Stereotactic Radiosurgery/Radiotherapy. What is Stereotaxis? Available Systems. Almon S. Shiu, Ph.D
|
|
|
- Caitlin Wilkinson
- 6 years ago
- Views:
Transcription

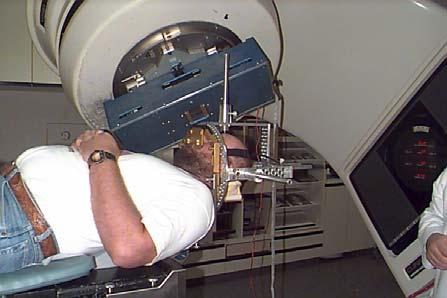
1 Stereotactic Radiosurgery/Radiotherapy Almon S. Shiu, Ph.D Radiation Physics Department University of Texas M. D. Anderson Cancer Center Houston, Texas What is Stereotaxis? A Method for locating points within the brain using an external, three- dimensional frame of reference, usually based on the Cartesian coordinate system Available Systems Gamma Knife Tyco/Radionics XKnife-RT/Xplan BrainLab CyberKnife Proton Facilities Others 1
 - ellipsoid or spherical dose distributions 11-15 15 fields shaped with mmlc or dynamic arcs - arbitrary dose distributions (conformal) 1 to 2 proton fields Indications Benign tumors")
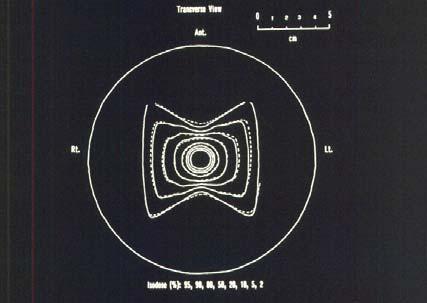
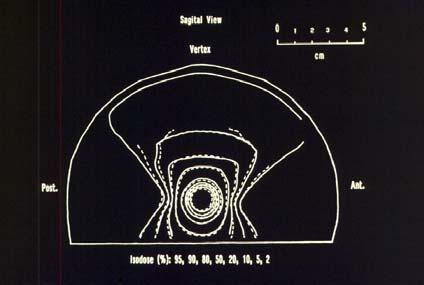
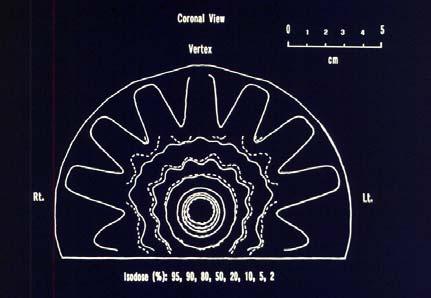
2 Delivery Techniques 201 (192) intersecting beams (Gamma Knife) - Spherical dose distributions Multiple arcs with circular collimators (0.5 cm to 4.0 cm cone) - ellipsoid or spherical dose distributions fields shaped with mmlc or dynamic arcs - arbitrary dose distributions (conformal) 1 to 2 proton fields Indications Benign tumors (acoustic neuroma.) AVMs Mets Boosts Salvage (e.g., recurrence after surgery and/or whole brain radiation) What is Linac-Based SRS? Linac-Based SRS delivers a narrowly collimated x-ray x beam while the gantry rotates around the target. Target is positioned at the center of gantry rotation. 2
 and spare the surrounding tissues.")

3 What is Linac-Based SRS? Process is repeated for a number of treatment couch angles. Target is caught in a cross fire of x-rayx beams, Which delivers a lethal dose to the target (red) and spare the surrounding tissues. Benefits Large dose to small (1-4 4 cm diameter) lesion with minimum dose to surrounding tissue. Single fraction - good for out-of of-town patients, patients in poor health, or other patients who might be burdened by six weeks of treatment. Prescription for SRS RTOG recommendations: 24 Gy for cones 1-2 cm 18 Gy for cones cm 15 Gy for cones cm Modify depending on disease radiosensitivity, prognosis, and other factors. 3
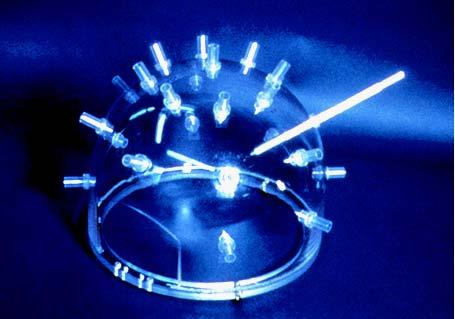
 201 60 CO sources Perfexion 192 60 CO sources Model: B, U, C, and Perfexion The first prototype of")

4 Development of the Leksell Gamma Knife SRS was first introduced by Leksell in 1951 The first gamma knife: in the late 1960s The second unit: in Initially CO sources; Currently (Model C) CO sources Perfexion CO sources Model: B, U, C, and Perfexion The first prototype of Leksell Gamma Knife was installed in Stockholm, Sweden, 1968 Model U 1994 Model C 2000 New Features with Leksell Gamma Knife C Designed for: Ease-of of-use Operator console Automatic Positioning System Color coded collimator s Safety Speed Selectivity Enhancements Leksell GammaPlan Hand control Integrated helmet changer 4

5 Advantages of Model C Link between computer planning and treatment unit. Coordinates are set by the computer preventing human error Collimator helmet is checked by the computer and treatment is not allowed unless the correct collimator is in place. Advantages of Model C Treatment time is set by the software and can not be changed by operator A completed treatment with detailed information is stored in a read only file for future reference Leksell Gamma Knife PERFEXION 5






6 Leksell Gamma Knife Treatable volume Leksell Gamma Knife C Leksell Gamma Knife PERFEXION 4-,, 8-, 8, and 16-mm Leksell Gamma Knife Focus access Leksell Gamma Knife C Leksell Gamma Knife PERFEXION Dynamic shaping 6


7 Radiation protection Body doses up to 100 times less than from alternative technology Leakage levels low enough to allow for a window into the operating room Room design can be optimized to space and cost What is Linac-Based SRT? Conventional fractionated treatment with non- invasive, reproducible stereotactic frame. Prescription for SRT MDACC recommendation: 30 Gy in 5 fractions, 6 Gy/fraction Modify depending on previous treatment history, dose tolerance of critical structures, and other factors. 7
 Basic")

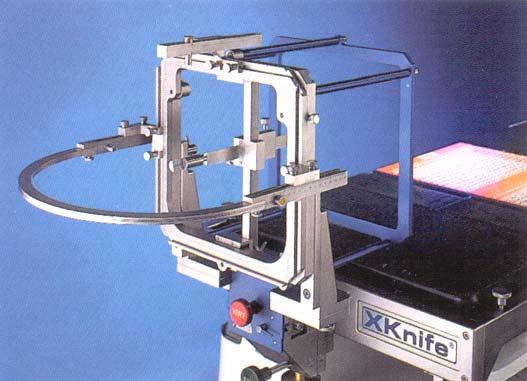
8 Stereotactic Instrumentation (In-House) Stereotactic Instrumentation (Integra/Radionics) Basic Requirements For SRS Mechanical precision Accurate localization Accurate and optimal dose calculation Patient safety 8
.")
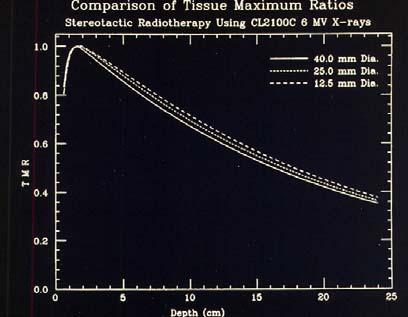
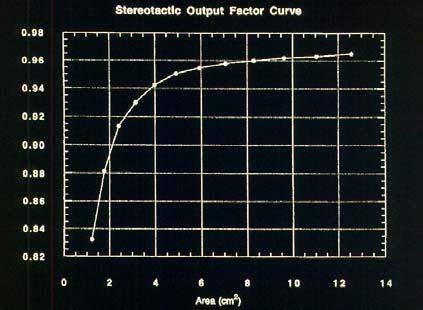
9 Mechanical Precision Linac gantry, collimator and couch Lasers Patient docking device Frame system Target verification device SRS system verification test Dose Measurements Use AAPM TG-51 protocol Output, Central-axis axis %DD and TMR measurement - using PTW 0.1 c.c. Chamber or Scanditronix diode (For diameter 10 mm). Beam Profile - using film or stereotactic diode. 9

10 10
11 Dose Verification 11

12 12




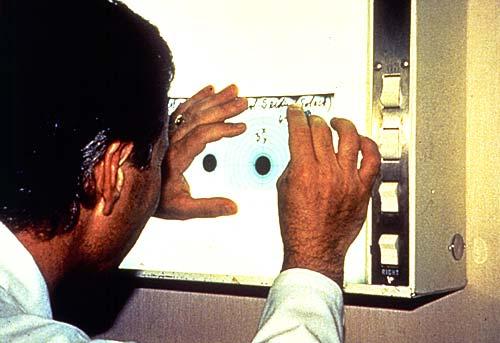
13 Quality Assurance for ImageFusion Measuring MRI Distortion with a Phantom Head During installation of the imagefusion system, a specially designed Geometric Phantom will be used to measure the spatial distortions inherent in the MRI scanner. These distortions will give an idea as to the magnitude of the errors to be expected. When scanning patients, use the same protocol that was used for the phantom, including slice spacing, slice thickness, field of view. Use the phantom to test distortion on a periodic basis, particularly after a scanner system or software upgrade. Spatial localization QA phantom 13
14 center of sphere AP LAT VERT D dist Fusion-CT Fusion-absolute CT-absolute tip of cone AP LAT VERT D dist Fusion-CT Fusion-absolute CT-absolute superior/anterior/left corner of cube AP LAT VERT D dist Fusion-CT Fusion-absolute CT-absolute



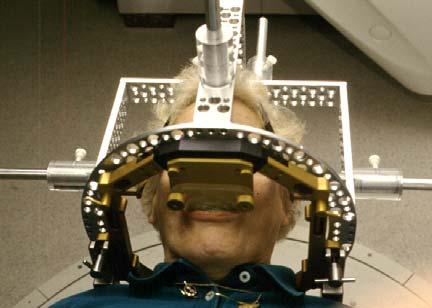
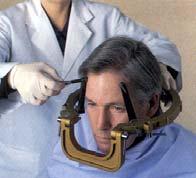
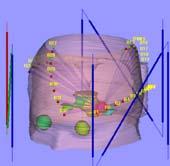
15 SRS Procedure Frame Fixation Imaging Scanning Auto Detecting Rods 15


