The Paris classification of colonic lesions
|
|
|
- Britton Byrd
- 6 years ago
- Views:
Transcription
1 The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker
2 Introduction Japanese classification morphology of superficial lesions of the gastrointestinal tract 2002 international Endoscopic Classification Review Group: the Paris Classification of Neoplastic Lesions in the digestive tract Adequate description of polyp morphology and size of importance Helps to determine appropriate method of treatment Has a predictive value for submucosal invasion Facilitates comparative research in colonoscopy practice However, thus far the validity and reproducibility of the classification has not been assessed.until now!
3 Aim & Methods To evaluate the interobserver agreement of the Paris classification and size of colorectal neoplasms among 7 western expert endoscopists 7 expert endoscopists assessed the Paris classification of 85 colonic polyps in short video clips (10-25 seconds) A Fleiss kappa using an absolute agreement definition was used to measure interobserver agreement with an interpretation of kappa values according to Landis and Koch 1 1. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977;33:
4 Results The interobserver agreement of the Paris classification of 85 polyps among 7 experts was moderate with a kappa of 0.42 (95% CI ) When analysing the data on polyp morphology assessments into just two categories, polypoid (Paris Ip, Isp, Is) vs. non-polypoid (Paris IIa, IIb, IIc, III) the Fleiss kappa remained moderate with a kappa of 0.45 (95% CI of )
5 Conclusion Interobserver agreement of the Paris classification for polyp morphology was only moderate No improvement when polyp classification was dichotomized to polypoid vs. non-polypoid categories Before the Paris classification of colonic neoplasms can be adequately used in western endoscopy units, it seems necessary to train endoscopists to achieve uniformity in classifying morphology of colonic lesions.
6 Training Training schedule Step 1: basics Step 2: examples Step 3: training Step 4: feedback Step 5: re-assessment of the same 85 polyps to evaluate agreement again

7 Step 1: basics The Paris classification is based on the Japanese classification of superficial neoplastic lesions in the gastrointestinal tract Lambert R et al. Endoscopic Classification Review Group. Update on the Paris Classification of Superficial Neoplastic Lesion in the Digestive Tract. Endoscopy 2005

8 Step 1: basics We will focus only on the main type of morphology (so no combined types) Lambert R et al. Endoscopic Classification Review Group. Update on the Paris Classification of Superficial Neoplastic Lesion in the Digestive Tract. Endoscopy 2005
9 Step 1: basics Protruding types (0-I) protrude above the surrounding surface at endoscopy: 0-Ip pedunculated 0-Isp subpedunculated 0-Is sessile Lambert R et al. Endoscopic Classification Review Group. Update on the Paris Classification of Superficial Neoplastic Lesion in the Digestive Tract. Endoscopy 2005

10 Step 1: basics Pedunculated (0-Ip): Base is more narrow than top of lesion M= mucosa, mm= muscularis mucosae, sm= submucosa The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.
11 Step 1: basics Subpedunculated (0-Isp): Intermediate and broad-based Same management as (0-Is) sessile polyps Lambert R et al. Endoscopic Classification Review Group. Update on the Paris Classification of Superficial Neoplastic Lesion in the Digestive Tract. Endoscopy 2005
12 Step 1: basics Sessile (0-Is): Base and top of lesion have same diameter The protrusion of the lesion is compared with the height of the closed cups of a biopsy forceps (2.5mm), dotted arrow passes under top of lesion M= mucosa, mm= muscularis mucosae, sm= submucosa The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.
13 Step 1: basics Non-protruding non-excaved types (0-II): Slightly elevated (0-IIa) Completely flat (0-IIb) Slightly depressed (0-IIc) Lambert R et al. Endoscopic Classification Review Group. Update on the Paris Classification of Superficial Neoplastic Lesion in the Digestive Tract. Endoscopy 2005
14 Step 1: basics Slightly elevated (0-IIa) Slightly higher than adjacent mucosa The protrusion of the lesion is compared with the height of the closed cups of a biopsy forceps (2.5mm), dotted arrow passes under top of lesion M= mucosa, mm= muscularis mucosae, sm= submucosa The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.
15 Step 1: basics Slightly elevated (0-IIa) vs Sessile (0-Is) Easily misclassified Classification is made easier by placing a biopsy forceps as a calibrating gauge, for the height of the lesion Lesions protruding above the level of the closed jaws of the biopsy forceps (2.5mm), are classified as 0-Is, lesions protruding below this level are classified as 0-IIa The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.
16 Step 1: basics Completely flat (0-IIb) Lesion does not protrude above mucosal surface M= mucosa, mm= muscularis mucosae, sm= submucosa The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.
17 Step 1: basics Slightly depressed (0-IIc) Superficial erosions in a depressed lesion involve only the most superficial layers Absolutely depressed: level of depression is lower then the surface of the adjacent mucosa Relatively depressed: level of depression is still higher than the surface of the adjacent mucosa M= mucosa, mm= muscularis mucosae, sm= submucosa The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.

18 Step 1: basics Excavated/Ulcerated (0-III) Lesion with deep ulcer below mucosa Loss of the mucosa and often of the submucosa Distinction between a slightly depressed (0-IIc) and excavated (0-III) lesion: based on the depth of the depression from the adjacent mucosa Cut-off limit is 1.2 mm in columnar epithelium However: 0-III extremely rare in the colon The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.
19 Step 2: examples Assessing drawings is easier than assessing movies You will now see 8 examples of polyps in video clips with different types of morphology according to the Paris classification, some next to a biopsy forceps
20 Step 2: examples Difference between sessile (0-Is) and slightly elevated (0-IIa) is difficult Forceps cups next to lesion make differentiation easier Most of the examples will show sessile or slightly elevated lesions, as we think this causes the most interobserver variability If you click on the picture, the movie will start (duration varies from seconds)

21 Step 2: examples Example 1: pedunculated polyp (0-Ip)

22 Step 2: examples Example 2: sessile polyp (0-Is)

23 Step 2: examples Example 3: slightly elevated lesion (0-IIa)

24 Step 2: examples Example 4: slightly elevated lesion (0-IIa)

25 Step 2: examples Example 5: completely flat lesion (0-IIb)

26 Step 2: examples Example 6: sessile polyp (0-Is)

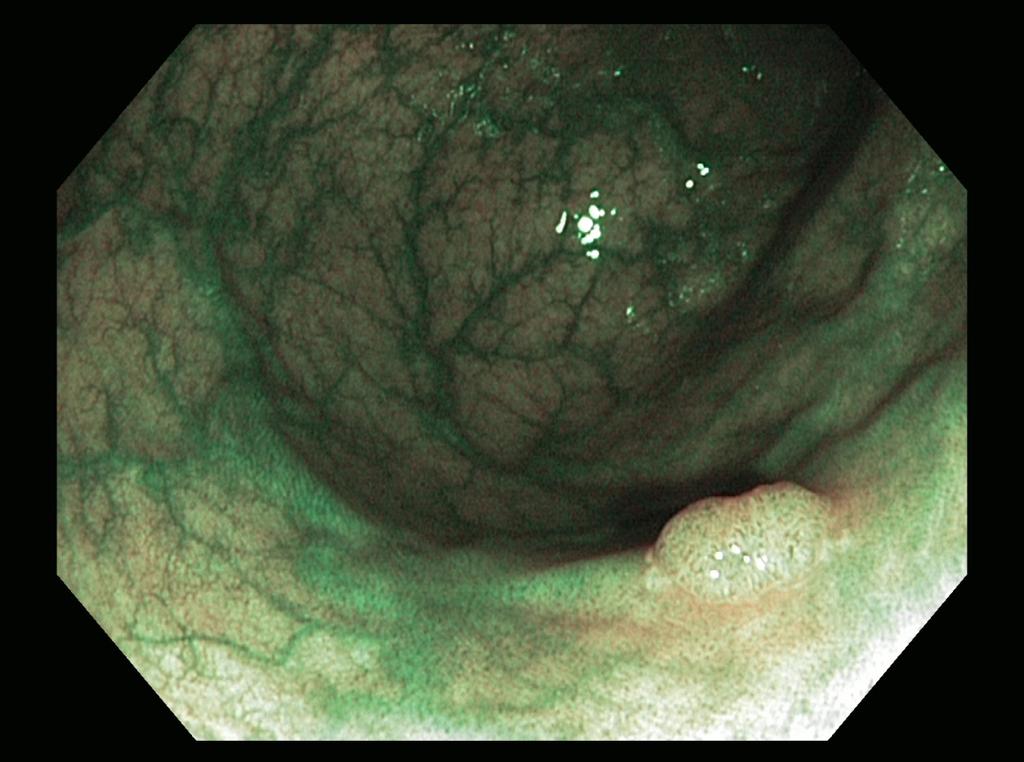
27 Step 2: examples Example 7: slightly elevated lesion (0-IIa)

28 Step 2: examples Example 8: slightly elevated lesion (0-IIa)
29 Step 2: examples In preparation of the photo training, 6 photo examples are shown from the original article of the Paris workshop 2002 The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.
, 2003 Gastrointestinal Endoscopy.")
30 Step 2: examples Photo example 1: 0-Is The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.
, 2003 Gastrointestinal Endoscopy.")
31 Step 2: examples Photo example 2: 0-IIa The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.
, 2003 Gastrointestinal Endoscopy.")
32 Step 2: examples Photo example 3: 0-IIa The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.
, 2003 Gastrointestinal Endoscopy.")
33 Step 2: examples Photo example 4: 0-IIc The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.

34 Step 2: examples Photo example 5: 0-IIc + IIa The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.
, 2003 Gastrointestinal Endoscopy.")
35 Step 2: examples Photo example 6: 0-IIc The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. November 30 to December 1, Paris Workshop Participants. Volume 58, No. 6 (Suppl), 2003 Gastrointestinal Endoscopy.
36 Step 3: training Next you will see 32 photographs of polyps Please classify the morphology of these polyps according to the Paris classification on the Training Assessment Form (word document in the WeTransfer file) Please do not look at the Feedback Form before you filled in the Assessment form

37 Step 3: training Photo 1

38 Step 3: training Photo 2


39 Step 3: training Photo 3
40 Step 3: training Photo 4

41 Step 3: training Photo 5

42 Step 3: training Photo 6

43 Step 3: training Photo 7

44 Step 3: training Photo 8

45 Step 3: training Photo 9

46 Step 3: training Photo 10

47 Step 3: training Photo 11

48 Step 3: training Photo 12

49 Step 3: training Photo 13

50 Step 3: training Photo 14

51 Step 3: training Photo 15

52 Step 3: training Photo 16

53 Step 3: training Photo 17

54 Step 3: training Photo 18

55 Step 3: training Photo 19

56 Step 3: training Photo 20

57 Step 3: training Photo 21

58 Step 3: training Photo 22

59 Step 3: training Photo 23

60 Step 3: training Photo 24

61 Step 3: training Photo 25

62 Step 3: training Photo 26

63 Step 3: training Photo 27

64 Step 3: training Photo 28

65 Step 3: training Photo 29

66 Step 3: training Photo 30

67 Step 3: training Photo 31

68 Step 3: training Photo 32
69 Step 3: training END of TRAINING
70 Step 4: feedback You can now check your answers with the Feedback form (word document in the WeTransfer file) As there is no golden standard, the correct classifications were determined by an panel of 3 physicians. Only the 32 polyps with total agreement were used for the training. The purpose of the training is to evaluate if the interobserver agreement improves after all 7 experts have been through the same basics and examples of the classification Your answers are private, no need to send these to the researcher
71 Step 5: re-assessment Please watch the 85 polyp movies again Classify them according to the Paris classification Also re-evaluate the other items The Clinical Record Form of the movies can be send to researcher by mail/ /fax Thank you very much!!
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions
 Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Formula One Study. Assessment criteria of pathological parameters. Ver.2. UK Japan Joint Study for Risk Factors of Lymph Node
 APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
Clinicopathological Characteristics of Superficial Type
 Diagnostic and Therapeutic Endoscopy, 1995, Vol. 2, pp. 99-105 Reprints available directly from the publisher Photocopying permitted by license only (C) 1995 Harwood Academic Publishers GmbH Printed in
Diagnostic and Therapeutic Endoscopy, 1995, Vol. 2, pp. 99-105 Reprints available directly from the publisher Photocopying permitted by license only (C) 1995 Harwood Academic Publishers GmbH Printed in
위암내시경진단 (2019) - 융기형위암을중심으로 성균관대학교의과대학내과이준행
 - 융기형위암을중심으로 성균관대학교의과대학내과이준행") 위암내시경진단 (2019) - 융기형위암을중심으로 성균관대학교의과대학내과이준행 위암내시경진단 (2019) 위암검진에대한짧지않은 comment 융기형암은융기되어있는가? 함몰형암은함몰되어있는가? Semi-pedunculated polyp Sentinel polyp or EGJ cancer? IIa + IIc 위암검진에대한짧지않은 comment 성균관대학교의과대학내과이준행
위암내시경진단 (2019) - 융기형위암을중심으로 성균관대학교의과대학내과이준행 위암내시경진단 (2019) 위암검진에대한짧지않은 comment 융기형암은융기되어있는가? 함몰형암은함몰되어있는가? Semi-pedunculated polyp Sentinel polyp or EGJ cancer? IIa + IIc 위암검진에대한짧지않은 comment 성균관대학교의과대학내과이준행
IN THE DEVELOPMENT and progression of colorectal
 Digestive Endoscopy 2014; 26 (Suppl. 2): 73 77 doi: 10.1111/den.12276 Treatment strategy of diminutive colorectal polyp
Digestive Endoscopy 2014; 26 (Suppl. 2): 73 77 doi: 10.1111/den.12276 Treatment strategy of diminutive colorectal polyp
Endoscopic Corner CASE 1. Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R
 170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Do any benign polyps require an operation?
 Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday
Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD
 SNARE THE CASE FOR EMR AND ESD") THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
Introduction. Piecemeal EMR (EPMR) Symposium
 Symposium") Symposium Symposium II - Lower GI : Colonoscopy Issues in 2015 Resection of Large Polyps Using Techniques other than Endoscopic Submucosal Dissection: Piecemeal Resection, Underwater Endoscopic Mucosal
Symposium Symposium II - Lower GI : Colonoscopy Issues in 2015 Resection of Large Polyps Using Techniques other than Endoscopic Submucosal Dissection: Piecemeal Resection, Underwater Endoscopic Mucosal
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Videoendoscopy of Colonic Early Cancer
 Diagnostic and Therapeutic Endoscopy, 1995, Vol. 1, pp. 125-130 Reprints available directly from the publisher Photocopying permitted by license only (C) 1995 Harwood Academic Publishers GmbH Printed in
Diagnostic and Therapeutic Endoscopy, 1995, Vol. 1, pp. 125-130 Reprints available directly from the publisher Photocopying permitted by license only (C) 1995 Harwood Academic Publishers GmbH Printed in
COLON: Innovations 3 steps, 3 parts..
 COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
Colon Polyps: Detection, Inspection and Characteristics
 Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD)
 & Endoscopic Submucosal Dissection (ESD)") Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD) Minimally Invasive Polyp Removal IE-02700-Understanding EMR and ESD Brochure_R3.indd 1 Occasionally, a polyp that infiltrates
Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD) Minimally Invasive Polyp Removal IE-02700-Understanding EMR and ESD Brochure_R3.indd 1 Occasionally, a polyp that infiltrates
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
EMR, ESD and Beyond. Peter Draganov MD. Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida
 EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease
 ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
Factors for Endoscopic Submucosal Dissection in Early Colorectal Neoplasms: A Single Center Clinical Experience in China
 ORIGINAL ARTICLE Clin Endosc 2015;48:405-410 http://dx.doi.org/10.5946/ce.2015.48.5.405 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Factors for Endoscopic Submucosal Dissection in Early Colorectal
ORIGINAL ARTICLE Clin Endosc 2015;48:405-410 http://dx.doi.org/10.5946/ce.2015.48.5.405 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Factors for Endoscopic Submucosal Dissection in Early Colorectal
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of endoscopic submucosal dissection of gastric lesions This procedure can be
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of endoscopic submucosal dissection of gastric lesions This procedure can be
Size of colorectal polyps determines time taken to remove them endoscopically
 Original article Size of colorectal polyps determines time taken to remove them endoscopically Authors Heechan Kang 1, Mo Hameed Thoufeeq 2 Institutions 1 Department of Medicine, Peterborough Hospitals
Original article Size of colorectal polyps determines time taken to remove them endoscopically Authors Heechan Kang 1, Mo Hameed Thoufeeq 2 Institutions 1 Department of Medicine, Peterborough Hospitals
Adenoma to Carcinoma Pathway
 It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Clinicopathological features of colorectal polyps in 2002 and 2012
 ORIGINAL ARTICLE Korean J Intern Med 2019;34:65-71 Clinicopathological features of colorectal polyps in 2002 and 2012 Yoon Jeong Nam, Kyeong Ok Kim, Chan Seo Park, Si Hyung Lee, and Byung Ik Jang Division
ORIGINAL ARTICLE Korean J Intern Med 2019;34:65-71 Clinicopathological features of colorectal polyps in 2002 and 2012 Yoon Jeong Nam, Kyeong Ok Kim, Chan Seo Park, Si Hyung Lee, and Byung Ik Jang Division
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Spartan Medical Research Journal
 Spartan Medical Research Journal Research at Michigan State University College of Osteopathic Medicine Volume 2 Number 2 Winter, 2017 Pages 14-21 Title: Endoscopic Combined Snare-Forceps Technique for
Spartan Medical Research Journal Research at Michigan State University College of Osteopathic Medicine Volume 2 Number 2 Winter, 2017 Pages 14-21 Title: Endoscopic Combined Snare-Forceps Technique for
Pathology in Slovenian CRC screening programme: Organisation and quality assurance. Snježana Frković Grazio and Matej Bračko
 Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
Incidence and Management of Hemorrhage after Endoscopic Removal of Colorectal Lesions
 Showa Univ J Med Sci 12(3), 253-258, September 2000 Original Incidence and Management of Hemorrhage after Endoscopic Removal of Colorectal Lesions Masaaki MATSUKAWA, Mototsugu FUJIMORI, Takahiko KOUDA,
Showa Univ J Med Sci 12(3), 253-258, September 2000 Original Incidence and Management of Hemorrhage after Endoscopic Removal of Colorectal Lesions Masaaki MATSUKAWA, Mototsugu FUJIMORI, Takahiko KOUDA,
Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom
 Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom What exactly will be required? Defining levels of polypectomy competency in terms of complexity/time/risk
Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom What exactly will be required? Defining levels of polypectomy competency in terms of complexity/time/risk
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
Fujiya M, Saitoh Y, Watari J, Moriichi K, Kohgo Y.
 Digestive Endoscopy (2007) 19(s1):S145-S149. Auto-Fluorescence Imaging is useful to assess the activity of ulcerative colitis Fujiya M, Saitoh Y, Watari J, Moriichi K, Kohgo Y. Auto-Fluorescence Imaging
Digestive Endoscopy (2007) 19(s1):S145-S149. Auto-Fluorescence Imaging is useful to assess the activity of ulcerative colitis Fujiya M, Saitoh Y, Watari J, Moriichi K, Kohgo Y. Auto-Fluorescence Imaging
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
The addition of high magnifying endoscopy improves rates of high confidence optical diagnosis of colorectal polyps
 E140 The addition of high magnifying endoscopy improves rates of high confidence optical diagnosis of colorectal polyps Authors Mineo Iwatate 1, Yasushi Sano 1, Santa Hattori 1, Wataru Sano 1, Noriaki
E140 The addition of high magnifying endoscopy improves rates of high confidence optical diagnosis of colorectal polyps Authors Mineo Iwatate 1, Yasushi Sano 1, Santa Hattori 1, Wataru Sano 1, Noriaki
Quality Measures In Colonoscopy: Why Should I Care?
 Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working Group chair: Michal F. Kaminski, Poland
 Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working chair: Michal F. Kaminski, Poland Population Interventions Comparator Outcome Additional evidence 1.1 Rate of adequate
Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working chair: Michal F. Kaminski, Poland Population Interventions Comparator Outcome Additional evidence 1.1 Rate of adequate
University Mainz. Early Gastric Cancer. Ralf Kiesslich. Johannes Gutenberg University Mainz, Germany. Early Gastric Cancer 15.6.
 Ralf Kiesslich Johannes Gutenberg University Mainz, Germany DIAGNOSIS Unmask lesions - Chromoendoscopy -NBI Red flag technology - Autofluorescence Surface and detail analysis - Magnifying endoscopy - High
Ralf Kiesslich Johannes Gutenberg University Mainz, Germany DIAGNOSIS Unmask lesions - Chromoendoscopy -NBI Red flag technology - Autofluorescence Surface and detail analysis - Magnifying endoscopy - High
High Resolution Colonoscopy With Chromoscopy Versus Standard Colonoscopy for the Detection of Colonic Neoplasia: A Randomized Study
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:349 354 High Resolution Colonoscopy With Chromoscopy Versus Standard Colonoscopy for the Detection of Colonic Neoplasia: A Randomized Study MARC LE RHUN,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:349 354 High Resolution Colonoscopy With Chromoscopy Versus Standard Colonoscopy for the Detection of Colonic Neoplasia: A Randomized Study MARC LE RHUN,*
Prevalence and Characteristics of Nonpolypoid Colorectal Neoplasm in an Asymptomatic and Average-Risk Chinese Population
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:463 470 Prevalence and Characteristics of Nonpolypoid Colorectal Neoplasm in an Asymptomatic and Average-Risk Chinese Population HAN MO CHIU,*,, JAW TOWN
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:463 470 Prevalence and Characteristics of Nonpolypoid Colorectal Neoplasm in an Asymptomatic and Average-Risk Chinese Population HAN MO CHIU,*,, JAW TOWN
2015 Winter School 대장종양성병변의진단과치료. Dong Kyung Chang. Sungkyunkwan University, School of Medicine Samsung Medical Center
 2017 gastroenterology Winter School 77 2015 Winter School 대장종양성병변의진단과치료 Dong Kyung Chang Sungkyunkwan University, School of Medicine Samsung Medical Center Colon Polyps (Epithelial origin) Neoplastic Premalignant
2017 gastroenterology Winter School 77 2015 Winter School 대장종양성병변의진단과치료 Dong Kyung Chang Sungkyunkwan University, School of Medicine Samsung Medical Center Colon Polyps (Epithelial origin) Neoplastic Premalignant
Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate
 Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate Authors Yasuhiro Abe 1,HaruakiNabeta 1, Ryota Koyanagi 1, Taro Nakamichi 1, Hayato Hirashima 1, Alan Kawarai
Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate Authors Yasuhiro Abe 1,HaruakiNabeta 1, Ryota Koyanagi 1, Taro Nakamichi 1, Hayato Hirashima 1, Alan Kawarai
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis
 Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Esophageal submucosal mass icd 10
 Esophageal submucosal mass icd 10 Search 6-6-2011 ICD-10; Risk Adjustment / HCC; Evaluation & Management (E/M). I'm hoping someone can help me with this DX, "soft tissue mass in. Upper gastrointestinal
Esophageal submucosal mass icd 10 Search 6-6-2011 ICD-10; Risk Adjustment / HCC; Evaluation & Management (E/M). I'm hoping someone can help me with this DX, "soft tissue mass in. Upper gastrointestinal
Endoscopic Resection of a Rectal. Carcinoid Tumor with an Esophageal. Variceal Ligation Device. Report of a Case and Literature Review
 2006 7 28-32 Endoscopic Resection of a Rectal Carcinoid Tumor with an Esophageal Variceal Ligation Device Report of a Case and Literature Review Wei-Feng Feng, An-Liang Chou, Jen-En Tzeng, and Kuo-Chih
2006 7 28-32 Endoscopic Resection of a Rectal Carcinoid Tumor with an Esophageal Variceal Ligation Device Report of a Case and Literature Review Wei-Feng Feng, An-Liang Chou, Jen-En Tzeng, and Kuo-Chih
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
How to treat early gastric cancer? Endoscopy
 How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
An Atlas of the Nonpolypoid Colorectal Neoplasms in Inflammatory Bowel Disease
 An Atlas of the Nonpolypoid Colorectal Neoplasms in Inflammatory Bowel Disease Roy Soetikno, MD a, *, Silvia Sanduleanu, MD, PhD b, Tonya Kaltenbach, MD a KEYWORDS Inflammatory bowel disease Nonpolypoid
An Atlas of the Nonpolypoid Colorectal Neoplasms in Inflammatory Bowel Disease Roy Soetikno, MD a, *, Silvia Sanduleanu, MD, PhD b, Tonya Kaltenbach, MD a KEYWORDS Inflammatory bowel disease Nonpolypoid
Risk factors for cervical lymph node metastasis in superficial head and neck squamous cell carcinoma
 J Med Dent Sci 2015; 62: 19-24 Original Article Risk factors for cervical lymph node metastasis in superficial head and neck squamous cell carcinoma Toru Sasaki, MD 1, 2), Seiji Kishimoto, MD, PhD 1),
J Med Dent Sci 2015; 62: 19-24 Original Article Risk factors for cervical lymph node metastasis in superficial head and neck squamous cell carcinoma Toru Sasaki, MD 1, 2), Seiji Kishimoto, MD, PhD 1),
B Barrett neoplasia, early, endoscopic mucosal resection of, in Europe, 297
 Note: Page numbers of article titles are in boldface type. A Achalasia, treatment of, history of, 258 259 Achalasia myotomy, 270 Adenocarcinomas, endoscopic management of, in Asia, 289 290 B Barrett neoplasia,
Note: Page numbers of article titles are in boldface type. A Achalasia, treatment of, history of, 258 259 Achalasia myotomy, 270 Adenocarcinomas, endoscopic management of, in Asia, 289 290 B Barrett neoplasia,
Measure #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clincal Care
 Measure #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clincal Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION: The percentage
Measure #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clincal Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION: The percentage
Comparison of the Diagnostic Usefulness of Conventional Magnification and Near-focus Methods with Narrow-band Imaging for Gastric Epithelial Tumors
 ORIGINAL ARTICLE ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2015.15.1.39 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2015;15(1):39-43 Comparison of the Diagnostic Usefulness
ORIGINAL ARTICLE ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2015.15.1.39 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2015;15(1):39-43 Comparison of the Diagnostic Usefulness
ESD for EGC with undifferentiated histology
 ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
The white globe appearance (WGA): a novel marker for a correct diagnosis of early gastric cancer by magnifying. endoscopy with narrow-band imaging (M-
: a novel marker for a correct diagnosis of early gastric cancer by magnifying. endoscopy with narrow-band imaging (M-") E120 The white globe appearance (WGA): a novel marker for a correct diagnosis of early gastric cancer by magnifying endoscopy with narrow-band imaging (M-NBI) Authors Hisashi Doyama 1, Naohiro Yoshida
E120 The white globe appearance (WGA): a novel marker for a correct diagnosis of early gastric cancer by magnifying endoscopy with narrow-band imaging (M-NBI) Authors Hisashi Doyama 1, Naohiro Yoshida
Pyogenic granuloma of the jejunum; diagnosis and treatment with double-balloon enteroscopy: A case report
 Pyogenic granuloma of the jejunum; diagnosis and treatment with double-balloon enteroscopy: A case report Granuloma piógeno de yeyuno. Diagnóstico y tratamiento con enteroscopia doble balón. Reporte de
Pyogenic granuloma of the jejunum; diagnosis and treatment with double-balloon enteroscopy: A case report Granuloma piógeno de yeyuno. Diagnóstico y tratamiento con enteroscopia doble balón. Reporte de
Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications
 and Clinicoradiologic Implications") Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications Poster No.: E-0060 Congress: ESTI 2012 Type: Scientific Exhibit Authors: K. Lee, T. J.
Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications Poster No.: E-0060 Congress: ESTI 2012 Type: Scientific Exhibit Authors: K. Lee, T. J.
Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations
 Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care
 Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
EXPERT WORKING GROUP Surveillance after neoplasia removal. Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum
 EXPERT WORKING GROUP Surveillance after neoplasia removal Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum AIM To improve the quality of the evidences we have regarding post- polypectomy
EXPERT WORKING GROUP Surveillance after neoplasia removal Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum AIM To improve the quality of the evidences we have regarding post- polypectomy
Corporate Medical Policy
 Corporate Medical Policy Chromoendoscopy as an Adjunct to Colonoscopy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: chromoendoscopy_as_an_adjunct_to_colonoscopy 7/2012 11/2017
Corporate Medical Policy Chromoendoscopy as an Adjunct to Colonoscopy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: chromoendoscopy_as_an_adjunct_to_colonoscopy 7/2012 11/2017
European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition
 SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN
 Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN Chief Complaint : 1)intermittent LLQ cramping pain for 2 months 2) LGI
Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN Chief Complaint : 1)intermittent LLQ cramping pain for 2 months 2) LGI
T. Shono, 1 K. Ishikawa, 1 Y. Ochiai, 1 M. Nakao, 1 O. Togawa, 1 M. Nishimura, 1 S. Arai, 1 K. Nonaka, 2 Y. Sasaki, 2 and H. Kita 1. 1.
 International Surgical Oncology Volume 2011, Article ID 948293, 6 pages doi:10.1155/2011/948293 Clinical Study Feasibility of Endoscopic Submucosal Dissection: A New Technique for En Bloc Resection of
International Surgical Oncology Volume 2011, Article ID 948293, 6 pages doi:10.1155/2011/948293 Clinical Study Feasibility of Endoscopic Submucosal Dissection: A New Technique for En Bloc Resection of
University of Groningen
 University of Groningen Incidence of small bowel neoplasia in Lynch syndrome assessed by video capsule endoscopy Haanstra, Jasmijn; Al-Toma, Abdul; Dekker, Evelien; Vanhoutvin, Steven A L W; Nagengast,
University of Groningen Incidence of small bowel neoplasia in Lynch syndrome assessed by video capsule endoscopy Haanstra, Jasmijn; Al-Toma, Abdul; Dekker, Evelien; Vanhoutvin, Steven A L W; Nagengast,
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Advances in Endoscopic Imaging
 Advances in Endoscopic Imaging SGNA meeting February 20, 2010 Amar R. Deshpande, MD Asst Professor of Medicine Division of Gastroenterology University of Miami Miller School of Medicine Objectives To recognize
Advances in Endoscopic Imaging SGNA meeting February 20, 2010 Amar R. Deshpande, MD Asst Professor of Medicine Division of Gastroenterology University of Miami Miller School of Medicine Objectives To recognize
Hidehiko; Kohno, Shigeru. Citation Acta medica Nagasakiensia. 1997, 42
 NAOSITE: Nagasaki University's Ac Title Author(s) Superficial Depressed Type (IIc) Ea Two Cases Iwamoto, Michiko; Makiyama, Kazuya; Yohei; Omagari, Katsuhisa; Yamakawa Shiro; Haraguchi, Masuho; Itsuno,
NAOSITE: Nagasaki University's Ac Title Author(s) Superficial Depressed Type (IIc) Ea Two Cases Iwamoto, Michiko; Makiyama, Kazuya; Yohei; Omagari, Katsuhisa; Yamakawa Shiro; Haraguchi, Masuho; Itsuno,
Endoscopic Ultrasonography (EUS) Medical Imaging of the Digestive Tract and Internal Organs
 Medical Imaging of the Digestive Tract and Internal Organs") Endoscopic Ultrasonography (EUS) Medical Imaging of the Digestive Tract and Internal Organs More Detailed Pictures for Better Diagnoses Endoscopic ultrasonography allows your doctor to examine your stomach
Endoscopic Ultrasonography (EUS) Medical Imaging of the Digestive Tract and Internal Organs More Detailed Pictures for Better Diagnoses Endoscopic ultrasonography allows your doctor to examine your stomach
Traction-assisted colonic endoscopic submucosal dissection using clip and line: a feasibility study
 E51 Traction-assisted colonic endoscopic submucosal dissection using clip and line: a feasibility study Authors Institution Yasushi Yamasaki, Yoji Takeuchi, Noriya Uedo, Minoru Kato, Kenta Hamada, Kenji
E51 Traction-assisted colonic endoscopic submucosal dissection using clip and line: a feasibility study Authors Institution Yasushi Yamasaki, Yoji Takeuchi, Noriya Uedo, Minoru Kato, Kenta Hamada, Kenji
removal of adenomatous polyps detects important effectively as follow-up colonoscopy after both constitute a low-risk Patients with 1 or 2
 Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Local recurrence after endoscopic resection of colorectal tumors
 Int J Colorectal Dis (2009) 24:225 230 DOI 10.1007/s00384-008-0596-8 ORIGINAL ARTICLE Local recurrence after endoscopic resection of colorectal tumors Kinichi Hotta & Takahiro Fujii & Yutaka Saito & Takahisa
Int J Colorectal Dis (2009) 24:225 230 DOI 10.1007/s00384-008-0596-8 ORIGINAL ARTICLE Local recurrence after endoscopic resection of colorectal tumors Kinichi Hotta & Takahiro Fujii & Yutaka Saito & Takahisa
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
EASTERN SHORE ENDOSCOPY, LLC (ESE)
") EASTERN SHORE ENDOSCOPY, LLC (ESE) Endoscopy Consent An endoscopy is a medical procedure where your doctor, using a flexible video instrument (endoscope), looks at various areas inside of your body, which
EASTERN SHORE ENDOSCOPY, LLC (ESE) Endoscopy Consent An endoscopy is a medical procedure where your doctor, using a flexible video instrument (endoscope), looks at various areas inside of your body, which
Chromoendoscopy - Should It Be Standard of Care in IBD?
 Chromoendoscopy - Should It Be Standard of Care in IBD? John F. Valentine, MD, FACG Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Utah What is the point of
Chromoendoscopy - Should It Be Standard of Care in IBD? John F. Valentine, MD, FACG Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Utah What is the point of
Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications
 Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications Authors: *Emil Salmo, 1 Najib Haboubi 2 1. Department of Histopathology, The Pennine Acute Hospitals NHS Trust,
Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications Authors: *Emil Salmo, 1 Najib Haboubi 2 1. Department of Histopathology, The Pennine Acute Hospitals NHS Trust,
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
The malignant colorectal polyp
 The malignant colorectal polyp Dr Ian Brown Envoi Pathology Envoi data reproduced from J Clin Path 2015 article Definition Adenocarcinoma found in an endoscopically resected polypoidal tumour Submucosal
The malignant colorectal polyp Dr Ian Brown Envoi Pathology Envoi data reproduced from J Clin Path 2015 article Definition Adenocarcinoma found in an endoscopically resected polypoidal tumour Submucosal
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
Research Article Endoscopic Management of Nonlifting Colon Polyps
 Diagnostic and Therapeutic Endoscopy Volume 2013, Article ID 412936, 5 pages http://dx.doi.org/10.1155/2013/412936 Research Article Endoscopic Management of Nonlifting Colon Polyps Shai Friedland, 1,2
Diagnostic and Therapeutic Endoscopy Volume 2013, Article ID 412936, 5 pages http://dx.doi.org/10.1155/2013/412936 Research Article Endoscopic Management of Nonlifting Colon Polyps Shai Friedland, 1,2
Risk Factors for Incomplete Polyp Resection during Colonoscopic Polypectomy
 Gut and Liver, Vol. 9, No. 1, January 2015, pp. 66-72 ORiginal Article Risk Factors for Incomplete Polyp Resection during Colonoscopic Polypectomy Sang Pyo Lee, In-Kyung Sung, Jeong Hwan Kim, Sun-Young
Gut and Liver, Vol. 9, No. 1, January 2015, pp. 66-72 ORiginal Article Risk Factors for Incomplete Polyp Resection during Colonoscopic Polypectomy Sang Pyo Lee, In-Kyung Sung, Jeong Hwan Kim, Sun-Young
WEO CRC SC Meeting. Barcelona, Spain October 23, 2015
 WEO CRC SC Meeting Barcelona, Spain October 23, 2015 Identification of serrated polyposis syndrome in the context of population-based CRC screening programs Evelien Dekker Academic Medical Center Amsterdam,
WEO CRC SC Meeting Barcelona, Spain October 23, 2015 Identification of serrated polyposis syndrome in the context of population-based CRC screening programs Evelien Dekker Academic Medical Center Amsterdam,
Research Article Diagnostic Accuracy of Mucosal Biopsy versus Endoscopic Mucosal Resection in Barrett s Esophagus and Related Superficial Lesions
 International Scholarly Research Notices Volume 2015, rticle ID 735807, 6 pages http://dx.doi.org/10.1155/2015/735807 Research rticle Diagnostic ccuracy of Mucosal iopsy versus Endoscopic Mucosal Resection
International Scholarly Research Notices Volume 2015, rticle ID 735807, 6 pages http://dx.doi.org/10.1155/2015/735807 Research rticle Diagnostic ccuracy of Mucosal iopsy versus Endoscopic Mucosal Resection
Philip Chiu Associate Professor Department of Surgery, Prince of Wales Hospital The Chinese University of Hong Kong
 Application of Chromoendoscopy, NBI and AFI in Esophagus why, who, and how? Philip Chiu Associate Professor Department of Surgery, Prince of Wales Hospital The Chinese University of Hong Kong Cancer of
Application of Chromoendoscopy, NBI and AFI in Esophagus why, who, and how? Philip Chiu Associate Professor Department of Surgery, Prince of Wales Hospital The Chinese University of Hong Kong Cancer of
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
CT Colonography: Image interpretation. Beth G. McFarland, MD
 CT Colonography: Image interpretation Beth G. McFarland, MD Part III CTC Overview of different morphologic types:» Focal polyp vs stool» Sessile lesion and flat lesions» Pedunculated lesion» Cancer vs
CT Colonography: Image interpretation Beth G. McFarland, MD Part III CTC Overview of different morphologic types:» Focal polyp vs stool» Sessile lesion and flat lesions» Pedunculated lesion» Cancer vs
GI Screening/Surveillance in Lynch Syndrome
 GI Screening/Surveillance in Lynch Syndrome M Appleyard Royal Brisbane and Women s Hospital Brisbane, Australia GI Disease and Lynch Syndrome What are risks of GI disease in Lynch? Who do we screen for
GI Screening/Surveillance in Lynch Syndrome M Appleyard Royal Brisbane and Women s Hospital Brisbane, Australia GI Disease and Lynch Syndrome What are risks of GI disease in Lynch? Who do we screen for
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the