Image based Brachytherapy- HDR applications in Gynecological Tumors
|
|
|
- Diane Charles
- 6 years ago
- Views:
Transcription
1 Image based Brachytherapy- HDR applications in Gynecological Tumors Yakov Pipman, D. Sc. North Shore LIJ Health System
2 Sites amenable to treatment with HDR Brachytherapy GYN Breast Prostate Head and Neck Extremities Superficial lessions
3 FIGURE 2 Estimated Numbers of New Cancer Cases (Incidence) and Deaths (Mortality) in 2002 From Parkin, D. M. et al. CA Cancer J Clin 2005;55: Copyright 2005 American Cancer Society
4 FIGURE 3 Estimated Numbers of New Cancer Cases (Incidence) and Prevalent Cases (Five-year Survival) in 2002 From Parkin, D. M. et al. CA Cancer J Clin 2005;55: Copyright 2005 American Cancer Society

5 FIGURE 11 Age-standardized Incidence and Mortality Rates for Cervix Uteri Cancer From Parkin, D. M. et al. CA Cancer J Clin 2005;55: Copyright 2005 American Cancer Society
6 US statistics on Cervix Stag e 5-year Ca. (updated August 2006) IA IB1 IB2 IIA/B IIIA/B IV survival Above 95% Around 90% Around 80%- 85% Around 75%- 78% Around 47%- 50% Around 20%- 30%
7
8 BRACHYTHERAPY can be highly CONFORMAL Conforms (high) dose to the target volume for improved tumor control Conforms (low) dose to sensitive structures to reduce complications But where is the target
9 Staging of Cervix Ca. Stage 0: Carcinoma in situ. Very superficial, in the layer of cells lining the cervix, and has not invaded the cervix. Stage I: Invaded the cervix, but it has not spread anywhere else. Stage IA: Earliest form of stage I. Small and seen only under microscope. Stage IA1: Invasion less than 3 mm deep and 7 mm wide. Stage IA2: Invasion between 3 mm and 5 mm deep and less than 7 mm wide. Stage IB: Can be seen without a microscope. Also includes cancers that have spread deeper than 5 mm into connective tissue of the cervix or are wider than 7 mm and can only be seen using a microscope. Stage IB1: Visible but no larger than 4 cm Stage IB2: Visible and larger than 4 cm. Stage II: Spread beyond the cervix to nearby areas, but it is still inside the pelvic area. Stage IIA: Spread beyond the cervix to the upper part of the vagina but not in the lower third of the vagina. Stage IIB: Spread to the tissue next to the cervix (parametrial tissue). Stage III: Spread to the lower vagina or pelvic wall. May be blocking the ureters. Stage IIIA: Spread to the lower third of the vagina but not to the pelvic wall. Stage IIIB: Extends to the pelvic wall and/or blocks urine flow to the bladder. [Note: In AJCC alternate staging system is defined by spread to pelvic lymph nodes]. Stage IV: Spread to nearby organs or other parts of the body. Stage IVA: Spread to the bladder or rectum, which are organs close to the cervix. Stage IVB: Spread to distant organs beyond the pelvic area, such as the lungs.
10 US statistics on Cervix Ca. Stage IA IB1 IB2 IIA/B IIIA/B IV 5-year survival Above 95% Around 90% Around 80%- Around 75%- Around 85% 78% 47%- Around 50% 20%- 30%


11 HDR unit and source cable
12 Clinical Considerations Post Hysterectomy Intact Cervix Unresected Uterus with wide involvement Significant Lateral involvement of
13 RTOG A PHASE II STUDY OF ADJUVANT POSTOPERATIVE IRRADIATION COMBINED WITH CISPLATIN/TAXOLCHEMOTHERAP Y FOLLOWING TAH/BSO FOR PATIENTS WITH HIGH-RISK ENDOMETRIAL CANCER
14 RTOG External Radiotherapy Pelvic radiation to 45 Gy, 1.8 Gy per day, five days per week (25 fractions). Intracavitary RT boost Within two weeks after completion of external beam. Intracavitary insertions will be given with either a single low dose rate (LDR) application of 20 Gy to the vaginal surface or three high dose rate (HDR) applications to deliver an additional 18 Gy to the vaginal surface. If HDR brachytherapy is used, the three insertions should be completed before day 56. More than one insertion may be given per week.
15 RTOG 9708-Endometrium Intracavitary Radiotherapy Technique and Dose Specifications Iridium OR Cesium sources are to be used for intracavitary application(s (s) with vaginal applicators for after-loading applicator system. Preferable to treat the vaginal cuff only (treatment of the entire length of the vagina is discouraged and may increase morbidity). Not more than 2/3 of the vagina should be included in the treatment volume. Colpostats/ovoids or cylinders may be used.
16
17 RTOG 9708-Endometrium For HDR applications: Three applications of 6 Gy each prescribed to the vaginal surface. This will give a total of 18 Gy prescribed at the vaginal surface. A report of dose to rectum and bladder and vaginal surface is mandatory.
18 RTOG 9708-Endometrium Bladder dose calculated at a proximal reference point on a Foley catheter. Balloon filled with 7cm 3 of radio- opaque fluid. On the lateral radiograph, the reference point is obtained on an AP line drawn through the center of the balloon, at the posterior surface of the balloon On the AP radiograph, the reference point is taken at the center of the balloon. Rectal dose calculated by Introducing contrast material in the rectum and marking a point on the rectal wall adjacent to the applicator system or At a point 0.5 cm posterior to the vaginal ovoids or vaginal packing in the lateral projection. Vaginal surface dose calculated at the vaginal surface lateral to the midpoint of the surface of the ovoid or cylinder.
19 RTOG Endometrium protocol APPENDIX VI Definition of Bladder and Rectal Points

20 A vaginal cylinder applicator set
21 The Classic MSKCC prescription scheme for Vaginal Cylinder Applications The dose optimization point configuration on the Memorial System for a 5.0 mm in tissue prescription is defined at the midpoint of the Prescription Length. The rest of the dose optimization points taper in both directions, such that: around the hemisphere they lay at 3 mm from the surface of the dome and at the introitus the distance is reduced to zero. The Prescription Length is measured from the introitus to the tip of the
22
23
24 Two Factors affect the dose distribution at the tip of the Vaginal Cylinder The first dwell position The dose optimization points around the tip of the cylinder

25

26 Distribution superimposed on the cylinder s geometry
27 Q: How important is a small source position error in terms of dosimetry? Typical tolerance in source position is quoted as +/- 1mm. On a QA test of coincidence between radio-opaque opaque marker and source autoradiograph we detect a discrepancy of program position and marker of 1.5 mm. Simulation films indicated that the first dwell position is at 6.5 mm (center of source to tip of cylinder), while the dosimetry templates for time calculation based on a MSKCC type of loading assumed the first source position at 5.0 mm from the tip of the cylinder.
28 The dose variation at points along the cylinder axis, beyond the tip, for a cylinder of 2 cm diameter At 3.0 mm cgy At 4.0 mm 460 cgy At 4.5 mm.435 cgy At 5.0 mm 410 cgy A 1.5 mm displacement in actual source position, corresponds to an underdose at the vaginal apex of 13%. (435/500= 0.87) A: In the case of a vaginal Cylinder, not so small!

29 3D distributions for single-channel vaginal cylinder Rectal wall and bladder doses can be determined better.
30 Asymmetric vaginal cuff target



31 Modification to vaginal cylinder to treat asymmetric lesions Vaginal cylinder with 9 peripheral channels. It allows planning a biased and customized dose distribution.

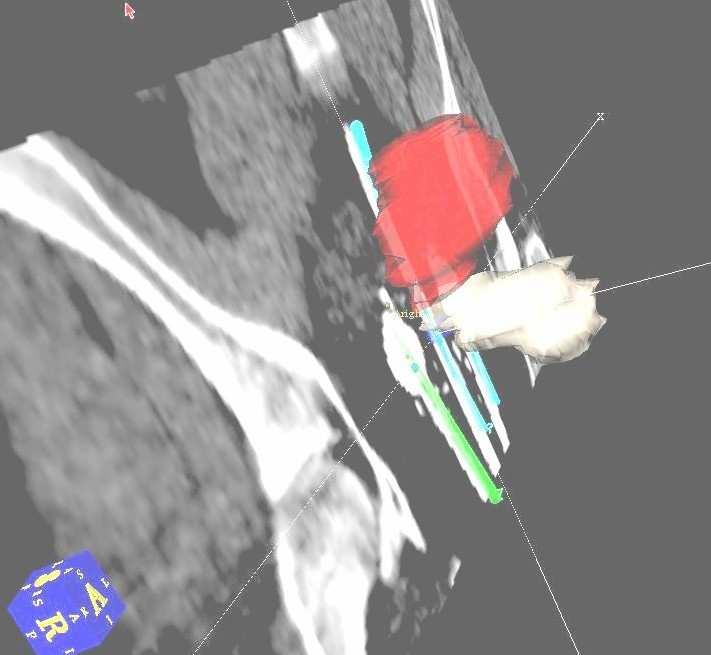
32 3D views isodoses for 9-channel 9 applicator Stand-off sleeve and differential loading allow better targeting of asymmetric target volume
33 3D view for 9-channel 9 applicator Differential loading allows biasing the distribution Dose to bladder and rectum can be reduced

34 Thick Axial red isodoses the target for 9-channel 9 while the applicator thin red is the prescribed isodose line. 150% and 200% lines are inside the cylinder
35 Intrauterine brachytherapy treatment is also shifting from LDR to HDR
36 Intrauterine brachytherapy treatment is also shifting from LDR to HDR
37 RTOG 9708-Endometrium protocol APPENDIX VI Definition of Bladder and Rectal Points

38 Rotte Applicator Sizes 2.0 cm 3.2 cm 4.0 cm 5.0 cm

39 Endometrial Dose coverage V100, V150, and V200 are documented. Since the applicator is inside the uterus, contouring is used to define the volume for calculating statistics.
40 6.5 Dose to Critical, Sensitive Structures (RTOG( 9708) Maximal doses suggested for the entire radiotherapy regimen Small bowel: 55 Gy Bladder: 70 Gy Rectum: 65 Gy Vaginal surface: 100 Gy


41 Intrauterine double tandem Rotte applicator Fibroid in the uterus caused a rotation of the applicator. Physician aborted the application.

42

43

44 CT based dosimetry with a Martinez double tandem uterine applicator

45 HDR Martinez Applicator (Lateral 3D view)

46 HDR Martinez Applicator Antero-inferior View
47

48 Henschke HDR Applicator

49 HDR Shields and source locations

:235-345.) Fig.")
50 RTOG 0417 A PHASE II STUDY OF BEVACIZUMAB IN COMBINATION WITH DEFINITIVE RADIOTHERAPY AND CISPLATIN CHEMOTHERAPY IN UNTREATED PATIENTS WITH LOCALLY ADVANCED CERVICAL CARCINOMA Recommendations for recording and reporting 3D gynecological brachytherapy Fig. 1. Schematic diagram for cervix cancer, limited disease, with GTV, high risk CTV and intermediate risk CTV for definitive treatment: coronal and transversal view(courtesy of Haie-Meder et al, Radiotherapy and Oncology 74(2005): ) Fig. 5 Schematic anatomical diagram (sagittal view) indicating the most irradiated tissue volumes adjacent to the applicator for rectum, sigmoid and bladder: 0.1, 1, and 2 cm3 (identical patient as in Figs. 1 and 2, dose volume parameters for this schematic patient example can be taken from Fig. 5). (Courtesy of Potter et al Radiotherapy and Oncology 78 (2006) 67 77)


51 Cervix and Endometrium - a case study LDR Tandem and Ovoids Placement Lateral Simulation Film. LDR planning based on orthogonal films shows normal applicator placement.

52 Cervix and Endometrium - a case study LDR planning based on orthogon al films shows normal applicat or placeme nt.

53 Cervix and Endometrium - a case study Physician had difficulty placing the Tandem applicator and decides to have CT scan. DRR shows antero- verted uterus and tandem perforation. Treatment
54

55 Second attempt with HDR applicator Physicians decide to use HDR applicator since it is smaller and easier to place. Laparoscopic pictures show that even the tandem with the largest curvature still perforates the uterus. Procedure is aborted.

56 Third Attempt A flexible plastic HDR Tandem that can adapt better to the patient s uterus, and Ovoids, are placed again under laparoscopic guidance. Better placement results in somewhat better dose coverage.
57 Extensive lateral and bulky involvement

58 Syed LDR Template (1.5mm diameter steel needles)
59 Why use the Syed-Neblett Technique? The standard Henschke or Fletcher applicators irradiate a volume that is symmetric around the tandem. Large and asymmetric target volumes may not be covered without overdosing the normal structures surrounding them. Interstitial implants using the Syed-Neblett template can be customized to irradiate asymmetric target volumes, typical in advance stage III or IV disease. Improved local control rates were reported in cases with advanced stage tumors treated with implants using the above technique.
60 Why use the CT based Syed- Neblett Technique? Film based simulation and planning are laborious. (Six hours or more) CT-based simulation and planning can be done in about 3 hours. Easier to track individual needles on CT than using radiographs. Only CT based dosimetry can correlate dose distributions with the target and normal structure volumes, such as rectum and bladder. For quite some time, Syed template based implantation for GYN were not widely performed, in spite of favorable outcome reports. Ref: CT-based planning for the Syed-Neblett Template Interstitial Gynecological implant- J. Roy, H. Gaballa, T. Ho, F. Diaz-Molina, M. Lim, L. Marin and Y. Pipman AAPM 2002
61 Syed Interstitial Brachytherapy Procedure 1. CT Simulation 2. CT/MRI Fusion 3. Physics Planning (Needles positioning and OR Guidelines) 4. Needles Placement 5. Post implant CT Based Simulation 6. Post implant physics treatment planning 7. HDR Treatments
62 Advantages of Syed LDR GYN Implant Relatively big clinical experience when compared to HDR Quite good clinical outcome with large tumors
63 Why change from LDR to HDR? -Better Treatment Planning Optimization a) Better Dose Coverage b) Less Dose Inhomogeneity within the Clinical Target Volume, i.e. lesser Hot Spots -Better monitoring of needles/implant placement during the course of treatment ( Daily CT scan of Treatment Volume) -Usually there is less chance for clinical complications related to stasis in bed, i.e. thrombophlebitis -Nursing/medical staff not exposed to radiation

64 the perception of radiation risk to personnel. This perception can lead to very real consequences.

65 Syed HDR Template 1.9 mm diameter Plastic Needles
66 Pre-OR planning Goal: Determine appropriate number of needles and source distribution pattern for the intended target volume. Syed template, mounted on a vaginal obturator, is pressed against the perineum and the CT images are acquired with contiguous 5 mm slices. The vaginal obturator controls the geometry of the vaginal surface and stabilizes the template. The axial images are transferred to the planning system the target and normal structures are outlined by the physician. The intended needle-entry entry points and needle depths are estimated based on the location of the tumor volume relative to the template and the obturator. The needle plan is used in the OR to guide the

67 Instructions for the OR Each catheter location at the template plane is a needle entry-point and marked on the template diagram. The depth of a particular needle is calculated from the distance of the catheter tip from the most caudal surface of the template. Since the needle length is known (20 cm), the length of the protruding portion out of the template is recorded for the OR.
68 OR procedure The patient is on the OR table in the lithotomy position. A Foley catheter may be inserted in the urethra for visualizing it in the post-or CT- images. The Syed-Neblett template is mounted on the vaginal obturator and the template is pushed against the perineum and sutured in place. Special flexible catheters are inserted with a metal obturator to the planned depth. Additional needles may be inserted at this time for potential use if needed. All needles are filled-in in with a removable solid plastic thread to prevent them from kinking or collapsing. Fillers are used at all times when the patient is not treated. The entry-points for the additional needles are marked on the template diagram for identification during the post-or

69 Post-OR CT-data acquisition The scanning region extends from the caudal surface of the template up to the abdomen region encompassing the bladder volume. Only dilute contrast for the bladder and the urethra should be used to reduce artifacts. The axial images are transferred into the planning system and the physician once again outlines the target and the normal structures. Catheter identification starts from the image at the template level, where entry-points are easily identified. Each catheter track is followed scan-by by-scan up to its tip. In the planning system, the pre- planned source configuration can be modified as necessary. A final plan can be obtained in about 2 hours.

70 Proper identification of the transfer tube that connects to each needle is critical! Few things are worse than a great plan when it is executed wrong!

71 HDR Dose Conformity Coronal View

72 HDR Dose Conformity- Sagital View

73 3D view

74 HDR Dose Distribution (High Conformity)
75 HDR: CTV dose CTV dose inhomogeneity and Max. Dose to the rectum are minimized Lower Hot region LDR DVH

76 LDR Dose Vol. Histogram
77 Conclusion When compared to LDR, Brachytherapy HDR Brachytherapy offers more flexibility in terms of optimizing Treatment Plans At LIJ 2004 and 2005 Statistics indicate that Fractionated HDR Treatment Schemes led to a gradual increase in the number of outpatient gynecologic brachytherapy treatments
78 Summary of CT based HDR brachytherapy Volumetric imaging, such as CT datasets, allows for target and organ delineation in 3D but it requires training in CT anatomy. Higher demands on soft tissue contrast. Enhanced knowledge of the target to be treated is required. Source/applicator position may be corrected. They require repeat CT acquisitions. Margins to the target volume, to account for uncertainties in localization, for patient repositioning and immobilization and for organ motion, typical of EBRT, are not necessary as the sources are placed directly into the tissue. Highly conformal dose distributions are similar to those achieved with IMRT, provided that the applicators or catheters are carefully placed. While inhomogeneities are higher than in EBRT, they can be kept within the target and at a clinically safe level.
Definitions. Brachytherapy in treatment of cancer. Implantation Techniques and Methods of Dose Specifications. Importance of Brachytherapy in GYN
 Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
GYNECOLOGIC CANCER and RADIATION THERAPY. Jon Anders M.D. Radiation Oncology
 GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
 https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป
 ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w
 Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w Quality assurance Classical implant systems w Manchester
Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w Quality assurance Classical implant systems w Manchester
Brachytherapy Planning and Quality Assurance
 Brachytherapy Planning and Quality Assurance Classical implant systems Most common clinical applications and modern dosimetry methods Quality assurance Classical implant systems Manchester (Paterson-Parker)
Brachytherapy Planning and Quality Assurance Classical implant systems Most common clinical applications and modern dosimetry methods Quality assurance Classical implant systems Manchester (Paterson-Parker)
Brachytherapy an Overview
 Brachytherapy an Overview Yakov Pipman, D Sc North Shore LIJ Health System Monterrey, Nov30-Dec1, 2007 Brachytherapy A procedure in therapeutic radiology that involves the irradiation of a target with
Brachytherapy an Overview Yakov Pipman, D Sc North Shore LIJ Health System Monterrey, Nov30-Dec1, 2007 Brachytherapy A procedure in therapeutic radiology that involves the irradiation of a target with
The New ICRU/GEC ESTRO Report in Clinical Practice. Disclosures
 The New ICRU/GEC ESTRO Report in Clinical Practice Christian Kirisits, MSc, PhD; Richard Pötter, MD Medical University of Vienna, Vienna, Austria On behalf of the Committee: B. Erickson, C. Haie Meder,
The New ICRU/GEC ESTRO Report in Clinical Practice Christian Kirisits, MSc, PhD; Richard Pötter, MD Medical University of Vienna, Vienna, Austria On behalf of the Committee: B. Erickson, C. Haie Meder,
3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER
 SAUDI JOURNAL OF OBSTETRICS AND GYNECOLOGY VOLUME 11 NO. 2 1430 H - 2009 G 3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER DR YASIR BAHADUR 1, DR CAMELIA CONSTANTINESCU 2,
SAUDI JOURNAL OF OBSTETRICS AND GYNECOLOGY VOLUME 11 NO. 2 1430 H - 2009 G 3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER DR YASIR BAHADUR 1, DR CAMELIA CONSTANTINESCU 2,
MRI Guided GYN Brachytherapy: Clinical Considerations
 MRI Guided GYN Brachytherapy: Clinical Considerations AAPM Junzo Chino MD Duke Radiation Oncology 8/8/2013 Disclosures none Learning Objectives Historical Context: Film based Brachytherapy Advantages of
MRI Guided GYN Brachytherapy: Clinical Considerations AAPM Junzo Chino MD Duke Radiation Oncology 8/8/2013 Disclosures none Learning Objectives Historical Context: Film based Brachytherapy Advantages of
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005 Advantages of inflatable multichannel endorectal applicator in the neo-adjuvant treatment of patients with locally advanced
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005 Advantages of inflatable multichannel endorectal applicator in the neo-adjuvant treatment of patients with locally advanced
ARROCase: Locally Advanced Endometrial Cancer
 ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
INTRODUCTION PATIENT. J. Radiat. Res., 52, (2011)
") J. Radiat. Res., 52, 54 58 (2011) Regular Paper Intracavitary Combined with CT-guided Interstitial Brachytherapy for Locally Advanced Uterine Cervical Cancer: Introduction of the Technique and a Case Presentation
J. Radiat. Res., 52, 54 58 (2011) Regular Paper Intracavitary Combined with CT-guided Interstitial Brachytherapy for Locally Advanced Uterine Cervical Cancer: Introduction of the Technique and a Case Presentation
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer
 for Gynaecological Cancer") Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring)
") Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Outline - MRI - CT - US. - Combinations of imaging modalities for treatment planning
 Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Advances in Gynecologic Brachytherapy
 Advances in Gynecologic Brachytherapy Anuj V Peddada, M.D. Director Department of Radiation Oncology Penrose Cancer Center Colorado Springs, CO USA Brachytherapy Issues in Gyn/onc Cervix Endometrial Rational
Advances in Gynecologic Brachytherapy Anuj V Peddada, M.D. Director Department of Radiation Oncology Penrose Cancer Center Colorado Springs, CO USA Brachytherapy Issues in Gyn/onc Cervix Endometrial Rational
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
MR-Guided Brachytherapy
 MR-Guided Brachytherapy Joann I. Prisciandaro, Ph.D. The Department of Radiation Oncology University of Michigan Outline Traditional 2D technique for brachytherapy treatment planning Transition to MR-guided
MR-Guided Brachytherapy Joann I. Prisciandaro, Ph.D. The Department of Radiation Oncology University of Michigan Outline Traditional 2D technique for brachytherapy treatment planning Transition to MR-guided
Interstitial Brachytherapy. Low dose rate brachytherapy. Brachytherapy alone cures some cervical cancer. Learning Objectives
 Interstitial Learning Objectives To discuss practical aspects of selection and insertion techniques for interstitial brachytherapy and their relation to clinical trials Akila Viswanathan, MD MPH Johns
Interstitial Learning Objectives To discuss practical aspects of selection and insertion techniques for interstitial brachytherapy and their relation to clinical trials Akila Viswanathan, MD MPH Johns
Staging and Treatment Update for Gynecologic Malignancies
 Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Basic Fundamentals & Tricks of the Trade for Intracavitary Radiotherapy for Cervix Cancer. Paula A. Berner, B.S., CMD, FAAMD
 Basic Fundamentals & Tricks of the Trade for Intracavitary Radiotherapy for Cervix Cancer Paula A. Berner, B.S., CMD, FAAMD Conflicts of Interest None to disclose Equipment Philips Healthcare, USA Nucletron
Basic Fundamentals & Tricks of the Trade for Intracavitary Radiotherapy for Cervix Cancer Paula A. Berner, B.S., CMD, FAAMD Conflicts of Interest None to disclose Equipment Philips Healthcare, USA Nucletron
Challenging Cases in Cervical Cancer: Parametrial Boosting. Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin
 Challenging Cases in Cervical Cancer: Parametrial Boosting Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin Disclosure Chart Rounds participant No COI Learning Objectives Discuss the challenges
Challenging Cases in Cervical Cancer: Parametrial Boosting Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin Disclosure Chart Rounds participant No COI Learning Objectives Discuss the challenges
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy
 Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
University of Kentucky. Markey Cancer Center
 University of Kentucky Markey Cancer Center Invasive Cancer of the Vagina and Urethra Fred Ueland, MD No matter what you accomplish in your life, the size of your funeral will still be determined by the
University of Kentucky Markey Cancer Center Invasive Cancer of the Vagina and Urethra Fred Ueland, MD No matter what you accomplish in your life, the size of your funeral will still be determined by the
Basics of Cervix Cancer Brachytherapy
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Cancer Brachytherapy David Gaffney MDPhD, FASTRO, FACR University of Utah Huntsman Cancer Institute Incidence Cervix: 445,000
Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Cancer Brachytherapy David Gaffney MDPhD, FASTRO, FACR University of Utah Huntsman Cancer Institute Incidence Cervix: 445,000
presenting Brachytherapy with focus on Gynecological Cancers
 Good Afternoon I am Bulent Aydogan and I will be presenting Brachytherapy with focus on Gynecological Cancers 1 I have nothing to disclose 2 3 4 Now IstheQuiztime time 5 6 7 Brachtheray has a long history
Good Afternoon I am Bulent Aydogan and I will be presenting Brachytherapy with focus on Gynecological Cancers 1 I have nothing to disclose 2 3 4 Now IstheQuiztime time 5 6 7 Brachtheray has a long history
CT Guided Contouring: Challenges and Pitfalls
 CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
2015 Radiology Coding Survival Guide
 2015 Radiology Coding Survival Guide Chapter 31: Clinical Brachytherapy (77750-77799) Clinical brachytherapy involves applying radioelements into or around a treatment field. CPT guidelines clarify that
2015 Radiology Coding Survival Guide Chapter 31: Clinical Brachytherapy (77750-77799) Clinical brachytherapy involves applying radioelements into or around a treatment field. CPT guidelines clarify that
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer
 A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
Version A European study on MRI-guided brachytherapy in locally advanced cervical cancer EMBRACE (ENDORSED BY GEC ESTRO)
") A European study on MRI-guided brachytherapy in locally advanced cervical cancer EMBRACE (ENDORSED BY GEC ESTRO) 1 Contents: 1. ABBREVIATIONS... 4 2. SUMMARY... 5 3. INTRODUCTION AND PRINCIPLES OF IMAGE
A European study on MRI-guided brachytherapy in locally advanced cervical cancer EMBRACE (ENDORSED BY GEC ESTRO) 1 Contents: 1. ABBREVIATIONS... 4 2. SUMMARY... 5 3. INTRODUCTION AND PRINCIPLES OF IMAGE
Advances in Image-guided Brachytherapy
 Advances in Image-guided Brachytherapy Hospital Authority Convention 2016 Terry Wong, Physicist Department of Medical Physics Pamela Youde Nethersole Eastern Hospital Introduction What is Brachytherapy?
Advances in Image-guided Brachytherapy Hospital Authority Convention 2016 Terry Wong, Physicist Department of Medical Physics Pamela Youde Nethersole Eastern Hospital Introduction What is Brachytherapy?
Changing Paradigms in Radiotherapy
 Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
IMRT - the physician s eye-view. Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia
 IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical
 The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical sites. The final aim will be to be able to make out these
The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical sites. The final aim will be to be able to make out these
How ICD-10 Affects Radiation Oncology. Presented by, Lashelle Bolton CPC, COC, CPC-I, CPMA
 How ICD-10 Affects Radiation Oncology Presented by, Lashelle Bolton CPC, COC, CPC-I, CPMA ICD-10 ICD-10-CM has added new challenges to the radiation oncology specialty. Approximately 220 ICD-9-CM codes
How ICD-10 Affects Radiation Oncology Presented by, Lashelle Bolton CPC, COC, CPC-I, CPMA ICD-10 ICD-10-CM has added new challenges to the radiation oncology specialty. Approximately 220 ICD-9-CM codes
Pulsed Dose Rate for GYN Brachytherapy
 Pulsed Dose Rate for GYN Brachytherapy Firas Mourtada,, Ph.D. Department of Radiation Physics Dose equivalency to LDR Brief Introduction Radiobiology Dose Distribution: Radial dose function Source anisotropy
Pulsed Dose Rate for GYN Brachytherapy Firas Mourtada,, Ph.D. Department of Radiation Physics Dose equivalency to LDR Brief Introduction Radiobiology Dose Distribution: Radial dose function Source anisotropy
Course Directors: Teaching Staff: Guest Lecturers: Local Organiser: ESTRO coordinator: Melissa Vanderijst, project manager (BE)
") ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2017 Course Directors: Richard
ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2017 Course Directors: Richard
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
Original Article ABSTRACT INTRODUCTION
 Original Article Free full text available from www.cancerjournal.net Significance of ovoid separation with various applications of high-dose-rate-intracavitary radiotherapy in carcinoma of uterine cervix:
Original Article Free full text available from www.cancerjournal.net Significance of ovoid separation with various applications of high-dose-rate-intracavitary radiotherapy in carcinoma of uterine cervix:
Trina Lynd, M.S. Medical Physicist Lifefirst Imaging & Oncology Cullman, AL Tri-State Alabama, Louisiana and Mississippi Spring 2016 Meeting April
 Trina Lynd, M.S. Medical Physicist Lifefirst Imaging & Oncology Cullman, AL Tri-State Alabama, Louisiana and Mississippi Spring 2016 Meeting April 17, 2016 Discuss permanent prostate brachytherapy and
Trina Lynd, M.S. Medical Physicist Lifefirst Imaging & Oncology Cullman, AL Tri-State Alabama, Louisiana and Mississippi Spring 2016 Meeting April 17, 2016 Discuss permanent prostate brachytherapy and
20 Prostate Cancer Dan Ash
 20 Prostate Cancer Dan Ash 1 Introduction Prostate cancer is a disease of ageing men for which the aetiology remains unknown. The incidence rises up to 30 to 40% in men over 80. The symptoms of localised
20 Prostate Cancer Dan Ash 1 Introduction Prostate cancer is a disease of ageing men for which the aetiology remains unknown. The incidence rises up to 30 to 40% in men over 80. The symptoms of localised
The Evolution of RT Techniques for Gynaecological Cancers in a developing country context
 The Evolution of RT Techniques for Gynaecological Cancers in a developing country context Hannah Simonds Stellenbosch University/ Tygerberg Academic Hospital ESMO Africa 2017 I have no disclosures External
The Evolution of RT Techniques for Gynaecological Cancers in a developing country context Hannah Simonds Stellenbosch University/ Tygerberg Academic Hospital ESMO Africa 2017 I have no disclosures External
MRI Based treatment planning for with focus on prostate cancer. Xinglei Shen, MD Department of Radiation Oncology KUMC
 MRI Based treatment planning for with focus on prostate cancer Xinglei Shen, MD Department of Radiation Oncology KUMC Overview How magnetic resonance imaging works (very simple version) Indications for
MRI Based treatment planning for with focus on prostate cancer Xinglei Shen, MD Department of Radiation Oncology KUMC Overview How magnetic resonance imaging works (very simple version) Indications for
Image guided brachytherapy in cervical cancer Clinical Aspects
 Image guided brachytherapy in cervical cancer Clinical Aspects Richard Pötter MD Department of Radiation Oncology, Medical University of Vienna, Austria ICARO-2, IAEA, Vienna, June, 22, 2017 Outline Tumor
Image guided brachytherapy in cervical cancer Clinical Aspects Richard Pötter MD Department of Radiation Oncology, Medical University of Vienna, Austria ICARO-2, IAEA, Vienna, June, 22, 2017 Outline Tumor
Dose-Volume Histogram Analysis in Point A-based Dose Prescription of High-dose-rate Brachytherapy for Cervical Carcinoma
 Showa Univ J Med Sci 30 2, 227 235, June 2018 Original Dose-Volume Histogram Analysis in Point A-based Dose Prescription of High-dose-rate Brachytherapy for Cervical Carcinoma Rei KOBAYASHI 1, Yoshikazu
Showa Univ J Med Sci 30 2, 227 235, June 2018 Original Dose-Volume Histogram Analysis in Point A-based Dose Prescription of High-dose-rate Brachytherapy for Cervical Carcinoma Rei KOBAYASHI 1, Yoshikazu
HDR Brachytherapy: Results and Future Studies in Monotherapy
 HDR Brachytherapy: Results and Future Studies in Monotherapy Nikolaos Zamboglou and Nikolaos Tselis Strahlenklinik Klinikum Offenbach - Germany Prostate Brachytherapy UK & Ireland Conference 2013 Comparison
HDR Brachytherapy: Results and Future Studies in Monotherapy Nikolaos Zamboglou and Nikolaos Tselis Strahlenklinik Klinikum Offenbach - Germany Prostate Brachytherapy UK & Ireland Conference 2013 Comparison
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Quality management for Breast Brachytherapy.
 Quality management for Breast Brachytherapy. DORIN TODOR, Ph.D. Medical College of Virginia Campus Department of Radiation Oncology New England AAPM Chapter 2012 Summer Meeting, Providence, RI Quality
Quality management for Breast Brachytherapy. DORIN TODOR, Ph.D. Medical College of Virginia Campus Department of Radiation Oncology New England AAPM Chapter 2012 Summer Meeting, Providence, RI Quality
Course Directors: Teaching Staff: Guest Lecturers: Local Organiser: ESTRO coordinator: Melissa Vanderijst, project manager (BE)
") ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2016 Course Directors: Richard
ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2016 Course Directors: Richard
Dosimetric comparison of interstitial brachytherapy with multi-channel vaginal cylinder plans in patients with vaginal tumors
 Mendez et al. Radiation Oncology (2017) 12:84 DOI 10.1186/s13014-017-0821-0 RESEARCH Open Access Dosimetric comparison of interstitial brachytherapy with multi-channel vaginal cylinder plans in patients
Mendez et al. Radiation Oncology (2017) 12:84 DOI 10.1186/s13014-017-0821-0 RESEARCH Open Access Dosimetric comparison of interstitial brachytherapy with multi-channel vaginal cylinder plans in patients
A Study on Dosimetry of Gynaecological Cancer and Quality Assurance of HDR Brachytherapy in BPKMCH, Nepal
 A Study on Dosimetry of Gynaecological Cancer and Quality Assurance of HDR Brachytherapy in BPKMCH, Nepal SB Chand, PP Chaursia, MP Adhikary, AK Jha, and S Shrestha Dept. of Radiation Oncology, BPKM Cancer
A Study on Dosimetry of Gynaecological Cancer and Quality Assurance of HDR Brachytherapy in BPKMCH, Nepal SB Chand, PP Chaursia, MP Adhikary, AK Jha, and S Shrestha Dept. of Radiation Oncology, BPKM Cancer
PROSTATE CANCER BRACHYTHERAPY. Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College
 PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
NIA MAGELLAN HEALTH RADIATION ONCOLOGY CODING STANDARD. Dosimetry Planning
 NIA MAGELLAN HEALTH RADIATION ONCOLOGY CODING STANDARD Dosimetry Planning CPT Codes: 77295, 77300, 77301, 77306, 77307, 77321, 77316, 77317, 77318, 77331, 77399 Original Date: April, 2011 Last Reviewed
NIA MAGELLAN HEALTH RADIATION ONCOLOGY CODING STANDARD Dosimetry Planning CPT Codes: 77295, 77300, 77301, 77306, 77307, 77321, 77316, 77317, 77318, 77331, 77399 Original Date: April, 2011 Last Reviewed
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer?
 Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas Dept. of Medical Physics & Engineering, Strahlenklinik, Klinikum Offenbach GmbH 63069 Offenbach, Germany
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas Dept. of Medical Physics & Engineering, Strahlenklinik, Klinikum Offenbach GmbH 63069 Offenbach, Germany
Modern Interstitial GYN Brachytherapy. Conflicts: 8/3/2016. Modern Interstitial GYN Brachytherapy. 1. Use of MR
 Advances and Innovations in Image-Guided Brachytherapy Modern Interstitial GYN Brachytherapy Antonio Damato, PhD Brigham and Women s Hospital Conflicts: Travel grant from Elekta Consulting agreement with
Advances and Innovations in Image-Guided Brachytherapy Modern Interstitial GYN Brachytherapy Antonio Damato, PhD Brigham and Women s Hospital Conflicts: Travel grant from Elekta Consulting agreement with
Original Date: June 2013 Page 1 of 7 Radiation Oncology Last Review Date: September Implementation Date: December 2014 Clinical Operations
 National Imaging Associates, Inc. Clinical guideline CERVICAL CANCER Original Date: June 2013 Page 1 of 7 Radiation Oncology Last Review Date: September 2014 Guideline Number: NIA_CG_223 Last Revised Date:
National Imaging Associates, Inc. Clinical guideline CERVICAL CANCER Original Date: June 2013 Page 1 of 7 Radiation Oncology Last Review Date: September 2014 Guideline Number: NIA_CG_223 Last Revised Date:
Role of IMRT in the Treatment of Gynecologic Malignancies. John C. Roeske, PhD Associate Professor The University of Chicago
 Role of IMRT in the Treatment of Gynecologic Malignancies John C. Roeske, PhD Associate Professor The University of Chicago Acknowledgements B Aydogan, PhD Univ of Chicago P Chan, MD Princess Margaret
Role of IMRT in the Treatment of Gynecologic Malignancies John C. Roeske, PhD Associate Professor The University of Chicago Acknowledgements B Aydogan, PhD Univ of Chicago P Chan, MD Princess Margaret
KEY WORDS: Carcinoma cervix, high-dose-rate brachytherapy, radiotherapy
 Technical Report Free full text available from www.cancerjournal.net Vandana S Jain, Mukund B Sarje, Kailash K Singh, R Umberkar, Rajeev Shrivastava, Shailendra M Jain Department of Radiotherapy and Clinical
Technical Report Free full text available from www.cancerjournal.net Vandana S Jain, Mukund B Sarje, Kailash K Singh, R Umberkar, Rajeev Shrivastava, Shailendra M Jain Department of Radiotherapy and Clinical
Abstract Purpose: Material and methods: Results: Conclusions: Key words: Purpose Address for correspondence:
 Original paper Physics Contributions The impact of activating source dwell positions outside the CTV on the dose to treated normal tissue volumes in TRUS guided 3D conformal interstitial HDR brachytherapy
Original paper Physics Contributions The impact of activating source dwell positions outside the CTV on the dose to treated normal tissue volumes in TRUS guided 3D conformal interstitial HDR brachytherapy
CT Guided Contouring: Challenges and Pitfalls
 CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
The Role of Radiation in the Management of Gynecologic Cancers. Scott Glaser, MD
 The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD Nothing to disclose DISCLOSURE Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical
The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD Nothing to disclose DISCLOSURE Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical
TRANS-TASMAN RADIATION ONCOLOGY GROUP INC. Quality Assurance. Treatment Planning Benchmark
 TRANS-TASMAN RADIATION ONCOLOGY GROUP INC. Quality Assurance Treatment Planning Benchmark PORTEC-3/ TROG 08.04 Randomised Phase III Trial Comparing Concurrent Chemoradiation and Adjuvant Chemotherapy with
TRANS-TASMAN RADIATION ONCOLOGY GROUP INC. Quality Assurance Treatment Planning Benchmark PORTEC-3/ TROG 08.04 Randomised Phase III Trial Comparing Concurrent Chemoradiation and Adjuvant Chemotherapy with
Basics of Cervix Brachytherapy. William Small, Jr., MD Professor and Chairman Loyola University Chicago
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Brachytherapy William Small, Jr., MD Professor and Chairman Loyola University Chicago Cervix Cancer Education Symposium, January
Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Brachytherapy William Small, Jr., MD Professor and Chairman Loyola University Chicago Cervix Cancer Education Symposium, January
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
IMRT for Prostate Cancer
 IMRT for Cancer All patients are simulated in the supine position. Reproducibility is achieved using a custom alpha cradle cast that extends from the mid-back to mid-thigh. The feet are positioned in a
IMRT for Cancer All patients are simulated in the supine position. Reproducibility is achieved using a custom alpha cradle cast that extends from the mid-back to mid-thigh. The feet are positioned in a
Gynecologic Vaginal Brachytherapy (Mostly Post-Op Endometrial)
") Gynecologic Vaginal Brachytherapy (Mostly Post-Op Endometrial) D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director Brachytherapy UCLA David Geffen School of Medicine Brachytherapy 11 (2012) 58-67 1 Manual
Gynecologic Vaginal Brachytherapy (Mostly Post-Op Endometrial) D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director Brachytherapy UCLA David Geffen School of Medicine Brachytherapy 11 (2012) 58-67 1 Manual
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
Venezia Advanced Gynecological Applicator Reaching beyond
 Venezia Advanced Gynecological Applicator Reaching beyond Advanced Gynecological Applicator Venezia is FDA cleared and CE marked, but is not available in all markets. 1 Helping clinicians improve patients
Venezia Advanced Gynecological Applicator Reaching beyond Advanced Gynecological Applicator Venezia is FDA cleared and CE marked, but is not available in all markets. 1 Helping clinicians improve patients
Proposed All Wales Vulval Cancer Guidelines. Dr Amanda Tristram
 Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
A B S T R A C T. 1. Introduction
 Using Digitally Reconstructed Radiographs from MRI (MRI-DRR) to Localize Pelvic Lymph Nodes on 2D X-ray Simulator-Based Brachytherapy Treatment Planning Mohammad Ali Oghabian *1, Reza Riazi 2, Esmail Parsai
Using Digitally Reconstructed Radiographs from MRI (MRI-DRR) to Localize Pelvic Lymph Nodes on 2D X-ray Simulator-Based Brachytherapy Treatment Planning Mohammad Ali Oghabian *1, Reza Riazi 2, Esmail Parsai
HDR Applicators and Dosimetry*
 HDR Applicators and Dosimetry* Jason Rownd, MS Medical College of Wisconsin *with a too much radiobiology Objectives Review the radiobiology of brachytherapy-linear quadratic model. Understand how to convert
HDR Applicators and Dosimetry* Jason Rownd, MS Medical College of Wisconsin *with a too much radiobiology Objectives Review the radiobiology of brachytherapy-linear quadratic model. Understand how to convert
HDR Brachytherapy I: Overview of Clinical Application and QA. Disclosures. Learning Objectives 7/23/2014. Consultant, Varian Medical Systems
 HDR Brachytherapy I: Overview of Clinical Application and QA Timothy Showalter, MD Associate Professor tns3b@virginia.edu Disclosures Consultant, Varian Medical Systems Learning Objectives To understand
HDR Brachytherapy I: Overview of Clinical Application and QA Timothy Showalter, MD Associate Professor tns3b@virginia.edu Disclosures Consultant, Varian Medical Systems Learning Objectives To understand
Outline. Contour quality control. Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT)
") Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT) James Kavanaugh, MS DABR Department of Radiation Oncology Division of Medical Physics Outline Importance
Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT) James Kavanaugh, MS DABR Department of Radiation Oncology Division of Medical Physics Outline Importance
Review of brachytherapy in
 Medical Physics in the Baltic States 2017 Review of brachytherapy in Klaipėda University Hospital Romas Vilkas Rasa Dagienė Klaipėda University Hospital 1 Aims of presentation: To show progress of brachytherapy
Medical Physics in the Baltic States 2017 Review of brachytherapy in Klaipėda University Hospital Romas Vilkas Rasa Dagienė Klaipėda University Hospital 1 Aims of presentation: To show progress of brachytherapy
Does the apex optimization line matter for single-channel vaginal cylinder brachytherapy planning?
 Received: 24 May 2017 Revised: 2 April 2018 Accepted: 5 April 2018 DOI: 10.1002/acm2.12351 TECHNICAL NOTE Does the apex optimization line matter for single-channel vaginal cylinder brachytherapy planning?
Received: 24 May 2017 Revised: 2 April 2018 Accepted: 5 April 2018 DOI: 10.1002/acm2.12351 TECHNICAL NOTE Does the apex optimization line matter for single-channel vaginal cylinder brachytherapy planning?
Assessment of air pockets in high-dose-rate vaginal cuff brachytherapy using cylindrical applicators
 Original paper Clinical Investigations Assessment of air pockets in high-dose-rate vaginal cuff brachytherapy using cylindrical applicators Ashraf Hassouna, MD 1,2, Prof. Yasir Abdulaziz Bahadur 3, Camelia
Original paper Clinical Investigations Assessment of air pockets in high-dose-rate vaginal cuff brachytherapy using cylindrical applicators Ashraf Hassouna, MD 1,2, Prof. Yasir Abdulaziz Bahadur 3, Camelia
3D CONFORMATIONAL INTERSTITIAL BRACHYTHERAPY PLANNING FOR SOFT TISSUE SARCOMA
 3D CONFORMATIONAL INTERSTITIAL BRACHYTHERAPY PLANNING FOR SOFT TISSUE SARCOMA Alina TĂNASE 1,3, M. DUMITRACHE 2,3, O. FLOREA 1 1 Emergency Central Military Hospital Dr. Carol Davila Bucharest, Romania,
3D CONFORMATIONAL INTERSTITIAL BRACHYTHERAPY PLANNING FOR SOFT TISSUE SARCOMA Alina TĂNASE 1,3, M. DUMITRACHE 2,3, O. FLOREA 1 1 Emergency Central Military Hospital Dr. Carol Davila Bucharest, Romania,
Brachytherapy in Africa
 Brachytherapy in Africa Deanine Halliman PhD Sr. Director Medical Affairs Elekta Brachytherapy Burden of cervical cancer in Africa est. 2012 incidence per 100,000 women Bouassa M, et al. Cervical cancer
Brachytherapy in Africa Deanine Halliman PhD Sr. Director Medical Affairs Elekta Brachytherapy Burden of cervical cancer in Africa est. 2012 incidence per 100,000 women Bouassa M, et al. Cervical cancer
GYN GEC-ESTRO/ICRU 89 Target Concept. Richard Pötter Medical University Vienna
 GYN GEC-ESTRO/ICRU 89 Target Concept Richard Pötter Medical University Vienna GYN GEC ESTRO RECOMMENDATIONS-BACKGROUND From 2D to 3D/4D Historical difficulties in communicating results of cervical BT due
GYN GEC-ESTRO/ICRU 89 Target Concept Richard Pötter Medical University Vienna GYN GEC ESTRO RECOMMENDATIONS-BACKGROUND From 2D to 3D/4D Historical difficulties in communicating results of cervical BT due
Course Directors : Teaching Staff : Guest Lecturer: Local Organiser: ESTRO coordinators: Melissa Vanderijst and Marta Jayes, project managers (BEL)
") ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Florence, Italy 28 September -2 October 2014 Course Directors
ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Florence, Italy 28 September -2 October 2014 Course Directors
IGRT Solution for the Living Patient and the Dynamic Treatment Problem
 IGRT Solution for the Living Patient and the Dynamic Treatment Problem Lei Dong, Ph.D. Associate Professor Dept. of Radiation Physics University of Texas M. D. Anderson Cancer Center Houston, Texas Learning
IGRT Solution for the Living Patient and the Dynamic Treatment Problem Lei Dong, Ph.D. Associate Professor Dept. of Radiation Physics University of Texas M. D. Anderson Cancer Center Houston, Texas Learning
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
Patterns of Care in Patients with Cervical Cancer:
 Patterns of Care in Patients with Cervical Cancer: Power and Pitfalls of Claims-Based Analysis Grace Smith, MD, PhD, MPH Resident, PGY-5 Department of Radiation Oncology, MD Anderson Cancer Center Acknowledgments
Patterns of Care in Patients with Cervical Cancer: Power and Pitfalls of Claims-Based Analysis Grace Smith, MD, PhD, MPH Resident, PGY-5 Department of Radiation Oncology, MD Anderson Cancer Center Acknowledgments
Bladder and rectum dose estimations on digitized radiographs for vaginal brachytherapy after hysterectomy
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 15, NUMBER 6, 2014 Bladder and rectum dose estimations on digitized radiographs for vaginal brachytherapy after hysterectomy Winson Zhang, 1 Sudershan
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 15, NUMBER 6, 2014 Bladder and rectum dose estimations on digitized radiographs for vaginal brachytherapy after hysterectomy Winson Zhang, 1 Sudershan
Intracavitary + Interstitial Techniques Rationale
 Vienna, 14. 15. May, 2018 Intracavitary + Interstitial Techniques Rationale Primoz Petric NCCCR, HMC, Doha Dimensions of prescribed dose: different levels Prescribed dose Standard loading Modified loading
Vienna, 14. 15. May, 2018 Intracavitary + Interstitial Techniques Rationale Primoz Petric NCCCR, HMC, Doha Dimensions of prescribed dose: different levels Prescribed dose Standard loading Modified loading
Quality Assurance of Ultrasound Imaging in Radiation Therapy. Zuofeng Li, D.Sc. Murty S. Goddu, Ph.D. Washington University St.
 Quality Assurance of Ultrasound Imaging in Radiation Therapy Zuofeng Li, D.Sc. Murty S. Goddu, Ph.D. Washington University St. Louis, Missouri Typical Applications of Ultrasound Imaging in Radiation Therapy
Quality Assurance of Ultrasound Imaging in Radiation Therapy Zuofeng Li, D.Sc. Murty S. Goddu, Ph.D. Washington University St. Louis, Missouri Typical Applications of Ultrasound Imaging in Radiation Therapy
Linking DVH-parameters to clinical outcome. Richard Pötter, Medical University of Vienna, General Hospital of Vienna, Austria
 Linking DVH-parameters to clinical outcome Richard Pötter, Medical University of Vienna, General Hospital of Vienna, Austria Outline DVH parameters for HR CTV (D90) and OAR (2 ccm) simple integration of
Linking DVH-parameters to clinical outcome Richard Pötter, Medical University of Vienna, General Hospital of Vienna, Austria Outline DVH parameters for HR CTV (D90) and OAR (2 ccm) simple integration of
Three fraction high dose rate brachytherapy schedule for treatment of locally advanced uterine cervix cancer center:
 Huerta et al, Cancerología 3 (008): 105-110 Three fraction high dose rate brachytherapy schedule for treatment of locally advanced uterine cervix cancer center: Clinical results, emphasis in dosimetric
Huerta et al, Cancerología 3 (008): 105-110 Three fraction high dose rate brachytherapy schedule for treatment of locally advanced uterine cervix cancer center: Clinical results, emphasis in dosimetric
Patient Safety Focused QA. LDR Brachytherapy Vrinda Narayana
 Patient Safety Focused QA LDR Brachytherapy Vrinda Narayana D < 2 Gy/h Old LDR Brachytherapy? Ra-226; Cs-137; Ir-192 New Gynecological; interstitial Pd-103; I-125; Cs-131 Prostate implants Eye plaques
Patient Safety Focused QA LDR Brachytherapy Vrinda Narayana D < 2 Gy/h Old LDR Brachytherapy? Ra-226; Cs-137; Ir-192 New Gynecological; interstitial Pd-103; I-125; Cs-131 Prostate implants Eye plaques
National Medical Policy
 National Medical Policy Subject: Policy Number: Brachytherapy for Gynecological Cancer NMP454 Effective Date*: May 2009 Updated: July 2015 This National Medical Policy is subject to the terms in the IMPORTANT
National Medical Policy Subject: Policy Number: Brachytherapy for Gynecological Cancer NMP454 Effective Date*: May 2009 Updated: July 2015 This National Medical Policy is subject to the terms in the IMPORTANT
NSABP PROTOCOL B-39B RTOG PROTOCOL 0413
 NSABP PROTOCOL B-39B RTOG PROTOCOL 0413 (A RANDOMIZED PHASE III STUDY OF CONVENTIONAL WHOLE BREAST IRRADIATION WBI) VERSUS PARTIAL BREAST IRRADIATION (PBI) FOR WOMEN WITH STAGE 0, I, OR II BREAST CANCER
NSABP PROTOCOL B-39B RTOG PROTOCOL 0413 (A RANDOMIZED PHASE III STUDY OF CONVENTIONAL WHOLE BREAST IRRADIATION WBI) VERSUS PARTIAL BREAST IRRADIATION (PBI) FOR WOMEN WITH STAGE 0, I, OR II BREAST CANCER
ART for Cervical Cancer: Dosimetry and Technical Aspects
 ART for Cervical Cancer: Dosimetry and Technical Aspects D.A. Jaffray, Ph.D. Radiation Therapy Physics Princess Margaret Cancer Centre/Techna/Ontario Cancer Institute Professor Departments of Radiation
ART for Cervical Cancer: Dosimetry and Technical Aspects D.A. Jaffray, Ph.D. Radiation Therapy Physics Princess Margaret Cancer Centre/Techna/Ontario Cancer Institute Professor Departments of Radiation
Role of MRI in Intracavitary Brachytherapy for Cervical Cancer: What the Radiologist Needs to Know
 Women s Imaging Pictorial Essay Beddy et al. MRI-Guided Brachytherapy for Cervical Cancer Women s Imaging Pictorial Essay WOMEN S IMAGING Peter Beddy 1 R. Deepa Rangarajan Evis Sala Beddy P, Rangarajan
Women s Imaging Pictorial Essay Beddy et al. MRI-Guided Brachytherapy for Cervical Cancer Women s Imaging Pictorial Essay WOMEN S IMAGING Peter Beddy 1 R. Deepa Rangarajan Evis Sala Beddy P, Rangarajan
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS
 THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
PORTEC-4. Patient seqnr. Age at inclusion (years) Hospital:
 Hospital:") May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
Use of imaging systems for patient modeling - PET and SPECT
 Use of imaging systems for patient modeling - PET and SPECT Sasa Mutic Department of Radiation Oncology Siteman Cancer Center Mallinckrodt Institute of Radiology Washington University School of Medicine
Use of imaging systems for patient modeling - PET and SPECT Sasa Mutic Department of Radiation Oncology Siteman Cancer Center Mallinckrodt Institute of Radiology Washington University School of Medicine
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer?
 Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas 1,3, Natasa Milickovic 1, Nikolaos Zamboglou 2 1 Dept. of Medical Physics & Engineering, 2 Strahlenklinik,
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas 1,3, Natasa Milickovic 1, Nikolaos Zamboglou 2 1 Dept. of Medical Physics & Engineering, 2 Strahlenklinik,