MANAGEMENT OF CA HYPOPHARYNX
|
|
|
- Joleen Wilkins
- 6 years ago
- Views:
Transcription
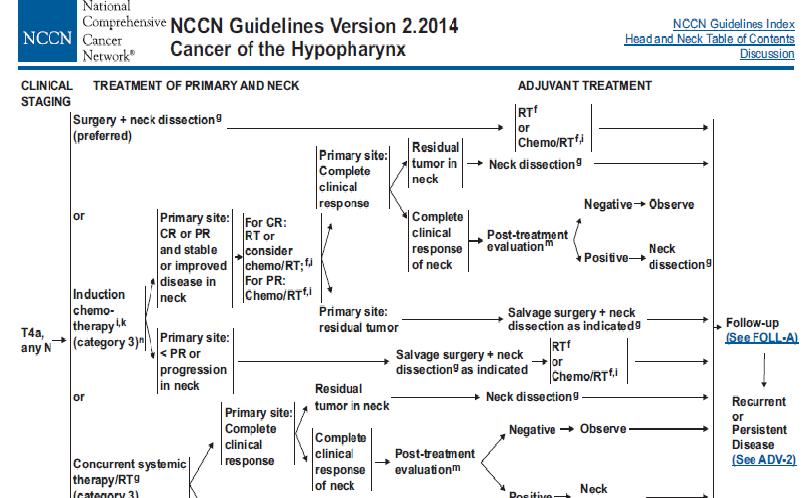
1 MANAGEMENT OF CA HYPOPHARYNX

2 GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE
3 For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable and acceptable treatment options. The vast majority of patients, however, present with stage III or IV disease and warrant multimodality treatment.
4 Primary Surgery T1 and T2 Tumors Indications for primary surgical management of patients with early cancers of the hypopharynx History of previous H&N radiation Organ conservation approaches possible Those who refuse radiation
5 Role of surgeon in Ca hypo pharynx patients who undergo non operative treatment approaches Performing Endoscopic biopsy Detailed assessment of tumor extent Methods to secure the airway (tracheotomy or laser debulking) Methods to ensure adequate nutrition (gastrostomy) Multidisciplinary oncologic follow-up after nonoperative treatment
6 Selected T1 and T2 hypopharynx cancers may lend themselves to surgical excision. Favorable subsites include Upper pyriform sinus Posterior pharyngeal wall. The standard supraglottic laryngectomy encompasses the aryepiglottic fold and may be extended to include part of the arytenoids, the base of the tongue, and the upper pyriform sinus.
7 Relative contraindications to organ conservation surgery for hypopharynx cancers Cartilage invasion Vocal fold fixation Postcricoid invasion Deep pyriform sinus invasion Extension beyond the larynx
8 In recent years, advancements in organ preservation surgery have included the use of Transoral laser microsurgery Transoral robotic surgery. For selected cases, these approaches can achieve oncologic tumor removal, while limiting normal tissue disruption, thereby potentially avoiding tracheostomy and the use of feeding tubes
9 Recent results have demonstrated that appropriately selected T1 or T2 lesions can achieve negative margins by transoral laser microsurgery or transoral robotic surgery. Oncologic outcomes appear similar to open surgical approaches using this technique and are likely accompanied by lower rates of permanent gastrostomy tube or tracheostomy placement

10 FIVE-YEAR ONCOLOGIC OUTCOMES FOR TRANSORAL MICROLASER SURGERY FOR T1 OR T2 HYPOPHARYNGEAL TUMORS
11 T3 or T4 Resectable Tumors Most T3 and T4 hypopharynx cancers that are treated surgically will require total laryngectomy with efforts to preserve a posterior strip of the hypopharynx spanning the oropharynx to the esophagus.
12 For more bulky tumors of the hypopharynx, total laryngopharyngectomy, removal of the larynx and the entire hypopharynx, is required. This procedure creates a gap between the oropharynx and esophagus that must be reconstructed with a tubed fasciocutaneous flap such as the radial forearm free flap or anterolateral thigh flap, a free jejunum, or a tubed pedicled myocutaneous flap
13 Types of surgeries in T3 T4 Ca hypopharynx Partial laryngo pharyngectomy Total laryngo pharyngectomy For small medial and anterior PF sinus lesions Removes false cords,epiglottis,areyepiglottic folds, PF sinus but True vocal cords are preserved For more advanced hypopharyngeal lesions Total laryngectomy with removal of variable amount of pharyngeal wall.
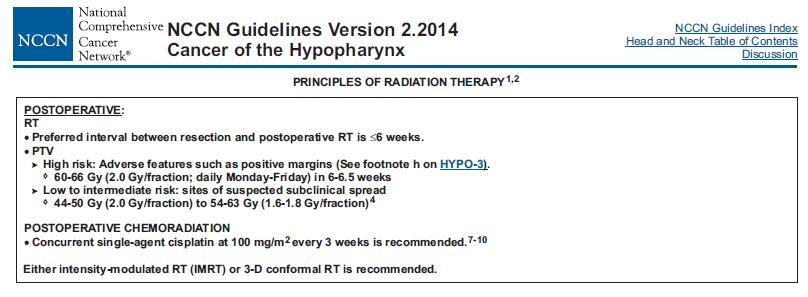
14 Postoperative Radiation Therapy Most advanced hypopharynx cancers that are treated with initial surgical resection Postoperative radiation therapy can be added in an effort to enhance locoregional control rates
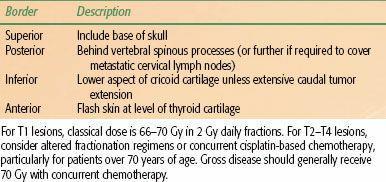
15 Indications for postoperative radiation T4 primary tumors Close or positive microscopic margins Cartilage or bony invasion More than one metastatic lymph node Extracapsular extension (ECE) Conventional therapy involves the use of a shrinkingfield technique to deliver 54 to 63 Gy to all areas at risk and a boost to 60 to 66 Gy to regions of ECE or positive margins. The entire cervical nodal chain from the skull base to the clavicle bilaterally should be included
16

17 RESULTS OF RTOG 9501 POSTOP CHEMORADIATION TRIAL

18 RESULTS OF EORTC POSTOPERATIVE CHEMORADIATION TRIAL
19 Definitive Radiation Therapy T1 and T2 Tumors Curative radiation therapy (RT) is generally the preferred treatment option for patients with T1 or T2 hypopharynx tumors. Affords good potential for organ preservation without compromise in clinical outcome A classical course of radiation therapy for hypopharynx cancer lasts 6 to 7 weeks, with treatment delivered 5 days per week
20 Conventional treatment involves a shrinking-field technique that initiates with opposed lateral fields encompassing the primary tumor and upper neck lymphatics with a matched anterior field to complete treatment of the lower neck One of the most common worldwide fractionation regimens involves the delivery of 2 Gy daily fractions to 70 Gy over 7 weeks
21

22 Digitally reconstructed radiograph depicting a classical lateral field designed to encompass the T2 pyriform sinus cancer. plus bilateral cervical lymphatics from skull base to cricoid, with a matching anterior low-neck field to extend the lymphatic coverage to the level of the clavicle
23
24 Due to the high likelihood of subclinical nodal metastases even in the clinically N0 neck, patients traditionally receive comprehensive radiation to encompass nodal regions from the skull base to the clavicle. Due to the varying thicknesses of the head and neck, custom compensators or wedges should be used for the lateral fields to improve dose homogeneity.
25 Shrinking field techniques to spare direct spinal cord dose after approximately 45 Gy, as well as final mucosal reductions after 54 to 60 Gy, are often appropriate with posterior neck boosting, with electrons to supplement posterior chain nodal dosing without excessive dose to the spinal cord
26 Altered fractionation techniques Hyperfractionation (e.g., Gy twice daily) Accelerated fractionation (e.g., 6 fraction per week or concomitant boost regimens). Improved locoregional control rates for H&N cancer patients
27 A recent meta-analysis examined 15 trials that compared conventional fractionation to altered fractionation, either Hyperfractionation or accelerated fractionation Small but statistically significant survival benefit of 3.4% at 5 years with altered fractionation. The benefit was higher with hyperfractionation compared to accelerated fractionation and was more pronounced for patients younger than age 50.
