Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
|
|
|
- Roland Allen
- 6 years ago
- Views:
Transcription

 of interest to disclose. Differential diagnosis of neuroendocrine carcinoma Problems 1.")

1 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner have, or have had, within the past 12 months, which relates to the content of this educational activity and creates a conflict of interest. Dr. Alain Borczuk declares he/she has no conflict(s) of interest to disclose. Differential diagnosis of neuroendocrine carcinoma Problems 1. Small cell carcinoma vs. large cell neuroendocrine carcinoma Combined small cell or pure large cell neuroendocrine Organ localized small cell carcinoma 2. Adenocarcinoma or large cell neuroendocrine carcinoma 3. Carcinoid tumors and large cell neuroendocrine carcinoma Ki 67, mitoses 4. Mimics of neuroendocrine carcinoma CD56 perils and problems Morphologic imitators What is the problem? Problem 1: Small cell carcinoma vs. large cell neuroendocrine carcinoma vs. Combined small cell Partial sampling Small samples Crush artifact Morphologic overlap 1
 with IHC IHC Panel was variable Often CK, TTF1 and at least one NE marker Small cell carcinoma vs.")
 High recurrence rate Paraneoplastic syndromes rare Peripheral, lobulated>spiculated High PET SUV Smokers Thunnissen E et al J Thorac Oncol. 2017 Feb;12(2):334 346.")
2 Reproducibility in small cell carcinoma diagnosis Images of 79 tumors, mostly neuroendocrine in 3 tiers morphology first tier then increasing number of IHC Moderate agreement (65%) improved to good (78%) with IHC IHC Panel was variable Often CK, TTF1 and at least one NE marker Small cell carcinoma vs. Large cell neuroendocrine carcinoma clinical Small cell carcinoma Advanced disease Paraneoplastic syndrome often Peripheral, early rare High PET SUV Smokers Large cell neuroendocrine Early stage (50%) High recurrence rate Paraneoplastic syndromes rare Peripheral, lobulated>spiculated High PET SUV Smokers Thunnissen E et al J Thorac Oncol Feb;12(2): The Use of Immunohistochemistry Improves the Diagnosis of Small Cell Lung Cancer and Its Differential Diagnosis. An International Reproducibility Study in a Demanding Set of Cases. Small cell carcinoma vs. Large cell neuroendocrine carcinoma pathology Small cell carcinoma vs. Large cell neuroendocrine carcinoma IHC Small cell carcinoma Smaller cells, scant cytoplasm Fine salt and pepper chromatin Nuclear molding Crush artifact Apoptosis frequent Mitoses frequent (?hard to see) Necrosis Large cell neuroendocrine Larger cells, Visible cytoplasm Nucleoli, small (coarse chromatin) Rosettes, palisading (?related to cytoplasm) Apoptosis Mitoses frequent Necrosis Small cell carcinoma Cytokeratin weak, patchy, dot like Up to 10% of cases negative TTF1 90% positive Neuroendocrine markers Often but not always positive CD56 most sensitive Ki 67 high Large cell neuroendocrine Cytokeratin membranous TTF1 50% positive (or higher) Neuroendocrine markers By definition Ki 67 high 2
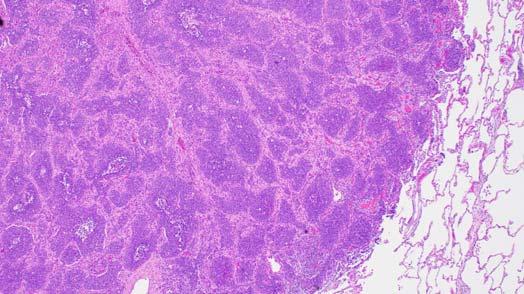


3 3





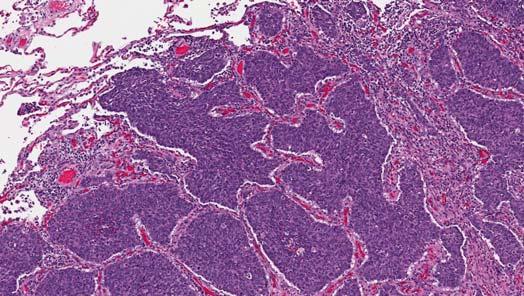
4 Architecture Nuclear morphology Rosette Palisading DO NOT FORGET COMBINED SMALL CELL IS SMALL CELL! LARGE CELL NEUROENDOCRINE AS PART OF COMBINED SMALL CELL CARCINOMA IS COMMON! Problem 1 Small cell ca vs LCNEC Take home lessons Mostly morphologic Don t ignore clinical clues (paraneoplastic syndrome, organ localized) IHC pattern Cytokeratin can reveal dual cell population If Age <40 or more chest wall than lung (see Problem 4!) 4





5 What is the problem? Problem 2: Solid type adenocarcinoma vs. large cell neuroendocrine carcinoma IHC definition of neuroendocrine differentiation NSCLC with neuroendocrine differentiation vs. LCNEC Morphologic overlap What is the key criterion? Solid adenocarcinoma vs. Large cell neuroendocrine carcinoma Solid adenocarcinoma Nuclear chromatin vesicular with macronucleoli Ample cytoplasm TTF1 positive about 70 80% Neuroendocrine markers neuroendocrine differentiation Mitotic rate intermediate Ki 67 intermediate Synaptophysin Large cell neuroendocrine Nuclear chromatin coarse salt and pepper and small nucleoli Visible cytoplasm TTF1 >50% positive Neuroendocrine markers By definition Mitotic rate high Ki 67 high Nuclear? Cytoplasm? Architecture? Nuclear Cytoplasm Architecture Nuclear Cytoplasm Architecture 5










6 PROBLEM: Adenocarcinoma or squamous carcinoma with neuroendocrine differentiation Solid AdCa? LCNEC? Clear cell? TTF1 positive Mucin neg SYN p40 CD56 Synaptophysin Definition of LCNEC Any NAPSIN then not LCNEC P40 squamous Chromogranin Neuroendocrine Molecular story Do criteria for LCNEC determine molecular results? Focal NE staining did not exclude AdenoCA or Squamous CA RESULT: NO KRAS positive tumors Rossi et al Many KRAS positive NSCLC like Overview of key driver mutations and other activating mutations in LCNEC of the lung. KRAS 3 cases (6%) All resected tumors Two of three one NE marker only One combined with AdCa Natasha Rekhtman et al. Clin Cancer Res 2016;22: by American Association for Cancer Research Tomohiro Miyoshi et al. Clin Cancer Res 2017;23: by American Association for Cancer Research 6


? NO!")
7 Solid adenocarcinoma vs. Large cell neuroendocrine carcinoma Solid adenocarcinoma Nuclear chromatin vesicular with nucleoli Ample cytoplasm TTF1 positive about 70 80% Neuroendocrine markers neuroendocrine differentiation Mitotic rate intermediate Ki 67 intermediate Large cell neuroendocrine Nuclear chromatin coarse salt and pepper and small nucleoli Identifiable cytoplasm TTF1 >50% positive Neuroendocrine markers By definition Mitotic rate high Ki 67 high Or in other words. For nucleoli how big is too big? For cytoplasm what is visible versus ample? Solid Adenocarcinoma Did not do neuroendocrine markers (should I have)? NO! Nucleoli +/, vesicular Ample cytoplasm Not architecturally NE KRAS positive Nucleoli Yes, macro Cytoplasm present Architecture no KRAS positive Nucleoli +/ Ample cytoplasm Not architecturally NE KRAS positive 7




8 Nucleoli no Cytoplasm present Palisading some KRAS positive MAYBE? Oops. Did NE markers? Regretted it Nucleoli yes, variable Cytoplasm present Architecture depends on who you ask KRAS positive Synatophysin Problem 2 Solid adenocarcinoma vs. LCNEC SUMMARY Adenocarcinoma, solid predominant Nuclear features, ample cytoplasm, lack of palisading/rosettes LCNEC molecular small cell like Nuclear features, less ample cytoplasm, architecture High mitotic rate/ apoptosis Solid adenocarcinoma with neuroendocrine IHC vs. LCNEC adenocarcinoma like Napsin A and lower mitotic rate/ki 67 = AdCA KRAS rate seems similar Molecular adeno like 8

9 Problem 2 Solid adenocarcinoma vs. LCNEC Take home message LCNEC small cell like criteria as in Problem 1 Molecular is small cell like Blurring between some LCNEC NSCLC like and solid adenocarcinoma Molecular more AdenoCa like Criteria and clinical impact need further study Problem 3: Atypical carcinoid vs. large cell neuroendocrine carcinoma What is the problem? Small samples Mitotic counting Including undercalling carcinoids Ki 67 Atypical carcinoid vs. Large cell neuroendocrine carcinoma Atypical carcinoid Nuclear chromatin salt and pepper and small nucleoli Round nuclei Visible cytoplasm Necrosis Mitotic rate 2 9 in 2mm 2 Ki 67 low/lower Large cell neuroendocrine Nuclear chromatin coarse, salt and pepper and small nucleoli Irregular nuclear contour Visible cytoplasm Necrosis Mitotic rate 10 or greater in 2mm 2 Ki 67 high Mitotic counting IASLC/WHO classification 2015 If initial counts are near the cutoff between categories, then the average of 3 sets of fields must be counted. Impacts lower end more than upper Upper end most LCNEC have many more than 10 in 2mm 2 Ki67 in pulmonary NE tumors TUMOR KI 67 TC AC SCLC LCNEC J Thorac Oncol Mar;9(3):

10 Natasha Rekhtman et al. Clin Cancer Res 2016;22: by American Association for Cancer Research Problem 3 Atypical carcinoid vs. LCNEC Take home messages Careful mitotic counting when possible Ki 67 when small sample Rare LCNEC may arise from atypical carcinoids Problem 4: Mimickers of high grade neuroendocrine carcinomas What is the problem? Not considered at sign out, especially when overlapping epidemiology with small cell carcinoma Presentation in metastatic sites Small samples Rare tumors IHC marker overlap CD56 Cytokeratin Mimics of neuroendocrine carcinoma Primitive neuroectodermal tumor (PNET) Usually under age 40 Chest wall more often than lung Pitfalls Cytokeratin can be positive; calretinin can be positive; CD56 can be positive TTF1 negative, WT1 negative CD99 membranous; FLI1 positive EWSR1 translocations 10

 Neuropil CD99")


11 Mimics of neuroendocrine carcinoma Pulmonary neuroblastoma Pediatric tumors often extra pulmonary Adult tumors can be pulmonary Ganglion cells (ganglioneuroblastoma) Neuropil CD99 Mimics of neuroendocrine carcinoma Pulmonary paraganglioma Rare Depends on definition Any trabecular pattern, spindle or oncocytic carcinoid. Cytokeratin negative S100 sustentacular cells, even if only focal. 11
 Merkel cell carcinoma Wilms tumor Papillary thyroid Carcinoma Medullary thyroid CA Rhabdomyosarcoma")
 Ovarian/endometrial stromal Mesenchymal chondrosarcoma NK cell tumors AML Myeloma Granular cell tumor Solid")


12 CD56 POSITIVE TUMORS Neuroendocrine tumors Non neuroendocrine tumors High rate (>50%) Non neuroendocrine tumors Low rate (25%) Merkel cell carcinoma Wilms tumor Papillary thyroid Carcinoma Medullary thyroid CA Rhabdomyosarcoma Mesothelioma Small cell carcinoma Desmoplastic round cell tumor Paraganglioma/Pheochromo Synovial sarcoma PNET (20%) Ovarian/endometrial stromal Mesenchymal chondrosarcoma NK cell tumors AML Myeloma Granular cell tumor Solid pseudopapillary Panel approach for CD56 positive tumor What trigger? Small cell is unusual (age, location, distribution, non smoker) Morphology is variant or non classical E.g. no crush or molding, rare apoptosis CD56 is the only neuroendocrine marker positive Panel approach for CD56 positive tumor What panel? CD56, Cytokeratin and TTF1 positive combination favors small cell Rare exceptions Add WT1, desmin, SMA or actin/hhf35 Molecular/FISH testing as needed 12

13 Problem 4 mimics of neuroendocrine carcinoma Take home messages High grade pulmonary neuroendocrine tumors ALERTS! Age <40, chest wall, no lung tumor Diagnosis in metastatic site Non smoker Variant histology Immunohistochemistry panels be careful when single NE marker is CD56 Molecular testing/fish testing Armita Bahrami, Luan D. Truong, and Jae Y. Ro (2008) Undifferentiated Tumor: True Identity by Immunohistochemistry. Archives of Pathology & Laboratory Medicine: March 2008, Vol. 132, No. 3, pp
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS
 LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
Neuroendocrine Lung Tumors Myers
 Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Neuroendocrine neoplasms of the lung
 Neuroendocrine neoplasms of the lung M Papotti, L Righi, & M Volante University of Turin at San Luigi Hospital TORINO NETs OF THE LUNG Menu - Spectrum of NE lung tumors - CARCINOID TUMORS - SCLC /LCNEC
Neuroendocrine neoplasms of the lung M Papotti, L Righi, & M Volante University of Turin at San Luigi Hospital TORINO NETs OF THE LUNG Menu - Spectrum of NE lung tumors - CARCINOID TUMORS - SCLC /LCNEC
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
3/27/2017. Pulmonary Pathology Specialty Conference. Disclosure of Relevant Financial Relationships. Clinical History:
 Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens
 is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens") Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens Kartik Viswanathan, M.D., Ph.D New York Presbyterian - Weill
Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens Kartik Viswanathan, M.D., Ph.D New York Presbyterian - Weill
Impact of immunostaining of pulmonary and mediastinal cytology
 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Immunohistochemistry in Bone and Soft Tissue Tumors. Sahar Rassi Zankoul, MD
 Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Disclosure of Relevant Financial Relationships
 Ewing and Ewing like sarcomas Using Genetic Signatures in Refining Small Blue Round Cell Tumor Classification Cristina Antonescu, MD Department of Pathology Disclosure of Relevant Financial Relationships
Ewing and Ewing like sarcomas Using Genetic Signatures in Refining Small Blue Round Cell Tumor Classification Cristina Antonescu, MD Department of Pathology Disclosure of Relevant Financial Relationships
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
ACCME/Disclosures. Diagnosing Mesothelioma in Limited Tissue Samples. Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016
 Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Small (and large) Blue Cell Tumors of the Skull Base
 Blue Cell Tumors of the Skull Base") Small (and large) Blue Cell Tumors of the Skull Base Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Small (and large) Blue Cell Tumors of the Skull Base Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
I have nothing to disclose
 A 47 year old female with multiple lung nodules Disclosure of Relevant Financial Relationships Tamar Giorgadze, MD, PhD Professor of Pathology Medical College of Wisconsin Milwaukee, Wisconsin USCAP requires
A 47 year old female with multiple lung nodules Disclosure of Relevant Financial Relationships Tamar Giorgadze, MD, PhD Professor of Pathology Medical College of Wisconsin Milwaukee, Wisconsin USCAP requires
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Ascitic Fluid and Use of Immunocytochemistry. Mercè Jordà, University of Miami
 Ascitic Fluid and Use of Immunocytochemistry Mercè Jordà, University of Miami Is It Malignant? Yes? No Ascitic Fluid Cytomorphologic Useful Findings Tight clusters with smooth borders Cellular and nuclear
Ascitic Fluid and Use of Immunocytochemistry Mercè Jordà, University of Miami Is It Malignant? Yes? No Ascitic Fluid Cytomorphologic Useful Findings Tight clusters with smooth borders Cellular and nuclear
3/24/2017. Disclosure of Relevant Financial Relationships. Mixed Epithelial Endometrial Carcinoma. ISGyP Endometrial Cancer Project
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Lung Neoplasia II Resection specimens Pathobasic. Lukas Bubendorf Pathology
 Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Case 2. Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset
 Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
3/23/2017. Differentiation: Differentiation: Immunohistochemistry. Well Differentiated vs. Poorly Differentiated Neuroendocrine Neoplasms
 Disclosure Statement When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 Dr. Klimstra receives royalty payments
Disclosure Statement When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 Dr. Klimstra receives royalty payments
Special slide seminar
 Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
EBUS-TBNA Diagnosis and Staging of Lung Cancer
 EBUS-TBNA Diagnosis and Staging of Lung Cancer Nirag Jhala MD, MIAC Professor of Pathology and Lab Med. Director of Anatomic Pathology and Cytopathology Lewis Katz School of Medicine@ Temple University
EBUS-TBNA Diagnosis and Staging of Lung Cancer Nirag Jhala MD, MIAC Professor of Pathology and Lab Med. Director of Anatomic Pathology and Cytopathology Lewis Katz School of Medicine@ Temple University
Small cell lung cancer and large cell neuroendocrine tumours interobserver variability. Michael den Bakker Erasmus MC
 Small cell lung cancer and large cell neuroendocrine tumours interobserver variability Michael den Bakker Erasmus MC PPC London 2007 WEB presentation Pulmonary pathology Club presentation, London, November
Small cell lung cancer and large cell neuroendocrine tumours interobserver variability Michael den Bakker Erasmus MC PPC London 2007 WEB presentation Pulmonary pathology Club presentation, London, November
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000
 Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
ACCME/Disclosures. Case 4 USCAP Pulmonary Panel Case 4 History
 Case 4 USCAP Pulmonary Panel 2016 Andrew Churg, MD Department of Pathology Vancouver General Hospital & University of British Columbia Vancouver, BC achurg@mail.ubc.ca. ACCME/Disclosures The USCAP requires
Case 4 USCAP Pulmonary Panel 2016 Andrew Churg, MD Department of Pathology Vancouver General Hospital & University of British Columbia Vancouver, BC achurg@mail.ubc.ca. ACCME/Disclosures The USCAP requires
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden
 and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden") What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
Pathology Mystery and Surprise
 Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
Thyroid follicular neoplasms in cytology. Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia
 Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Unknown Slides Conference
 Unknown Slides Conference Jae Y. Ro, MD, PhD Weill Medical College of Cornell Univ. The Methodist Hospital, and UT MD Anderson Cancer Center Houston, TX November 9, 2013 Amman, Jordan 25 th Congress of
Unknown Slides Conference Jae Y. Ro, MD, PhD Weill Medical College of Cornell Univ. The Methodist Hospital, and UT MD Anderson Cancer Center Houston, TX November 9, 2013 Amman, Jordan 25 th Congress of
Differential diagnosis of HCC
 Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
The clinically challenging entity of liver metastasis from tumors of unknown primary
 The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
Medullary Thyroid Carcinoma. This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands
 Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Effusion Cytology: Diagnostic Challenges
 Effusion Cytology: Diagnostic Challenges Tarik M. Elsheikh, MD Professor and Medical Director, Anatomic Pathology Cleveland Clinic Outside Consult Case 45 year old woman, presented with nausea, dyspnea,
Effusion Cytology: Diagnostic Challenges Tarik M. Elsheikh, MD Professor and Medical Director, Anatomic Pathology Cleveland Clinic Outside Consult Case 45 year old woman, presented with nausea, dyspnea,
Disclosures. The Thin Red Line Between Neuropathology and Head & Neck Pathology. Introduction CASE 1. Current Issues Tihan
 Disclosures I have nothing to disclose The Thin Red Line Between Neuropathology and Head & Neck Pathology Tarik Tihan, MD, PhD UCSF, Department of Pathology Neuropathology Division Introduction Three cases
Disclosures I have nothing to disclose The Thin Red Line Between Neuropathology and Head & Neck Pathology Tarik Tihan, MD, PhD UCSF, Department of Pathology Neuropathology Division Introduction Three cases
Lung tumors & pleural lesions
 Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Evening Specialty Conference: Cytopathology
 : Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
: Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
Lung Cytology: Lessons Learned from Errors in Practice
 Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms
: Neuroendocrine Neoplasms") When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 David S. Klimstra, MD Chairman, Department of Pathology James
When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 David S. Klimstra, MD Chairman, Department of Pathology James
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
What s New in Pathology of Genitourinary Tumors. Jiaoti Huang, MD, PhD Department of Pathology Duke University School of Medicine
 What s New in Pathology of Genitourinary Tumors Jiaoti Huang, MD, PhD Department of Pathology Duke University School of Medicine Kidney Tumors Multilocular cystic renal neoplasm of low malignant potential
What s New in Pathology of Genitourinary Tumors Jiaoti Huang, MD, PhD Department of Pathology Duke University School of Medicine Kidney Tumors Multilocular cystic renal neoplasm of low malignant potential
Immunohistochemical Profile of Lung Tumors in Image Guided Biopsies
 Original Article DOI: 10.21276/APALM.1342 Immunohistochemical Profile of Lung Tumors in Image Guided Biopsies T. Pavithra 1 *, A. Dhanalakshmi 1, C. Lalitha 1, K.B. Lavanya 1 and S. Shifa 2 Department
Original Article DOI: 10.21276/APALM.1342 Immunohistochemical Profile of Lung Tumors in Image Guided Biopsies T. Pavithra 1 *, A. Dhanalakshmi 1, C. Lalitha 1, K.B. Lavanya 1 and S. Shifa 2 Department
Histology: Its Influence on Therapeutic Decision Making
 Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
Non-Small Cell Lung Carcinoma - Myers
 Role of Routine Histology and Special Testing in Managing Patients with Non- Small Cell Lung Carcinoma Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of
Role of Routine Histology and Special Testing in Managing Patients with Non- Small Cell Lung Carcinoma Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Basaloid Carcinoma of the Lung: A Really Dismal Histologic Variant?
 Carcinoma of the Lung: A Really Dismal Histologic Variant? Dae Joon Kim, MD, Kil Dong Kim, MD, Dong Hwan Shin, MD, Jae Y Ro, MD, and Kyung Young Chung, MD Departments of Thoracic and Cardiovascular Surgery,
Carcinoma of the Lung: A Really Dismal Histologic Variant? Dae Joon Kim, MD, Kil Dong Kim, MD, Dong Hwan Shin, MD, Jae Y Ro, MD, and Kyung Young Chung, MD Departments of Thoracic and Cardiovascular Surgery,
Follicular Derived Thyroid Tumors
 Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas
 Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Associate Professor, Harvard Medical School Boston, MA Disclosures
Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Associate Professor, Harvard Medical School Boston, MA Disclosures
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix
 The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
Disclosure of Relevant Financial Relationships NON-SMALL CELL LUNG CANCER: 70% PRESENT IN ADVANCED STAGE
 MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
Neuroendocrine Carcinoma. Lebanon Neuroendocrine Neoplasms of H&N Nov /7/2011. Broad Classification:
 H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy.
 November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
Diagnosis of lung cancer. Diagnosis Subtyping. Morphologic features Approach to small samples
 Lung Cytology Lung Cytology Pınar Fırat,MD,MIAC Diagnosis of lung cancer Detection of infections Evaluation of interstitial diseases Morphologic features Approach to small samples Lung Cancer Second most
Lung Cytology Lung Cytology Pınar Fırat,MD,MIAC Diagnosis of lung cancer Detection of infections Evaluation of interstitial diseases Morphologic features Approach to small samples Lung Cancer Second most
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
Interesting Cases in Gynecologic Pathology. Michael Ward, MD Surgical Pathology Fellow University of Utah Health Sciences Center Salt Lake City, UT
 Interesting Cases in Gynecologic Pathology Michael Ward, MD Surgical Pathology Fellow University of Utah Health Sciences Center Salt Lake City, UT Case 1 History: 50 year old woman with a uterine mass
Interesting Cases in Gynecologic Pathology Michael Ward, MD Surgical Pathology Fellow University of Utah Health Sciences Center Salt Lake City, UT Case 1 History: 50 year old woman with a uterine mass
Lung/Thoracic Neoplasms. Manish Powari
 Lung/Thoracic Neoplasms Manish Powari Biopsy Techniques in Lung cancer diagnosis Decreased cellularity and architecture; thereby influencing subtyping Thoracotomy, resection VATS biopsy/resection L.node
Lung/Thoracic Neoplasms Manish Powari Biopsy Techniques in Lung cancer diagnosis Decreased cellularity and architecture; thereby influencing subtyping Thoracotomy, resection VATS biopsy/resection L.node
Renal tumours: use of immunohistochemistry & molecular pathology. Dr Lisa Browning John Radcliffe Hospital Oxford
 Renal tumours: use of immunohistochemistry & molecular pathology Dr Lisa Browning John Radcliffe Hospital Oxford Renal tumours: the use of immunohistochemistry & molecular pathology Classification of RCC
Renal tumours: use of immunohistochemistry & molecular pathology Dr Lisa Browning John Radcliffe Hospital Oxford Renal tumours: the use of immunohistochemistry & molecular pathology Classification of RCC
Evening Specialty Conference Bone and Soft Tissue Pathology. Diagnostic pitfalls in bone and soft tissue pathology
 Evening Specialty Conference Bone and Soft Tissue Pathology. Case 1 Elizabeth G Demicco, MD, PhD Mount Sinai Hospital, New York Disclosure of Relevant Financial Relationships USCAP requires that all planners
Evening Specialty Conference Bone and Soft Tissue Pathology. Case 1 Elizabeth G Demicco, MD, PhD Mount Sinai Hospital, New York Disclosure of Relevant Financial Relationships USCAP requires that all planners
Histopathological diagnosis of CUP
 Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Case of the month. Dr Charles Bénière, Institut universitaire de pathologie, Lausanne
 Case of the month Dr Charles Bénière, Institut universitaire de pathologie, Lausanne Clinical history 39 years old male, smoker (19 pack-year) without any prior medical record nor professional exposure.
Case of the month Dr Charles Bénière, Institut universitaire de pathologie, Lausanne Clinical history 39 years old male, smoker (19 pack-year) without any prior medical record nor professional exposure.
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS
 ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
4/17/2015. Case 1. A 37 year old man with a 2.2 cm solitary left thyroid mass.
 Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Breast - ductal carcinoma CK7 ER PR GATA3 Mammaglobin (50-70%) GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2 on all newly diagnosed cases
 GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2 on all newly diagnosed cases") Adrenal cortical carcinoma Inhibin Synap Melan-A Calretinin Vimentin Chromogr CK7 CK20 Breast - ductal carcinoma CK7 ER PR GATA3 Mammaglobin (50-70%) GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2
Adrenal cortical carcinoma Inhibin Synap Melan-A Calretinin Vimentin Chromogr CK7 CK20 Breast - ductal carcinoma CK7 ER PR GATA3 Mammaglobin (50-70%) GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2
Diagnostically Challenging Cases in Gynecologic Pathology
 Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP
 What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
5/1/2009. Squamous Dysplasia/CIS AAH DIPNECH. Adenocarcinoma
 Pathological Assessment of Diagnostic Specimens Keith Kerr Department of Pathology Aberdeen University Medical School Aberdeen Royal Infirmary Foresterhill, Aberdeen, Scotland, UK Tumours of the Lung:
Pathological Assessment of Diagnostic Specimens Keith Kerr Department of Pathology Aberdeen University Medical School Aberdeen Royal Infirmary Foresterhill, Aberdeen, Scotland, UK Tumours of the Lung:
HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY
 HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY 7 TH Annual New York Lung Cancer Symposium Saturday, November 10, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering
HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY 7 TH Annual New York Lung Cancer Symposium Saturday, November 10, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering
3/27/2017. Disclosure of Relevant Financial Relationships
 Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources
 Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
The Panel Approach to Diagnostics. Lauren Hopson International Product Specialist Cell Marque Corporation
 The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
NO DISCLOSURES. 1. Incipient neoplasia: Dysplasia/Tis NEUROENDOCRINE TUMORS OF THE GI AND PANCREATOBILIARY TRACT
 3002: CYTO- HISTOLOGY OF NEUROENDOCRINE NEOPLASMS OF LUNG, GASTROINTESTINAL TRACT AND PANCREAS Momin Siddiqui, MD, FIAC Professor Divisional Director and Chief of Cytopathology Emory University Hospital
3002: CYTO- HISTOLOGY OF NEUROENDOCRINE NEOPLASMS OF LUNG, GASTROINTESTINAL TRACT AND PANCREAS Momin Siddiqui, MD, FIAC Professor Divisional Director and Chief of Cytopathology Emory University Hospital
Disclosure of Relevant Financial Relationships
 Evening Specialty Conference - Genitourinary Pathology Case 2 Disclosure of Relevant Financial Relationships Sean R Williamson, MD Henry Ford Health System, Detroit, MI @Williamson_SR USCAP requires that
Evening Specialty Conference - Genitourinary Pathology Case 2 Disclosure of Relevant Financial Relationships Sean R Williamson, MD Henry Ford Health System, Detroit, MI @Williamson_SR USCAP requires that
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Histopathology of NSCLC, IHC markers and ptnm classification
 ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
Combined Large Cell Neuroendocrine Carcinoma and Spindle Cell Carcinoma of the Lung
 Case Reports Jpn J Clin Oncol 2011;41(6)797 802 doi:10.1093/jjco/hyr034 Advance Access Publication 16 March 2011 Combined Large Cell Neuroendocrine Carcinoma and Spindle Cell Carcinoma of the Lung Taichiro
Case Reports Jpn J Clin Oncol 2011;41(6)797 802 doi:10.1093/jjco/hyr034 Advance Access Publication 16 March 2011 Combined Large Cell Neuroendocrine Carcinoma and Spindle Cell Carcinoma of the Lung Taichiro
A Century of observations
 PARAGANGLIOMAS OF THE HEAD & NECK: AN OVERVIEW Michelle D. Williams, MD Associate Professor Dept. of Pathology Head & Neck Section UT MD Anderson Cancer Center Disclosure of Relevant Financial Relationships
PARAGANGLIOMAS OF THE HEAD & NECK: AN OVERVIEW Michelle D. Williams, MD Associate Professor Dept. of Pathology Head & Neck Section UT MD Anderson Cancer Center Disclosure of Relevant Financial Relationships
Financial disclosures
 An update on immunohistochemical markers in mesenchymal neoplasms By Konstantinos Linos MD, FCAP, FASDP Assistant Professor of Pathology Geisel School of Medicine at Dartmouth Dartmouth-Hitchcock Medical
An update on immunohistochemical markers in mesenchymal neoplasms By Konstantinos Linos MD, FCAP, FASDP Assistant Professor of Pathology Geisel School of Medicine at Dartmouth Dartmouth-Hitchcock Medical
PITFALLS AND TRAPS IN THE DIAGNOSIS AND STAGING OF RENAL TUMOURS OF CHILDHOOD. Gordan M. Vujanić Cardiff, U.K.
 PITFALLS AND TRAPS IN THE DIAGNOSIS AND STAGING OF RENAL TUMOURS OF CHILDHOOD Gordan M. Vujanić Cardiff, U.K. RENAL TUMOURS OF CHILDHOOD - CLASSIFICATION (2016) Nephroblastic tumours Mesenchymal tumours
PITFALLS AND TRAPS IN THE DIAGNOSIS AND STAGING OF RENAL TUMOURS OF CHILDHOOD Gordan M. Vujanić Cardiff, U.K. RENAL TUMOURS OF CHILDHOOD - CLASSIFICATION (2016) Nephroblastic tumours Mesenchymal tumours
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Biopsy diagnosis of renal tumors. Current applications Ondřej Hes Department of Pathology Charles University and University Hospital Plzeň Czech Republic Dealing
Enterprise Interest Nothing to declare Biopsy diagnosis of renal tumors. Current applications Ondřej Hes Department of Pathology Charles University and University Hospital Plzeň Czech Republic Dealing
Cutaneous metastases. Thaddeus Mully. University of California, San Francisco Professor, Departments of Pathology and Dermatology
 Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia
 Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia Sílvia Bagué Servei de Patologia Hospital de Sant Pau Barcelona Soft tissue sarcomas Heterogeneous group
Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia Sílvia Bagué Servei de Patologia Hospital de Sant Pau Barcelona Soft tissue sarcomas Heterogeneous group
Cerebral Parenchymal Lesions: I. Metastatic Neoplasms
 Chapter 4 Cerebral Parenchymal Lesions: I. Metastatic Neoplasms After one has reasonably ruled out the possibility of a nonneoplastic diagnosis (see Chap. 3), one is left with considering a diagnosis of
Chapter 4 Cerebral Parenchymal Lesions: I. Metastatic Neoplasms After one has reasonably ruled out the possibility of a nonneoplastic diagnosis (see Chap. 3), one is left with considering a diagnosis of
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as