Oncological Management of Brain Tumours. Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013
|
|
|
- Daniel Ellis
- 6 years ago
- Views:
Transcription
1 Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013
2 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis Treatment of Low Grade Gliomas Treatment of High Grade Gliomas Radiotherapy How is it done? Radiotherapy toxicity Brain Metastases
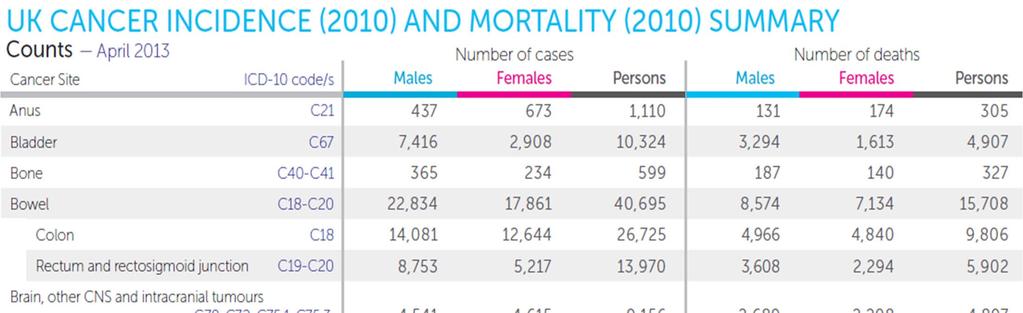
3 Epidemiology Incidence of 9000 per annum in the UK all CNS tumours ; 58% of which are intracranial tumours 14 new cases per each year ( UK) new cases worldwide Lifetime risk 1/77 Brain tumours are 1.6% of all cancers On average each GP diagnoses one patient with brain tumour every 7 years. Peak disease incidence years

4
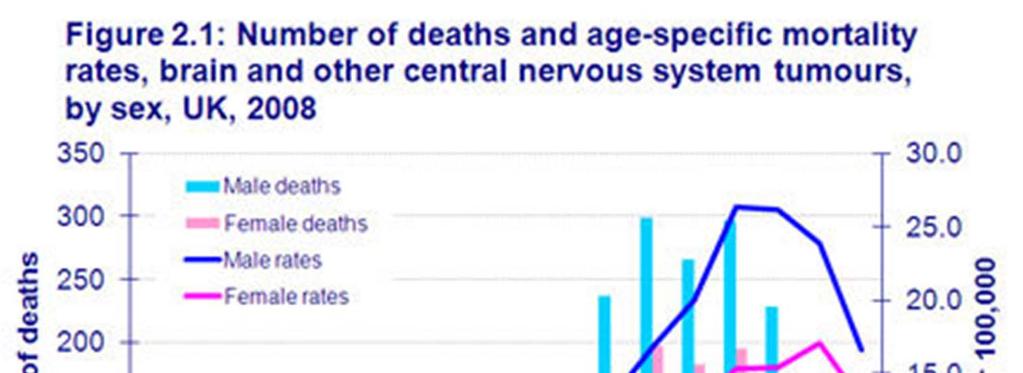
5 Mortality
6 Risk Factors Increasing age Higher socio economic status Mostly sporadic AIDS / immunocompromised cerebral lymphoma Ionising radiation (gliomas, meningiomas) Inherited cancer syndromes (neurofibromatosis type 1, von Hippel Lindau symdrome, tuberous sclerosis, Li Faumeni)
7 Gliomas
8
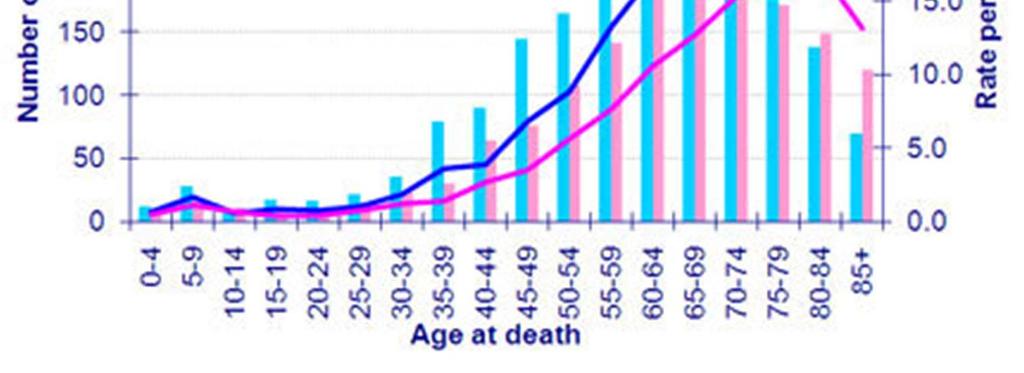
9 Pathology Gliomas most common WHO I low proliferative potential, discrete WHO II Infiltrating, can progress to high grade WHO III High mitotic activity, infiltration, anaplastic WHO IV tumour necrosis, rapid pre/ post operative growth Molecular tests Deletions of 1p and 19q O6 Methylguanine DNA methyltransferase (MGMT) silencing by promoter methylation. Ki 67 proliferative potential Highly infiltrative spread along white matter to other parts of the brain Rarely metastasise outside the CNS CSF spread medulloblastoma, ependymoma Haematogeneous medulloblastoma ( lung, liver, bone)
10 Clinical presentation Symptoms/signs of increased intracranial pressure : Headache, nausea, vomiting 70% of patients have headache at presentation Principal presenting symptoms: Headache 50% Seizures 20% Cognitive disturbance 12% Motor deficit 8% Speech disturbance 5% Visual disturbance 4% Sensory disturbance 2% Collateral History is important
11 Investigations/ Diagnosis History ( including from friends and family) Examination MRI location, oedema, necrosis, haemorrhage, mass effect T1 pre and post gadolinium T2 oedema, Fluid attenuated inversion recovery (FLAIR), removes CSF signal. CT contrast if MRI not possible lower sensitivity (temporal, posterior fossa) Magnetic resonance spectroscopy High grade Vs Low grade, primary Vs metastatic Dynamic contrast enhanced perfusion MRI assesses blood flow, increased gliomas (blood brain barrier) PET increased FDG uptake with increased grade Biopsy/ histological diagnosis when possible stereotactic/needle/ Open/ image guided
12 Treatment General Considerations Acute management Control Symptoms Steroids (8mg Dexamethasone BD) Anti epileptic medication reach therapeutic levels! ( phenytoin, carbamazepine, levetiracetam) Analgesia Psychological support to pt and family clear and honest discussion of poor prognosis. Early involvement of Palliative care and community teams. MDT discussion Neurosurgery, Neuroradiologist, Neuropathologist, Oncology, Clinical Nurse Specialists, Physiotherapy, Rehabilitation
 > 40 years Astrocytoma histology Tumour > 6cm Crossing midline")
13 Low Grade Gliomas Prognostic evaluation: EORTC criteria (Pignatti et al. JCO 2002) > 40 years Astrocytoma histology Tumour > 6cm Crossing midline Neurological deficit
14 Low grade Gliomas No clear consensus for treatment. Usually resection complete histopathologic evaluation, potentially curative, relief of symptoms. Gross tumour resection Vs Subtotal resection Maximal safe resection attempted. With GTR reduced rates of recurrence (Claus EB et al 2005 Cancer). Needs to be balanced against QOL and morbidity from extent of resection.
15 Low Grade Gliomas Radiotherapy Watch and Wait Vs immediate post op radiotherapy EORTC trial (van den Bent MJ et al 2005, Lancet) randomised to observation vs post op RT RT improved median progression free survival (5.3 vs 3.4 years) (5yr PFS 55% vs 35%) No significant difference in Overall Survival (68% vs 66%). QOL gained by delaying recurrence needs to be weighted against QOL lost due to potential neurotoxicity of Radiotherapy. Studies show progressive deterioration in some patients from baseline cognitive function after RT (with no tumour progression). Advancing neuroimaging techniques and radiotherapy techniques may limit RT induced neurotoxicity.
16 Low Grade Gliomas RT or not? Balance risk of recurrence Vs potential toxicity Factors to consider: < 40 years Histology GTR Vs STR How symptomatic is the patient Standard Regime 54 Gy / 30 fractions higher doses tested in RCTs showed increased neurotoxicity with no difference in Overall Survival ( Shaw et al JCO 2002)
17 High Grade Gliomas Anaplastic types (Anaplastic Astrocytoma) and GBM 85% are GBM late presentation Median age of presentation 64 years Prognostic factors: Age > 50 years Performance status Histology ( Grade III Vs IV) Symptoms/ mental status Resection Gross Total Resection Vs Partial Resection Median Survival Ranges from 60 months in better prognostic groups to 5 months in worst prognostic groups
18 High Grade Gliomas Treatment Symptoms control Steroids, Anti epileptics, Surgical decompression if increased ICP MDT discussion patient PS, co morbidities, extent and location of tumour. Maximum feasible neurosurgical resection. RT benefits established in late 1970s in patients with anaplastic gliomas increase in MS from 14 weeks to 35 weeks in arms receiving WBRT compared to chemotherapy or observation (Walker MD et al J. Neurosurg 1978) Better MS with increased WBRT doses (Walker et al IJOP 1979). RT regime established to 60Gy in 30 fraction no benefit in OS with higher RT doses)
19 High Grade Gliomas Treatment EORTC/ NCIC (Stupp et al, NEJM 2005). Phase III trial, 573 glioblastoma patients 84% GTR/ PR, randomised to RT alone Vs RT + Temozolamide (Concurrently + Adjuvant 6 months / 5 days/ every 4 weeks). Improved MS 12.1 mo 14.6 mo Improved 2 yr OS 10.4% 26.5% Improved median PFS 5.0 mo 6.9 mo Only 7% Grade 3 or 4 haematologic toxicity RT with Temozolamide standard of care post op or first line if inoperable, with pts with good PS.
20 High Grade Gliomas Treatment The STUPP regime : RT in 30 sessions/ fractions 60Gy = Mon Fri 6 weeks Temozolamide concurrent (75mg/m 2 /d) Temozolamide adjuvant mg/m 2 /d for 5 days every 4 weeks, for 6 months. Temozolamide: Alkylating agent Alkylates/ methylates DNA DNA damage promotes cancer cell death Main side effects Bone marrow suppression Low WBC, Hb/ platelets/ Risk of Neutropenic Sepsis /Nausea/ vomiting/ Fatigue/Constipation
21 High Grade Gliomas Treatment O6 Methylguanine DNA methyltransferase (MGMT) DNA repair gene encodes for DNA repair protein Methylation of its promoter makes the gene inactive Decreased ability to repair DNA. Tumours with inactive gene more susceptible to chemotherapy. Patients with methylated MGMT promoter in tumour benefit from Temozolamide ( Hegi et al 2004 Clin. Cancer Res)
22 HGG Treatment / Elderly patients Mean age of HGG 61 years 60% of HGG occuring in patients > 60 years With an ageing population incidence expected to increase. Age is a prognostic factor and survival decreases for each decade > 50 years. Elderly patients under represented in clinical trials. The EORTC/ NCIC 2004 trial recruitment was up to 70 years. Elderly patients may be frail and in view of poorer prognosis in this group treatment of 6 weeks of RT with TMZ may not be justifiable.
23 HGG Treatment/ Elderly patients Shorter RT regimes can be currently considered some studies 40 Gy in 15 fractions showed equivalence (Roa W et al 2004 JCO) 40 Gy/ 15 fractions; 30 Gy in 10 fractions can be considered depending on PS/ co morbidities. Nordic randomised phase III trial (Malmstrom A et al 2012 Lancet Oncol) compared: TMZ alone Vs 34Gy / 10 fractions Vs 60 Gy/ 30 fractions Similar OS in TMZ and short course RT group > 70 yrs longer survival in TMZ/ short course RT than long course RT high number of patients unable to complete long course RT treatment Patients treated with TMZ and had MGMT methylation had improved OS (9.7 months Vs 6.8 months), good toxicity profile.
24 HGG Treatment / Elderly patients Short course RT treatment or treatment with TMZ alone can be considered in elderly patients as an alternative to standard treatment. MGMT status assessment important in the elderly to decide treatment. MGMT not routinely available in most centres in the UK Cost to test 2500 cases in the UK.
25 HGG Anaplastic oligodendrogliomas Have sensitivity to chemotherapy PVC procarbazine, lomustine, and vincristine Loss of chromosomal arms 1p and 19q in 50% 70% of tumors. 1p deletion is a statistically significant predictor of chemosensitivity ( Cairncross JG J Natl Cancer Inst) Combined loss 1p and 19q is statistically significantly associated with both chemosensitivity and longer recurrence free survival after chemotherapy. 1p and 19q loss strongly associated with longer overall survival. Adjuvant PCV chemotherapy after RT increase PFS (23 Vs 13.2 months; P = ). no change in OS (Van den Bent MJ et al 2006 JCO).
26 HGG Treatment / Relapse Steroids/ Maximise symptom control If local recurrence consider surgery and chemo. If inoperable and no RT previously RT If diffuse relapse chemotherapy if good performance status If poor performance status best supportive care.
27 Brain Radiotherapy How is it done? CT scanning with contrast 3 mm slices CT scan images fused/ co registered with T2 MRI images. CT scan allows planning of RT/ MRI allows better identification of tumour.

28 Brain RT Patient immobilisation at planning CT. Thermoplastic shell/ Perspex shell
29 Brain RT Reference points marked on shell. Patient placed in position using with laser beams. Opaque markers placed on reference points so that they are seen on the planning CT scan.
30 Linear Accelerator
31 Brain RT Contours: GTV : Gross Tumour volume CTV: Clinical Tumour volume (GTV mm) PTV: Planned Tumour volume (CTV + 5mm) OAR: Organs at Risk Lenses, Optic Nerve, Optic Chiasm, Brain Stem Avoid bone Clinical decision about relative risks and benefits if PTV volumes and OAR overlap
32 Beam arrangement to encompass PTV conformal, tailored to avoid treating normal tissue and OAR reduce toxicity Shielding (Green areas)
33 -ICRU 50/62 Recommendations PTV 95%- 107% of dose no structures outside PT > 95%
34 Brain RT Verification by portal images to check whether actual treatment delivered matches what is planned. IMRT Intensity Modulated Radiotherapy Treatment Multiple beams used with variable shielding to improve geometric shape of treatment delivered, achieve more uniformity of dose, reduce toxicity to critical structures.
35 Brain RT Toxicity Acute: alopecia radiation dermatitis / erythema fatigue increase in oedema with side effects of headache, nausea, vomiting, seizures, increased neurological deficit Impaired short term memory and concentration Increase steroids, anti emetics, anti epileptics Regular on treat review (doctor, MacMillan Radiographer Subside 4 6 weeks post treatment
36 Brain RT Practical issues Shells can be claustrophobic cutting out part of shells. Shells can increase erythema cutting out parts of shell Transport an every day treatment. Regular blood tests if concurrent Temozolamide Acute deterioration may necessitate stopping RT. Psychological support to patient and family
37 Brain RT Toxicity Late (3 months 3 years post RT) Memory impairment Increased risk of stroke Visual Loss/ retinopathy/ cataracts Impaired hormone production (hypothalamus, pituitary) Fatigue Hair Loss
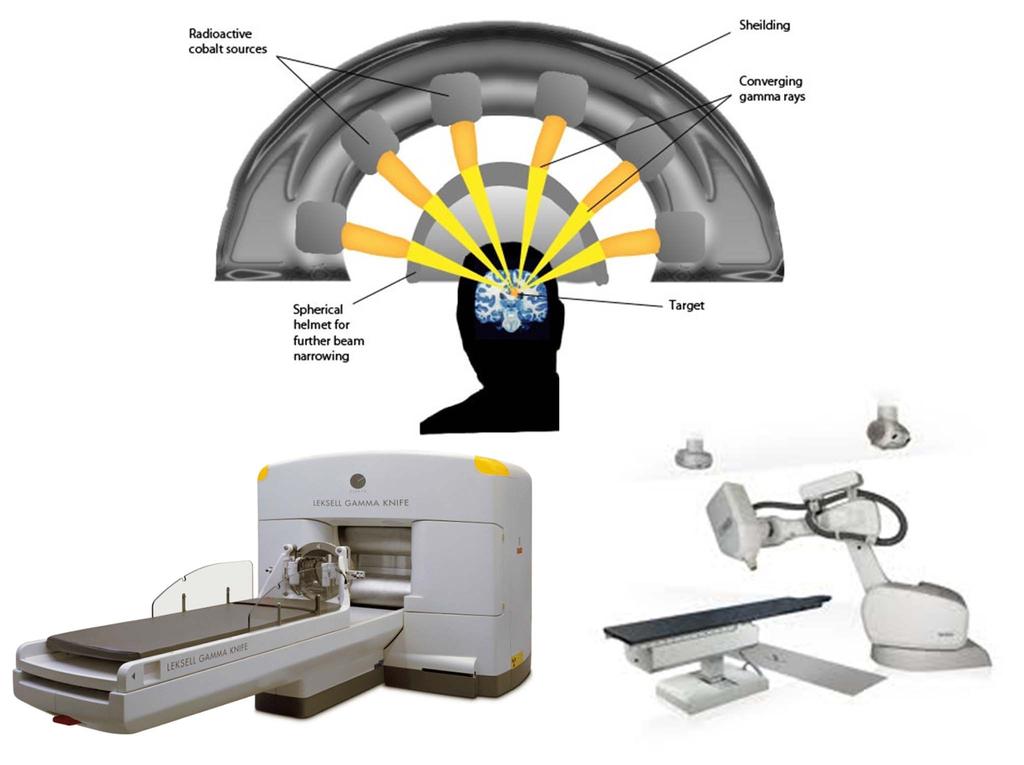
38 Stereotactic radiotherapy Stereotactic radiotherapy (SRt) is used to deliver focused, relatively large doses of radiation to a small, precisely defined target. Gammaknife Cyberknife The role of SRT in the management of patients with HGG is not well established. Addition of an SRT boost prior to standard XRT provides no survival benefit. Possible survival benefit when SRS is performed after XRT
39
40 Brain Metastases Occur in 20% 40% of patients with other cancer. Most common lung, breast, melanoma, renal, GI. Solitary tumours should be considered for neurosurgical resection if operable. Post op Radiotherapy may reduce intracranial relapse. SRS may be appropriate in small lesions ( < 3cm) Palliative Whole Brain Radiotherapy Treatment (WBRT) in multiple lesions. RT planning is simpler covers the whole skull, two lateral beams used. Common regimes: 12Gy in 2 fractions; 20Gy in 5 fractions; 30Gy in 10 fractions.
41 Current Challenges/ Summary Most Primary brain tumours are Gliomas, most of which present at Grades III/ IV and carry a poor prognosis. Age, histology and performance status are prognostic factors for both LGG and HGG. Careful MDT assessment needed as there is a fine line between increasing life expectancy and improving QOL in these patients. Early involvement of palliative care / community support/ honest discussion regarding prognosis/ family support. Acute oncological management to improve symptoms as much as possible. RT +/ chemotherapy as standard treatment STUPP for HGG. Careful assessment in elderly patients and treatment decision. RT induced Toxicity/ Chemo Toxicity Vs Performance status and prognosis. Steroid Use side effects/ patient education/ access for advice.
42 QUESTIONS?
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Radioterapia no Tratamento dos Gliomas de Baixo Grau
 Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment
![Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment](/thumbs/87/96032554.jpg "Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment") Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: GLIOBLASTOMA MULTIFORME (CNS) Patient information given at each stage following agreed
Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: GLIOBLASTOMA MULTIFORME (CNS) Patient information given at each stage following agreed
Systemic Treatment. Third International Neuro-Oncology Course. 23 May 2014
 Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
21/03/2017. Disclosure. Practice Changing Articles in Neuro Oncology for 2016/17. Gliomas. Objectives. Gliomas. No conflicts to declare
 Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES
 MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
CNS Tumors: The Med Onc Perspective. Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U.
 CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
Scottish Medicines Consortium
 Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Precision medicine for gliomas
 Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study
 temozolomide and radiation to treat glioblastoma: A retrospective study") Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES
 DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
Imaging for suspected glioma
 Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS
 UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
Update on management of metastatic brain disease. Peter Hoskin Mount Vernon Cancer Centre Northwood UK
 Update on management of metastatic brain disease Peter Hoskin Mount Vernon Cancer Centre Northwood UK Incidence 15-30% of patients with solid tumours will develop brain metastases Most common primary sites
Update on management of metastatic brain disease Peter Hoskin Mount Vernon Cancer Centre Northwood UK Incidence 15-30% of patients with solid tumours will develop brain metastases Most common primary sites
Pediatric Brain Tumors: Updates in Treatment and Care
 Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to.
 Stratified Medicine Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to. Looking in detail at cancer cells and their genetic make up. Permit
Stratified Medicine Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to. Looking in detail at cancer cells and their genetic make up. Permit
Oligodendrogliomas & Oligoastrocytomas
 Oligodendrogliomas & Oligoastrocytomas ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization dedicated solely
Oligodendrogliomas & Oligoastrocytomas ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization dedicated solely
THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION. Mustafa Rashid Issa
 THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION Mustafa Rashid Issa ABSTRACT: Illustrate malignant tumors that form either in the brain or in the nerves originating in the brain.
THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION Mustafa Rashid Issa ABSTRACT: Illustrate malignant tumors that form either in the brain or in the nerves originating in the brain.
Target Delineation in Gliomas. Prof PK Julka Department of Radiotherapy and Oncology AIIMS, New Delhi
 Target Delineation in Gliomas Prof PK Julka Department of Radiotherapy and Oncology AIIMS, New Delhi 1 What is a glioma? A primary brain tumour that originated from a cell of the nervous system 2 Recommendations:
Target Delineation in Gliomas Prof PK Julka Department of Radiotherapy and Oncology AIIMS, New Delhi 1 What is a glioma? A primary brain tumour that originated from a cell of the nervous system 2 Recommendations:
Glioblastoma: Current Treatment Approach 8/20/2018
 Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen?
 Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
NON MALIGNANT BRAIN TUMOURS Facilitator. Ros Taylor Advanced Neurosurgical Nurse Practitioner Southmead Hospital Bristol
 NON MALIGNANT BRAIN TUMOURS Facilitator Ros Taylor Advanced Neurosurgical Nurse Practitioner Southmead Hospital Bristol Neurosurgery What will be covered? Meningioma Vestibular schwannoma (acoustic neuroma)
NON MALIGNANT BRAIN TUMOURS Facilitator Ros Taylor Advanced Neurosurgical Nurse Practitioner Southmead Hospital Bristol Neurosurgery What will be covered? Meningioma Vestibular schwannoma (acoustic neuroma)
AMERICAN BRAIN TUMOR ASSOCIATION. Oligodendroglioma and Oligoastrocytoma
 AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
Tumors of the Nervous System
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준. KNS-MT-03 (April 15, 2015)
") 성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
Clinical Guidelines for the Management of Neuro-Oncology
 Clinical Guidelines for the Management of Neuro-Oncology For approvals and version control see Document Management Record on page 37 Version: 3 Ref: AngCN_SSG_BC3_v3_NeuroOncology_Guidlines Page 1 of 47
Clinical Guidelines for the Management of Neuro-Oncology For approvals and version control see Document Management Record on page 37 Version: 3 Ref: AngCN_SSG_BC3_v3_NeuroOncology_Guidlines Page 1 of 47
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Cilengitide (Impetreve) for glioblastoma multiforme. February 2012
 for glioblastoma multiforme. February 2012") Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation
 Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation Background Histology/Tumor Characteristics Presenting Symptoms/diagnosis Treatment/outcome Patient cohort Research on HRQOL Slow growing indolent
Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation Background Histology/Tumor Characteristics Presenting Symptoms/diagnosis Treatment/outcome Patient cohort Research on HRQOL Slow growing indolent
Radiotherapy and Brain Metastases. Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem
 Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Neurosurgical Management of Brain Tumours. Nicholas Little Neurosurgeon RNSH
 Neurosurgical Management of Brain Tumours Nicholas Little Neurosurgeon RNSH General Most common tumours are metastatic 10x more common than primary Incidence of primary neoplasms is 20 per 100000 per year
Neurosurgical Management of Brain Tumours Nicholas Little Neurosurgeon RNSH General Most common tumours are metastatic 10x more common than primary Incidence of primary neoplasms is 20 per 100000 per year
CNS SESSION 3/8/ th Multidisciplinary Management of Cancers: A Case based Approach
 CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
Clinical Trials for Adult Brain Tumors - the Imaging Perspective
 Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
Brain Tumor Treatment
 Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
It s s Always Something!
 It s s Always Something! New Approaches in Brain Tumor Treatment Virginia Stark-Vance, M.D. When Something Is a Brain Tumor Brain tumors aren t rare: there are over 100,000/yr Most originate as other cancers
It s s Always Something! New Approaches in Brain Tumor Treatment Virginia Stark-Vance, M.D. When Something Is a Brain Tumor Brain tumors aren t rare: there are over 100,000/yr Most originate as other cancers
Brain tumours (primary) and brain metastases in adults
 and brain metastases in adults") Brain tumours (primary) and brain metastases in adults NICE guideline Draft for consultation, January 0 This guideline covers diagnosing, monitoring and managing any type of primary brain tumour or brain
Brain tumours (primary) and brain metastases in adults NICE guideline Draft for consultation, January 0 This guideline covers diagnosing, monitoring and managing any type of primary brain tumour or brain
Chemotherapy in malignant brain tumors
 Chemotherapy in malignant brain tumors Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH 4031 Basel zimmermannf@uhbs.ch Tumor types Neuro-epithelial tumors - Glioblastoma
Chemotherapy in malignant brain tumors Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH 4031 Basel zimmermannf@uhbs.ch Tumor types Neuro-epithelial tumors - Glioblastoma
AMERICAN BRAIN TUMOR ASSOCIATION. Oligodendroglioma and Oligoastrocytoma
 AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
Corporate Medical Policy
 Corporate Medical Policy Brachytherapy, Intracavitary Balloon Catheter for Brain Cancer File Name: Origination: Last CAP Review: Next CAP Review: Last Review: brachytherapy_intracavitary_balloon_catheter_for_brain_cancer
Corporate Medical Policy Brachytherapy, Intracavitary Balloon Catheter for Brain Cancer File Name: Origination: Last CAP Review: Next CAP Review: Last Review: brachytherapy_intracavitary_balloon_catheter_for_brain_cancer
Dr Eddie Mee. Neurosurgeon Auckland City Hospital, Ascot Integrated Hospital, MercyAscot Hospitals, Auckland
 Dr Eddie Mee Neurosurgeon Auckland City Hospital, Ascot Integrated Hospital, MercyAscot Hospitals, Auckland 16:30-17:25 WS #48: Current Management of Brain Bleeds and Tumours 17:35-18:30 WS #58: Current
Dr Eddie Mee Neurosurgeon Auckland City Hospital, Ascot Integrated Hospital, MercyAscot Hospitals, Auckland 16:30-17:25 WS #48: Current Management of Brain Bleeds and Tumours 17:35-18:30 WS #58: Current
NICE guideline Published: 11 July 2018 nice.org.uk/guidance/ng99
 Brain tumours (primary) and brain metastases in adults NICE guideline Published: 11 July 2018 nice.org.uk/guidance/ng99 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Brain tumours (primary) and brain metastases in adults NICE guideline Published: 11 July 2018 nice.org.uk/guidance/ng99 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Pediatr Blood Cancer 2014
 Low grade Glioma! 40% of pediatric brain tumors Pathologically, anatomically, clinically and biologically heterogeneous Leptomeningeal metastases in 5% Frequently protracted clinical course Long-Term Outcome
Low grade Glioma! 40% of pediatric brain tumors Pathologically, anatomically, clinically and biologically heterogeneous Leptomeningeal metastases in 5% Frequently protracted clinical course Long-Term Outcome
EORTC (RTOG 0834 Endorsed) Opened: July 22, 2009
 Opened: July 22, 2009") January 2011 0834-1 EORTC 26053 22054 (RTOG 0834 Endorsed) Protocol Status: Opened: July 22, 2009 Title: Phase III Trial on Concurrent and Adjuvant Temozolomide Chemotherapy in Non-1P/19Q Deleted Anaplastic
January 2011 0834-1 EORTC 26053 22054 (RTOG 0834 Endorsed) Protocol Status: Opened: July 22, 2009 Title: Phase III Trial on Concurrent and Adjuvant Temozolomide Chemotherapy in Non-1P/19Q Deleted Anaplastic
Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma
 National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy: A Retrospective Comparative Study
 Original Article Research in Oncology June 2017; Vol. 13, No. 1: 18-22. DOI: 10.21608/resoncol.2017.552.1022 Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy:
Original Article Research in Oncology June 2017; Vol. 13, No. 1: 18-22. DOI: 10.21608/resoncol.2017.552.1022 Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy:
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
Animal chemotherapy Film radiotherapy Music cancer treatment
 Cancer treatments Animal chemotherapy Film radiotherapy Music cancer treatment What are the main treatments? Hormone therapy Surgery Chemotherapy Radiotherapy Targeted anti-cancer therapy (immunotherapy)
Cancer treatments Animal chemotherapy Film radiotherapy Music cancer treatment What are the main treatments? Hormone therapy Surgery Chemotherapy Radiotherapy Targeted anti-cancer therapy (immunotherapy)
Update on Pediatric Brain Tumors
 Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
Corporate Medical Policy
 Corporate Medical Policy Analysis of MGMT Promoter Methylation in Malignant Gliomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: analysis_of_mgmt_promoter_methylation_in_malignant_gliomas
Corporate Medical Policy Analysis of MGMT Promoter Methylation in Malignant Gliomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: analysis_of_mgmt_promoter_methylation_in_malignant_gliomas
Dosimetry, see MAGIC; Polymer gel dosimetry. Fiducial tracking, see CyberKnife radiosurgery
 Subject Index Acoustic neuroma, neurofibromatosis type 2 complications 103, 105 hearing outcomes 103, 105 outcome measures 101 patient selection 105 study design 101 tumor control 101 105 treatment options
Subject Index Acoustic neuroma, neurofibromatosis type 2 complications 103, 105 hearing outcomes 103, 105 outcome measures 101 patient selection 105 study design 101 tumor control 101 105 treatment options
Prior to 1993, the only data available in the medical
 Neuro-Oncology Prospective clinical trials of intracranial low-grade glioma in adults and children Edward G. Shaw 1 and Jeffrey H. Wisoff Department of Radiation Oncology, Wake Forest University School
Neuro-Oncology Prospective clinical trials of intracranial low-grade glioma in adults and children Edward G. Shaw 1 and Jeffrey H. Wisoff Department of Radiation Oncology, Wake Forest University School
Neurosurgery Review. Mudit Sharma, MD May 16 th, 2008
 Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM GERM CELL TUMOURS CNS Site Group Germ Cell Tumours Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM GERM CELL TUMOURS CNS Site Group Germ Cell Tumours Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Institute of Oncology & Radiobiology. Havana, Cuba. INOR
 Institute of Oncology & Radiobiology. Havana, Cuba. INOR 1 Transition from 2-D 2 D to 3-D 3 D conformal radiotherapy in high grade gliomas: : our experience in Cuba Chon. I, MD - Chi. D, MD - Alert.J,
Institute of Oncology & Radiobiology. Havana, Cuba. INOR 1 Transition from 2-D 2 D to 3-D 3 D conformal radiotherapy in high grade gliomas: : our experience in Cuba Chon. I, MD - Chi. D, MD - Alert.J,
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA
 NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
-Proton Beam Therapy in Paediatric Radiation Oncology -
 -Proton Beam Therapy in Paediatric Radiation Oncology - Beate Timmermann, M.D. West German Proton Therapy Centre Essen Germany Preview Survival Toxicity Why protons? (theoretically) Experiences so far
-Proton Beam Therapy in Paediatric Radiation Oncology - Beate Timmermann, M.D. West German Proton Therapy Centre Essen Germany Preview Survival Toxicity Why protons? (theoretically) Experiences so far
Neuro-oncology Update Andrew Kokkino, MD Medical Director, The Neurosciences Institute at Sacred Heart at Riverbend May 20, 2013
 Neuro-oncology Update 2013 Andrew Kokkino, MD Medical Director, The Neurosciences Institute at Sacred Heart at Riverbend May 20, 2013 Case 1 58 year old man with recent facial droop and HA s Thin, cachectic
Neuro-oncology Update 2013 Andrew Kokkino, MD Medical Director, The Neurosciences Institute at Sacred Heart at Riverbend May 20, 2013 Case 1 58 year old man with recent facial droop and HA s Thin, cachectic
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
Low grade glioma: a journey towards a cure
 Editorial Page 1 of 5 Low grade glioma: a journey towards a cure Ali K. Choucair SIU School of Medicine, Springfield, IL, USA Correspondence to: Ali K. Choucair, MD. Professor of Neurology, Director of
Editorial Page 1 of 5 Low grade glioma: a journey towards a cure Ali K. Choucair SIU School of Medicine, Springfield, IL, USA Correspondence to: Ali K. Choucair, MD. Professor of Neurology, Director of
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING
 PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms. Overall Clinical Significance 8/3/13
 Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
PRESURGICAL PLANNING. Strongly consider neuropsychological evaluation before functional imaging study Strongly consider functional imaging study
 NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
Hong Kong Hospital Authority Convention 2018
 Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Anticonvulsive therapy. Roberta Rudà Division of Neuro-Oncology, Dept. of Neuroscience City of Health and Science and University of Turin, Italy
 Anticonvulsive therapy Roberta Rudà Division of Neuro-Oncology, Dept. of Neuroscience City of Health and Science and University of Turin, Italy Symposium on Brain Metastases, Zurich, 19 Jan 2018 DISCLOSURE
Anticonvulsive therapy Roberta Rudà Division of Neuro-Oncology, Dept. of Neuroscience City of Health and Science and University of Turin, Italy Symposium on Brain Metastases, Zurich, 19 Jan 2018 DISCLOSURE
HSV1716 Dose levels and Cohort size Dose level No of Patients HSV1716 Dosage 1* 3 to 6 1 ml of 1 x 10 5 infectious units HSV1716 per ml 2
 Abstract and Schema: Description and Rationale: Pediatric high grade gliomas have a progressive initial course and high risk of relapse/ progression; making the 5-year overall survival rate 15-35% with
Abstract and Schema: Description and Rationale: Pediatric high grade gliomas have a progressive initial course and high risk of relapse/ progression; making the 5-year overall survival rate 15-35% with
Defining Target Volumes and Organs at Risk: a common language
 Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
Background. Central nervous system (CNS) tumours. High-grade glioma
 tumours. High-grade glioma") 25 4. Central nervous system (CNS) tumours Background Two important considerations underpin the choice of treatment fractionation in neurooncology. First, the results of treatment vary widely and, second,
25 4. Central nervous system (CNS) tumours Background Two important considerations underpin the choice of treatment fractionation in neurooncology. First, the results of treatment vary widely and, second,
Peter Canoll MD. PhD.
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased
 Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased analysis Roel Schlijper Fellow Radiation Oncology BC Cancer, Prince George Disclosures No conflicts
Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased analysis Roel Schlijper Fellow Radiation Oncology BC Cancer, Prince George Disclosures No conflicts
Gamma Knife Radiosurgery A tool for treating intracranial conditions. CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop
 Gamma Knife Radiosurgery A tool for treating intracranial conditions CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop ANGELA McBEAN Gamma Knife CNC State-wide Care Coordinator Gamma Knife
Gamma Knife Radiosurgery A tool for treating intracranial conditions CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop ANGELA McBEAN Gamma Knife CNC State-wide Care Coordinator Gamma Knife
Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey
 Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide
 405 Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide Walter Taal, MD 1 Dieta Brandsma, MD, PhD 1 Hein G. de Bruin, MD, PhD
405 Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide Walter Taal, MD 1 Dieta Brandsma, MD, PhD 1 Hein G. de Bruin, MD, PhD
Response to postoperative radiotherapy as a prognostic factor for patients with low-grade gliomas
 ONCOLOGY LETTERS 4: 455-460, 2012 Response to postoperative radiotherapy as a prognostic factor for patients with low-grade gliomas MICHAL SPYCH 1,2, LESZEK GOTTWALD 3, EMILIA JESIEŃ LEWANDOWICZ 1,2, SŁAWOMIR
ONCOLOGY LETTERS 4: 455-460, 2012 Response to postoperative radiotherapy as a prognostic factor for patients with low-grade gliomas MICHAL SPYCH 1,2, LESZEK GOTTWALD 3, EMILIA JESIEŃ LEWANDOWICZ 1,2, SŁAWOMIR
Radiotherapy approaches to pituitary tumors
 Disclosures No relevant disclosures Radiotherapy approaches to pituitary tumors Pituitary Disorders: Advances in Diagnosis and Management Steve Braunstein, MD, PhD UCSF Department of Radiation Oncology
Disclosures No relevant disclosures Radiotherapy approaches to pituitary tumors Pituitary Disorders: Advances in Diagnosis and Management Steve Braunstein, MD, PhD UCSF Department of Radiation Oncology
Chapter 1 Introduction
 Chapter 1 Introduction Men think epilepsy divine, merely because they do not understand it. But if they called everything divine which they do not understand, why, there would be no end to divine things.
Chapter 1 Introduction Men think epilepsy divine, merely because they do not understand it. But if they called everything divine which they do not understand, why, there would be no end to divine things.
Challenging Paediatric Brain Tumours. ASP Belfast March 2017 Dr Jane Pears Consultant Paediatric Oncologist, Dublin
 Challenging Paediatric Brain Tumours ASP Belfast March 2017 Dr Jane Pears Consultant Paediatric Oncologist, Dublin Overview (i) Paediatric malignancy (ii) Central nervous system tumours (iii) Diffuse Intrinsic
Challenging Paediatric Brain Tumours ASP Belfast March 2017 Dr Jane Pears Consultant Paediatric Oncologist, Dublin Overview (i) Paediatric malignancy (ii) Central nervous system tumours (iii) Diffuse Intrinsic
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors
 research article 213 3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors Yilmaz Tezcan and Mehmet Koc Department
research article 213 3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors Yilmaz Tezcan and Mehmet Koc Department
Radiotherapy Protocols
 Radiotherapy Protocols Cranial Irradiation for Palliative Whole Brain for Metastases and Prophylactic Whole Brain for SCLC Prepared by: Dr C Blesing, Dr N Warner, Dr D Cutter, Ms R Watson, Ms L Drummond,
Radiotherapy Protocols Cranial Irradiation for Palliative Whole Brain for Metastases and Prophylactic Whole Brain for SCLC Prepared by: Dr C Blesing, Dr N Warner, Dr D Cutter, Ms R Watson, Ms L Drummond,
Minesh Mehta, Northwestern University. Chicago, IL
 * Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
* Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
Neodjuvant chemotherapy
 Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY th March
 SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY 2018 15th March 13h 13h45 ROOM 1 ROOM 2 ROOM 3 Imaging and pathology case discussion Lymphomas case discussion- Meningeomas Moderator:
SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY 2018 15th March 13h 13h45 ROOM 1 ROOM 2 ROOM 3 Imaging and pathology case discussion Lymphomas case discussion- Meningeomas Moderator:
Temozolomide with Radiotherapy for the Treatment of Malignant Gliomas, Center Experience
 Temozolomide with Radiotherapy for the Treatment of Malignant Gliomas, Center Experience *Ehab Abdou and **Mohamed Gaafar *Department of Radiation Oncology, Faculty of Medicine, Al-Azhar University, Cairo,
Temozolomide with Radiotherapy for the Treatment of Malignant Gliomas, Center Experience *Ehab Abdou and **Mohamed Gaafar *Department of Radiation Oncology, Faculty of Medicine, Al-Azhar University, Cairo,
MANAGEMENT N OF PRIMARY BRAIN TUMOURS IN THE ELDERLY
 MANAGEMENT N OF PRIMARY BRAIN TUMOURS IN THE ELDERLY Meningioma, Glioma, Lymphoma Cornu Ph, Keime-Guibert F, Hoang-Xuan K, Pierga JY, Delattre JY Neuro-oncology Group of Pitie-Salpetriere hospital-paris-france
MANAGEMENT N OF PRIMARY BRAIN TUMOURS IN THE ELDERLY Meningioma, Glioma, Lymphoma Cornu Ph, Keime-Guibert F, Hoang-Xuan K, Pierga JY, Delattre JY Neuro-oncology Group of Pitie-Salpetriere hospital-paris-france
Selecting the Optimal Treatment for Brain Metastases
 Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Management of Glioma: The Basics Glioma Update The clinical challenge. Glioma a malignant disease of the CNS
 Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121
 Carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121 NICE 2018. All rights reserved.
Carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121 NICE 2018. All rights reserved.
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Management of Brain Metastases Dr. Luis Souhami Professor Department of Radiation Oncology University,
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Management of Brain Metastases Dr. Luis Souhami Professor Department of Radiation Oncology University,
STEREOTACTIC RADIATION THERAPY. Monique Blanchard ANUM Radiation Oncology Epworth HealthCare
 STEREOTACTIC RADIATION THERAPY Monique Blanchard ANUM Radiation Oncology Epworth HealthCare Overview Stereotactic radiation therapy at Epworth Healthcare What is stereotactic radiation therapy? Delivery
STEREOTACTIC RADIATION THERAPY Monique Blanchard ANUM Radiation Oncology Epworth HealthCare Overview Stereotactic radiation therapy at Epworth Healthcare What is stereotactic radiation therapy? Delivery
Description. Section: Therapy Effective Date: July 15, 2015 Subsection: Original Policy Date: September 13, 2012 Subject: Page: 1 of 10
 Last Review Status/Date: June 2015 Page: 1 of 10 Description Radiotherapy (RT) is an integral component in the treatment of many brain tumors, both benign and malignant. Intensity-modulated radiation therapy
Last Review Status/Date: June 2015 Page: 1 of 10 Description Radiotherapy (RT) is an integral component in the treatment of many brain tumors, both benign and malignant. Intensity-modulated radiation therapy
REVISITING ICRU VOLUME DEFINITIONS. Eduardo Rosenblatt Vienna, Austria
 REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a