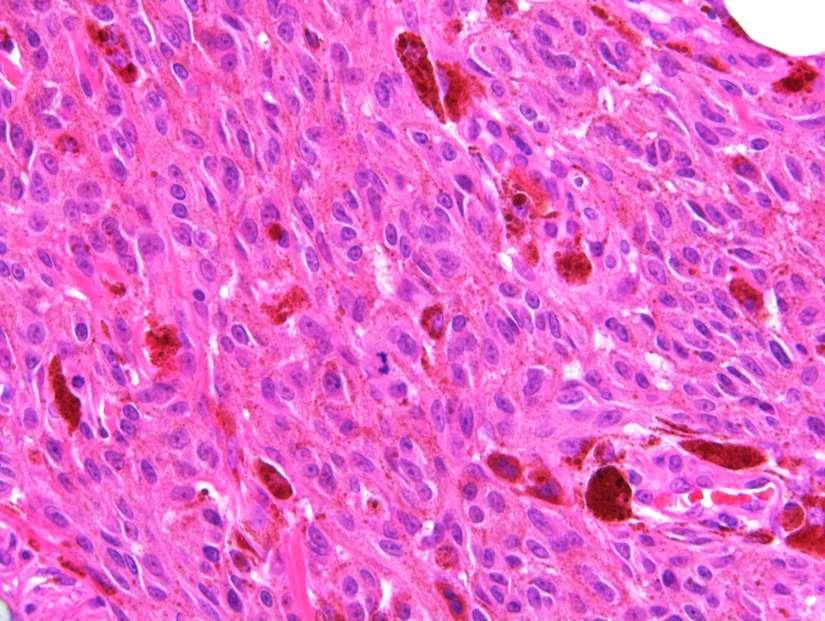
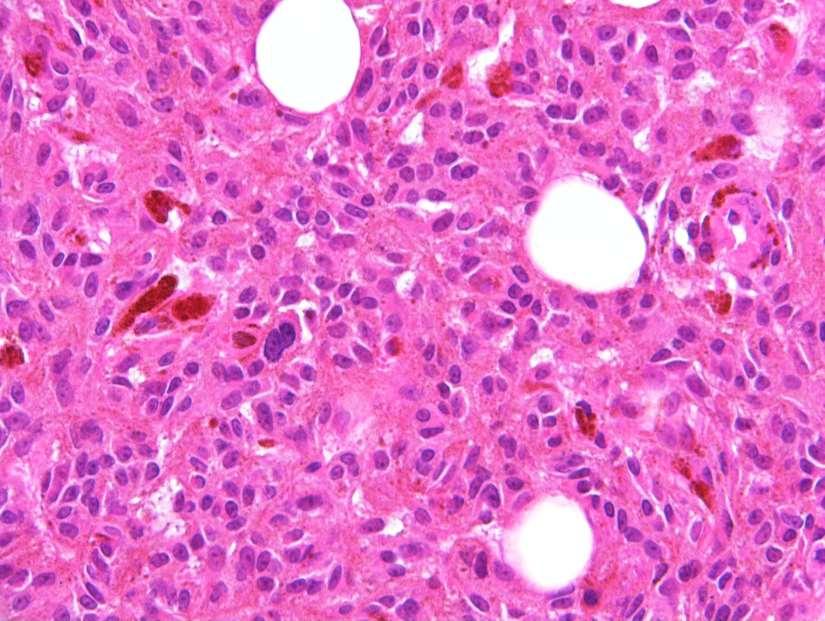
Case RAC7783. M46. Ear. Mole. r/o MM.?Blue naevus RAC7783
|
|
|
- Erick Bradford
- 5 years ago
- Views:
Transcription

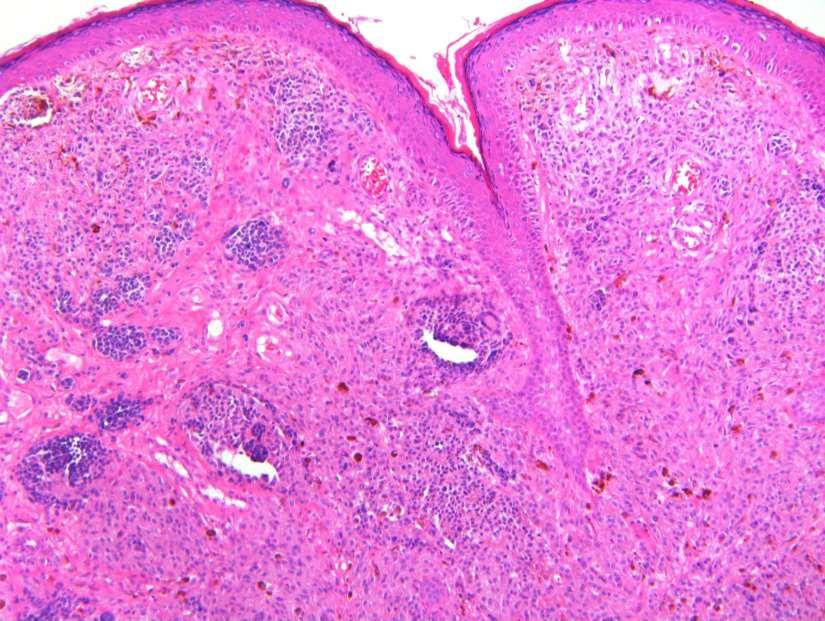
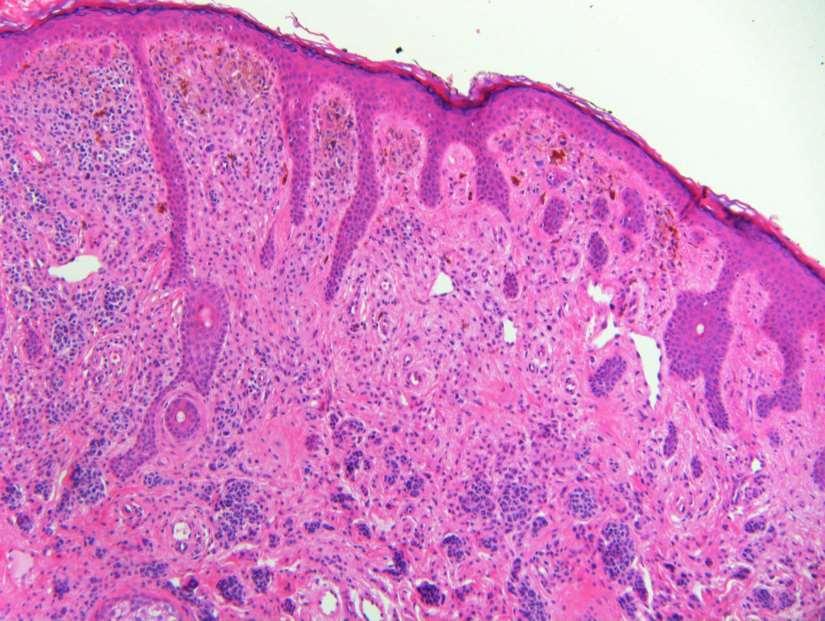
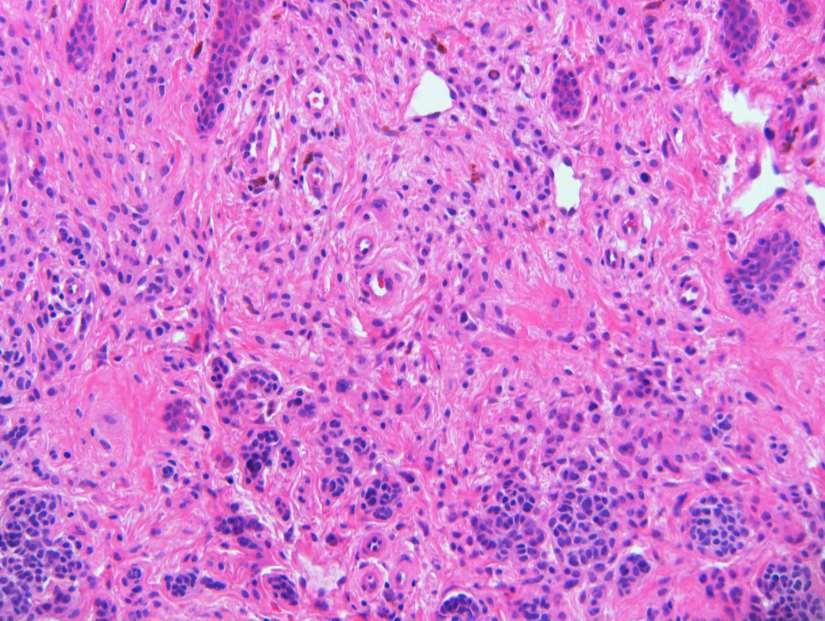
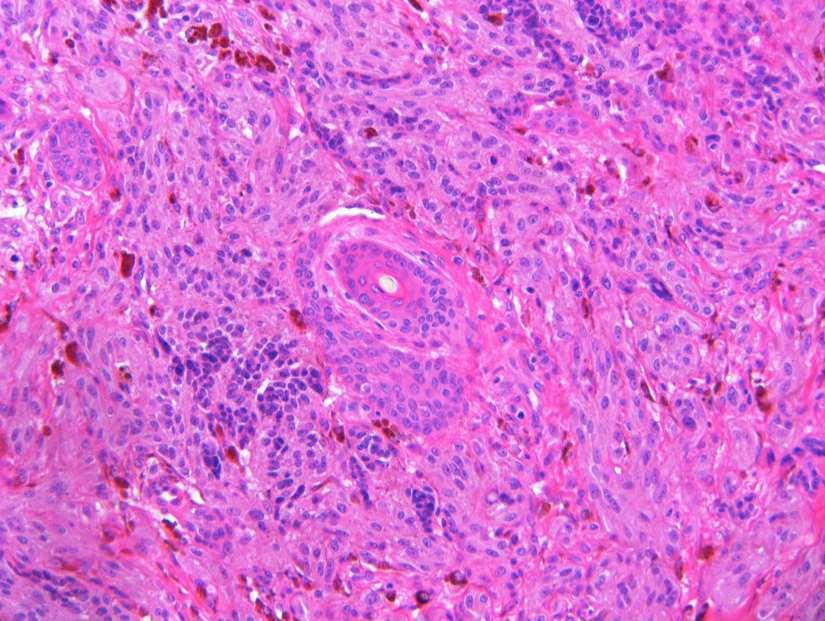
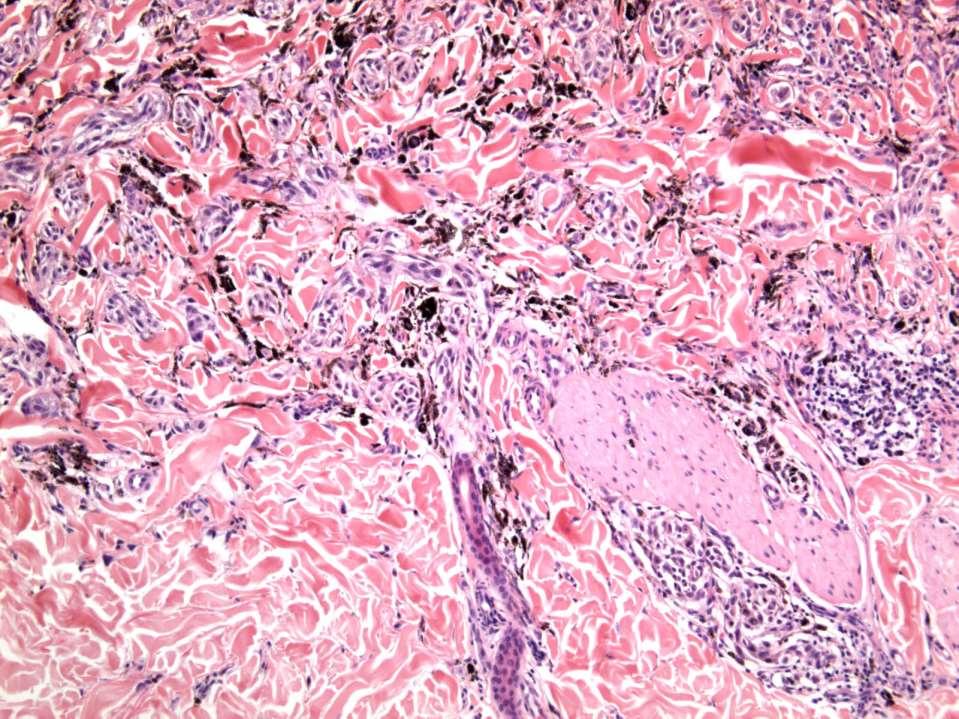
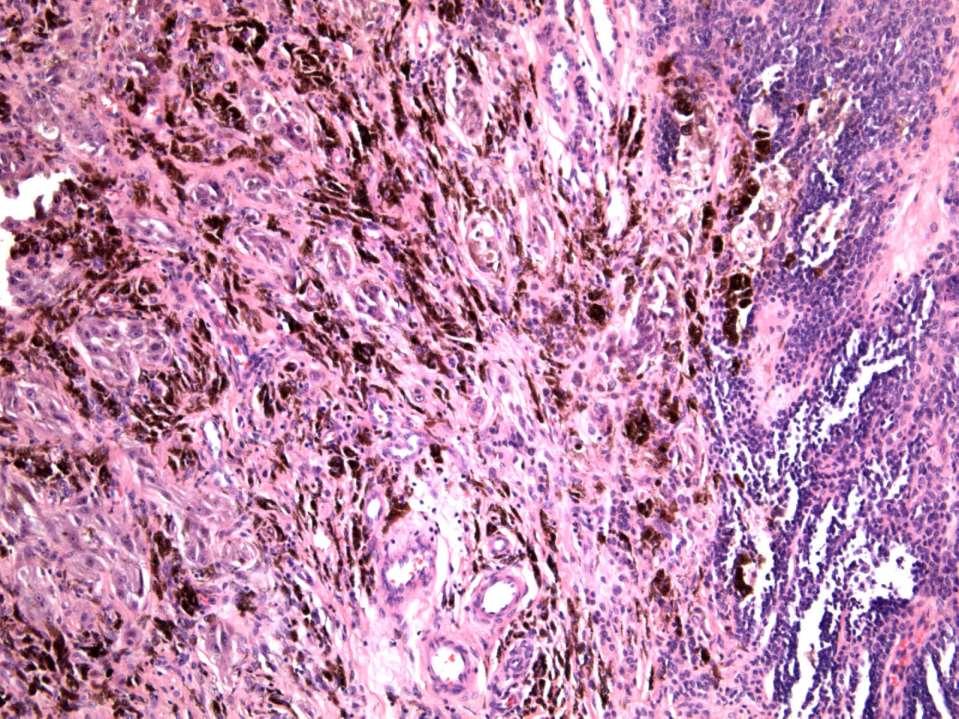
1 Case RAC7783. M46. Ear. Mole. r/o MM.?Blue naevus RAC7783
2
3
4
5
6
7
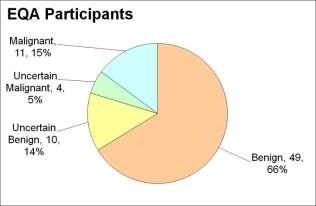
8 Pie Chart Participants N=74
9 Benign: 48 N=74 Blue naevus: 38 Intradermal: 12 DPN: 10 Compound 3 Clonal: 3; Spitz 2; Special Site: 1; Congenital: 1 Benign unclassifiable: 1 Uncertain favour benign 10 Uncertain favour malignant 4 Malignant 11 Nodular: 5 Malignant blue: 3 SSMM: 1, Naevoid: 1

10 Table for Malignant Responses

11 MPathDx* *I: Leave as is even if incompletely excised; II: Complete excision <5mm; III: 5mm; IV: as pt1a, pt1b; 1cm +/-; V: as pt2 or greater e.g. >1cm
12 EQA Participants: Benign N=49 Combined naevus - intradermal naevus and cellular blue naevus several Combined naevus with naevocellular and DPN like elements Differential diagnosis is deep penetrating naevus or blue naevus Sub 5mm reasonably symmetrical combined lesion with conventional nevus and deep penetrating nevus like components. Mitotically active, but DPN component cells uniform and I see no atypical mitoses. Patient on edge of age range for new presentations of this lesion, so worth getting history of lesional behaviour at MDT prior to sign out. Epithelioid cellular blue naevus x4 Depending on Beta-Catenin and Cyclin D1; DPN or Cellular blue naevus
13 EQA Participants: Uncertain favour benign N=10 A pigmented melanocytic lesion which is very cellulra and dual cell population in keeping with cellular blue naevus. However there are clearly some cells that show atypia and some mitoses are located in the deep part of the lesion.i do not think the features are of melanoma arising in blue naevus or a blue naevus -like melanoma. On balance I favour cellular bleu naevus with atypia Need BAP1 staining DPN-like but with reverse wedge shape and slightly older age than usual. A combined naevus with superficial ordinary intradermal naevus and deeper DPN component. Could do Beta-catenin to help confirm this. One mitosis identified in DPN component but no atypical forms seen.
14 EQA Participants: Uncertain favour malignant N=4 Combined naevus - compound melanocytic and epithelioid blue. The blue component is atypical with deep mitoses and extends into subcutis. Unceratin malignant potential, but would treat as malignant.
15 EQA Participants: Malignant N=11 Superficial spreading melanoma arising on intradermal naevus spitzoid, but several mid/deep mitoses, 2 very close together ( 3 in 1mm2.some atypical junctional nests Deep mitotic figures (up to 2/mm2 ), infiltrating edge. No necrosis.?nevoid melanoma?atypical CBN Mitoses: Can t see on digital slide

16 Pie Chart Slide Club N=23
17 SLIDE CLUB RESPONSES combined banal and epithelioid blue Combined naevus with a cellular blue naevus component. Heavily pigmented compound melanocytic proliferation which I think is benign and belongs to the deep penetrating naevus / combined naevus spectrum. I would recommend conservative reexcision given the very close deep margin. Combined melanocytic dermal tumor with a common nevus component at the sides and superficially. Centrally a DPN-like component but growing less nested than usual and with a more compact/expansile base. I do not see mitoses or necrosis. Fat cells in the deeper part. I would prefer a benign lesion, in the spectrum of combined nevus, common & DPN. I would perform additional MIB, HMB,beta-catenin and BAP1 stain. I would comment on the unusual growth and I would like clear margins (seems very close to the margin), otherwise advise a (small) re-excision. Combined congenital-like cellular naevus with deep penetrating-like pigmented clone. The latter shows mild cellular pleomorphic and scanty mitotic activity.given the diagnosis challenges in these cases, excision with clear margins may be advisable. Favor benign based on silhouette, absence of junctional component, and relatively regular distribution of melanin pigment / melanophages. Biphenotypic pattern with smaller nevus cell aggregates at periphery of larger DPN-like lesion is common presentation of a combined nevus, however, given patient age, ctyologic atypia, and a possible (deep) mitotic figure, re-excision seems warranted. Cellular blue naevus, benign.
18 SLIDE CLUB RESPONSES Uncertain favour benign. Combined naevus with intradermal naevus and component with some features of deep penetrating naevus Combined common acquired naevus which merges with a more cellular, pigmented clone of larger melanoytes.differential diangosis deep penetrating naevus (so do beta catenin), and an atypical cellular blue naevus - would do FISH.. Combined nevus with components of congenital pattern nevus and melanocytoma c/w deep penetrating nevus with atypical features (confluence of nests and fascicles but without severe atypia or mitoses) compound melanocytic lesion with modest component of usual type naevus. Admixed and dominating the coventional naevus is a heavily pigmented and cellular component of short spindle cells. It is difficult to define mitotic activity (I have found just one in the lower third). There is no thinning of the epidermis and although the lesion pushes out into subcutis it stops rather abruptly. On balance I favour a combined naevus with usual and cellular blue types although a combined lesion with DPN component is a further consideration but one I think less likely. Atypical DPN ( with some worrying features such as the patients age, few mitotic figures, asymmetry, increased cellularity and somewhat unusual location on the ear which is a special and UV exposed site). There are remnants of the conventional dermal naevus in papillary dermis. Complete excision with 5 mm margin and surveillance should be a sufficient treatment. BRAF and Beta catenin immunostains could confirm the diagnosis.
19 SLIDE CLUB RESPONSES 1 st : [Uncertain favour benign] This is a very difficult-to-diagnose case. There is a fascicular and sheet-like growth of pigmented spindle melanocytes which merge with a banal-appearing naevocytic component close to the surface. The tumor bulges into the subcutis more or less like a cellular blue naevus; I see no relevant mitotic activity and no foci of necrosis (on the digital slide). I would sign out a provisional diagnosis of atypical (cellular blue naevus-like) dendritic cell melanocytic tumor. My gut feeling is that this lesion will behave in a benign fashion. PS - Funny that the ear is considered as a special site for naevi, because melanomas are even commoner than naevi in such a location 2 nd : This is a combined tumor with a good merging between a banal nevus and a cellular blue nevus-like melanocytic tumor. I don't know how to correctly call the latter if not 'atypical cellular blue [nevus-like] tumour' (a kind of dendritic cell counterpart of atypical Spitz tumour). In my experience, the rule of 'merging' as a criterion for benignity has some exceptions. And this case may be an exception. I think that this tumour is a low-grade melanocytic malignancy. a peculiar form of blue nevus of the face. I suggest serial sections to rule out intralesional malignant evolution. I saw 3 similar lesions with limited follow up of the patients (all consultation cases). All lesions were on the face of adults or elderly. Two had negative 4-6 years long follow-up. The third lesion had an obvious melanoma nodule in the middle (but without metastasis, at least until I could follow up the case). Two types of cell in the dermis. One ordinary type naevus, the other lager pigmented plump spindle cell. Mininal junctional component. Minimal variation in cell size/ shape. No mitoses. Favour Deep penetrating naevus. Would be interesting to see Beta-catenin benign compound with deep penetrating component
20 SLIDE CLUB RESPONSES favour the idea of a combined naevus, with a small superficial / peripheral common acquired naevus component, and a rather massively cellular but monomorphic plump-spindle cell component that does not mature and is and apparently devoid of mitotic figures. I wonder whether that component could be related to DPN, even though it looks rather different; I would ask for a beta-catenin stain all the same. Of course, if I could lay may hands on the materials, I would study it more extensively for absence of mitotic figures &c. Combined nevus: Conventional intradermal melanocytic nevus + cellular blue nevus (digital). Combined melanocytic nevus (glass) [Uncertain favour malignant] A blue/cellular blue lesion, albeit with an admixed common acquired component, arising on sun-damaged skin, with readily identifiable mitoses. No necrosis, but there is some cytological atypia. Recommend NGS. [Uncertain favour benign] Common naevus and spindle and epithelioid cells but low mitotic rate and little pleomorphism, some form of combined phenotype. Worrying size and close margin, so would like wider excision because of uncertainty favour a combined melanocytic naevus with dysplastic compound naevus and (atypical) deep penetrating naevus components (glass). Combined naevus: classic acquired and cellular blue Deep penetrating naevus; to confirm with Beta-Catenin stain. Advise complete excision There are nests of small round melanocytes in the superficial dermis. The cytologic features of the melanocytes are reminiscent of those in deep penetrating nevus, or tumors with PRKCA fusion.
21 Original Report [Y]: Combined naevocellular and deep penetrating naevus. Mitotic rate = low (<1/50hpf). Depth 4mm Close to deep (0.5 mm) and focally abutting deep radial margin. Comment: In view of known challenge for diagnosis in such cases complete excision with a clear margin may be advisable. Dear X, 1.?worth using for slide club 2. Would you recommend a re-excision for a DPN abutting the margin on someone s ear?
22 MICRO REPORT: [X] That lesion is combined with a superficial common component especially visible in the junction that it is associated with a deep penetrating component underneath but that latter presents atypia with hyperdensity and confluent nests into large sheets. The melanocytes are of large size with enucleated ovular nuclei. Mitotic activity reaches 2/mm2. There is no inflammatory phenomenon associated. The IHC study found a strong nuclear staining with Beta-Catenin and negativity of antibodies against BRAF V600E. In the deep part, proliferation rate reaches 20% of stained nuclei. Mutation by NGS shows the presence of a canonical HRAS mutation and an exon Beta-Catenine mutation. The array-cgh could not be performed because of the depletion of material. Excision of the ear: Combined melanocytic tumour associating a common nevus and deep penetrating nevus in the latter atypia with high density and a high proliferation rate. A complementary resection is advised for this lesion which reaches 4 mm in depth. These aspects suggest a transformed malignant DPN component. The resection should be decided in a multidisciplinary meeting (personal suggestions: complementary resection of at least 1 cm). The French version of this text prevails.
23 Repeat Array CGH: Flat profile Lame _3 DLRS = 0,18 BM (ABRA) Comment from [X]: Paper from C Magro described DPN with flat CGH that went malignant if I recall [Y] Given overwhelming weight of opinion for benign/favour benign would you alter you opinion of atypical and suggests transformed malignant DPN component? Obviously the CGH was a different block but I think it had the DPN component. I appreciate the lesion could have in the future taken another step. RAC [X] I agree this would tend to have me downstage from favor malignant to atypical with unknown prognosis.
24 ATYPICAL/ BORDERLINE DPN A small subset of DPN Cytologic atypia Architectural atypia Mitotic activity SUMMARY: BORDERLINE DPN SLN+ve in 1/3 Cases treated aggressively were free of dis. All 6 examined by CGH showed no abnormalities 7/9 normal by FISH 3 cases of progression from borderline DPN to overt melanoma SUMMARY: PLEXIFORM MELANOMA 4/6 died of disease CONCLUSION: BORDERLINE DPN Incidence of regional LN involvement Potential progression to over melanoma Management: at least local reexcision & consideration of SLN regardless of cytogenetic data

25 M21. History not available RAC3172
26
27

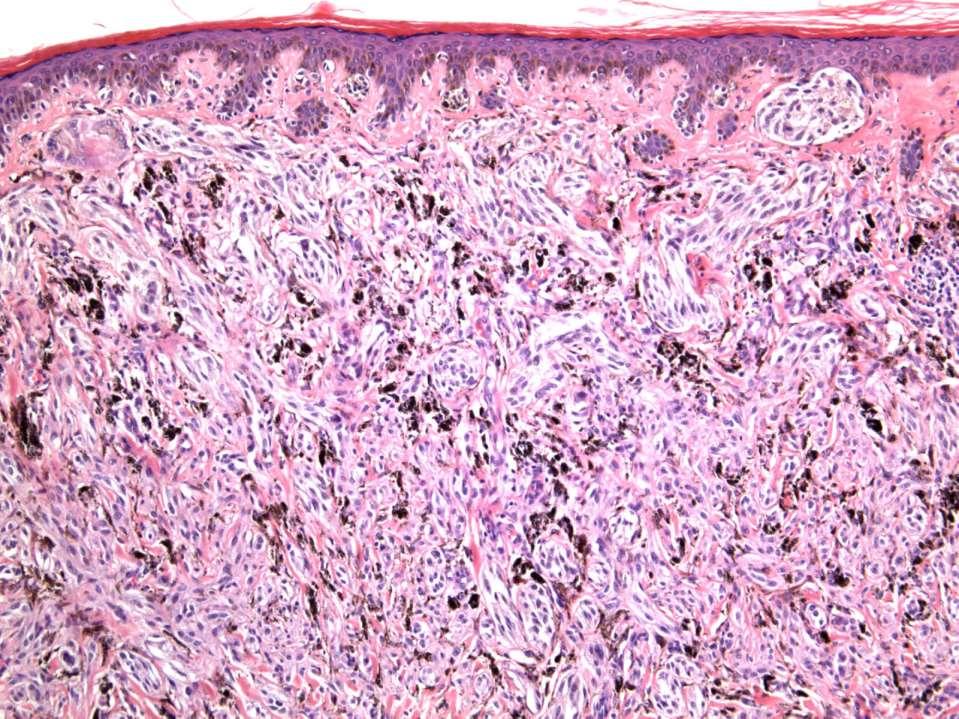
28 Diagnosis? DEEP PENETRATING NAEVUS


29 DEEP PENETRATING NAEVUS Fairly symmetrical wedge-shaped Extension in to deep dermis or subcutis Adnexal and neurovascular tropism Variable focal junctional component Finely pigmented epithelioid cells Clear cells, multinucleate cells, Spindle cells in deeper areas Conspicuous macrophages Elongated pigmented dendritic cells Mild cytological atypia Occassional normal mitotic figures Lymphocytic infiltrate Often component of combined naevus

30 M18. Congenital naevus with darker area RAC3163
31

32 Diagnosis? CONGENTIAL NAEVUS, PIGMENTED EPITHELIOID CLONE (possibly DPN-type)





33 Combined activation of -catenin signaling and MAP kinase pathway define DPN Courtesy of Dr. Pauline Guyot Yeh, Iwei et al. Combined Activation of MAP Kinase Pathway and β-catenin Signaling Cause Deep Penetrating Nevi. Nature Communications 8, no. 1 (September 21, 2017): 644. c/o Dr Arnaud de la Fouchardiere


 Inflammatory features")
34 c/o Arnaud de la Fouchardiere. Recent tumour referred as?pigmented epithelioid melanocytoma?atypical cellular BN Atypical Deep penetrating nevus Cellularity (density) Inflammatory features Mitotic activity: 3/mm² Breslow: 5mm


35 Beta-catenin IHC Diffuse HMB45 positivity P16 slightly heterogeneous Ki67: 10-20% nuclear positivity in some areas BRAF V600E: negative Beta-catenin staining: strong nuclear staining Array CGH Exon 3 CTNNB1 G34E mutation No hotspot mutations in BRAF, NRAS, KIT c/o Dr Arnaud de la Fouchardiere DEEP PENETRATING NAEVUS MESSAGES Recent clarification of genetics: 2 alternations 1: MAPK pathway BRAF, MAPK2, HRAS 2: βcatenin pathway CTNNB1, APC «Intermediate tumor» that can progress towards malignancy Beta-catenin IHC is useful in recognizing DPN






36 Combined DPN: Less Pigment, High Cellularity Combined PEM: More Pigment, Low cellularity, Numerous melanophages CTNNB1 PRKAR1A c/o Arnaud de la Fouchardiere
37 Discussion Many EQA participants and a few panel members (8) did not appreciate unlikely to be naevocellular combined with blue as they are mutually exclusive Greater proportion of panel favoured DPN (13) Interesting the MAPK abnormality is in HRAS (present in a proportion of Spitz, particularly desmoplastic type) but the naevus is naevocellular in Case 232 However N. spilus is characterised by HRAS mutation (and these lesions are usually naevocellular) Of concern 8/17 EQA MPathDx responses were happy to leave a challening case such as this without re-excision Even typical DPN should probably be regarded as a difficult case for diagnosis and given possibility for malignant transformation complete excision with clear margins recommended as for a melanocytoma


38 Dutch Master? Without Title, 1986 Prof Wolter Mooi Amsterdam, NL Thank You Arnaud de la Fouchardiere All responding EQA members and panel members Cases 231 & 232 are dedicated to Professor Wolter Mooi PS: this might be my last contribution to your excellent slide club... I plan to quit pathology by the end of this year, in order to devote my time entirely to some of the humanities (at a modest level of achievement, no doubt). THANK YOU WOLTER!
39 REFERENCE Eur J Dermatol Sep-Oct;24(5): doi: /ejd Deep penetrating nevus-like borderline tumors: A unique subset of ambiguous melanocytic tumors with malignant potential and normal cytogenetics. Magro CM 1, Abraham RM 2, Guo R 3, Li S 4, Wang X 1, Proper S 5, Crowson AN 6, Mihm M 7. Author information BACKGROUND: Deep penetrating nevi (DPN) are a relatively uncommon subtype of melanocytic nevi. A small subset of these lesions exhibit atypical features (cytologic and architectural atypia, mitotic activity) seen in melanoma. These lesions we term the deep penetrating nevuslike borderline tumor. Unequivocal melanomas can show overlapping morphologic features of DPN, which have been termed plexiform melanomas. PATIENTS AND METHODS: 40 cases of DPN-like borderline tumor were identified along with 6 cases of plexiform melanoma. Clinical follow up was obtained, along with cytogenetic analysis in the form of fluorescent in situ hybridization (FISH) and/or comparative genomic hybridization (CGH). RESULTS: The DPN-like borderline tumor cases included 24 females and 16 males. Of sentinel lymph node biopsies performed, 1/3 of cases showed lymph node involvement. All patients where an aggressive clinical approach was adopted remain free of disease. All 6 DPNlike borderline tumor cases tested by CGH showed normal cytogenetics, as did 7 of 9 cases tested by FISH. Of the plexiform melanomas, 4/6 patients died of disease. In 3 cases there was morphologic progression from a DPN-like borderline tumor to overt melanoma. In one case of progression, cytogenetics was normal in the DPN-like borderline tumor and then abnormal in the progressed melanoma. CONCLUSION: DPN-like borderline tumors are melanocytic tumors associated with a high incidence of regional lymph node disease and exhibiting the potential for melanoma progression despite a normal cytogenetic profile. Patients with these lesions should be aggressively managed, with at least complete re-excision and consideration of sentinel node biopsy, regardless of cytogenetic data.
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is:
 Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
21/07/2017. The «gray zone» of diagnosis is visible. Nevus Atypical nevus Melanoma. Melanoma ex-blue nevus
 Update on the Clinico- Pathological and Molecular Diagnosis of Melanocytic Lesions None to declare Conflicts of interest Belfast pathology Arnaud de la Fouchardière MD, PhD Lyon, France What is new? Today
Update on the Clinico- Pathological and Molecular Diagnosis of Melanocytic Lesions None to declare Conflicts of interest Belfast pathology Arnaud de la Fouchardière MD, PhD Lyon, France What is new? Today
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is:
 Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Case 231: F7. Exophytic naevus over left trapezious. Grown over a few weeks. Iniitally flat.?spitz naevus,?malignant
 Case 231: F7. Exophytic naevus over left trapezious. Grown over a few weeks. Iniitally flat.?spitz naevus,?malignant Dermoscopy: coarse vascular structures. c/o A, B, C RAC7750 Case 231: F7. Exophytic
Case 231: F7. Exophytic naevus over left trapezious. Grown over a few weeks. Iniitally flat.?spitz naevus,?malignant Dermoscopy: coarse vascular structures. c/o A, B, C RAC7750 Case 231: F7. Exophytic
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018
 Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy
 Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Vernon K. Sondak. Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida
 Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
10/2/17. MELTUMP, SAMPUS, AST.An Algorithmic Approach to Challenging (Often Borderline) Melanocytic Tumors. An Introduction to SNP Arrays
 Melanocytic Tumors. An Introduction to SNP Arrays") MELTUMP, SAMPUS, AST.An Algorithmic Approach to Challenging (Often ) Melanocytic Tumors An Introduction to SNP Arrays Rajiv M. Patel, M.D. RCPA NZ ASM 2017 (11:45-12:30pm, Saturday, 23-09-17) Why do we
MELTUMP, SAMPUS, AST.An Algorithmic Approach to Challenging (Often ) Melanocytic Tumors An Introduction to SNP Arrays Rajiv M. Patel, M.D. RCPA NZ ASM 2017 (11:45-12:30pm, Saturday, 23-09-17) Why do we
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Blue Melanocytic Proliferations
 Blue Melanocytic Proliferations Labib R. Zakka M.D., M.A. Research Fellow Melanoma Program Department of Dermatology Brigham and Women s Hospital Harvard Medical School Conflicts of Interest No conflicts
Blue Melanocytic Proliferations Labib R. Zakka M.D., M.A. Research Fellow Melanoma Program Department of Dermatology Brigham and Women s Hospital Harvard Medical School Conflicts of Interest No conflicts
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble at bay
 Pitfalls in the diagnosis of melanocytic tumors Timothy McCalmont, MD University of California, San Francisco Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble
Pitfalls in the diagnosis of melanocytic tumors Timothy McCalmont, MD University of California, San Francisco Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble
Michael T. Tetzlaff MD, PhD
 Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Conflict of Interest 9/2/2014. Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma
 Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
The Enigmatic Spitz Lesion
 The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Guy Perrot (Ги Перро)
") НАУЧНО-ПРАКТИЧЕСКАЯ КОНФЕРЕНЦИЯ (МАСТЕР-КЛАСС) «ПРАКТИЧЕСКИЕ АСПЕКТЫ ДИАГНОСТИКИ И ЛЕЧЕНИЯ МЕЛАНОМЫ КОЖИ» DIAGNOSTIC AND PITFALLS IN MELANOMA Guy Perrot (Ги Перро) MD PHD pathologist, University Hospital
НАУЧНО-ПРАКТИЧЕСКАЯ КОНФЕРЕНЦИЯ (МАСТЕР-КЛАСС) «ПРАКТИЧЕСКИЕ АСПЕКТЫ ДИАГНОСТИКИ И ЛЕЧЕНИЯ МЕЛАНОМЫ КОЖИ» DIAGNOSTIC AND PITFALLS IN MELANOMA Guy Perrot (Ги Перро) MD PHD pathologist, University Hospital
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors
 Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
5/21/2018. Disclosures. Consulting: Myriad Genetics SciBase. Superficial Atypical Melanocytic Proliferations. SSM, LMM and (some of) their Simulants
 their Simulants") Disclosures Consulting: Myriad Genetics SciBase Superficial Atypical Melanocytic Proliferations SSM, LMM and (some of) their Simulants 1 Melanomas and Nevi. Nevi are important mainly in relation to melanoma
Disclosures Consulting: Myriad Genetics SciBase Superficial Atypical Melanocytic Proliferations SSM, LMM and (some of) their Simulants 1 Melanomas and Nevi. Nevi are important mainly in relation to melanoma
1/10/2018. Soft Tissue Tumors Showing Melanocytic Differentiation. Overview. Desmoplastic/ Spindle Cell Melanoma
 2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Reviewers' comments: Reviewer #1 (Remarks to the Author):
:") Reviewers' comments: Reviewer #1 (Remarks to the Author): In this study the authors analysed 18 deep penetrating nevi for oncogenic genomic changes (single nucleotide variations, insertions/deletions,
Reviewers' comments: Reviewer #1 (Remarks to the Author): In this study the authors analysed 18 deep penetrating nevi for oncogenic genomic changes (single nucleotide variations, insertions/deletions,
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis
 Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Dermatologica Sinica
 DERMATOLOGICA SINICA 30 (2012) 57e61 Contents lists available at SciVerse ScienceDirect Dermatologica Sinica journal homepage: http://www.derm-sinica.com CASE REPORT Pigmented epithelioid melanocytoma:
DERMATOLOGICA SINICA 30 (2012) 57e61 Contents lists available at SciVerse ScienceDirect Dermatologica Sinica journal homepage: http://www.derm-sinica.com CASE REPORT Pigmented epithelioid melanocytoma:
Melanocytic proliferations in sundamaged
 Atypical Spitzoid Tumor: What Does It Mean And How Should It Be Managed? Melanocytic proliferations in sundamaged skin Jane L. Messina, Jane L. Messina MD International Melanoma Pathology Working Group
Atypical Spitzoid Tumor: What Does It Mean And How Should It Be Managed? Melanocytic proliferations in sundamaged skin Jane L. Messina, Jane L. Messina MD International Melanoma Pathology Working Group
The Dermal Melanocytoses. Conflicts of Interest 5/22/2018. The Nevi of Ota and Ito. Martin C. Mihm M.D.
 The Dermal Melanocytoses Martin C. Mihm M.D. Director Mihm Cutaneous Pathology Consultative Service (MCPCS) Brigham and Women s Hospital Director Melanoma Program Brigham and Women s Hospital and Harvard
The Dermal Melanocytoses Martin C. Mihm M.D. Director Mihm Cutaneous Pathology Consultative Service (MCPCS) Brigham and Women s Hospital Director Melanoma Program Brigham and Women s Hospital and Harvard
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
There is NO single Melanoma Stain. > 6000 Mutations in Melanoma. What else can be done to discriminate atypical nevi from melanoma?
 Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Management of pediatric melanocytic lesions
 Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
EARLY ONLINE RELEASE
 EARLY ONLINE RELEASE Note: This article was posted on the Archives Web site as an Early Online Release. Early Online Release articles have been peer reviewed, copyedited, and reviewed by the authors. Additional
EARLY ONLINE RELEASE Note: This article was posted on the Archives Web site as an Early Online Release. Early Online Release articles have been peer reviewed, copyedited, and reviewed by the authors. Additional
Histopathology of Melanoma
 THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 2. Variations on the acquired nevus 3. Dermal melanocytosis
 Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Associate Clinical Professor of Dermatology MUSC
 Re-excision of Moderately Dysplastic Nevi: Should we or shouldn t we? John C. Maize, Jr, M.D. Dermatologist and Dermatopathologist Trident Dermatology, Charleston SC Associate Clinical Professor of Dermatology
Re-excision of Moderately Dysplastic Nevi: Should we or shouldn t we? John C. Maize, Jr, M.D. Dermatologist and Dermatopathologist Trident Dermatology, Charleston SC Associate Clinical Professor of Dermatology
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors
 The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Pathology of Neoplasia Part II
 The Pathology of Neoplasia Part II February 2018 PAUL BOGNER, MD A S S O C I A T E P R O F E S S O R O F O N C O L O G Y P A T H O L O G Y A N D D E R M A T O L O G Y Clinical goals of cancer pathology
The Pathology of Neoplasia Part II February 2018 PAUL BOGNER, MD A S S O C I A T E P R O F E S S O R O F O N C O L O G Y P A T H O L O G Y A N D D E R M A T O L O G Y Clinical goals of cancer pathology
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
6/22/2015. Original Paradigm. Correlating Histology and Molecular Findings in Melanocytic Neoplasms
 6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
Mole mapping and monitoring. Dr Stephen Hayes. Associate Specialist in Dermatology, University Hospital Southampton
 Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
K Blessing, J J H Grant, D S A Sanders, M M Kennedy, A Husain, P Coburn
 J Clin Pathol 2000;53:591 595 591 Papers Pathology, Aberdeen University, Foresterhill, Aberdeen AB25 2ZD, K Blessing Pathology, Birmingham University, Birmingham B15 2TT, D S A Sanders Pathology, Heartlands
J Clin Pathol 2000;53:591 595 591 Papers Pathology, Aberdeen University, Foresterhill, Aberdeen AB25 2ZD, K Blessing Pathology, Birmingham University, Birmingham B15 2TT, D S A Sanders Pathology, Heartlands
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma. Michael T. Tetzlaff MD, PhD
 Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Brief Report. Shivanand Gundalli 1, Smita Kadadavar 1, Somil Singhania 1, Rutuja Kolekar 2 INTRODUCTION. Melanocytic Nevus
 Our Dermatology Online Histopathological spectrum of benign melanocytic nevi our experience in a tertiary care centre Shivanand Gundalli 1, Smita Kadadavar 1, Somil Singhania 1, Rutuja Kolekar 2 1 Department
Our Dermatology Online Histopathological spectrum of benign melanocytic nevi our experience in a tertiary care centre Shivanand Gundalli 1, Smita Kadadavar 1, Somil Singhania 1, Rutuja Kolekar 2 1 Department
Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis
 DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis Temeida Alendar 1, Harald Kittler
DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis Temeida Alendar 1, Harald Kittler
Simulators of melanoma
 Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Supplementary Figure 1. Spitzoid Melanoma with PPFIBP1-MET fusion. (a) Histopathology (4x) shows a domed papule with melanocytes extending into the
 Histopathology (4x) shows a domed papule with melanocytes extending into the") Supplementary Figure 1. Spitzoid Melanoma with PPFIBP1-MET fusion. (a) Histopathology (4x) shows a domed papule with melanocytes extending into the deep dermis. (b) The melanocytes demonstrate abundant
Supplementary Figure 1. Spitzoid Melanoma with PPFIBP1-MET fusion. (a) Histopathology (4x) shows a domed papule with melanocytes extending into the deep dermis. (b) The melanocytes demonstrate abundant
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
Special slide seminar
 Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
PDF hosted at the Radboud Repository of the Radboud University Nijmegen
 PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/27367
PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/27367
Whitney A. High, MD, JD, MEng
 ADS Dermatopathology Meeting 2014 Selected Adnexal Tumors Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of Colorado School
ADS Dermatopathology Meeting 2014 Selected Adnexal Tumors Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of Colorado School
Molecular Aspects of Melanocytic Neoplasia. Iwei Yeh MD, PhD University of California, San Francisco
 Molecular Aspects of Melanocytic Neoplasia Iwei Yeh MD, PhD University of California, San Francisco Thanks to: Boris Bastian Timothy McCalmont Philip LeBoit Beth Ruben Jeff North Laura Pincus Thaddeus
Molecular Aspects of Melanocytic Neoplasia Iwei Yeh MD, PhD University of California, San Francisco Thanks to: Boris Bastian Timothy McCalmont Philip LeBoit Beth Ruben Jeff North Laura Pincus Thaddeus
ARTICLE INFO ABSTRACT
 Melanocytic Pigmentation: A Single Manifestation of Myriad of Pathologies [PP: 05-09] Dr. Swapna Honwad Department of Oral Pathology dr.swapnahonwad@gmail.com Dr. Elsy P. Simon Department of Endodontics
Melanocytic Pigmentation: A Single Manifestation of Myriad of Pathologies [PP: 05-09] Dr. Swapna Honwad Department of Oral Pathology dr.swapnahonwad@gmail.com Dr. Elsy P. Simon Department of Endodontics
Spitz nevi in the classic histopathological pattern - lamb in wolf`s clothing *
 DERMATOPATHOLOGY 91 Spitz nevi in the classic histopathological pattern - lamb in wolf`s clothing * Gustavo Costa Verardino 1 Mayra Carrijo Rochael 1 DOI: http://dx.doi.org/10.1590/abd1806-4841.20153310
DERMATOPATHOLOGY 91 Spitz nevi in the classic histopathological pattern - lamb in wolf`s clothing * Gustavo Costa Verardino 1 Mayra Carrijo Rochael 1 DOI: http://dx.doi.org/10.1590/abd1806-4841.20153310
Pathological diagnosis of melanocytic tumours: clues and pitfalls # Richard A. Scolyer 1,2,3* and Stanley W. McCarthy 1,2,3
 Pathological diagnosis of melanocytic tumours: clues and pitfalls # Richard A. Scolyer 1,2,3* and Stanley W. McCarthy 1,2,3 1 Tissue Pathology and Diagnostic Oncology, Royal Prince Alfred Hospital, Sydney,
Pathological diagnosis of melanocytic tumours: clues and pitfalls # Richard A. Scolyer 1,2,3* and Stanley W. McCarthy 1,2,3 1 Tissue Pathology and Diagnostic Oncology, Royal Prince Alfred Hospital, Sydney,
S everal morphological features are frequently used in the
 1194 ORIGINAL ARTICLE Interobserver reproducibility of histological features in cutaneous malignant melanoma C Urso, F Rongioletti, D Innocenzi, C Saieva, D Batolo, S Chimenti, R Filotico, R Gianotti,
1194 ORIGINAL ARTICLE Interobserver reproducibility of histological features in cutaneous malignant melanoma C Urso, F Rongioletti, D Innocenzi, C Saieva, D Batolo, S Chimenti, R Filotico, R Gianotti,
Type IV collagen and laminin staining patterns in benign
 J Clin Pathol 1989;42:1173-1177 Type IV collagen and laminin staining patterns in benign and malignant cutaneous lesions RONA M MacKIE, D B CLELLAND, CHRISTINE J SKERROW From the Department ofdermatology,
J Clin Pathol 1989;42:1173-1177 Type IV collagen and laminin staining patterns in benign and malignant cutaneous lesions RONA M MacKIE, D B CLELLAND, CHRISTINE J SKERROW From the Department ofdermatology,
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Index. Springer-Verlag Berlin Heidelberg 2017 J.A. Plaza, V.G. Prieto, Pathology of Pigmented Skin Lesions, DOI /
 A Acral lentiginous (mucosal lentiginous) melanoma, 483 Acral lentiginous melanoma (ALM) asymmetric and irregular lentiginous junctional growth, 431 clinical features, 427 428 differential diagnosis, 428
A Acral lentiginous (mucosal lentiginous) melanoma, 483 Acral lentiginous melanoma (ALM) asymmetric and irregular lentiginous junctional growth, 431 clinical features, 427 428 differential diagnosis, 428
Melanocytic Tumours. Molecular Biology 02/06/2015. Cutaneous Melanocytic Tumours Introduction. Thomas Brenn. Intermediate Malignancy
 Cutaneous Melanocytic Tumours Introduction Melanocytic Tumours: Update on Epidemiology and Molecular Biology Thomas Brenn Wide clinical and morphological spectrum Ranging from benign naevi to melanoma
Cutaneous Melanocytic Tumours Introduction Melanocytic Tumours: Update on Epidemiology and Molecular Biology Thomas Brenn Wide clinical and morphological spectrum Ranging from benign naevi to melanoma
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
F006 Imaging in Dermatology Melanocytic Neoplasia Clinical-Confocal-Pathological-Correlations
 F006 Imaging in Dermatology Melanocytic Neoplasia Clinical-Confocal-Pathological-Correlations Melissa Gill, MD SkinMedical Research and Diagnostics Dobbs Ferry, NY, USA Department of Pathology SUNY Downstate
F006 Imaging in Dermatology Melanocytic Neoplasia Clinical-Confocal-Pathological-Correlations Melissa Gill, MD SkinMedical Research and Diagnostics Dobbs Ferry, NY, USA Department of Pathology SUNY Downstate
Pathology. Skin Tumor. Bayan N. Mohammad 15/10/2015. Mohammad al-orjani. Page 0 of 23
 #7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
#7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
Patricia Chevez-Barrrios AAOOP-USCAP /12/2016
 Biomarkers in Ocular Melanoma Patricia Chévez-Barrios, MD Pathology and Genomic Medicine, Houston Methodist Hospital Professor of Pathology and Laboratory Medicine and Ophthalmology, Weill Cornell Medical
Biomarkers in Ocular Melanoma Patricia Chévez-Barrios, MD Pathology and Genomic Medicine, Houston Methodist Hospital Professor of Pathology and Laboratory Medicine and Ophthalmology, Weill Cornell Medical
Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor
 Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Atypical Nevi When to Re-excise. Catherine Barry, DO Dermatopathologist
 Atypical Nevi When to Re-excise Catherine Barry, DO Dermatopathologist Why talk about skin cancer? Because it s the most common type of cancer! Non-melanoma Skin Cancers Basal Cell Carcinoma Squamous Cell
Atypical Nevi When to Re-excise Catherine Barry, DO Dermatopathologist Why talk about skin cancer? Because it s the most common type of cancer! Non-melanoma Skin Cancers Basal Cell Carcinoma Squamous Cell
Melanoma. Consultation on draft guideline - stakeholder comments. Comments to be submitted before 5pm on Friday 13 March 2015
 Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
Multiple Primary Melanoma in a Thai Male: A Case Report
 Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Cellular Neurothekeoma
 Cellular Neurothekeoma Scott W Binder, MD Pritzker Professor of Pathology & Dermatology Sr. Vice Chair Director, Pathology Clinical Services Chief, Dermatopathology Geffen/UCLA School of Medicine Clinical
Cellular Neurothekeoma Scott W Binder, MD Pritzker Professor of Pathology & Dermatology Sr. Vice Chair Director, Pathology Clinical Services Chief, Dermatopathology Geffen/UCLA School of Medicine Clinical
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Michael T. Tetzlaff MD, PhD
 Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
SMOOTH MUSCLE TUMOURS
 SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
Dilemmas in Cytopathology and Histopathology
 Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
BAP-oma & BEYOND MICHAEL A NOWAK, MD
 BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
Basics in Dermoscopy
 Basics in Dermoscopy Manal Bosseila Professor of Dermatology, Cairo University Member of European Academy Dermatology & Venereology EADV Member of International Dermoscopy Society IDS Member of Aesthetic
Basics in Dermoscopy Manal Bosseila Professor of Dermatology, Cairo University Member of European Academy Dermatology & Venereology EADV Member of International Dermoscopy Society IDS Member of Aesthetic
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5