Relapsing APL. Pierre Fenaux Hôpital St Louis, Paris 7 University French Belgian Swiss APL group DES
|
|
|
- Ross Morris
- 6 years ago
- Views:
Transcription


1 Relapsing APL Pierre Fenaux Hôpital St Louis, Paris 7 University French Belgian Swiss APL group DES GET LAP Groupe d Etude et de Travail Sur les Leucémies Aigues Promyélocytaires
2 Frequency of relapse in APL? In our ongoing APL 2006 trial: 350 standard risk patients aged <70 years included between Dec 2006 and Dec % CR 7 relapses GET LAP Groupe d Etude et de Travail Sur les Leucémies Aigues Promyélocytaires
3 Relapsing APL How do APL relapse? When should relapse be treated? Treatment of hematological relapse Treatment of extra hematological relapse
4 Relapsing APL How do APL relapse? When should relapse be treated? Treatment of hematological relapse Treatment of extra hematological relapse
5 How do APL relapse? Clinical relapse Hematological Extra hematological Molecular relapse
6 How do APL relapse? Clinical relapse Hematological Extra hematological Molecular relapse
7 Hematological relapses Generally during the first 3 years Late relapses : Beyond 4 years: 12% of relapses (Kelaidi, Leukemia, 2007) Nine (4.6%) relapses>3 years from CR, the last occurred after 4.6 years (Douer, Leuk Res, 2013)
8 Extra hematological relapses 1.5% (De Botton, 2006; Montesinos, 2009) to 3% (Vega- Ruiz, 2009) APL develop extramedullary relapse Largely predominate in the CNS 10/14 (De Botton) 7/8 (Vega-Ruiz) Often associated to molecular marrow relapse
9 Predictive factors of Extra hematological relapses De Botton (Leukemia, 2006): age < 45 WBC >10 G/L bcr 3 Montesinos(Haematologica,2009) WBC >10G/L CNS bleeding during induction Role of High dose AraC and/or intrathecal MTX+ AraC to prevent CNS relapse in patients with WBC > 10G/L? (De Botton, 2006; Lengfelder, 2008)
10 Outcome of extramedullary(emd) relapse EMD carry a poor prognosis Median survival from EMD relapse: 6.7 months (vs 26.3 for marrow relapses (De Botton, Leukemia, 2006) 13 months (Montesinos, Haematologica,2009) 5 of 7 patients died within 4 months (Vega- Ruiz, Int J Hem, 2009)
11 How do APL relapse? Clinical relapse Hematological Extra hematological Molecular relapse
12 Molecular relapse Defined by 2 successive PCR positive assays, with stable or rising PML-RAR transcript levels detected in independent samples analyzed in 2 laboratories Evidence demonstrated with low sensitivity assays ( 10-4) RQ-PCR can also capture most relapses at the molecular level (Grimwade, JCO, 2009) Justifies monitoring of mrd every 3 months?
13 Relapsing APL How do APL relapse? When should relapse be treated? Treatment of hematological relapse Treatment of extra hematological relapse
14 Should APL relapse be treated when only molecular? Lo Coco (Blood, 1999) 14 molecular relapses Salvage treatment: ATRA+ CT +/- transplantation 12/14 molecular CR achieved 2 year outcome Molecular relapse: 92% OS Hematological relapse(historical): 44% OS
15 Should APL relapse be treated when only molecular? Esteve (Leukemia, 2007) 52 relapses: 16 MOL, 36 HEM Salvage treatment: ATRA+ CT +/- transplantation 88 vs 81 % second molecular CR 5 year outcome Hematological relapse: 64 % relapse, 24% OS Molecular relapse: 30% relapse, 64% OS
16 Management of APL: recommendations from an expert panel on behalf of the European LeukemiaNet Miguel A. Sanz,1 David Grimwade,2 Martin S. Tallman,3 Bob Lowenberg,4 Pierre Fenaux,5 Elihu H. Estey,6 Tomoki Naoe,7 Eva Lengfelder,8 Thomas Bu chner,9 Hartmut Do hner,10 Alan K. Burnett,11 and Francesco Lo-Coco BLOOD 2009 Recommendation : For patients with confirmed molecular relapse (defined as 2 successive PCRpositive assays, with stable or rising PML-RARA transcript levels detected in independent samples analyzed in 2 laboratories) preemptive therapy has to be started promptly to prevent frank relapse. Level of evidence: IIa Grade of recommendation: B
17 Relapsing APL How do APL relapse? When should relapse be treated? Treatment of hematological relapse Treatment of extra hematological relapse
18 Arsenic trioxide in relapsing APL Ref Dosing Nb pts CR rate Post induction Long term outcome As 2 O 3 alone (n =18) 12/18 relapses Niu 0.15mg/kg/ % As 2 O 3 + CT (n =11) 2/11 relapses Shen 0.08 mg/kg % variable 2 year relapse free survival : 61 % Kwong 10 mg % Ida 7/8 still in CR 6 in molecular CR Soignet 0.15 mg/k % Allo or auto (n=12) 11 still in CR As 2 O 3 (n = 21) 9 still in CR Ohnishi 0.15 mg/k % As 2 O 3 median CR duration : 8 months
19 Treatment of APLmolecular relapse by Gentuzumab ozogamycin(go) (Lo Coco,Blood,2004) 16 pts with molecular relapse (8,5,2,1) GO 6mg/m2 x molecular CR achieved 7 pts still in CR (7+ to 31+ months),7 relapses after 3 to 15 months
20 GO in relapsed APL Sustained molecular remission after low dose gemtuzumab-ozogamicin in elderly patients with advanced acute promyelocytic leukemia. Breccia M, Haematologica Gemtuzumab ozogamicin successfully induced molecular remission in relapsed therapy-related acute promyelocytic leukemia].shimokawa T, Rinsho Ketsueki Sustained molecular remission after arsenic trioxide and gemutuzumab ozogamicin in a pediatric patient with relapsed acute promyelocytic leukemia. Inoue A,Pediatr Hematol Oncol Molecular remission induced by gemtuzumab ozogamicin in an elderly patient with relapsed acute promyelocytic leukemia]. Yago K,Rinsho Ketsueki Treatment of relapsed acute promyelocytic leukemia with gemtuzumab ozogamicin and all-trans retinoic acid. Tageja N, J Chemother. 2009
21 Other retinoids in relapsing APL? Tamibarotene (Am 80) Differentiation(10 fold vs ATRA) Reduced affinity for CRABP Tobita (Blood, 1997): 24 relapses after ATRA. 58% CR Takeuchi (GTKR, 2006): 23 relapses. 78% CR Naina HV (JCO. 2011) Successful treatment of relapsed and refractory extramedullary APL with tamibarotene. Di Veroli (BJH. 2010) Molecular remission in advanced APL after treatment with the oral synthetic retinoid Tamibarotene.
22 Other retinoids in relapsing APL? Liposomal ATRA (Tsimberidou, Leuk Lymphoma, 2006) 10 of 26 newly diagnosed APL treated with liposomal ATRA alone were still in CR at 5 years
23 Management of APL: recommendations from an expert panel on behalf of the European LeukemiaNet Miguel A. Sanz,1 David Grimwade,2 Martin S. Tallman,3 Bob Lowenberg,4 Pierre Fenaux,5 Elihu H. Estey,6 Tomoki Naoe,7 Eva Lengfelder,8 Thomas Bu chner,9 Hartmut Do hner,10 Alan K. Burnett,11 and Francesco Lo-Coco BLOOD Although ATRA in combination with chemotherapy can be used as salvage therapy, ATObased regimens are presently regarded the first option for treatment of relapsed APL. IV C
24 Management of APL: recommendations from an expert panel on behalf of the European LeukemiaNet Miguel A. Sanz,1 David Grimwade,2 Martin S. Tallman,3 Bob Lowenberg,4 Pierre Fenaux,5 Elihu H. Estey,6 Tomoki Naoe,7 Eva Lengfelder,8 Thomas Bu chner,9 Hartmut Do hner,10 Alan K. Burnett,11 and Francesco Lo-Coco BLOOD Patients achieving second CR should receive intensification with SCT or chemotherapy, if possible. IV C
25 Prognostic relevance of RT-PCR pretransplant in APL autografted in CR 2 (Meloni, Blood, 1997) 15 patients autografted in CR 2 7 PCR + in their pretransplant marrow: all relapsed after a median of 5 months 8 PCR-: 1 relapse, other patients in CR2 at a median of 26 months
 50 21% ( 7 yrs) 79%(7 yrs.) 60%(7 yrs.")
