Clinicopathological Diagnosis of Gliomatosis Cerebri
|
|
|
- Annice Perkins
- 6 years ago
- Views:
Transcription
1 20 Clinicopathological Diagnosis of Gliomatosis Cerebri Jiro Akimoto Department of Neurosurgery, Tokyo Medical University Japan 1. Introduction Regarding the definition of gliomatosis cerebri (hereinafter referred to as "GC"), the 3rd edition of the WHO Classification of Central Nervous System Tumors (hereinafter referred to as "3rd ed.") provides only a five-line description that GC is a diffuse, frequently bilateral, glioma that infiltrates the brain, involving more than two lobes. It often extends to the infratentorial structures and even to the spinal cord. Compared with this, the definition in its 4th edition (hereinafter referred to as "4th ed.") is described in 13 lines, stating that GC involves at least 3 lobes and is usually bilateral, extending from the cerebral white matter, including the deep and subcortical portions, and often infiltrating the brain stem and the spinal cord. In the 4th ed., GC is characterized by a widespread infiltration of the brain by tumor, occurring as bilateral lesions involving commissural fibers, and frequently infiltrating from the brain stem to the spinal cord. Moreover, the 4th ed. states that GC is mainly astrocytic tumor but, in some cases, mainly consists of oligodendroglial tumor cells (Akimoto, 2004; Balko, 1996; Levin, 2004; Sanson, 2004, Taillibert, 2006). Unlike the 3rd ed., which specifies the histological malignancy as Grade III, the 4th ed. rates it basically as Grade III, without specifying it, although recognizing the importance of the evaluation of histological malignancy, in consideration of the possibility that the grade may be underestimated in some cases due to tissue sampling problems (Akimoto, 2004; Nishioka, 1996). These changes in the description of the definition in the WHO Classification have reflected the findings of many clinicopathological researches on GC. This situation requires us neuro-oncologists to diagnose GC before operation and to provide appropriate treatment. In that sense, it is important to evaluate the extent of tumor progression by imaging diagnosis, mainly using MRI, and to perform adequate tissue sampling to enable accurate histopathological diagnosis, in accordance with the 4th ed. (Akimoto et al., 2004). In addition, it is important to establish a treatment protocol mainly consisting of adjunctive therapy. 2. Clinical cases (Table 1) We have encountered 8 cases in which GC was suspected based on the neuroradiological definition of the 4th ed. and was diagnosed pathologically. These cases aged 46 to 73 years (median age: 55.5 years) consisted of 3 men and 5 women. The initial symptoms were mainly cognitive impairment and seizure. The symptoms of ordinary brain tumor,
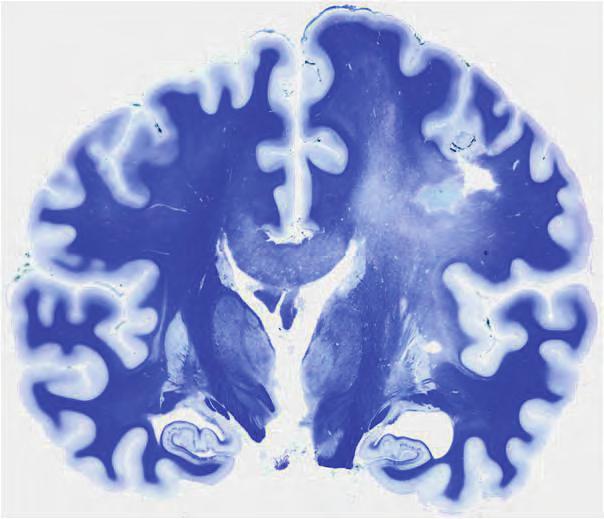
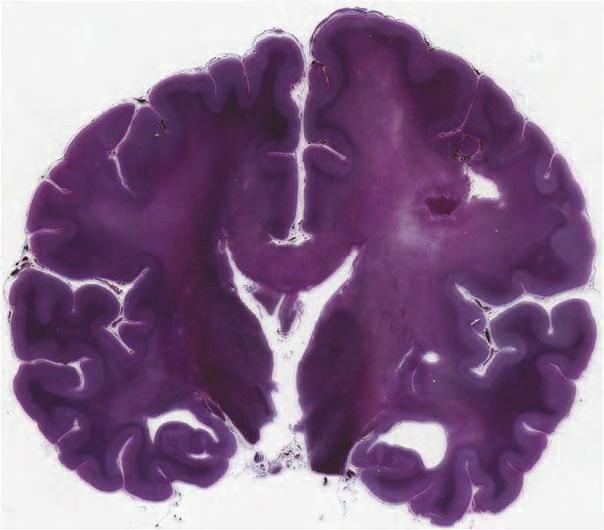
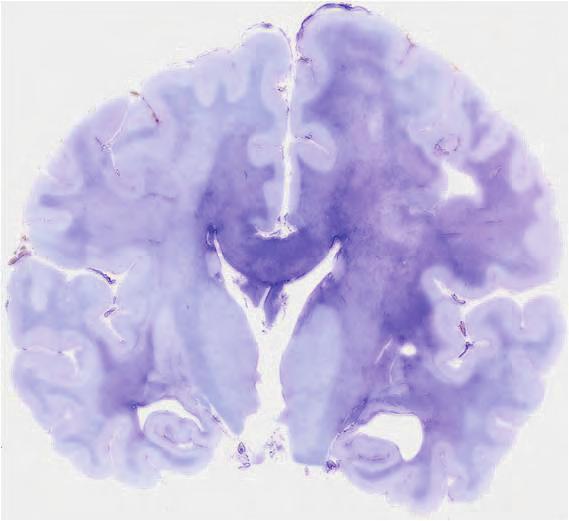
2 450 Management of CNS Tumors including increased intracranial pressure, as well as focal signs, including hemiparesis, were less frequent. The tumoral topography based on CT or MRI revealed that most of the lesions were diffused in the white matter, often extending to the basal ganglia, brain stem or cerebellum which is unlikely to be invaded by ordinary diffuse glioma. These lesions were characterized by bilateral progression accompanied by hypertrophy of the corpus callosum. Wide resection of tissue, including areas over the white matter and cortical regions, was considered preferable as the surgical procedure to obtain a reliable pathological diagnosis. Therefore, anterior temporal lobectomy and maximally possible tumor resection were performed. Pathological diagnosis was anaplastic astrocytoma (Grade III) in most of the cases. However, GC consisting of oligodendroglial tumor cells was found in 2 cases. Basic treatment was radiation therapy (30 Gy to whole brain and 30 Gy focal boost) combined with chemotherapy (ACNU, Temozolomide). Except for a patient who developed central brain herniation in the early phase after operation, patients receiving sufficient adjunctive therapy tended to maintain partial response or stable disease. 2.1 Case 2 A 46-year old woman. She was admitted with a 2-month history of clumsiness and numbness of the right hand as well as gradual development of disorientation and right hemiparesis. The head MRI on admission revealed a lesion arising primarily in the left corona radiata and extending to the right parietal lobe and frontal lobe white matter through the corpus callosum, showing no obvious contrast enhancement (Fig. 1 A-D). CT-guided stereotactic biopsy of the left frontal lobe white matter was performed to make a definite diagnosis. Infiltration of large cells with abundant cytoplasm and thick processes, suggestive of reactive astrocytes, was observed in the matrix of the edematous white matter. However, a diagnosis of neoplastic lesion was not reached. Triggered by status epileptics, her condition deteriorated. Two months after the operation, she died of brain herniation. Cerebral autopsy revealed a widespread edema over the region from the left corona radiata to the basal ganglia, further extending to the right frontal lobe and the temporal lobe white matter through the corpus callosum. KB staining, Bodian staining, Holtzer staining, etc. demonstrated the extent of the lesion (Fig. 2 A-D). The pathological features of each section showed infiltration of gemistocytic cells, forming parallel rows along the nerve fibers. Although lack of nuclear atypism was noted, most of the nuclei were MIB-1 positive. The degree of myelin destruction varied across sections, being the most severe in the corpus callosum. However, Bodian staining demonstrated that the involved axis cylinder was preserved even in the corpus callosum. (Fig. 2 E, F) The autopsy-based diagnosis was GC consisting of gemistocytic astrocytoma. 2.2 Case 8 A 47-year old women. She was admitted to the hospital because of having abrupt cognitive impairment 1 month previously and gradual development of ataxic gait and urinary incontinence thereafter. Head MRI showed a lesion with enlargement of the corpus callosum in the white matter of the bilateral frontal lobe. Although the lesion extended from the bilateral corona radiata to the white matter of the parietal lobe, no obvious contrast enhancement was observed (Fig. 3 A-D). The partial removal of the tumor was performed to
3 Clinicopathological Diagnosis of Gliomatosis Cerebri 451 Case Age/Sex Initial symptom Tumoral Topography Surgery Pathological Dx Treatment Prognosi s 1 54/ Male Headache, Depression White matter, Basal ganglia, Brain Stem, Cerebellum ATL Anaplastic oligodendroglioma RTx D: 2 months 2 46/ Female Disorientation, Heminumbne ss White matter, Basal ganglia, Corpus callosum Biopsy Gemistocytic astrocytoma None D: 2 weeks 3 71/ Female Seizure, Hemiparesis White matter, Corpus callosum Partial removal Glioblastoma none D: 8 months 4 50/ Female Seizure, Cognitive impairment White matter, Basal ganglia Biopsy Anaplastic astrocytoma RTx, Chemo Tx D: 26 months 5 66/ Male Cognitive impairment White matter, Corpus callosum Biopsy Anaplastic astrocytoma RTx, Chemo Tx A: 49 months 6 73/ Male Seizure White matter, Basal ganglia ATL Anaplastic astrocytoma RTx, Chemo Tx D: 4 months 7 57/ Female Cognitive impairment White matter, Basal ganglia ATL Anapalstic astrocytoma RTx, Chemo Tx D: 20 months 8 47/ Female Cognitive impairment White matter, Corpus callosum Partial removal Anaplastic oligodendroglio ma RTx, Chemo Tx A: 11 months ATL: anterior temporal lobectomy, RTx: radiation therapy, Chemo Tx: chemotherapy, D: dead, A: alive Table 1. Case summary
 demonstrated diffuse high intensity in the")


4 452 Management of CNS Tumors (a) (b) (c) (d) T2-weighted MRI (A, B) demonstrated diffuse high intensity in the white matter of both cerebral hemispheres, with enlargement of the corpus callosum. T1-weighted MRI with Gd-DTPA (C, D) demonstrated slightly low intensity in the white matter without enhancement. Fig. 1. MRI on admission (A-D)
5 Clinicopathological Diagnosis of Gliomatosis Cerebri 453 a b
6 454 Management of CNS Tumors c d

 demonstrated the broad area of reactive gliosis.")
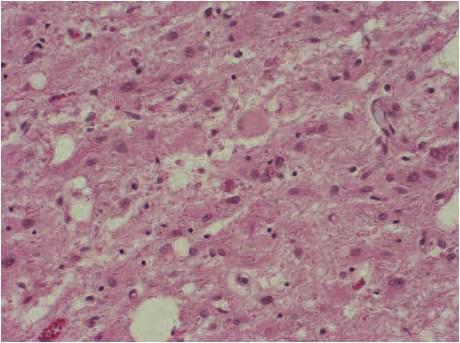
7 Clinicopathological Diagnosis of Gliomatosis Cerebri 455 e f Klüver-Barrera stain (A) demonstrated the affected region to be a broad region of myelin destruction extending from the white matter of the left parietal lobe to the basal ganglia and to the corpus callosum and in a part of the right hemisphere. Bodian stain (B) demonstrated the preservation of axons, but the intensity of staining of the white matter and corpus callosum was slightly decreased owing to edematous change. Holzer stain (C) demonstrated the broad area of reactive gliosis. The region showed increased atypical gemistocyte-like cells of various sizes and forms [D: hematoxylin and eosin (HE) stain, 100], Immunohistochemically, most tumor cells were positive for GFAP (E). Klüver-Barrera stain (F) showed extensive destruction of myelin. Fig. 2. Coronal section of the autopsy brain (A-C) and microscopic appearance of autopsy material (D-F)

 make a definite diagnosis showed a dense proliferation of tumor cells with round nuclei, scant cytoplasm and perinuclear")

8 456 Management of CNS Tumors (a) (b) (c) (d) FLAIR MRI (A, B) demonstrated diffuse high intensity in the white matter of both frontal lobe and bilateral corona radiata, with enlargement of the corpus callosum. T1-weighted with Gd-DTPA (C, D) demonstrated low intensity in the white matter of the left frontal lobe without enhancement. Fig. 3. MRI on admission (A-D) make a definite diagnosis showed a dense proliferation of tumor cells with round nuclei, scant cytoplasm and perinuclear halo in the left superior frontal gyrus. The perineuronal satellitosis-like infiltration of tumor cells was observed even in the deep layer of the cerebral cortex. Myelin was preserved although partially destroyed by tumor cell infiltration (Fig. 4 A, B). The tumor cells were found to be Olig-2 positive, and the proportion of MIB-1 positive patients was also high. As a result of analysis using

9 Clinicopathological Diagnosis of Gliomatosis Cerebri 457 fluorescence in situ hybridization (FISH), she was found to be positive for 1pLOH (1p36) and 19qLOH (19q36) (Fig. 4 C, D). Based on these results, she was diagnosed with GC consisting of anaplastic oligodendroglioma cells. After the operation, she underwent radiation therapy (60 Gy) combined with chemotherapy using oral temozolomide. At 11 months post-operative, a reduction in the lesion size was observed, with an improvement in cognitive function. a

10 458 Management of CNS Tumors b

11 Clinicopathological Diagnosis of Gliomatosis Cerebri 459 c
. Immunohistochemically, most tumor cells were positive for olig2 (C) and MIB-1 (D). Fig. 4.")
12 460 Management of CNS Tumors d The region showed increased atypical oligodendroglial cells of various sizes and forms (A: HE stain, 100). Luxol fast blue and HE stain showed extensive destruction of myelin (B, 100). Immunohistochemically, most tumor cells were positive for olig2 (C) and MIB-1 (D). Fig. 4. Microscopic appearance of resected tissue (A-D)
13 Clinicopathological Diagnosis of Gliomatosis Cerebri Discussion 3.1 Points to be noted in radiological diagnosis Based on the definition of the 4th ed., confirmation of the presence of bilateral lesions over at least 3 lobes as well as the absence of an obvious focal tumor mass is considered essential to make an imaging-based diagnosis of GC. In addition, detection of infiltration of the basal ganglia, brain stem, cerebellum and spinal cord lends more confidence to the imaging-based diagnosis of GC. In other words, GC is considered a pathological condition where great emphasis is placed only on the invasive potential among the two growth mechanisms of ordinary glioma, i.e., the proliferative potential and invasive potential (Akimoto, 2004; Peretti-Viton, 2002; Saraf-Lavi, 2003). According to one report (Sanson et al., 2004), factors determining the diagnosis of GC based on MRI are: (1) a high signal area over at least 3 lobes on T2-weighted and FLAIR images; (2) absence of a contrast-enhanced tumor mass of 1 cm or greater; and (3) thickening of the corpus callosum or anterior commissure. These factors are the criteria adopted in the 4th ed. Such a clear definition may make it possible to suspect the presence of GC by performing MRI. However, these imaging findings are also obtained in white matter lesions other than tumors, such as demyelinating disease, encephalitis and venous sinus thrombosis (Essig, 2001; Saraf-Lavi, 2003). Therefore, it becomes necessary to confirm the presence of tumor cells by histological diagnosis. In recent years, studies evaluating GC by MR spectroscopy have been published (Bendszus, 2000; Galanaud, 2003; Saraf-Lavi, 2003). According to these studies, increased choline and decreased NAA levels, which are findings characteristic of glioma, are not necessarily observed in GC, but rather increased NAA levels are often observed. Increased myoinositol (m-ins), which indicates increased activity of glia cells, has been reported as a finding characteristic of GC. Although the 4th ed. only states that multivoxel MRS is useful for determining the target of biopsy, it appears that biopsy of the sites with increased choline or m-ins levels lends more confidence to the histological diagnosis of GC. 3.2 Points to be noted in pathological diagnosis It is important to be faithful to the criteria for the pathological diagnosis of GC (Scheinker & Evans, 1943). More specifically, GC is basically defined as an invasive and tumoral lesion, with no tumor mass centered in the white matter, and the axis cylinder is preserved even when myelin destruction takes place (Akimoto, 2004; Peretto-Viton, 2002; Vates, 2003). To thoroughly carry out these evaluations, stereotactic biopsy sampling is often difficult. We previously reported the need to remove, as much as possible, the cerebral lobes with lesions detectable by imaging (Akimoto, 2004). In other words, not only the evaluation of tumor cells but also the evaluation of normal tissue is necessary for making the pathological diagnosis of GC. The cases presented in this article demonstrate the significance of the additional response evaluation for myelin by KB staining, axis cylinder by Bodian staining and reactive glia by Holtzer staining. The evaluation of tumor cells infiltrating between normal nerve fibers is by no means easy. In addition, the shape of the nuclei varies greatly from elongated-form or fusiform to round-form, and no consistency is found regarding the presence or absence of atypical cells. In fact, there are some reports on cases of GC consisting of oligodendroglioma-like cells, as shown in Case 8 (Akimoto, 2004; Balko, 1996; Benjelloun, 2001; Sanson, 2004; Vates, 2003). Confirmation of the preservation of the axonal structure after evaluation of the proliferative potential of infiltrating cells by MIB-1 and
14 462 Management of CNS Tumors AgNORs can contribute to the diagnosis of GC (Akimoto, 2004). In the 4th ed., the range of MIB-1 index is specified to be from not more than 1% to 30%, which is difficult to understand. However, it is also the fact that objective calculation of MIB-1 index is extremely difficult in tissues containing responsive glia cells due to normal tissue infiltration (Akimoto, 2004; Nishioka, 1996; Vates, 2003). Therefore, we consider it useful to evaluate the proliferative potential of each cell by AgNORs. However, there have only been two case reports on AgNORs in GC(Hara et al., 1991). A recent study has reported that L1, which is a cell adhesion factor, is expressed more abundantly in GC than in ordinary glioma (Suzuki et al., 2010). Since L1 is a glycoprotein that plays an important role in the migration of the immature neurons in the development stage, L1 might be significantly involved in the invasive potential of GC. In addition, it was reported that the control of L1-functions might contribute to the treatment of GC. Moreover, according to a study (Seiz et al., 2005) evaluating the mutation of IDH1 in GC, the frequency of IDH1 mutations is relatively high in the secondary GC, caused by the progression of diffuse astrocytoma, whereas no IDH1 mutation was observed in primary GC. This suggests the possibility that the evaluation of IDH1 mutations may become important for making the diagnosis of GC, as suggested in the molecular analysis of the development of glioblastoma. 3.3 Topics regarding treatment According to the 3rd ed., GC has extremely poor prognosis, and 1-, 2- and 3-year survival rates are 48%, 37% and 27%, respectively, being similar to those in glioblastoma. The 3rd ed. specifies only MIB-1 as a prognostic factor. However, the 4th ed. is not intended to provide data, and states only that age, performance status and histological features, especially for grade and subtype (oligodendroglioma), are important as prognostic factors. The deletion of the description on MIB-1 suggests the difficulty of the evaluation (Akimoto, 2004; Nishioka, 1996; Vates, 2003). There are many reports discussing the extremely poor prognosis of GC (Taillibert, 2006; Vates, 2003). However, recent studies have reported some cases with relatively better prognosis due to greater sensitivity to adjuvant therapy (Levin, 2004; Sanson, 2004; Taillibert, 2006). Of these, one report (Taillibert et al., 2006) summarizing 296 cases from the literature showed that the overall survival (OS) in GC was 14.5 months. Examined for each prognostic factor, OS was 27 months and 9 months in KPS of 80 and 80, respectively, and 20 months and 8.5 months in Grade 2 and 4, respectively, showing significant differences. However, no significant difference was observed between cases with and without radiation therapy, and there was a trend for prolonged OS in patients receiving additional chemotherapy. The most noteworthy was the difference between cases of astrocytic tumor and oligodendroglial tumor: the OS was 11 months for the former and 36 months for the latter, showing a marked difference. Moreover, one study reported (Levin et al., 2004) that, in the use of temozolomide (TMZ), which is regarded as the standard treatment for ordinary glioma, the response rate was 45%, the median TTP to time to progression (TTP) was 13 months, with 1- and 2-year progression-free survival (PFS) rates of 55% and 23%, respectively. In another study (Sanson et al., 2004) where PCV and TMZ were used as first-line treatment in the 63 cases they encountered, no significant difference was observed in the response rate between the two treatment groups. In the study, no significant differences were observed in PFS and OS between patients stratified by age, tumor grade, KPS, etc.
15 Clinicopathological Diagnosis of Gliomatosis Cerebri 463 However, in GC consisting of oligodendroglial tumor cells, significantly better responses were observed in both PFS and OS, with PFS of 21.2 months and OS of 33.9 months. Therefore, also for the treatment of GC, it is considered important to determine 1p, 19qLOH and the methylation status of MGMT by adequate tissue sampling in GC, for additional evaluation of the sensitivity to chemotherapy. 4. Conclusion In terms of diagnosis, we are focusing on the application of chemical shift imaging MR spectroscopy with m-ins, application of in vivo imaging technique using L1 and integrin as markers, and accurate detection of oligodendroglial GC by adequate tissue sampling and detailed evaluations of pathological morphology and gene mutations. In terms of treatment, focus is being placed on the evaluation of sensitivity to chemotherapy and the establishment of a treatment protocol for TMZ. The algorithm from the diagnosis of GC to treatment, we propose currently, is shown in Table 2. The pathological conditions for the diagnosis of GC have been specified in the 4th ed., but GC is still stated as an orphan disease. We believe that a multicenter study on the treatment of patients definitely diagnosed as having GC should be started. Table 2. Proposed algorithm of the management of gliomatosis cerebri
16 464 Management of CNS Tumors 5. References Akimoto J, Nishioka H, Miki T et al: Clinical diagnosis of gliomatosis cerebri. Brain Tumor Pathology 21, 87-95, 2004 Balko MG, Brisard KS, Samaha FJ: Oligodendoglial gliomatosis cerebri. Br J Neurosurg 10, , 1996 Bendszus M, Warmuth-Metz M, Klein R et al: MR spectroscopy in gliomatosis cerebri. Am J Neuroradiol 21, , 2000 Benjelloun A, Delavelle J, Lazeyras F et al: Possible efficacy of temozolomide in a patient with gliomatosis cerebri. Neurol 57, , 2001 Essig M, Schlemmer HP, Tronnier V et al: Fluid-attenuated inversion recovery MR imaging of gliomatosis cerebri. Eur Radiol 11, , 2001 Galanaud D, Chinot O, Nicoli F et al: Use of proton magnetic resonance spectroscopy of thebrain to differentiate gliomatosis cerebri from low-grade glioma. J Neurosurg 98, ,2003 Hara A, Sakai N, Yamada H et al: Assessment of proliferative potential in gliomatosis cerebri. JNeurol 238, 80-82, 1991 Levin N, Gomori JM, Siegal T: Chemotherapy as initial treatment in gliomatosis cerebri. Neurol 63, , 2004 Nishioka H, Ito H, Miki T et al: Difficulties in the antemorten diagnosis of gliomatosis cerebri. Br J Neurosurg 10, , 1996 Peretti-Viton P, Brunel H, Chinot O et al: Histological and MR correlation in gliomatosis cerebri. J Neurooncol 59, , 2002 Sanson M, Caralat-Carel S, Taillibert M et al: Initial chemotherapy in gliomatosis cerebri. Neurol 63, , 2004 Saraf-Lavi E, Bowen BC, Pattany PM et al: Proton MR spectroscopy of gliomatosis cerebri: Case report of elevated myoinositol with normal choline levels. Am J Neuroradiol 24, , 2003 Seiz M, Tuettenberg J, Meyer J et al.: Detection of IDI1 mutations in gliomatosis cerebri, but only in tumors with additional solid component: evidence for molecular subtypes.acta Neuropathol 2010, 120: Scheinker IM, Evans JP: Diffuse cerebral glioblastomatosis. J Neuropathol Exp Neurol 2, , 1943 Suzuki T, Izumoto S, Fujimoto Y et al: Clinicopathological study of cellular proliferation and invasion in gliomatosis cerebri: important role of neural cell adhesion molecule L1 in tumour invasion. J Clin Pathol 58, , 2005 Taillibert S, Chodkiewitcz C, Laigle-Donadey F et al: Gliomatosis cerebri: a review of 296 cases from the ANOCEF database and the literature. J Neurooncol 76, , 2006 Vates GE, Chang S, Lamborn KR et al: Gliomatosis cerebri. A review of 22 cases. Neurosurg 53, , 2003
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative
 is a progressive neurodegenerative") ORIGINAL RESEARCH E. Matsusue S. Sugihara S. Fujii T. Kinoshita T. Nakano E. Ohama T. Ogawa Cerebral Cortical and White Matter Lesions in Amyotrophic Lateral Sclerosis with Dementia: Correlation with MR
ORIGINAL RESEARCH E. Matsusue S. Sugihara S. Fujii T. Kinoshita T. Nakano E. Ohama T. Ogawa Cerebral Cortical and White Matter Lesions in Amyotrophic Lateral Sclerosis with Dementia: Correlation with MR
Five Most Common Problems in Surgical Neuropathology
 Five Most Common Problems in Surgical Neuropathology If the brain were so simple that we could understand it, we would be so simple that we couldn t Emerson Pugh What is your greatest difficulty in neuropathology?
Five Most Common Problems in Surgical Neuropathology If the brain were so simple that we could understand it, we would be so simple that we couldn t Emerson Pugh What is your greatest difficulty in neuropathology?
Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to.
 Stratified Medicine Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to. Looking in detail at cancer cells and their genetic make up. Permit
Stratified Medicine Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to. Looking in detail at cancer cells and their genetic make up. Permit
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준. KNS-MT-03 (April 15, 2015)
") 성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
Gliomatosis Cerebri: Imaging Findings on Traditional and Advanced Techniques
 Gliomatosis Cerebri: Imaging Findings on Traditional and Advanced Techniques Poster No.: C-1464 Congress: ECR 2015 Type: Educational Exhibit Authors: L. M. Cruz Hernandez, I. Herrera, A. L. Reyes Ortiz,
Gliomatosis Cerebri: Imaging Findings on Traditional and Advanced Techniques Poster No.: C-1464 Congress: ECR 2015 Type: Educational Exhibit Authors: L. M. Cruz Hernandez, I. Herrera, A. L. Reyes Ortiz,
Tumors of the Nervous System
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
General: Brain tumors are lesions that have mass effect distorting the normal tissue and often result in increased intracranial pressure.
 1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
MOLECULAR DIAGNOSTICS OF GLIOMAS
 MOLECULAR DIAGNOSTICS OF GLIOMAS Arie Perry, M.D. Director, Neuropathology Division DIFFUSE GLIOMAS Cell types Astrocytomas (A) Oligodendrogliomas (O) Mixed oligoastrocytoma (MOA) Three WHO grades: II,
MOLECULAR DIAGNOSTICS OF GLIOMAS Arie Perry, M.D. Director, Neuropathology Division DIFFUSE GLIOMAS Cell types Astrocytomas (A) Oligodendrogliomas (O) Mixed oligoastrocytoma (MOA) Three WHO grades: II,
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES
 MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
Primary Central Nervous System Lymphoma with Lateral Ventricle Involvement
 The Open Medical Imaging Journal, 2012, 6, 103-107 103 Open Access Primary Central Nervous System Lymphoma with Lateral Ventricle Involvement Yumi Oie 1,*, Kazuhiro Murayama 1, Shinya Nagahisa 2, Masato
The Open Medical Imaging Journal, 2012, 6, 103-107 103 Open Access Primary Central Nervous System Lymphoma with Lateral Ventricle Involvement Yumi Oie 1,*, Kazuhiro Murayama 1, Shinya Nagahisa 2, Masato
Radioterapia no Tratamento dos Gliomas de Baixo Grau
 Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Assessment of Gliomatosis Cerebri
 MRS of Gliomatosis Cerebri Neuroradiology Original Research Juan A. Guzmán-de-Villoria 1 Javier Sánchez-González 2 Lucia Muñoz 1 Santiago Reig 2 Carlos Benito 3 Pedro García-Barreno 2 Manuel Desco 2 Guzmán-de-Villoria
MRS of Gliomatosis Cerebri Neuroradiology Original Research Juan A. Guzmán-de-Villoria 1 Javier Sánchez-González 2 Lucia Muñoz 1 Santiago Reig 2 Carlos Benito 3 Pedro García-Barreno 2 Manuel Desco 2 Guzmán-de-Villoria
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
Anaplastic Pilocytic Astrocytoma: The fusion of good and bad
 Anaplastic Pilocytic Astrocytoma: The fusion of good and bad Alexandrina Nikova 1, Charalampos-Chrysovalantis Chytoudis-Peroudis 2, Penelope Korkolopoulou 3 and Dimitrios Kanakis 4 Abstract 5 Pilocytic
Anaplastic Pilocytic Astrocytoma: The fusion of good and bad Alexandrina Nikova 1, Charalampos-Chrysovalantis Chytoudis-Peroudis 2, Penelope Korkolopoulou 3 and Dimitrios Kanakis 4 Abstract 5 Pilocytic
Pathologic Analysis of CNS Surgical Specimens
 2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
General Identification. Name: 江 X X Age: 29 y/o Gender: Male Height:172cm, Weight: 65kg Date of admission:95/09/27
 General Identification Name: 江 X X Age: 29 y/o Gender: Male Height:172cm, Weight: 65kg Date of admission:95/09/27 Chief Complaint Sudden onset of seizure for several minutes Present illness This 29-year
General Identification Name: 江 X X Age: 29 y/o Gender: Male Height:172cm, Weight: 65kg Date of admission:95/09/27 Chief Complaint Sudden onset of seizure for several minutes Present illness This 29-year
Zurich Open Repository and Archive. Procarbazine and CCNU as initial treatment in gliomatosis cerebri
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2008 Procarbazine and CCNU as initial treatment in gliomatosis cerebri Glas, M;
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2008 Procarbazine and CCNU as initial treatment in gliomatosis cerebri Glas, M;
1 MS Lesions in T2-Weighted Images
 1 MS Lesions in T2-Weighted Images M.A. Sahraian, E.-W. Radue 1.1 Introduction Multiple hyperintense lesions on T2- and PDweighted sequences are the characteristic magnetic resonance imaging (MRI) appearance
1 MS Lesions in T2-Weighted Images M.A. Sahraian, E.-W. Radue 1.1 Introduction Multiple hyperintense lesions on T2- and PDweighted sequences are the characteristic magnetic resonance imaging (MRI) appearance
Chapter 1 Introduction
 Chapter 1 Introduction Men think epilepsy divine, merely because they do not understand it. But if they called everything divine which they do not understand, why, there would be no end to divine things.
Chapter 1 Introduction Men think epilepsy divine, merely because they do not understand it. But if they called everything divine which they do not understand, why, there would be no end to divine things.
CNS SESSION 3/8/ th Multidisciplinary Management of Cancers: A Case based Approach
 CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
Systemic Treatment. Third International Neuro-Oncology Course. 23 May 2014
 Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
CS Tumor Size CS Extension CS Tumor Size/Ext Eval CS Lymph Nodes CS Lymph Nodes Eval Reg LN Pos Reg LN Exam CS Mets at DX CS Mets Eval
 C70.0, C71.0-C71.9 C70.0 Cerebral meninges C71.0 Cerebrum C71.1 Frontal lobe C71.2 Temporal lobe C71.3 Parietal lobe C71.4 Occipital lobe C71.5 Ventricle, NOS C71.6 Cerebellum, NOS C71.7 Brain stem C71.8
C70.0, C71.0-C71.9 C70.0 Cerebral meninges C71.0 Cerebrum C71.1 Frontal lobe C71.2 Temporal lobe C71.3 Parietal lobe C71.4 Occipital lobe C71.5 Ventricle, NOS C71.6 Cerebellum, NOS C71.7 Brain stem C71.8
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS
 UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
Neuropathology Evening Session: Case 3
 Neuropathology Evening Session: Case 3 Christine E. Fuller, MD Cincinnati Children s Hospital Medical Center Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position
Neuropathology Evening Session: Case 3 Christine E. Fuller, MD Cincinnati Children s Hospital Medical Center Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position
ADSS Case 1. A 31-year-old male with a seizure. Se-Hoon Kim
 ADSS Case 1 A 31-year-old male with a seizure Se-Hoon Kim Department of Pathology, Yonsei University College of Medicine, Severance Hospital, Seoul, Korea A 31-year-old male patient without specific medical
ADSS Case 1 A 31-year-old male with a seizure Se-Hoon Kim Department of Pathology, Yonsei University College of Medicine, Severance Hospital, Seoul, Korea A 31-year-old male patient without specific medical
SURGICAL MANAGEMENT OF BRAIN TUMORS
 SURGICAL MANAGEMENT OF BRAIN TUMORS LIGIA TATARANU, MD, Ph D NEUROSURGICAL CLINIC, BAGDASAR ARSENI CLINICAL HOSPITAL BUCHAREST, ROMANIA SURGICAL INDICATIONS CONFIRMING HISTOLOGIC DIAGNOSIS REDUCING TUMOR
SURGICAL MANAGEMENT OF BRAIN TUMORS LIGIA TATARANU, MD, Ph D NEUROSURGICAL CLINIC, BAGDASAR ARSENI CLINICAL HOSPITAL BUCHAREST, ROMANIA SURGICAL INDICATIONS CONFIRMING HISTOLOGIC DIAGNOSIS REDUCING TUMOR
Sawada J, Orimoto R, Misu T, Katayama T, Aizawa H, Asanome A, Takahashi K, Saito T, Anei R, Kamada K, Miyokawa N, Takahashi T, Fujihara K, Hasebe N.
 Mult Scler (2014.9) 20(10):1413-1416. A case of pathology-proven neuromyelitis optica spectrum disorder with Sjögren syndrome manifesting aphasia and apraxia due to a localized cerebral white matter lesion.
Mult Scler (2014.9) 20(10):1413-1416. A case of pathology-proven neuromyelitis optica spectrum disorder with Sjögren syndrome manifesting aphasia and apraxia due to a localized cerebral white matter lesion.
Understanding general brain tumor pathology, Part I: The basics. Craig Horbinski, M.D., Ph.D. Department of Pathology University of Kentucky
 Understanding general brain tumor pathology, Part I: The basics Craig Horbinski, M.D., Ph.D. Department of Pathology University of Kentucky plan of attack what IS a pathologist, anyway? what s so special
Understanding general brain tumor pathology, Part I: The basics Craig Horbinski, M.D., Ph.D. Department of Pathology University of Kentucky plan of attack what IS a pathologist, anyway? what s so special
The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas
 The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas Stefan Prokop, MD Neuropathology Fellow Hospital of the University of Pennsylvania Background
The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas Stefan Prokop, MD Neuropathology Fellow Hospital of the University of Pennsylvania Background
Oligodendrogliomas & Oligoastrocytomas
 Oligodendrogliomas & Oligoastrocytomas ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization dedicated solely
Oligodendrogliomas & Oligoastrocytomas ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization dedicated solely
Tumors of the Central Nervous System
 Tumors of the Central Nervous System 1 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Introduction General: Brain tumors are lesions that have mass effect
Tumors of the Central Nervous System 1 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Introduction General: Brain tumors are lesions that have mass effect
2017 Diagnostic Slide Session Case 3
 2017 Diagnostic Slide Session Case 3 Andrew Gao, MD Lili-Naz Hazrati, MD, PhD Cynthia Hawkins, MD, PhD Hospital for Sick Children and University of Toronto, Toronto, Canada Disclosures: none Clinical History
2017 Diagnostic Slide Session Case 3 Andrew Gao, MD Lili-Naz Hazrati, MD, PhD Cynthia Hawkins, MD, PhD Hospital for Sick Children and University of Toronto, Toronto, Canada Disclosures: none Clinical History
Peter Canoll MD. PhD.
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
21/03/2017. Disclosure. Practice Changing Articles in Neuro Oncology for 2016/17. Gliomas. Objectives. Gliomas. No conflicts to declare
 Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
CNS TUMORS. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
Diffusion-Weighted and Conventional MR Imaging Findings of Neuroaxonal Dystrophy
 AJNR Am J Neuroradiol 25:1269 1273, August 2004 Diffusion-Weighted and Conventional MR Imaging Findings of Neuroaxonal Dystrophy R. Nuri Sener BACKGROUND AND PURPOSE: Neuroaxonal dystrophy is a rare progressive
AJNR Am J Neuroradiol 25:1269 1273, August 2004 Diffusion-Weighted and Conventional MR Imaging Findings of Neuroaxonal Dystrophy R. Nuri Sener BACKGROUND AND PURPOSE: Neuroaxonal dystrophy is a rare progressive
Imaging for suspected glioma
 Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Site Specific Coding Rules MALIGNANT CENTRAL NERVOUS SYSTEM TUMORS
 Multiple Primary and Histology Site Specific Coding Rules MALIGNANT CENTRAL NERVOUS SYSTEM TUMORS 1 Prerequisites 2 Completion of Multiple Primary and Histology General Coding Rules 3 There are many ways
Multiple Primary and Histology Site Specific Coding Rules MALIGNANT CENTRAL NERVOUS SYSTEM TUMORS 1 Prerequisites 2 Completion of Multiple Primary and Histology General Coding Rules 3 There are many ways
Q&A. Fabulous Prizes. Collecting Cancer Data:CNS 2/7/12. NAACCR Webinar Series Collecting Cancer Data Central Nervous System
 Collecting Cancer Data Central Nervous System NAACCR 2012 2013 Webinar Series 2/7/2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data Central Nervous System NAACCR 2012 2013 Webinar Series 2/7/2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Helpful Information for evaluation of new neurological symptoms in patients receiving TYSABRI
 Helpful Information for evaluation of new neurological symptoms in patients receiving TYSABRI This information is provided as an educational resource for healthcare providers and should be considered current
Helpful Information for evaluation of new neurological symptoms in patients receiving TYSABRI This information is provided as an educational resource for healthcare providers and should be considered current
CT and MR findings of systemic lupus erythematosus involving the brain: Differential diagnosis based on lesion distribution
 CT and MR findings of systemic lupus erythematosus involving the brain: Differential diagnosis based on lesion distribution Poster No.: C-2723 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro
CT and MR findings of systemic lupus erythematosus involving the brain: Differential diagnosis based on lesion distribution Poster No.: C-2723 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro
FUNCTIONAL MAGNETIC RESONANCE IMAGING IN FOLLOW-UP OF CEREBRAL GLIAL TUMORS
 Anvita Bieza FUNCTIONAL MAGNETIC RESONANCE IMAGING IN FOLLOW-UP OF CEREBRAL GLIAL TUMORS Summary of Doctoral Thesis to obtain PhD degree in medicine Specialty Diagnostic Radiology Riga, 2013 Doctoral thesis
Anvita Bieza FUNCTIONAL MAGNETIC RESONANCE IMAGING IN FOLLOW-UP OF CEREBRAL GLIAL TUMORS Summary of Doctoral Thesis to obtain PhD degree in medicine Specialty Diagnostic Radiology Riga, 2013 Doctoral thesis
NACC Vascular Consortium. NACC Vascular Consortium. NACC Vascular Consortium
 NACC Vascular Consortium NACC Vascular Consortium Participating centers: Oregon Health and Science University ADC Rush University ADC Mount Sinai School of Medicine ADC Boston University ADC In consultation
NACC Vascular Consortium NACC Vascular Consortium Participating centers: Oregon Health and Science University ADC Rush University ADC Mount Sinai School of Medicine ADC Boston University ADC In consultation
Gross Organization I The Brain. Reading: BCP Chapter 7
 Gross Organization I The Brain Reading: BCP Chapter 7 Layout of the Nervous System Central Nervous System (CNS) Located inside of bone Includes the brain (in the skull) and the spinal cord (in the backbone)
Gross Organization I The Brain Reading: BCP Chapter 7 Layout of the Nervous System Central Nervous System (CNS) Located inside of bone Includes the brain (in the skull) and the spinal cord (in the backbone)
American Journal of. Medical Case Reports. CAM5.2 Expression in Metastatic Tumours of CNS: A Diagnostic Tool
 American Journal of American Journals of Medical Case Reports http://ivyunion.org/index.php/ajmcr/index Medical Case Reports Mathur SK et al. American Journal of Medical Case Reports 2014, 2:1-8 Vol 2,
American Journal of American Journals of Medical Case Reports http://ivyunion.org/index.php/ajmcr/index Medical Case Reports Mathur SK et al. American Journal of Medical Case Reports 2014, 2:1-8 Vol 2,
Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma
 AJNR Am J Neuroradiol 23:243 247, February 2002 Case Report Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma John D. Port, Daniel J. Brat, Peter C. Burger, and Martin G.
AJNR Am J Neuroradiol 23:243 247, February 2002 Case Report Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma John D. Port, Daniel J. Brat, Peter C. Burger, and Martin G.
THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION. Mustafa Rashid Issa
 THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION Mustafa Rashid Issa ABSTRACT: Illustrate malignant tumors that form either in the brain or in the nerves originating in the brain.
THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION Mustafa Rashid Issa ABSTRACT: Illustrate malignant tumors that form either in the brain or in the nerves originating in the brain.
Supratentorial Gangliocytoma Mimicking Extra-axial Tumor: A Report of Two Cases
 Supratentorial Gangliocytoma Mimicking Extra-axial Tumor: A Report of Two Cases Ho Sung Kim, MD 1 Ho Kyu Lee, MD 1 Ae Kyung Jeong, MD 1 Ji Hoon Shin, MD 1 Choong Gon Choi, MD 1 Shin Kwang Khang, MD 2 We
Supratentorial Gangliocytoma Mimicking Extra-axial Tumor: A Report of Two Cases Ho Sung Kim, MD 1 Ho Kyu Lee, MD 1 Ae Kyung Jeong, MD 1 Ji Hoon Shin, MD 1 Choong Gon Choi, MD 1 Shin Kwang Khang, MD 2 We
AMERICAN BRAIN TUMOR ASSOCIATION. Oligodendroglioma and Oligoastrocytoma
 AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Carrera J-P, Forrester N, Wang E, et al. Eastern equine encephalitis
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Carrera J-P, Forrester N, Wang E, et al. Eastern equine encephalitis
Histopathological Study and Categorisation of Brain Tumors
 Histopathological Study and Categorisation of Brain Tumors Ruchira Wadhwa 1*, Purvi Patel 2, Hansa Goswami 3 1 Third Year Resident, 2 Assistant Professor, 3 Professor and Head, Department of Pathology,
Histopathological Study and Categorisation of Brain Tumors Ruchira Wadhwa 1*, Purvi Patel 2, Hansa Goswami 3 1 Third Year Resident, 2 Assistant Professor, 3 Professor and Head, Department of Pathology,
CHINESE MEDICAL ASSOCIATION
 Zhu et al. Chinese Neurosurgical Journal (2017) 3:22 DOI 10.1186/s41016-017-0087-2 CHINESE NEUROSURGICAL SOCIETY CASE REPORT CHINESE MEDICAL ASSOCIATION Anaplastic pleomorphic xanthoastrocytoma with disseminated
Zhu et al. Chinese Neurosurgical Journal (2017) 3:22 DOI 10.1186/s41016-017-0087-2 CHINESE NEUROSURGICAL SOCIETY CASE REPORT CHINESE MEDICAL ASSOCIATION Anaplastic pleomorphic xanthoastrocytoma with disseminated
Structural and functional imaging for the characterization of CNS lymphomas
 Structural and functional imaging for the characterization of CNS lymphomas Cristina Besada Introduction A few decades ago, Primary Central Nervous System Lymphoma (PCNSL) was considered as an extremely
Structural and functional imaging for the characterization of CNS lymphomas Cristina Besada Introduction A few decades ago, Primary Central Nervous System Lymphoma (PCNSL) was considered as an extremely
LOW GRADE ASTROCYTOMAS
 LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas
 MOLECULAR AND CLINICAL ONCOLOGY 3: 909-913, 2015 Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas HIROSHI KAWAJI, TSUTOMU TOKUYAMA, TOMOHIRO YAMASAKI,
MOLECULAR AND CLINICAL ONCOLOGY 3: 909-913, 2015 Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas HIROSHI KAWAJI, TSUTOMU TOKUYAMA, TOMOHIRO YAMASAKI,
Corporate Medical Policy
 Corporate Medical Policy Analysis of MGMT Promoter Methylation in Malignant Gliomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: analysis_of_mgmt_promoter_methylation_in_malignant_gliomas
Corporate Medical Policy Analysis of MGMT Promoter Methylation in Malignant Gliomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: analysis_of_mgmt_promoter_methylation_in_malignant_gliomas
Gliomas in the 2016 WHO Classification of CNS Tumors
 Gliomas in the 2016 WHO Classification of CNS Tumors Hindi N Al-Hindi, MD, FCAP Consultant Neuropathologist and Head Section of Anatomic Pathology Department of Pathology and Laboratory Medicine King Faisal
Gliomas in the 2016 WHO Classification of CNS Tumors Hindi N Al-Hindi, MD, FCAP Consultant Neuropathologist and Head Section of Anatomic Pathology Department of Pathology and Laboratory Medicine King Faisal
Masses of the Corpus Callosum
 Masses of the Corpus Callosum Kesav Raghavan, HMS Year III Dr. Agenda Corpus Callosum Development and Anatomy Our Patient: Clinical Presentation Differential Diagnosis of Masses in the Corpus Callosum
Masses of the Corpus Callosum Kesav Raghavan, HMS Year III Dr. Agenda Corpus Callosum Development and Anatomy Our Patient: Clinical Presentation Differential Diagnosis of Masses in the Corpus Callosum
A case of multinodular high-grade neuroepithelial tumor
 Brain Tumor Pathol (2011) 28:253 257 DOI 10.1007/s10014-011-0032-6 CASE REPORT A case of multinodular high-grade neuroepithelial tumor with ependymal differentiation Kensaku Kamada Yuko Tanaka Takayuki
Brain Tumor Pathol (2011) 28:253 257 DOI 10.1007/s10014-011-0032-6 CASE REPORT A case of multinodular high-grade neuroepithelial tumor with ependymal differentiation Kensaku Kamada Yuko Tanaka Takayuki
Overview of the Nervous System (some basic concepts) Steven McLoon Department of Neuroscience University of Minnesota
 Steven McLoon Department of Neuroscience University of Minnesota") Overview of the Nervous System (some basic concepts) Steven McLoon Department of Neuroscience University of Minnesota 1 Coffee Hour Tuesday (Sept 11) 10:00-11:00am Friday (Sept 14) 8:30-9:30am Surdyk s
Overview of the Nervous System (some basic concepts) Steven McLoon Department of Neuroscience University of Minnesota 1 Coffee Hour Tuesday (Sept 11) 10:00-11:00am Friday (Sept 14) 8:30-9:30am Surdyk s
Clinical Manifestations and Imaging Characteristics of Gliomatosis Cerebri with Pathological Confirmation
 RESEARCH ARTICLE Clinical Manifestations and Imaging Characteristics of Gliomatosis Cerebri with Pathological Confirmation Chun-Pu Zhang 1, Hua-Qing Li 2, Wei-Tao Zhang 3, Ming-Hui Liu 4 *, Wen-Jing Pan
RESEARCH ARTICLE Clinical Manifestations and Imaging Characteristics of Gliomatosis Cerebri with Pathological Confirmation Chun-Pu Zhang 1, Hua-Qing Li 2, Wei-Tao Zhang 3, Ming-Hui Liu 4 *, Wen-Jing Pan
Pediatric Brain Tumors: Updates in Treatment and Care
 Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
Contemporary Management of Glioblastoma
 Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls. Rob Macaulay Neuropathologist, MCC October 21, 2017
 Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
MRI and CT of the CNS
 MRI and CT of the CNS Dr.Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Computed Tomography CT is used for the detection of intracranial lesions. CT relies
MRI and CT of the CNS Dr.Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Computed Tomography CT is used for the detection of intracranial lesions. CT relies
Leah Militello, class of 2018
 Leah Militello, class of 2018 Objectives 1. Describe the general organization of cerebral hemispheres. 2. Describe the locations and features of the different functional areas of cortex. 3. Understand
Leah Militello, class of 2018 Objectives 1. Describe the general organization of cerebral hemispheres. 2. Describe the locations and features of the different functional areas of cortex. 3. Understand
Meningeal carcinomatosis presenting with leukoencephalopathylike imaging findings
 Accepted Manuscript Meningeal carcinomatosis presenting with leukoencephalopathylike imaging findings Hiroshi Tsuji, Shioya Ayako, Norio Takayashiki, Toshiyuki Irie, Satoshi Itoi, Taisuke Kodama, Yuki
Accepted Manuscript Meningeal carcinomatosis presenting with leukoencephalopathylike imaging findings Hiroshi Tsuji, Shioya Ayako, Norio Takayashiki, Toshiyuki Irie, Satoshi Itoi, Taisuke Kodama, Yuki
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Cerebrovascular diseases-2
 Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
PROPOSED/DRAFT Local Coverage Determination (LCD): MolDX: Chromosome 1p/19q deletion analysis (DL36483)
: MolDX: Chromosome 1p/19q deletion analysis (DL36483)") moldx: Chromosome 1p/19q deletion analysis (DL36483) Page 1 of 8 PROPOSED/DRAFT Local Coverage Determination (LCD): MolDX: Chromosome 1p/19q deletion analysis (DL36483) Close Section Navigation
moldx: Chromosome 1p/19q deletion analysis (DL36483) Page 1 of 8 PROPOSED/DRAFT Local Coverage Determination (LCD): MolDX: Chromosome 1p/19q deletion analysis (DL36483) Close Section Navigation
Accuracy of intra-operative rapid diagnosis by Squash smear in CNS lesions An early institutional experience. KK Bansal,
 Accuracy of intra-operative rapid diagnosis by Squash smear in CNS lesions An early institutional experience. KK Bansal, Monika Bansal, Sanjeev Kishore, Anuradha K, Meena H, Dushyant G. Department of Neurosurgery
Accuracy of intra-operative rapid diagnosis by Squash smear in CNS lesions An early institutional experience. KK Bansal, Monika Bansal, Sanjeev Kishore, Anuradha K, Meena H, Dushyant G. Department of Neurosurgery
MRS and Perfusion of Brain Tumors
 Department of Radiology University of California San Diego MRS and Perfusion of Brain Tumors John R. Hesselink, M.D. MRS & Perfusion of Brain Tumors Tumor histology Degree of malignancy Delineate tumor
Department of Radiology University of California San Diego MRS and Perfusion of Brain Tumors John R. Hesselink, M.D. MRS & Perfusion of Brain Tumors Tumor histology Degree of malignancy Delineate tumor
AMERICAN BRAIN TUMOR ASSOCIATION. Oligodendroglioma and Oligoastrocytoma
 AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
Case Report Complex Form Variant of Dysembryoplastic Neuroepithelial Tumor of the Cerebellum
 Case Reports in Pathology Volume 2012, Article ID 718651, 4 pages doi:10.1155/2012/718651 Case Report Complex Form Variant of Dysembryoplastic Neuroepithelial Tumor of the Cerebellum Jesús Vaquero, 1,
Case Reports in Pathology Volume 2012, Article ID 718651, 4 pages doi:10.1155/2012/718651 Case Report Complex Form Variant of Dysembryoplastic Neuroepithelial Tumor of the Cerebellum Jesús Vaquero, 1,
Neurosurgery Review. Mudit Sharma, MD May 16 th, 2008
 Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Case Report Multiple Sclerosis and Oligodendroglioma: An Exceptional Association
 Hindawi Publishing Corporation Case Reports in Neurological Medicine Volume 2014, Article ID 546817, 5 pages http://dx.doi.org/10.1155/2014/546817 Case Report Multiple Sclerosis and Oligodendroglioma:
Hindawi Publishing Corporation Case Reports in Neurological Medicine Volume 2014, Article ID 546817, 5 pages http://dx.doi.org/10.1155/2014/546817 Case Report Multiple Sclerosis and Oligodendroglioma:
P. Hitchcock, Ph.D. Department of Cell and Developmental Biology Kellogg Eye Center. Wednesday, 16 March 2009, 1:00p.m. 2:00p.m.
 Normal CNS, Special Senses, Head and Neck TOPIC: CEREBRAL HEMISPHERES FACULTY: LECTURE: READING: P. Hitchcock, Ph.D. Department of Cell and Developmental Biology Kellogg Eye Center Wednesday, 16 March
Normal CNS, Special Senses, Head and Neck TOPIC: CEREBRAL HEMISPHERES FACULTY: LECTURE: READING: P. Hitchcock, Ph.D. Department of Cell and Developmental Biology Kellogg Eye Center Wednesday, 16 March
USCAP Neuropathology. Case No. 3 Elisabeth J. Rushing, MD Armed Forces Institute of Pathology Washington, DC
 USCAP Neuropathology Case No. 3 Elisabeth J. Rushing, MD Armed Forces Institute of Pathology Washington, DC Clinical history The patient is a 9 year-old boy who has had seizures since age 2, at which time
USCAP Neuropathology Case No. 3 Elisabeth J. Rushing, MD Armed Forces Institute of Pathology Washington, DC Clinical history The patient is a 9 year-old boy who has had seizures since age 2, at which time
Neurocytoma a Rare Intraventricular Tumor
 Neurocytoma a Rare Intraventricular Tumor J. A. Mallick,S. A. Ali ( Department of Oncology, Liaquat National Postgraduate Medical Centre, Karachi. ) Introduction Central neurocytoma was first recognized
Neurocytoma a Rare Intraventricular Tumor J. A. Mallick,S. A. Ali ( Department of Oncology, Liaquat National Postgraduate Medical Centre, Karachi. ) Introduction Central neurocytoma was first recognized
Cilengitide (Impetreve) for glioblastoma multiforme. February 2012
 for glioblastoma multiforme. February 2012") Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
CISC 3250 Systems Neuroscience
 CISC 3250 Systems Neuroscience Levels of organization Central Nervous System 1m 10 11 neurons Neural systems and neuroanatomy Systems 10cm Networks 1mm Neurons 100μm 10 8 neurons Professor Daniel Leeds
CISC 3250 Systems Neuroscience Levels of organization Central Nervous System 1m 10 11 neurons Neural systems and neuroanatomy Systems 10cm Networks 1mm Neurons 100μm 10 8 neurons Professor Daniel Leeds
SPECIAL SLIDE SEMINAR CASE 3
 SPECIAL SLIDE SEMINAR CASE 3 Tihana Džombeta, MD Leo Pažanin, MD, PhD Department of Pathology, School of Medicine, University of Zagreb Department of Pathology, Clinical Hospital Centre Sestre milosrdnice
SPECIAL SLIDE SEMINAR CASE 3 Tihana Džombeta, MD Leo Pažanin, MD, PhD Department of Pathology, School of Medicine, University of Zagreb Department of Pathology, Clinical Hospital Centre Sestre milosrdnice
LETTER INTENT
 2016-2017 LETTER INTENT Using CRISPR Induced Deletions on Chromosome 1p and 19q of human tissue models to Determine the Effectiveness of Temozolomide Chemotherapy Treatment on Grade II Oligodendroglioma
2016-2017 LETTER INTENT Using CRISPR Induced Deletions on Chromosome 1p and 19q of human tissue models to Determine the Effectiveness of Temozolomide Chemotherapy Treatment on Grade II Oligodendroglioma
Atypical ganglioneurocytoma: case report and review of literature
 CASE REPORT Atypical ganglioneurocytoma: case report and review of literature Javed Khader Eliyas 1, Peter Pytel 2, Rimas V. Lukas 3, Patrik Gabikian 4 1. Section of Neurosurgery, University of Chicago,
CASE REPORT Atypical ganglioneurocytoma: case report and review of literature Javed Khader Eliyas 1, Peter Pytel 2, Rimas V. Lukas 3, Patrik Gabikian 4 1. Section of Neurosurgery, University of Chicago,
2015 Diagnostic Slide Session
 2015 Diagnostic Slide Session Case 3 R.S. Tashjian, MD A.M. Langer-Gould, MD S. Natarajan, MD B.K. Kleinschmidt-DeMasters, MD H.V. Vinters, MD Disclosures No financial disclosures or conflicts of interest
2015 Diagnostic Slide Session Case 3 R.S. Tashjian, MD A.M. Langer-Gould, MD S. Natarajan, MD B.K. Kleinschmidt-DeMasters, MD H.V. Vinters, MD Disclosures No financial disclosures or conflicts of interest
Supratentorial multiple little meningiomas with transitory stroke symptoms like. MRI case presentation
 114 Romanian Neurosurgery (2010) XVII 1: 114-121 Supratentorial multiple little meningiomas with transitory stroke symptoms like. MRI case presentation E. Moldovanu 1,2, Adriana Moldovanu 1,2, Carmen Gherman
114 Romanian Neurosurgery (2010) XVII 1: 114-121 Supratentorial multiple little meningiomas with transitory stroke symptoms like. MRI case presentation E. Moldovanu 1,2, Adriana Moldovanu 1,2, Carmen Gherman
Attenuation value in HU From -500 To HU From -10 To HU From 60 To 90 HU. From 200 HU and above
 Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Gliomatosis Cerebri. Xingli Zhao 1 Yu Tian 1 Zhaohui Li 1 Wei Ji 2 Chao Du 1. Introduction. Definition
 242 Chin J Clin Oncol (2008) 5: 242~250 DOI 10.1007/s11805-008-0242-9 Gliomatosis Cerebri Xingli Zhao 1 Yu Tian 1 Zhaohui Li 1 Wei Ji 2 Chao Du 1 1 Department of Neurosurgery, China-Japan Union Hospital,
242 Chin J Clin Oncol (2008) 5: 242~250 DOI 10.1007/s11805-008-0242-9 Gliomatosis Cerebri Xingli Zhao 1 Yu Tian 1 Zhaohui Li 1 Wei Ji 2 Chao Du 1 1 Department of Neurosurgery, China-Japan Union Hospital,
Oligodendroglioma: imaging findings, radio-pathological correlation and evolution
 Oligodendroglioma: imaging findings, radio-pathological correlation and evolution Poster No.: C-2104 Congress: ECR 2013 Type: Authors: Keywords: DOI: Scientific Exhibit A. Hernandez Castro, M. D. Monedero
Oligodendroglioma: imaging findings, radio-pathological correlation and evolution Poster No.: C-2104 Congress: ECR 2013 Type: Authors: Keywords: DOI: Scientific Exhibit A. Hernandez Castro, M. D. Monedero
5-hydroxymethylcytosine loss is associated with poor prognosis for
 5-hydroxymethylcytosine loss is associated with poor prognosis for patients with WHO grade II diffuse astrocytomas Feng Zhang 1,*, Yifan Liu 2, Zhiwen Zhang 1, Jie Li 1, Yi Wan 3, Liying Zhang 1, Yangmei
5-hydroxymethylcytosine loss is associated with poor prognosis for patients with WHO grade II diffuse astrocytomas Feng Zhang 1,*, Yifan Liu 2, Zhiwen Zhang 1, Jie Li 1, Yi Wan 3, Liying Zhang 1, Yangmei
Neuroradiology of AIDS
 Neuroradiology of AIDS Frank Minja,, HMS IV Gillian Lieberman MD September 2002 AIDS 90% of HIV patients have CNS involvement 1 10% of AIDS patients present first with neurological symptoms 2 73-80% of
Neuroradiology of AIDS Frank Minja,, HMS IV Gillian Lieberman MD September 2002 AIDS 90% of HIV patients have CNS involvement 1 10% of AIDS patients present first with neurological symptoms 2 73-80% of
CEREBRUM. Dr. Jamila EL Medany
 CEREBRUM Dr. Jamila EL Medany Objectives At the end of the lecture, the student should be able to: List the parts of the cerebral hemisphere (cortex, medulla, basal nuclei, lateral ventricle). Describe
CEREBRUM Dr. Jamila EL Medany Objectives At the end of the lecture, the student should be able to: List the parts of the cerebral hemisphere (cortex, medulla, basal nuclei, lateral ventricle). Describe
MolDX: Chromosome 1p/19q deletion analysis
 MolDX: Chromosome 1p/19q deletion analysis CGS Administrators, LLC Jump to Section... Please Note: This is a Proposed LCD. Proposed LCDs are works in progress and not necessarily a reflection of the current
MolDX: Chromosome 1p/19q deletion analysis CGS Administrators, LLC Jump to Section... Please Note: This is a Proposed LCD. Proposed LCDs are works in progress and not necessarily a reflection of the current
Clinical Trials for Adult Brain Tumors - the Imaging Perspective
 Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
Anatomic locations in high grade glioma
 Romanian Neurosurgery (2015) XXIX 3: 271-277 271 Anatomic locations in high grade glioma A. Oslobanu 1, St.I. Florian 2 University of Medicine and Pharmacy, Iuliu Hatieganu Cluj-Napoca 1 Assistant Professor
Romanian Neurosurgery (2015) XXIX 3: 271-277 271 Anatomic locations in high grade glioma A. Oslobanu 1, St.I. Florian 2 University of Medicine and Pharmacy, Iuliu Hatieganu Cluj-Napoca 1 Assistant Professor
Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation
 Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation Background Histology/Tumor Characteristics Presenting Symptoms/diagnosis Treatment/outcome Patient cohort Research on HRQOL Slow growing indolent
Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation Background Histology/Tumor Characteristics Presenting Symptoms/diagnosis Treatment/outcome Patient cohort Research on HRQOL Slow growing indolent