Neuronal and Mixed Neuronal- Glial and Embryonal Tumors
|
|
|
- Noreen Ball
- 6 years ago
- Views:
Transcription
 Pathologist-in-Chief Children s Hospital Los Angeles Associate Professor (Clinical Scholar) & Vice")
1 Neuronal and Mixed Neuronal- Glial and Embryonal Tumors Alexander R. Judkins, MD, FRCP (Edin) Pathologist-in-Chief Children s Hospital Los Angeles Associate Professor (Clinical Scholar) & Vice Chair Department of Pathology, Keck School of Medicine of USC
2 Considerations Complex Topic Many of these tumors have been re-classified at least once or are new entities Tumors that are commoner in, but not exclusive to pediatric populations Tumors that more often than not demonstrate divergent differentiation (glial and neuronal, +/- other) Brain Tumor Classifications Virchow, 1867 Brain tumors arise from brain tissue Golgi, 1875 Brain tumors contain cells that have the features of cells in the brain Cushing & Bailey, Studied series of 414 cases Grouped by length of survival Detailed clinical descriptions Identified 13 categories of brain tumors based on demonstration of cell type
3 Considerations The First Brain Tumor Classification, circa 1926 A Few Things Have changed Clinically Refined surgical techniques, intra- post-operative care Diagnostic and interventional imaging Non-surgical treatment modalities Scientifically More detailed understanding of CNS development IHC, EM, FISH, SNPs, gene arrays Genomics

4 Considerations

5 Considerations Most of These Are Either: Tumors that have histologic evidence of neuronal differentiation Exclusively neuronal neoplasms are relatively rare (gangliocytoma, central neurocytoma) Tumors that show evidence of bi- or polyphenotypic differentiation Histologically these are usually comprised of small undifferentiated cells Evidence for neuronal differentiation based on special techniques Electron microscopy (EM) detection of ultrastructural features Immunohistochemical (IHC) detection of protein expression FISH, gene expression, CNV or sequencing based detection of molecular genetic changes associated with neuronal phenotypes Neuronal Histologic Features
6 Considerations Synaptophysin Structural & Functional Elements of Neurons NeuN Neurofilament (NFP)
 that is associated with astrocytic differentiation are used to define")
7 Considerations Glial Differentiation Glial derived cell types Astrocytes Oligodendrocytes Ependyma and Choroid Plexus More prominent epithelial features Histologically defined IHC Astrocytes (GFAP) Oligodendrocytes Practically Speaking While more complex glial differentiation exists, histology and a single IHC marker (GFAP) that is associated with astrocytic differentiation are used to define
8 Considerations Neuronal Differentiation Histology: what is a neoplastic neuron? Neurons present where none would normally be found Neurons that are irregularly arranged Neurons that are cytologically atypical (binucleation) Ganglioid cells (small, less prominent nucleoli, inconspicuous Nissl substance) IHC to identify biphenotypic differentiation in an embryonal tumor Neuronal Structures Indirect histologic evidence Homer Wright rosettes (MB, PNET) Neurocytic rosettes (Neurocytoma, Pineocytoma) Schematics from:
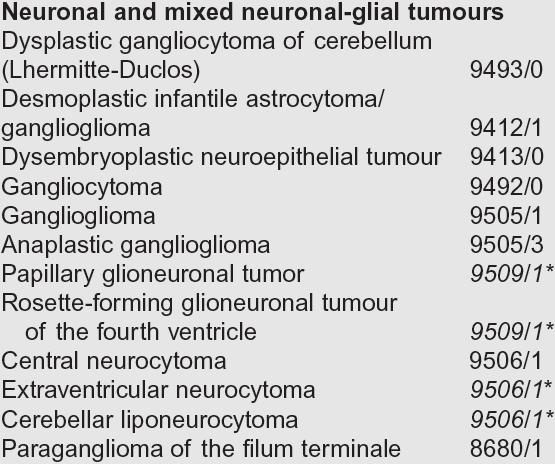
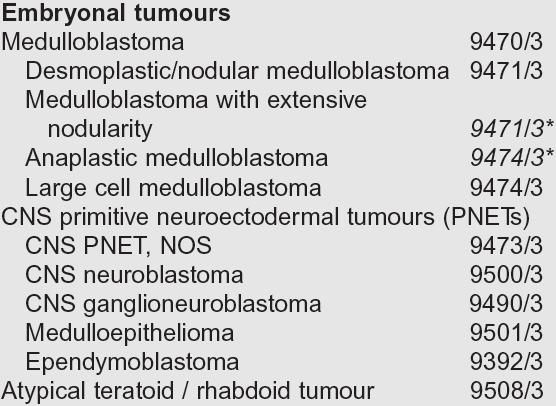
9 Archetypal Tumors Neuronal & Mixed Neuronal-Glial (mostly biphenotypic tumors) Ganglioglioma Gangliocytoma Dysembryoplastic neuroepithelial tumor (DNET) Central Neurocytoma Embryonal (tumors w/ bi- or polyphenotypic differentiation) Medulloblastoma Most common embryonal tumor (90%) 20% of all pediatric brain tumors CNS Primitive neuroectodermal tumor (CNS PNET) Relationship to MB Specific histologic patterns or subtypes of PNET Atypical Teratoid / Rhabdoid Tumor (AT/RT)
10 Neuronal & Mixed Neuronal-Glial Ganglioglioma, Dysembryoplastic Neuroepithelial Tumor (DNET), Central Neurocytoma
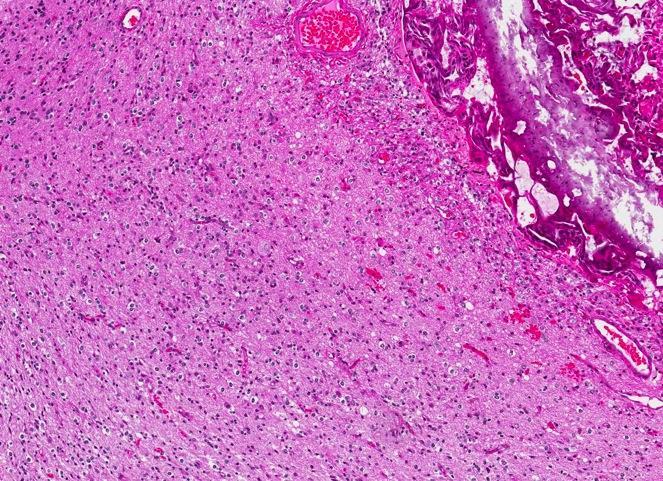
11 Ganglioglioma Terminology Definition Tumor containing welldifferentiated neoplastic neurons (ganglion cells) with or without (gangliocytoma) associated neoplastic glial cells Clinical Issues Epidemiology Age (diagnosis) years Gender (M:F) 1.1:1 to 1.9:1 Presentation Seizures 15-25% of surgery for seizures Most common tumors associated with temporal lobe epilepsy Length of duration of seizures prior to diagnosis correlates with location: Cerebrum (6-25 years) Brainstem / spinal cord (~1.5 years) Mass effect for brainstem and spinal cord Prognosis Benign tumors (WHO grade I) with exception of small number that present with or develop anaplastic features in glial component (anaplastic ganglioglioma, WHO grade III) Surgical resection is typically curative

12 Ganglioglioma Image Findings General Features Location Supratentorial, particularly temporal lobe (>80%) Anywhere along neuraxis Morphology Cortically based Most commonly cystic with mural nodule Can be solid Typically enhancing


13 Ganglioglioma Macroscopic Features Pale - gray Firm - rubbery Variably gritty due to focal calcification Presence of hemorrhage or necrosis can be seen in anaplastic lesions

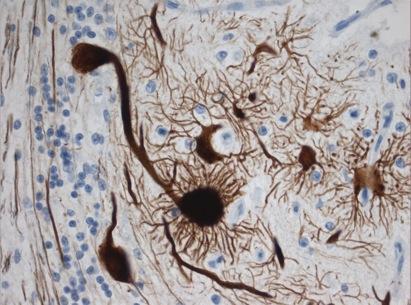
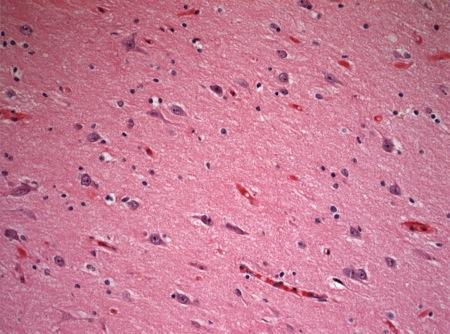
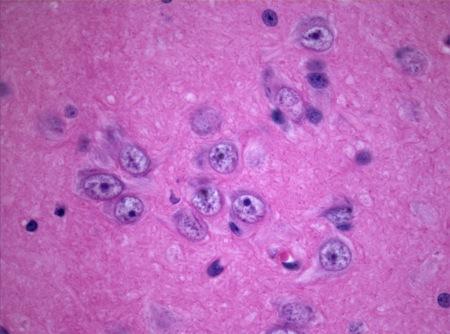
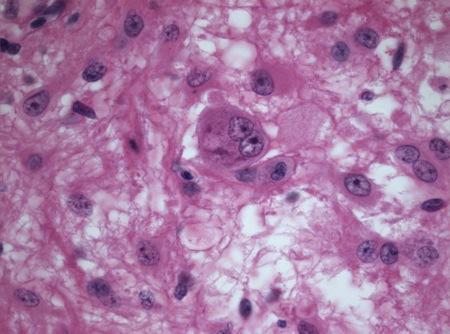
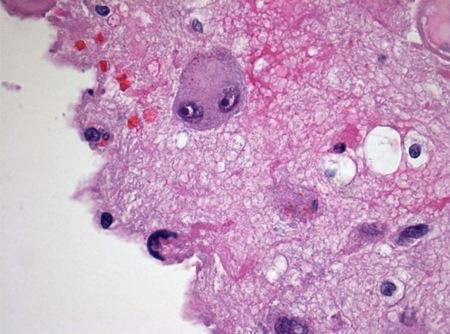
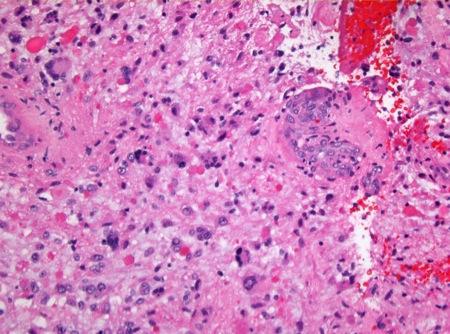
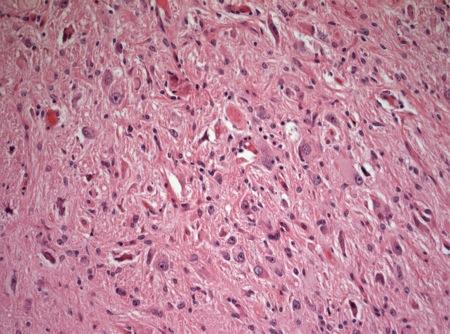
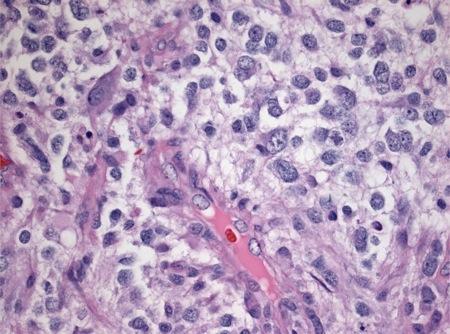
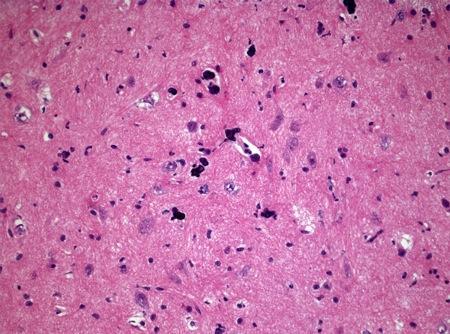
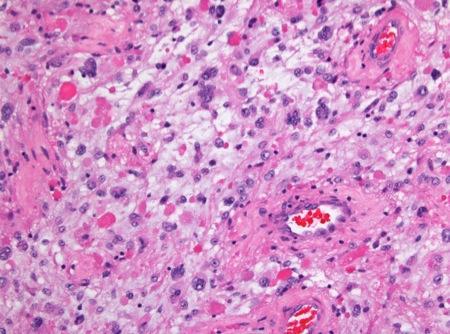
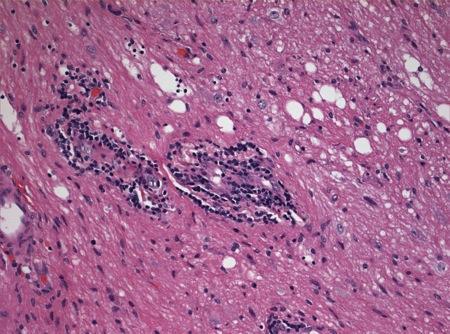
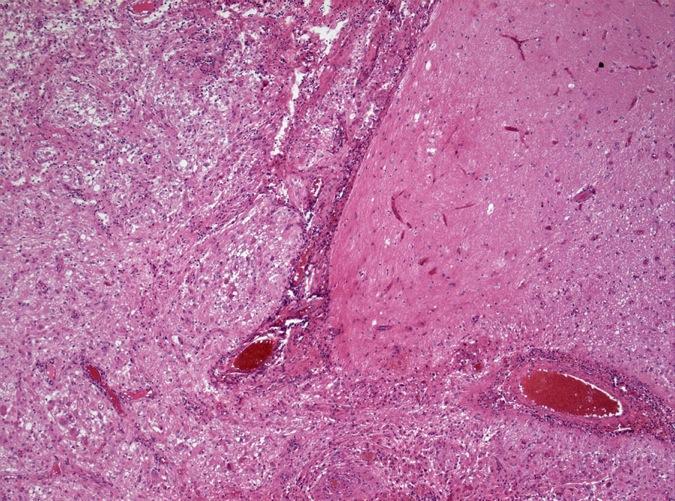
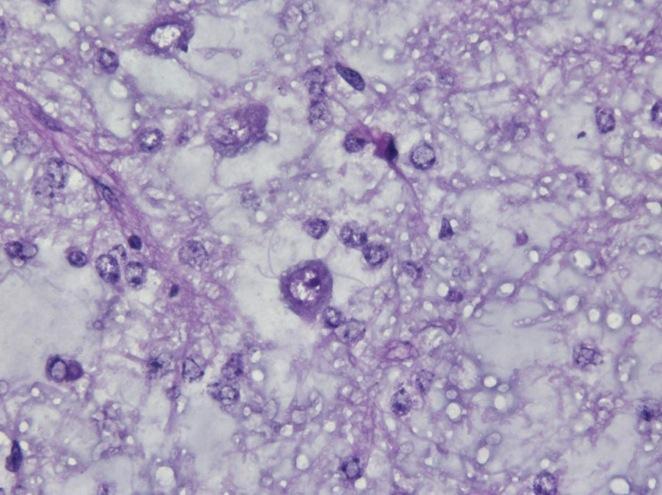
14 Ganglioglioma Microscopic Pathology Predominant Pattern Type Ill-defined lobules, non-infiltrative growth Predominant Cell Type Ganglion cells Wrong location Wrong parts Too many nuclei Glial cells Fibrillary or pilocytic astrocytoma, occasionally oligodendroglial Typically low grade Large swollen astrocytes that may mimic neurons
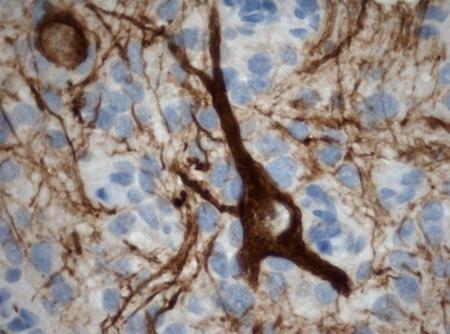
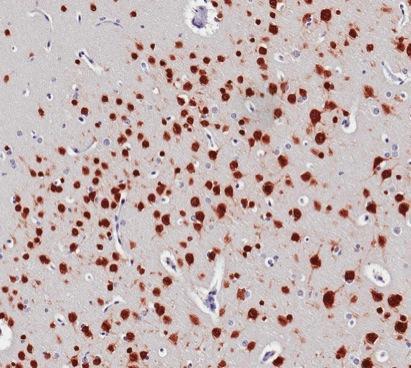
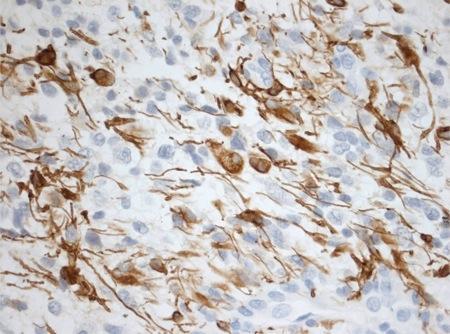
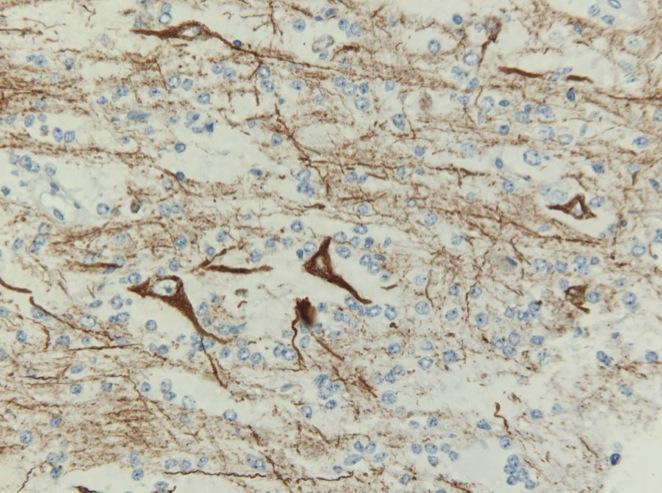
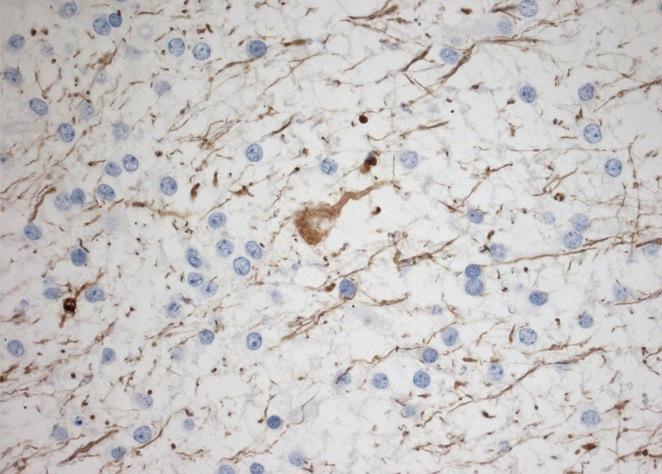
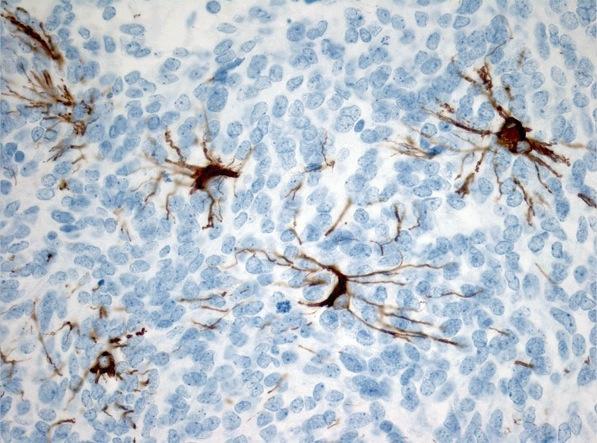
15 Ganglioglioma NFP
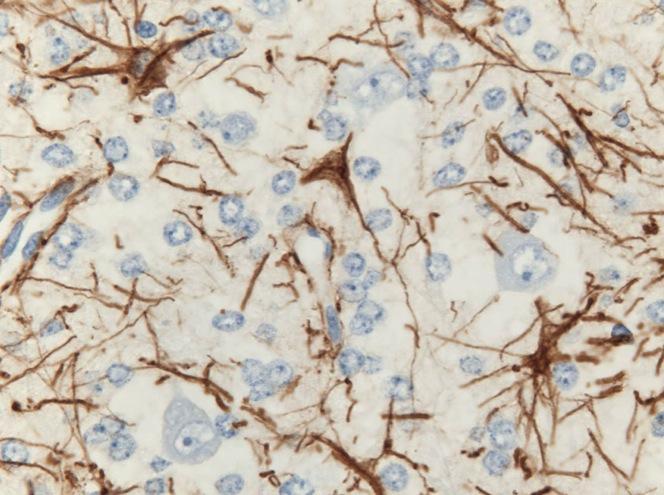
16 Ganglioglioma GFAP
 Calcification Eosinophilic granular bodies are common Glial and neuronal elements may be admixed or")
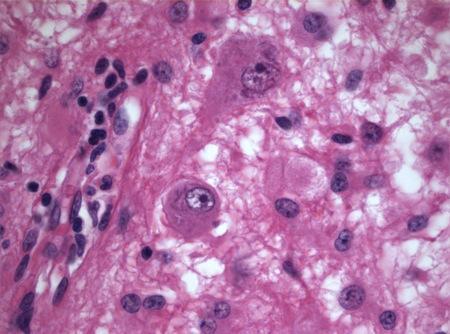
17 Microscopic Pathology, Cont d. Histologic Features Perivascular inflammatory infiltrates (vascular hyalinization is not uncommon) Calcification Eosinophilic granular bodies are common Glial and neuronal elements may be admixed or separate Leptomeningeal infiltration (not a sign of malignancy) Neuronal element may relative inconspicuous in some tumors, highlighted with IHC markers (NFP, synaptophysin, etc.) Ganglioglioma
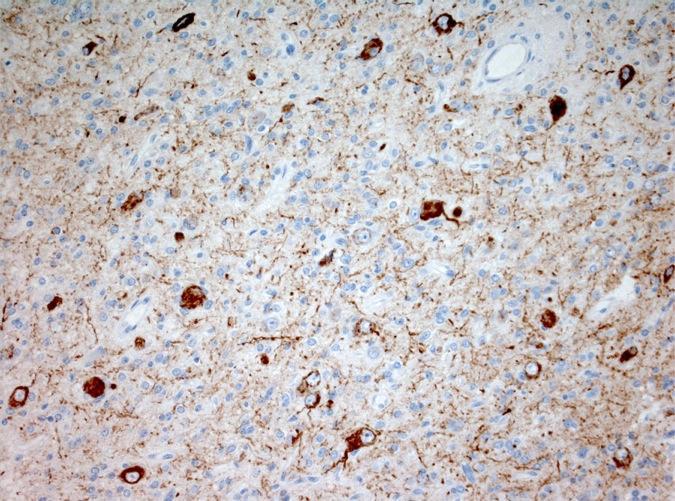
18 Ganglioglioma NFP
19 Neuronal & Mixed Neuronal-Glial Ganglioglioma, Dysembryoplastic Neuroepithelial Tumor (DNET), Central Neurocytoma
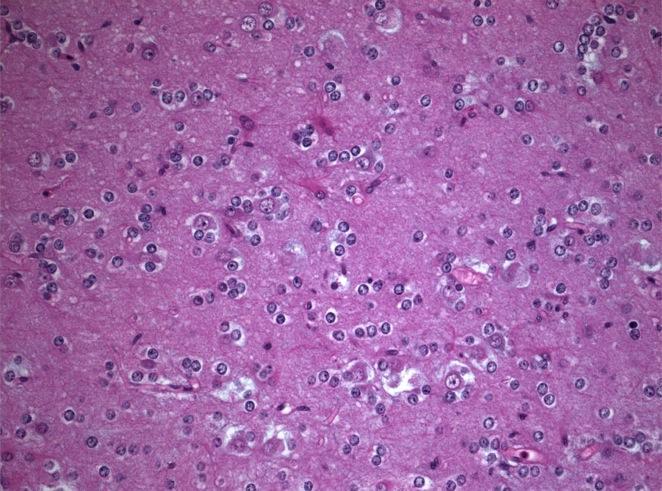
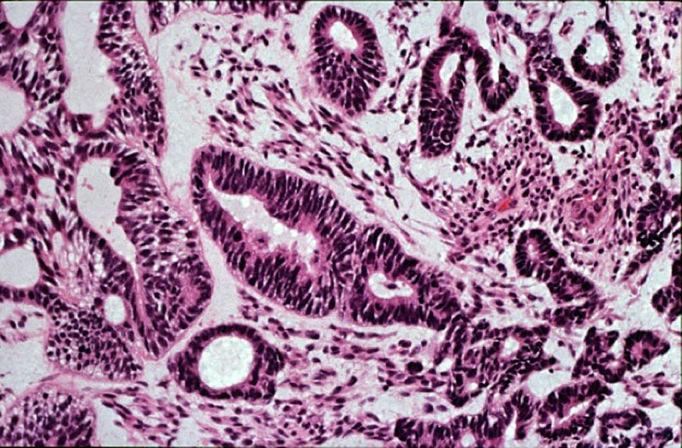
20 Dysembryoplastic Neuroepithelial Tumor (DNET) Terminology Definition A multinodular cortical tumor associated with refractory epilepsy Clinical Issues Epidemiology Age (diagnosis) Diagnosis typically in 2 nd -3 rd decade Gender Males > Females Presentation Seizure 90% present with first seizure before age 20 Prognosis Benign tumors (WHO grade I) Cured by gross total resection in most cases

21 Dysembryoplastic Neuroepithelial Image Findings General Features Location Temporal lobe, particularly mesial structures Any supratentorial cortex Erosion, deformation, thinning of overlying skull Morphology Cortically based Ribbon-like multi-nodular areas of cortical thickening and abnormal signal Tumor (DNET)

22 Dysembryoplastic Neuroepithelial Macroscopic Features Cortex thickened by one or more mucoid nodules Semi-translucent Gray color Blurred gray-white junction May have exophytic or raised component associated with secondary changes in overlying skull Tumor (DNET)
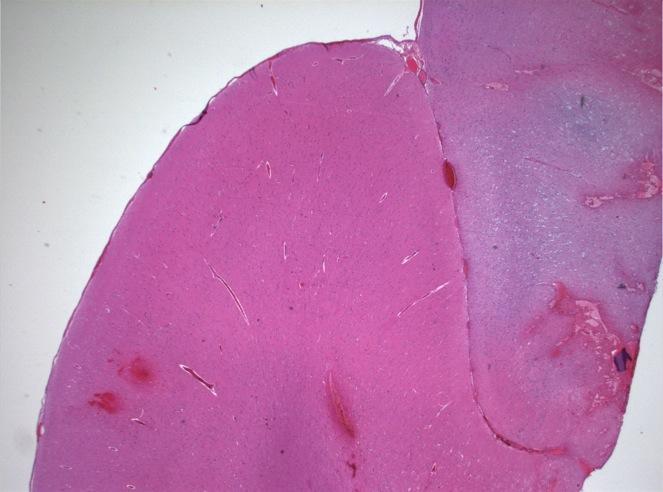
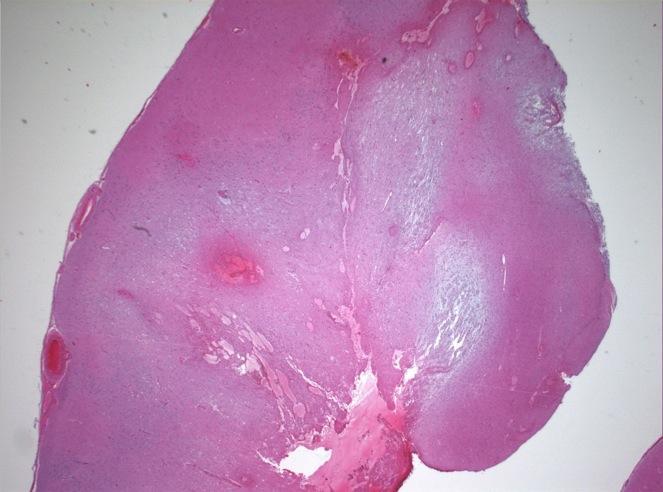
23 Dysembryoplastic Neuroepithelial Tumor (DNET)
 Variable amounts of extracellular")
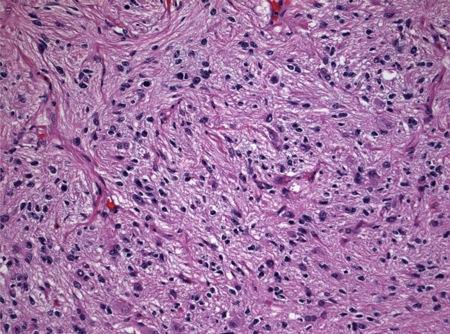
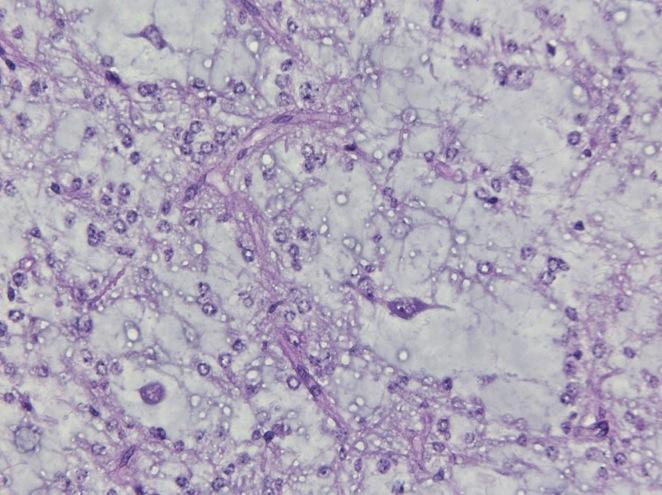
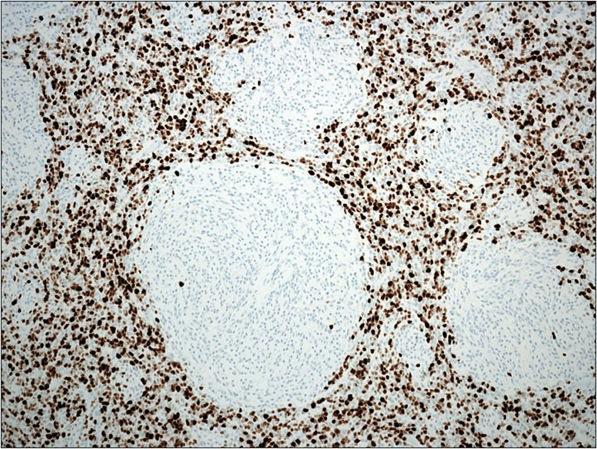
24 Dysembryoplastic Neuroepithelial Microscopic Pathology Predominant Pattern Type Nodular Predominant Cell Type Glioneuronal Oligodendrocyte like cells (OLCs) Ganglion cells Histologic Features Loosely textured cortical nodules Well-defined OLCs arrayed along bundled axons and blood vessels, perpendicular to cortical surface ( specific glioneuronal element ) Variable amounts of extracellular mucopolysaccharide (MPS) Ganglion cells floating in pools of MPS Tumor (DNET)
25 NFP GFAP
 Nuclear atypia and")
26 Dysembryoplastic Neuroepithelial Microscopic Pathology Cont d. Histologic Features Internodular areas OLCs infiltrate cortex Mimics oligodendroglioma May extend into and through the subpial surface Complex DNET Compact elongated cells (JPA) Nuclear atypia and hyperchromasia (diffuse astroctyoma) Arcades of proliferative glomeruloid vasculature and scattered mitotic activity are NOT indicators of malignant transformation Associated cortical dysplasia Tumor (DNET)
27 Dysembryoplastic Neuroepithelial Tumor (DNET)
28 Neuronal & Mixed Neuronal-Glial Ganglioglioma, Dysembryoplastic Neuroepithelial Tumor (DNET), Central Neurocytoma
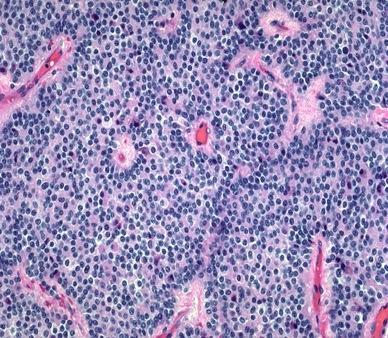
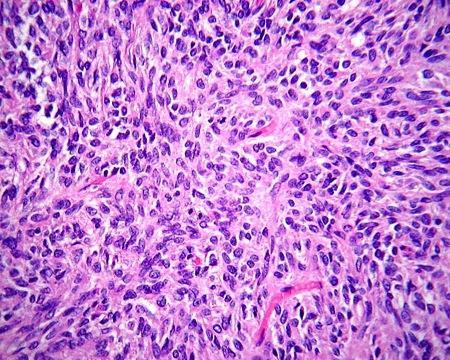
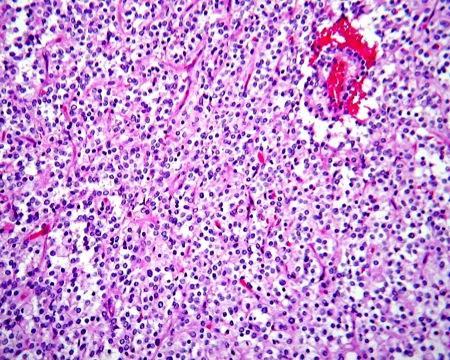
29 Neurocytoma Terminology Definition A neuronal tumor comprised primarily of neurocytes (small to medium sized cells lacking overt histologic evidence of neuronal differentiation) WHO 2007 added recognition for extraventricular occurrence of this tumor with slightly broader spectrum of histologic features Clinical Issues Epidemiology Age Young adults, mean age of 29 yrs at presentation 2/3 of tumors between yrs. Have been reported in patients up to the 7 th decade Gender (M:F) Equal Presentation Increased intracranial pressure in central neurocytomas; less commonly, hormonal disturbances Typically short duration of symptoms (~3 months) Extraventricular neurocytomas associated with mass effect and seizures Prognosis Generally benign tumors (WHO grade II) Surgical resection is mainstay of therapy with XRT for subtotal excision Partial resection and increased Ki-67 labeling (> 2%) may be associated with increased risk of recurrence; dissemination is rare

30 Neurocytoma Image Findings General Features Location Supratentorial, involving lateral and 3 rd ventricles 50% in anterior portion of one of the lateral ventricles Attachment to the septum pellucidum is frequent Often adjacent to the foramen of Monro Frequently extend into opposite ventricle, less often the 3 rd Extraventricular locations Intraparenchymal w/ or w/o impinging on ventricles Morphology Intraventricular Often partially calcified Enhancing Extraventricular tumors can be solid or cystic with mural nodule
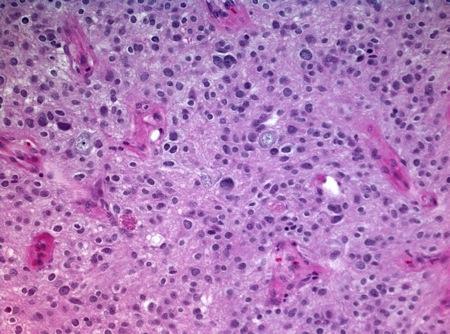
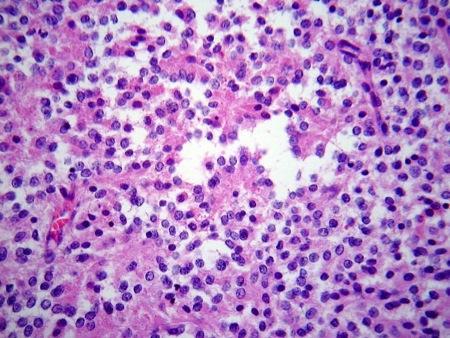
31 Neurocytoma Macroscopic Features Well circumscribed Fleshy Soft Flecks of calcification Microscopic Pathology Predominant Pattern Type solid, non-infiltrative growth Predominant Cell Type Central Neurocytoma Neurocytes Small, mature round neurons Artifactual nuclear halo (oligodendroglial mimic) Extraventricular Neurocytoma Ganglioid cells Ganglion cells Histologic Features Fine fibrillary neuropil matrix Neurocytic rosettes (ependymoma mimic) Occasional necrosis, not prognostic Rarely cytologic atypia, vascular proliferation, not clearly prognostic Mitotic activity is rare Ki-67 labeling > 2% is associated with increased risk of recurrence and designated as atypical neurocytoma
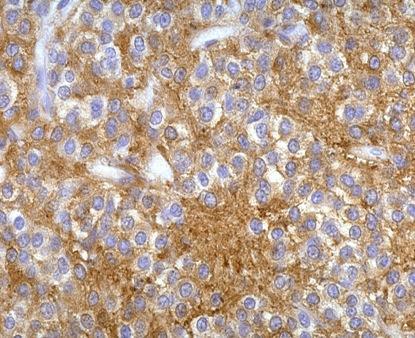
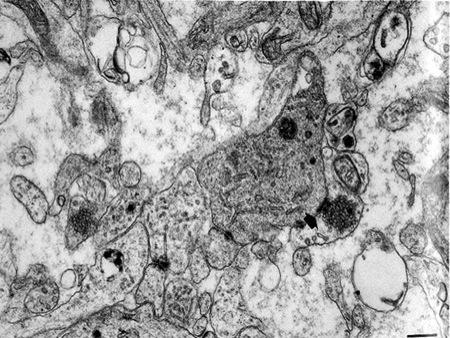
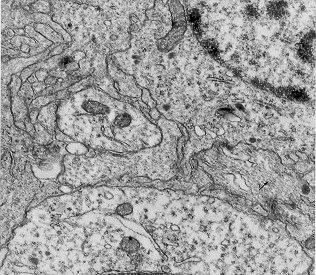

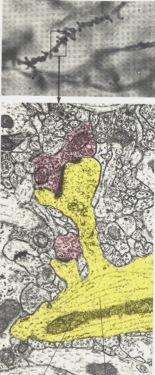
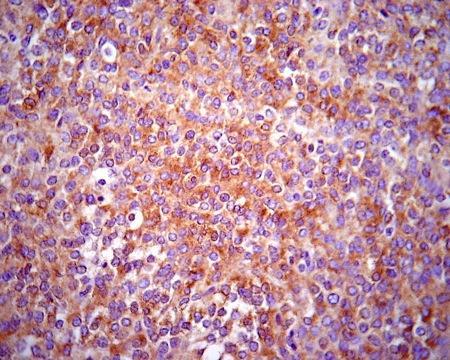
32 Neurocytoma Microtubules Synapses & secretory vesicles SYN
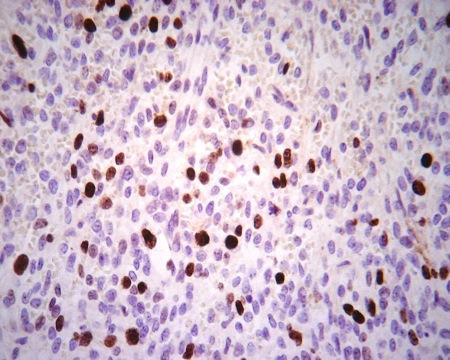
33 Atypical Neurocytoma SYN Ki-67
34 Embryonal Tumors Medulloblastoma (MB), CNS Primitive Neuroectodermal Tumors (CNS PNET), Atypical Teratoid / Rhabdoid Tumors (AT/RT)
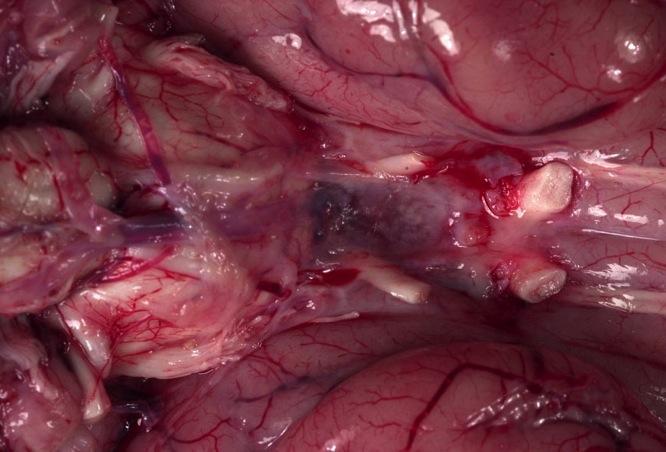
35 Medulloblastoma Terminology Definition Embryonal tumor comprised of primitive neuroectodermal cells involving the cerebellum, with a propensity for CSF dissemination Clinical Issues Epidemiology Age (diagnosis) Median age ~ 8 yrs. Most occur between ages 3 10 yrs. In patients age = < 1 yr. Accounts or nearly 25% of all pediatric brain tumors Not exclusively a pediatric tumor, 20-25% of all MB reportedly occur beyond the age of 20 years. Gender (M:F) 1.6 : 1 Presentation Increased ICP due to obstructive hydrocephalus H/A (morning), vomiting, lethargy Ataxia (with tumor progression) Increased head circumference Backache, voiding difficulties (CSF dissemination)
36 Medulloblastoma Clinical Issues, cont d. Prognosis Crude risk based stratification (age, extent of post-operative disease, metastasis) Metastatic staging of MB M0 - No gross subarachnoid or hematogenous metastasis M1 - Microscopic tumor cells found in CSF M2 - Gross nodular seeding in cerebellum, cerebral subarachnoid space, or in the third or fourth ventricles M3 - Gross nodular seeding in spinal subarachnoid space M4 - Extraneuraxial metastasis. Clinical Issues, cont d. Three basic categories: Average risk (> 3 years, < 1.5 cm 2, M0) 5-year survival rate > 80% Poor risk (> 3 years, > 1.5 cm 2, M1-M4) 5-year survival rate 40 60% Infants (< 3 years irrespective of other variables) 5-year survival rate ~ 30% Worse with metastatic disease Better survival with desmoplastic tumors


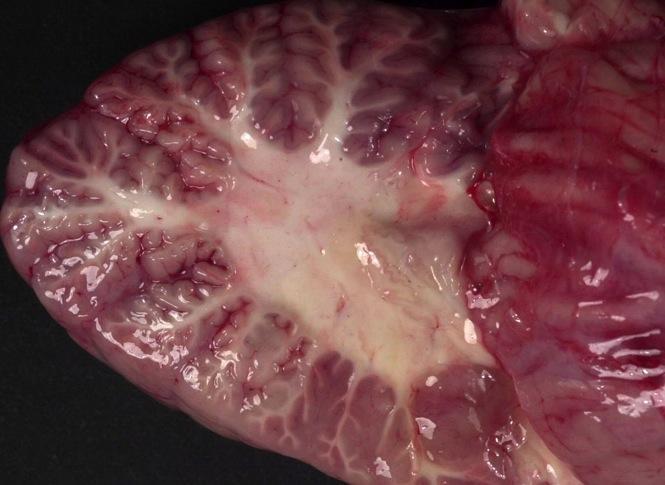
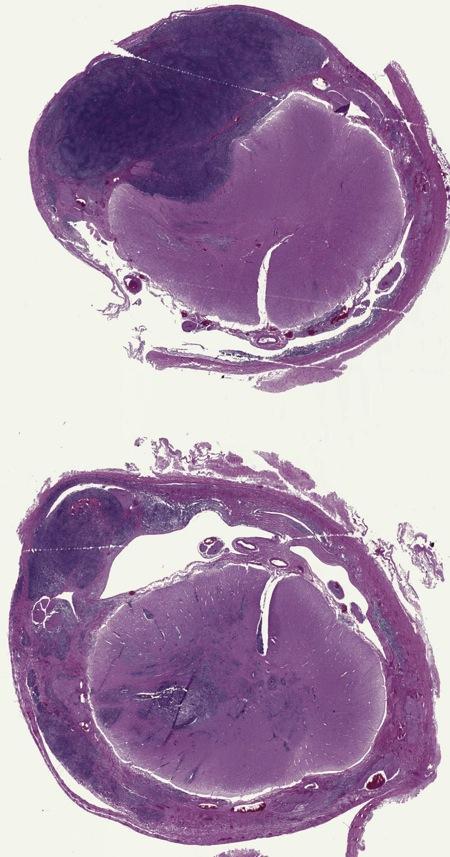
37 Image Findings General Features Location Cerebellum, midline/vermis (children) Cerebellum, hemispheres In children as tumor enlarges In some adults as primary site Maybe associated with nodular/desmoplastic MBs Extension into 4 th ventricle where it may form a discrete mass Gelatinous opacification of SA ( sugar icing ) with CSF dissemination Morphology Well circumscribed Solid, sometimes cystic or nodular Contrast enhancing Medulloblastoma


38 Medulloblastoma Macroscopic Features Gray pink Soft and gelatinous firm (depending on degree of desmoplasia) Necrosis typically limited to small foci


39 Medulloblastoma
 Extensive nodularity and advanced neuronal differentiation (3%) Large cell/anaplastic")
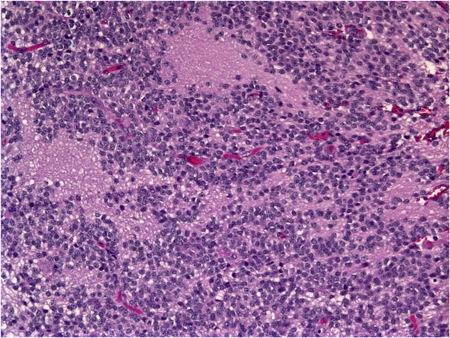
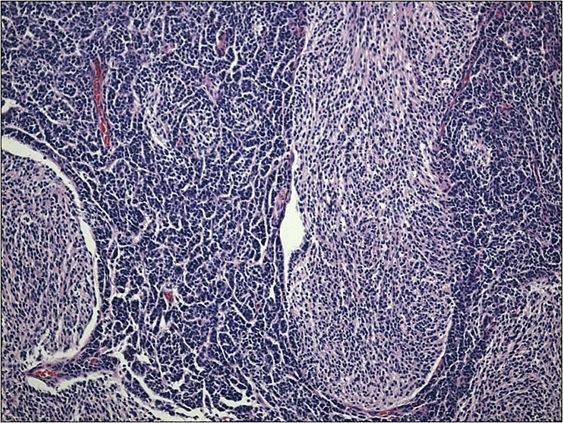
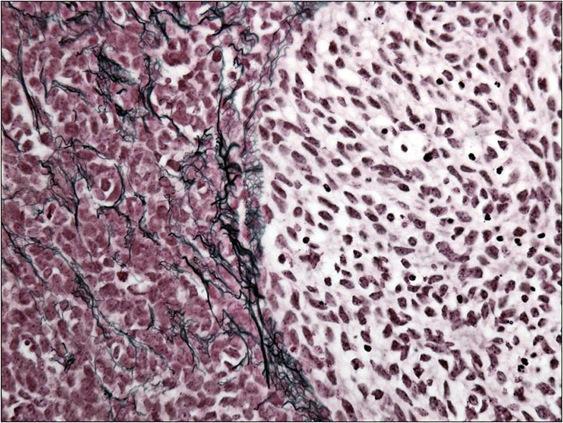
40 Medulloblastoma Microscopic Pathology WHO 2007 recognizes four types of MB Classic/undifferentiated (73%) Desmoplastic/Nodular (7%) Extensive nodularity and advanced neuronal differentiation (3%) Large cell/anaplastic (17%)
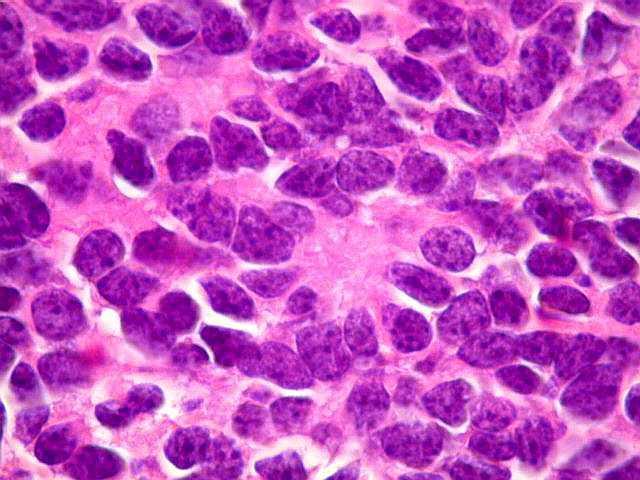
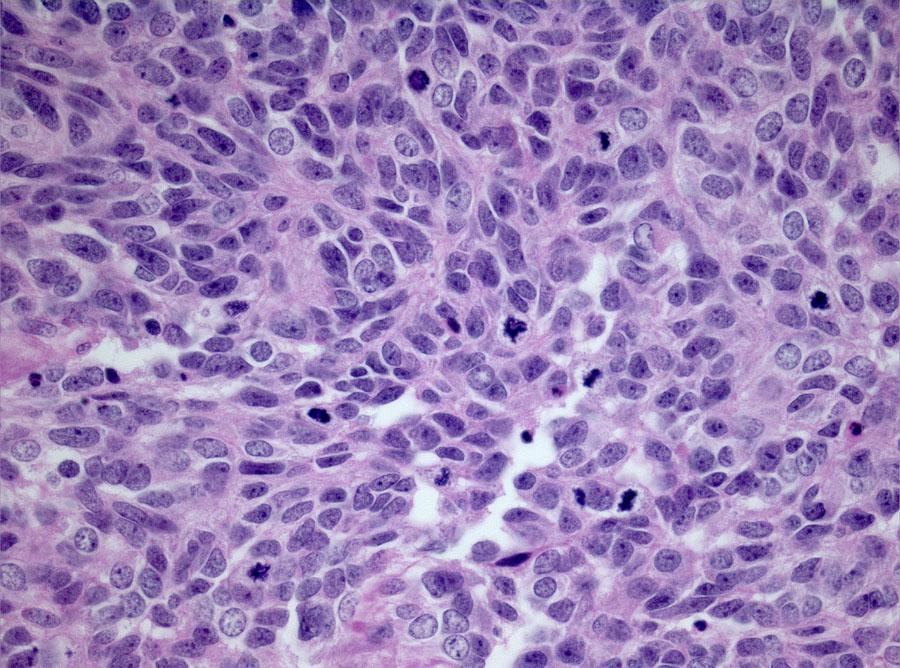
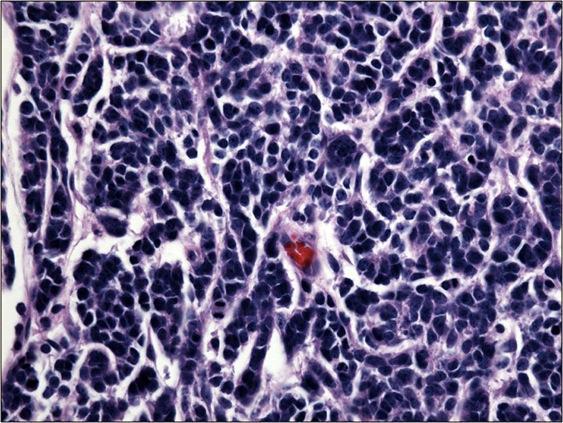
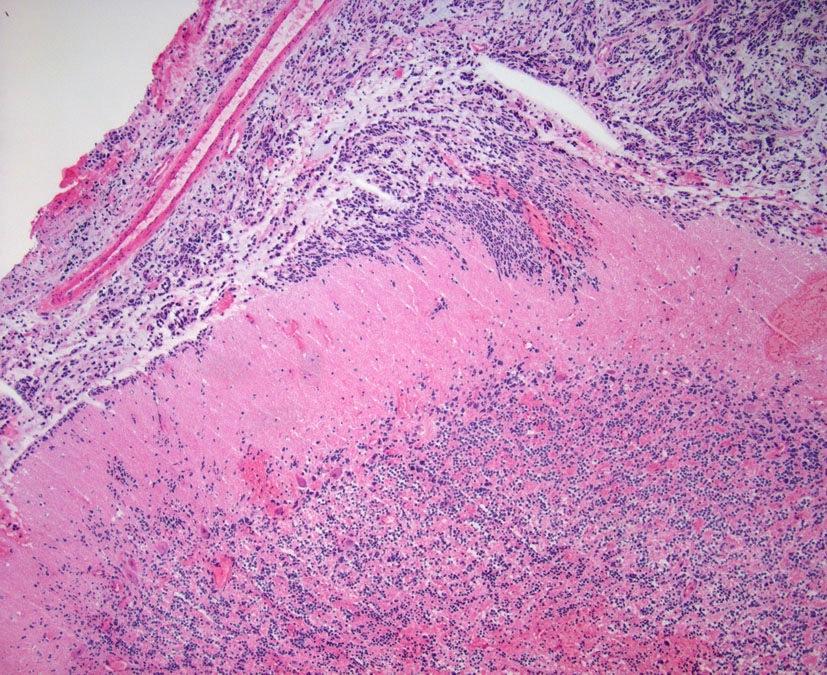
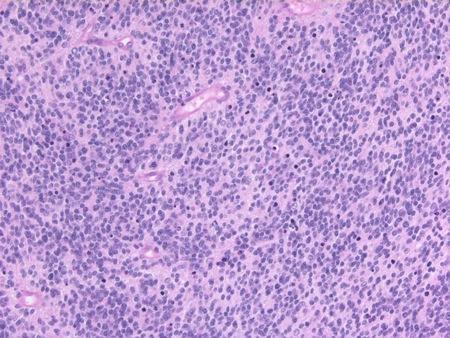
41 Medulloblastoma Microscopic Pathology cont d. Predominant Pattern Type Classic/undifferentiated Patternless sheets Desmoplastic/nodular Not leptomeningeal reaction Collagen rich, separating tumor cells into think columns Nodular collagen free zones (pale islands) w/ neuropil diff. Predominant Cell Type Primitive neuroectodermal cells Small, inconspicuous cytoplasm, oval to carrot shaped hyperchromatic nuclei Anaplastic/large cell Anaplasia, elevated mitotic and apoptotic indices, cell wrapping Large nuclei with prominent nucleoli (rare) Eberhardt Cancer Cell 2012; 21(2):137
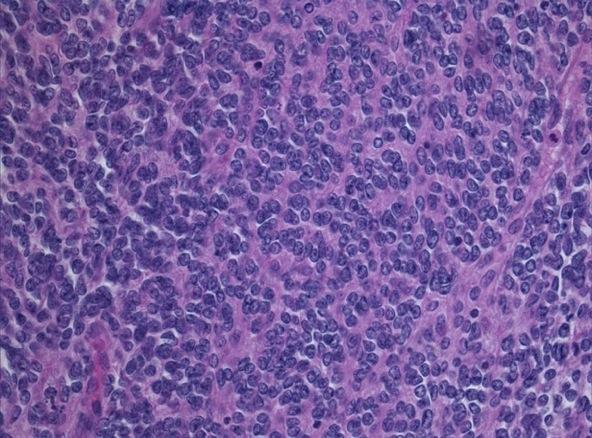
42 Medulloblastoma Classic MB Classic MB
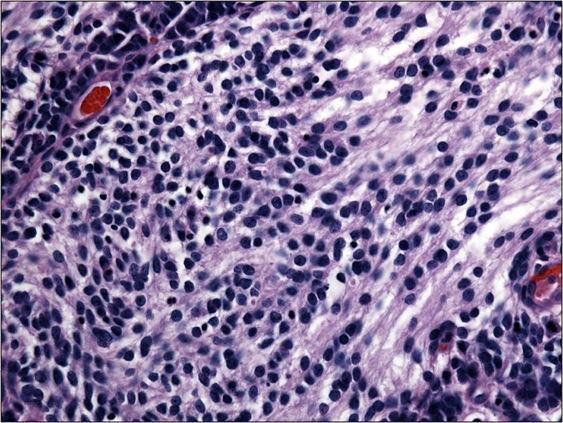
43 Medulloblastoma Nodular Desmoplastic MB
44 Medulloblastoma

 More vesicular chromatin staining")
45 Medulloblastoma Microscopic Pathology, Cont d. Cytologic Features Desmoplastic/nodular Ganglioid ganglion cell Atypia in internodular region Anaplastic MB Modestly larger nuclei Irregular nuclear morphology Cell wrapping Large cell MB Large nuclei (2x > classical MB) More vesicular chromatin staining pattern Nucleoli Anaplastic MB Large Cell MB
 Proliferative activity (Ki-67) Patterns of expression of these markers are")
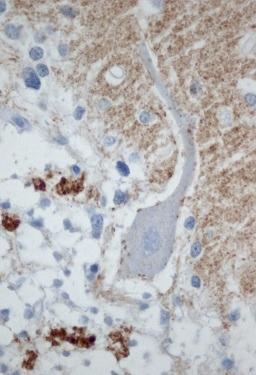
46 Medulloblastoma Microscopic Pathology, Cont d. Immunohistochemistry Polyphenotypic tumors Markers of Divergent neuroepithelial differentiation (GFAP, NFP, Synaptophysin) Proliferative activity (Ki-67) Patterns of expression of these markers are variable within and between tumors Desmoplastic/nodular Nodules (neuronal) Internodular region (proliferative activity) Entrapped/reactive astrocytes NFP
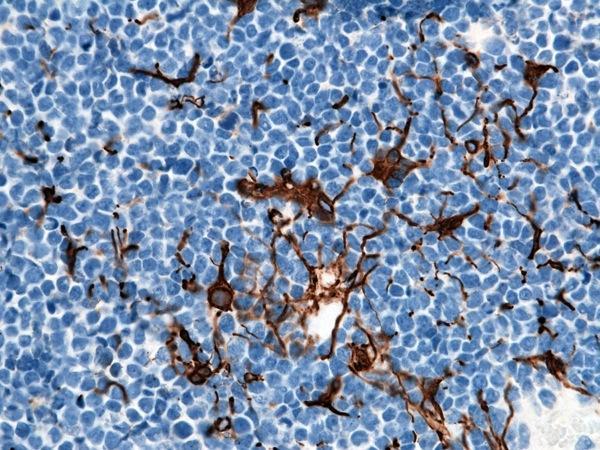
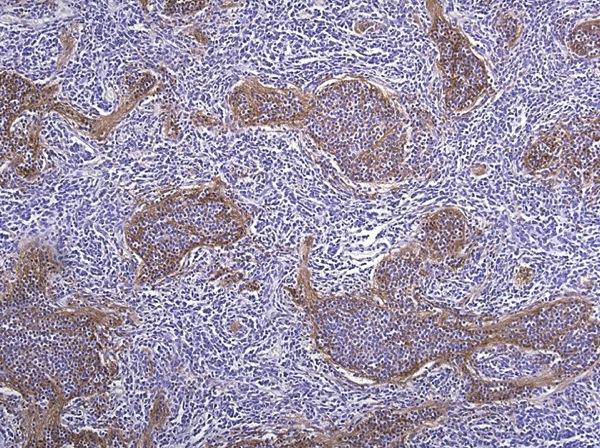
47 Medulloblastoma Syn Ki-67 GFAP GFAP
48 Medulloblastoma Histopathology based MB stratification Infants with desmoplastic tumors are classified as low-risk Children with large cell or anaplastic tumors are classified as high-risk
49 Medulloblastoma Genetics informed hereditary tumor syndromes Gorlin syndrome (PTCH1) SHH pathway: PTCH1/SUFU/SMOH mutations in ~25% sporadic tumors Turcot type 2 / mismatch repair (APC) WNT pathway: CTNNB1/APC/AXINI1/2 mutations in ~15% sporadic tumors

50 Medulloblastoma Eberhardt Cancer Cell 2008; 10(26):2821
51 medulloblastomas in infants, and LCA tumours are associated with a poorer outcome than classic or desmoplastic tumours in children aged 3 years On the basis of these findings, two ongoing clinical trials 23,24 are assigning therapy according to histological variants, in addition to clinical risk. This strategy recognizes the importance of t horoughly characterizing each tumour before initiating treatment, owing to intertumour variability, but it does not reflect the differences that exist within the same h istological variants of medulloblastoma. The current molecular classification Our understanding of medulloblastoma biology has been substantially enhanced by high-throughput genomic and proteomic methods, such as transcriptomic and methylomic analyses. An early genomics study from 2006, 25 demonstrated that medulloblastoma might consist of biologically distinct subgroups of tumours. The groups, which were distinguished by transcriptomic differences, exhibited intragroup similarities in mutation profiles, structural chromosomal alterations, histology, demographics, and clinical outcome. 25 These initial data have been validated in several laboratories worldwide using large cohorts of patients with tumours and technologically more-advanced transcriptomic techniques than those used in the 2006 study. 16,26,27 The result of these efforts is a consensus that medulloblastoma consists of four clinical and molecular subtypes of disease: the Wnt subtype, in which canonical Wnt signalling is upregulated; the sonic hedgehog (SHH) subtype, with hallmark activation of the SHH-signalling cascade; and group 3 and group 4 medulloblastomas. 28 tumours are typically uniform in their genetic aberrations, h istological pattern, and clinical presentation. 31 Genetics All medulloblastomas with nuclear accumulation of β-catenin are categorized as Wnt-subtype tumours; 5,29,30 nuclear β-catenin interacts with members of the transcription factor/lymphoid enhancer-binding factor (TCF/LEF) family of transcription factors to activate the canonical Wnt-signalling pathway. 32,33 More than 90% of the Wntsubtype medulloblastomas harbour mutations in CTNNB1, the gene that encodes β-catenin (Box 1); 31,34 36 the resulting mutant β-catenin protein is resistant to degra dation, leading to its accumulation in the cell nucleus. 37 Wntsubtype medulloblastomas also frequently have deletions of one copy of chromosome 6 (monosomy 6; Box 1), 25,29 although some Wnt tumours retain two copies of this chromosome. Other than monosomy 6, Wnt-subtype medullo blastoma is associated with limited occurrence of gains and/or losses of chromosomal regions across the genome. 31 Thus, monosomy 6, in conjunction with nuclear β-catenin accumulation, serves as a sensitive and highly specific marker for this subtype of disease. 30 Whole-genome sequencing (WGS) studies have identified recurrent mutations specific to this medulloblastoma subgroup. The most prevalently mutated genes, in addition to CTNNB1, are DDX3X, SMARCA4, TP53, KMT2D, CSNK2B, and CREBBP (Box 1). Many of these genes (that is, CREBBP, SMARCA4, and KMT2D) encode proteins that interact with nuclear β-catenin and remodel chromatin, suggesting that cooperative mutations occur in the development of this tumour subtype. 34 NATURE REVIEWS CLINICAL ONCOLOGY VOLUME 11 DECEMBER
52 The Grand Challenge: Medulloblastoma Classification Medulloblastoma, histologically defined -Medulloblastoma, classic -Desmoplastic/nodular medulloblastoma -Medulloblastoma with extensive nodularity -Large cell/anaplastic medulloblastoma Medulloblastoma, genetically defined -Medulloblastoma, WNT-activated -Medulloblastoma, SHH-activated -Medulloblastoma, non-wnt/non-shh
53 CNS Embryonal Tumors Medulloblastoma (MB), CNS Primitive Neuroectodermal Tumors (CNS PNET), Atypical Teratoid / Rhabdoid Tumors (AT/RT)
54 CNS PNET Terminology Definition Embryonal tumor comprised of primitive neuroectodermal cells outside of the cerebellum Evolving terminology CNS embryonal tumors Clinical Issues Epidemiology Age (diagnosis) Median age ~ 5.5 yrs. Age range 4 weeks 20 years Gender (M:F) 1.2 : 1 Presentation Increased ICP Epilepsy Focal neurological signs Prognosis Malignant (WHO IV) Worse overall 5 yr survival than MB < 2 yrs worse prognosis than older children Prone to dissemination outside CNS

55 CNS PNET (embryonal tumors) Image Findings General Features Location Most often supratentorial May involve the spinal cord or other locations Morphology Well circumscribed Solid, sometimes cystic May have necrotic areas Majority show calcification
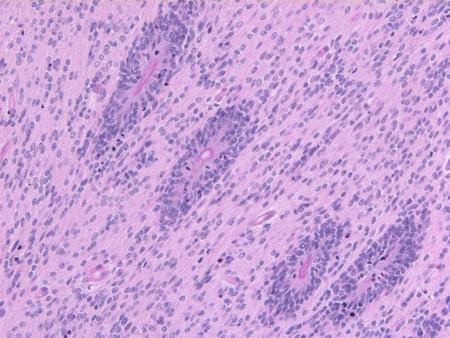
56 CNS PNET (embryonal tumors) Macroscopic Pathology Not substantially different from that encountered in MB No desmoplastic form Gray pink Soft and gelatinous Necrosis typically limited to small foci Microscopic Pathology Histologic Features Densely packed cells with little cytoplasm Infiltrative growth pattern Neuroblastic (Homer Wright) rosettes Proliferative activity and apoptosis are common Necrosis may produce cystic change
 Ependymoblastoma (")
57 CNS PNET (embryonal tumors) Microscopic Pathology, Cont d. Specific histologic patterns are recognized in WHO 2007 as subtypes of CNS PNET Cerebral neuroblastoma or ganglioneuroblastoma (neuronal differentiation) Ependymoblastoma ( ependymal differentiation) Embryonal tumors with multilayered rosettes (ETMR) First decade Aggressive, poor prognosis
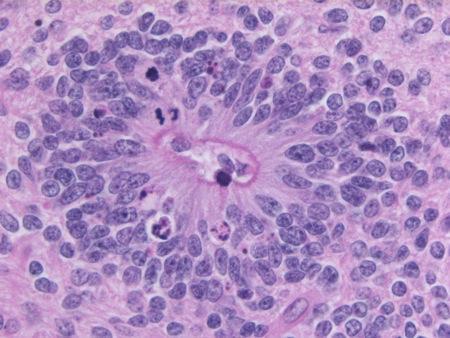

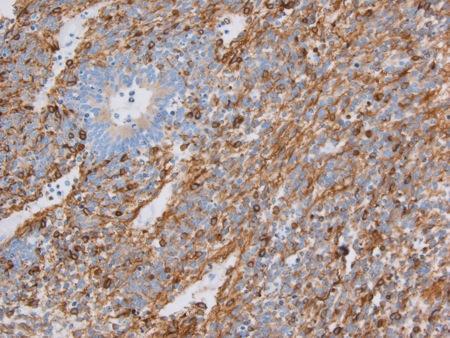
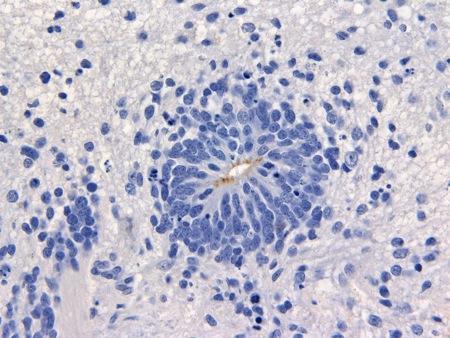
58 CNS PNET (embryonal tumors w/ multilayered rosettes) Ki-67 NFP EMA
, rare but Early childhood Aggressive, poor prognosis")
59 CNS PNET (embryonal tumors) Microscopic Pathology, Cont d. Medulloepithelioma ( neural tube features), rare but Early childhood Aggressive, poor prognosis Often intraventricular, anywhere along neuraxis

60 CNS PNET (embryonal tumors) - Medulloepithelioma




61 CNS PNET (embryonal tumors) Microscopic Pathology, Cont d. Immunohistochemistry Polyphenotypic tumors Markers of Divergent neuroepithelial differentiation (GFAP, NFP, Synaptophysin) Proliferative activity (Ki-67) Patterns of expression of these markers are variable within and between tumors Additional markers (EMA on luminal surface of ependymoblastoma/etaner; nestin on basal surface of medulloepitheliomas) NFP Ki-67 GFAP Nestin


62 Molecular Genetics of CNS PNET (embronal tumors)




63 CNS PNET History Repeats Itself EB CN ME PNET spnet ETMR (C19MCaltered or NOS) CNS embryonal tumor, NOS ETANTR ME
64 Embryonal Tumors Medulloblastoma (MB), CNS Primitive Neuroectodermal Tumors (CNS PNET), Atypical Teratoid / Rhabdoid Tumors (AT/RT)
65 Atypical Teratoid / Rhabdoid Tumor Terminology Definition Embryonal tumor containing cells with rhabdoid or epithelioid features and/or evidence of loss of INI1/SMARCB1 expression Evolving consensus that diagnosis requires demonstration of inactivation of INI1/SMARCB1 by IHC or other means; and absent this confirmation these should be classified as CNS embryonal tumors with rhabdoid features. Clinical Issues Epidemiology Age (diagnosis) Median age = 5 mos. (CHOP) Typically < 3 yrs., with greatest frequency < 1 yr. 40% of all embryonal tumors in infants (CHOP) Rarely encountered in older children and adults Gender (M:F) : 1 Presentation Increased ICP or seizures, depending on location Prognosis Malignant (WHO grade IV) with mean post-surgery survival of months




66 Atypical Teratoid / Rhabdoid Tumor General Features Location Macroscopic Cystic Heterogeneous Hemorrhage or necrosis Data courtesy of Dr. Rorke-Adams; images Drs. Rorke-Adams & Parham


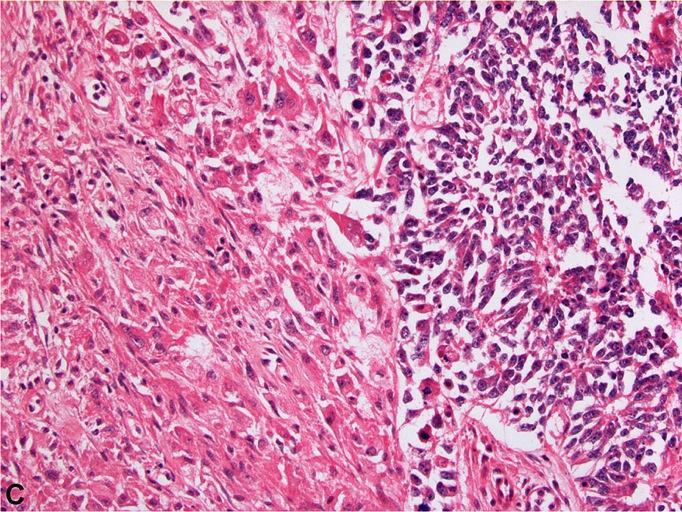
67 Atypical Teratoid / Rhabdoid Tumor Microscopic Pathology Predominant Pattern Type Sheets of tumor with infiltrative growth through adjacent parenchymal and leptomeninges Predominant Cell Type Primitive neuroectodermal cells Rhabdoid cells Mesenchymal/epithelial cells Cytology of Rhabdoid cells Vesicular chromatin staining Prominent eosinophilic nucleoli




68 Atypical Teratoid / Rhabdoid Tumor Microscopic Pathology, Cont d. Histologic Features Prominent cell borders Abundant eosinophilic cytoplasm Vacuolar cytoplasmic degeneration Variable mitotic activity Karyorrhectic debris Necrosis



69 Atypical Teratoid / Rhabdoid Tumor Microscopic Pathology, Cont d. Histologic Features Rhabdoid cells may be focal or rare Epithelioid cells may be more common than rhabdoid cells PNET/MB component often predominates and occasionally is all there is Poorly differentiated epithelial structures are occasionally identified Spindle cell mesenchymal differentiation Chordoid pattern with abundant extracellular myxohyaline material vimentin SMA EMA AE1/3 GFAP (br.)/nfp (red)


70 Atypical Teratoid / Rhabdoid Tumor & Non-CNS MRT: Common Features Histology Rhabdoid cells* Polymorphic features Primitive, epithelial and mesenchymal elements are most frequently identified Spectrum of histologic patterns can be observed in all rhabdoid tumors Biologically aggressive Infiltrative margins Frequent lymphatic invasion Necrosis High proliferative rate/mitotic rate (typically)
71 Atypical Teratoid / Rhabdoid Tumor & Non-CNS MRT: Common Features Immunohistochemistry Polyphenotypic tumors Markers of divergent differentiation: Neuroepithelial Epithelial Mesenchymal Intermediate filaments Markers of myogenic differentiation are not typically expressed Vimentin EMA Actin* GFAP Neural (NSE, synapto, NFP) Cytokeratin CD99 Desmin Myogenin/Myoglo bin Expression All Most - All Most - All Most Most Many Many Some Negative (?)
72 Atypical Teratoid / Rhabdoid Tumor Molecular Genetics Nearly all cases of AT/RT have deletion or mutation in SMARCB1/INI1 (22q11.2) Component of the SWI/SNF chromatin remodeling complex Typically results in stop or premature truncation ~25% have homozygous deletion of entire coding region Tumors are both sporadic and due to constitutional loss or inactivation of SMARCB1/IN1 (RTPS) Germline mutations in ~35% of cases of AT/RT


73 Atypical Teratoid / Rhabdoid Tumor Molecular genetics SMARCB1/INI1 is ubiquitously expressed in nuclei of normal cells IHC staining for SMARCB1/INI1 is a sensitive and specific method for detecting loss of expression and correlates with mutation and deletion of the gene Staining should be performed on ALL embryonal CNS tumors Genetic screening for all newly diagnosed atypical teratoid / rhabdoid tumors INI1 INI1


 Have")

74 Atypical Teratoid / Rhabdoid Tumor Rhabdoid Tumors May (Very Rarely!!!) Have Retained SMARCB1 Expression SMARCB1 SMARCA4


75 Atypical Teratoid / Rhabdoid Tumor PMID:



76 Atypical Teratoid / Rhabdoid Tumor c-myc CCND1 GLI1 AURKA Epigenetically Driven Changes in Gene Expression PI3K- AKT Hippo ID proteins, EZH2 Cyclin D1
77 Acknowledgements Children s Hospital of Philadelphia Dr. Lucy Rorke-Adams Dr. Mariarita Santi AFIP Dr. Elisabeth Rushing
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
General: Brain tumors are lesions that have mass effect distorting the normal tissue and often result in increased intracranial pressure.
 1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
CNS TUMORS. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
Tumors of the Nervous System
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Tumors of the Central Nervous System
 Tumors of the Central Nervous System 1 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Introduction General: Brain tumors are lesions that have mass effect
Tumors of the Central Nervous System 1 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Introduction General: Brain tumors are lesions that have mass effect
Peter Canoll MD. PhD.
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Pleomorphic Xanthoastrocytoma
 Pleomorphic Xanthoastrocytoma Christine E. Fuller Keywords Pleomorphic xanthoastrocytoma; Pleomorphic xanthoastrocytoma with anaplastic features 2.1 OVERVIEW Pleomorphic xanthoastrocytoma (PXA) is an uncommon
Pleomorphic Xanthoastrocytoma Christine E. Fuller Keywords Pleomorphic xanthoastrocytoma; Pleomorphic xanthoastrocytoma with anaplastic features 2.1 OVERVIEW Pleomorphic xanthoastrocytoma (PXA) is an uncommon
Pathologic Analysis of CNS Surgical Specimens
 2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
Case 1. Maysa Al-Hussaini MD FRCPath
 Case 1 Maysa Al-Hussaini MD FRCPath MAYSA King AL-HUSSAINI Hussein Cancer MD Center MRCPATH KING HUSSEIN Amman CANCER Jordan CENTER Clinical history 4 year old boy History of frontal headache, sleepiness.
Case 1 Maysa Al-Hussaini MD FRCPath MAYSA King AL-HUSSAINI Hussein Cancer MD Center MRCPATH KING HUSSEIN Amman CANCER Jordan CENTER Clinical history 4 year old boy History of frontal headache, sleepiness.
Neuropathology Evening Session: Case 3
 Neuropathology Evening Session: Case 3 Christine E. Fuller, MD Cincinnati Children s Hospital Medical Center Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position
Neuropathology Evening Session: Case 3 Christine E. Fuller, MD Cincinnati Children s Hospital Medical Center Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position
Brain Tumors. Medulloblastoma. Pilocytic astrocytoma: Ahmed Koriesh, MD. Pathological finding
 NeuroPathology Page 8 Brain Tumors Pathological finding Pseudorosette Rosenthal fibers Rosettes Wet Keratin Psammoma bodies Fried egg Tumor Ependymoma, SEGA Pilocytic astrocytoma Medulloblastoma Craniopharyngioma
NeuroPathology Page 8 Brain Tumors Pathological finding Pseudorosette Rosenthal fibers Rosettes Wet Keratin Psammoma bodies Fried egg Tumor Ependymoma, SEGA Pilocytic astrocytoma Medulloblastoma Craniopharyngioma
Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child
 Case Reports in Oncological Medicine Volume 2013, Article ID 815923, 4 pages http://dx.doi.org/10.1155/2013/815923 Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child Y. T.
Case Reports in Oncological Medicine Volume 2013, Article ID 815923, 4 pages http://dx.doi.org/10.1155/2013/815923 Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child Y. T.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
SPECIAL SLIDE SEMINAR CASE 3
 SPECIAL SLIDE SEMINAR CASE 3 Tihana Džombeta, MD Leo Pažanin, MD, PhD Department of Pathology, School of Medicine, University of Zagreb Department of Pathology, Clinical Hospital Centre Sestre milosrdnice
SPECIAL SLIDE SEMINAR CASE 3 Tihana Džombeta, MD Leo Pažanin, MD, PhD Department of Pathology, School of Medicine, University of Zagreb Department of Pathology, Clinical Hospital Centre Sestre milosrdnice
In 1988 Dumas-Duport et al. first used
 Copyright 2009, Barrow Neurological Institute Dysembryoplastic Neuroepithelial Tumor: A Review Mark Garrett, MD Jennifer Eschbacher, MD Peter Nakaji, MD Most DNETs are benign, low-grade lesions. However,
Copyright 2009, Barrow Neurological Institute Dysembryoplastic Neuroepithelial Tumor: A Review Mark Garrett, MD Jennifer Eschbacher, MD Peter Nakaji, MD Most DNETs are benign, low-grade lesions. However,
Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma
 AJNR Am J Neuroradiol 23:243 247, February 2002 Case Report Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma John D. Port, Daniel J. Brat, Peter C. Burger, and Martin G.
AJNR Am J Neuroradiol 23:243 247, February 2002 Case Report Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma John D. Port, Daniel J. Brat, Peter C. Burger, and Martin G.
Site Specific Coding Rules MALIGNANT CENTRAL NERVOUS SYSTEM TUMORS
 Multiple Primary and Histology Site Specific Coding Rules MALIGNANT CENTRAL NERVOUS SYSTEM TUMORS 1 Prerequisites 2 Completion of Multiple Primary and Histology General Coding Rules 3 There are many ways
Multiple Primary and Histology Site Specific Coding Rules MALIGNANT CENTRAL NERVOUS SYSTEM TUMORS 1 Prerequisites 2 Completion of Multiple Primary and Histology General Coding Rules 3 There are many ways
Case 2. Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset
 Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
2. Subependymal giant cell astrocytoma:
 I. Astrocytomas: A. Diffusely infiltrating ( astrocytoma, anaplastic astrocytoma, GBM) B. Localised (pilocytic astrocytoma, pleomorphic xanthoastrocytoma, SGCA) *Grading: Diffuse: 1. Astrocytoma WHO grade
I. Astrocytomas: A. Diffusely infiltrating ( astrocytoma, anaplastic astrocytoma, GBM) B. Localised (pilocytic astrocytoma, pleomorphic xanthoastrocytoma, SGCA) *Grading: Diffuse: 1. Astrocytoma WHO grade
Anaplastic Pilocytic Astrocytoma: The fusion of good and bad
 Anaplastic Pilocytic Astrocytoma: The fusion of good and bad Alexandrina Nikova 1, Charalampos-Chrysovalantis Chytoudis-Peroudis 2, Penelope Korkolopoulou 3 and Dimitrios Kanakis 4 Abstract 5 Pilocytic
Anaplastic Pilocytic Astrocytoma: The fusion of good and bad Alexandrina Nikova 1, Charalampos-Chrysovalantis Chytoudis-Peroudis 2, Penelope Korkolopoulou 3 and Dimitrios Kanakis 4 Abstract 5 Pilocytic
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Five Most Common Problems in Surgical Neuropathology
 Five Most Common Problems in Surgical Neuropathology If the brain were so simple that we could understand it, we would be so simple that we couldn t Emerson Pugh What is your greatest difficulty in neuropathology?
Five Most Common Problems in Surgical Neuropathology If the brain were so simple that we could understand it, we would be so simple that we couldn t Emerson Pugh What is your greatest difficulty in neuropathology?
USCAP Neuropathology. Case No. 3 Elisabeth J. Rushing, MD Armed Forces Institute of Pathology Washington, DC
 USCAP Neuropathology Case No. 3 Elisabeth J. Rushing, MD Armed Forces Institute of Pathology Washington, DC Clinical history The patient is a 9 year-old boy who has had seizures since age 2, at which time
USCAP Neuropathology Case No. 3 Elisabeth J. Rushing, MD Armed Forces Institute of Pathology Washington, DC Clinical history The patient is a 9 year-old boy who has had seizures since age 2, at which time
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
Joana Ramalho, MD C. Ryan Miller, MD, PhD
 Joana Ramalho, MD C. Ryan Miller, MD, PhD Case 1 3 month old baby girl Presented with new onset of seizures Newborn. Questionable blurring of the gray-white junction within the right occipital lobe. Findings
Joana Ramalho, MD C. Ryan Miller, MD, PhD Case 1 3 month old baby girl Presented with new onset of seizures Newborn. Questionable blurring of the gray-white junction within the right occipital lobe. Findings
Supra- and infratentorial brain tumors from childhood to maternity
 Supra- and infratentorial brain tumors from childhood to maternity What to expect? I am going to show you the characteristic imaging findings of following tumors: Thierry A.G.M. Huisman, MD, FICIS, EQNR
Supra- and infratentorial brain tumors from childhood to maternity What to expect? I am going to show you the characteristic imaging findings of following tumors: Thierry A.G.M. Huisman, MD, FICIS, EQNR
MOLECULAR DIAGNOSTICS OF GLIOMAS
 MOLECULAR DIAGNOSTICS OF GLIOMAS Arie Perry, M.D. Director, Neuropathology Division DIFFUSE GLIOMAS Cell types Astrocytomas (A) Oligodendrogliomas (O) Mixed oligoastrocytoma (MOA) Three WHO grades: II,
MOLECULAR DIAGNOSTICS OF GLIOMAS Arie Perry, M.D. Director, Neuropathology Division DIFFUSE GLIOMAS Cell types Astrocytomas (A) Oligodendrogliomas (O) Mixed oligoastrocytoma (MOA) Three WHO grades: II,
Part 1. Slides 1-38, Rita Alaggio Soft tissue tumors Trondheim 14. mars 2013
 Part 1 Slides 1-38, Rita Alaggio Soft tissue tumors Trondheim 14. mars 2013 Pediatric Pathology Soft Tissue Tumors AN UPDATE Rita Alaggio Azienda Ospedaliera Università di Padova Soft Tissue Tumors More
Part 1 Slides 1-38, Rita Alaggio Soft tissue tumors Trondheim 14. mars 2013 Pediatric Pathology Soft Tissue Tumors AN UPDATE Rita Alaggio Azienda Ospedaliera Università di Padova Soft Tissue Tumors More
We are IntechOpen, the first native scientific publisher of Open Access books. International authors and editors. Our authors are among the TOP 1%
 We are IntechOpen, the first native scientific publisher of Open Access books 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our authors are among the 151 Countries
We are IntechOpen, the first native scientific publisher of Open Access books 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our authors are among the 151 Countries
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Report Disseminated Cerebrospinal Embryonal Tumor in the Adult
 Case Reports in Pathology Volume 2016, Article ID 6785459, 5 pages http://dx.doi.org/10.1155/2016/6785459 Case Report Disseminated Cerebrospinal Embryonal Tumor in the Adult Alessandro Caporlingua, 1 Daniele
Case Reports in Pathology Volume 2016, Article ID 6785459, 5 pages http://dx.doi.org/10.1155/2016/6785459 Case Report Disseminated Cerebrospinal Embryonal Tumor in the Adult Alessandro Caporlingua, 1 Daniele
Nodule Formation and Desmoplasia in Medulloblastomas Defining the Nodular/Desmoplastic Variant and Its Biological Behavior
 RESEARCH ARTICLE DOI 10.1111/j.1750-3639.2007.00058.x Nodule Formation and Desmoplasia in Medulloblastomas Defining the Nodular/Desmoplastic Variant and Its Biological Behavior Charles S. McManamy 1,2
RESEARCH ARTICLE DOI 10.1111/j.1750-3639.2007.00058.x Nodule Formation and Desmoplasia in Medulloblastomas Defining the Nodular/Desmoplastic Variant and Its Biological Behavior Charles S. McManamy 1,2
Pediatric CNS Tumors. Disclosures. Acknowledgements. Introduction. Introduction. Posterior Fossa Tumors. Whitney Finke, MD
 Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
Special slide seminar
 Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls. Rob Macaulay Neuropathologist, MCC October 21, 2017
 Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
Case 1. Clinical history
 Case 1 Case 1 Clinical history 17-month-old boy with a kidney tumor found during routine childhood care program. CT scan showed a solid mass. Chemotherapy was given for 4 weeks using actinomycin D and
Case 1 Case 1 Clinical history 17-month-old boy with a kidney tumor found during routine childhood care program. CT scan showed a solid mass. Chemotherapy was given for 4 weeks using actinomycin D and
Brain Tumors in Children
 Brain Tumors in Children Michael A. Grotzer University Children s Hospital of Zurich, Switzerland Incidence of Childhood Cancer CNS Tumors Acute lymphoblastic Leukemia Neuroblastoma Non-Hodgkin Lymphoma
Brain Tumors in Children Michael A. Grotzer University Children s Hospital of Zurich, Switzerland Incidence of Childhood Cancer CNS Tumors Acute lymphoblastic Leukemia Neuroblastoma Non-Hodgkin Lymphoma
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
The recently updated World Health Organization (WHO)
") REVIEW ARTICLE The Expanding Family of Glioneuronal Tumors Daniela S. Allende, MD and Richard A. Prayson, MD Abstract: Three new entities have been recently added to the group of glioneuronal tumors in
REVIEW ARTICLE The Expanding Family of Glioneuronal Tumors Daniela S. Allende, MD and Richard A. Prayson, MD Abstract: Three new entities have been recently added to the group of glioneuronal tumors in
Pathologic features and clinical outcome of central neurocytoma: analysis of 15 cases
 Original Article Pathologic features and clinical outcome of central neurocytoma: analysis of 15 cases Yu Li, Xiu-Feng Ye, Guo Qian, Yu Yin, Qian-Guan Pan Institute of Neuroscience, Department of Pathology,
Original Article Pathologic features and clinical outcome of central neurocytoma: analysis of 15 cases Yu Li, Xiu-Feng Ye, Guo Qian, Yu Yin, Qian-Guan Pan Institute of Neuroscience, Department of Pathology,
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
ACCME/Disclosures ALK FUSION-POSITIVE MESENCHYMAL TUMORS. Tumor types with ALK rearrangements. Anaplastic Lymphoma Kinase. Jason L.
 Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
BAH1 - Primary Glioblastoma
 BAH1 - Primary Glioblastoma R frontal tumour for frozen section. No known primary. Contrast enhancing lesion. Cholecystectomy. FROZEN SECTION REPORT Right frontal tumour: The specimen consists of multiple
BAH1 - Primary Glioblastoma R frontal tumour for frozen section. No known primary. Contrast enhancing lesion. Cholecystectomy. FROZEN SECTION REPORT Right frontal tumour: The specimen consists of multiple
WHO 2016 CNS Tumor Classification Update. DISCLOSURES (Arie Perry, MD) PATTERN RECOGNITION. Arie Perry, M.D. Director, Neuropathology
 PATTERN RECOGNITION. Arie Perry, M.D. Director, Neuropathology") WHO 2016 CNS Tumor Classification Update Arie Perry, M.D. Director, Neuropathology DISCLOSURES (Arie Perry, MD) I have no financial relationships to disclose. - and - I will not discuss off label use or
WHO 2016 CNS Tumor Classification Update Arie Perry, M.D. Director, Neuropathology DISCLOSURES (Arie Perry, MD) I have no financial relationships to disclose. - and - I will not discuss off label use or
University Journal of Pre and Para Clinical Sciences
 ISSN 2455 2879 Volume 2 Issue 1 2016 Metaplastic carcinoma breast a rare case report Abstract : Metaplastic carcinoma of the breast is a rare malignancy with two distinct cell lines described as a breast
ISSN 2455 2879 Volume 2 Issue 1 2016 Metaplastic carcinoma breast a rare case report Abstract : Metaplastic carcinoma of the breast is a rare malignancy with two distinct cell lines described as a breast
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
2017 Diagnostic Slide Session Case 3
 2017 Diagnostic Slide Session Case 3 Andrew Gao, MD Lili-Naz Hazrati, MD, PhD Cynthia Hawkins, MD, PhD Hospital for Sick Children and University of Toronto, Toronto, Canada Disclosures: none Clinical History
2017 Diagnostic Slide Session Case 3 Andrew Gao, MD Lili-Naz Hazrati, MD, PhD Cynthia Hawkins, MD, PhD Hospital for Sick Children and University of Toronto, Toronto, Canada Disclosures: none Clinical History
A case of multinodular high-grade neuroepithelial tumor
 Brain Tumor Pathol (2011) 28:253 257 DOI 10.1007/s10014-011-0032-6 CASE REPORT A case of multinodular high-grade neuroepithelial tumor with ependymal differentiation Kensaku Kamada Yuko Tanaka Takayuki
Brain Tumor Pathol (2011) 28:253 257 DOI 10.1007/s10014-011-0032-6 CASE REPORT A case of multinodular high-grade neuroepithelial tumor with ependymal differentiation Kensaku Kamada Yuko Tanaka Takayuki
Case #3. USCAP Neuropathology Evening Seminar/Companion Meeting
 Case #3 USCAP Neuropathology Evening Seminar/Companion Meeting Clinical History A 71-year year-old man presented with a 4-4 week history of word finding difficulty. An initial screening head CT followed
Case #3 USCAP Neuropathology Evening Seminar/Companion Meeting Clinical History A 71-year year-old man presented with a 4-4 week history of word finding difficulty. An initial screening head CT followed
No financial or other disclosures
 Case 2014-5 Esther N. Bit-Ivan, DO Northwestern University Jason Wang, MD Jason Park, MD Korgun Koral, MD Children s Medical Center Charles Timmons, MD Veena Rajaram, MD No financial or other disclosures
Case 2014-5 Esther N. Bit-Ivan, DO Northwestern University Jason Wang, MD Jason Park, MD Korgun Koral, MD Children s Medical Center Charles Timmons, MD Veena Rajaram, MD No financial or other disclosures
Histopathological Study and Categorisation of Brain Tumors
 Histopathological Study and Categorisation of Brain Tumors Ruchira Wadhwa 1*, Purvi Patel 2, Hansa Goswami 3 1 Third Year Resident, 2 Assistant Professor, 3 Professor and Head, Department of Pathology,
Histopathological Study and Categorisation of Brain Tumors Ruchira Wadhwa 1*, Purvi Patel 2, Hansa Goswami 3 1 Third Year Resident, 2 Assistant Professor, 3 Professor and Head, Department of Pathology,
Embryonal tumor with multilayered rosettes, C19MC-altered: Report of an extremely rare malignant pediatric central nervous system neoplasm
 745208SCO0010.1177/2050313X17745208SAGE Open Medical Case ReportsTariq et al. case-report2017 Case Report SAGE Open Medical Case Reports Embryonal tumor with multilayered rosettes, C19MC-altered: Report
745208SCO0010.1177/2050313X17745208SAGE Open Medical Case ReportsTariq et al. case-report2017 Case Report SAGE Open Medical Case Reports Embryonal tumor with multilayered rosettes, C19MC-altered: Report
Immunohistochemistry in Bone and Soft Tissue Tumors. Sahar Rassi Zankoul, MD
 Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
CHAPTER 11 Tumors Originating in the Brain Medulloblastomas, PNETs and Ependymomas
 Tumors Originating in the Brain Medulloblastomas, PNETs and Ependymomas Foolishly, I waited 7 months before I joined this (or any) group. By that time, my son had radiation, chemo, and a recurrence of
Tumors Originating in the Brain Medulloblastomas, PNETs and Ependymomas Foolishly, I waited 7 months before I joined this (or any) group. By that time, my son had radiation, chemo, and a recurrence of
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Brain tumors: tumor types
 Brain tumors: tumor types Tumor types There are more than 120 types of brain tumors. Today, most medical institutions use the World Health Organization (WHO) classification system to identify brain tumors.
Brain tumors: tumor types Tumor types There are more than 120 types of brain tumors. Today, most medical institutions use the World Health Organization (WHO) classification system to identify brain tumors.
AMERICAN ASSOCIATION OF NEUROPATHOLOGISTS COMPANION SOCIETY MEETING at the 106 th ANNUAL MEETING OF THE USCAP San Antonio, March 4, 2017
 AMERICAN ASSOCIATION OF NEUROPATHOLOGISTS COMPANION SOCIETY MEETING at the 106 th ANNUAL MEETING OF THE USCAP San Antonio, March 4, 2017 SYLLABUS Papillary Tumor of the Pineal Region and the Differential
AMERICAN ASSOCIATION OF NEUROPATHOLOGISTS COMPANION SOCIETY MEETING at the 106 th ANNUAL MEETING OF THE USCAP San Antonio, March 4, 2017 SYLLABUS Papillary Tumor of the Pineal Region and the Differential
PATHOLOGY OF LIVER TUMORS
 PATHOLOGY OF LIVER TUMORS Pathobasic, 31.05.2016 WHO Classification Approach to a Liver Mass Lesion in a patient with chronic liver disease? Lesion in a patient without chronic liver disease? Malignant
PATHOLOGY OF LIVER TUMORS Pathobasic, 31.05.2016 WHO Classification Approach to a Liver Mass Lesion in a patient with chronic liver disease? Lesion in a patient without chronic liver disease? Malignant
A 25 year old female with a palpable mass in the right lower quadrant of her abdomen
 May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Gangliogliomas: A Report of Five Cases
 Case Report Gangliogliomas: A Report of Five Cases Nair V, Suri VS, Tatke M, Saran RK, Malhotra V, Singh D* Departments of Pathology and *Neurosurgery, G. B. Pant Hospital, New Delhi, India. Correspondence
Case Report Gangliogliomas: A Report of Five Cases Nair V, Suri VS, Tatke M, Saran RK, Malhotra V, Singh D* Departments of Pathology and *Neurosurgery, G. B. Pant Hospital, New Delhi, India. Correspondence
Chapter 1 Introduction
 Chapter 1 Introduction Men think epilepsy divine, merely because they do not understand it. But if they called everything divine which they do not understand, why, there would be no end to divine things.
Chapter 1 Introduction Men think epilepsy divine, merely because they do not understand it. But if they called everything divine which they do not understand, why, there would be no end to divine things.
Case Report Complex Form Variant of Dysembryoplastic Neuroepithelial Tumor of the Cerebellum
 Case Reports in Pathology Volume 2012, Article ID 718651, 4 pages doi:10.1155/2012/718651 Case Report Complex Form Variant of Dysembryoplastic Neuroepithelial Tumor of the Cerebellum Jesús Vaquero, 1,
Case Reports in Pathology Volume 2012, Article ID 718651, 4 pages doi:10.1155/2012/718651 Case Report Complex Form Variant of Dysembryoplastic Neuroepithelial Tumor of the Cerebellum Jesús Vaquero, 1,
1/10/2018. Soft Tissue Tumors Showing Melanocytic Differentiation. Overview. Desmoplastic/ Spindle Cell Melanoma
 2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
ESS: Pathologic Insights
 GEIS XVI INTERNATIONAL SYMPOSIUM Seville 4th October 2018 ESS: Pathologic Insights Sílvia Bagué The Royal Marsden Hospital London (United Kingdom) I have no conflicts of interest Endometrial stromal sarcoma
GEIS XVI INTERNATIONAL SYMPOSIUM Seville 4th October 2018 ESS: Pathologic Insights Sílvia Bagué The Royal Marsden Hospital London (United Kingdom) I have no conflicts of interest Endometrial stromal sarcoma
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis
 Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
3/27/2017. Pulmonary Pathology Specialty Conference. Disclosure of Relevant Financial Relationships. Clinical History:
 Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Anna Maria Buccoliero Department of Biomedicine, Careggi Hospital Florence
 PEDIATRIC RHABDOID MENINGIOMA Anna Maria Buccoliero Department of Biomedicine, Careggi Hospital Florence CLINICAL HISTORY A 3-year-old boy, with a recent history of seizures, was admitted to the Neurosurgery
PEDIATRIC RHABDOID MENINGIOMA Anna Maria Buccoliero Department of Biomedicine, Careggi Hospital Florence CLINICAL HISTORY A 3-year-old boy, with a recent history of seizures, was admitted to the Neurosurgery
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Case 7391 Intraventricular Lesion
 Case 7391 Intraventricular Lesion Bastos Lima P1, Marques C1, Cabrita F2, Barbosa M2, Rebelo O3, Rio F1. 1Neuroradiology, 2Neurosurgery, 3Neuropathology, Coimbra University Hospitals, Portugal. University
Case 7391 Intraventricular Lesion Bastos Lima P1, Marques C1, Cabrita F2, Barbosa M2, Rebelo O3, Rio F1. 1Neuroradiology, 2Neurosurgery, 3Neuropathology, Coimbra University Hospitals, Portugal. University
Case of the month. Dr Charles Bénière, Institut universitaire de pathologie, Lausanne
 Case of the month Dr Charles Bénière, Institut universitaire de pathologie, Lausanne Clinical history 39 years old male, smoker (19 pack-year) without any prior medical record nor professional exposure.
Case of the month Dr Charles Bénière, Institut universitaire de pathologie, Lausanne Clinical history 39 years old male, smoker (19 pack-year) without any prior medical record nor professional exposure.
I have no conflicts of interest in relation to this presentation. Vogel FS & Burger PC 3/28/2016
 IF THIS IS NOT GLIOBLASTOMA, THEN WHAT IS IT? Murat Gokden, MD Department of Pathology/Neuropathology University of Arkansas for Medical Sciences Little Rock, AR mgokden@uams.edu I have no conflicts of
IF THIS IS NOT GLIOBLASTOMA, THEN WHAT IS IT? Murat Gokden, MD Department of Pathology/Neuropathology University of Arkansas for Medical Sciences Little Rock, AR mgokden@uams.edu I have no conflicts of
SUPPLEMENTARY INFORMATION
 VOLUME: 1 ARTICLE NUMBER: 0027 In the format provided by the authors and unedited. Rapid intraoperative histology of unprocessed surgical specimens via fibre-laser-based stimulated Raman scattering microscopy
VOLUME: 1 ARTICLE NUMBER: 0027 In the format provided by the authors and unedited. Rapid intraoperative histology of unprocessed surgical specimens via fibre-laser-based stimulated Raman scattering microscopy
Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor
 Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Disclosures. The Thin Red Line Between Neuropathology and Head & Neck Pathology. Introduction CASE 1. Current Issues Tihan
 Disclosures I have nothing to disclose The Thin Red Line Between Neuropathology and Head & Neck Pathology Tarik Tihan, MD, PhD UCSF, Department of Pathology Neuropathology Division Introduction Three cases
Disclosures I have nothing to disclose The Thin Red Line Between Neuropathology and Head & Neck Pathology Tarik Tihan, MD, PhD UCSF, Department of Pathology Neuropathology Division Introduction Three cases
Case Presentation. Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD. Department of Pathology Jordan University Hospital Amman, Jordan
 Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
The new WHO 2016 classification of brain tumors what neurosurgeons need to know
 DOI 10.1007/s00701-016-3062-3 REVIEW ARTICLE - BRAIN TUMORS The new WHO 2016 classification of brain tumors what neurosurgeons need to know Rouzbeh Banan 1 & Christian Hartmann 1 Received: 8 July 2016
DOI 10.1007/s00701-016-3062-3 REVIEW ARTICLE - BRAIN TUMORS The new WHO 2016 classification of brain tumors what neurosurgeons need to know Rouzbeh Banan 1 & Christian Hartmann 1 Received: 8 July 2016
Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on
 Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on imaging. There is no significant past medical history.
Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on imaging. There is no significant past medical history.
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
Cerebral Parenchymal Lesions: I. Metastatic Neoplasms
 Chapter 4 Cerebral Parenchymal Lesions: I. Metastatic Neoplasms After one has reasonably ruled out the possibility of a nonneoplastic diagnosis (see Chap. 3), one is left with considering a diagnosis of
Chapter 4 Cerebral Parenchymal Lesions: I. Metastatic Neoplasms After one has reasonably ruled out the possibility of a nonneoplastic diagnosis (see Chap. 3), one is left with considering a diagnosis of
International Journal of Pharma and Bio Sciences CHROMOPHOBE VARIANT OF RENAL CELL CARCINOMA MASQUARDING AS RENAL ONCOCYTOMA ON CYTOLOGY.
 Case Report Pathology International Journal of Pharma and Bio Sciences ISSN 0975-6299 CHROMOPHOBE VARIANT OF RENAL CELL CARCINOMA MASQUARDING AS RENAL ONCOCYTOMA ON CYTOLOGY. DR.MAMATHA K*, DR. ARAKERI
Case Report Pathology International Journal of Pharma and Bio Sciences ISSN 0975-6299 CHROMOPHOBE VARIANT OF RENAL CELL CARCINOMA MASQUARDING AS RENAL ONCOCYTOMA ON CYTOLOGY. DR.MAMATHA K*, DR. ARAKERI
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
TUMORS of nervous system
 TUMORS of nervous system By: Shifaa Alqa qa Done By : Ola Hijjawi CNS tumors : The annual incidence of CNS tumors ranges from 10 to 17 per 100,000 persons for intracranial tumors and 1 to 2 per 100,000
TUMORS of nervous system By: Shifaa Alqa qa Done By : Ola Hijjawi CNS tumors : The annual incidence of CNS tumors ranges from 10 to 17 per 100,000 persons for intracranial tumors and 1 to 2 per 100,000
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain
 December 2016 59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain Contributed by: Divya Sharma, MD. Fellow, Gastrointestinal Pathology, Department of Pathology
December 2016 59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain Contributed by: Divya Sharma, MD. Fellow, Gastrointestinal Pathology, Department of Pathology
An Overview of Genital Stromal Tumors
 An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine
An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Oligodendroglioma: imaging findings, radio-pathological correlation and evolution
 Oligodendroglioma: imaging findings, radio-pathological correlation and evolution Poster No.: C-2104 Congress: ECR 2013 Type: Authors: Keywords: DOI: Scientific Exhibit A. Hernandez Castro, M. D. Monedero
Oligodendroglioma: imaging findings, radio-pathological correlation and evolution Poster No.: C-2104 Congress: ECR 2013 Type: Authors: Keywords: DOI: Scientific Exhibit A. Hernandez Castro, M. D. Monedero
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no