28 Early T-stage hypopharynx patients with N0 or N1 neck disease can be considered for treatment with radiation alone or concurrent radiation plus chemotherapy. In this setting, gross disease should receive 70 Gy and the contralateral neck (N0) should receive 50 to 54 Gy
29 T1N0 lesions, patients may achieve 5-year diseasespecific survival (DSS) on the order of 90%. T2N0 lesions may achieve DSS above 70%.

30 LOCAL CONTROL FOR CARCINOMA OF THE POSTERIOR PHARYNGEAL WALL TREATED WITH RADIATION ALONE

31 CAUSE-SPECIFIC AND OVERALL SURVIVAL FOR CARCINOMA OF THE PYRIFORM SINUS TREATED WITH RADIATION ALONE
32 IMRT IMRT in H&N cancer as a means of diminishing normal tissue toxicities Particularly xerostomia resulting from irradiation of major salivary glands. Excellent candidates for IMRT include patients with unilateral T1 to T3 primary lesions with N2b or less neck disease.
33 A recent randomized trial of conventional radiotherapy versus IMRT in patients with T1-4N0-3 oropharyngeal and hypopharyngeal tumors at high risk for xerostomia highlighted the benefits of IMRT for parotid sparing
34 Patients were treated either postoperatively or definitively Contralateral parotid was constrained to <24 Gy to the whole gland. Grade 2 or worse xerostomia was significantly reduced at both 12 months (74% conventional vs 38% IMRT) At 24 months (83% conventional vs 29% IMRT). 5 These benefits translated to significantly better qualityof-life scores in the IMRT group and strongly support a role for IMRT in H&N SCC radiotherapy.

35 Beam s eye projections of intensity-modulated radiation therapy target contours for patient with T2N2bM0 tumor of the right pyriform sinus
36 T3 and T4 Tumors Hypopharynx cancer patients who are technically resectable may not undergo primary surgery. These include age (e.g., patients over 70 to 80 years old), Presence of significant medical comorbidities, or patient unwillingness to accept total laryngectomy. Curative-intent radiation or chemoradiation is often pursued in these setting
37 Conventional radiation therapy commonly involves a shrinking three-field technique to deliver approximately 70 Gy in 2-Gy daily fractions to areas of gross disease and 50 to 60 Gy to areas of microscopic disease. If patients are scheduled to undergo postradiotherapy neck dissection, then gross nodal disease can be limited to 60 to 63 Gy If patients are not candidates for postradiotherapy neck dissection, then gross nodal disease should be carried to 70 Gy
38 In patients with adequate performance status, concurrent chemoradiation strategies using platinum-based chemotherapy should be considered. Once-daily radiation regimens without concurrent chemotherapy may be quite reasonable for hypopharynx patients over 70 years of age or for those patients with modest performance status
39 Molecular-targeted therapies in the treatment of H&N cancer patients Another alternative to concomitant chemotherapy or accelerated fractionation is the more recent introduction of molecular-targeted therapies in the treatment of H&N cancer patients The most mature clinical dataset in H&N cancer involves the use of EGFR inhibitors such as cetuximab (monoclonal antibody against the EGFR)
40 International phase III trial High-dose radiation alone versus radiation plus cetuximab in advanced H&N cancer patients confirmed a locoregional control improvement (10% at 5 years). Overall survival advantage (10% at 5 years) with the addition of cetuximab. A relatively small subset of patients with hypopharynx cancer was enrolled in this study of 424 patients, and this subset did not demonstrate a clear advantage with use of the EGFR inhibitor treatment.
41 Data from the NCDB Benchmark Reports addressing 16,136 cases diagnosed in 2000 to 2008 reveal the combination of radiation and chemotherapy to be the most common initial treatment overall for stage II (32.6%), stage III (47.8%), and stage IV (43.8%) disease. Over 50% of stage III and stage IV cases received initial treatment with chemotherapy in some form either alone or in combination with radiation or surgery.
42 It has been reported that approximately 35% to 45% of patients with advanced hypopharyngeal tumors treated with concurrent chemoradiotherapy utilizing IMRT can be expected to live 5 years, with laryngeal preservation in approximately two-thirds of survivors.

43 The stage-specific first course of treatment for hypopharyngeal cancer in the United States from 2000 to 2008 is presented with unknown stage excluded. S, surgery; XRT, radiotherapy; Ch, chemotherapy. (From National Cancer Data Base. Commission on Cancer. American College of Surgeons. Benchmark Reports

44 ONCOLOGIC OUTCOMES FOR PATIENTS UNDERGOING CONCURRENT CHEMORADIOTHERAPY AND INTENSITY-MODULATED RADIATION THERAPY FOR ADVANCED HYPOPHARYNGEAL CANCERS
45 Induction Chemotherapy and Sequential (Chemo)radiation For patients with locoregionally advanced H&N cancer. EORTC conducted a randomized trial for patients with tumors that would require total laryngectomy as the surgical approach.
46 EORTC trial Induction chemotherapy with cisplatin and 5- florouracil (5-FU) definitive radiation With a median follow-up of 10 years, this trial demonstrated no significant difference in 5- or 10-year overall survival or progressionfree survival Larynx was preserved in 2/3 of patients in this arm Primary surgical resection and postoperative radiation. With a median follow-up of 10 years, this trial demonstrated no significant difference in 5- or 10-year overall survival or progressionfree survival Laryngectomy was done
47 TAX-324, which utilized similar induction chemotherapy arms (TPF vs. PF), followed by concurrent chemoradiotherapy with carboplatin. Five-year survival in the TPF arm was 52% versus 42% receiving PF, while no increased rates of gastric feeding tubes or tracheostomies were noted between groups
48 . The EORTC study (TAX-323) randomized patients with locoregionally advanced, unresectable disease induction 5-FU and cisplatin followed by definative RxT induction cisplatin and fluorouracil (PF) No survival benefit indutction 5-FU, cisplatin, plus a taxane followed by defenative RxT induction docetaxel, cisplatin, and fluorouracil (TPF) TPF improved the median overall survival from 14.5 months to 18.8 months, with a 27% reduction in the risk of death
49 Post radiotherapy Neck Dissection N0 or N1 patients treated with primary radiation or chemoradiation Adjuvant neck dissection not necessary N2 or N3 neck disease Adjuvant neck dissection necessary Detailed imaging of the neck 12 weeks postradiation with FDG-PET can serve as a valuable guide to help select those patients warranting adjuvant neck dissection.
50 Palliative Radiotherapy Patients with poor performance status who are not considered candidates for aggressive radiation or chemoradiation approaches should be managed with palliative intent. This may include short course radiation regimens such as 4 to 5 Gy 5 fractions over 1 to 2 weeks with repeat of the same 3 weeks hence if favorable initial tolerance and response is achieved.
51 A recent study suggests using a 3.7 Gy fraction twice daily 2 consecutive days for 3 cycles every 2 to 3 weeks Described in RTOG-85-02, Similar palliative efficacy with less toxicity as compared to other palliative regimens. Other approaches described include 50 Gy in 16 fractions and 30 Gy in 5 fractions, 2 fractions per week.
52 Palliative Chemotherapy Patients with adequate or good performance status should be considered for palliative chemotherapy. Median overall survival for patients with metastatic disease is 6 to 10 months. Single-agent cisplatin is usually the first regimen, as it has been shown to improve overall survival. In combination with cisplatin as first-line treatment, cetuximab improved overall survival from 7.4 months to 10.1 months over cisplatin alone.
53 MANAGEMENT OF RECURRENCE After completion of treatment, patients should be followed closely for signs of recurrent or persistent disease. If recurrence is suspected, this should be confirmed by biopsy. If biopsy is confirmatory Patient should undergo complete restaging to assess the extent of disease.
54 Recurrent patients who initially received comprehensive H&N radiation have traditionally not been considered good candidates for repeat high-dose radiation in light of normal tissue tolerances. However, two recent prospective RTOG studies have demonstrated that reirradiation to the H&N is feasible. With the advent of highly conformal radiation delivery techniques, selected patients may benefit from reirradiation approaches in conjunction with systemic chemotherapy.
55 Many patients with recurrent disease, however, are not good candidates for aggressive surgery or salvage radiation therapy and are best served with systemic chemotherapy or best supportive care approaches.
56 COMPLICATIONS CHEMORADIATION Therapy Mucositis Fatigue Loss of taste acuity Radiation dermatitis Xerostomia Nausea Low counts Majority of patients who receive high-dose radiation across major segments of the larynx and hypopharynx will manifest some degree of edema, mucosal congestion, and eventual fibrosis.
57
58 Long term followup During the first 6 months after treatment, patients should be followed every 4 to 6 weeks with clinical examination, including fiberoptic nasopharyngoscopy. Recommended guidelines include a follow-up visit every 1 to 3 months during the first year, every 2 to 4 months for the second year, every 4 to 6 months for years 3 through 5, and every 6 to 12 months thereafter.
59 If the patient received comprehensive H&N radiation, the serum thyroid-stimulating hormone level should be measured every 6 to 12 months. Imaging evaluation of the neck, most commonly with CT or MRI scan, are obtained at 3- to 6-month intervals during the first 2 years or as indicated based on clinical findings Functional imaging with FDG-PET can sometimes prove valuable to help differentiate post treatment fibrosis from persistent or recurrent disease.
60 Conclusion Despite an aggressive approach in the overall management of hypopharynx cancer patients, ultimate cure rates remain quite poor. There are relatively few early-stage patients; and for many advanced-stage patients, it is difficult to achieve long-term control. Even for those patients with excellent response to therapy, there exists a continuous risk for the development of second malignancies, particularly of the upper aerodigestive track with long-term follow-up.
61 Post treatment patients often require aggressive speech and swallow therapy to maximize their functional outcome. There is significant interest in the incorporation of molecular targeted therapies in combination with traditional cytotoxic therapy and radiation in an effort to improve outcomes.
62
63
64
65
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Head and Neck Reirradiation: Perils and Practice
 Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221. Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS
 Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer
 Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
3/12/2018. Head & Neck Cancer Review INTRODUCTION
 Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Q&A. Fabulous Prizes. Collecting Cancer Data: Pharynx 12/6/12. NAACCR Webinar Series Collecting Cancer Data Pharynx
 Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Self-Assessment Module 2016 Annual Refresher Course
 LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
Survey of Laryngeal Cancer at SBUH comparing 108 cases seen here from to the NCDB of 9,256 cases diagnosed nationwide in 2000
 Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
PRINCIPLES OF RADIATION ONCOLOGY
 PRINCIPLES OF RADIATION ONCOLOGY Ravi Pachigolla, MD Faculty Advisor: Anna Pou, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2000 HISTORY
PRINCIPLES OF RADIATION ONCOLOGY Ravi Pachigolla, MD Faculty Advisor: Anna Pou, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2000 HISTORY
Protocol of Radiotherapy for Head and Neck Cancer
 106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS
 MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Head and Neck Cancer Treatment
 Scan for mobile link. Head and Neck Cancer Treatment Head and neck cancer overview The way a particular head and neck cancer behaves depends on the site in which it arises (the primary site). For example,
Scan for mobile link. Head and Neck Cancer Treatment Head and neck cancer overview The way a particular head and neck cancer behaves depends on the site in which it arises (the primary site). For example,
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no
 67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing.
 The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
Diagnosis and what happens after referral
 Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1 Treatment Modalities Early stage disease -larynx
Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1 Treatment Modalities Early stage disease -larynx
Cancer of the upper aerodigestive tract: assessment and management in people aged 16 and over
 Cancer of the upper aerodigestive tract: assessment and management in people aged and over NICE guideline Draft for consultation, March 0 This guideline covers This guideline covers assessing and managing
Cancer of the upper aerodigestive tract: assessment and management in people aged and over NICE guideline Draft for consultation, March 0 This guideline covers This guideline covers assessing and managing
ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER
 ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER Vasu Divi, MD, 1 * Francis P. Worden, MD, 1,2 * Mark E. Prince, MD, 1 Avraham Eisbruch, MD, 3 Julia S. Lee, MD, 4
ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER Vasu Divi, MD, 1 * Francis P. Worden, MD, 1,2 * Mark E. Prince, MD, 1 Avraham Eisbruch, MD, 3 Julia S. Lee, MD, 4
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
SAMO MASTERCLASS HEAD & NECK CANCER. Nicolas Mach, PD Geneva University Hospital
 SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
The Role of Docetaxel in the Treatment of Head and Neck Cancer
 GBMC Head and Neck Conference The Role of Docetaxel in the Treatment of Head and Neck Cancer Simon Best December 7, 2007 Needs assessment: Providers who participate in the care of head and neck cancer
GBMC Head and Neck Conference The Role of Docetaxel in the Treatment of Head and Neck Cancer Simon Best December 7, 2007 Needs assessment: Providers who participate in the care of head and neck cancer
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer. American Society of Clinical Oncology Clinical Practice Guideline
 Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
CURRENT TRENDS IN INITIAL MANAGEMENT OF HYPOPHARYNGEAL CANCER: THE DECLINING USE OF OPEN SURGERY
 CLINICAL REVIEW David W. Eisele, MD, Section Editor CURRENT TRENDS IN INITIAL MANAGEMENT OF HYPOPHARYNGEAL CANCER: THE DECLINING USE OF OPEN SURGERY Robert P. Takes, MD, PhD, 1 Primož Strojan, MD, PhD,
CLINICAL REVIEW David W. Eisele, MD, Section Editor CURRENT TRENDS IN INITIAL MANAGEMENT OF HYPOPHARYNGEAL CANCER: THE DECLINING USE OF OPEN SURGERY Robert P. Takes, MD, PhD, 1 Primož Strojan, MD, PhD,
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma
 Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
The management of advanced supraglottic and
 ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Protons for Head and Neck Cancer. William M Mendenhall, M.D.
 Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Oral Cavity Cancer Combined modality therapy
 Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Neoplasie del laringe Diagnosi e trattamento
 Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Hypopharynx. 1. Introduction. 1.1 General Information and Aetiology
 Hypopharynx 1. Introduction 1.1 General Information and Aetiology The human pharynx is the part of the throat situated between the nasal cavity and the esophagus and can be divided into three parts: the
Hypopharynx 1. Introduction 1.1 General Information and Aetiology The human pharynx is the part of the throat situated between the nasal cavity and the esophagus and can be divided into three parts: the
CANCERS of OROPHARYNX and HYPOPHARYNX. STAGING and TREATMENT
 1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies 3 1. Staging
1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies 3 1. Staging
MULTIDISCIPLINARY MGMT. OF INTERMEDIATE STAGE LARYNGEAL CANCER, ROBERT L. FERRIS, MD 1
 CANCER, ROBERT L. FERRIS, MD 1 Thank you Dr. Johnston, good morning. I m pleased to present the grand rounds for the University of Pittsburgh, the Division of Head and Neck Surgery, and the topic for this
CANCER, ROBERT L. FERRIS, MD 1 Thank you Dr. Johnston, good morning. I m pleased to present the grand rounds for the University of Pittsburgh, the Division of Head and Neck Surgery, and the topic for this
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
ORIGINAL ARTICLE. Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx
 ORIGINAL ARTICLE Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx Sandro J. Stoeckli, MD; Andreas B. Pawlik, MD; Margareta Lipp, MD; Alexander Huber, MD;
ORIGINAL ARTICLE Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx Sandro J. Stoeckli, MD; Andreas B. Pawlik, MD; Margareta Lipp, MD; Alexander Huber, MD;
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Laser Cordectomy. Glottic Carcinoma
 Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck. Mei Tang, MD
 Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK HYPOPHARYNX Head & Neck Site Group Hypopharynx 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND EARLY DETECTION 3 4. DIAGNOSIS
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK HYPOPHARYNX Head & Neck Site Group Hypopharynx 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND EARLY DETECTION 3 4. DIAGNOSIS
9.5. CONVENTIONAL RADIOTHERAPY TECHNIQUE FOR TREATING THYROID CANCER
 9.5. CONVENTIONAL RADIOTHERAPY TECHNIQUE FOR TREATING THYROID CANCER ROBERT J. AMDUR, MD, SIYONG KIM, PhD, JONATHAN GANG LI, PhD, CHIRAY LIU, PhD, WILLIAM M. MENDENHALL, MD, AND ERNEST L. MAZZAFERRI, MD,
9.5. CONVENTIONAL RADIOTHERAPY TECHNIQUE FOR TREATING THYROID CANCER ROBERT J. AMDUR, MD, SIYONG KIM, PhD, JONATHAN GANG LI, PhD, CHIRAY LIU, PhD, WILLIAM M. MENDENHALL, MD, AND ERNEST L. MAZZAFERRI, MD,
Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology
 Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology The head and neck cancer service provides training in the diagnosis, management, treatment, and follow-up care of head
Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology The head and neck cancer service provides training in the diagnosis, management, treatment, and follow-up care of head
Dr. P. Gullane Wharton Chair Head & Neck Surgery Professor Department of Otolaryngology -Head & Neck Surgery University of Toronto
 Wharton Head and Neck Centre The Toronto General Hospital Dr. P. Gullane Wharton Chair Head & Neck Surgery Professor Department of Otolaryngology -Head & Neck Surgery University of Toronto Controversies
Wharton Head and Neck Centre The Toronto General Hospital Dr. P. Gullane Wharton Chair Head & Neck Surgery Professor Department of Otolaryngology -Head & Neck Surgery University of Toronto Controversies
Principles of Management of Head & Neck Cancer. Jinka Sathya Associate professor of Oncology
 Principles of Management of Head & Neck Cancer Jinka Sathya Associate professor of Oncology Oral cavity Oro-pharynx Larynx Hypopharynx Nasophaynx Major sites of Mucosal H&N Cancers Head & Neck Cancer Oral
Principles of Management of Head & Neck Cancer Jinka Sathya Associate professor of Oncology Oral cavity Oro-pharynx Larynx Hypopharynx Nasophaynx Major sites of Mucosal H&N Cancers Head & Neck Cancer Oral
Head & Neck Cancer: When to Irradiate
 Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Head and Neck cancer
 Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
NAACCR Webinar Series 11/2/2017
 COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Oral cancer: Prognosis & Treatment. Dr. Hani Al Sheikh Radhi
 Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Treatment for Supraglottic Ca History: : Total Laryngectomy y was routine until early 50 s, when XRT was developed Ogura and Som developed the one-sta
 Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City.
 JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City. HNSCC with a global incidence of over 500,000 cases and 200,000 deaths annually is the leading cause of mortality and
JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City. HNSCC with a global incidence of over 500,000 cases and 200,000 deaths annually is the leading cause of mortality and
Adjuvant Therapy in Locally Advanced Head and Neck Cancer. Ezra EW Cohen University of Chicago. Financial Support
 Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer
 to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer") The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
Title. CitationInternational Journal of Clinical Oncology, 20(6): 1. Issue Date Doc URL. Rights. Type. File Information
: 1. Issue Date Doc URL. Rights. Type. File Information") Title Clinical outcomes of weekly cisplatin chemoradiother Sakashita, Tomohiro; Homma, Akihiro; Hatakeyama, Hir Author(s) Takatsugu; Iizuka, Satoshi; Onimaru, Rikiya; Tsuchiy CitationInternational Journal
Title Clinical outcomes of weekly cisplatin chemoradiother Sakashita, Tomohiro; Homma, Akihiro; Hatakeyama, Hir Author(s) Takatsugu; Iizuka, Satoshi; Onimaru, Rikiya; Tsuchiy CitationInternational Journal
Sanguineti s (2)Comment: When it was initially published in 2003 with a median follow-up of 3.8 years (4), the RTOG study led to a change in
Comment: When it was initially published in 2003 with a median follow-up of 3.8 years (4), the RTOG study led to a change in") Commento di due Soci AIRO pubblicati su due prestigiose riviste internazionali al Trial della forastiere et al. Long term results of RTOG:91-11 (a cura di Dr. Russi e Dr. Testolin )! Forastiere)et)al.)Long/Term)Results)of)RTOG)91/11:)A)Comparison)of)
Commento di due Soci AIRO pubblicati su due prestigiose riviste internazionali al Trial della forastiere et al. Long term results of RTOG:91-11 (a cura di Dr. Russi e Dr. Testolin )! Forastiere)et)al.)Long/Term)Results)of)RTOG)91/11:)A)Comparison)of)
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
T1/T2 LARYNX CANCER. Click to edit Master Presentation Date. Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery
 ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
L ARYNX S TAGING F ORM
 CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
Adenoid Cystic Carcinoma Minor Salivary Gland Origin
 Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
NEWER DRUGS IN HEAD AND NECK CANCER. Prof. Anup Majumdar. HOD, Radiotherapy, IPGMER Kolkata
 NEWER DRUGS IN HEAD AND NECK CANCER Prof. Anup Majumdar HOD, Radiotherapy, IPGMER Kolkata 1 Included Oral cavity Nasal cavity Pharynx Larynx Lymph node in upper part of neck Excluded Brain Eye Cancer arising
NEWER DRUGS IN HEAD AND NECK CANCER Prof. Anup Majumdar HOD, Radiotherapy, IPGMER Kolkata 1 Included Oral cavity Nasal cavity Pharynx Larynx Lymph node in upper part of neck Excluded Brain Eye Cancer arising
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient
 Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
and Strength of Recommendations
 ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
Neck Dissection. Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL)
, BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL)") Neck Dissection Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL) History radical neck Henry Butlin proposed enbloc removal of upper
Neck Dissection Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL) History radical neck Henry Butlin proposed enbloc removal of upper
Emerging Role of Immunotherapy in Head and Neck Cancer
 Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Surgery. Head and Neck Cancers III: Treatment and Survival. Lip. Surgery might be the only treatment
 Head and Neck Cancers III: Treatment and Survival 2004 A.D.A.M., Inc. Division of Cancer Prevention and Control NCCDPHP, CoCHP Centers for Disease Control and Prevention Atlanta, Georgia Surgery 2 Lip
Head and Neck Cancers III: Treatment and Survival 2004 A.D.A.M., Inc. Division of Cancer Prevention and Control NCCDPHP, CoCHP Centers for Disease Control and Prevention Atlanta, Georgia Surgery 2 Lip
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER
 CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience. Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore
 Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
The following images were all acquired using a CTI Biograph
 Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations
 Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S.
 Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and NeckCancer: multi-modal therapeuticintegration
 Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
External Beam Radiation Therapy for Thyroid Cancer
 External Beam Radiation Therapy for Thyroid Cancer C. Jillian Tsai, M.D, PH.D. Assistant Attending Director of Head and Neck Cancer Research Department of Radiation Oncology Memorial Sloan Kettering Cancer
External Beam Radiation Therapy for Thyroid Cancer C. Jillian Tsai, M.D, PH.D. Assistant Attending Director of Head and Neck Cancer Research Department of Radiation Oncology Memorial Sloan Kettering Cancer
Head and Neck Service
 Head and Neck Service University of California, San Francisco, Department of Radiation Oncology Residency Training Program Head and Neck and Thoracic Service Educational Objectives for PGY-5 Residents
Head and Neck Service University of California, San Francisco, Department of Radiation Oncology Residency Training Program Head and Neck and Thoracic Service Educational Objectives for PGY-5 Residents
Management of unknown primary with neck node metastasis: Current evidence
 Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad Introduction- Approach to Topic What is
Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad Introduction- Approach to Topic What is
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
Protocol of Radiotherapy for Small Cell Lung Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX
 Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX Disclosures I have nothing to disclose. 3 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX Disclosures I have nothing to disclose. 3 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
FACULTY OF MEDICINE SIRIRAJ HOSPITAL
 Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
1/14/2019 CRITICAL PATHWAYS IN HEAD AND NECK CANCER DISCLOSURES OBJECTIVES
 CRITICAL PATHWAYS IN HEAD AND NECK CANCER Caroline Nickel, MS CCC-SLP Baylor University Medical Center Dallas, Texas DISCLOSURES Caroline Nickel is employed by Baylor Institute for Rehabilitation. Caroline
CRITICAL PATHWAYS IN HEAD AND NECK CANCER Caroline Nickel, MS CCC-SLP Baylor University Medical Center Dallas, Texas DISCLOSURES Caroline Nickel is employed by Baylor Institute for Rehabilitation. Caroline
Head and Neck Cancer Service
 Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. Head and Neck Cancer Service Dr Hoda Al Booz Consultant in Clinical Oncology Bristol Cancer Institute Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. documents/
Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. Head and Neck Cancer Service Dr Hoda Al Booz Consultant in Clinical Oncology Bristol Cancer Institute Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. documents/
Indications and techniques of surgery for the primary treatment of HNSCC
 Prof. Christian Simon Chef-de-service Service d ORL et chirurgie cervico-faciale Centre Hospitalier Universitaire Vaudois (CHUV) Université de Lausanne Lausanne, Suisse Indications and techniques of surgery
Prof. Christian Simon Chef-de-service Service d ORL et chirurgie cervico-faciale Centre Hospitalier Universitaire Vaudois (CHUV) Université de Lausanne Lausanne, Suisse Indications and techniques of surgery