26 APL in CR2:Allo and auto SCT (De Botton,JCO,2005) No. Pts Relapse DFS OS TRM Auto SCT APL Study Group** (Europe) 50 21% ( 7 yrs) 79%(7 yrs.) 60%(7 yrs.) 6% Allo SCT APL Study Group** (Europe) 25 8% 52% 52% 39%
27 P(No event) Event-free survival (EFS) from transplantation AUTO ALLO Days from transplant
28 Allo or auto in relapsing APL? Autologous and allogeneic SCT in APL in CR2 (Kohno, Int J Hemat, 2008) 15 autos and 13 allos between 1999 and year DFS 68.9% (auto) vs 46.2% (allo) Outcomes in patients with relapsed or refractory APL treated with or without auto or allo SCT. (Pemmaraju N, Clin Lymphoma Myeloma Leuk. 2013) 7-year overall survival was 85.7%, 49.4%, and 40% in the auto-hct, allo-hct, and CT groups, respectively (P =.48). Autologous and allogeneic SCT in APL (Sanz, BMT, 2007) 625 auto or allo after year leukemia free survival CR 2: 69% (auto) 68% ( allo) CR 1: 51% (auto) 59% ( allo)
29 Allo SCT after ATO Salvage Post-transplant survival (Soignet,Dombret, Sem Oncol, 2002) % % 8 0 % 8 0 % 60 % 40 % At risk deaths 2-year est % 60 % 40 % 1 st rel. > 2 nd rel. At risk deaths 2-year est % % 2 0 % 2 0 % 0 % Months 0 % Months Median follow-up: 30 months post SCT (range, 9.5 to 45)
30 Role of hematopoietic stem cell transplantation for relapsed acute promyelocytic leukemia: A retrospective analysis of JALSG-APL97 Hiroyuki Fujita, 1,19 Norio Asou, 2 Masako Iw anaga, 3 Rie Hyo, 4 Shosaku Nomura, 5 Hitoshi Kiyoi, 6 Masaya Okada, 7 Youko Inaguma, 8 Mitsuhiro Matsuda, 9 Takahiro Yamauchi, 10 Shigeki Ohtake, 11 Tohru Izumi, 12 Chiaki Nakaseko, 13 Yoshiaki Ishigatsubo, 14 Katsuji Shinagaw a, 15 Akihiro Takeshita, 16 Yasushi Miyazaki, 17 Kazunori Ohnishi, 16 Shuichi Miyaw aki, 18 Tomoki Naoe 6 and for the Japan Adult Leukemia Study Group 1 Department of Hematology, Yokohama Saiseikai Nanbu Hospital, Yokohama; 2 Department of Hematology, Kumamoto University School of Medicine, Kumamoto; 3 Graduate School of Public Health, Teikyo University, Tokyo; 4 Department of HSCT Data Management and Biostat istics, Nagoya University School of Medicine, Nagoya; 5 First Department of Internal Medicine, Kansai Medical University, Moriguchi; 6 Department of Hematology and Oncology, Nagoya University Graduate School of Medicine, Aichi; 7 Department of Internal Medicine, Division of Hematology, Hyogo College of Medicine, Nishinomiya; 8 Department of Hematology, Fujita Health University, Toyoake; 9 Department of Internal Medicine, PL General Hospital, Tondabayashi; 10 Department of Hematology and Oncology, University of Fukui, Fukui; 11 School of Health Sciences, Kanazawa University, Kanazawa; 12 Department of Hematology, Tochigi Cancer Center, Utsunomiya; 13 Department of Hematology, Chiba University, Chiba; 14 Department of Internal Medicine and Clinical Immunology, Yokohama City University Graduate School of Medicine, Yokohama; 15 Department of Hematology and Oncology, Okayama University Graduate of School, Okayama; 16 Department of Internal Medicine III, Hamamatsu University School of Medicine, Hamamatsu; 17 Department of Hematology, Atomic Bomb Disease and Hibakusya Medicine Unit, Atomic Bomb Disease Institute, Nagasaki University Graduate School of Biomedical Sciences, Nagasaki; 18 Division of Hematology, Tokyo Metropolit an Ohtsuka Hospital, Tokyo, Japan (Received April 2, 2013 Revised June 25, 2013 Accepted July 1, 2013 Accepted manuscript online July 10, 2013) For patients with relapsed acute promyelocytic leukemia (APL), all-trans retinoic acid-based salvage regimens can achieve second complete remission (CR2), but the optimal post-remission strategy for APL patients after CR2 remains unclear. Hematopoietic stem cell transplantation (HSCT) during CR2 might be effective, but data on the role of HSCT for APL patients after CR2 are limited in Japan. We retrospectively analyzed outcomes for 57 relapsed APL patients w ho achieved CR2 in the JALSG APL97 study. Of those, six received autologous (auto)-hsct, 21 received allogeneic (allo)-hsct, and 30 received various regimens other than HSCT. The 5-year event-free survival (EFS) rate, overall survival (OS) rate and cumulative incidence of relapse (CIR) w ere 50.7%, 77.4% and 51.0% in the non-hsct group, 41.7%, 83.3% and 58.3% in the auto-hsct group and 71.1%, 76.2% and 9.8% in the allo-hsct group, respectively. Both the EFS rate and CIR w ere signifi cantly better in the allo-hsct group than in other groups. Allo-HSCT appears effective in APL patients in CR2, with a low relapse rate beyond a relatively early transplantationrelated mortality (19%). Among older patients (age 40 years), the 5-year OS was signifi cantly better in the non-hsct group than in the HSCT group (78.0% vs 40.5%; P = 0.04). Further prospective studies with larger patient numbers are required to confi rm the impact of HSCT alone and in combination with arsenic trioxide on outcomes for patients with APL in CR2. (Cancer Sci, doi: /cas.12230, 2013) he introduction of all-trans retinoic acid (ATRA) has Tbrought about marked progress in the treatment of acute promyelocytic leukemia (APL), but relapse still occurs in approximately 15 25% of patients. (1 3) Most of the relapsed patients were able to achieve second complete remission (CR2) using ATRA-based salvage regimens (4 6) or recent arsenic trioxide (ATO)-based salvage regimens. (7,8) After achieving CR2, most patients need to receive post-remission treatments to reduce minimal residual disease (MRD). A variety of post-remission strategies have been used, including further consolidation chemotherapy, (3) hematopoietic stem cell transplantation (HSCT), (6,9 11) continued treatment with ATO (7,8,12) or a combination of such therapies; however, the optimal post-remission therapy remains controversial. Previous studies have reported that ATO-based post-remission therapy for patients with APL in CR2 resulted in superior survival compared with chemotherapy alone or HSCT alone. (13) Likewise, HSCT strategies for patients with APL in CR2 resulted in better outcomes than chemotherapy alone, despite being associated with high transplantation-related mortality (TRM). (9 11) Moreover, autologous HSCT (auto-hsct) was much better than allogeneic HSCT (allo-hsct) for patients in CR2 who achieved molecular remission. (6,9) Recently, in a phase 2 prospective study, our Japan Adult Leukemia Study Group (JALSG) reported the efficacy of sequential treatment using ATO followed by auto-hsct for 25 patients with relapsed APL. (14) However, evidence has been lacking in terms of the role of auto-hsct alone on the cumulative relapse rate or efficacy for patients with APL in CR2 who were ineligible for the phase 2 study regimens. Moreover, in situations where no guidelines regarding the optimal choice of auto- or allo-hsct in CR2 have been determined, the role of HSCT alone in post-remission therapies for patients with APL in CR2 is yet to be evaluated. Therefore, the present study aimed to evaluate in detail the efficacies of HSCT alone for APL patients in CR2 by comparing outcomes, including cumulative relapse rate, both for APL patients who underwent auto-hsct or allo-hsct during CR2 and for those who did not receive HSCT during long-term follow up. Materials and Methods Data source. Information on patients with APL in CR2 and the salvage treatment applied were obtained from the JALSG APL97 study. (15) Between May 1997 and June 2002, a total of 302 adult patients with previously untreated de novo APL were registered in this study. The main eligibility criteria included diagnosis of APL with t(15;17) and or the PML-RARA fusion gene and age between 15 and 70 years. For remission induction therapy, patients received ATRA either 19 To whom correspondence should be addressed. hfujita@feel.ocn.ne.jp This study isregistered at under C doi: /cas Cancer Sci Japanese Cancer Association
31
32 haematologica 2011; 96(9) Nine patients with relapsed APL treated with prolonged ATRA and ATO All patients received ATO/ATRA according to the schedule reported by Estey et al Of the 9 patients, 8 remained in prolonged second CRm for a median time of 25 months (range 11-50)
33 Management of APL: recommendations from an expert panel on behalf of the European LeukemiaNet Miguel A. Sanz,1 David Grimwade,2 Martin S. Tallman,3 Bob Lowenberg,4 Pierre Fenaux,5 Elihu H. Estey,6 Tomoki Naoe,7 Eva Lengfelder,8 Thomas Bu chner,9 Hartmut Do hner,10 Alan K. Burnett,11 and Francesco Lo-Coco BLOOD Allogeneic HSCT is recommended for patients failing to achieve a second molecular remission. IV C
34 Management of APL: recommendations from an expert panel on behalf of the European LeukemiaNet Miguel A. Sanz,1 David Grimwade,2 Martin S. Tallman,3 Bob Lowenberg,4 Pierre Fenaux,5 Elihu H. Estey,6 Tomoki Naoe,7 Eva Lengfelder,8 Thomas Bu chner,9 Hartmut Do hner,10 Alan K. Burnett,11 and Francesco Lo-Coco BLOOD Autologous HSCT is a valid option for patients without detectable MRD in the marrow and with an adequate PCR negative harvest. IIa B
35 Management of APL: recommendations from an expert panel on behalf of the European LeukemiaNet Miguel A. Sanz,1 David Grimwade,2 Martin S. Tallman,3 Bob Lowenberg,4 Pierre Fenaux,5 Elihu H. Estey,6 Tomoki Naoe,7 Eva Lengfelder,8 Thomas Bu chner,9 Hartmut Do hner,10 Alan K. Burnett,11 and Francesco Lo-Coco BLOOD For patients in whom HSCT is not feasible, the available options include repeated cycles of ATO with or without ATRA with or without chemotherapy. IV C
36 As203 in relapsing APL: French Belgian Swiss experience (X Thomas et al, Hematologica, 2006) 28 pts (R1=22;R>1=6) between 2002 and 2005 Median previous CR duration 20 m (1-74) 24 CR, 2 early deaths, 2 leukemic resistance GET LAP Groupe d Etude et de Travail Sur les Leucémies Aigues Promyélocytaires

37 As203 in relapsing APL: French Belgian Swiss experience (X Thomas et al) 2 y LFS 2y OS Grade III-IV infections With As2O3 84% 79% 24% Without As2O3 47% 51% 54%
38 Relapsing APL How do APL relapse? When should relapse be treated? Treatment of hematological relapse Treatment of extra hematological relapse
39 Management of APL: recommendations from an expert panel on behalf of the European LeukemiaNet Miguel A. Sanz,1 David Grimwade,2 Martin S. Tallman,3 Bob Lowenberg,4 Pierre Fenaux,5 Elihu H. Estey,6 Tomoki Naoe,7 Eva Lengfelder,8 Thomas Bu chner,9 Hartmut Do hner,10 Alan K. Burnett,11 and Francesco Lo-Coco BLOOD 2009 For patients with CNS relapse, induction treatment consists of weekly triple intrathecal therapy (ITT) with methotrexate, hydrocortisone, and cytarabine until complete clearance of blasts in the cerebrospinal fluid, followed by 6 to 10 more spaced out ITT treatments as consolidation. Systemic treatment should also be given. IV C
40 New treatmemts in extramedullary(emd) relapse ATO Au(Blood, 2009): cerebrospinal fluid arsenic linearly correlated to plasma arsenic level (17.7%), with individual variations Plasma/CSF ratio not influenced by intrathecal chemotherapy or blasts in CSF Therapeutic levels obtained in CSF in all patients tested intrathecal liposomal Ara C?
41 CNS at First Relapse In APL. A Report on 2 Multicenter Trials (APL 93 and APL 2000) G Ferini (ASH, 2011) -6 first relapses involving the CNS, representing 3% of the relapses -pts salvaged by intrathecal CT, combined to ATRA and systemic CT in APL 93, and ATO in APL 2000 trial. -4 pts durably salvaged by auto SCT (n= 3 ) and 1 after ATO and CT GET LAP Groupe d Etude et de Travail Sur les Leucémies Aigues Promyélocytaires
42 Perspectives in relapsing/refractory APL Very few truly resistant cases (< 0.5%) Fewer relapses but more difficult to treat Mechanisms of relapse/resistance? PML- RAR gene mutations RAR (Gallagher, Blood,2102) PML (Goto, Blood,2011) Other mechanisms? Whole genome sequencing
43 Treatment of APL in specific subgroups Older patients children
44 Treatment of newly diagnosed APL in the elderly (Ades, ASH 2009) Joint analysis of elderly patients included in: PETHEMA group trials (LPA96 and LPA99) European APL group trials (APL93 and APL2000) consecutive newly diagnosed APL pts enrolled in the 4 trials, 1288 (81%), aged <60 y 105 (6.6%), aged y 91 (5.7%) aged y 91 (5.7%) and aged > 70 y
45 Patient characteristics Age = <60 Age = Age = Age >=70 Age WBC Platelets Fibrinogen Sanz s Score Low Int High 19.7% 51.9% 28.3% 27.6% 37.4% 35.2% 29.6% 39.6% 30.7% 28.6% 46.1% 25.3%
46 Complete Remission(CR) Rate CR rate was significantly higher in younger patients And decreased with age (p=0.002) Only reason for decreased CR rate in elderly patients: more early deaths Age <60 y y y >70 y CR Rate (%) 94.6% 84.8% 81.8% 78.4%
47 Cumulative incidence of Relapse(CIR) 5y-CIR similar in young and elderly patients (p=0.63) Death in CR increased with age Age <60 y y y >70 y 5y CIR (%) 16.5% 19.1% 11.9% 13.5% Death in CR 3.1% 11.8% 14.6% 17.8%
48 Overall Survival (%) Overall Survival curve 0.8 Less than 60 y y y >70 y Time (Months)
49 Relapse-free survival (%) 100 >70 y y P = Time (months)




50 Children Adolescent APL in children ( Bally, JCO, 2012) Adults 833 patients, 84 enfants n % Protocol APL APL Age 0-12y y y
51 Pt characteristics Age <12 Age = Age = P value Age (y) WBC (G/L) Platelets(G/L) Fibrinogen (g/l) Sanz s Score Low Int High 3 (12%) 10 (38%) 13 (50%) 15 (26%) 27 (47%) 16 (28%) 336 (34%) 415 (42%) 244 (24%) %M3v
52 Complete Remission Rate Complete Remission rate was similar across all age groups Age CR Rate (%) <12 y 13-18y y 92% 100% 94.5%
53 Cumulative incidence of Relapse The 5 year cumulative incidence of relapse (CIR) was rather similar across age groups Age <12 y 13-18y y 5y-CIR (%) 33% 20% 23% p=0.3 p=0.5
 10 (38%) 13 (50%) %M3v 23 Age 2 10,5 WBC 8 14,8 Platelets 13 36 Fibrinogen 1,75 1,4 Sanz s Score")
54 Children 0-4 years 5-12 years 0-12 y Age (y) 6 WBC (G/L) 10,8 Platelets(G/L) 23 Fibrinogen (g/l) 1.4 Sanz s Score Low Int High 3 (12%) 10 (38%) 13 (50%) %M3v 23 Age 2 10,5 WBC 8 14,8 Platelets Fibrinogen 1,75 1,4 Sanz s Score Low Int High %M3v 4/12 2/14
55 Outcome of children <4 years 0-4 years 5-12 years P value CR rate 11/12 13/14 NS 5 year Cumulative incidence of relapse 47% year Overall Survival 72% 78.9 NS

 0 1000 2000 3000 4000 5000 Time (Days) Aged 5-12 y 0 1000 2000 3000 4000")
56 Cumulative incidence of Relapse Cumulative incidence of Relapse Very young children 0-4 years 5-12 years Children Adolescent Adults Aged 0-4 y Aged 0-12 y 47% vs 18.9% (p=0.03) Time (Days) Aged 5-12 y Time (Days)
57
58 European Project for Salvage Therapy of Relapsed APL Treatment Recommendation Registry 10 th Annual Symposium of the European LeukemiaNet 5 th February 2013 Eva Lengfelder III. Medizinische Universitätsklinik Mannheim, University of Heidelberg
59
60 European Recommendation for Salvage Therapy in Relapsed APL with ATO HLA typing & Donor search Induction ATO Consolidation ATO + ATRA Molecular assessment (RT-PCR) Available therapeutic options 1. Intensification therapy a. AutoSCT b. AlloSCT c. ATRA + HD/CHT ± AutoSCT 2. Maintenance therapy a. ATRA + LD/CHT b. ATRA + ATO ± GO Criteria for choice 1. PCR status: AutoSCT can be considered only in PCR -ve cases 2. Donor availability 3. Age, clinical condition, and other considerations, at centre discretion, can determine the option of either intensification or maintenance therapy.
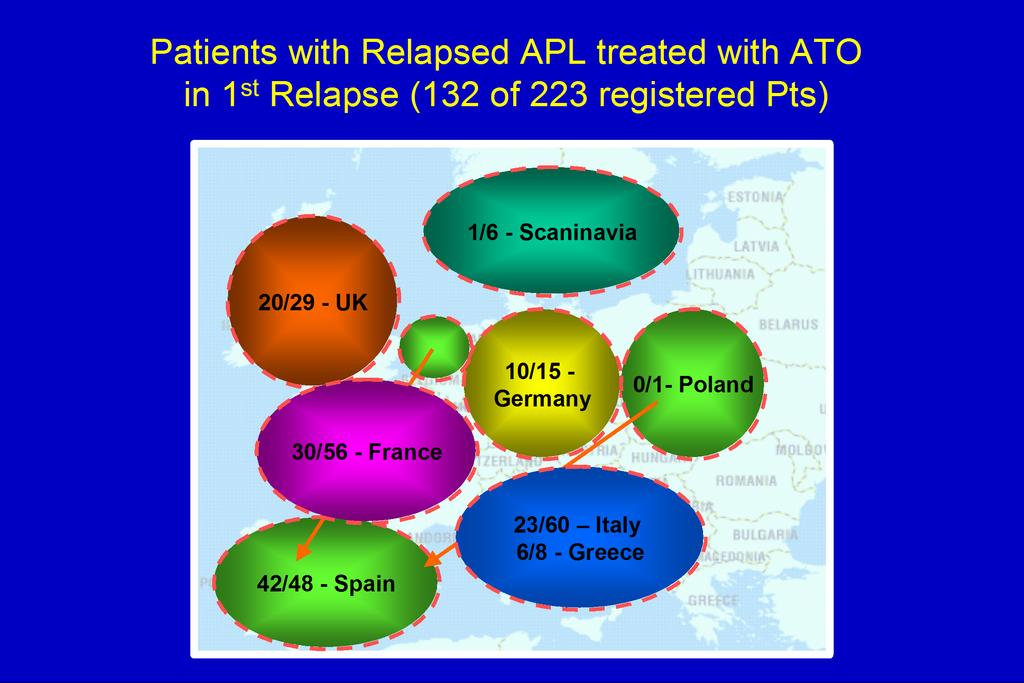
61 Registered Patients with Relapsed APL (26 th of Jan., 2013) Therapy with ATO in first relapse n = 132 hematological n = 84 (bone marrow) molecular n = 38 (bone marrow) extramedullary n = 10 (CNS 8, other 2)
62 Treatment (n=132) ATO: ATRA: 0.15 mg/m²/day (or comparable regimens) 45 mg/m²/day Induction therapy (n=132): median duration: 34 d (16-93) ATO mono 67 % ATO + ATRA 34% First consol. cycle (n=100): 5 days weekly for 5 weeks ATO mono 50 % ATO + ATRA 35 % other 15 % Intrathecal therapy: hydrocortisone CNS relapse (prophylaxis, few cases) methotrexate ± ara-c irradiation chemotherapy
63 Treatment Results (n=126) Molecular relapse (n=37) Hematological relapse (n=79) Extramedullary relapse (n=10) Results after induction CR (hematological) 70/79 88% 9/9 100% Death 0 6/79 8% 0 Resistance 3/79 4% 0 PCR -ve 19/36 53% 30/62 48% 9/9 100% PCR +ve) 17/36 47% 32/62 52% 0 Results after consolidation 1 Molecular remission 16/25 64% 29/42 69% 6/7 86%
64 Symptoms/ Side Effects during Induction Therapy with ATO Symptoms during Mol. + extramed. Hematolog. induction with ATO relapse relapse (evaluable patients) n=47 n=79 P - value APL diff. Syndrome (n=111) 2 % 19 % <0.01 Dexamethason (n=110) 2 % 25 % <0.001 Leukocytosis/ chemoth. ( n=122) 0 35 % < Interruption of ATO (n=113) 2 % 18 % <0.01
65 Overall Survival after First Relapse n = % Median follow up 2.7 y (5 d 9.5 y)
66 Event Free Survival after First Relapse n = %
67 Postconsolidation Therapy (n=126) Patients RT-PCR at transplantation positive negative no inform. n % n n n Allo. transpl. 23 (18) 10 (43%) 7 (30%) 6 (26%) Auto. transpl. 46 (37) 1 (2%) 37 (80%) 8 (17%) No transpl. 57 (45) (further ATO GO, chemotherapy, too early)
68 Overall Survival according to Postconsolidation Therapy n=23 n=46 n=54
Which is the best treatment for relapsed APL?
 Which is the best treatment for relapsed APL? 7th International Symposium on Acute Promyelocytic Leukemia, Rome, September 24 27, 2017 Eva Lengfelder Department of Hematology and Oncology University Hospital
Which is the best treatment for relapsed APL? 7th International Symposium on Acute Promyelocytic Leukemia, Rome, September 24 27, 2017 Eva Lengfelder Department of Hematology and Oncology University Hospital
Objectives. I do not have anything to disclose.
 Treatment of APL Objectives I do not have anything to disclose. Objectives 1. Urgency of early recognition and treatment 2. Treatment based on risk stratification 3. Monitoring for relapse 4. Treatment
Treatment of APL Objectives I do not have anything to disclose. Objectives 1. Urgency of early recognition and treatment 2. Treatment based on risk stratification 3. Monitoring for relapse 4. Treatment
Management of Relapsed APL
 THE INAUGURAL ASEAN FEDERATION OF HAEMATOLOGY SCIENTIFIC MEETING AND THE VIIITH MALAYSIAN NATIONAL HAEMATOLOGY SCIENTIFIC MEETING - SHANGRILA HOTEL KUALA LUMPUR, 22-24 APRIL 2010 Management of Relapsed
THE INAUGURAL ASEAN FEDERATION OF HAEMATOLOGY SCIENTIFIC MEETING AND THE VIIITH MALAYSIAN NATIONAL HAEMATOLOGY SCIENTIFIC MEETING - SHANGRILA HOTEL KUALA LUMPUR, 22-24 APRIL 2010 Management of Relapsed
Treatment of APL. M a tth e w M e i, M.D. A s s is ta n t P ro fe s s o r C ity o f H o p e C o m p re h e n s iv e C a n c e r C e n te r
 Treatment of APL M a tth e w M e i, M.D. A s s is ta n t P ro fe s s o r C ity o f H o p e C o m p re h e n s iv e C a n c e r C e n te r Disclosures I have nothing to disclose Objectives 1. Urgency of
Treatment of APL M a tth e w M e i, M.D. A s s is ta n t P ro fe s s o r C ity o f H o p e C o m p re h e n s iv e C a n c e r C e n te r Disclosures I have nothing to disclose Objectives 1. Urgency of
Tamibarotene As Maintenance Therapy for Acute Promyelocytic Leukemia: Results From a Randomized Controlled Trial
 VOLUME 32 NUMBER 33 NOVEMBER 20 2014 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Tamibarotene As Maintenance Therapy for Acute Promyelocytic Leukemia: Results From a Randomized Controlled
VOLUME 32 NUMBER 33 NOVEMBER 20 2014 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Tamibarotene As Maintenance Therapy for Acute Promyelocytic Leukemia: Results From a Randomized Controlled
Matthew Mei, M.D. Assistant t Professor City of Hope Comprehensive Cancer Center
 Treatment of APL Matthew Mei, M.D. Assistant t Professor City of Hope Comprehensive Cancer Center Objectives 1. Urgency of early recognition and treatment 2. Treatment based on risk stratification 3. Monitoring
Treatment of APL Matthew Mei, M.D. Assistant t Professor City of Hope Comprehensive Cancer Center Objectives 1. Urgency of early recognition and treatment 2. Treatment based on risk stratification 3. Monitoring
Belgium recommendations for the management of acute promyelocytic leukaemia
 6 Belgium recommendations for the management of acute promyelocytic leukaemia S. Wittnebel, MD, PhD 1 The management of acute promyelocytic leukaemia has evolved considerably. The standard front-line approach
6 Belgium recommendations for the management of acute promyelocytic leukaemia S. Wittnebel, MD, PhD 1 The management of acute promyelocytic leukaemia has evolved considerably. The standard front-line approach
Progress in the treatment of acute promyelocytic leukemia. Lionel Adès, MD PhD Hopital Saint Louis, Paris Diderot University
 Progress in the treatment of acute promyelocytic leukemia Lionel Adès, MD PhD Hopital Saint Louis, Paris Diderot University 대한혈액학회 Korean Society of Hematology COI disclosure Name of author : Lionel Adès
Progress in the treatment of acute promyelocytic leukemia Lionel Adès, MD PhD Hopital Saint Louis, Paris Diderot University 대한혈액학회 Korean Society of Hematology COI disclosure Name of author : Lionel Adès
MOLECULAR AND CLINICAL ONCOLOGY 3: , 2015
 MOLECULAR AND CLINICAL ONCOLOGY 3: 449-453, 2015 Evaluation of the efficacy of maintenance therapy for low to intermediate risk acute promyelocytic leukemia in molecular remission: A retrospective single
MOLECULAR AND CLINICAL ONCOLOGY 3: 449-453, 2015 Evaluation of the efficacy of maintenance therapy for low to intermediate risk acute promyelocytic leukemia in molecular remission: A retrospective single
Characteristics and Outcome of Therapy-Related Acute Promyelocytic Leukemia After Different Front-line Therapies
 Characteristics and Outcome of Therapy-Related Acute Promyelocytic Leukemia After Different Front-line Therapies Sabine Kayser, * Julia Krzykalla, Michelle A. Elliott, Kelly Norsworthy, Patrick Gonzales,
Characteristics and Outcome of Therapy-Related Acute Promyelocytic Leukemia After Different Front-line Therapies Sabine Kayser, * Julia Krzykalla, Michelle A. Elliott, Kelly Norsworthy, Patrick Gonzales,
Prise en Charge des LAM-3. Hervé Dombret Hôpital Saint-Louis Institut Universitaire d Hématologie Université Paris Diderot
 Prise en Charge des LAM-3 Hervé Dombret Hôpital Saint-Louis Institut Universitaire d Hématologie Université Paris Diderot Basal transcription therapy by ATRA h Transcrip onal repression PML RA PML Blast
Prise en Charge des LAM-3 Hervé Dombret Hôpital Saint-Louis Institut Universitaire d Hématologie Université Paris Diderot Basal transcription therapy by ATRA h Transcrip onal repression PML RA PML Blast
Disclosures of Massimo Breccia
 Disclosures of Massimo Breccia Company name Research support Employee Consultant Stockholder Speakers bureau Advisory board Other Novar
Disclosures of Massimo Breccia Company name Research support Employee Consultant Stockholder Speakers bureau Advisory board Other Novar
Improvements with Risk-adapted PETHEMA Protocols in New Diagnosed Acute Promyelocytic Leukemia
 Improvements with Risk-adapted PETHEMA Protocols in New Diagnosed Acute Promyelocytic Leukemia Miguel A. Sanz Chairman, Spanish PETHEMA Group University Hospital La Fe Valencia, Spain 7 th International
Improvements with Risk-adapted PETHEMA Protocols in New Diagnosed Acute Promyelocytic Leukemia Miguel A. Sanz Chairman, Spanish PETHEMA Group University Hospital La Fe Valencia, Spain 7 th International
Current standard treatment of adult acute promyelocytic leukaemia
 review Current standard treatment of adult acute promyelocytic leukaemia Francesco Lo-Coco, 1,2 Laura Cicconi 1,2 and Massimo Breccia 3 1 Department of Biomedicine and Prevention, Tor Vergata University,
review Current standard treatment of adult acute promyelocytic leukaemia Francesco Lo-Coco, 1,2 Laura Cicconi 1,2 and Massimo Breccia 3 1 Department of Biomedicine and Prevention, Tor Vergata University,
Acute promyelocytic leukemia
 Acute promyelocytic leukemia Laura Cicconi University Tor Vergata Rome, Italy Acute Myeloid Leukemia Meeting Ravenna, Italy (October 2017) APL. From highly fatal to curable disease Fatal outcome if not
Acute promyelocytic leukemia Laura Cicconi University Tor Vergata Rome, Italy Acute Myeloid Leukemia Meeting Ravenna, Italy (October 2017) APL. From highly fatal to curable disease Fatal outcome if not
7th International Symposium on Acute Promyelocytic Leukemia, Rome, September 24 27, Eva Lengfelder
 Frontline therapy of acute promyelocytic leukemia: randomized comparison of ATRA and intensified chemotherapy including high dose cytosine-arabinoside versus ATRA and anthracyclines - A prospective multicenter
Frontline therapy of acute promyelocytic leukemia: randomized comparison of ATRA and intensified chemotherapy including high dose cytosine-arabinoside versus ATRA and anthracyclines - A prospective multicenter
Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients
 Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients Olivier Hermine MD, PhD Department of Hematology INSERM and CNRS, Imagine Institute Necker Hospital Paris, France
Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients Olivier Hermine MD, PhD Department of Hematology INSERM and CNRS, Imagine Institute Necker Hospital Paris, France
The Role of ATRA Followed by Chemotherapy in the Treatment of Acute Promyelocytic Leukemia
 ORIGINAL ARTICLE The Role of ATRA Followed by Chemotherapy in the Treatment of Acute Promyelocytic Leukemia Hasan Jalaeikhoo 1, Mohsen Rajaeinejad 1, Manoutchehr Keyhani 2, and Mohammad Zokaasadi 1 1 Department
ORIGINAL ARTICLE The Role of ATRA Followed by Chemotherapy in the Treatment of Acute Promyelocytic Leukemia Hasan Jalaeikhoo 1, Mohsen Rajaeinejad 1, Manoutchehr Keyhani 2, and Mohammad Zokaasadi 1 1 Department
A Canadian consensus on the management of newly diagnosed and relapsed acute promyelocytic leukemia in adults
 ABSTRACT The use of all-trans-retinoic acid (atra) and anthracyclines (with or without cytarabine) in the treatment of acute promyelocytic leukemia (apl) has dramatically changed the manment and outcome
ABSTRACT The use of all-trans-retinoic acid (atra) and anthracyclines (with or without cytarabine) in the treatment of acute promyelocytic leukemia (apl) has dramatically changed the manment and outcome
Reduced-intensity Conditioning Transplantation
 Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
AIH, Marseille 30/09/06
 ALLOGENEIC STEM CELL TRANSPLANTATION FOR MYELOID MALIGNANCIES Transplant and Cellular Therapy Unit Institut Paoli Calmettes Inserm U599 Université de la Méditerranée ée Marseille, France AIH, Marseille
ALLOGENEIC STEM CELL TRANSPLANTATION FOR MYELOID MALIGNANCIES Transplant and Cellular Therapy Unit Institut Paoli Calmettes Inserm U599 Université de la Méditerranée ée Marseille, France AIH, Marseille
CREDIT DESIGNATION STATEMENT
 CME Information LEARNING OBJECTIVES Recall the dose-limiting toxicity and preliminary clinical response results with 14- and 21-day extended treatment schedules of daily oral azacitidine. Apply new research
CME Information LEARNING OBJECTIVES Recall the dose-limiting toxicity and preliminary clinical response results with 14- and 21-day extended treatment schedules of daily oral azacitidine. Apply new research
Acute Lymphoblastic Leukemia (ALL) Ryan Mattison, MD University of Wisconsin March 2, 2010
 Ryan Mattison, MD University of Wisconsin March 2, 2010") Acute Lymphoblastic Leukemia (ALL) Ryan Mattison, MD University of Wisconsin March 2, 2010 ALL Epidemiology 20% of new acute leukemia cases in adults 5200 new cases in 2007 Most are de novo Therapy-related
Acute Lymphoblastic Leukemia (ALL) Ryan Mattison, MD University of Wisconsin March 2, 2010 ALL Epidemiology 20% of new acute leukemia cases in adults 5200 new cases in 2007 Most are de novo Therapy-related
Correspondence should be addressed to Chen Xue-Liang; chenxl and Hou Ming; houming
 Evidence-Based Complementary and Alternative Medicine, Article ID 987560, 7 pages http://dx.doi.org/10.1155/2014/987560 Research Article Clinical Study on Prospective Efficacy of All-Trans Acid, Realgar-Indigo
Evidence-Based Complementary and Alternative Medicine, Article ID 987560, 7 pages http://dx.doi.org/10.1155/2014/987560 Research Article Clinical Study on Prospective Efficacy of All-Trans Acid, Realgar-Indigo
PETHEMA; 2 HOVON; 3 PLAG and 4 GATLA Groups.
 Clinical significance of complex karyotype at diagnosis in Pa7ents with Acute Promyelocy7c Leukemia Treated with ATRA and chemotherapy based PETHEMA trials Labrador J 1, Montesinos P 1, Bernal T 1, Vellenga
Clinical significance of complex karyotype at diagnosis in Pa7ents with Acute Promyelocy7c Leukemia Treated with ATRA and chemotherapy based PETHEMA trials Labrador J 1, Montesinos P 1, Bernal T 1, Vellenga
perc deliberated upon: a pcodr systematic review other literature in the Clinical Guidance Report providing clinical context
 require close monitoring. perc noted that induction therapy is generally administered in-hospital while consolidation therapy is administered on an out-patient basis. Because of the potential for serious
require close monitoring. perc noted that induction therapy is generally administered in-hospital while consolidation therapy is administered on an out-patient basis. Because of the potential for serious
MUD SCT for Paediatric AML?
 7 th South African Symposium on Haematopoietic Stem Cell Transplantation MUD SCT for Paediatric AML? Alan Davidson Haematology / Oncology Service Red Cross Children s Hospital THE SCENARIO A 10 year old
7 th South African Symposium on Haematopoietic Stem Cell Transplantation MUD SCT for Paediatric AML? Alan Davidson Haematology / Oncology Service Red Cross Children s Hospital THE SCENARIO A 10 year old
Remission induction in acute myeloid leukemia
 Int J Hematol (2012) 96:164 170 DOI 10.1007/s12185-012-1121-y PROGRESS IN HEMATOLOGY How to improve the outcome of adult acute myeloid leukemia? Remission induction in acute myeloid leukemia Eytan M. Stein
Int J Hematol (2012) 96:164 170 DOI 10.1007/s12185-012-1121-y PROGRESS IN HEMATOLOGY How to improve the outcome of adult acute myeloid leukemia? Remission induction in acute myeloid leukemia Eytan M. Stein
Risk-adapted therapy of AML in younger adults. Sergio Amadori Tor Vergata University Hospital Rome
 Risk-adapted therapy of AML in younger adults Sergio Amadori Tor Vergata University Hospital Rome Pescara 11/2010 AML: treatment outcome Age CR % ED % DFS % OS %
Risk-adapted therapy of AML in younger adults Sergio Amadori Tor Vergata University Hospital Rome Pescara 11/2010 AML: treatment outcome Age CR % ED % DFS % OS %
Clinical commissioning policy statement: Arsenic trioxide for the treatment of high risk acute promyelocytic leukaemia (all ages)
") Clinical commissioning policy statement: Arsenic trioxide for the treatment of high risk acute promyelocytic leukaemia (all ages) NHS England Reference: 170072P 1 Contents 1 Plain language summary... 3
Clinical commissioning policy statement: Arsenic trioxide for the treatment of high risk acute promyelocytic leukaemia (all ages) NHS England Reference: 170072P 1 Contents 1 Plain language summary... 3
Philadelphia-positive Acute Lymphoblastic Leukemia
 Philadelphia-positive Acute Lymphoblastic Leukemia Nicolas Boissel Service d Hématologie Unité Adolescents et Jeunes Adultes Hôpital Saint-Louis, Paris Ph+ acute lymphoblastic leukemia DR+, CD19+, CD22+,
Philadelphia-positive Acute Lymphoblastic Leukemia Nicolas Boissel Service d Hématologie Unité Adolescents et Jeunes Adultes Hôpital Saint-Louis, Paris Ph+ acute lymphoblastic leukemia DR+, CD19+, CD22+,
Acute Promyelocytic Leukemia
 Acute Promyelocytic Leukemia Outline of Management Suleimman AlSweedan,MD,MS,FAAP Consultant Pediatric Hematology/oncology TABLE OF CONTENTS Background 3 Pediatric APL Trials 4 Adult APL Trials 4 Diagnostic
Acute Promyelocytic Leukemia Outline of Management Suleimman AlSweedan,MD,MS,FAAP Consultant Pediatric Hematology/oncology TABLE OF CONTENTS Background 3 Pediatric APL Trials 4 Adult APL Trials 4 Diagnostic
Prior Authorization Review Panel MCO Policy Submission
 Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Molecularly Targeted Therapies - Strategies of the AMLSG
 Molecularly Targeted Therapies - Strategies of the AMLSG Richard Schlenk Department of Internal Medicine III Ulm University, Germany Genotype-adapted Leukemia Program NAPOLEON GIMEMA/AMLSG/SAL APL [t(15;17)]
Molecularly Targeted Therapies - Strategies of the AMLSG Richard Schlenk Department of Internal Medicine III Ulm University, Germany Genotype-adapted Leukemia Program NAPOLEON GIMEMA/AMLSG/SAL APL [t(15;17)]
Acute myeloid leukemia. M. Kaźmierczak 2016
 Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Clinical Policy Bulletin: Hematopoietic Cell Transplantation for Selected Leukemias
 Go Clinical Policy Bulletin: Hematopoietic Cell Transplantation for Selected Leukemias Number: 0640 Policy *Please see amendment for Pennsylvania Medicaid at the end of this CPB. Additional Information
Go Clinical Policy Bulletin: Hematopoietic Cell Transplantation for Selected Leukemias Number: 0640 Policy *Please see amendment for Pennsylvania Medicaid at the end of this CPB. Additional Information
Tools for MRD in AML: flow cytometry
 ACUTE MYELOID LEUKEMIA MEETING Ravenna - October 27, 2017 Tools for MRD in AML: flow cytometry Francesco Buccisano Can MRD improve outcome determina3on? No. of leukemic cells 10 12 10 10 10 8 10 6 10 4
ACUTE MYELOID LEUKEMIA MEETING Ravenna - October 27, 2017 Tools for MRD in AML: flow cytometry Francesco Buccisano Can MRD improve outcome determina3on? No. of leukemic cells 10 12 10 10 10 8 10 6 10 4
AML Emerging Treatment Strategies
 Welcome and Introduction Clare Karten, MS Senior Director, Mission Education The Leukemia & Lymphoma Society AML Emerging Treatment Strategies Wendy Stock, MD Professor of Medicine, Section of Hematology/Oncology
Welcome and Introduction Clare Karten, MS Senior Director, Mission Education The Leukemia & Lymphoma Society AML Emerging Treatment Strategies Wendy Stock, MD Professor of Medicine, Section of Hematology/Oncology
Extending Our Reach. Developing Safer Treatments. Interviews with Dr. Furman, Dr. Owen, and Dr. Stewart
 C A N A D I A N V I S I O N F O R O N C O L O G Y Number 22 May 214 Extending Our Reach Developing Safer Treatments INSIDE THIS ISSUE LEUKEMIAS Novel Combination Regimens Display Efficacy with Reduced
C A N A D I A N V I S I O N F O R O N C O L O G Y Number 22 May 214 Extending Our Reach Developing Safer Treatments INSIDE THIS ISSUE LEUKEMIAS Novel Combination Regimens Display Efficacy with Reduced
Minimal residual disease (MRD) in AML; coming of age. Dr. Mehmet Yılmaz Gaziantep University Medical School Sahinbey Education and Research hospital
 in AML; coming of age. Dr. Mehmet Yılmaz Gaziantep University Medical School Sahinbey Education and Research hospital") Minimal residual disease (MRD) in AML; coming of age Dr. Mehmet Yılmaz Gaziantep University Medical School Sahinbey Education and Research hospital 1. The logistics of MRD assessment in AML 2. The clinical
Minimal residual disease (MRD) in AML; coming of age Dr. Mehmet Yılmaz Gaziantep University Medical School Sahinbey Education and Research hospital 1. The logistics of MRD assessment in AML 2. The clinical
Leukemia. Andre C. Schuh. Princess Margaret Cancer Centre Toronto
 Leukemia Andre C. Schuh Princess Margaret Cancer Centre Toronto AGENDA Ø Overview Ø Key News This Year Ø Key News out of ASH 2016 Sessions Abstracts Ø Canadian Perspective Ø Overview 2015- Stone, R. et
Leukemia Andre C. Schuh Princess Margaret Cancer Centre Toronto AGENDA Ø Overview Ø Key News This Year Ø Key News out of ASH 2016 Sessions Abstracts Ø Canadian Perspective Ø Overview 2015- Stone, R. et
Stem cell transplantation for patients with AML in Republic of Macedonia: - 15 years of experience -
 Stem cell transplantation for patients with AML in Republic of Macedonia: - 15 years of experience - R E S E A R C H A S S O C I A T E P R O F. D - R Z L A T E S T O J A N O S K I Definition Acute myeloid
Stem cell transplantation for patients with AML in Republic of Macedonia: - 15 years of experience - R E S E A R C H A S S O C I A T E P R O F. D - R Z L A T E S T O J A N O S K I Definition Acute myeloid
Therapy-related MDS/AML with KMT2A (MLL) Rearrangement Following Therapy for APL Case 0328
 Rearrangement Following Therapy for APL Case 0328") Therapy-related MDS/AML with KMT2A (MLL) Rearrangement Following Therapy for APL Case 0328 Kenneth N. Holder, Leslie J. Greebon, Gopalrao Velagaleti, Hongxin Fan, Russell A. Higgins Initial Case: Clinical
Therapy-related MDS/AML with KMT2A (MLL) Rearrangement Following Therapy for APL Case 0328 Kenneth N. Holder, Leslie J. Greebon, Gopalrao Velagaleti, Hongxin Fan, Russell A. Higgins Initial Case: Clinical
Thrombohemorrhagic disorders in APL: the unsolved issue
 Thrombohemorrhagic disorders in APL: the unsolved issue Pau Montesinos Hospital La Fe. Valencia, Spain 7th International Symposium on Acute Promyelocytic Leukemia Rome, Italy (September 2017) Background
Thrombohemorrhagic disorders in APL: the unsolved issue Pau Montesinos Hospital La Fe. Valencia, Spain 7th International Symposium on Acute Promyelocytic Leukemia Rome, Italy (September 2017) Background
Adult ALL: NILG experience
 Adult ALL: NILG experience R Bassan USC Ematologia, Ospedali Riuniti, Bergamo SIE Interregionale, Padova 12 5 2011 Now and then Northern Italy Leukemia Group 2000-10 Prospective clinical trials 09/00 10/07
Adult ALL: NILG experience R Bassan USC Ematologia, Ospedali Riuniti, Bergamo SIE Interregionale, Padova 12 5 2011 Now and then Northern Italy Leukemia Group 2000-10 Prospective clinical trials 09/00 10/07
Autologous Stem Cell Transplanation as First line Treatment? (Against) Joan Bladé Berlin, September 9 th, 2011
 Joan Bladé Berlin, September 9 th, 2011") Autologous Stem Cell Transplanation as First line Treatment? (Against) Joan Bladé Berlin, September 9 th, 2011 Significant impact of ASCT before the availability of novel agents? Randomized trials: Single
Autologous Stem Cell Transplanation as First line Treatment? (Against) Joan Bladé Berlin, September 9 th, 2011 Significant impact of ASCT before the availability of novel agents? Randomized trials: Single
Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway. Acute Myeloid Leukaemia
 Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway Acute Myeloid Leukaemia 1 BACKGROUND The Hull and North Lincolnshire Haematology Multidisciplinary
Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway Acute Myeloid Leukaemia 1 BACKGROUND The Hull and North Lincolnshire Haematology Multidisciplinary
Hematopoietic Cell Transplantation for Acute Lymphoblastic Leukemia
 Hematopoietic Cell Transplantation for Acute Lymphoblastic Leukemia Policy Number: 8.01.32 Last Review: 7/2018 Origination: 7/2002 Next Review: 7/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue
Hematopoietic Cell Transplantation for Acute Lymphoblastic Leukemia Policy Number: 8.01.32 Last Review: 7/2018 Origination: 7/2002 Next Review: 7/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue
Treatment concepts of acute promyelocytic leukemia
 Critical Reviews in Oncology/Hematology 56 (2005) 261 274 Treatment concepts of acute promyelocytic leukemia Eva Lengfelder a,, Susanne Saussele a, Andreas Weisser a, Thomas Büchner b, Rüdiger Hehlmann
Critical Reviews in Oncology/Hematology 56 (2005) 261 274 Treatment concepts of acute promyelocytic leukemia Eva Lengfelder a,, Susanne Saussele a, Andreas Weisser a, Thomas Büchner b, Rüdiger Hehlmann
Inotuzumab Ozogamicin in ALL. Hagop Kantarjian M.D. May 2016 Bologna, Italy
 Inotuzumab Ozogamicin in ALL Hagop Kantarjian M.D. May 2016 Bologna, Italy Immuno Oncology in ALL Monoclonals + cytotoxic agents e.g.inotuzumab Bispecific monoclonals (CD3 + CD19) e.g.blinatumomab Modified
Inotuzumab Ozogamicin in ALL Hagop Kantarjian M.D. May 2016 Bologna, Italy Immuno Oncology in ALL Monoclonals + cytotoxic agents e.g.inotuzumab Bispecific monoclonals (CD3 + CD19) e.g.blinatumomab Modified
Ph+ALL : a new era. Said Y Mohamed KFSHRC, Riyadh Ain Shams University, Cairo, Egypt
 Ph+ALL : a new era Said Y Mohamed KFSHRC, Riyadh Ain Shams University, Cairo, Egypt A 30 Y/O patient with Ph+ ALL What would you start as an induction? 1. BFM/CALGB/UKALL Plus TKI? 2. Some chemo + TKI.
Ph+ALL : a new era Said Y Mohamed KFSHRC, Riyadh Ain Shams University, Cairo, Egypt A 30 Y/O patient with Ph+ ALL What would you start as an induction? 1. BFM/CALGB/UKALL Plus TKI? 2. Some chemo + TKI.
Controversies in Hematology: Case-Based Discussion. Acute leukemia in Adolescents and Young adults October 2018, Chiang Mai Thailand
 Controversies in Hematology: Case-Based Discussion Acute leukemia in Adolescents and Young adults 25-26 October 2018, Chiang Mai Thailand Associate Prof. Adisak Tantiworawit, MD Division of Hematology,
Controversies in Hematology: Case-Based Discussion Acute leukemia in Adolescents and Young adults 25-26 October 2018, Chiang Mai Thailand Associate Prof. Adisak Tantiworawit, MD Division of Hematology,
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University
 Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
Breakthroughs in the treatment of APL: role of arsenic in newlydiagnosed
 Breakthroughs in the treatment of APL: role of arsenic in newlydiagnosed patients Jiong Hu, Zhi-Xiang Shen Department of Hematology, RuiJin Hospital, Shanghai JiaoTong Unviersity School of Medicine 1.
Breakthroughs in the treatment of APL: role of arsenic in newlydiagnosed patients Jiong Hu, Zhi-Xiang Shen Department of Hematology, RuiJin Hospital, Shanghai JiaoTong Unviersity School of Medicine 1.
First relapsed childhood ALL Role of chemotherapy
 First relapsed childhood ALL Role of chemotherapy Thirachit Chotsampancharoen, M.D. Division of Pediatric Hematology/Oncology Department of Pediatrics Prince of Songkla University Hat-Yai, Songkhla 25
First relapsed childhood ALL Role of chemotherapy Thirachit Chotsampancharoen, M.D. Division of Pediatric Hematology/Oncology Department of Pediatrics Prince of Songkla University Hat-Yai, Songkhla 25
MRD detection in AML. Adriano Venditti Hematology Fondazione Policlinico Tor Vergata Rome
 MRD detection in AML Adriano Venditti Hematology Fondazione Policlinico Tor Vergata Rome Determinants of Treatment Response Leukemia Tumor burden Growth potential Drug resistance Karyotype Genetics Host
MRD detection in AML Adriano Venditti Hematology Fondazione Policlinico Tor Vergata Rome Determinants of Treatment Response Leukemia Tumor burden Growth potential Drug resistance Karyotype Genetics Host
Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham
 Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham What is cure after all? Getting rid of it? Stopping treatment without
Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham What is cure after all? Getting rid of it? Stopping treatment without
Should patients with higher risk MDS (or AML in «early relapse») proceed directly to allo SCT without prior chemotherapy?
 proceed directly to allo SCT without prior chemotherapy?") Should patients with higher risk MDS (or AML in «early relapse») proceed directly to allo SCT without prior chemotherapy? Pierre Fenaux Cohem 2012 Barcelona Should patients with higher risk MDS (or AML
Should patients with higher risk MDS (or AML in «early relapse») proceed directly to allo SCT without prior chemotherapy? Pierre Fenaux Cohem 2012 Barcelona Should patients with higher risk MDS (or AML
Acute Myeloid Leukemia
 Acute Myeloid Leukemia Pimjai Niparuck Division of Hematology, Department of Medicine Ramathibodi Hospital, Mahidol University Outline Molecular biology Chemotherapy and Hypomethylating agent Novel Therapy
Acute Myeloid Leukemia Pimjai Niparuck Division of Hematology, Department of Medicine Ramathibodi Hospital, Mahidol University Outline Molecular biology Chemotherapy and Hypomethylating agent Novel Therapy
All-trans retinoic acid in acute promyelocytic leukemia: long-term outcome and prognostic factor analysis from the North American Intergroup protocol
 CLINICAL OBSERVATIONS, INTERVENTIONS, AND THERAPEUTIC TRIALS All-trans retinoic acid in acute promyelocytic leukemia: long-term outcome and prognostic factor analysis from the North American Intergroup
CLINICAL OBSERVATIONS, INTERVENTIONS, AND THERAPEUTIC TRIALS All-trans retinoic acid in acute promyelocytic leukemia: long-term outcome and prognostic factor analysis from the North American Intergroup
LA LEUCEMIA SECONDARIA: QUALI OPZIONI TERAPEUTICHE. Livio Pagano Istituto di Ematologia Università Cattolica S. Cuore Roma
 LA LEUCEMIA SECONDARIA: QUALI OPZIONI TERAPEUTICHE Livio Pagano Istituto di Ematologia Università Cattolica S. Cuore Roma saml: Incidence In USA, NCI / SEER data - 1998 10,600 new patients with AML / year
LA LEUCEMIA SECONDARIA: QUALI OPZIONI TERAPEUTICHE Livio Pagano Istituto di Ematologia Università Cattolica S. Cuore Roma saml: Incidence In USA, NCI / SEER data - 1998 10,600 new patients with AML / year
Jordi Esteve Hospital Clínic (Barcelona) Acute Leukemia Working Party. The European Group for Blood and Marrow Transplantation
 Acute Leukemia Working Party. The European Group for Blood and Marrow Transplantation") 36th EBMT & 9th Data Management Group Annual Meeting Vienna, 23 March 2010 Jordi Esteve Hospital Clínic (Barcelona) Acute Leukemia Working Party The European Group for Blood and Marrow Transplantation
36th EBMT & 9th Data Management Group Annual Meeting Vienna, 23 March 2010 Jordi Esteve Hospital Clínic (Barcelona) Acute Leukemia Working Party The European Group for Blood and Marrow Transplantation
National Institute for Health and Care Excellence. Single Technology Appraisal (STA)
") Single Technology Appraisal (STA) Gemtuzumab ozogamacin for untreated de novo acute myeloid leukaemia Response to consultee and commentator comments re-scope Please note: Comments received in the course
Single Technology Appraisal (STA) Gemtuzumab ozogamacin for untreated de novo acute myeloid leukaemia Response to consultee and commentator comments re-scope Please note: Comments received in the course
Dr Claire Burney, Lymphoma Clinical Fellow, Bristol Haematology and Oncology Centre, UK
 EMBT LWP 2017-R-05 Research Protocol: Outcomes of patients treated with Ibrutinib post autologous stem cell transplant for mantle cell lymphoma. A retrospective analysis of the LWP-EBMT registry. Principle
EMBT LWP 2017-R-05 Research Protocol: Outcomes of patients treated with Ibrutinib post autologous stem cell transplant for mantle cell lymphoma. A retrospective analysis of the LWP-EBMT registry. Principle
STATUS OF EARLY MORTALITY IN NEWLY DIAGNOSED CASES OF ACUTE PROMYELOCYTIC LEUKAEMIA (APL) IN BSMMU HOSPITAL
 IN BSMMU HOSPITAL") STATUS OF EARLY MORTALITY IN NEWLY DIAGNOSED CASES OF ACUTE PROMYELOCYTIC LEUKAEMIA (APL) IN BSMMU HOSPITAL RAHMAN F 1, YUNUS ABM 2, KABIR AL 3, BEGUM M 4, AZIZ A 3, SHAH S 3, RAHMAN F 5, RAHMAN MJ 6 Abstract:
STATUS OF EARLY MORTALITY IN NEWLY DIAGNOSED CASES OF ACUTE PROMYELOCYTIC LEUKAEMIA (APL) IN BSMMU HOSPITAL RAHMAN F 1, YUNUS ABM 2, KABIR AL 3, BEGUM M 4, AZIZ A 3, SHAH S 3, RAHMAN F 5, RAHMAN MJ 6 Abstract:
ALLOGENEIC STEM CELL TRANSPLANTATION FOR ACUTE MYELOBLASTIC LEUKEMIAS
 ALLOGENEIC STEM CELL TRANSPLANTATION FOR ACUTE MYELOBLASTIC LEUKEMIAS Didier Blaise, MD Transplant and Cellular Therapy Unit (U2T) Department of Hematology Centre de Recherche en Cancérologie, Inserm U891
ALLOGENEIC STEM CELL TRANSPLANTATION FOR ACUTE MYELOBLASTIC LEUKEMIAS Didier Blaise, MD Transplant and Cellular Therapy Unit (U2T) Department of Hematology Centre de Recherche en Cancérologie, Inserm U891
Reference: NHS England 1602
 Clinical Commissioning Policy Proposition: Clofarabine for refractory or relapsed acute myeloid leukaemia (AML) as a bridge to stem cell transplantation Reference: NHS England 1602 First published: TBC
Clinical Commissioning Policy Proposition: Clofarabine for refractory or relapsed acute myeloid leukaemia (AML) as a bridge to stem cell transplantation Reference: NHS England 1602 First published: TBC
Evolving Targeted Management of Acute Myeloid Leukemia
 Evolving Targeted Management of Acute Myeloid Leukemia Jessica Altman, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University Learning Objectives Identify which mutations should be assessed
Evolving Targeted Management of Acute Myeloid Leukemia Jessica Altman, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University Learning Objectives Identify which mutations should be assessed
Mantle Cell Lymphoma. A schizophrenic disease
 23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
Can ALL be managed without chemotherapy/transplant? (Position: NO) D.Hoelzer J.W.Goethe University Frankfurt
 D.Hoelzer J.W.Goethe University Frankfurt") Can ALL be managed without chemotherapy/transplant? (Position: NO) D.Hoelzer J.W.Goethe University Frankfurt Barcelona, September 2012 First report of Monotherapy in childhood ALL 10/16 children with acute
Can ALL be managed without chemotherapy/transplant? (Position: NO) D.Hoelzer J.W.Goethe University Frankfurt Barcelona, September 2012 First report of Monotherapy in childhood ALL 10/16 children with acute
London Cancer ALL guidelines
 London Cancer ALL guidelines Page 1 of 7 CONTENTS OVERVIEW - main points in ALL management... 3 AGE-SPECIFIC THERAPEUTIC APPROACHES... 4 SPECIFIC THERAPEUTIC PROBLEMS... 5 SUPPORTIVE CARE... 6 PATIENTS
London Cancer ALL guidelines Page 1 of 7 CONTENTS OVERVIEW - main points in ALL management... 3 AGE-SPECIFIC THERAPEUTIC APPROACHES... 4 SPECIFIC THERAPEUTIC PROBLEMS... 5 SUPPORTIVE CARE... 6 PATIENTS
MS.4/ Acute Leukemia: AML. Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD
 MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
Advances in the Treatment of APL in Children SLOP Vina del Mar April 2014
 Advances in the Treatment of APL in Children SLOP Vina del Mar April 2014 Outline Advances in suppor3ve care of pediatric acute promyelocy3c leukemia (APL) Advances in specific treatment of pediatric APL
Advances in the Treatment of APL in Children SLOP Vina del Mar April 2014 Outline Advances in suppor3ve care of pediatric acute promyelocy3c leukemia (APL) Advances in specific treatment of pediatric APL
NK/T cell lymphoma Recent advances. Y.L Kwong University Department of Medicine Queen Mary Hospital
 NK/T cell lymphoma Recent advances Y.L Kwong University Department of Medicine Queen Mary Hospital Natural killer cell lymphomas NK cell lymphomas are mainly extranodal lymphomas Clinical classification
NK/T cell lymphoma Recent advances Y.L Kwong University Department of Medicine Queen Mary Hospital Natural killer cell lymphomas NK cell lymphomas are mainly extranodal lymphomas Clinical classification
EBMT2008_22_44:EBMT :29 Pagina 454 CHAPTER 30. HSCT for Hodgkin s lymphoma in adults. A. Sureda
 EBMT2008_22_44:EBMT2008 6-11-2008 9:29 Pagina 454 * CHAPTER 30 HSCT for Hodgkin s lymphoma in adults A. Sureda EBMT2008_22_44:EBMT2008 6-11-2008 9:29 Pagina 455 CHAPTER 30 HL in adults 1. Introduction
EBMT2008_22_44:EBMT2008 6-11-2008 9:29 Pagina 454 * CHAPTER 30 HSCT for Hodgkin s lymphoma in adults A. Sureda EBMT2008_22_44:EBMT2008 6-11-2008 9:29 Pagina 455 CHAPTER 30 HL in adults 1. Introduction
Johann Hitzler, MD, FRCPC, FAAP Jacqueline Halton, MD, FRCPC Jason D. Pole, PhD
 Photo by Tynan Studio Johann Hitzler, MD, FRCPC, FAAP Jacqueline Halton, MD, FRCPC Jason D. Pole, PhD 96 Atlas of Childhood Cancer in Ontario (1985-2004) Chapter 6: Leukemia 6 Leukemia Atlas of Childhood
Photo by Tynan Studio Johann Hitzler, MD, FRCPC, FAAP Jacqueline Halton, MD, FRCPC Jason D. Pole, PhD 96 Atlas of Childhood Cancer in Ontario (1985-2004) Chapter 6: Leukemia 6 Leukemia Atlas of Childhood
All patients with FLT3 mutant AML should receive midostaurin-based induction therapy. Not so fast!
 All patients with FLT3 mutant AML should receive midostaurin-based induction therapy Not so fast! Harry P. Erba, M.D., Ph.D. Professor, Internal Medicine Director, Hematologic Malignancy Program University
All patients with FLT3 mutant AML should receive midostaurin-based induction therapy Not so fast! Harry P. Erba, M.D., Ph.D. Professor, Internal Medicine Director, Hematologic Malignancy Program University
Acute myeloid leukemia: prognosis and treatment. Dimitri A. Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Campus Stuivenberg
 Acute myeloid leukemia: prognosis and treatment Dimitri A. Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Campus Stuivenberg Patient Female, 39 years History: hypothyroidism Present:
Acute myeloid leukemia: prognosis and treatment Dimitri A. Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Campus Stuivenberg Patient Female, 39 years History: hypothyroidism Present:
What s new in Blood and Marrow Transplant? Saar Gill, MD PhD Jan 22, 2016
 What s new in Blood and Marrow Transplant? Saar Gill, MD PhD Jan 22, 2016 Division of Hematology-Oncology University of Pennsylvania Perelman School of Medicine 1 Who should be transplanted and how? Updates
What s new in Blood and Marrow Transplant? Saar Gill, MD PhD Jan 22, 2016 Division of Hematology-Oncology University of Pennsylvania Perelman School of Medicine 1 Who should be transplanted and how? Updates
5/21/2018. Disclosures. Objectives. Normal blood cells production. Bone marrow failure syndromes. Story of DNA
 AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
Single Technology Appraisal (STA) Arsenic trioxide for treating acute promyelocytic leukaemia
 Arsenic trioxide for treating acute promyelocytic leukaemia") Single Technology Appraisal (STA) Arsenic trioxide for treating acute promyelocytic leukaemia Response to consultee and commentator comments on the draft remit and draft scope (pre-referral) Please note:
Single Technology Appraisal (STA) Arsenic trioxide for treating acute promyelocytic leukaemia Response to consultee and commentator comments on the draft remit and draft scope (pre-referral) Please note:
Bendamustine for Hodgkin lymphoma. Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service
 Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Best of ASH: Acute leukemia. Frédéric Baron
 Best of ASH: Acute leukemia Frédéric Baron I Acute Myeloid Leukemia Flt3 inhibitors (ratify, sorafenib after HCT) 5 other important abstracts (in brief) Mutated genes in AML FLT3: The Cancer Genome Atlas
Best of ASH: Acute leukemia Frédéric Baron I Acute Myeloid Leukemia Flt3 inhibitors (ratify, sorafenib after HCT) 5 other important abstracts (in brief) Mutated genes in AML FLT3: The Cancer Genome Atlas
OUTCOME OF ACUTE MYELOID LEUKEMIA IN PATIENTS UP TO 65 YEARS OF AGE AT HEMATOLOGY AND BONE MARROW TRANSPLANTATION UNIT IN ALGIERS DURING 14 YEARS
 OUTCOME OF ACUTE MYELOID LEUKEMIA IN PATIENTS UP TO 65 YEARS OF AGE AT HEMATOLOGY AND BONE MARROW TRANSPLANTATION UNIT IN ALGIERS DURING 14 YEARS S.Akhrouf, F.Belhadri, A.Talbi, H.Moussaoui, M.Benakli,
OUTCOME OF ACUTE MYELOID LEUKEMIA IN PATIENTS UP TO 65 YEARS OF AGE AT HEMATOLOGY AND BONE MARROW TRANSPLANTATION UNIT IN ALGIERS DURING 14 YEARS S.Akhrouf, F.Belhadri, A.Talbi, H.Moussaoui, M.Benakli,
Meet-the-Expert: AML Treating older patients with AML
 Meet-the-Expert: AML Treating older patients with AML Sergio Amadori Tor Vergata University Hospital Rome Istanbul 2012 AML in older patients Poor prognosis Minority treated with intensive Cx Treatment
Meet-the-Expert: AML Treating older patients with AML Sergio Amadori Tor Vergata University Hospital Rome Istanbul 2012 AML in older patients Poor prognosis Minority treated with intensive Cx Treatment
Therapeutic Advances in Treatment of Aplastic Anemia. Seiji Kojima MD. PhD.
 Therapeutic Advances in Treatment of Aplastic Anemia Seiji Kojima MD. PhD. Department of Pediatrics Nagoya University Graduate School of Medicine Chairman of the Severe Aplastic Anemia Working Party Asia-Pacific
Therapeutic Advances in Treatment of Aplastic Anemia Seiji Kojima MD. PhD. Department of Pediatrics Nagoya University Graduate School of Medicine Chairman of the Severe Aplastic Anemia Working Party Asia-Pacific
Treatment of acute myeloid leukemia (AML): Recent results and new directions Thomas Büchner University of Münster, Germany
: Recent results and new directions Thomas Büchner University of Münster, Germany") Treatment of acute myeloid leukemia (AML): Recent results and new directions Thomas Büchner University of Münster, Germany Acute myeloid leukemia (AML) is a major indication for hematopoietic stem cell
Treatment of acute myeloid leukemia (AML): Recent results and new directions Thomas Büchner University of Münster, Germany Acute myeloid leukemia (AML) is a major indication for hematopoietic stem cell
Abstract 861. Stein AS, Topp MS, Kantarjian H, Gökbuget N, Bargou R, Litzow M, Rambaldi A, Ribera J-M, Zhang A, Zimmerman Z, Forman SJ
 Treatment with Anti-CD19 BiTE Blinatumomab in Adult Patients With Relapsed/Refractory B-Precursor Acute Lymphoblastic Leukemia (R/R ALL) Post-Allogeneic Hematopoietic Stem Cell Transplantation Abstract
Treatment with Anti-CD19 BiTE Blinatumomab in Adult Patients With Relapsed/Refractory B-Precursor Acute Lymphoblastic Leukemia (R/R ALL) Post-Allogeneic Hematopoietic Stem Cell Transplantation Abstract
Elisabeth Koller 3rd Medical Dept., Center for Hematology and Oncology, Hanusch Hospital, Vienna, Austria
 Elisabeth Koller 3rd Medical Dept., Center for Hematology and Oncology, Hanusch Hospital, Vienna, Austria Incidence Diagnosis Prognostic factors Treatment Induction therapy - HSCT Indications for HSCT
Elisabeth Koller 3rd Medical Dept., Center for Hematology and Oncology, Hanusch Hospital, Vienna, Austria Incidence Diagnosis Prognostic factors Treatment Induction therapy - HSCT Indications for HSCT
AML:Transplant or ChemoTherapy?
 AML:Transplant or ChemoTherapy? 1960 s: Importance of HLA type in Animal Models Survival of Dogs Given 1000 RAD TBI and a Marrow Infusion from a Littermate Matched or Mismatched for Dog Leucocyte Antigens
AML:Transplant or ChemoTherapy? 1960 s: Importance of HLA type in Animal Models Survival of Dogs Given 1000 RAD TBI and a Marrow Infusion from a Littermate Matched or Mismatched for Dog Leucocyte Antigens
Outcome of acute leukemia patients with central nervous system (CNS) involvement treated with total body or CNS irradiation before transplantation
 involvement treated with total body or CNS irradiation before transplantation") Original Article Page 1 of 9 Outcome of acute leukemia patients with central nervous system (CNS) involvement treated with total body or CNS irradiation before transplantation Wen-Han Kuo 1, Yu-Hsuan Chen
Original Article Page 1 of 9 Outcome of acute leukemia patients with central nervous system (CNS) involvement treated with total body or CNS irradiation before transplantation Wen-Han Kuo 1, Yu-Hsuan Chen
Current Strategies for Relapsed/Refractory ALL in AYAs and Adults: Where We Are Now
 Current Strategies for Relapsed/Refractory ALL in AYAs and Adults: Where We Are Now Eunice S. Wang, MD Roswell Park Cancer Institute Buffalo, New York, United States Relapsed ALL Carries a Poor Prognosis
Current Strategies for Relapsed/Refractory ALL in AYAs and Adults: Where We Are Now Eunice S. Wang, MD Roswell Park Cancer Institute Buffalo, New York, United States Relapsed ALL Carries a Poor Prognosis
Consolidation after Autologous Stem Cell Transplantion
 Consolidation after Autologous Stem Cell Transplantion Joan Bladé Laura Rosiñol Department of Hematology Hospital Clínic de Barcelona Berlin, September 11 th 2011 Autologous Stem Cell Transplant in Younger
Consolidation after Autologous Stem Cell Transplantion Joan Bladé Laura Rosiñol Department of Hematology Hospital Clínic de Barcelona Berlin, September 11 th 2011 Autologous Stem Cell Transplant in Younger
Guidelines and real World: Management of CML in chronic and advanced phases. Carolina Pavlovsky. FUNDALEU May 2017 Frankfurt
 Guidelines and real World: Management of CML in chronic and advanced phases Carolina Pavlovsky. FUNDALEU 26-28 May 217 Frankfurt Some Issues in CML 217 First Line treatment: Imatinib vs 2nd generation
Guidelines and real World: Management of CML in chronic and advanced phases Carolina Pavlovsky. FUNDALEU 26-28 May 217 Frankfurt Some Issues in CML 217 First Line treatment: Imatinib vs 2nd generation
Treatment of elderly multiple myeloma patients
 SAMO Interdisciplinary Workshop on Myeloma March 30 th -31 st 2012, Seehotel Hermitage, Lucerne Treatment of elderly multiple myeloma patients Federica Cavallo, MD, PhD Federica Cavallo, MD, PhD Division
SAMO Interdisciplinary Workshop on Myeloma March 30 th -31 st 2012, Seehotel Hermitage, Lucerne Treatment of elderly multiple myeloma patients Federica Cavallo, MD, PhD Federica Cavallo, MD, PhD Division
Acute Lymphoblastic Leukaemia Guidelines
 Acute Lymphoblastic Leukaemia Guidelines Approved by Pathway Board for Haematological Malignancies Coordinating author: Adele Fielding, Royal Free London NHS Trust Date of issue: 12.03.2015 Version number:
Acute Lymphoblastic Leukaemia Guidelines Approved by Pathway Board for Haematological Malignancies Coordinating author: Adele Fielding, Royal Free London NHS Trust Date of issue: 12.03.2015 Version number:
A.M.W. van Marion. H.M. Lokhorst. N.W.C.J. van de Donk. J.G. van den Tweel. Histopathology 2002, 41 (suppl 2):77-92 (modified)
:77-92 (modified)") chapter 4 The significance of monoclonal plasma cells in the bone marrow biopsies of patients with multiple myeloma following allogeneic or autologous stem cell transplantation A.M.W. van Marion H.M. Lokhorst
chapter 4 The significance of monoclonal plasma cells in the bone marrow biopsies of patients with multiple myeloma following allogeneic or autologous stem cell transplantation A.M.W. van Marion H.M. Lokhorst
Background CPX-351. Lancet J, et al. J Clin Oncol. 2017;35(suppl): Abstract 7035.
: Abstract 7035.") Overall Survival (OS) With Versus in Older Adults With Newly Diagnosed, Therapy-Related Acute Myeloid Leukemia (taml): Subgroup Analysis of a Phase 3 Study Abstract 7035 Lancet JE, Rizzieri D, Schiller
Overall Survival (OS) With Versus in Older Adults With Newly Diagnosed, Therapy-Related Acute Myeloid Leukemia (taml): Subgroup Analysis of a Phase 3 Study Abstract 7035 Lancet JE, Rizzieri D, Schiller
LAL Ph+ dell adulto. Sabina Chiare+, MD, PhD Divisione di Ematologia Sapienza Università di Roma
 LAL Ph+ dell adulto Sabina Chiare+, MD, PhD Divisione di Ematologia Sapienza Università di Roma Pre-imatinib era 3- yrs esamated survival 3- yrs DFS with transplant w/o transplant Donor: 37% at 3 yrs BCR/ABL-
LAL Ph+ dell adulto Sabina Chiare+, MD, PhD Divisione di Ematologia Sapienza Università di Roma Pre-imatinib era 3- yrs esamated survival 3- yrs DFS with transplant w/o transplant Donor: 37% at 3 yrs BCR/ABL-