Head and Neck Reirradiation: Perils and Practice
|
|
|
- Anastasia West
- 6 years ago
- Views:
Transcription
1 Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital
2 Conflicts of Interest No conflicts of interest
3 Introduction Radiotherapy (RT) and chemoradiotherapy (CRT) have become established as standard treatment options in head and neck cancer Locoregional failure rates are still high
4 Locoregional Failure Rates Trial Site Treatment LRR Failure Standard 59.1% (5 y) RTOG All except NP Accelerated 51.2% (5 y) Hyperfrac 51.7% (5 y) RTOG Larynx PF RT CRT 36% (2 y) 20% (2 y) RTOG All except NP CRT A-CRT 28% 31% TAX 324 All except NP PF CRT TPF CRT 38% 30% GORTEC Oropharynx RT CRT 75% (5 y) 52% (5 y)

5 Fundamental Problem TUMOR TREATMENT
6 Risks of Reirradiation Acute and chronic dysphagia Osteoradionecrosis/soft tissue necrosis Trismus/fibrosis Carotid rupture 6-7 weeks of treatment plus 2-3 months of recovery
7 Not All Recurrences Are Equal Chemoradio-resistance True recurrent (i.e. resistant) disease vs. second primary In-field failure (i.e. resistant) vs. marginal/out-of-field miss Surgical resectability Performance status
8 Early Experience Institut Gustave-Roussy (De Crevoisier et al, 1993) 169 patients with unresectable disease in irradiated field 3 different RT regimens Daily RT (2 Gy/fx) alone Chicago protocol (4-7 weekly cycles) BID RT with chemotherapy
9 Institut Gustave-Roussy Results Median survival: 10 months 2-year overall survival: 21% 5-year overall survival: 9% Patterns-of-failure Local only: 53% Nodal only: 20% Metastatic only: 7% Local and nodal: 8% Locoregional and metastatic: 12%
10 Toxicity Acute Grade 3 mucositis: 32% Grade 4 mucositis: 14% Late Grade 2/3 cervical fibrosis: 41% Mucosal necrosis: 21% Mild-severe trismus: 30% Osteonecrosis: 8% 5 deaths due to carotid hemorrhage
11 University of Chicago Data Salama et al, reirradiated patients treated on serial phase I-II protocols between Treatment paradigm 5 days of chemort, 9 day break x 4-7 cycles Chemotherapy: 5-FU, HU +/- 3 rd agent RT: daily (1.8 2 Gy/fx) or BID (1.5 Gy/fx)
12 Results Overall survival Median 11 months 3-year: 22% Patterns of failure 42% any locoregional 29% any metastatic
13 Toxicity 19 patients (17%) died of treatmentrelated toxicity 9 during treatment 4 sepsis 3 respiratory arrest 1 carotid blowout 1 pulmonary embolism 10 patients after treatment 4 carotid blowout 1 massive epistaxis 1 soft tissue necrosis
14 Toxicity 13 patients (11%) required surgery for osteoradionecrosis 57% of patients dependent on gastrostomy 1 myelopathy
15 Prognostic Factors Favorable for OS, PFS, and LRC Surgery Increasing radiation dose Triple-agent chemotherapy Favorable for OS and PFS PS 0-1 Favorable for DM Triple-agent chemotherapy
16 Recent Series University of Michigan (Popovtzer et al, 2009) 66 patients treated with 3D-CRT or IMRT 54% daily, 46% BID Median re-rt dose: 68 Gy PTV margin: 5 mm on GTV 71% received concurrent chemotherapy
17 Results Overall survival 2-year: 40% 5-year: 22% Locoregional progression-free survival 2-year actuarial: 27% 5-year actuarial: 19% Total: 71% locoregional failure
18 Failure Patterns 46 patients (71%) had locoregional failure 96% in-field (within 95% isodose line) 4% out-of-field 18 patients (27%) had distant metastasis 15 (83%) also had locoregional failure
19 Toxicity Late grade 3-5 complications: 19 patients (29%) 12 patients (18%) long-term gastrostomy 2 patients with stricture 2 patients chrondronecrosis 1 patient temporal lobe necrosis 3 patients tracheostomy dependent 2 carotid blowouts (neither lethal)
20 Moffitt Experience Tanvetyanon et al, patients treated with reirradiation Median reirradiation dose: 60 Gy 46 patients underwent salvage surgery 70% received concurrent chemotherapy Overall survival: median 19.3 months 1-year: 64.8% 2-year: 40.0%
21 Toxicity Acute: 43.7% developed at least 1 > g3 toxicity (GI 40%) Late: 47.5% developed at least 1 > g3 toxicity
22 Prognostic Factors Charlson comorbidity index No comorbity: median survival 22.6 mo > 1 comorbidity: median survival 12.8 mo Organ dysfunction Absent: median survival 30.7 mo Present: median survival 11.3 mo Comorbidity and organ dysfunction None: median survival 59.6 months Both: median survival 16.5 months
23 Multivariable Analysis Favorable prognostic variables Increased time since prior RT No organ dysfunction No comorbidity Smaller T stage Smaller tumor bulk after surgery Reirradiation dose
24 Nomogram
25 Phase III Trial of Reirradiation Institution: GETTC and GORTEC Eligibility Prior RT (at least 45 Gy) Deep infiltration of tumor KPS > 70 No severe sequelae after first RT R0 or R1 salvage surgery without woundhealing complications Treatment Observation versus chemoradiotherapy
26 Treatment Regimen 5 days in a row: 2 Gy RT per day with concurrent hydroxyurea and continuous infusion 5-FU 9 day break Total of 6 cycles Treatment summary: 11 weeks 60 Gy
27 Results 130 patients randomized between 1999 and 2005
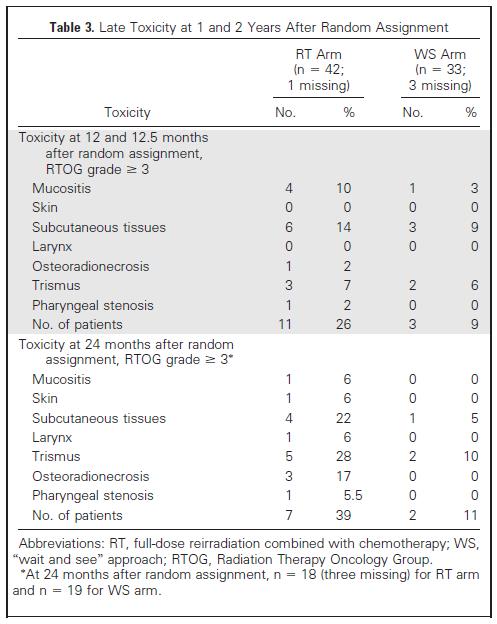
28 Toxicity
29 Conclusions In patients who undergo salvage surgery, repeat CRT have substantially reduced locoregional failure Does not translate into survival benefit Associated with significant toxicity BUT morbidity of recurrence not considered
30 DFCI Experience Retrospective study of patients treated at Dana-Farber Cancer Institute with IMRTbased reirradiation Eligibility History of definitive or adjuvant RT for squamous cell carcinoma of the head and neck Diagnosis of recurrent or second primary squamous cell carcinoma Treated at DFCI with IMRT with radical intent between August 2004 and December 2008 Analyzed October patients met criteria
31 Recurrence Characteristics Age at recurrence (median, IQR) ECOG Perfomance Status Prior disease-free interval (median, IQR) Diagnosis Nasopharynx Oropharynx Oral cavity Larynx/hypopharynx Neck failure only Stage I II III IV Number (%) 57 years (51-63 years) 18 (51%) 16 (46%) 1 (3%) 2.5 years ( years) 2 (6%) 7 (20%) 4 (11%) 13 (37%) 9 (26%) 0 6 (17%) 7 (20%) 22 (63%)
32 Treatment Characteristics Treatment regimen Surgery plus CRT Definitive CRT Induction chemotherapy plus CRT Concurrent chemotherapy Platinum alone Platinum/taxane Platinum/cetuximab Platinum/taxane/cetuximab Cetuximab alone Radiation PTV dose (median, IQR) - No prophylactic nodal RT Number (%) 17 (49%) 8 (23%) 10 (28%) 10 (29%) 10 (29%) 6 (17%) 6 (17%) 3 (8%) 60 Gy (60-64 Gy)
33 Survival Median F/U: 2.3 years (IQR years) Minimum F/U 9 months Overall survival 1-year: 59% 2-year: 48% Median: 1.9 years Locoregional progression-free survival 1-year: 67% 2-year: 67% Distant metastasis-free survival 1-year: 85% 2-year: 73%
34 Patterns-of-Failure 14 total recurrences 7 (50%) first developed locoregional recurrence 4 (29%) first developed distant metastasis 3 (21%) developed simultaneous locoregional and distant failure
35 Local Recurrence Patterns 11 patients developed locoregional recurrence 8 (73%) in-field 2 (18%) out-of-field 1 (9%) both in- and out-of-field All 3 out-of-field failures occurred in nodal basins Out of entire population 26% developed in-field recurrence
36 Acute Toxicity 91% developed at least one grade 3 or 4 toxicity 15 (43%) grade 3 or 4 mucositis 11 (32%) grade 3 or 4 dermatitis 1 emergent tracheostomy 5 (14%) developed acute grade 4 toxicity 14 patients (40%) developed more than 1 grade 3 or 4 toxicity 31 (91%) patients had gastrostomy
37 Late Toxicity 16 patients (46%) developed grade 3 or higher late toxicity Necrosis: 4 (12%) Respiratory: 5 (15%) Skin: 4 (12%) Trismus: 4 (11%) 9 patients (26%) developed more than one grade 3 or 4 late toxicity
38 Treatment-Related Mortality Four deaths in patients with no evidence of disease 1 clearly related to treatment 1 fatal oropharyngeal hemorrhage (10 months) 3 possibly related to treatment 2 aspiration events (8 months and 2.6 years) 1 persistent infection leading to debilitation and hospice (6 months)
39 Gastrostomy Tube Outcomes 55% (17/31) of patients had PEG removed at median 3 months after RT (IQR, months) Of all patients surviving 1 year, 78% (16/18) were free from PEG-dependence Of all patients surviving 2 years, 89% (8/9) were free from PEG-dependence
40 Treatment Paradigm Question #1 Can this be surgically resected with a functionally-acceptable outcome? Question #2 Is this resistant disease? Evidence Time since completion of RT In-field vs. marginal or out-of-field miss
41 Treatment Paradigm Question #3 What are the complications of reirradiation? Swallowing Hemorrhage Myelitis Osteonecrosis
42 Balance Treatment-related toxicity Tumor-related morbidity
43 Clinical Example 68 yo woman who developed 2 cm soft palate mass in October 2008 Past Medical History HTN, T2DM, COPD, h/o ARDS, prosthetic aortic valve Treatment 68.4 Gy with weekly carboplatin
44 Follow-Up Restaging PET-CT in May 2008 disclosed enlarged JD node Clinical exam also showed right soft palate lesion Palate biopsy: undifferentiated carcinoma
45 Three Questions Question #1: Surgically resectable? Answer: Yes June 2009: Transoral resection plus right modified radical neck dissection Pathology Palate: 5 mm grade 2 SqCC, ~4 mm margin Neck: 2.4 cm mass in level 2 with ECE 1 additional node in level 2
46 Is Reirradiation Feasible? Question 2: Is this resistant disease? Answer: Yes Reason 1: Recurrence presented ~ 4 months from treatment Reason 2: In-field failure Always look at original plan

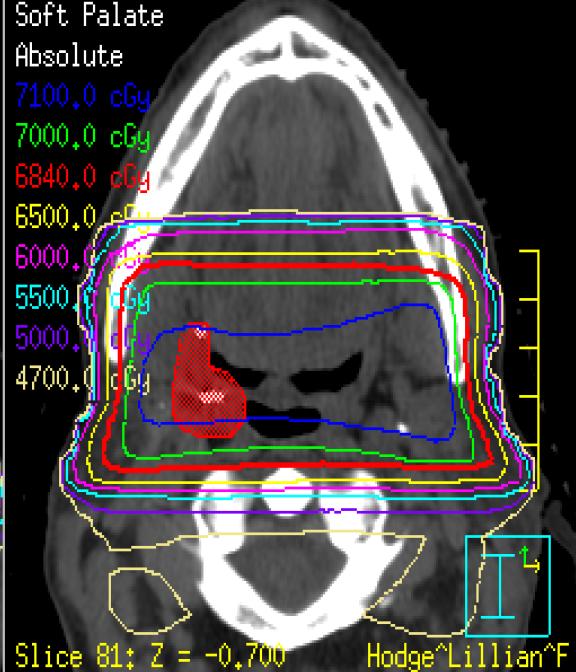
47 Prior RT Plan
48 Recommendation Question 3: Complications of reirradiation Answer: Potentially severe Carotid blowout (prior surgery, prior dose) Oropharyngeal hemorrhage Permanent dysphagia Recommendation: Best supportive care
49 Clinical Example 74 yo man who developed T4N2b left base-of-tongue SqCC in 1996 Past Medical History Atrial fibrillation, HTN, hyperlipidemia Treatment TPFL induction chemotherapy 72 Gy to primary and bilateral neck
50 Recurrence March 2009: coughing with food Clinical examination: Cratered tumor with large, hard margins, extending towards vallecula Biopsy of tongue and pharyngeal wall Squamous cell carcinoma, HPV-negative
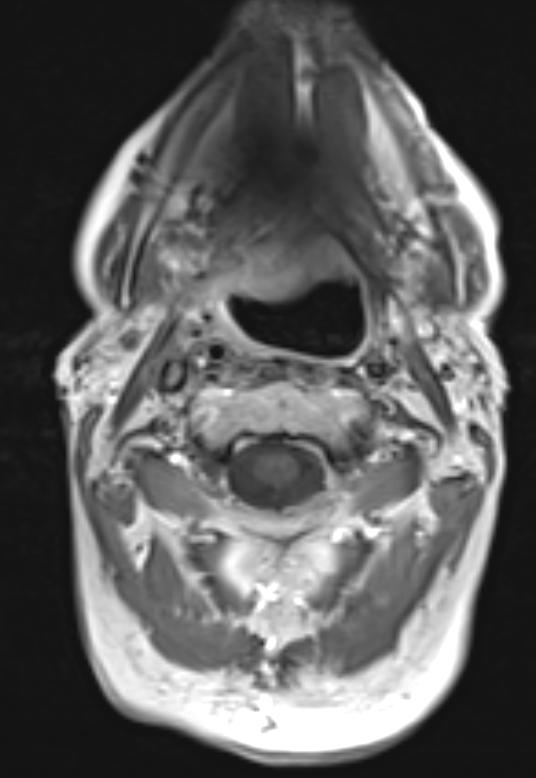

51 Imaging
52 Three Questions Question #1: Surgically resectable? Answer: Not without profound functional compromise Patient refused Question #2: Is this resistant disease? Answer: No Original treatment 13 years ago!
53 Recommendation Question 3: Complications of reirradiation Answer: Modest Oropharyngeal hemorrhage Permanent dysphagia Complications of tumor progression? Certain oropharyngeal hemorrhage Certain permanent dysphagia Recommendation: chemoradiotherapy Concurrent carboplatin, paclitaxel, cetuximab
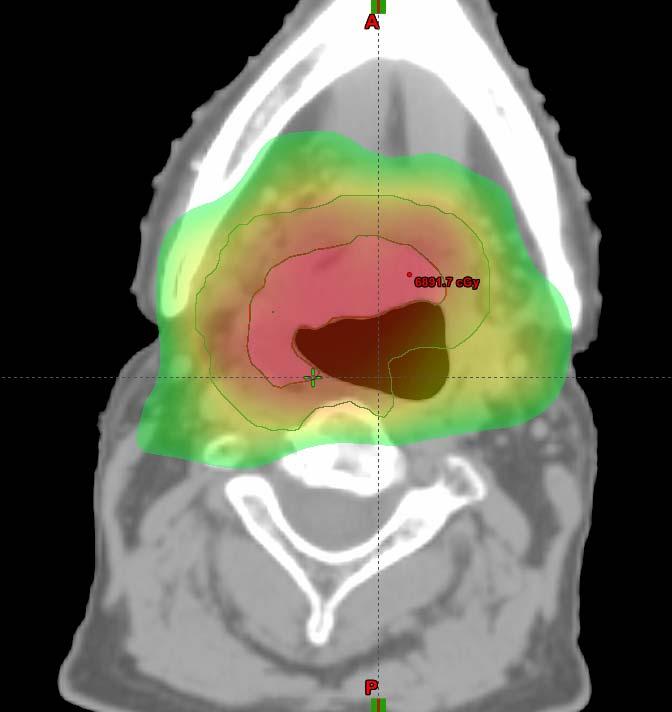

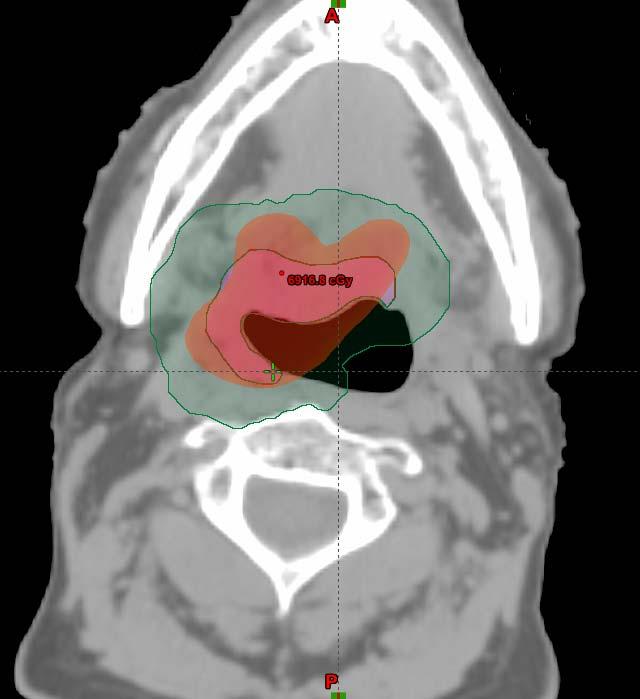
54 Radiotherapy Plan Gy 66 Gy Gy PTV 66 PTV 54
55 Follow-Up NED 8 months following reirradiation Persistent PEG-dependence No other significant grade 3 toxicities
56 Conclusions There is a non-trivial cohort of patients with recurrence who can be salvaged Trimodality therapy is associated with optimal outcomes Reirradiation is associated with substantial acute and late toxicity Must carefully balance risks and benefits of treatment and inaction
57 Questions? Contact information
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer
 Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer
 to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer") The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
Emerging Role of Immunotherapy in Head and Neck Cancer
 Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
Nasopharynx Cancer. 1 Feb Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar)
 Dr Peter Luk (Pathology Registrar)") Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck. Mei Tang, MD
 Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations
 Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221. Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS
 Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Re-irradiation with or without chemotherapy. Jozsef Lövey National Institute of Oncology, Budapest, Hungary
 Re-irradiation with or without chemotherapy Jozsef Lövey National Institute of Oncology, Budapest, Hungary Disclosures Occasional advisory board and educational activity to Merck, Roche, Nutricia, Takeda,
Re-irradiation with or without chemotherapy Jozsef Lövey National Institute of Oncology, Budapest, Hungary Disclosures Occasional advisory board and educational activity to Merck, Roche, Nutricia, Takeda,
TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy
 TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy Anurag K. Singh, MD Professor of Medicine University at Buffalo School of Medicine Professor of Oncology Director of Radiation Research Roswell Park
TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy Anurag K. Singh, MD Professor of Medicine University at Buffalo School of Medicine Professor of Oncology Director of Radiation Research Roswell Park
Self-Assessment Module 2016 Annual Refresher Course
 LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
REIRRADIATION OF HEAD & NECK TARGETS
 REIRRADIATION OF HEAD & NECK TARGETS WORKSHOP-Current challenges of patient re-irradiation 6-7 september 2018, Stockholm, Sweden Claes Mercke Karolinska Institute and Karolinska University Hospital STOCKHOLM
REIRRADIATION OF HEAD & NECK TARGETS WORKSHOP-Current challenges of patient re-irradiation 6-7 september 2018, Stockholm, Sweden Claes Mercke Karolinska Institute and Karolinska University Hospital STOCKHOLM
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Nasopharyngeal Cancer/Multimodality Treatment
 Nasopharyngeal Cancer/Multimodality Treatment PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 22/10/2016 1 st Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
Nasopharyngeal Cancer/Multimodality Treatment PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 22/10/2016 1 st Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
State of the art for radiotherapy of SCCHN
 State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
Adjuvant Therapy in Locally Advanced Head and Neck Cancer. Ezra EW Cohen University of Chicago. Financial Support
 Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Oral Cavity Cancer Combined modality therapy
 Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS
 MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
RTOG Lung Cancer Committee 2012 Clinical Trial Update. Wally Curran RTOG Group Chairman
 RTOG Lung Cancer Committee 2012 Clinical Trial Update Wally Curran RTOG Group Chairman 1 RTOG Lung Committee: Active Trials Small Cell Lung Cancer Limited Stage (Intergroup Trial) Extensive Stage (RTOG
RTOG Lung Cancer Committee 2012 Clinical Trial Update Wally Curran RTOG Group Chairman 1 RTOG Lung Committee: Active Trials Small Cell Lung Cancer Limited Stage (Intergroup Trial) Extensive Stage (RTOG
Head and Neck cancer
 Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
SALIVARY GLAND TUMORS TREATED WITH ADJUVANT INTENSITY-MODULATED RADIOTHERAPY WITH OR WITHOUT CONCURRENT CHEMOTHERAPY
 doi:10.1016/j.ijrobp.2010.09.042 Int. J. Radiation Oncology Biol. Phys., Vol. 82, No. 1, pp. 308 314, 2012 Copyright Ó 2012 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/$ - see front
doi:10.1016/j.ijrobp.2010.09.042 Int. J. Radiation Oncology Biol. Phys., Vol. 82, No. 1, pp. 308 314, 2012 Copyright Ó 2012 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/$ - see front
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Head and Neck Cancer:
 Head and Neck Cancer: Robert Haddad M.D. Clinical Director Head and Neck Oncology Program Dana Farber Cancer Institute Boston, MA Predictive Biomarkers: HPV Abstract 6003: Survival Outcomes By HPV Status
Head and Neck Cancer: Robert Haddad M.D. Clinical Director Head and Neck Oncology Program Dana Farber Cancer Institute Boston, MA Predictive Biomarkers: HPV Abstract 6003: Survival Outcomes By HPV Status
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER
 CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Service Line: Rapid Response Service Version: 1.0 Publication Date: Month XX, 2017 Report Length: 79 Pages
 CADTH RAPID RESPONSE REPORT: SYSTEMATIC REVIEW Treatments for Locally Advanced Oropharyngeal Cancer: A Systematic Review of Clinical Effectiveness and Cost- Effectiveness Service Line: Rapid Response Service
CADTH RAPID RESPONSE REPORT: SYSTEMATIC REVIEW Treatments for Locally Advanced Oropharyngeal Cancer: A Systematic Review of Clinical Effectiveness and Cost- Effectiveness Service Line: Rapid Response Service
Accepted 12 August 2010 Published online 15 December 2010 in Wiley Online Library (wileyonlinelibrary.com). DOI: /hed.21624
. DOI: /hed.21624") ORIGINAL ARTICLE IMPACT OF EARLY PERCUTANEOUS ENDOSCOPIC GASTROSTOMY TUBE PLACEMENT ON NUTRITIONAL STATUS AND HOSPITALIZATION IN PATIENTS WITH HEAD AND NECK CANCER RECEIVING DEFINITIVE CHEMORADIATION THERAPY
ORIGINAL ARTICLE IMPACT OF EARLY PERCUTANEOUS ENDOSCOPIC GASTROSTOMY TUBE PLACEMENT ON NUTRITIONAL STATUS AND HOSPITALIZATION IN PATIENTS WITH HEAD AND NECK CANCER RECEIVING DEFINITIVE CHEMORADIATION THERAPY
Neoplasie del laringe Diagnosi e trattamento
 Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
3/12/2018. Head & Neck Cancer Review INTRODUCTION
 Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
SAMO MASTERCLASS HEAD & NECK CANCER. Nicolas Mach, PD Geneva University Hospital
 SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
Nasopharyngeal Cancer:Role of Chemotherapy
 Nasopharyngeal Cancer:Role of Chemotherapy PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 16/9/2017 2 nd Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
Nasopharyngeal Cancer:Role of Chemotherapy PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 16/9/2017 2 nd Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
External Beam Radiation Therapy for Thyroid Cancer
 External Beam Radiation Therapy for Thyroid Cancer C. Jillian Tsai, M.D, PH.D. Assistant Attending Director of Head and Neck Cancer Research Department of Radiation Oncology Memorial Sloan Kettering Cancer
External Beam Radiation Therapy for Thyroid Cancer C. Jillian Tsai, M.D, PH.D. Assistant Attending Director of Head and Neck Cancer Research Department of Radiation Oncology Memorial Sloan Kettering Cancer
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer. Dr P Vijay Anand Reddy Director Apollo Cancer Hospital
 Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER
 ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER Vasu Divi, MD, 1 * Francis P. Worden, MD, 1,2 * Mark E. Prince, MD, 1 Avraham Eisbruch, MD, 3 Julia S. Lee, MD, 4
ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER Vasu Divi, MD, 1 * Francis P. Worden, MD, 1,2 * Mark E. Prince, MD, 1 Avraham Eisbruch, MD, 3 Julia S. Lee, MD, 4
Concurrent chemoradiotherapy for N2 or N3 squamous cell carcinoma of the head and neck from an occult primary
 Original article Annals of Oncology 14: 1306 1311, 2003 DOI: 10.1093/annonc/mdg330 Concurrent chemoradiotherapy for N2 or N3 squamous cell carcinoma of the head and neck from an occult primary A. Argiris
Original article Annals of Oncology 14: 1306 1311, 2003 DOI: 10.1093/annonc/mdg330 Concurrent chemoradiotherapy for N2 or N3 squamous cell carcinoma of the head and neck from an occult primary A. Argiris
Disclosure. Access 10/4/2013. The emerging role of TransOralRobotic Surgery (TORS) Organ preservation in the management of head and neck cancer
 Organ preservation in the management of head and neck cancer") Disclosure The emerging role of TransOralRobotic Surgery (TORS) Intuitive Surgical, Inc. Proctor/Honoraria Eddie Méndez, MD, MS, FACS Associate Professor, Department of Otolaryngology: Head & Neck Surgery
Disclosure The emerging role of TransOralRobotic Surgery (TORS) Intuitive Surgical, Inc. Proctor/Honoraria Eddie Méndez, MD, MS, FACS Associate Professor, Department of Otolaryngology: Head & Neck Surgery
Treatments for Locally Advanced Oropharyngeal Cancer: A Systematic Review of Clinical Effectiveness and Cost-Effectiveness
 CADTH RAPID RESPONSE REPORT: SYSTEMATIC REVIEW Treatments for Locally Advanced Oropharyngeal Cancer: A Systematic Review of Clinical Effectiveness and Cost-Effectiveness Service Line: Rapid Response Service
CADTH RAPID RESPONSE REPORT: SYSTEMATIC REVIEW Treatments for Locally Advanced Oropharyngeal Cancer: A Systematic Review of Clinical Effectiveness and Cost-Effectiveness Service Line: Rapid Response Service
EFFICACY OF NECK DISSECTION FOR LOCOREGIONAL FAILURES VERSUS ISOLATED NODAL FAILURES IN NASOPHARYNGEAL CARCINOMA
 ORIGINAL ARTICLE EFFICACY OF NECK DISSECTION FOR LOCOREGIONAL FAILURES VERSUS ISOLATED NODAL FAILURES IN NASOPHARYNGEAL CARCINOMA Raymond King Yin Tsang, FRCSEd, Joseph Chun Kit Chung, MRCSEd, Yiu Wing
ORIGINAL ARTICLE EFFICACY OF NECK DISSECTION FOR LOCOREGIONAL FAILURES VERSUS ISOLATED NODAL FAILURES IN NASOPHARYNGEAL CARCINOMA Raymond King Yin Tsang, FRCSEd, Joseph Chun Kit Chung, MRCSEd, Yiu Wing
Survey of Laryngeal Cancer at SBUH comparing 108 cases seen here from to the NCDB of 9,256 cases diagnosed nationwide in 2000
 Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
The management of advanced supraglottic and
 ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
Management of metastatic squamous cell carcinoma cervical lymphadenopathy with occult primary The role of surgery
 Management of metastatic squamous cell carcinoma cervical lymphadenopathy with occult primary The role of surgery Dr Gary Fetter General surgeon Waterfall City Hospital Midrand Excalibur II Garable Lector
Management of metastatic squamous cell carcinoma cervical lymphadenopathy with occult primary The role of surgery Dr Gary Fetter General surgeon Waterfall City Hospital Midrand Excalibur II Garable Lector
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive tract: assessment and management in people aged 16 and over
 Cancer of the upper aerodigestive tract: assessment and management in people aged and over NICE guideline Draft for consultation, March 0 This guideline covers This guideline covers assessing and managing
Cancer of the upper aerodigestive tract: assessment and management in people aged and over NICE guideline Draft for consultation, March 0 This guideline covers This guideline covers assessing and managing
REIRRADIATION WITH INTENSITY-MODULATED RADIOTHERAPY IN RECURRENT HEAD AND NECK CANCER
 ORIGINAL ARTICLE REIRRADIATION WITH INTENSITY-MODULATED RADIOTHERAPY IN RECURRENT HEAD AND NECK CANCER Felix Zwicker, MD, 1,2 Falk Roeder, MD, 1,2 Henrik Hauswald, MD, 1 Christian Thieke, MD, PhD, 2 Carmen
ORIGINAL ARTICLE REIRRADIATION WITH INTENSITY-MODULATED RADIOTHERAPY IN RECURRENT HEAD AND NECK CANCER Felix Zwicker, MD, 1,2 Falk Roeder, MD, 1,2 Henrik Hauswald, MD, 1 Christian Thieke, MD, PhD, 2 Carmen
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma
 Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Protons for Head and Neck Cancer. William M Mendenhall, M.D.
 Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Cancer of the Head and Neck and. HPV Infection. Andrew Urquhart MD, FACS Dept. Otolaryngology/Head and Neck Surgery Marshfield Clinic
 Cancer of the Head and Neck and HPV Infection Andrew Urquhart MD, FACS Dept. Otolaryngology/Head and Neck Surgery Marshfield Clinic Disclaimer I have no relevant financial relationships with the manufacturer(s)
Cancer of the Head and Neck and HPV Infection Andrew Urquhart MD, FACS Dept. Otolaryngology/Head and Neck Surgery Marshfield Clinic Disclaimer I have no relevant financial relationships with the manufacturer(s)
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Diagnosis and what happens after referral
 Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1 Treatment Modalities Early stage disease -larynx
Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1 Treatment Modalities Early stage disease -larynx
Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX
 Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX Disclosures I have nothing to disclose. 3 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX Disclosures I have nothing to disclose. 3 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
Accepted 28 April 2005 Published online 13 September 2005 in Wiley InterScience ( DOI: /hed.
 DEFINING RISK LEVELS IN LOCALLY ADVANCED HEAD AND NECK CANCERS: A COMPARATIVE ANALYSIS OF CONCURRENT POSTOPERATIVE RADIATION PLUS CHEMOTHERAPY TRIALS OF THE EORTC (#22931) AND RTOG (#9501) Jacques Bernier,
DEFINING RISK LEVELS IN LOCALLY ADVANCED HEAD AND NECK CANCERS: A COMPARATIVE ANALYSIS OF CONCURRENT POSTOPERATIVE RADIATION PLUS CHEMOTHERAPY TRIALS OF THE EORTC (#22931) AND RTOG (#9501) Jacques Bernier,
Head and NeckCancer: multi-modal therapeuticintegration
 Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
Title. CitationInternational Journal of Clinical Oncology, 20(6): 1. Issue Date Doc URL. Rights. Type. File Information
: 1. Issue Date Doc URL. Rights. Type. File Information") Title Clinical outcomes of weekly cisplatin chemoradiother Sakashita, Tomohiro; Homma, Akihiro; Hatakeyama, Hir Author(s) Takatsugu; Iizuka, Satoshi; Onimaru, Rikiya; Tsuchiy CitationInternational Journal
Title Clinical outcomes of weekly cisplatin chemoradiother Sakashita, Tomohiro; Homma, Akihiro; Hatakeyama, Hir Author(s) Takatsugu; Iizuka, Satoshi; Onimaru, Rikiya; Tsuchiy CitationInternational Journal
RE-IRRADIATION IN HEAD AND NECK CANCERS: A WISE SELECTION FROM AVAILABLE DATA
 REVIEW ARTICLE RE-IRRADIATION IN HEAD AND NECK CANCERS: A WISE SELECTION FROM AVAILABLE DATA Rubu Sunku 1, Vikas Kantilal Jagtap 2 Author s Affiliations: 1 Registrar, 2 Assistant Professor, Dept. of Radiotherapy,
REVIEW ARTICLE RE-IRRADIATION IN HEAD AND NECK CANCERS: A WISE SELECTION FROM AVAILABLE DATA Rubu Sunku 1, Vikas Kantilal Jagtap 2 Author s Affiliations: 1 Registrar, 2 Assistant Professor, Dept. of Radiotherapy,
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
ORIGINAL ARTICLE. Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx
 ORIGINAL ARTICLE Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx Sandro J. Stoeckli, MD; Andreas B. Pawlik, MD; Margareta Lipp, MD; Alexander Huber, MD;
ORIGINAL ARTICLE Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx Sandro J. Stoeckli, MD; Andreas B. Pawlik, MD; Margareta Lipp, MD; Alexander Huber, MD;
State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck. Raul Giglio
 State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck Raul Giglio Disclosures Nothing to disclose SCCHN Outline 1. General considerations: MTD 2. Epidemiology 3. Locoregional disease
State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck Raul Giglio Disclosures Nothing to disclose SCCHN Outline 1. General considerations: MTD 2. Epidemiology 3. Locoregional disease
The Role of Docetaxel in the Treatment of Head and Neck Cancer
 GBMC Head and Neck Conference The Role of Docetaxel in the Treatment of Head and Neck Cancer Simon Best December 7, 2007 Needs assessment: Providers who participate in the care of head and neck cancer
GBMC Head and Neck Conference The Role of Docetaxel in the Treatment of Head and Neck Cancer Simon Best December 7, 2007 Needs assessment: Providers who participate in the care of head and neck cancer
Research and Reviews Journal of Medical and Clinical Oncology
 Comparison and Prognostic Analysis of Elective Nodal Irradiation Using Definitive Radiotherapy versus Chemoradiotherapy for Treatment of Esophageal Cancer Keita M 1,2, Zhang Xueyuan 1, Deng Wenzhao 1,
Comparison and Prognostic Analysis of Elective Nodal Irradiation Using Definitive Radiotherapy versus Chemoradiotherapy for Treatment of Esophageal Cancer Keita M 1,2, Zhang Xueyuan 1, Deng Wenzhao 1,
Transoral Robotic Surgery (TORS) for Oropharyngeal Cancer
 for Oropharyngeal Cancer") Transoral Robotic Surgery (TORS) for Oropharyngeal Cancer Ellie Maghami, MD, FACS Professor of Otolaryngology / Head and Neck Surgery Chief, Division of Head and Neck Surgery Norman and Sadie Lee Professor
Transoral Robotic Surgery (TORS) for Oropharyngeal Cancer Ellie Maghami, MD, FACS Professor of Otolaryngology / Head and Neck Surgery Chief, Division of Head and Neck Surgery Norman and Sadie Lee Professor
Locoregional recurrences are the most frequent
 ORIGINAL ARTICLE SECOND SALVAGE SURGERY FOR RE-RECURRENT ORAL CAVITY AND OROPHARYNX CARCINOMA Ivan Marcelo Gonçalves Agra, MD, PhD, 1 João Gonçalves Filho, MD, PhD, 2 Everton Pontes Martins, MD, PhD, 2
ORIGINAL ARTICLE SECOND SALVAGE SURGERY FOR RE-RECURRENT ORAL CAVITY AND OROPHARYNX CARCINOMA Ivan Marcelo Gonçalves Agra, MD, PhD, 1 João Gonçalves Filho, MD, PhD, 2 Everton Pontes Martins, MD, PhD, 2
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer
 in Cervical Cancer") Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Combined Modality Therapy State of the Art. Everett E. Vokes The University of Chicago
 Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej. The role of brachytherapy in recurrent. oral cavity
 Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej The role of brachytherapy in recurrent tumours of the tongue and fundus of the oral cavity Janusz Skowronek, MD, PhD, Ass. Prof.
Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej The role of brachytherapy in recurrent tumours of the tongue and fundus of the oral cavity Janusz Skowronek, MD, PhD, Ass. Prof.
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no
 67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
PILOT STUDY OF CONCURRENT CHEMO-RADIOTHERAPY FOR ADVANCED NASOPHARYNGEAL CARCINOMA (Forum for Nuclear Cooperation in Asia)
") PILOT STUDY OF CONCURRENT CHEMO-RADIOTHERAPY FOR ADVANCED NASOPHARYNGEAL CARCINOMA (Forum for Nuclear Cooperation in Asia) Dr. Miriam Joy C. Calaguas Dept. of Radiation Oncology St. Luke s Medical Center
PILOT STUDY OF CONCURRENT CHEMO-RADIOTHERAPY FOR ADVANCED NASOPHARYNGEAL CARCINOMA (Forum for Nuclear Cooperation in Asia) Dr. Miriam Joy C. Calaguas Dept. of Radiation Oncology St. Luke s Medical Center
ACOSOG (NCCTG, CALGB) Alliance Thoracic Committee Kemp H. Kernstine, MD PhD
 Alliance Thoracic Committee Kemp H. Kernstine, MD PhD") ACOSOG (NCCTG, CALGB) Alliance Thoracic Committee Kemp H. Kernstine, MD PhD 7-12-12 ACOSOG Thoracic Committee Chair: Bryan Meyers, M.D., MPH Vice Chairs: Malcolm Brock, MD Tom DiPetrillo, M.D. Ramaswamy
ACOSOG (NCCTG, CALGB) Alliance Thoracic Committee Kemp H. Kernstine, MD PhD 7-12-12 ACOSOG Thoracic Committee Chair: Bryan Meyers, M.D., MPH Vice Chairs: Malcolm Brock, MD Tom DiPetrillo, M.D. Ramaswamy
North of Scotland Cancer Network Clinical Management Guideline for Oropharyngeal Cancer
 Nth of Scotland Cancer Netwk Clinical Management Guideline f Oropharyngeal Cancer UNCONTROLLED WHEN PRINTED Based on NHST CMG with further extensive consultation within NOSCAN DOCUMENT CONTROL Original
Nth of Scotland Cancer Netwk Clinical Management Guideline f Oropharyngeal Cancer UNCONTROLLED WHEN PRINTED Based on NHST CMG with further extensive consultation within NOSCAN DOCUMENT CONTROL Original
ARROCase Nasopharynx Cancer. Kara D. Romano, MD Daniel M. Trifiletti, MD Paul W. Read, MD University of Virginia
 ARROCase Nasopharynx Cancer Kara D. Romano, MD Daniel M. Trifiletti, MD Paul W. Read, MD University of Virginia Case: History H&P: 37 yo male presents with left-sided neck mass, ear pressure, otalgia,
ARROCase Nasopharynx Cancer Kara D. Romano, MD Daniel M. Trifiletti, MD Paul W. Read, MD University of Virginia Case: History H&P: 37 yo male presents with left-sided neck mass, ear pressure, otalgia,
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Dose escalation for NSCLC using conformal RT: 3D and IMRT. Hasan Murshed
 Dose escalation for NSCLC using conformal RT: 3D and IMRT. Hasan Murshed Take home message Preliminary data shows CRT technique in NSCLC allows dose escalation to an unprecedented level maintaining cancer
Dose escalation for NSCLC using conformal RT: 3D and IMRT. Hasan Murshed Take home message Preliminary data shows CRT technique in NSCLC allows dose escalation to an unprecedented level maintaining cancer
Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK
 Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Head & Neck Cancer: When to Irradiate
 Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部
 肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
Oral Cavity. 1. Introduction. 1.1 General Information and Aetiology. 1.2 Diagnosis and Treatment
 Oral Cavity 1. Introduction 1.1 General Information and Aetiology The oral cavity extends from the lips to the palatoglossal folds and consists of the anterior two thirds of the tongue, floor of the mouth,
Oral Cavity 1. Introduction 1.1 General Information and Aetiology The oral cavity extends from the lips to the palatoglossal folds and consists of the anterior two thirds of the tongue, floor of the mouth,
A Case Review: Treatment-Naïve Patient with Head and Neck Cancer
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer
 Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer Faye Johnson MD, PhD Associate Professor Thoracic/Head and Neck Medical Oncology August 2017 Objectives Review data that support concurrent chemo-
Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer Faye Johnson MD, PhD Associate Professor Thoracic/Head and Neck Medical Oncology August 2017 Objectives Review data that support concurrent chemo-