Pitfalls in Sinonasal Pathology
|
|
|
- Arron May
- 6 years ago
- Views:
Transcription
1 Pitfalls in Sinonasal Pathology Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences 1
2 Agenda Inflammatory Conditions Fungal sinusitis Invasive fungal disease Mid-line destructive diseases Epithelial proliferations Low and high grade carcinomas 2
3 Allergic Fungal Sinusitis 3
4 Incidence Allergic Fungal Sinusitis 5-10% of chronic sinusitis Gross Polyposis Thick, green mucus Peanut butter consistency 4

5 Allergic mucus
6 Allergic Fungal Sinusitis Histopathology Fungus Ball Allergic type mucus Allergic fungal sinusitis 6

7 Fungus ball 7
8 Fungus ball 8

9 Allergic mucus 9

10 Allergic mucus
11 Invasive Fungal Sinusitis Classification Acute necrotizing (immunocompromised) Chronic invasive (diabetics) Granulomatous (immunocompetent) Histology Necrosis Vascular invasion Granulomas and giant cells 11

12 Invasive fungal sinusitis 12

13 Invasive fungal sinusitis 13

14 Invasive fungal sinusitis 14

15 Invasive fungal sinusitis

16 Invasive fungal sinusitis 16
17 Treatment of Fungal Disease Non-invasive Surgery to remove mucus Oral then inhaled steroids (up to 1 year) Invasive Complete debridement to viable tissue Intravenous antifungal drugs 17
18 Pitfalls Midline Destructive Diseases Traumatic Infectious Toxic Inflammatory Neoplastic Physical trauma Bacterial Cocaine Sarcoid Basal cell carcinoma Iatrogenic trauma Mycobacterial Chromium salts Foreign body Squamous cell carcinoma Self-induced Fungal Wegener s Lymphoma Vasculitis Other tumors 18
19 Wegener s Granulomatosis 19
20 Clinical Wegener s Granulomatosis C-ANCA Respiratory tract & Kidney Localized vs. systemic disease Histopathology Necrotizing granulomatous inflammation Vasculitis Neutrophilic microabscesses 20

21 Wegener s 21

22 Wegener s 22

23 Wegener s 23

24 Wegener s, elastic stain 24
25 Agenda Inflammatory Conditions Fungal sinusitis Invasive fungal disease Mid-line destructive diseases Epithelial proliferations Low and high grade carcinomas 25


26 Inverted Papilloma 26
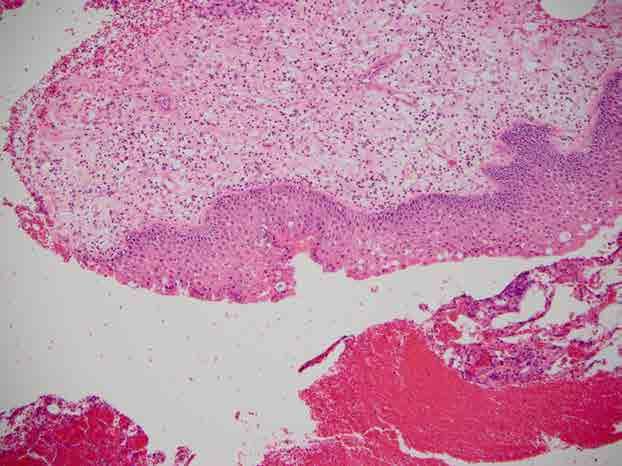
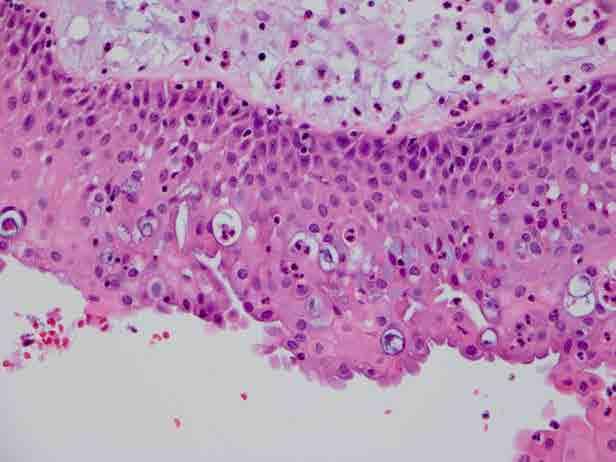
27 Incidence Schneiderian Papilloma Men > women Adult age Clinical Mass lesion, nasal obstruction Three types Inverted, Exophytic, Oncocytic 27
28 Histology Inverted Papilloma Epithelium >10 cell layers thick Epithelial morphology Transitional Squamous, respiratory, mucinous Transmigrating neutrophils Decreased or absent minor salivary glands 28

29 Inverted papilloma 29

30 Inverted papilloma 30

31 Inverted papilloma
32 Exophytic Papilloma Location: Septum Histologoy Resembles squamous papilloma of skin Residual goblet cells 32

33 Exophytic papilloma 33

34 Exophytic papilloma 34

35 Oncocytic Schneiderian Papilloma 35
36 Oncocytic Schneiderian Papilloma Location: Usually lateral nasal wall Histology Oncocytic epithelium Microcysts in epithelium Containing inflammatory debris or mucin 36

37 Oncocytic schneiderian papilloma 37

38 Oncocytic schneiderian papilloma 38
39 Pitfalls Early changes of inverted papilloma Frozen section diagnosis Identifying malignant transformation 39
40 Schneiderian Papilloma
41 Schneiderian Papilloma
42 Malignant Transformation Clinical course Synchronous tumors (61%) Asynchronous tumors (29%) Classification Dysplasia (5-20%) Invasive carcinoma (2-27%) Tumor types: squamous cell carcinoma, schneiderian carcinoma, other 42
43 Agenda Inflammatory Conditions Fungal sinusitis Invasive fungal disease Mid-line destructive diseases Epithelial proliferations Low and high grade carcinomas 43

