Benefits of Radiation Therapy in the Palliative Cancer Patient
|
|
|
- Gilbert Byrd
- 6 years ago
- Views:
Transcription

1 Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1
2 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid response palliative radiotherapy program Brain metastases Radiotherapy emergencies Malignant spinal cord compression Superior vena cava obstruction Page 2
3 Why better palliative Radiotherapy? With better systemic therapy, patients with advanced disease are living longer and management of toxicity and quality of life are important treatment outcomes Palliative Radiotherapy Overall Pain Relief 80-90% Average Response Duration is around 6 months Rates of re-irradiation 10-25% Therefore re-irradiation is becoming a more significant issue in our contemporary era due to improving survival amongst patients with metastatic disease. Page 3
4 Adelaide Radiotherapy Centre has recently introduced a new protocol to align the management of palliative cases with that offered to curative cases to ensure quality and best practice patient care outcomes. Page 4
5 Survival rates Colorectal Cancer Patients with unresectable metastases have median survival exceeding 2 years with modern chemotherapy and biological agents 1 (FOLFOX4, XELOX, Avastin) compared with 5FU alone 2 (11.5 mths) 1. Cassidy et al. NO16966 trial BJC Advanced CRC Meta-Analysis JCO 1992 Page 5
6 Survival rates Breast Cancer Patients with metastases have median survivals approaching 2 years for a 5 year interval with modern chemotherapy, hormonal and immunotherapy compared with 10 months when only more limited options were available for the period 3 Median survival can exceed many years depending on hormone receptor status, Her 2 status and location of metastases (bone versus visceral) 3. M Sundquist et al. Katnor Sweden EBCC 2010 Page 6
7 Survival rates Prostate Cancer Patients with metastases have median survivals approaching 6 years with hormonal therapy and chemotherapy (taxanes) Enzalutamide AFFIRM Median OS improved from 13 to 18 months Page 7
8 Palliative radiotherapy Traditionally large doses were delivered via simple beam arrangements this restricted our ability to deliver reirradiation. A traditional PA Plan of D5cm Peak dose of 33Gy to Spinal Cord with EQD 2 44Gy Plus poor coverage of target volume Page 8
9 Palliative radiotherapy This severely restricts our ability or willingness to RE-IRRADIATE as we approach the limits of the critical normal tissue tolerance. This will DENY patients the opportunity to have further benefit from radiotherapy with 50-80% deriving pain relief with re-irradiation. Page 9
10 Palliative radiotherapy Using a conformal planning and treatment approach aligning palliative treatment with treatment given to radical cases, the total dose and dose per fraction is kept at or below our prescription and we achieve far better coverage of our target volume. A conformal plan of 30Gy Peak dose of 30Gy to spinal Cord with EQD2 of 36Gy Improved coverage/control of symptoms and decreased acute and late toxicities In general, better management of the high dose region, including absolute value (the hot spot) and location (avoid OARs) is now required for every palliative plan. Page 10

11 Examples: 2D vs 3D Conformality Page 11

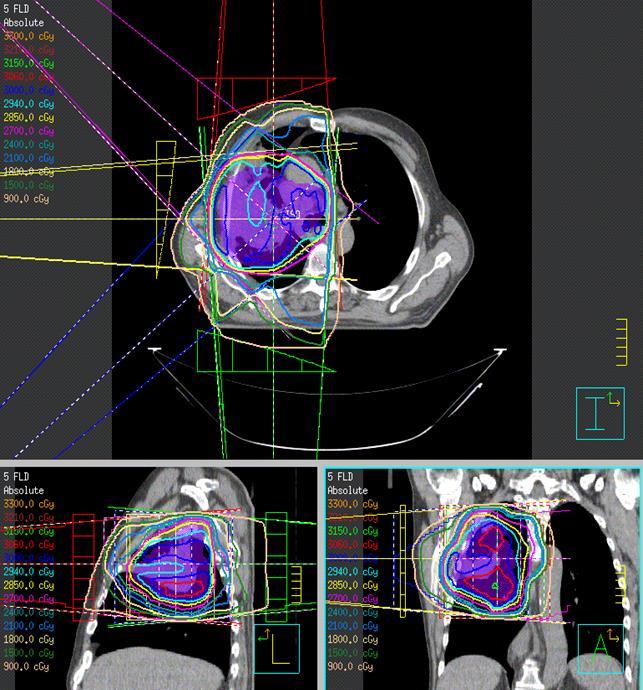
12 Examples: 2D vs 3D Conformality Page 12

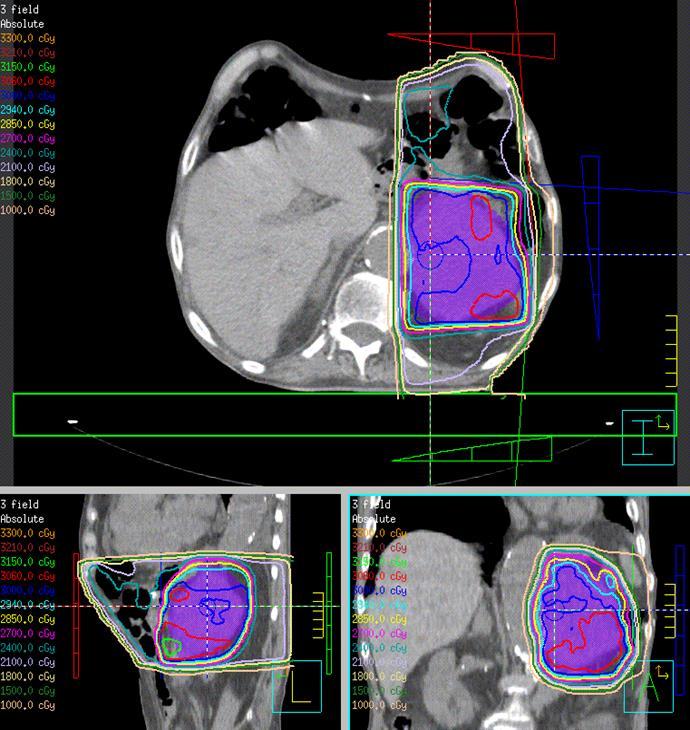
13 Examples: 2D vs 3D Conformality Page 13
14 Burden of bone metastases Bone metastases are the most common cause of cancer-related pain 60-80% of patients with advanced cancer will develop bony metastases >70% of patients with bone metastases are symptomatic Bony metastases account for 20% of all radiotherapy treatments In addition to pain, skeletal complications from bone metastases include: Pathological fractures (10-30% long bone mets) Spinal cord/cauda equina compression (5-10%) Page 14
15 Role of palliative RTx for bone mets Aims of palliative radiotherapy for bone metastases: Relieve pain Delay/prevent skeletal complications Improve/preserve function and QOL Radiotherapy is one of the most effective treatments for cancer pain 70-80% response rate to palliative RTx for painful bone mets Page 15
16 Bone mets Mechanism of analgesic effects of RTx not completely understood: Inhibition of release of chemical pain mediators Tumor shrinkage and recalcification of bone lesions Onset of response within 2-4 wks in 80% patients Median duration of pain relief varies b/w 3-6mths Common side effects include: Fatigue Pain flare: %; usually within first 5 days after RTx Nausea/vomiting: 10-17% Others are site dependent: eg mucositis, diarrhoea Page 16
17 Bone mets For patients with uncomplicated bony mets experiencing distressing pain, poor mobility/performance status and limited life-expectancies, a single fraction will be more convenient/acceptable and costeffective. * Uncomplicated bony metastases - absence of: neuropathic pain large soft tissue masses impending/actual pathological fracture or cord compression RTx generally involves a series of appointments: Initial clinic consultation Radiotherapy simulation/planning Radiotherapy treatment: Single fraction or 5-10 fractions Page 17
18 Rapid Response Palliative Radiotherapy (RRPR) Program Aims of the RRPR program for bone metastases: Provide quick/easy access for referring doctors Reduce waiting times for: Initial consultation, Simulation/planning Start of treatment Reduce the number of visits required before delivery of treatment Improve the underutilization of palliative RTx for bone mets, esp in rural populations Page 18
19 Rapid Response Palliative Radiotherapy (RRPR) Program Patient Suitability: Public and private patients Symptomatic bony metastases requiring palliation Nb. Actual/impending cord compression: RTx emergency NOT for RRPR Clinic Referral Process: Direct referral to the RRPR Clinic Standardized RRPR Clinic referral form Ensure availability of all necessary patient investigations/info Facilitate prebooking of planning and treatment start date Page 19
20 Brain mets Approx 25% of patients with systemic cancers possible increase due to more effective local and systemic control (most chemo doesn t cross blood brain barrier) Most common breast, lung, colorectal, melanoma Confers poor prognosis with MS of 4-5mths and 1yr OS 10% no treatment 1mth Steroids 2mths RTx - 4-6mths Surg+RTx 8-12mths General prognostic factors Age, performance status, status of extracranial disease, disease free interval, size of mets, mass effect, histology Page 20
21 Whole Brain Radiotherapy (WBRT) The main goal of WBRT Improve neurologic deficits caused by the metastases and surrounding oedema Prevent any further deterioration of neurologic function. The extent of improvement after WBRT is directly related to the time from diagnosis to radiation therapy, and early treatment is generally associated with a better outcome. Page 21
22 WBRT WBRT is the treatment of choice for Patients with single or multiple brain metastases not amenable to surgery or radiosurgery Complete and partial responses have been reported in approximately 60% of patients, with symptom improvement that is in part attributable to concomitant steroids. Tumour volume reduction after WBRT is associated with prolonged survival and better neurocognitive function preservation. Page 22
23 Indications for WBRT Histological or radiological evidence of metastatic disease involving the brain Multiple brain metastases or solitary metastasis unsuitable for surgical resection ECOG 0-2 (KPS of >70 ~ equates to ECOG 0-1) No prior cranial radiotherapy Stereotactic radiotherapy may be considered in patients with 1-3 brain metastases who have controlled extracranial disease Page 23
24 Side Effects of WBRT Short term side effects during or within a few weeks of finishing radiotherapy (usually temporary) Alopecia Fatigue Skin erythema and desquamation Headaches Nausea and/or Vomiting Neurological deficits Sub acute Somnolence Long term side effects that may be permanent Cerebrovascular disease Cognitive impairment Fatigue Page 24
25 Stereotactic Radiosurgery May be considered in 1-3 mets and in eloquent or deep areas where surgery not feasible Lesion <4cm >1cm from optic apparatus Newer frameless techniques making it more convenient and less resource intensive for treatment Page 25
26 Malignant Spinal cord/cauda equina Compression (MSCC) Actual cord compression = radiological compression of dural sac AND clinical features Back pain Motor deficits Sensory abnormalities Sphincter dysfunction Impending cord compression = radiological evidence of cord compression but without neurological deficits Page 26
27 MSCC - Epidemiology 5-10% of all cancer Pts Common malignancies Prostate, Breast, Lung Others: myeloma/plasmacytoma, NHL 20% are first presentations of the malignancy 1/3 have multilevel disease Page 27
28 MSCC - Investigations 1. Confirm MSCC and nature/extent MRI WHOLE spine with Gad: Gold standard 2. Obtain histological diagnosis Favourable histo Intent of Rx Type of Rx 3. Staging Prognosis No known malignancy Primary Another site for Bx Page 28
29 MSCC Treatment - Surgery Generally accepted indications: Instability Bony compression Progression on/after RTx No histo Dx if single level compression Page 29
30 MSCC Treatment - Surgery Direct decompressive surgery/postop RTx superior to RTx alone Patchell et al (NEJM 2005; 366: 643) Multi-institutional RCT; N=101 Stopped early Med survival: Surg/RTx 126 days RTx alone 100 days (p=0.03) Page 30
31 MSCC Treatment - Radiotherapy RTx main Rx modality for most Pts Intent: Palliative (most) Improving pain, maintaining function/delaying progression, ± improving function Timing: Upfront RTx started within 24hrs the longer the duration of Sx, esp motor, the poorer the outcomes Page 31

32 MSCC Treatment - Radiotherapy Strongest PF for functional outcome is prerx ambulatory status 20-30% of nonambulatory Pts will regain ambulation with RTx alone Page 32

33 MSCC Treatment - Radiotherapy Only ~ 15% regain sphincter control/ continence Strongest PF for survival is also prerx ambulatory status Page 33
34 MSCC Treatment - Radiotherapy Est. survival < 4-6 mths: Short course Equally effective for functional outcome More convenient/less distressing for Pt Despite apparent higher rate of in-field recurrences, re-irradiation safer Est. survival > 4-6 mths: Longer course Apparent lower rate of in-field recurrences (but more difficult to re-irradiate) Better bone recalcification (several mths; prospective German study cf single 8 Gy) Page 34
35 Malignant Superior Vena Caval Obstruction (SVCO) Invasion or external compression of SVC by disease involving: Rt lung, LNs, mediastinal disease ± thrombosis within SVC SVCO causes venous collaterals to form rate determines rate of onset of Sx/signs Page 35
36 SVCO - Epidemiology Malignancy most common cause (80-85%) Others: Infection, Thrombosis (± catheter related) 2 most common malig causes (~ 95% cases): Lung Ca: Most common ~5% of lung Ca Pts SCLC: 20% will develop SVCO (central) Lymphoma: ~5% of lymphoma Pts NHL > HL Page 36
37 SVCO - Investigations EMERGENCY Rx if STRIDOROUS indicative of central airway obstruction by tumor Otherwise most cases now emphasis is on: accurate but prompt diagnosis of the underlying malig allows the most approp Rx to be given in a timely manner Page 37
38 Conclusion More conformal palliative treatment will hopefully decrease toxicities of treatment and allow more retreatment if necessary leading to improved quality of life Page 38
39 Thank you Page 39
Radiotherapy symptoms control in bone mets. Francesco Cellini GemelliART. Ernesto Maranzano,MD. Session 5: Symptoms management
 Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Palliative RT. Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University
 Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Palliative radiotherapy in lung cancer
 New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Palliative treatments for lung cancer: What can the oncologist do?
 Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Radiotherapy and Brain Metastases. Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem
 Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. Version:
 GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Clinical Case Conference
 Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation
Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation
VINCENT KHOO. 8 th EIKCS Symposium: May 2013
 8 th EIKCS Symposium: May 2013 VINCENT KHOO Royal Marsden NHS Foundation Trust & Institute of Cancer Research St George s Hospital & University of London Austin Health & University of Melbourne Disclosures
8 th EIKCS Symposium: May 2013 VINCENT KHOO Royal Marsden NHS Foundation Trust & Institute of Cancer Research St George s Hospital & University of London Austin Health & University of Melbourne Disclosures
Enterprise Interest None
 Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Minesh Mehta, Northwestern University. Chicago, IL
 * Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
* Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
Gamma Knife Radiosurgery A tool for treating intracranial conditions. CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop
 Gamma Knife Radiosurgery A tool for treating intracranial conditions CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop ANGELA McBEAN Gamma Knife CNC State-wide Care Coordinator Gamma Knife
Gamma Knife Radiosurgery A tool for treating intracranial conditions CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop ANGELA McBEAN Gamma Knife CNC State-wide Care Coordinator Gamma Knife
Radiotherapy physics & Equipments
 Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
The Role of Radiotherapy in Metastatic Breast Cancer. Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health
 The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
DRAFT FOR CONSULTATION. Clinical Commissioning Policy Proposition: Palliative radiotherapy for bone pain
 Clinical Commissioning Policy Proposition: Palliative radiotherapy for bone pain Information Reader Box (IRB) to be inserted on inside front cover for documents of 6 pages and over, with Publications Gateway
Clinical Commissioning Policy Proposition: Palliative radiotherapy for bone pain Information Reader Box (IRB) to be inserted on inside front cover for documents of 6 pages and over, with Publications Gateway
Guidelines for the Management. Malignant Spinal Cord Compression. Final Guideline
 Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Metastatic Spinal Cord Compression
 Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK Introduction 2-5% of cancer patients have an episode of MSCC Initial
Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK Introduction 2-5% of cancer patients have an episode of MSCC Initial
Treating Multiple. Brain Metastases (BM)
") ESTRO 36 5-9 May 2017, Vienna Austria, Accuray Symposium Treating Multiple Brain Metastases (BM) with CyberKnife System Frederic Dhermain MD PhD, Radiation Oncologist Gustave Roussy University Hospital,
ESTRO 36 5-9 May 2017, Vienna Austria, Accuray Symposium Treating Multiple Brain Metastases (BM) with CyberKnife System Frederic Dhermain MD PhD, Radiation Oncologist Gustave Roussy University Hospital,
Update on management of metastatic brain disease. Peter Hoskin Mount Vernon Cancer Centre Northwood UK
 Update on management of metastatic brain disease Peter Hoskin Mount Vernon Cancer Centre Northwood UK Incidence 15-30% of patients with solid tumours will develop brain metastases Most common primary sites
Update on management of metastatic brain disease Peter Hoskin Mount Vernon Cancer Centre Northwood UK Incidence 15-30% of patients with solid tumours will develop brain metastases Most common primary sites
Disclosures. Overview 8/3/2016. SRS: Cranial and Spine
 SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
AND CHEMOTHERAPY IN PALLIATIVE CARE
 THE ROLE OF RADIOTHERAPY AND CHEMOTHERAPY IN PALLIATIVE CARE Top Ten Cancers in Public Hospital KNH 2008 (CTC) Multidisciplinary Approach Radiotherapist Radiologist Medical Oncologist PALLIATIVE CARE/ONCOLOGY
THE ROLE OF RADIOTHERAPY AND CHEMOTHERAPY IN PALLIATIVE CARE Top Ten Cancers in Public Hospital KNH 2008 (CTC) Multidisciplinary Approach Radiotherapist Radiologist Medical Oncologist PALLIATIVE CARE/ONCOLOGY
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia
 for Brain Metastasis in Nova Scotia") A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
Disclosures. Disclosures 27/01/2019. Modern approach and pitfalls in metastatic spine surgery. None.. Jeremy Reynolds
 Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Malignant Spinal cord Compression. Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania
 Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Isotopes and Palliative Radiotherapy for bone metastases
 Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Northern Suburbs Clinic for Lung Cancer (NSCLC): Targeting Lung Cancer
: Targeting Lung Cancer") Northern Suburbs Clinic for Lung Cancer (NSCLC): Targeting Lung Cancer Page 1 Phuong Tran (Rad Onc) Lung Cancer Most common cause of cancer related deaths in Australia 19% of all cancer deaths Survival
Northern Suburbs Clinic for Lung Cancer (NSCLC): Targeting Lung Cancer Page 1 Phuong Tran (Rad Onc) Lung Cancer Most common cause of cancer related deaths in Australia 19% of all cancer deaths Survival
Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey
 Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Spinal cord compression as a first presentation of cancer: A case report
 J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
Hong Kong Hospital Authority Convention 2018
 Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen?
 Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Radiation Treatment for Breast. Cancer. Melissa James Radiation Oncologist August 2015
 Radiation Treatment for Breast Cancer Melissa James Radiation Oncologist August 2015 OUTLINE External Beam Radiation treatment. (What is Radiation, doctor?) Role of radiation. (Why am I getting radiation,
Radiation Treatment for Breast Cancer Melissa James Radiation Oncologist August 2015 OUTLINE External Beam Radiation treatment. (What is Radiation, doctor?) Role of radiation. (Why am I getting radiation,
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms. Overall Clinical Significance 8/3/13
 Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Metastatic Spinal Disease
 Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Emergencies in Palliative Medicine
 Emergencies in Palliative Medicine Objectives Recognise palliative care emergencies Be aware of their existence Recognise signs and symptoms of common emergencies Anticipate occurrence of emergencies Manage
Emergencies in Palliative Medicine Objectives Recognise palliative care emergencies Be aware of their existence Recognise signs and symptoms of common emergencies Anticipate occurrence of emergencies Manage
Metastatic prostate carcinoma. Lee Say Bob July 2017
 Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Is it cost-effective to treat brain metastasis with advanced technology?
 Is it cost-effective to treat brain metastasis with advanced technology? Cost-effectiveness analysis of whole brain RT, stereotactic radiosurgery and craniotomy in HA setting Lam, Tai-Chung, Choi CW Horace,
Is it cost-effective to treat brain metastasis with advanced technology? Cost-effectiveness analysis of whole brain RT, stereotactic radiosurgery and craniotomy in HA setting Lam, Tai-Chung, Choi CW Horace,
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Isotopes and Palliative Radiotherapy for bone metastases
 Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015
 Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015 Most common brain tumor, affecting 8.5-15% of cancer patients. Treatment options: Whole brain radiation
Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015 Most common brain tumor, affecting 8.5-15% of cancer patients. Treatment options: Whole brain radiation
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Management of Brain Metastases Dr. Luis Souhami Professor Department of Radiation Oncology University,
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Management of Brain Metastases Dr. Luis Souhami Professor Department of Radiation Oncology University,
Brain Tumor Treatment
 Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Radiation 2012 econference
 Copyright 2012 Oncology Nursing Society. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, without
Copyright 2012 Oncology Nursing Society. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, without
Management of single brain metastasis: a practice guideline
 PRACTICE GUIDELINE SERIES Management of single brain metastasis: a practice guideline A. Mintz MD,* J. Perry MD, K. Spithoff BHSc, A. Chambers MA, and N. Laperriere MD on behalf of the Neuro-oncology Disease
PRACTICE GUIDELINE SERIES Management of single brain metastasis: a practice guideline A. Mintz MD,* J. Perry MD, K. Spithoff BHSc, A. Chambers MA, and N. Laperriere MD on behalf of the Neuro-oncology Disease
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
Challenging Paediatric Brain Tumours. ASP Belfast March 2017 Dr Jane Pears Consultant Paediatric Oncologist, Dublin
 Challenging Paediatric Brain Tumours ASP Belfast March 2017 Dr Jane Pears Consultant Paediatric Oncologist, Dublin Overview (i) Paediatric malignancy (ii) Central nervous system tumours (iii) Diffuse Intrinsic
Challenging Paediatric Brain Tumours ASP Belfast March 2017 Dr Jane Pears Consultant Paediatric Oncologist, Dublin Overview (i) Paediatric malignancy (ii) Central nervous system tumours (iii) Diffuse Intrinsic
Management of Acute Oncological emergencies
 Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased
 Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased analysis Roel Schlijper Fellow Radiation Oncology BC Cancer, Prince George Disclosures No conflicts
Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased analysis Roel Schlijper Fellow Radiation Oncology BC Cancer, Prince George Disclosures No conflicts
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Oncological Management of Brain Tumours. Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013
 Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Community care of Prostate Cancer. Shaun Costello Southern Cancer Network
 Community care of Prostate Cancer Shaun Costello Southern Cancer Network Introduction Why is GP follow up of prostate cancer important 4Years In Waikato Faster Cancer Treatment Reporting against the 3
Community care of Prostate Cancer Shaun Costello Southern Cancer Network Introduction Why is GP follow up of prostate cancer important 4Years In Waikato Faster Cancer Treatment Reporting against the 3
Palliative Care Emergencies
 Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer
 Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Pancreatic Cancer and Radiation Therapy
 Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Oncologic Emergencies
 Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer
 Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer Kazi S. Manir MD,DNB,ECMO,PDCR Clinical Tutor Department of Radiotherapy R. G. Kar Medical College and Hospital, Kolkata SCLC 15% of lung
Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer Kazi S. Manir MD,DNB,ECMO,PDCR Clinical Tutor Department of Radiotherapy R. G. Kar Medical College and Hospital, Kolkata SCLC 15% of lung
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advances in Radiation Therapy
 Advances in Radiation Therapy 2017 Recent Advances in Oncology Michelle Alonso-Basanta, MD PhD Helene Blum Assistant Professor Associate Chief of Clinical Operations Director of Quality Assurance Chief,
Advances in Radiation Therapy 2017 Recent Advances in Oncology Michelle Alonso-Basanta, MD PhD Helene Blum Assistant Professor Associate Chief of Clinical Operations Director of Quality Assurance Chief,
Metastasi cerebrali La Radioterapia: tecnica, frazionamento, radiosensibilizzanti
 Metastasi cerebrali La Radioterapia: tecnica, frazionamento, radiosensibilizzanti Brain Metastases Radiation Therapy of multiple brain metastases Is treatment appropriate? - Survival - QoL Brain Metastases
Metastasi cerebrali La Radioterapia: tecnica, frazionamento, radiosensibilizzanti Brain Metastases Radiation Therapy of multiple brain metastases Is treatment appropriate? - Survival - QoL Brain Metastases
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
Radiotherapy Physics and Equipment
 Radiological Sciences Department Radiotherapy Physics and Equipment RAD 481 Lecture s Title: Introduction Dr. Mohammed EMAM Ph.D., Paris-Sud 11 University Vision :IMC aspires to be a leader in applied
Radiological Sciences Department Radiotherapy Physics and Equipment RAD 481 Lecture s Title: Introduction Dr. Mohammed EMAM Ph.D., Paris-Sud 11 University Vision :IMC aspires to be a leader in applied
Prophylactic Cranial Irradiation and Thoracic Radiotherapy in Extensive Stage Small-Cell Lung Cancer
 Prophylactic Cranial Irradiation and Thoracic Radiotherapy in Extensive Stage Small-Cell Lung Cancer Dr Neil Bayman Consultant Clinical Oncology ESMO-Christie Preceptorship Programme in Lung Cancer, March
Prophylactic Cranial Irradiation and Thoracic Radiotherapy in Extensive Stage Small-Cell Lung Cancer Dr Neil Bayman Consultant Clinical Oncology ESMO-Christie Preceptorship Programme in Lung Cancer, March
Stereotactic Radiosurgery. Extracranial Stereotactic Radiosurgery. Linear accelerators. Basic technique. Indications of SRS
 Stereotactic Radiosurgery Extracranial Stereotactic Radiosurgery Annette Quinn, MSN, RN Program Manager, University of Pittsburgh Medical Center Using stereotactic techniques, give a lethal dose of ionizing
Stereotactic Radiosurgery Extracranial Stereotactic Radiosurgery Annette Quinn, MSN, RN Program Manager, University of Pittsburgh Medical Center Using stereotactic techniques, give a lethal dose of ionizing
Recognition & Treatment of Malignant Spinal Cord Compression
 Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
CNS Metastases in Breast Cancer
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer CNS Metastases in Breast Cancer CNS Metastases in Breast Cancer Version 2006: Maass / Junkermann Version 2007 2009: Bischoff
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer CNS Metastases in Breast Cancer CNS Metastases in Breast Cancer Version 2006: Maass / Junkermann Version 2007 2009: Bischoff
ONLINE CONTINUING EDUCATION ACTIVITY
 ONLINE CONTINUING EDUCATION ACTIVITY Take free quizzes online at acsjournals.com/ce ARTICLE TITLE: Palliative Radiotherapy at the End of Life: A Critical Review CONTINUING MEDICAL EDUCATION ACCREDITATION
ONLINE CONTINUING EDUCATION ACTIVITY Take free quizzes online at acsjournals.com/ce ARTICLE TITLE: Palliative Radiotherapy at the End of Life: A Critical Review CONTINUING MEDICAL EDUCATION ACCREDITATION
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
Update on Management of Malignant Spinal Cord Compression. Heino Hugel Consultant in Palliative Medicine University Hospital Aintree
 Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
This LCD recognizes these two distinct treatment approaches and is specific to treatment delivery:
 National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: 77371, 77372, 77373 LCD ID Number: L33410 J-N FL Responsible
National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: 77371, 77372, 77373 LCD ID Number: L33410 J-N FL Responsible
North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO)
") North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO) UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Original Prepared by NMcL April 2016
North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO) UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Original Prepared by NMcL April 2016
Session 5: Isotope therapies and palliative radiotherapy
 Session 5: Isotope therapies and palliative radiotherapy Jeffrey Tuan, FRCR Radiation Oncology National Cancer Centre Singapore 15 Dec 2016 Bone metastases SREs are clinically important endpoints The burden
Session 5: Isotope therapies and palliative radiotherapy Jeffrey Tuan, FRCR Radiation Oncology National Cancer Centre Singapore 15 Dec 2016 Bone metastases SREs are clinically important endpoints The burden
Radiotherapy What are our options and what is on the horizon. Dr Kevin So Specialist Radiation Oncologist Epworth Radiation Oncology
 Radiotherapy What are our options and what is on the horizon Dr Kevin So Specialist Radiation Oncologist Epworth Radiation Oncology Outline Advances in radiotherapy technique Oligo - disease Advancements
Radiotherapy What are our options and what is on the horizon Dr Kevin So Specialist Radiation Oncologist Epworth Radiation Oncology Outline Advances in radiotherapy technique Oligo - disease Advancements
MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION
 CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Selecting the Optimal Treatment for Brain Metastases
 Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Combined modality treatment for N2 disease
 Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
20. Background. Oligometastases. Oligometastases: bone (including spine) and lymph nodes
 and lymph nodes") 125 20. Oligometastases Background The oligometastatic state can be defined as 1 3 isolated metastatic sites, typically occurring more than six months after successful treatment of primary disease. 1 In
125 20. Oligometastases Background The oligometastatic state can be defined as 1 3 isolated metastatic sites, typically occurring more than six months after successful treatment of primary disease. 1 In
Cécile Le Péchoux Department of Radiation Oncology, Institut Gustave Roussy, Villejuif France Amsterdam 2010
 Prophylactic Cranial Irradiation in Lung Cancer Cécile Le Péchoux Department of Radiation Oncology, Institut Gustave Roussy, Villejuif France Amsterdam 2010 Prophylactic cranial irradiation PCI was introduced
Prophylactic Cranial Irradiation in Lung Cancer Cécile Le Péchoux Department of Radiation Oncology, Institut Gustave Roussy, Villejuif France Amsterdam 2010 Prophylactic cranial irradiation PCI was introduced
Conflict of interest disclosure
 Stereotactic Body Radiation Therapy (SBRT) I: Radiobiology and Clinical Experience Brian Kavanagh, M.D., MPH University of Colorado Eric Chang, M.D. UT MD Anderson Conflict of interest disclosure I have
Stereotactic Body Radiation Therapy (SBRT) I: Radiobiology and Clinical Experience Brian Kavanagh, M.D., MPH University of Colorado Eric Chang, M.D. UT MD Anderson Conflict of interest disclosure I have
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Malignant melanoma: assessment and management of malignant melanoma 1.1 Short title Malignant Melanoma 2 The remit The Department
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Malignant melanoma: assessment and management of malignant melanoma 1.1 Short title Malignant Melanoma 2 The remit The Department
a Phase II Randomised Controlled Trial Matthias Guckenberger
 Dose-intensified Image-guided Fractionated Stereotactic Body Radiation Therapy for Painful Spinal Metastases (DOSIS) versus Conventional Radiation Therapy: a Phase II Randomised Controlled Matthias Guckenberger
Dose-intensified Image-guided Fractionated Stereotactic Body Radiation Therapy for Painful Spinal Metastases (DOSIS) versus Conventional Radiation Therapy: a Phase II Randomised Controlled Matthias Guckenberger
Brain metastases: changing visions
 Brain metastases: changing visions Roberto Spiegelmann, MD Baiona, 2014 Head, Stereotactic Radiosurgery Unit Dept of Neurosurgery, Chaim Sheba Medical Center Tel Hashomer, Israel The best current estimate
Brain metastases: changing visions Roberto Spiegelmann, MD Baiona, 2014 Head, Stereotactic Radiosurgery Unit Dept of Neurosurgery, Chaim Sheba Medical Center Tel Hashomer, Israel The best current estimate
Palliative Care Emergencies. Additional module if needed
 Palliative Care Emergencies Additional module if needed Learning objectives Understand emergency /urgent / important Describe common emergencies in PC Explore principles of essential management Outline
Palliative Care Emergencies Additional module if needed Learning objectives Understand emergency /urgent / important Describe common emergencies in PC Explore principles of essential management Outline
Opportunity for palliative care Research
 Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Treatment of Brain Metastases
 1 Treatment of Brain Metastases An Overview and Pending Research Questions To Answer Olav E. Yri, MD, PhD www.ntnu.no/prc European Palliative Care Research Centre (PRC) The brain metastases diagnosis Outline
1 Treatment of Brain Metastases An Overview and Pending Research Questions To Answer Olav E. Yri, MD, PhD www.ntnu.no/prc European Palliative Care Research Centre (PRC) The brain metastases diagnosis Outline
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
รศ.นพ. ประเสร ฐ เล ศสงวนส นช ย
 รศ.นพ. ประเสร ฐ เล ศสงวนส นช ย Position: ผ อำนวยกำรฝ ำยด แลผ ป วยโรคมะเร ง โรงพยำบำลว ฒโนสถ อำจำรย พ เศษสำขำร งส ร กษำและมะเร งว ทยำ ภำคว ชำร งส ว ทยำ คณะแพทย ศำสตร จ ฬำลงกรณ มหำว ทยำล ย และอด ตนำยกสมำคมร
รศ.นพ. ประเสร ฐ เล ศสงวนส นช ย Position: ผ อำนวยกำรฝ ำยด แลผ ป วยโรคมะเร ง โรงพยำบำลว ฒโนสถ อำจำรย พ เศษสำขำร งส ร กษำและมะเร งว ทยำ ภำคว ชำร งส ว ทยำ คณะแพทย ศำสตร จ ฬำลงกรณ มหำว ทยำล ย และอด ตนำยกสมำคมร
Radiotherapy for Patients with Symptomatic Intramedullary Spinal Cord Metastasis
 J. Radiat. Res., 52, 641 645 (2011) Regular Paper Radiotherapy for Patients with Symptomatic Intramedullary Spinal Cord Metastasis Haruko HASHII 1,4 *, Masashi MIZUMOTO 1,4 *, Ayae KANEMOTO 1,4, Hideyuki
J. Radiat. Res., 52, 641 645 (2011) Regular Paper Radiotherapy for Patients with Symptomatic Intramedullary Spinal Cord Metastasis Haruko HASHII 1,4 *, Masashi MIZUMOTO 1,4 *, Ayae KANEMOTO 1,4, Hideyuki