The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas. W Glenn McCluggage Belfast, Northern Ireland
|
|
|
- Jayson Robinson
- 6 years ago
- Views:
Transcription
1 The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas W Glenn McCluggage Belfast, Northern Ireland

2 Enterprise Interest None
3 OVARIAN SEROUS CARCINOMA (OSC) RECENT DEVELOPMENTS two distinct tumour types (called low grade and high grade OSC) (WHO 2014) not two grades of same neoplasm different neoplasms with different underlying pathogenesis, molecular events, behaviour, prognosis high grade much more common than low grade (approx 18-19:1) use instead of traditional grading schemes
4 PATHOGENESIS (LOW GRADE SEROUS) low grade arise from pre-existing benign and borderline tumour (probably not all cases) micropapillary variant of serous borderline may be intermediate stage in development of low grade serous carcinoma well-defined adenoma-carcinoma sequence
5 PATHOGENESIS (HIGH GRADE SEROUS) traditionally thought to arise directly from ovarian surface epithelium or epithelium of cortical inclusion cysts; now clear that most cases arise from epithelium of distal fallopian tube precursor lesion is serous tubal intraepithelial carcinoma (STIC) doesn t arise from borderline tumour
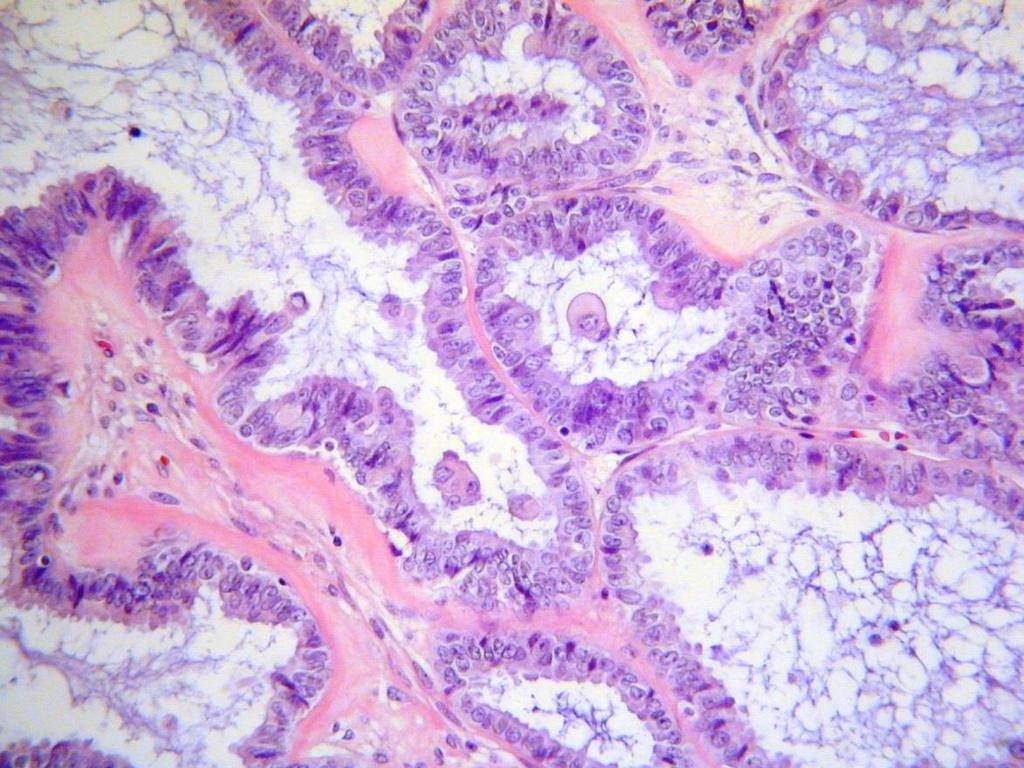
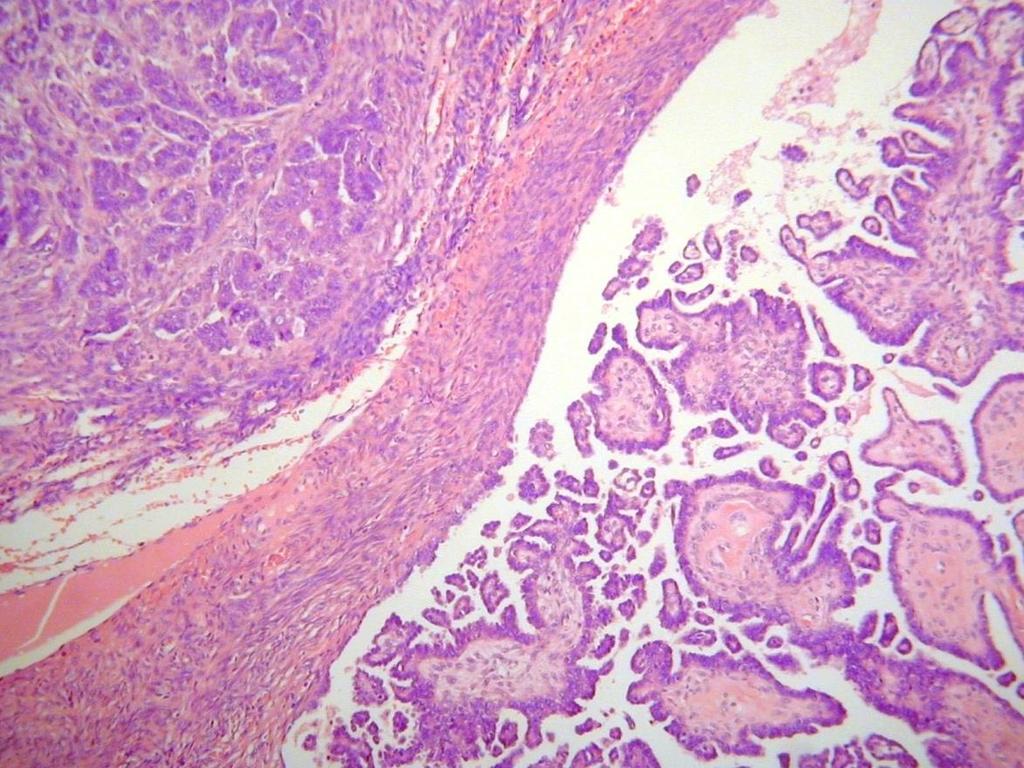
6 MORPHOLOGY classification as high grade or low grade serous is reproducible (MD Anderson system) distinction based mainly on nuclear atypia (not on architecture) in worst area of tumour BUT low grade serous uniform nuclei with mild atypia; < 12 mitoses per 10 HPFs; usually approximately 2/10 HPFs; no necrosis or multinucleation high grade serous moderate to marked atypia; >12 mitoses per 10 HPFs; often necrosis and multinucleate cells
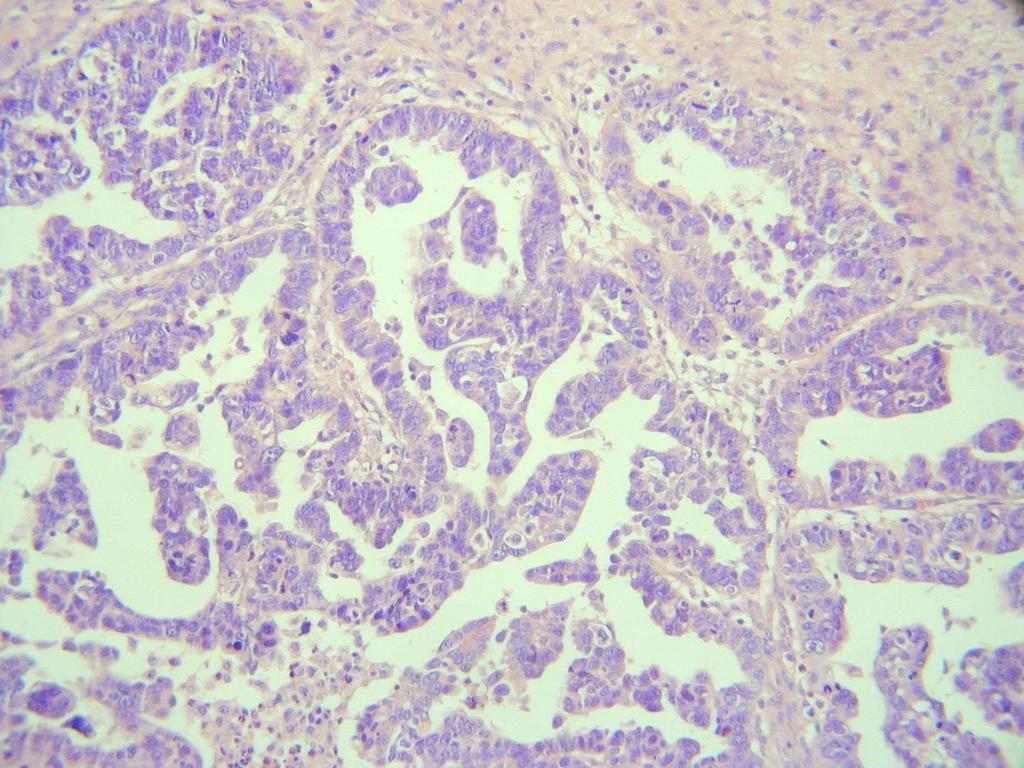
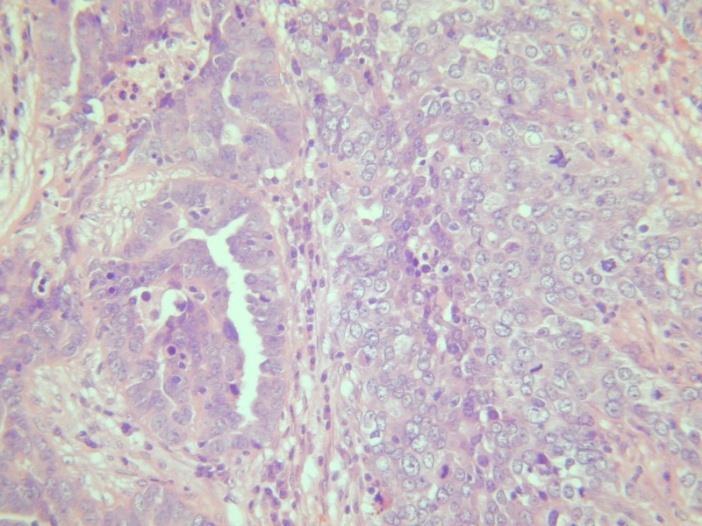
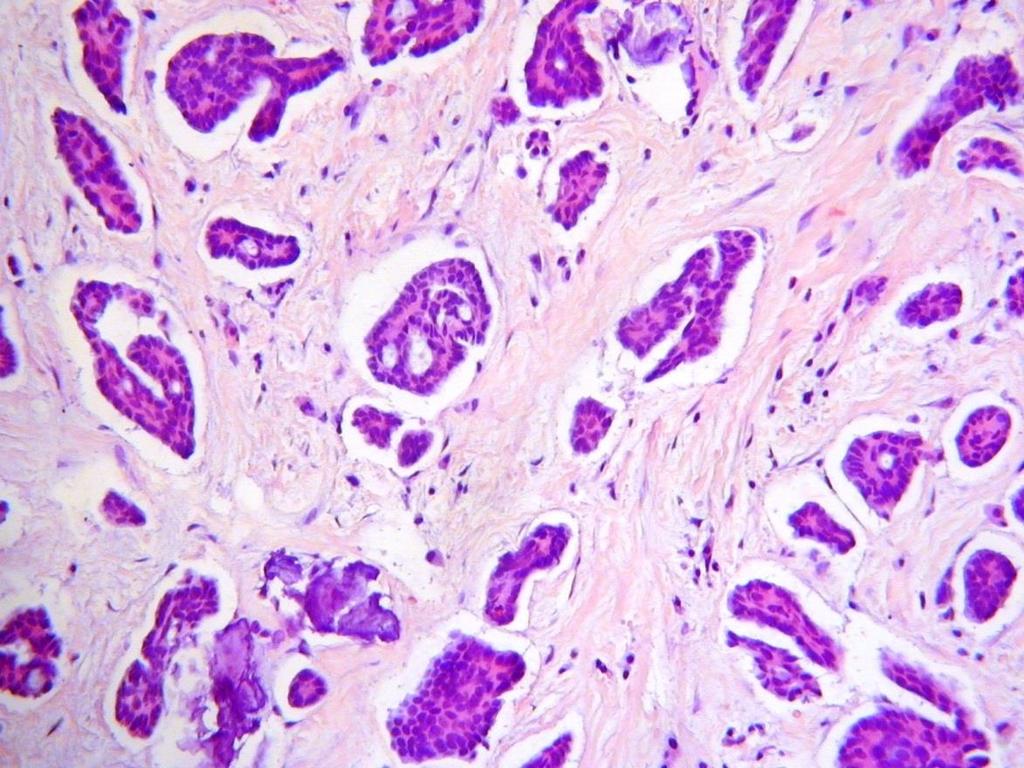
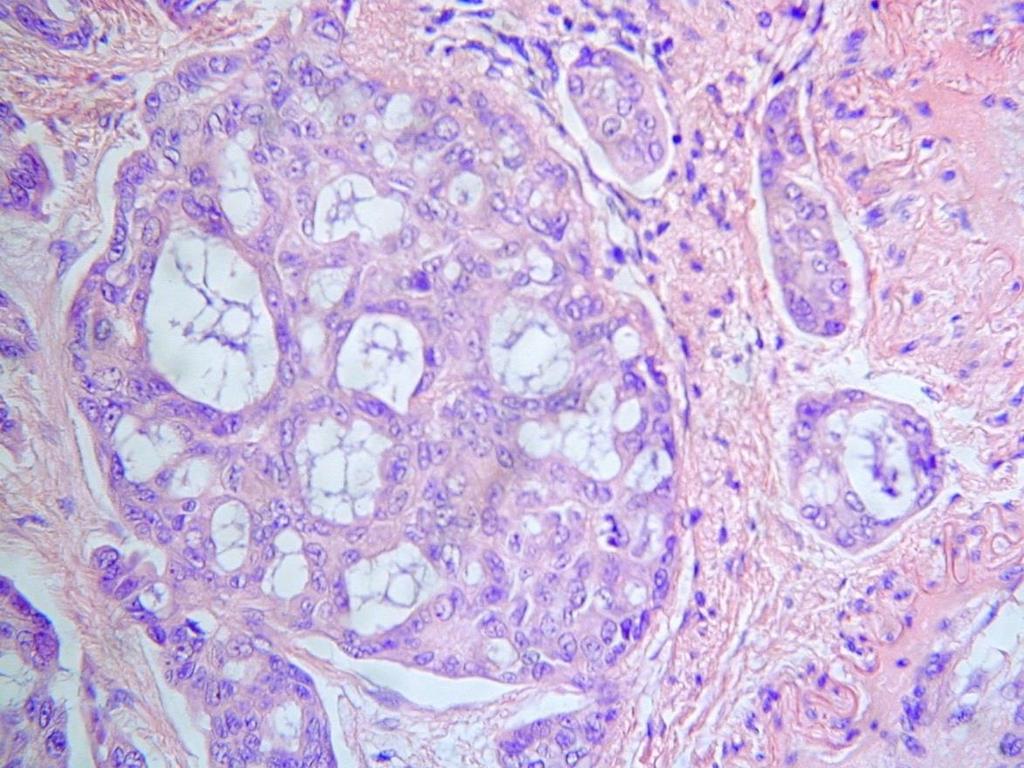
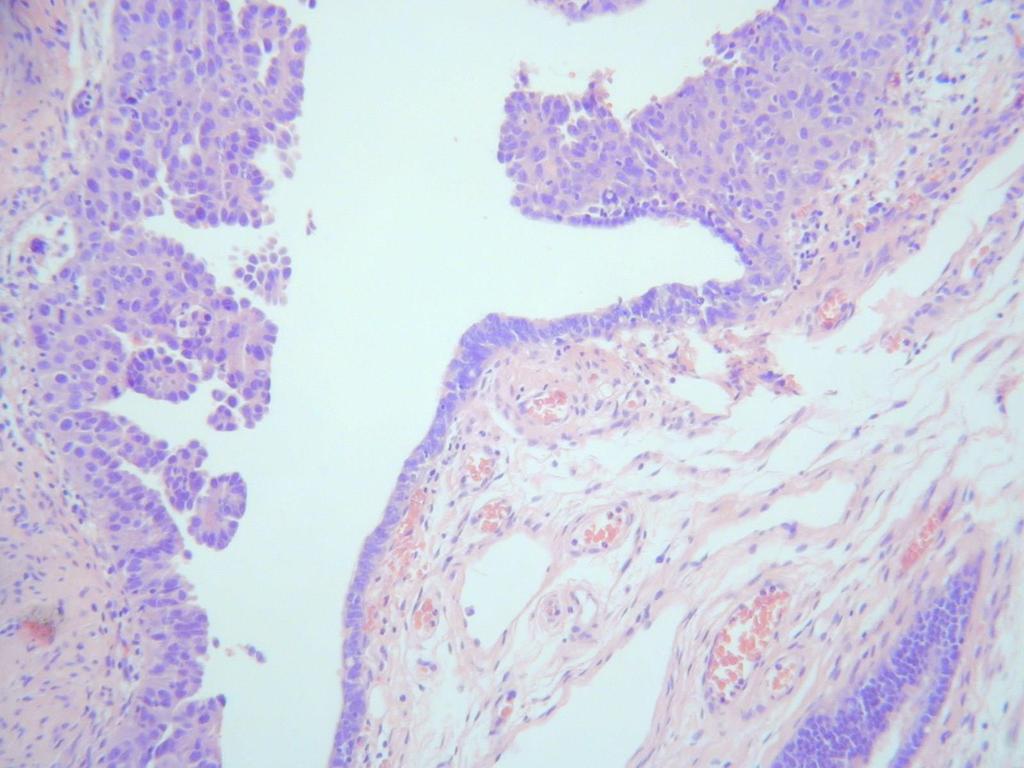
7 HIGH GRADE SEROUS CARCINOMA- MORPHOLOGIC DIVERSITY Papillary/ micropapillary Slit-like Glandular Microglandular/ microcystic Cystic Solid Multinucleate cells Signet ring cells Blue appearance Oncocytic/ clear cell OFTEN ADMIXTURE OF PATTERNS
8

9
10 PSEUDOENDOMETRIOID


11 CLEAR CELL CHANGE IN SEROUS CARCINOMA (SOMETIMES POSTCHEMOTHERAPY)
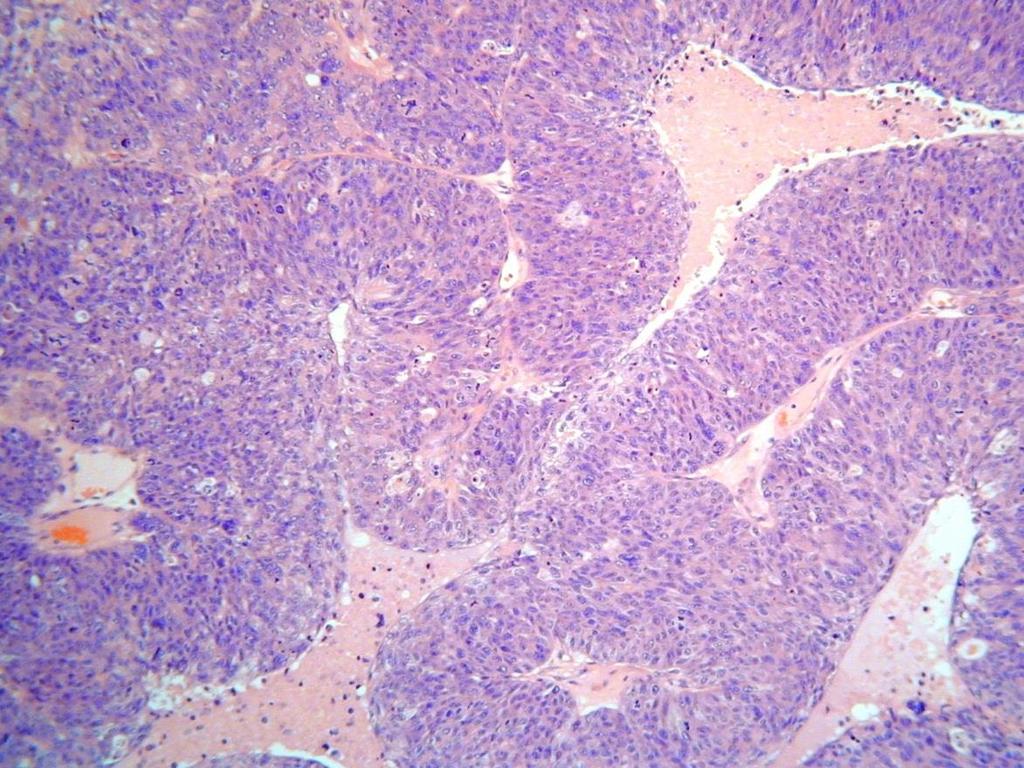
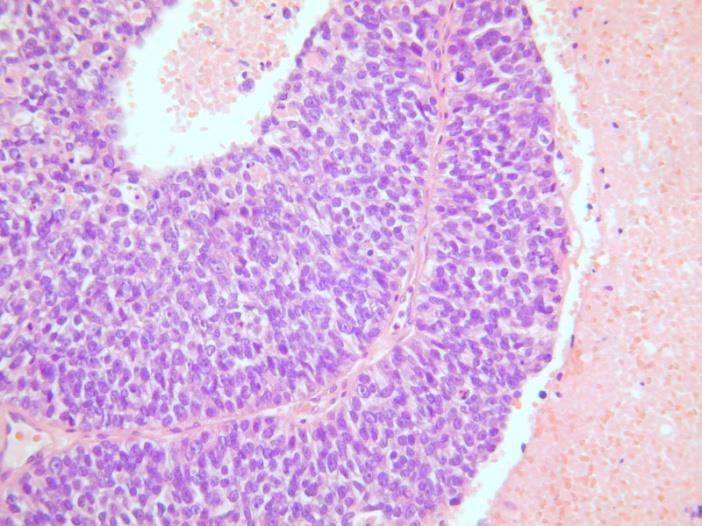
12 TRANSITIONAL- LIKE
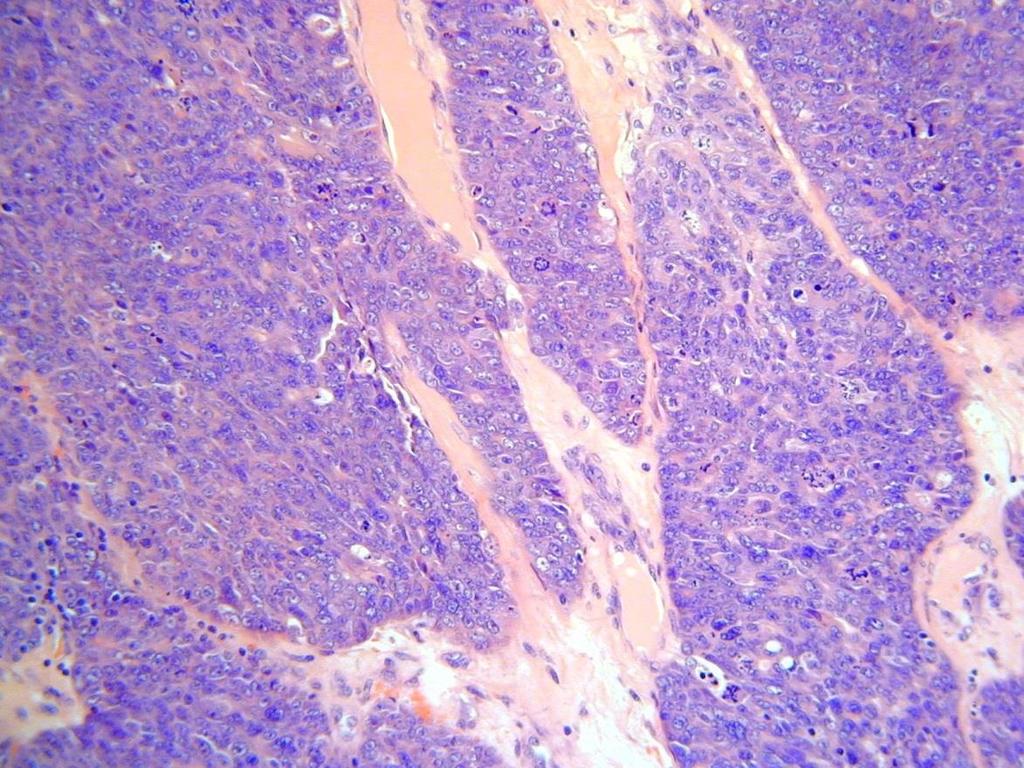
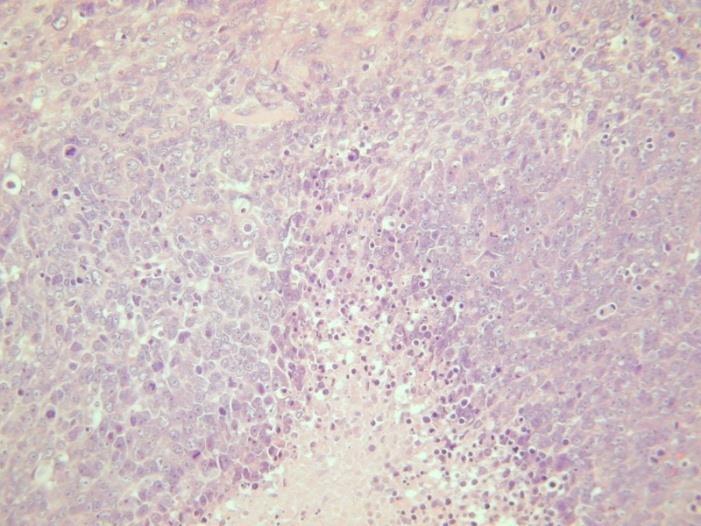
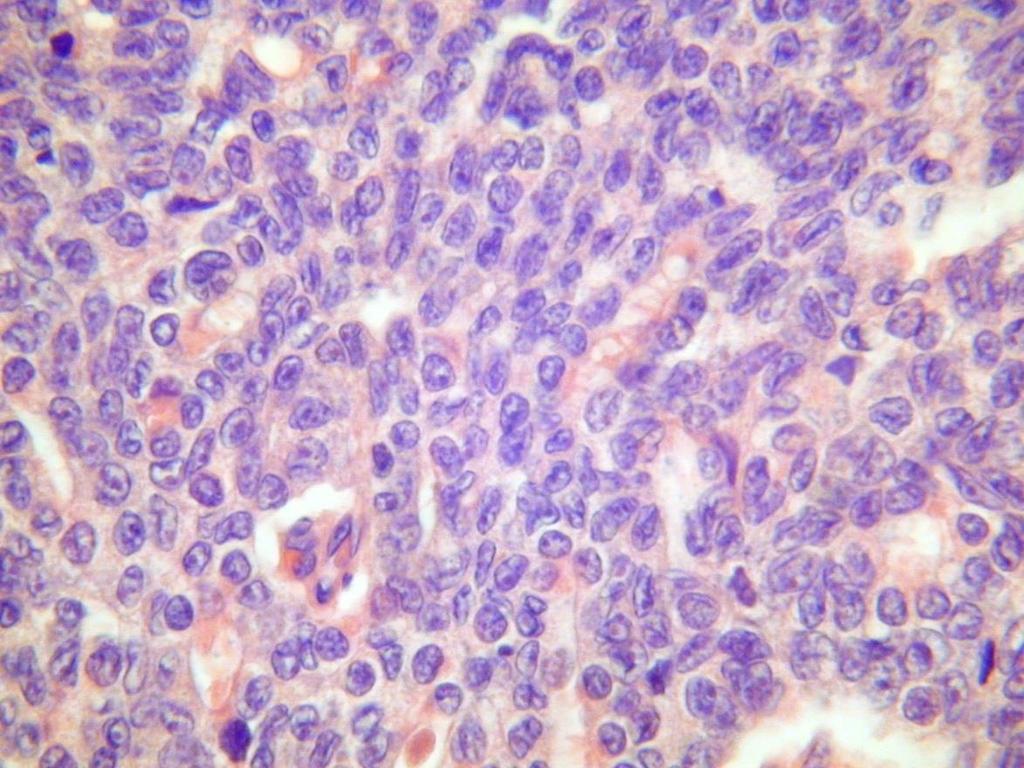
13 SOLID- UNDIFFERENTIATED AREAS



14 OVARIAN HIGH GRADE SEROUS CARCINOMA

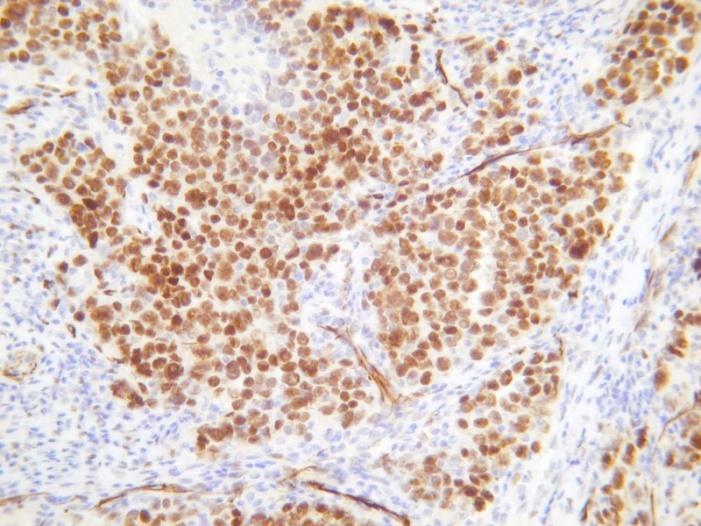
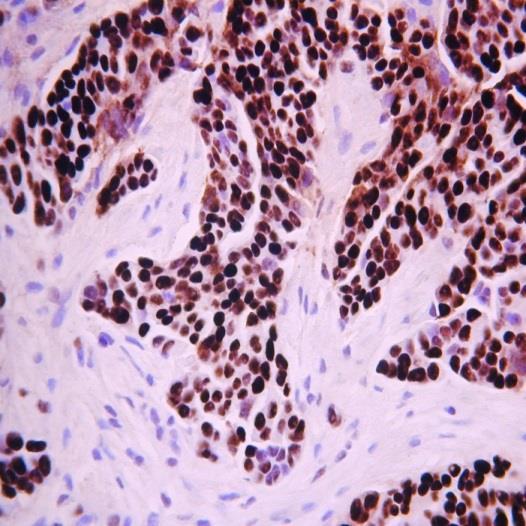
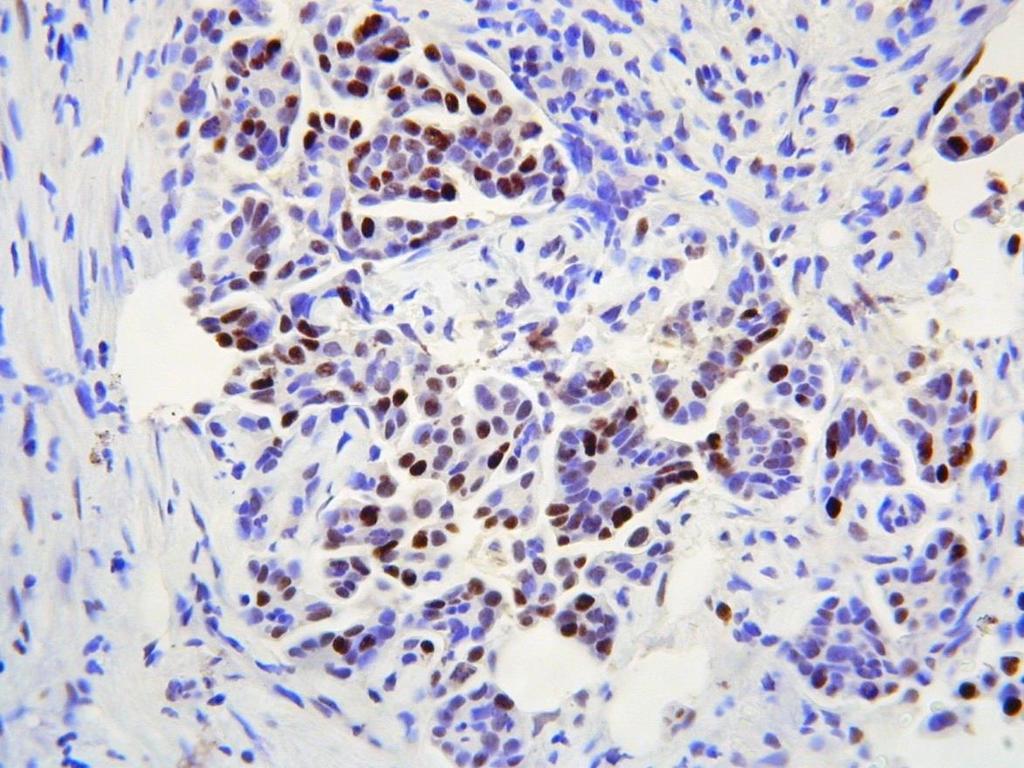
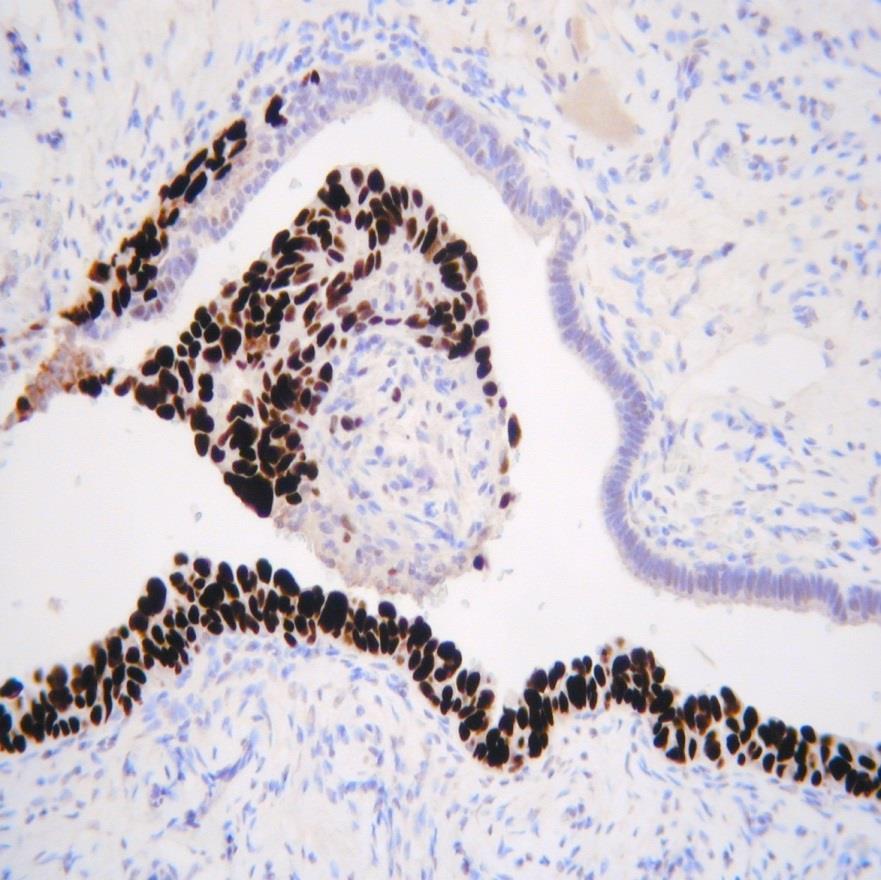
15 WT1 in PSEUDOENDOMETRIOID AREAS IN HIGH GRADE SEROUS CARCINOMA

16 WT1 in CLEAR CELL AREAS IN HIGH GRADE SEROUS CARCINOMA p53 WT1
17 WT1 IN TRANSITIONAL-LIKE AREAS IN HIGH GRADE SEROUS CARCINOMA
18 UNDIFFERENTIATED OVARIAN CARCINOMA WT1
19 MORPHOLOGY OF BRCA ASSOCIATED HIGH GRADE SEROUS CARCINOMAS SET pattern (Solid, pseudoendometrioid, Transitional) Higher mitoses; more geographical necrosis? Increased tumour intraepithelial T lymphocytes Different patterns of metastatic disease ( pushing rather than infiltrative ) Similarities to breast carcinomas in BRCA ALL PATIENTS WITH HGSC SHOULD UNDERGO GERMLINE BRCA TESTING- FUNDING QUESTIONS
20 MIXED OVARIAN CARCINOMAS historically quite common (up to 10-20%) most commonly historically reported were mixed serous/ endometrioid; mixed serous/clear cell; mixed serous/undifferentiated; mixed serous/transitional (mostly variants of high grade serous carcinoma- doubtful if these combinations exist) occasionally get mixed endometrioid/ clear cell (association with endometriosis) occasionally others CATEGORY OF MIXED CARCINOMA DROPPED FROM WHO 2014 CATEGORY OF TRANSITIONAL CARCINOMA ALSO DROPPED FROM WHO 2014
21 Mixed Ovarian Carcinomas Improved recognition of types has virtually abolished mixed tumours 15 of 871 cases reviewed (1.7%) by H/E using modern diagnostic criteria 22 cases thought to be mixed were investigated further by immunohistochemistry and molecular testing Only 13 true mixed carcinomas when immunohistochemistry and molecular data incorporated Mixed carcinomas account for less than 1% of ovarian carcinomas Mackenzie et al. Am J Surg Pathol 2015; 39:
22 MARKERS IN HGSC WT1- good marker of serous carcinomas (extrauterine)- low grade and high grade (occasional low grade endometrioid adenocarcinomas positive) (approximately 5% HGSCs negative) p16- about two thirds of HGSCs block - type positivity (other morphological types patchy) p53 (about 95% mutation-type ) ER (positive 70-80%) PAX8, CA125, CK7 positive HMGA2, IMP3 often positive
23 p53 p53 immunohistochemistry- lot of confusion only consider positive/significant if diffuse strong nuclear immunoreactivity (75-80% cells suggested- associated with missence mutation) p53 null consistent with serous carcinoma (different type of mutation (nonsense) or deletion resulting in truncated protein which is not detected by immunohistochemistry) third pattern of mutation-type staining- cytoplasmic (rare pattern) most normal tissues and tumours exhibit focal, weak, heterogenous staining ( wild-type staining) (usually <50%) (about 5% of HGSCs with Tp53 mutation exhibit wild-type staining) DON T REPORT AS POSITIVE OR NEGATIVE- REPORT AS WILD- TYPE / NORMAL or MUTATION-TYPE /ABERRANT OCCASIONALLY DIFFICULT TO INTERPRET ( wild-type at upper end; negative mutation-type versus wild-type )




24 Interpretation of p53 immunohistochemistry No TP53 mutation Normal Wild type pattern Nonsynonymous =missense Stopgain Indel Splicing Stopgain Indel Splicing p53 overexpression p53 complete absence p53 cytoplasmic abnormal; mutation-type J Pathol Clin Res 2016;2:247
25 2016:
26 p16 IN OVARIAN/ TUBAL (and uterine) HIGH GRADE SEROUS CARCINOMA Diffusely positive in most cases (Modern Pathology 2014; 27; ) Low grade serous, endometrioid, clear cell, mucinousfocally positive Approximately 2/3 homogeneous; 1/3 heterogeneous TMA- 115 HGSC (49 heterogenous; 63 homogenous) In stage I- III cases, homogeneous p16 worse prognosis (OS- significantly better with heterogenous stainingp=0.0367) (Histopathology 2016;68; )
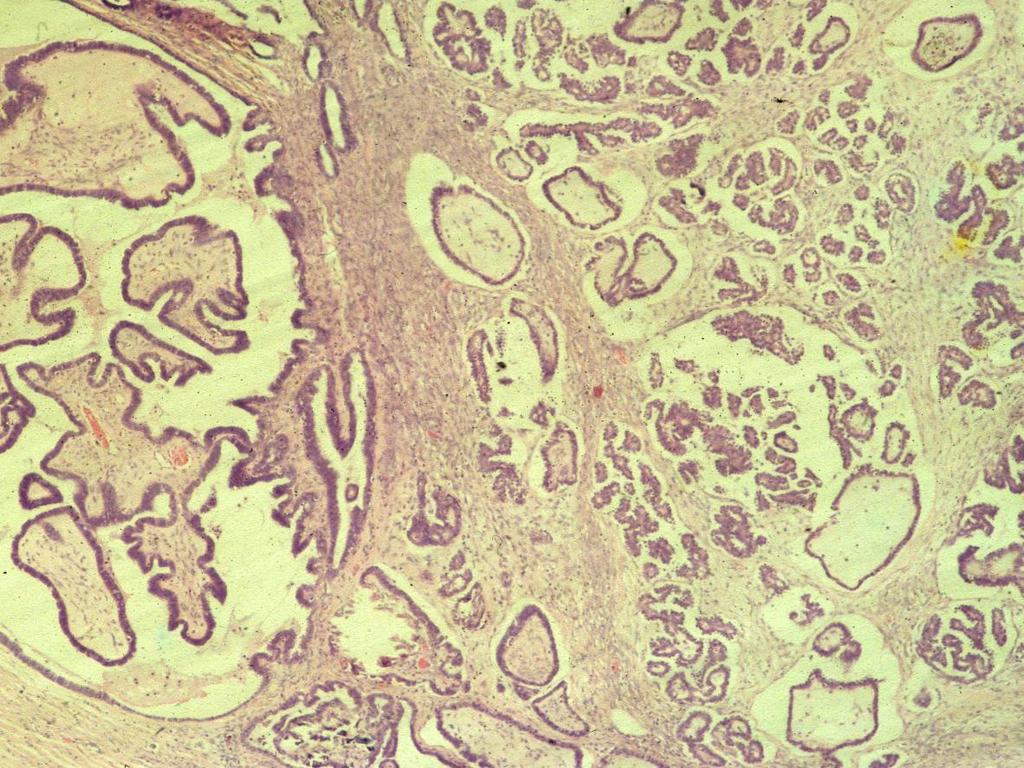
27 LOW GRADE SEROUS CARCINOMA Management may differ significantly from HGSC Surgery much more likely No chemotherapy for early stage No chemotherapy for advanced stage in some places (if totally debulked) Targetted therapies Specific trials Invasive implants in association with ovarian serous borderline tumour (extraovarian low grade serous carcinoma) (sometimes looks invasive in nodes in association with serous borderline in ovary)
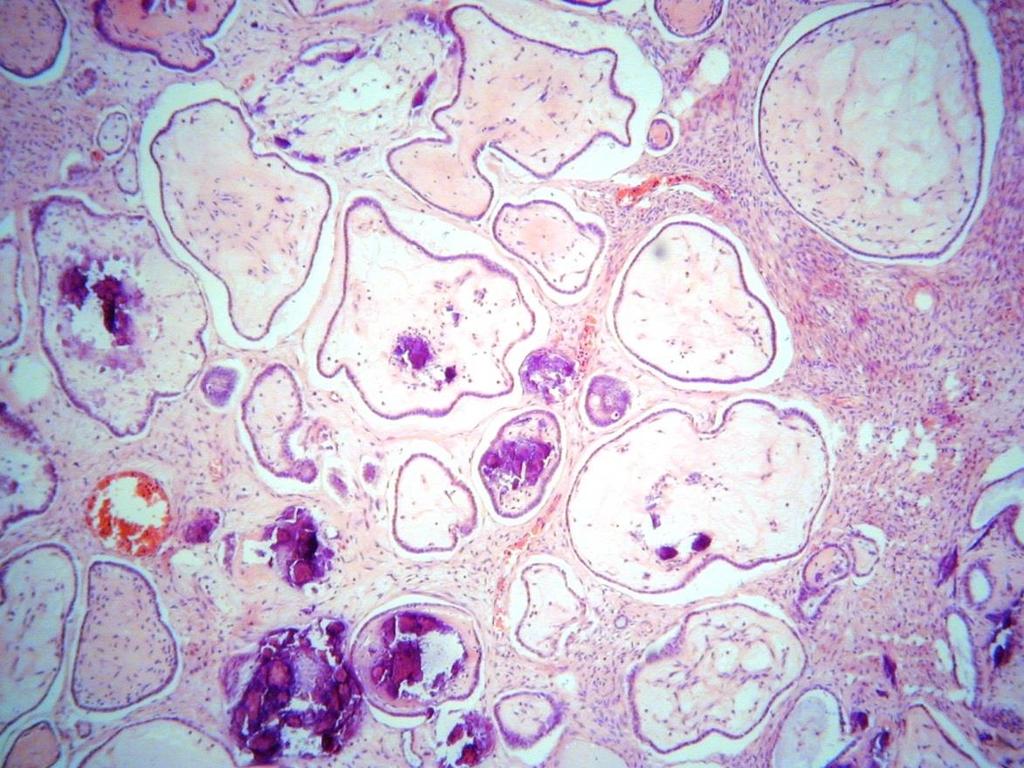
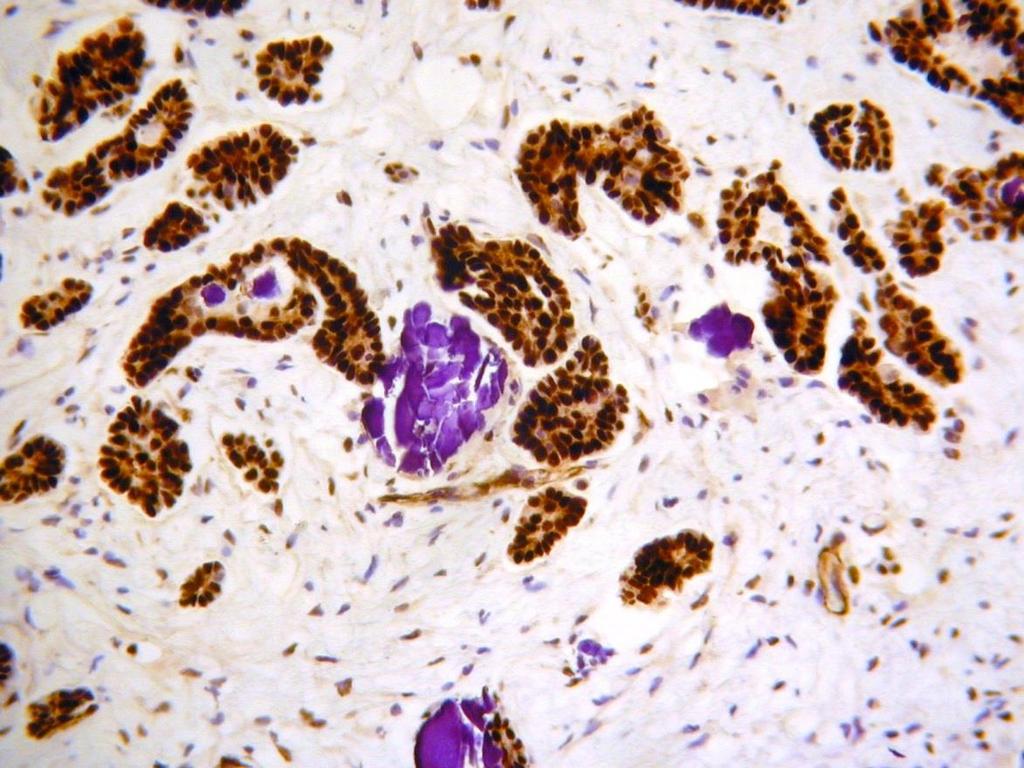
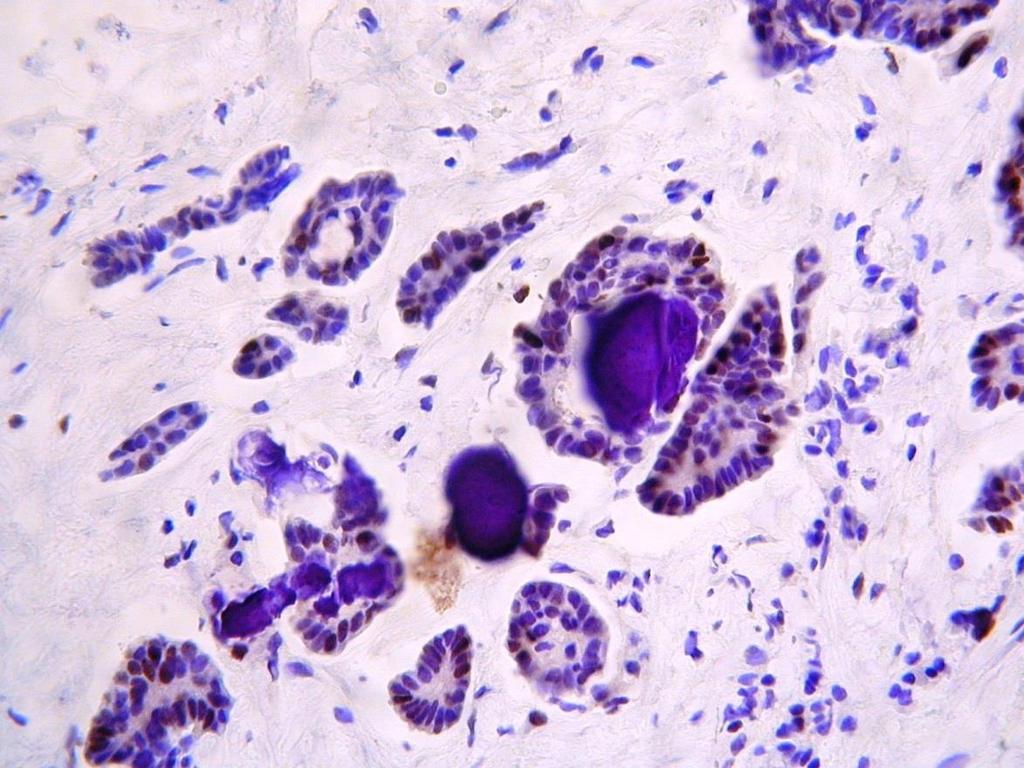
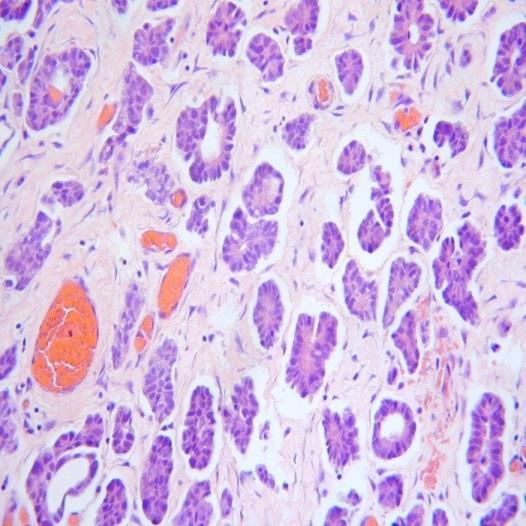
28 LOW GRADE SEROUS- MORPHOLOGIC DIVERSITY Papillary/ micropapillary Glandular Solid Mucinous areas Clefts Often numerous psammoma bodies (psammocarcinoma is a low grade serous carcinoma with abundant psammoma bodies)
29

30
31

32 Psammocarcinoma- LGSC with many psammoma bodies
33
34
35
36
37 MARKERS IN LGSC WT1- good marker of serous carcinomas (extrauterine)- low grade and high grade (occasional low grade endometrioid adenocarcinomas positive) (approximately 5% HGSCs negative) p16- patchy positivity p53 ( wild-type )- ALWAYS ER (positive >90%); PR (usually, but not always, positive) PAX8, CA125, CK7 positive
38 WT1
39 p53
40 CLINICAL BEHAVIOUR- LGSC and HGSC LGSC (mean 52) younger than HGSC (mean 62) HGSC poor prognosis (usually presents at advanced stage, responds well initially to chemo but usually recurs; occasional long term survivors) LGSC more indolent (good prognosis for early stage; advanced stage- patients usually die of tumour) (IJGP 2013; 32; stage 2-4, <30% survival at 10 years; not significantly different to HGSC); (AJSP 2016;40; ; 5 year survival 62.3% LGSC, 43.9% HGSC but no survival difference at 10 years)
41 DISTINCTION BETWEEN LOW GRADE AND HIGH GRADE SEROUS CARCINOMA Usually straightforward Occasionally difficult (especially in small biopsies) Rarely get admixtures (transformation low grade into high grade) Only reliable marker is p53
42 p53 high grade serous carcinomas 95% mutationtype staining low grade serous exhibit wild-type staining


43 HIGH GRADE SEROUS MIMICKING LOW GRADE p53

44 LOW GRADE OSC WITH BIGGER NUCLEI

45 LOW GRADE OSC
46 p53
47 TRANSFORMATION LOW GRADE INTO HIGH GRADE rare (AJSP 2012; 36; ) (serous borderline or low grade serous carcinoma) can be misdiagnosed (bigger nuclei in low grade serous) can transform to HGSC, anaplastic carcinoma, carcinosarcoma p53 NOT reliable in such cases (may not be TP53 mutated)
48
49 TRADITIONAL VIEW OF PATHOGENESIS OF HIGH GRADE SEROUS CARCINOMA traditionally thought to arise directly from ovarian surface epithelium (OSE) or epithelium of cortical inclusion cysts thought that some cases might arise from secondary Mullerian system doesn t arise from borderline tumour
50 IS TUBAL FIMBRIA THE ORIGIN OF EXTRAUTERINE HIGH GRADE SEROUS CARCINOMA? proposal that tubal fimbria (distal tube) (secretory cells) is site of origin of many/most extrauterine high grade serous carcinomas (ovary, peritoneum and fallopian tube)
51 INITIAL EVIDENCE came from prophylactic risk reducing salpingooophorectomy specimens (RRSO) (BRCA1/2) once tubes were examined in their entirety, tubal lesions (distal) were seen with little/ nothing in ovary tubal lesions may be STIC (serous tubal intraepithelial carcinoma) or small HGSCs now well established in BRCA patients that tube is origin of HGSCs? does same hold true for sporadic HGSCs

52
53

54 p53 in STIC
55 WHAT ABOUT SPORADIC HGSCs Usually present at advanced stage Tube (s) often obliterated and embedded in tubo-ovarian mass Difficult to study precursor lesions STIC/ mucosal HGSC found in carefully sectioned tubes (when both visible) in significant percentage of cases (up to twothirds) of sporadic HGSC

56 Implications for specimen handling SEE-FIM protocol ESSENTIAL for identifying STIC/early tubal involvement- now routinely done in tubo-ovarian HGSC
57 ? FIELD-EFFECT IN HGSC same TP53 mutations in HGSC at multiple sites evidence that clonally related and not part of field-effect no evidence of field-effect in HGSC one site is primary with metastasis to the others other molecular evidence- common clonal ancestry at multiple sites
58 BUT IS TUBAL LESION PRIMARY OR METASTATIC? Intramucosal metastasis from a variety of sites may occur in tubes and mimic an in-situ lesion Gynaecological or non-gynaecological tumours when spread to tube exhibit mucosal involvement and even mimic STIC (AJSP 2015;39;35-51) Some molecular evidence that tube is initial site but difficult to prove by molecular techniques RECENT OBSERVATIONAL STUDIES PROVIDE FIRM EVIDENCE


59 USC INVOLVING FALLOPIAN TUBE WT1

60 HPV RELATED CERVICAL ADENOCA INVOLVING TUBE
61 INCIDENTAL SPORADIC HIGH GRADE SEROUS CARCINOMA established that incidental tumours in patients with BRCA1/2 mutation are of tubal origin 3 papers recently published- unsuspected STIC/ HGSC incidentally detected (ours= AJSP 2015; 39; ) PROVES that sporadic HGSC of tubal origin (FINAL PIECE OF EVIDENCE)
62 Summary of findings of incidental HGSC in a non-prophylactic setting Study Total Cases Invasive Invasive Organ- Organ- Organ- cases with HGSC HGSC in confined confined: confined: STIC in tube ovary Disease tube ovary (tube OR ovary) Rabban, Morrison, Gilks, Total
63 EXTRAUTERINE HIGH GRADE SEROUS CARCINOMA- SITE OF ORIGIN FIGO same staging system (ovary, tube, peritoneum, undesignated) FIGO 2014 and WHO no recommendations regarding designating site of origin WHO- the decision as to primary site should be pragmatic, based on experience and professional judgement DOMINANT MASS THEORY TRADITIONALLY USED (ovary designated as primary site in most cases) possibilities- pelvic high grade serous; extrauterine; Mullerian; tubo-ovarian; undesignated implications:- epidemiology, tumour incidence/mortality, cancer registries, entry into clinical trials different viewpoints- STIC/ in situ criteria; dominant mass criteria
64 Ovarian? Peritoneal? Tubal? Undesignated?. CHAOS!
65 SURVEY: INTERNATIONAL JOURNAL OF GYNECOLOGICAL PATHOLOGY PMID respondents Widespread acceptance of tubal origin (86% pathologists, 92% clinicians) Clinicians thought it more important to correctly assign a primary site than pathologists (71% versus 49%)
66 PROPOSAL FOR DESIGNATING SITE OF ORIGIN OF HGSC extensive examination of tube (SEE-FIM) any STIC or mucosal serous ca in tube- tubal origin if fallopian tube or fimbria not identified (obliterated by mass)- tubal origin ovarian primary if tumour in ovary and nothing in mucosa of tube (STIC or invasive) (both tubes need to be clearly visible and examined by SEE-FIM protocol) primary peritoneal- nothing in tube or ovary (vanishingly rare- will likely disappear) (WHO 2014) post-chemo (if no residual) or on small biopsy- designate as tubo-ovarian USING THESE CRITERIA- approximately 80% tubal primaries undesignated- very small proportion (Histopathology 2014; 65; ; Gynecological Oncology 2016;141; ; International Journal of Gynecological Pathology 2016;35; ) CRITERIA ADOPTED BY ICCR site assignment is reproducible using these criteria
67 Summary of site assignment guidelines proposals Criteria Primary site Comment STIC present Fallopian tube Regardless of presence and size of ovarian and peritoneal disease Invasive mucosal carcinoma in tube, with or without STIC Distal end or entire tube incorporated into ovarian mass No STIC or invasive mucosal carcinoma in either tube in presence of ovarian mass Both tubes and both ovaries grossly and microscopically normal or involved by benign process in presence of peritoneal HGSC Fallopian tube Fallopian tube Ovary Primary peritoneal HGSC Regardless of presence and size of ovarian and peritoneal disease Regardless of presence and size of ovarian and peritoneal disease Regardless of presence and size of peritoneal disease As recommended in WHO blue book
68 RETROSPECTIVE (n=151) PROSPECTIVE (n=111) Primary site T O P U T O P U Chemo naive (79%) (20%) (0%) (1%) (83%) (17%) (0%) (0%) Post NACT (68%) (22%) (10%) (0%) (76%) (12%) (7%) (5%) Singh et al, 2015
69 Basis for tubal assignment in 44 chemonaive cases Criterion Number (%) STIC only 5 (11%) Invasive mucosal +/- STIC 26 (59%) Entire tube or part of tube incorporated in mass 13 (30%) Total 44
70 Unilateral vs bilateral tubal and ovarian involvement in HGSC Unilateral Bilateral Total Ovary 18 (38%) 29 (62%) 47 Fallopian tube 37 (84%) 7 (16%) 44 Bilaterality = strong indicator of secondary spread In 53 chemo-naïve cases, ovarian involvement in HGSC was significantly more frequently bilateral Tubal involvement unilateral in 84% supporting primary rather than metastatic involvement Singh et al, 2015
71 CONCLUSIONS Majority of extrauterine HGSC, hereditary and sporadic, arise in the fallopian tube, mostly its fimbrial end Multiple sites of HGSC arise from a single ancestral clone Molecular evidence does not support the concept of multifocal origin Primary peritoneal HGSC can only be diagnosed if both tubes and both ovaries show no STIC/HGSC Following a defined protocol results in reproducible site assignment Thus assigned, sporadic HGSC shows a similar site distribution to hereditary cases Witnessing a major paradigm shift
Section 1. Biology of gynaecological cancers: our current understanding
 Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
of 20 to 80 and subsequently declines [2].
![of 20 to 80 and subsequently declines [2].](/thumbs/80/81450506.jpg "of 20 to 80 and subsequently declines [2].") - - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
- - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
Current Concept in Ovarian Carcinoma: Pathology Perspectives
 Current Concept in Ovarian Carcinoma: Pathology Perspectives Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine Current Concept in Ovarian
Current Concept in Ovarian Carcinoma: Pathology Perspectives Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine Current Concept in Ovarian
Interpretation of p53 Immunostains. P53 Mutations are Ubiquitous in High Grade Serous Carcinoma. Diffuse strong positive nuclear staining
 Stains for Tumor Classification p53 p16 WT1 HMGA2 P53 Mutations are Ubiquitous in High Grade Serous Carcinoma Source Ahmed et al Australian Ovarian Cancer Study Cancer Genome Atlas Research Network Cases
Stains for Tumor Classification p53 p16 WT1 HMGA2 P53 Mutations are Ubiquitous in High Grade Serous Carcinoma Source Ahmed et al Australian Ovarian Cancer Study Cancer Genome Atlas Research Network Cases
Case 1. Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno
 Luca Mazzucchelli Istituto cantonale di patologia Locarno") Case 1 Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno SAMO Interdisciplinary Workshop on Gynecological Tumors Lucern, October
Case 1 Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno SAMO Interdisciplinary Workshop on Gynecological Tumors Lucern, October
5/26/2016. Pelvic Serous Carcinoma: 2014 W.H.O. Update. Outline of Talk. Changes to 2014 WHO system for pelvic serous tumors
 Pelvic Serous Carcinoma: 2014 W.H.O. Update Outline of Talk Practical Implications for Pathologists Changes to 2014 WHO system for pelvic serous tumors High grade serous carcinoma versus low grade serous
Pelvic Serous Carcinoma: 2014 W.H.O. Update Outline of Talk Practical Implications for Pathologists Changes to 2014 WHO system for pelvic serous tumors High grade serous carcinoma versus low grade serous
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens
 How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden
 and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden") What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
Ovarian carcinoma classification. Robert A. Soslow, MD
 Ovarian carcinoma classification Robert A. Soslow, MD soslowr@mskcc.org WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction Rationale
Ovarian carcinoma classification Robert A. Soslow, MD soslowr@mskcc.org WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction Rationale
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
ACCME/Disclosures. Risk of Gyne Ca in HBOC. Molecular basis of HBOC. Hereditary Ovarian and Breast Cancer Syndrome
 Hereditary Ovarian and Breast Cancer Syndrome C. Blake Gilks, MD Dept of Pathology Vancouver General Hospital University of British Columbia Blake.gilks@vch.ca The USCAP requires that anyone in a position
Hereditary Ovarian and Breast Cancer Syndrome C. Blake Gilks, MD Dept of Pathology Vancouver General Hospital University of British Columbia Blake.gilks@vch.ca The USCAP requires that anyone in a position
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
CASE 4 21/07/2017. Ectopic Prostatic Tissue in Cervix. Female 31. LLETZ for borderline nuclear abnormalities
 Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
Low-grade serous neoplasia. Robert A. Soslow, MD
 Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Epithelial Ovarian Cancer 8/2/2013. Tu-be or Not Tu-be: Is the Fallopian Tube the Source of Ovarian Cancer?
 Tu-be or Not Tu-be: Is the Fallopian Tube the Source of Ovarian Cancer? Ann E. Smith Sehdev, MD Director, Center for Gynecologic Pathology Cascade Pathology, Portland, Oregon Ann E. Smith Sehdev has no
Tu-be or Not Tu-be: Is the Fallopian Tube the Source of Ovarian Cancer? Ann E. Smith Sehdev, MD Director, Center for Gynecologic Pathology Cascade Pathology, Portland, Oregon Ann E. Smith Sehdev has no
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Mousa. Najat kayed &Renad Al-Awamleh. Nizar Alkhlaifat
 6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal cells
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal cells
Ovarian Clear Cell Carcinoma
 Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Atypical Hyperplasia/EIN
 EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
3/24/2017. Disclosure of Relevant Financial Relationships. Mixed Epithelial Endometrial Carcinoma. ISGyP Endometrial Cancer Project
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Ovarian cancer: 2012 Update Srini Prasad MD Univ Texas MD Anderson Cancer Center
 Ovarian cancer: 2012 Update Srini Prasad MD Univ Texas MD Anderson Cancer Center Ovarian cancer is not a single disease Ovarian Epithelial Tumors: Histological Spectrum* Type Frequency Histology High-Grade
Ovarian cancer: 2012 Update Srini Prasad MD Univ Texas MD Anderson Cancer Center Ovarian cancer is not a single disease Ovarian Epithelial Tumors: Histological Spectrum* Type Frequency Histology High-Grade
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Important Recent Advances in Gynaecological Pathology
 Important Recent Advances in Gynaecological Pathology Sanjiv Manek Consultant Gynaecological Pathologist Oxford, UK In recent years there have been a significant number of changes in gynaecological pathology
Important Recent Advances in Gynaecological Pathology Sanjiv Manek Consultant Gynaecological Pathologist Oxford, UK In recent years there have been a significant number of changes in gynaecological pathology
Mucinous Tumors of the Ovary Beirut, Lebanon. Anaís Malpica, M.D. Professor Department of Pathology
 Mucinous Tumors of the Ovary Beirut, Lebanon Anaís Malpica, M.D. Professor Department of Pathology Primary Mucinous Tumors of the Ovary Cystadenoma Borderline (Tumor of Low Malignant Potential/Atypical
Mucinous Tumors of the Ovary Beirut, Lebanon Anaís Malpica, M.D. Professor Department of Pathology Primary Mucinous Tumors of the Ovary Cystadenoma Borderline (Tumor of Low Malignant Potential/Atypical
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Case # 4 Low-Grade Serous Carcinoma (Macropapillary) of the Ovary Arising in an Atypical Proliferative Serous Tumor
 of the Ovary Arising in an Atypical Proliferative Serous Tumor") Case # 4 Low-Grade Serous Carcinoma (Macropapillary) of the Ovary Arising in an Atypical Proliferative Serous Tumor Robert J Kurman, M.D. Johns Hopkins University School of Medicine Case History A 53 year
Case # 4 Low-Grade Serous Carcinoma (Macropapillary) of the Ovary Arising in an Atypical Proliferative Serous Tumor Robert J Kurman, M.D. Johns Hopkins University School of Medicine Case History A 53 year
Adenocarcinoma of Mullerian origin: review of pathogenesis, molecular biology, and emerging treatment paradigms
 Cobb et al. Gynecologic Oncology Research and Practice (2015) 2:1 DOI 10.1186/s40661-015-0008-z REVIEW Adenocarcinoma of Mullerian origin: review of pathogenesis, molecular biology, and emerging treatment
Cobb et al. Gynecologic Oncology Research and Practice (2015) 2:1 DOI 10.1186/s40661-015-0008-z REVIEW Adenocarcinoma of Mullerian origin: review of pathogenesis, molecular biology, and emerging treatment
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 3 - GYN. History: 66 year old, routine Pap test. Dr. Stelow
 Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Modern Pathology (2015) 28,
 28,") 2015 USCAP, Inc All rights reserved 0893-3952/15 $32.00 1101 Data set for reporting of ovary, fallopian tube and primary peritoneal carcinoma: recommendations from the International Collaboration on Cancer
2015 USCAP, Inc All rights reserved 0893-3952/15 $32.00 1101 Data set for reporting of ovary, fallopian tube and primary peritoneal carcinoma: recommendations from the International Collaboration on Cancer
Endosalpingiosis. Case report
 Case report Endosalpingiosis Michael D. Holmes, M.D. Howard S. Levin M.D. Department of Pathology Lester A. Ballard, Jr., M.D. Department of Gynecology Endosalpingiosis, a term referring to tuballike epithelium
Case report Endosalpingiosis Michael D. Holmes, M.D. Howard S. Levin M.D. Department of Pathology Lester A. Ballard, Jr., M.D. Department of Gynecology Endosalpingiosis, a term referring to tuballike epithelium
Pathology of Ovarian Tumours. Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh
 AFMC Pune PDCC (Cytopathology) PGI Chandigarh") Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Unknown Slides Conference
 Unknown Slides Conference Jae Y. Ro, MD, PhD Weill Medical College of Cornell Univ. The Methodist Hospital, and UT MD Anderson Cancer Center Houston, TX November 9, 2013 Amman, Jordan 25 th Congress of
Unknown Slides Conference Jae Y. Ro, MD, PhD Weill Medical College of Cornell Univ. The Methodist Hospital, and UT MD Anderson Cancer Center Houston, TX November 9, 2013 Amman, Jordan 25 th Congress of
Presenter: Yeh-Han Wang M.D.
 Korea-Taiwan-Japan Joint Meeting for Gynecological Pathology Mini-lecture Female Adnexal Tumor of Probable Wolffian Origin (FATWO) in Taiwan: A Small Case Series and Literature Review Presenter: Yeh-Han
Korea-Taiwan-Japan Joint Meeting for Gynecological Pathology Mini-lecture Female Adnexal Tumor of Probable Wolffian Origin (FATWO) in Taiwan: A Small Case Series and Literature Review Presenter: Yeh-Han
Adenocarcinoma of the Cervix
 Question 1. Each of the following statements about cervical adenocarcinoma is true except: Adenocarcinoma of the Cervix SAMS a) A majority of women with cervical adenocarcinoma have stage I tumors at diagnosis.
Question 1. Each of the following statements about cervical adenocarcinoma is true except: Adenocarcinoma of the Cervix SAMS a) A majority of women with cervical adenocarcinoma have stage I tumors at diagnosis.
The Origin of Pelvic Low-Grade Serous Proliferative Lesions
 The Origin of Pelvic Low-Grade Serous Proliferative Lesions Ovarian Atypical Proliferative (Borderline) Serous Tumors, Noninvasive Implants and Endosalpingiosis Robert J. Kurman, M.D. Kurman RJ, Vang R,
The Origin of Pelvic Low-Grade Serous Proliferative Lesions Ovarian Atypical Proliferative (Borderline) Serous Tumors, Noninvasive Implants and Endosalpingiosis Robert J. Kurman, M.D. Kurman RJ, Vang R,
Carcinoma mammario: le istologie non frequenti. Valentina Guarneri Università di Padova IOV-IRCCS
 Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
ACCME/Disclosures. Diagnosing Mesothelioma in Limited Tissue Samples. Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016
 Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Bases biológicas del cáncer de ovario en el siglo XXI
 Bases biológicas del cáncer de ovario en el siglo XXI Iñigo Espinosa, M.D. Clínica Universidad de Navarra Epithelial Ovarian Tumors WHO 1973-2014 Serous Mucinous Endometrioid Clear cell Transitional Squamous
Bases biológicas del cáncer de ovario en el siglo XXI Iñigo Espinosa, M.D. Clínica Universidad de Navarra Epithelial Ovarian Tumors WHO 1973-2014 Serous Mucinous Endometrioid Clear cell Transitional Squamous
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Dall istologia alla caratterizzazione biomolecolare
 Il carcinoma ovarico: approccio multidisciplinare e prospettive terapeutiche Dall istologia alla caratterizzazione biomolecolare Anna Pesci Ospedale SC Don Calabria, Negrar anna.pesci@sacrocuore.it Ovarian
Il carcinoma ovarico: approccio multidisciplinare e prospettive terapeutiche Dall istologia alla caratterizzazione biomolecolare Anna Pesci Ospedale SC Don Calabria, Negrar anna.pesci@sacrocuore.it Ovarian
Bibliography. Serous Tumors of the Ovary. Nomenclature
 Bibliography Serous Tumors of the Ovary Nomenclature 1. Allison KH, Swisher EM, Kerkering KM, et al. Defining an appropriate threshold for the diagnosis of serous borderline tumor of the ovary: when is
Bibliography Serous Tumors of the Ovary Nomenclature 1. Allison KH, Swisher EM, Kerkering KM, et al. Defining an appropriate threshold for the diagnosis of serous borderline tumor of the ovary: when is
ACCME/Disclosures. Case History 4/13/2016. USCAP GU Specialty Conference Case 3. Ann Arbor, MI
 USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Follicular Derived Thyroid Tumors
 Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Institute of Pathology First Faculty of Medicine Charles University. Ovary
 Ovary Barrett esophagus ph in vagina between 3.8 and 4.5 ph of stomach varies from 1-2 (hydrochloric acid) up to 4-5 BE probably results from upward migration of columnar cells from gastroesophageal junction
Ovary Barrett esophagus ph in vagina between 3.8 and 4.5 ph of stomach varies from 1-2 (hydrochloric acid) up to 4-5 BE probably results from upward migration of columnar cells from gastroesophageal junction
Fast Facts: Ovarian Cancer
 Fast Facts Fast Facts: Ovarian Cancer Christina Fotopoulou MD PhD Consultant Gynaecological Oncologist Queen Charlotte s and Chelsea Hospital London, UK Thomas J Herzog MD Professor of Obstetrics and Gynecology
Fast Facts Fast Facts: Ovarian Cancer Christina Fotopoulou MD PhD Consultant Gynaecological Oncologist Queen Charlotte s and Chelsea Hospital London, UK Thomas J Herzog MD Professor of Obstetrics and Gynecology
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Borderline tumors. Borderline tumors. Serous borderline tumor are NOT benign. Low grade serous carcinoma: pathogenesis. Serous carcinoma: pathogenesis
 Serous borderline tumor are NOT benign Robert A. Soslow, MD Memorial Sloan-Kettering Cancer Center soslowr@mskcc.org Borderline tumors Serous BTs and seromucinous BTs are both histopathologically borderline
Serous borderline tumor are NOT benign Robert A. Soslow, MD Memorial Sloan-Kettering Cancer Center soslowr@mskcc.org Borderline tumors Serous BTs and seromucinous BTs are both histopathologically borderline
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Morphological effects of chemotherapy on ovarian carcinoma
 27 ORIGINAL ARTICLE Morphological effects of chemotherapy on ovarian carcinoma W G McCluggage, R W Lyness, R J Atkinson, S P Dobbs, I Harley, H R McClelland, J H Price... See end of article for authors
27 ORIGINAL ARTICLE Morphological effects of chemotherapy on ovarian carcinoma W G McCluggage, R W Lyness, R J Atkinson, S P Dobbs, I Harley, H R McClelland, J H Price... See end of article for authors
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine
 Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS
 ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
Gestione dei tumori borderline iniziali e avanzati nelle donne in età fertile
 Gestione dei tumori borderline iniziali e avanzati nelle donne in età fertile Pierandrea De Iaco pierandrea.deiaco@aosp.bo.it SSD ONCOLOGIA GINECOLOGICA AOU SANT ORSOLA-MALPIGHI BOLOGNA Borderline ovarian
