Nervous About Nerve Sheath Tumours?
|
|
|
- Ashlyn Caldwell
- 6 years ago
- Views:
Transcription
 Review spectrum of cutaneous nerve sheath tumors Vast majority are benign & include neurofibromas, schwannomas, perineuriomas, granular cell tumors,")
1 Goals Nervous About Nerve Sheath Tumours? Rajiv M. Patel, M.D. RCPA NZ ASM 2017 (3:30-4:15pm, Saturday, ) Review spectrum of cutaneous nerve sheath tumors Vast majority are benign & include neurofibromas, schwannomas, perineuriomas, granular cell tumors, & various neuroma subtypes Malignant granular cell tumor & malignant peripheral nerve sheath tumor are also rarely encountered in the skin Diagnostic criteria and practical considerations are emphasized 2 Benign nerve sheath tumors Malignant nerve sheath tumors Neuromas Neurofibroma Diffuse Plexiform Schwannoma Cellular Neuroblastoma-like Plexiform Perineurioma Hybrid nerve sheath tumor Granular cell tumor Malignant peripheral nerve sheath tumor (MPNST) Atypical neurofibroma vs MPNST Epithelioid MPNST Malignant granular cell tumor year-old-female with a left cheek papulonodule 6 1
 Key pathologic features: Solitary circumscribed neuroma AKA palisaded encapsulated neuroma Usually present on head and neck, especially face Well circumscribed")
2 Diagnosis? Solitary circumscribed neuroma (SCN) Key pathologic features: Solitary circumscribed neuroma AKA palisaded encapsulated neuroma Usually present on head and neck, especially face Well circumscribed with thin incomplete capsule Some may have a plexiform growth pattern Fascicles of spindled cells with distinct clefting S100+, NF+ axons, EMA+ perineurium Differential: Solitary circumscribed neuroma Schwannoma Developed capsule Cellular Antoni A and hypocellular Antoni B areas Verocay bodies Lack clefting artifact Neuofibroma More heterogeneous appearance Plexiform NF must be distinguished from SCN with plexiform growth pattern Mucosal neuromas Multiple lesions MEN2b Leiomyoma SMA+, S Other neuromas Traumatic Sites of previous injury or trauma prone areas Disorganized, but relatively normal nerve twigs Often present in a fibrotic stroma related to the prior injury Morton s neuroma a painful variant of traumatic neuroma that typically arises between the 2 nd and 3 rd toes Pacinian Rare Occur on the digits at sites of trauma Clusters of enlarged pacinian corpuscles Rudimentary polydactyly (supernumerary digit) Polypoid lesion at base of 5th finger Almost always present at birth




3 13 14 SND 15 Key pathologic features: Neuromas Disorganized but relatively normal nerves or neural structures Some degenerative changes common Rudimentary polydactyly: polypoid lesion at base of 5th finger Neurofibromas: Clinical features Most common cutaneous NST Young adults, but any age M=F Polypoid, may resemble IDN & skin tags, or be deeper dermal papulonodules Most sporadic some associated with NF1 Multiple Deep locations
4 year-old-male with an elevated plaque on the neck


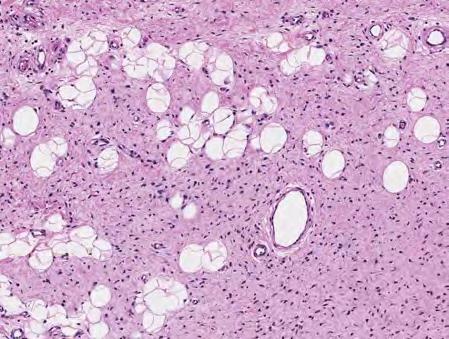
5 Diagnosis? 26 Diffuse neurofibroma: Clinical features Diffuse neurofibroma Head & neck of children & young adults Subset of pts have NF1 Plaque-like elevation of the skin Rare cases may be quite large May contain melanin pigment or mature fat and ectatic vessels in pts with NF1 28 Diffuse neurofibroma: Pathologic features Components same as localized neurofibroma, but: Poorly circumscribed, infiltrates around preexisting dermal structures, extends into subcutis tumor cells more evenly distributed compared to conventional neurofibroma Meissner body-like formations S100+, CD34 +/

,")
")


6 31 32 Diffuse neurofibroma: Differential Dermatofibrosarcoma protruberans (DFSP), particularly myxoid DFSP CD34+, S100 -, t(17;22) Dermatofibromas Collagen trapping, secondary elements, S-100- Neurotized nevi Superficial nested component, lacks NF stroma Other benign nerve sheath tumors 33 DFSP DF Myxoid DFSP 6






7 Ankle-type DF 22-year-old female with 8-year history of a slow growing mass involving the buttock & right leg Chiu H, Liao Y. N Engl J Med 2013;368:e
 Two or more cutaneous/subcutaneous neurofibromas or one plexiform neurofibroma Axillary or groin freckling Optic pathway glioma Two or more Lisch nodules (iris hamartomas) Bony")
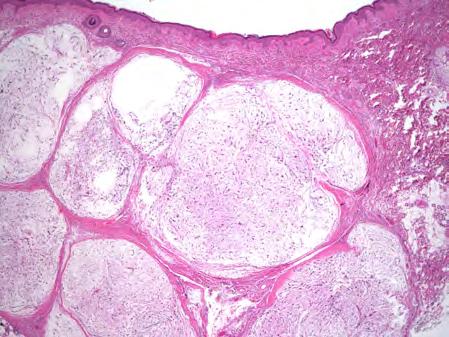
8 Diagnosis? Plexiform neurofibroma Diagnostic criteria for NF1 Six or more café au lait macules (>0.5 cm in children or >1.5cm in adults) Two or more cutaneous/subcutaneous neurofibromas or one plexiform neurofibroma Axillary or groin freckling Optic pathway glioma Two or more Lisch nodules (iris hamartomas) Bony dysplasia (sphenoid wing dysplasia, bowing of long bone +/- pseudoarthrosis) First degree relative with NF1 Plexiform neurofibroma: Clinical features Pathognomic for NF1 Develop early in life Soft tissue mass with overlying loose hyperpigmented skin (elephantiasis neuromatosa) Dx macroscopically based on imaging or gross features Large plexiform soft tissue masses with bag of worms appearance Must be distinguished from neurofibromas with merely a microscopic plexiform growth pattern, which is not associated with NF1 Significant risk of transformation to MPNST National Institutes of Health Consensus Development Conference Statement: Neurofibromatosis Arch Neurol Chicago. 1988;45: Plexiform neurofibroma: Pathologic features Components same as localized neurofibroma: Tangled, markedly expanded nerve fibers composed of spindled to comma-shaped nuclei that resemble the tumor cells of conventional neurofibroma May also have areas resembling diffuse neurofibroma



 Bilateral vestibular nerve schwannomas are a well-known pathognomonic feature of neurofibromatosis type 2 Benign tumors with simple enucleation being curative benign tumors with simple")
9 Plexiform neurofibroma: Differential Other forms of neurofibroma Plexiform schwannomas much smaller & have distinct Antoni A and Antoni B areas Often difficult, if not impossible, to make a diagnosis of plexiform neurofibroma on small skin biopsies. Diagnosis is reserved for large tumors that are suspected to be plexiform neurofibromas by gross examination or imaging Key pathologic features: Neurofibroma Bland spindled cells with wavy nuclei in collagenous to myxoid stroma May have focal atypia Variably positive for S100, EMA, CD34 Diffuse neurofibroma Infiltrative growth pattern Meissner corpuscle-like bodies Plexiform neurofibroma Plexiform growth pattern by imaging or gross pathologic examination Associated with neurofibromatosis Schwannomas: Clinical features Wide age range, no gender predisposition In cutaneous lesions, the dermis & subcutis of the head & neck & the flexor surfaces of the extremities are most commonly involved, but can arise in any superficial location Solitary, slow-growing, asymptomatic mass present for a few years Occasional patients have pain or paresthesia Schwannomas: Clinical features Most sporadic, multiple lesions should prompt evaluation for syndromic or familial causes (10%) Bilateral vestibular nerve schwannomas are a well-known pathognomonic feature of neurofibromatosis type 2 Benign tumors with simple enucleation being curative benign tumors with simple enucleation being curative Cellular schwannoma has a higher risk of local recurrence. Plexiform schwannoma can recur and be locally infiltrative and aggressive, metastasis does not occur Malignant transformation is exceptionally rare Key pathologic features: Schwannoma Fibrous capsule Hypercellular (Antoni A) and hypocellular (Antoni B) areas composed of bland spindled cells Hyalinized vessels often present May have degenerative atypia Spindled cells strongly positive for S100, but negative for CD




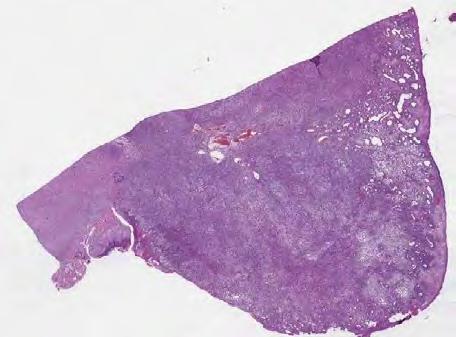
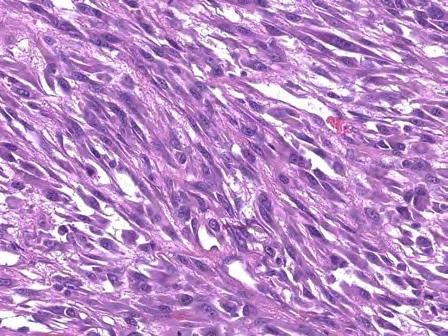
10 50-year-old male with a 5cm subcutaneous thigh mass 56 S Diagnosis? Cellular schwannoma 10

 Circumscription and encapsulation are crucial hints to its benign nature Careful sampling")
 63 64 41 year-old-male with a multinodular")
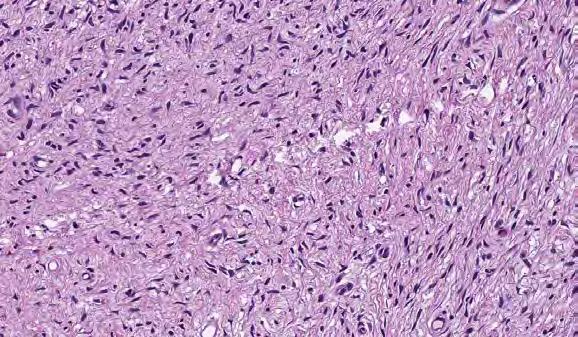
11 Pathologic features: Cellular schwannoma Composed almost exclusively of cellular Antoni A areas without Verocay body formation or nuclear palisading Arranged in long fascicles similar to the herringbone pattern seen in fibrosarcoma Loose or cystic areas account for no more than 10% of the entire tumor Most cases are deeply located, but subcutaneous cases are occasionally seen Mitotic figures are more common compared to conventional schwannoma and range from 0-4/10 per high power fields Pathologic features: Cellular schwannoma Misdiagnosed as spindle cell sarcomas (MPNST, LMS) Circumscription and encapsulation are crucial hints to its benign nature Careful sampling and searching for the paucicellular Antoni B areas of conventional schwannoma can be helpful if present Diffuse and intense S100 positivity is not a feature of typical MPNST, if seen in a biopsy of a cellular spindle cell neoplasm it strongly suggests cellular schwannoma (there are exceptions) year-old-male with a multinodular mass in left hand 66 11


12 67 68 Diagnosis? Plexiform schwannoma Pathologic features: Plexiform schwannoma Dermis or subcutaneous tissue May recur & be locally infiltrative & aggressive in some cases, metastasis does not occur Multinodular growth pattern, individual thin fibrous capsules Cytomorphology is predominantly Antoni A although cellularity is usually higher & Verocay bodies less frequently Antoni B areas with hyalinized vessels and foci of cystic change may be seen Mitotic activity is typically inconspicuous, but cases with as many as 8/10 HPF have been reported Pathologic features: Plexiform schwannoma In some cases significant nuclear atypia is also present Melanin pigment has been reported in rare cases Can be congenital and present extremely worrisome features including, infiltrative growth, high cellularity & mitotic counts (up to 31/10HPF), & lack features characteristics of conventional schwannomas occasional cases arise in patients with NF1 or NF2, but association is weak at best Must be distinguished from plexiform neurofibroma, which is diagnostic of NF1 & carries risk of malignant transformation to MPNST S100 protein strongly & diffusely positive in plexiform schwannoma, only highlights a subset of cells in plexiform neurofibroma



13 56-year-old male with a papule on the nose 74 Diagnosis? 75 Microcystic/reticular schwannoma 78 13


, deep seated, multinodular, EWSR1- NR4A3 translocation 79 80 Key pathologic features: Schwannoma Cellular schwannoma Lacks hypocellular areas May have mitotic rate up to 4/10 HPF Plexiform")
14 Pathologic features: Reticular/microcystic schwannoma Predilection for the gastrointestinal tract, dermal and subcutaneous cases have been described Well-circumscribed or multilobular, may not be entirely encapsulated Microcystic and reticular areas composed of anastomosing cords and strands of tumor cells embedded in a variably myxoid to collagenous stroma Individual cells are spindled to ovoid & may be signet-like in some cases Areas of conventional schwannoma, seen in some cases, can be a helpful diagnostic clue S100+, variably GFAP+ Differential: Reticular/microcystic schwannoma Reticulated perineurioma EMA+, S100 & GFAP-, lacks microcystic areas, acral sites favored Myoepithelial neoplasms CK & EMA, SMA, p63, GFAP, S100+ Dermal nerve sheath myxoma GFAP & S100+, variable NSE & CD57, distinctly myxoid, arises in fingers Ossifying fibromyxoid tumor Bony shell (80%), S100+ (less diffuse & intense), SOX10- Extraskeletal myxoid chondrosarcoma Only 20% S100+ (usually scattered), deep seated, multinodular, EWSR1- NR4A3 translocation Key pathologic features: Schwannoma Cellular schwannoma Lacks hypocellular areas May have mitotic rate up to 4/10 HPF Plexiform schwannoma Multinodular growth pattern Microcystic/reticular schwannoma Rare Reticulated, cord-like growth pattern 38-year-old male with dermal/ subcutaneous mass in the upper extremity 81 Diagnosis? 83 14




15 Epithelioid schwannoma Clinicopathologic features: Epithelioid schwannoma Predominantly epithelioid cells (>50%) Dermis & subcutis of the extremities <5cm, well-circumscribed, perineurium, ¼ multinodular Hyalinized vessels (95%), giant collagen rosettes may be seen Atypical variants (nuclear atypia, nuclear size variation > 3:1, mitoses >3/10HPF) fall short of criteria for dx of epithelioid MPNST, prognosis no different from typical schwannoma



 SMARCB1/INI1 loss in 50% 44-year-old")
16 Differential: Epithelioid schwannoma Long list of epithelioid neoplasms in differential Nodular or metastatic melanoma Unencapsulated, more atypia & mitotic activity, melanocytic markers+ (e.g., HMB45, MelanA, MiTF) Epithelioid MPNST Multinodular, superficial Significant atypia & mitotic activity, necrosis, myxoid stroma Lacks secondary elements of schwannoma (hyalinized vessesl, hemosiderin, foam cells) SMARCB1/INI1 loss in 50% 44-year-old female with a rapidly enlarging mass of the posterolateral neck Diagnosis? 96 16





17 Neuroblastoma-like schwannoma 98 Clinicopathologic features: Neuroblastoma-like schwannoma Tumor cells palisade around central collagenous cores mimicking rosettes of neuroblastoma Neuroblastoma deep seated tumor of infants, typically in adrenal gland Have a capsule & immunophenotype of conventional schwannoma Resembles hyalinizing spindle cell tumor with giant collagen rosettes variant of LGFMS Lacks capsule MUC4+, S100-, FUS-CREB3L fusion Key pathologic features: Schwannoma Epithelioid schwannoma Predominantly composed of epithelioid Schwann cells 25% multinodular Mitotic rate low Neuroblastoma-like schwannoma Collagenous nodules surrounded by tumor cells Also has features of conventional schwannoma Clinicopathologic features: Perineurioma Benign PNST with perineurial differentiation No association with neurofibromatosis Intraneural Females under 40 Ulnar, radial, median, peroneal and sciatic nerves most affected with deficits Imaging show segmental enlargement of involved nerve Extraneural/soft tissue (most common) Wide age range, equal sex distribution Extremities & trunk fewer cases in head & neck 10% dermal, 50% subcutaneous, 1/3 deep soft tissues Most painless, but a subset painful
, variably positive for CD34, negative for")



18 Key pathologic features: Perineurioma Positive for EMA (may be very focal), variably positive for CD34, negative for S100 Soft tissue perineurioma Swirling to fascicular growth pattern Myxoid to collagenous stroma Bland spindled cells with elongated cytoplasmic processes Intraneural perineurioma Concentric proliferation of perineurial cells around nerves imparting an onion bulb appearance 10-year-old male with a nodule on the thumb EMA Diagnosis? GLUT

19 Sclerosing perineurioma 110 Clinicopathologic features: Sclerosing perineurioma Distinct variant of perineurioma Almost exclusively occurs in the dermis & /or subcutis of acral sites of young people with a male predominance Non-acral examples have been described Benign tumors, very low risk of local recurrence Cell spindled to distinctly rounded, arranged in cords, trabeculae & chains within dense sclerotic stroma EMA & GLUT1+, 50% SMA+, CD34+/- fingerprint pattern, laminin and collagen IV surround tumor cells MUC4, desmin, S100, CK- Loss of chrm 22, rearrangement/deletions of 10q & deletions of NF2 Differential: Sclerosing perineurioma Other acral tumors Fibroma of tendon sheath Variant of fasciitis, lacks cord-like growth pattern, EMA- Superficial acral fibromyxoma Spindled to stellate, rather than epithelioid, cells, random to fascicular growth pattern, myxoid change CD34+, variable EMA, claudin Key pathologic features: Perineurioma Sclerosing perineurioma Usually acral location Spindled to epithelioid cells in cord-like pattern Dense collagenous stroma 32-year-old female with a back mass




20 EMA S Diagnosis? Hybrid schwannoma/ perineurioma Clinicopathologic features: Hybrid schwannoma/ perineurioma Young to middle-aged adults, affecting men and women equally Painless masses of the subcutis &/ or dermis and have a wide anatomic distribution Benign tumor with rare local recurrence after excision Circumscribed but unencapsulated Distinct areas of schwannoma & perineurioma Degenerative atypia & some mitotic activity Hybrid lesions are immunoreactive for S100 protein, EMA and CD34. Most tumors also express Claudin-1 The S100 protein-positive cells and EMA-positive cells are arranged in parallel layers in a laminated fashion
 Resembles perineurioma component MUC4 positive, t(7;16)")



21 Differential: Hybrid schwannoma/perineurioma Low-grade fibromyxoid sarcoma (LGFMS) Resembles perineurioma component MUC4 positive, t(7;16) by PCR or FISH Soft tissue perineurioma S100- Neurofibroma Schwann cells tend to be shorter & perineurial cells more scattered than in hybrid schwannoma-perineurioma Lacks lamellar pattern Key pathologic features: Hybrid schwannoma/ perineurioma Sclerosing perineurioma Usually acral location Spindled to epithelioid cells in cord-like pattern Dense collagenous stroma year-old male with hyperkeratotic nodule of left thigh


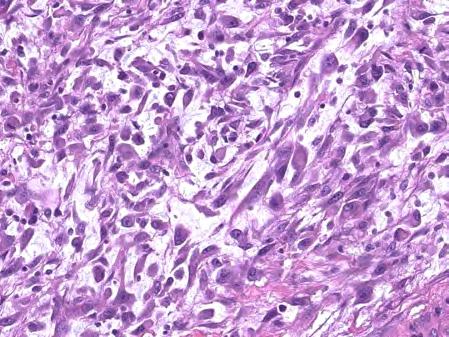
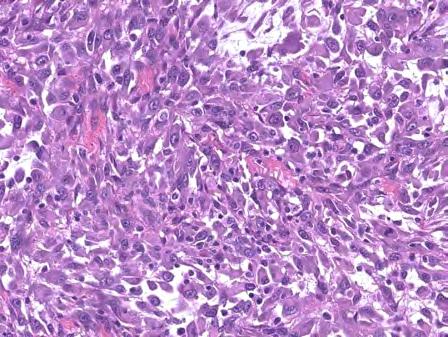
22 Diagnosis? Granular cell tumor Clinical features: Granular cell tumor Described 1926 by Abrikossoff Adults 3 rd & 4 th decades, but all age groups are affected, males=females, predilection for people of African descent Tongue one of the most common sites, a significant portion occur in the skin In 5-10% of cases lesions may be multiple Association between multiple lentigines (LEOPARD) syndrome & multiple granular cell tumors Asymptomatic or pruritic, small, cutaneous nodule averaging just over 1 cm in size Benign, simple excision, recurrence rare 129 Pathologic features: Granular cell tumor Large, polygonal cells in vague nests or trabeculae, syncytial appearance due indistinct cell borders, spindling in some cases Cytoplasm granular & eosinophilic (phagolysosomes), PAS positive, diastase resistant Pustulo-ovoid bodies of Milan: eosinophilic granule surrounded by halo Nuclei small & hyperchromatic to vesicular with nucleoli Degenerative nuclear atypia pseudoepitheliomatous hyperplasia
 No nuclear")



23 GCT - Pseudoepitheliomatous hyperplasia (PEH) Irregular rete ridges proliferating into underlying GCT/stroma often with squamous pearls *(mimics SCCa) No nuclear atypia or dyskeratosis Squamous epithelium of PEH does not extend beyond limits of GCT Pathogenesis unclear (humoral, EGF, TGFα?) Pathologic features: Granular cell tumor Dense fibrosis mimicking desmoplasia seen in malignancy Intimate association with small nerves misinterpreted as perineural invasion Strongly & diffusely positive for S100 protein, SOX10, TFE3, calretinin, & inhibin. CD68, CD163, NKI-C3, Melan-A (rare), MiTF +/- but nonspecific Desmin, cytokeratin, GFAP, & HMB S-100 protein CD






24 Differential Diagnosis Squamous cell carcinoma Adult rhabdomyoma Hibernoma Oncocytic salivary gland tumors Paraganglioma Crystal storing histiocytosis Congenital granular cell epulis 139 Rhabdomyoma Rhabdomyoma Hibernoma Oncocytoma 24

 lesions CD68 (KP1) Key pathologic features: Granular")



25 Paraganglioma Synaptophysin Crystal-storing histiocytosis GCT - Treatment Complete local excision usually curative True recurrences rare in histologically benign tumors (~ 6%) Recurrences most likely represent residual or separate (multifocal) lesions CD68 (KP1) Key pathologic features: Granular cell tumor Large polygonal cells with abundant eosinophilic granular cytoplasm Usually bland nuclear features May have overlying pseudoepitheliomatous hyperplasia S100+, SOX10+, TFE3+, calretinin+, inhibin+, PAS+ Key pathologic features: Malignant granular cell tumor Similar to conventional granular cell tumor Must have 3 of following 6 features Necrosis, spindling, high N:C ratio, vesicular nuclei with large nucleoli, increased mitotic activity (>2/10 HPF 200X fields)



26 Prognosis: Malignant granular cell tumor In the AFIP series, 39% of malignant granular cell tumors with follow-up information succumbed to disease within a median interval of 3 years Unfavorable prognostic indicators: older age, large tumor size, local recurrence, metastasis, Ki-67 labeling index greater than 10%, & p53 immunoreactivity Behavior of atypical granular cell tumor appears to be the same as conventional granular cell tumor None of the atypical AFIP cases metastasized Still recommend complete excision of atypical granular cell tumors given the limited experience with this entity Differential: Malignant granular cell tumor Other tumors with eosinophilic cytoplasm & significant atypia Melanoma positive for melanocyte specific markers (e.g., HMB45, Melan-A & MiTF) Other S100+, melanocyte marker negative tumors (NST) Myoepithelial carcinoma Variable positivity for cytokeratins, EMA, p63, calponin & smooth muscle actin Epithelioid MPNST Lobulated growth pattern, lacks granular cytoplasm Loss of INI1 staining (50% of cases) is helpful in confirming the diagnosis 41-year-old female with a multinodular mass of her right index finger



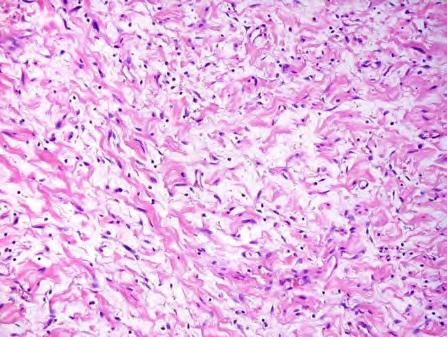
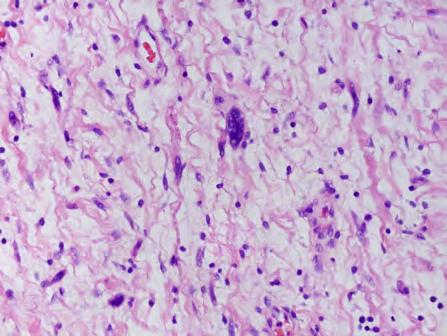
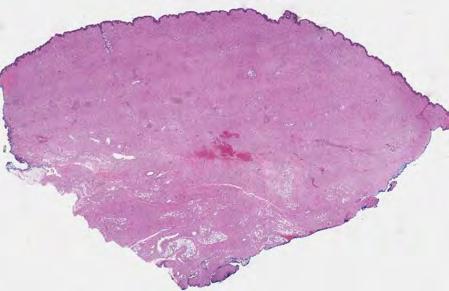
27 S-100 GFAP Diagnosis? Nerve sheath myxoma
,")
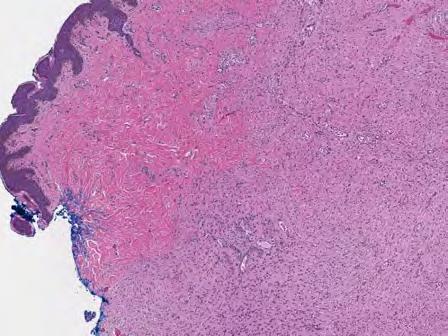
28 Clinicopathologic features: Nerve sheath myxoma Young to middle aged adults (3 rd -5 th decades), M=F Extremities (particularly hands & fingers), head & neck Flesh-colored papules or nodules Nodular growth pattern, fibrous septae Paucicellular, abundant myxoid stroma, avascular Bland spindled to stellate cells S-100 protein, GFAP and type IV collagen Extremities, local recurrence (40%-50%), complete excision 163 Differential: Nerve sheath myxoma Myxofibrosarcoma Subcutis of the extremities of older adults Atypia & pleomorphism, distinict curvilinear vasculature S100- Acral fibromyxoma Lacks multinodular growth S100- Plexiform neurofibroma with myxoid change NF1 Cells with buckled nuclei, shredded carrot collagen bundles S100 not as uniform & strong as in nerve sheath myxoma Differential: Nerve sheath myxoma Cellular neurothekeoma Nodular to nested appearance, less compact, less myxoid & not separated by distinct fibrous septations in most cases Epithelioid to spindled cells with more abundant eosinophilic cytoplasm Variably positive for non-specific markers NKI/C3, PGP9.5, CD68, MiTF & SMA Negative for S100 protein & GFAP Key pathologic features: Dermal nerve sheath myxoma Myxoid nodules separated by fibrous septae Spindled to stellate cells in myxoid stroma S100+ and GFAP+ Benign, but local recurrence rate ~40-50% A 72-year-old female presented with an ulcerated, polypoid, right upper arm tumor

29 29
 10-20% therapeutic or occupational radiation (>15 yr latency) Subset epithelioid (E-MPNST) Heterologous differentiation may")


30 S-100 Cutaneous MPNST arising in neurofibroma MPNST 5-10% of all STS 25-50% in setting of NF1 10% lifetime risk 30% in patients with symptomatic PNF Long latency (10 to 20 yrs) 10-20% therapeutic or occupational radiation (>15 yr latency) Subset epithelioid (E-MPNST) Heterologous differentiation may be seen MPNST: Clinical Features years of age (median 35) Present earlier & with larger lesions in NF1 M > F in NF1 Ratio equal in sporadic cases Enlarging mass arising from major nerve trunk Sensory & motor symptoms Sudden pain and enlargement in the setting of NF1 should prompt immediate bx Cutaneous MPNST Most often seen in association with NF1 E-MPNSTs typically not NF1 associated Nearly all arise in pre-existing diffuse NF E-MPNST may arise in schwannomas Most low-grade with spindle cell morphology 5% E-MPNST In general indolent protracted course as compared to deep seated counterparts 30
")




31 Key pathologic features: Malignant peripheral nerve sheath tumor (MPNST) Rare Often arise in association with precursor neurofibroma Conventional MPNST Fascicles of atypical hyperchromatic spindled cells Variably positive for S100 Frequent loss of histone H3K27 methylation Epithelioid MPNST Sheets of atypical epithelioid cells Strongly positive for S MPNST in NF MPNST in NF MPNST in NF 31

: 286-96.")
 HMB45, Melan-A, MiTF, tyrosinase negative No marker sensitive & specific enough to establish diagnosis with certainty S-100")
32 Cutaneous Epithelioid MPNST Epithelioid malignant cells May arise from schwannomas Infrequent associated with NF1 Most superficial LE, trunk Mostly adults but wide age range Diffuse S-100+, 2/3 loss of INI-1 Low risk for recurrence & metastases, recent series suggests aggressive potential Complete excision & LTFU Luzar B, Shanesmith R, Ramakrishnan R, Fisher C, Calonje E. Cutaneous epithelioid malignant peripheral nerve sheath tumor: a clinicopathological analysis of 11 cases. Histopathology 2016; 68(2): Epithelioid MPNST Immunohistochemistry Subset express markers of Schwann cell differentiation SOX 10 (30%) S-100 (40-50%, often focal) Epithelioid & superficial MPNSTs may be strongly & diffusely positive GFAP (30%) HMB45, Melan-A, MiTF, tyrosinase negative No marker sensitive & specific enough to establish diagnosis with certainty S-100 Differential of Superficial MPNST Melanoma CCS CBN Fibrosarcomatous DFSP Metaplastic carcinoma Myxofibrosarcoma LMS AFX Metastatic sarcoma Atypical neurofibroma Cellular schwannoma Cellular BFH 32











33 194 MPNST: Molecular & Cytogenetic Findings Many complex karyotypic abnormalities described Gains: 7p, 8q & 17q Losses: 9p, 11q, 13q, 17p Homozygous deletion of CDKN2A common Germ line mutations in NF1 Biallelic mutations of NF1 seen in high percentage of MPNSTs Recent evidence suggest stepwise molecular progression from NF to ANF to MPNST Conventional MPNST Alterations Gains: 5q22, 7p, 7q36, 17q, 18p11 Losses: 1p, 3p, 4p, 9p, 10p, 13q33, 17p, Chromothripsis: 10q, 17q, 19q, 20, 22 Neurofibroma MPNST (6 cases) Neurofibroma (3 cases) Alterations None 33

, 19 NF Gains: 5p, 8q Losses: 17q11.")


34 MPNST (6 cases) MPNST (6 cases) Neurofibroma (3 cases) Neurofibroma (3 cases) NF1 deletion SNP array: MPNST component SNP array: MPNST component NF component MPNST Gains: 5p, 8q, 11, 22 Losses: 2, 5q, 8p, 9p, 12, 15, 15, 17q11.2 (NF1), 19 MPNST Gains: 5p, 8q, 11, 22 Losses: 2, 5q, 8p, 9p, 12, 15, 15, 17q11.2 (NF1), 19 NF Gains: 5p, 8q Losses: 17q11.2 (NF1) Key Points Dermatopathology Molecular Diagnostic and Research Laboratory MPNST may superficial locations both sporadically & in patients with NF1 Must be distinguished from histologic mimics as treatment & prognosis differ Superficial MPNST generally have a more indolent & protracted course as compared to deep seated counterparts Diagnosis of conventional MPNST are relatively straightforward for the experience observer Borderline & difficult to classify lesions remain problematic for generalists & experts Rapidly evolving area with many new developments Min Wang Doru Andea 34


35 35
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis
 Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors
 The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Evening Specialty Conference Bone and Soft Tissue Pathology. Diagnostic pitfalls in bone and soft tissue pathology
 Evening Specialty Conference Bone and Soft Tissue Pathology. Case 1 Elizabeth G Demicco, MD, PhD Mount Sinai Hospital, New York Disclosure of Relevant Financial Relationships USCAP requires that all planners
Evening Specialty Conference Bone and Soft Tissue Pathology. Case 1 Elizabeth G Demicco, MD, PhD Mount Sinai Hospital, New York Disclosure of Relevant Financial Relationships USCAP requires that all planners
1/10/2018. Soft Tissue Tumors Showing Melanocytic Differentiation. Overview. Desmoplastic/ Spindle Cell Melanoma
 2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Case 1 10/2/17. Myxoid Soft Tissue Tumors & Tumor-like Lesions. Myxofibro- or Fibromyxo-?: Myxoid Soft Tissue Tumours We Are All Mixed Up About
 Myxoid Soft Tissue Tumors & Tumor-like Lesions Myxofibro- or Fibromyxo-?: Myxoid Soft Tissue Tumours We Are All Mixed Up About Rajiv M. Patel, M.D. RCPA NZ ASM 2017 (4:15-5:00pm, Saturday, 23-09-17) Heterogenous
Myxoid Soft Tissue Tumors & Tumor-like Lesions Myxofibro- or Fibromyxo-?: Myxoid Soft Tissue Tumours We Are All Mixed Up About Rajiv M. Patel, M.D. RCPA NZ ASM 2017 (4:15-5:00pm, Saturday, 23-09-17) Heterogenous
CASE REPORT Benign epithelioid peripheral nerve sheath tumour resembling schwannoma
 Malaysian J Pathol 2014; 36(3) : 217 221 CASE REPORT Benign epithelioid peripheral nerve sheath tumour resembling schwannoma Thejasvi KRISHNAMURTHY MD and SR NIVEDITHA MD, DNB Department of Pathology,
Malaysian J Pathol 2014; 36(3) : 217 221 CASE REPORT Benign epithelioid peripheral nerve sheath tumour resembling schwannoma Thejasvi KRISHNAMURTHY MD and SR NIVEDITHA MD, DNB Department of Pathology,
Special slide seminar
 Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
SOFT TISSUE TUMOR PATHOLOGY: AN UPDATE
 SOFT TISSUE TUMOR PATHOLOGY: AN UPDATE Jason L. Hornick, MD, PhD July 18, 2013 Department of Pathology Brigham and Women s Hospital Harvard Medical School Boston, MA, USA I have no disclosures. New Soft
SOFT TISSUE TUMOR PATHOLOGY: AN UPDATE Jason L. Hornick, MD, PhD July 18, 2013 Department of Pathology Brigham and Women s Hospital Harvard Medical School Boston, MA, USA I have no disclosures. New Soft
A 25 year old female with a palpable mass in the right lower quadrant of her abdomen
 May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
Newer soft tissue entities
 Newer soft tissue entities Examples among fibroblastic tumors Turku, May 6, 2010 Markku Miettinen, M.D. AFIP, Washington, DC Fibroblastic neoplasms Solitary fibrous tumor /Hemangiopericytoma Low-grade
Newer soft tissue entities Examples among fibroblastic tumors Turku, May 6, 2010 Markku Miettinen, M.D. AFIP, Washington, DC Fibroblastic neoplasms Solitary fibrous tumor /Hemangiopericytoma Low-grade
Cellular Neurothekeoma
 Cellular Neurothekeoma Scott W Binder, MD Pritzker Professor of Pathology & Dermatology Sr. Vice Chair Director, Pathology Clinical Services Chief, Dermatopathology Geffen/UCLA School of Medicine Clinical
Cellular Neurothekeoma Scott W Binder, MD Pritzker Professor of Pathology & Dermatology Sr. Vice Chair Director, Pathology Clinical Services Chief, Dermatopathology Geffen/UCLA School of Medicine Clinical
21/07/2017. Hobnail endothelial cells are not the same as epithelioid endothelial cells
 UPDATE IN CUTANEOUS VASCULAR S DERMATOPATHOLOGY SESSION BELFAST PATHOLOGY JUNE 21/2017 Dr E Calonje St John s Institute of Dermatology, London, United Kingdom THE FAMILY OF VASCULAR S WITH EPITHELIOID
UPDATE IN CUTANEOUS VASCULAR S DERMATOPATHOLOGY SESSION BELFAST PATHOLOGY JUNE 21/2017 Dr E Calonje St John s Institute of Dermatology, London, United Kingdom THE FAMILY OF VASCULAR S WITH EPITHELIOID
Essential Dermatopathology: Neoplastic American Academy of Dermatology Annual Meeting NEURAL AND SMOOTH MUSCLE NEOPLASMS
 Essential Dermatopathology: Neoplastic American Academy of Dermatology Annual Meeting NEURAL AND SMOOTH MUSCLE NEOPLASMS Kevin P. White M.D. Oregon Health and Science University Associate Professor of
Essential Dermatopathology: Neoplastic American Academy of Dermatology Annual Meeting NEURAL AND SMOOTH MUSCLE NEOPLASMS Kevin P. White M.D. Oregon Health and Science University Associate Professor of
Update on Cutaneous Mesenchymal Tumors. Thomas Brenn
 Update on Cutaneous Mesenchymal Tumors Thomas Brenn Cutaneous Mesenchymal Tumours Wide morphological and biological spectrum Myofibroblastic, smooth muscle, neural, vascular, apidocytic, undifferentiated;
Update on Cutaneous Mesenchymal Tumors Thomas Brenn Cutaneous Mesenchymal Tumours Wide morphological and biological spectrum Myofibroblastic, smooth muscle, neural, vascular, apidocytic, undifferentiated;
Spindle Cell Lesions Of The Breast. Emad Rakha Professor of Breast Pathology and Consultant Pathologist
 Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
5/10. Pathology Soft tissue tumors. Farah Bhani. Mohammed Alorjani
 5/10 Pathology Soft tissue tumors Mohammed Alorjani Farah Bhani Slides are included in this sheet. Objectives: Soft tissue tumors 1. Describe soft tissue tumors. 2. Understand the classification of soft
5/10 Pathology Soft tissue tumors Mohammed Alorjani Farah Bhani Slides are included in this sheet. Objectives: Soft tissue tumors 1. Describe soft tissue tumors. 2. Understand the classification of soft
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology
 IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
Post-test Self-assessment Cases
 Post-test Self-assessment Cases Ibrahim Khalifeh, M.D. Associate Professor Department of Pathology American University of Beirut Medical Center Beirut, Lebanon Case I History A 69 year old gentleman presenting
Post-test Self-assessment Cases Ibrahim Khalifeh, M.D. Associate Professor Department of Pathology American University of Beirut Medical Center Beirut, Lebanon Case I History A 69 year old gentleman presenting
USCAP Pediatrics Evening Subspecialty Conference 2015
 USCAP Pediatrics Evening Subspecialty Conference 2015 Sunday 22 March 2015 Alexander Lazar MD/PhD Department of Pathology S Section of Bone Soft TIssue Pathology Sarcoma Research Center The Case Patient
USCAP Pediatrics Evening Subspecialty Conference 2015 Sunday 22 March 2015 Alexander Lazar MD/PhD Department of Pathology S Section of Bone Soft TIssue Pathology Sarcoma Research Center The Case Patient
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Slide Seminar Spanish Society of Pathology
 Slide Seminar Spanish Society of Pathology John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine 1921 Original
Slide Seminar Spanish Society of Pathology John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine 1921 Original
Fun with Fat. General Rules. Case
 Fun with Fat General Rules Imaging: location (deep vs. superficial) Superficial lesions are seldom liposarcomas Deep lesions may be benign or malignant Myxoid stroma is common in benign and malignant lesions
Fun with Fat General Rules Imaging: location (deep vs. superficial) Superficial lesions are seldom liposarcomas Deep lesions may be benign or malignant Myxoid stroma is common in benign and malignant lesions
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
ACCME/Disclosures. Everything is spindle - how far can we go with limited FNA material? Everything is spindle how far can we go? Everything is spindle
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures ALK FUSION-POSITIVE MESENCHYMAL TUMORS. Tumor types with ALK rearrangements. Anaplastic Lymphoma Kinase. Jason L.
 Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Myxo-inflammatory Fibroblastic sarcoma
 AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
Classification (1) Classification (3) Classification (2) Spindle cell lesions. Spindle cell lesions of bladder (Mills et al.
 Classification (3) Classification (2) Spindle cell lesions. Spindle cell lesions of bladder (Mills et al.") Non-epithelial tumours and nonepithelial tumour-like lesions of the bladder Dr Jonathan H Shanks The Christie NHS Foundation Trust, Manchester, UK Classification (1) Myofibroblastic proliferations and
Non-epithelial tumours and nonepithelial tumour-like lesions of the bladder Dr Jonathan H Shanks The Christie NHS Foundation Trust, Manchester, UK Classification (1) Myofibroblastic proliferations and
Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology
 David M. Parham, MD Chief of Anatomic Pathology") Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology Tumors of skeletal muscle: Rhabdomyomas and rhabdomyosarcomas Embryonal muscle 2 3 4 5 6 7 8 Rhabdomyoma Benign
Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology Tumors of skeletal muscle: Rhabdomyomas and rhabdomyosarcomas Embryonal muscle 2 3 4 5 6 7 8 Rhabdomyoma Benign
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
General: Brain tumors are lesions that have mass effect distorting the normal tissue and often result in increased intracranial pressure.
 1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
Notice of Faculty Disclosure
 Mesenchymal Tumors of the Vulva: Old, New, Something(s) Different Napa Valley Conference Pathology Education Partners Inc May 15, 2018 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University,
Mesenchymal Tumors of the Vulva: Old, New, Something(s) Different Napa Valley Conference Pathology Education Partners Inc May 15, 2018 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University,
Tumors of the Central Nervous System
 Tumors of the Central Nervous System 1 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Introduction General: Brain tumors are lesions that have mass effect
Tumors of the Central Nervous System 1 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Introduction General: Brain tumors are lesions that have mass effect
Self assessment case. Dr Saleem Taibjee Dorset County Hospital, Dorchester
 Self assessment case Dr Saleem Taibjee saleemtaibjee@gmail.com Dorset County Hospital, Dorchester Clinical details 34-year-old man: Shave excision Skin tag / papilloma left thigh The best diagnosis is:
Self assessment case Dr Saleem Taibjee saleemtaibjee@gmail.com Dorset County Hospital, Dorchester Clinical details 34-year-old man: Shave excision Skin tag / papilloma left thigh The best diagnosis is:
An Overview of Genital Stromal Tumors
 An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine
An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine
Soft Tissue Perineurioma
 The Korean Journal of Pathology 2009; 43: 266-70 DOI: 10.4132/KoreanJPathol.2009.43.3.266 Soft Tissue Perineurioma - A Case Report - Jun Mo Kim Joon Hyuk Choi Department of Pathology, Yeungnam University
The Korean Journal of Pathology 2009; 43: 266-70 DOI: 10.4132/KoreanJPathol.2009.43.3.266 Soft Tissue Perineurioma - A Case Report - Jun Mo Kim Joon Hyuk Choi Department of Pathology, Yeungnam University
59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain
 December 2016 59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain Contributed by: Divya Sharma, MD. Fellow, Gastrointestinal Pathology, Department of Pathology
December 2016 59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain Contributed by: Divya Sharma, MD. Fellow, Gastrointestinal Pathology, Department of Pathology
SMOOTH MUSCLE TUMOURS
 SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
An Overview of Cutaneous Vascular Neoplasms
 An Overview of Cutaneous Vascular Neoplasms By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School
An Overview of Cutaneous Vascular Neoplasms By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on
 Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on imaging. There is no significant past medical history.
Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on imaging. There is no significant past medical history.
PLEOMORPHIC ADENOMA ( BENIGN MIXED TUMOR )
") ( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
Year 2003 Paper two: Questions supplied by Tricia
 question 43 A 42-year-old man presents with a two-year history of increasing right facial numbness. He has a history of intermittent unsteadiness, mild hearing loss and vertigo but has otherwise been well.
question 43 A 42-year-old man presents with a two-year history of increasing right facial numbness. He has a history of intermittent unsteadiness, mild hearing loss and vertigo but has otherwise been well.
Endometrial Stromal Tumors
 Endometrial Stromal Tumors WHO Categories: Endometrial Stromal Nodule (ESN) Endometrial Stromal Sarcoma, low grade (LGESS) Endometrial Stromal Sarcoma, high grade (HGESS) Undifferentiated Uterine Sarcoma
Endometrial Stromal Tumors WHO Categories: Endometrial Stromal Nodule (ESN) Endometrial Stromal Sarcoma, low grade (LGESS) Endometrial Stromal Sarcoma, high grade (HGESS) Undifferentiated Uterine Sarcoma
Slide seminar. Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana
 Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
My Journey into the World of Salivary Gland Sebaceous Neoplasms
 My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY
 PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY") SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
Disclosures. An update on ancillary techniques in the diagnosis of soft tissue tumors. Ancillary techniques. Introduction
 Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Ocular Neoplasia What s Common? What s New? Richard R Dubielzig
 Ocular Neoplasia What s Common? What s New? Richard R Dubielzig Orbit 288 6% Tumors of the globe make up 3225 out of 6110 total neoplasms = 53%. Tumors of the conjunctiva make up 1192 out of 6110 total
Ocular Neoplasia What s Common? What s New? Richard R Dubielzig Orbit 288 6% Tumors of the globe make up 3225 out of 6110 total neoplasms = 53%. Tumors of the conjunctiva make up 1192 out of 6110 total
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
3/27/2017. Disclosure of Relevant Financial Relationships
 Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Disclosure of Relevant Financial Relationships
 Neuropathology Evening Specialty Conference Disclosure of Relevant Financial Relationships The USCAP requires that anyone in a position to influence or control the content of all CME activities disclose
Neuropathology Evening Specialty Conference Disclosure of Relevant Financial Relationships The USCAP requires that anyone in a position to influence or control the content of all CME activities disclose
Journal of International Academy of Forensic Science & Pathology (JIAFP)
") Journal of International Academy of Forensic Science & Pathology (JIAFP) ISSN 2395-0722 MICROCYSTIC ADNEXAL CARCINOMA-A CASE REPORT WITH REVIEW OF LITERATURE Case Report Sulakshana M S 1,Natarajan M 2
