Imaging: When to get MRI, CT or PET-CT?
|
|
|
- Amy Sabina Townsend
- 5 years ago
- Views:
Transcription


1 Imaging: When to get MRI, CT or PET-CT? Alina Uzelac, D.O. Assistant Clinical Professor Neuroradiology UCSF Department of Radiology and Biomedical Imaging San Francisco General Hospital Overview CT MRI PET-CT Advanced Imaging Techniques 1
2 Imaging Studies Initial Assessment Head and Neck Ca: degree of local infiltration regional lymph nodes involvement presence of distant metastases second primary tumors Local Infiltration/Tumor Extent 2




3 Orbital and Intracranial Extension Sinonasal Undifferentiated Carcinoma Ax CT Inseparable medial rectus muscle 59 F w/ trauma. Orbital and Intracranial Extension Sinonasal Undifferentiated Carcinoma Floor of anterior cranial fossa Medial rectus Cor CT 3
4 CT or MRI All Pts. initial staging MRI or CT for HEAD and NECK SCCa. particularly useful in Pts. with clinically N0 neck. CT vs MRI CT and MRI are complementary to the clinical examination. and may also be complementary to each other. 4




5 33 M with an inverted papilloma degenerated into SCCa CT = superior for cortical bone erosion Bone window Ax CT w/ Local Invasion Paraglottic fat extension 56 F w/ epiglottic mass 5


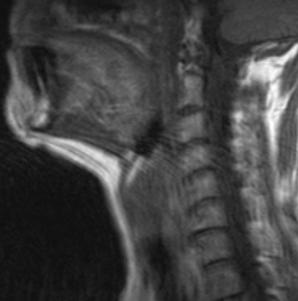
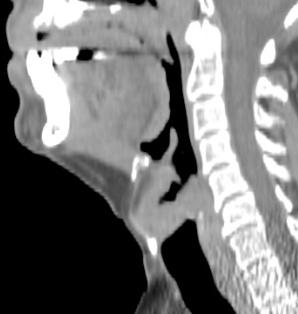
6 CT versus MRI? Ax CT w/ CT Ax T1 MRI Preepiglottic Space Extension Base of Tongue SCCa CT versus MRI? Preepiglottic Space Extension Supraglottic SCCa Sag CT w/ CT Sag T1 Motion MRI 6





7 Prevertebral Extension Pyriform Sinus SCCa Imaging Studies Initial Assessment Head and Neck Ca: degree of local infiltration regional lymph nodes involvement presence of distant metastases second primary tumors 7

8 CT versus MRI? Small Abnormal LNs Ethmoid Sinus SCCa Recurrence Preserved fatty hilum Thickened cortex 8




9 PET-CT Clinical N0 neck can be PET negative, given small node volume (<1mL). PET-CT Tongue SCCA Ax CT Small LN for PET 9



10 Thyroid Cartilage Invasion Laryngeal SCCa Ax CT w/ Ax CT w/ CT adequate for ossified cartilage Thyroid Cartilage Invasion Laryngeal SCCa Ax T1 Ax T1 w/ Gd MRI superior for marrow infiltration 10



11 Thyroid Cartilage Invasion Laryngeal SCCa Loss of nl fat bright signal Abnormal enhancement Ax T1 Ax T1 w/ Gd MRI superior for marrow infiltration Thyroid Cartilage Invasion Laryngeal SCCa Loss of fat suppression Ax T2 MRI superior marrow infiltration 11


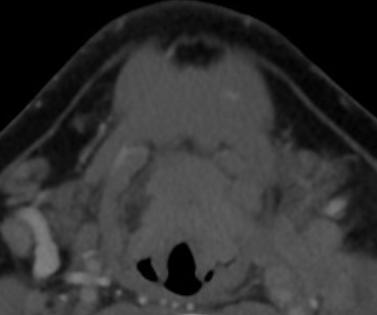
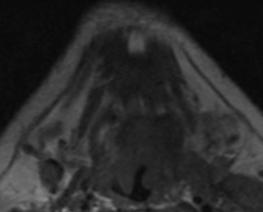
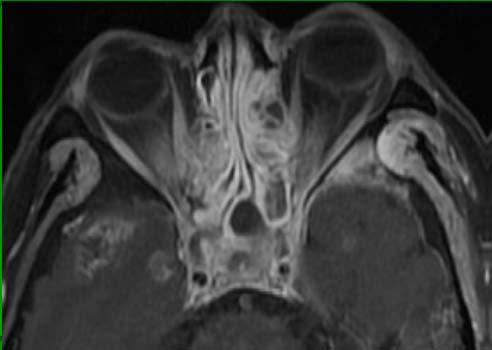
12 33 M w/ sinonasal SCCa s/p resection returns w/ brain abscess MRI Cor T2 MRI Cor T1 w/ MRI > CT for distinguishing malignancy from mucus SCCa recurrence MRI Cor T2 MRI Cor T1 w/ MRI > CT for distinguishing malignancy from mucus 12




13 SCCa recurrence ax CT w/ cor CT w/ Returns w/ erythema and swelling Ax CT SCCa recurrence perineural spread cavernous sinus 13




.")

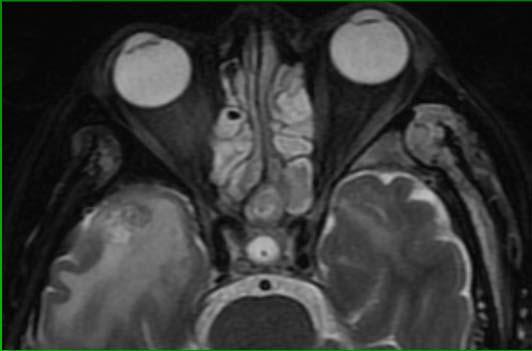
14 MRI over CT Perineural spread of tumor (use thinner slice thickness - 3 mm) Intracranial extension Nasopharyngeal Ca (initial staging and follow up). Intracranial Extension Nasopharyngeal Ca bone erosion along vidian canal Ax T1 w/ ax CT 14

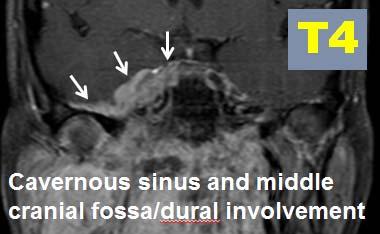
15 Intracranial Direct Extension SNUC Dural invasion Cor T1 Gd MRI Staging of NPC 15
16 PET-CT? Routine PET for initial staging, unless: Equivocal findings on CT or MRI. High risk of distant metastatic disease. Search for 2 nd primary. Nodal SCCa unknown primary. PET-CT To be done before Bx: Guide to area of highest yield Bx can result in high uptake. 16




17 PET-CT Superior to CT Cor PET- CT ax CT Cricoid Cartilage Invasion Subglottic SCCa Treatment Response MRI PET-CT Done 3 months post treatment completion (prevent false positives). 17
18 Nonsurgical Treatment Response - radiologic resolution = cure - reduction in size < 50% = failure % reduction = indeterminate (close surveillance) Advanced Imaging Techniques Predicting Tumor Response PET: High SUV = poor response Diffusion (DWI) MRI. Dynamic perfusion MRI (vs CT): Tumor hypoxia = radioresistance (and chemoresistance). Increased tumor perfusion => improved locoregional control. 18



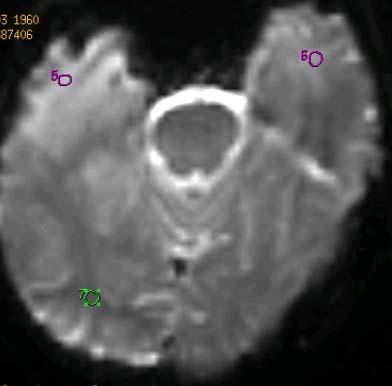
19 MRI Diffusion Weighted Sequence for Tx response prediction ax DWI ax ADC Nodal metastasis Staging MRI tongue SCCa MRI Diffusion Weighted Sequence for Tx response Staging MRI Follow up ax DWI ax DWI Nodal metastasis resolution of abnl diffusion = Tx response 19
 PET-CT (metastases)")



20 Recurrence Imaging MRI (extent of tumor) PET-CT (metastases) MRI Diffusion Weighted Sequence for recurrence ax DWI ax ADC Hx mod diff SCCa tongue p-hemiglossectomy, chemort, followed by LND. Recurrence, then radical neck dissection w/ pectoralis flap. 20








21 Recurrence MRI for extent of tumor 52 M w/ Hx NPCA s/p XRT in China 4 years prior Recurrence PET for metastases 35 M presents with back pain 2 years after NPC treatment Solitary NPC metastasis biopsy-proven. 21






22 Recurrence PET for flap flap 64-year-old male status post left total maxillectomy and free ALT flap for SCCa, post chemo and radiation therapy. Treatment Complications Imaging Complications occasionally incidentally imaged. MRI PET-CT 22

23 Post XRT Complications Skull base XRT changes PET negative 44yo s/p XRT for NPC. Post XRT Complications Skull base XRT changes PET negative 44yo s/p XRT for NPC. 23




24 Post XRT Complications Ax T1 w/ Gd Cor FLAIR Bitemporal XRT necrosis Post XRT Complications No abnormal hypermetabolism Ax T1 w/ Gd Cor FLAIR Ax PET Bitemporal XRT necrosis 24

25 Post XRT Complications Brain necrosis 5 years post XRT for NPC Post XRT Complications Ax Gd perfusion Bitemporal XRT necrosis 25


26 Oxaliplatin and CyberKnife Completed 07/2013 for recurrent NPC Returns 12/2013 w/ L jaw pain and trismus Oxaliplatin and CyberKnife Completed 07/2013 for recurrent NPC XRT necrosis central skull base and nasopharynx 26

27 Acute Muscle Denervation P-XRT Masticator mm. acute denervation XRT necrosis central skull base and NP PET Pitfall Acute Muscle Denervation = High Uptake Right extraocular mucles acute denervation 27



28 PET Pitfall Acute Muscle Denervation = High Uptake Right extraocular mucles acute denervation 84 M recurrent parotid malignancy perineural spread cavernous sinus. Whole Body PET-MRI 28





29 Siemens integrated PET-MRI = simultaneous imaging = superior registration Whole Body PET-MRI PET-MRI Siemens integrated PET-MRI = simultaneous imaging = superior registration 29
30 TAKE HOME POINTS Head and Neck Ca Imaging Initial Staging: CT or MRI. MRI for NPC Consider PET-CT: Distant metastases Positive neck nodes without identifiable primary Look for second primary TAKE HOME POINTS Head and Neck Ca Imaging Predicting response ADVANCED imaging: MRI Diffusion and Perfusion tumor oxygenation PET MRI-PET! 30




31 TAKE HOME POINTS Head and Neck Ca Imaging Surveillance: MRI Recurrence: MRI and PET Thank you! 31
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
The many faces of extranodal lymphoma
 The many faces of extranodal lymphoma Frank Pameijer Departments of Radiology and Radiation Oncology University Medical Center Utrecht Special thanks to Ilona M Schmalfuss, MD University of Florida Gainesville,
The many faces of extranodal lymphoma Frank Pameijer Departments of Radiology and Radiation Oncology University Medical Center Utrecht Special thanks to Ilona M Schmalfuss, MD University of Florida Gainesville,
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
Neuroradiology Case of the Day
 Neuroradiology Case of the Day 76 th CAR Annual Meeting, Montreal, Quebec April 27, 2013 Eugene Yu, MD Assistant Professor of Radiology and Otolaryngology-Head and Neck Surgery Head and Neck Imaging Princess
Neuroradiology Case of the Day 76 th CAR Annual Meeting, Montreal, Quebec April 27, 2013 Eugene Yu, MD Assistant Professor of Radiology and Otolaryngology-Head and Neck Surgery Head and Neck Imaging Princess
Neck Imaging Reporting and Data System: An Atlas of NI-RADS Categories for Head and Neck Cancer
 Neck Imaging Reporting and Data System: An Atlas of NI-RADS Categories for Head and Neck Cancer Bethany Cavazuti Patricia Hudgins Tanya Rath Char Branstetter Kristen Baugnon Amanda Corey Ashley Aiken Disclosures
Neck Imaging Reporting and Data System: An Atlas of NI-RADS Categories for Head and Neck Cancer Bethany Cavazuti Patricia Hudgins Tanya Rath Char Branstetter Kristen Baugnon Amanda Corey Ashley Aiken Disclosures
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
RADIOLOGY TEACHING CONFERENCE
 RADIOLOGY TEACHING CONFERENCE John Athas, MD Monica Tadros, MD Columbia University, College of Physicians & Surgeons Department of Otolaryngology- Head & Neck Surgery September 27, 2007 CT SCAN IMAGING
RADIOLOGY TEACHING CONFERENCE John Athas, MD Monica Tadros, MD Columbia University, College of Physicians & Surgeons Department of Otolaryngology- Head & Neck Surgery September 27, 2007 CT SCAN IMAGING
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Case Studies in the Skull Base
 Case Studies in the Skull Base Amy C Tsai, MD Neuroradiology Fellow Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA No disclosures related
Case Studies in the Skull Base Amy C Tsai, MD Neuroradiology Fellow Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA No disclosures related
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Nasopharyngeal Carcinoma. Rusty Stevens, MD Christopher Rassekh, MD
 Nasopharyngeal Carcinoma Rusty Stevens, MD Christopher Rassekh, MD Introduction Rare in the US, more common in Asia High index of suspicion required for early diagnosis Nasopharyngeal malignancies SCCA
Nasopharyngeal Carcinoma Rusty Stevens, MD Christopher Rassekh, MD Introduction Rare in the US, more common in Asia High index of suspicion required for early diagnosis Nasopharyngeal malignancies SCCA
(loco-regional disease)
") (loco-regional disease) (oral cavity) (circumvillae papillae) (subsite) A (upper & lower lips) B (buccal membrane) C (mouth floor) D (upper & lower gingiva) E (hard palate) F (tongue -- anterior 2/3 rds
(loco-regional disease) (oral cavity) (circumvillae papillae) (subsite) A (upper & lower lips) B (buccal membrane) C (mouth floor) D (upper & lower gingiva) E (hard palate) F (tongue -- anterior 2/3 rds
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Perineural Tumor Spread. In Head & Neck Cancer
 Head and Neck Imaging Conference University of Perineural Tumor Spread In Head & Neck Cancer Philip Chapman MD University of Alabama, Birmingham OBJECTIVES: 1. Define (PNTS) 2. Distinguish from pathologic
Head and Neck Imaging Conference University of Perineural Tumor Spread In Head & Neck Cancer Philip Chapman MD University of Alabama, Birmingham OBJECTIVES: 1. Define (PNTS) 2. Distinguish from pathologic
Sinonasal Tumors. Objectives. Objectives. Incidence of Paranasal Sinus Tumors. Demographics of Paranasal Sinus Tumors. Paranasal Sinus Tumors
 Sinonasal Tumors Objectives Incidence and demographics of sinonasal tumors Separating tumors from inflammatory changes Common and notable histologic types of sinonasal tumors Staging of sinonasal tumors
Sinonasal Tumors Objectives Incidence and demographics of sinonasal tumors Separating tumors from inflammatory changes Common and notable histologic types of sinonasal tumors Staging of sinonasal tumors
Oral cancer: Prognosis & Treatment. Dr. Hani Al Sheikh Radhi
 Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
AJCC update Disclosures. AJCC TNM staging system. Objectives:
 Disclosures AJCC update 2018 Remy Lobo, MD remylobo@med.umich.edu remy.lobo@hsc.utah.edu No relevant disclosures Information is based on the 8 th AJCC manual Amin MB, Edge SB, Greene FL et al, eds. AJCC
Disclosures AJCC update 2018 Remy Lobo, MD remylobo@med.umich.edu remy.lobo@hsc.utah.edu No relevant disclosures Information is based on the 8 th AJCC manual Amin MB, Edge SB, Greene FL et al, eds. AJCC
Disclosures. Diffusion and Perfusion Imaging in the Head and Neck. Learning objectives ???
 Disclosures No relevant financial disclosures Diffusion and Perfusion Imaging in the Head and Neck Ashok Srinivasan, MD Associate Professor Director of Neuroradiology University of Michigan Health System
Disclosures No relevant financial disclosures Diffusion and Perfusion Imaging in the Head and Neck Ashok Srinivasan, MD Associate Professor Director of Neuroradiology University of Michigan Health System
Learning Objectives. Head and Neck Cancer: Post-Treatment Changes. Neck Dissection Classification * Radical neck dissection. Radical Neck Dissection
 Head and Neck Cancer: Post-Treatment Changes Daniel W. Williams III, MD Learning Objectives In patients treated for H/N Cancer: Describe the various types of neck dissections Explain reconstruction techniques
Head and Neck Cancer: Post-Treatment Changes Daniel W. Williams III, MD Learning Objectives In patients treated for H/N Cancer: Describe the various types of neck dissections Explain reconstruction techniques
You Can t Avoid Errors
 Avoiding Errors in Head and Neck Cancer Imaging Lawrence E. Ginsberg, M.D. Departments of Diagnostic Imaging and Head and Neck Surgery University of Texas M.D. Anderson Cancer Center Houston, Texas You
Avoiding Errors in Head and Neck Cancer Imaging Lawrence E. Ginsberg, M.D. Departments of Diagnostic Imaging and Head and Neck Surgery University of Texas M.D. Anderson Cancer Center Houston, Texas You
PILOT STUDY OF CONCURRENT CHEMO-RADIOTHERAPY FOR ADVANCED NASOPHARYNGEAL CARCINOMA (Forum for Nuclear Cooperation in Asia)
") PILOT STUDY OF CONCURRENT CHEMO-RADIOTHERAPY FOR ADVANCED NASOPHARYNGEAL CARCINOMA (Forum for Nuclear Cooperation in Asia) Dr. Miriam Joy C. Calaguas Dept. of Radiation Oncology St. Luke s Medical Center
PILOT STUDY OF CONCURRENT CHEMO-RADIOTHERAPY FOR ADVANCED NASOPHARYNGEAL CARCINOMA (Forum for Nuclear Cooperation in Asia) Dr. Miriam Joy C. Calaguas Dept. of Radiation Oncology St. Luke s Medical Center
Management of Salivary Gland Malignancies. No Disclosures or Conflicts of Interest. Anatomy 10/4/2013
 Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient
 Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
PET/CT F-18 FDG. Objectives. Basics of PET/CT Imaging. Objectives. Basic PET imaging
 Basics of PET/CT Imaging Kevin Robinson, DO Department of Radiology Michigan State University Objectives Basic PET imaging Evaluating the therapeutic response Evaluating the big 5 Lymphoma Breast Lung
Basics of PET/CT Imaging Kevin Robinson, DO Department of Radiology Michigan State University Objectives Basic PET imaging Evaluating the therapeutic response Evaluating the big 5 Lymphoma Breast Lung
JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City.
 JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City. HNSCC with a global incidence of over 500,000 cases and 200,000 deaths annually is the leading cause of mortality and
JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City. HNSCC with a global incidence of over 500,000 cases and 200,000 deaths annually is the leading cause of mortality and
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
L ARYNX S TAGING F ORM
 CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
The following images were all acquired using a CTI Biograph
 Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
NI-RADS: Structured Reporting for Head and Neck Cancer
 NI-RADS: Structured Reporting for Head and Neck Cancer ASHNR 2018 Disclosures Part of group that initiated NI-RADS Colleagues A. Aiken & P. Hudgins: ACR NIRADS committee members Kristen Lloyd Baugnon,
NI-RADS: Structured Reporting for Head and Neck Cancer ASHNR 2018 Disclosures Part of group that initiated NI-RADS Colleagues A. Aiken & P. Hudgins: ACR NIRADS committee members Kristen Lloyd Baugnon,
NASOPHARYNX MALIGNANT NEOPLASM MOHAMMED ALESSA MBBS, FRCSC ASSISTANT PROFESSOR, CONSULTANT OTOLARYNGOLOGY, HEAD & NECK SURGRY KING SAUD UNIVERSITY
 NASOPHARYNX MALIGNANT NEOPLASM MOHAMMED ALESSA MBBS, FRCSC ASSISTANT PROFESSOR, CONSULTANT OTOLARYNGOLOGY, HEAD & NECK SURGRY KING SAUD UNIVERSITY Epidemiology Anatomy Histopathology Clinical presentation
NASOPHARYNX MALIGNANT NEOPLASM MOHAMMED ALESSA MBBS, FRCSC ASSISTANT PROFESSOR, CONSULTANT OTOLARYNGOLOGY, HEAD & NECK SURGRY KING SAUD UNIVERSITY Epidemiology Anatomy Histopathology Clinical presentation
ARTICLE. Imaging the cranial nerves in cancer
 Cancer Imaging (2004) 4, S1 S5 DOI: 10.1102/1470-7330.2004.0006 CI ARTICLE Vincent Chong Department of Diagnostic Radiology, Singapore General Hospital, Outram Road, Singapore 169608, Singapore Corresponding
Cancer Imaging (2004) 4, S1 S5 DOI: 10.1102/1470-7330.2004.0006 CI ARTICLE Vincent Chong Department of Diagnostic Radiology, Singapore General Hospital, Outram Road, Singapore 169608, Singapore Corresponding
Anatomy of Head of Neck Cancer
 Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Imaging of Pediatric MSK Tumors
 Imaging of Pediatric MSK Tumors Kirsten Ecklund, M.D. Boston Children s Hospital Harvard Medical School kirsten.ecklund@childrens.harvard.edu Tumor Imaging Goals Diagnosis Lesion characterization Benign
Imaging of Pediatric MSK Tumors Kirsten Ecklund, M.D. Boston Children s Hospital Harvard Medical School kirsten.ecklund@childrens.harvard.edu Tumor Imaging Goals Diagnosis Lesion characterization Benign
New Visions in PET: Surgical Decision Making and PET/CT
 New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
Merkel Cell Carcinoma Case # 2
 DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Whole Body MRI. Dr. Nina Tunariu. Prostate Cancer recurrence, progression and restaging
 Whole Body MRI Prostate Cancer recurrence, progression and restaging Dr. Nina Tunariu Consultant Radiology Drug Development Unit and Prostate Targeted Therapies Group 12-13 Janeiro 2018 Evolving Treatment
Whole Body MRI Prostate Cancer recurrence, progression and restaging Dr. Nina Tunariu Consultant Radiology Drug Development Unit and Prostate Targeted Therapies Group 12-13 Janeiro 2018 Evolving Treatment
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER
 CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic space
 Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
PET IMAGING (POSITRON EMISSION TOMOGRAPY) FACT SHEET
 FACT SHEET") Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
1. Resident Doctor, 2. Professor, Geetanjali Medical College & Hospital, Udaipur, Rajasthan.
 International Journal of Medical Science and Education An official Publication of Association for Scientific and Medical Education (ASME) www.ijmse.com Original Research Article pissn- 2348 4438 eissn-2349-3208
International Journal of Medical Science and Education An official Publication of Association for Scientific and Medical Education (ASME) www.ijmse.com Original Research Article pissn- 2348 4438 eissn-2349-3208
TEDDY PET/CT AT THE U OF U READY FOR THE UNCLEAR MEDICINE? Case #1. Case #1 60 y/o male with MGUS, PET/CT to evaluate for active multiple myeloma
 PET/CT AT THE U OF U READY FOR THE UNCLEAR MEDICINE? STOP DICTATING SO LOUD OR I WILL EAT YOU TEDDY Case #1 60 y/o male with MGUS, PET/CT to evaluate for active multiple myeloma Case #1 1.5 cm midline
PET/CT AT THE U OF U READY FOR THE UNCLEAR MEDICINE? STOP DICTATING SO LOUD OR I WILL EAT YOU TEDDY Case #1 60 y/o male with MGUS, PET/CT to evaluate for active multiple myeloma Case #1 1.5 cm midline
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
Cancer of the Oral Cavity
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Cancer of the Oral Cavity Ashok Shaha Principals of Management of Oral Cancer A)
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Cancer of the Oral Cavity Ashok Shaha Principals of Management of Oral Cancer A)
Nasal Cavity CS Tumor Size (Revised: 02/03/2010)
") Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor
Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor
2. Guidelines for Reporting Head and Neck Tumours
 39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
Unknown Cases from the Participants
 Unknown Cases from the Participants Case 1: 1 Case 1: Case 1: DDX? Answer on next slide Case 1: MS V5 Neuropathy Case 2: Case 2: 76 year old woman Ultrasound for multinodular goiter finds suspicious nodule
Unknown Cases from the Participants Case 1: 1 Case 1: Case 1: DDX? Answer on next slide Case 1: MS V5 Neuropathy Case 2: Case 2: 76 year old woman Ultrasound for multinodular goiter finds suspicious nodule
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
MALIGNANT TUMOURS OF THE JAWS
 MALIGNANT TUMOURS OF THE JAWS MALIGNANT TUMOURS OF THE JAWS Squamous cell carcinoma Osteogenic sarcoma Chondrosarcoma Fibrosarcoma Malignant lymphomas (incl. Burkitt s) Multiple myeloma Ameloblastoma Secondary
