Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma
|
|
|
- Bruce Turner
- 5 years ago
- Views:
Transcription


1 Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma Taylor S. Riall, MD, PhD CERCIT Workshop October 19, 2012 Department of Surgery Center for Comparative Effectiveness and Cancer Outcomes The University of Texas Medical Branch, Galveston, TX
2 INTRODUCTION Second leading cause of cancer death In 2012: 143,460 cases of colorectal cancer 51,690 deaths Approximately 20% present with distant metastases Majority are unresectable at the time of presentation Overall 5-year survival for stage IV disease: 10-15%
3 SITES OF METASTASES Common sites of metastatic disease Liver Lungs Carcinomatosis Distant nodal metastases Uncommon Brain Bone
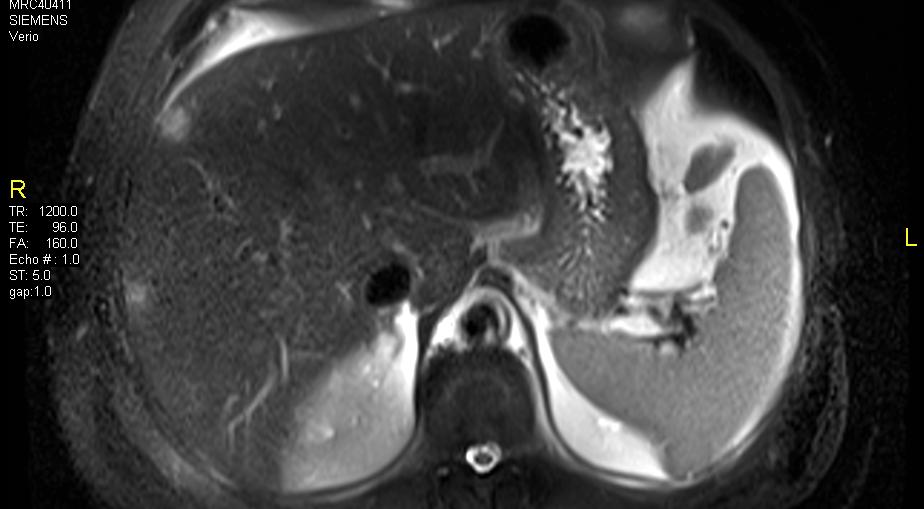
4 LIVER METASTASES
5 CARCINOMATOSIS
6 CHEMOTHERAPY Chemotherapy is the primary treatment Before 2000 (standard chemotherapy): 5-FU Leucovorin Phase III studies in 2000: Oxaliplatin (FULFOX) Irinotecan (FULFIRI) FULFOX and FULFIRI now first line regimens (modern chemotherapy)
7 CHEMOTHERAPY Newer agents: Bevacizumab (avastin) Monoconal Ab against VEGF-A Angiogenesis inhibitor Approved in 2004 for metastatic colon cancer Cetuximab Monoclonal Ab against EGFR Used in k-ras wild type colon cancers Approved in 2008 for colon cancer
8 RESECTION OF PRIMARY TUMOR Done to prevent tumor complications Bleeding Obstruction Perforation May improve survival but studies done are subject to significant selection bias
9 TIMING OF RESECTION AND CHEMO Historically done BEFORE initiation of chemotherapy Prevent complications requiring surgery during chemotherapy/immunosuppression Now controversial New techniques for palliation Improved tumor response with modern chemotherapy
10 TIMING OF RESECTION AND CHEMO Historically done BEFORE initiation of chemotherapy Prevent complications requiring surgery during chemotherapy/immunosuppression Now controversial New techniques for palliation Improved tumor response with modern chemotherapy
11 TIMING OF RESECTION AND CHEMO Proponents of immediate resection Prevents tumor related complications Allows for accurate abdominal staging Potentially improves the efficacy of chemotherapy by decreasing tumor burden May improve survival
12 TIMING OF RESECTION AND CHEMO Opponents of immediate resection High morbidity and mortality rates May delay onset or preclude receipt of chemothterapy Chemotherapy first may prevent unnecessary resection in patients with rapid disease progression
13 MANAGEMENT OF LIVER METS Modalities have evolved over the last decade For resectable disease in good surgical candidates Resection preferred Concurrent or sequential with resection of primary tumor When resection not possible Ablation (thermal, radiofrequency, chemoembolization) Hepatic arterial infusion chemotherapy
14 PREVIOUS SEER STUDIES Analysis of SEER data ( ) 27,654 patients with stage IV colon cancer 66% underwent resection of primary tumor Younger Right-sided tumors Survival better in resected patients No attempt to control for selection bias Cook et al. Ann Surg Oncol 2005; 12:
15 PREVIOUS SEER STUDIES 2004 role of surgery to remove primary tumor is controversial SEER: 9,011 beneficiaries with stage IV colorectal cancer 72% underwent CDS (excluded diverting colostomy) 3.9% underwent metastectomy Conclude that practice patterns needs to be reevaluated, given the improvement in the efficacy of chemotherapy Temple et al. J Clin Oncol 2004; 22:
16 CURRENT TRENDS Little is known regarding current trends in the management of stage IV colorectal cancer Use of resection Timing of resection relative to chemotherapy Management of liver mets Analysis of SEER data ( )
17 OBJECTIVE Used Texas Cancer Registry and linked Medicare claims data to: Describe patterns and trends in the management of stage IV colorectal cancer including: Resection of the primary tumor Receipt/type of chemotherapy Management of hepatic metastases.
18 COHORT TCR-Medicare Colon or rectal cancer (claims ) Aged 66 and older Stage IV disease based on SEER historic stage First primary cancer only Not diagnosed on autopsy or death certificate Part A and B coverage one year before and two years after diagnosis
19 METHODS TCR-Medicare Colon or rectal cancer (claims ) Aged 66 and older Stage IV disease based on SEER historic stage First primary cancer only Not diagnosed on autopsy or death certificate Part A and B coverage one year before and two years after diagnosis
20 COLORECTAL CANCERS BY YEAR N = 3,343
21 DEMOGRAPHICS Mean age /- 7.2 years Age group % % % % % Gender 46.7% male Race White 80.9% Black 12.8% Hispanic 4.2% Other 2.1% Charlson = %
22 TUMOR CHARACTERISTICS Colon 87.8% Right 36.3% Transverse 4.2% Left 36.1% Indeterminate 11.1% Rectum 12.2% Differentiation Well/moderate 50.5% Poor 25.7% Unknown 23.8% Positive nodes (N=1931) 78.8%
23 SITES OF METASTATIC DISEASE ICD-9 codes in Medicare claims to identify: Liver mets: Secondary neoplasm of liver OR liver resection Lung mets: Secondary neoplasm of lung, pleura, mediastinum OR lung resection Carcinomatosis: Carcinomatosis OR secondary neoplasm of retroperitoneum, small bowel, other digestive organs Brain: Secondary neoplasm of brain, spinal cord, or meninges Previous studies suggest that Medicare claims alone not accurate in identifying stage Good PPV in the subset of stage IV cancers identified in TCR?
24 SITES OF METASTATIC DISEASE Liver 73.1% Liver mets only 20.4% Lung 32.4% Carcinomatosis 36.4% Distant nodal metastases 38.9% Brain 4.7%
25 RESECTION OF PRIMARY TUMOR
26 CHEMOTHERAPY
27 STANDARD VS. MODERN
28 AVASTIN
29 RESECTION AND CHEMO Resection only 26.4% Chemotherapy only 11.8% Resection + chemotherapy 37.4% Surgery first 89.1% Emergent 19.3% Chemotherapy first 10.9% No treatment 24.4%
30 MANAGEMENT OF LIVER METS All patients with stage IV colon cancer: 19.7% liver resection 3.5% ablation 1.4% chemoembolization 73.1% of patients had documented liver mets (N=2,444) Of 2,444 with documented liver mets: 25.7% liver resection
31 MANAGEMENT OF LIVER METS
32 SURVIVAL 30-day operative mortality = 13.5% 291 deaths in 5-year follow-up period 103 censored before 5-years
33 SURVIVAL RESECTION ONLY
34 SURVIVAL CHEMO ONLY
35 SURVIVAL RESECTION + CHEMO
36 SURVIVAL RESECTION ONLY Factor (REF) OR and 95% CI Black (white) 0.84 (0.67, 1.08) Hispanic (white) 1.11 (0.77, 1.63) Rectum (colon) 1.11 (0.79,1.57) Liver metastases (no) 1.99 (1.62, 2.40) Lung metastases (no) 0.94 (0.78, 1.14) Carcinomatosis (no) 1.21 (1.03, 1.42) ( ) 0.96 (0.82, 1.12) Liver resection 0.89 (0.74, 1.08) *Model controls for age, gender, race, comorbidity, SES, as well as factors shown above. If not shown, factor is not significant.
37 SURVIVAL CHEMO ONLY Factor (REF) OR and 95% CI Modern chemotherapy (standard) 0.61 (0.44, 0.83) Black (white) 0.99 (0.66, 1.50) Hispanic (white) 2.42 (1.15, 5.12) Rectum (colon) 0.88 (0.63, 1.22) Liver metastases (no) 1.36 (0.90, 2.04) Lung metastases (no) 0.89 (0.67, 1.19) Carcinomatosis (no) 1.04 (0.79, 1.39) ( ) 1.01 (0.75, 1.36) *Model controls for age, gender, race, comorbidity, SES, as well as factors shown above. If not shown, factor is not significant.
38 SURVIVAL RESECTION + CHEMO Factor (REF) OR and 95% CI Modern chemotherapy (standard) 1.03 (0.86, 1.23) years (85+) 0.60 (0.40, 0.89) years 0.64 (0.43, 0.95) years 0.69 (0.47, 1,03) years 0.91 (0.60, 1.39) Rectum (colon) 0.84 (0.64, 1.09) Liver metastases (no) 1.25 (1.02, 1.53) Lung metastases (no) 0.93 (0.80, 1.09) Carcinomatosis (no) 1.35 (1.15, 1.57) ( ) 0.60 (0.51, 0.72) *Model controls for age, gender, race, comorbidity, SES, as well as factors shown above. If not shown, factor is not significant.
39 SURVIVAL NO TREATMENT Factor (REF) OR and 95% CI Black (white) 0.94 (0.75, 1.18) Hispanic (white) 0.69 (0.45, 1.08) Rectum (colon) 0.89 (0.70, 1.12) Liver metastases (no) 1.36 (1.14, 1.63) Lung metastases (no) 0.74 (0.60, 0.92) Carcinomatosis (no) 1.35 (1.11, 1.64) ( ) 0.95 (0.80, 1.12) *Model controls for age, gender, race, comorbidity, SES, as well as factors shown above. If not shown, factor is not significant.
40 OBJECTIVE Evaluate the comparative effectiveness of timing of surgery and resection of the primary tumor Resection before chemotherapy Chemotherapy before resection
41 METHODS Identify a group of treated patients Resection of primary tumor OR Chemotherapy Exclude patients who underwent emergent colectomy/diverting colostomy 18.7% emergent surgery


42 ASSUMPTIONS Resection Resection + chemotherapy Chemotherapy Resection first Chemotherapy first
43 OUTCOMES Overall survival Disease-specific survival Need for emergent surgery Complications after original elective operation Surgery done <4 weeks after completion of a course of chemotherapy or mid-cycle Completion of chemotherapy
44 SELECTION BIAS Stratify Surgery and chemotherapy only group? Patients with carcinomatosis? Liver mets? Propensity score analysis with inverse probability of treatment weighting? IV? Link to MDS
45 NURSING HOME PATIENTS Link to TCR or SEER-Medicare to MDS Provides serial detailed cognitive and functional assessements Describe current treatment patterns in colon cancer Evaluate factors predicting resection and/or chemotherapy Evaluate hospital days, ICU days, overall survival, and functional decline with various treatment strategies Stratified by life expectancy using modified mortality risk index (uses MDS data)
Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer
 Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer Gabriela M. Vargas, MD Kristin M. Sheffield, PhD, Abhishek Parmar, MD, Yimei Han, MS, Kimberly M. Brown,
Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer Gabriela M. Vargas, MD Kristin M. Sheffield, PhD, Abhishek Parmar, MD, Yimei Han, MS, Kimberly M. Brown,
DAYS IN PANCREATIC CANCER
 HOSPITAL AND MEDICAL CARE DAYS IN PANCREATIC CANCER Annals of Surgical Oncology, March 27, 2012 Casey B. Duncan, Kristin M. Sheffield, Daniel W. Branch, Yimei Han, Yong-Fang g Kuo, James S. Goodwin, Taylor
HOSPITAL AND MEDICAL CARE DAYS IN PANCREATIC CANCER Annals of Surgical Oncology, March 27, 2012 Casey B. Duncan, Kristin M. Sheffield, Daniel W. Branch, Yimei Han, Yong-Fang g Kuo, James S. Goodwin, Taylor
THE SURVIVORSHIP EXPERIENCE IN PANCREATIC CANCER
 THE SURVIVORSHIP EXPERIENCE IN PANCREATIC CANCER Casey A. Boyd, Jaime Benarroch, Kristin M. Sheffield, Yimei Han, Catherine D. Cooksley, Taylor S. Riall Department of Surgery The University of Texas Medical
THE SURVIVORSHIP EXPERIENCE IN PANCREATIC CANCER Casey A. Boyd, Jaime Benarroch, Kristin M. Sheffield, Yimei Han, Catherine D. Cooksley, Taylor S. Riall Department of Surgery The University of Texas Medical
Surveillance of Pancreatic Cancer Patients Following Surgical Resection
 Surveillance of Pancreatic Cancer Patients Following Surgical Resection Jaime Benarroch-Gampel, M.D., M.S. CERCIT Scholar CERCIT Workshops March 16, 2012 INTRODUCTION Pancreatic cancer is the 4 th leading
Surveillance of Pancreatic Cancer Patients Following Surgical Resection Jaime Benarroch-Gampel, M.D., M.S. CERCIT Scholar CERCIT Workshops March 16, 2012 INTRODUCTION Pancreatic cancer is the 4 th leading
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Using claims data to investigate RT use at the end of life. B. Ashleigh Guadagnolo, MD, MPH Associate Professor M.D. Anderson Cancer Center
 Using claims data to investigate RT use at the end of life B. Ashleigh Guadagnolo, MD, MPH Associate Professor M.D. Anderson Cancer Center Background 25% of Medicare budget spent on the last year of life.
Using claims data to investigate RT use at the end of life B. Ashleigh Guadagnolo, MD, MPH Associate Professor M.D. Anderson Cancer Center Background 25% of Medicare budget spent on the last year of life.
Surgical Management of Metastatic Colon Cancer: analysis of the Surveillance, Epidemiology and End Results (SEER) database
 database") Surgical Management of Metastatic Colon Cancer: analysis of the Surveillance, Epidemiology and End Results (SEER) database Hadi Khan, MD 1, Adam J. Olszewski, MD 2 and Ponnandai S. Somasundar, MD 1 1 Department
Surgical Management of Metastatic Colon Cancer: analysis of the Surveillance, Epidemiology and End Results (SEER) database Hadi Khan, MD 1, Adam J. Olszewski, MD 2 and Ponnandai S. Somasundar, MD 1 1 Department
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options
 State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: diagnosis and management of colorectal cancer 1.1 Short title Colorectal cancer 2 The remit The Department
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: diagnosis and management of colorectal cancer 1.1 Short title Colorectal cancer 2 The remit The Department
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Disclosures. Colorectal Cancer Update GAFP November Risk Assessment. Colon and Rectal Cancer The Challenge. Issues in Colon and Rectal Cancer
 Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Patient Presentation. 32 y.o. female complains of lower abdominal mass CEA = 433, CA125 = 201
 Patient Presentation 32 y.o. female complains of lower abdominal mass CEA = 433, CA125 = 201 CT shows: Thickening of the right hemidiaphragm CT shows: Fluid in the right paracolic sulcus CT shows: Large
Patient Presentation 32 y.o. female complains of lower abdominal mass CEA = 433, CA125 = 201 CT shows: Thickening of the right hemidiaphragm CT shows: Fluid in the right paracolic sulcus CT shows: Large
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Clinical Policy: Ramucirumab (Cyramza) Reference Number: CP.PHAR.119
 Reference Number: CP.PHAR.119") Clinical Policy: (Cyramza) Reference Number: CP.PHAR.119 Effective Date: 05/15 Last Review Date: 04/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: (Cyramza) Reference Number: CP.PHAR.119 Effective Date: 05/15 Last Review Date: 04/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
COLORECTAL CANCER CASES
 COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study
 Original article Annals of Gastroenterology (2013) 26, 346-352 Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study Subhankar Chakraborty
Original article Annals of Gastroenterology (2013) 26, 346-352 Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study Subhankar Chakraborty
Cost-Effectiveness of Second-Line Chemotherapy/ Biologics among Elderly Metastatic Colon Cancer Patients
 Adv Ther (2014) 31:724 734 DOI 10.1007/s12325-014-0134-8 ORIGINAL RESEARCH Cost-Effectiveness of Second-Line Chemotherapy/ Biologics among Elderly Metastatic Colon Cancer Patients Zhiyuan Zheng Eberechukwu
Adv Ther (2014) 31:724 734 DOI 10.1007/s12325-014-0134-8 ORIGINAL RESEARCH Cost-Effectiveness of Second-Line Chemotherapy/ Biologics among Elderly Metastatic Colon Cancer Patients Zhiyuan Zheng Eberechukwu
Stage III Colon Cancer Susquehanna Cancer Center Warren L Robinson, MD, FACP May 9, 2007
 Stage III Colon Cancer Susquehanna Cancer Center 1997-21 Warren L Robinson, MD, FACP May 9, 27 Stage III Colon Cancer Susquehanna Cancer Center 1997-21 Colorectal cancer is the third most common cancer
Stage III Colon Cancer Susquehanna Cancer Center 1997-21 Warren L Robinson, MD, FACP May 9, 27 Stage III Colon Cancer Susquehanna Cancer Center 1997-21 Colorectal cancer is the third most common cancer
Avastin Sample Coding
 First- and Second-line Metastatic Colorectal Cancer C18.0 Malignant neoplasm of the cecum C18.1 Malignant neoplasm of appendix C18.2-C18.9 C19 C20 C21.8 Malignant neoplasm of the colon, various sites Malignant
First- and Second-line Metastatic Colorectal Cancer C18.0 Malignant neoplasm of the cecum C18.1 Malignant neoplasm of appendix C18.2-C18.9 C19 C20 C21.8 Malignant neoplasm of the colon, various sites Malignant
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION
 CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
COLORECTAL CANCER 44
 COLORECTAL CANCER 44 Colorectal Cancer Highlights from the 2009 Annual Meeting of the American Society of Clinical Oncology Edited by Stuart M. Lichtman, MD Memorial Sloan-Kettering Cancer Center Commack,
COLORECTAL CANCER 44 Colorectal Cancer Highlights from the 2009 Annual Meeting of the American Society of Clinical Oncology Edited by Stuart M. Lichtman, MD Memorial Sloan-Kettering Cancer Center Commack,
Erbitux. Erbitux (cetuximab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.84 Subject: Erbitux Page: 1 of 6 Last Review Date: December 2, 2016 Erbitux Description Erbitux (cetuximab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.84 Subject: Erbitux Page: 1 of 6 Last Review Date: December 2, 2016 Erbitux Description Erbitux (cetuximab)
Systemic Therapy for Metastatic Colorectal Cancer: Patterns of Chemotherapy and Biologic Therapy Use in US Medical Oncology Practice
 Original Contribution Systemic Therapy for Metastatic Colorectal Cancer: Patterns of Chemotherapy and Biologic Therapy Use in US Medical Oncology Practice By Gregory P. Hess, MD, MSc, Peter Feng Wang,
Original Contribution Systemic Therapy for Metastatic Colorectal Cancer: Patterns of Chemotherapy and Biologic Therapy Use in US Medical Oncology Practice By Gregory P. Hess, MD, MSc, Peter Feng Wang,
Current standard in treatment of peritoneal carcinomotisis. Data behind the HIPEC trials
 Current standard in treatment of peritoneal carcinomotisis Data behind the HIPEC trials Overview Peritoneal carcinomatosis STANDARD treatment HIPEC Results of treatment Counter side of treatment Peritoneal
Current standard in treatment of peritoneal carcinomotisis Data behind the HIPEC trials Overview Peritoneal carcinomatosis STANDARD treatment HIPEC Results of treatment Counter side of treatment Peritoneal
CLINICAL MEDICAL POLICY
 CLINICAL MEDICAL POLICY Policy Name: Avastin (bevacizumab) Policy Number: MP-030-MD-DE Responsible Department(s): Medical Management; Clinical Pharmacy Provider Notice Date: 10/01/2017 Original Effective
CLINICAL MEDICAL POLICY Policy Name: Avastin (bevacizumab) Policy Number: MP-030-MD-DE Responsible Department(s): Medical Management; Clinical Pharmacy Provider Notice Date: 10/01/2017 Original Effective
Diagnosed with Metastatic Colorectal Cancer?
 ESSENTIALS Metastatic Colorectal Cancer Diagnosed with Metastatic Colorectal Cancer? It can be frightening to learn you or a loved one has been diagnosed with metastatic colorectal cancer. It is important
ESSENTIALS Metastatic Colorectal Cancer Diagnosed with Metastatic Colorectal Cancer? It can be frightening to learn you or a loved one has been diagnosed with metastatic colorectal cancer. It is important
Management Of Patients With Metastatic Colorectal Cancer in Lebanese Hospitals and Associated Direct Cost: A Multicenter Cohort Study
 Management Of Patients With Metastatic Colorectal Cancer in Lebanese Hospitals and Associated Direct Cost: A Multicenter Cohort Study Henaine AM; Chahine G; Massoud M; Salameh P; Awada S; Lahoud N; El
Management Of Patients With Metastatic Colorectal Cancer in Lebanese Hospitals and Associated Direct Cost: A Multicenter Cohort Study Henaine AM; Chahine G; Massoud M; Salameh P; Awada S; Lahoud N; El
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Chemotherapy of colon cancers
 Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
ADVANCES IN COLON CANCER
 ADVANCES IN COLON CANCER Peter T. Silberstein, M.D., FACP Professor, Creighton University Chief Hematology/Oncology UNIVERSAL SCREENING FOR LYNCH SYNDROME OF ALL PATIENTS WITH COLON CANCER ADOPTED BY CHI
ADVANCES IN COLON CANCER Peter T. Silberstein, M.D., FACP Professor, Creighton University Chief Hematology/Oncology UNIVERSAL SCREENING FOR LYNCH SYNDROME OF ALL PATIENTS WITH COLON CANCER ADOPTED BY CHI
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Treatment of Colorectal Liver Metastases State of the Art
 Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Department of Epidemiology, University of Iowa College of Public Health, Iowa City, IA, 2. College of Medicine, Iowa City, I
 Variation in staging and treatment of rectal cancer by National Cancer Institute (NCI) designation and medical school affiliation: Analysis of Surveillance, Epidemiology 1 Department of Epidemiology, University
Variation in staging and treatment of rectal cancer by National Cancer Institute (NCI) designation and medical school affiliation: Analysis of Surveillance, Epidemiology 1 Department of Epidemiology, University
Hospital and Medical Care Days in Pancreatic Cancer
 Ann Surg Oncol (12) 19:243 2442 DOI.124/s434-012-2326-2 ORIGINAL ARTICLE HEALTHCARE POLICY AND OUTCOMES Hospital and Medical Care Days in Pancreatic Cancer Casey A. Boyd, MD 1, Daniel W. Branch, MS 1,
Ann Surg Oncol (12) 19:243 2442 DOI.124/s434-012-2326-2 ORIGINAL ARTICLE HEALTHCARE POLICY AND OUTCOMES Hospital and Medical Care Days in Pancreatic Cancer Casey A. Boyd, MD 1, Daniel W. Branch, MS 1,
Pharmacy Management Drug Policy
 11/13, 10/12, 11/11, 1, 6/10, Page 1 of 5 DESCRIPTION: Cetuximab is a recombinant humanized monoclonal antibody that binds specifically to the extracellular domain of the human epidermal growth factor
11/13, 10/12, 11/11, 1, 6/10, Page 1 of 5 DESCRIPTION: Cetuximab is a recombinant humanized monoclonal antibody that binds specifically to the extracellular domain of the human epidermal growth factor
UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER. Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists
 UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists WHAT IS COLON CANCER? WHAT CAUSES COLORECTAL CANCER? WHAT ARE THE RISK
UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists WHAT IS COLON CANCER? WHAT CAUSES COLORECTAL CANCER? WHAT ARE THE RISK
CON: Removal of the Breast Primary in Patients with Metastatic Breast Cancer
 CON: Removal of the Breast Primary in Patients with Metastatic Breast Cancer Amelia B. Zelnak, M.D., M.Sc. Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University
CON: Removal of the Breast Primary in Patients with Metastatic Breast Cancer Amelia B. Zelnak, M.D., M.Sc. Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University
Vectibix. Vectibix (panitumumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.85 Subject: Vectibix Page: 1 of 5 Last Review Date: December 2, 2016 Vectibix Description Vectibix
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.85 Subject: Vectibix Page: 1 of 5 Last Review Date: December 2, 2016 Vectibix Description Vectibix
A clinical study of metastasized rectal cancer treatment: assessing a multimodal approach
 Med Oncol (2014) 31:839 DOI 10.1007/s12032-014-0839-1 ORIGINAL PAPER A clinical study of metastasized rectal cancer treatment: assessing a multimodal approach Michaela Jung Annica Holmqvist Xiao-Feng Sun
Med Oncol (2014) 31:839 DOI 10.1007/s12032-014-0839-1 ORIGINAL PAPER A clinical study of metastasized rectal cancer treatment: assessing a multimodal approach Michaela Jung Annica Holmqvist Xiao-Feng Sun
TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS
 TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS Anna Lepistö, MD, PhD Department of Colorectal Surgery, Abdominal Center, Helsinki University Hospital Incidence, prevalence and risk factors for peritoneal
TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS Anna Lepistö, MD, PhD Department of Colorectal Surgery, Abdominal Center, Helsinki University Hospital Incidence, prevalence and risk factors for peritoneal
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
CERCIT Project 2: Assessing the Quality of Cancer Treatment in Texas. Sharon Giordano
 CERCIT Project 2: Assessing the Quality of Cancer Treatment in Texas Sharon Giordano October 21, 2011 Specific Aims Determine the agreement of the Texas Cancer Registry and claims databases for the rates
CERCIT Project 2: Assessing the Quality of Cancer Treatment in Texas Sharon Giordano October 21, 2011 Specific Aims Determine the agreement of the Texas Cancer Registry and claims databases for the rates
Unplanned Hospitalizations and Readmissions among Elderly Patients with GI Cancer
 Unplanned Hospitalizations and Readmissions among Elderly Patients with GI Cancer September 19, 2014 Joanna-Grace M. Manzano, MD Assistant Professor Department of General Internal Medicine UT MD Anderson
Unplanned Hospitalizations and Readmissions among Elderly Patients with GI Cancer September 19, 2014 Joanna-Grace M. Manzano, MD Assistant Professor Department of General Internal Medicine UT MD Anderson
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Stivarga) Reference Number: CP.CPA.157 Effective Date: 11.16.17 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Stivarga) Reference Number: CP.CPA.157 Effective Date: 11.16.17 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
Clinical Policy: Bevacizumab (Avastin) Reference Number: ERX.SPMN.127
 Reference Number: ERX.SPMN.127") Clinical Policy: (Avastin) Reference Number: ERX.SPMN.127 Effective Date: 03/14 Last Review Date: 09/16 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: (Avastin) Reference Number: ERX.SPMN.127 Effective Date: 03/14 Last Review Date: 09/16 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
Colon, Rectum, and Appendix
 Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colon, Rectum, and Appendix. Presentation Outline. Overview Tumor Characteristics
 Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
reviews Staging, and in the Diagnosis, Managed Care Considerations therapy
 reviews therapy Managed Care Considerations in the Diagnosis, Staging, and Treatment of Colorectal Cancer by Johanna Bendell, MD, Director, GI Oncology Research; Associate Director, Drug Development Unit,
reviews therapy Managed Care Considerations in the Diagnosis, Staging, and Treatment of Colorectal Cancer by Johanna Bendell, MD, Director, GI Oncology Research; Associate Director, Drug Development Unit,
Measure Specifications Measure Description
 CMS ID/CMS QCDR ID: CAP 15 Title: BRAF Biomarker Testing to Inform Clinical Management and Treatment Decisions in Patients with Metastatic Colorectal Adenocarcinoma Specifications Description Denominator
CMS ID/CMS QCDR ID: CAP 15 Title: BRAF Biomarker Testing to Inform Clinical Management and Treatment Decisions in Patients with Metastatic Colorectal Adenocarcinoma Specifications Description Denominator
Clinical Policy: Cetuximab (Erbitux) Reference Number: PA.CP.PHAR.317
 Reference Number: PA.CP.PHAR.317") Clinical Policy: (Erbitux) Reference Number: PA.CP.PHAR.317 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that patients
Clinical Policy: (Erbitux) Reference Number: PA.CP.PHAR.317 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that patients
Indeterminate Pulmonary Nodules in Patients with Colorectal Cancer
 Indeterminate Pulmonary Nodules in Patients with Colorectal Cancer Jai Sule 1, Kah Wai Cheong 2, Stella Bee 2, Bettina Lieske 2,3 1 Dept of Cardiothoracic and Vascular Surgery, University Surgical Cluster,
Indeterminate Pulmonary Nodules in Patients with Colorectal Cancer Jai Sule 1, Kah Wai Cheong 2, Stella Bee 2, Bettina Lieske 2,3 1 Dept of Cardiothoracic and Vascular Surgery, University Surgical Cluster,
Staging Laparoscopy in the Management of Gastric Cancer: A Population-Based Analysis
 Staging Laparoscopy in the Management of Gastric Cancer: A Population-Based Analysis Paul J Karanicolas, MD, PhD, Elena B Elkin, PhD, Lindsay M Jacks, MSc, Coral L Atoria, MPH, Vivian E Strong, MD, FACS,
Staging Laparoscopy in the Management of Gastric Cancer: A Population-Based Analysis Paul J Karanicolas, MD, PhD, Elena B Elkin, PhD, Lindsay M Jacks, MSc, Coral L Atoria, MPH, Vivian E Strong, MD, FACS,
THE VALIDITY OF ADMINISTRATIVE DATA AND PATTERNS OF CHEMOTHERAPY USE AMONG ELDERLY COLORECTAL CANCER PATIENTS. Jennifer L.
 THE VALIDITY OF ADMINISTRATIVE DATA AND PATTERNS OF CHEMOTHERAPY USE AMONG ELDERLY COLORECTAL CANCER PATIENTS Jennifer L. Lund, MSPH A dissertation submitted to the faculty of the University of North Carolina
THE VALIDITY OF ADMINISTRATIVE DATA AND PATTERNS OF CHEMOTHERAPY USE AMONG ELDERLY COLORECTAL CANCER PATIENTS Jennifer L. Lund, MSPH A dissertation submitted to the faculty of the University of North Carolina
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
2/20/14& Medical Management of Colon and Rectal Cancer: An Overview. Outline / Learning Objectives. How common is colon cancer?
 Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Ethnic Disparities in the Treatment of Stage I Non-small Cell Lung Cancer. Juan P. Wisnivesky, MD, MPH, Thomas McGinn, MD, MPH, Claudia Henschke, PhD,
 Ethnic Disparities in the Treatment of Stage I Non-small Cell Lung Cancer Juan P. Wisnivesky, MD, MPH, Thomas McGinn, MD, MPH, Claudia Henschke, PhD, MD, Paul Hebert, PhD, Michael C. Iannuzzi, MD, and
Ethnic Disparities in the Treatment of Stage I Non-small Cell Lung Cancer Juan P. Wisnivesky, MD, MPH, Thomas McGinn, MD, MPH, Claudia Henschke, PhD, MD, Paul Hebert, PhD, Michael C. Iannuzzi, MD, and
Avastin (bevacizumab)
") Avastin (bevacizumab) Policy Number: 5.02.502 Last Review: 04/2018 Origination: 03/2017 Next Review: 04/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Avastin
Avastin (bevacizumab) Policy Number: 5.02.502 Last Review: 04/2018 Origination: 03/2017 Next Review: 04/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Avastin
A Bridge to Health Men s Health and Cancer
 A Bridge to Health Men s Health and Cancer Bertrand Tuan, M.D. Pacific Hematology-Oncology Associates California Pacific Medical Center San Francisco, CA Causes of Cancer Death in California Asian Men
A Bridge to Health Men s Health and Cancer Bertrand Tuan, M.D. Pacific Hematology-Oncology Associates California Pacific Medical Center San Francisco, CA Causes of Cancer Death in California Asian Men
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Doctor Discussion Guide
 Talking to your healthcare provider about LONSURF (trifluridine and tipiracil) tablets If you have colon or rectal cancer that has spread to other parts of your body and have previously been treated with
Talking to your healthcare provider about LONSURF (trifluridine and tipiracil) tablets If you have colon or rectal cancer that has spread to other parts of your body and have previously been treated with
PAPER. Initial Presentation With Stage IV Colorectal Cancer
 Initial Presentation With Stage IV Colorectal Cancer How Aggressive Should We Be? PAPER Seth A. Rosen, MD; Joseph F. Buell, MD; Atsushi Yoshida, MD; Scott Kazsuba, BS; Roger Hurst, MD; Fabrizio Michelassi,
Initial Presentation With Stage IV Colorectal Cancer How Aggressive Should We Be? PAPER Seth A. Rosen, MD; Joseph F. Buell, MD; Atsushi Yoshida, MD; Scott Kazsuba, BS; Roger Hurst, MD; Fabrizio Michelassi,
Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association
 Cytoreduction and Hyperthermic Page 1 of 10 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy for the
Cytoreduction and Hyperthermic Page 1 of 10 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy for the
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT?
 DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
Kaoru Takeshima, Kazuo Yamafuji, Atsunori Asami, Hideo Baba, Nobuhiko Okamoto, Hidena Takahashi, Chisato Takagi, and Kiyoshi Kubochi
 Case Reports in Surgery Volume 2016, Article ID 4548798, 5 pages http://dx.doi.org/10.1155/2016/4548798 Case Report Successful Resection of Isolated Para-Aortic Lymph Node Recurrence from Advanced Sigmoid
Case Reports in Surgery Volume 2016, Article ID 4548798, 5 pages http://dx.doi.org/10.1155/2016/4548798 Case Report Successful Resection of Isolated Para-Aortic Lymph Node Recurrence from Advanced Sigmoid
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
Discover the facts about
 Avastin is approved to treat metastatic colorectal cancer (mcrc) for: First- or second-line treatment in combination with intravenous 5-fluorouracil based chemotherapy Second-line treatment when used with
Avastin is approved to treat metastatic colorectal cancer (mcrc) for: First- or second-line treatment in combination with intravenous 5-fluorouracil based chemotherapy Second-line treatment when used with
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Nivolumab for previously treated metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Nivolumab for previously treated metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy
 Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Provider Contribution to Overuse and Underuse of Colorectal Cancer Screening (mostly colonoscopy)
") Provider Contribution to Overuse and Underuse of Colorectal Cancer Screening (mostly colonoscopy) James S. Goodwin, MD George and Cynthia Mitchell Distinguished Chair in Geriatric Medicine Director, Sealy
Provider Contribution to Overuse and Underuse of Colorectal Cancer Screening (mostly colonoscopy) James S. Goodwin, MD George and Cynthia Mitchell Distinguished Chair in Geriatric Medicine Director, Sealy
WHAT FACTORS INFLUENCE AN ANALYSIS OF HOSPITALIZATIONS AMONG DYING CANCER PATIENTS? AGGRESSIVE END-OF-LIFE CANCER CARE. Deesha Patel May 11, 2011
 WHAT FACTORS INFLUENCE HOSPITALIZATIONS AMONG DYING CANCER PATIENTS? AN ANALYSIS OF AGGRESSIVE END-OF-LIFE CANCER CARE. Deesha Patel May 11, 2011 WHAT IS AGGRESSIVE EOL CARE? Use of ineffective medical
WHAT FACTORS INFLUENCE HOSPITALIZATIONS AMONG DYING CANCER PATIENTS? AN ANALYSIS OF AGGRESSIVE END-OF-LIFE CANCER CARE. Deesha Patel May 11, 2011 WHAT IS AGGRESSIVE EOL CARE? Use of ineffective medical
Clinical Policy: Regorafenib (Stivarga) Reference Number: CP.PHAR.107 Effective Date: 12/12 Last Review Date: 11/16
 Reference Number: CP.PHAR.107 Effective Date: 12/12 Last Review Date: 11/16") Clinical Policy: (Stivarga) Reference Number: CP.PHAR.107 Effective Date: 12/12 Last Review Date: 11/16 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Stivarga) Reference Number: CP.PHAR.107 Effective Date: 12/12 Last Review Date: 11/16 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Management of colorectal cancer liver metastases
 Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Preoperative Data Colorectal Cancer Database
 Preoperative Data Please place patient label here Patient Information Patient s Last Name First Middle Initial UR MH MP Birth Date Sex Post Code / / M F ECOG (see codes below) Date of Diagnosis Consultant
Preoperative Data Please place patient label here Patient Information Patient s Last Name First Middle Initial UR MH MP Birth Date Sex Post Code / / M F ECOG (see codes below) Date of Diagnosis Consultant
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies
 Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 of the clinical trial data for this outcome. Therefore, perc considered that the cost-effectiveness of cetuximab plus FOLFIRI would be at the higher end of the EGP s range of best estimates. Therefore,
of the clinical trial data for this outcome. Therefore, perc considered that the cost-effectiveness of cetuximab plus FOLFIRI would be at the higher end of the EGP s range of best estimates. Therefore,
The impact of extrahepatic disease among patients undergoing liver-directed therapy for neuroendocrine liver metastasis
 Received: 1 May 2017 Accepted: 23 May 2017 DOI: 10.1002/jso.24727 RESEARCH ARTICLE The impact of extrahepatic disease among patients undergoing liver-directed therapy for neuroendocrine liver metastasis
Received: 1 May 2017 Accepted: 23 May 2017 DOI: 10.1002/jso.24727 RESEARCH ARTICLE The impact of extrahepatic disease among patients undergoing liver-directed therapy for neuroendocrine liver metastasis
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Bevacizumab 5mg/kg Therapy 14 days
 INDICATIONS FOR USE: Bevacizumab 5mg/kg Therapy 14 days Regimen Code 00211a *Reimbursement status Hospital INDICATION ICD10 In combination with fluoropyrimidine-based chemotherapy C18 for treatment of
INDICATIONS FOR USE: Bevacizumab 5mg/kg Therapy 14 days Regimen Code 00211a *Reimbursement status Hospital INDICATION ICD10 In combination with fluoropyrimidine-based chemotherapy C18 for treatment of
Κίκα Πλοιαρχοπούλου. Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών
 Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA. TIMUR MITIN, MD, PhD
 THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
NATIONAL BOWEL CANCER AUDIT The feasibility of reporting Patient Reported Outcome Measures as part of a national colorectal cancer audit
 NATIONAL BOWEL CANCER AUDIT The feasibility of reporting Patient Reported Outcome Measures as part of a national colorectal cancer audit NBOCA: Feasibility Study Date of publication: Thursday 9 th August
NATIONAL BOWEL CANCER AUDIT The feasibility of reporting Patient Reported Outcome Measures as part of a national colorectal cancer audit NBOCA: Feasibility Study Date of publication: Thursday 9 th August
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
COLORECTAL CANCER RESEARCH Month Ending May 15, 2009
 COLORECTAL CANCER RESEARCH Month Ending May 15, 2009 The following colorectal cancer research update extends from April 18 May 15, 2009 inclusive and is intended for informational purposes only. DRUGS
COLORECTAL CANCER RESEARCH Month Ending May 15, 2009 The following colorectal cancer research update extends from April 18 May 15, 2009 inclusive and is intended for informational purposes only. DRUGS
COME HOME Innovative Oncology Business Solutions, Inc.
 COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
Introduction. Original Article. Sudeep Karve*, Maria Lorenzo 1, Astra M Liepa 2, Lisa M Hess 2, James A Kaye, and Brian Calingaert
 In the United States (US), it is estimated that a total of 22,220 cases of gastric cancer will be diagnosed in 2014, representing 1.3% of all new cancer cases, and 10,990 deaths will occur as a result.
In the United States (US), it is estimated that a total of 22,220 cases of gastric cancer will be diagnosed in 2014, representing 1.3% of all new cancer cases, and 10,990 deaths will occur as a result.
The 2010 Gastrointestinal Cancers Symposium Oral Abstract Session: Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract
 The 2010 Gastrointestinal Cancers Symposium : Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract Abstract #131: Phase I study of MK 0646 (dalotuzumab), a humanized monoclonal antibody against
The 2010 Gastrointestinal Cancers Symposium : Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract Abstract #131: Phase I study of MK 0646 (dalotuzumab), a humanized monoclonal antibody against
Current Status of Adjuvant Therapy for Colorectal Cancer
 Review Article [1] May 01, 2004 By Michael J. O connell, MD [2] Adjuvant therapy with chemotherapy and/or radiation therapy in addition to surgery improves outcome for patients with high-risk carcinomas
Review Article [1] May 01, 2004 By Michael J. O connell, MD [2] Adjuvant therapy with chemotherapy and/or radiation therapy in addition to surgery improves outcome for patients with high-risk carcinomas