44 Sinonasal Adenocarcinomas Salivary ITAC Non-ITAC Site % Nasal 40% Ethmoid 30% Maxillary 13% Multiple 18% 44
45 Clinical Low Grade Non-ITAC: Histology Rare lesion with generally good prognosis Histology Highly variable architecture Papillary, cystadenomatous, tubular Back-to-back glands with no myoepithelial cells Usually no vascular or perineural invasion Cytology Single layer of bland epithelial lining cells Bland nuclei 45

46 Low grade Adenocarcinoma, non-itac 46 46

47 Low grade Adenocarcinoma, non-itac 47

48 Low grade Adenocarcinoma, non-itac 48
49 Incidence Intestinal Type Adenocarcinoma Rare Men>Women Ethmoid sinus in >80% Clinical Sinonasal symptoms Occupational exposure Wood and leather dust Formaldehyde 49
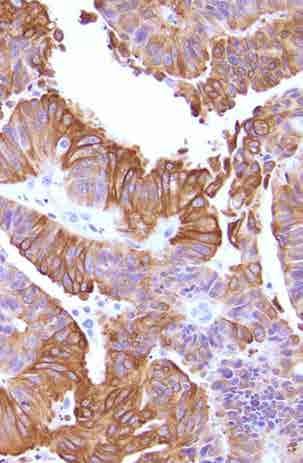
50 Intestinal Type Adenocarcinoma Histopathology: Resembles GI tumors IHC CDX2 positive CK20 positive CK 7 positive (most cases) 50

51 Intestinal type adenocarcinoma 51

52 Intestinal type adenocarcinoma 52 52

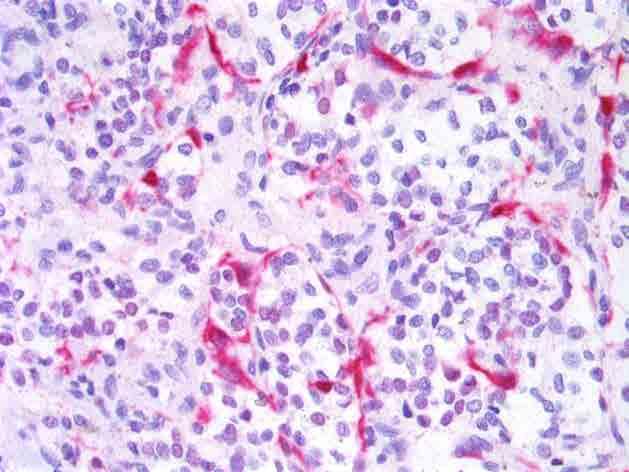
53 ITAC, CDX2 ITAC, CK20 53
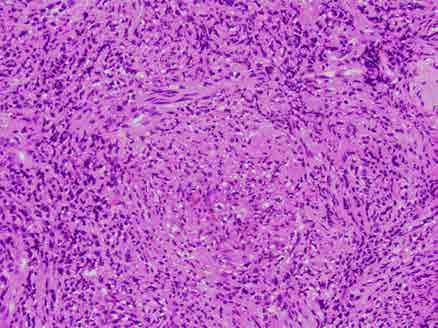
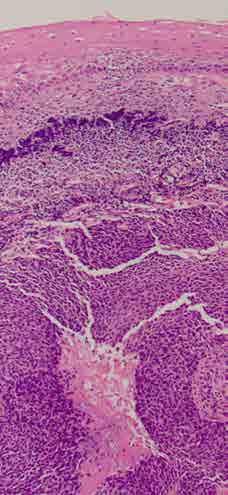
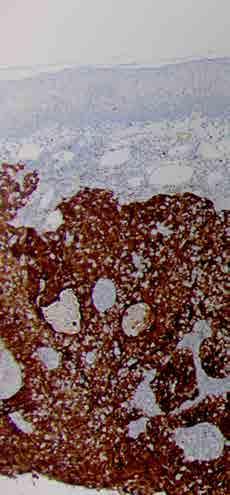
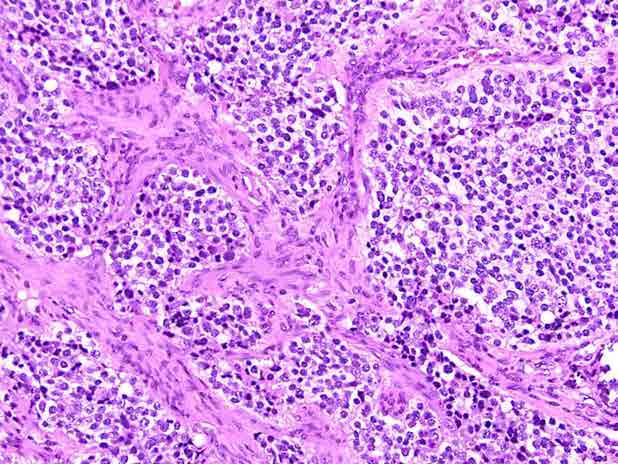
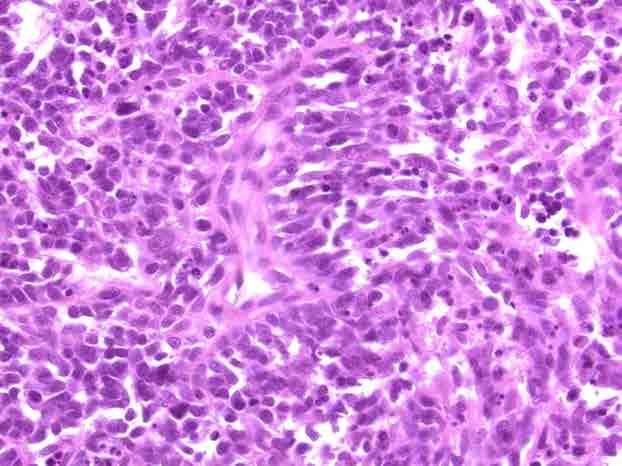
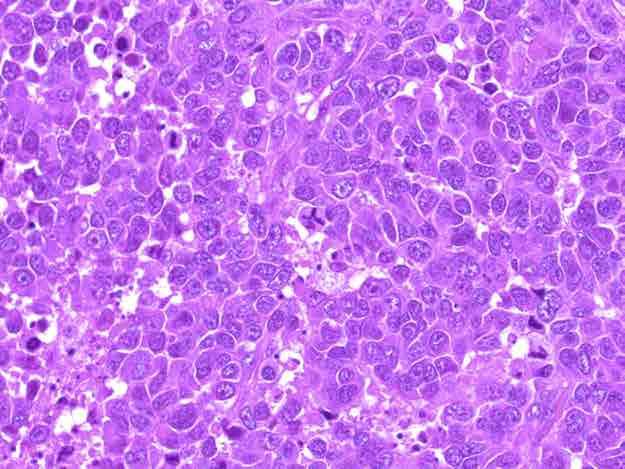
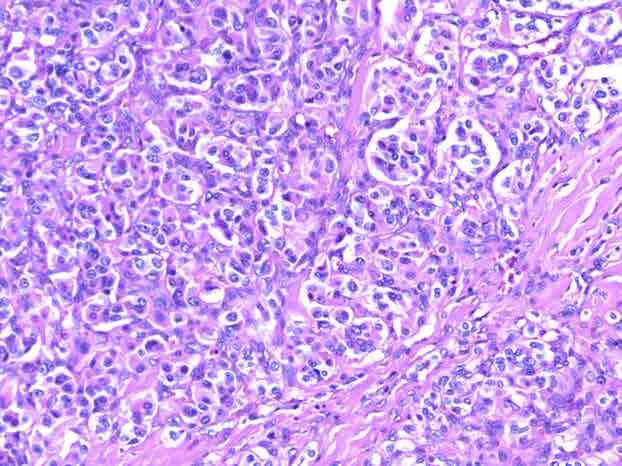
54 Sinonasal Undifferentiated Carcinoma Clinical Rare and very aggressive tumors Histopathology Undifferentiated tumor cells Mitoses and necrosis Vascular invasion and adjacent structures Immunohistochemistry Positive for Cytokeratin Rarely positive for NSE 54

