Comparing Current Options in Radiation Therapy. Howard M. Sandler, MD Ronald H. Bloom Family Chair in Cancer Therapeutics Cedars-Sinai Medical Center
|
|
|
- Trevor Wilkerson
- 6 years ago
- Views:
Transcription
1 Comparing Current Options in Radiation Therapy Howard M. Sandler, MD Ronald H. Bloom Family Chair in Cancer Therapeutics Cedars-Sinai Medical Center
 Cooperberg JCO 28:1117,")
2 Time Trends for Radiotherapy (and other treatments) Cooperberg JCO 28:1117, 2010
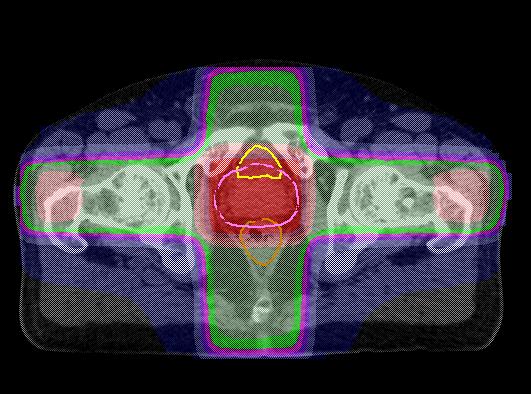
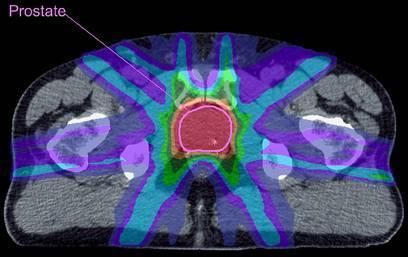
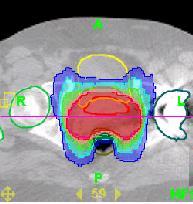
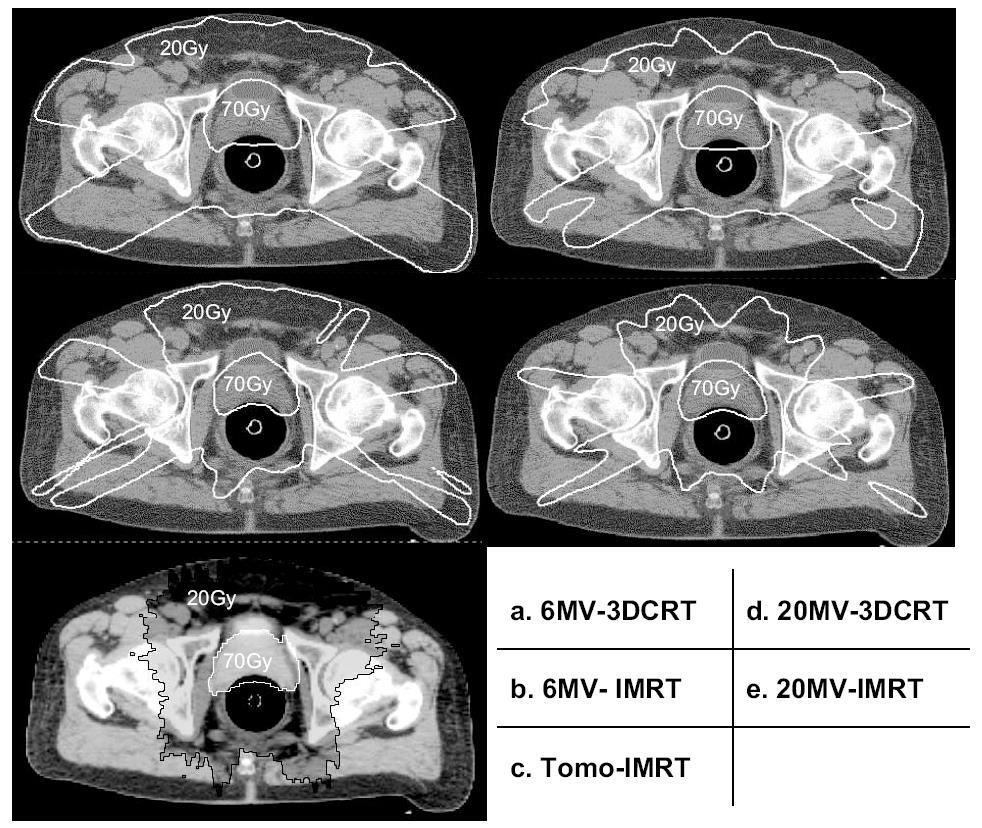
3 Dose Distribution 3D-CRT IMRT
4

5
6 Institution UM Rectal Constraint <20% over 70 Gy, <50% over 50 Gy Beaumont <40% over 70, <25% over 75.6 Wash U <17% over 65, <35% over 40 Peter Mac <25% over 70, <30% over 60, <50% over 50 Duke <10% over 75, <17% over 65, <40% over 40 Cedars <20% over 65, <50% over 45 ROC <20% over 65, <45% over 40 MCW <20% over 70, <45% over 50 Mayo < 5% over 75, <15% over 70, <25% over 65, <35% over 60, <50% over 50 MSKCC <53% over 47, <30% over 75.6, max dose 85.5 FCCC <17% over 65, <35% over 40

7 Rectal DVH Example 40 Gy < 35% < 40% < 45% 45 Gy < 50% 50 Gy < 45% < 50% 65 Gy < 17% < 20% < 25% 70 Gy < 15% < 20% 75 Gy < 5% < 10% < 20% Lower Dose Constraint High Dose Constraint
8 Dose volume analysis of grade 2+ late GI toxicity on RTOG 0126 after highdose 3DCRT or IMRT 3DCRT 55.8 to P+pSV, then 23.4 to P only IMRT 79.2 to P+pSV in single plan Data examined: Gr 2+ late rectal toxicity and D eff to rectum 708 available patients (473 3DCRT) 3DCRT 25% IMRT 21% No differences once corrected for D eff No impact on rectal toxicity related to doses <60 Gy

9 ALWAYS insert new slide when adding new text Adding a text box will result in bullets not formatting correctly All text should be single-spaced Always use Lucida Sans font Upper and lower case point size of text should be 14 point 9
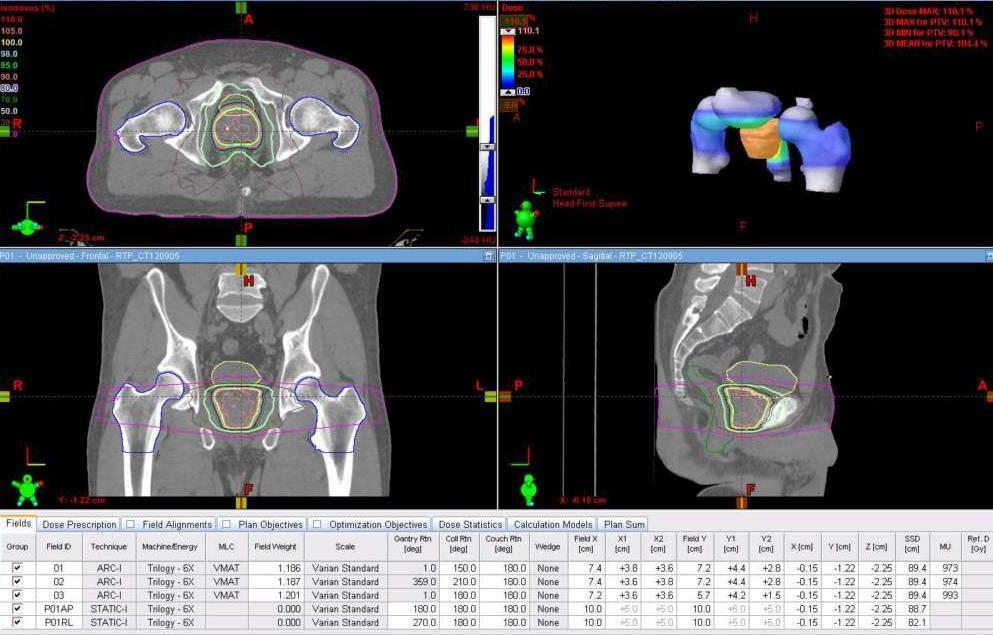
10 VMAT vs. Fixed Field IMRT Treatment time shorter, more rapid Low dose is spread more widely VMAT = 360 correlated fixed fields Anecdotal cases: 7 field prostate IMRT: 898 MU (128 MU/field) 2 arc VMAT: 904 MU (452 MU/arc) 10
11 RART: Single arc asymmetry
12 RART: Single arc asymmetry PTV CTV Bladder Rectum Femoral Heads Penile Bulb
13 Combined single arc vs Integrated two arc plan Combined single arcs: Plans obtained for half-rx dose for each of: Two arcs, one CW, one CCW Arithmetic dose sum to obtain full RX plan Optimization for the arcs obtained sequentially Integral plan using two arcs, same CW and CCW specifications as for the above single arc plans Optimization for the arcs obtained concurrently
14 Combined single arc vs Integrated two arc plan Combined, Max 70.4, 527MU Integral, Max 70Gy, 580MU
15 Combined single arc vs Integrated two arc plan

16 7 field IMRT vs 2 arc RART IMRT, Max 72, 915MU RART, Max 70Gy, 580MU
17 7 field IMRT vs 2 arc RART RA IM CTV PTV Bladder RA IM RA Rectum IM Penile Bulb Femoral Heads

18 Implanted Fiducials


19 AC Wireless Magnetic Tracking 1.8 mm Calypso System 8 mm


20 Implanted Transponders

21 AC Wireless Magnetic Tracking May treat through array Measurements at 10 Hz Sub-mm resolution Real-time tracking during treatment Potential for fast correction

22 Intra-Fraction Motion Study Subset of 3 patients out of 42 Supine, knees raised Set to isocenter with Calypso (+/- 0.5 mm) Time to start of fraction (1-2 min) Tracked for 8 10 minutes at 10 Hz

23 Position (mm) Data Patient 1 IS AP LR

24 Position (mm) Data Patient 2 IS AP LR

25 Position (mm) Data Patient 3 1 IS AP LR

26 26
27 Implanted Fiducials Have become standard care Potential to reduce margins required for set up uncertainty Potential to decrease target misses Real time tracking important Reimbursable as part of IGRT
28
29 29
30 Free-Breathing CT DIBH CT
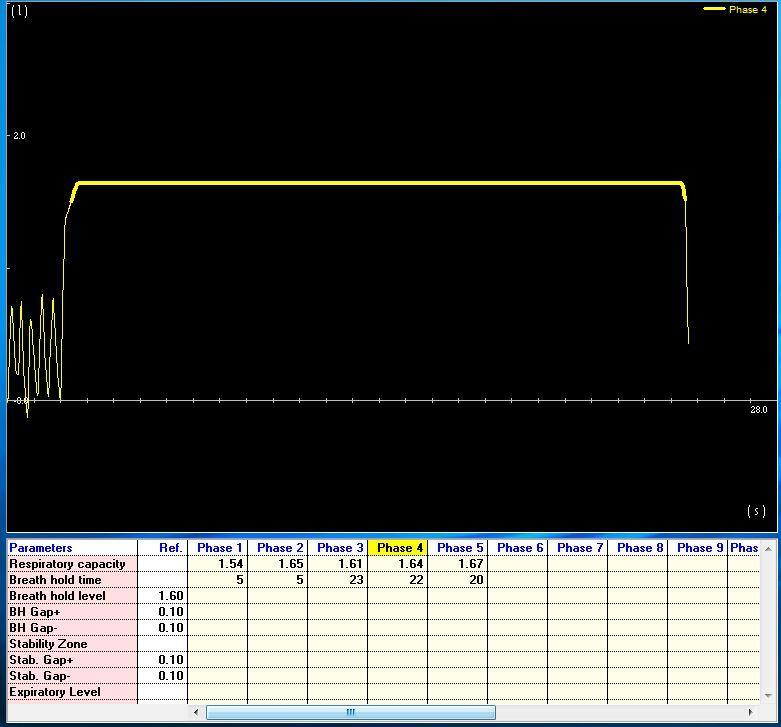
31


32 Fuse DIBH CT to FB CT according to Breast location 3cm 3cm FB heart DIBH heart
33 Institution Dose/Fractionation, LHRH? UM FCCC Wash U Wisconsin Duke Jefferson ROC MCW Mayo MSKCC 1.85 to 77.7, No 2 to 80, No 1.8 to 75.6, No 2.5 to 70, No 2 to 76, +/- based on potency 1.8 to 79.2, No 1.8 to 75.6, Yes 1.8 to 75.6, No 1.8 to 75.6, No 1.8 to 86.4, No
34 Pelvic LN? RTOG 9413
35
36
37 α/β ratio: Tumor & Early ~ 10 Late ~ 1-3 Dose-Response Relationship: Early vs. Late responding tissues
38 α and β S = e -αd-βd^2
39 Biologically Effective Dose (BED) BED Total Dose x Relative Effectiveness E /α = n * d x [1+ d/(α/β)] n=# fx s Late: α/β ~ 3 d=dose/fx Early: α/β ~ 10
40 RTOG 0415 Schema 73.8 Gy/41 Fx T1c-2a GS <7 PSA <10 70 Gy/28 Fx n=800 Endpoint is 5 Year BFFF Non-inferiority margin 7% (Control 85%, Exp 78%)
41 Clinical Trial Michigan-led, multicenter, hypofractionation trial for low-intermediate prostate cancer. 41
42 Clinical Trial Needed? Stereotactic body radiotherapy for primary management of early-stage, low- to intermediate-risk prostate cancer: report of the American Society for Therapeutic Radiology and Oncology Emerging Technology Committee The authors of this report believe further clinical trials addressing the uncertainties in the clinical implementation of this new approach to prostate cancer treatment should be conducted. The technique holds sufficient promise to warrant further investigation. Buyyounouski IJROBP 76:1297,
43 Primary Objectives To evaluate the safety of the proposed hypofractionation regimen and to compare it to that expected from conventional treatment. To assess the frequency of required interventions based on real-time prostate translations and rotations to verify that the proposed planning target volume (PTV) margins and action level are appropriate and practical.
44 Eligibility Prostate cancer, Gleason score 7 If Gleason 7, then <50% of biopsy cores must be positive If Gleason score <7 then there is no limit on the percentage of biopsy cores involved PSA 15 ng/ml prior to start of therapy if Gleason 6 and 10 ng/ml prior to start of therapy if Gleason 7 T1c-T2b No hormone use Exclusion Criteria: Implants in the pelvic region that contain metal Body habitus not conducive to tracking with Calypso Beacons AUA score > 15 (alpha blockers allowed) CT, MRI, or ultrasound estimate of prostate volume > 100 grams 44
45 UMHS SBRT Protocol Instead of 39 fractions of 2 Gy to 78 Gy over 8 weeks, 5 fractions of 7.4 Gy to 37 Gy over 2.5 weeks. This is predicted to have toxicity similar to the 80 Gy regimen but with efficacy in the vicinity of 94 Gy Using Calypso guidance will use smaller margins then previously reported
46 46



47 Treatment Success % PSA Progression Free INTERMEDIATE RISK RESULTS Weighted /18/2013 BJU Int, 2012, Vol. 109(Supp 1) EBRT Years from Treatment Brachy Prostate Cancer Results Study Group Numbers within symbols refer to references Prostate Cancer Center of Seattle EBRT & Seeds Surgery 40 + Robot RP Seeds + ADT EBRT & Seeds Hypo EBRT Brachy Seeds Alone Surgery EBRT CRYO HIFU HDR EBRT, Seeds + ADT Protons 47
48 RT Technology Tomotherapy IMRT device Cyberknife Stereotactic device Protons Carbon Ion


49

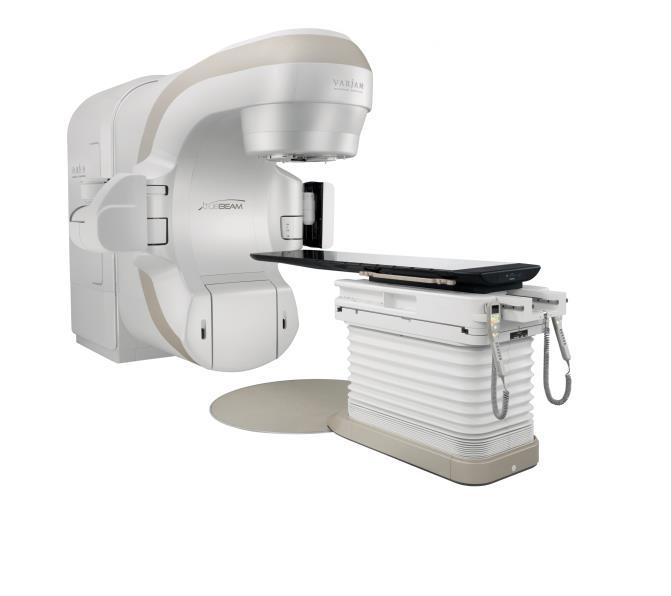

50 Current Linear Accelerators Varian TrueBeam Siemens Elekta Versa HD

51 Tomotherapy
52
53


54 SHARP 40 pt phase I/II No grade 3 toxicity Madsen IJROBP 67:1099,2007

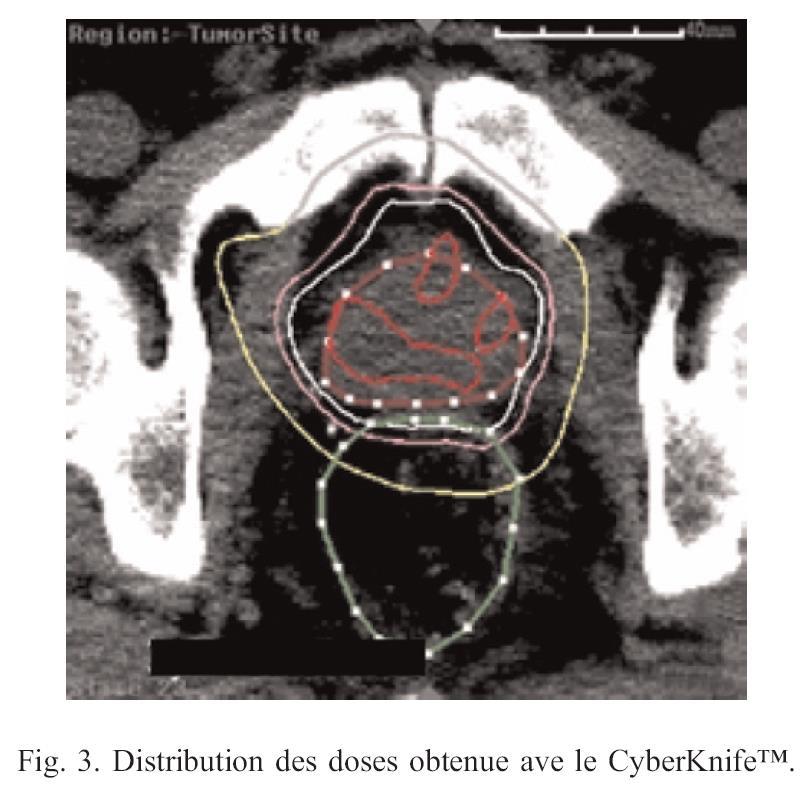
55 Cyberknife Hannoun-Levi Cancer/Radiothérapie 11:476,2007

56 Cyberknife Near real time target tracking (q30-90 sec) Take 40 min for prostate rx 7.25 Gy/fx to Gy Pawlicki Med Dosim 32:71,2007
57 Particle Therapy Protons Bragg peak gives finite range Photons (X-rays) Penetrate deeply, attenuate gradually
58
59 proton

60 The Bragg Peak and Protons Benefits Bragg Peak Potential to spare more healthy tissue Potential to bring higher dose to targets at depth Can be added together to produce a flat top SOBP Charged particles Can be deflected and focused by magnets quickly
61 Proton Therapy Potential Benefits May allow delivery of more dose to the tumor for same dose to normal tissue Possible increased tumor control Reduced occurrence of treatment-related tissue damage Early toxicity Second cancers: especially important for pediatric cases Less toxicity when RT and chemo are combined
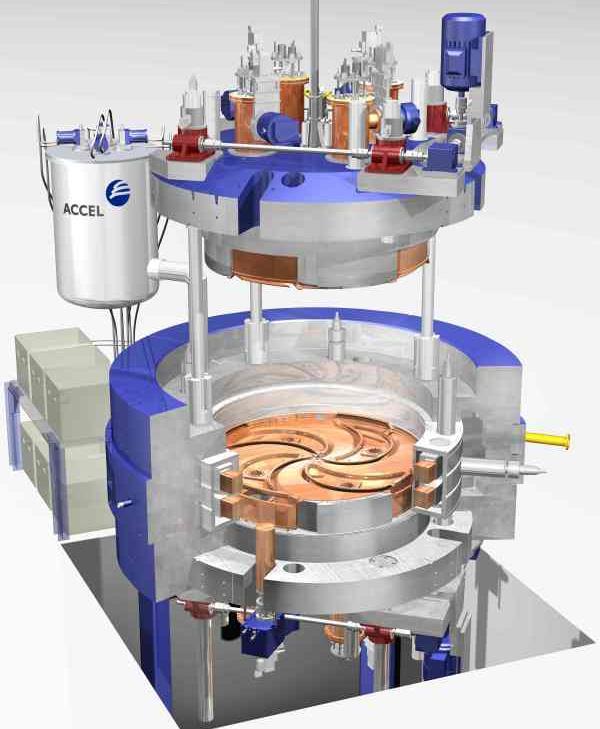
62 Superconducting Cyclotron Diagram Superconducting Coil


63 Gantry and Treatment Table Treatment Room Gantry at Manufacturer


64 System Layout I. S.C. Cyclotron Single Gantry Room Section III. Gantry Rooms Eye Treatment Room II. Energy Selection System/Beam Transfer Line Rinecker Proton Therapy Center (Munich)
65 Proton Therapy Sites Active Loma Linda MPRI (Indiana U) MD Anderson Univ Florida (Jacksonville) MGH Oklahoma City Univ Penn New Jersey/Princeton Hampton Univ/VA Chicagoland Planned Scripps Seattle (Cancer Alliance) Wash U Maryland Rutgers New York Emory UT Southwestern Mayo/Rochester+Phoenix Johns Hopkins/Washington Flint
66 What is the evidence in favor of proton therapy? Reviewed 36 published studies (only 2 phase III) Chordomas, ocular tumors, prostate, head and neck cancer Brada, et al JCO 2007
67 Protons and Prostate? The phenomenon continues among men diagnosed with prostate cancer that began with the opening in 1990 of Loma Linda University Medical Center s proton facility. Prostate patients top all other cancerous conditions treated with proton therapy between the five U.S. operating protons centers. About 8,000 men have been treated with outstanding outcomes reported in the last 17 years... A vast majority of men self-referred themselves to proton treatment centers around the country after learning about the advantages of the proton beam that minimizes serious side effects and helps to maintain a patient s quality-of-life.
68 Evidence Review The claim by proton therapy supporters that protons are the treatment of choice for chordoma and chondrosarcoma is no longer tenable based on the currently available evidence. there are currently no studies demonstrating improved tumor control or survival in the treatment of localized prostate cancer with protons compared with best available photon RT. In addition, there is no clear evidence that high-dose proton boost is associated with less toxicity than the toxicity expected with photons. Proton and other particle therapies need to be explored as potentially more effective and less toxic RT techniques. Brada, et al JCO 2007

69 P r o s t a t e IMRT Protons Trofimov, et al. IJROBP 2007
70 Cost Effective? Markov model (91.8 Gy proton vs. 81 Gy IMRT) $63,500/QALY for 70 yo, $55,700 for 60 yo. Even when based on the unproven assumption that protons will permit a 10-Gy escalation of prostate dose compared with IMRT photons, proton beam therapy is not cost effective for most patients with prostate cancer using the commonly accepted standard of $50,000/QALY. Consideration should be given to limiting the number of proton facilities to allow comprehensive evaluation of this modality. Konski, et al. JCO 2007
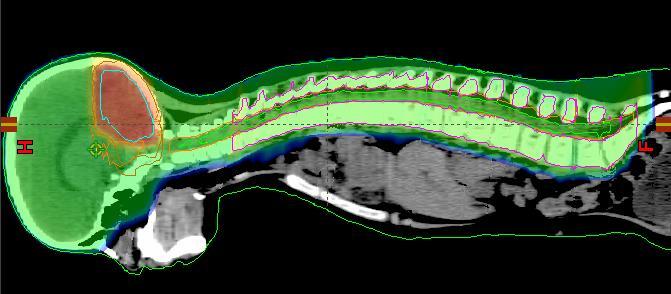
71 Protons for medulloblastoma
72
73 Carbon Ion Higher LET?Fewer fractions needed
74 Proton Summary Proton therapy has the potential to benefit a subset of cancer patients, especially children. Benefit for prostate cancer not established. More research is needed to define what patients will benefit from proton technology Given the cost benefit ratio, regional centers should be considered IMRT has reduced toxicity of high dose RT
75
76 Why doesn t someone do a study?? Finally, someone is MGH/UPenn Efficacy of PBT vs. IMRT Compare the reduction in mean EPIC bowel scores for men with low or lowintermediate risk PCa treated with PBT versus IMRT at 24 months following radiation 461 patients Study to be reported in
77

78 Endorectal Balloons 78

79 Summary Dose sparing during 3DCRT, less evidence for benefit with IMRT Use with care or omit for patients with pre-existing anorectal disease Reproducibility? 79

80 Spacers? Hyaluronan gel Wilder IJROBP 77:824,


81 Spacers? PEG-based hydrogels Song ASTRO Abs
82 Institution IGRT? UM EM Transponder >> fiducials with CBCT > CBCT alone Beaumont Wash U Peter Mac Duke Cedars ROC MCW Mayo Adaptive with CBCT alone EM Transponder, MV with fiducials, kv and fiducials EM Transponder, CBCT and fiducials, EM Transponder (preferred), CBCT EM Transponder, CBCT and fiducials, CBCT without fiducials kv and fiducials MSKCC FCCC EM Transponder, kv and fiducials EM Transponder, fiducials +/- kv or CBCT

83 Institution UM Beaumont Wash U Peter Mac Duke Cedars ROC MCW Mayo MSKCC FCCC CTV-PTV Margin (mm) 5 everywhere Adaptive based on wk 1 CBCT 5 everywhere 7 post, 10 elsewhere 5 everywhere 5 everywhere 4 posteriorly, 6 inf, 5 elsewhere 3 post, 5 elsewhere 4-5 post, 5-7 laterally, 5 elsewhere 6 everywhere 3-5 mm post, 6-8 elsewhere
84 Current Practice Intermediate risk patient: Insert Calypso Beacons, if the patient is a candidate CT simulation 7+ days after insertion (MR before Beacons if necessary) Contour, verify Beacon location with dosimetry PTV margin generally 5 mm Plan, usually RapidArc with two arcs Deliver RT with 3 mm action threshold 84
IMRT RTOG Definitive IMRT for Low Risk Prostate Cancer. All about dose and dose matters, probably Although hormones may matter
 Definitive for Low Risk Prostate Cancer Howard Sandler, MD, MS Bloom Family Chair in Cancer Therapeutics Cedar-Sinai Medical Center All about dose and dose matters, probably Although hormones may matter
Definitive for Low Risk Prostate Cancer Howard Sandler, MD, MS Bloom Family Chair in Cancer Therapeutics Cedar-Sinai Medical Center All about dose and dose matters, probably Although hormones may matter
Advances in external beam radiotherapy
 International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT
 Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments
 Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Andrew K. Lee, MD, MPH Associate Professor Department tof fradiation Oncology M.D. Anderson Cancer Center
 Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor Department tof fradiation Oncology M.D. Anderson Cancer Center Seungtaek Choi, MD Assistant Professor Department tof fradiation
Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor Department tof fradiation Oncology M.D. Anderson Cancer Center Seungtaek Choi, MD Assistant Professor Department tof fradiation
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery
 Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy?
 Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
New Technologies for the Radiotherapy of Prostate Cancer
 Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division
 IMRT / Tomo / VMAT / Cyberknife / HDR Brachytherapy: Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division Should Choices be Based on Dosimetric and
IMRT / Tomo / VMAT / Cyberknife / HDR Brachytherapy: Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division Should Choices be Based on Dosimetric and
Vaginal Sparing with Volumetric Modulated Arc Therapy (VMAT) for Rectal Cancer. Scott Boulet BSc, RT(T)
 for Rectal Cancer. Scott Boulet BSc, RT(T)") Vaginal Sparing with Volumetric Modulated Arc Therapy (VMAT) for Rectal Cancer Scott Boulet BSc, RT(T) Outline Background Objectives Design Results Discussion Conclusion Acknowledgements Questions Background
Vaginal Sparing with Volumetric Modulated Arc Therapy (VMAT) for Rectal Cancer Scott Boulet BSc, RT(T) Outline Background Objectives Design Results Discussion Conclusion Acknowledgements Questions Background
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR
 Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Stereotactic ablative body radiation for prostate cancer SABR
 Stereotactic ablative body radiation for prostate cancer SABR John Armstrong. Sinead Callinan. Luke Rock. Beacon Hospital, Dublin, Ireland Low- Intermediate Risk Prostate Comparing treatment choices IMRT
Stereotactic ablative body radiation for prostate cancer SABR John Armstrong. Sinead Callinan. Luke Rock. Beacon Hospital, Dublin, Ireland Low- Intermediate Risk Prostate Comparing treatment choices IMRT
1. CyberKnife Centers of San Diego, CA 2. Coast Urology La Jolla, CA 3. Sletten Cancer Center Great Falls, MT
 Donald B. Fuller, M.D. 1, John Naitoh, M.D. 2, Mark Reilly, M.D. 3, Chad Lee, Ph.D 1. 1. CyberKnife Centers of San Diego, CA 2. Coast Urology La Jolla, CA 3. Sletten Cancer Center Great Falls, MT Typically,
Donald B. Fuller, M.D. 1, John Naitoh, M.D. 2, Mark Reilly, M.D. 3, Chad Lee, Ph.D 1. 1. CyberKnife Centers of San Diego, CA 2. Coast Urology La Jolla, CA 3. Sletten Cancer Center Great Falls, MT Typically,
CyberKnife SBRT for Prostate Cancer
 CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
Disclosures. Proton therapy advantages. Why are comparing therapies difficult? Proton Therapy for Low Risk Prostate Cancer
 Proton Therapy for Low Risk Prostate Cancer Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments Andrew K. Lee, MD, MPH Associate Professor
Proton Therapy for Low Risk Prostate Cancer Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments Andrew K. Lee, MD, MPH Associate Professor
External Beam Radiation Therapy for Low/Intermediate Risk Prostate Cancer
 External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
Prostate Cancer. 3DCRT vs IMRT : Hasan Murshed
 Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Innovazioni tecnologiche in Radioterapia" Sergio Fersino Radioterapia Oncologica
 Innovazioni tecnologiche in Radioterapia" Sergio Fersino Radioterapia Oncologica 2014 HYPOFRACTIONATION & PROSTATE CANCER HYPOFRACTIONATION & PROSTATE CANCER: TECHNOLOGY: HIGH CONFORMAL DOSE & IMAGING
Innovazioni tecnologiche in Radioterapia" Sergio Fersino Radioterapia Oncologica 2014 HYPOFRACTIONATION & PROSTATE CANCER HYPOFRACTIONATION & PROSTATE CANCER: TECHNOLOGY: HIGH CONFORMAL DOSE & IMAGING
ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER
 ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER Bro. Dr. Collie Miller IARC/WHO Based on trends in the incidence of cancer, the International Agency for Research on Cancer (IARC) and WHO
ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER Bro. Dr. Collie Miller IARC/WHO Based on trends in the incidence of cancer, the International Agency for Research on Cancer (IARC) and WHO
FROM ICARO1 TO ICARO2: THE MEDICAL PHYSICS PERSPECTIVE. Geoffrey S. Ibbott, Ph.D. June 20, 2017
 FROM ICARO1 TO ICARO2: THE MEDICAL PHYSICS PERSPECTIVE Geoffrey S. Ibbott, Ph.D. June 20, 2017 1 DISCLOSURES My institution holds Strategic Partnership Research Agreements with Varian, Elekta, and Philips
FROM ICARO1 TO ICARO2: THE MEDICAL PHYSICS PERSPECTIVE Geoffrey S. Ibbott, Ph.D. June 20, 2017 1 DISCLOSURES My institution holds Strategic Partnership Research Agreements with Varian, Elekta, and Philips
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER
 PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
Particle (proton) Therapy Randomized trials vs. Prospective registry. Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology
 Therapy Randomized trials vs. Prospective registry. Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology") Particle (proton) Therapy Randomized trials vs. Prospective registry Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Should we do randomized trials? Are randomized trials needed
Particle (proton) Therapy Randomized trials vs. Prospective registry Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Should we do randomized trials? Are randomized trials needed
IMRT for Prostate Cancer
 IMRT for Cancer All patients are simulated in the supine position. Reproducibility is achieved using a custom alpha cradle cast that extends from the mid-back to mid-thigh. The feet are positioned in a
IMRT for Cancer All patients are simulated in the supine position. Reproducibility is achieved using a custom alpha cradle cast that extends from the mid-back to mid-thigh. The feet are positioned in a
Subject: Image-Guided Radiation Therapy
 04-77260-19 Original Effective Date: 02/15/10 Reviewed: 01/25/18 Revised: 01/01/19 Subject: Image-Guided Radiation Therapy THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
04-77260-19 Original Effective Date: 02/15/10 Reviewed: 01/25/18 Revised: 01/01/19 Subject: Image-Guided Radiation Therapy THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer
 Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer Ciro Franzese, G D Agostino, E Clerici, E Villa, A Tozzi, T Comito, C Iftode, AM Ascolese, F De Rose, S Pentimalli,
Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer Ciro Franzese, G D Agostino, E Clerici, E Villa, A Tozzi, T Comito, C Iftode, AM Ascolese, F De Rose, S Pentimalli,
Changing Paradigms in Radiotherapy
 Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
Motion gating and tracking techniques: overview and recent developments
 Motion gating and tracking techniques: overview and recent developments Gig S Mageras, PhD, FAAPM Department of Medical Physics Memorial Sloan Kettering Cancer Center, New York MSK/gsm 15-Jun-2018 1 Disclosure
Motion gating and tracking techniques: overview and recent developments Gig S Mageras, PhD, FAAPM Department of Medical Physics Memorial Sloan Kettering Cancer Center, New York MSK/gsm 15-Jun-2018 1 Disclosure
NEWER RADIATION (3 D -CRT, IMRT, IGRT) TECHNIQUES FOR CERVICAL CANCERS (COMMON PELVIC TUMORS)
 TECHNIQUES FOR CERVICAL CANCERS (COMMON PELVIC TUMORS)") NEWER RADIATION (3 D -CRT, IMRT, IGRT) TECHNIQUES FOR CERVICAL CANCERS (COMMON PELVIC TUMORS) Umesh Mahantshetty, DMRT, MD, DNBR Associate Professor, Radiation Oncology Convener: Urology Disease Management
NEWER RADIATION (3 D -CRT, IMRT, IGRT) TECHNIQUES FOR CERVICAL CANCERS (COMMON PELVIC TUMORS) Umesh Mahantshetty, DMRT, MD, DNBR Associate Professor, Radiation Oncology Convener: Urology Disease Management
Intensity-Modulated and Image- Guided Radiation Treatment. Outline. Conformal Radiation Treatment
 Intensity-Modulated and Image- Guided Radiation Treatment J. Daniel Bourland, PhD Professor Departments of Radiation Oncology, Physics, and Biomedical Engineering Wake Forest University School of Medicine
Intensity-Modulated and Image- Guided Radiation Treatment J. Daniel Bourland, PhD Professor Departments of Radiation Oncology, Physics, and Biomedical Engineering Wake Forest University School of Medicine
Clinical Implementation of a New Ultrasound Guidance System. Vikren Sarkar Bill Salter Martin Szegedi
 Clinical Implementation of a New Ultrasound Guidance System Vikren Sarkar Bill Salter Martin Szegedi Disclosure The University of Utah has research agreements with Elekta Agenda Historical Review Trans-Abdominal
Clinical Implementation of a New Ultrasound Guidance System Vikren Sarkar Bill Salter Martin Szegedi Disclosure The University of Utah has research agreements with Elekta Agenda Historical Review Trans-Abdominal
Helical Tomotherapy Experience. TomoTherapy Whole Brain Head & Neck Prostate Lung Summary. HI-ART TomoTherapy System. HI-ART TomoTherapy System
 The Challenges Associated with Differential Dose Delivery using IMRT Chester Ramsey, Ph.D. Director of Medical Physics Thompson Cancer Center Knoxville, Tennessee, U.S.A Collaborators Chester Ramsey, Ph.D.
The Challenges Associated with Differential Dose Delivery using IMRT Chester Ramsey, Ph.D. Director of Medical Physics Thompson Cancer Center Knoxville, Tennessee, U.S.A Collaborators Chester Ramsey, Ph.D.
Proton Therapy for Prostate Cancer. Andrew K. Lee, MD, MPH Director Proton Therapy Center
 Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Director Proton Therapy Center Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments
Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Director Proton Therapy Center Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments
Radiation Therapy: From Fallacy to Science
 27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
Radiation Therapy 2013 The Role of Protons. Bob Gaston, D.O.
 Radiation Therapy 2013 The Role of Protons Bob Gaston, D.O. Disclosures Oklahoma ProCure Treatment Center Radiation Medicine Associates Goal of Radiation Therapy Increase the Therapeutic Ratio Therapeutic
Radiation Therapy 2013 The Role of Protons Bob Gaston, D.O. Disclosures Oklahoma ProCure Treatment Center Radiation Medicine Associates Goal of Radiation Therapy Increase the Therapeutic Ratio Therapeutic
Neoplasie prostatiche Radioterapia: le nuove strategie
 Neoplasie prostatiche Radioterapia: le nuove strategie Dr. PL Losardo U.O.C di Radioterapia Azienda Ospedaliero-Universitaria di Parma Parma, 19.5.2015 VS Very Low risk Low risk Intermediate risk High
Neoplasie prostatiche Radioterapia: le nuove strategie Dr. PL Losardo U.O.C di Radioterapia Azienda Ospedaliero-Universitaria di Parma Parma, 19.5.2015 VS Very Low risk Low risk Intermediate risk High
Results of Stereotactic radiotherapy for Stage I and II NSCLC Is There a Need for Image Guidance?
 Results of Stereotactic radiotherapy for Stage I and II NSCLC Is There a Need for Image Guidance? Frank Zimmermann Institute of Radiation Oncolgy University Clinic Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch
Results of Stereotactic radiotherapy for Stage I and II NSCLC Is There a Need for Image Guidance? Frank Zimmermann Institute of Radiation Oncolgy University Clinic Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch
The Wellness Community Prostate Cancer
 The Wellness Community Prostate Cancer Large Discussion Group July 28, 2010 Kevin Chaffee Knowledge Navigator Tonight s Agenda Review peer reviewed informagon on proton therapy for prostate cancer treatment
The Wellness Community Prostate Cancer Large Discussion Group July 28, 2010 Kevin Chaffee Knowledge Navigator Tonight s Agenda Review peer reviewed informagon on proton therapy for prostate cancer treatment
Therapeutic Medical Physics. Stephen J. Amadon Jr., Ph.D., DABR
 Therapeutic Medical Physics Stephen J. Amadon Jr., Ph.D., DABR Outline 1. Why physicists are needed in medicine 2. Branches of medical physics 3. Physics in Radiation Oncology 4. Treatment types and Treatment
Therapeutic Medical Physics Stephen J. Amadon Jr., Ph.D., DABR Outline 1. Why physicists are needed in medicine 2. Branches of medical physics 3. Physics in Radiation Oncology 4. Treatment types and Treatment
Radiotherapy Advances
 Radiotherapy Advances Not Radiotherapy Principles IMRT IGRT Image Fusion Planning Introduction IMRT = Intensity Modulated RadioTherapy Restriction: IMRT with photon beams IMRT: Highly conformal technique
Radiotherapy Advances Not Radiotherapy Principles IMRT IGRT Image Fusion Planning Introduction IMRT = Intensity Modulated RadioTherapy Restriction: IMRT with photon beams IMRT: Highly conformal technique
The role of Radiation Oncologist: Hi-tech treatments for liver metastases
 The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
EORTC Member Facility Questionnaire
 Page 1 of 9 EORTC Member Facility Questionnaire I. Administrative Data Name of person submitting this questionnaire Email address Function Phone Institution Address City Post code Country EORTC No Enter
Page 1 of 9 EORTC Member Facility Questionnaire I. Administrative Data Name of person submitting this questionnaire Email address Function Phone Institution Address City Post code Country EORTC No Enter
Management. Localized Prostate Cancer. Andrew K. Lee, MD, MPH Associate Professor M.D. Anderson Cancer Center
 Management of Localized Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor M.D. Anderson Cancer Center Disclosure Information Ad Andrew K. KLee Dr. Lee has indicated no financial relationships,
Management of Localized Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor M.D. Anderson Cancer Center Disclosure Information Ad Andrew K. KLee Dr. Lee has indicated no financial relationships,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer
 A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
Imaging of Scattered Radiation for Real Time Tracking of Tumor Motion During Lung SBRT
 Imaging of Scattered Radiation for Real Time Tracking of Tumor Motion During Lung SBRT April 25 nd, 2015 Lung Cancer Lung cancer is the most lethal cancer: Over 224,000 new diagnoses in the U.S. predicted
Imaging of Scattered Radiation for Real Time Tracking of Tumor Motion During Lung SBRT April 25 nd, 2015 Lung Cancer Lung cancer is the most lethal cancer: Over 224,000 new diagnoses in the U.S. predicted
Treatment Planning & IGRT Credentialing for NRG SBRT Trials
 Treatment Planning & IGRT Credentialing for NRG SBRT Trials Hania Al Hallaq, Ph.D. Department of Radiation & Cellular Oncology The University of Chicago Learning Objectives Explain rationale behind credentialing
Treatment Planning & IGRT Credentialing for NRG SBRT Trials Hania Al Hallaq, Ph.D. Department of Radiation & Cellular Oncology The University of Chicago Learning Objectives Explain rationale behind credentialing
Radiation Therapy for Prostate Cancer. Resident Dept of Urology General Surgery Grand Round November 24, 2008
 Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
HALF. Who gets radiotherapy? Who gets radiotherapy? Half of all cancer patients get radiotherapy. By 1899 X rays were being used for cancer therapy
 The Physical and Biological Basis of By 1899 X rays were being used for cancer therapy David J. Brenner, PhD, DSc Center for Radiological Research Department of Radiation Oncology Columbia University Medical
The Physical and Biological Basis of By 1899 X rays were being used for cancer therapy David J. Brenner, PhD, DSc Center for Radiological Research Department of Radiation Oncology Columbia University Medical
3/22/2014. Goals of this Presentation: in 15 min & 5 min Q & A. Radiotherapy for. Localized Prostate Cancer: What is New in 2014?
 3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
MRI Applications in Radiation Oncology:
 MRI Applications in Radiation Oncology: Physician s Perspective Jeff Olsen, MD Department of Radiation Oncology Washington University, St. Louis, MO Disclosures Washington University has research and service
MRI Applications in Radiation Oncology: Physician s Perspective Jeff Olsen, MD Department of Radiation Oncology Washington University, St. Louis, MO Disclosures Washington University has research and service
Has radiotherapy the potential being focal?
 Has radiotherapy the potential being focal? György Kovács & Alexander Schlaefer* Interdisciplinary Brachytherapy Unit and *Institute of Robotics and Cognitive Systems, University of Lübeck / 1 100% 90%
Has radiotherapy the potential being focal? György Kovács & Alexander Schlaefer* Interdisciplinary Brachytherapy Unit and *Institute of Robotics and Cognitive Systems, University of Lübeck / 1 100% 90%
The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation. Roberto Alonzi Mount Vernon Cancer Centre
 The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation Roberto Alonzi Mount Vernon Cancer Centre Overview Introduction and rationale for focused dose escalation
The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation Roberto Alonzi Mount Vernon Cancer Centre Overview Introduction and rationale for focused dose escalation
Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT)
") Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT) The Institute for Clinical and Economic Review (ICER) has published appraisals on multiple management options for clinically-localized,
Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT) The Institute for Clinical and Economic Review (ICER) has published appraisals on multiple management options for clinically-localized,
Salvage HDR Brachytherapy. Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK
 Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Future Directions in Prostate Cancer: The Case for Protons. John J. Coen, MD Helen & Harry Gray Cancer Center
 Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
Status of H 1 and C 12
 Status of H 1 and C 12 Herman Suit No Conflict of Interest 1 Goal of a New Treatment Modality Tumor Control Probability or No in Complication Rate 2 Truism No Advantage to: any Patient for any Radiation
Status of H 1 and C 12 Herman Suit No Conflict of Interest 1 Goal of a New Treatment Modality Tumor Control Probability or No in Complication Rate 2 Truism No Advantage to: any Patient for any Radiation
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer
 for Gynaecological Cancer") Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Demands and Perspectives of Hadron Therapy
 Demands and Perspectives of Hadron Therapy Alexander Lin, M.D. Assistant Professor University of Pennsylvania Direction of Operations Roberts Proton Therapy Center Disclosures Teva Pharmaceuticals: Advisory
Demands and Perspectives of Hadron Therapy Alexander Lin, M.D. Assistant Professor University of Pennsylvania Direction of Operations Roberts Proton Therapy Center Disclosures Teva Pharmaceuticals: Advisory
An Update on Radiation Therapy for Prostate Cancer
 An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
Implementation of advanced RT Techniques
 Implementation of advanced RT Techniques Tibor Major, PhD National Institute of Oncology Budapest, Hungary 2. Kongres radiološke tehnologije, Vukovar, 23-25. September 2016. Current RT equipments at NIO,
Implementation of advanced RT Techniques Tibor Major, PhD National Institute of Oncology Budapest, Hungary 2. Kongres radiološke tehnologije, Vukovar, 23-25. September 2016. Current RT equipments at NIO,
Implementing SBRT Protocols: A NRG CIRO Perspective. Ying Xiao, Ph.D. What is NRG Oncology?
 Implementing SBRT Protocols: A NRG CIRO Perspective Ying Xiao, Ph.D. What is NRG Oncology? One of five new NCI-supported National Clinical Trials Network (NCTN) groups. NCTN officially started March 1,
Implementing SBRT Protocols: A NRG CIRO Perspective Ying Xiao, Ph.D. What is NRG Oncology? One of five new NCI-supported National Clinical Trials Network (NCTN) groups. NCTN officially started March 1,
8/3/2016. Outline. Site Specific IGRT Considerations for Clinical Imaging Protocols. Krishni Wijesooriya, PhD University of Virginia
 Site Specific IGRT Considerations for Clinical Imaging Protocols Krishni Wijesooriya, PhD University of Virginia Outline Image registration accuracies for different modalities What imaging modality best
Site Specific IGRT Considerations for Clinical Imaging Protocols Krishni Wijesooriya, PhD University of Virginia Outline Image registration accuracies for different modalities What imaging modality best
Integrating the Radixact into a Highly Comprehensive Center
 Integrating the Radixact into a Highly Comprehensive Center Alonso N. Gutiérrez, PhD, MBA ASTRO Meeting 2018 Disclosures An honorarium is provided by Accuray for this presentation (donated) Accuray and
Integrating the Radixact into a Highly Comprehensive Center Alonso N. Gutiérrez, PhD, MBA ASTRO Meeting 2018 Disclosures An honorarium is provided by Accuray for this presentation (donated) Accuray and
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
A Thesis. entitled. based on CBCT Data Dose Calculation. Sukhdeep Kaur Gill. Master of Science Degree in Biomedical Science
 A Thesis entitled A Study of Evaluation of Optimal PTV Margins for Patients Receiving Prostate IGRT based on CBCT Data Dose Calculation by Sukhdeep Kaur Gill Submitted to the Graduate Faculty as partial
A Thesis entitled A Study of Evaluation of Optimal PTV Margins for Patients Receiving Prostate IGRT based on CBCT Data Dose Calculation by Sukhdeep Kaur Gill Submitted to the Graduate Faculty as partial
Pancreatic Cancer and Radiation Therapy
 Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
PACE Study. Hypofractionation 17/12/2014. Traditional Model of Fractionation 200 Response. What s the fraction sensitivity of prostate cancer?
 0 0 17/12/2014 2 Outline of today s talk PACE Study Background rationale for PACE? Dr Nicholas van As A bit about technology. What is PACE? How can I get involved? London: 1 December 2014 250 Hypofractionation
0 0 17/12/2014 2 Outline of today s talk PACE Study Background rationale for PACE? Dr Nicholas van As A bit about technology. What is PACE? How can I get involved? London: 1 December 2014 250 Hypofractionation
8/1/2017. Clinical Indications and Applications of Realtime MRI-Guided Radiotherapy
 Clinical Indications and Applications of Realtime MRI-Guided Radiotherapy Michael F Bassetti MD PhD Assistant Professor, Department of Human Oncology University of Wisconsin, Madison. Carbone Cancer Center
Clinical Indications and Applications of Realtime MRI-Guided Radiotherapy Michael F Bassetti MD PhD Assistant Professor, Department of Human Oncology University of Wisconsin, Madison. Carbone Cancer Center
Potential conflicts-of-interest. Respiratory Gated and Four-Dimensional Tumor Tracking Radiotherapy. Educational objectives. Overview.
 Respiratory Gated and Four-Dimensional Tumor Tracking Radiotherapy Potential conflicts-of-interest I am PI of a sponsored research agreement between Stanford University and Varian Medical Systems P Keall
Respiratory Gated and Four-Dimensional Tumor Tracking Radiotherapy Potential conflicts-of-interest I am PI of a sponsored research agreement between Stanford University and Varian Medical Systems P Keall
Use of SpaceOAR for Prostate Radiotherapy Preliminary Report
 Date: April 28 2016 Use of SpaceOAR for Prostate Radiotherapy Preliminary Report Soon N. Huh (ho), Ph.D., DABR University Of Florida Health Proton Therapy Institute (UFHPTI) Presented to the Florida Chapter
Date: April 28 2016 Use of SpaceOAR for Prostate Radiotherapy Preliminary Report Soon N. Huh (ho), Ph.D., DABR University Of Florida Health Proton Therapy Institute (UFHPTI) Presented to the Florida Chapter
Stereotaxy. Outlines. Establishing SBRT Program: Physics & Dosimetry. SBRT - Simulation. Body Localizer. Sim. Sim. Sim. Stereotaxy?
 Establishing SBRT Program: Physics & Dosimetry Lu Wang, Ph.D. Radiation Oncology Department Fox Chase Cancer Center Outlines Illustrate the difference between SBRT vs. CRT Introduce the major procedures
Establishing SBRT Program: Physics & Dosimetry Lu Wang, Ph.D. Radiation Oncology Department Fox Chase Cancer Center Outlines Illustrate the difference between SBRT vs. CRT Introduce the major procedures
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924
 EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
Rectal dose and toxicity dosimetric evaluation for various beam arrangements using pencil beam scanning protons with and without rectal spacers
 Rectal dose and toxicity dosimetric evaluation for various beam arrangements using pencil beam scanning protons with and without rectal spacers 2015 MAC-AAPM Annual Meeting, Baltimore, MD Heeteak Chung,
Rectal dose and toxicity dosimetric evaluation for various beam arrangements using pencil beam scanning protons with and without rectal spacers 2015 MAC-AAPM Annual Meeting, Baltimore, MD Heeteak Chung,
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
Sarcoma and Radiation Therapy. Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington
 Sarcoma and Radiation Therapy Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington Objective: Helping you make informed decisions Introduction Process Radiation
Sarcoma and Radiation Therapy Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington Objective: Helping you make informed decisions Introduction Process Radiation
8/2/2012. Transitioning from 3D IMRT to 4D IMRT and the Role of Image Guidance. Part II: Thoracic. Peter Balter, Ph.D.
 8/2/2012 Transitioning from 3D IMRT to 4D IMRT and the Role of Image Guidance Part II: Thoracic Peter Balter, Ph.D. Disclosure Dr. Balter is Physics PI on a trial comparing Cyberknife based SBRT with surgery,
8/2/2012 Transitioning from 3D IMRT to 4D IMRT and the Role of Image Guidance Part II: Thoracic Peter Balter, Ph.D. Disclosure Dr. Balter is Physics PI on a trial comparing Cyberknife based SBRT with surgery,
IGRT Solution for the Living Patient and the Dynamic Treatment Problem
 IGRT Solution for the Living Patient and the Dynamic Treatment Problem Lei Dong, Ph.D. Associate Professor Dept. of Radiation Physics University of Texas M. D. Anderson Cancer Center Houston, Texas Learning
IGRT Solution for the Living Patient and the Dynamic Treatment Problem Lei Dong, Ph.D. Associate Professor Dept. of Radiation Physics University of Texas M. D. Anderson Cancer Center Houston, Texas Learning
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE
 CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
IMRT - the physician s eye-view. Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia
 IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
Clinical experience with TomoDirect System Tangential Mode
 Breast Cancer Clinical experience with TomoDirect System Tangential Mode European Institute of Oncology Milan, Italy Disclosure & Disclaimer An honorarium is provided by Accuray for this presentation The
Breast Cancer Clinical experience with TomoDirect System Tangential Mode European Institute of Oncology Milan, Italy Disclosure & Disclaimer An honorarium is provided by Accuray for this presentation The
Overview of Advanced Techniques in Radiation Therapy
 Overview of Advanced Techniques in Radiation Therapy Jacob (Jake) Van Dyk Manager, Physics & Engineering, LRCP Professor, UWO University of Western Ontario Acknowledgements Glenn Bauman Jerry Battista
Overview of Advanced Techniques in Radiation Therapy Jacob (Jake) Van Dyk Manager, Physics & Engineering, LRCP Professor, UWO University of Western Ontario Acknowledgements Glenn Bauman Jerry Battista
Credentialing for the Use of IGRT in Clinical Trials
 Credentialing for the Use of IGRT in Clinical Trials James M. Galvin, DSc Thomas Jefferson University Hospital Jefferson Medical College Philadelphia, PA and The Radiation Therapy Oncology Group RADIATION
Credentialing for the Use of IGRT in Clinical Trials James M. Galvin, DSc Thomas Jefferson University Hospital Jefferson Medical College Philadelphia, PA and The Radiation Therapy Oncology Group RADIATION
2/14/09. Why Discuss this topic? Managing Local Recurrences after Radiation Failure. PROSTATE CANCER Second Treatment
 Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
CLINICAL TRIALS Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Partial Breast Irradiation using adaptive MRgRT
 Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
MRI Based treatment planning for with focus on prostate cancer. Xinglei Shen, MD Department of Radiation Oncology KUMC
 MRI Based treatment planning for with focus on prostate cancer Xinglei Shen, MD Department of Radiation Oncology KUMC Overview How magnetic resonance imaging works (very simple version) Indications for
MRI Based treatment planning for with focus on prostate cancer Xinglei Shen, MD Department of Radiation Oncology KUMC Overview How magnetic resonance imaging works (very simple version) Indications for
Embracing Technology & Timing of Salvage Hormones
 Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October
Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October
Questions may be submitted anytime during the presentation.
 Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Department of Radiotherapy & Nuclear Medicine, National Cancer Institute, Cairo University, Cairo, Egypt.
 Original article Res. Oncol. Vol. 12, No. 1, Jun. 2016:10-14 Dosimetric comparison of 3D conformal conventional radiotherapy versus intensity-modulated radiation therapy both in conventional and high dose
Original article Res. Oncol. Vol. 12, No. 1, Jun. 2016:10-14 Dosimetric comparison of 3D conformal conventional radiotherapy versus intensity-modulated radiation therapy both in conventional and high dose
Implementing New Technologies for Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy
 Implementing New Technologies for Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Implementation of radiosurgery and SBRT requires a fundamentally sound approach Errors don t blur out
Implementing New Technologies for Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Implementation of radiosurgery and SBRT requires a fundamentally sound approach Errors don t blur out
Illawarra Cancer Care Centre
 The Audience Who? No apologies! Radiation Oncologists State of Mind Our business Our business is medical Our records are medical records Our information system is electronic medical record Primacy of our
The Audience Who? No apologies! Radiation Oncologists State of Mind Our business Our business is medical Our records are medical records Our information system is electronic medical record Primacy of our
Research Article Implant R100 Predicts Rectal Bleeding in Prostate Cancer Patients Treated with IG-IMRT to 45 Gy and Pd-103 Implant
 Radiotherapy, Article ID 130652, 6 pages http://dx.doi.org/10.1155/2014/130652 Research Article Implant R100 Predicts Rectal Bleeding in Prostate Cancer Patients Treated with IG-IMRT to 45 Gy and Pd-103
Radiotherapy, Article ID 130652, 6 pages http://dx.doi.org/10.1155/2014/130652 Research Article Implant R100 Predicts Rectal Bleeding in Prostate Cancer Patients Treated with IG-IMRT to 45 Gy and Pd-103
Current and Emerging Standards in Radiation Therapy for Prostate Cancer
 Current and Emerging Standards in Radiation Therapy for Prostate Cancer Amandeep R. Mahal, BS, and James B. Yu, MD, MHS Abstract Improved radiation technology has allowed physicians to precisely target
Current and Emerging Standards in Radiation Therapy for Prostate Cancer Amandeep R. Mahal, BS, and James B. Yu, MD, MHS Abstract Improved radiation technology has allowed physicians to precisely target
Treatment Efficiency and Optimization of Patient Care with IBA ProteusOne
 Treatment Efficiency and Optimization of Patient Care with IBA ProteusOne Terry Wu, Ph.D. Chief Physicist, Radiation Oncology Department Willis-Knighton Cancer Center/Proton Therapy Center Shreveport,
Treatment Efficiency and Optimization of Patient Care with IBA ProteusOne Terry Wu, Ph.D. Chief Physicist, Radiation Oncology Department Willis-Knighton Cancer Center/Proton Therapy Center Shreveport,
SBRT in early stage NSCLC
 SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia
 Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies
 UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies A SINGLE INSTITUTION S EXPERIENCE IN DEVELOPING A PURPOSEFUL AND EFFICIENT OFF-LINE TECHNIQUE FOR ADAPTIVE RADIOTHERAPY IN A CLINICAL ENVIRONMENT A Research
UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies A SINGLE INSTITUTION S EXPERIENCE IN DEVELOPING A PURPOSEFUL AND EFFICIENT OFF-LINE TECHNIQUE FOR ADAPTIVE RADIOTHERAPY IN A CLINICAL ENVIRONMENT A Research
Future of Radiation Therapy
 Future of Radiation Therapy JP Morgan Healthcare Conference January 12, 2016 Deepak Khuntia, MD, VP of Medical Affairs Patrick Kupelian, MD, VP of Clinical Affairs Cancer as a cause of death CANCER TREATMENT
Future of Radiation Therapy JP Morgan Healthcare Conference January 12, 2016 Deepak Khuntia, MD, VP of Medical Affairs Patrick Kupelian, MD, VP of Clinical Affairs Cancer as a cause of death CANCER TREATMENT