Alessandra Gorgulho, MD, MSc
|
|
|
- Maryann Parks
- 6 years ago
- Views:
Transcription




1 Manejo do Meningioma que compromete o seio cavernoso: quando eu irradio Alessandra Gorgulho, MD, MSc Chefe Clínico-Científica Centro HCor de Neurociências Professora Visitante, Departamento de Neurocirurgia, UCLA Presidente Sociedade Brasileira de Radiocirurgia V Congresso Internacional de Neuro- Oncologia de Abril 2017, São Paulo

2 Meningiomas Most frequent primary CNS tumor (34%) Simpson Grade Grade I Complete with attached dura 9% Grade II Complete with 19% dural coagulation Grade III Partial resection Grade IV Biopsy 29% 40% Recurrence Rate of III and IV is high: 50-90%


3 SRS Simpson I
4 SKULL BASE Meningioma Location difficulty to achieve Simpson Grade I in skull base lesions. Simpson grade of resection is more important than location of the lesion. Keep in mind that SRS results DO NOT depend on the level of resectability of a skull base meningioma! Radiosurgery is a BETTER option for non-resectable small to medium size SKULL BASE meningiomas (i.e., WITHOUT mass effect)!


5 Sphenoid Wing Meningioma Treatment? Microsurgery or Radiosurgery

6 Sphenoid Wing Meningioma with Cavernous Sinus Invasion Treatment? Radiosurgery


7 Mass Effect! Treatment? Decompressive Microsurgery SRS or SRT to the residual






8 This is NOT Decompressive Microneurosurgery!



9 Cavernous Sinus Lesions When Histological confirmation is necessary? Mandatory to have histological diagnosis: Atypical presentation: pain, fever, rapid progression, malignancy elsewhere Atypical radiological findings: rapid progression, edema and necrosis Surgical Options: Foramen Ovale Needle Biopsy Endoscopic or Open Surgery Diagnosis obtained: 86% cases Sensitivity = 0.83 Specificity = 1
10 UCLA Grading System for Para-sellar and other locations Meningiomas* Grade I: Restricted to the cavernous sinus/parasellar region (<3cm) Grade II: Expansion to the clivus/petrous region Grade III: Compression of the optic structures (>3cm) Grade IV: Compression of the Brainstem Grade V: Bilateral involvement of the cavernous sinus Grade VI: Optic Sheath *Modified from De Salles et al 2001 Grade I: Tumors smaller than 3 cm in largest diameter (14 cc) in any locations Grade III: Tumors larger than 3 cm in largest diameter (14 cc) in any locations



11 Cavernous Sinus Meningiomas Eligibility to Single Fraction Grade I: safety to - Optic Apparatus - Cranial Nerves (within cavernous sinus) - Brainstem Torres, Frighetto, De Salles et al - NS Focus 2003



12 Axial Sagittal Coronal Grade II 3D SRS 13 Gy 1.3 cc > 9.0Gy

13 Dose Constrains to II, III, IV, V and VI NN OA: 8 Gy III, IV,V & VI: Up to 40 Gy
14 Dose Constrains to Optic Apparatus GK, retrospective, 222 pts, cv meningioma (143), pit adenoma (72), craniopharyngioma (7) mean clinical fup: 83 mo (7y), mean radiological fup: 123 mo (10y) Visual Preservation using Single Dose (SRS) Maximum Radiation Dose OA RION 8 Gy 0% >8 to 10 Gy 0% >10 to 12 Gy 0% 12 Gy 10% Maximum Dose Point of 10 Gy : RION of < 1% Leavitt et al IJROBP 2013



15 SRT Treatment 3 years post-srt 4 years post-srt GRADE III = SRT 58y, female, blind on the left Tumor involving the chiasm SRT to preserve vision on the right ON & Chiasm 50.4 Gy, 28fx, 1.8 Gy/fx

16 IMRT PLAN: 50.4 Gy, 28 Fx GRADE III Involvement OA 7 IMRT Beams PTV=90.11cm 3 GTV=65.79cm 3 SRT



17 Axial Sagittal Coronal 12cc > 40Gy 3D 4cc > 50Gy 47 y, female, Optic and Brainstem compression Gy, 29 cc, IMRT plan, 2 mm margin PLAN: COVERS THE TAIL GRADE IV SRT
18 Visual Preservation in Stereotactic Radiation Tolerance of the Optic Apparatus Total Dose Incidence of Optic Neuropathy Dose per fraction 1.8 Gy > 1.8 Gy < 59 Gy 0/87 (0%) 0/8 (0%) 59 Gy 5/61 (8%) 10/25 (40%) Parsons IJROBP 30: , 1994; Mayo et al IJROBP 2010

 GRADE V SRT 46.8 Gy, 1.")
19 SRT as primary treatment modality Incomplete resection: difficulty to define the target - postoperative changes vs. residual tumor Mistarget: local tumor control Overcome with fractions (larger margins) GRADE V SRT 46.8 Gy, 1.8 Gy/26 fx 5 dynarcs, 2mm margin cc

20 Optic Nerve Meningioma GRADE VI SRT Gy 28 Fx of 1.8 Gy Preservation and Improvement of Vision

21 115 cases, 40% had previous surgery Median dose: 16Gy, median fup: 89 mo LTC: 99% at 5 years and 93% at 10 years Cranial Nerve Deficits Improvement: 42/136 (31%) Primary SRS : improvement = 41% With Prior Surgery = 20% (p <0.01) Permanent Complications: 14/114 (12%) TN dysfunction: 9 Diplopia: 2 Ischemic Stroke: 2 Hypopituitarism: 1 Multivariate Analysis: predictor of complications - larger tumor volume 9.3 cc = 3% vs. > 9.3 cc = 21% JNS 119:675, 2013

22 LTC: 99% at 5 years 93% at 10 years 2-year, 5-year, and 10-year rates of complications were 7%, 10%, and 15% Cranial Nerve Improvement: 42/136 (31%)
 stable tumor Tumor Volume Reduction: < 5y f-up: 43% Onset time prior to SRS: 2 (2%) tumors grew (36 & 84mo after SRS) >5y f-up: 65% (p=0.")
23 LINAC SRS Spiegelman et al J NeuroOncol Cavernous Sinus Meningiomas, Mean Fup: 68 months ( mo) Actuarial 5-year control rate = 98% Radiological Outcome: 59pts (58%) reduction of 20 95% 41 pts (40%) stable tumor Tumor Volume Reduction: < 5y f-up: 43% Onset time prior to SRS: 2 (2%) tumors grew (36 & 84mo after SRS) >5y f-up: 65% (p=0.05 chi square test) <1 year prior to SRS = 43 cranial neuropathies Resolution/ Improvement: 21 (49%) Overall Improvement or Resolution = 32% > 1 year prior to SRS = 58 cranial neuropathies Improvement = 11 (19%) (p= 0.03 chi square test)
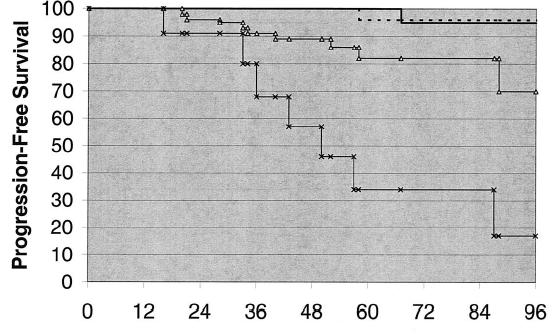
24 5300 Meningiomas
 PFS at 3, 5, 8, 10, 12 ys = 97, 93, 87, 84, 80 % respectively Clinical Response: 93.")

25 254 pts North American Gamma Knife Consortium 140 pts: upfront SRS 114 pts: w/ prior surgery Mean follow-up: 71.1 mo (range: months) PFS at 3, 5, 8, 10, 12 ys = 97, 93, 87, 84, 80 % respectively Clinical Response: 93.6 % of patients = no change or improvement 6.4 % = progression of neurological symptoms Radiological Response: Tumor Volume Increased = 9 % Stable = 52 % Decreased = 39 % Complications: 7 shunts (1 tu progression), 7 resections, 1 SRT (all tu progression)




26 Oct 1992 At 75 y Jun 2004 At 87 y Several previous operations for a large petroclival meningioma First resection: 25 years before, at age 50 SRS 12 Gy Conventional radiation therapy Neurological examination: R side facial numbness hearing loss MRI Fup: tumor growth 87 years old 12 Years Fup Karnofsky 90 Dizziness
 Median Dose: 50.")
 at 18 mo post SRT")

 During SRT: 4 HA, 3 fatigue, 1 retroorbital pain")
27 45 pts, 44 with cranial neuropathies Compression OA: 30 pts Mean Vol: 14.4cc (3.8cm) Median Dose: 50.4 Gy Median fup: 36 mo LTC: 97.4% at 3 years Tumor Growth: 1 (2%) at 18 mo post SRT Tumor shrinkage: 18% CRANIAL NERVES FUNCTION: Diplopia: 4/9 Visual deficit: 3/14 Facial numbness: 1/9 Headache: 1/6 No New Deficits Cranial NN Improvement: 20% (80% stable) During SRT: 4 HA, 3 fatigue, 1 retroorbital pain 12 mo post SRT 51 y, female 48.6 Gy, cc


28 2001: SRT 50.4 Gy, 28 fr, cc 2005: 4y post SRT 42y, female 1996: HA & vision MRI: multiple meningiomas 2000: resection of a cavernous sinus meningioma. Postop: R eye blindness, recovered a little bit overtime GRADE V: Bilateral CS & Chiasm

29 SRS SRS & SRT Series SRT
 3 Mo Post SRS A.")
 5 Mo Post -SRS A.")
 5 Mo Post -SRS B.")
 29 Mo Post -SRS 66")




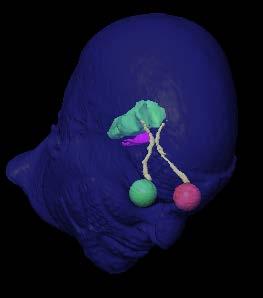
30 A.1) Date of SRS B.1) 3 Mo Post SRS A.2) 3 Mo Post -SRS A.3) 5 Mo Post -SRS A.4) 7 Mo Post -SRS B.2) 5 Mo Post -SRS B.3) 7 Mo Post -SRS B.4) 29 Mo Post -SRS 66 y female, 2 cm sphenoid wing meningioma in relation to the sphenoid venous drainage Treatment: SRS with 16 Gy, 4.2 cc, 4 dyn arcs Seizure and mental confusion - Management: steroids (2mo) & anticonvulsivants
 39 mo later: Stroke -hemiparesis and expressive aphasia Roche et al: 1 patient w/ temporary central facial palsy 14 mo after SRS & shown to have occlusion of her")
31 Carotid Artery Obliteration 66-y, female, diplopia, 10 iso, 16.8 cc lesion, 16Gy (max= 32 Gy) 39 mo later: Stroke -hemiparesis and expressive aphasia Roche et al: 1 patient w/ temporary central facial palsy 14 mo after SRS & shown to have occlusion of her intracavernous internal carotid artery. Dose to the artery: 36Gy Caution: attempt to minimize the radiation dose to major arteries whenever possible Pollock et al IJROBP 2005


32 SRS Date 5 years post-srs Dura Tail FAILURE! Grade IV - 45y female, status postop + post SRS with 12 Gy Tail no standard guidelines: Encompass some of the tail into the target volume

33 Literature Review - Surgery/SRS/SRT

34 Summary SRS/SRT Results for CV Meningiomas Established treatment modality: - Adjuvant to partial resection - Primary tt for lesions not amenable to complete resection - LOCAL TUMOR CONTROL (LTC) SRS = 97% LTC in 5 y & 93% LTC in 10 y SRT = 97.5% LTC in 5 years and 90% LTC in 10 y Improvement of Previous Cranial Deficits: 20-42% Complications: Cranial nerve deficits Post radiation peri-tumoral edema Motor deficit/vascular occlusion Hydrocephalus

35 Small & Asymptomatic: Follow up MRI Convexity: Resection: goal = GTR SRS/SRT: adjuvant if needed advanced age, bad clinical status Skull Base: Small & Symptomatic or Growing: SRS Large: Surgery: DECOMPRESSION SRT Combination






36 HCor Neurosurgery, Radiation Oncology & Medical Physics: Antonio De Salles, MD, PhD Alessandra Gorgulho, MD, MSc Bruno Fernandes, MD João Vitor Salvajoli, MD, PhD Bernardo Salvajoli, MD Crystian Saraiva, PhD Anderson Pássaro, MD Paula Toledo, NP Research Team: Camila Lasagno, Coordinator Lucas Petri Damiani, PhD 7 Congresso SBRC 3 Congresso Íbero- Americano RC Nov 2018 ISR S
Impact of Gamma Knife Radiosurgery on the neurosurgical management of skull-base lesions: The Combined Approach
 Radiosurgery as part of the neurosurgical armamentarium: Educational Symposium November 24 th 2011 Impact of Gamma Knife Radiosurgery on the neurosurgical management of skull-base lesions: The Combined
Radiosurgery as part of the neurosurgical armamentarium: Educational Symposium November 24 th 2011 Impact of Gamma Knife Radiosurgery on the neurosurgical management of skull-base lesions: The Combined
Otolaryngologist s Perspective of Stereotactic Radiosurgery
 Otolaryngologist s Perspective of Stereotactic Radiosurgery Douglas E. Mattox, M.D. 25 th Alexandria International Combined ORL Conference April 18-20, 2007 Acoustic Neuroma Benign tumor of the schwann
Otolaryngologist s Perspective of Stereotactic Radiosurgery Douglas E. Mattox, M.D. 25 th Alexandria International Combined ORL Conference April 18-20, 2007 Acoustic Neuroma Benign tumor of the schwann
Gamma knife radiosurgery for Koos grade 4 vestibular schwannomas
 Gamma knife radiosurgery for Koos grade 4 vestibular schwannomas David Mathieu MD FRCSC, Christian Iorio-Morin MD PhD, Fahd Al Subaie MD MSc FRCSC Division of neurosurgery, Université de Sherbrooke, Centre
Gamma knife radiosurgery for Koos grade 4 vestibular schwannomas David Mathieu MD FRCSC, Christian Iorio-Morin MD PhD, Fahd Al Subaie MD MSc FRCSC Division of neurosurgery, Université de Sherbrooke, Centre
Hypofractionated radiosurgery for meningiomas a safer alternative for large tumors?
 Original Article Hypofractionated radiosurgery for meningiomas a safer alternative for large tumors? Damon E. Smith 1, Sanjay Ghosh 2, Michael O Leary 2, Colin Chu 1, David Brody 2 1 Genesis Healthcare
Original Article Hypofractionated radiosurgery for meningiomas a safer alternative for large tumors? Damon E. Smith 1, Sanjay Ghosh 2, Michael O Leary 2, Colin Chu 1, David Brody 2 1 Genesis Healthcare
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
AAPM WGSBRT NTCP Optic Apparatus (chiasm and nerve)
") AAPM WGSBRT NTCP Optic Apparatus (chiasm and nerve) Michael T. Milano, MD PhD Department of Radiation Oncology University of Rochester, Rochester, NY 07/16/15 AAPM WGSBRT Optic Apparatus NTCP Issam El
AAPM WGSBRT NTCP Optic Apparatus (chiasm and nerve) Michael T. Milano, MD PhD Department of Radiation Oncology University of Rochester, Rochester, NY 07/16/15 AAPM WGSBRT Optic Apparatus NTCP Issam El
STEREOTACTIC RADIATION THERAPY. Monique Blanchard ANUM Radiation Oncology Epworth HealthCare
 STEREOTACTIC RADIATION THERAPY Monique Blanchard ANUM Radiation Oncology Epworth HealthCare Overview Stereotactic radiation therapy at Epworth Healthcare What is stereotactic radiation therapy? Delivery
STEREOTACTIC RADIATION THERAPY Monique Blanchard ANUM Radiation Oncology Epworth HealthCare Overview Stereotactic radiation therapy at Epworth Healthcare What is stereotactic radiation therapy? Delivery
Meningioma tumor. Meningiomas are named according to their location (Fig. 1) and cause various symptoms: > 1
 and cause various symptoms: > 1") Meningioma tumor Overview A meningioma is a type of tumor that grows from the protective membranes, called meninges, which surround the brain and spinal cord. Most meningiomas are benign (not cancer) and
Meningioma tumor Overview A meningioma is a type of tumor that grows from the protective membranes, called meninges, which surround the brain and spinal cord. Most meningiomas are benign (not cancer) and
11/27/2017. Modern Treatment of Meningiomas. Disclosures. Modern is Better? No disclosures relevant to this presentation
 Modern Treatment of Meningiomas Michael A. Vogelbaum MD, PhD Professor of Neurosurgery Cleveland Clinic Disclosures No disclosures relevant to this presentation IP and royalties related to drug and device
Modern Treatment of Meningiomas Michael A. Vogelbaum MD, PhD Professor of Neurosurgery Cleveland Clinic Disclosures No disclosures relevant to this presentation IP and royalties related to drug and device
NANOS Patient Brochure
 NANOS Patient Brochure Pituitary Tumor Copyright 2015. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for informational
NANOS Patient Brochure Pituitary Tumor Copyright 2015. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for informational
Overview of radiosurgery for benign brain tumors
 Overview of radiosurgery for benign brain tumors Anuj V. Peddada, M.D. Department of Radiation Oncology Penrose Cancer Center Colorado Springs, CO Objectives Provide overview of benign brain tumors meningiomas
Overview of radiosurgery for benign brain tumors Anuj V. Peddada, M.D. Department of Radiation Oncology Penrose Cancer Center Colorado Springs, CO Objectives Provide overview of benign brain tumors meningiomas
Fractionated Stereotactic Radiotherapy. Rationale, indications, & treatment techniques
 Fractionated Stereotactic Radiotherapy Rationale, indications, & treatment techniques Radiobiological principles The BED (Gy) = D(1 + d/α/β) Assume BED 1 = BED 2 for tissue of an unknown α/β: Optic
Fractionated Stereotactic Radiotherapy Rationale, indications, & treatment techniques Radiobiological principles The BED (Gy) = D(1 + d/α/β) Assume BED 1 = BED 2 for tissue of an unknown α/β: Optic
Dosimetry, see MAGIC; Polymer gel dosimetry. Fiducial tracking, see CyberKnife radiosurgery
 Subject Index Acoustic neuroma, neurofibromatosis type 2 complications 103, 105 hearing outcomes 103, 105 outcome measures 101 patient selection 105 study design 101 tumor control 101 105 treatment options
Subject Index Acoustic neuroma, neurofibromatosis type 2 complications 103, 105 hearing outcomes 103, 105 outcome measures 101 patient selection 105 study design 101 tumor control 101 105 treatment options
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
Update on IGKRF Activities
 Stereotactic radiosurgery research, education and publishing for the purpose of improving public health Fall 2016 In this issue: Update on IGKRF Activities The IGKRF Recently Published Articles Topics
Stereotactic radiosurgery research, education and publishing for the purpose of improving public health Fall 2016 In this issue: Update on IGKRF Activities The IGKRF Recently Published Articles Topics
NON MALIGNANT BRAIN TUMOURS Facilitator. Ros Taylor Advanced Neurosurgical Nurse Practitioner Southmead Hospital Bristol
 NON MALIGNANT BRAIN TUMOURS Facilitator Ros Taylor Advanced Neurosurgical Nurse Practitioner Southmead Hospital Bristol Neurosurgery What will be covered? Meningioma Vestibular schwannoma (acoustic neuroma)
NON MALIGNANT BRAIN TUMOURS Facilitator Ros Taylor Advanced Neurosurgical Nurse Practitioner Southmead Hospital Bristol Neurosurgery What will be covered? Meningioma Vestibular schwannoma (acoustic neuroma)
Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015
 Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015 Most common brain tumor, affecting 8.5-15% of cancer patients. Treatment options: Whole brain radiation
Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015 Most common brain tumor, affecting 8.5-15% of cancer patients. Treatment options: Whole brain radiation
Stereotactic Radiosurgery of World Health Organization Grade II and III Intracranial Meningiomas
 Stereotactic Radiosurgery of World Health Organization Grade II and III Intracranial Meningiomas Treatment Results on the Basis of a 22-Year Experience Bruce E. Pollock, MD 1,2 ; Scott L. Stafford, MD
Stereotactic Radiosurgery of World Health Organization Grade II and III Intracranial Meningiomas Treatment Results on the Basis of a 22-Year Experience Bruce E. Pollock, MD 1,2 ; Scott L. Stafford, MD
Overview of MLC-based Linac Radiosurgery
 SRT I: Comparison of SRT Techniques 1 Overview of MLC-based Linac Radiosurgery Grace Gwe-Ya Kim, Ph.D. DABR 2 MLC based Linac SRS Better conformity for irregular target Improved dose homogeneity inside
SRT I: Comparison of SRT Techniques 1 Overview of MLC-based Linac Radiosurgery Grace Gwe-Ya Kim, Ph.D. DABR 2 MLC based Linac SRS Better conformity for irregular target Improved dose homogeneity inside
Effectiveness and Safety of Spot Scanning Proton Radiation Therapy for Skull Base Tumors: First Long Term Report of the PSI Experience
 Effectiveness and Safety of Spot Scanning Proton Radiation Therapy for Skull Base Tumors: First Long Term Report of the PSI Experience Carmen Ares, Antony J Lomax, Eugen B Hug, Alessandra Bolsi, Beate
Effectiveness and Safety of Spot Scanning Proton Radiation Therapy for Skull Base Tumors: First Long Term Report of the PSI Experience Carmen Ares, Antony J Lomax, Eugen B Hug, Alessandra Bolsi, Beate
Literature Review: Neurosurgery
 NANOS 2018 Kona, Hawaii Literature Review: Neurosurgery Neil R. Miller, MD FACS Frank B. Walsh Professor of Neuro-Ophthalmology Professor of Ophthalmology, Neurology & Neurosurgery Johns Hopkins University
NANOS 2018 Kona, Hawaii Literature Review: Neurosurgery Neil R. Miller, MD FACS Frank B. Walsh Professor of Neuro-Ophthalmology Professor of Ophthalmology, Neurology & Neurosurgery Johns Hopkins University
Paraganglioma of the Skull Base. Ross Zeitlin, MD Medical College of Wisconsin Milwaukee, WI
 Paraganglioma of the Skull Base Ross Zeitlin, MD Medical College of Wisconsin Milwaukee, WI Case Presentation 63-year-old female presents with right-sided progressive conductive hearing loss for several
Paraganglioma of the Skull Base Ross Zeitlin, MD Medical College of Wisconsin Milwaukee, WI Case Presentation 63-year-old female presents with right-sided progressive conductive hearing loss for several
Specialised Services Policy: CP22. Stereotactic Radiosurgery
 Specialised Services Policy: CP22 Document Author: Assistant Director of Planning Executive Lead: Director of Planning ad Performance Approved by: Management Group Issue Date: 01 July 2015 Review Date:
Specialised Services Policy: CP22 Document Author: Assistant Director of Planning Executive Lead: Director of Planning ad Performance Approved by: Management Group Issue Date: 01 July 2015 Review Date:
ANALYSIS OF TREATMENT OUTCOMES WITH LINAC BASED STEREOTACTIC RADIOSURGERY IN INTRACRANIAL ARTERIOVENOUS MALFORMATIONS
 ANALYSIS OF TREATMENT OUTCOMES WITH LINAC BASED STEREOTACTIC RADIOSURGERY IN INTRACRANIAL ARTERIOVENOUS MALFORMATIONS Dr. Maitri P Gandhi 1, Dr. Chandni P Shah 2 1 Junior resident, Gujarat Cancer & Research
ANALYSIS OF TREATMENT OUTCOMES WITH LINAC BASED STEREOTACTIC RADIOSURGERY IN INTRACRANIAL ARTERIOVENOUS MALFORMATIONS Dr. Maitri P Gandhi 1, Dr. Chandni P Shah 2 1 Junior resident, Gujarat Cancer & Research
Radiotherapy approaches to pituitary tumors
 Disclosures No relevant disclosures Radiotherapy approaches to pituitary tumors Pituitary Disorders: Advances in Diagnosis and Management Steve Braunstein, MD, PhD UCSF Department of Radiation Oncology
Disclosures No relevant disclosures Radiotherapy approaches to pituitary tumors Pituitary Disorders: Advances in Diagnosis and Management Steve Braunstein, MD, PhD UCSF Department of Radiation Oncology
Radioterapia degli adenomi ipofisari
 Radioterapia degli adenomi ipofisari G Minniti Radiation Oncology, Sant Andrea Hospital, University of Rome Sapienza, and IRCCS Neuromed, Pozzilli (IS) Roma 6-9 Novembre 14 ! Outline " Radiation techniques
Radioterapia degli adenomi ipofisari G Minniti Radiation Oncology, Sant Andrea Hospital, University of Rome Sapienza, and IRCCS Neuromed, Pozzilli (IS) Roma 6-9 Novembre 14 ! Outline " Radiation techniques
Selected radiosurgery cases from the Rotating Gamma Institute Debrecen, Hungary
 Selected radiosurgery cases from the Rotating Gamma Institute Debrecen, Hungary László Bognár M.D., Ph.D., József G. Dobai M.D., Gábor Csiky and Imre Fedorcsák M.D., Ph.D. Department of Neurosurgery, Medical
Selected radiosurgery cases from the Rotating Gamma Institute Debrecen, Hungary László Bognár M.D., Ph.D., József G. Dobai M.D., Gábor Csiky and Imre Fedorcsák M.D., Ph.D. Department of Neurosurgery, Medical
Brain and Spine Tumors
 Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Brain Tumors. Andrew J. Fabiano, MD FAANS. Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine
 Brain Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases Brain
Brain Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases Brain
Neuro-oncology Update Andrew Kokkino, MD Medical Director, The Neurosciences Institute at Sacred Heart at Riverbend May 20, 2013
 Neuro-oncology Update 2013 Andrew Kokkino, MD Medical Director, The Neurosciences Institute at Sacred Heart at Riverbend May 20, 2013 Case 1 58 year old man with recent facial droop and HA s Thin, cachectic
Neuro-oncology Update 2013 Andrew Kokkino, MD Medical Director, The Neurosciences Institute at Sacred Heart at Riverbend May 20, 2013 Case 1 58 year old man with recent facial droop and HA s Thin, cachectic
Leptomeningeal metastasis: management and guidelines. Emilie Le Rhun Lille, FR Zurich, CH
 Leptomeningeal metastasis: management and guidelines Emilie Le Rhun Lille, FR Zurich, CH Definition of LM LM is defined as the spread of tumor cells within the leptomeninges and the subarachnoid space
Leptomeningeal metastasis: management and guidelines Emilie Le Rhun Lille, FR Zurich, CH Definition of LM LM is defined as the spread of tumor cells within the leptomeninges and the subarachnoid space
FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR PILOCYTIC ASTROCYTOMA
 1 EVIDENCE SUMMARY REPORT FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR PILOCYTIC ASTROCYTOMA QUESTIONS TO BE ADDRESSED: SUMMARY 1. What is the evidence for the clinical
1 EVIDENCE SUMMARY REPORT FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR PILOCYTIC ASTROCYTOMA QUESTIONS TO BE ADDRESSED: SUMMARY 1. What is the evidence for the clinical
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Tumor and Skull Base Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Tumor / Skull Base Neurosurgery
Introduction to Neurosurgical Subspecialties: Tumor and Skull Base Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Tumor / Skull Base Neurosurgery
Fractionated stereotactic radiation therapy improves cranial neuropathies in patients with skull base meningiomas: a retrospective cohort study.
 Thomas Jefferson University Jefferson Digital Commons Department of Radiation Oncology Faculty Papers Department of Radiation Oncology 1-1-2012 Fractionated stereotactic radiation therapy improves cranial
Thomas Jefferson University Jefferson Digital Commons Department of Radiation Oncology Faculty Papers Department of Radiation Oncology 1-1-2012 Fractionated stereotactic radiation therapy improves cranial
A lthough more than 90% of intracranial meningiomas are
 226 PAPER Complications after gamma knife radiosurgery for benign meningiomas J H Chang, J W Chang, J Y Choi, Y G Park, S S Chung... See end of article for authors affiliations... Correspondence to: Professor
226 PAPER Complications after gamma knife radiosurgery for benign meningiomas J H Chang, J W Chang, J Y Choi, Y G Park, S S Chung... See end of article for authors affiliations... Correspondence to: Professor
Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland. In patients
Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland. In patients
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Imaging pituitary gland tumors
 November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
Neurosurgery Review. Mudit Sharma, MD May 16 th, 2008
 Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Radiation Technology, Hyogo Ion Beam Medical Center, Tatsuno, Hyogo, JAPAN
 Analysis of Visual Loss Due to Radiation- Induced Optic Neuropathy After Particle Therapy for Head and Neck and Skull Base Tumors Adjacent to Optic Nerves Y. Demizu 1, M. Murakami 1, D. Miyawaki 1, Y.
Analysis of Visual Loss Due to Radiation- Induced Optic Neuropathy After Particle Therapy for Head and Neck and Skull Base Tumors Adjacent to Optic Nerves Y. Demizu 1, M. Murakami 1, D. Miyawaki 1, Y.
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
No Financial Interest
 Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
Case Report Carbon Ion Beam Radiotherapy for Sinonasal Malignant Tumors Invading Skull Base
 Case Reports in Otolaryngology, Article ID 241856, 4 pages http://dx.doi.org/10.1155/2014/241856 Case Report Carbon Ion Beam Radiotherapy for Sinonasal Malignant Tumors Invading Skull Base Nobuo Ohta,
Case Reports in Otolaryngology, Article ID 241856, 4 pages http://dx.doi.org/10.1155/2014/241856 Case Report Carbon Ion Beam Radiotherapy for Sinonasal Malignant Tumors Invading Skull Base Nobuo Ohta,
DISCLOSURES LEARNING OBJECTIVES WE WILL NOT DISCUSS. CSB: Birdseye View MESSAGE NAVIGATING THE SELLA AND CENTRAL SKULL BASE
 NAVIGATING THE SELLA AND CENTRAL SKULL BASE Christopher P. Hess, M.D., Ph.D. DISCLOSURES Research Support, General Electric SLIDES: http://www.radiology.ucsf.edu/research/meetings/rsna LEARNING OBJECTIVES
NAVIGATING THE SELLA AND CENTRAL SKULL BASE Christopher P. Hess, M.D., Ph.D. DISCLOSURES Research Support, General Electric SLIDES: http://www.radiology.ucsf.edu/research/meetings/rsna LEARNING OBJECTIVES
Sponsored by: Congress of Neurological Surgeons (CNS) and the Section on Tumors
 and the Section on Tumors") 1 2 3 4 5 6 7 8 CONGRESS OF NEUROLOGICAL SURGEONS SYSTEMATIC REVIEW AND EVIDENCE-BASED GUIDELINE ON THE ROLE OF RADIOSURGERY AND RADIATION THERAPY IN THE MANAGEMENT OF PATIENTS WITH VESTIBULAR SCHWANNOMAS
1 2 3 4 5 6 7 8 CONGRESS OF NEUROLOGICAL SURGEONS SYSTEMATIC REVIEW AND EVIDENCE-BASED GUIDELINE ON THE ROLE OF RADIOSURGERY AND RADIATION THERAPY IN THE MANAGEMENT OF PATIENTS WITH VESTIBULAR SCHWANNOMAS
FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR HAEMANGIOBLASTOMA
 1 EVIDENCE SUMMARY REPORT FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR HAEMANGIOBLASTOMA QUESTIONS TO BE ADDRESSED: 1. What is the evidence for the clinical effectiveness
1 EVIDENCE SUMMARY REPORT FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR HAEMANGIOBLASTOMA QUESTIONS TO BE ADDRESSED: 1. What is the evidence for the clinical effectiveness
Imaging for suspected glioma
 Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology. Tim Lucas, MD, PhD Neurosurgery
 in Neuro-Oncology. Tim Lucas, MD, PhD Neurosurgery") Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology Tim Lucas, MD, PhD Neurosurgery Timothy.Lucas@uphs.upenn.edu 2016 Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology Tim Lucas, MD,
Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology Tim Lucas, MD, PhD Neurosurgery Timothy.Lucas@uphs.upenn.edu 2016 Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology Tim Lucas, MD,
Proton-Radiotherapy for Tumors of the Skull Base: Indications, Advantages, Limitations
 Proton-Radiotherapy for Tumors of the Skull Base: Indications, Advantages, Limitations Eugen B. Hug, MD Director, Center for Proton-Radiotherapy, Paul Scherrer Institut, Villigen and Chair of Proton-Radiotherapy.
Proton-Radiotherapy for Tumors of the Skull Base: Indications, Advantages, Limitations Eugen B. Hug, MD Director, Center for Proton-Radiotherapy, Paul Scherrer Institut, Villigen and Chair of Proton-Radiotherapy.
Selecting the Optimal Treatment for Brain Metastases
 Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen?
 Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Proton Therapy for tumors of the skull base - RESULTS. Eugen B. Hug, MD Medical Director, ProCure Proton Therapy Centers, NY
 Proton Therapy for tumors of the skull base - RESULTS Eugen B. Hug, MD Medical Director, ProCure Proton Therapy Centers, NY Petroclival Chondrosarcoma: 68 72 Gy(RBE) at 1.8 or 2.0 Gy(RBE) GTV: 70.2 Gy(RBE)
Proton Therapy for tumors of the skull base - RESULTS Eugen B. Hug, MD Medical Director, ProCure Proton Therapy Centers, NY Petroclival Chondrosarcoma: 68 72 Gy(RBE) at 1.8 or 2.0 Gy(RBE) GTV: 70.2 Gy(RBE)
PITUITARY PARASELLAR LESIONS. Kim Learned, MD
 PITUITARY PARASELLAR LESIONS Kim Learned, MD DIFFERENTIALS Pituitary Sella Clivus, Sphenoid Sinus Suprasellar Optic chiasm, Hypothalamus, Circle of Willis Parasellar Cavernous Sinus Case 1 17 YEAR-OLD
PITUITARY PARASELLAR LESIONS Kim Learned, MD DIFFERENTIALS Pituitary Sella Clivus, Sphenoid Sinus Suprasellar Optic chiasm, Hypothalamus, Circle of Willis Parasellar Cavernous Sinus Case 1 17 YEAR-OLD
Clinical Commissioning Policy: Arteriovenous Malformations. December Reference : NHSCB/D5/4
 Clinical Commissioning Policy: Arteriovenous Malformations December 2012 Reference : NHSCB/D5/4 NHS Commissioning Board Clinical Commissioning Policy: Arteriovenous Malformations First published: December
Clinical Commissioning Policy: Arteriovenous Malformations December 2012 Reference : NHSCB/D5/4 NHS Commissioning Board Clinical Commissioning Policy: Arteriovenous Malformations First published: December
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Classification of Facial Pain. Surgical Treatment of Facial Pain. Typical trigeminal neuralgia. Atypical trigeminal neuralgia
 Surgical Treatment of Facial Pain Nicholas M. Barbaro, MD University of California at San Francisco Classification of Facial Pain Trigeminal neuralgia Atypical trigeminal neuralgia Neuropathic facial pain
Surgical Treatment of Facial Pain Nicholas M. Barbaro, MD University of California at San Francisco Classification of Facial Pain Trigeminal neuralgia Atypical trigeminal neuralgia Neuropathic facial pain
ARROCase Brain Metastases
 ARROCase Brain Metastases Colin Hill*, Daniel M. Trifiletti*, Timothy N. Showalter*, Jason P. Sheehan Radiation Oncology* and Neurosurgery University of Virginia Charlottesville, VA Case: HPI 64 year old
ARROCase Brain Metastases Colin Hill*, Daniel M. Trifiletti*, Timothy N. Showalter*, Jason P. Sheehan Radiation Oncology* and Neurosurgery University of Virginia Charlottesville, VA Case: HPI 64 year old
Surgical therapeutic strategy for giant pituitary adenomas.
 Biomedical Research 2017; 28 (19): 8284-8288 ISSN 0970-938X www.biomedres.info Surgical therapeutic strategy for giant pituitary adenomas. Han-Shun Deng, Zhi-Quan Ding, Sheng-fan Zhang, Zhi-Qiang Fa, Qing-Hua
Biomedical Research 2017; 28 (19): 8284-8288 ISSN 0970-938X www.biomedres.info Surgical therapeutic strategy for giant pituitary adenomas. Han-Shun Deng, Zhi-Quan Ding, Sheng-fan Zhang, Zhi-Qiang Fa, Qing-Hua
What Is an Arteriovenous malformation (AVM)?
?") American Society of Neuroradiology What Is an Arteriovenous malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall
American Society of Neuroradiology What Is an Arteriovenous malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall
TABLES. Imaging Modalities Evidence Tables Table 1 Computed Tomography (CT) Imaging. Conclusions. Author (Year) Classification Process/Evid ence Class
 Imaging. Conclusions. Author (Year) Classification Process/Evid ence Class") TABLES Imaging Modalities Evidence Tables Table 1 Computed Tomography (CT) Imaging Author Clark (1986) 9 Reformatted sagittal images in the differential diagnosis meningiomas and adenomas with suprasellar
TABLES Imaging Modalities Evidence Tables Table 1 Computed Tomography (CT) Imaging Author Clark (1986) 9 Reformatted sagittal images in the differential diagnosis meningiomas and adenomas with suprasellar
Background Principles and Technical Development
 Contents Part I Background Principles and Technical Development 1 Introduction and the Nature of Radiosurgery... 3 Definitions of Radiosurgery... 5 Consequences of Changing Definitions of Radiosurgery...
Contents Part I Background Principles and Technical Development 1 Introduction and the Nature of Radiosurgery... 3 Definitions of Radiosurgery... 5 Consequences of Changing Definitions of Radiosurgery...
10/23/2010. Excludes Single Surgeon Pituitary (N=~140) Skull Base Volume 12 Month UC SF. Patients. Anterior/Midline. Pituitary CSF Leak.
 Skull Base Volume 12 Month UC SF. Patients. Anterior/Midline. Pituitary CSF Leak.") Advances in Pituitary Surgery Ivan El-Sayed MD, FACS Director- Otolaryngology Minimally Invasive Skull Base Surgery Program Otolaryngology-Head and Neck Surgery University of California-San Francisco Minimally
Advances in Pituitary Surgery Ivan El-Sayed MD, FACS Director- Otolaryngology Minimally Invasive Skull Base Surgery Program Otolaryngology-Head and Neck Surgery University of California-San Francisco Minimally
Image-guided, intensity-modulated radiation therapy (IG-IMRT) for skull base chordoma and chondrosarcoma: preliminary outcomes
 for skull base chordoma and chondrosarcoma: preliminary outcomes") Neuro-Oncology Neuro-Oncology 17(6), 889 894, 2015 doi:10.1093/neuonc/nou347 Advance Access date 27 December 2014 Image-guided, intensity-modulated radiation therapy (IG-IMRT) for skull base chordoma and
Neuro-Oncology Neuro-Oncology 17(6), 889 894, 2015 doi:10.1093/neuonc/nou347 Advance Access date 27 December 2014 Image-guided, intensity-modulated radiation therapy (IG-IMRT) for skull base chordoma and
Sphenoid rhinosinusitis associated with abducens nerve palsy Case report
 Romanian Journal of Rhinology, Volume 8, No. 30, April-June 2018 CASE REPORT Sphenoid rhinosinusitis associated with abducens nerve palsy Case report Lucian Lapusneanu 1, Marlena Radulescu 1, Florin Ghita
Romanian Journal of Rhinology, Volume 8, No. 30, April-June 2018 CASE REPORT Sphenoid rhinosinusitis associated with abducens nerve palsy Case report Lucian Lapusneanu 1, Marlena Radulescu 1, Florin Ghita
Craniopharyngiomas (from Greek: κρανίον, skull
 J Neurosurg 119:1194 1207, 2013 AANS, 2013 Endoscopic endonasal surgery for craniopharyngiomas: surgical outcome in 64 patients Clinical article Maria Koutourousiou, M.D., 1 Paul A. Gardner, M.D., 1 Juan
J Neurosurg 119:1194 1207, 2013 AANS, 2013 Endoscopic endonasal surgery for craniopharyngiomas: surgical outcome in 64 patients Clinical article Maria Koutourousiou, M.D., 1 Paul A. Gardner, M.D., 1 Juan
ACOUSTIC NEUROMAS. Being invited to Florence, Italy to address an international medical meeting about our work for
 ACOUSTIC NEUROMAS Being invited to Florence, Italy to address an international medical meeting about our work for head and neck tumors was a great honor. The symposium organized under the auspices of the
ACOUSTIC NEUROMAS Being invited to Florence, Italy to address an international medical meeting about our work for head and neck tumors was a great honor. The symposium organized under the auspices of the
Urgent and Emergent Pituitary Conditions
 Urgent and Emergent Pituitary Conditions PANKAJ A. GORE, MD DIRECTOR, BRAIN AND SKULL BASE T UMOR SURGERY PROVIDENCE B R AIN AND S PINE I NSTITUTE Urgent and Emergent Pituitary Conditions Neurosurgical
Urgent and Emergent Pituitary Conditions PANKAJ A. GORE, MD DIRECTOR, BRAIN AND SKULL BASE T UMOR SURGERY PROVIDENCE B R AIN AND S PINE I NSTITUTE Urgent and Emergent Pituitary Conditions Neurosurgical
Target Delineation in Gliomas. Prof PK Julka Department of Radiotherapy and Oncology AIIMS, New Delhi
 Target Delineation in Gliomas Prof PK Julka Department of Radiotherapy and Oncology AIIMS, New Delhi 1 What is a glioma? A primary brain tumour that originated from a cell of the nervous system 2 Recommendations:
Target Delineation in Gliomas Prof PK Julka Department of Radiotherapy and Oncology AIIMS, New Delhi 1 What is a glioma? A primary brain tumour that originated from a cell of the nervous system 2 Recommendations:
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES
 DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
Treatment of Recurrent Brain Metastases
 Treatment of Recurrent Brain Metastases Penny K. Sneed, M.D. Dept. of Radiation Oncology University of California San Francisco Background Brain metastases occur in 8.5-15% of cancer pts in population-
Treatment of Recurrent Brain Metastases Penny K. Sneed, M.D. Dept. of Radiation Oncology University of California San Francisco Background Brain metastases occur in 8.5-15% of cancer pts in population-
Skullbase Lesions. Skullbase Surgery Open vs endoscopic. Choice Of Surgical Approaches 12/28/2015. Skullbase Surgery: Evolution
 Skullbase Lesions Skullbase Surgery Open vs endoscopic Prof Asim Mahmood,FRCS,FACS,FICS,FAANS, Professor of Neurosurgery Henry Ford Hospital Detroit, MI, USA Anterior Cranial Fossa Subfrontal meningioma
Skullbase Lesions Skullbase Surgery Open vs endoscopic Prof Asim Mahmood,FRCS,FACS,FICS,FAANS, Professor of Neurosurgery Henry Ford Hospital Detroit, MI, USA Anterior Cranial Fossa Subfrontal meningioma
Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey
 Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia
 for Brain Metastasis in Nova Scotia") A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR EPENDYMOMA
 1 EVIDENCE SUMMARY REPORT FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR EPENDYMOMA QUESTIONS TO BE ADDRESSED: 1. What is the evidence for the clinical effectiveness
1 EVIDENCE SUMMARY REPORT FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR EPENDYMOMA QUESTIONS TO BE ADDRESSED: 1. What is the evidence for the clinical effectiveness
The View through the Nose: ENT considerations for Pituitary/Skull Base Surgery
 The View through the Nose: ENT considerations for Pituitary/Skull Base Surgery Edsel Kim, M.D. Otolaryngology-Head and Neck Surgery The Oregon Clinic Providence Brain and Spine Institute Pituitary, Thyroid
The View through the Nose: ENT considerations for Pituitary/Skull Base Surgery Edsel Kim, M.D. Otolaryngology-Head and Neck Surgery The Oregon Clinic Providence Brain and Spine Institute Pituitary, Thyroid
S tereotactic radiosurgery, whether delivered by a gamma
 1536 PAPER Gamma knife stereotactic radiosurgery for unilateral acoustic neuromas J G Rowe, M W R Radatz, L Walton, A Hampshire, S Seaman, A A Kemeny... See end of article for authors affiliations... Correspondence
1536 PAPER Gamma knife stereotactic radiosurgery for unilateral acoustic neuromas J G Rowe, M W R Radatz, L Walton, A Hampshire, S Seaman, A A Kemeny... See end of article for authors affiliations... Correspondence
Imaging The Turkish Saddle. Russell Goodman, HMS III Dr. Gillian Lieberman
 Imaging The Turkish Saddle Russell Goodman, HMS III Dr. Gillian Lieberman Learning Objectives Review the anatomy of the sellar region Discuss the differential diagnosis of sellar masses Discuss typical
Imaging The Turkish Saddle Russell Goodman, HMS III Dr. Gillian Lieberman Learning Objectives Review the anatomy of the sellar region Discuss the differential diagnosis of sellar masses Discuss typical
Stereotactic Radiosurgery for Glossopharyngeal Neuralgia: An International Multicenter Study
 Stereotactic Radiosurgery for Glossopharyngeal Neuralgia: An International Multicenter Study University of Pittsburgh Hideyuki Kano, MD, PhD L. Dade Lunsford, MD Hospital Na Homolce, Prague Dusan Urgosik,
Stereotactic Radiosurgery for Glossopharyngeal Neuralgia: An International Multicenter Study University of Pittsburgh Hideyuki Kano, MD, PhD L. Dade Lunsford, MD Hospital Na Homolce, Prague Dusan Urgosik,
Postoperative LINAC-Based Stereotactic Radiotherapy for Grade I Intracranial Meningioma in Subtype Classification
 Postoperative LINAC-Based Stereotactic Radiotherapy for Grade I Intracranial Meningioma in Subtype Classification Peerapong Lueangapapong MD*, Mantana Dhanachai MD**, Ake Hansasuta MD* * Division of Neurosurgery,
Postoperative LINAC-Based Stereotactic Radiotherapy for Grade I Intracranial Meningioma in Subtype Classification Peerapong Lueangapapong MD*, Mantana Dhanachai MD**, Ake Hansasuta MD* * Division of Neurosurgery,
Hong Kong Hospital Authority Convention 2018
 Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Proton Radiotherapy for Skull Base and Para-spinal Tumors
 Proton Radiotherapy for Skull Base and Para-spinal Tumors Carmen Ares Primary tumors Tumors of the Skull Base - Chordomas, Chondrosarcomas Secondary infiltration or involvement by intracranial tumors -
Proton Radiotherapy for Skull Base and Para-spinal Tumors Carmen Ares Primary tumors Tumors of the Skull Base - Chordomas, Chondrosarcomas Secondary infiltration or involvement by intracranial tumors -
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
Treatment Strategy of Intracranial Hemangiopericytoma
 ORIGINAL ARTICLE Brain Tumor Res Treat 2015;3(2):68-74 / pissn 2288-2405 / eissn 2288-2413 http://dx.doi.org/10.14791/btrt.2015.3.2.68 Treatment Strategy of Intracranial Hemangiopericytoma Young-Joo Kim
ORIGINAL ARTICLE Brain Tumor Res Treat 2015;3(2):68-74 / pissn 2288-2405 / eissn 2288-2413 http://dx.doi.org/10.14791/btrt.2015.3.2.68 Treatment Strategy of Intracranial Hemangiopericytoma Young-Joo Kim
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Leksell Gamma Knife Icon. Treatment information
 Leksell Gamma Knife Icon Treatment information You may be feeling frightened or overwhelmed by your recent diagnosis. It can be confusing trying to process a diagnosis, understand a new and challenging
Leksell Gamma Knife Icon Treatment information You may be feeling frightened or overwhelmed by your recent diagnosis. It can be confusing trying to process a diagnosis, understand a new and challenging
Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy
 Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Policy Number: Original Effective Date: MM.05.008 05/12/1999 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 03/01/2013 Section:
Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Policy Number: Original Effective Date: MM.05.008 05/12/1999 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 03/01/2013 Section:
ARRO Case: Diffuse Intrinsic Pontine Glioma
 ARRO Case: Diffuse Intrinsic Pontine Glioma Nicholas DeNunzio, MD, PhD (PGY-3) Faculty Advisor: Louis S. Constine, MD, FASTRO Department of Radiation Oncology University of Rochester Case Presentation
ARRO Case: Diffuse Intrinsic Pontine Glioma Nicholas DeNunzio, MD, PhD (PGY-3) Faculty Advisor: Louis S. Constine, MD, FASTRO Department of Radiation Oncology University of Rochester Case Presentation
IMAGE-GUIDED RADIOSURGERY USING THE GAMMA KNIFE
 IMAGE-GUIDED RADIOSURGERY USING THE GAMMA KNIFE L. D. LUNSFORD INTRODUCTION Image guided brain surgery became a reality in the mid-1970s after the introduction of the first methods to obtain axial imaging
IMAGE-GUIDED RADIOSURGERY USING THE GAMMA KNIFE L. D. LUNSFORD INTRODUCTION Image guided brain surgery became a reality in the mid-1970s after the introduction of the first methods to obtain axial imaging
Proton Therapy for Ependymoma and Craniopharyngioma at the University of Florida: Lessons Learned About Efficacy and Toxicity
 Proton Therapy for Ependymoma and Craniopharyngioma at the University of Florida: Lessons Learned About Efficacy and Toxicity Danny Indelicato, MD Mendenhall Chair of Pediatric Radiotherapy University
Proton Therapy for Ependymoma and Craniopharyngioma at the University of Florida: Lessons Learned About Efficacy and Toxicity Danny Indelicato, MD Mendenhall Chair of Pediatric Radiotherapy University
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
Protons for Head and Neck Cancer. William M Mendenhall, M.D.
 Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Update on Pediatric Brain Tumors
 Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
Untangling Cerebral Dural Arteriovenous Fistulas
 Untangling Cerebral Dural Arteriovenous Fistulas Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh September 2017 davfs Definition Clinical Presentation Natural History
Untangling Cerebral Dural Arteriovenous Fistulas Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh September 2017 davfs Definition Clinical Presentation Natural History
Endovascular Treatment of Cerebral Arteriovenous Malformations. Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh
 Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Minesh Mehta, Northwestern University. Chicago, IL
 * Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
* Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
Radiotherapy and Brain Metastases. Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem
 Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Gamma Knife Radiosurgery
 Gamma Knife Radiosurgery A Team Approach to Treating Patients George Bovis, MD Patrick Sweeney, MD Jagan Venkatesan, MS Matt White, MS Illinois Gamma Knife Center Elk Grove Village, IL Disclosures Shareholders
Gamma Knife Radiosurgery A Team Approach to Treating Patients George Bovis, MD Patrick Sweeney, MD Jagan Venkatesan, MS Matt White, MS Illinois Gamma Knife Center Elk Grove Village, IL Disclosures Shareholders
Neuro-Ocular Grand Rounds
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Brain tumours (primary) and brain metastases in adults
 and brain metastases in adults") Brain tumours (primary) and brain metastases in adults NICE guideline Draft for consultation, January 0 This guideline covers diagnosing, monitoring and managing any type of primary brain tumour or brain
Brain tumours (primary) and brain metastases in adults NICE guideline Draft for consultation, January 0 This guideline covers diagnosing, monitoring and managing any type of primary brain tumour or brain
Estimating the Risks of Adverse Radiation Effects After Gamma Knife Radiosurgery for Arteriovenous Malformations
 Estimating the Risks of Adverse Radiation Effects After Gamma Knife Radiosurgery for Arteriovenous Malformations Hideyuki Kano, MD, PhD; John C. Flickinger, MD; Daniel Tonetti, MD; Alan Hsu, MD; Huai-che
Estimating the Risks of Adverse Radiation Effects After Gamma Knife Radiosurgery for Arteriovenous Malformations Hideyuki Kano, MD, PhD; John C. Flickinger, MD; Daniel Tonetti, MD; Alan Hsu, MD; Huai-che