Journal of International Academy of Forensic Science & Pathology (JIAFP) ISSN 2395-0722 MICROCYSTIC ADNEXAL CARCINOMA-A CASE REPORT WITH REVIEW OF LITERATURE Case Report Sulakshana M S 1,Natarajan M 2
Atypical Palisaded Myofibroblastoma of Lymph Node: Report of a rare case.
 ISPUB.COM The Internet Journal of Pathology Volume 10 Number 1 Atypical Palisaded Myofibroblastoma of Lymph Node: Report of a rare case. V Kinnera, R Nandyala, M Yootla, K Mandyam Citation V Kinnera, R
ISPUB.COM The Internet Journal of Pathology Volume 10 Number 1 Atypical Palisaded Myofibroblastoma of Lymph Node: Report of a rare case. V Kinnera, R Nandyala, M Yootla, K Mandyam Citation V Kinnera, R
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Nerve Sheath Myxoma Presenting as Finger Nodule in 39 year old Female
 ISPUB.COM The Internet Journal of Pathology Volume 10 Number 1 Nerve Sheath Myxoma Presenting as Finger Nodule in 39 year old Female M Hamodat, A Alhumidi Citation M Hamodat, A Alhumidi.. The Internet
ISPUB.COM The Internet Journal of Pathology Volume 10 Number 1 Nerve Sheath Myxoma Presenting as Finger Nodule in 39 year old Female M Hamodat, A Alhumidi Citation M Hamodat, A Alhumidi.. The Internet
Klinisch belang van chromosomale translocatie detectie in sarcomen
 Translocations in sarcomas Klinisch belang van chromosomale translocatie detectie in sarcomen Judith V.M.G. Bovée, M.D., Ph.D. Department of Pathology Leiden University Medical Center RNA binding DNA binding
Translocations in sarcomas Klinisch belang van chromosomale translocatie detectie in sarcomen Judith V.M.G. Bovée, M.D., Ph.D. Department of Pathology Leiden University Medical Center RNA binding DNA binding
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Tumors of Adipose Tissue Tumors Epidemiology Clinical Features. Morphology. Mature Adipocytes Separated by delicate fibrous septa
 Tumors of Adipose Tissue Lipoma Liposarcoma Most commonly happens in female The most common soft tissue tumor o Originates from matured Adipocytes Most commonly happes at the 4 th and 5 th decade of life
Tumors of Adipose Tissue Lipoma Liposarcoma Most commonly happens in female The most common soft tissue tumor o Originates from matured Adipocytes Most commonly happes at the 4 th and 5 th decade of life
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP
 What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Financial disclosures
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON
 Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON Presentation outline Background and epidemiology of sarcomas Sarcoma classification Sarcoma
Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON Presentation outline Background and epidemiology of sarcomas Sarcoma classification Sarcoma
- Selected Tumors of the Skin Appendages - Primary vs. Metastasis
 - Selected Tumors of the Skin Appendages - Primary vs. Metastasis Napa Valley 2018 Victor G. Prieto, MD, PhD Chair of Pathology UT MD Anderson Cancer Center vprieto@mdanderson.org Napa Valley in May Introduction
- Selected Tumors of the Skin Appendages - Primary vs. Metastasis Napa Valley 2018 Victor G. Prieto, MD, PhD Chair of Pathology UT MD Anderson Cancer Center vprieto@mdanderson.org Napa Valley in May Introduction
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Update On Lipomatous Tumors: Old Standbys and New Concepts
 Update On Lipomatous Tumors: Old Standbys and New Concepts John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine
Update On Lipomatous Tumors: Old Standbys and New Concepts John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine
Update in Salivary Gland Pathology. Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016
 Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Tumors of the Nervous System
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Case Presentation. Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD. Department of Pathology Jordan University Hospital Amman, Jordan
 Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
SEBACEOUS NEOPLASMS. Dr. Prachi Saraogi Clinical Fellow in Dermatology
 SEBACEOUS NEOPLASMS Dr. Prachi Saraogi Clinical Fellow in Dermatology Sebaceous neoplasms Sebaceous adenoma (Benign) Sebaceous carcinoma (Malignant) SEBACEOUS ADENOMA Benign tumours composed of incompletely
SEBACEOUS NEOPLASMS Dr. Prachi Saraogi Clinical Fellow in Dermatology Sebaceous neoplasms Sebaceous adenoma (Benign) Sebaceous carcinoma (Malignant) SEBACEOUS ADENOMA Benign tumours composed of incompletely
The Genetics of Myoepithelial Tumors: salivary glands, soft tissue and bone
 The Genetics of Myoepithelial Tumors: salivary glands, soft tissue and bone Cristina Antonescu, MD Memorial Sloan-Kettering Cancer Center, New York Nothing to declare Disclosure Spectrum of Myoepithelial
The Genetics of Myoepithelial Tumors: salivary glands, soft tissue and bone Cristina Antonescu, MD Memorial Sloan-Kettering Cancer Center, New York Nothing to declare Disclosure Spectrum of Myoepithelial
04/09/2018. Squamous Cell Neoplasia and Precursor Lesions. Agenda. Squamous Dysplasia. Squamo-proliferative lesions. Architectural features
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is:
 Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
CNS TUMORS. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
Inflammatory pseudotumor
 Inflammatory pseudotumor Inflammatory pseudotumor (IPT) Heterogeneous group of lesions of obscure etiology On physical and radiographic examination often confused with malignancy Synonyms Plasma cell granuloma
Inflammatory pseudotumor Inflammatory pseudotumor (IPT) Heterogeneous group of lesions of obscure etiology On physical and radiographic examination often confused with malignancy Synonyms Plasma cell granuloma
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Disclosures. An update on ancillary techniques in the diagnosis of soft tissue tumors. Ancillary techniques. Introduction
 Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Diagnostic Approach to Soft Tissue Tumors
 SECTION 2 Diagnostic Approach to Soft Tissue Tumors Overview Biopsy and Resection of Soft Tissue Tumors 20 Clinical Approach Age- and Location-Based Approach to Diagnosis 24 Histologic Approach Pattern-Based
SECTION 2 Diagnostic Approach to Soft Tissue Tumors Overview Biopsy and Resection of Soft Tissue Tumors 20 Clinical Approach Age- and Location-Based Approach to Diagnosis 24 Histologic Approach Pattern-Based
Case Report Intraneural malignant perineurioma: a case report and review of literature
 Int J Clin Exp Pathol 2014;7(7):4503-4507 www.ijcep.com /ISSN:1936-2625/IJCEP0000923 Case Report Intraneural malignant perineurioma: a case report and review of literature Yong Huang 1, Hongwei Li 1, Zhengwen
Int J Clin Exp Pathol 2014;7(7):4503-4507 www.ijcep.com /ISSN:1936-2625/IJCEP0000923 Case Report Intraneural malignant perineurioma: a case report and review of literature Yong Huang 1, Hongwei Li 1, Zhengwen
Case 27 Male 42. Painless, static, well-circumscribed, subcutaneous nodule right lower leg,?lipoma. The best diagnosis is:
 Case 27 Male 42. Painless, static, well-circumscribed, subcutaneous nodule right lower leg,?lipoma. The best diagnosis is: A. Angiosarcoma B. Haemangiopericytoma C.Myopericytoma D.Myofibroma E. Angioleiomyoma
Case 27 Male 42. Painless, static, well-circumscribed, subcutaneous nodule right lower leg,?lipoma. The best diagnosis is: A. Angiosarcoma B. Haemangiopericytoma C.Myopericytoma D.Myofibroma E. Angioleiomyoma
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial