Surgery for NET Challenges and specific aspects
|
|
|
- Sharon Blair
- 5 years ago
- Views:
Transcription
 Leuven, Belgium, 28-29")
1 Surgery for NET Challenges and specific aspects Raymond Aerts, MD Department of Abdominal Surgery and Liver Transplantation University Clinics Leuven ESMO Preceptorship on GI neuroendocrine tumours (NETs) Leuven, Belgium, November 2014
2 Incidence and Prevalence NET (SEER ) Rare Increasing Incidence : 1/ / y : 5/ /y 29 y Prevalence: 35/ Yao, J Clin Oncol 2008;26:

3 Incidence GEP-NET 60% GEP-NET small bowel rectum pancreas stomach caecum colon appendix Yao, J Clin Oncol 2008;26:
4 Prognosis GEP-NET Better A. Frilling et al, Lancet Oncol 2014; 15: e8-21
5 Surgery for NET Rationale: only chance for cure prolong survival control symptoms prevent, control local complications Primary tumour: aggressive resection Metastases: 15-25% surgical candidates only for G1-G2 tumours curative resection: R0-R1 primary tumour curative resected or resectable no extrahepatic non resectable metastases resectable liver lesions debulking: R2 > 90%: control symptoms (limited indication) transplantation (limited indication) primary tumour curative resected no extrahepatic metastases


6 Aggressive surgery primary tumour SiNET Prevention of complications Ohrvall et al, WJS 2000; 24: Akerstrom et al, Best Pract,2007; 21:


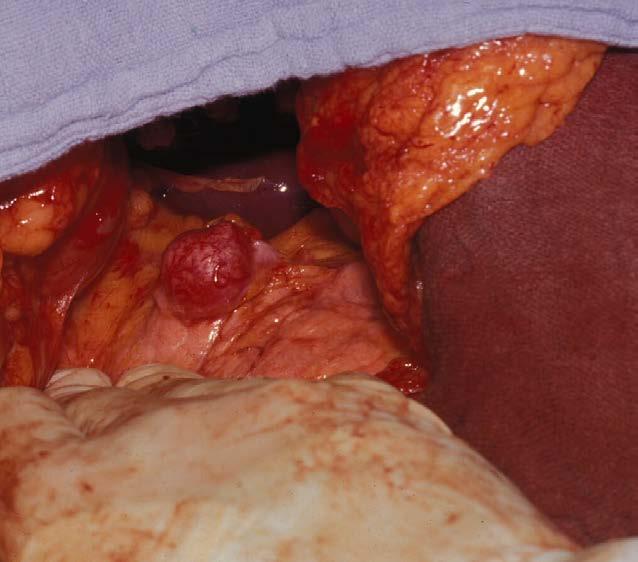
7 nodal complex primary tumour

8 ischemia necrosis
9 Aggressive surgery primary tumour SiNET Impact on survival Uppsala 314 patients Intestinal resection + lymphadenectomy only 11 liver resections Biotherapy: SSA, IFN Hellman, WJS 2002; 26:


10



11 Case SiNET 55 y old male patient 3 mo history of abdominal cramps and obstipation 8 kg weight loss


12 Case SiNET Tumour markers CEA 2,4 µg/l CA19,9 20 ku/l CgA 156 µg/l FDG-PET/CT
13 Case SiNET Surgery: SiNET type 4 Mesenterial mass Retraction Ischemia terminal ileum Extended right hemicolectomy and resection 2 m ileum Resection tail pancreas, splenectomy, splenic flexure colon Pathology SiNET: 3 small G2 tumours Ki67: 3-20% pt3n1 (17/25) Inflammatory myofibroblast tumour in Mesenteric fibrotic mass Pancreatic tail
14 Incidence and malignancy in PNET frequency malignant % Non functional PNET > 50% 50-90% Insulinoma 25% 10% Gastrinoma 10% > 60% Glucagonoma > 60% VIPoma 60-80% Somatostatinoma 80% PTH-RP 80-90% GRF 30% ACTH > 90% Carcinoid pancreas 70-90%
15 PNET Hormone secretion endocrinopathy Non functional mass effect Mostly malignant metastases LN peritoneum, liver >> bone > lung Slowly growing = natural history better prognosis than other pancreatic malignancy Association MEN-1
16 Diagnosis PNET Insulinoma < 2 cm Gastrinoma < 2cm (0,5 cm) Others large > 5-15 cm localisation think PNET Tumour markers Chromogranin A Neuron specific enolase
17 Non functional PNET large: 5-15 cm mass effect 60% head pancreas Mostly solitary 80-90% malignant Diagnosis: think PNET! surgery: PD, debulking Prognosis Cure: 25-40% 50-65% 5 y survival

18 Non functional PNET


19 Aggressive surgery primary tumour Prevention of complications
20 Insulinoma 1 / million/ year Solitary: 90% (10% MEN-1: multiple) <2cm benigne > 90% Diffuse distribution in pancreas (tail > head?) Symptoms: neuroglycopenia Diagnosis Hypoglycemie < 40 mg/dl Fasting proof Control Diet Diazoxine Ca blockers
21 Insulinoma treatment: Enucleation: Wirsung! Resection tail Central pancreatic resection Rarely PD Prognosis Benign: cure Malignant: 75% 10 y survival Special cases Nesidioblastosis Insulinomatosis

22 Insulinoma
23 Gastrinoma 0.5/million/year > 50% multiple 25% MEN-1 < 2 cm Gastrinoma triangle >60% in wall proximal duodenum: 2-5 mm Primary in LN, liver, ovary? > 60% malignant (> 90% if > 1-2 cm) 1/2 metastases at diagnosis! early diagnosis ZES: recurrent peptic ulcera, oesophagitis, diarrhoea
24 Gastrinoma Diagnosis: Gastrine > pg/ml Secretine stimulation > 200 pg/ml increase Control: PPI surgery Enucleation for small duodenal wall tumours palpation, transillumination, duodenotomy Oncological resection for large tumours Potentially resection or debulking metastases Prognosis Without metastases: 95% 10 year survival With metastases : 5 y: 50%, 10 y: 30 % survival
25 Case gastrinoma 2006: 61 y old woman 3 mo history of peptic ulcer, esophagitis, diarrhoea and weight loss (diet?) Gastrin > 1000pg/ml ZES No family history sporadic R/ 160 mg pantoprazol/day 111In Octreotide: negative 18-FDG-PET/CT: negative 2007 CgA: 2200 µg/l 68Ga-Dotatoc PET/CT: 2 metastatic LN Good clinical control with PPI 2010 Recurrent episodes deshydration due to vomiting and diarrhoea CgA: 6860 µg/l Gastrin: 2930 pg/ml Surgical exploration 3 mm gastrinoma in the bulbus 3 metastatic LN No complaints, no PPI since 4 mo postoperatively CgA: 260 µg/l Gastrin: 49 pg/ml
26 MEN-1 syndrome Hypohysis prolactinoma, parathyroid adenoma, multiple PNET MEN-1 gen chromosome 11q13 Multiple PNET with mostly dominant secretion and multiple non functioning tumours 50% gastrinoma 20% insulinoma Prognosis MEN-1 gastrinoma better than sporadic resection if > 2 cm
27 MEN-1 syndrome 1994 diagnosis ZES in known MEN-1 family Resection 3 parathyroid glands for primary hyperparathyroidy Gastrin 600 pg/ml Liver metastasis segment1, 2 hypervascular pancreas lesions Reluctant to take PPI 1995: surgical exploration Resection metastasis segment 1: NET metastasis, gastrin + Resection 5 PNET, gastrin - Normalisation gastrin 2003: CgA: 345 µg/l, gastrin: 162 pg/ml (nl <111) normal Ca 2007 CgA: 850 µg/l, gastrin 360 pg/ml Liver metastasis segment 5: reresection Since then no complaints except tiredness (2-2014) normalisation Ca, CgA, gastrin
28 Epidemiology NELM SEER database (Yao) ref centers Localized 50% preselection Regional 24% Distal 26% 44-73% M+ correlates with differentiation, proliferation G1 21% 38% (Spanisch registry) G2 30% G3 50% 67% (Spanisch registry) G4 100% M+ correlates with primary tumor localisation Pancreas 64% 77% Caecum 44% Colon 32% Small bowel 30% 91% Rectum, duodenum, appendix, stomach: 5-15%
29 Incidence LM vs size primary GI NET M+ correlates with primary tumor size (carcinoid) Rorstad, J Surg Oncol 2005; 89: ) Rorstad, J Surg Oncol 2005; 89:

30 Incidence NET and NELM different data depending on the composition of the registry - population based - reference centers synchronous : 50-75% metachronous: 25-50% B. Lawrence, End Met Clin NA 2011; 40:1-18 A. Frilling, Lancet Oncol 2014; 15: e8-21
 or unilateral 20-25% Type II isolated")


31 Type NELM Type I single metastasis (size independent) or unilateral 20-25% Type II isolated metastatic bulk accompaniesd by smaller deposits, always bilateral 10-15% Type III disseminated metastatic spread always bilateral varying size of single lesion 60-70% T. Steinmüller, Neuroendocrinology 2008; 87: 47-62
32 Therapy for NELM: multimodal Surgical Resection +/- local ablation transplantation Medical SSA IF Targetted therapy: sunitinib, everolimus chemotherapy Radiologic TAE, TACE, SIRT, DEB Nuclear medicin PRRT
33 Surgery for NELM Well to moderately differentiated G1-G2 tumours Absence non resectable intra or extraabdominal metastases Curative resectable lesion: (resection ± RFA) lesions can be completely resected (R0) preservation of enough functional liver tissue with adequate vascular inflow and outflow and biliary drainage the volume of the liver remaining after resection ie future remnant liver (FRL) will be adequate % for normal liver % for steatosis or after chemotherapy Debulking: > 90 tumour reduction: limited indication for symptom control (resection ± RFA) General condition Absence right heart failure Prevention carcinoid crisis: SSA Acceptable mortality, morbidity
34 Surgery for NELM Timing Synchronous Simultaneous resection (primary + limited NELM) Staged resection (primary + left lobe), right lobe in second step Metachronous 1 or 2 step

35 Surgical anatomy and anatomical surgery right hemihepatectomy right trisectionectomy bisegmentectomies 6-7, 5-8, 5-6 left hemihepatectomy left trisectionectomy bisegmentectomy 2-3 central hepatectomy segmentectomy

36 Nonanatomical resections
37 Strategies to increase resectability Surgical strategies: Portal vein embolisation Combination resection with local ablation techniques Staged hepatectomy ALPPS (in situ splitting +PVL) Repeat hepatectomy Neo-adjuvant therapy
38 Staged hepatectomy R. Adam
39 A. Saxena, Surgical Oncology 2012; 21:e131-e141
40 A. Saxena, Surgical Oncology 2012; 21:e131-e141
41 A. Saxena, Surgical Oncology 2012; 21:e131-e141
42 Prognostic factors NELM systematic review Overall survival Univeriate multivariate R2 resection Extrahepatic disease Synchronous presentation Non-functional/pancreatic histopathology Tumour burden Poorly differentiation PFS Univariate Pancreatic/non-colonic poor differentiation Synchronous presentation postop complications R2 resection Tumour burden A. Saxena, Surgical Oncology 2012; 21:e131-e141
43 S. Mayo, Ann Surg Oncol 2010; 17:

44 Skye et al, J Am Coll Surg 2013; 26:
45 Aggressive surgery for NELM D. Elias et al D. Elias, Surgery 2003; 133: D. Elias, EJSO 2009; 35:
.")
46 Patients and Methods: Eleven patients with a metastatic endocrine tumor were selected before undergoing a right hepatectomy or a left hepatectomy passing along the median hepatic vein. Before the hepatectomy, patients underwent somatostatin receptor scintigraphy, computed tomography, magnetic resonance imaging, and ultrasonography (US). An intraoperative assessment (palpation and US) was also performed. Liver specimens were systematically cut into thin serial slices, 3- to 4-mm thick. A final histologic count of the total number of LM was obtained and compared with findings from each imaging technique Results: Compared with the final histologic count of LM, fewer than 50% of the LM were detected preoperatively. The accuracy was 24% for somatostatin receptor scintigraphy, 38% for computed tomography and US, and 49% for magnetic resonance imaging (the only imaging technique that detected half the number of LM). The size of the smallest LM was not greater than 2 mm in 54% of the patients. Conclusion: Half the number of LM from neuroendocrine tumors are undetectable on preoperative imaging. (Ann Surg 2010;251: ) D. Elias, Ann Surg 2010; 251:

47 S. Mayo, Ann Surg Oncol 2010; 17:

48 S. Fan, HPB 2014

49 S. Fan et al, HPB 2014

50 Y. Le Treut et al, Ann Surg 2013; 257:
51 Criteria for LTX for NELM Mazzaferro Well differentiated Ki67 < 5% Primary curative resected No associated extrahepatic resection No extrahepatic Mets Tumor load < 50% Portal drainage Age < 55 year Stable disease > 6 mo Le Treut Well differentiated Ki67 < 10% (up to 20?) Primary curative resected No associated extrahepatic resection No extrahepatic Mets No hepatomegaly Age < 45 Longer waiting time V. Mazzafferro, Journal of Hepatology 2007; 47: Y. Le Treut et al, Ann Surg 2013; 257:
52 Results therapy for NELM No RCT Selection bias? A. Frilling et al, Lancet Oncol 2014; 15: e8-21
53 Effect of therapy on survival NELM 40% 25% Yao, J Clin Oncol 2008;26:
54 Conclusion NET Rare but increasing Natural history: slowly growing Treatment Surgery at the moment only potential curative treatment Surgery important in Treatment primary tumour Treatment LM in G1-G2 tumours but high recurrence rate Multimodal multidisciplinary discussion No RCT
GEP NEN. Personalised approach. Curative and Palliative Surgery. ESMO Preceptorship Programme Neuroendocrine Neoplasms Lugano April 2018
 GEP NEN Personalised approach Curative and Palliative Surgery ESMO Preceptorship Programme Neuroendocrine Neoplasms Lugano 13 14 April 2018 Professor Andrea Frilling Department of Surgery and Cancer Imperial
GEP NEN Personalised approach Curative and Palliative Surgery ESMO Preceptorship Programme Neuroendocrine Neoplasms Lugano 13 14 April 2018 Professor Andrea Frilling Department of Surgery and Cancer Imperial
NEUROENDOCRINE CARCINOID TUMORS PANCREATIC NEUROENDOCRINE TUMORS
 University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Update on Surgical Management of NETs
 Update on Surgical Management of Neuroendocrine Tumors James R. Howe, M.D. Director, Surgical Oncology and Endocrine Surgery University of Iowa College of Medicine Distribution of NETs 2000-2004 27% ---
Update on Surgical Management of Neuroendocrine Tumors James R. Howe, M.D. Director, Surgical Oncology and Endocrine Surgery University of Iowa College of Medicine Distribution of NETs 2000-2004 27% ---
PNET 3/7/2015. GI and Pancreatic NETs. The Postgraduate Course in Breast and Endocrine Surgery. Decision Tree. GI and Pancreatic NETs.
 GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
Diagnosis abnormal morphology and /or abnormal biochemistry
 Diagnosis abnormal morphology and /or abnormal biochemistry MEN 1 GEP Tumours Pancreatico-Nodal (-Duodenal) Affects 35-80% of MEN1 patients Functioning or non functioning Hyperplasia microadenoma macrotumours
Diagnosis abnormal morphology and /or abnormal biochemistry MEN 1 GEP Tumours Pancreatico-Nodal (-Duodenal) Affects 35-80% of MEN1 patients Functioning or non functioning Hyperplasia microadenoma macrotumours
Index. Surg Oncol Clin N Am 15 (2006) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Gastrinoma: Medical Management. Haley Gallup
 Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
How to integrate surgery in the treatment of patients with liver-only metastatic disease
 How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
AN ARGUMENT FOR SURGERY FOR GASTRINOMA. Lauren Wilson R1 General Surgery
 AN ARGUMENT FOR SURGERY FOR GASTRINOMA Lauren Wilson R1 General Surgery WHAT IS A GASTRINOMA? Gastrin secreting cells derived from multipotential stem cells of endodermal origin or enteroendocrine cells
AN ARGUMENT FOR SURGERY FOR GASTRINOMA Lauren Wilson R1 General Surgery WHAT IS A GASTRINOMA? Gastrin secreting cells derived from multipotential stem cells of endodermal origin or enteroendocrine cells
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
SURGERY OF NETS. Iakovos N Nomikos MD FACS. Director and Chairman, Department of Surgery METAXA Memorial Cancer Hospital Piraeus Greece
 SURGERY OF NETS Iakovos N Nomikos MD FACS Director and Chairman, Department of Surgery METAXA Memorial Cancer Hospital Piraeus Greece Epidemiology 5-fold increase in occurrence of NETS over past 30 years
SURGERY OF NETS Iakovos N Nomikos MD FACS Director and Chairman, Department of Surgery METAXA Memorial Cancer Hospital Piraeus Greece Epidemiology 5-fold increase in occurrence of NETS over past 30 years
An Overview of NETS. Richard R.P. Warner M.D
 An Overview of NETS Richard R.P. Warner M.D Diagnosis and Treatment Approaches Carcinoid (and other NETs) not as benign as originally described 13-50% of all carcinoids have distant metastases when first
An Overview of NETS Richard R.P. Warner M.D Diagnosis and Treatment Approaches Carcinoid (and other NETs) not as benign as originally described 13-50% of all carcinoids have distant metastases when first
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Imaging of Neuroendocrine Metastases
 Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
MEDICAL MANAGEMENT OF METASTATIC GEP-NET
 MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
Case Presentation. Marianne Ellen Pavel. Charité University Medicine Berlin. ESMO Preceptorship on GI Neuroendocrine Tumors
 Case Presentation Marianne Ellen Pavel Charité University Medicine Berlin ESMO Preceptorship on GI Neuroendocrine Tumors Session 3; Singapore November 2, 2012 06.11.2012 Medical History 46-year-old man
Case Presentation Marianne Ellen Pavel Charité University Medicine Berlin ESMO Preceptorship on GI Neuroendocrine Tumors Session 3; Singapore November 2, 2012 06.11.2012 Medical History 46-year-old man
Unusual Pancreatic Neoplasms RTC 2/11/2011
 Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Diagnosing and monitoring NET
 Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
Type 2 gastric neuroendocrine tumor: report of one case
 Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS
 TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC
 Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Surgical treatment of neuroendocrine metastases
 Best Practice & Research Clinical Gastroenterology Vol. 19, No. 4, pp. 577 583, 2005 doi:10.1016/j.bpg.2005.04.003 available online at http://www.sciencedirect.com 6 Surgical treatment of neuroendocrine
Best Practice & Research Clinical Gastroenterology Vol. 19, No. 4, pp. 577 583, 2005 doi:10.1016/j.bpg.2005.04.003 available online at http://www.sciencedirect.com 6 Surgical treatment of neuroendocrine
NET εντέρου Τι νεότερο/ Νέες μελέτες. Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ
 NET εντέρου Τι νεότερο/ Νέες μελέτες Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ NET: A Diverse Group of Malignancies 1-3 Wide spectrum of malignancies arising in neuroendocrine cells throughout the body
NET εντέρου Τι νεότερο/ Νέες μελέτες Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ NET: A Diverse Group of Malignancies 1-3 Wide spectrum of malignancies arising in neuroendocrine cells throughout the body
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Friday, November 4, 2005 11:00-12:20 a. m. Pancreatic Tumors, Session 3 Chairman: D. O Toole, Clichy, France 11:20-11:50 a. m. Working Group Session Pathology and Genetics Group leaders: J. Y. Scoazec,
Friday, November 4, 2005 11:00-12:20 a. m. Pancreatic Tumors, Session 3 Chairman: D. O Toole, Clichy, France 11:20-11:50 a. m. Working Group Session Pathology and Genetics Group leaders: J. Y. Scoazec,
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust
 GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
Treatment of Colorectal Liver Metastases State of the Art
 Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Neuroendocrine Tumors: Just the Basics. George Fisher, MD PhD
 Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization
 Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization JP King PGY2 May 22, 2015 Neuroendocrine Tumor (NET) WHO Classification Location
Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization JP King PGY2 May 22, 2015 Neuroendocrine Tumor (NET) WHO Classification Location
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear
: CT, MRI, EUS, Nuclear") Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Grade 2 Ileum NET with liver and bone metastasis
 Grade 2 Ileum NET with liver and bone metastasis BERNARDO MARQUES ENDOCRINOLOGY DEPARTMENT PORTUGUESE INSTITUTE OF ONCOLOGY - COIMBRA April 2018, Lugano, Switzerland JPB, male, 67 years old April 2015
Grade 2 Ileum NET with liver and bone metastasis BERNARDO MARQUES ENDOCRINOLOGY DEPARTMENT PORTUGUESE INSTITUTE OF ONCOLOGY - COIMBRA April 2018, Lugano, Switzerland JPB, male, 67 years old April 2015
SIRT in the Management of Metastatic Neuroendocrine Tumors
 SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
Management of Stage IV Colorectal Cancer: Expanding the Horizon
 Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction
 NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
EXOCRINE: 93% Acinar Cells Duct Cells. ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others
 EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case
 Case Report Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case Yang Wang, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital,
Case Report Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case Yang Wang, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital,
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
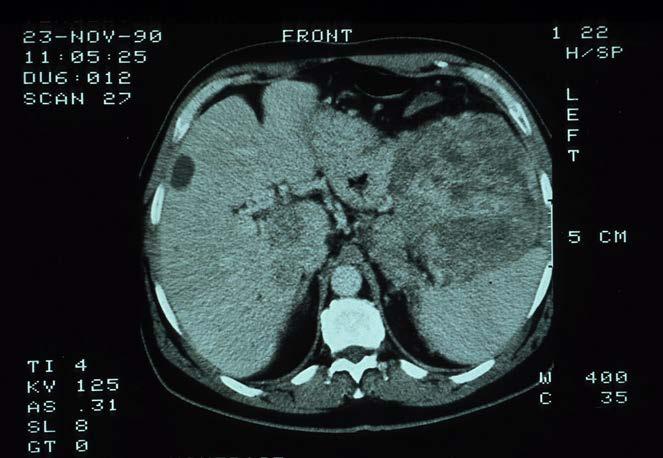
SECONDARIES: A PRELIMINARY REPORT
 HPB Surgery, 1990, Vol. 2, pp. 69-72 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORTS
HPB Surgery, 1990, Vol. 2, pp. 69-72 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORTS
Neuro-endocrine and pancreatic non-adenocarcinomas. Marc Engelbrecht, AMC, Amsterdam
 Neuro-endocrine and pancreatic non-adenocarcinomas Marc Engelbrecht, AMC, Amsterdam Pancreatic Tumors q Epithelial Exocrine q Mesenchymal Ductal Adenocarcinoma (85-95%) Metastasis Lymfoma Acinar Cell Carcinoma
Neuro-endocrine and pancreatic non-adenocarcinomas Marc Engelbrecht, AMC, Amsterdam Pancreatic Tumors q Epithelial Exocrine q Mesenchymal Ductal Adenocarcinoma (85-95%) Metastasis Lymfoma Acinar Cell Carcinoma
Liver surgery, acute GI tract bleeding
 Semmelweis University, Faculty of Medicine, 1 st Department of Surgery Liver surgery, acute GI tract bleeding Oszkár HAHN M.D. LIVER CYST US, CT, MRI Parasite (ELISA, eosinophil, anaphylaxy) Echinococcus
Semmelweis University, Faculty of Medicine, 1 st Department of Surgery Liver surgery, acute GI tract bleeding Oszkár HAHN M.D. LIVER CYST US, CT, MRI Parasite (ELISA, eosinophil, anaphylaxy) Echinococcus
Metastatic multiple endocrine neoplasia type 1: report of one case
 Case Report Metastatic multiple endocrine neoplasia type 1: report of one case Cheng Huang 1 *, Xiaodong Zhu 1 *, Xu Han 2 *, Wenhui Lou 2 1 Department of Liver Surgery, Fudan University Zhongshan Hospital,
Case Report Metastatic multiple endocrine neoplasia type 1: report of one case Cheng Huang 1 *, Xiaodong Zhu 1 *, Xu Han 2 *, Wenhui Lou 2 1 Department of Liver Surgery, Fudan University Zhongshan Hospital,
NICaN Pancreatic Neuroendocrine Tumour SACT protocols. 1.0 Dr M Eatock Final version issued
 Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
Community Case. Saeed Awan R5
 Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
The Surgical Management of Colorectal Metastases
 11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
Hot of the press. Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ
 Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear
: CT, MRI, EUS, Nuclear") Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Trattamento chirurgico delle lesioni epatiche secondarie difficili. Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica
 Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Treatment algorithm Neuroendocrine tumours. Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece
 Treatment algorithm Neuroendocrine tumours Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece Outline Presenting a meaningful algorithm Means used to develop algorithm
Treatment algorithm Neuroendocrine tumours Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece Outline Presenting a meaningful algorithm Means used to develop algorithm
Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide)
") GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Carcinoembryonic Antigen
 Other Names/Abbreviations CEA 190.26 - Carcinoembryonic Antigen Carcinoembryonic antigen (CEA) is a protein polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring
Other Names/Abbreviations CEA 190.26 - Carcinoembryonic Antigen Carcinoembryonic antigen (CEA) is a protein polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring
Rare GI Malignancies
 Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine Outline Gastrointestinal
Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine Outline Gastrointestinal
Carcinoid Tumors: The Beginning and End. Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011
 Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options
 State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
A retrospective analysis of neuroendocrine tumour of pancreas: a single institute study
 International Journal of Research in Medical Sciences Chheda YP et al. Int J Res Med Sci. 2015 Nov;3(11):3041-3045 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20150928
International Journal of Research in Medical Sciences Chheda YP et al. Int J Res Med Sci. 2015 Nov;3(11):3041-3045 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20150928
Neuroendocrine Tumors
 Neuroendocrine Tumors FCDS Annual Conference Boca Raton Marriott at Boca Center July 28, 2016 Steven Peace, BS, CTR Anatomy and Physiology of the (Neuro)Endocrine System WHO Classification, Tumor Grade
Neuroendocrine Tumors FCDS Annual Conference Boca Raton Marriott at Boca Center July 28, 2016 Steven Peace, BS, CTR Anatomy and Physiology of the (Neuro)Endocrine System WHO Classification, Tumor Grade
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Ronald C. Walker, MD, Prof of Radiology Vanderbilt University Medical Center Nashville, TN. Ga-DOTATATE PET/CT imaging Initial Vanderbilt experience
 Ronald C. Walker, MD, Prof of Radiology Vanderbilt University Medical Center Nashville, TN 68 Ga-DOTATATE PET/CT imaging Initial Vanderbilt experience Disclosures: No financial disclosures or conflicts
Ronald C. Walker, MD, Prof of Radiology Vanderbilt University Medical Center Nashville, TN 68 Ga-DOTATATE PET/CT imaging Initial Vanderbilt experience Disclosures: No financial disclosures or conflicts
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Case Report Pancreatic Aetiology for Massive Upper Gastrointestinal Haemorrhage in Pregnancy
 Case Reports in Surgery Volume 2016, Article ID 5491851, 4 pages http://dx.doi.org/10.1155/2016/5491851 Case Report Pancreatic Aetiology for Massive Upper Gastrointestinal Haemorrhage in Pregnancy Alexandra
Case Reports in Surgery Volume 2016, Article ID 5491851, 4 pages http://dx.doi.org/10.1155/2016/5491851 Case Report Pancreatic Aetiology for Massive Upper Gastrointestinal Haemorrhage in Pregnancy Alexandra
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
ITALIAN SURGICAL SOCIETY ENDOCRINE SURGERY SCHOOL LIVER METASTASIS FROM NEUROENDOCRINE TUMORS
 ITALIAN SURGICAL SOCIETY ENDOCRINE SURGERY SCHOOL LIVER METASTASIS FROM NEUROENDOCRINE TUMORS Gennaro Favia Liver metastasis from NETs Incidence 75% in NETs Knox CD, J Gastroint Surg 2006 .but 28-45% cases
ITALIAN SURGICAL SOCIETY ENDOCRINE SURGERY SCHOOL LIVER METASTASIS FROM NEUROENDOCRINE TUMORS Gennaro Favia Liver metastasis from NETs Incidence 75% in NETs Knox CD, J Gastroint Surg 2006 .but 28-45% cases
Strategies in the Management of Neuroendocrine Tumors. Dr. Jean Maroun Dr. Elena Tsvetkova
 Strategies in the Management of Neuroendocrine Tumors Dr. Jean Maroun Dr. Elena Tsvetkova 1 A ZORSE 2 Neuroendocrine Tumour Classification Neuroendocrine Tumours Carcinoid Tumours Pancreatic Neuroendocrine
Strategies in the Management of Neuroendocrine Tumors Dr. Jean Maroun Dr. Elena Tsvetkova 1 A ZORSE 2 Neuroendocrine Tumour Classification Neuroendocrine Tumours Carcinoid Tumours Pancreatic Neuroendocrine
Colorectal Liver Metastases Metachronous
 Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: Pancreatic NET Case ESMO preceptorship - Singapore
 NeuroEndocrine Tumors Diagnostic and therapeutic challenges: Pancreatic NET Case presentation @ ESMO preceptorship - Singapore Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Mr AR Real
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: Pancreatic NET Case presentation @ ESMO preceptorship - Singapore Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Mr AR Real
Multimodal management of neuroendocrine liver metastases
 DOI:10.1111/j.1477-2574.2010.00175.x HPB REVIEW ARTICLE Multimodal management of neuroendocrine liver metastases Andrea Frilling 1, Georgios C. Sotiropoulos 2, Jun Li 3, Oskar Kornasiewicz 1 & Ursula Plöckinger
DOI:10.1111/j.1477-2574.2010.00175.x HPB REVIEW ARTICLE Multimodal management of neuroendocrine liver metastases Andrea Frilling 1, Georgios C. Sotiropoulos 2, Jun Li 3, Oskar Kornasiewicz 1 & Ursula Plöckinger
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid
 Neuroendocrine Tumors and Lung Carcinoid") Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
A Nationwide Population-Based Study on the Survival of Patients with Pancreatic Neuroendocrine Tumors in The Netherlands
 World J Surg (2018) 42:490 497 DOI 10.1007/s00268-017-4278-y ORIGINAL SCIENTIFIC REPORT A Nationwide Population-Based Study on the Survival of Patients with Pancreatic Neuroendocrine Tumors in The Netherlands
World J Surg (2018) 42:490 497 DOI 10.1007/s00268-017-4278-y ORIGINAL SCIENTIFIC REPORT A Nationwide Population-Based Study on the Survival of Patients with Pancreatic Neuroendocrine Tumors in The Netherlands
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Liver surgery for colorectal liver metastases. Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham
 Liver surgery for colorectal liver metastases Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham Introduction: what do we do? UHB Liver Unit: Liver resections
Liver surgery for colorectal liver metastases Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham Introduction: what do we do? UHB Liver Unit: Liver resections
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy
 Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Chirurgie beim oligo-metastatischen NSCLC
 24. Ärzte-Fortbildungskurs in Klinischer Onkologie 20.-22. Februar 2014, Kantonsspital St. Gallen Chirurgie beim oligo-metastatischen NSCLC Prof. Dr. med. Walter Weder Klinikdirektor Thoraxchirurgie, UniversitätsSpital
24. Ärzte-Fortbildungskurs in Klinischer Onkologie 20.-22. Februar 2014, Kantonsspital St. Gallen Chirurgie beim oligo-metastatischen NSCLC Prof. Dr. med. Walter Weder Klinikdirektor Thoraxchirurgie, UniversitätsSpital
Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
 Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Management of Rare Liver Tumours
 Gian Luca Grazi Hepato-Biliary-Pancreatic Surgery National Cancer Institute Regina Elena Rome Fibrolamellar Carcinoma Mixed Hepato Cholangiocellular Carcinoma Hepatoblastoma Carcinosarcoma Primary Hepatic
Gian Luca Grazi Hepato-Biliary-Pancreatic Surgery National Cancer Institute Regina Elena Rome Fibrolamellar Carcinoma Mixed Hepato Cholangiocellular Carcinoma Hepatoblastoma Carcinosarcoma Primary Hepatic
How to deal with synchronous primary and liver metastases
 How to deal with synchronous primary and liver metastases Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB) Department of Surgery.
How to deal with synchronous primary and liver metastases Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB) Department of Surgery.
Endocrine Tumors of the Gastrointestinal System. F. V. Nowak Ohio University March 22, 2005
 Endocrine Tumors of the Gastrointestinal System F. V. Nowak Ohio University March 22, 2005 Gastroenteropancreatic Endocrine System Clear cells of endodermal origin found in the pancreas, stomach, small
Endocrine Tumors of the Gastrointestinal System F. V. Nowak Ohio University March 22, 2005 Gastroenteropancreatic Endocrine System Clear cells of endodermal origin found in the pancreas, stomach, small
Survivorship care of Neuroendocrine Tumours(NETs) from a Specialised Nursing Perspective
 from a Specialised Nursing Perspective") Survivorship care of Neuroendocrine Tumours(NETs) from a Specialised Nursing Perspective Avril Hull, Auckland District Health Board, New Zealand Kate Wakelin, Unicorn Foundation, Australia Philippa Davies,
Survivorship care of Neuroendocrine Tumours(NETs) from a Specialised Nursing Perspective Avril Hull, Auckland District Health Board, New Zealand Kate Wakelin, Unicorn Foundation, Australia Philippa Davies,
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Management of Liver Metastasis from Colorectal Carcinoma. Aisha White, M.D. SUNY Downstate Division of Transplantation
 Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Pancreatic Neuroendocrine Tumours
 UCLH Cancer Collaborative Pancreas Update Meeting 12 th July 2017 Pancreatic Neuroendocrine Tumours Dr. Christos Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior
UCLH Cancer Collaborative Pancreas Update Meeting 12 th July 2017 Pancreatic Neuroendocrine Tumours Dr. Christos Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior
WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer
 WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer Institute Overview Diagnosis: Gallium scan Biomarkers
WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer Institute Overview Diagnosis: Gallium scan Biomarkers
Title: What is the role of pre-operative PET/PET-CT in the management of patients with
 Title: What is the role of pre-operative PET/PET-CT in the management of patients with potentially resectable colorectal cancer liver metastasis? Pablo E. Serrano, Julian F. Daza, Natalie M. Solis June
Title: What is the role of pre-operative PET/PET-CT in the management of patients with potentially resectable colorectal cancer liver metastasis? Pablo E. Serrano, Julian F. Daza, Natalie M. Solis June
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Update on pancreatic neuroendocrine tumors
 Review Article Update on pancreatic neuroendocrine tumors Logan R. McKenna, Barish H. Edil Department of Surgery, University of Colorado, Academic Office One, Aurora, CO, USA Correspondence to: Barish
Review Article Update on pancreatic neuroendocrine tumors Logan R. McKenna, Barish H. Edil Department of Surgery, University of Colorado, Academic Office One, Aurora, CO, USA Correspondence to: Barish
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology
 Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Management of colorectal cancer liver metastases
 Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Intraoperative staging of GIT cancer using Intraoperative Ultrasound
 Intraoperative staging of GIT cancer using Intraoperative Ultrasound Thesis For Fulfillment of MSc Degree In Surgical Oncology By Abdelhalim Salah Abdelhalim Moursi M.B.B.Ch (Cairo University ) Supervisors
Intraoperative staging of GIT cancer using Intraoperative Ultrasound Thesis For Fulfillment of MSc Degree In Surgical Oncology By Abdelhalim Salah Abdelhalim Moursi M.B.B.Ch (Cairo University ) Supervisors
Evaluation and Management of Neuroendocrine Tumors
 Evaluation and Management of Neuroendocrine Tumors Jennifer Chan, MD, MPH Clinical Director, Program in Neuroendocrine and Carcinoid Tumors Dana-Farber/Brigham and Women's Cancer Center October 14, 2017
Evaluation and Management of Neuroendocrine Tumors Jennifer Chan, MD, MPH Clinical Director, Program in Neuroendocrine and Carcinoid Tumors Dana-Farber/Brigham and Women's Cancer Center October 14, 2017