55 SNUC, H&E 55

56 SNUC, H&E 56

57 SNUC, H&E 57

58 SNUC, H&E 58

59 SNUC, CAM5.2 59
60 Differential Diagnosis Melanoma Ewings/PNET Rhabdomyosarcoma NUT midline carcinoma Lymphoepithelial carcinoma Lymphoma Neuroendocrine carcinoma 60
61 Work-Up of High Grade Tumor Cytokeratin stains Neuroendocrine stains S100 HMB45 CD99 Myogenin Desmin Lymphoma markers 61
62 Summary Inflammatory Conditions Fungal sinus disease Mid-line destructive diseases Epithelial proliferations Low and high grade carcinomas 62
63 Head and Neck Lesions Every Pathologist Should Know Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences 63
64 Agenda Differential diagnosis for cysts in the neck Differential diagnosis for neuroendocrine tumors (sinonasal and beyond) 64
65 Neck Cysts Differential diagnosis for cysts in the neck Benign developmental cysts Metastatic cystic squamous cell carcinoma 65
66 Clinical Branchial Cleft Cyst Relatively common Usually in children and young adults Asymptomatic mass lesion Draining sinus Variable location 66
67 Auditory canal Palatine tonsil II I 1 External auditory meatus Parathyroid (inferior) Thymus Parathyroid (superior) Ultimobranchial body IV III Branchial pouches Pharyngeal grooves (clefts) 67
68 Branchial Cleft Cysts Type Location Lining Special features First Arch (type 1 and type 2) Second Arch Third and Fourth Arches Near the ear Tract in supratonsillar fossa Cyst in the low anterolateral neck Tract in pyriform sinus Cyst at anterior border of SCM Keratinized squamous Squamous and/or respiratory Lymphoid stroma Squamous and/or respiratory Lymphoid stroma Cartilage can be seen in type 2 95% are this type <1% Can present with suppurative thyroiditis 68

69 Branchial Cleft 69

70 Branchial Cleft 70

71 Branchial Cleft 71
72 Differential Diagnosis Thyroglossal duct cyst Thymic cyst Metastatic cystic squamous cell carcinoma 72

73 Thyroglossal duct cyst 73

74 Thymic cyst 74
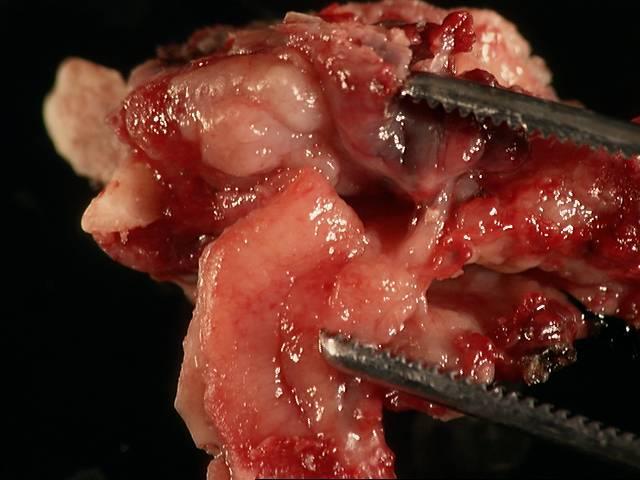
75 Clinical Cystic Metastasis Mass lesion in upper to mid-level neck 3.9 cm average size Male >> Female Average age: 54 75
76 Gross Cystic Metastasis Well circumscribed Thick capsule Multilocular Thick purulent or gumous material 76
77 Histology Cystic Metastasis Ribbon like epithelium Thickness of tonsillar type epithelium Can have endophytic or exophytic areas Cytology Moderate N:C ratio No maturation Bland appearance 77

