GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
|
|
|
- Eleanore Franklin
- 6 years ago
- Views:
Transcription

1 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles
2
3 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner have, or have had, within the past 12 months, which relates to the content of this educational activity and creates a conflict of interest.
4 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner have, or have had, within the past 12 months, which relates to the content of this educational activity and creates a conflict of interest. Dr. Hanlin Wang declares he has no conflict(s) of interest to disclose.
5 2010 WHO Classification of Neuroendocrine Neoplasms of the Appendix Neuroendocrine tumor (NET) NET G1 (carcinoid) NET G2 Neuroendocrine carcinoma (NEC) Large cell NEC Small cell NEC Mixed adenoneuroendocrine carcinoma EC cell, serotonin-producing NET L cell, glucagon-like peptide-producing and PP/PYY-producing NETs Goblet cell carcinoid (GCC) Tubular carcinoid

6 Tubular Carcinoid of the Appendix Always small (<1 cm) Found at the tip or distal half Primarily in the submucosa but may involve the muscularis propria, and rarely the subserosa Discrete small tubules and/or short solid cords Abundant fibrotic stroma

7 Tubular Carcinoid of the Appendix Cuboidal to low columnar cells with no cytologic atypia May have inspissated mucin in the lumens No mitotic figures Never recur or metastasize Not confused with metastatic adenocarcinoma
8 Goblet Cell Carcinoid A unique neoplasm with glandular and endocrine differentiation Almost exclusively seen in the appendix Rarely seen in the stomach, small bowel and colon Synonyms Adenocarcinoid Mucinous carcinoid Microglandular carcinoma Crypt cell carcinoma Amphicrine neoplasm Mucin-producing neuroendocrine tumor/carcinoma
9 Goblet Cell Carcinoid Found in % of appendectomies Mean age: 59 years (18-89 years) ~20 years older than that for classic carcinoid of the appendix Affecting males and females equally Initial presentation Acute appendicitis in most cases Lower abdominal palpable mass

10 Goblet Cell Carcinoid Rarely forms a mass lesion Usually infiltrates the appendiceal wall circumferentially in a concentric manner Lacks desmoplastic reaction


11 Typically spares the mucosa, but may show focal connection with the base of crypts No adenomatous change in the mucosa


12 Goblet or signet-ring cell morphology Small tight clusters, nests or cords of tumor cells, typically without overt luminal formation

13 Small extracellular mucin pools

14 Minimal nuclear atypia
15 Immunophenotypical and Molecular Features of GCC in Comparison with Classic Carcinoid and Conventional Adenocarcinoma Marker GCC Classic Carcinoid Adenocarcinoma CEA CK7 +/- - +/- CK20 +/- - + CDX2 + +/- + CD56 +/- + - Synaptophysin +/- + - Chromogranin +/- + - Beta-catenin (nuclear) p Ki67 intermediate low high MUC MUC /- KRAS mutation - - +/- BRAF mutation - - +/- MSI - - +/-
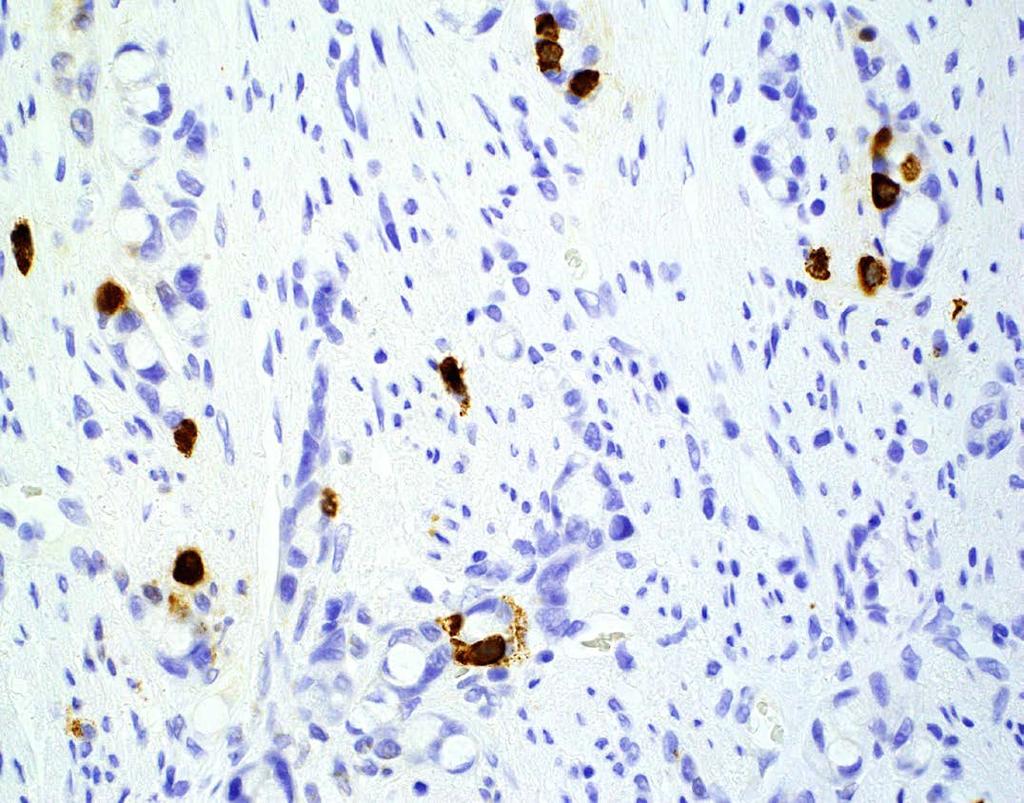
16 Chromogranin
17 GCC with A Component of Adenocarcinoma Mixed adenoneuroendocrine carcinoma Mixed carcinoid-adenocarcinoma Mixed goblet cell carcinoid-adenocarcinoma Adenocarcinoma ex goblet cell carcinoid Signet-ring cell type Poorly differentiated carcinoma type
18 Am J Clin Pathol 1990; 94:27-35 Goblet cell carcinoid N=25 Negative appendectomy or right hemicolectomy margins Average follow-up: 19 months No metastasis or death *Carcinomatous growth patterns included fused or cribriform glands, single file structures, infiltrating signet-ring cells or sheets of solid cells; accounting for >50% of the tumor volume Mixed carcinoid-adenocarcinoma* N=10 Average follow-up: 16 months 8 died of metastatic carcinoma 1 alive with disease 1 alive without disease following radiation therapy
19 Tang LH, et al. Am J Surg Pathol 2008; 32:



20 Gland-forming Confluent sheets of signet-ring cells Minimal differentiation Adenocarcinoma ex GCC, poorly differentiated adenocarcinoma type Tang LH, et al. Am J Surg Pathol 2008; 32:

21 Adenocarcinoma ex GCC Signet-ring cell type Large irregular clusters Lack confluent sheets Tang LH, et al. Am J Surg Pathol 2008; 32:

22 Adenocarcinoma ex GCC Signet-ring cell type Discohesive single cell and single file infiltration Architectural distortion of the appendiceal wall and desmoplastic reaction Tang LH, et al. Am J Surg Pathol 2008; 32:

23 Adenocarcinoma ex GCC Signet-ring cell type Marked nuclear atypia with hyperchromatic nuclei Tang LH, et al. Am J Surg Pathol 2008; 32:

24 Tang LH, et al. Am J Surg Pathol 2008; 32:
25 Group 1: GCC or GCC with <25% adenocarcinoma Group 2: GCC with 25-50% adenocarcinoma Group 3: GCC with >50% adenocarcinoma Group 4: Adenocarcinoma without GCC component Taggart MW, et al. Arch Pathol Lab Med 2015;139: Group Stage; N (%) Overall Survival II III IV Unknown Mean (SD), mo 1 (n=23) 20 (87) 1 (4) 1 (4) 1 (4) 83.8 (34.6) 2 (n=27) 18 (67) 2 (7) 6 (22) 1 (4) 60.6 (30.3) 3 (n=24) 7 (29) 1 (4) 16 (67) (39.7) 4 (n=68) 13 (19) 4 (6) 51 (75) (27.6)
26 Individual dyshesive cells Solid sheets of cells Definition of Adenocarcinoma Infiltrative cords of cells (not within muscularis propria) or larger cords incompatible with GCC Complex glandular architecture (irregular, angulated, cribriform, tufting) Clusters of cells simulating GCC but with increased cytologic or architectural atypia beyond typical GCC nests (enlarged or irregular nests/glands, increased cytologic atypia, increased mitotic activity) Destructive invasion or desmoplasia Taggart MW, et al. Arch Pathol Lab Med 2015;139:782-90


27 Group 3 (>50%) Solid sheets of goblet/signet-ring cells Infiltrating single cells Taggart MW, et al. Arch Pathol Lab Med 2015;139:782-90

28 Group 2 (25-50%) An area of poorly differentiated signet-ring cell adenocarcinoma in a GCC Taggart MW, et al. Arch Pathol Lab Med 2015;139:782-90
29 Group 2 (25-50%) Group 3 (>50%) (70.7±10.5 mons) (72.3±16.5 mons) (74.9±10.6 mons) (25.1±3.8 mons) Taggart MW, et al. Arch Pathol Lab Med 2015;139:782-90

30 Simplified 2-Tier Histologic Grading System * *** ** *Four contiguous high power fields (x400) with a 0.55-mm field diameter are used to assess a 1 mm 2 area. At least one cytologically atypical tumor cell is required to be in each high power field. **Desmoplasia of the submucosa or subserosal fat or serosal adhesions are insufficient. ***Spatially separate small foci of solid growth pattern, which aggregate to a total of 1 mm 2, are insufficient. Lee LH, et al. Hum Pathol 2015; 46:1881-9
31 Lee LH, et al. Hum Pathol 2015; 46:1881-9

32 Cytologic atypia: enlarged hyperchromatic nuclei, irregular nuclear contour, variable loss of cytoplasmic mucin Lee LH, et al. Hum Pathol 2015; 46:1881-9

33 Peritumoral stromal desmoplasia that replaces the smooth muscle of the appendiceal wall Lee LH, et al. Hum Pathol 2015; 46:1881-9
34 Recognition of Adenocarcinoma in GCC Histologic Features Complex glandular architecture Loss of clustered architecture Infiltrating individual discohesive cells Solid sheets or irregular large clusters of cells Significant cytologic atypia Desmoplasia Tumor Volume >50% (Burke, 1990) >One low power field or 1 mm 2 for Tang s group C (2008) Partial or near complete loss of GCC clustered architecture for Tang s group B (2008) >30% (WHO, 2010) >25% and >50% (Taggart, 2015) > 1 mm 2 (Lee, 2015)


35 Poorly differentiated adenocarcinoma with focal glandular formation


36 Solid sheets of goblet/signet-ring cells Irregular large clusters of goblet/signet-ring cells Desmoplasia


37 Infiltrating individual goblet/signet-ring cells with cytologic atypia Solid cords with cytologic atypia and loss of intracytoplasmic mucin


38 Cytologic atypia with mitoses Desmoplasia


39 Adv Anat Pathol 2009; 16:247-54
40 Goblet Cell Carcinoid Staging and Management Staged as adenocarcinoma of the appendix Ki-67 labeling index is not required for grading Treatment options are primarily based on tumor stage and the presence or absence of adenocarcinoma
41 Management of Goblet Cell Carcinoid Appendectomy alone Stage I (pt1 or pt2) pure GCC with negative margin Comorbidities that do not allow further surgical intervention Lifelong surveillance for metastasis Right hemicolectomy Higher stage (pt3 or pt4) disease Positive appendectomy margin Presence of adenocarcinoma Perforated appendix Cytoreductive surgery and intraperitoneal chemotherapy Peritoneal spread Systemic chemotherapy Stages III and IV disease Recurrent disease Prophylactic oophorectomy, particularly for postmenopausal women Candidates for right hemicolectomy and/or chemotherapy Tang LH, et al. Am J Surg Pathol 2008;32: Shenoy S. World J Gastrointest Surg 2016;8:660-9 Lamarca A, et al. Neuroendocrinology 2016;103:500-17
42 Summary GCC is a unique clinicopathologic entity that is frequently associated with adenocarcinoma Histologic identification and quantification of adenocarcinoma is important in determining prognosis and thus in guiding clinical management The entire appendectomy specimen should be histologically examined when a GCC case is encountered; and the margin status should be reported
43 Important Information Regarding CME/SAMs The Online CME/Evaluations/SAMs claim process will only be available on the USCAP website until September 30, No claims can be processed after that date! After September 30, 2017 you will NOT be able to obtain any CME or SAMs credits for attending this meeting.

44
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
Syllabus. Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix. Appendiceal tumors. Summary provided Complete presentation
 2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
3/22/2017. Disclosure of Relevant Financial Relationships. Disclosure of Relevant Financial Relationships. Grading G1. Grading. Ki67 index V.
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
3/27/2017. Pulmonary Pathology Specialty Conference. Disclosure of Relevant Financial Relationships. Clinical History:
 Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Despite advances in our understanding of appendiceal. An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms
 REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
Neuroendocrine tumors of GI and Pancreatobiliary tracts. N. Volkan Adsay, MD
 Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Chapter 6 Frozen Section Evaluation of the Appendix
 Chapter 6 Frozen Section Evaluation of the Appendix Abstract Appendiceal tumors are rarely diagnosed preoperatively, and their classification is both challenging and controversial owing to their tendency
Chapter 6 Frozen Section Evaluation of the Appendix Abstract Appendiceal tumors are rarely diagnosed preoperatively, and their classification is both challenging and controversial owing to their tendency
Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms
 Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
3/28/2017. Disclosure of Relevant Financial Relationships. GU Evening Subspecialty Case Conference. Differential Diagnosis:
 GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
3/30/2017. Disclosure of Relevant Financial Relationships. Case 5: Polypoid mass in ulcerative colitis. Case 5. TC Smyrk
 Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
3/24/2017. Disclosure of Relevant Financial Relationships. Mixed Epithelial Endometrial Carcinoma. ISGyP Endometrial Cancer Project
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Serotonin- and Somatostatin-Positive Goblet Cell Carcinoid of the Duodenum
 2012 66 4 351 356 Serotonin- and Somatostatin-Positive Goblet Cell Carcinoid of the Duodenum a b* c c c a a b d a c b d 352 Ohara et al. received remedies at another hospital. Hematemesis then recurred
2012 66 4 351 356 Serotonin- and Somatostatin-Positive Goblet Cell Carcinoid of the Duodenum a b* c c c a a b d a c b d 352 Ohara et al. received remedies at another hospital. Hematemesis then recurred
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Goblet Cell Carcinoid Tumor, Mixed Goblet Cell Carcinoid-Adenocarcinoma, and Adenocarcinoma of the Appendix
 Goblet Cell Carcinoid Tumor, Mixed Goblet Cell Carcinoid-Adenocarcinoma, and Adenocarcinoma of the Appendix Comparison of Clinicopathologic Features and Prognosis Melissa W. Taggart, MD; Susan C. Abraham,
Goblet Cell Carcinoid Tumor, Mixed Goblet Cell Carcinoid-Adenocarcinoma, and Adenocarcinoma of the Appendix Comparison of Clinicopathologic Features and Prognosis Melissa W. Taggart, MD; Susan C. Abraham,
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
G3.02 The malignant potential of the neoplasm should be recorded. CG3.02a
 G3.02 The malignant potential of the neoplasm should be recorded. CG3.02a Conventional adrenocortical neoplasm. Each of the below parameters is scored 0 when absent and 1 when present. 3 or more of these
G3.02 The malignant potential of the neoplasm should be recorded. CG3.02a Conventional adrenocortical neoplasm. Each of the below parameters is scored 0 when absent and 1 when present. 3 or more of these
They Do Look Alike : Mimics of Prostate Cancer in Biopsy Samples
 They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
USCAP 2012: Companion Meeting of the AAOOP. Update on lacrimal gland neoplasms: Molecular pathology of interest
 USCAP 2012: Companion Meeting of the AAOOP Vancouver BC, Canada, March 17, 2012 Update on lacrimal gland neoplasms: Molecular pathology of interest Valerie A. White MD, MHSc, FRCPC Department of Pathology
USCAP 2012: Companion Meeting of the AAOOP Vancouver BC, Canada, March 17, 2012 Update on lacrimal gland neoplasms: Molecular pathology of interest Valerie A. White MD, MHSc, FRCPC Department of Pathology
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Supplemental Figure 1
 A1 A A5 A7 A9 A A4 A6 A8 A10 A1/A Gleason Score +=6 A/A4 Gleason Score +=6 Small glands with well defined Prominent feature of size variation lumen of various size infiltrating in to and distinct lumina
A1 A A5 A7 A9 A A4 A6 A8 A10 A1/A Gleason Score +=6 A/A4 Gleason Score +=6 Small glands with well defined Prominent feature of size variation lumen of various size infiltrating in to and distinct lumina
Gastric and Oesophageal Neuroendocrine tumours. Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath
 Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Intrahepatic cholangiocarcinoma Histologic spectrum, novel markers and molecular assays
 2018 Current Issues in Surgical Pathology Summary (not actual lecture) Intrahepatic cholangiocarcinoma Histologic spectrum, novel markers and molecular assays Sanjay Kakar, MD University of California,
2018 Current Issues in Surgical Pathology Summary (not actual lecture) Intrahepatic cholangiocarcinoma Histologic spectrum, novel markers and molecular assays Sanjay Kakar, MD University of California,
3/28/2017. Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center
 Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial
Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial
Disclosure of Relevant Financial Relationships
 Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
Case 3 - GYN. History: 66 year old, routine Pap test. Dr. Stelow
 Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Copyright information:
 Adenocarcinoma ex-goblet cell carcinoid (appendiceal-type crypt cell adenocarcinoma) is a morphologically distinct entity with highly aggressive behavior and frequent association with peritoneal/intra-abdominal
Adenocarcinoma ex-goblet cell carcinoid (appendiceal-type crypt cell adenocarcinoma) is a morphologically distinct entity with highly aggressive behavior and frequent association with peritoneal/intra-abdominal
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX
 Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
MVST BOD & NST PART IB Thurs. 2 nd & Fri. 3 rd March 2017 Pathology Practical Class 23
 MVST BOD & NST PART IB Thurs. 2 nd & Fri. 3 rd March 2017 Pathology Practical Class 23 Neoplasia I Neoplasia I: Benign and malignant neoplasms in glandular epithelium and mesenchyme 1.0. Aims 1. To understand
MVST BOD & NST PART IB Thurs. 2 nd & Fri. 3 rd March 2017 Pathology Practical Class 23 Neoplasia I Neoplasia I: Benign and malignant neoplasms in glandular epithelium and mesenchyme 1.0. Aims 1. To understand
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Evening Specialty Conference: Cytopathology
 : Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
: Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
A Concurrence of Adenocarcinoma with Micropapillary Features and Composite Glandular-Endocrine. cell carcinoma in the stomach.
 pissn : 2093-582X, eissn : 2093-5641 J Gastric Cancer 2016;16(4):266-270 https://doi.org/10.5230/jgc.2016.16.4.266 Case Report A Concurrence of Adenocarcinoma with Micropapillary Features and Composite
pissn : 2093-582X, eissn : 2093-5641 J Gastric Cancer 2016;16(4):266-270 https://doi.org/10.5230/jgc.2016.16.4.266 Case Report A Concurrence of Adenocarcinoma with Micropapillary Features and Composite
APPENDIX 5 PATHOLOGY 1. Handling and gross examination of gastrointestinal and pancreatic NETs
 APPENDIX 5 PATHOLOGY 1. Handling and gross examination of gastrointestinal and pancreatic NETs Specimen handling and gross examination should be performed according to the Royal College of Pathologists
APPENDIX 5 PATHOLOGY 1. Handling and gross examination of gastrointestinal and pancreatic NETs Specimen handling and gross examination should be performed according to the Royal College of Pathologists
Carcinoma mammario: le istologie non frequenti. Valentina Guarneri Università di Padova IOV-IRCCS
 Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box?
 When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
Mucinous Tumors of the Ovary Beirut, Lebanon. Anaís Malpica, M.D. Professor Department of Pathology
 Mucinous Tumors of the Ovary Beirut, Lebanon Anaís Malpica, M.D. Professor Department of Pathology Primary Mucinous Tumors of the Ovary Cystadenoma Borderline (Tumor of Low Malignant Potential/Atypical
Mucinous Tumors of the Ovary Beirut, Lebanon Anaís Malpica, M.D. Professor Department of Pathology Primary Mucinous Tumors of the Ovary Cystadenoma Borderline (Tumor of Low Malignant Potential/Atypical
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
Objectives. Terminology 03/11/2013. Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors. Pathology Update 2013
 Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Signet-Ring Cell Carcinoma of the Colon: A Case Report and Review of the Literature
 Published online: November 4, 2015 2015 The Author(s) Published by S. Karger AG, Basel 1662 6575/15/0083 0466$39.50/0 This article is licensed under the Creative Commons Attribution-NonCommercial 4.0 International
Published online: November 4, 2015 2015 The Author(s) Published by S. Karger AG, Basel 1662 6575/15/0083 0466$39.50/0 This article is licensed under the Creative Commons Attribution-NonCommercial 4.0 International
Diagnostically Challenging Cases in Gynecologic Pathology
 Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Part 3. Case #7 History:
 Part 3 Case #7 History: The patient is a 25 year old woman who had a colectomy for familial adenomatous polyposis 2 years ago. No carcinoma was found in her colectomy specimen. She presents now with 2
Part 3 Case #7 History: The patient is a 25 year old woman who had a colectomy for familial adenomatous polyposis 2 years ago. No carcinoma was found in her colectomy specimen. She presents now with 2
A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy.
 November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Section 1. Biology of gynaecological cancers: our current understanding
 Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Overview. Collecting Cancer Data: Colon 11/5/2009. Collecting Cancer Data: NAACCR Webinar Series 1. Agenda NAACCR WEBINAR SERIES
 Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Goblet Cell Carcinoids of the Appendix. Immunophenotype and Ultrastructural Study
 Goblet Cell Carcinoids of the Appendix Immunophenotype and Ultrastructural Study R. Kanthan, MBBS, MS, FRCS, FRCPC; A. Saxena, MBBS, MD, FRCPC, FCAP; S. C. Kanthan, MBBS, FRCS, FRCSC Background. Goblet
Goblet Cell Carcinoids of the Appendix Immunophenotype and Ultrastructural Study R. Kanthan, MBBS, MS, FRCS, FRCPC; A. Saxena, MBBS, MD, FRCPC, FCAP; S. C. Kanthan, MBBS, FRCS, FRCSC Background. Goblet
ACCME/Disclosures. Case History 4/13/2016. USCAP GU Specialty Conference Case 3. Ann Arbor, MI
 USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
Bibliography. Serous Tumors of the Ovary. Nomenclature
 Bibliography Serous Tumors of the Ovary Nomenclature 1. Allison KH, Swisher EM, Kerkering KM, et al. Defining an appropriate threshold for the diagnosis of serous borderline tumor of the ovary: when is
Bibliography Serous Tumors of the Ovary Nomenclature 1. Allison KH, Swisher EM, Kerkering KM, et al. Defining an appropriate threshold for the diagnosis of serous borderline tumor of the ovary: when is
Small Cell Carcinoma ex-pleomorphic Adenoma of the Parotid Gland
 Head and Neck Pathol (2012) 6:502 506 DOI 10.1007/s12105-012-0376-1 CASE REPORT Small Cell Carcinoma ex-pleomorphic Adenoma of the Parotid Gland Ashley Cimino-Mathews Brian M. Lin Steven S. Chang Kofi
Head and Neck Pathol (2012) 6:502 506 DOI 10.1007/s12105-012-0376-1 CASE REPORT Small Cell Carcinoma ex-pleomorphic Adenoma of the Parotid Gland Ashley Cimino-Mathews Brian M. Lin Steven S. Chang Kofi
Division of Pathology
 Case 38 Adult woman with a 35mm right breast lump at the 10 o clock position. Excision performed. (Case contributed by Dr Mihir Gudi, KKH) Division of Pathology Merlion, One Fullerton Singapore Diagnosis
Case 38 Adult woman with a 35mm right breast lump at the 10 o clock position. Excision performed. (Case contributed by Dr Mihir Gudi, KKH) Division of Pathology Merlion, One Fullerton Singapore Diagnosis
3/23/2017. Significant Changes in Prostate Cancer Classification, Grading, Staging and Reporting. Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships Staging and Reporting of Prostate Cancer: Major Changes in 8 th Edition AJCC Staging and CAP Cancer Checklists USCAP requires that all planners (Education
Disclosure of Relevant Financial Relationships Staging and Reporting of Prostate Cancer: Major Changes in 8 th Edition AJCC Staging and CAP Cancer Checklists USCAP requires that all planners (Education
Appendix cancer mimicking ovarian cancer
 Int J Gynecol Cancer 2002, 12, 768 772 CORRESPONDENCE AND BRIEF REPORTS Appendix cancer mimicking ovarian cancer P. A. GEHRIG *, J. F. BOGGESS*, D. W. OLLILA, P. A. GROBEN & L. VAN LE* *Division of Gynecologic
Int J Gynecol Cancer 2002, 12, 768 772 CORRESPONDENCE AND BRIEF REPORTS Appendix cancer mimicking ovarian cancer P. A. GEHRIG *, J. F. BOGGESS*, D. W. OLLILA, P. A. GROBEN & L. VAN LE* *Division of Gynecologic
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Protocol for the Examination of Specimens From Patients With Carcinoma of the Appendix
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Appendix Version: Appendix 4.0.0.1 Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC
Protocol for the Examination of Specimens From Patients With Carcinoma of the Appendix Version: Appendix 4.0.0.1 Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
BLADDER CANCER EPIDEMIOLOGY
 BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
Diagnostic Difficulties Encountered Among Colorectal Polyps
 Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis.
 Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Appendiceal Adenocarcinoma with Suppurative Appendicitis: Case Report and Literature Review
 Appendiceal adenocarcinoma presenting with acute appendicitis 155 Appendiceal Adenocarcinoma with Suppurative Appendicitis: Case Report and Literature Review Va-Kei Kok 1, Teh-Kuang Wang 2, Hsi-Che Shen
Appendiceal adenocarcinoma presenting with acute appendicitis 155 Appendiceal Adenocarcinoma with Suppurative Appendicitis: Case Report and Literature Review Va-Kei Kok 1, Teh-Kuang Wang 2, Hsi-Che Shen
Dr Sanjiv Manek Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications. Andres A. Roma, MD Cleveland Clinic
 Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications Andres A. Roma, MD Cleveland Clinic No Disclosures In the past 12 months, I have not had
Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications Andres A. Roma, MD Cleveland Clinic No Disclosures In the past 12 months, I have not had
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors
 Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Formula One Study. Assessment criteria of pathological parameters. Ver.2. UK Japan Joint Study for Risk Factors of Lymph Node
 APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Serrated Lesions in the Bowel Cancer Screening Programme
 Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,