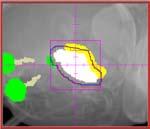
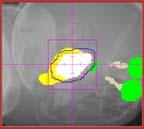
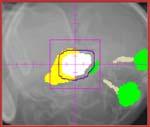
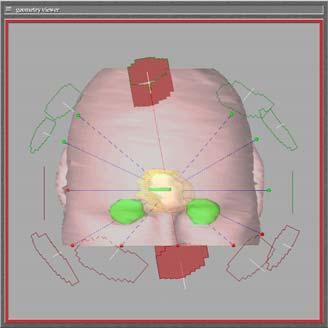
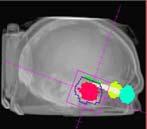
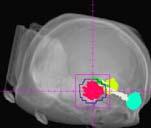
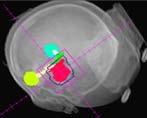
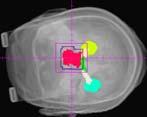
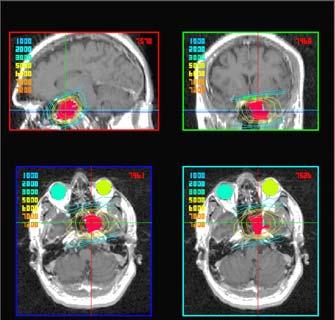
16 RT Frontal Metastasis RT Temporal Metastasis LT Temporal Metastasis 16





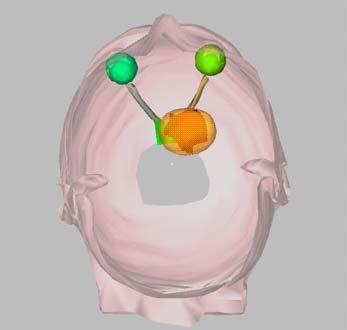
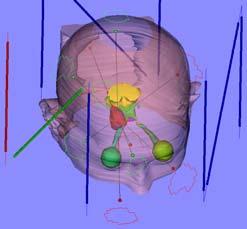
17 LT Temporal RT Temporal Auto Plan RT Frontal 3D Display LT Temporal RT Temporal Conformal ARCS RT Frontal 17
18 18


19 MU Calculation (for Arc) isocenter Ψ = S.F. * TMR where S.F. = Scatter factor Then, MU = D * w/ Ψ where D = isocenter w = beam weight arc length Pre-treatment QA 19

20 20



21 Setup Patient for Treatment Treatment Delivery 21


22 Treatment Typically 5 arcs, about each 300 MU/min 1 2 min per arc Total treatment is 5 to 10 min of beam on time. Room entries between arcs to move couch and re-check patient alignment. 22
 Projected Leaf Width: 4.")
 Collimator to Isocenter Distance: ~ 37.")
23 Computer-Controlled Controlled Miniature Multileaf Collimator (mmlc) TYCO/RADIONICS Maximum Field Size: 13.5 cm x 11.3 isocenter Number of Leaves: 31 leaf pairs (62 leaves) Projected Leaf Width: cm SAD Each Leaf Travel (@ isocenter): -55 cm to 5 cm Leaf Transmit Time Rate: ~ 30 mm/sec Leaf Material: Tungsten Alloy (7 cm thick) Collimator to Isocenter Distance: ~ 37.5 cm Interleaf Transmission SF 6 Gantry 23


24 % leakage (norm to 10x10) mmlc inplane leakage 1.6 Leaf Leaf off-axis Position (cm) Leaf repositioning test mmlc Leaf Positioning The reproducibility of each leaf is 0.2 mm± 0.07mm. Uncertainty for the multiple scans on each set of leaf positioning tests is within 0.1 mm. 24



25 Novalis Hardware Components a-si Flatpanel a-si Flatpanel X-ray source X-ray source Clinical Applications SRS and SRT for intracranial tumors and metastases SRT for head and neck lesions SRT for the small tumors in the thorax and abdomen 25

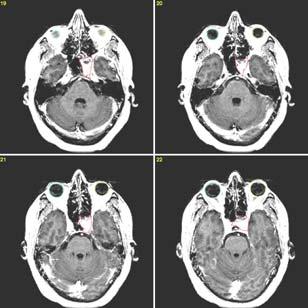
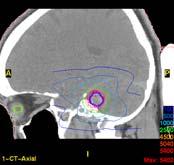
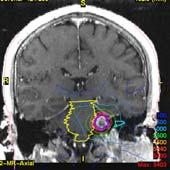
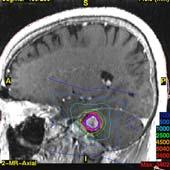
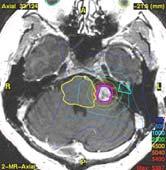
26 Case Presentation Primary Site and Histopathology: Recurrent posterior fossa ependymoma Stage: Recurrent History: A 40-year year-old gentleman who was initially see in 1972 at the age of 15. He underwent a resection of his posterior fossa ependymoma and was treated with 36 fractions of external beam radiation therapy. He was without disease recurrence until 1998 when he noticed the onset of left facial paresis. History (continued): He had a repeat surgical resection at MDACC and the tumor was removed in the pontine and prepontine areas. Approximately two years later, regrowth was identified in 1993, and the patient underwent chemotherapy treatment over 12-month time and since that time slow progression of tumor has been noted. In early 1998, he had the onset of occipital pain and also also decreased function in the left hand. 26

27 History (continued): Although his tumor was relatively indolent but it had been increasing since Surgery and stereotactic radiotherapy (SRT) were presented to the patient at that time. Patient underwent serious injuries with his two previous surgeries and has expressed his desire for SRT. MRI Finding: an MRI of the brain with & without contrast on 4/28/98, it showed a large nodular enhancing tumor in the prepontine cistern and the cerebral pontine angle predominantly on the left side. Basic Treatment Plan: The recurrent tumor was treated to a total dose of 25 Gy in 5 fraction (twice per week). The dose was prescribed at the 90 th percentile. 27

28 28

29 29
30 30
 History: A 47-year year-old gentleman who had a history of T2, N1 carcinoma of the nasopharynx.")

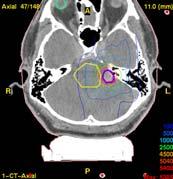
31 Case Presentation Primary Site and Histopathology: Carcinoma of the nasopharynx Stage: Recurrent (a recurrent mass filling the sphenoid sinus mostly on the left with possible invasion into left cavernous sinus.) History: A 47-year year-old gentleman who had a history of T2, N1 carcinoma of the nasopharynx. Previous Treatment: (1997) Radiotherapy - 70 Gy/35 fractions Chemoradiotherapy - cis-platimum and 5-FU5 Risk of Radiation Therapy: Significant risk of left optic neuropathy and the optic chiasm has a low probability but real risk for neuropathy. Basic Treatment Plan: Treated with salvage radiotherapy to a dose of 70 Gy in 35 fractions. 31
32 32
33 33

34 34


35 35
36 36

37 Meningioma Diagnosis: Meningioma of the right cavernous sinus Stage: Locally recurrent History: A male patient is now 12 years out from a previous surgery for a right cavernous sinus hemangioma.. Serial evaluation by MRI for this process has revealed a slight interval growth in residual disease within this region in comparison to MRI that was performed in Although he remains asymtomatic, he will receive a course of definitive radiation in this setting to prevent further growth which could conceivably result in neurologic compromise. 37



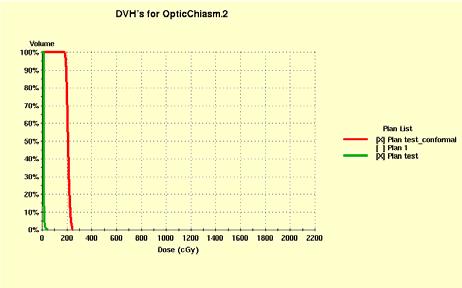
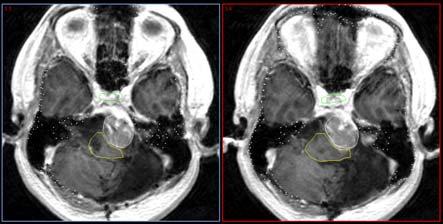
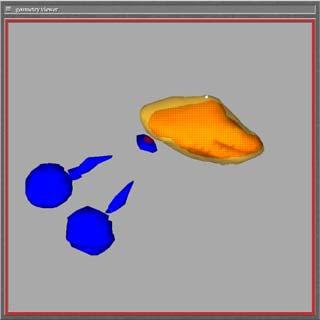
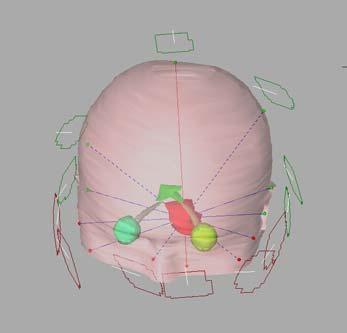
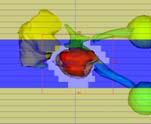
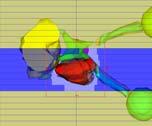
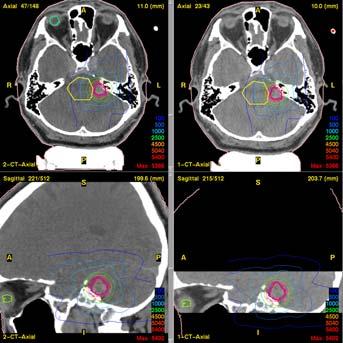
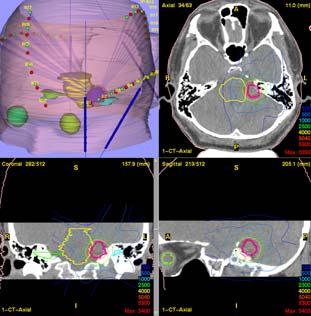
38 Case (Continued) Basic Radiation Treatment Plan: The plan at this time will be to treat the area of recurrent meningoma within the right cavernous sinus. We will likely utilize stereotactic SRT to treat this region to a dose of 50 Gy in 25 fractions, precise aiming the lesion and sparing the optic nerves and optic chiasm. Fused Images GTV and Critical Structures on MRT Images 38

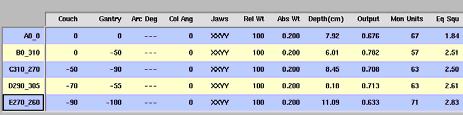


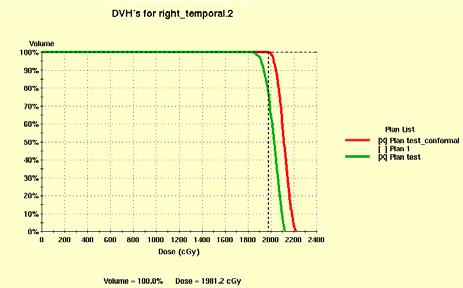
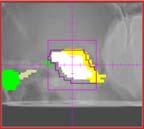
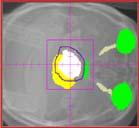
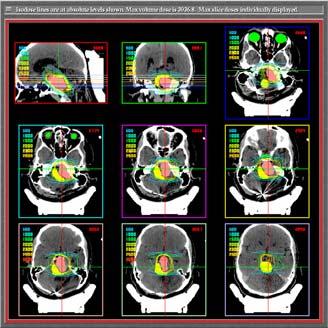
39 GTV and Critical Structures on CT Images A0_0 B0_310 C110_270 D290_305 E270_260 39

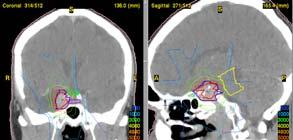
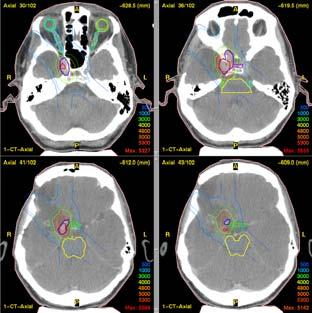
40 Central Axes Plan Isodose distributions Isodose Distributions DVH 40

41 Heaven meet Earth Image-Guided Non-Invasive SRS/SRT Almon Shiu, Ph.D. Radiation Physics Department UTMDACC Houston, TX Objective Develop a non-invasive intracranial stereotactic radiosurgery technique with the same high degree of accuracy as that of the current invasive head-ring SRS Technique. 41




42 42


43 Planning CT Planning MRI 43



44 Daily 44

45 45

46 /8/2006 3/8/ /1/2006 3/1/ /21/2006 2/21/ /13/2006 2/13/ /3/2006 2/3/ /2/2006 2/2/ /1/2006 2/1/ /31/2006 1/31/ /30/2006 1/30/ /27/2006 (planning) 1/27/2006 (planning) VERT(mm) VERT(mm) LAT (mm) LAT (mm) AP (mm) AP (mm) Date Date STD STD mean mean-ref Ref Ref Ref STD STD mean mean - Planning Planning mean mean /27/2006 (planning) 1/27/2006 (planning) VERT(mm) VERT(mm) LAT (mm) LAT (mm) AP (mm) AP (mm) Date Date




47 AP RT LAT Planned DRR Portal Conclusions The The image-guided guided non-invasive stereotactic radiosurgery has the capability of delivering high level accuracy of dose to the lesion without the pain and discomfort due to the pins fixed to the patient s s skull. Revise Revise the fractionated SRT procedures by using image registration for the initial five treatments. Based on the variations of the isocenter, use the Ref isocenter for the remaining SRT treatments without performing the image registration process daily. Thank you 47
 Almon Sh")
48 Image-Guided Stereotactic Body Radiotherapy (Featuring a 6D Robotic Couch-Top ) Almon S. Shiu, Ph.D. Radiation Physics Department The University of Texas M.D. Anderson Cancer Ctr. Houston, Texas Research Team (2002) Almon Shiu, Ph.D. Eric Chang, M.D. Jin-Song Ye, M.S. Jim Lii, M.S. Introduction Spinal Spinal metastases are a common component of metastatic disease afflicting 40% of all cancer patients which can cause severe pain, and neurologic sequelae Conventional radiation therapy widely used but is inherently limited by spinal cord tolerance leaving little possibility for re-irradiation in case of recurrence Stereotactic body radiotherapy (SBRT) is an emerging technology designed to precisely deliver higher doses, improve tumor control, and permit re- irradiation of the spine 48
49 Introduction Research workshop on 4/3/02 to propose the development of image-guided guided stereotactic body radiotherapy Phase I development finished in August, Ongoing ID Clinical Trial Nov 2002 SBRT first introduced to MDACC through Phase I/II clinical trial for patients with spinal or paraspinal metastases as a joint collaboration between Radiation Oncology, Neurosurgery, and Radiation Physics Primary objective to establish safety, feasibility, and efficacy using CT-on on-rails based SBRT to treat spinal and paraspinal metastases Patient population Protocol intended for patients with spinal metastases occurring in a variety of situations felt to be candidates after discussion in multi- disciplinary tumor board GENERAL INDICATIONS PRIMARY - Newly diagnosed solitary or oligo- spinal metastases. Radioresistant subtypes POST-OP OP adjuvant or elective treatment SALVAGE - surgical or RT recurrences 49





.")
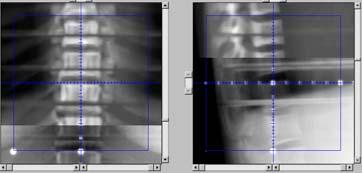
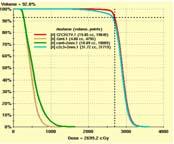
50 LINAC/CT-on on-rails Image-guided guided Stereotactic Body Radiotherapy Immobilization: Tyco/Radionics Body System consisting of a carbon base plate, vacuum cushions, a vacuum system and Fixation sheets. A A Varian ExactCT targeting system A GE CT scanner and a Varian Clinic 21 EX LINAC, shared the same couch between CT and LINAC. Treatment planning IMRT Linkage between patient anatomy and stereotactic body frame and update daily isocenter based on 3D image fusion. A. Shiu, et al. IJROBP 57(3): ,2003 Spinal IMRT Radiotherapy Treating Planning Prescription: 30 Gy/5 TX, 27 Gy/3 TX, or 18 Gy to 26 Gy/1 TX Beam Arrangement: 6- and 18-MV Photons 280º Axial and sagittal views of isodose distributions normalized to GTV mean dose Typical prescribed dose to the volume included by the 90% isodose line The ultimate prescription dose was constrained by our IRB requirement for protocol approval that the dose to the spinal cord could not exceed a total of 10 Gy over five Tx (9 Gy over three Tx,, 8 Gy over 1 Tx ). Dose volume histogram - another way to evaluate the treatment plan Normalized Volume Isodose Distribution Dose Volume Histogram RT Kidney LT Kidney Cord Cord+2mm Dose (cgy) L1 (CTV) 50


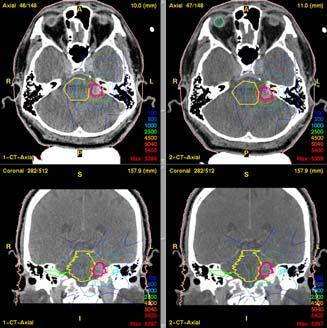
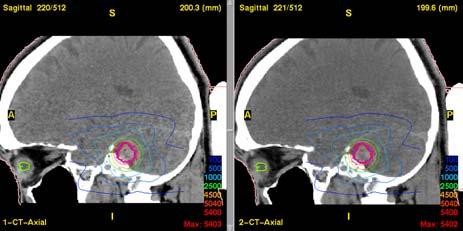
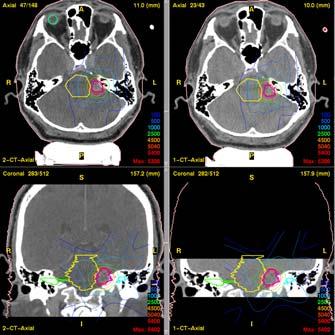
51 IGSBRT Treatment Process Flow Chart Planning CT Scan With Frame Plan Iso On Frame Plan DRRs Daily CT Scan Anatomy Image Registration Daily Iso Daily DRRs Frame Registration DRR Registration Patient Positioning DRR & Portal Registration Portal Images Treatment Daily Treatment Setup Image-guided guided stereotactic Target alignment CT imaging prior treatment Fuse Fuse the planning images with the current CT images to calculate the shift and the rotation from the planning isocenter to the daily isocenter Automatic On-Line Image Registration Based on Mutual Information Automation of Image Registration And Verification for Image-Guided Stereotactic Body Radiotherapy 51






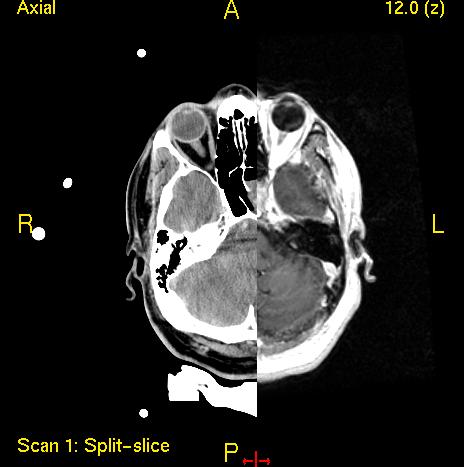
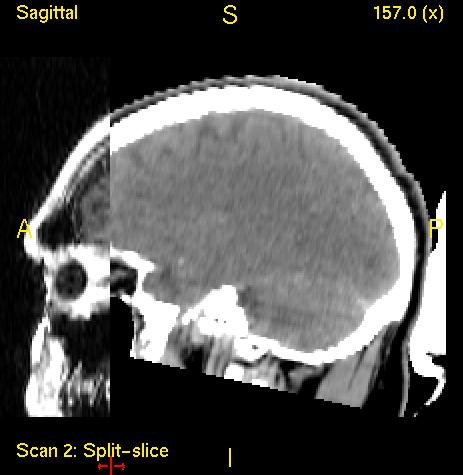
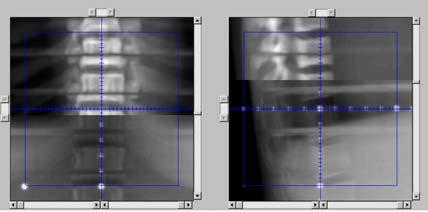
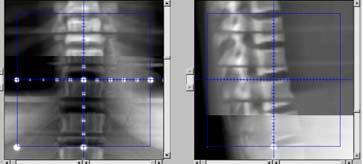
52 DRR Comparison Convention method: side-by by-side comparison DRR Comparison Split Screen By displaying two corresponding DRRs in one frame in a split screen format, sub- millimeter shifts can be readily detected. Daily Treatment Setup Image-guided guided stereotactic alignment Apply the shift from the planning isoccenter and align the updated isocenter with lasers RT ANT LT 52








53 Deviation (mm) Daily Frame Center Deviated from Ref CT Frame Center Number of Daily CT LAT AP SI HexaPOD Robotically Controlled 6D Couch Top Daily Treatment Setup Image-guided guided stereotactic alignment Verify the target isocenter coincided with the LINAC radiation isocenter (Portal films) Planning DRR Portal Film AP RT LAT 53




54 Portal EPID Image Registration with DRR Deliver the IMRT treatment Repeat CT scan after treatment to confirm setup accuracy Post-Iso 1/27/03 Planning Iso Post -Iso 2/5/03 54

 10.00 5.")



 5.")

55 Deviation from Planned Isocenter Using Daily Pre-treatment CT Deviation (mm) Treatment Number Assessment of Setup Accuracy Using Immediate Post-Treatment CT LAT AP SI Deviation (mm) Treatment Number LAT AP SI Phantom Study for HexaPOD Setup Accuracy 55

56 Portal Image Verification with DRR 56



 mm 1 0 0 0 0")
 mm 1 0 0 0 0 0 L 3")


57 Positioning Accuracy of Hexapod After the automatic position of Hexapod, additional shifts needed for a perfect alignment (rounded to the nearest mm) Fraction Lat (x) mm AP (Y) mm SI (Z) mm L 3 Case1: 46 M previously irradiated (40 Gy in 16 fxs) Lung cancer T12 metastasis progressed (biopsy proven) July 2004 July





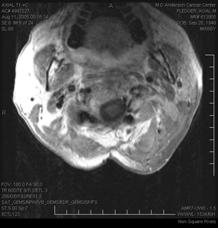
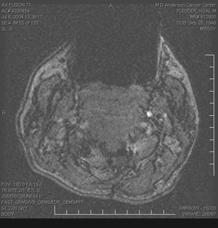
58 Case2: 52 M solitary renal cell carcinoma metastasis centered on cervical vertebrae 2 58
59 Case3: 20 F plasmacytoma causing back pain Extradural extension causing cord compression at T10 Needle bx revealed plasmacytoma 45 Gy in 25 fractions to T9-11 previous irradiated 3 mos later MRI - recurred below: Epidural dz T RT was not an option at the time Laminectomy, facetectomy,, resection tumor 4 mo later recurred above: Rt T7-8 neuroforamen Received stereotactic radiation to epidural disease Attending college and remains disease-free 3 years later Neuroforaminal and Epidural Disease Case4: 48 F breast cancer Feb 03 - Metastasis at T9 previously irradiated at outside institution to 40 Gy/16fx/2.5Gy Feb 04 MR progressive dz at T9, metastasis at posterior elements of T6. Worst pain 5/10 Mar 04-Pre Pre-treatment PET/CT showed T9 SUV 6.2, T6 SUV 14.1 Apr 04 -SBRT 20 Gy/5 fx given to T6 spinous process and T9 vertebra with pain relief 59







60 T6 Spinous Process Sagittal T6 + T9 T9 Vertebral Body Pre/Post treatment MRI Feb 2004 May 2004 F-18 FDG CT-PET T6 SUV14.1 T9 SUV 6.2 T6 SUV3 T9 SUV 0 March 2004 May



61 ACTUARIAL TUMOR CONTROL % 75 Proportion Months Stereotactic Lung Prescription: 50Gy in 5 fractions 61


62 Isocenter Plane, Bone Window Isocenter Plane, Lung Window PTV Display PTV 62

63 7.5mm Inferior, Bone Window 7.5mm Inferior, Lung Window 7.5mm Superior, Bone Window 63

64 7.5mm Superior, Lung Window Conclusions Near-simultaneous CT image-guided guided verification technique can be used as a new platform technology for extra-cranial applications of stereotactic radiotherapy to spine and paraspinal tumors. Treatment is totally non-invasive. The use of SBFS only can not achieve the setup accuracy comparable to that of intracranial SRS. The isocenter setup accuracy of image-guided guided stereotactic spine treatment is within 1 mm and comparable to the setup accuracy of intracranial SRS. Conclusions The 3D navigation guided 6D robotic couch- top demonstrated that it could enhance the isocenter setup accuracy of image-guided guided body radiotherapy and improve the treatment- process efficiency. the automatic repositioning process could remove the possibility of the human errors for updating the target isocenter incorrectly. 64

65 Conclusions Combine with 4-D 4 D CT to generate ITV and PTV, the image-guided guided Radiotherapy technique can be used to treat small lesions, e.g., lung, liver, kidney, etc. Radiation Oncology Eric Chang, M.D. Chester Wang, Ph.D Jim Lii, M.S. Ram Sadogopan MS Narayan Sahoo, Ph.D Anita Mahajan, MD Shiao Woo, M.D. Moshe Maor, MD Haihong Cai, APN Research Barry Brown, Ph.D Leni Mathews, RN Pamela Allen, MPH Acknowledgements M.D. Anderson Medical Oncologists Neurosurgery Laurence Rhines, M.D. Ehud Mendel, M.D. Jeff Weinberg, M.D. Symptom Research Charles Cleeland, Ph.D Shelley Wang, M.D. Ibraham Gning Administration James Cox, MD Ray Sawaya, MD Radhe Mohan, PhD Mike Gillin, PhD Mitch Latinkic Paul Ortiz Charles Washington Thank You 65
Can we hit the target? Can we put the dose where we want it? Quality Assurance in Stereotactic Radiosurgery and Fractionated Stereotactic Radiotherapy
 Quality Assurance in Stereotactic Radiosurgery and Fractionated Stereotactic Radiotherapy David Shepard, Ph.D. Swedish Cancer Institute Seattle, WA Timothy D. Solberg, Ph.D. University of Texas Southwestern
Quality Assurance in Stereotactic Radiosurgery and Fractionated Stereotactic Radiotherapy David Shepard, Ph.D. Swedish Cancer Institute Seattle, WA Timothy D. Solberg, Ph.D. University of Texas Southwestern
Implementing New Technologies for Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy
 Implementing New Technologies for Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Implementation of radiosurgery and SBRT requires a fundamentally sound approach Errors don t blur out
Implementing New Technologies for Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Implementation of radiosurgery and SBRT requires a fundamentally sound approach Errors don t blur out
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR
 Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Stereotactic Radiosurgery. Extracranial Stereotactic Radiosurgery. Linear accelerators. Basic technique. Indications of SRS
 Stereotactic Radiosurgery Extracranial Stereotactic Radiosurgery Annette Quinn, MSN, RN Program Manager, University of Pittsburgh Medical Center Using stereotactic techniques, give a lethal dose of ionizing
Stereotactic Radiosurgery Extracranial Stereotactic Radiosurgery Annette Quinn, MSN, RN Program Manager, University of Pittsburgh Medical Center Using stereotactic techniques, give a lethal dose of ionizing
Radiosurgery by Leksell gamma knife. Josef Novotny, Na Homolce Hospital, Prague
 Radiosurgery by Leksell gamma knife Josef Novotny, Na Homolce Hospital, Prague Radiosurgery - Definition Professor Lars Leksell The tools used by the surgeon must be adapted to the task and where the human
Radiosurgery by Leksell gamma knife Josef Novotny, Na Homolce Hospital, Prague Radiosurgery - Definition Professor Lars Leksell The tools used by the surgeon must be adapted to the task and where the human
Radiosurgery. Most Important! 8/2/2012. Stereotactic Radiosurgery: State of the Art Technology and Implementation Linear Accelerator Radiosurgery
 Therapy SAM Symposium: WE-A-BRCD-1 Stereotactic Radiosurgery: State of the Art Technology and Implementation Linear Accelerator Radiosurgery Kamil M. Yenice, PhD Associate Professor Chief of Clinical Physics
Therapy SAM Symposium: WE-A-BRCD-1 Stereotactic Radiosurgery: State of the Art Technology and Implementation Linear Accelerator Radiosurgery Kamil M. Yenice, PhD Associate Professor Chief of Clinical Physics
Conflict of interest disclosure
 Stereotactic Body Radiation Therapy (SBRT) I: Radiobiology and Clinical Experience Brian Kavanagh, M.D., MPH University of Colorado Eric Chang, M.D. UT MD Anderson Conflict of interest disclosure I have
Stereotactic Body Radiation Therapy (SBRT) I: Radiobiology and Clinical Experience Brian Kavanagh, M.D., MPH University of Colorado Eric Chang, M.D. UT MD Anderson Conflict of interest disclosure I have
Stereotactic Radiosurgery
 27 th ICRO-AROI 2017 Stereotactic Radiosurgery Dr Sajal Kakkar MD, FUICC (USA), FAROI (Fr) Consultant Radiation Oncologist Max Super Speciality Hospital, Mohali SRS Introduction Stereotactic techniques
27 th ICRO-AROI 2017 Stereotactic Radiosurgery Dr Sajal Kakkar MD, FUICC (USA), FAROI (Fr) Consultant Radiation Oncologist Max Super Speciality Hospital, Mohali SRS Introduction Stereotactic techniques
Overview of MLC-based Linac Radiosurgery
 SRT I: Comparison of SRT Techniques 1 Overview of MLC-based Linac Radiosurgery Grace Gwe-Ya Kim, Ph.D. DABR 2 MLC based Linac SRS Better conformity for irregular target Improved dose homogeneity inside
SRT I: Comparison of SRT Techniques 1 Overview of MLC-based Linac Radiosurgery Grace Gwe-Ya Kim, Ph.D. DABR 2 MLC based Linac SRS Better conformity for irregular target Improved dose homogeneity inside
Case Study. Institution Farrer Park Hospital
 Case Study Single isocenter high definition dynamic radiosurgery (HDRS) for multiple brain metastases HDRS with Monaco, Versa HD and HexaPOD allows multiple brain metastases treatment within standard 15-minute
Case Study Single isocenter high definition dynamic radiosurgery (HDRS) for multiple brain metastases HDRS with Monaco, Versa HD and HexaPOD allows multiple brain metastases treatment within standard 15-minute
Advanced Technology Consortium (ATC) Credentialing Procedures for 3D Conformal Therapy Protocols 3D CRT Benchmark*
 Credentialing Procedures for 3D Conformal Therapy Protocols 3D CRT Benchmark*") Advanced Technology Consortium (ATC) Credentialing Procedures for 3D Conformal Therapy Protocols 3D CRT Benchmark* Purpose: To evaluate an institution s 3D treatment planning process and the institution
Advanced Technology Consortium (ATC) Credentialing Procedures for 3D Conformal Therapy Protocols 3D CRT Benchmark* Purpose: To evaluate an institution s 3D treatment planning process and the institution
Stereotaxy. Outlines. Establishing SBRT Program: Physics & Dosimetry. SBRT - Simulation. Body Localizer. Sim. Sim. Sim. Stereotaxy?
 Establishing SBRT Program: Physics & Dosimetry Lu Wang, Ph.D. Radiation Oncology Department Fox Chase Cancer Center Outlines Illustrate the difference between SBRT vs. CRT Introduce the major procedures
Establishing SBRT Program: Physics & Dosimetry Lu Wang, Ph.D. Radiation Oncology Department Fox Chase Cancer Center Outlines Illustrate the difference between SBRT vs. CRT Introduce the major procedures
Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI)
 for Craniospinal Irradiation (CSI)") Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI) Tagreed AL-ALAWI Medical Physicist King Abdullah Medical City- Jeddah Aim 1. Simplify and standardize
Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI) Tagreed AL-ALAWI Medical Physicist King Abdullah Medical City- Jeddah Aim 1. Simplify and standardize
Current Concepts and Trends in Spinal Radiosurgery. Edward M. Marchan
 Current Concepts and Trends in Spinal Radiosurgery Edward M. Marchan Spinal Neoplasia The spine is the most common site of skeletal metastatic disease. (70%) 40% of bony metastases involve the vertebrae
Current Concepts and Trends in Spinal Radiosurgery Edward M. Marchan Spinal Neoplasia The spine is the most common site of skeletal metastatic disease. (70%) 40% of bony metastases involve the vertebrae
Unrivaled, End-to-End
 PHANTOMS Unrivaled, End-to-End Stereotactic QA Industry-leading 0.1mm accuracy minimizes errors at each link in the stereotactic quality assurance chain. Stereotactic radiosurgery (SRS) is governed by
PHANTOMS Unrivaled, End-to-End Stereotactic QA Industry-leading 0.1mm accuracy minimizes errors at each link in the stereotactic quality assurance chain. Stereotactic radiosurgery (SRS) is governed by
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases
 Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
Credentialing for the Use of IGRT in Clinical Trials
 Credentialing for the Use of IGRT in Clinical Trials James M. Galvin, DSc Thomas Jefferson University Hospital Jefferson Medical College Philadelphia, PA and The Radiation Therapy Oncology Group RADIATION
Credentialing for the Use of IGRT in Clinical Trials James M. Galvin, DSc Thomas Jefferson University Hospital Jefferson Medical College Philadelphia, PA and The Radiation Therapy Oncology Group RADIATION
Original Date: April 2016 Page 1 of 7 FOR CMS (MEDICARE) MEMBERS ONLY
 MEMBERS ONLY") National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIATION THERAPY: STEREO RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: Please refer to pages 5-6 LCD
National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIATION THERAPY: STEREO RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: Please refer to pages 5-6 LCD
Lung Spine Phantom. Guidelines for Planning and Irradiating the IROC Spine Phantom. MARCH 2014
 Lung Spine Phantom Guidelines for Planning and Irradiating the IROC Spine Phantom. MARCH 2014 The study groups are requesting that each institution keep the phantom for no more than 2 week. During this
Lung Spine Phantom Guidelines for Planning and Irradiating the IROC Spine Phantom. MARCH 2014 The study groups are requesting that each institution keep the phantom for no more than 2 week. During this
RPC Liver Phantom Highly Conformal Stereotactic Body Radiation Therapy
 RPC Liver Phantom Highly Conformal Stereotactic Body Radiation Therapy Guidelines for Planning and Irradiating the RPC Liver Phantom. Revised Dec 2005 Credentialing for this protocol requires four steps:
RPC Liver Phantom Highly Conformal Stereotactic Body Radiation Therapy Guidelines for Planning and Irradiating the RPC Liver Phantom. Revised Dec 2005 Credentialing for this protocol requires four steps:
IROC Liver Phantom. Guidelines for Planning and Irradiating the IROC Liver Phantom. Revised July 2015
 IROC Liver Phantom Guidelines for Planning and Irradiating the IROC Liver Phantom. Revised July 2015 The study groups are requests that each institution keep the phantom for no more than 2 weeks. During
IROC Liver Phantom Guidelines for Planning and Irradiating the IROC Liver Phantom. Revised July 2015 The study groups are requests that each institution keep the phantom for no more than 2 weeks. During
Disclosures. Overview 8/3/2016. SRS: Cranial and Spine
 SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
In-Room Radiographic Imaging for Localization
 In-Room Radiographic Imaging for Localization Fang-Fang Yin, Zhiheng Wang, Sua Yoo, Devon Godfrey, Q.-R. Jackie Wu Department of Radiation Oncology Duke University Medical Center Durham, North Carolina
In-Room Radiographic Imaging for Localization Fang-Fang Yin, Zhiheng Wang, Sua Yoo, Devon Godfrey, Q.-R. Jackie Wu Department of Radiation Oncology Duke University Medical Center Durham, North Carolina
Helical Tomotherapy Experience. TomoTherapy Whole Brain Head & Neck Prostate Lung Summary. HI-ART TomoTherapy System. HI-ART TomoTherapy System
 The Challenges Associated with Differential Dose Delivery using IMRT Chester Ramsey, Ph.D. Director of Medical Physics Thompson Cancer Center Knoxville, Tennessee, U.S.A Collaborators Chester Ramsey, Ph.D.
The Challenges Associated with Differential Dose Delivery using IMRT Chester Ramsey, Ph.D. Director of Medical Physics Thompson Cancer Center Knoxville, Tennessee, U.S.A Collaborators Chester Ramsey, Ph.D.
Work partially supported by VisionRT
 Work partially supported by VisionRT Background of frameless intracranial stereotactic radiosurgery UCSD SRS/SRT procedure Clinical Results Summary Total prescribed doses : order of 10 50 Gy Planning targets
Work partially supported by VisionRT Background of frameless intracranial stereotactic radiosurgery UCSD SRS/SRT procedure Clinical Results Summary Total prescribed doses : order of 10 50 Gy Planning targets
Chapters from Clinical Oncology
 Chapters from Clinical Oncology Lecture notes University of Szeged Faculty of Medicine Department of Oncotherapy 2012. 1 RADIOTHERAPY Technical aspects Dr. Elemér Szil Introduction There are three possibilities
Chapters from Clinical Oncology Lecture notes University of Szeged Faculty of Medicine Department of Oncotherapy 2012. 1 RADIOTHERAPY Technical aspects Dr. Elemér Szil Introduction There are three possibilities
brain SPINE 2 SRS Matures into breast lung spine LUNG Dr. Robert Timmerman Discusses SBRT for Inoperable Lung Cancer BRAIN
 NEWS AND ADVANCES IN THE MANAGEMENT AND TREATMENT OF SERIOUS DISEASE brain SPINE 2 SRS Matures into Mainstream Extracranial Technique lung spine breast LUNG Dr. Robert Timmerman Discusses SBRT for Inoperable
NEWS AND ADVANCES IN THE MANAGEMENT AND TREATMENT OF SERIOUS DISEASE brain SPINE 2 SRS Matures into Mainstream Extracranial Technique lung spine breast LUNG Dr. Robert Timmerman Discusses SBRT for Inoperable
Implementation of advanced RT Techniques
 Implementation of advanced RT Techniques Tibor Major, PhD National Institute of Oncology Budapest, Hungary 2. Kongres radiološke tehnologije, Vukovar, 23-25. September 2016. Current RT equipments at NIO,
Implementation of advanced RT Techniques Tibor Major, PhD National Institute of Oncology Budapest, Hungary 2. Kongres radiološke tehnologije, Vukovar, 23-25. September 2016. Current RT equipments at NIO,
SRS Plan Quality and Treatment Efficiency: VMAT vs Dynamic Conformal ARCs
 SRS Plan Quality and Treatment Efficiency: VMAT vs Dynamic Conformal ARCs Ahpa Plypoo, MS, CMD, DABR Clinical Medical Physicist, Department of Radiation Oncology Loyola University Health System, Maywood,
SRS Plan Quality and Treatment Efficiency: VMAT vs Dynamic Conformal ARCs Ahpa Plypoo, MS, CMD, DABR Clinical Medical Physicist, Department of Radiation Oncology Loyola University Health System, Maywood,
Additional Questions for Review 2D & 3D
 Additional Questions for Review 2D & 3D 1. For a 4-field box technique, which of the following will deliver the lowest dose to the femoral heads? a. 100 SSD, equal dmax dose to all fields b. 100 SSD, equal
Additional Questions for Review 2D & 3D 1. For a 4-field box technique, which of the following will deliver the lowest dose to the femoral heads? a. 100 SSD, equal dmax dose to all fields b. 100 SSD, equal
CyberKnife Technology in Ablative Radiation Therapy. Jun Yang PhD Cyberknife Center of Philadelphia Drexel University Jan 2017
 CyberKnife Technology in Ablative Radiation Therapy Jun Yang PhD Cyberknife Center of Philadelphia Drexel University Jan 2017 Objectives Components and work flow of CyberKnife Motion management of CyberKnife
CyberKnife Technology in Ablative Radiation Therapy Jun Yang PhD Cyberknife Center of Philadelphia Drexel University Jan 2017 Objectives Components and work flow of CyberKnife Motion management of CyberKnife
In-Room Radiographic Imaging for Localization
 In-Room Radiographic Imaging for Localization Fang-Fang Yin, Zhiheng Wang, Sua Yoo, Devon Godfrey, Q.-R. Jackie Wu Department of Radiation Oncology Duke University Medical Center Durham, North Carolina
In-Room Radiographic Imaging for Localization Fang-Fang Yin, Zhiheng Wang, Sua Yoo, Devon Godfrey, Q.-R. Jackie Wu Department of Radiation Oncology Duke University Medical Center Durham, North Carolina
Quality Assurance in Stereotactic. Radiotherapy. Swedish Cancer Institute Seattle, WA
 Quality Assurance in Stereotactic iosurgery and Fractionated Stereotactic Radiotherapy David Shepard, Ph.D. Swedish Cancer Institute Seattle, WA Timothy D. Solberg, Ph.D. University of Texas Southwestern
Quality Assurance in Stereotactic iosurgery and Fractionated Stereotactic Radiotherapy David Shepard, Ph.D. Swedish Cancer Institute Seattle, WA Timothy D. Solberg, Ph.D. University of Texas Southwestern
WHOLE-BRAIN RADIOTHERAPY WITH SIMULTANEOUS INTEGRATED BOOST TO MULTIPLE BRAIN METASTASES USING VOLUMETRIC MODULATED ARC THERAPY
 doi:10.1016/j.ijrobp.2009.03.029 Int. J. Radiation Oncology Biol. Phys., Vol. 75, No. 1, pp. 253 259, 2009 Copyright Ó 2009 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/09/$ see front
doi:10.1016/j.ijrobp.2009.03.029 Int. J. Radiation Oncology Biol. Phys., Vol. 75, No. 1, pp. 253 259, 2009 Copyright Ó 2009 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/09/$ see front
Clinical Implementation of SRS/SBRT
 Clinical Implementation of SRS/SBRT Anil Sethi, PhD, FAAPM Loyola University Medical Center November 4, 2017 Disclosures Speaker: BrainLAB Standard Imaging Research collaboration: RaySearch 2 Learning
Clinical Implementation of SRS/SBRT Anil Sethi, PhD, FAAPM Loyola University Medical Center November 4, 2017 Disclosures Speaker: BrainLAB Standard Imaging Research collaboration: RaySearch 2 Learning
SBRT fundamentals. Outline 8/2/2012. Stereotactic Body Radiation Therapy Quality Assurance Educational Session
 Stereotactic Body Radiation Therapy Quality Assurance Educational Session J Perks PhD, UC Davis Medical Center, Sacramento CA SBRT fundamentals Extra-cranial treatments Single or small number (2-5) of
Stereotactic Body Radiation Therapy Quality Assurance Educational Session J Perks PhD, UC Davis Medical Center, Sacramento CA SBRT fundamentals Extra-cranial treatments Single or small number (2-5) of
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer
 A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
ph fax
 This product is available through: JRT Associates www.standardimaging.com 800-261-4446. ph 608-831-0025. fax 608-831-2202 5 Nepperhan Avenue, Suite 2B 3120 Deming Way Middleton WIElmsford, 53562-1461 NY
This product is available through: JRT Associates www.standardimaging.com 800-261-4446. ph 608-831-0025. fax 608-831-2202 5 Nepperhan Avenue, Suite 2B 3120 Deming Way Middleton WIElmsford, 53562-1461 NY
A Patient s Guide to SRS
 A Patient s Guide to SRS Stereotactic Radiosurgery 230 Nebraska St. Sioux City, IA 51101 NOTES 230 Nebraska St. Sioux City, IA 51101 Contents page Introduction 1 SRS and how it works 2 The technology involved
A Patient s Guide to SRS Stereotactic Radiosurgery 230 Nebraska St. Sioux City, IA 51101 NOTES 230 Nebraska St. Sioux City, IA 51101 Contents page Introduction 1 SRS and how it works 2 The technology involved
RADIATION ONCOLOGY RESIDENCY PROGRAM Competency Evaluation of Resident
 Resident s Name: RADIATION ONCOLOGY RESIDENCY PROGRAM Competency Evaluation of Resident Rotation: PHYS 703: Clinical Rotation 2 Inclusive dates of rotation: Feb. 26, 2016 Aug. 25, 2016 Director or Associate
Resident s Name: RADIATION ONCOLOGY RESIDENCY PROGRAM Competency Evaluation of Resident Rotation: PHYS 703: Clinical Rotation 2 Inclusive dates of rotation: Feb. 26, 2016 Aug. 25, 2016 Director or Associate
Image Registration for Radiation Therapy Applications: Part 2: In-room Volumetric Imaging
 Image Registration for Radiation Therapy Applications: Part 2: In-room Volumetric Imaging Peter Balter Ph.D University of Texas M.D. Anderson Cancer Center Houston, TX, USA Disclosure Information Peter
Image Registration for Radiation Therapy Applications: Part 2: In-room Volumetric Imaging Peter Balter Ph.D University of Texas M.D. Anderson Cancer Center Houston, TX, USA Disclosure Information Peter
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS
 THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
AbstractID: 8073 Title: Quality Assurance, Planning and Clinical Results for Gamma Knife Radiosurgery S. Goetsch, Ph.D. Page 1 Seattle, WA May 2008
 Knife Radiosurgery S. Goetsch, Ph.D. Page 1 Quality Assurance, Planning and Clinical Results for Gamma Knife Radiosurgery Steven J. Goetsch, Ph.D., FAAPM ACMP 25 th Annual Meeting Seattle, WA May 2008
Knife Radiosurgery S. Goetsch, Ph.D. Page 1 Quality Assurance, Planning and Clinical Results for Gamma Knife Radiosurgery Steven J. Goetsch, Ph.D., FAAPM ACMP 25 th Annual Meeting Seattle, WA May 2008
Page 1. Helical (Spiral) Tomotherapy. UW Helical Tomotherapy Unit. Helical (Spiral) Tomotherapy. MVCT of an Anesthetized Dog with a Sinus Tumor
 Tomotherapy. UW Helical Tomotherapy Unit. Helical (Spiral) Tomotherapy. MVCT of an Anesthetized Dog with a Sinus Tumor") Helical (Spiral) Tomotherapy Novel Clinical Applications of IMRT Linac Ring Gantry CT Detector X-Ray Fan Beam Binary Multileaf Collimator Binary MLC Leaves James S Welsh, MS, MD Department of Human Oncology
Helical (Spiral) Tomotherapy Novel Clinical Applications of IMRT Linac Ring Gantry CT Detector X-Ray Fan Beam Binary Multileaf Collimator Binary MLC Leaves James S Welsh, MS, MD Department of Human Oncology
CURRICULUM OUTLINE FOR TRANSITIONING FROM 2-D RT TO 3-D CRT AND IMRT
 CURRICULUM OUTLINE FOR TRANSITIONING FROM 2-D RT TO 3-D CRT AND IMRT Purpose The purpose of this curriculum outline is to provide a framework for multidisciplinary training for radiation oncologists, medical
CURRICULUM OUTLINE FOR TRANSITIONING FROM 2-D RT TO 3-D CRT AND IMRT Purpose The purpose of this curriculum outline is to provide a framework for multidisciplinary training for radiation oncologists, medical
IROC Head and Neck Phantom. Guidelines for Planning and Irradiating the IROC IMRT Phantom. Revised MARCH 2014
 IROC Head and Neck Phantom Guidelines for Planning and Irradiating the IROC IMRT Phantom. Revised MARCH 2014 The study groups are requesting that each institution keep the phantom for a period of time
IROC Head and Neck Phantom Guidelines for Planning and Irradiating the IROC IMRT Phantom. Revised MARCH 2014 The study groups are requesting that each institution keep the phantom for a period of time
Intensity modulated radiotherapy (IMRT) for treatment of post-operative high grade glioma in the right parietal region of brain
 for treatment of post-operative high grade glioma in the right parietal region of brain") 1 Carol Boyd March Case Study March 11, 2013 Intensity modulated radiotherapy (IMRT) for treatment of post-operative high grade glioma in the right parietal region of brain History of Present Illness:
1 Carol Boyd March Case Study March 11, 2013 Intensity modulated radiotherapy (IMRT) for treatment of post-operative high grade glioma in the right parietal region of brain History of Present Illness:
Canadian Partnership for Quality Radiotherapy. Technical Quality Control Guidelines for Gamma Knife Radiosurgery. A guidance document on behalf of:
 Canadian Partnership for Quality Radiotherapy Technical Quality Control Guidelines for Gamma Knife Radiosurgery A guidance document on behalf of: Canadian Association of Radiation Oncology Canadian Organization
Canadian Partnership for Quality Radiotherapy Technical Quality Control Guidelines for Gamma Knife Radiosurgery A guidance document on behalf of: Canadian Association of Radiation Oncology Canadian Organization
Stereotactic radiotherapy
 Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
IMRT QUESTIONNAIRE. Address: Physicist: Research Associate: Dosimetrist: Responsible Radiation Oncologist(s)
") IMRT QUESTIONNAIRE Institution: Date: / / Address: Physicist: e-mail: Telephone: Fax: Research Associate: email: Telephone: Fax: Dosimetrist: email: Telephone: Fax: Responsible Radiation Oncologist(s)
IMRT QUESTIONNAIRE Institution: Date: / / Address: Physicist: e-mail: Telephone: Fax: Research Associate: email: Telephone: Fax: Dosimetrist: email: Telephone: Fax: Responsible Radiation Oncologist(s)
Automated Plan Quality Check with Scripting. Rajesh Gutti, Ph.D. Clinical Medical Physicist
 Automated Plan Quality Check with Scripting Rajesh Gutti, Ph.D. Clinical Medical Physicist Veera.Gutti@BSWHealth.org Outline Introduction - BSW Automation in Treatment planning Eclipse Scripting API Script
Automated Plan Quality Check with Scripting Rajesh Gutti, Ph.D. Clinical Medical Physicist Veera.Gutti@BSWHealth.org Outline Introduction - BSW Automation in Treatment planning Eclipse Scripting API Script
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
Normal tissue doses from MV image-guided radiation therapy (IGRT) using orthogonal MV and MV-CBCT
 using orthogonal MV and MV-CBCT") Received: 28 September 2017 Revised: 17 November 2017 Accepted: 28 December 2017 DOI: 10.1002/acm2.12276 RADIATION ONCOLOGY PHYSICS Normal tissue doses from MV image-guided radiation therapy (IGRT) using
Received: 28 September 2017 Revised: 17 November 2017 Accepted: 28 December 2017 DOI: 10.1002/acm2.12276 RADIATION ONCOLOGY PHYSICS Normal tissue doses from MV image-guided radiation therapy (IGRT) using
EORTC Member Facility Questionnaire
 Page 1 of 9 EORTC Member Facility Questionnaire I. Administrative Data Name of person submitting this questionnaire Email address Function Phone Institution Address City Post code Country EORTC No Enter
Page 1 of 9 EORTC Member Facility Questionnaire I. Administrative Data Name of person submitting this questionnaire Email address Function Phone Institution Address City Post code Country EORTC No Enter
Otolaryngologist s Perspective of Stereotactic Radiosurgery
 Otolaryngologist s Perspective of Stereotactic Radiosurgery Douglas E. Mattox, M.D. 25 th Alexandria International Combined ORL Conference April 18-20, 2007 Acoustic Neuroma Benign tumor of the schwann
Otolaryngologist s Perspective of Stereotactic Radiosurgery Douglas E. Mattox, M.D. 25 th Alexandria International Combined ORL Conference April 18-20, 2007 Acoustic Neuroma Benign tumor of the schwann
IROC Lung Phantom 3D CRT / IMRT. Guidelines for Planning and Irradiating the IROC Lung Phantom. Revised Dec 2015
 IROC Lung Phantom 3D CRT / IMRT Guidelines for Planning and Irradiating the IROC Lung Phantom. Revised Dec 2015 The IROC requests that each institution keep the phantom for no more than 2 weeks. During
IROC Lung Phantom 3D CRT / IMRT Guidelines for Planning and Irradiating the IROC Lung Phantom. Revised Dec 2015 The IROC requests that each institution keep the phantom for no more than 2 weeks. During
IMRT FOR CRANIOSPINAL IRRADIATION: CHALLENGES AND RESULTS. A. Miller, L. Kasulaitytė Institute of Oncolygy, Vilnius University
 IMRT FOR CRANIOSPINAL IRRADIATION: CHALLENGES AND RESULTS A. Miller, L. Kasulaitytė Institute of Oncolygy, Vilnius University Content 1.Introduction 2.Methods and materials 3.Results and discussion 4.Conclusion
IMRT FOR CRANIOSPINAL IRRADIATION: CHALLENGES AND RESULTS A. Miller, L. Kasulaitytė Institute of Oncolygy, Vilnius University Content 1.Introduction 2.Methods and materials 3.Results and discussion 4.Conclusion
Introduction. Modalities used in imaging guidance. Flat panel detector. X-ray Imaging Dose to Patients in the Era of Image-Guided Radiation Therapy
 X-ray Imaging Dose to Patients in the Era of Image-Guided Radiation Therapy George Ding, Ron Price, Charles Coffey Vanderbilt-Ingram Cancer Center Vanderbilt University Medical Center, Nashville, TN Introduction
X-ray Imaging Dose to Patients in the Era of Image-Guided Radiation Therapy George Ding, Ron Price, Charles Coffey Vanderbilt-Ingram Cancer Center Vanderbilt University Medical Center, Nashville, TN Introduction
Defining Target Volumes and Organs at Risk: a common language
 Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
Reena Phurailatpam. Intensity Modulated Radiation Therapy of Medulloblastoma using Helical TomoTherapy: Initial Experience from planning to delivery
 Intensity Modulated Radiation Therapy of Medulloblastoma using Helical TomoTherapy: Initial Experience from planning to delivery Reena Phurailatpam Tejpal Gupta, Rakesh Jalali, Zubin Master, Bhooshan Zade,
Intensity Modulated Radiation Therapy of Medulloblastoma using Helical TomoTherapy: Initial Experience from planning to delivery Reena Phurailatpam Tejpal Gupta, Rakesh Jalali, Zubin Master, Bhooshan Zade,
Leksell Gamma Knife Icon A New User s Perspective
 Leksell Gamma Knife Icon A New User s Perspective Steve Herchko, DMP 2017 MFMER slide-1 Disclosures None 2017 MFMER slide-2 Outline Icon Overview Mayo Clinic Experience Frame-Based System Mask-Based System
Leksell Gamma Knife Icon A New User s Perspective Steve Herchko, DMP 2017 MFMER slide-1 Disclosures None 2017 MFMER slide-2 Outline Icon Overview Mayo Clinic Experience Frame-Based System Mask-Based System
SRS Uncertainty: Linac and CyberKnife Uncertainties
 SRS Uncertainty: Linac and CyberKnife Uncertainties Sonja Dieterich, PhD Linac/CyberKnife Technological Uncertainties 1 Linac Mechanical/Radiation Isocenters Depuydt, Tom, et al. "Computer aided analysis
SRS Uncertainty: Linac and CyberKnife Uncertainties Sonja Dieterich, PhD Linac/CyberKnife Technological Uncertainties 1 Linac Mechanical/Radiation Isocenters Depuydt, Tom, et al. "Computer aided analysis
Disclosures. Clinical Implementation of SRS/SBRT. Overview. Anil Sethi, PhD. Speaker: BrainLAB Standard Imaging Research collaboration: RaySearch
 Clinical Implementation of SRS/SBRT Anil Sethi, PhD Loyola University Medical Center August 3, 2017 Disclosures Speaker: BrainLAB Standard Imaging Research collaboration: RaySearch 2 Overview Physics Considerations
Clinical Implementation of SRS/SBRT Anil Sethi, PhD Loyola University Medical Center August 3, 2017 Disclosures Speaker: BrainLAB Standard Imaging Research collaboration: RaySearch 2 Overview Physics Considerations
X-Ray Guided Robotic Radiosurgery for Solid Tumors
 X-Ray Guided Robotic Radiosurgery for Solid Tumors Mohan Bodduluri Accuray Incorporated 570 Del Rey Avenue Sunnyvale, CA 94085 USA and J. M. McCarthy Department of Mechanical and Aerospace Engineering
X-Ray Guided Robotic Radiosurgery for Solid Tumors Mohan Bodduluri Accuray Incorporated 570 Del Rey Avenue Sunnyvale, CA 94085 USA and J. M. McCarthy Department of Mechanical and Aerospace Engineering
MAX-HD SRS PHANTOM THE COMPREHENSIVE END-TO-END SRS PHANTOM SCAN PLAN LOCALIZE TREAT. distributed by:
 SRS PHANTOM SCAN PLAN LOCALIZE TREAT THE COMPREHENSIVE END-TO-END SRS PHANTOM distributed by: Tel: +33 (0) 42 88 68 41 info@orion-france.com www.orion-france.com 2, Avenue du General Balfourier 75016 Paris,
SRS PHANTOM SCAN PLAN LOCALIZE TREAT THE COMPREHENSIVE END-TO-END SRS PHANTOM distributed by: Tel: +33 (0) 42 88 68 41 info@orion-france.com www.orion-france.com 2, Avenue du General Balfourier 75016 Paris,
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
8/3/2016. Outline. Site Specific IGRT Considerations for Clinical Imaging Protocols. Krishni Wijesooriya, PhD University of Virginia
 Site Specific IGRT Considerations for Clinical Imaging Protocols Krishni Wijesooriya, PhD University of Virginia Outline Image registration accuracies for different modalities What imaging modality best
Site Specific IGRT Considerations for Clinical Imaging Protocols Krishni Wijesooriya, PhD University of Virginia Outline Image registration accuracies for different modalities What imaging modality best
Results of Stereotactic radiotherapy for Stage I and II NSCLC Is There a Need for Image Guidance?
 Results of Stereotactic radiotherapy for Stage I and II NSCLC Is There a Need for Image Guidance? Frank Zimmermann Institute of Radiation Oncolgy University Clinic Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch
Results of Stereotactic radiotherapy for Stage I and II NSCLC Is There a Need for Image Guidance? Frank Zimmermann Institute of Radiation Oncolgy University Clinic Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch
Image Guided Stereotactic Radiotherapy of the Lung
 Image Guided Stereotactic Radiotherapy of the Lung Jamie Marie Harris, MS DABR Avera McKennan Radiation Oncology September 25, 2015 Stereotactic Body Radiotherapy - Clinical Dose/Fractionation - Normal
Image Guided Stereotactic Radiotherapy of the Lung Jamie Marie Harris, MS DABR Avera McKennan Radiation Oncology September 25, 2015 Stereotactic Body Radiotherapy - Clinical Dose/Fractionation - Normal
Dosimetry of the Gamma Knife TM
 Dosimetry of the Gamma Knife TM Sheridan Griffin Meltsner, Ph.D. Aurora Health Care St. Luke s Medical Center NCCAAPM Spring Meeting Outline Introduction to stereotactic radiosurgery Elekta Gamma Knife
Dosimetry of the Gamma Knife TM Sheridan Griffin Meltsner, Ph.D. Aurora Health Care St. Luke s Medical Center NCCAAPM Spring Meeting Outline Introduction to stereotactic radiosurgery Elekta Gamma Knife
Evaluation of Three-dimensional Conformal Radiotherapy and Intensity Modulated Radiotherapy Techniques in High-Grade Gliomas
 1 Carol Boyd Comprehensive Case Study July 11, 2013 Evaluation of Three-dimensional Conformal Radiotherapy and Intensity Modulated Radiotherapy Techniques in High-Grade Gliomas Abstract: Introduction:
1 Carol Boyd Comprehensive Case Study July 11, 2013 Evaluation of Three-dimensional Conformal Radiotherapy and Intensity Modulated Radiotherapy Techniques in High-Grade Gliomas Abstract: Introduction:
IGRT Solution for the Living Patient and the Dynamic Treatment Problem
 IGRT Solution for the Living Patient and the Dynamic Treatment Problem Lei Dong, Ph.D. Associate Professor Dept. of Radiation Physics University of Texas M. D. Anderson Cancer Center Houston, Texas Learning
IGRT Solution for the Living Patient and the Dynamic Treatment Problem Lei Dong, Ph.D. Associate Professor Dept. of Radiation Physics University of Texas M. D. Anderson Cancer Center Houston, Texas Learning
Leksell Gamma Knife Icon. Treatment information
 Leksell Gamma Knife Icon Treatment information You may be feeling frightened or overwhelmed by your recent diagnosis. It can be confusing trying to process a diagnosis, understand a new and challenging
Leksell Gamma Knife Icon Treatment information You may be feeling frightened or overwhelmed by your recent diagnosis. It can be confusing trying to process a diagnosis, understand a new and challenging
EXACTRAC HIGHLY ACCURATE PATIENT MONITORING
 EXACTRAC HIGHLY ACCURATE PATIENT MONITORING PATIENT POSITION MONITORING ExacTrac is an in-room based monitoring system that detects intrafractional motion during treatment delivery. Two kv X-Ray units
EXACTRAC HIGHLY ACCURATE PATIENT MONITORING PATIENT POSITION MONITORING ExacTrac is an in-room based monitoring system that detects intrafractional motion during treatment delivery. Two kv X-Ray units
4D Radiotherapy in early ca Lung. Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla
 4D Radiotherapy in early ca Lung Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla Presentation focus on ---- Limitation of Conventional RT Why Interest in early lung cancer
4D Radiotherapy in early ca Lung Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla Presentation focus on ---- Limitation of Conventional RT Why Interest in early lung cancer
Independent Dose Verification for IMRT Using Monte Carlo. C-M M Charlie Ma, Ph.D. Department of Radiation Oncology FCCC, Philadelphia, PA 19111, USA
 Independent Dose Verification for IMRT Using Monte Carlo C-M M Charlie Ma, Ph.D. Department of Radiation Oncology FCCC, Philadelphia, PA 19111, USA Outline Why Monte Carlo for IMRT QA? Experimental verification
Independent Dose Verification for IMRT Using Monte Carlo C-M M Charlie Ma, Ph.D. Department of Radiation Oncology FCCC, Philadelphia, PA 19111, USA Outline Why Monte Carlo for IMRT QA? Experimental verification
Proton Stereotactic Radiotherapy: Clinical Overview. Brian Winey, Ph.D. Physicist, MGH Assistant Professor, HMS
 Proton Stereotactic Radiotherapy: Clinical Overview Brian Winey, Ph.D. Physicist, MGH Assistant Professor, HMS Acknowledgements Radiation Oncologists and Physicists at various institutions (MGH, MDACC,
Proton Stereotactic Radiotherapy: Clinical Overview Brian Winey, Ph.D. Physicist, MGH Assistant Professor, HMS Acknowledgements Radiation Oncologists and Physicists at various institutions (MGH, MDACC,
Brain Tumor Radiosurgery. Gabor Fichtinger, PhD
 Brain Tumor Radiosurgery Gabor Fichtinger, PhD Surgical CAD/CAM Preoperative Computerassisted planning Surgical Intraoperative Update Model Update Plan Surgical CAD CAM Patient-specific Model Computer-
Brain Tumor Radiosurgery Gabor Fichtinger, PhD Surgical CAD/CAM Preoperative Computerassisted planning Surgical Intraoperative Update Model Update Plan Surgical CAD CAM Patient-specific Model Computer-
IROC Head and Neck Phantom. Guidelines for Planning and Irradiating the IROC IMRT Phantom. Revised April 2014
 IROC Head and Neck Phantom Guidelines for Planning and Irradiating the IROC IMRT Phantom. Revised April 2014 The IROC Houston is requesting that each institution keep the phantom for two weeks. During
IROC Head and Neck Phantom Guidelines for Planning and Irradiating the IROC IMRT Phantom. Revised April 2014 The IROC Houston is requesting that each institution keep the phantom for two weeks. During
SBRT REQUIRES: STEREOTACTIC BODY RADIOTHERAPY STEREOTACTIC BODY RADIOTHERAPY (SBRT) (SBRT) What s s in a name? Stereotactic Body Radiotherapy
 (SBRT) What s s in a name? Stereotactic Body Radiotherapy") INTRODUCTION TO STEREOTACTIC BODY RADIOTHERAPY: (I) Physics and Technology (II) Clinical Experience & (III) Radiobiological Considerations and Future Directions Stanley H. Benedict, Ph.D., Danny Song,
INTRODUCTION TO STEREOTACTIC BODY RADIOTHERAPY: (I) Physics and Technology (II) Clinical Experience & (III) Radiobiological Considerations and Future Directions Stanley H. Benedict, Ph.D., Danny Song,
Fiducial-Free Lung Tracking and Treatment with the CyberKnife System: A Non-Invasive Approach
 Fiducial-Free Lung Tracking and Treatment with the CyberKnife System: A Non-Invasive Approach Jesse McKay, MS, DABR Erlanger Health System Chattanooga, TN JASTRO 2014, Yokohama Japan Disclosure I have
Fiducial-Free Lung Tracking and Treatment with the CyberKnife System: A Non-Invasive Approach Jesse McKay, MS, DABR Erlanger Health System Chattanooga, TN JASTRO 2014, Yokohama Japan Disclosure I have
Strategies and Technologies for Cranial Radiosurgery Planning: Gamma Knife
 Conflicts of Interest Strategies and Technologies for Cranial Radiosurgery Planning: Gamma Knife David Schlesinger, Ph.D. Research support: Elekta Instruments, AB Lars Leksell Gamma Knife Center University
Conflicts of Interest Strategies and Technologies for Cranial Radiosurgery Planning: Gamma Knife David Schlesinger, Ph.D. Research support: Elekta Instruments, AB Lars Leksell Gamma Knife Center University
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments
 Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Cyberknife Stereotactic Treatment
 Cyberknife Stereotactic Treatment Eugene Lief, Ph.D. Christ Hospital Jersey City, New Jersey USA DISCLAIMER: I am not affiliated with any vendor and did not receive any financial support from any vendor.
Cyberknife Stereotactic Treatment Eugene Lief, Ph.D. Christ Hospital Jersey City, New Jersey USA DISCLAIMER: I am not affiliated with any vendor and did not receive any financial support from any vendor.
Institute of Oncology & Radiobiology. Havana, Cuba. INOR
 Institute of Oncology & Radiobiology. Havana, Cuba. INOR 1 Transition from 2-D 2 D to 3-D 3 D conformal radiotherapy in high grade gliomas: : our experience in Cuba Chon. I, MD - Chi. D, MD - Alert.J,
Institute of Oncology & Radiobiology. Havana, Cuba. INOR 1 Transition from 2-D 2 D to 3-D 3 D conformal radiotherapy in high grade gliomas: : our experience in Cuba Chon. I, MD - Chi. D, MD - Alert.J,
3D Conformal Radiation Therapy for Mucinous Carcinoma of the Breast
 1 Angela Kempen February Case Study February 22, 2012 3D Conformal Radiation Therapy for Mucinous Carcinoma of the Breast History of Present Illness: JE is a 45 year-old Caucasian female who underwent
1 Angela Kempen February Case Study February 22, 2012 3D Conformal Radiation Therapy for Mucinous Carcinoma of the Breast History of Present Illness: JE is a 45 year-old Caucasian female who underwent
Spatially Fractionated Radiation Therapy: GRID Sponsored by.decimal Friday, August 22, Pamela Myers, Ph.D.
 Spatially Fractionated Radiation Therapy: GRID Sponsored by.decimal Friday, August 22, 2014 Pamela Myers, Ph.D. Introduction o o o o o Outline GRID compensator Purpose of SFRT/GRID therapy Fractionation
Spatially Fractionated Radiation Therapy: GRID Sponsored by.decimal Friday, August 22, 2014 Pamela Myers, Ph.D. Introduction o o o o o Outline GRID compensator Purpose of SFRT/GRID therapy Fractionation
Varian Edge Experience. Jinkoo Kim, Ph.D Henry Ford Health System
 Varian Edge Experience Jinkoo Kim, Ph.D Henry Ford Health System Disclosures I participate in research funded by Varian Medical Systems. Outline of Presentation Review advanced imaging in Varian Edge Linear
Varian Edge Experience Jinkoo Kim, Ph.D Henry Ford Health System Disclosures I participate in research funded by Varian Medical Systems. Outline of Presentation Review advanced imaging in Varian Edge Linear
Stereotactic Body Radiotherapy for Lung Lesions using the CyberKnife of-the-art and New Innovations
 Stereotactic Body Radiotherapy for Lung Lesions using the CyberKnife State-of of-the-art and New Innovations Chad Lee, PhD CK Solutions, Inc. and CyberKnife Centers of San Diego Outline Basic overview
Stereotactic Body Radiotherapy for Lung Lesions using the CyberKnife State-of of-the-art and New Innovations Chad Lee, PhD CK Solutions, Inc. and CyberKnife Centers of San Diego Outline Basic overview
IMRT - the physician s eye-view. Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia
 IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
Accuracy Requirements and Uncertainty Considerations in Radiation Therapy
 Departments of Oncology and Medical Biophysics Accuracy Requirements and Uncertainty Considerations in Radiation Therapy Introduction and Overview 6 August 2013 Jacob (Jake) Van Dyk Conformality 18 16
Departments of Oncology and Medical Biophysics Accuracy Requirements and Uncertainty Considerations in Radiation Therapy Introduction and Overview 6 August 2013 Jacob (Jake) Van Dyk Conformality 18 16
What do we Know About Adaptive Radiotherapy? Lei Dong, Ph.D. Scripps Proton Therapy Center San Diego, California
 What do we Know About Adaptive Radiotherapy? Lei Dong, Ph.D. Scripps Proton Therapy Center San Diego, California AAMD Region II Meeting Houston, Texas September 13-14, 2012 Learning Objectives To gain
What do we Know About Adaptive Radiotherapy? Lei Dong, Ph.D. Scripps Proton Therapy Center San Diego, California AAMD Region II Meeting Houston, Texas September 13-14, 2012 Learning Objectives To gain
Extracranial doses in stereotactic and conventional radiotherapy for pituitary adenomas
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 7, NUMBER 2, SPRING 2006 Extracranial doses in stereotactic and conventional radiotherapy for pituitary adenomas Thomas Samuel Ram, a Paul B. Ravindran,
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 7, NUMBER 2, SPRING 2006 Extracranial doses in stereotactic and conventional radiotherapy for pituitary adenomas Thomas Samuel Ram, a Paul B. Ravindran,
Disclosure. Outline. Machine Overview. I have received honoraria from Accuray in the past. I have had travel expenses paid by Accuray in the past.
 Clinical Implementation of the CyberKnife Disclosure I have received honoraria from Accuray in the past. I have had travel expenses paid by Accuray in the past. Mary Ellen Masterson-McGary McGary CyberKnife
Clinical Implementation of the CyberKnife Disclosure I have received honoraria from Accuray in the past. I have had travel expenses paid by Accuray in the past. Mary Ellen Masterson-McGary McGary CyberKnife
SBRT in early stage NSCLC
 SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
SHIELDING TECHNIQUES FOR CURRENT RADIATION THERAPY MODALITIES
 SHIELDING TECHNIQUES FOR CURRENT RADIATION THERAPY MODALITIES MELISSA C. MARTIN, M.S., FACR, FAAPM PRESIDENT AAPM - 2017 PRESIDENT - THERAPY PHYSICS INC., GARDENA, CA MELISSA@THERAPYPHYSICS.COM AAPM Spring
SHIELDING TECHNIQUES FOR CURRENT RADIATION THERAPY MODALITIES MELISSA C. MARTIN, M.S., FACR, FAAPM PRESIDENT AAPM - 2017 PRESIDENT - THERAPY PHYSICS INC., GARDENA, CA MELISSA@THERAPYPHYSICS.COM AAPM Spring
Radiation treatment planning in lung cancer
 Radiation treatment planning in lung cancer Georg Dietmar 1,2 1 Div. Medical Rad. Phys., Dept. of Radiation Oncology / Medical Univ. Vienna & AKH Wien 2 Christian Doppler Laboratory for Medical Radiation
Radiation treatment planning in lung cancer Georg Dietmar 1,2 1 Div. Medical Rad. Phys., Dept. of Radiation Oncology / Medical Univ. Vienna & AKH Wien 2 Christian Doppler Laboratory for Medical Radiation
biij Initial experience in treating lung cancer with helical tomotherapy
 Available online at http://www.biij.org/2007/1/e2 doi: 10.2349/biij.3.1.e2 biij Biomedical Imaging and Intervention Journal CASE REPORT Initial experience in treating lung cancer with helical tomotherapy
Available online at http://www.biij.org/2007/1/e2 doi: 10.2349/biij.3.1.e2 biij Biomedical Imaging and Intervention Journal CASE REPORT Initial experience in treating lung cancer with helical tomotherapy
ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER
 ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER Bro. Dr. Collie Miller IARC/WHO Based on trends in the incidence of cancer, the International Agency for Research on Cancer (IARC) and WHO
ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER Bro. Dr. Collie Miller IARC/WHO Based on trends in the incidence of cancer, the International Agency for Research on Cancer (IARC) and WHO