78 Cystic Metastatic Squamous Carcinoma

79 Cystic Metastatic Squamous Carcinoma

80 Cystic Metastatic Squamous Carcinoma 80
81 Controversies Branchiogenic carcinoma vs. metastatic squamous carcinoma Bland metastasis vs. branchial cleft cyst 81
82 Differentiating Features Feature Metastasis Branchial cleft cyst Gross Cyst contents Unilocular Keratin Debris Multilocular Clear fluid Lining Dysplastic Respiratory & squamous Age Older Younger 82
83 Carcinoma in Branchial Cleft Cyst Diagnostic Criteria Anatomy Anterior to the sternocleidomastoid Between the tragus and the clavicle Association with sinus tract Histology Benign branchial cleft tissue Carcinoma with transition from benign to dysplastic and malignant epithelium Clinical course No primary tumor identified Minimum of five-year follow-up period 83
84 Clinical Metastatic Cystic Carcinoma May be first presenting symptom Primary tumor may be extremely small 64% come from the tonsil or tongue base Other sites include larynx and nasopharynx 84
85 Tonsil and Tongue Base SCC Oropharynx: >50% of tumors are positive for HPV HPV in cystic lymph node metastases Between 50 and 80% will be positive when originating from an oropharyngeal site Desai PC, Exp Mol Pathol, 87:94, 2009 Goldenberg D, Head Neck, 30:898,
86 HPV and Tumor Characteristics HPV Positive Demographics 5 years younger Non-smokers/non-drinkers HPV Negative Typical ages Tobacco and alcohol Site Tonsil & Tongue base All locations Histology Genetics Non-keratinizing, basaloid, and lymphoepithelial p53 inactivated by E6 Rb inactivated by E7 p16 over-expressed Keratinizing SCC p53 inactivated by mutation Rb inactivated by cyclin D1 amplification Inactivation of p16 86
87 HPV Detection Methods In situ hybridization DNA based either multiplexed or single type probes RNA based transcriptionally active virus Polymerase chain reaction Other methods Hybrid capture (cytology samples) p16 immunohistochemistry 87

88 H&E HPV ISH p16 IHC
89 p16 Immunohistochemistry Excellent surrogate marker for HPV p16 staining should be strong and diffuse 89
90 Why test for HPV? Diagnostic marker (cystic metastases) Prognostic marker To select therapeutic approaches De-escalation therapy 90
91 Agenda Differential diagnosis for cysts in the neck Differential diagnosis for neuroendocrine tumors in the sinonasal cavity Olfactory neuroblastoma Neuroendocrine carcinoma Paraganglioma Ectopic pituitary lesions 91
92 Olfactory Neuroblastoma 92
93 Incidence Olfactory Neuroblastoma Relatively rare (2% of sinonasal tumors) Broad age range Clinical Peaks in 2 nd and 6 th decades Sinonasal symptoms: nasal obstruction, epistaxis, non-specific symptoms Usually arises in the upper nasal cavity (superior nasal concha, upper septum, roof of nose, cribriform plate) 93
94 Olfactory Neuroblastoma Histopathology Small to medium sized cells in nests Minimal pleomorphism Rosettes Homer Wright: Central fibrillary material Up to 50% Flexner-Wintersteiner: True lumen Rare Neuropil Grading: Hyam s Grading system 94
95 Olfactory neuroblastoma 95

96 Olfactory neuroblastoma, Homer Wright rosettes 96

97 Olfactory neuroblastoma, Flexner-Wintersteiner rosettes 97
98 Olfactory Neuroblastoma Immunohistochemistry Synpatophysin, chromogranin positive S100 with sustentacular pattern CAM5.2 occasionally positive 98

99 Olfactory neuroblastoma, Synaptophysin 99

100 Olfactory neuroblastoma, S100 stain 100

101 Olfactory neuroblastoma with divergent differentiation

102 Olfactory neuroblastoma with divergent differentiation, S100


103 Olfactory neuroblastoma with divergent differentiation Synaptophysin Cytokeratin
104 Neuroendocrine Carcinomas Nomenclature Carcinoid Atypical carcinoid Neuroendocrine carcinoma, small cell type Neuroendocrine carcinoma, large cell type 104
105 Neuroendocrine Carcinoma, large cell type Incidence Rare tumor Locations: Throughout the head and neck Histology Solid sheets, ribbons, or trabeculae Large cells with coarse chromatin and nucleoli Necrosis and mitoses IHC Chromogranin, syaptophysin, NSE Cytokeratin 105
106 Neuroendocrine carcinoma 106
107 Neuroendocrine carcinoma 107

108 Neuroendocrine carcinoma, synaptophysin
109 Incidence Paraganglioma Adrenal (pheochromocytoma) >> extra-adrenal Head and Neck Clinical Originate from carotid body (most), middle ear, and vagal body Mass lesion, pulsatile Usually not functional in the head and neck 109
110 Histology Paraganglioma Neuroendocrine chromaffin cells Supporting sustentacular cells 110
111 Paraganglioma 111
112 Paraganglioma Immunohistochemistry Neuroendocrine chromaffin cells Chromogranin, Synaptophysin Negative for cytokeratins Supporting sustentacular cells S100 positive 112
113 Paraganglioma S
114 Paraganglioma Hereditary Von Hippel Lindau MEN syndromes Neurofibromatosis Familial paragangliomatosis 114
115 Clinical Ectopic Pituitary Occur along the embryological migration and invagination pathway of Rathke s Pouch Distinguish radiologically, clinically and surgically from invasive pituitary adenoma Broad age range; most common in 6 th decade Frequently mis-diagnosed 115
116 Pathology Ectopic Pituitary Bland appearing neuroendocrine lesion Hormones: FSH, LH, GH, TSH, ACTH, PRL, Calcitonin 116

117 Ectopic pituitary adenoma

118 Ectopic pituitary adenoma, ACTH
119 Summary Cystic lesions in the neck Branchial cleft cyst Thyroglossal duct and thymic cysts Cystic metastasis from squamous carcinoma HPV associated SCC Neuroendocrine tumors Olfactory neuroblastoma Neuroendocrine carcinoma, large cell type Paraganglioma Ectopic pituitary 119
Small (and large) Blue Cell Tumors of the Skull Base
 Blue Cell Tumors of the Skull Base") Small (and large) Blue Cell Tumors of the Skull Base Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Small (and large) Blue Cell Tumors of the Skull Base Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Nasal Cavity and Paranasal Sinuses
 Chapter 2 Nasal Cavity and Paranasal Sinuses Introduction Included in this chapter are nasal cavities, frontal sinus, ethmoid complex, sphenoid sinus, and maxillary sinuses. These cavities and sinuses
Chapter 2 Nasal Cavity and Paranasal Sinuses Introduction Included in this chapter are nasal cavities, frontal sinus, ethmoid complex, sphenoid sinus, and maxillary sinuses. These cavities and sinuses
Neuroendocrine Carcinoma. Lebanon Neuroendocrine Neoplasms of H&N Nov /7/2011. Broad Classification:
 H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
Head and Neck Squamous Subtypes
 1 Head and Neck Squamous Subtypes Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas HNSCC 5 th -6 th most common cancer 400,000/year 50% mortality Considerable
1 Head and Neck Squamous Subtypes Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas HNSCC 5 th -6 th most common cancer 400,000/year 50% mortality Considerable
Pathology of Selected Head and Neck Lesions. Adel Assaad MD Department of Pathology
 Pathology of Selected Head and Neck Lesions Adel Assaad MD Department of Pathology 1 NOSE Infections 2 Zygomycosis (Mucormycosis) Opportunistic infection caused by "bread mold fungi," including Rhizopus,
Pathology of Selected Head and Neck Lesions Adel Assaad MD Department of Pathology 1 NOSE Infections 2 Zygomycosis (Mucormycosis) Opportunistic infection caused by "bread mold fungi," including Rhizopus,
04/09/2018. Squamous Cell Neoplasia and Precursor Lesions. Agenda. Squamous Dysplasia. Squamo-proliferative lesions. Architectural features
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Human Papillomavirus and Head and Neck Cancer. Ed Stelow, MD
 Human Papillomavirus and Head and Neck Cancer Ed Stelow, MD No conflict of interest Declaration Cancer 1974 Lancet Oncol 2016; 17: e477-8 JAMA 1984; 252: 1857 JAMA 1988;259(13):1943-1944 Clin Cancer Res
Human Papillomavirus and Head and Neck Cancer Ed Stelow, MD No conflict of interest Declaration Cancer 1974 Lancet Oncol 2016; 17: e477-8 JAMA 1984; 252: 1857 JAMA 1988;259(13):1943-1944 Clin Cancer Res
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Basaloid neoplasms of the head and neck. Basaloid SCC. Clinico-pathologic features 5/5/11. Basaloid Tumors Head and Neck
 Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
Squamous Cell Neoplasia and Precursor Lesions
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies. Agenda
 Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Reporting HPV related carcinomas of the head and neck. dr. Nina Zidar Institute of Pathology Faculty of Medicine University of Ljubljana Slovenia
 Reporting HPV related carcinomas of the head and neck dr. Nina Zidar Institute of Pathology Faculty of Medicine University of Ljubljana Slovenia Conflict of interest/funding X None Company: Product royalties
Reporting HPV related carcinomas of the head and neck dr. Nina Zidar Institute of Pathology Faculty of Medicine University of Ljubljana Slovenia Conflict of interest/funding X None Company: Product royalties
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland
 Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland Two Main Topics Molecular insights in salivary gland
Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland Two Main Topics Molecular insights in salivary gland
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
4/17/2015. Case 1. A 37 year old man with a 2.2 cm solitary left thyroid mass.
 Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Nutn but a Small Biopsy How to approach small biopsy samples of the sinonasal tract
 California Society of Pathology Saturday Slide Seminar Nutn but a Small Biopsy How to approach small biopsy samples of the sinonasal tract Lester D. R. Thompson www.lester-thompson.com Learning Objectives
California Society of Pathology Saturday Slide Seminar Nutn but a Small Biopsy How to approach small biopsy samples of the sinonasal tract Lester D. R. Thompson www.lester-thompson.com Learning Objectives
Notice of Faculty Disclosures
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF SQUAMOUS CYSTS OF THE HEAD AND
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF SQUAMOUS CYSTS OF THE HEAD AND
Case Studies in the Skull Base
 Case Studies in the Skull Base Amy C Tsai, MD Neuroradiology Fellow Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA No disclosures related
Case Studies in the Skull Base Amy C Tsai, MD Neuroradiology Fellow Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA No disclosures related
Squamous Cell Carcinoma of Thyroid: possible thymic origin, so-called ITET/CASTLE 2012/03/22
 Squamous Cell Carcinoma of Thyroid: possible thymic origin, so-called ITET/CASTLE 2012/03/22 History of ITET/CASTLE First Report Gross Appearance and Prognosis 1) Miyauchi A et al: Intrathyroidal epithelial
Squamous Cell Carcinoma of Thyroid: possible thymic origin, so-called ITET/CASTLE 2012/03/22 History of ITET/CASTLE First Report Gross Appearance and Prognosis 1) Miyauchi A et al: Intrathyroidal epithelial
EQA Circulation 43 Educational Cases
 EQA Circulation 43 Educational Cases E1-E2 Monica Agarwal Monklands Hospital E1 38 yrs male Submandibular gland tumour E1 Formal excision following diagnosis of poorly differentiated carcinoma on core
EQA Circulation 43 Educational Cases E1-E2 Monica Agarwal Monklands Hospital E1 38 yrs male Submandibular gland tumour E1 Formal excision following diagnosis of poorly differentiated carcinoma on core
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Epithelial tumors. Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev
 Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Neoplasms of the Canine, Feline and Lemur Liver:
 Neoplasms of the Canine, Feline and Lemur Liver: Classification and Prognosis Annual Seminar of the French Society of Veterinary Pathology John M. Cullen VMD PhD DACVP North Carolina State University Primary
Neoplasms of the Canine, Feline and Lemur Liver: Classification and Prognosis Annual Seminar of the French Society of Veterinary Pathology John M. Cullen VMD PhD DACVP North Carolina State University Primary
Moffitt Weekends in Pathology Head & Neck, and Endocrine Pathology Course Outline
 Moffitt Weekends in Pathology Head & Neck, and Endocrine Pathology Course Outline Squamous Cell Lesions Lecture BMW: 8:30-9:15 Break: 9:15-9:30 Case Review LK: 9:30-10:15 Case Review JHP: 10:30-11:15 Break:
Moffitt Weekends in Pathology Head & Neck, and Endocrine Pathology Course Outline Squamous Cell Lesions Lecture BMW: 8:30-9:15 Break: 9:15-9:30 Case Review LK: 9:30-10:15 Case Review JHP: 10:30-11:15 Break:
Chapter 13: Mass in the Neck. Raymond P. Wood II:
 Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Nasal Cavity and Paranasal Sinuses
 2017 Head and Neck Tumors Selected Topics Lester D. R. Thompson 1 2 Inclusion Criteria Nasal Cavity and Paranasal Sinuses 2005 edition: 76 diagnoses 2017 edition: 39 diagnoses 3 1. The tumor occurs exclusively
2017 Head and Neck Tumors Selected Topics Lester D. R. Thompson 1 2 Inclusion Criteria Nasal Cavity and Paranasal Sinuses 2005 edition: 76 diagnoses 2017 edition: 39 diagnoses 3 1. The tumor occurs exclusively
ONCOLOGY. Csaba Bödör. Department of Pathology and Experimental Cancer Research november 19., ÁOK, III.
 ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
EDUCATIONAL CASES E1 & E2. Natasha Inglis 20/03/15
 EDUCATIONAL CASES E1 & E2 Natasha Inglis 20/03/15 CASE E1 79 year old female Rectum. Altemeier operation Histology Superficial erosions and mucosal congestion volcano lesion and pseudomembrane formation
EDUCATIONAL CASES E1 & E2 Natasha Inglis 20/03/15 CASE E1 79 year old female Rectum. Altemeier operation Histology Superficial erosions and mucosal congestion volcano lesion and pseudomembrane formation
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Eight Groups are Revised for 2018 Head & Neck Colon (includes rectosigmoid and rectum for cases diagnosed 1/1/2018 forward) Lung (2018 Draft not yet
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Eight Groups are Revised for 2018 Head & Neck Colon (includes rectosigmoid and rectum for cases diagnosed 1/1/2018 forward) Lung (2018 Draft not yet
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches
 Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
My Journey into the World of Salivary Gland Sebaceous Neoplasms
 My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
Educational Cases EQA November T.J. Palmer Raigmore Hospital Inverness
 Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
Development of the Pharyngeal Arches
 Development of the Pharyngeal Arches Thomas A. Marino, Ph.D. Temple University School of Medicine Competencies: Upon completion of this section of the course, the student must be able to: 1. Recall the
Development of the Pharyngeal Arches Thomas A. Marino, Ph.D. Temple University School of Medicine Competencies: Upon completion of this section of the course, the student must be able to: 1. Recall the
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Keratinizing Dysplasia and Select Variants of Head & Neck Squamous Cell Carcinoma
 Keratinizing Dysplasia and Select Variants of Head & Neck Squamous Cell Carcinoma Napa Valley Pathology Conference Silverado Resort & Spa May 18, 2018 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL
Keratinizing Dysplasia and Select Variants of Head & Neck Squamous Cell Carcinoma Napa Valley Pathology Conference Silverado Resort & Spa May 18, 2018 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL
ATLAS OF HEAD AND NECK PATHOLOGY METAPLASIA
 Metaplasia is the conversion of one adult differentiated cell type to another. Generally it is the result of persistent cellular trauma and serves as a protective mechanism. Thus anteriorly along the nasal
Metaplasia is the conversion of one adult differentiated cell type to another. Generally it is the result of persistent cellular trauma and serves as a protective mechanism. Thus anteriorly along the nasal
Disclosure of Relevant Financial Relationships
 Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
Ben Witt, MD University of Utah/ARUP Laboratories Assistant Professor of Anatomic Pathology
 Ben Witt, MD University of Utah/ARUP Laboratories Assistant Professor of Anatomic Pathology Review some of the more common cytodiagnoses of the Head and Neck Establish an approach to some of the diagnostic
Ben Witt, MD University of Utah/ARUP Laboratories Assistant Professor of Anatomic Pathology Review some of the more common cytodiagnoses of the Head and Neck Establish an approach to some of the diagnostic
- Selected Tumors of the Skin Appendages - Primary vs. Metastasis
 - Selected Tumors of the Skin Appendages - Primary vs. Metastasis Napa Valley 2018 Victor G. Prieto, MD, PhD Chair of Pathology UT MD Anderson Cancer Center vprieto@mdanderson.org Napa Valley in May Introduction
- Selected Tumors of the Skin Appendages - Primary vs. Metastasis Napa Valley 2018 Victor G. Prieto, MD, PhD Chair of Pathology UT MD Anderson Cancer Center vprieto@mdanderson.org Napa Valley in May Introduction
FINALIZED SEER SINQ QUESTIONS
 0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
Cystic carcinoma of the neck
 Case Report Brunei Int Med J. 2010; 6 (1): 56-60 Cystic carcinoma of the neck Prathibha Parampalli SUBRHAMANYA, Ghazala KAFEEL, Hla OO, Pemasiri Upali TELISINGHE, Department of Pathology, RIPAS Hospital,
Case Report Brunei Int Med J. 2010; 6 (1): 56-60 Cystic carcinoma of the neck Prathibha Parampalli SUBRHAMANYA, Ghazala KAFEEL, Hla OO, Pemasiri Upali TELISINGHE, Department of Pathology, RIPAS Hospital,
3/28/2017. Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center
 Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial
Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Human Papillomavirus Testing in Head and Neck Carcinomas
 Human Papillomavirus Testing in Head and Neck Carcinomas Guideline from the College of American Pathologists Early Online Release Publication: Archives of Pathology & Laboratory Medicine 12/18/2017 Overview
Human Papillomavirus Testing in Head and Neck Carcinomas Guideline from the College of American Pathologists Early Online Release Publication: Archives of Pathology & Laboratory Medicine 12/18/2017 Overview
Case 2. Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset
 Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Sinonasal Tumors. Objectives. Objectives. Incidence of Paranasal Sinus Tumors. Demographics of Paranasal Sinus Tumors. Paranasal Sinus Tumors
 Sinonasal Tumors Objectives Incidence and demographics of sinonasal tumors Separating tumors from inflammatory changes Common and notable histologic types of sinonasal tumors Staging of sinonasal tumors
Sinonasal Tumors Objectives Incidence and demographics of sinonasal tumors Separating tumors from inflammatory changes Common and notable histologic types of sinonasal tumors Staging of sinonasal tumors
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
NEOPLASIA-I CANCER. Nam Deuk Kim, Ph.D.
 NEOPLASIA-I CANCER Nam Deuk Kim, Ph.D. 1 2 Tumor in the hieroglyphics of the Edwin Smith papyrus (1,600 B.C., Breasted s translation 1930) 3 War on Cancer (National Cancer Act, 1971) 4 Cancer Acts in Korea
NEOPLASIA-I CANCER Nam Deuk Kim, Ph.D. 1 2 Tumor in the hieroglyphics of the Edwin Smith papyrus (1,600 B.C., Breasted s translation 1930) 3 War on Cancer (National Cancer Act, 1971) 4 Cancer Acts in Korea
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Congenital Neck Masses C. Stefan Kénel-Pierre, MD
 Congenital Neck Masses C. Stefan Kénel-Pierre, MD SUNY-LICH Medical Center Department of Surgery Case Presentation xx year old male presents with sudden onset left lower neck swelling x 1 week Denies pain,
Congenital Neck Masses C. Stefan Kénel-Pierre, MD SUNY-LICH Medical Center Department of Surgery Case Presentation xx year old male presents with sudden onset left lower neck swelling x 1 week Denies pain,
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
04/13/2017. Sinonasal Pathology. Sinonasal Tract Pathology Outline. 24 th Annual Seminar in Pathology Pittsburgh, PA April 27, 2017
 Sinonasal Pathology 24 th Annual Seminar in Pathology Pittsburgh, PA April 27, 2017 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL Sinonasal Tract Pathology Outline Sinonasal (Schneiderian) papillomas
Sinonasal Pathology 24 th Annual Seminar in Pathology Pittsburgh, PA April 27, 2017 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL Sinonasal Tract Pathology Outline Sinonasal (Schneiderian) papillomas
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu
 Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS. Dr. Pamela Hanson DO PGY3
 PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Zubair W. Baloch, MD, PhD: Consultant for Veracyyte, INC Tarik M. Elsheikh, MD: Nothing to disclose
 Cytology Works shop #8 Zubair W. Baloch, MD, PhD: Consultantt for Veracyte, INC Tarik M. Elsheik kh, MD: Nothing to disclose Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair
Cytology Works shop #8 Zubair W. Baloch, MD, PhD: Consultantt for Veracyte, INC Tarik M. Elsheik kh, MD: Nothing to disclose Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
The many faces of extranodal lymphoma
 The many faces of extranodal lymphoma Frank Pameijer Departments of Radiology and Radiation Oncology University Medical Center Utrecht Special thanks to Ilona M Schmalfuss, MD University of Florida Gainesville,
The many faces of extranodal lymphoma Frank Pameijer Departments of Radiology and Radiation Oncology University Medical Center Utrecht Special thanks to Ilona M Schmalfuss, MD University of Florida Gainesville,
HEAD AND NECK PATHOLOGY
 Bosnian-British School of Pathology November 2012 HEAD AND NECK PATHOLOGY Slide seminar: Oral Pathology Preferred Diagnoses Dr A Sandison, Slide seminar: Pathology of the Oral Cavity Page 1 of 5 1. Female
Bosnian-British School of Pathology November 2012 HEAD AND NECK PATHOLOGY Slide seminar: Oral Pathology Preferred Diagnoses Dr A Sandison, Slide seminar: Pathology of the Oral Cavity Page 1 of 5 1. Female
Rare Presentation Of Adenoidcystic Carcinoma Of External Auditory Canal With Subcutaneous Metastasis In Temporal Region
 ISPUB.COM The Internet Journal of Otorhinolaryngology Volume 13 Number 2 Rare Presentation Of Adenoidcystic Carcinoma Of External Auditory Canal With Subcutaneous Metastasis In Temporal Region S Kaushik,
ISPUB.COM The Internet Journal of Otorhinolaryngology Volume 13 Number 2 Rare Presentation Of Adenoidcystic Carcinoma Of External Auditory Canal With Subcutaneous Metastasis In Temporal Region S Kaushik,
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosures. The Thin Red Line Between Neuropathology and Head & Neck Pathology. Introduction CASE 1. Current Issues Tihan
 Disclosures I have nothing to disclose The Thin Red Line Between Neuropathology and Head & Neck Pathology Tarik Tihan, MD, PhD UCSF, Department of Pathology Neuropathology Division Introduction Three cases
Disclosures I have nothing to disclose The Thin Red Line Between Neuropathology and Head & Neck Pathology Tarik Tihan, MD, PhD UCSF, Department of Pathology Neuropathology Division Introduction Three cases
 Drawings illustrating the human pharyngeal apparatus. Drawings illustrating the human pharyngeal apparatus. Drawings illustrating the human pharyngeal apparatus. Drawings illustrating the human pharyngeal
Drawings illustrating the human pharyngeal apparatus. Drawings illustrating the human pharyngeal apparatus. Drawings illustrating the human pharyngeal apparatus. Drawings illustrating the human pharyngeal
HPV and Head and Neck Cancer: What it means for you and your patients
 HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
My personal experience at University of Toronto and recent updates of
 My personal experience at University of Toronto and recent updates of Endocrine Pathology Toshitetsu Hayashi M.D. Ph.D. ¹Department of Diagnostic Pathology, Takamatsu Red Cross Hospital, Japan ²Laboratory
My personal experience at University of Toronto and recent updates of Endocrine Pathology Toshitetsu Hayashi M.D. Ph.D. ¹Department of Diagnostic Pathology, Takamatsu Red Cross Hospital, Japan ²Laboratory
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Scotland and Northern Ireland EQA Scheme. Circulation 46
 Scotland and Northern Ireland EQA Scheme Circulation 46 Special Educational Cases E1 and E2 Presented by Dr K Robertson Case E1 Female 42 year old with heavy menstrual and intermenstrual bleeding. IUS
Scotland and Northern Ireland EQA Scheme Circulation 46 Special Educational Cases E1 and E2 Presented by Dr K Robertson Case E1 Female 42 year old with heavy menstrual and intermenstrual bleeding. IUS
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Low-Grade Papillary Schneiderian Carcinoma: A Case Report
 DOI 10.1007/s12105-017-0832-z CASE REPORT Low-Grade Papillary Schneiderian Carcinoma: A Case Report Hui Jeong Jeong 1 Jin Roh 1 Bong Jae Lee 2 Kyung Ja Cho 1 Received: 13 March 2017 / Accepted: 13 June
DOI 10.1007/s12105-017-0832-z CASE REPORT Low-Grade Papillary Schneiderian Carcinoma: A Case Report Hui Jeong Jeong 1 Jin Roh 1 Bong Jae Lee 2 Kyung Ja Cho 1 Received: 13 March 2017 / Accepted: 13 June
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD
 PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD Topics 1. Cervical lymphadenopathy 2. Lymphatic malformation 3. Thyroglossal duct cysts 4. Branchial cleft cysts 5. Thyroid masses CASE 1 Case 1 A 2
PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD Topics 1. Cervical lymphadenopathy 2. Lymphatic malformation 3. Thyroglossal duct cysts 4. Branchial cleft cysts 5. Thyroid masses CASE 1 Case 1 A 2
Pharyngeal Apparatus. Pouches Endoderm Grooves Ectoderm Arch Neural Crest Somitomeres Aortic Arch - Vessel
 Pharyngeal Apparatus Pouches Endoderm Grooves Ectoderm Arch Neural Crest Somitomeres Aortic Arch - Vessel Segmental Organization Humans: Arch 1-4 prominent Arch 5 absent Arch 6 - transient First Arch Face
Pharyngeal Apparatus Pouches Endoderm Grooves Ectoderm Arch Neural Crest Somitomeres Aortic Arch - Vessel Segmental Organization Humans: Arch 1-4 prominent Arch 5 absent Arch 6 - transient First Arch Face
Diagnostic Cytology of Cancer Cases
 Diagnostic Cytology of Cancer Cases Somporn Techangamsuwan Companion Animal Cancer Research Unit (CAC-RU) Department of Pathology, Faculty of Veterinary Science, Chulalongkorn University 1 Tumor or Non-tumor
Diagnostic Cytology of Cancer Cases Somporn Techangamsuwan Companion Animal Cancer Research Unit (CAC-RU) Department of Pathology, Faculty of Veterinary Science, Chulalongkorn University 1 Tumor or Non-tumor
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a Pseudocapsule
 GENITOURINARY PATHOLOGY Kathleen M. O Toole, M.D. Renal Cell Carcinoma 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow Necrotic Mass Grossly is a Bright
GENITOURINARY PATHOLOGY Kathleen M. O Toole, M.D. Renal Cell Carcinoma 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow Necrotic Mass Grossly is a Bright
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Dr Nick McIvor. Dr John Chaplin. Head & Neck Surgeon Auckland City Hospital Auckland. Auckland Head & Neck Surgeon Gillies Hospital Auckland
 Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Founders Seminar. Handout material. Challenging Cases in Head and Neck Surgical Pathology
 Founders Seminar Handout material Challenging Cases in Head and Neck Surgical Pathology Robert A. Robinson Department of Pathology University of Iowa American Academy of Oral and Maxillofacial Pathology
Founders Seminar Handout material Challenging Cases in Head and Neck Surgical Pathology Robert A. Robinson Department of Pathology University of Iowa American Academy of Oral and Maxillofacial Pathology
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2: