Objectives. Intraoperative Consultation of the Whipple Resection Specimen. Pancreas Anatomy. Pancreatic ductal carcinoma 11/10/2014
|
|
|
- Josephine Allison
- 6 years ago
- Views:
Transcription

 portal vein bile duct neck head duodenum uncinate SMV SMA aorta body tail pancreas")
1 Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook Health Sciences Centre Objectives Review of anatomy, orientation of Whipple resection Variations in specimen dissection, reporting of Whipple specimens Does FS during Whipple resection improve outcome? Examples of FS in Whipple resections Pancreas Anatomy vena cava The Whipple Resection (Pancreaticoduodenectomy) portal vein bile duct neck head duodenum uncinate SMV SMA aorta body tail pancreas Resection of tumours involving the head of pancreas Partial or total pancreatectomy Entire duodenum, distal stomach Bile duct, gallbladder May include portion of portal vein, SMV, SMA The Whipple resection Pancreatic ductal carcinoma Neoplasms of Pancreas Peri ampullary and ampullary regions Second part of duodenum Distal bile duct Chronic pancreatitis Aggressive tumour with poor survival XRT and chemo limited benefit Resection only chance for cure Only 10 20% are deemed resectable 75 85% recur post resection (local & distant) Reported R1 resection rate 15 80% Role of FS in improving R0 rate and survival? 1



, 11:282 9 The Whipple Specimen Anatomical Relationships The Whipple Specimen bile duct margin Anterior")


2 Margin status in Whipple Margin status is a key prognostic factor Reported R1 rates very variable, but outcomes similar Margin status is determined by Surgeon surgical technique Pathologist sampling and assessment of margins A low R1 rate may not be an indicator of high quality surgical technique, but suboptimal margin assessment by pathologist Verbele CS, Menon KV. HPB (2009), 11:282 9 Margin status in Whipple Variability in terminology of margins, grossing of specimen, pathological reporting Terminology of margins Pancreatic neck, anterior Uncinate, SMA, retroperitoneal Posterior, retroperitoneal Portal vein groove, medial Verbele CS, Menon KV. HPB (2009), 11:282 9 The Whipple Specimen Anatomical Relationships The Whipple Specimen bile duct margin Anterior BILE DUCT STOMACH neck margin vein groove uncinate margin posterior margin GB vena cava splenic v. portal v. SMA left renal v. aorta PANCREAS anterior surface Medial View Right T1 vertebra Posterior Transverse View Left DUODENUM Modified from Verbeke 2009 POSTERIOR VIEW The Whipple Specimen Margin status in Whipple Specimen dissection techniques Axial slicing favored in Europe More extensive assessment of margins, higher R1 rates Openingof ducts favored in North America Better anatomic orientation for ampullary tumours Definition of R1 0 mm in North America <=1 mm in Europe POSTERIOR VIEW Verbele CS, Menon KV. HPB (2009), 11:
3 True positive margin? LVI, PNI Tumour in lymph node Detached tumour in lumen of duct At FS, report the presence of tumour cells and their location to surgeon Is revision required for margin? R1 rate and survival pancreatic carcinoma Study # cases R1/R2 rate (%) R1/R2 median survival (months) R0 median survival (months) Menon (2009) >55 Verbeke (2006) Raut (2007) Sohn (2000) R0 survival in studies with low R1 rate remain low similar to R1 group R0 survival in studies with high R1 rate is much higher than R1 group Implies studies with low R1 rate has many R0 cases that are really under sampled R1 cases In several institutions, modifying specimen dissection protocol increases R1 rate Table modified from: Verbele CS, Menon KV. HPB (2009), 11:282 9 Effect of FS on survival Hernandez J et al Survival after pancreaticoduodenectomy is not improved by extending resections to achieve negative margins Annuals of Surgery (2009) 250:76 80 Mathur A et al Margin status impacts survival after Pancreaticoduodenectomy but negative margins should not be pursued The American Surgeon (2014) 80: (from U South Florida, Tampa, FL) Effect of FS on survival Lad NL et al Is it time to stop checking frozen section neck margins during pancreaticoduodenectomy? Annuals of Surgical Oncology (2013) 20: Kooby DA et al Value of intraoperative neck margin analysis during Whipple for pancreatic adenocarcinoma. A multicenter analysis of 1399 patients. Annuals of Surgery (2014) 260(3): Kooby et al. Value of intraoperative neck margin analysis during Whipple for pancreatic adenocarcinoma. Annuals of Surgery (2014), 260: Distribution of cases by FS & PS neck margin status Multi institutional retrospective analysis of cases from the Central Pancreas Consortium Emory U, U Wisconsin, Northwestern U, U Cincinnati, U North Carolina, U Louisville, Vanderbuilt U, Washington U 1399 cases of pancreatic ductal adenocarcinoma with FS of neck margin Cases associated with IPMN excluded R0 > 1mm Kooby et al. Ann Surg (2014), 260:
4 OS by margin status, all patients OS stratified by neck margin status Kooby et al. Ann Surg (2014), 260: Kooby et al. Ann Surg (2014), 260: OS stratified by neck margin status, negative uncinate margin patients only Effect of FS on Survival Negative initial margin at FS correlates with better survival Revised negative margin after initial positive margin has same survival as those with unrevised positive margin Positive initial margin at FS is associated with Larger tumour size More node positivity PV/SMA resection Trend toward more frequent uncinate margin positivity Kooby et al. Ann Surg (2014), 260: Kooby et al. Ann Surg (2014), 260: FS of Whipple Specimen Be prepared History, radiological dx, previous biopsy / cytology Many cases have no prior tissue diagnosis Initial FS In the old days, sample from tumour for confirmation of malignancy From metastatic sites liver, peritoneum, LN s, if positive, may abort procedure FS margin assessment separately submitted pieces dissected from Whipple specimen Ask surgeon which margin is needed! FS of Whipple Specimen Whipple margins for FS Bile duct margin Pancreatic neck margin (if partial) Pancreatic neck margin (if partial) Uncinate margin Vascular margin, if present 4






 Reported as positive if any")

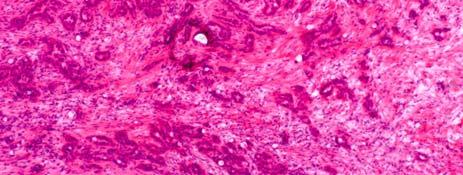
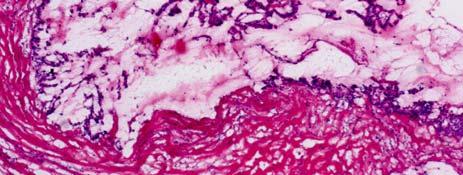
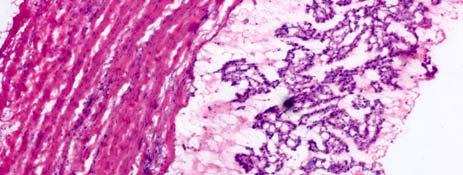
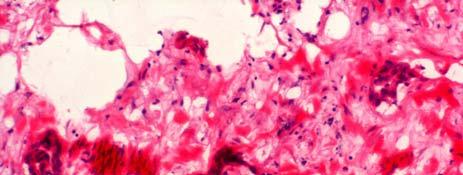
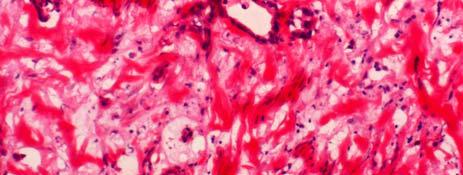
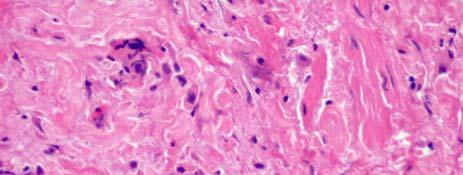
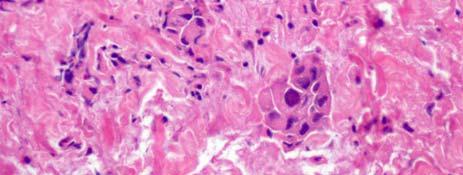
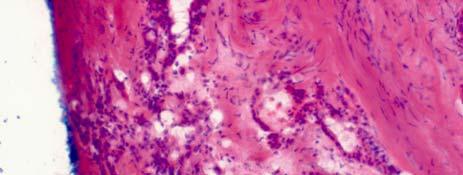
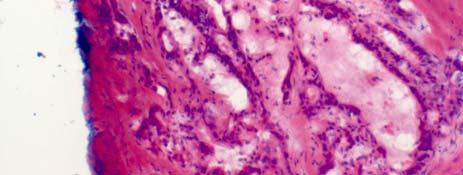
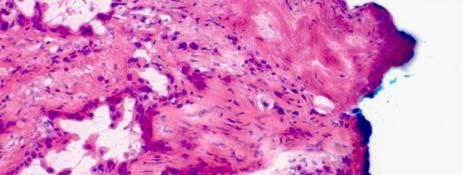
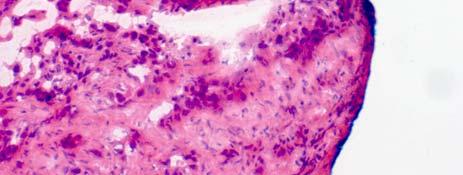
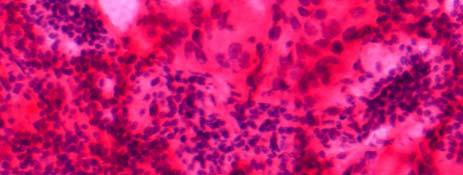
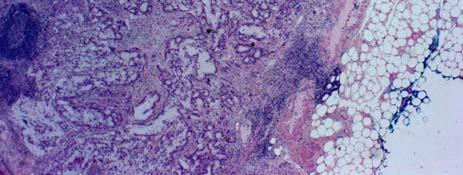
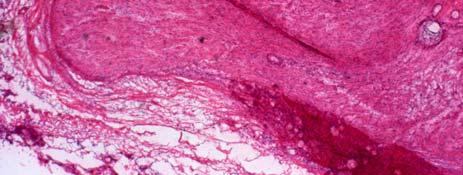
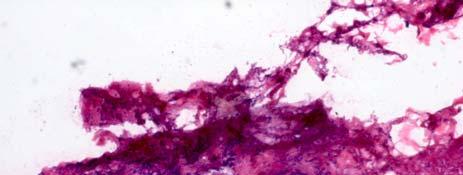
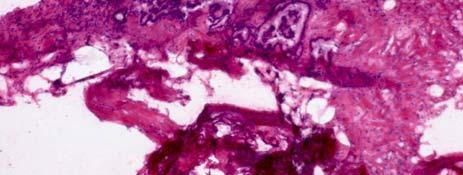
5 FS of Whipple Specimen Histological challenges Pancreatic pathology difficult even on paraffin sections. FS artifacts add to difficulty. Tumour may be difficult to distinguish from chronic pancreatitis Tumour desmoplasia versus fibrosis Residual islets versus NET Inflammatory changes in bile duct from obstruction, stent Features favoring carcinoma Disorganized duct distribution Variation in nuclear size >= 4:1 Incomplete duct lumen Disorganized stroma Single cell infiltration Cribriform glands Epithelial mitoses Necrotic glandular debris Large nucleoli Perineural invasion Pancreatic margin Routinely sampled in most cases requiring FS Usually sectioned en face (shaved) Reported as positive if any tumour cells present on slide Report high grade dysplasia in ducts if present Cioc AM et al. Arch Pathol Lab Med 2002(126): PNI! benign benign atrophic ducts & residual islets 5






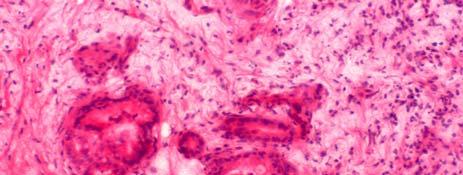

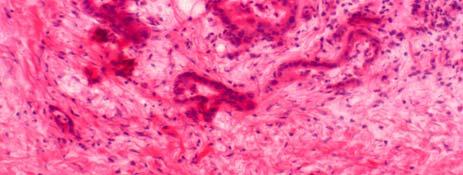
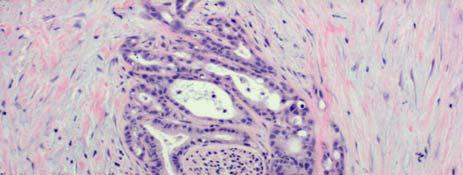

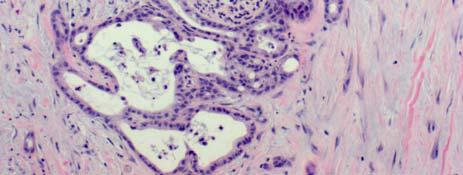
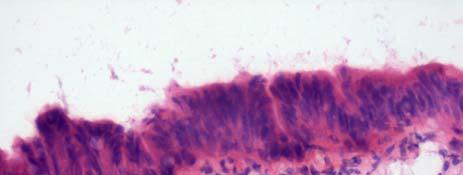
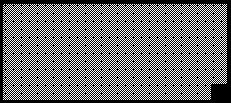
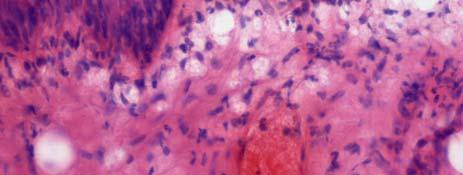
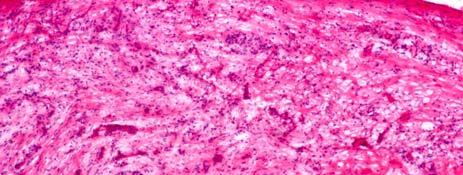
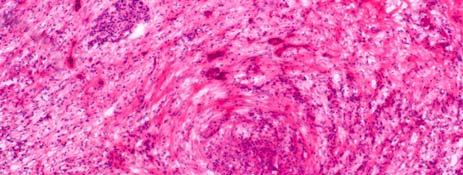
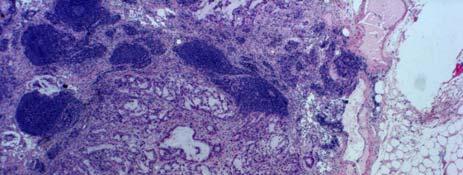
6 PNI! PNI! atrophic ducts & residual islets PS neck margin CASE 2 high grade dysplasia benign atrophic ducts & residual islets 6









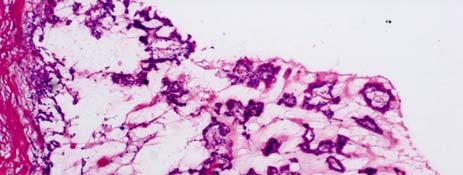

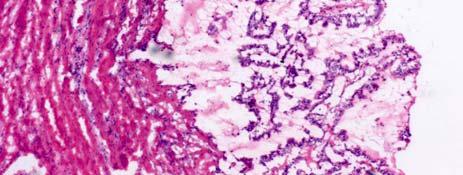
7 CASE 2 CASE 2 CASE 2 CASE 2 FS revised neck margin bigger tumour focus present atrophic ducts & residual islets CASE 3 IPMN in main duct CASE 3 IPMN in main duct surgeon proceeded with completion pancreatectomy 7













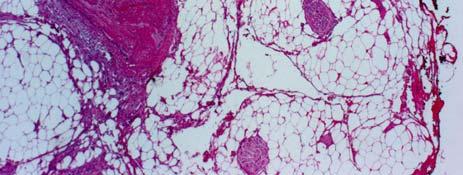
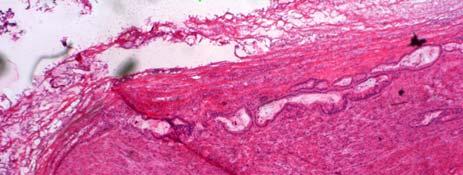
8 CASE 3 PS distal pancreas IPMN & adenocarcinoma in completion pancreatectomy CASE 4 cystic mucinous lesion CASE 4 cystic mucinous lesion CASE 4 cystic mucinous lesion CASE 4 PS pancreas IPMN & adenocarcinoma Uncinate Margin Area inked, removed and serially sectioned perpendicularly May require many FS blocks Often fatty, hard to cut on cryostat Is FS really needed? Current surgical protocol specifies removal of all tissues around the SMA, so even if margin is positive on FS, no additional tissue can be removed. 8







