one-sided log-rank test; Hazard ratio is obtained from stratified Cox model. CI, confidence interval; HR, hazard ratio. Yao JC, et al. Lancet 2016
9 Probability of Overall Survival (%) INTERIM OVERALL SURVIVAL ANALYSIS First interim OS analysis performed with 37% of information fraction favored the everolimus arm Everolimus vs Placebo HR = 0.64 (95% CI, ); P = (NS)* Censoring Times Everolimus (n/n = 42/205) Placebo (n/n = 28/97) Next interim analysis is expected in Months No. of patients still at risk Everolimus Placebo *P-value boundary for significance = P-value is obtained from the stratified one-sided log-rank test; Hazard ratio is obtained from stratified Cox model. NS, not significant. Yao JC, et al. Lancet 2016
10 PFS HR BY PRIMARY TUMOR ORIGIN RETROSPECTIVE ANALYSIS, CENTRAL REVIEW Subgroups* No. Hazard Ratio (95% CI) Lung ( ) GI ( ) NET of unknown primary ( ) Everolimus Better Placebo Better *One patient with thymus as primary tumor origin was not included. Stomach, colon, rectum, appendix, cecum, ileum, duodenum, and jejunum are grouped under GI. Hazard ratio obtained from unstratified Cox model. GI, gastrointestinal; NET, neuroendocrine tumors. Yao JC, et al. Lancet 2016


11 Pavel M, et al. Lancet, 2011
12 NETTER -1 STUDY DESIGN Aim Design Evaluate the efficacy and safety of 177 Lu-Dotatate (Lutathera ) plus Octreotide30 mg compared to Novartis Octreotide LAR 60mg (off-label use) 1 in patients with inoperable, somatostatin receptor positive, midgut NET, progressive under Octreotide LAR 30mg (label use) International, multicenter, randomized, comparator-controlled, parallelgroup Treatment and Assessments Progression free survival (Recist criteria) every 12 weeks Dose 1 Dose 2 Dose 3 Dose 4 Baseline and Randomization n = 115 n = administrations of 7.4 GBq of LUTATHERA every 8 weeks + Octreotide30 mg Octreotide LAR 60mg every 4 weeks 5 Years follow up Strosberg J, et al. N Engl J Med 2017
13 POPULATION CHARACTERISTICS AT ENROLLMENT (N=229) 177 Lu-Dotatate (n=116) Octreotide LAR 60mg (n=113) Age (years), mean (SD) 63 (±9) 64 (±10) Gender, n (%) Male Female Primary tumor site, n (%) Jejunum Ileum Appendix Right colon Other Site of metastasis, n (%) Liver Lymph nodes Bone Lungs Other 53 (46%) 63 (54%) 6 (5%) 86 (74%) 1 (1%) 3 (3%) 20 (17%) 97 (84%) 77 (66%) 13 (11%) 11 (10%) 40 (35%) 60 (53%) 53 (47%) 9 (8%) 82 (73%) 2 (2%) 1 (1%) 19 (17%) 94 (83%) 65 (58%) 12 (11%) 5 (4%) 37 (33%) Strosberg J, et al. N Engl J Med 2017
14 PRIMARY ENDPOINT: PROGRESSION-FREE SURVIVAL Strosberg J, et al. ENETS 2018
15 SECONDARY ENDPOINT: OVERALL SURVIVAL Strosberg J, et al. ENETS 2018
16 SWOG S0518 STUDY DESIGN Study population Advanced G1/2 NET with poor prognosis Progressive disease Refractory syndrome G2 with 6+ lesion Colorectal or gastric primary R A N D O M I Z E 1:1 Bevacizumab 15 mg/kg q21 d octreotide LAR 20 mg q21 d Treatment until disease progression Interferon α-2b 5 mu 3 d/wk octreotide LAR 20 mg q21 d Multiphasic CT or MRI performed every 9 wk Primary endpoint: PFS (Central radiology review) Stratification factors: Primary site: Midgut vs others PD since diagnosis Histologic grade: G1 vs G2 Octreotide 2 months prior to registration Yao JC, et al. ASCO 2015



 Serotonin")
17 TELOTRISTAT ETIPRATE THE PHASE III TELESTAR CLINICAL TRIAL Serotonin Hormonal syndrome Diarrhoea... 5-HIAA Urine 5-HIAA: 5-hydroxyindole acetic acid SSA somatostatin analogue SSTR somatostatin receptor Serotonin Tryptophanhydroxylase Tryptophan 5-Hydroxytryptophan (5- HTP) Serotonin (5-HT) NET-cell Telotristat etiprate SSTR SSA
18 TELESTAR PHASE 3 STUDY DESIGN 3- to 4-week run-in (n=135) Run in: Evaluation of bowel movement (BM) frequency 1:1:1 R Placebo TID (n=45) Telotristat etiprate 250 mg TID (n=45) Telotristat etiprate 500 mg TID* (n=45) Telotristat etiprate 500 mg TID Evaluation of primary endpoint: Reduction in number of daily BMs from baseline (averaged over 12- week double-blind treatment phase) All patients required to be on SSA at enrollment and continue SSA therapy throughout study period Kulke M, et al. J Clin Oncol 2017

 0.69 for telotristat etiprate 500 mg dose (P<0.001) BM, bowel movement.")
