Case Report Prolonged Survival following Repetitive Stereotactic Radiosurgery in a Patient with Intracranial Metastatic Renal Cell Carcinoma
|
|
|
- Carmella Cross
- 6 years ago
- Views:
Transcription
1 Case Reports in Neurological Medicine Volume 2015, Article ID , 5 pages Case Report Prolonged Survival following Repetitive Stereotactic Radiosurgery in a Patient with Intracranial Metastatic Renal Cell Carcinoma Ethan A. Ferrel, 1,2,3 Andrew T. Roehrig, 1,2,3 Wayne T. Lamoreaux, 1,2 Alexander R. Mackay, 1,2 Robert K. Fairbanks, 1,2 Jason A. Call, 1,2 Jonathan D. Carlson, 1,4 Benjamin C. Ling, 4 John J. Demakas, 1,5 Barton S. Cooke, 1 Aaron Wagner, 1,2 and Christopher M. Lee 1,2 1 GammaKnifeofSpokane,910W5thAvenue,Suite102,Spokane,WA99204,USA 2 CancerCareNorthwest,910W5thAvenue,Suite102,Spokane,WA99204,USA 3 University of Washington School of Medicine, 1959 NE Pacific Street, Seattle, WA 98195, USA 4 Inland Neurosurgery & Spine Associates, 105 W 8th Avenue, Suite 200, Spokane, WA 99204, USA 5 Rockwood Clinic, 801 W 5th Avenue, Suite 525, Spokane, WA 99204, USA Correspondence should be addressed to Christopher M. Lee; lee@ccnw.net Received 28 August 2015; Accepted 13 October 2015 Academic Editor: Mehmet Turgut Copyright 2015 Ethan A. Ferrel et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Patients with metastatic renal cell carcinoma (RCC) to the brain have a very poor prognosis of three months if left untreated. SRS is an effective treatment modality in numerous patients. This case exemplifies the utility of stereotactic radiosurgery (SRS) in prolonging survival and maintaining quality of life in a patient with RCC. This 64-year-old female patient initially presented to her primary care physician 22 months after a left nephrectomy for RCC with complaints of mild, intermittent headaches and difficulty with balance. An MRI revealed five cerebellar lesions suspicious for intracranial metastasis. The patient s first GKRS treatment targeted four lesions with 22 Gy at the 50% isodose line. She underwent a total of seven GKRS treatments over the next 60 months for recurrent metastases to the brain. 72 months and 12 months have now passed since her brain metastases were first discovered and since her last GKRS treatment, respectively, and this woman is alive with considerable quality of life and no evidence of metastatic reoccurrence. This case shows that repeated GKRS treatments, with minimal surgical intervention, can effectively treat multiple intracranial lesions in select patients, prolonging survival and avoiding iatrogenic neurocognitive decline while maintaining a high quality of life. 1. Introduction Secondary metastasis to the brain continues to be a leading cause of death in cancer patients. Each year in the US, roughly 170,000 new cases of brain metastasis are diagnosed, an estimated 1,200 5,100 of which are secondary to renal cell carcinoma (RCC) [1 5]. Advancements in imaging and treatments of systemic disease have led to an increased prevalence of these tumors across all RCC patients. Due to theverypoorprognosisforpatientswithintracranialrcc, rapid and effective treatment has become vitally important for overall survival and quality of life. Standard therapies for these tumors include corticosteroids, surgical resection, whole brain radiation therapy (WBRT), and stereotactic radiosurgery (SRS) [6]. Treatment regimens are generally multimodal. Metastases from RCC are notoriously difficult to treat with conventional whole brain radiation due to the radioresistant nature of these tumors [7]. In response, SRS has emerged as an effective alternative, especially for patients with a single metastasis [8]. WBRT is
2 2 Case Reports in Neurological Medicine still recommended for patients with >3 metastases,but few studies have examined the effectiveness of treating multiple RCC metastases without adjuvant WBRT [9]. In this report, we discuss the results of a nephrectomized patient with multiple brain metastases from RCC treated with surgery, steroids, and a total of eight GKRS procedures over a 60-month period. At this time, she is alive with no evidence of reoccurrence. 2. Case Report We report on a 64-year-old woman who initially presented to the emergency department with complaints of chest pain following a motor vehicle crash. A CT incidentally found renal abnormalities, and a postnephrectomy biopsy confirmed renal cell carcinoma. The patient was asymptomatic at that time and remained so for ten months, after which she visited her primary care physician with complaints of mild intermittent headaches and difficulty with balance. An MRI revealed five cerebellar lesions measuring cm, cm, cm, cm, and cm, as well as extensive vasogenic edema. Her treatment team recommended against resection due to the sensitive location of her tumors. GKRS was recommended over WBRT due to concern that avoiding previous radiation fields from treatment for oropharyngeal carcinoma 14 years earlier would not adequately address her relatively caudal metastatic tumors. The patient then underwent her first GKRS treatment at a dose of 22 Gy at the 50% isodose line (Figures 1 and 2). On the day of treatment, her Karnofsky Performance Status score was 100. Following GKRS, she was placed on dexamethasone 2 mg daily. Within several weeks she had experienced significant resolution of symptoms. Over the next 51 months, she underwent a subsequent six GKRS treatments, all of which treated between one and four metastases. Many of these metastases were in new locations within the cerebellum, while several appeared in the brainstem itself. 49 months after her initial treatment, she underwent a craniotomy to relieve obstructive hydrocephalus with a ventricular shunt placement. An 8.0 mm cerebellar lesion was successfully resected in the same procedure. Around the same time, she underwent SBRT for liver metastases, which was tolerated well. The patient s most recent GKRS treatment occurred 60 months after the first and was suggested when the patient presented with complaints of consistent falls. A CT demonstrated five lesions, four of which were localized to the cerebellumandonelimitedtothepons.threeofthelesions had increased in size since her previous CT several months earlier. Three lesions were treated with a dose of 20 Gy at the50%isodoseline,onelesionwastreatedwith18gyat the 75% isodose line, and one was treated with 18 Gy at the 55% isodose line. A posttreatment CT demonstrated reduced dimensions of all lesions. Her most recent CT was taken 5 months later and demonstrated reduced or stable sizes of all lesions. 65 months after her initial diagnosis of brain metastasis, the patient began treatment with Votrient 800 mg for her liver metastases, which was tapered down to 400 mg and eventually held completely for after severe GI side effects and elevated liver enzymes. One month prior to this paper, a PET scan was obtained, showing no new evidence of systemic or metastatic disease. At that time, she remained symptom-free with a high quality of life a total of 72 months after her brain metastases were diagnosed. 3. Discussion Brain metastasis from renal cell carcinoma remains one of most frequently encountered intracranial secondary cancers, with 4 11% of RCCs spreading to the brain [7]. The poor prognosis of these patients has led to much research into ideal treatment modalities which extend overall survival and maximize quality of life. As new treatments and technologies become more effective in treating the primary disease, intracranial spread is becoming more commonplace [1, 3 5]. Nephrectomy is the first-line treatment for renal cell carcinoma, but a large autopsy study found that nephrectomized patients were not significantly less likely to develop distant metastases than nonnephrectomized patients [10, 11]. Chemotherapeutic treatments, while sometimes effective in treating the primary cancer, seem to have little effect on cerebral tumors [11]. In response, many researchers now focus on how to best address and treat intracranial metastases [9] Current Treatment Modalities and Benefits of SRS. Much debate exists over the appropriate treatment modalities for these tumors. RCC has long been considered to have radioresistant histology, rendering WBRT of questionable efficacy [11]. A study by Nieder et al. of 336 metastatic lesions treated with WBRT (30 Gy in 10 fractions) showed a complete response rate of 0% for RCC, while small cell carcinoma and breast cancer showed 37% and 35% response rates, respectively [12]. WBRT has also been shown in multiple studies to accelerate neurocognitive decline [13 15]. In a recent study by Brown et al., 91.7% of patients with brain metastasis treated with both SRS and WBRT experienced a cognitive decline compared to 63.5% of patients who underwent SRS alone [15].Due to these concerns,wbrt is more frequently being recommended only to patients with advanced disease and especially poor prognoses [9]. Surgical resection, while ideal in removing large lesions, is not always capable of treating multiple metastases. Resection couldbeimpracticalduetoatumor slocation,suchaswhen metastases are distant from each other or lie near critical structures. Metastatic lesions of the brainstem are particularly difficult to resect due to the highly concentrated nuclei and neural tracts. If the tumor can be safely resected, adjuvant radiation to the tumor bed is often applied in order to achieve optimal margins. Important to note is how metastatic RCC is a negative prognostic factor for peritumoral edema [16, 17].AstudybyShutoetal.foundthatSRSisaneffective way of managing symptomatic peritumoral edema especially from small tumors, while removal of a large tumor can be advantageous in relieving severe edema and its symptoms, as was in the case of our patient [16]. Regardless, the invasive



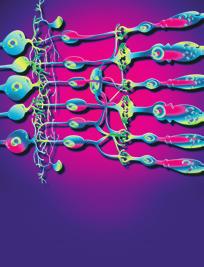
![hasproventobeaneffectivetreatmentmodality[11, 16, 18 20].](/docs-images/77/76066271/images/3-3.jpg "SRS is often capable of safely reaching lesions that")

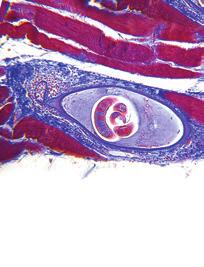
![while boasting improved local control rates [15, 16, 19].](/docs-images/77/76066271/images/3-5.jpg "A retrospective study of metastatic RCC patients treated with")










3 Case Reports in Neurological Medicine 3 Figure 1: Multiple T-1 postgadolinium axial images illustrating tumor location and Gamma Knife isodose plans (22 Gy, 50% isodose line). and lengthy nature of surgery has rendered faster, less invasive treatments more appealing. In response to the shortfalls of surgery and WBRT, SRS hasproventobeaneffectivetreatmentmodality[11, 16, 18 20]. SRS is often capable of safely reaching lesions that neurosurgeons cannot and has been shown to minimize the harmful neurocognitive effects of widespread radiation, all while boasting improved local control rates [15, 16, 19]. A retrospective study of metastatic RCC patients treated with SRS alone found that SRS resulted in a local control rate of 94% and median overall survival of 11.4 months [19]. Another study by Sheehan et al. found that patients with metastatic RCC treated with SRS alone experienced a local control rate of 96% and median overall survival of 15 months [18]. In addition to being effective, SRS is a rapid and minimally invasive procedure with a low rate of complications that can often be completed in a single treatment. A study by Hong et al. analyzed adverse effects of 279 SRS procedures and found that <2% of patients experienced sequelae requiring hospitalization, and 34% experienced mild to moderate side effects [21]. SRS has repeatedly demonstrated its utility in treating brain metastases and ought to be considered a firstline therapy for patients with positive prognostic factors Prognostic Factors and SRS Dosing Considerations. Many studies have attempted to determine prognostic factors for patients with brain metastasis. Currently, the Radiation Therapy Oncology Group s (RTOG) recursive partitioning analysis (RPA) system is used most frequently to establish prognosis [22]. The RPA categorizes patients into three classes basedontheirkarnofskyperformancescore(kps),age, number of extracranial metastases, and status of primary

4 4 Case Reports in Neurological Medicine Acknowledgments The authors would like to thank Jill Adams, Eric Reynolds, and the entire research staff at Cancer Care Northwest for their contributions to this report. References Figure 2: Axial image revealing 3-dimensional wire view of the Gamma Knife radiation dose cloud. cancer, where a higher RPA class indicates a worse prognosis [1, 3 5]. Muacevic et al. determined that a KPS > 70 and RPA Class 1 were correlated to a better survival prognosis [19].AsizeablestudybyKanoetal.foundthatnumberof intracranial metastases is a significant prognostic factor as well as age and KPS, while a study by Powell et al. found that KPS was a better prognostic indicator than number of intracranial metastases [20, 23]. These observations are essential in establishing treatment guidelines for physicians. Tailored treatment plans of modality, dosages, and other factors require such insights to achieve optimal outcomes in individual patients. SRS dosage also seems to be an important factor in the treatment of intracranial RCC. A 2015 study by Rades et al. determined that treatment with 20 Gy results in better 12-month survival rates than Gy at 81% and 50%, respectively, in patients with brain metastatic RCC [24]. To date, this is the only study on the impact of dose on survival in patients with RCC treated solely with SRS. Lorenzoni et al. found that a dose higher than 18 Gy was associated with longer survival in a multivariate analysis of patients with intracranial tumors from a variety of cancers treated with SRS [25]. Further research on the effect of SRS dose on overall survival is necessary to understand this potentially important correlation. 4. Conclusion Our report demonstrates the efficacy of treating multiple metastases from renal cell carcinoma with SRS without adjuvant WBRT. Few reported cases have demonstrated such extended survival times of patients with metastatic RCC treated with SRS alone. This patient demonstrates extended survival and high quality of life after undergoing repeated GKRS treatments. 72 months after the diagnosis of her brain metastases, she is alive with an appreciable quality of life. SRS ought to be strongly considered as the primary treatment for multiple intracranial metastases in RCC patients. Conflict of Interests The authors report no conflict of interests. [1] J. B. Posner, Management of brain metastases, Revue Neurologique,vol.148,no.6-7,pp ,1992. [2]S.R.Rapp,L.DougCase,A.Peifferetal., Donepezilfor irradiated brain tumor survivors: a phase III randomized placebo-controlled clinical trial, Clinical Oncology, vol. 33, no. 15, pp , [3] R. A. Patchell, The management of brain metastases, Cancer Treatment Reviews,vol.29,no.6,pp ,2003. [4] N.F.Marko,L.Angelov,S.A.Tomsetal., Stereotacticradiosurgery as single-modality treatment of incidentally identified renalcellcarcinomabrainmetastases, World Neurosurgery,vol. 73,no.3,pp ,2010. [5] W.E.Samlowski,G.A.Watson,M.Wangetal., Multimodality treatment of melanoma brain metastases incorporating stereotactic radiosurgery (SRS), Cancer, vol. 109, no. 9, pp , [6] R. Soffietti, R. Ruda, and R. Mutani, Management of brain metastases, Neurology,vol.249,no.10,pp , [7] Y. H. Kim, J. W. Kim, H. T. Chung, S. H. Paek, D. G. Kim, and H. W. Jung, Brain metastasis from renal cell carcinoma, Progress in Neurological Surgery,vol.25,pp ,2012. [8]J.W.Clarke,S.Register,J.M.McGregoretal., Stereotactic radiosurgery with or without whole brain radiotherapy for patients with a single radioresistant brain metastasis, American Clinical Oncology,vol.33,no.1,pp.70 74,2010. [9] E.Fokas,M.Henzel,K.Hamm,G.Surber,G.Kleinert,andR. Engenhart-Cabillic, Radiotherapy for brain metastases from renal cell cancer: should whole-brain radiotherapy be added to stereotactic radiosurgery? Strahlentherapie und Onkologie, vol. 186, no. 4, pp , [10] H. Saitoh, M. Nakayama, K. Nakamura, and T. Satoh, Distant metastasis of renal adenocarcinoma in nephrectomized cases, Urology,vol.127,no.6,pp ,1982. [11] H. T. Cohen and F. J. McGovern, Renal-cell carcinoma, The New England Medicine, vol.353,no.23,pp , [12] C. Nieder, W. Berberich, and K. Schnabel, Tumor-related prognostic factors for remission of brain metastases after radiotherapy, International Radiation Oncology Biology Physics,vol.39,no.1,pp.25 30,1997. [13] N. B. Dye, V. Gondi, and M. P. Mehta, Strategies for preservation of memory function in patients with brain metastases, Chinese Clinical Oncology,vol.4,no.2,article24,2015. [14] E. L. Chang, J. S. Wefel, K. R. Hess et al., Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: a randomised controlled trial, The Lancet Oncology,vol.10,no.11,pp , [15] P.A.Brown,A.L.Asher,K.V.Ballmanetal., NCCTGN0574 (Alliance): a phase III randomized trial of whole brain radiation therapy (WBRT) in addition to radiosurgery (SRS) in patients with 1 to 3 brain metastases, Clinical Oncology, vol. 33, no. 15, abstract LBA4, 2015.
5 Case Reports in Neurological Medicine 5 [16] T. Shuto, S. Matsunaga, J. Suenaga, S. Inomori, and H. Fujino, Treatment strategy for metastatic brain tumors from renal cell carcinoma: selection of gamma knife surgery or craniotomy for control of growth and peritumoral edema, Neuro- Oncology, vol. 98, no. 2, pp , [17] T. Shuto, S. Matsunaga, S. Inomori, and H. Fujino, Efficacy of gamma knife surgery for control of peritumoral oedema associated with metastatic brain tumours, Neurology, Neurosurgery and Psychiatry,vol.79,no.9,pp ,2008. [18] J. P. Sheehan, M.-H. Sun, D. Kondziolka, J. Flickinger, and L. D. Lunsford, Radiosurgery in patients with renal cell carcinoma metastasis to the brain: long-term outcomes and prognostic factors influencing survival and local tumor control, Neurosurgery,vol.98,no.2,pp ,2003. [19] A. Muacevic, F. W. Kreth, A. Mack, J.-C. Tonn, and B. Wowra, Stereotactic radiosurgery without radiation therapy providing high local tumor control of multiple brain metastases from renal cell carcinoma, Minimally Invasive Neurosurgery, vol. 47, no. 4, pp ,2004. [20]J.W.Powell,C.T.Chung,H.R.Shahetal., GammaKnife surgery in the management of radioresistant brain metastases in high-risk patients with melanoma, renal cell carcinoma, and sarcoma, neurosurgery, vol. 109, supplement, pp , [21] T.S.Hong,W.A.Tomé, L. Hayes et al., Acute sequelae of stereotactic radiosurgery, in Radiosurgery, vol. 5, pp , Karger, Basel, Switzerland, [22] A. L. Elaimy, A. R. MacKay, W. T. Lamoreaux et al., Clinical outcomes of stereotactic radiosurgery in the treatment of patients with metastatic brain tumors, World Neurosurgery, vol. 75, no. 5-6, pp , [23] H. Kano, A. Iyer, D. Kondziolka, A. Niranjan, J. C. Flickinger, and L. D. Lunsford, Outcome predictors of gamma knife radiosurgery for renal cell carcinoma metastases, Neurosurgery,vol. 69, no. 6, pp , [24] D. Rades, S. Huttenlocher, N. Gebauer et al., Impact of stereotactic radiosurgery dose on control of cerebral metastases from renalcellcarcinoma, Anticancer Research, vol.35,no.6,pp , [25] J. G. Lorenzoni, D. Devriendt, N. Massager et al., Brain stem metastases treated with radiosurgery: prognostic factors of survival and life expectancy estimation, Surgical Neurology, vol. 71, no. 2, pp , 2009.










6 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
1. Introduction. Correspondence should be addressed to Christopher M. Lee; Received 9 July 2013; Accepted 27 August 2013
 Case Reports in Oncological Medicine Volume 2013, Article ID 431857, 5 pages http://dx.doi.org/10.1155/2013/431857 Case Report Long-Term Survival and Improved Quality of Life following Multiple Repeat
Case Reports in Oncological Medicine Volume 2013, Article ID 431857, 5 pages http://dx.doi.org/10.1155/2013/431857 Case Report Long-Term Survival and Improved Quality of Life following Multiple Repeat
Survival and Intracranial Control of Patients With 5 or More Brain Metastases Treated With Gamma Knife Stereotactic Radiosurgery
 ORIGINAL ARTICLE Survival and Intracranial Control of Patients With 5 or More Brain Metastases Treated With Gamma Knife Stereotactic Radiosurgery Ann C. Raldow, BS,* Veronica L. Chiang, MD,w Jonathan P.
ORIGINAL ARTICLE Survival and Intracranial Control of Patients With 5 or More Brain Metastases Treated With Gamma Knife Stereotactic Radiosurgery Ann C. Raldow, BS,* Veronica L. Chiang, MD,w Jonathan P.
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms. Overall Clinical Significance 8/3/13
 Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
ARROCase Brain Metastases
 ARROCase Brain Metastases Colin Hill*, Daniel M. Trifiletti*, Timothy N. Showalter*, Jason P. Sheehan Radiation Oncology* and Neurosurgery University of Virginia Charlottesville, VA Case: HPI 64 year old
ARROCase Brain Metastases Colin Hill*, Daniel M. Trifiletti*, Timothy N. Showalter*, Jason P. Sheehan Radiation Oncology* and Neurosurgery University of Virginia Charlottesville, VA Case: HPI 64 year old
Management of single brain metastasis: a practice guideline
 PRACTICE GUIDELINE SERIES Management of single brain metastasis: a practice guideline A. Mintz MD,* J. Perry MD, K. Spithoff BHSc, A. Chambers MA, and N. Laperriere MD on behalf of the Neuro-oncology Disease
PRACTICE GUIDELINE SERIES Management of single brain metastasis: a practice guideline A. Mintz MD,* J. Perry MD, K. Spithoff BHSc, A. Chambers MA, and N. Laperriere MD on behalf of the Neuro-oncology Disease
Evidence Based Medicine for Gamma Knife Radiosurgery. Metastatic Disease GAMMA KNIFE SURGERY
 GAMMA KNIFE SURGERY Metastatic Disease Evidence Based Medicine for Gamma Knife Radiosurgery Photos courtesy of Jean Régis, Timone University Hospital, Marseille, France Brain Metastases The first report
GAMMA KNIFE SURGERY Metastatic Disease Evidence Based Medicine for Gamma Knife Radiosurgery Photos courtesy of Jean Régis, Timone University Hospital, Marseille, France Brain Metastases The first report
Neurological Change after Gamma Knife Radiosurgery for Brain Metastases Involving the Motor Cortex
 ORIGINAL ARTICLE Brain Tumor Res Treat 2016;4(2):111-115 / pissn 2288-2405 / eissn 2288-2413 http://dx.doi.org/10.14791/btrt.2016.4.2.111 Neurological Change after Gamma Knife Radiosurgery for Brain Metastases
ORIGINAL ARTICLE Brain Tumor Res Treat 2016;4(2):111-115 / pissn 2288-2405 / eissn 2288-2413 http://dx.doi.org/10.14791/btrt.2016.4.2.111 Neurological Change after Gamma Knife Radiosurgery for Brain Metastases
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia
 for Brain Metastasis in Nova Scotia") A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Radiotherapy and Brain Metastases. Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem
 Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Department of Oncology and Palliative Medicine, Nordland Hospital, 8092 Bodø, Norway 2
 The Scientific World Journal Volume 212, Article ID 69323, 5 pages doi:1.11/212/69323 The cientificworldjournal Clinical Study Towards Improved Prognostic Scores Predicting Survival in Patients with Brain
The Scientific World Journal Volume 212, Article ID 69323, 5 pages doi:1.11/212/69323 The cientificworldjournal Clinical Study Towards Improved Prognostic Scores Predicting Survival in Patients with Brain
Laboratory data from the 1970s first showed that malignant melanoma
 2265 Survival by Radiation Therapy Oncology Group Recursive Partitioning Analysis Class and Treatment Modality in Patients with Brain Metastases from Malignant Melanoma A Retrospective Study Jeffrey C.
2265 Survival by Radiation Therapy Oncology Group Recursive Partitioning Analysis Class and Treatment Modality in Patients with Brain Metastases from Malignant Melanoma A Retrospective Study Jeffrey C.
Hong Kong Hospital Authority Convention 2018
 Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus Irinotecan and Radiotherapy
 Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
Stereotactic radiosurgery for the treatment of melanoma and renal cell carcinoma brain metastases
 ONCOLOGY REPORTS 29: 407-412, 2013 Stereotactic radiosurgery for the treatment of melanoma and renal cell carcinoma brain metastases SHELLY LWU 1, PABLO GOETZ 1, ERIC MONSALVES 1, MANDANA ARYAEE 1, JULIUS
ONCOLOGY REPORTS 29: 407-412, 2013 Stereotactic radiosurgery for the treatment of melanoma and renal cell carcinoma brain metastases SHELLY LWU 1, PABLO GOETZ 1, ERIC MONSALVES 1, MANDANA ARYAEE 1, JULIUS
Gamma Knife Surgery for Brain Metastasis from Renal Cell Carcinoma : Relationship Between Radiological Characteristics and Initial Tumor Response
 online ML Comm www.jkns.or.kr Clinical Article Jin Wook Kim, M.D. Jung Ho Han, M.D. Chul-Kee Park, M.D. Hyun-Tai Chung, Ph.D. Sun Ha Paek, M.D. Dong Gyu Kim, M.D. Department of Neurosurgery Seoul National
online ML Comm www.jkns.or.kr Clinical Article Jin Wook Kim, M.D. Jung Ho Han, M.D. Chul-Kee Park, M.D. Hyun-Tai Chung, Ph.D. Sun Ha Paek, M.D. Dong Gyu Kim, M.D. Department of Neurosurgery Seoul National
Clinical Study Does Time between Imaging Diagnosis and Initiation of Radiotherapy Impact Survival after Whole-Brain Radiotherapy for Brain Metastases?
 ISRN Oncology Volume 2013, Article ID 214304, 4 pages http://dx.doi.org/10.1155/2013/214304 Clinical Study Does Time between Imaging Diagnosis and Initiation of Radiotherapy Impact Survival after Whole-Brain
ISRN Oncology Volume 2013, Article ID 214304, 4 pages http://dx.doi.org/10.1155/2013/214304 Clinical Study Does Time between Imaging Diagnosis and Initiation of Radiotherapy Impact Survival after Whole-Brain
Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015
 Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015 Most common brain tumor, affecting 8.5-15% of cancer patients. Treatment options: Whole brain radiation
Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015 Most common brain tumor, affecting 8.5-15% of cancer patients. Treatment options: Whole brain radiation
Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma of Thyroid
 Case Reports in Urology Volume 2013, Article ID 651081, 4 pages http://dx.doi.org/10.1155/2013/651081 Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma
Case Reports in Urology Volume 2013, Article ID 651081, 4 pages http://dx.doi.org/10.1155/2013/651081 Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma
SUCCESSFUL TREATMENT OF METASTATIC BRAIN TUMOR BY CYBERKNIFE: A CASE REPORT
 SUCCESSFUL TREATMENT OF METASTATIC BRAIN TUMOR BY CYBERKNIFE: A CASE REPORT Cheng-Ta Hsieh, 1 Cheng-Fu Chang, 1 Ming-Ying Liu, 1 Li-Ping Chang, 2 Dueng-Yuan Hueng, 3 Steven D. Chang, 4 and Da-Tong Ju 1
SUCCESSFUL TREATMENT OF METASTATIC BRAIN TUMOR BY CYBERKNIFE: A CASE REPORT Cheng-Ta Hsieh, 1 Cheng-Fu Chang, 1 Ming-Ying Liu, 1 Li-Ping Chang, 2 Dueng-Yuan Hueng, 3 Steven D. Chang, 4 and Da-Tong Ju 1
Update on management of metastatic brain disease. Peter Hoskin Mount Vernon Cancer Centre Northwood UK
 Update on management of metastatic brain disease Peter Hoskin Mount Vernon Cancer Centre Northwood UK Incidence 15-30% of patients with solid tumours will develop brain metastases Most common primary sites
Update on management of metastatic brain disease Peter Hoskin Mount Vernon Cancer Centre Northwood UK Incidence 15-30% of patients with solid tumours will develop brain metastases Most common primary sites
VINCENT KHOO. 8 th EIKCS Symposium: May 2013
 8 th EIKCS Symposium: May 2013 VINCENT KHOO Royal Marsden NHS Foundation Trust & Institute of Cancer Research St George s Hospital & University of London Austin Health & University of Melbourne Disclosures
8 th EIKCS Symposium: May 2013 VINCENT KHOO Royal Marsden NHS Foundation Trust & Institute of Cancer Research St George s Hospital & University of London Austin Health & University of Melbourne Disclosures
Selecting the Optimal Treatment for Brain Metastases
 Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Case Report Cerebral Metastasis from a Previously Undiagnosed Appendiceal Adenocarcinoma
 Case Reports in Oncological Medicine Volume 2012, Article ID 192807, 4 pages doi:10.1155/2012/192807 Case Report Cerebral Metastasis from a Previously Undiagnosed Appendiceal Adenocarcinoma Antonio Biroli,
Case Reports in Oncological Medicine Volume 2012, Article ID 192807, 4 pages doi:10.1155/2012/192807 Case Report Cerebral Metastasis from a Previously Undiagnosed Appendiceal Adenocarcinoma Antonio Biroli,
Prescription dose and fractionation predict improved survival after stereotactic radiotherapy for brainstem metastases
 Leeman et al. Radiation Oncology 2012, 7:107 RESEARCH Open Access Prescription dose and fractionation predict improved survival after stereotactic radiotherapy for brainstem metastases Jonathan E Leeman
Leeman et al. Radiation Oncology 2012, 7:107 RESEARCH Open Access Prescription dose and fractionation predict improved survival after stereotactic radiotherapy for brainstem metastases Jonathan E Leeman
We have previously reported good clinical results
 J Neurosurg 113:48 52, 2010 Gamma Knife surgery as sole treatment for multiple brain metastases: 2-center retrospective review of 1508 cases meeting the inclusion criteria of the JLGK0901 multi-institutional
J Neurosurg 113:48 52, 2010 Gamma Knife surgery as sole treatment for multiple brain metastases: 2-center retrospective review of 1508 cases meeting the inclusion criteria of the JLGK0901 multi-institutional
Cerebral metastases occur in 20% 40% of cancer
 See the corresponding editorial, DOI: 10.3171/2012.1.JNS12103. DOI: 10.3171/2012.4.JNS11870 Stereotactic radiosurgery using the Leksell Gamma Knife Perfexion unit in the management of patients with 10
See the corresponding editorial, DOI: 10.3171/2012.1.JNS12103. DOI: 10.3171/2012.4.JNS11870 Stereotactic radiosurgery using the Leksell Gamma Knife Perfexion unit in the management of patients with 10
RESEARCH HUMAN CLINICAL STUDIES
 TOPIC RESEARCH HUMAN CLINICAL STUDIES RESEARCH HUMAN CLINICAL STUDIES Radiosurgery to the Surgical Cavity as Adjuvant Therapy for Resected Brain Metastasis Jared R. Robbins, MD* Samuel Ryu, MD* Steven
TOPIC RESEARCH HUMAN CLINICAL STUDIES RESEARCH HUMAN CLINICAL STUDIES Radiosurgery to the Surgical Cavity as Adjuvant Therapy for Resected Brain Metastasis Jared R. Robbins, MD* Samuel Ryu, MD* Steven
Management of Single Brain Metastases Practice Guideline Report #9-1
 Management of Single Brain Metastases Practice Guideline Report #9-1 A.P. Mintz, J. Perry, G. Cairncross, A. Chambers and members of the Neuro-oncology Disease Site Group Report Date: August 17, 2004 SUMMARY
Management of Single Brain Metastases Practice Guideline Report #9-1 A.P. Mintz, J. Perry, G. Cairncross, A. Chambers and members of the Neuro-oncology Disease Site Group Report Date: August 17, 2004 SUMMARY
Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule
 Case Reports in Oncological Medicine Volume 2013, Article ID 865032, 4 pages http://dx.doi.org/10.1155/2013/865032 Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule M. Casali, 1 A.
Case Reports in Oncological Medicine Volume 2013, Article ID 865032, 4 pages http://dx.doi.org/10.1155/2013/865032 Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule M. Casali, 1 A.
Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication for Repeat Metastasectomy
 Respiratory Medicine Volume 2015, Article ID 570314, 5 pages http://dx.doi.org/10.1155/2015/570314 Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication
Respiratory Medicine Volume 2015, Article ID 570314, 5 pages http://dx.doi.org/10.1155/2015/570314 Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication
Br a i n metastases occur in 20 40% of all patients. The results of resection after stereotactic radiosurgery for brain metastases.
 J Neurosurg 111:825 831, 2009 The results of resection after stereotactic radiosurgery for brain metastases Clinical article Hi d e y u k i Ka n o, M.D., Ph.D., 1,3 Do u g l a s Ko n d z i o l k a, M.D.,
J Neurosurg 111:825 831, 2009 The results of resection after stereotactic radiosurgery for brain metastases Clinical article Hi d e y u k i Ka n o, M.D., Ph.D., 1,3 Do u g l a s Ko n d z i o l k a, M.D.,
Research Article Have Changes in Systemic Treatment Improved Survival in Patients with Breast Cancer Metastatic to the Brain?
 Oncology Volume 2008, Article ID 417137, 5 pages doi:10.1155/2008/417137 Research Article Have Changes in Systemic Treatment Improved Survival in Patients with Breast Cancer Metastatic to the Brain? Carsten
Oncology Volume 2008, Article ID 417137, 5 pages doi:10.1155/2008/417137 Research Article Have Changes in Systemic Treatment Improved Survival in Patients with Breast Cancer Metastatic to the Brain? Carsten
Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen?
 Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Br a i n metastases are the tumors most frequently. Safety and efficacy of Gamma Knife surgery for brain metastases in eloquent locations
 J Neurosurg 113:79 83, 2010 Safety and efficacy of Gamma Knife surgery for brain metastases in eloquent locations Clinical article Ni c o l a s De a, M.D., Mar t i n Bo r d u a s, Br e n d a n Ke n n y,
J Neurosurg 113:79 83, 2010 Safety and efficacy of Gamma Knife surgery for brain metastases in eloquent locations Clinical article Ni c o l a s De a, M.D., Mar t i n Bo r d u a s, Br e n d a n Ke n n y,
Solitary Contralateral Adrenal Metastases after Nephrectomy for Renal Cell Carcinoma
 Original Report ISSN 1537-744X; DOI 10.1100/tsw.2004.39 Solitary Contralateral Adrenal after Nephrectomy for Renal Cell Carcinoma Nikolaos Antoniou, M.D. and Demetrios Karanastasis, M.D. General Hospital
Original Report ISSN 1537-744X; DOI 10.1100/tsw.2004.39 Solitary Contralateral Adrenal after Nephrectomy for Renal Cell Carcinoma Nikolaos Antoniou, M.D. and Demetrios Karanastasis, M.D. General Hospital
Gamma Knife Treatment of Brainstem Metastases
 Int. J. Mol. Sci. 2014, 15, 9748-9761; doi:10.3390/ijms15069748 Article OPEN ACCESS International Journal of Molecular Sciences ISSN 1422-0067 www.mdpi.com/journal/ijms Gamma Knife Treatment of Brainstem
Int. J. Mol. Sci. 2014, 15, 9748-9761; doi:10.3390/ijms15069748 Article OPEN ACCESS International Journal of Molecular Sciences ISSN 1422-0067 www.mdpi.com/journal/ijms Gamma Knife Treatment of Brainstem
Case Report Multiple Intracranial Meningiomas: A Review of the Literature and a Case Report
 Case Reports in Surgery Volume 2013, Article ID 131962, 4 pages http://dx.doi.org/10.1155/2013/131962 Case Report Multiple Intracranial Meningiomas: A Review of the Literature and a Case Report F. Koech,
Case Reports in Surgery Volume 2013, Article ID 131962, 4 pages http://dx.doi.org/10.1155/2013/131962 Case Report Multiple Intracranial Meningiomas: A Review of the Literature and a Case Report F. Koech,
Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome to Cutaneous Melanoma
 ISRN Dermatology Volume 2013, Article ID 586915, 5 pages http://dx.doi.org/10.1155/2013/586915 Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome
ISRN Dermatology Volume 2013, Article ID 586915, 5 pages http://dx.doi.org/10.1155/2013/586915 Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome
Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey
 Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report of Neoadjuvant Use Enabling Complete Surgical Resection
 Case Reports in Oncological Medicine Volume 2013, Article ID 496351, 4 pages http://dx.doi.org/10.1155/2013/496351 Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report
Case Reports in Oncological Medicine Volume 2013, Article ID 496351, 4 pages http://dx.doi.org/10.1155/2013/496351 Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report
Mandana Moosavi 1 and Stuart Kreisman Background
 Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Evidence Based Medicine for Gamma Knife Radiosurgery. Metastatic Disease GAMMA KNIFE SURGERY
 GAMMA KNIFE SURGERY Metastatic Disease Evidence Based Medicine for Gamma Knife Radiosurgery Photos courtesy of Jean Régis, Timone University Hospital, Marseille, France Brain Metastases The first report
GAMMA KNIFE SURGERY Metastatic Disease Evidence Based Medicine for Gamma Knife Radiosurgery Photos courtesy of Jean Régis, Timone University Hospital, Marseille, France Brain Metastases The first report
R. F. Falkenstern-Ge, 1 S. Bode-Erdmann, 2 G. Ott, 2 M. Wohlleber, 1 and M. Kohlhäufl Introduction. 2. Histology
 Case Reports in Oncological Medicine Volume 2013, Article ID 167585, 4 pages http://dx.doi.org/10.1155/2013/167585 Case Report Late Lung Metastasis of a Primary Eccrine Sweat Gland Carcinoma 10 Years after
Case Reports in Oncological Medicine Volume 2013, Article ID 167585, 4 pages http://dx.doi.org/10.1155/2013/167585 Case Report Late Lung Metastasis of a Primary Eccrine Sweat Gland Carcinoma 10 Years after
Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach
 Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Correspondence should be addressed to Taha Numan Yıkılmaz;
 Advances in Medicine Volume 2016, Article ID 8639041, 5 pages http://dx.doi.org/10.1155/2016/8639041 Research Article External Validation of the Cancer of the Prostate Risk Assessment Postsurgical Score
Advances in Medicine Volume 2016, Article ID 8639041, 5 pages http://dx.doi.org/10.1155/2016/8639041 Research Article External Validation of the Cancer of the Prostate Risk Assessment Postsurgical Score
Research Article Predictions of the Length of Lumbar Puncture Needles
 Computational and Mathematical Methods in Medicine, Article ID 732694, 5 pages http://dx.doi.org/10.1155/2014/732694 Research Article Predictions of the Length of Lumbar Puncture Needles Hon-Ping Ma, 1,2
Computational and Mathematical Methods in Medicine, Article ID 732694, 5 pages http://dx.doi.org/10.1155/2014/732694 Research Article Predictions of the Length of Lumbar Puncture Needles Hon-Ping Ma, 1,2
Bilateral Renal Angiomyolipomas with Invasion of the Renal Vein: A Case Report
 Case Study TheScientificWorldJOURNAL (2008) 8, 145 148 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2008.29 Bilateral Renal Angiomyolipomas with Invasion of the Renal Vein: A Case Report C. Blick, N. Ravindranath,
Case Study TheScientificWorldJOURNAL (2008) 8, 145 148 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2008.29 Bilateral Renal Angiomyolipomas with Invasion of the Renal Vein: A Case Report C. Blick, N. Ravindranath,
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR PILOCYTIC ASTROCYTOMA
 1 EVIDENCE SUMMARY REPORT FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR PILOCYTIC ASTROCYTOMA QUESTIONS TO BE ADDRESSED: SUMMARY 1. What is the evidence for the clinical
1 EVIDENCE SUMMARY REPORT FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR PILOCYTIC ASTROCYTOMA QUESTIONS TO BE ADDRESSED: SUMMARY 1. What is the evidence for the clinical
Local control of brain metastases by stereotactic radiosurgery in relation to dose to the tumor margin
 J Neurosurg 104:907 912, 2006 Local control of brain metastases by stereotactic radiosurgery in relation to dose to the tumor margin MICHAEL A. VOGELBAUM, M.D., PH.D., LILYANA ANGELOV, M.D., SHIH-YUAN
J Neurosurg 104:907 912, 2006 Local control of brain metastases by stereotactic radiosurgery in relation to dose to the tumor margin MICHAEL A. VOGELBAUM, M.D., PH.D., LILYANA ANGELOV, M.D., SHIH-YUAN
Minesh Mehta, Northwestern University. Chicago, IL
 * Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
* Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
Surgery for recurrent brain metastases
 Surgery for recurrent brain metastases Pr Philippe METELLUS Neurosurgeon, Clairval Hospital Center, Marseille 8th Annual Brain Metastases Research and Emerging Therapy Conference September 21st, 2018 Conflict
Surgery for recurrent brain metastases Pr Philippe METELLUS Neurosurgeon, Clairval Hospital Center, Marseille 8th Annual Brain Metastases Research and Emerging Therapy Conference September 21st, 2018 Conflict
Nonsmall Cell Lung Cancer Presenting with Synchronous Solitary Brain Metastasis
 1998 Nonsmall Cell Lung Cancer Presenting with Synchronous Solitary Brain Metastasis Chaosu Hu, M.D. 1 Eric L. Chang, M.D. 2 Samuel J. Hassenbusch III, M.D., Ph.D. 3 Pamela K. Allen, Ph.D. 2 Shiao Y. Woo,
1998 Nonsmall Cell Lung Cancer Presenting with Synchronous Solitary Brain Metastasis Chaosu Hu, M.D. 1 Eric L. Chang, M.D. 2 Samuel J. Hassenbusch III, M.D., Ph.D. 3 Pamela K. Allen, Ph.D. 2 Shiao Y. Woo,
CME. Special Article. Received 27 October 2011; revised 9 December 2011; accepted 15 December Practical Radiation Oncology (2012) 2,
 2,") Practical Radiation Oncology (2012) 2, 210 225 CME www.practicalradonc.org Special Article Radiotherapeutic and surgical management for newly diagnosed brain metastasis(es): An American Society for Radiation
Practical Radiation Oncology (2012) 2, 210 225 CME www.practicalradonc.org Special Article Radiotherapeutic and surgical management for newly diagnosed brain metastasis(es): An American Society for Radiation
SBRT for lung metastases: Case report
 SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
Research Article Prognostic Factors in Advanced Non-Small-Cell Lung Cancer Patients: Patient Characteristics and Type of Chemotherapy
 SAGE-Hindawi Access to Research Lung Cancer International Volume 2011, Article ID 152125, 4 pages doi:10.4061/2011/152125 Research Article Prognostic Factors in Advanced Non-Small-Cell Lung Cancer Patients:
SAGE-Hindawi Access to Research Lung Cancer International Volume 2011, Article ID 152125, 4 pages doi:10.4061/2011/152125 Research Article Prognostic Factors in Advanced Non-Small-Cell Lung Cancer Patients:
Correspondence should be addressed to Alicia McMaster;
 Cancer Research Volume 2013, Article ID 308236, 5 pages http://dx.doi.org/10.1155/2013/308236 Research Article Taxpas: Epidemiological and Survival Data in Breast Cancer Patients Treated with a Docetaxel-Based
Cancer Research Volume 2013, Article ID 308236, 5 pages http://dx.doi.org/10.1155/2013/308236 Research Article Taxpas: Epidemiological and Survival Data in Breast Cancer Patients Treated with a Docetaxel-Based
CNS Metastases in Breast Cancer
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer CNS Metastases in Breast Cancer CNS Metastases in Breast Cancer Version 2006: Maass / Junkermann Version 2007 2009: Bischoff
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer CNS Metastases in Breast Cancer CNS Metastases in Breast Cancer Version 2006: Maass / Junkermann Version 2007 2009: Bischoff
Case Report Carbon Ion Beam Radiotherapy for Sinonasal Malignant Tumors Invading Skull Base
 Case Reports in Otolaryngology, Article ID 241856, 4 pages http://dx.doi.org/10.1155/2014/241856 Case Report Carbon Ion Beam Radiotherapy for Sinonasal Malignant Tumors Invading Skull Base Nobuo Ohta,
Case Reports in Otolaryngology, Article ID 241856, 4 pages http://dx.doi.org/10.1155/2014/241856 Case Report Carbon Ion Beam Radiotherapy for Sinonasal Malignant Tumors Invading Skull Base Nobuo Ohta,
Clinical Study Clinical Outcomes of Stereotactic Body Radiotherapy for Patients with Lung Tumors in the State of Oligo-Recurrence
 Pulmonary Medicine Volume 2012, Article ID 369820, 5 pages doi:10.1155/2012/369820 Clinical Study Clinical Outcomes of Stereotactic Body Radiotherapy for Patients with Lung Tumors in the State of Oligo-Recurrence
Pulmonary Medicine Volume 2012, Article ID 369820, 5 pages doi:10.1155/2012/369820 Clinical Study Clinical Outcomes of Stereotactic Body Radiotherapy for Patients with Lung Tumors in the State of Oligo-Recurrence
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
Clinical Study Survival Prediction Score: A Simple but Age-Dependent Method Predicting Prognosis in Patients Undergoing Palliative Radiotherapy
 ISRN Oncology, Article ID 912865, 5 pages http://dx.doi.org/10.1155/2014/912865 Clinical Study Survival Prediction Score: A Simple but Age-Dependent Method Predicting Prognosis in Patients Undergoing Palliative
ISRN Oncology, Article ID 912865, 5 pages http://dx.doi.org/10.1155/2014/912865 Clinical Study Survival Prediction Score: A Simple but Age-Dependent Method Predicting Prognosis in Patients Undergoing Palliative
Case Report Intracranial Capillary Hemangioma in the Posterior Fossa of an Adult Male
 Case Reports in Radiology Volume 2016, Article ID 6434623, 4 pages http://dx.doi.org/10.1155/2016/6434623 Case Report Intracranial Capillary Hemangioma in the Posterior Fossa of an Adult Male Jordan Nepute,
Case Reports in Radiology Volume 2016, Article ID 6434623, 4 pages http://dx.doi.org/10.1155/2016/6434623 Case Report Intracranial Capillary Hemangioma in the Posterior Fossa of an Adult Male Jordan Nepute,
Case Report Tackling a Recurrent Pinealoblastoma
 Case Reports in Oncological Medicine, Article ID 135435, 4 pages http://dx.doi.org/10.1155/2014/135435 Case Report Tackling a Recurrent Pinealoblastoma Siddanna Palled, 1 Sruthi Kalavagunta, 1 Jaipal Beerappa
Case Reports in Oncological Medicine, Article ID 135435, 4 pages http://dx.doi.org/10.1155/2014/135435 Case Report Tackling a Recurrent Pinealoblastoma Siddanna Palled, 1 Sruthi Kalavagunta, 1 Jaipal Beerappa
Potential role for LINAC-based stereotactic radiosurgery for the treatment of 5 or more radioresistant melanoma brain metastases
 clinical article J Neurosurg 123:1261 1267, 2015 Potential role for LINAC-based stereotactic radiosurgery for the treatment of 5 or more radioresistant melanoma brain metastases *Jessica M. Frakes, MD,
clinical article J Neurosurg 123:1261 1267, 2015 Potential role for LINAC-based stereotactic radiosurgery for the treatment of 5 or more radioresistant melanoma brain metastases *Jessica M. Frakes, MD,
Surgical Management of Brain Metastases
 Surgical Management of Brain Metastases Christopher P. Kellner, MD a, Anthony L. D Ambrosio, MD a,b,c, * KEYWORDS Brain Management Metastasis Metastases Resection Surgery Secondary metastases to the brain
Surgical Management of Brain Metastases Christopher P. Kellner, MD a, Anthony L. D Ambrosio, MD a,b,c, * KEYWORDS Brain Management Metastasis Metastases Resection Surgery Secondary metastases to the brain
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Management of Brain Metastases Dr. Luis Souhami Professor Department of Radiation Oncology University,
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Management of Brain Metastases Dr. Luis Souhami Professor Department of Radiation Oncology University,
STEREOTACTIC RADIOSURGERY FOR LIMITED BRAIN METASTASES IN IRANIAN BREAST CANCER PATIENTS
 STEREOTACTIC RADIOSURGERY FOR LIMITED BRAIN METASTASES IN IRANIAN BREAST CANCER PATIENTS Yousefi Kashi A. SH, Mofid B. 1 Department of Radiation Oncology,Shohada Tajrish Hospital,Shahid Beheshti University
STEREOTACTIC RADIOSURGERY FOR LIMITED BRAIN METASTASES IN IRANIAN BREAST CANCER PATIENTS Yousefi Kashi A. SH, Mofid B. 1 Department of Radiation Oncology,Shohada Tajrish Hospital,Shahid Beheshti University
Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
 Case Reports in Cardiology Volume 2016, Article ID 4979182, 4 pages http://dx.doi.org/10.1155/2016/4979182 Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
Case Reports in Cardiology Volume 2016, Article ID 4979182, 4 pages http://dx.doi.org/10.1155/2016/4979182 Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
Prognostic Factors for Survival in Patients Treated With Stereotactic Radiosurgery for Recurrent Brain Metastases After Prior Whole Brain Radiotherapy
 International Journal of Radiation Oncology biology physics www.redjournal.org Clinical Investigation: Metastases Prognostic Factors for Survival in Patients Treated With Stereotactic Radiosurgery for
International Journal of Radiation Oncology biology physics www.redjournal.org Clinical Investigation: Metastases Prognostic Factors for Survival in Patients Treated With Stereotactic Radiosurgery for
AUTHOR S PERSONAL COPY
 Clinical Outcomes of Stereotactic Radiosurgery in the Treatment of Patients with Metastatic Brain Tumors Ameer L. Elaimy 1,2, Alexander R. Mackay 1,3, Wayne T. Lamoreaux 1,2, Robert K. Fairbanks 1,2, John
Clinical Outcomes of Stereotactic Radiosurgery in the Treatment of Patients with Metastatic Brain Tumors Ameer L. Elaimy 1,2, Alexander R. Mackay 1,3, Wayne T. Lamoreaux 1,2, Robert K. Fairbanks 1,2, John
Clinical Study High-Dose Interleukin-2 (HD IL-2) Therapy Should Be Considered for Treatment of Patients with Melanoma Brain Metastases
 Therapy Should Be Considered for Treatment of Patients with Melanoma Brain Metastases") Chemotherapy Research and Practice Volume 2013, Article ID 726925, 7 pages http://dx.doi.org/10.1155/2013/726925 Clinical Study High-Dose Interleukin-2 (HD IL-2) Therapy Should Be Considered for Treatment
Chemotherapy Research and Practice Volume 2013, Article ID 726925, 7 pages http://dx.doi.org/10.1155/2013/726925 Clinical Study High-Dose Interleukin-2 (HD IL-2) Therapy Should Be Considered for Treatment
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Case Report Three-Dimensional Dual-Energy Computed Tomography for Enhancing Stone/Stent Contrasting and Stone Visualization in Urolithiasis
 Case Reports in Urology Volume 2013, Article ID 646087, 4 pages http://dx.doi.org/10.1155/2013/646087 Case Report Three-Dimensional Dual-Energy Computed Tomography for Enhancing Stone/Stent Contrasting
Case Reports in Urology Volume 2013, Article ID 646087, 4 pages http://dx.doi.org/10.1155/2013/646087 Case Report Three-Dimensional Dual-Energy Computed Tomography for Enhancing Stone/Stent Contrasting
Is it cost-effective to treat brain metastasis with advanced technology?
 Is it cost-effective to treat brain metastasis with advanced technology? Cost-effectiveness analysis of whole brain RT, stereotactic radiosurgery and craniotomy in HA setting Lam, Tai-Chung, Choi CW Horace,
Is it cost-effective to treat brain metastasis with advanced technology? Cost-effectiveness analysis of whole brain RT, stereotactic radiosurgery and craniotomy in HA setting Lam, Tai-Chung, Choi CW Horace,
Review Article Surgical Brain Metastases: Management and Outcome Related to Prognostic Indexes: A Critical Review of a Ten-Year Series
 International Scholarly Research Network ISRN Surgery Volume 2011, Article ID 207103, 8 pages doi:10.5402/2011/207103 Review Article Surgical Brain Metastases: Management and Outcome Related to Prognostic
International Scholarly Research Network ISRN Surgery Volume 2011, Article ID 207103, 8 pages doi:10.5402/2011/207103 Review Article Surgical Brain Metastases: Management and Outcome Related to Prognostic
Place of tumor bed radiosurgery and focal radiotherapy following resec7on of brain metastases: A new paradigm Lucyna Kepka
 Place of tumor bed radiosurgery and focal radiotherapy following resec7on of brain metastases: A new paradigm Lucyna Kepka Department of Radia7on Oncology; M. Sklodowska- Curie Memorial Cancer Center and
Place of tumor bed radiosurgery and focal radiotherapy following resec7on of brain metastases: A new paradigm Lucyna Kepka Department of Radia7on Oncology; M. Sklodowska- Curie Memorial Cancer Center and
Lung cancer is the most common malignancy in the. Gamma Knife radiosurgery for the management of cerebral metastases from non small cell lung cancer
 clinical article J Neurosurg 122:766 772, 2015 Gamma Knife radiosurgery for the management of cerebral metastases from non small cell lung cancer Greg Bowden, MD, MSc, 1,3,5 Hideyuki Kano, MD, PhD, 1,3
clinical article J Neurosurg 122:766 772, 2015 Gamma Knife radiosurgery for the management of cerebral metastases from non small cell lung cancer Greg Bowden, MD, MSc, 1,3,5 Hideyuki Kano, MD, PhD, 1,3
See the corresponding editorial in this issue, pp J Neurosurg 114: , 2011
 See the corresponding editorial in this issue, pp 790 791. J Neurosurg 114:792 800, 2011 Stereotactic radiosurgery as primary and salvage treatment for brain metastases from breast cancer Clinical article
See the corresponding editorial in this issue, pp 790 791. J Neurosurg 114:792 800, 2011 Stereotactic radiosurgery as primary and salvage treatment for brain metastases from breast cancer Clinical article
Brain and Spine Tumors
 Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Clinical Study on Prognostic Factors and Nursing of Breast Cancer with Brain Metastases
 Clinical Study on Prognostic Factors and Nursing of Breast Cancer with Brain Metastases Ying Zhou 1#, Kefang Zhong 1#, Fang Zhou* 2 ABSTRACT This paper aims to explore the clinical features and prognostic
Clinical Study on Prognostic Factors and Nursing of Breast Cancer with Brain Metastases Ying Zhou 1#, Kefang Zhong 1#, Fang Zhou* 2 ABSTRACT This paper aims to explore the clinical features and prognostic
Radiotherapy for Brain Metastases
 Radiotherapy for Brain Metastases Robert B. Den, MD a, David W. Andrews, MD b, * KEYWORDS Brain metastases Treatment approaches SRS WBRT The optimal treatment of brain metastases remains controversial.
Radiotherapy for Brain Metastases Robert B. Den, MD a, David W. Andrews, MD b, * KEYWORDS Brain metastases Treatment approaches SRS WBRT The optimal treatment of brain metastases remains controversial.
Case Report Metastatic Malignant Melanoma of Parotid Gland with a Regressed Primary Tumor
 Case Reports in Otolaryngology Volume 2016, Article ID 5393404, 4 pages http://dx.doi.org/10.1155/2016/5393404 Case Report Metastatic Malignant Melanoma of Parotid Gland with a Regressed Primary Tumor
Case Reports in Otolaryngology Volume 2016, Article ID 5393404, 4 pages http://dx.doi.org/10.1155/2016/5393404 Case Report Metastatic Malignant Melanoma of Parotid Gland with a Regressed Primary Tumor
Treatment of Recurrent Brain Metastases
 Treatment of Recurrent Brain Metastases Penny K. Sneed, M.D. Dept. of Radiation Oncology University of California San Francisco Background Brain metastases occur in 8.5-15% of cancer pts in population-
Treatment of Recurrent Brain Metastases Penny K. Sneed, M.D. Dept. of Radiation Oncology University of California San Francisco Background Brain metastases occur in 8.5-15% of cancer pts in population-
Outcome of Surgical Resection of Symptomatic Cerebral Lesions in Non-Small Cell Lung Cancer Patients with Multiple Brain Metastases
 ORIGIL ARTICLE Brain Tumor Res Treat 2013;1:64-70 / Print ISSN 2288-2405 / Online ISSN 2288-2413 online ML Comm Outcome of Surgical Resection of Symptomatic Cerebral Lesions in Non-Small Cell Lung Cancer
ORIGIL ARTICLE Brain Tumor Res Treat 2013;1:64-70 / Print ISSN 2288-2405 / Online ISSN 2288-2413 online ML Comm Outcome of Surgical Resection of Symptomatic Cerebral Lesions in Non-Small Cell Lung Cancer
Palliative radiotherapy in lung cancer
 New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
Original Date: April 2016 Page 1 of 7 FOR CMS (MEDICARE) MEMBERS ONLY
 MEMBERS ONLY") National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIATION THERAPY: STEREO RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: Please refer to pages 5-6 LCD
National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIATION THERAPY: STEREO RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: Please refer to pages 5-6 LCD
Clinical Study The Value of Programmable Shunt Valves for the Management of Subdural Collections in Patients with Hydrocephalus
 The Scientific World Journal Volume 2013, Article ID 461896, 4 pages http://dx.doi.org/10.1155/2013/461896 Clinical Study The Value of Programmable Shunt Valves for the Management of Subdural Collections
The Scientific World Journal Volume 2013, Article ID 461896, 4 pages http://dx.doi.org/10.1155/2013/461896 Clinical Study The Value of Programmable Shunt Valves for the Management of Subdural Collections
Prognostic indices in stereotactic radiotherapy of brain metastases of non-small cell lung cancer
 Kaul et al. Radiation Oncology (2015) 10:244 DOI 10.1186/s13014-015-0550-1 RESEARCH Open Access Prognostic indices in stereotactic radiotherapy of brain metastases of non-small cell lung cancer David Kaul
Kaul et al. Radiation Oncology (2015) 10:244 DOI 10.1186/s13014-015-0550-1 RESEARCH Open Access Prognostic indices in stereotactic radiotherapy of brain metastases of non-small cell lung cancer David Kaul
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
Case Report Complex Form Variant of Dysembryoplastic Neuroepithelial Tumor of the Cerebellum
 Case Reports in Pathology Volume 2012, Article ID 718651, 4 pages doi:10.1155/2012/718651 Case Report Complex Form Variant of Dysembryoplastic Neuroepithelial Tumor of the Cerebellum Jesús Vaquero, 1,
Case Reports in Pathology Volume 2012, Article ID 718651, 4 pages doi:10.1155/2012/718651 Case Report Complex Form Variant of Dysembryoplastic Neuroepithelial Tumor of the Cerebellum Jesús Vaquero, 1,
FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR HAEMANGIOBLASTOMA
 1 EVIDENCE SUMMARY REPORT FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR HAEMANGIOBLASTOMA QUESTIONS TO BE ADDRESSED: 1. What is the evidence for the clinical effectiveness
1 EVIDENCE SUMMARY REPORT FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR HAEMANGIOBLASTOMA QUESTIONS TO BE ADDRESSED: 1. What is the evidence for the clinical effectiveness
Brain metastases: changing visions
 Brain metastases: changing visions Roberto Spiegelmann, MD Baiona, 2014 Head, Stereotactic Radiosurgery Unit Dept of Neurosurgery, Chaim Sheba Medical Center Tel Hashomer, Israel The best current estimate
Brain metastases: changing visions Roberto Spiegelmann, MD Baiona, 2014 Head, Stereotactic Radiosurgery Unit Dept of Neurosurgery, Chaim Sheba Medical Center Tel Hashomer, Israel The best current estimate
Treatment of Brain Metastases
 1 Treatment of Brain Metastases An Overview and Pending Research Questions To Answer Olav E. Yri, MD, PhD www.ntnu.no/prc European Palliative Care Research Centre (PRC) The brain metastases diagnosis Outline
1 Treatment of Brain Metastases An Overview and Pending Research Questions To Answer Olav E. Yri, MD, PhD www.ntnu.no/prc European Palliative Care Research Centre (PRC) The brain metastases diagnosis Outline
Clinical Commissioning Policy: Stereotactic Radiosurgery / Radiotherapy For Cerebral Metastases. December Reference : NHSCB/D5/1
 Clinical Commissioning Policy: Stereotactic Radiosurgery / Radiotherapy For Cerebral Metastases December 2012 Reference : NHSCB/D5/1 NHS Commissioning Board Clinical Commissioning Policy: Stereotactic
Clinical Commissioning Policy: Stereotactic Radiosurgery / Radiotherapy For Cerebral Metastases December 2012 Reference : NHSCB/D5/1 NHS Commissioning Board Clinical Commissioning Policy: Stereotactic
Comparative Analysis of Efficacy and Safety of Multisession Radiosurgery to Single Dose Radiosurgery for Metastatic Brain Tumors
 ORIGINAL ARTICLE Brain Tumor Res Treat 2015;3(2):95-102 / pissn 2288-2405 / eissn 2288-2413 http://dx.doi.org/10.14791/btrt.2015.3.2.95 Comparative Analysis of Efficacy and Safety of Multisession Radiosurgery
ORIGINAL ARTICLE Brain Tumor Res Treat 2015;3(2):95-102 / pissn 2288-2405 / eissn 2288-2413 http://dx.doi.org/10.14791/btrt.2015.3.2.95 Comparative Analysis of Efficacy and Safety of Multisession Radiosurgery
Clinical significance of conformity index and gradient index in patients undergoing stereotactic radiosurgery for a single metastatic tumor
 CLINICAL ARTICLE J Neurosurg (Suppl) 129:103 110, 2018 Clinical significance of conformity index and gradient index in patients undergoing stereotactic radiosurgery for a single metastatic tumor Hitoshi
CLINICAL ARTICLE J Neurosurg (Suppl) 129:103 110, 2018 Clinical significance of conformity index and gradient index in patients undergoing stereotactic radiosurgery for a single metastatic tumor Hitoshi
Case Report A Case of Primary Submandibular Gland Oncocytic Carcinoma
 Case Reports in Otolaryngology Volume 2013, Article ID 384238, 4 pages http://dx.doi.org/10.1155/2013/384238 Case Report A Case of Primary Submandibular Gland Oncocytic Carcinoma Kunihiko Tokashiki, Kiyoaki
Case Reports in Otolaryngology Volume 2013, Article ID 384238, 4 pages http://dx.doi.org/10.1155/2013/384238 Case Report A Case of Primary Submandibular Gland Oncocytic Carcinoma Kunihiko Tokashiki, Kiyoaki