9 CASE 5 CASE 5 PS uncinate margin CASE 5 CASE 5 PS uncinate margin CASE 6 CASE 6 tumour at inked surface tumour at inked surface 9






10 CASE 6 FS revised uncinate margin CASE 7 PNI inked margin CASE 7 CASE 7 PS uncinate margin lymph node? negative at inked margin but < 1 mm, no additional margin taken CASE 7 CASE 8 PNI 10










11 CASE 8 PS uncinate margin negative at ink Bile Duct Margin FS performed frequently, but seldom positive Usually provided as separate tissue piece Reactive changes common, especially if prior stent in place Normal intramural glands versus adenocarcinoma Look for tumour in nerves, LN s Vascular Margin CASE 9 FS PV margin Uncommon FS Segment of vessel (take end margins en face) Patch of vessel (depending on size, may section en face circumferentially or serially section perpendicularly like skin ellipse) Ask surgeon if FS desired May take more vessel if positive May proceed to resection of vessel + graft CASE 9 FS PV margin References Kooby DA et al. Value of intraoperative neck margin analysis during Whipple for pancreatic adenocarcinoma. Annuals of Surgery 2014; 260: Mather A et al. Margin status impacts survival after pancreaticoduodenectomy but negative margins should not be pursued. The American Surgeon 2014;80: Verbeke CS, Menon KV. Refining resection margin status in pancreatic cancer. HPB 2009; 11:282 9 Khalifa MA. Intraoperative assessment of the Whipple resection specimen. J Clin Pathol 2007;60: Cioc AM et al. Frozen section diagnosis of pancreatic lesions. Arch Pathol Lab Med 2002, 126:
Pancreatobiliary Frozen Section Nightmares
 Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Gross examination of pancreaticobiliary cancer specimens. Dr Vlad Maksymov MD, PhD, FRCPC OPA meeting September
 Gross examination of pancreaticobiliary cancer specimens Dr Vlad Maksymov MD, PhD, FRCPC OPA meeting September 17 2017 Learning Objectives Review issues related to the surgical anatomy and gross examination
Gross examination of pancreaticobiliary cancer specimens Dr Vlad Maksymov MD, PhD, FRCPC OPA meeting September 17 2017 Learning Objectives Review issues related to the surgical anatomy and gross examination
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Evaluation of All Surgical Margins in Pancreatic Resection Specimens by Proper Grossing Techniques: Surgical Pathology Experience of 285 Cases
 Original Article doi: 0.6/tjpath.08.06 Evaluation of All Surgical Margins in Pancreatic Resection Specimens by Proper Grossing Techniques: Surgical Pathology Experience of 8 Cases Özgür EKİNCİ Department
Original Article doi: 0.6/tjpath.08.06 Evaluation of All Surgical Margins in Pancreatic Resection Specimens by Proper Grossing Techniques: Surgical Pathology Experience of 8 Cases Özgür EKİNCİ Department
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas.
 Protocol applies to all carcinomas of the exocrine pancreas.") Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Is it Time to Stop Checking Frozen Section Neck Margins During Pancreaticoduodenectomy?
 Ann Surg Oncol (2013) 20:3626 3633 DOI 10.1245/s10434-013-3080-9 ORIGINAL ARTICLE PANCREATIC TUMORS Is it Time to Stop Checking Frozen Section Neck Margins During Pancreaticoduodenectomy? Neha L. Lad,
Ann Surg Oncol (2013) 20:3626 3633 DOI 10.1245/s10434-013-3080-9 ORIGINAL ARTICLE PANCREATIC TUMORS Is it Time to Stop Checking Frozen Section Neck Margins During Pancreaticoduodenectomy? Neha L. Lad,
An anatomical-based mapping analysis of the pancreaticoduodenectomy retroperitoneal margin highlights the urgent need for standardized assessment
 DOI:10.1111/j.1477-2574.2012.00561.x HPB ORIGINAL ARTICLE An anatomical-based mapping analysis of the pancreaticoduodenectomy retroperitoneal margin highlights the urgent need for standardized assessment
DOI:10.1111/j.1477-2574.2012.00561.x HPB ORIGINAL ARTICLE An anatomical-based mapping analysis of the pancreaticoduodenectomy retroperitoneal margin highlights the urgent need for standardized assessment
Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment
 Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment Andrew W. Bowman, MD PhD Assistant Professor of Radiology Mayo Clinic Florida SCBT-MR Annual Meeting Nashville,
Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment Andrew W. Bowman, MD PhD Assistant Professor of Radiology Mayo Clinic Florida SCBT-MR Annual Meeting Nashville,
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Pancreaticoduodenectomy the anatomy and the surgical approaches
 Pancreaticoduodenectomy the anatomy and the surgical approaches Paul BS LAI Division of Hepato biliary and Pancreatic Surgery Department of Surgery The Chinese Univesity of Hong Kong Whipple s operation
Pancreaticoduodenectomy the anatomy and the surgical approaches Paul BS LAI Division of Hepato biliary and Pancreatic Surgery Department of Surgery The Chinese Univesity of Hong Kong Whipple s operation
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012
 Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Topics: Staging and treatment for pancreatic cancer. Staging systems for pancreatic cancer: Differences between the Japanese and UICC systems
 M. J Hep Kobari Bil Pancr and S. Surg Matsuno: (1998) Staging 5:121 127 system for pancreatic cancer 121 Topics: Staging and treatment for pancreatic cancer Staging systems for pancreatic cancer: Differences
M. J Hep Kobari Bil Pancr and S. Surg Matsuno: (1998) Staging 5:121 127 system for pancreatic cancer 121 Topics: Staging and treatment for pancreatic cancer Staging systems for pancreatic cancer: Differences
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Endoscopic Ultrasonography Assessment for Ampullary and Bile Duct Malignancy
 Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors
 AJCP / REPORTING RECOMMENDATIONS FOR PANCREATIC SPECIMENS CONTAINING MALIGNANT TUMORS Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors Jorge AlboresSaavedra, David
AJCP / REPORTING RECOMMENDATIONS FOR PANCREATIC SPECIMENS CONTAINING MALIGNANT TUMORS Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors Jorge AlboresSaavedra, David
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
ONCOLOGY. Csaba Bödör. Department of Pathology and Experimental Cancer Research november 19., ÁOK, III.
 ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
Cattell-Braasch maneuver combined with superior mesenteric artery first approach for resection of borderline resectable pancreatic cancer
 Masters of Surgery Page 1 of 5 Cattell-Braasch maneuver combined with superior mesenteric artery first approach for resection of borderline resectable pancreatic cancer Tingsong Yang 1, Fairweather Mark
Masters of Surgery Page 1 of 5 Cattell-Braasch maneuver combined with superior mesenteric artery first approach for resection of borderline resectable pancreatic cancer Tingsong Yang 1, Fairweather Mark
Accessory Glands of Digestive System
 Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Measure Specifications Measure Description
 CMS ID/CMS QCDR ID: CAP 25 Title: Time for Pancreas Specifications Description Percentage of all eligible pancreatic exocrine carcinoma (including small cell and large cell (poorly differentiated) neuroendocrine
CMS ID/CMS QCDR ID: CAP 25 Title: Time for Pancreas Specifications Description Percentage of all eligible pancreatic exocrine carcinoma (including small cell and large cell (poorly differentiated) neuroendocrine
PAPER. Experience With 208 Resections for Intraductal Papillary Mucinous Neoplasm of the Pancreas
 PAPER Experience With 0 Resections for Intraductal Papillary Mucinous Neoplasm of the Pancreas Thomas Schnelldorfer, MD; Michael G. Sarr, MD; David M. Nagorney, MD; Lizhi Zhang, MD; Thomas C. Smyrk, MD;
PAPER Experience With 0 Resections for Intraductal Papillary Mucinous Neoplasm of the Pancreas Thomas Schnelldorfer, MD; Michael G. Sarr, MD; David M. Nagorney, MD; Lizhi Zhang, MD; Thomas C. Smyrk, MD;
Frank Burton Memorial Update on Pancreato-biliary Cancers
 Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Cholangiocarcinoma. Judy Wyatt Dundee November 2010
 Cholangiocarcinoma Judy Wyatt Dundee November 2010 Making sense of cholangiocarcinoma Difficulties with diagnostic criteria How many entities within cholangiocarcinoma? Rapidly evolving Intrahepatic cholangiocarcinoma
Cholangiocarcinoma Judy Wyatt Dundee November 2010 Making sense of cholangiocarcinoma Difficulties with diagnostic criteria How many entities within cholangiocarcinoma? Rapidly evolving Intrahepatic cholangiocarcinoma
Pancreatic Cancer. BIOLOGY: Not well defined (genetic and enviromental factors) CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.
 CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.") EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
6 th August 2018 Day 1 - Gallbladder & Bile duct Topic
 Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
Hilar cholangiocarcinoma. Frank Wessels, Maarten van Leeuwen, UMCU utrecht
 Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Interactive Exhibit On Imaging Updates For Staging And Response Assessment In Pancreatic Cancer
 Interactive Exhibit On Imaging Updates For Staging And Response Assessment In Pancreatic Cancer 1 Vinit Baliyan, MD; 1 Hamed Kordbacheh, MD; 2 Eric P Tamm, MD; 3 Theodore S Hong, MD; 4 Carlos Fernandez-Del
Interactive Exhibit On Imaging Updates For Staging And Response Assessment In Pancreatic Cancer 1 Vinit Baliyan, MD; 1 Hamed Kordbacheh, MD; 2 Eric P Tamm, MD; 3 Theodore S Hong, MD; 4 Carlos Fernandez-Del
Cystic pancreatic lesions A proposal for a network approach. Chris Briggs Consultant HPB Surgeon Peninsula HPB Unit Derriford Hospital, Plymouth
 Cystic pancreatic lesions A proposal for a network approach Chris Briggs Consultant HPB Surgeon Peninsula HPB Unit Derriford Hospital, Plymouth Aims Brief overview of cystic pancreatic lesions International
Cystic pancreatic lesions A proposal for a network approach Chris Briggs Consultant HPB Surgeon Peninsula HPB Unit Derriford Hospital, Plymouth Aims Brief overview of cystic pancreatic lesions International
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Jacob Elebro 1,2* and Karin Jirström 1
 Elebro and Jirström Diagnostic Pathology 2014, 9:80 RESEARCH Open Access Use of a standardized diagnostic approach improves the prognostic information of histopathologic factors in pancreatic and periampullary
Elebro and Jirström Diagnostic Pathology 2014, 9:80 RESEARCH Open Access Use of a standardized diagnostic approach improves the prognostic information of histopathologic factors in pancreatic and periampullary
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Autoimmune Pancreatitis: A Great Imitator
 Massachusetts General Hospital Harvard Medical School Autoimmune Pancreatitis: A Great Imitator Dushyant V Sahani MD dsahani@partners.org Autoimmune Pancreatitis: Learning Objectives Clinical manifestations
Massachusetts General Hospital Harvard Medical School Autoimmune Pancreatitis: A Great Imitator Dushyant V Sahani MD dsahani@partners.org Autoimmune Pancreatitis: Learning Objectives Clinical manifestations
Pancreas and Biliary System
 Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
د. عصام طارق. Objectives:
 GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
Citation American Journal of Surgery, 196(5)
") NAOSITE: Nagasaki University's Ac Title Author(s) Multifocal branch-duct pancreatic i neoplasms Tajima, Yoshitsugu; Kuroki, Tamotsu Amane; Adachi, Tomohiko; Mishima, T Kanematsu, Takashi Citation American
NAOSITE: Nagasaki University's Ac Title Author(s) Multifocal branch-duct pancreatic i neoplasms Tajima, Yoshitsugu; Kuroki, Tamotsu Amane; Adachi, Tomohiko; Mishima, T Kanematsu, Takashi Citation American
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD
 CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
I patients with nonendocrine pancreas carcinoma
 LYMPH NODE INVOLVEMENT IN CARCINOMA OF THE HEAD OF THE PANCREAS AREA ANTONIO L. CUBILLA, MD,* JOSEPH FORTNER, MD,+~ AND PATRICK J. FITZGERALD, MD*~ A prospective study to determine the lymph node involvement
LYMPH NODE INVOLVEMENT IN CARCINOMA OF THE HEAD OF THE PANCREAS AREA ANTONIO L. CUBILLA, MD,* JOSEPH FORTNER, MD,+~ AND PATRICK J. FITZGERALD, MD*~ A prospective study to determine the lymph node involvement
WHICH LYMPH NODES SHOULD BE
 Y.K.: 82 Y.O. WOMAN WITH ANEMIA No GI symptoms. Chronic AF taking coumadin: INR=2.1. HCT=24. Anemia persists despite Rx. Colonoscopy: tumor in ascending colon. Bx: adenocarcinoma. Rx: Laparoscopic right
Y.K.: 82 Y.O. WOMAN WITH ANEMIA No GI symptoms. Chronic AF taking coumadin: INR=2.1. HCT=24. Anemia persists despite Rx. Colonoscopy: tumor in ascending colon. Bx: adenocarcinoma. Rx: Laparoscopic right
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
ORIGINAL ARTICLE. Fate of the Pancreatic Remnant After Resection for an Intraductal Papillary Mucinous Neoplasm
 ONLINE FIRST ORIGINAL ARTICLE Fate of the Pancreatic Remnant After Resection for an Intraductal Papillary Mucinous Neoplasm A Longitudinal Level II Cohort Study Toshiyuki Moriya, MD, PhD; L. William Traverso,
ONLINE FIRST ORIGINAL ARTICLE Fate of the Pancreatic Remnant After Resection for an Intraductal Papillary Mucinous Neoplasm A Longitudinal Level II Cohort Study Toshiyuki Moriya, MD, PhD; L. William Traverso,
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Radical nerve dissection for the carcinoma of head of pancreas: report of 30 cases
 Original Article Radical nerve dissection for the carcinoma of head of pancreas: report of 30 cases Qing Lin, Langping Tan, Yu Zhou, Quanbo Zhou, Rufu Chen Department of Biliary and Pancreatic Surgery,
Original Article Radical nerve dissection for the carcinoma of head of pancreas: report of 30 cases Qing Lin, Langping Tan, Yu Zhou, Quanbo Zhou, Rufu Chen Department of Biliary and Pancreatic Surgery,
Citation Hepato-Gastroenterology, 55(86-87),
,") NAOSITE: Nagasaki University's Ac Title Author(s) Combined pancreatic resection and p multiple lesions of the pancreas: i of the pancreas concomitant with du Kuroki, Tamotsu; Tajima, Yoshitsugu Tomohiko;
NAOSITE: Nagasaki University's Ac Title Author(s) Combined pancreatic resection and p multiple lesions of the pancreas: i of the pancreas concomitant with du Kuroki, Tamotsu; Tajima, Yoshitsugu Tomohiko;
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Collecting Cancer Data: Pancreas
 Collecting Cancer Data: Pancreas NAACCR 2011 2012 Webinar Series 1/5/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Pancreas NAACCR 2011 2012 Webinar Series 1/5/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
5/17/2013. Pancreatic Cancer. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Case presentation. Differential diagnosis
 Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
ORIGINAL ARTICLE. Helical Computed Tomography in the Diagnosis of Portal Vein Invasion by Pancreatic Head Carcinoma
 ORIGINAL ARTICLE Helical Computed Tomography in the Diagnosis of Portal Vein Invasion by Pancreatic Head Carcinoma Usefulness for Selecting Surgical Procedures and Predicting the Outcome Hiroyoshi Furukawa,
ORIGINAL ARTICLE Helical Computed Tomography in the Diagnosis of Portal Vein Invasion by Pancreatic Head Carcinoma Usefulness for Selecting Surgical Procedures and Predicting the Outcome Hiroyoshi Furukawa,
21/07/2017. CS Verbeke. Non-neoplastic disease of the pancreas PATHOLOGY OF NON-NEOPLASTIC PANCREATIC DISEASES
 Non-neoplastic disease of the pancreas No indication for surgical resection of non-neoplastic disease (except end-stage chronic pancreatitis) Unexpected benign disease in 5-13% of pancreatic resections
Non-neoplastic disease of the pancreas No indication for surgical resection of non-neoplastic disease (except end-stage chronic pancreatitis) Unexpected benign disease in 5-13% of pancreatic resections
X-Plain Pancreatic Cancer Reference Summary
 X-Plain Pancreatic Cancer Reference Summary Introduction Pancreatic cancer is the 4th leading cause of cancer deaths in the U.S. About 37,000 new cases of pancreatic cancer are diagnosed each year in the
X-Plain Pancreatic Cancer Reference Summary Introduction Pancreatic cancer is the 4th leading cause of cancer deaths in the U.S. About 37,000 new cases of pancreatic cancer are diagnosed each year in the
Kyle L. Ziegler, CTR. California Cancer Registry U.C. Davis Health System
 Kyle L. Ziegler, CTR California Cancer Registry U.C. Davis Health System Overview New Data Items Reportability Clarifications New Coding Rules Grade ICD-O-3 Changes Collaborative Stage v0205 2 New Data
Kyle L. Ziegler, CTR California Cancer Registry U.C. Davis Health System Overview New Data Items Reportability Clarifications New Coding Rules Grade ICD-O-3 Changes Collaborative Stage v0205 2 New Data
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER
 1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
3/28/2012. Periampullary Tumors. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Eric K. Nakakura Ko Olina, HI
 Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
EDUCATIONAL CASES E1 & E2. Natasha Inglis 20/03/15
 EDUCATIONAL CASES E1 & E2 Natasha Inglis 20/03/15 CASE E1 79 year old female Rectum. Altemeier operation Histology Superficial erosions and mucosal congestion volcano lesion and pseudomembrane formation
EDUCATIONAL CASES E1 & E2 Natasha Inglis 20/03/15 CASE E1 79 year old female Rectum. Altemeier operation Histology Superficial erosions and mucosal congestion volcano lesion and pseudomembrane formation
An Innovative Option for Venous Reconstruction After Pancreaticoduodenectomy: the Left Renal Vein
 J Gastrointest Surg (2007) 11:425 431 DOI 10.1007/s11605-007-0131-1 An Innovative Option for Venous Reconstruction After Pancreaticoduodenectomy: the Left Renal Vein Rory L. Smoot & John D. Christein &
J Gastrointest Surg (2007) 11:425 431 DOI 10.1007/s11605-007-0131-1 An Innovative Option for Venous Reconstruction After Pancreaticoduodenectomy: the Left Renal Vein Rory L. Smoot & John D. Christein &
Small Plicae Circularis. Short Closely packed together. Sparse, completely absent at distal part Lymphoid Nodule
 Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Anatomy of the liver and pancreas
 Anatomy of the liver and pancreas Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk abdulameerh@yahoo.com Liver Aorta Pulm. Trunk Rt. At, Duct. Art. Lt. Ven. Rt. Ven. Internal Posterior
Anatomy of the liver and pancreas Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk abdulameerh@yahoo.com Liver Aorta Pulm. Trunk Rt. At, Duct. Art. Lt. Ven. Rt. Ven. Internal Posterior
Pylorus Preserving Pancreaticoduodenectomy
 REVIEW Pylorus Preserving Pancreaticoduodenectomy Jacqueline M. Garonzik-Wang, M. B. Majella Doyle Pancreaticoduodenectomy (PD) has become the standard of care for resectable pancreatic cancer and premalignant
REVIEW Pylorus Preserving Pancreaticoduodenectomy Jacqueline M. Garonzik-Wang, M. B. Majella Doyle Pancreaticoduodenectomy (PD) has become the standard of care for resectable pancreatic cancer and premalignant
-12. -Renad Habahbeh. -Dr Mohammad mohtasib
 -12 -Renad Habahbeh - -Dr Mohammad mohtasib The Gallbladder -The gallbladder has a body, a fundus (a rounded end), a neck, Hartmann s pouch before the neck and a cystic duct that meets the common hepatic
-12 -Renad Habahbeh - -Dr Mohammad mohtasib The Gallbladder -The gallbladder has a body, a fundus (a rounded end), a neck, Hartmann s pouch before the neck and a cystic duct that meets the common hepatic
4/9/2018 OBJECTIVES PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS
 PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer?
 Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer? Lee H, Park JY, Youn S, Kwon W, Heo JS, Choi SH, Choi DW Department of Surgery, Samsung Medical Center Sungkyunkwan
Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer? Lee H, Park JY, Youn S, Kwon W, Heo JS, Choi SH, Choi DW Department of Surgery, Samsung Medical Center Sungkyunkwan
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
Neoplasia literally means "new growth.
 NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Image guided core biopsies:
 Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Evaluation of Breast Specimens Removed by Needle Localization Technique
 Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Neoadjuvant radiotherapy for pancreatic cancer: rationale and outcomes
 Review Article Neoadjuvant radiotherapy for pancreatic cancer: rationale and outcomes Rohan Deraniyagala, Emily D. Tanzler The University of Florida College of Medicine Department of Radiation Oncology,
Review Article Neoadjuvant radiotherapy for pancreatic cancer: rationale and outcomes Rohan Deraniyagala, Emily D. Tanzler The University of Florida College of Medicine Department of Radiation Oncology,
What to expect with major vascular reconstruction during Whipple procedures: a single institution experience and literature review
 Original Article What to expect with major vascular reconstruction during Whipple procedures: a single institution experience and literature review Matthew S. Jorgensen 1, Tariq Almerey 2, Houssam Farres
Original Article What to expect with major vascular reconstruction during Whipple procedures: a single institution experience and literature review Matthew S. Jorgensen 1, Tariq Almerey 2, Houssam Farres
6/5/2010. Renal vein invasion & Capsule Penetration (T3a) Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).
 Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).") GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review
 Review Article Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review Min-Jie Yang, Su Li, Yong-Guang Liu, Na Jiao, Jing-Shan Gong Department of Radiology, Shenzhen
Review Article Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review Min-Jie Yang, Su Li, Yong-Guang Liu, Na Jiao, Jing-Shan Gong Department of Radiology, Shenzhen
Prostate cancer staging and datasets: The Nitty-Gritty. What determines our pathological reports? 06/07/2018. Dan Berney Maastricht 2018
 Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Anatomy of the SMALL INTESTINE. Dr. Noman Ullah Wazir PMC
 Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the