19 TELESTAR: REDUCTION IN DAILY BOWEL MOVEMENT FREQUENCY AVERAGED OVER DOUBLE-BLIND TREATMENT PHASE Hodges Lehmann estimator of treatment differences showed a median reduction versus placebo of 0.81 BMs daily for telotristat etiprate 250 mg dose (P<0.001) 0.69 for telotristat etiprate 500 mg dose (P<0.001) BM, bowel movement. Kulke M, et al. J Clin Oncol 2017
20 TREATMENT ALGORITHM IN sinets 1 st Treatment option SOMATOSTATIN ANALOGUES: Functioning & non-functioning Octreoscan +ive & -ive Ki67 up to 10% 2 nd Treatment option 3 rd Treatment option 4 th Treatment option EVEROLIMUS (EVEROLIMUS + SSAs) Non-functioning (functioning) Octreoscan +ive & -ive High & low tumor burden 177 Lu-DOTATATE Functioning & non-functioning Octreoscan +ive INTERFERON Indication based on a negative trial & old trials
21 ADVANCED NENS THERAPEUTIC ALGORITHM Unresectable NENs Si-NET pannet LUNG NET NEN G3 G1 G2 G1 G2 G1 G2 NETG3 NECG3 Octreotide (PROMID) Everolimus RADIANT-4 Chemotherapy Lanreotide (CLARINET) Somatostatin Analogues Somatostatin Analogues? Everolimus RADIANT-3 & RADIANT-4 Chemotherapy Targeted agents? PRRT NETTER-1 Interferon Sunitinib Chemotherapy
22 Patients Alive and With No Progression, % CLARINET PFS IN ENTEROPANCREATIC NET PFS in midgut vs pancreatic NET 100 Mi d g u t NE T s ( n = 7 3 ) La nr e ot i de Au t o g e l vs p l aceb o P = HR = [ 9 5 % C I : , ] 100 pn E T s (n = 9 1 ) La nr e ot i de Au t o g e l vs p l aceb o P = HR = [ 9 5 % C I : , ] Lan r eot i de A u t ogel 120 m g 8 e v e n t s / 3 3 p a t i e n t s m e d i a n, n o t r e a ch e d Lan r eot i de A u t ogel 120 m g 1 8 e v e n t s / 4 2 p a t i e n t s m e d i a n, n o t r e a ch e d P l a ce b o 2 1 e v e n t s / 4 0 p a t i e n t s m e d i a n, m o n t h s [ 9 5 % C I : , N C ] P l a ce b o 3 1 e v e n t s / 4 9 p a t i e n t s m e d i a n, m o n t h s [ 9 5 % C I : 9. 4, ] Ti m e, m o nt hs Ti m e, m o nt hs Caplin ME, et al. N Engl J Med. 2014

23 RADIANT-3: STUDY DESIGN Phase III, Double-Blind, Placebo-Controlled Trial Patients with advanced pnet (N = 410) Advanced well or moderately differentiated Radiologic progression 12 months Prior antitumour therapy allowed WHO PS 2 Stratified by: WHO PS Prior chemotherapy R A N D O M I S E 1:1 Everolimus 10 mg/d + best supportive care 1 n = 207 Crossover at disease progression Placebo + best supportive care 1 n = 203 Multiphasic CT or MRI performed every 12 weeks Treatment until disease progression Primary Endpoint: Progression-free survival By investigator review Secondary Endpoints: OS, ORR, biomarkers, safety, pharmacokinetics (PK) 1 Concurrent somatostatin analogues allowed Yao JC, et al. N Engl J Med. 2011
24 % Event-free RADIANT-3 PFS BY CENTRAL REVIEW COMMITTEE Kaplan-Meier median PFS Everolimus: 11.0 months Placebo: 4.6 months Hazard ratio = 0.35; 95% CI P value: < Censoring times Everolimus (n/n = 109/207) Placebo (n/n = 165/203) Time (months) Yao JC, et al. N Engl J Med. 2011
25 EVEROLIMUS IS CLINICALLY BENEFICIAL REGARDLESS OF PRIOR CHEMOTHERAPY USE p value is obtained from the unstratified one-sided log-rank test. Hazard ratio is obtained from unstratified unadjusted Cox model. In the everolimus arm, median PFS did not significantly differ in patients who did and did not receive prior chemotherapy In the placebo arm, a trend toward shorter median PFS was observed in patients who had received prior chemotherapy compared with chemo-naive patients Lombard-Bohas C, et al. J Clin Oncol. 2012; 30 suppl. 34; abstract # 224.
26 SUNITINIB VS PLACEBO IN ADVANCED PNET Phase III randomised, placebo-controlled, double-blind trial Trial terminated after unplanned early analysis Well differentiated advanced pnet patients (N = 171 enrolled / 340 planned) Disease progression in past 12 mos Not amenable to curative treatment R A N D O M I S E 1:1 Sunitinib 37.5 mg/day orally Continuous daily dosing* n = 86 Placebo* n = 85 * With best supportive care Somatostatin analogues were permitted Primary Endpoint: PFS Secondary Endpoints: OS ORR TTR Duration of response Safety Patient-reported outcomes Raymond E, et al. N Engl J Med. 2011
27 Percentage of event-free SUNITINIB VS PLACEBO IN ADVANCED PNET Kaplan-Meier median PFS Sunitinib: 11.4 months Placebo: 5.5 months HR = 0.42 ; 95% CI [ ] P value <.001; nominal critical z value = Number at risk: Sunitinib Placebo 20 0 Censoring times Sunitinib (n/n = 30/86) Placebo (n/n = 51/85) Time (months) * Local review Raymond E, et al. N Engl J Med. 2011

28 Change from baseline (%) DEGREE OF TUMOUR SHRINKAGE IN THE SUNITINIB PHASE III STUDY Maximum change from baseline of target lesions in patients from the sunitinib phase III study* Sunitinib Placebo SD PD: 20% increase PR: 30% decrease Confirmed partial or complete response The RECIST-defined ORR in patients receiving sunitinib was 9.3%; however, the majority of patients had some degree of tumour shrinkage (Clinical Benefit Rate 72%) Raymond E, et al. N Engl J Med. 2011
29 ESTIMATES OF OVERALL SURVIVAL Faivre S, et al. Ann Oncol 2016
30 STZ-BASED CHEMOTHERAPY IN PNETS Moertel C, et al. N Engl J Med, 1992

31 TEMOZOLOMIDE + CAPECITABINE Crespo G, et al. Future Oncol 2016

32 TEMOZOLOMIDE + CAPECITABINE
 G3-4 AEs: 22% vs 44% (p=0.")
33 TEMOZOLOMIDE + CAPECITABINE RR: 28% vs 33% (p=0.47) G3-4 AEs: 22% vs 44% (p=0.007)

34 THERAPEUTIC ALGORITHM FOR pannets 1 st Treatment option SOMATOSTATIN ANALOGUES: Functioning & non-functioning Octreoscan +ive Ki up to 10% Not too much liver involvement 2 nd Treatment option 1 st Treatment option EVEROLIMUS / SUNITINIB / CHT Progressive disease Higher tumor burden Symptoms related with tumor burden EVEROLIMUS / SUNITINIB / CHT Sequential therapies
35 ADVANCED NENS THERAPEUTIC ALGORITHM Unresectable NENs Si-NET pannet LUNG NET NEN G3 G1 G2 G1 G2 G1 G2 NETG3 NECG3 Octreotide (PROMID) Everolimus RADIANT-4 Chemotherapy Lanreotide (CLARINET) Somatostatin Analogues Somatostatin Analogues? Everolimus RADIANT-3 & RADIANT-4 Chemotherapy Targeted agents? PRRT NETTER-1 Interferon Sunitinib Chemotherapy
36 PFS HR BY PRIMARY TUMOR ORIGIN RETROSPECTIVE ANALYSIS, CENTRAL REVIEW Subgroups No. Hazard Ratio (95% CI) Lung ( ) GI* ( ) NET of unknown primary (n=36) or Others (n=8) ( ) Everolimus Better Placebo Better *Stomach, colon, rectum, appendix, cecum, ileum, duodenum, and jejunum are grouped under GI tract. Yao JC, et al. Lancet 2016

37 LOW EFFICACY EVIDENCE OF CHEMOTHERAPY IN G1/G2 LUNG NETS Granberg D, et al. Ann Oncol 2011

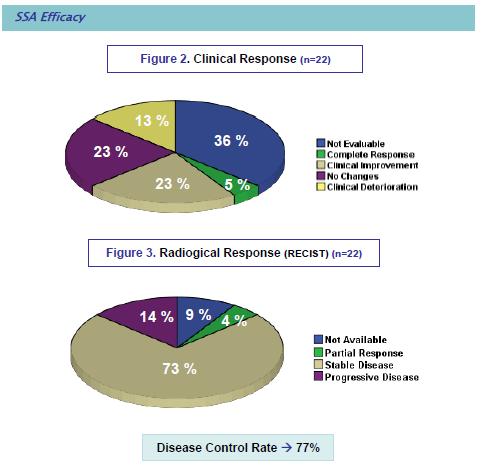
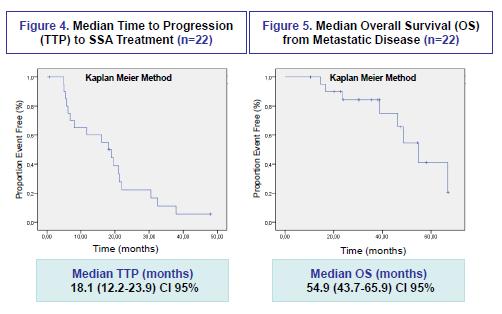
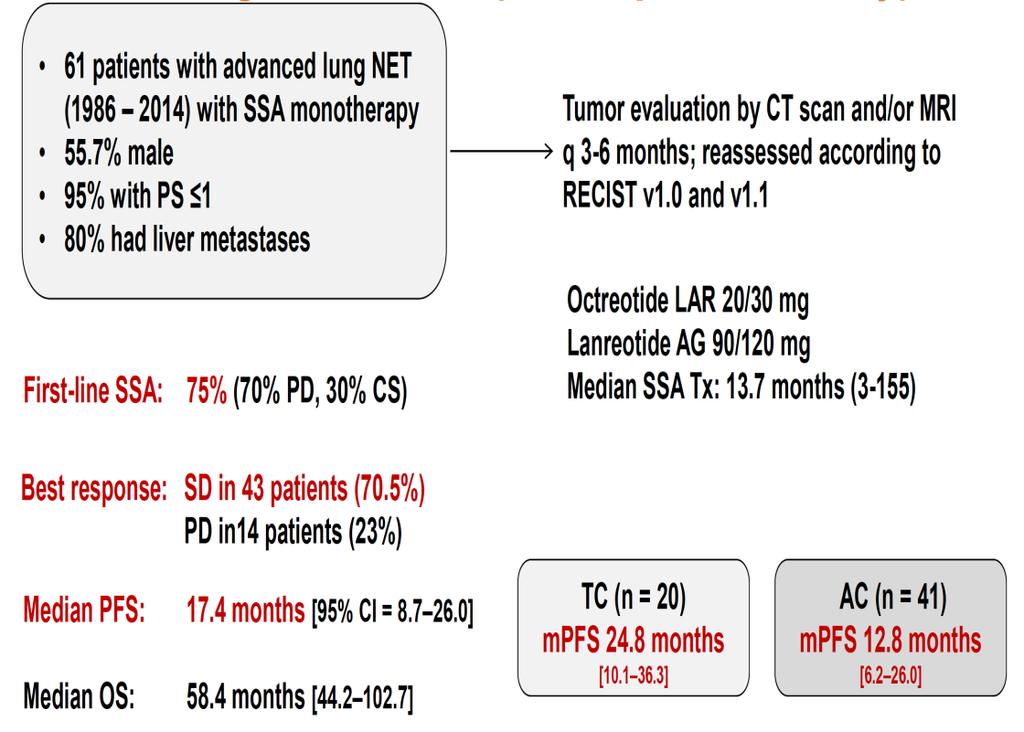
38 RETROSPECTIVE EFFICACY EVIDENCE OF SSAs IN LUNG NETS Sullivan I, et al. Eur J Cancer 2017
 Typical (atypical) 2 nd Treatment option EVEROLIMUS 3 rd Treatment")
39 THERAPEUTIC ALGORITHM FOR LUNG NETS 1 st Treatment option SOMATOSTATIN ANALOGUES Functioning & non-functioning Octreoscan +ive (mainly) Typical (atypical) 2 nd Treatment option EVEROLIMUS 3 rd Treatment option CHT / PRRT
40 ADVANCED NENS THERAPEUTIC ALGORITHM Unresectable NENs Si-NET pannet LUNG NET NEN G3 G1 G2 G1 G2 G1 G2 NETG3 NECG3 Octreotide (PROMID) Everolimus RADIANT-4 Chemotherapy Lanreotide (CLARINET) Somatostatin Analogues Somatostatin Analogues? Everolimus RADIANT-3 & RADIANT-4 Chemotherapy Targeted agents? PRRT NETTER-1 Interferon Sunitinib Chemotherapy
")
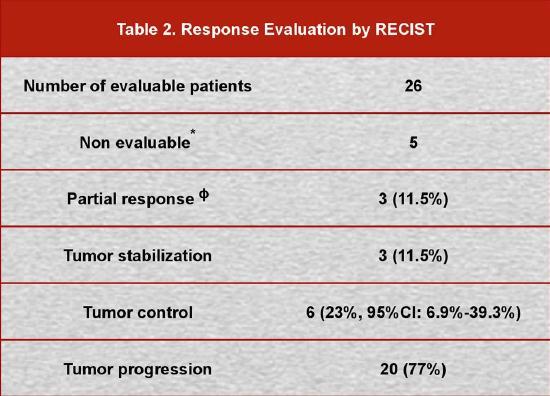
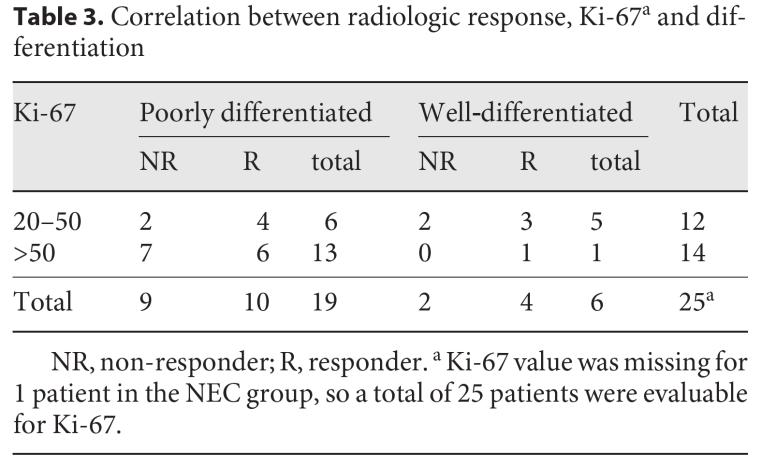
41 NET G3 (40%) Small cellnec G3 (95%) Ki-67
42
43
44 Nuñez-Valdovinos B, et al. The Oncologist 2018

45 SUGGESTED CHEMOTHERAPY IN FIRST-LINE REGARDING NEW CLASSIFICATION Fazio N & Milione M. Cancer Treatment Reviews 2016

46 Pellat A, et al. Neuroendocrinology 2017 SUNITINIB IN NET G3
47 PRRT IN NET G3 G1 & G2 tumors show comparable response to PRRT Up to Ki67 of 20%, no impaired response Potential cut-off for treatment failure >30-40% 1 (up to 55% last ENETS 2018 meeting 2 ) No differences of PRRT benefit comparing Ki67 index of 10, 15 and 20% 1 1.Ezziddin S, et al. Eur J Nucl Med Skovgaard D, et al. ENETS 2018

48
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS
 TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
NET εντέρου Τι νεότερο/ Νέες μελέτες. Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ
 NET εντέρου Τι νεότερο/ Νέες μελέτες Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ NET: A Diverse Group of Malignancies 1-3 Wide spectrum of malignancies arising in neuroendocrine cells throughout the body
NET εντέρου Τι νεότερο/ Νέες μελέτες Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ NET: A Diverse Group of Malignancies 1-3 Wide spectrum of malignancies arising in neuroendocrine cells throughout the body
Review of Gastrointestinal Carcinoid Tumors: Latest Therapies
 Review of Gastrointestinal Carcinoid Tumors: Latest Therapies Arvind Dasari, MD, MS Department of Gastrointestinal Medical Oncology The University of Texas MD Anderson Cancer Center Houston, TX, USA Neuroendocrine
Review of Gastrointestinal Carcinoid Tumors: Latest Therapies Arvind Dasari, MD, MS Department of Gastrointestinal Medical Oncology The University of Texas MD Anderson Cancer Center Houston, TX, USA Neuroendocrine
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology
 Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
MEDICAL MANAGEMENT OF METASTATIC GEP-NET
 MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS
 OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS Dr Mairéad McNamara Senior lecturer, University of Manchester & Honorary Consultant in Medical Oncology, The Christie NHS Foundation Trust
OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS Dr Mairéad McNamara Senior lecturer, University of Manchester & Honorary Consultant in Medical Oncology, The Christie NHS Foundation Trust
Selection of Appropriate Treatment
 Expert Review in Metastatic Gastroenteropancreatic Neuroendocrine Tumors (GEP-NETs): Selection of Appropriate Treatment Reference Slide Deck Neuroendocrine Tumors (NETs): A Diverse Group of Malignancies
Expert Review in Metastatic Gastroenteropancreatic Neuroendocrine Tumors (GEP-NETs): Selection of Appropriate Treatment Reference Slide Deck Neuroendocrine Tumors (NETs): A Diverse Group of Malignancies
Evaluation and Management of Neuroendocrine Tumors
 Evaluation and Management of Neuroendocrine Tumors Jennifer Chan, MD, MPH Clinical Director, Program in Neuroendocrine and Carcinoid Tumors Dana-Farber/Brigham and Women's Cancer Center October 14, 2017
Evaluation and Management of Neuroendocrine Tumors Jennifer Chan, MD, MPH Clinical Director, Program in Neuroendocrine and Carcinoid Tumors Dana-Farber/Brigham and Women's Cancer Center October 14, 2017
2015: Year in Review Results of Recent Trials
 2015: Year in Review Results of Recent Trials Pamela L. Kunz, MD Assistant Professor of Medicine / GI Oncology Director, Stanford NET Program Stanford University School of Medicine Disclosures Research
2015: Year in Review Results of Recent Trials Pamela L. Kunz, MD Assistant Professor of Medicine / GI Oncology Director, Stanford NET Program Stanford University School of Medicine Disclosures Research
GEP NET: algoritmo terapeutico. Dottor Nicola Fazio
 GEP NET: algoritmo terapeutico Dottor Nicola Fazio Basi per il trattamento Caratteristiche del paziente Caratteristiche del tumore P.S., sindrome, comorbidità Differenziazione, Ki-67 Imaging morfologico
GEP NET: algoritmo terapeutico Dottor Nicola Fazio Basi per il trattamento Caratteristiche del paziente Caratteristiche del tumore P.S., sindrome, comorbidità Differenziazione, Ki-67 Imaging morfologico
Teresa Alonso Gordoa Servicio Oncología Médica Hospital Universitario Ramón y Cajal
 Teresa Alonso Gordoa Servicio Oncología Médica Hospital Universitario Ramón y Cajal Incidence per 100,000 EPIDEMIOLOGY Incidence rates of neuroendocrine tumors by primary tumor site 1.4 1.2 1.0 0.8 0.6
Teresa Alonso Gordoa Servicio Oncología Médica Hospital Universitario Ramón y Cajal Incidence per 100,000 EPIDEMIOLOGY Incidence rates of neuroendocrine tumors by primary tumor site 1.4 1.2 1.0 0.8 0.6
Pancreatic NeuroEndocrine Tumors. Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium
 Pancreatic NeuroEndocrine Tumors Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Epidemiology Overall incidence 1.8 to 2.6 SEER, Europe Peak in 5 th and 6 th decade Incidence
Pancreatic NeuroEndocrine Tumors Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Epidemiology Overall incidence 1.8 to 2.6 SEER, Europe Peak in 5 th and 6 th decade Incidence
Recent developments of oncology in neuroendocrine tumors (NETs)
") Recent developments of oncology in neuroendocrine tumors (NETs) Marc Peeters MD, PhD Coordinator Multidisciplinary Oncological Center Antwerpen (MOCA) Head of the Oncology Department UZA, Professor in
Recent developments of oncology in neuroendocrine tumors (NETs) Marc Peeters MD, PhD Coordinator Multidisciplinary Oncological Center Antwerpen (MOCA) Head of the Oncology Department UZA, Professor in
WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer
 WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer Institute Overview Diagnosis: Gallium scan Biomarkers
WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer Institute Overview Diagnosis: Gallium scan Biomarkers
New Developments in the Care and Management of Patients with Gastroenteropancreatic Neuroendocrine Tumors Dr. Tim Asmis The Ottawa Hospital Cancer
 New Developments in the Care and Management of Patients with Gastroenteropancreatic Neuroendocrine Tumors Dr. Tim Asmis The Ottawa Hospital Cancer Centre MD, FRCPC CAGPO September 2018 Disclosures Consultant
New Developments in the Care and Management of Patients with Gastroenteropancreatic Neuroendocrine Tumors Dr. Tim Asmis The Ottawa Hospital Cancer Centre MD, FRCPC CAGPO September 2018 Disclosures Consultant
Le target therapy nei Tumori Neuroendocrini
 Le target therapy nei Tumori Neuroendocrini Take home messages Franco Grimaldi SOC Endocrinologia e Malattie del Metabolismo Nutrizione Clinica Azienda Ospedaliero-Universitaria Santa Maria della Misericordia
Le target therapy nei Tumori Neuroendocrini Take home messages Franco Grimaldi SOC Endocrinologia e Malattie del Metabolismo Nutrizione Clinica Azienda Ospedaliero-Universitaria Santa Maria della Misericordia
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Hot of the press. Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ
 Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives
 Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives Moderator: Ashley Grossman, MD, FRCP Professor of Neuroendocrinology William Harvey Research Institute Barts
Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives Moderator: Ashley Grossman, MD, FRCP Professor of Neuroendocrinology William Harvey Research Institute Barts
NET del pancreas ben differenziato: la terapia oncologica. Alfredo Berru: Università degli Studi di Brescia Azienda Ospedaliera Spedali Civili Brescia
 NET del pancreas ben differenziato: la terapia oncologica Alfredo Berru: Università degli Studi di Brescia Azienda Ospedaliera Spedali Civili Brescia Systemic treatment op:ons Somatosta:n analogues Interpheron
NET del pancreas ben differenziato: la terapia oncologica Alfredo Berru: Università degli Studi di Brescia Azienda Ospedaliera Spedali Civili Brescia Systemic treatment op:ons Somatosta:n analogues Interpheron
Antiangiogenics are effective treatments in NETs
 RENET: A randomized phase III trial comparing REgorafenib to placebo in patients with advanced, progressive, well-differentiated NEuroendocrine Tumors (NETs). Coordinators: Dr Julien Hadoux & Dr David
RENET: A randomized phase III trial comparing REgorafenib to placebo in patients with advanced, progressive, well-differentiated NEuroendocrine Tumors (NETs). Coordinators: Dr Julien Hadoux & Dr David
Pancreatic Neuroendocrine Tumours
 UCLH Cancer Collaborative Pancreas Update Meeting 12 th July 2017 Pancreatic Neuroendocrine Tumours Dr. Christos Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior
UCLH Cancer Collaborative Pancreas Update Meeting 12 th July 2017 Pancreatic Neuroendocrine Tumours Dr. Christos Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior
TUMORES NEUROENDOCRINOS. Miguel Navarro. Salamanca
 TUMORES NEUROENDOCRINOS Miguel Navarro. Salamanca Introduction to Neuroendocrine Tumours (NETs) NETs are relatively RARE At least 40 different entities are described arising in different organs. Different
TUMORES NEUROENDOCRINOS Miguel Navarro. Salamanca Introduction to Neuroendocrine Tumours (NETs) NETs are relatively RARE At least 40 different entities are described arising in different organs. Different
Chair s presentation Lutetium (177lu) oxodotreotide for treating unresectable or metastatic neuroendocrine tumours in people with progressive disease
 oxodotreotide for treating unresectable or metastatic neuroendocrine tumours in people with progressive disease") Public slides Chair s presentation Lutetium (177lu) oxodotreotide for treating unresectable or metastatic neuroendocrine tumours in people with progressive disease 2 nd Appraisal Committee meeting Committee
Public slides Chair s presentation Lutetium (177lu) oxodotreotide for treating unresectable or metastatic neuroendocrine tumours in people with progressive disease 2 nd Appraisal Committee meeting Committee
Background. Capdevila J, et al. Ann Oncol. 2018;29(Suppl 8): Abstract 1307O. 1. Dasari A, et al. JAMA Oncol. 2017;3(10):
: Abstract 1307O. 1. Dasari A, et al. JAMA Oncol. 2017;3(10):") Efficacy of Lenvatinib in Patients With Advanced Pancreatic (pannets) and Gastrointestinal (ginets) WHO Grade 1/2 (G1/G2) Neuroendocrine Tumors: Results of the International Phase II TALENT Trial (GETNE
Efficacy of Lenvatinib in Patients With Advanced Pancreatic (pannets) and Gastrointestinal (ginets) WHO Grade 1/2 (G1/G2) Neuroendocrine Tumors: Results of the International Phase II TALENT Trial (GETNE
Octreotide LAR in neuroendocrine tumours a summary of the experience
 Endocrinology in oncology Review article Octreotide LAR in neuroendocrine tumours a summary of the experience Agnieszka Kolasińska-Ćwikła, MD, PhD Department of Chemotherapy, Oncology Clinic, Maria Sklodowska-Curie
Endocrinology in oncology Review article Octreotide LAR in neuroendocrine tumours a summary of the experience Agnieszka Kolasińska-Ćwikła, MD, PhD Department of Chemotherapy, Oncology Clinic, Maria Sklodowska-Curie
Tumor Growth Rate (TGR) A New Indicator of Antitumor Activity in NETS? IPSEN NET Masterclass Athens, 12 th November 2016
 A New Indicator of Antitumor Activity in NETS? IPSEN NET Masterclass Athens, 12 th November 2016") 1 Tumor Growth Rate (TGR) A New Indicator of Antitumor Activity in NETS? IPSEN NET Masterclass Athens, 12 th November 2016 Philippe RUSZNIEWSKI ENETS Centre of Excellence, Beaujon Hospital, Clichy, France
1 Tumor Growth Rate (TGR) A New Indicator of Antitumor Activity in NETS? IPSEN NET Masterclass Athens, 12 th November 2016 Philippe RUSZNIEWSKI ENETS Centre of Excellence, Beaujon Hospital, Clichy, France
NICaN Pancreatic Neuroendocrine Tumour SACT protocols. 1.0 Dr M Eatock Final version issued
 Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
QOL Improvements in NETTER-1 Phase III Trial in Patients With Progressive Midgut Neuroendocrine Tumors
 QOL Improvements in NETTER-1 Phase III Trial in Patients With Progressive Midgut Neuroendocrine Tumors Abstract C-33 Strosberg J, Wolin E, Chasen B, Kulke M, Bushnell D, Caplin M, Baum RP, Kunz P, Hobday
QOL Improvements in NETTER-1 Phase III Trial in Patients With Progressive Midgut Neuroendocrine Tumors Abstract C-33 Strosberg J, Wolin E, Chasen B, Kulke M, Bushnell D, Caplin M, Baum RP, Kunz P, Hobday
Management of Neuroendocrine Tumors
 Management of Neuroendocrine Tumors Professor Barbro Eriksson Department of Endocrine Oncology ENETS Centre of Excellence Uppsala University Hospital Diagnostic Challenges in NET Heterogeneous group of
Management of Neuroendocrine Tumors Professor Barbro Eriksson Department of Endocrine Oncology ENETS Centre of Excellence Uppsala University Hospital Diagnostic Challenges in NET Heterogeneous group of
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust
 GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
SUPPLEMENTARY INFORMATION
 Supplementary Table 1. Therapies for non-men1 pancreatic neuroendocrine tumours (NETs) (published after 2011) Somatostatin analogues Tumour type a Intervention Number of participants/information available
Supplementary Table 1. Therapies for non-men1 pancreatic neuroendocrine tumours (NETs) (published after 2011) Somatostatin analogues Tumour type a Intervention Number of participants/information available
Ongoing and future clinical investigation in GEP NENs
 ESMO PRECEPTORSHIP PROGRAMME Multidisciplinary management, standards of care and future perspectives Lugano, Switzerland 13-14 April 2018 CHAIR: Nicola Fazio, Italy George Pentheroudakis, Greece Ongoing
ESMO PRECEPTORSHIP PROGRAMME Multidisciplinary management, standards of care and future perspectives Lugano, Switzerland 13-14 April 2018 CHAIR: Nicola Fazio, Italy George Pentheroudakis, Greece Ongoing
Carcinoma de Tiroide: Teràpies Diana
 Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
OVERVIEW OF THE DIAGNOSIS AND TREATMENT OF GI NETS
 OVERVIEW OF THE DIAGNOSIS AND TREATMENT OF GI NETS Dr Christos G. Toumpanakis MD PhD FRCP FEBGH Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University College of London Neuroendocrine
OVERVIEW OF THE DIAGNOSIS AND TREATMENT OF GI NETS Dr Christos G. Toumpanakis MD PhD FRCP FEBGH Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University College of London Neuroendocrine
NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες
 NETMASTERCLASS 2017: an interactive workshop NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες Νικόλαος Τσουκαλάς MD, MSc, PhD Ογκολόγος - Παθολόγος, MSc Βιοπληροφορική Επιμελητής Α, Ογκολογικό Τμήμα Νοσηλευτικό
NETMASTERCLASS 2017: an interactive workshop NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες Νικόλαος Τσουκαλάς MD, MSc, PhD Ογκολόγος - Παθολόγος, MSc Βιοπληροφορική Επιμελητής Α, Ογκολογικό Τμήμα Νοσηλευτικό
A New Proposal for Metabolic Classification of NENs Stefano Severi IRST Meldola Italy
 RADIONUCLIDE THERAPY AND ALLIED SCIENCE President: Giovanni Paganelli Chairman: Maria Salvato Baltimore USA Domenico Barone Meldola Italy A New Proposal for Metabolic Classification of NENs Stefano Severi
RADIONUCLIDE THERAPY AND ALLIED SCIENCE President: Giovanni Paganelli Chairman: Maria Salvato Baltimore USA Domenico Barone Meldola Italy A New Proposal for Metabolic Classification of NENs Stefano Severi
PNET 3/7/2015. GI and Pancreatic NETs. The Postgraduate Course in Breast and Endocrine Surgery. Decision Tree. GI and Pancreatic NETs.
 GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT )
") An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT02267967) J.M. Xu a, J. Li b, C.M. Bai c, N. Xu d, Z.W. Zhou e, Z.P. Li f, C.C. Zhou g, W. Wang h, J. Li
An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT02267967) J.M. Xu a, J. Li b, C.M. Bai c, N. Xu d, Z.W. Zhou e, Z.P. Li f, C.C. Zhou g, W. Wang h, J. Li
*Bert Bakker was an employee of Novartis Pharmaceuticals Corporation until June 06, 2014.
 Page 1 of 20 Accepted Preprint first posted on 15 September 2015 as Manuscript ERC-15-0314 1 2 Efficacy of Octreotide LAR in Neuroendocrine Tumors: RADIANT-2 Placebo Arm Post Hoc Analysis 3 4 Authors:
Page 1 of 20 Accepted Preprint first posted on 15 September 2015 as Manuscript ERC-15-0314 1 2 Efficacy of Octreotide LAR in Neuroendocrine Tumors: RADIANT-2 Placebo Arm Post Hoc Analysis 3 4 Authors:
Systematic Review of the Role of Targeted Therapy in Metastatic Neuroendocrine Tumors
 At the Cutting Edge Received: February 29, 2016 Accepted: April 12, 2016 Published online: April 16, 2016 Systematic Review of the Role of Targeted Therapy in Metastatic Neuroendocrine Tumors Adrian Lee
At the Cutting Edge Received: February 29, 2016 Accepted: April 12, 2016 Published online: April 16, 2016 Systematic Review of the Role of Targeted Therapy in Metastatic Neuroendocrine Tumors Adrian Lee
The Antiproliferative Role of Lanreotide in Controlling Growth of Neuroendocrine Tumors: A Systematic Review
 Gastrointestinal Cancer The Antiproliferative Role of Lanreotide in Controlling Growth of Neuroendocrine Tumors: A Systematic Review MICHAEL MICHAEL, a ROCIO GARCIA-CARBONERO, b MATTHIAS M. WEBER, c CATHERINE
Gastrointestinal Cancer The Antiproliferative Role of Lanreotide in Controlling Growth of Neuroendocrine Tumors: A Systematic Review MICHAEL MICHAEL, a ROCIO GARCIA-CARBONERO, b MATTHIAS M. WEBER, c CATHERINE
Guideline A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO)
, Cancer Care Ontario (CCO)") A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Systemic Therapy of Incurable Gastroenteropancreatic Neuroendocrine Tumours S. Singh, D. Sivajohanathan, T.
A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Systemic Therapy of Incurable Gastroenteropancreatic Neuroendocrine Tumours S. Singh, D. Sivajohanathan, T.
Recent Advances in Gastrointestinal Cancers
 Recent Advances in Gastrointestinal Cancers Ursina R. Teitelbaum, MD Section of Hematology/Oncology Abramson Cancer Center PENN 2016 Updates in Oncology June 23, 2016 none Disclosures ASCO 2016 Highlights:
Recent Advances in Gastrointestinal Cancers Ursina R. Teitelbaum, MD Section of Hematology/Oncology Abramson Cancer Center PENN 2016 Updates in Oncology June 23, 2016 none Disclosures ASCO 2016 Highlights:
Inhibidores de PARP en cáncer de ovario
 Inhibidores de PARP en cáncer de ovario Ma Pilar Barretina Ginesta Servicio Oncología Médica Hospital Universitari Dr. J. Trueta Institut Català d Oncologia Coordinación científica: Dr. Fernando Rivera
Inhibidores de PARP en cáncer de ovario Ma Pilar Barretina Ginesta Servicio Oncología Médica Hospital Universitari Dr. J. Trueta Institut Català d Oncologia Coordinación científica: Dr. Fernando Rivera
Telotristat Ethyl (etiprate) : a new kid on the block Dr. Christos G. Toumpanakis MD PhD FRCP
 : a new kid on the block Dr. Christos G. Toumpanakis MD PhD FRCP") Telotristat Ethyl (etiprate) : a new kid on the block Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University College of London Neuroendocrine
Telotristat Ethyl (etiprate) : a new kid on the block Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University College of London Neuroendocrine
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Everolimus, lutetium-177 DOTATATE and sunitinib for treating unresectable or metastatic neuroendocrine tumours with disease progression MTA
 Everolimus, lutetium-177 DOTATATE and sunitinib for treating unresectable or metastatic neuroendocrine tumours with disease progression MTA 1 st Appraisal Committee meeting Cost Effectiveness Committee
Everolimus, lutetium-177 DOTATATE and sunitinib for treating unresectable or metastatic neuroendocrine tumours with disease progression MTA 1 st Appraisal Committee meeting Cost Effectiveness Committee
IART Cremona,
 IART Cremona, 06-06-2018 Quale spazio per la terapia biologica? Nicola Fazio, M.D., Ph. D. Unit of Gastrointestinal Medical Oncology and Neuroendocrine Tumors European Institute of Oncology Milan, Italy
IART Cremona, 06-06-2018 Quale spazio per la terapia biologica? Nicola Fazio, M.D., Ph. D. Unit of Gastrointestinal Medical Oncology and Neuroendocrine Tumors European Institute of Oncology Milan, Italy
Collaborative Practice in the Management of Patients With Gastrointestinal and Pancreatic Neuroendocrine Tumors
 Collaborative Practice in the Management of Patients With Gastrointestinal and Pancreatic Neuroendocrine Tumors Collaborative Practice in the Management of Patients With Gastrointestinal and Pancreatic
Collaborative Practice in the Management of Patients With Gastrointestinal and Pancreatic Neuroendocrine Tumors Collaborative Practice in the Management of Patients With Gastrointestinal and Pancreatic
Treatment algorithm Neuroendocrine tumours. Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece
 Treatment algorithm Neuroendocrine tumours Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece Outline Presenting a meaningful algorithm Means used to develop algorithm
Treatment algorithm Neuroendocrine tumours Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece Outline Presenting a meaningful algorithm Means used to develop algorithm
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO. Dra. Ruth Vera Complejo Hospitalario de Navarra
 MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
CRITICAL ANALYSIS OF NEN GUIDELINES. G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines
 CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
Prior Authorization Review Panel MCO Policy Submission
 Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors?
 Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
PANCREATIC NEUROENDOCRINE TUMORS DECEMBER 12, 2017 IF YOU EXPERIENCE TECHNICAL DIFFICULTY DURING THE PRESENTATION:
 PANCREATIC NEUROENDOCRINE TUMORS DECEMBER 12, 2017 IF YOU EXPERIENCE TECHNICAL DIFFICULTY DURING THE PRESENTATION: CONTACT WEBEX TECHNICAL SUPPORT DIRECTLY AT: US TOLL FREE: 1-866-779-3239 TOLL ONLY: 1-408-435-7088
PANCREATIC NEUROENDOCRINE TUMORS DECEMBER 12, 2017 IF YOU EXPERIENCE TECHNICAL DIFFICULTY DURING THE PRESENTATION: CONTACT WEBEX TECHNICAL SUPPORT DIRECTLY AT: US TOLL FREE: 1-866-779-3239 TOLL ONLY: 1-408-435-7088
An Overview of NETS. Richard R.P. Warner M.D
 An Overview of NETS Richard R.P. Warner M.D Diagnosis and Treatment Approaches Carcinoid (and other NETs) not as benign as originally described 13-50% of all carcinoids have distant metastases when first
An Overview of NETS Richard R.P. Warner M.D Diagnosis and Treatment Approaches Carcinoid (and other NETs) not as benign as originally described 13-50% of all carcinoids have distant metastases when first
An Immunotherapy Clinical Trial for NETs
 An Immunotherapy Clinical Trial for NETs Pamela L. Kunz, MD Assistant Professor of Medicine / Oncology Stanford Cancer InsEtute March 1, 2015 Outline Clinical trial basics What have we learned from recent
An Immunotherapy Clinical Trial for NETs Pamela L. Kunz, MD Assistant Professor of Medicine / Oncology Stanford Cancer InsEtute March 1, 2015 Outline Clinical trial basics What have we learned from recent
Therapeutic Radiopharmaceuticals in Oncology
 Therapeutic Radiopharmaceuticals in Oncology Policy Number: 6.01.60 Last Review: 9/2018 Origination: 9/2018 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Therapeutic Radiopharmaceuticals in Oncology Policy Number: 6.01.60 Last Review: 9/2018 Origination: 9/2018 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Factors Affecting Survival in Neuroendocrine Tumors: A 15-Year Single Center Experience
 RESEARCH ARTICLE Editorial Process: Submission:00/00/0000 Acceptance:00/00/0000 : A 15-Year Single Center Experience Abdullah Sakin 1 *, Makbule Tambas 2, Saban Secmeler 3, Orçun Can 3, Serdar Arici 3,
RESEARCH ARTICLE Editorial Process: Submission:00/00/0000 Acceptance:00/00/0000 : A 15-Year Single Center Experience Abdullah Sakin 1 *, Makbule Tambas 2, Saban Secmeler 3, Orçun Can 3, Serdar Arici 3,
The PET-NET Study 2016 CNETS Grant Award
 The PET-NET Study 2016 CNETS Grant Award CANM Meeting April 21, 2017 Hagen Kennecke, MD, MHA, FRCPC Medical Oncology, BC Cancer Agency Associate Professor, University of British Columbia Raja Ampat, Indonesia
The PET-NET Study 2016 CNETS Grant Award CANM Meeting April 21, 2017 Hagen Kennecke, MD, MHA, FRCPC Medical Oncology, BC Cancer Agency Associate Professor, University of British Columbia Raja Ampat, Indonesia
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC
 Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Neuroendocrine Tumors Positron Emission Tomography (PET) Imaging and Peptide Receptor Radionuclide Therapy
 Imaging and Peptide Receptor Radionuclide Therapy") Neuroendocrine Tumors Positron Emission Tomography (PET) Imaging and Peptide Receptor Radionuclide Therapy Lawrence Saperstein, M.D. Assistant Professor of Radiology and Biomedical Imaging Chief, Nuclear
Neuroendocrine Tumors Positron Emission Tomography (PET) Imaging and Peptide Receptor Radionuclide Therapy Lawrence Saperstein, M.D. Assistant Professor of Radiology and Biomedical Imaging Chief, Nuclear
Advanced typical and atypical carcinoid tumours of the lung: management recommendations
 REVIEW ARTICLE Advanced typical and atypical carcinoid tumours of the lung: management recommendations B. Melosky md* ABSTRACT Background Neuroendocrine tumours (nets) are classified by site of origin,
REVIEW ARTICLE Advanced typical and atypical carcinoid tumours of the lung: management recommendations B. Melosky md* ABSTRACT Background Neuroendocrine tumours (nets) are classified by site of origin,
Inmunoterapia en el carcinoma de Células de Merkel. Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona
 Inmunoterapia en el carcinoma de Células de Merkel Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Epidemiology Merkel cell carcinoma is an uncommon neuroendocrine carcinoma that mostly arises
Inmunoterapia en el carcinoma de Células de Merkel Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Epidemiology Merkel cell carcinoma is an uncommon neuroendocrine carcinoma that mostly arises
Development of New Treatment Modalities Oncolytic Viruses and Nanotechnique
 Development of New Treatment Modalities Oncolytic Viruses and Nanotechnique By Professor Kjell Öberg, M.D., Ph.D. Dept. of Endocrine Oncology, University Hospital, Uppsala, Sweden Nashville Oct. 2011 Hallmarks
Development of New Treatment Modalities Oncolytic Viruses and Nanotechnique By Professor Kjell Öberg, M.D., Ph.D. Dept. of Endocrine Oncology, University Hospital, Uppsala, Sweden Nashville Oct. 2011 Hallmarks
Lu 177-Dotatate (Lutathera) Therapy Information
 Therapy Information") Lu 177-Dotatate (Lutathera) Therapy Information Information for Lu 177-dotatate therapy also known as Lutathera, for the treatment of metastatic midgut neuroendocrine tumor and other metastatic neuroendocrine
Lu 177-Dotatate (Lutathera) Therapy Information Information for Lu 177-dotatate therapy also known as Lutathera, for the treatment of metastatic midgut neuroendocrine tumor and other metastatic neuroendocrine
Strategies in the Management of Neuroendocrine Tumors. Dr. Jean Maroun Dr. Elena Tsvetkova
 Strategies in the Management of Neuroendocrine Tumors Dr. Jean Maroun Dr. Elena Tsvetkova 1 A ZORSE 2 Neuroendocrine Tumour Classification Neuroendocrine Tumours Carcinoid Tumours Pancreatic Neuroendocrine
Strategies in the Management of Neuroendocrine Tumors Dr. Jean Maroun Dr. Elena Tsvetkova 1 A ZORSE 2 Neuroendocrine Tumour Classification Neuroendocrine Tumours Carcinoid Tumours Pancreatic Neuroendocrine
Everolimus Plus Octreotide Long-Acting Repeatable in Patients With Advanced Lung Neuroendocrine Tumors
 CHEST Original Research Everolimus Plus Octreotide Long-Acting Repeatable in Patients With Advanced Lung Neuroendocrine Tumors Analysis of the Phase 3, Randomized, Placebo-Controlled RADIANT-2 Study LUNG
CHEST Original Research Everolimus Plus Octreotide Long-Acting Repeatable in Patients With Advanced Lung Neuroendocrine Tumors Analysis of the Phase 3, Randomized, Placebo-Controlled RADIANT-2 Study LUNG
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT
 ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
NEUROENDOCRINE TUMOURS Updated December 2015 by Dr. Doreen Ezeife (PGY-5 Medical Oncology Resident, University of Calgary)
") NEUROENDOCRINE TUMOURS Updated December 2015 by Dr. Doreen Ezeife (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Cynthia Card (Staff Medical Oncologist, University of Calgary)
NEUROENDOCRINE TUMOURS Updated December 2015 by Dr. Doreen Ezeife (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Cynthia Card (Staff Medical Oncologist, University of Calgary)
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Session 6 NEW TECHNIQUES IN RADIATION TREATMENT. Chairman : Françoise MORNEX
 Session 6 NEW TECHNIQUES IN RADIATION TREATMENT Chairman : Françoise MORNEX INTERNAL IRRADIATION FOR ENDOCRINE TUMORS Emmanuel DESHAYES INTERNAL IRRADIATION FOR ENDOCRINE TUMORS Dr Emmanuel DESHAYES Nuclear
Session 6 NEW TECHNIQUES IN RADIATION TREATMENT Chairman : Françoise MORNEX INTERNAL IRRADIATION FOR ENDOCRINE TUMORS Emmanuel DESHAYES INTERNAL IRRADIATION FOR ENDOCRINE TUMORS Dr Emmanuel DESHAYES Nuclear
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction
 NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
PRRT in Management of NETs. Ioannis Karfis, MD PhD Assistant Head of Clinic Nuclear Medicine Dept IJB, Brussels
 PRRT in Management of NETs Ioannis Karfis, MD PhD Assistant Head of Clinic Nuclear Medicine Dept IJB, Brussels THERAPEUTIC TARGETS in NENs Pavel M: Neuroendocrinology 2013;97:99-112 THERAPEUTIC ARENA in
PRRT in Management of NETs Ioannis Karfis, MD PhD Assistant Head of Clinic Nuclear Medicine Dept IJB, Brussels THERAPEUTIC TARGETS in NENs Pavel M: Neuroendocrinology 2013;97:99-112 THERAPEUTIC ARENA in
Horizon Scanning in Oncology
 Horizon Scanning in Oncology Everolimus (Afinitor ) for the treatment of unresectable or metastatic neuroendocrine tumours of pancreatic origin DSD: Horizon Scanning in Oncology Nr. 024 ISSN online 2076-5940
Horizon Scanning in Oncology Everolimus (Afinitor ) for the treatment of unresectable or metastatic neuroendocrine tumours of pancreatic origin DSD: Horizon Scanning in Oncology Nr. 024 ISSN online 2076-5940
Impact of Functioning Metastatic Neuroendocrine Tumors
 Clinical Overview and Treatment Advances in Carcinoid Syndrome Sponsored by Lexicon Pharmaceuticals Impact of Functioning Metastatic Neuroendocrine Tumors Evaluation & Management 1 Presentation objectives
Clinical Overview and Treatment Advances in Carcinoid Syndrome Sponsored by Lexicon Pharmaceuticals Impact of Functioning Metastatic Neuroendocrine Tumors Evaluation & Management 1 Presentation objectives
DALLA CAPECITABINA AL TAS 102
 DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid
 Neuroendocrine Tumors and Lung Carcinoid") Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We
 Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide)
") GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
Evidenze cliniche nel trattamento del RCC
 Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Neuroendocrine Tumors: Just the Basics. George Fisher, MD PhD
 Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-028 Study
 Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
EXOCRINE: 93% Acinar Cells Duct Cells. ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others
 EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
SIRT in the Management of Metastatic Neuroendocrine Tumors
 SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
THERANOSTICS MOLEKULARE BILDGEBUNG MITTELS PET/CT
 THERANOSTICS MOLEKULARE BILDGEBUNG MITTELS PET/CT UND RADIOREZEPTORTHERAPIE VON NET Richard P. Baum Klinik für Molekulare Radiotherapie / Zentrum für Molekulare Bildgebung (PET/CT) ENETS Center of Excellence,
THERANOSTICS MOLEKULARE BILDGEBUNG MITTELS PET/CT UND RADIOREZEPTORTHERAPIE VON NET Richard P. Baum Klinik für Molekulare Radiotherapie / Zentrum für Molekulare Bildgebung (PET/CT) ENETS Center of Excellence,
lutetium ( 177 Lu) oxodotreotide 370MBq/mL solution for infusion (Lutathera ) SMC No 1337/18 Advanced Accelerator Applications
 oxodotreotide 370MBq/mL solution for infusion (Lutathera ) SMC No 1337/18 Advanced Accelerator Applications") lutetium ( 177 Lu) oxodotreotide 370MBq/mL solution for infusion (Lutathera ) SMC No 1337/18 Advanced Accelerator Applications 8 June 2018 The Scottish Medicines Consortium (SMC) has completed its assessment
lutetium ( 177 Lu) oxodotreotide 370MBq/mL solution for infusion (Lutathera ) SMC No 1337/18 Advanced Accelerator Applications 8 June 2018 The Scottish Medicines Consortium (SMC) has completed its assessment
EVEROLIMUS SANDOZ (everolimus)
") EVEROLIMUS SANDOZ (everolimus) NAME OF THE MEDICINE The active ingredient of EVEROLIMUS SANDOZ is everolimus. The chemical name is 40-O-(2-hydroxyethyl)-rapamycin or 40-O-(2-hydroxyethyl)-sirolimus. Its
EVEROLIMUS SANDOZ (everolimus) NAME OF THE MEDICINE The active ingredient of EVEROLIMUS SANDOZ is everolimus. The chemical name is 40-O-(2-hydroxyethyl)-rapamycin or 40-O-(2-hydroxyethyl)-sirolimus. Its
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Peptide Receptor Radionuclide Therapy (PRRT) of NET
 of NET") Peptide Receptor Radionuclide Therapy (PRRT) of NET Dr. Tuba Kendi Associate Prof of Radiology, Mayo Clinic, Rochester, MN 2014 MFMER slide-1 Relevant Financial Relationship(s) None Off Label Usage None
Peptide Receptor Radionuclide Therapy (PRRT) of NET Dr. Tuba Kendi Associate Prof of Radiology, Mayo Clinic, Rochester, MN 2014 MFMER slide-1 Relevant Financial Relationship(s) None Off Label Usage None
DISCLOSURE SLIDE. ARGOS: research funding, scientific advisory board
 INTERIM ANALYSIS OF THE PHASE 3 ADAPT TRIAL EVALUATING ROCAPULDENCEL-T (AGS-003), AN INDIVIDUALIZED IMMUNOTHERAPY FOR THE TREATMENT OF NEWLY-DIAGNOSED PATIENTS WITH METASTATIC RENAL CELL CARCINOMA (MRCC)
INTERIM ANALYSIS OF THE PHASE 3 ADAPT TRIAL EVALUATING ROCAPULDENCEL-T (AGS-003), AN INDIVIDUALIZED IMMUNOTHERAPY FOR THE TREATMENT OF NEWLY-DIAGNOSED PATIENTS WITH METASTATIC RENAL CELL CARCINOMA (MRCC)
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer
 Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab