Imaging for suspected glioma
|
|
|
- Silas Edwards
- 5 years ago
- Views:
Transcription

1
2 Imaging for suspected glioma Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless MRI is contraindicated Refer people with a suspected glioma to a specialist multidisciplinary team at first radiological diagnosis for management of their tumour Consider advanced MRI techniques, such as MR perfusion and MR spectroscopy, to assess the potential of a high-grade transformation in a tumour appearing to be low grade on standard structural MRI.
3 1.1.4 Report all glioma specimens according to the latest version of the World Health Organization (WHO) classification. As well as histopathological assessment, include molecular markers such as: IDH1 and IDH2 mutations ATRX mutations to identify IDH mutant astrocytomas and glioblastomas 1p/19q codeletion to identify oligodendrogliomas histone H3.3 K27M mutations in midline gliomas BRAF fusion and gene mutation to identify pilocytic astrocytoma Test all high-grade glioma specimens for MGMT promoter methylation to inform prognosis and guide treatment Consider testing IDH-wildtype glioma specimens for TERT promoter mutations to inform prognosis.
4 Initial surgery for suspected low-grade glioma The surgical expertise in the multidisciplinary team should include: access to awake craniotomy with language and other appropriate functional monitoring and expertise in intraoperative neurophysiological monitoring and access to neuro-radiological support and access to intraoperative image guidance Consider surgical resection as part of initial management (within 6 months of radiological diagnosis) to: obtain a histological and molecular diagnosis and remove as much of the tumour as safely possible after discussion of the possible extent of resection at multidisciplinary meeting and with the person with the brain tumour, and their relatives and carers If surgical resection is not appropriate, consider biopsy to obtain a histological and molecular diagnosis Consider active monitoring without a histological diagnosis, for lesions with radiological features typical of very low-grade tumours, for example, DNET (dysembryoplastic neuroepithelial tumour) or optic pathway glioma If people having active monitoring show radiological or clinical disease progression, discuss this at a multidisciplinary team meeting and consider: surgical resection or biopsy if surgical resection is not possible.
5 1.2.6 After surgery, offer radiotherapy followed by up to 6 cycles of PCV chemotherapy (procarbazine, CCNU [lomustine] and vincristine) for people who: have a 1p/19q codeleted, IDH-mutated low-grade glioma (oligodendroglioma) and are aged around 40 or over, or have residual tumour on postoperative MRI After surgery, consider radiotherapy followed by up to 6 cycles of PCV chemotherapy for people who: have a 1p/19q non-codeleted, IDH-mutated low-grade glioma (astrocytoma) and are aged around 40 or over, or have residual tumour on postoperative MRI Consider active monitoring for people who are aged around 40 or under with an IDH-mutated low-grade glioma and have no residual tumour on postoperative MRI Consider radiotherapy followed by up to 6 cycles of PCV chemotherapy for people with an IDHmutated low-grade glioma who have not had radiotherapy before if they have: progressive disease on radiological follow-up or intractable seizures When delivering radiotherapy for people with IDH-mutated low-grade glioma, do not use a treatment dose of more than 54 Gy at 1.8 Gy per fraction Be aware that the prognosis for people with histologically confirmed IDH wildtype grade II glioma may be similar to that of people with glioblastoma if other molecular features are consistent with glioblastoma. Take this into account when thinking about management options.
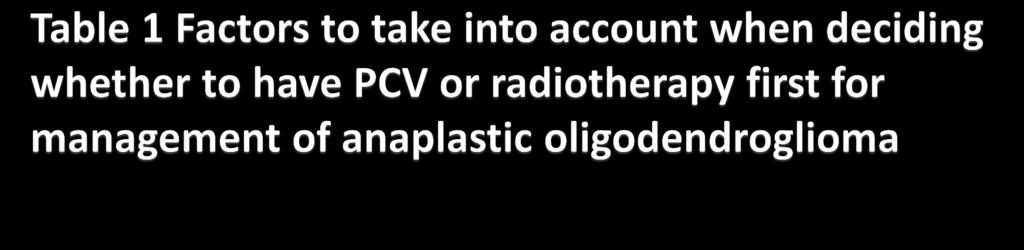
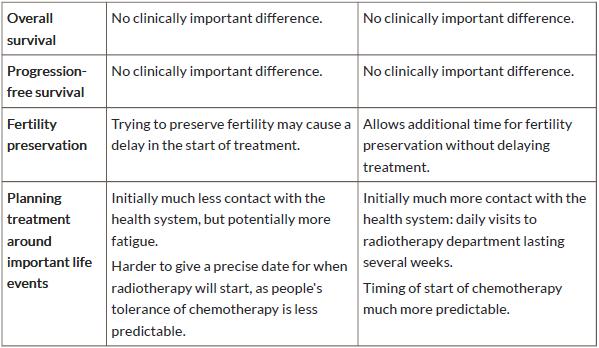
6 For guidance on using temozolomide for treating newly diagnosed grade III glioma, see the NICE technology appraisal guidance on carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma After surgery, offer sequential radiotherapy and 4 to 6 cycles of PCV chemotherapy to people who have: a Karnofsky performance status of 70 or more and a newly diagnosed grade III glioma with 1p/19q codeletion (anaplastic oligodendroglioma) Agree with the person with the anaplastic oligodendroglioma the order of PCV chemotherapy and radiotherapy after discussing the potential advantages and disadvantages of each option with them (see table 1).
7
8 After surgery, offer radiotherapy followed by up to 12 cycles of adjuvant temozolomide to people who have: a Karnofsky performance status of 70 or more and a newly diagnosed IDH-wildtype or mutated grade III glioma without 1p/19q codeletion (anaplastic astrocytoma) Do not offer nitrosoureas (for example, CCNU [lomustine]) concurrently with radiotherapy to people with newly diagnosed grade III glioma If asked, advise people with an initial diagnosis of grade III glioma (and their relatives and carers, as appropriate) that the available evidence does not support the use of: cannabis oil immunotherapy ketogenic diets Metformin statins valganciclovir.
9 For guidance on using temozolomide for treating newly diagnosed grade IV glioma (glioblastoma), see the NICE technology appraisal guidance on carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Offer radiotherapy using 60 Gy in 30 fractions with concomitant temozolomide, followed by up to 6 cycles of adjuvant temozolomide, for people aged around 70 or under who have: a Karnofsky performance status of 70 or more and had maximal safe resection, or biopsy when resection is not possible, for a newly diagnosed grade IV glioma (glioblastoma) Offer radiotherapy using 40 Gy in 15 fractions with concomitant and up to 12 cycles of adjuvant temozolomide for people aged around 70 or over who have: a Karnofsky performance status of 70 or more and a newly diagnosed grade IV glioma (glioblastoma) with MGMT methylation Consider radiotherapy using 40 Gy in 15 fractions with concomitant and up to 12 cycles of adjuvant temozolomide for people aged around 70 or over who have: a Karnofsky performance status of 70 or more and a newly diagnosed grade IV glioma (glioblastoma) without MGMT methylation or forwhich methylation status is unavailable.
10 Consider best supportive care alone for people aged around 70 or over who have: a grade IV glioma (glioblastoma) and a Karnofsky performance status of under For people with an initial diagnosis of grade IV glioma (glioblastoma) not covered in recommendations to , consider the treatment options of: radiotherapy using 60 Gy in 30 fractions with concurrent and up to 6 cycles of adjuvant temozolomide radiotherapy alone using 60 Gy in 30 fractions hypofractionated radiotherapy up to 6 cycles of temozolomide alone if the tumour has MGMT methylation and the person is aged around 70 or over best supportive care alone Assess the person's performance status throughout the postoperative period and review treatment options for grade IV glioma (glioblastoma) if their performance status changes Do not offer bevacizumab as part of management of a newly diagnosed grade IV glioma (glioblastoma) Do not offer tumour-treating fields (TTF) as part of management of a newly diagnosed grade IV glioma (glioblastoma) If asked, advise people with an initial diagnosis of grade IV glioma (and their relatives and carers, as appropriate) that the available evidence does not support the use of: cannabis oilimmunotherapy ketogenic diets metformin statins valganciclovir.
11 When deciding on treatment options for people with recurrent high-grade glioma, take into account: Karnofsky performance status the person's preferences time from last treatment tumour molecular markers what their last treatment was Consider PCV or single agent CCNU (lomustine) as an alternative to temozolomide for people with recurrent high-grade glioma For guidance on using temozolomide as an option for treating recurrent highgrade glioma, see the NICE technology appraisal guidance on temozolomide for the treatment of recurrent malignant glioma (brain cancer) Consider best supportive care alone for high-grade glioma if other treatments are not likely to be of benefit, or if the person would prefer this. Refer to the NICE guidance on improving supportive and palliative care for adults with cancer For people with focally recurrent high-grade glioma, the multidisciplinary team should also consider the treatment options of: further surgery further radiotherapy Do not offer bevacizumab, erlotinib or cediranib, either alone or in combination with chemotherapy, as part of management of recurrent high-grade glioma Do not offer tumour treating fields (TTF) as part of management of recurrent high-grade glioma If asked, advise people who have recurrent high-grade glioma (and their relatives and carers, as appropriate) that the available evidence does not support the use of: cannabis oil, immunotherapy, ketogenic diets, metformin, statins, valganciclovir.
12 If a person has a radiologically enhancing suspected high-grade glioma and the multidisciplinary team thinks that surgical resection of all enhancing tumour is possible, offer 5- aminolevulinic acid (5-ALA)-guided resection as an adjunct to maximise resection at initial surgery Consider intraoperative MRI to help achieve surgical resection of both lowgrade and highgrade glioma while preserving neurological function, unless MRI is contraindicated Consider intraoperative ultrasound to help achieve surgical resection of both low-grade and high-grade glioma Consider diffusion tensor imaging overlays in addition to standard neuronavigation techniques to minimise damage to functionally important fibre tracts during resection of both lowgrade and high-grade glioma Consider awake craniotomy for people with low-grade or high-grade glioma to help preserve neurological function Discuss awake craniotomy and its potential benefits and risks with the person and their relatives and carers (as appropriate) so that they can make an informed choice about whether to have it. Only consider the procedure if the person is likely not to be significantly distressed by it Involve other specialists as appropriate, such as neuropsychologists and speech and language therapists, before, during and after awake craniotomy.
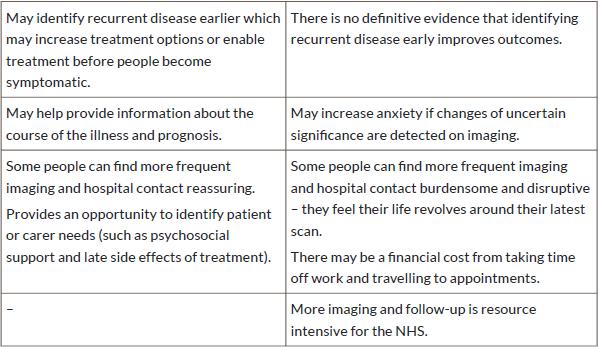
13 1.3.1 Offer regular clinical review for people with glioma to assess changes in their physical, psychological and cognitive wellbeing Base decisions on the timing of regular clinical reviews and follow-up imaging for people with glioma on: any residual tumour life expectancy the person's preferences (see table 2 for factors to discuss with them) treatments used before treatment options available tumour subtype.

14
15 1.3.3 Consider the follow-up schedule given in table 3 for people with glioma Consider standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 preand post-contrast volume) as part of regular clinical review for people with glioma, to assess for progression or recurrence, unless MRI is contraindicated Consider advanced MRI techniques, such as MR perfusion, diffusion tensor imaging and MR spectroscopy, if findings from standard imaging are unclear about whether there is recurrence and early identification is potentially clinically useful For people with glioma having routine imaging: explain to them, and their relatives and carers, that imaging can be difficult to interpret and results can be of uncertain significance and be aware that having routine imaging and waiting for the results may cause anxiety Consider a baseline MRI scan within 72 hours of surgical resection for all types of glioma Consider a baseline MRI scan 3 months after the completion of radiotherapy for all types of glioma Arrange a clinical review, including appropriate imaging, for people with glioma who develop new or changing neurological symptoms or signs at any time.
16
17 1.4.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected meningioma, unless MRI is contraindicated Consider CT imaging for meningioma (if not already performed) to assess bone involvement if this is suspected. Management of confirmed meningioma following surgery or if surgery is not possible (or has been declined) Base management of meningioma after surgery, or if surgery is not possible or the person declines surgery, on the extent of any surgery and grade of meningioma, as described in table 4.
18
19 1.4.4 Before a decision is made on radiotherapy for meningioma, take into account: comorbidities life expectancy neurological function Oedema performance status rate of tumour progression size and location of tumour surgical and radiotherapy morbidity the person's preferences (see table 5 for factors to discuss with them) treatments used before.
20
21
22 1.4.5 When deciding on the radiotherapy technique for people with meningioma, take into account: the preferences of the person (for example, to minimise the number of appointments or travel distance) tumour grade tumour location (proximity to optic nerves, optic chiasm and brainstem) tumour size. From the suitable radiotherapy techniques, choose the one which maximises the chances of local tumour control while minimising the radiation dose to normal brain tissue If the multidisciplinary team thinks that radiotherapy may be appropriate, offer the person the opportunity to discuss the potential benefits and risks with an oncologist.
23 1.5.1 Offer regular clinical review for people with meningioma to assess changes in their physical, psychological and cognitive wellbeing Base decisions on the timing of regular clinical reviews and follow-up imaging for people with meningioma on: any residual tumour life expectancy the person's preferences (see table 6 for factors to discuss with them) treatments used before treatment options available tumour grade.
24
25 1.5.3 Consider the follow-up schedule given in table 7 for people with meningioma Consider standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as part of regular clinical review for people with meningioma, to assess for progression or recurrence, unless MRI is contraindicated For people with meningioma having routine imaging, be aware that having routine imaging and waiting for the results may cause anxiety Arrange a clinical review, including appropriate imaging, for people with meningioma (including incidental meningioma) who develop new or changing neurological symptoms or signs at any time.
26
27 1.6.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected brain metastases, unless MRI is contraindicated To help establish current disease status, offer extracranial imaging (appropriate to the primary tumour type) to people with any radiologically suspected brain metastases that may be suitable for focal treatment Perform all intracranial and extracranial diagnostic imaging and, if appropriate, biopsy of extracranial disease, before referral to the neuro-oncology multidisciplinary team.
28 1.7.1 When choosing management options for brain metastases, take into account: extracranial disease leptomeningeal disease location of metastases resection cavity size the number and volume of metastases the person's preference (based on a discussion of the factors listed in tables 8 and 9) their age their performance status the primary tumour site, type, and molecular profile Consider systemic anti-cancer therapy for people who have brain metastases likely to respond effectively, for example, germ cell tumours or small-cell lung cancer Consider maximal local therapy with either surgery, stereotactic radiosurgery or stereotactic radiotherapy for people with a single brain metastasis Base the choice of treatment for people with a single brain metastasis on: comorbidities extent of oedema location of metastasis the person's preference (see table 8) tumour size.
29
30 1.7.5 Do not offer adjuvant whole-brain radiotherapy to people with a single brain metastasis treated with stereotactic radiosurgery/radiotherapy or surgery Consider adjuvant stereotactic radiosurgery/radiotherapy to the surgical cavities for people with 1 to 3 brain metastases that have been resected Consider stereotactic radiosurgery/radiotherapy for people with multiple brain metastases who have controlled or controllable extracranial disease and Karnofsky performance status of 70 or more. Take into account the number and total volume of metastases Do not offer whole-brain radiotherapy to people with: non-small-cell lung cancer and brain metastases that are not suitable for surgery or stereotactic radiosurgery/radiotherapy and a Karnofsky performance status of under For people with multiple brain metastases who have not had stereotactic radiosurgery/radiotherapy or surgery, decide with them whether to use wholebrain radiotherapy after a discussion with them and their relatives and carers (as appropriate) of the potential benefits and risks (see table 9).
31 Do not offer memantine in addition to whole-brain radiotherapy to people with multiple brain metastases, unless as part of a clinical trial Do not offer concurrent systemic therapy to enhance the efficacy of wholebrain radiotherapy to people with multiple brain metastases, unless as part of a clinical trial.
32 1.8.1 Offer regular clinical review for people with brain metastases to assess changes in their physical, psychological and cognitive wellbeing Base decisions on the timing of regular clinical reviews and follow-up imaging for people with brain metastases on: extracranial disease status life expectancy primary cancer the person's preferences (see table 10 for factors to discuss with them) treatment options available.
 as part of regular clinical review for people with brain metastases, to assess for progression or recurrence, unless MRI is")
33 1.8.3 Consider the follow-up schedule given in table 11 for people with brain metastases Consider standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as part of regular clinical review for people with brain metastases, to assess for progression or recurrence, unless MRI is contraindicated.

34 1.8.5 Consider advanced MRI techniques, such as MR perfusion, diffusion tensor imaging and MR spectroscopy, if findings from standard imaging are unclear about whether there is recurrence and early identification is potentially clinically useful For people with brain metastases having routine imaging: explain to them, and their relatives and carers, that imaging can be difficult to interpret and results can be of uncertain significance and be aware that having routine imaging and waiting for the results may cause anxiety Arrange a clinical review, including appropriate imaging, for people with brain metastases who develop new or changing neurological symptoms or signs at any time. Table 11 Possible regular clinical review schedule for people with brain metastases
35 1.9.1 Be aware that the care needs of people with brain tumours represent a unique challenge, because (in addition to physical disability) the tumour and treatment can have effects on: behaviour Cognition personality Discuss health and social care support needs with the person with a brain tumour and their relatives and carers (as appropriate). Take into account the complex health and social care support needs people with any type of brain tumour and their relatives and carers may have (for example, psychological, cognitive, physical, spiritual, emotional) Set aside enough time to discuss the impact of the brain tumour on the person and their relatives and carers (as appropriate), and to elicit and discuss their health and social care support needs Health and social care professionals involved in the care of people with brain tumours should address additional complex needs during or at the end of treatment and throughout follow-up. These include:
36 changes to cognitive functioning fatigue loss of personal identity loss of independence maintaining a sense of hope potential for change in personal and sexual relationships the challenges of living with uncertainty the impact of brain tumour-associated epilepsy on wellbeing (see the NICE guideline on epilepsies: diagnosis and management) Provide a named healthcare professional with responsibility for coordinating health and social care support for people with brain tumours and their relatives and carers, for example, a key worker (often a clinical nurse specialist) as defined in NICE guidance on improving outcomes for people with brain and other central nervous system tumours.
37 1.9.6 Give information to the person with a brain tumour and their relatives and carers (as appropriate): in a realistic and empathetic manner in suitable formats (written and spoken, with information available to take away), following the principles in the NICE guideline on patient experience in adult NHS services[1] at appropriate times throughout their care pathway Explain to the person that they have a legal obligation to notify the Driver and Vehicle Licensing Agency (DVLA) if they have a brain tumour, and that this may have implications for their driving Provide and explain clinical results, for example, imaging and pathology reports, to the person with a brain tumour and their relatives and carers (as appropriate) as soon as possible Offer supportive care to people with brain tumours and their relatives and carers (as appropriate) throughout their treatment and care pathway In people aged between 16 and 24 years old, refer to the NICE quality standard on cancer services for children and young people Discuss the potential preservation of fertility with people with brain tumours where treatment may have an impact on their fertility (see the recommendations on people with cancer who wish to preserve fertility in NICE's guidance on fertility problems) If the person with a brain tumour is likely to be in their last year of life, refer to the NICE quality standards on end of life care for adults and, when appropriate, care of dying adults in the last days of life.
38 Consider referring the person with a brain tumour for a neurological rehabilitation assessment of physical, cognitive and emotional function at diagnosis and every stage of follow-up Offer people with brain tumours and their relatives and carers (as appropriate) information on accessing neurological rehabilitation, and on what needs it can help address Give people with brain tumours and their relatives and carers (as appropriate) information on: neurological rehabilitation options in the community, as an outpatient, or an inpatient and how to get a neurological rehabilitation assessment.
39 Be aware that people with brain tumours can develop side effects of treatment months or years after treatment, which can include: Cataracts Cavernoma Cognitive decline Epilepsy Hearing loss Hypopituitarism Infertility Neuropathy (for example, nerve damage causing visual loss, numbness, pain or weakness) Radionecrosis Secondary tumours SMART (stroke-like migraine attacks after radiotherapy) Stroke.
40 Assess the person's individual risk of developing late effects when they finish treatment. Record these in their written treatment summary and explain them to the person (and their relatives and carers, as appropriate) Encourage people who have had cranial radiotherapy to follow a healthy lifestyle, including exercise, a healthy diet and stopping smoking (if applicable), to decrease their risk of stroke. See the NICE guidelines on obesity prevention, physical activity and smoking cessation For people who are at risk of stroke, consider checking their blood pressure, HbA1c level and cholesterol profile regularly Consider ongoing neuropsychology assessment for people at risk of cognitive decline If a person has had a radiotherapy dose that might affect pituitary function, consider checking their endocrine function regularly after the end of treatment Consider referring people who are at risk of visual impairment for an ophthalmological assessment Consider referring people who are at risk of hearing loss to audiology for a hearing test Consider referring the person to stroke services if an MRI during active monitoring identifies asymptomatic ischaemic stroke.
NICE guideline Published: 11 July 2018 nice.org.uk/guidance/ng99
 Brain tumours (primary) and brain metastases in adults NICE guideline Published: 11 July 2018 nice.org.uk/guidance/ng99 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Brain tumours (primary) and brain metastases in adults NICE guideline Published: 11 July 2018 nice.org.uk/guidance/ng99 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Brain tumours (primary) and brain metastases in adults
 and brain metastases in adults") Brain tumours (primary) and brain metastases in adults NICE guideline Draft for consultation, January 0 This guideline covers diagnosing, monitoring and managing any type of primary brain tumour or brain
Brain tumours (primary) and brain metastases in adults NICE guideline Draft for consultation, January 0 This guideline covers diagnosing, monitoring and managing any type of primary brain tumour or brain
Primary brain tumours and cerebral metastases workshop
 Primary brain tumours and cerebral workshop 22.4.16 Summary of workshop group discussions on the content of the scope Scope section Title: Primary brain tumours and cerebral Who the guideline is for People
Primary brain tumours and cerebral workshop 22.4.16 Summary of workshop group discussions on the content of the scope Scope section Title: Primary brain tumours and cerebral Who the guideline is for People
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES
 MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
CNS SESSION 3/8/ th Multidisciplinary Management of Cancers: A Case based Approach
 CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121
 Carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121 NICE 2018. All rights reserved.
Carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121 NICE 2018. All rights reserved.
Cilengitide (Impetreve) for glioblastoma multiforme. February 2012
 for glioblastoma multiforme. February 2012") Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
Precision medicine for gliomas
 Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
NON MALIGNANT BRAIN TUMOURS Facilitator. Ros Taylor Advanced Neurosurgical Nurse Practitioner Southmead Hospital Bristol
 NON MALIGNANT BRAIN TUMOURS Facilitator Ros Taylor Advanced Neurosurgical Nurse Practitioner Southmead Hospital Bristol Neurosurgery What will be covered? Meningioma Vestibular schwannoma (acoustic neuroma)
NON MALIGNANT BRAIN TUMOURS Facilitator Ros Taylor Advanced Neurosurgical Nurse Practitioner Southmead Hospital Bristol Neurosurgery What will be covered? Meningioma Vestibular schwannoma (acoustic neuroma)
Cancer Survivorship NEURO-ONCOLOGY PATIENT SURVIVORSHIP PLAN. Resources and Tools for the Multidisciplinary Team
 NEURO-ONCOLOGY PATIENT SURVIVORSHIP PLAN Cancer Survivorship Resources and Tools for the Multidisciplinary Team Your survivorship care plan is a summary of your tumor treatments and recommendations for
NEURO-ONCOLOGY PATIENT SURVIVORSHIP PLAN Cancer Survivorship Resources and Tools for the Multidisciplinary Team Your survivorship care plan is a summary of your tumor treatments and recommendations for
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Malignant melanoma: assessment and management of malignant melanoma 1.1 Short title Malignant Melanoma 2 The remit The Department
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Malignant melanoma: assessment and management of malignant melanoma 1.1 Short title Malignant Melanoma 2 The remit The Department
PRESURGICAL PLANNING. Strongly consider neuropsychological evaluation before functional imaging study Strongly consider functional imaging study
 NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
Oligodendrogliomas & Oligoastrocytomas
 Oligodendrogliomas & Oligoastrocytomas ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization dedicated solely
Oligodendrogliomas & Oligoastrocytomas ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization dedicated solely
Scottish Medicines Consortium
 Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Radioterapia no Tratamento dos Gliomas de Baixo Grau
 Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Corporate Medical Policy
 Corporate Medical Policy Brachytherapy, Intracavitary Balloon Catheter for Brain Cancer File Name: Origination: Last CAP Review: Next CAP Review: Last Review: brachytherapy_intracavitary_balloon_catheter_for_brain_cancer
Corporate Medical Policy Brachytherapy, Intracavitary Balloon Catheter for Brain Cancer File Name: Origination: Last CAP Review: Next CAP Review: Last Review: brachytherapy_intracavitary_balloon_catheter_for_brain_cancer
Specialised Services Policy: CP22. Stereotactic Radiosurgery
 Specialised Services Policy: CP22 Document Author: Assistant Director of Planning Executive Lead: Director of Planning ad Performance Approved by: Management Group Issue Date: 01 July 2015 Review Date:
Specialised Services Policy: CP22 Document Author: Assistant Director of Planning Executive Lead: Director of Planning ad Performance Approved by: Management Group Issue Date: 01 July 2015 Review Date:
National Institute for Health and Clinical Excellence. Single Technology Appraisal (STA)
") National Institute for Health and Clinical Excellence Appendix C Comment 1: the draft scope Single Technology Appraisal (STA) Carmustine implants for the treatment of recurrent glioblastoma multiforme
National Institute for Health and Clinical Excellence Appendix C Comment 1: the draft scope Single Technology Appraisal (STA) Carmustine implants for the treatment of recurrent glioblastoma multiforme
Brain Tumor Treatment
 Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to.
 Stratified Medicine Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to. Looking in detail at cancer cells and their genetic make up. Permit
Stratified Medicine Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to. Looking in detail at cancer cells and their genetic make up. Permit
Challenging Paediatric Brain Tumours. ASP Belfast March 2017 Dr Jane Pears Consultant Paediatric Oncologist, Dublin
 Challenging Paediatric Brain Tumours ASP Belfast March 2017 Dr Jane Pears Consultant Paediatric Oncologist, Dublin Overview (i) Paediatric malignancy (ii) Central nervous system tumours (iii) Diffuse Intrinsic
Challenging Paediatric Brain Tumours ASP Belfast March 2017 Dr Jane Pears Consultant Paediatric Oncologist, Dublin Overview (i) Paediatric malignancy (ii) Central nervous system tumours (iii) Diffuse Intrinsic
Supporting patients with brain tumours
 Supporting patients with brain tumours Alison Corbett Macmillan Clinical Nurse Specialist Neuro-Oncology Women's cancers Breast cancer introduction 1 Key contributions that CNSs make to cancer care Tumour
Supporting patients with brain tumours Alison Corbett Macmillan Clinical Nurse Specialist Neuro-Oncology Women's cancers Breast cancer introduction 1 Key contributions that CNSs make to cancer care Tumour
SURGICAL MANAGEMENT OF BRAIN TUMORS
 SURGICAL MANAGEMENT OF BRAIN TUMORS LIGIA TATARANU, MD, Ph D NEUROSURGICAL CLINIC, BAGDASAR ARSENI CLINICAL HOSPITAL BUCHAREST, ROMANIA SURGICAL INDICATIONS CONFIRMING HISTOLOGIC DIAGNOSIS REDUCING TUMOR
SURGICAL MANAGEMENT OF BRAIN TUMORS LIGIA TATARANU, MD, Ph D NEUROSURGICAL CLINIC, BAGDASAR ARSENI CLINICAL HOSPITAL BUCHAREST, ROMANIA SURGICAL INDICATIONS CONFIRMING HISTOLOGIC DIAGNOSIS REDUCING TUMOR
21/03/2017. Disclosure. Practice Changing Articles in Neuro Oncology for 2016/17. Gliomas. Objectives. Gliomas. No conflicts to declare
 Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Corporate Medical Policy
 Corporate Medical Policy Analysis of MGMT Promoter Methylation in Malignant Gliomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: analysis_of_mgmt_promoter_methylation_in_malignant_gliomas
Corporate Medical Policy Analysis of MGMT Promoter Methylation in Malignant Gliomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: analysis_of_mgmt_promoter_methylation_in_malignant_gliomas
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: tumor_treatment_fields_therapy 9/2013 11/2017 11/2018 6/2018 Description of Procedure or Service Tumor-treatment
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: tumor_treatment_fields_therapy 9/2013 11/2017 11/2018 6/2018 Description of Procedure or Service Tumor-treatment
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
CNS Tumors: The Med Onc Perspective. Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U.
 CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
Gamma Knife Radiosurgery A tool for treating intracranial conditions. CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop
 Gamma Knife Radiosurgery A tool for treating intracranial conditions CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop ANGELA McBEAN Gamma Knife CNC State-wide Care Coordinator Gamma Knife
Gamma Knife Radiosurgery A tool for treating intracranial conditions CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop ANGELA McBEAN Gamma Knife CNC State-wide Care Coordinator Gamma Knife
Thierry M. Muanza, MSc, MD, FRCPC,, McGill University Segal Cancer Centre, Jewish General Hospital Montreal, QC, Canada
 Thierry M. Muanza, MSc, MD, FRCPC,, McGill University Segal Cancer Centre, Jewish General Hospital Montreal, QC, Canada Déclarations Aucun conflit d intérêt Objectifs d apprentissage Évolution de la radiothérapie
Thierry M. Muanza, MSc, MD, FRCPC,, McGill University Segal Cancer Centre, Jewish General Hospital Montreal, QC, Canada Déclarations Aucun conflit d intérêt Objectifs d apprentissage Évolution de la radiothérapie
Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment
![Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment](/thumbs/87/96032554.jpg "Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment") Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: GLIOBLASTOMA MULTIFORME (CNS) Patient information given at each stage following agreed
Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: GLIOBLASTOMA MULTIFORME (CNS) Patient information given at each stage following agreed
Skull Base Tumour Service. The Multi-Disciplinary Team (MDT) Explained. Jan 2018 v1
 Explained. Jan 2018 v1") Skull Base Tumour Service The Multi-Disciplinary Team (MDT) Explained Jan 2018 v1 Skull base tumours grow in the bones of the skull that form the bottom of the head and the body ridge between the nose
Skull Base Tumour Service The Multi-Disciplinary Team (MDT) Explained Jan 2018 v1 Skull base tumours grow in the bones of the skull that form the bottom of the head and the body ridge between the nose
LOW GRADE ASTROCYTOMAS
 LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
Neurosurgical Management of Brain Tumours. Nicholas Little Neurosurgeon RNSH
 Neurosurgical Management of Brain Tumours Nicholas Little Neurosurgeon RNSH General Most common tumours are metastatic 10x more common than primary Incidence of primary neoplasms is 20 per 100000 per year
Neurosurgical Management of Brain Tumours Nicholas Little Neurosurgeon RNSH General Most common tumours are metastatic 10x more common than primary Incidence of primary neoplasms is 20 per 100000 per year
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Radiotherapy and Brain Metastases. Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem
 Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Brain and CNS Cancer. Measurability of Quality Performance Indicators Version 3.0
 Brain and CNS Cancer Measurability of Quality Permance Indicators Version 3.0 To be read in conjunction with: Brain and Central Nervous System Cancer Clinical Quality Permance Indicators Brain and Central
Brain and CNS Cancer Measurability of Quality Permance Indicators Version 3.0 To be read in conjunction with: Brain and Central Nervous System Cancer Clinical Quality Permance Indicators Brain and Central
Watch and wait (active monitoring)
") Watch and wait (active monitoring) When you re diagnosed with a brain tumour, you may expect to have immediate treatment, possibly involving surgery and/or radiotherapy and chemotherapy. However, with
Watch and wait (active monitoring) When you re diagnosed with a brain tumour, you may expect to have immediate treatment, possibly involving surgery and/or radiotherapy and chemotherapy. However, with
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls. Rob Macaulay Neuropathologist, MCC October 21, 2017
 Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma
 National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
Oncological Management of Brain Tumours. Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013
 Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
National Breast Cancer Audit next steps. Martin Lee
 National Breast Cancer Audit next steps Martin Lee National Cancer Audits Current Bowel Cancer Head & Neck Cancer Lung cancer Oesophagogastric cancer New Prostate Cancer - undergoing procurement Breast
National Breast Cancer Audit next steps Martin Lee National Cancer Audits Current Bowel Cancer Head & Neck Cancer Lung cancer Oesophagogastric cancer New Prostate Cancer - undergoing procurement Breast
Glioblastoma. In this fact sheet:
 Glioblastoma Glioblastomas are the most common primary brain tumours in adults. (Primary means the tumour starts in the brain, rather than starting elsewhere in the body then spreading to the brain.) It
Glioblastoma Glioblastomas are the most common primary brain tumours in adults. (Primary means the tumour starts in the brain, rather than starting elsewhere in the body then spreading to the brain.) It
Update on Management of Malignant Spinal Cord Compression. Heino Hugel Consultant in Palliative Medicine University Hospital Aintree
 Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
AMERICAN BRAIN TUMOR ASSOCIATION. Oligodendroglioma and Oligoastrocytoma
 AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
Chapter 5 Section 3.1
 Radiology Chapter 5 Section 3.1 Issue Date: March 27, 1991 Authority: 32 CFR 199.4(b)(2), (b)(2)(x), (c)(2)(viii), and (g)(15) 1.0 CPT 1 PROCEDURE CODES 37243, 61793, 61795, 77261-77421, 77427-77799, 0073T
Radiology Chapter 5 Section 3.1 Issue Date: March 27, 1991 Authority: 32 CFR 199.4(b)(2), (b)(2)(x), (c)(2)(viii), and (g)(15) 1.0 CPT 1 PROCEDURE CODES 37243, 61793, 61795, 77261-77421, 77427-77799, 0073T
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
NICE Quality Standards and COF
 NICE Quality Standards and COF David Baldwin Consultant Respiratory Physician NUH Hon Senior Lecturer Nottingham University Clinical lead NICE lung cancer GL Chair NICE QS Topic Expert Group Quality Standards
NICE Quality Standards and COF David Baldwin Consultant Respiratory Physician NUH Hon Senior Lecturer Nottingham University Clinical lead NICE lung cancer GL Chair NICE QS Topic Expert Group Quality Standards
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Clinical Policy: Temozolomide (Temodar) Reference Number: ERX.SPA.138 Effective Date:
 Reference Number: ERX.SPA.138 Effective Date:") Clinical Policy: (Temodar) Reference Number: ERX.SPA.138 Effective Date: 03.01.14 Last Review Date: 05.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Temodar) Reference Number: ERX.SPA.138 Effective Date: 03.01.14 Last Review Date: 05.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Stereotactic ablative body radiotherapy for renal cancer
 1 EVIDENCE SUMMARY REPORT Stereotactic ablative body radiotherapy for renal cancer Questions to be addressed 1. What is the clinical effectiveness of stereotactic ablative body radiotherapy for inoperable
1 EVIDENCE SUMMARY REPORT Stereotactic ablative body radiotherapy for renal cancer Questions to be addressed 1. What is the clinical effectiveness of stereotactic ablative body radiotherapy for inoperable
AMERICAN BRAIN TUMOR ASSOCIATION. Oligodendroglioma and Oligoastrocytoma
 AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
Clinical guideline Published: 27 April 2011 nice.org.uk/guidance/cg122
 Ovarian cancer: recognition and initial management Clinical guideline Published: 27 April 2011 nice.org.uk/guidance/cg122 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Ovarian cancer: recognition and initial management Clinical guideline Published: 27 April 2011 nice.org.uk/guidance/cg122 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Gliomas in the 2016 WHO Classification of CNS Tumors
 Gliomas in the 2016 WHO Classification of CNS Tumors Hindi N Al-Hindi, MD, FCAP Consultant Neuropathologist and Head Section of Anatomic Pathology Department of Pathology and Laboratory Medicine King Faisal
Gliomas in the 2016 WHO Classification of CNS Tumors Hindi N Al-Hindi, MD, FCAP Consultant Neuropathologist and Head Section of Anatomic Pathology Department of Pathology and Laboratory Medicine King Faisal
European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas
 guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas") European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas Michael Weller, Martin van den Bent, Jörg C Tonn, Roger Stupp, Matthias
European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas Michael Weller, Martin van den Bent, Jörg C Tonn, Roger Stupp, Matthias
Brain & Central Nervous System (CNS) Cancer Clinical Guidelines
 Cancer Clinical Guidelines") Brain & Central Nervous System (CNS) Cancer Clinical Guidelines Brain and CNS EAG on behalf of NCA Title: NCA Brain & CNS Cancer Clinical Guidelines Authors: Brain EAG members Circulation List: See page
Brain & Central Nervous System (CNS) Cancer Clinical Guidelines Brain and CNS EAG on behalf of NCA Title: NCA Brain & CNS Cancer Clinical Guidelines Authors: Brain EAG members Circulation List: See page
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
NICE guideline Published: 24 January 2018 nice.org.uk/guidance/ng83
 Oesophago-gastric cancer: assessment and management in adults NICE guideline Published: 24 January 18 nice.org.uk/guidance/ng83 NICE 18. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Oesophago-gastric cancer: assessment and management in adults NICE guideline Published: 24 January 18 nice.org.uk/guidance/ng83 NICE 18. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Table 1 Standards and items to set up a PCU: general requirements and critical mass
 Table 1 Standards and items to set up a PCU: general requirements and critical mass General requirements and European Prostate Cancer Units are structures managing sufficient volumes of patients with on-site
Table 1 Standards and items to set up a PCU: general requirements and critical mass General requirements and European Prostate Cancer Units are structures managing sufficient volumes of patients with on-site
Corporate Medical Policy Tumor-Treatment Fields Therapy for Glioblastoma
 Corporate Medical Policy Tumor-Treatment Fields Therapy for Glioblastoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: tumor-treatment_fields_therapy_for_glioblastoma 9/2013 11/2017
Corporate Medical Policy Tumor-Treatment Fields Therapy for Glioblastoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: tumor-treatment_fields_therapy_for_glioblastoma 9/2013 11/2017
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
Glioblastoma: Current Treatment Approach 8/20/2018
 Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
NICE BULLETIN Diagnosis & treatment of prostate cancer
 Diagnosis & treatment of prostate cancer NICE provided the content for this booklet which is independent of any company or product advertised Diagnosis and treatment of prostate cancer Introduction In
Diagnosis & treatment of prostate cancer NICE provided the content for this booklet which is independent of any company or product advertised Diagnosis and treatment of prostate cancer Introduction In
Small Cell Lung Cancer
 Small Cell Lung Cancer Small cell lung cancer (SCLC) affects 15% of all lung cancer patients. SCLC is the most aggressive type of lung cancer. It may be treated with chemotherapy and radiation. SCLC has
Small Cell Lung Cancer Small cell lung cancer (SCLC) affects 15% of all lung cancer patients. SCLC is the most aggressive type of lung cancer. It may be treated with chemotherapy and radiation. SCLC has
Brain Tumors. Andrew J. Fabiano, MD FAANS. Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine
 Brain Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases Brain
Brain Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases Brain
Dr Eddie Mee. Neurosurgeon Auckland City Hospital, Ascot Integrated Hospital, MercyAscot Hospitals, Auckland
 Dr Eddie Mee Neurosurgeon Auckland City Hospital, Ascot Integrated Hospital, MercyAscot Hospitals, Auckland 16:30-17:25 WS #48: Current Management of Brain Bleeds and Tumours 17:35-18:30 WS #58: Current
Dr Eddie Mee Neurosurgeon Auckland City Hospital, Ascot Integrated Hospital, MercyAscot Hospitals, Auckland 16:30-17:25 WS #48: Current Management of Brain Bleeds and Tumours 17:35-18:30 WS #58: Current
SCIENTIFIC PROGRAMME SNOLA UPDATE ON NEURO- ONCOLOGY th March
 SCIENTIFIC PROGRAMME SNOLA UPDATE ON NEURO- ONCOLOGY 2016 24th March 13h 13h45 pathology case case parasellar meningeoma case : posterior fossa pediatric tumor 13h45 16h Imaging for CNS lymphomas Parasellar
SCIENTIFIC PROGRAMME SNOLA UPDATE ON NEURO- ONCOLOGY 2016 24th March 13h 13h45 pathology case case parasellar meningeoma case : posterior fossa pediatric tumor 13h45 16h Imaging for CNS lymphomas Parasellar
Neuro-oncology Update Andrew Kokkino, MD Medical Director, The Neurosciences Institute at Sacred Heart at Riverbend May 20, 2013
 Neuro-oncology Update 2013 Andrew Kokkino, MD Medical Director, The Neurosciences Institute at Sacred Heart at Riverbend May 20, 2013 Case 1 58 year old man with recent facial droop and HA s Thin, cachectic
Neuro-oncology Update 2013 Andrew Kokkino, MD Medical Director, The Neurosciences Institute at Sacred Heart at Riverbend May 20, 2013 Case 1 58 year old man with recent facial droop and HA s Thin, cachectic
Pediatr Blood Cancer 2014
 Low grade Glioma! 40% of pediatric brain tumors Pathologically, anatomically, clinically and biologically heterogeneous Leptomeningeal metastases in 5% Frequently protracted clinical course Long-Term Outcome
Low grade Glioma! 40% of pediatric brain tumors Pathologically, anatomically, clinically and biologically heterogeneous Leptomeningeal metastases in 5% Frequently protracted clinical course Long-Term Outcome
Neurocognitive Assessment in Patients with Brain Metastases. Martin Klein VU University Medical Center Amsterdam, The Netherlands
 Neurocognitive Assessment in Patients with Brain Metastases Martin Klein VU University Medical Center Amsterdam, The Netherlands Treatment Outcomes I Traditional/primary endpoints of efficacy:! Physician
Neurocognitive Assessment in Patients with Brain Metastases Martin Klein VU University Medical Center Amsterdam, The Netherlands Treatment Outcomes I Traditional/primary endpoints of efficacy:! Physician
National Optimal Lung Cancer Pathway
 National Optimal Lung Cancer Pathway This document was produced by the Lung Clinical Expert Group 2017 Document Title: National Optimal Lung Cancer Pathway and Implementation Guide Date of issue: August
National Optimal Lung Cancer Pathway This document was produced by the Lung Clinical Expert Group 2017 Document Title: National Optimal Lung Cancer Pathway and Implementation Guide Date of issue: August
University of Colorado Cancer Center Brain Disease Site Schema
 GBM FIRST LINE 18 0376/Kazia Phase 2a study (Part 1): A phase 2a study to evaluate the safety, pharmacokinetics and clinical activity of the PI3K/mTOR inhibitor GDC 0084 administered to patients with glioblastoma
GBM FIRST LINE 18 0376/Kazia Phase 2a study (Part 1): A phase 2a study to evaluate the safety, pharmacokinetics and clinical activity of the PI3K/mTOR inhibitor GDC 0084 administered to patients with glioblastoma
Dosimetry, see MAGIC; Polymer gel dosimetry. Fiducial tracking, see CyberKnife radiosurgery
 Subject Index Acoustic neuroma, neurofibromatosis type 2 complications 103, 105 hearing outcomes 103, 105 outcome measures 101 patient selection 105 study design 101 tumor control 101 105 treatment options
Subject Index Acoustic neuroma, neurofibromatosis type 2 complications 103, 105 hearing outcomes 103, 105 outcome measures 101 patient selection 105 study design 101 tumor control 101 105 treatment options
Prior to 1993, the only data available in the medical
 Neuro-Oncology Prospective clinical trials of intracranial low-grade glioma in adults and children Edward G. Shaw 1 and Jeffrey H. Wisoff Department of Radiation Oncology, Wake Forest University School
Neuro-Oncology Prospective clinical trials of intracranial low-grade glioma in adults and children Edward G. Shaw 1 and Jeffrey H. Wisoff Department of Radiation Oncology, Wake Forest University School
Hypofractionated radiation therapy for glioblastoma
 Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS
 UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Leslie Riley. Sarcoma Program AT SMILOW CANCER HOSPITAL
 Leslie Riley Sarcoma Program AT SMILOW CANCER HOSPITAL The Sarcoma Program at Smilow Cancer Hospital is a multidisciplinary team of physicians specialized in the diagnosis, treatment, and care of patients
Leslie Riley Sarcoma Program AT SMILOW CANCER HOSPITAL The Sarcoma Program at Smilow Cancer Hospital is a multidisciplinary team of physicians specialized in the diagnosis, treatment, and care of patients
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준. KNS-MT-03 (April 15, 2015)
") 성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
Background. Central nervous system (CNS) tumours. High-grade glioma
 tumours. High-grade glioma") 25 4. Central nervous system (CNS) tumours Background Two important considerations underpin the choice of treatment fractionation in neurooncology. First, the results of treatment vary widely and, second,
25 4. Central nervous system (CNS) tumours Background Two important considerations underpin the choice of treatment fractionation in neurooncology. First, the results of treatment vary widely and, second,
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
Glioblastoma. In this fact sheet: What is a glioblastoma?
 Glioblastoma Glioblastomas are the most common primary brain tumours in adults. (Primary means the tumour starts in the brain, rather than starting elsewhere in the body then spreading to the brain). It
Glioblastoma Glioblastomas are the most common primary brain tumours in adults. (Primary means the tumour starts in the brain, rather than starting elsewhere in the body then spreading to the brain). It
This information explains the advice about the care and treatment of people with stable angina that is set out in NICE clinical guideline 126.
 Information for the public Published: 1 July 2011 nice.org.uk About this information NICE clinical guidelines advise the NHS on caring for people with specific conditions or diseases and the treatments
Information for the public Published: 1 July 2011 nice.org.uk About this information NICE clinical guidelines advise the NHS on caring for people with specific conditions or diseases and the treatments
National Horizon Scanning Centre. Bevacizumab (Avastin) for glioblastoma multiforme - relapsed. August 2008
 for glioblastoma multiforme - relapsed. August 2008") Bevacizumab (Avastin) for glioblastoma multiforme - relapsed August 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not intended
Bevacizumab (Avastin) for glioblastoma multiforme - relapsed August 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not intended
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM)
") SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician ASWCN TAUNTON AND SOMERSET Taunton Lung MDT (11-2C-1) - 2011/12 Dr Sarah Foster Compliance Self Assessment LUNG MDT
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician ASWCN TAUNTON AND SOMERSET Taunton Lung MDT (11-2C-1) - 2011/12 Dr Sarah Foster Compliance Self Assessment LUNG MDT
Cancer Management Chapter 23: Primary and metastatic brain tumors
 Cancer Management: A Multidisciplinary Approach, 12th Edition (2009). Cancer Management Chapter 23: Primary and metastatic brain tumors By Lisa M. DeAngelis, MD, Jay S. Loeffler, MD, and Adam N. Mamelak,
Cancer Management: A Multidisciplinary Approach, 12th Edition (2009). Cancer Management Chapter 23: Primary and metastatic brain tumors By Lisa M. DeAngelis, MD, Jay S. Loeffler, MD, and Adam N. Mamelak,
Advancements in Neuro- Oncology
 Advancements in Neuro- Oncology Ricky Chen, MD Director, Neuro-Oncology Providence St Vincent Medical Center November 30 th, 2018 No disclosures Recognizing a brain tumor New and *Persistent Headaches*
Advancements in Neuro- Oncology Ricky Chen, MD Director, Neuro-Oncology Providence St Vincent Medical Center November 30 th, 2018 No disclosures Recognizing a brain tumor New and *Persistent Headaches*
Northern Suburbs Clinic for Lung Cancer (NSCLC): Targeting Lung Cancer
: Targeting Lung Cancer") Northern Suburbs Clinic for Lung Cancer (NSCLC): Targeting Lung Cancer Page 1 Phuong Tran (Rad Onc) Lung Cancer Most common cause of cancer related deaths in Australia 19% of all cancer deaths Survival
Northern Suburbs Clinic for Lung Cancer (NSCLC): Targeting Lung Cancer Page 1 Phuong Tran (Rad Onc) Lung Cancer Most common cause of cancer related deaths in Australia 19% of all cancer deaths Survival
Audit Report. Brain and CNS Cancer Quality Performance Indicators. Report of the 2014 Clinical Audit Data
 North, South East and West of Scotland Cancer Networks Neuro-Oncology Cancers Audit Report Brain and CNS Cancer Quality Performance Indicators Report of the 2014 Clinical Audit Data Dr Avinash Kanodia
North, South East and West of Scotland Cancer Networks Neuro-Oncology Cancers Audit Report Brain and CNS Cancer Quality Performance Indicators Report of the 2014 Clinical Audit Data Dr Avinash Kanodia
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
Brain tumours (primary) and brain metastases in adults
 and brain metastases in adults") National Institute for Health and Care Excellence Final Brain tumours (primary) and brain metastases in adults Methods NICE guideline NG99 July 2018 Final These evidence reviews were developed by the National
National Institute for Health and Care Excellence Final Brain tumours (primary) and brain metastases in adults Methods NICE guideline NG99 July 2018 Final These evidence reviews were developed by the National
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Jennie W Taylor, MD 02/15/2019. Patient 1 Presentation
 Patient 1 Presentation Jennie W Taylor, MD 02/15/2019 A 34 year old right handed woman presents in 07/2015 with 9 years of stereotyped spells of olfactory change, nausea, and altered awareness. Imaging
Patient 1 Presentation Jennie W Taylor, MD 02/15/2019 A 34 year old right handed woman presents in 07/2015 with 9 years of stereotyped spells of olfactory change, nausea, and altered awareness. Imaging
A Framework of Competences for Special Interest Module in Paediatric Epilepsies
 A Framework of Competences for Special Interest Module in Paediatric Epilepsies 2 Section 1 CONTENTS Introduction 5 Section 2 Specific Competences in Paediatric Epilepsies 7 Knowledge and Understanding
A Framework of Competences for Special Interest Module in Paediatric Epilepsies 2 Section 1 CONTENTS Introduction 5 Section 2 Specific Competences in Paediatric Epilepsies 7 Knowledge and Understanding
Systemic Treatment. Third International Neuro-Oncology Course. 23 May 2014
 Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
CAPITAL HEALTH CENTER FOR ONCOLOGY. capitalhealth.org/oncology
 CAPITAL HEALTH CENTER FOR ONCOLOGY capitalhealth.org/oncology Cancer can be a life altering illness. That s why the Capital Health Center for Oncology offers compassionate, personalized care led by a closely
CAPITAL HEALTH CENTER FOR ONCOLOGY capitalhealth.org/oncology Cancer can be a life altering illness. That s why the Capital Health Center for Oncology offers compassionate, personalized care led by a closely