LGM International, Inc.
|
|
|
- Ami Floyd
- 5 years ago
- Views:
Transcription




1 Liqui-PREP TM Cytology Atlas
2 Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It will be noticed that descriptions of similar pictures are duplicated. The different pictures for a giving description are to show the observed consistency of actual the Liqui-PREP TM produced slides. It should be noted, the Liqui-PREP TM System uses classical laboratory techniques to process a cytology specimen. The resulting slides are from randomized homogeneous aliquots of the cytology specimen. Once the Liqui-PREP TM processed slide is made and stained, diagnosis is performed by trained professionals by reading the prepared Liqui-PREP TM slide. The specimens used for this atlas are from evaluation studies made by the following sources: Studies and End User Quality Assurance program. Selected Routine Specimen Pictures N. Anontwatanawong, National Cancer Institute, Thailand. We want to thank the following professionals that have reviewed slides and pictures, made the interpretations and/or reviewed this Atlas for technical quality. Dr. Ivan Rapado, M.D. Pathologist: Consulting Medical Director LGM International, Inc. Dr. Jose de Jesus Curiel-Valdes, M.D., ASCP Laboratorio de Patologia Notre Dame Hospital, Mexico City, Mexico



3 QUALIFICATION 101-Endocervical Cells: 40 x magnification picture of numerous columnar cells. Columnar cells with basally located nuclei, vacuolated cytoplasm and prominent cell borders. 102-Endocervical Cells: 40 x magnification picture of two columnar cells. Columnar cells with basally located nuclei, vacuolated cytoplasm and prominent cell borders.
4 QUALIFICATION 103-Endocervical Cells: 40 x magnification picture of several columnar cells. Columnar cells with basally located nuclei, vacuolated cytoplasm and prominent cell borders. 104-Endocervical Cells: 40 x magnification picture of numerous columnar cells, some isolated and a group arranged in a honeycomb configuration.



5 QUALIFICATION 107-Endocervical Cells: 40 x magnification picture of columnar cells arranged in a honeycomb configuration along with superficial squamous cells. The group of cells remain attached at their basal plate. 0705S-Endocervical Cells: 40 x magnification picture of numerous columnar cells, some isolated and a group arranged in The picket Fence configuration.
6 WITHIN NORMAL LIMITS 109-Negative within Normal Limits: 10x magnification picture shows a well dispersed population of superficial squamous cells. A few inflammatory cells are present in the background. The nuclei are round, small (pyknotic). The chromatin are dense and the nucleoli are absent. The cytoplasm are polygonal, abundant, pale, clear (transparent) and eosinophilic The N/C ratio is 1: Negative within Normal Limits: 10x magnification picture shows a well dispersed population of superficial squamous cells. A few inflammatory cells are present in the background. The nuclei are round, small (pyknotic). The chromatin are dense and the nucleoli are absent. The cytoplasm are polygonal, abundant, pale, clear (transparent) and eosinophilic The N/C ratio is 1:10.
7 WITHIN NORMAL LIMITS 111-Negative within Normal Limits : 40x magnification picture shows a well dispersed population p of superficial squamous cells. A few inflammatory cells are present in the background. The nuclei are round, small (pyknotic). The chromatin are dense and the nucleoli are absent. The cytoplasm are polygonal, abundant, pale, clear (transparent) and eosinophilic The N/C ratio is 1: Negative within Normal Limits : 10x magnification picture shows a well dispersed population p of superficial squamous cells. A few inflammatory cells are present in the background. The nuclei are round, small (pyknotic). The chromatin are dense and the nucleoli are absent. The cytoplasm are polygonal, abundant, pale, clear (transparent) and eosinophilic The N/C ratio is 1:10.
.")
 and eosinophilic The N/C ratio is 1:10.")

8 WITHIN NORMAL LIMITS 113-Negative within Normal Limits: 10x magnification picture shows a well dispersed population p of superficial squamous cells. A few inflammatory cells are present in the background. The nuclei are round, small (pyknotic). The chromatin are dense and the nucleoli are absent. The cytoplasm are polygonal, abundant, pale, clear (transparent) and eosinophilic The N/C ratio is 1: Negative within Normal Limits: 10x magnification picture shows a well dispersed population p of superficial squamous cells. A few inflammatory cells are present in the background. The nuclei are round, small (pyknotic). The chromatin are dense and the nucleoli are absent. The cytoplasm are polygonal, abundant, pale, clear (transparent) and eosinophilic The N/C ratio is 1:10.
9 BENIGN CELLULAR CHANGES Cellular Changes due to Inflammation: 40X magnification picture of superficial cells. A few inflammatory cells are covering the squamous cells. The nuclei are mildly enlarged due to inflammation. 118-Cellular Changes due to Inflammation: 10X magnification picture of superficial, intermediate (1) and metaplastic cells (2). Numerous inflammatory cells are covering but not obscuring squamous cells. The squamous cells show mild nuclear enlargement.



10 BENIGN CELLULAR CHANGES Cellular Changes due to Inflammation: 10X magnification picture of superficial cells. Numerous inflammatory cells are covering but not obscuring squamous cells. The nuclei are mildly enlarged due to inflammation. 120-Cellular Changes due to Inflammation: 40X magnification of superficial, intermediate cells and inflammatory cells covering but not obscuring the squamous cells. There is mild to moderate nuclear enlargement. Moderate enlargement (1) The chromatin is smudgy and pale. Micro nucleoli are seen and slight there is perinuclear clearing.


.")


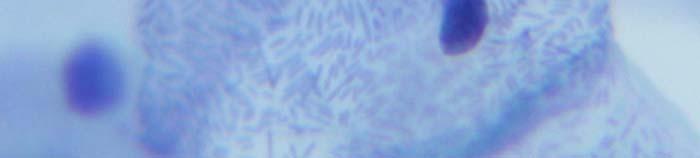
11 BENIGN CELLULAR CHANGES 127-Bacterial Flora Shift Clue Cell : 40X picture of intermediate squamous cells covered by bacteria ( Clue Cell ). Consistent with Gardnerella vaginalis. 128-Bacterial Flora Shift Clue Cell : 40X picture of intermediate squamous cells covered by bacteria ( Clue Cell ). Consistent with Gardnerella vaginalis.






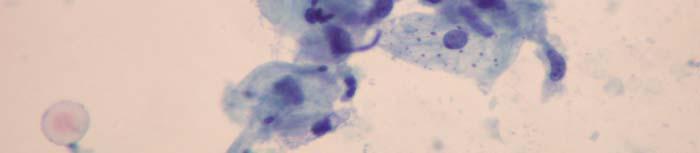
12 BENIGN CELLULAR CHANGES 129-Cellular Changes associated with Herpes virus: 10X picture of Herpes group infection. Transformed squamous cells with cytomegaly, multi-nucleation, molded nuclei with ground glass appearance. Intra nuclear inclusions and perinuclear clearing. Inflammatory cells are present. 130-Cellular Changes associated with Herpes virus: 40X picture of Herpes group infection. Transformed squamous cells with cytomegaly, multi-nucleation, molded nuclei with ground glass appearance. Intra nuclear inclusions and perinuclear clearing. Inflammatory cells are present.






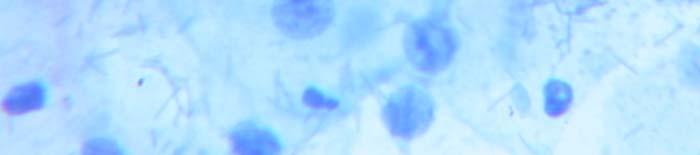
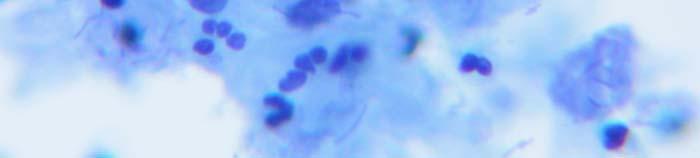
13 BENIGN CELLULAR CHANGES Cellular Changes associated with Herpes virus: 40X picture of Herpes group infection. Transformed squamous cells with cytomegaly, multi-nucleation (1), molded nuclei with ground glass appearance. Intra nuclear inclusions and perinuclear clearing. Inflammatory cells are present. 132-Actinomyces species: 40X picture of an infection of a IUD. Delicate filamentous bacterium which branch freely, resembling fungal hyphae in loose aggregates. Close observations show dense basophilic balls. Inflammatory cells are present.






14 BENIGN CELLULAR CHANGES 133-Actinomycetes species.: 10X picture of an infection of a IUD. Delicate filamentous bacterium which branch freely, resembling fungal hyphae in loose aggregates. Close observations show dense basophilic balls. Inflammatory cells are present. 134-Actinomycetes species: 40X picture of an infection of a IUD. Delicate filamentous bacterium which branch freely, resembling fungal hyphae in loose aggregates. Close observations show dense basophilic balls. Inflammatory cells are present.

 139-Changes due to Radiation: 40X magnification shows squamous cells")

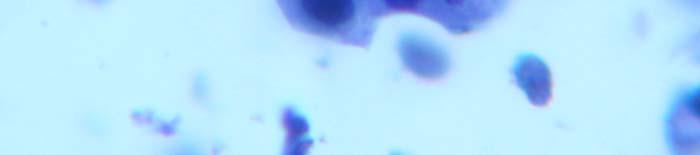
15 BENIGN CELLULAR CHANGES 1 136A-Atrophic Atrophic Cells.: 40X magnification of a cervical sample in atrophy. Small, rounded, this basophilic parabasal squamous cells is typical of Atrophic cells. Atrophic cell (1) 139-Changes due to Radiation: 40X magnification shows squamous cells with fine vacuolization of the cytoplasm, cytomegaly, kariomegaly. Nuclei are multinucleated with wrinkling of the nuclear membrane. Pleomorphic shapes and smudged nuclear chromatin are observed along with Inflammatory cells and amorphous debris.
16 BENIGN CELLULAR CHANGES 139A-Para-Keratosis: 40x magnification of mature squamous cells with hyper-keratinized cytoplasm and pyknotic nuclei. Consistent with uterine prolapse. 139B-Candida albicans: 40x magnification of squamous cells and multiple yeast forms with budding or delicate pseudo septate filaments (pseudo-hyphae). Acute branching intra and extra cellular.
)")


17 BENIGN CELLULAR CHANGES 1 139C-Candida Candida albicans: 40x magnification of squamous cells and multiple yeast forms with budding or delicate pseudo septate filaments (pseudo-hyphae (1)).). Acute branching intra and extra cellular. 140A-Benign Endometrial Cell: 40x magnification of cell mass with double contouring, compact central stromal cells. Peripheral glandular cells, surrounded by Inflammatory cells. Few Inflammatory cells are noted. The glandular cells are round to oval, scant cytoplasm and small nuclei. Nucleoli indistinct with coarsely granular to compact chromatin.
,,")


18 BENIGN CELLULAR CHANGES Post coital smear: 40x magnification picture of spermatozoa (1),, histio-cytic cells and superficial cells. The spermatozoa has a long tail and pointed pear shaped head. The distal half of the head is pale and the portion adjacent to the tail is stained dark.
 with enlargement of the nuclear size.")


19 SQUAMOUS CELL ABNORMALITIES 141-ASCUS: 40x magnification of atypical squamous cells (of undetermined significance) with enlargement of the nuclear size. The increase in nuclear size is more marked than reactive changes and less than LSIL. Nucleus size are of intermediated and parabasal cells or of mature metaplastic cells. 142-ASCUS: 40x magnification of atypical squamous cells (of undetermined significance) with enlargement of the nuclear size. The increase in nuclear size is more marked than reactive changes and less than LSIL. Nucleus size are of intermediated and parabasal cells or of mature metaplastic cells.
 with enlargement of the nuclear size.")

20 SQUAMOUS CELL ABNORMALITIES 144-ASCUS: 40x magnification atypical squamous cells (of undetermined significance) with enlargement of the nuclear size. The increase in nuclear size is more marked than reactive changes and less than LSIL. Nucleus size are of intermediated and parabasal cells or of mature metaplastic cells. 145-ASCUS: 40x magnification atypical squamous cells (of undetermined significance) with enlargement of the nuclear size. The increase in nuclear size is more marked than reactive changes and less than LSIL. Nucleus size are of intermediated and parabasal cells or of mature metaplastic cells.





21 SQUAMOUS CELL ABNORMALITIES 146-ASCUS: 40x magnification atypical squamous cells (of undetermined significance) with enlargement of the nuclear size. The increase in nuclear size is more marked than reactive changes and less than LSIL. Nucleus size are of intermediated and parabasal cells or of mature metaplastic cells. 147-ASCUS: 40x magnification atypical squamous cells (of undetermined significance) with enlargement of the nuclear size. The increase in nuclear size is more marked than reactive changes and less than LSIL. Nucleus size are of intermediated and parabasal cells or of mature metaplastic cells.





22 SQUAMOUS CELL ABNORMALITIES 149-ASCUS: 40x magnification of atypical squamous cells (of undetermined significance) with enlargement of the nuclear size. The increase in nuclear size is more marked than reactive changes and less than LSIL. Nucleus size are of intermediated and parabasal cells or of mature metaplastic cells. 150-ASCUS: 40x magnification of atypical squamous cells (of undetermined significance) with enlargement of the nuclear size. The increase in nuclear size is more marked than reactive changes and less than LSIL. Nucleus size are of intermediated and parabasal cells or of mature metaplastic cells.



23 SQUAMOUS CELL ABNORMALITIES 153-ASCUS: 40x magnification atypical squamous cells (of undetermined significance) with enlargement of the nuclear size. The increase in nuclear size is more marked than reactive changes and less than LSIL. Nucleus size are of intermediated and parabasal cells or of mature metaplastic cells.






24 SQUAMOUS CELL ABNORMALITIES 157-LSIL: 40x magnification of low grade squamous intra-epithelial lesion/mild dysplasia/cin I. Intermediate squamous cells with enlargement of the nuclei. Hyperchromasia, elevated N/C ratio (3 to 4 times the normal intermediate t cells), no nucleoli. Coarsely granulated chromatin. Cytoplasm is abundant, transparent. 158-LSIL: 10x magnification of low grade squamous intra-epithelial lesion/mild dysplasia/cin I. Intermediate squamous cells with enlargement of the nuclei. Hyperchromasia, elevated N/C ratio (3 to 4 times the normal intermediate cells), no nucleoli. li Coarsely granulated chromatin. Cytoplasm is abundant, transparent.





25 SQUAMOUS CELL ABNORMALITIES 159-LSIL: 40x magnification of low grade squamous intra-epithelial lesion/mild dysplasia/cin I. Intermediate t squamous cells with enlargement of the nuclei. Hyperchromasia, elevated N/C ratio (3 to 4 times the normal intermediate cells), no nucleoli. Coarsely granulated chromatin. Cytoplasm is abundant, transparent. 160-LSIL: 10x magnification of low grade squamous intra-epithelial lesion/mild dysplasia/cin I. Intermediate squamous cells with enlargement of the nuclei. Hyperchromasia, elevated N/C ratio (3 to 4 times the normal intermediate cells), no nucleoli. li Coarsely granulated chromatin. Cytoplasm is abundant, transparent.


, no nucleoli.")

 ), no nucleoli.")
26 SQUAMOUS CELL ABNORMALITIES 161-LSIL: 40x magnification of low grade squamous intra-epithelial lesion/mild dysplasia/cin I. Intermediate squamous cells with enlargement of the nuclei. Hyperchromasia, elevated N/C ratio (3 to 4 times the normal intermediate cells), no nucleoli. Coarsely granulated chromatin. Cytoplasm is abundant, transparent. 162-LSIL: 40x magnification of low grade squamous intra-epithelial lesion/mild dysplasia/cin I. Intermediate squamous cells with enlargement of the nuclei. Hyperchromasia, elevated N/C ratio (3 to 4 times the normal intermediate cells) ), no nucleoli. Coarsely granulated chromatin. Cytoplasm is abundant, transparent. Cytoplasm is abundant, transparent.
27 SQUAMOUS CELL ABNORMALITIES 163-LSIL: 40x magnification of low grade squamous intra-epithelial lesion/mild dysplasia/cin I. Intermediate squamous cells with enlargement of the nuclei. Hyperchromasia, elevated N/C ratio (3 to 4 times the normal intermediate cells), no nucleoli. Coarsely granulated chromatin. Cytoplasm is abundant, transparent.





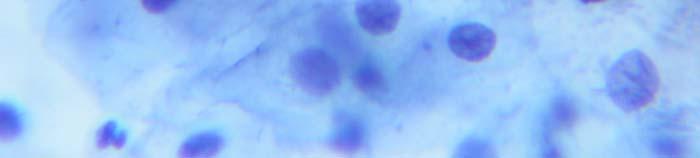
28 SQUAMOUS CELL ABNORMALITIES 166-HSIL: 40x magnification of cells in loosely cohesive groups, parabasal, metaplastic or basal type. The cells are round, oval (size of parabasal cells), the cell borders are rigid. The nuclei are enlarged and hyperchromatic, high N/C ratio. The chromatin is fine to coarsely clumped. The nuclear membranes are irregular. Nucleoli are absent. The cytoplasm is variable, scant to moderate. 167-HSIL : 40x magnification of cells in loosely cohesive groups, parabasal, metaplastic or basal type. The cells are round, oval (size of parabasal cells), the cell borders are rigid. The nuclei are enlarged and hyperchromatic, high N/C ratio. The chromatin is fine to coarsely clumped. The nuclear membranes are irregular. Nucleoli are absent. The cytoplasm is variable, scant to moderate.




29 SQUAMOUS CELL ABNORMALITIES 169-HSIL: 40x magnification cells in loosely cohesive groups, parabasal, metaplastic or basal type. The cells are round, oval (size of parabasal cells), the cell borders are rigid. The nuclei are enlarged and hyperchromatic, high N/C ratio. The chromatin is fine to coarsely clumped. The nuclear membranes are irregular. Nucleoli are absent. The cytoplasm is variable, scant to moderate. 171-HSIL: 40x magnification of cells in loosely cohesive groups, parabasal, metaplastic or basal type. The cells are round, oval (size of parabasal cells), the cell borders are rigid. The nuclei are enlarged and hyperchromatic, high N/C ratio. The chromatin is fine to coarsely clumped. The nuclear membranes are irregular. Nucleoli are absent. The cytoplasm is variable, scant to moderate.




30 SQUAMOUS CELL ABNORMALITIES 173-HSIL : 40x magnification of cells in loosely cohesive groups, parabasal, metaplastic or basal type. The cells are round, oval (size of parabasal cells), the cell borders are rigid. The nuclei are enlarged and hyperchromatic, high N/C ratio. The chromatin is fine to coarsely clumped. The nuclear membranes are irregular. Nucleoli are absent. The cytoplasm is variable, scant to moderate. 176-HSIL: 40x magnification of cells in loosely cohesive groups, parabasal, metaplastic or basal type. The cells are round, oval (size of parabasal cells), the cell borders are rigid. The nuclei are enlarged and hyperchromatic, high N/C ratio. The chromatin is fine to coarsely clumped. The nuclear membranes are irregular. Nucleoli are absent. The cytoplasm is variable, scant to moderate.






31 SQUAMOUS CELL ABNORMALITIES 180-HSIL: 40x magnification of cells in loosely cohesive groups, parabasal, metaplastic or basal type. The cells are round, oval (size of parabasal cells), the cell borders are rigid. The nuclei are enlarged and hyperchromatic, high N/C ratio. The chromatin is fine to coarsely clumped. The nuclear membranes are irregular. Nucleoli are absent. The cytoplasm is variable, scant to moderate. 181-HSIL: 40x magnification cells in loosely cohesive groups, parabasal, metaplastic or basal type. The cells are round, oval (size of parabasal cells), the cell borders are rigid. The nuclei are enlarged and hyperchromatic, high N/C ratio. The chromatin is fine to coarsely clumped. The nuclear membranes are irregular. Nucleoli are absent. The cytoplasm is variable, scant to moderate.






32 SQUAMOUS CELL ABNORMALITIES 182-HSIL: 40x magnification of cells in loosely cohesive groups, parabasal, metaplastic or basal type. The cells are round, oval (size of parabasal cells), the cell borders are rigid. The nuclei are enlarged and hyperchromatic, high N/C ratio. The chromatin is fine to coarsely clumped. The nuclear membranes are irregular. Nucleoli are absent. The cytoplasm is variable, scant to moderate. 186-HSIL: 40x magnification cells in loosely cohesive groups, parabasal, metaplastic or basal type. The cells are round, oval (size of parabasal cells), the cell borders are rigid. The nuclei are enlarged and hyperchromatic, high N/C ratio. The chromatin is fine to coarsely clumped. The nuclear membranes are irregular. Nucleoli are absent. The cytoplasm is variable, scant to moderate.
, the cell borders are rigid.")


33 SQUAMOUS CELL ABNORMALITIES 188-HSIL: 40x magnification cells in loosely cohesive groups, parabasal, metaplastic or basal type. The cells are round, oval (size of parabasal cells), the cell borders are rigid. The nuclei are enlarged and hyperchromatic, high N/C ratio. The chromatin is fine to coarsely clumped. The nuclear membranes are irregular. Nucleoli are absent. The cytoplasm is variable, scant to moderate. 189-HSIL: 40x magnification of cells in loosely cohesive groups, parabasal, metaplastic or basal type. The cells are round, oval (size of parabasal cells), the cell borders are rigid. The nuclei are enlarged and hyperchromatic, high N/C ratio. The chromatin is fine to coarsely clumped. The nuclear membranes are irregular. Nucleoli are absent. The cytoplasm is variable, scant to moderate.

, caudate and tadpole.")


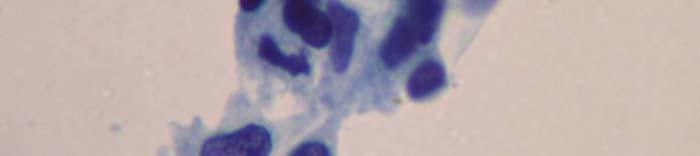
34 SQUAMOUS CELL ABNORMALITIES 193-Squamous Cell Carcinoma poorly 195-Squamous Cell Carcinoma: differentiated: 40x magnification of cells isolated, in loosely 40x magnification of malignant cells in loosely cohesive groups and syncytial arrangement. cohesive groups, mostly round, polygonal, Marked pleomorphism with variation in size and size variable. shape (small, round, oval, oblong to elongated The borders are not well defined. (spindle), caudate and tadpole. The nuclei are large, hyper-chromatic. Cells wrapping around adjacent cells are present. The nuclear membranes are smooth to The nuclear are enlarged and hyperchromatic. irregular, the chromatin is coarsely granular The nuclear membranes are smooth to irregular. The having irregular chromocenters. chromatin is dark stained. Micronucleoili are Micronucleoli are seen. present. The cytoplasm is scant. No Keratinization is The cell borders are rigid and not well defined. The present. cytoplasm is variable (scant to abundant). The N/C ratio is high.

, caudate and tadpole (1). Cells wrapping around adjacent cells are present.")

 198-Squamous Cell Carcinoma: 40x magnification of")


35 SQUAMOUS CELL ABNORMALITIES Squamous Cell Carcinoma: 40x magnification of cells isolated, in loosely cohesive groups and syncytial arrangement. Marked pleomorphism with variation in size and shape (small, round, oval, oblong to elongated (spindle), caudate and tadpole (1). Cells wrapping around adjacent cells are present. The nuclear are enlarged and hyperchromatic. The nuclear membranes are smooth to irregular. The chromatin is dark stained. Micronucleoili are present. The cell borders are rigid and not well defined. The cytoplasm is variable (scant to abundant) 198-Squamous Cell Carcinoma: 40x magnification of cells isolated, in loosely cohesive groups and syncytial arrangement. Marked pleomorphism with variation in size and shape (small, round, oval, oblong to elongated (spindle) (1), caudate and tadpole. Keratinized squamous pearls and cells wrapping around adjacent cells are present. The nuclear are enlarged and hyperchromatic. The nuclear membranes are smooth to irregular. The chromatin is dark stained. Micronucleoili are present. The cell borders are rigid and not well defined. The cytoplasm is variable (scant to abundant)

, caudate and tadpole.")




36 SQUAMOUS CELL ABNORMALITIES 200-Squamous Cell Carcinoma: 40x magnification of cells isolated, in loosely cohesive groups and syncytial arrangement. Marked pleomorphism with variation in size and shape (small, round, oval, oblong to elongated (spindle), caudate and tadpole. Keratinized squamous pearls and cells wrapping around adjacent cells are present. The nuclear are enlarged and hyperchromatic. The nuclear membranes are smooth to irregular. The chromatin is dark stained. Micronucleoili are present. The cell borders are rigid and not well defined. The cytoplasm is variable (scant to abundant) 201-Squamous Cell Carcinoma: 40x magnification cells isolated, in loosely cohesive groups and syncytial arrangement. Marked pleomorphism with variation in size and shape (small, round, oval, oblong to elongated (spindle), caudate and tadpole. Cells wrapping around adjacent cells are present. The nuclear are enlarged and hyperchromatic. The nuclear membranes are smooth to irregular. The chromatin is dark stained. Micronucleoili are present. The cell borders are rigid and not well defined. The cytoplasm is variable (scant to abundant)

, caudate and tadpole. Cells wrapping around adjacent cells are present.")

37 SQUAMOUS CELL ABNORMALITIES 202-Squamous Cell Carcinoma: 40x magnification cells isolated, in loosely cohesive groups and syncytial arrangement. Marked pleomorphism with variation in size and shape (small, round, oval, oblong to elongated (spindle), caudate and tadpole. Cells wrapping around adjacent cells are present. The nuclear are enlarged and hyperchromatic. The nuclear membranes are smooth to irregular. The chromatin is dark stained. Micronucleoili are present. The cell borders are rigid and not well defined. The cytoplasm is variable (scant to abundant)






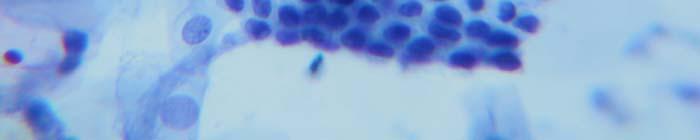
38 GLANDULAR ABNORMALITIES 204-Endocervical adenocarcinoma (morules): 205-Endocervical adenocarcinoma: 40x magnification of cells in tissue fragments, 40x magnification of cells in tissue fragments, loosely cohesive groups and syncythial loosely cohesive groups and syncythial arrangement with acinar pattern, branching, arrangement with acinar pattern, branching, glandular like (nuclei around the opening with glandular like (nuclei around the opening with vertical polarity, nuclei at the periphery vertical polarity, nuclei at the periphery stringing out with a feathering pattern and stringing out with a feathering pattern and palisading of nuclei palisading of nuclei The nuclei are round, oval, central and The nuclei are round, oval, central and paracentric, variable size, hyperchromatic, the paracentric, variable size, hyperchromatic, the chromatin is coarsely granular. chromatin is coarsely granular. Loss of nuclear polarity. Micronucleoli are present. The cytoplasm is variable and micro- vacuolization is seen. Loss of nuclear polarity. Micronucleoli are present. The cytoplasm is variable and micro- vacuolization is seen.



: 40x magnification of cells periphery stringing")


39 GLANDULAR ABNORMALITIES 206-Endocervical adenocarcinoma (Morules): 40x magnification of cells in tissue fragments, loosely cohesive groups and syncythial arrangement with acinar pattern, branching, glandular like (nuclei around the opening with vertical polarity, nuclei at the periphery stringing g out with a feathering pattern and palisading of nuclei The nuclei are round, oval, central and paracentric, variable size, hyperchromatic, the chromatin is coarsely granular. Loss of nuclear polarity. Micronucleoli o are present. The cytoplasm is variable and micro- vacuolization is seen. 209-Endocervical adenocarcinoma (Syncytial): 40x magnification of cells in tissue fragments, loosely cohesive groups and syncythial arrangement with acinar pattern, branching, glandular like (nuclei around the opening with vertical polarity, nuclei at the periphery stringing out with a feathering pattern and palisading of nuclei The nuclei are round, oval, central and paracentric, variable size, hyperchromatic, the chromatin is coarsely granular. Loss of nuclear polarity. Micronucleoli are present. The cytoplasm is variable and micro-vacuolization is seen.




40 GLANDULAR ABNORMALITIES 208-Endocervical adenocarcinoma (Morules): 209-Endocervical adenocarcinoma (Syncytial): 40x magnification of cells in tissue fragments, loosely cohesive groups and 40x magnification of cells in tissue fragments, syncythial arrangement with acinar pattern, loosely cohesive groups and syncythial arrangement branching, glandular like (nuclei around the with acinar pattern, branching, glandular like (nuclei opening with vertical polarity, nuclei at the around the opening with vertical polarity, nuclei at periphery p stringing g out with a feathering pattern and palisading of nuclei the periphery stringing out with a feathering pattern The nuclei are round, oval, central and and palisading of nuclei paracentric, variable size, hyperchromatic, The nuclei are round, oval, central and paracentric, the chromatin is coarsely granular. variable size, hyperchromatic, the chromatin is Loss of nuclear polarity. coarsely granular. Micronucleoli o are present. Loss of nuclear polarity. The cytoplasm is variable and micro- vacuolization is seen. Micronucleoli are present. The cytoplasm is variable and micro-vacuolization is seen.
: groups): 40x magnification of cells in tissue fragments,")





41 GLANDULAR ABNORMALITIES 210-Endocervical adenocarcinoma (Glandular 211-Endocervical adenocarcinoma (Loosely cohesive like): groups): 40x magnification of cells in tissue fragments, loosely cohesive groups and 40x magnification of cells in tissue fragments, loosely syncythial arrangement with acinar cohesive groups and syncythial arrangement with pattern, branching, glandular like (nuclei acinar pattern, branching, glandular like (nuclei around the opening with vertical polarity, nuclei at the periphery stringing out with a around the opening with vertical polarity, nuclei at feathering pattern and palisading of nuclei the periphery stringing out with a feathering pattern The nuclei are round, oval, central and and palisading of nuclei paracentric, variable size, hyperchromatic, The nuclei are round, oval, central and paracentric, the chromatin is coarsely granular. variable size, hyperchromatic, the chromatin is Loss of nuclear polarity. coarsely granular. Micronucleoli are present. The cytoplasm is variable and micro- Loss of nuclear polarity. vacuolization is seen. Micronucleoli are present. The cytoplasm is variable and micro-vacuolization is seen.
: groups): 40x magnification of cells in tissue fragments,")





42 GLANDULAR ABNORMALITIES 212-Endocervical adenocarcinoma (loosely 213-Endocervical adenocarcinoma (loosely l cohesive cohesive groups): groups): 40x magnification of cells in tissue fragments, loosely cohesive groups and 40x magnification of cells in tissue fragments, loosely syncythial arrangement with acinar pattern, cohesive groups and syncythial arrangement with branching, glandular like (nuclei around the acinar pattern, branching, glandular like (nuclei opening with vertical polarity, nuclei at the periphery stringing out with a feathering around the opening with vertical polarity, nuclei at the pattern and palisading of nuclei periphery stringing out with a feathering pattern and The nuclei are round, oval, central and palisading of nuclei paracentric, variable size, hyperchromatic, The nuclei are round, oval, central and paracentric, the chromatin is coarsely granular. variable size, hyperchromatic, the chromatin is Loss of nuclear polarity. coarsely granular. Micronucleoli are present. The cytoplasm is variable and micro- Loss of nuclear polarity. vacuolization is seen. Micronucleoli are present. The cytoplasm is variable and micro-vacuolization is seen.



43 GLANDULAR ABNORMALITIES 214-Endocervical adenocarcinoma (palisading): 40x magnification of cells in tissue fragments, loosely cohesive groups and syncythial arrangement with acinar pattern, branching, glandular like (nuclei around the opening with vertical polarity, nuclei at the periphery stringing out with a feathering pattern and palisading of nuclei The nuclei are round, oval, central and paracentric, variable size, hyperchromatic, the chromatin is coarsely granular. Loss of nuclear polarity. Micronucleoli are present. The cytoplasm is variable and micro- vacuolization is seen.
44 NON GYN CYTOLOGY 215-Thyroid: (40x magnification) 216-Thyroid: (40x magnification) Atypical cells grouped with irregular contours. Isolated follicular cells. Nuclear inclusions and grooves Finely granular chromatin and squamoid cytoplasm. Nuclear enlargement, hyperchromatic (suggestive of papillary carcinoma)
45 NON GYN CYTOLOGY 219-Urine smear: (40x magnification) Consistent with bladder urotellium Transitional epithelial cells in cohesive group. The cells are large and elliptical with abundant eosinophilic cytoplasm Well defined borders. 221-Thyroid: (40x magnification) Atypical cells grouped with irregular contours. Nuclear inclusions and grooves Finely granular chromatin and squamoid cytoplasm. Nuclear enlargement, hyperchromatic (suggestive of papillary carcinoma)
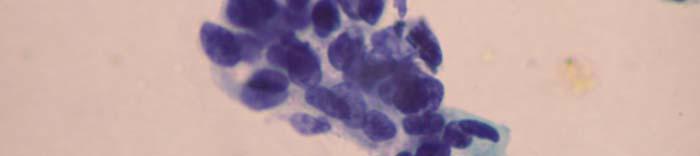
46 NON GYN CYTOLOGY 223-Pleural Fluids: (40x magnification) Many small round cells with hyperchromatic nuclei and very scant cytoplasm (consistent with lymphocytes.)
CINtec p16 INK4a Staining Atlas
 CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Morphology I Slide: 1
 Morphology I Slide: 1 Morphology I Slide: 2 ThinPrep Morphology Normal Cytology Morphology I Slide: 3 CT & Pathologist Training Training program begins with ThinPrep morphology presentation Microscopic
Morphology I Slide: 1 Morphology I Slide: 2 ThinPrep Morphology Normal Cytology Morphology I Slide: 3 CT & Pathologist Training Training program begins with ThinPrep morphology presentation Microscopic
SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H)
 - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H)") SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H) ASC refers to cytologic changes suggestive of SIL, which are qualitativley or quantitatively
SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H) ASC refers to cytologic changes suggestive of SIL, which are qualitativley or quantitatively
Cytoplasmic changes Nuclear changes
 The presence of infection in the female genital tract may procure certain cellular changes in the epithelium. Such changes are seen in nucleus and cytoplasm surrounding the nucleus. Cytoplasmic changes
The presence of infection in the female genital tract may procure certain cellular changes in the epithelium. Such changes are seen in nucleus and cytoplasm surrounding the nucleus. Cytoplasmic changes
PRESENTATION PLAN. Aim: Bethesda System 2001
 REACTIVE CELLULAR CHANGES AND INFECTIONS OF FEMALE GENITAL TRACT Aysun Uğuz, Prof, MD, FIAC Çukurova Üniv. Tıp Fak. Pathology Department-Cytology Division 18.Nisan.2015 Aim: The aim of the presentation
REACTIVE CELLULAR CHANGES AND INFECTIONS OF FEMALE GENITAL TRACT Aysun Uğuz, Prof, MD, FIAC Çukurova Üniv. Tıp Fak. Pathology Department-Cytology Division 18.Nisan.2015 Aim: The aim of the presentation
Workshop for O& G trainees and paramedics 17 Dec 2011 Cytological Interpretation
 Workshop for O& G trainees and paramedics 17 Dec 2011 Cytological Interpretation May Yu Director of Cytology Laboratory Service Department of Anatomical & Cellular Pathology Prince of Wales Hospital Cervical
Workshop for O& G trainees and paramedics 17 Dec 2011 Cytological Interpretation May Yu Director of Cytology Laboratory Service Department of Anatomical & Cellular Pathology Prince of Wales Hospital Cervical
Maturation Index 3/29/2017. Disclosure of Relevant Financial Relationships. Gynecologic Cytology. Normal Maturation of Squamous Epithelium : :
 Gynecologic Cytology Fadi W. Abdul Karim, MD MEd Department of Anatomic Pathology Vice Chair Education RT PLMI Professor of Pathology Cleveland Clinic. Cleveland Ohio Disclosure of Relevant Financial Relationships
Gynecologic Cytology Fadi W. Abdul Karim, MD MEd Department of Anatomic Pathology Vice Chair Education RT PLMI Professor of Pathology Cleveland Clinic. Cleveland Ohio Disclosure of Relevant Financial Relationships
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo. Case Discussions. 60 year old woman Routine gynecologic control LBC
 BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000
 Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Cytology Report Format
 Squamous Precursor Lesions and Malignancies In Pap Test Dina R. Mody, MD, FCAP Director of Cytology The Methodist Hospital, Houston, TX Professor of Pathology and Laboratory Medicine Weill Medical College
Squamous Precursor Lesions and Malignancies In Pap Test Dina R. Mody, MD, FCAP Director of Cytology The Methodist Hospital, Houston, TX Professor of Pathology and Laboratory Medicine Weill Medical College
Case 3 - GYN. History: 66 year old, routine Pap test. Dr. Stelow
 Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Cytyc Corporation - Case Presentation Archive - July 2002
 ThinPrep Pap Test History: 34 Year Old Female LMP: Day 20 Specimen Type: Cervical/Vaginal Case provided by Mark Tulecke, M.D. and Gabrielle Trawinski CT (ASCP), Mount Auburn Hospital, Cambridge, Massachusetts.
ThinPrep Pap Test History: 34 Year Old Female LMP: Day 20 Specimen Type: Cervical/Vaginal Case provided by Mark Tulecke, M.D. and Gabrielle Trawinski CT (ASCP), Mount Auburn Hospital, Cambridge, Massachusetts.
Histopathology: Cervical HPV and neoplasia
 Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
Morphologic Clues and Pitfalls for High Grade Lesions in Cervical Cytology
 Morphologic Clues and Pitfalls for High Grade Lesions in Cervical Cytology Ritu Nayar, MD Northwestern University, Feinberg School of Medicine Chicago, IL, USA Disclosures Editor, Cervical Cytology Bethesda
Morphologic Clues and Pitfalls for High Grade Lesions in Cervical Cytology Ritu Nayar, MD Northwestern University, Feinberg School of Medicine Chicago, IL, USA Disclosures Editor, Cervical Cytology Bethesda
Thyroid follicular neoplasms in cytology. Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia
 Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology
 New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
Cervical Cytology Preparations
 GYN Cytology Cervical Cytology Preparations CS TP SP Fadi W. Abdul-Karim, MD MSMedu Department of Anatomic Pathology Vice Chair Education Professor of Pathology Cleveland Clinic Cleveland Ohio Conventional
GYN Cytology Cervical Cytology Preparations CS TP SP Fadi W. Abdul-Karim, MD MSMedu Department of Anatomic Pathology Vice Chair Education Professor of Pathology Cleveland Clinic Cleveland Ohio Conventional
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
EDUCATIONAL COMMENTARY MORPHOLOGIC ABNORMALITIES IN LEUKOCYTES
 EDUCATIONAL COMMENTARY MORPHOLOGIC ABNORMALITIES IN LEUKOCYTES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY MORPHOLOGIC ABNORMALITIES IN LEUKOCYTES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
number Done by Corrected by Doctor Maha Shomaf
 number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience
 Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
PAP SMEAR by Dr.Shantha Krishnamurthy MD Senior Consultant Pathology Fortis Hospitals
 PAP SMEAR by Dr.Shantha Krishnamurthy MD Senior Consultant Pathology Fortis Hospitals Historical Named after George Papanicolaou, a Greek American Studied cervical epithelium in menstrual cycle of guinea
PAP SMEAR by Dr.Shantha Krishnamurthy MD Senior Consultant Pathology Fortis Hospitals Historical Named after George Papanicolaou, a Greek American Studied cervical epithelium in menstrual cycle of guinea
QUALITY ASSURANCE PROGRAM CYTOLOGY CYCLE 01/2018 (TRIAL)
") [Pick the Date] FINAL REPORT QUALITY ASSURANCE PROGRAM CYTOLOGY CYCLE 01/2018 (TRIAL) NOTES FROM THE COORDINATOR 1. For this cycle 01/2018, a total of 32 pen drives had been circulated. Twenty-eight institutions
[Pick the Date] FINAL REPORT QUALITY ASSURANCE PROGRAM CYTOLOGY CYCLE 01/2018 (TRIAL) NOTES FROM THE COORDINATOR 1. For this cycle 01/2018, a total of 32 pen drives had been circulated. Twenty-eight institutions
Almost any suspected tumor can be aspirated easily and safely. Some masses are more risky to aspirate including:
 DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
A cyto-histopathological correlation study of lesions of uterine cervix
 Original Research Article Mandakini B. Tengli 1,*, Mohammed Mateen Ahmed 2 1 Associate Professor, 2 Assistant Professor, Dept. of Pathology, KBNIMS, Gulbarga *Corresponding Author: Email: mandakinibt@gmail.com
Original Research Article Mandakini B. Tengli 1,*, Mohammed Mateen Ahmed 2 1 Associate Professor, 2 Assistant Professor, Dept. of Pathology, KBNIMS, Gulbarga *Corresponding Author: Email: mandakinibt@gmail.com
Cervical Cancer : Pap smear
 Taking a PAP SMEAR Cervical Cancer : Pap smear George N Papanicolaou introduced cervical cytology in clinical practice in 1940 In 1945, PAP smear was endorsed by American cancer society as an effective
Taking a PAP SMEAR Cervical Cancer : Pap smear George N Papanicolaou introduced cervical cytology in clinical practice in 1940 In 1945, PAP smear was endorsed by American cancer society as an effective
Cytyc Corporation - Case Presentation Archive - October 2001
 ThinPrep Pap Test History: 82 Year Old Female Specimen Type: Peritoneal Washings Case provided by Dr. Berle Stratton, Southwest Washington Medical Center, Vancouver, Washington. *The images, analysis and
ThinPrep Pap Test History: 82 Year Old Female Specimen Type: Peritoneal Washings Case provided by Dr. Berle Stratton, Southwest Washington Medical Center, Vancouver, Washington. *The images, analysis and
A Study on Diagnostic Accuracy of Cervical Pap Smear by Correlating with Histopathology in a Tertiary Care Centre
 Original Article DOI: 10.21276/APALM.1878 A Study on Diagnostic Accuracy of Cervical Pap Smear by Correlating with Histopathology in a Tertiary Care Centre Rachana L Y, S.S. Hiremath*, Prabhu M H, S.S
Original Article DOI: 10.21276/APALM.1878 A Study on Diagnostic Accuracy of Cervical Pap Smear by Correlating with Histopathology in a Tertiary Care Centre Rachana L Y, S.S. Hiremath*, Prabhu M H, S.S
Case 1. Slide 1 History: 65 year old male presents with bilateral pleural effusions, a 40 pack year smoking history and peripheral and hilar lung
 Case 1. Slide 1 History: 65 year old male presents with bilateral pleural effusions, a 40 pack year smoking history and peripheral and hilar lung masses. Specimen shown is from a tap of the pleural effusion.
Case 1. Slide 1 History: 65 year old male presents with bilateral pleural effusions, a 40 pack year smoking history and peripheral and hilar lung masses. Specimen shown is from a tap of the pleural effusion.
Normal Morphology. Anatomic Considerations. Normal Urothelial Histology and Cytology
 1 Normal Morphology Anatomic Considerations The urinary tract can be divided into three regions: the kidney; the calyces, pelves and ureters (upper collecting system or upper tract); and the bladder and
1 Normal Morphology Anatomic Considerations The urinary tract can be divided into three regions: the kidney; the calyces, pelves and ureters (upper collecting system or upper tract); and the bladder and
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Proceeding of the SEVC Southern European Veterinary Conference
 www.ivis.org Proceeding of the SEVC Southern European Veterinary Conference Oct. 17-19, 2008 Barcelona, Spain http://www.sevc.info Reprinted in the IVIS website with the permission of the SEVC www.ivis.org
www.ivis.org Proceeding of the SEVC Southern European Veterinary Conference Oct. 17-19, 2008 Barcelona, Spain http://www.sevc.info Reprinted in the IVIS website with the permission of the SEVC www.ivis.org
Comparison of Cytologic Characteristics between Adenoid Cystic Carcinoma and Adenoid Basal Carcinoma in the Uterine Cervix
 Journal of Pathology and Translational Medicine 2015; 49: 396-402 ORIGINAL ARTICLE Comparison of Cytologic Characteristics between Adenoid Cystic Carcinoma and Adenoid Basal Carcinoma in the Uterine Cervix
Journal of Pathology and Translational Medicine 2015; 49: 396-402 ORIGINAL ARTICLE Comparison of Cytologic Characteristics between Adenoid Cystic Carcinoma and Adenoid Basal Carcinoma in the Uterine Cervix
Introduction. 23 rd Annual Seminar in Pathology. FLUIDS, Part 1. Pittsburgh, PA Gladwyn Leiman UVMMC, VT
 23 rd Annual Seminar in Pathology Pittsburgh, PA Gladwyn Leiman UVMMC, VT FLUIDS, Part 1 "Blue walls", Claudia Hansen, 2009 Introduction o Challenging to everyone o Almost any benign or malignant process
23 rd Annual Seminar in Pathology Pittsburgh, PA Gladwyn Leiman UVMMC, VT FLUIDS, Part 1 "Blue walls", Claudia Hansen, 2009 Introduction o Challenging to everyone o Almost any benign or malignant process
Conflict of Interest 9/7/2018. Dr. Mody 1. None with vendors of cytology equipment/testing/vaccines Amirsys (now Elsevier)
") Glandular Lesions in Cervicovaginal Cytology: Patterns, Pitfalls and Bethesda Updates Dina R Mody, MD Director of Cytology Laboratories Houston s Methodist Hospital and Bioreference Laboratory The Ibrahim
Glandular Lesions in Cervicovaginal Cytology: Patterns, Pitfalls and Bethesda Updates Dina R Mody, MD Director of Cytology Laboratories Houston s Methodist Hospital and Bioreference Laboratory The Ibrahim
GYN (Glandulars) Still Difficult After All These Years! Dina R Mody, MD Director of Cytology Laboratories and fellowship Program Methodist Hospital
 Still Difficult After All These Years! Dina R Mody, MD Director of Cytology Laboratories and fellowship Program Methodist Hospital") GYN (Glandulars) Still Difficult After All These Years! Dina R Mody, MD Director of Cytology Laboratories and fellowship Program Methodist Hospital and Bioreference Labs (Houston) Department of Pathology
GYN (Glandulars) Still Difficult After All These Years! Dina R Mody, MD Director of Cytology Laboratories and fellowship Program Methodist Hospital and Bioreference Labs (Houston) Department of Pathology
Diagnostic Cytology of Cancer Cases
 Diagnostic Cytology of Cancer Cases Somporn Techangamsuwan Companion Animal Cancer Research Unit (CAC-RU) Department of Pathology, Faculty of Veterinary Science, Chulalongkorn University 1 Tumor or Non-tumor
Diagnostic Cytology of Cancer Cases Somporn Techangamsuwan Companion Animal Cancer Research Unit (CAC-RU) Department of Pathology, Faculty of Veterinary Science, Chulalongkorn University 1 Tumor or Non-tumor
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Introduction 10/27/2011. Follicular Lesion/Atypia of Undetermined Significance
 Follicular Lesion/Atypia of Undetermined Significance Tarik M. Elsheikh, MD Cleveland Clinic Cleveland, Ohio Diagnostic Categories Proposed by Bethesda System/NCI Thyroid Conference 1. Benign 2. Follicular
Follicular Lesion/Atypia of Undetermined Significance Tarik M. Elsheikh, MD Cleveland Clinic Cleveland, Ohio Diagnostic Categories Proposed by Bethesda System/NCI Thyroid Conference 1. Benign 2. Follicular
Clinical Practice Guidelines June 2013
 Clinical Practice Guidelines June 2013 General Principles: The Papanicolaou (Pap) smear is widely credited with reducing mortality from cervical cancer, and remains the single best method for the early
Clinical Practice Guidelines June 2013 General Principles: The Papanicolaou (Pap) smear is widely credited with reducing mortality from cervical cancer, and remains the single best method for the early
The ABCs of TBS. A Novice's Guide to the Bethesda System
 CE U P D A T E W O M E N ' S HEALTH III Julia Woodruff Wildes, MD The ABCs of TBS A Novice's Guide to the Bethesda System This is the third and final article in a three-part series on women's health. The
CE U P D A T E W O M E N ' S HEALTH III Julia Woodruff Wildes, MD The ABCs of TBS A Novice's Guide to the Bethesda System This is the third and final article in a three-part series on women's health. The
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Pathological Classification of Hepatocellular Carcinoma
 3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH
 FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
EDUCATIONAL COMMENTARY BLOOD CELL IDENTIFICATION
 EDUCATIONAL COMMENTARY BLOOD CELL IDENTIFICATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
EDUCATIONAL COMMENTARY BLOOD CELL IDENTIFICATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
Thyroid master class. Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson
 Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Table of Contents. 1. Overview. 2. Interpretation Guide. 3. Staining Gallery Cases Negative for CINtec PLUS
 Staining Atlas Table of Contents 1. Overview 1.1 Introduction 1.2 Role of p16 INK4a 1.3 Role of Ki-67 1.4 Molecular Pathogenesis 1.5 p16 INK4a Expression in Cervical Dysplasia 1.6 The Concept of CINtec
Staining Atlas Table of Contents 1. Overview 1.1 Introduction 1.2 Role of p16 INK4a 1.3 Role of Ki-67 1.4 Molecular Pathogenesis 1.5 p16 INK4a Expression in Cervical Dysplasia 1.6 The Concept of CINtec
EDUCATIONAL COMMENTARY DISTINGUISHING MORPHOLOGIC LOOK-ALIKES
 EDUCATIONAL COMMENTARY DISTINGUISHING MORPHOLOGIC LOOK-ALIKES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY DISTINGUISHING MORPHOLOGIC LOOK-ALIKES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Mody. Atypical Glandular Cells(TBS 2001) Adenocarcinoma In Situ(TBS 2001)
 Adenocarcinoma In Situ(TBS 2001)") Glandular Lesions in Cervicovaginal Cytology Dina R. Mody, MD, FCAP Director of Cytology The Methodist Hospital, Houston, TX Professor of Pathology and Laboratory Medicine Weill Medical College of Cornell
Glandular Lesions in Cervicovaginal Cytology Dina R. Mody, MD, FCAP Director of Cytology The Methodist Hospital, Houston, TX Professor of Pathology and Laboratory Medicine Weill Medical College of Cornell
EDUCATIONAL COMMENTARY DIFFERENTIATING IMMATURE PERIPHERAL BLOOD CELLS
 Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Continuing Education on the left side of the
Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Continuing Education on the left side of the
Microscopic Sediment Epithelial Cells
 Epithelial Cells Cells sloughed from the kidney, urethra, bladder and genital track. Unless increased in number or abnormal forms, they are normal part of sediment. Three major types classified according
Epithelial Cells Cells sloughed from the kidney, urethra, bladder and genital track. Unless increased in number or abnormal forms, they are normal part of sediment. Three major types classified according
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS
 Shamlal Mangray, MB, BS") Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
EU guidelines for reporting gynaecological cytology
 EU guidelines for reporting gynaecological cytology Amanda Herbert Guy s & St Thomas Foundation NHS Trust 5th EFCS Annual Tutorial, Trondheim, Norway 28 th May 1 st June 2012 EU guidelines aim to harmonize
EU guidelines for reporting gynaecological cytology Amanda Herbert Guy s & St Thomas Foundation NHS Trust 5th EFCS Annual Tutorial, Trondheim, Norway 28 th May 1 st June 2012 EU guidelines aim to harmonize
Pathology Slides. [Pathology]
![Pathology Slides. [Pathology]](/thumbs/94/120604575.jpg "Pathology Slides. [Pathology]") Pathology Slides MedicoNotes provides real laboratory pathological slides to aid you to differentiate between different pathological structures under microscope. www.mediconotes.com Histology slides example
Pathology Slides MedicoNotes provides real laboratory pathological slides to aid you to differentiate between different pathological structures under microscope. www.mediconotes.com Histology slides example
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Participants Identification No. % Evaluation. Mitotic figure Educational Erythrocyte precursor, abnormal 1 0.
 Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES COPYRIGHTED MATERIAL SECOND EDITION
 VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES SECOND EDITION COPYRIGHTED MATERIAL CHAPTER ONE HEMATOPOIESIS GENERAL FEATURES All blood cells have a finite life span, but in normal
VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES SECOND EDITION COPYRIGHTED MATERIAL CHAPTER ONE HEMATOPOIESIS GENERAL FEATURES All blood cells have a finite life span, but in normal
ACGME Competency / Milestone Assessment. The Pap Test. Ricardo R. Lastra, MD Zubair W. Baloch, MD, PhD
 1 ACGME Competency / Milestone Assessment The Pap Test Ricardo R. Lastra, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman School of Medicine
1 ACGME Competency / Milestone Assessment The Pap Test Ricardo R. Lastra, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman School of Medicine
Differentiation of Renal Tubular Epithelium in Renal Transplantation Cytology
 Differentiation of Renal Tubular Epithelium in Renal Transplantation Cytology G. BERRY SCHUMANN, M.D., LAWRENCE J. PALMIERI, B.S., C.T.(ASCP), AND DAVID B. JONES, M.D. Schumann, G. Berry, Palmieri, Lawrence
Differentiation of Renal Tubular Epithelium in Renal Transplantation Cytology G. BERRY SCHUMANN, M.D., LAWRENCE J. PALMIERI, B.S., C.T.(ASCP), AND DAVID B. JONES, M.D. Schumann, G. Berry, Palmieri, Lawrence
Submission of samples. Cytology of Lumps and Bumps. Evaluation of samples. Use caution interpreting. Criteria of malignancy.
 Submission of samples Cytology of Lumps and Bumps Paul Avery VMD, PhD, DACVP paul.avery@colostate.edu Air dry only No wet fixation using formalin or ethanol Stain 1-2 on-site to evaluate quality Send all
Submission of samples Cytology of Lumps and Bumps Paul Avery VMD, PhD, DACVP paul.avery@colostate.edu Air dry only No wet fixation using formalin or ethanol Stain 1-2 on-site to evaluate quality Send all
Gastrooesophageal reflux disease. Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia
 Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
6/5/2010. Outline of Talk. Endometrial Alterations That Mimic Cancer & Vice Versa: Metaplastic / reactive changes. Problems in Biopsies/Curettages
 Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Demystifying Endometrial Hyperplasia
 Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
Medullary Thyroid Carcinoma. This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands
 Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
CELL AND TISSUE INJURY COURSE-II PATHOLOGY LABORATORY
 CELL AND TISSUE INJURY COURSE-II PATHOLOGY LABORATORY PATHOLOGY of INFECTIOUS DISEASES MICROSCOPY Rengin Ahıskalı Macroscopy samples are shown in the macroscopy presentations of the first two courses.
CELL AND TISSUE INJURY COURSE-II PATHOLOGY LABORATORY PATHOLOGY of INFECTIOUS DISEASES MICROSCOPY Rengin Ahıskalı Macroscopy samples are shown in the macroscopy presentations of the first two courses.
Pancreas. Atrophy, acinar cell. Pathogenesis: Diagnostic key features:
 Pancreas Atrophy, acinar cell Pathogenesis: Decrease in number and/or size of acinar cells may be due to spontaneous or experimentally induced degenerative changes, apoptosis, or a sequel of chronic inflammation.
Pancreas Atrophy, acinar cell Pathogenesis: Decrease in number and/or size of acinar cells may be due to spontaneous or experimentally induced degenerative changes, apoptosis, or a sequel of chronic inflammation.
CYTOMORPHOLOGY MODULE 28.1 INTRODUCTION OBJECTIVES 28.2 GENERAL GUIDELINES. Notes
 28 CYTOMORPHOLOGY 28.1 INTRODUCTION Light microscopic examination of stained cells in smears is the method of choice of diagnostic cytology. It allows classification of most normal cells as to type and
28 CYTOMORPHOLOGY 28.1 INTRODUCTION Light microscopic examination of stained cells in smears is the method of choice of diagnostic cytology. It allows classification of most normal cells as to type and
Epithelia will be discussed according to the following scheme: Type Number of layers Shape Line drawing. Squamous Cuboidal Columnar
 Epithelia Epithelia will be discussed according to the following scheme: Type Number of layers Shape Line drawing Simple Squamous Cuboidal Columnar Covering and Lining epithelium Pseudostratified Stratified
Epithelia Epithelia will be discussed according to the following scheme: Type Number of layers Shape Line drawing Simple Squamous Cuboidal Columnar Covering and Lining epithelium Pseudostratified Stratified
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines. June 2013
 Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines General Principles: Since its introduction in 1943, Papanicolaou (Pap) smear is widely
Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines General Principles: Since its introduction in 1943, Papanicolaou (Pap) smear is widely
Urine Sediment Photographs
 Urine Sediment Photographs Case History CMP-04 This urine sample is from a 35-year-old female as part of a routine exam. Laboratory data include: Specific Gravity = 1.015; ph = 7.0; ketones, glucose, protein,
Urine Sediment Photographs Case History CMP-04 This urine sample is from a 35-year-old female as part of a routine exam. Laboratory data include: Specific Gravity = 1.015; ph = 7.0; ketones, glucose, protein,
Blood Cell Identification Graded
 BCP-21 Blood Cell Identification Graded Case History The patient is a 37-year-old female with a history of multiple sickle cell crises. She now presents with avascular necrosis of the left hip. Laboratory
BCP-21 Blood Cell Identification Graded Case History The patient is a 37-year-old female with a history of multiple sickle cell crises. She now presents with avascular necrosis of the left hip. Laboratory
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies CYTOLOGIC DIAGNOSIS:
 1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
Urinary Cytology. Spasenija Savic Prince, MD Pathology, University Hospital Basel, Switzerland
 Urinary Cytology Spasenija Savic Prince, MD Pathology, University Hospital Basel, Switzerland Outline Pre-analytics The Paris System (TPS): Background Diagnostic categories Morphologic criteria for each
Urinary Cytology Spasenija Savic Prince, MD Pathology, University Hospital Basel, Switzerland Outline Pre-analytics The Paris System (TPS): Background Diagnostic categories Morphologic criteria for each
Index 179. Genital tract contaminants, 17, 20, 22, 150 papilloma virus-infected cells, 47 squamous cells, sources of, 7
 Index Accuracy of urinary cytology, 166 Acute inflammatory cells, 38 catheter sample, 39 herpes simplex infections, 44 carcinomas, 104, 105 non-viral inclusions, 52, 53 voided urine, 17 Adenocarcinoma
Index Accuracy of urinary cytology, 166 Acute inflammatory cells, 38 catheter sample, 39 herpes simplex infections, 44 carcinomas, 104, 105 non-viral inclusions, 52, 53 voided urine, 17 Adenocarcinoma
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Hematopathology Lab. Third year medical students
 Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Diagnostically Challenging Cases in Gynecologic Pathology
 Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Cervicovaginal Cytology: Normal and Abnormal Cells and Adequacy of Specimens
 Cervicovaginal Cytology: Normal and Abnormal Cells and Adequacy of Specimens 3 Christine Bergeron, MD, PhD Introduction Carcinoma of the cervix is a slow growing cancer, which is preceded by precancerous
Cervicovaginal Cytology: Normal and Abnormal Cells and Adequacy of Specimens 3 Christine Bergeron, MD, PhD Introduction Carcinoma of the cervix is a slow growing cancer, which is preceded by precancerous
Lessons From Cases of Screened Women Who Developed Cervical Carcinoma
 Lessons From Cases of Screened Women Who Developed Cervical Carcinoma R. Marshall Austin MD,PhD Magee-Womens Hospital of University of Pittsburgh Medical Center raustin@magee.edu Why Focus Study On Cases
Lessons From Cases of Screened Women Who Developed Cervical Carcinoma R. Marshall Austin MD,PhD Magee-Womens Hospital of University of Pittsburgh Medical Center raustin@magee.edu Why Focus Study On Cases
Spectrum of Lesions in Cystoscopic Bladder Biopsies -A Histopathological Study
 AJMS Al Ameen J Med Sci (2 012 )5 (2 ):1 3 2-1 3 6 (A US National Library of Medicine enlisted journal) I S S N 0 9 7 4-1 1 4 3 C O D E N : A A J M B G ORIGI NAL ARTICLE Spectrum of Lesions in Cystoscopic
AJMS Al Ameen J Med Sci (2 012 )5 (2 ):1 3 2-1 3 6 (A US National Library of Medicine enlisted journal) I S S N 0 9 7 4-1 1 4 3 C O D E N : A A J M B G ORIGI NAL ARTICLE Spectrum of Lesions in Cystoscopic
Basal cell carcinoma diagnosed on Fine-Needle Aspiration Cytology A. Pathological Case Report
 Basal cell carcinoma diagnosed on Fine-Needle Aspiration Cytology A Abstract Dr. Madhuri S.Kate 1, Dr. Preeti Jain 2, Dr. Shailesh S. Patne 3 Introduction: Basal cell carcinoma (BCC) is a locally invasive
Basal cell carcinoma diagnosed on Fine-Needle Aspiration Cytology A Abstract Dr. Madhuri S.Kate 1, Dr. Preeti Jain 2, Dr. Shailesh S. Patne 3 Introduction: Basal cell carcinoma (BCC) is a locally invasive
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
A neoplasm is defined as "an abnormal tissue proliferation, which exceeds that of adjacent normal tissue. This proliferation continues even after
 NEOPLASIA Neoplasia is a very important topic in pathology because neoplasms are both common and serious diseases. A neoplasm literally means a new growth, and this term is used interchangeably with a
NEOPLASIA Neoplasia is a very important topic in pathology because neoplasms are both common and serious diseases. A neoplasm literally means a new growth, and this term is used interchangeably with a
Potential Pitfalls for False Suspicion of Papillary Thyroid Carcinoma:
 SUPPLEMENT 1 SPECIAL ISSUE: CYTOPATHOLOGY OF THE THYROID GLAND Guest Editor: Zubair Baloch Potential Pitfalls for False Suspicion of Papillary Thyroid Carcinoma: A Cytohistologic Review of 22 Cases Xin
SUPPLEMENT 1 SPECIAL ISSUE: CYTOPATHOLOGY OF THE THYROID GLAND Guest Editor: Zubair Baloch Potential Pitfalls for False Suspicion of Papillary Thyroid Carcinoma: A Cytohistologic Review of 22 Cases Xin
Ascitic Fluid and Use of Immunocytochemistry. Mercè Jordà, University of Miami
 Ascitic Fluid and Use of Immunocytochemistry Mercè Jordà, University of Miami Is It Malignant? Yes? No Ascitic Fluid Cytomorphologic Useful Findings Tight clusters with smooth borders Cellular and nuclear
Ascitic Fluid and Use of Immunocytochemistry Mercè Jordà, University of Miami Is It Malignant? Yes? No Ascitic Fluid Cytomorphologic Useful Findings Tight clusters with smooth borders Cellular and nuclear
Lymphoma Tumor Board Quiz! Laboratory Hematology: Basic Cell Morphology
 Lymphoma Tumor Board Quiz! Laboratory Hematology: Basic Cell Morphology CABOT RINGS Cabot rings in a patient with hemolytic anemia. Cabot ring (red arrow) and Howell-Jolly body (blue arrow). Observed in
Lymphoma Tumor Board Quiz! Laboratory Hematology: Basic Cell Morphology CABOT RINGS Cabot rings in a patient with hemolytic anemia. Cabot ring (red arrow) and Howell-Jolly body (blue arrow). Observed in
Non-Neoplastic Findings
 Chapter 2 Non-Neoplastic Findings Nancy A. Young, Marluce Bibbo, Sally-Beth Buckner, Terence J. Colgan, and Marianne U. Prey Negative for Intraepithelial Lesion or Malignancy (when there is no cellular
Chapter 2 Non-Neoplastic Findings Nancy A. Young, Marluce Bibbo, Sally-Beth Buckner, Terence J. Colgan, and Marianne U. Prey Negative for Intraepithelial Lesion or Malignancy (when there is no cellular
By Dr. Mohamed Saad Daoud
 By Dr. Mohamed Saad Daoud Part I Introduction Types of White Blood Cells Genesis of the White Blood Cells Life Span of the White Blood Cells Dr. Mohamed Saad Daoud 2 Leucocytes Introduction: Infectious
By Dr. Mohamed Saad Daoud Part I Introduction Types of White Blood Cells Genesis of the White Blood Cells Life Span of the White Blood Cells Dr. Mohamed Saad Daoud 2 Leucocytes Introduction: Infectious
Case # year old man with a 2 cm right kidney mass
 Case # 4. 52 year old man with a 2 cm right kidney mass Figure 1 Figure 2 Figure 3 Figure 4 Diagnosis: Negative/Non-diagnostic Normal kidney tissue Fine needle aspiration (FNA) of the kidney is performed
Case # 4. 52 year old man with a 2 cm right kidney mass Figure 1 Figure 2 Figure 3 Figure 4 Diagnosis: Negative/Non-diagnostic Normal kidney tissue Fine needle aspiration (FNA) of the kidney is performed