MALIGNANT TUMOURS OF THE JAWS MALIGNANT TUMOURS OF THE JAWS Squamous cell carcinoma Osteogenic sarcoma Chondrosarcoma Fibrosarcoma Malignant lymphomas (incl. Burkitt s) Multiple myeloma Ameloblastoma Secondary
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Head and Neck Pathology. Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital)
") Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital) Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital) Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Lymphoma Read with the experts
 Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Imaging Work-Up of a Neck Mass - Adults & Children
 Disclosures Imaging Work-Up of a Neck Mass - Adults & Children I have nothing to disclose Christine M Glastonbury MBBS Professor of Radiology & Biomedical Imaging Otolaryngology-Head & Neck Surgery and
Disclosures Imaging Work-Up of a Neck Mass - Adults & Children I have nothing to disclose Christine M Glastonbury MBBS Professor of Radiology & Biomedical Imaging Otolaryngology-Head & Neck Surgery and
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Katsuro Sato. Department of Speech, Language and Hearing Sciences, Niigata University of Health and Welfare, Niigata, Japan
 Report Niigata Journal of Health and Welfare Vol. 12, No. 1 Retrospective analysis of head and neck cancer cases from the database of the Niigata Prefecture Head and Neck Malignant Tumor Registration Committee
Report Niigata Journal of Health and Welfare Vol. 12, No. 1 Retrospective analysis of head and neck cancer cases from the database of the Niigata Prefecture Head and Neck Malignant Tumor Registration Committee
Perineural Tumor Spread (PNS) Perineural Tumor Spread (PNS) PNS Anatomic Considerations. Perineural Tumor Spread-Imaging
 Perineural Tumor Spread (PNS) PNS Anatomic Considerations. Perineural Tumor Spread-Imaging") Imaging of Perineural Tumor Spread in Head and Neck Cancer Lawrence E. Ginsberg, MD Departments of Diagnostic Radiology and Head and Neck Surgery University of Texas M.D. Anderson Cancer Center Houston,
Imaging of Perineural Tumor Spread in Head and Neck Cancer Lawrence E. Ginsberg, MD Departments of Diagnostic Radiology and Head and Neck Surgery University of Texas M.D. Anderson Cancer Center Houston,
Treatment for Supraglottic Ca History: : Total Laryngectomy y was routine until early 50 s, when XRT was developed Ogura and Som developed the one-sta
 Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Laurie A. Loevner, MD
 Laurie A. Loevner, MD Chief, Division of Neuroradiology UPHS Professor of Radiology, Otorhinolaryngology: Head & Neck Surgery, Neurosurgery, and Ophthalmology University of Pennsylvania Health System Disclosures
Laurie A. Loevner, MD Chief, Division of Neuroradiology UPHS Professor of Radiology, Otorhinolaryngology: Head & Neck Surgery, Neurosurgery, and Ophthalmology University of Pennsylvania Health System Disclosures
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Neuroradiology MR Protocols
 Neuroradiology MR Protocols Brain protocols N 1: Brain MRI without contrast N 2: Pre- and post-contrast brain MRI N 3 is deleted N 4: Brain MRI without or pre-/post-contrast (seizure protocol) N 5: Pre-
Neuroradiology MR Protocols Brain protocols N 1: Brain MRI without contrast N 2: Pre- and post-contrast brain MRI N 3 is deleted N 4: Brain MRI without or pre-/post-contrast (seizure protocol) N 5: Pre-
NI-RADS: Head & Neck Cancer Imaging Surveillance. Goals of the RADS templates: Goals: Disclosures ACR NI-RADS
 NI-RADS: Head & Neck Cancer Imaging Surveillance ASHNR 2017 none Disclosures Ashley H. Aiken, M.D. Associate Professor of Radiology Emory University School of Medicine ACR RADS (Reporting and Data Systems)
NI-RADS: Head & Neck Cancer Imaging Surveillance ASHNR 2017 none Disclosures Ashley H. Aiken, M.D. Associate Professor of Radiology Emory University School of Medicine ACR RADS (Reporting and Data Systems)
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Abdominal applications of DWI
 Postgraduate course, SPR San Antonio (Texas), May 14-15, 2013 Abdominal applications of DWI Rutger A.J. Nievelstein Wilhelmina Children s s Hospital, Utrecht (NL) Outline What is DWI? How to perform? Challenges
Postgraduate course, SPR San Antonio (Texas), May 14-15, 2013 Abdominal applications of DWI Rutger A.J. Nievelstein Wilhelmina Children s s Hospital, Utrecht (NL) Outline What is DWI? How to perform? Challenges
Nasopharyngeal Cancer. Nasopharynx: Anatomy. Disclosures. Objectives. Head and Neck Cancer I. Thank you. Nasopharynx
 Head and Neck Cancer I Nasopharyngeal Cancer Nancy J. Fischbein, MD Neuroradiology Section Stanford Medical Center Disclosures None* Objectives To briefly review the anatomy of the nasopharynx To discuss
Head and Neck Cancer I Nasopharyngeal Cancer Nancy J. Fischbein, MD Neuroradiology Section Stanford Medical Center Disclosures None* Objectives To briefly review the anatomy of the nasopharynx To discuss
An Introduction to PET Imaging in Oncology
 January 2002 An Introduction to PET Imaging in Oncology Janet McLaren, Harvard Medical School Year III Basics of PET Principle of Physiologic Imaging: Allows in vivo visualization of structures by their
January 2002 An Introduction to PET Imaging in Oncology Janet McLaren, Harvard Medical School Year III Basics of PET Principle of Physiologic Imaging: Allows in vivo visualization of structures by their
Salivary Glands tumors
 Salivary Glands tumors Sal.Gl. 1 Salivary Glands tumors Work-up procedure TNM staging Primary treatment Follow-up Treatment of recurrent and/or metastatic disease References Sal.Gl. 2 Standard clinical
Salivary Glands tumors Sal.Gl. 1 Salivary Glands tumors Work-up procedure TNM staging Primary treatment Follow-up Treatment of recurrent and/or metastatic disease References Sal.Gl. 2 Standard clinical
Organ preservation in laryngeal cancer
 Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
ESMO Perceptorship H&N cancer Epidemiology, Anatomy and Workup 16 March 2018
 ESMO Perceptorship H&N cancer Epidemiology, Anatomy and Workup 16 March 2018 Dr. Victor Ho-Fun Lee MBBS, MD, FRCR, FHKCR, FHKAM (Radiology) Clinical Associate Professor Department of Clinical Oncology
ESMO Perceptorship H&N cancer Epidemiology, Anatomy and Workup 16 March 2018 Dr. Victor Ho-Fun Lee MBBS, MD, FRCR, FHKCR, FHKAM (Radiology) Clinical Associate Professor Department of Clinical Oncology
What is ACC? (Adenoid Cystic Carcinoma)
") What is ACC? (Adenoid Cystic Carcinoma) 10-9-10 Where ACC Occurs ACC (Adenoid Cystic Carcinoma) is a rare and unique form of cancer that is known to be unpredictable in nature, with a typical growth pattern
What is ACC? (Adenoid Cystic Carcinoma) 10-9-10 Where ACC Occurs ACC (Adenoid Cystic Carcinoma) is a rare and unique form of cancer that is known to be unpredictable in nature, with a typical growth pattern
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Survey of Laryngeal Cancer at SBUH comparing 108 cases seen here from to the NCDB of 9,256 cases diagnosed nationwide in 2000
 Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Guidelines for the Management of Head and Neck Cancer
 Guidelines for the Management of Head and Neck Cancer Version: 2 Ref: AngCN-SSG-NH5 Contents 1. Introduction... 3 2. General Principles... 3 3. Site Specific Guidelines... 4 3.1 Oral Cavity... 4 3.2 Oropharynx...
Guidelines for the Management of Head and Neck Cancer Version: 2 Ref: AngCN-SSG-NH5 Contents 1. Introduction... 3 2. General Principles... 3 3. Site Specific Guidelines... 4 3.1 Oral Cavity... 4 3.2 Oropharynx...
LYMPHATIC DRAINAGE IN THE HEAD & NECK
 LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Head & Neck Contouring
 Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
11/10/2015. Prostate cancer in the U.S. Multi-parametric MRI of Prostate Diagnosis and Treatment Planning. NIH estimates for 2015.
 Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS
 MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
A220: Larynx cancer tissues. (formalin fixed)
") A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
IMPACT OF MAGNETIC RESONANCE IMAGING VERSUS CT ON NASOPHARYNGEAL CARCINOMA: PRIMARY TUMOR TARGET DELINEATION FOR RADIOTHERAPY
 IMPACT OF MAGNETIC RESONANCE IMAGING VERSUS CT ON NASOPHARYNGEAL CARCINOMA: PRIMARY TUMOR TARGET DELINEATION FOR RADIOTHERAPY Na-Na Chung, MD, 1 Lai-Lei Ting, MD, 1,2 Wei-Chung Hsu, MD, 3 Louis Tak Lui,
IMPACT OF MAGNETIC RESONANCE IMAGING VERSUS CT ON NASOPHARYNGEAL CARCINOMA: PRIMARY TUMOR TARGET DELINEATION FOR RADIOTHERAPY Na-Na Chung, MD, 1 Lai-Lei Ting, MD, 1,2 Wei-Chung Hsu, MD, 3 Louis Tak Lui,
From GTV to CTV: A Critical Step Towards Cure. Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017
 From GTV to CTV: A Critical Step Towards Cure Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017 Head and Neck Cancer Model for Understanding CTV Expansion Radiation
From GTV to CTV: A Critical Step Towards Cure Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017 Head and Neck Cancer Model for Understanding CTV Expansion Radiation
Thoracic Recurrences. Soft tissue recurrence
 Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of