Gestione dei tumori borderline iniziali e avanzati nelle donne in età fertile Pierandrea De Iaco pierandrea.deiaco@aosp.bo.it SSD ONCOLOGIA GINECOLOGICA AOU SANT ORSOLA-MALPIGHI BOLOGNA Borderline ovarian
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Diagnostically Challenging Cases in Gynecologic Pathology
 Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
MPH Quiz. 1. How many primaries are present based on this pathology report? 2. What rule is this based on?
 MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box?
 When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
Histopathological Study of Spectrum of Lesions Seen in Surgically Resected Specimens of Fallopian Tube
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2016/613 Histopathological Study of Spectrum of Lesions Seen in Surgically Resected Specimens of Fallopian Tube Pratima
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2016/613 Histopathological Study of Spectrum of Lesions Seen in Surgically Resected Specimens of Fallopian Tube Pratima
In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis
 In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis Rouba Ali-Fehmi,MD The Karmanos Cancer Institute, Wayne State University School of Medicine Global incidence of cervical
In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis Rouba Ali-Fehmi,MD The Karmanos Cancer Institute, Wayne State University School of Medicine Global incidence of cervical
Invited Re vie W. Molecular genetics of ovarian carcinomas. Histology and Histo pathology
 Histol Histopathol (1 999) 14: 269-277 http://www.ehu.es/histol-histopathol Histology and Histo pathology Invited Re vie W Molecular genetics of ovarian carcinomas J. Diebold Pathological Institute, Ludwig-Maximilians-University
Histol Histopathol (1 999) 14: 269-277 http://www.ehu.es/histol-histopathol Histology and Histo pathology Invited Re vie W Molecular genetics of ovarian carcinomas J. Diebold Pathological Institute, Ludwig-Maximilians-University
Both type I and type II tumors develop from extraovarian tissue that implants on the ovary. Both for LGSC and HGSC, the fallopian tube appears to be
 Recent studies have led to the development of a new paradigm for the pathogenesis and origin of EOC, based on a dualistic model of carcinogenesis that divides EOC into 2 broad categories designated types
Recent studies have led to the development of a new paradigm for the pathogenesis and origin of EOC, based on a dualistic model of carcinogenesis that divides EOC into 2 broad categories designated types
Lavage of the uterine cavity as potential tool for diagnosis of epithelial ovarian cancer and its precursors
 Lavage of the uterine cavity as potential tool for diagnosis of epithelial ovarian cancer and its precursors Gynecologic Cancer Intergroup GCIG 2013 Autumn Meeting London, UK November 17 th 2013 Type II
Lavage of the uterine cavity as potential tool for diagnosis of epithelial ovarian cancer and its precursors Gynecologic Cancer Intergroup GCIG 2013 Autumn Meeting London, UK November 17 th 2013 Type II
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Update in Salivary Gland Pathology. Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016
 Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
New Developments in Immunohistochemistry for Gynecologic Pathology
 New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
Biomarker expression in normal fimbriae: Comparison of high- and low-grade serous ovarian carcinoma
 1008 Biomarker expression in normal fimbriae: Comparison of high- and low-grade serous ovarian carcinoma ZHANG XUYIN *, DING JINGXIN *, TAO XIANG, JIA LUOQI and HUA KEQIN Department of Obstetrics and Gynecology,
1008 Biomarker expression in normal fimbriae: Comparison of high- and low-grade serous ovarian carcinoma ZHANG XUYIN *, DING JINGXIN *, TAO XIANG, JIA LUOQI and HUA KEQIN Department of Obstetrics and Gynecology,
Borderline Ovarian Tumours. Andreas Obermair Brisbane
 Borderline Ovarian Tumours Andreas Obermair Brisbane Definition First described in 1929 Cellular features of malignancy Cellular atypia Mitotic activity No stromal invasion An entity per se??? (or precursor
Borderline Ovarian Tumours Andreas Obermair Brisbane Definition First described in 1929 Cellular features of malignancy Cellular atypia Mitotic activity No stromal invasion An entity per se??? (or precursor
A Serous Borderline Tumor of the Fallopian Tube Detected Incidentally
 A Serous Borderline Tumor of the Fallopian Tube Detected Incidentally Imrana Tanvir, Ghania Ali, Haseeb Ahmed Khan and Ahmed Nasir Hanifi* Dept. of Histopathology, FMH College of Medicine & Dentistry,
A Serous Borderline Tumor of the Fallopian Tube Detected Incidentally Imrana Tanvir, Ghania Ali, Haseeb Ahmed Khan and Ahmed Nasir Hanifi* Dept. of Histopathology, FMH College of Medicine & Dentistry,
Work up of a Pelvic Mass
 Work up of a Pelvic Mass Considerations from the north where primary care and CON clinic / GPO work interface Dr. Shannon Douglas, GPO Vanderhoof with support by Dr Margaret Smith and Dr. Ursula Lee Nov
Work up of a Pelvic Mass Considerations from the north where primary care and CON clinic / GPO work interface Dr. Shannon Douglas, GPO Vanderhoof with support by Dr Margaret Smith and Dr. Ursula Lee Nov
Molecular Subtyping of Endometrial Cancer: A ProMisE ing Change
 Molecular Subtyping of Endometrial Cancer: A ProMisE ing Change Charles Matthew Quick, M.D. Associate Professor of Pathology Director of Gynecologic Pathology University of Arkansas for Medical Sciences
Molecular Subtyping of Endometrial Cancer: A ProMisE ing Change Charles Matthew Quick, M.D. Associate Professor of Pathology Director of Gynecologic Pathology University of Arkansas for Medical Sciences
Biology Response Controversies and Advances
 Biology Response Controversies and Advances in BRCA related ovarian cancer Lessons learned and future directions Michael Friedlander The Prince of Wales Hospital and Royal Hospital for Women Sydney BREAST-CANCER
Biology Response Controversies and Advances in BRCA related ovarian cancer Lessons learned and future directions Michael Friedlander The Prince of Wales Hospital and Royal Hospital for Women Sydney BREAST-CANCER
Pathology of the female genital tract
 Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
6/5/2010. Outline of Talk. Endometrial Alterations That Mimic Cancer & Vice Versa: Metaplastic / reactive changes. Problems in Biopsies/Curettages
 Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Clinical History USCAP Specialty Conference. Gynecologic Pathology Case 3
 2010 USCA Specialty Conference Gynecologic athology Case Kathleen R. Cho, M.D. Department of athology Clinical History 46 yo woman presented with bilateral ovarian masses and elevated CA-125 TAH/BSO, pelvic
2010 USCA Specialty Conference Gynecologic athology Case Kathleen R. Cho, M.D. Department of athology Clinical History 46 yo woman presented with bilateral ovarian masses and elevated CA-125 TAH/BSO, pelvic
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Patologia Molecular del Carcinoma de Ovario
 Curso de Patologia Molecular XXVI Congreso Nacional de la SEAP Cadiz Patologia Molecular del Carcinoma de Ovario Jaime Prat Barcelona Ovarian Epithelial Tumors WHO 1999 and 2003 Serous Mucinous Endometrioid
Curso de Patologia Molecular XXVI Congreso Nacional de la SEAP Cadiz Patologia Molecular del Carcinoma de Ovario Jaime Prat Barcelona Ovarian Epithelial Tumors WHO 1999 and 2003 Serous Mucinous Endometrioid
Pathobiology of ovarian carcinomas
 Chinese Journal of Cancer Review Mojgan Devouassoux-Shisheboran 1 and Catherine Genestie 2 Abstract Ovarian tumors comprise a heterogeneous group of lesions, displaying distinct tumor pathology and oncogenic
Chinese Journal of Cancer Review Mojgan Devouassoux-Shisheboran 1 and Catherine Genestie 2 Abstract Ovarian tumors comprise a heterogeneous group of lesions, displaying distinct tumor pathology and oncogenic
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus
 Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
Various hereditary, acquired and neoplastic conditions can lead to cyst formation in the kidney.
 Dr. Fatima AlAl-Hashimi Hashimi,, MD, FRCPath Salmaniya Medical Complex, Bahrain Various hereditary, acquired and neoplastic conditions can lead to cyst formation in the kidney. The most frequently encountered
Dr. Fatima AlAl-Hashimi Hashimi,, MD, FRCPath Salmaniya Medical Complex, Bahrain Various hereditary, acquired and neoplastic conditions can lead to cyst formation in the kidney. The most frequently encountered
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Article begins on next page
 Pseudopapillary Granulosa Cell Tumor: A Case of This Rare Subtype Rutgers University has made this article freely available. Please share how this access benefits you. Your story matters. [https://rucore.libraries.rutgers.edu/rutgers-lib/50622/story/]
Pseudopapillary Granulosa Cell Tumor: A Case of This Rare Subtype Rutgers University has made this article freely available. Please share how this access benefits you. Your story matters. [https://rucore.libraries.rutgers.edu/rutgers-lib/50622/story/]
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Clonal evolution of human cancers
 Clonal evolution of human cancers -Pathology-based microdissection and genetic analysis precisely demonstrates molecular evolution of neoplastic clones- Hiroaki Fujii, MD Ageo Medical Laboratories, Yashio
Clonal evolution of human cancers -Pathology-based microdissection and genetic analysis precisely demonstrates molecular evolution of neoplastic clones- Hiroaki Fujii, MD Ageo Medical Laboratories, Yashio
Page # 1. Endometrium. Cellular Components. Anatomical Regions. Management of SIL Thomas C. Wright, Jr. Most common diseases:
 Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical