Expert panel observations
|
|
|
- Patricia Sherman
- 5 years ago
- Views:
Transcription
1 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory
2 Three big issues in BCSP pathology serrated pathology & what do we do about it expected polyp cancers (pt1 disease) & what we do about it expected the large adenomatous polyp of the sigmoid colon not expected (certainly not the amount nor the diagnostic difficulties) Gloucestershire Cellular Pathology Laboratory
3 Three big issues in BCSP pathology serrated pathology & what do we do about it expected polyp cancers (pt1 disease) & what we do about it expected the large adenomatous polyp of the sigmoid colon expected but not the amount nor the diagnostic difficulties Gloucestershire Cellular Pathology Laboratory
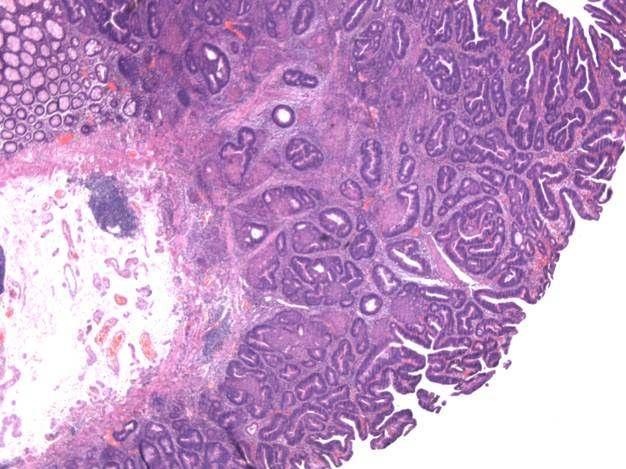
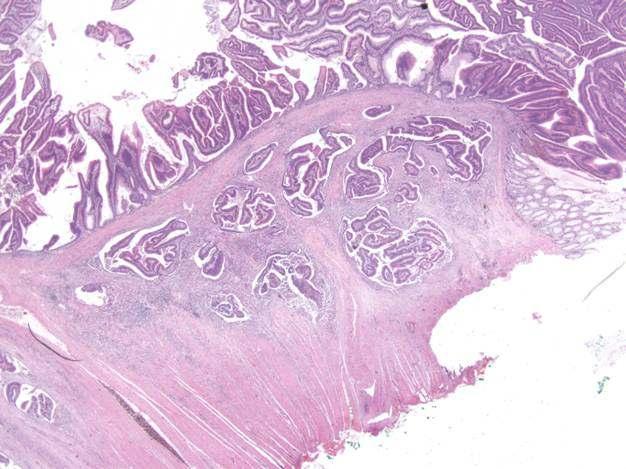
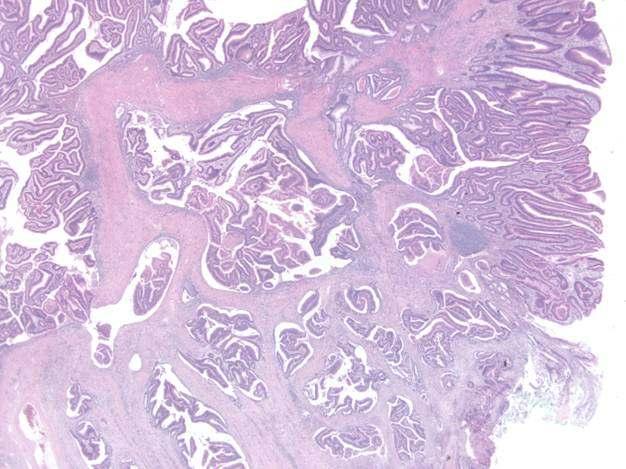
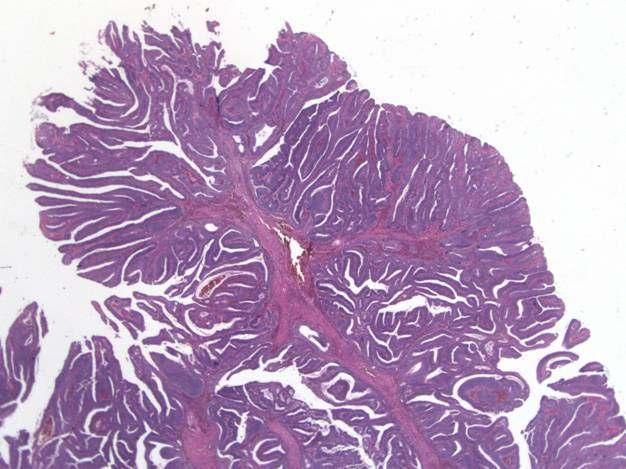
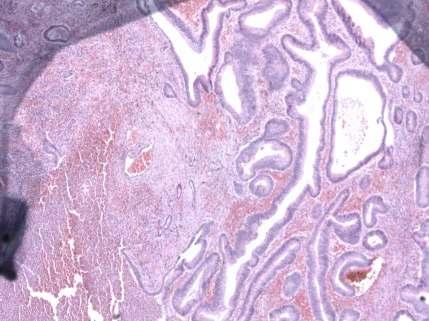
4 Epithelial misplacement in intestinal adenomatous polyps there are clues to the appropriate diagnosis site and size haemosiderin and accompaniment by lamina propria cytology similar to surface neoplasm large sigmoid colonic adenomatous polyps with such changes are selected into BCSP (they bleed)
5 Gloucestershire Cellular Pathology Laboratory


6 Gloucestershire Cellular Pathology Laboratory
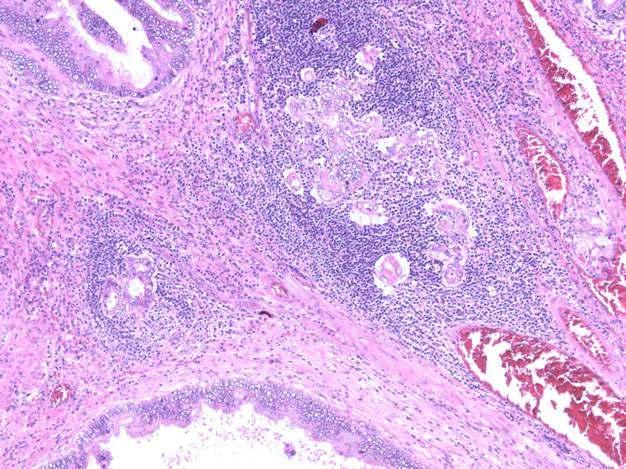
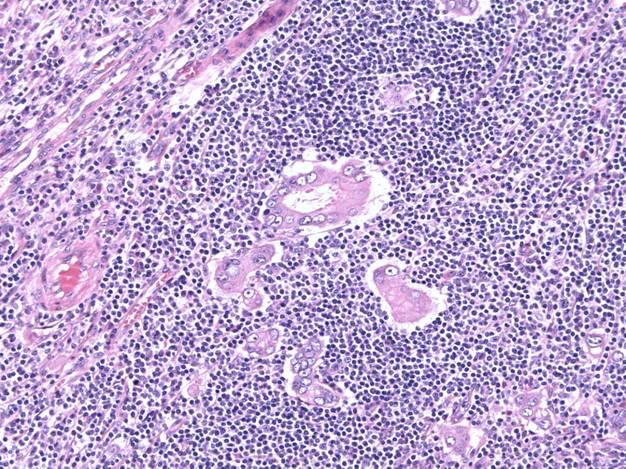
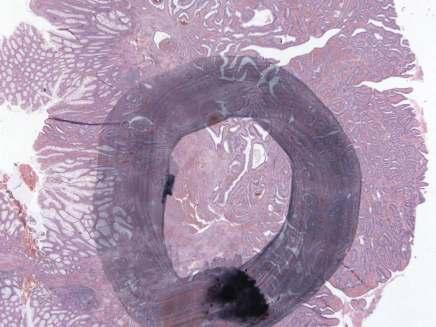
7 The question Is this cancer in the submucosa or is it the benign phenomenon of epithelial misplacement? Gloucestershire Cellular Pathology Laboratory
 same epithelium as surface, accompanied by lamina")

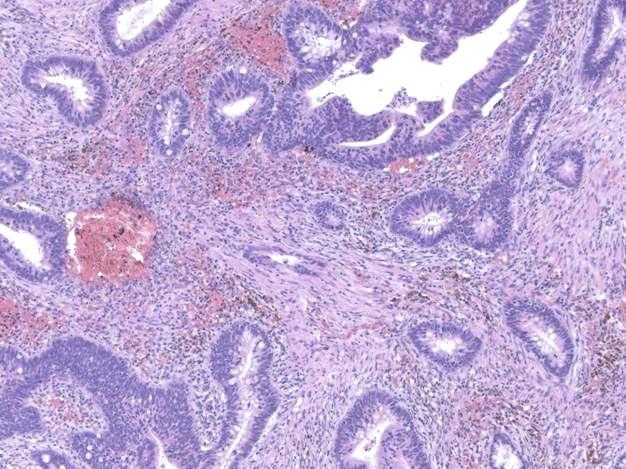
8 Epithelial misplacement in adenomas 85% in sigmoid colon unusual in rectum (unless there has been previous meddling) same epithelium as surface, accompanied by lamina propria, haemosiderin deposition what about misplaced epithelium at the diathermy margin? intense pathological mimicry of invasive cancer Gloucestershire Cellular Pathology Laboratory
9 Epithelial misplacement vs invasive carcinoma There is a very important adage in pathology: why make two diagnoses when one will do?
10 Epithelial misplacement continuity Gloucestershire Cellular Pathology Laboratory


11 67M. BCSP. Sigmoid colonic polyp. Diathermy artefact disconcerts the changes of epithelial misplacement can be made to look much worse by diathermy artefact and it s at that margin Gloucestershire Cellular Pathology Laboratory




12 67M. BCSP. Sigmoid polyp. Previous biopsies and now polypectomy it s the company it keeps Gloucestershire Cellular Pathology Laboratory
13 BCSP polyps we need to keep our minds open. 62M. Sigmoid colonic polyp difficult endoscopic resection (left) site tattooed subsequent perforation and resection (left) do we allow epithelial misplacement in the muscularis propria? Yes we have now seen it several times
14 Enhancement of dysplastic change with inflammation and superficial ulceration
15 Review mechanisms for difficult BCSP/BSW cases BCSP/BSW local reporting pathologist Review by local/network BCSP/BSW GI pathologists Review by regional lead for BCSP/BSW Pathology National Expert Board Gloucestershire Cellular Pathology Laboratory
16 National Expert Board three pathologists you need a majority for this highly subjective and difficult assessment funded by BCSP organised by NAS cases are getting more and more difficult but we are learning Gloucestershire Cellular Pathology Laboratory
17 Original pathologist(s) Expert Board Pathologist A Expert Board Pathologist B Expert Board Pathologist C Mixed Cancer Cancer Cancer Benign Benign Benign Benign Cancer Cancer Cancer Cancer Equivocal Cancer Cancer Cancer Cancer Benign Benign Benign Equivocal Cancer Cancer Cancer Benign Benign Benign Benign Mixed Benign Benign Benign Cancer Benign Benign Benign Benign Cancer Cancer Cancer Equivocal Cancer Cancer Cancer Equivocal Cancer Cancer Cancer Equivocal Cancer Benign Cancer Benign Benign Benign Benign Cancer Benign Equivocal Equivocal Cancer Benign Benign Benign Equivocal Benign Benign Benign Equivocal Benign Equivocal Benign Cancer Benign Equivocal Suspicious
18 Original Pathologist(s) Expert Board Pathologist A Expert Board Pathologist B Expert Board Pathologist C Mixed Cancer Cancer Cancer Benign Benign Benign Benign Cancer Cancer Cancer Cancer Equivocal Cancer Cancer Cancer Cancer Benign Benign Benign Equivocal Cancer Cancer Cancer Benign Benign Benign Benign Mixed Benign Benign Benign Cancer Benign Benign Benign Benign Cancer Cancer Cancer Equivocal Cancer Cancer Cancer Equivocal Cancer Cancer Cancer Equivocal Cancer Benign Cancer Benign Benign Benign Benign Cancer Benign Equivocal Equivocal Cancer Benign Benign Benign Equivocal Benign Benign Benign Equivocal Benign Equivocal Benign Cancer Benign Equivocal Suspicious
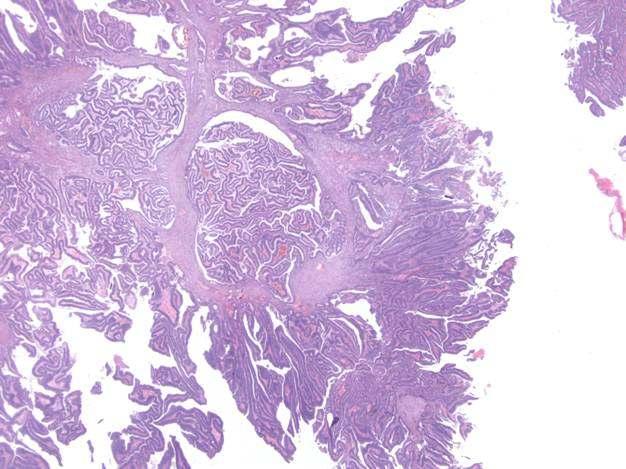
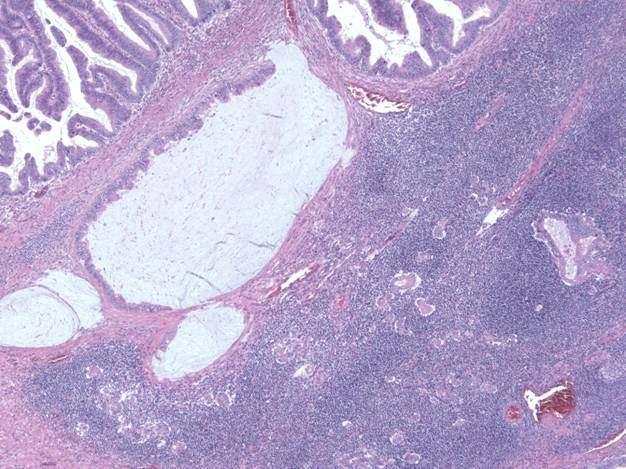
19 What helps lamina propria accompaniment haemosiderin mucus lakes Gloucestershire Cellular Pathology Laboratory
20 What helps site: 87% in SC. Elsewhere if previous meddling. DC and other parts occasionally: rectum very rare unless meddling continuity between surface component and submucosal component (we live in a 3D world ) similar cytology and architecture muscular proliferation and mucosal prolapse changes evidence of acute necrosis Gloucestershire Cellular Pathology Laboratory
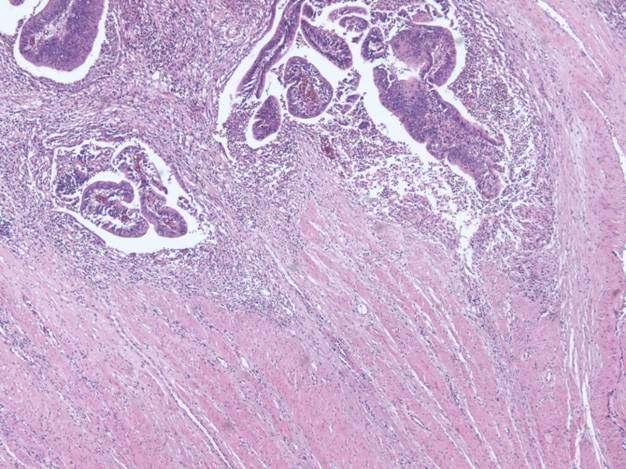
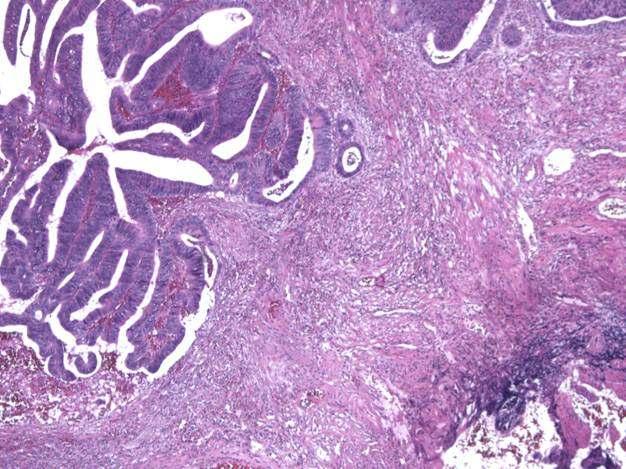
21 What helps.. why make two diagnoses? if there is classical misplacement in one area isolated glands budding desmoplastic reaction true vascular invasion (!) Gloucestershire Cellular Pathology Laboratory

22 Cancer Epithelial Epithelial Epithelial misplacement misplacement misplacement Misplacement of high grade dysplastic & non-neoplastic epithelium Previous biopsies and tattooing

23 Epithelial Epithelial Equivocal Epithelial misplacement misplacement misplacement
24 Descending colonic polyp Previous attempted removal Additional difficulty of morular change


25 Cancer Both: cancer Both: cancer Both: cancer and EM and EM and EM morphology different definite desmoplastic reaction definitely submucosal Gloucestershire Cellular Pathology Laboratory


26 Variable (5 GI Cancer but Equivocal Equivocal pathologists) very difficult



27 Cancer Epithelial Epithelial Epithelial misplacement misplacement misplacement low power lens, high power brain

28 Cancer Epithelial Epithelial Epithelial misplacement misplacement misplacement

29


30 Cancer Epithelial Epithelial Epithelial misplacement misplacement misplacement Epithelial destruction in EM because of inflammation & necrosis Gloucestershire Cellular Pathology Laboratory

31 Equivocal EM and intramucosal adenocarcinoma Superficial adenocarcinoma Can t make a firm diagnosis here

32 Malignant Epithelial Epithelial Epithelial misplacement misplacement misplacement
33 The results so far (December 2010) 65 cases referred to Expert Board (20 in 2009; 45 in 2010) Complete agreement between originating pathologist(s) and EB 17 Original diagnosis equivocal but EB diagnosis certain 22 Diametrically opposite diagnosis: originating pathologist(s) and EB 19 Both epithelial misplacement and cancer 4 Too difficult for EB 3 Gloucestershire Cellular Pathology Laboratory
34 Some questions is this the most extra-ordinary pathological phenomenon of all time? sudden high volume of very difficult cases: Jo/Jolene pathologist struggles; experts struggle all because of BCSP in the UK, are we too conservative when it comes to the diagnosis of colorectal cancer (thanks, Basil) (cf the Far East)? is cancer in continuity twixt its mucosal and submucosal components always, sometimes or never? is epithelial misplacement in continuity twixt its mucosal and submucosal components always, sometimes or never? Gloucestershire Cellular Pathology Laboratory
35 Practicalities this is effectively three second opinions it takes time we are aware of some 65 day breaches do you want a quick report or a good one? patient patience (and that of clinician and SSP) is the name of the game please get involved! Gloucestershire Cellular Pathology Laboratory
36 Practicalities unlikely to change immediate management more of a prognostic call for the patient (life insurance, etc) we advise a rapid return to the site & removal of anything remaining by EMR, etc we have no idea of the implication of epithelial misplacement at a margin and margin involvement alone is the most controversial aspect of the management of pt1 cancers Gloucestershire Cellular Pathology Laboratory
37 The team
38 Julietta Patnick and Richard Winder, BCSP Central
39 Gloucestershire Cellular Pathology Laboratory
40 Thanks for listening! Gloucestershire Cellular Pathology Laboratory
Pseudoinvasion and how to deal with it
 Pseudoinvasion and how to deal with it Professor Neil A Shepherd Gloucester & Cheltenham, UK European Society of Pathology Bilboa, 12 June 2018 Enterprise Interest None Pseudoinvasion and how to deal with
Pseudoinvasion and how to deal with it Professor Neil A Shepherd Gloucester & Cheltenham, UK European Society of Pathology Bilboa, 12 June 2018 Enterprise Interest None Pseudoinvasion and how to deal with
05/07/2018. What colorectal cancer screening is all about. Not so simple pathology: issues from the screening programme
 Not so simple pathology: issues from the screening programme Professor Neil A Shepherd Gloucester & Cheltenham, UK What colorectal cancer screening is all about. detecting early stage cancer D 25% A 8%
Not so simple pathology: issues from the screening programme Professor Neil A Shepherd Gloucester & Cheltenham, UK What colorectal cancer screening is all about. detecting early stage cancer D 25% A 8%
12/7/2011. Pathological mimics of malignancy in the GI tract. Professor Neil A Shepherd President, British Division of the IAP
 Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the
Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
The Kamal Ishak Lecture. The pathology of bowel cancer screening
 The Kamal Ishak Lecture The pathology of bowel cancer screening Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November
The Kamal Ishak Lecture The pathology of bowel cancer screening Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November
The Kristin Henry Lecture. Colorectal cancer screening: extraordinary conundra for pathology
 The Kristin Henry Lecture Colorectal cancer screening: extraordinary conundra for pathology Professor Neil A Shepherd Gloucester & Cheltenham, UK Edinburgh Pathology 2013 Friday, 21 June 2013 British Division
The Kristin Henry Lecture Colorectal cancer screening: extraordinary conundra for pathology Professor Neil A Shepherd Gloucester & Cheltenham, UK Edinburgh Pathology 2013 Friday, 21 June 2013 British Division
polyps of the colon and rectum
 J. clin. Path., 1973, 26, 25-31 Pseudo-carcinomatous invasion in adenomatous polyps of the colon and rectum T. MUTO, H. J. R. BUSSEY, AND B. C. MORSON From St Mark's Hospital, London SYNOPSIS The histology
J. clin. Path., 1973, 26, 25-31 Pseudo-carcinomatous invasion in adenomatous polyps of the colon and rectum T. MUTO, H. J. R. BUSSEY, AND B. C. MORSON From St Mark's Hospital, London SYNOPSIS The histology
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Pathology in Slovenian CRC screening programme: Organisation and quality assurance. Snježana Frković Grazio and Matej Bračko
 Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications
 Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications Authors: *Emil Salmo, 1 Najib Haboubi 2 1. Department of Histopathology, The Pennine Acute Hospitals NHS Trust,
Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications Authors: *Emil Salmo, 1 Najib Haboubi 2 1. Department of Histopathology, The Pennine Acute Hospitals NHS Trust,
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
3/30/2017. Disclosure of Relevant Financial Relationships. Case 5: Polypoid mass in ulcerative colitis. Case 5. TC Smyrk
 Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
S rectal polyps that show atypia, adenocarcinoma,
 HOW RELIABLE IS BIOPSY OF RECTAL POLYPS? A Clinical and Morphological Study of 107 Cases C. ALEXANDER HELLWIG, M.D., AND EDGARD BARBOSA. nr.d. OME OVERLY cautious pathologists call all S rectal polyps
HOW RELIABLE IS BIOPSY OF RECTAL POLYPS? A Clinical and Morphological Study of 107 Cases C. ALEXANDER HELLWIG, M.D., AND EDGARD BARBOSA. nr.d. OME OVERLY cautious pathologists call all S rectal polyps
Rectal biopsy as an aid to cancer control in ulcerative colitis
 Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
Physician s Cognitive and Communication Failures Result in Cancer Treatment Delay
 1 Physician s Cognitive and Communication Failures Result in Cancer Treatment Delay Abstract: The estate of a 60 year old male alleged negligence against a gastroenterologist in failing to properly evaluate
1 Physician s Cognitive and Communication Failures Result in Cancer Treatment Delay Abstract: The estate of a 60 year old male alleged negligence against a gastroenterologist in failing to properly evaluate
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Diagnostic Difficulties Encountered Among Colorectal Polyps
 Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
The malignant colorectal polyp
 The malignant colorectal polyp Dr Ian Brown Envoi Pathology Envoi data reproduced from J Clin Path 2015 article Definition Adenocarcinoma found in an endoscopically resected polypoidal tumour Submucosal
The malignant colorectal polyp Dr Ian Brown Envoi Pathology Envoi data reproduced from J Clin Path 2015 article Definition Adenocarcinoma found in an endoscopically resected polypoidal tumour Submucosal
NHS Bowel Cancer Screening Programme Guidance on reporting lesions. Public Health England leads the NHS Screening Programmes
 NHS Bowel Cancer Screening Programme Guidance on reporting lesions Public Health England leads the NHS Screening Programmes About Public Health England Public Health England (PHE) exists to protect and
NHS Bowel Cancer Screening Programme Guidance on reporting lesions Public Health England leads the NHS Screening Programmes About Public Health England Public Health England (PHE) exists to protect and
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
White Rose Research Online URL for this paper: Version: Accepted Version
 This is a repository copy of Challenging diagnostic issues in adenomatous polyps with epithelial misplacement in bowel cancer screening: five years' experience of the BCSP Expert Board. White Rose Research
This is a repository copy of Challenging diagnostic issues in adenomatous polyps with epithelial misplacement in bowel cancer screening: five years' experience of the BCSP Expert Board. White Rose Research
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition
 SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions
 Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS
 PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations
 Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
Pathology perspective of colonic polyposis syndromes
 Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Rectal EMR: Techniques and Tips
 Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
FINAL HISTOLOGICAL DIAGNOSIS: Villo-adenomatous polyp with in-situ-carcinomatous foci (involving both adenomatous and villous component).
.") SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD
 SNARE THE CASE FOR EMR AND ESD") THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
Billing Guideline. Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/14 Last revision effective 4/16
 Effective Date: 1/1/14 Last revision effective 4/16") Billing Guideline Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/14 Last revision effective 4/16 Florida Hospital Care Advantage plans include full coverage of in-network
Billing Guideline Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/14 Last revision effective 4/16 Florida Hospital Care Advantage plans include full coverage of in-network
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Colonic adenomas-a colonoscopy survey
 Gut, 1979, 20, 240-245 Colonic adenomas-a colonoscopy survey P. E. GILLESPIE, T. J. CHAMBERS, K. W. CHAN, F. DORONZO, B. C. MORSON, AND C. B. WILLIAMS From St Mark's Hospital, City Road, London SUMMARY
Gut, 1979, 20, 240-245 Colonic adenomas-a colonoscopy survey P. E. GILLESPIE, T. J. CHAMBERS, K. W. CHAN, F. DORONZO, B. C. MORSON, AND C. B. WILLIAMS From St Mark's Hospital, City Road, London SUMMARY
Polypoid lesions of the gastrointestinal tract
 Polypoid lesions of the gastrointestinal tract Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November 2015 Polypoid lesions
Polypoid lesions of the gastrointestinal tract Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November 2015 Polypoid lesions
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
The Paris classification of colonic lesions
 The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
BC CRC Update Malignant Polyp Who Needs Surgery
 BC CRC Update Malignant Polyp Who Needs Surgery Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary
BC CRC Update Malignant Polyp Who Needs Surgery Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN
 Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you)
") What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
Supplemental Digital Content 1. Endoscopic and histolological findings in INR and FR study subjects
 Supplemental Digital Content 1. Endoscopic and histolological findings in INR and FR study subjects Patient Group Macroscopic examination Ileum Histology Colon/rectum Histology 1 INR Normal Acute and chronic
Supplemental Digital Content 1. Endoscopic and histolological findings in INR and FR study subjects Patient Group Macroscopic examination Ileum Histology Colon/rectum Histology 1 INR Normal Acute and chronic
what is the alternative mechanism of histogenesis? Aspects of the morphology of the adenomacarcinoma Morphology of the
 Refer to: Morson B: Polyps and cancer of the large bowel. West J Med 125:93-99, Aug 1976 THE WESTERN Journal of Miedicine Polyps and Cancer of the Large Bowel BASIL MORSON, MD, London MORTALITY STATISTICS
Refer to: Morson B: Polyps and cancer of the large bowel. West J Med 125:93-99, Aug 1976 THE WESTERN Journal of Miedicine Polyps and Cancer of the Large Bowel BASIL MORSON, MD, London MORTALITY STATISTICS
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom
 Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom What exactly will be required? Defining levels of polypectomy competency in terms of complexity/time/risk
Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom What exactly will be required? Defining levels of polypectomy competency in terms of complexity/time/risk
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care
 Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Modern colonoscopy allows for both diagnosis and treatment
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:662 667 CLINICAL PATHOLOGY The Malignant Colon Polyp: Diagnosis and Therapeutic Recommendations MARIE E. ROBERT Department of Pathology, Yale University
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:662 667 CLINICAL PATHOLOGY The Malignant Colon Polyp: Diagnosis and Therapeutic Recommendations MARIE E. ROBERT Department of Pathology, Yale University
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
EMR, ESD and Beyond. Peter Draganov MD. Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida
 EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Adenoma to Carcinoma Pathway
 It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
Frequency of Diagnosis of Colorectal Cancer with Double Contrast Barium Enema
 Bahrain Medical Bulletin, Vol.24, No.3, September 2002 Frequency of Diagnosis of Colorectal Cancer with Double Contrast Barium Enema Najeeb S Jamsheer, MD, FRCR* Neelam. Malik, MD, MNAMS** Objective: To
Bahrain Medical Bulletin, Vol.24, No.3, September 2002 Frequency of Diagnosis of Colorectal Cancer with Double Contrast Barium Enema Najeeb S Jamsheer, MD, FRCR* Neelam. Malik, MD, MNAMS** Objective: To
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Factors for Endoscopic Submucosal Dissection in Early Colorectal Neoplasms: A Single Center Clinical Experience in China
 ORIGINAL ARTICLE Clin Endosc 2015;48:405-410 http://dx.doi.org/10.5946/ce.2015.48.5.405 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Factors for Endoscopic Submucosal Dissection in Early Colorectal
ORIGINAL ARTICLE Clin Endosc 2015;48:405-410 http://dx.doi.org/10.5946/ce.2015.48.5.405 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Factors for Endoscopic Submucosal Dissection in Early Colorectal
Primary mucinous adenocarcinoma developing in an ileostomy stoma
 Gut, 1988, 29, 1607-1612 Primary mucinous adenocarcinoma developing in an ileostomy stoma P J SMART, S SASTRY, AND S WELLS From the Departments of Histopathology and Surgery, Bolton General Hospital, Fan
Gut, 1988, 29, 1607-1612 Primary mucinous adenocarcinoma developing in an ileostomy stoma P J SMART, S SASTRY, AND S WELLS From the Departments of Histopathology and Surgery, Bolton General Hospital, Fan
12/7/2011. The reporting of colorectal cancer pathology: recent advances. Colorectal cancer resection specimens
 The reporting of colorectal cancer pathology: recent advances Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 Colorectal cancer resection specimens
The reporting of colorectal cancer pathology: recent advances Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 Colorectal cancer resection specimens
In-situ and invasive carcinoma of the colon in patients with ulcerative colitis
 Gut, 1972, 13, 566-570 In-situ and invasive carcinoma of the colon in patients with ulcerative colitis D. J. EVANS AND D. J. POLLOCK From the Departments of Pathology, Royal Postgraduate Medical School
Gut, 1972, 13, 566-570 In-situ and invasive carcinoma of the colon in patients with ulcerative colitis D. J. EVANS AND D. J. POLLOCK From the Departments of Pathology, Royal Postgraduate Medical School
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
proposed Vienna classification of gastrointestinal
 Gut 2;47:251 255 251 For list of authors ayliations, please see appendix. Correspondence to: Dr R Schlemper, Department of Internal Medicine, Fukuoka University School of Medicine, 7-45-1 Nanakuma, Jonan-ku,
Gut 2;47:251 255 251 For list of authors ayliations, please see appendix. Correspondence to: Dr R Schlemper, Department of Internal Medicine, Fukuoka University School of Medicine, 7-45-1 Nanakuma, Jonan-ku,
Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum
 Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments
Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Formula One Study. Assessment criteria of pathological parameters. Ver.2. UK Japan Joint Study for Risk Factors of Lymph Node
 APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
How to treat early gastric cancer? Endoscopy
 How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD)
 & Endoscopic Submucosal Dissection (ESD)") Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD) Minimally Invasive Polyp Removal IE-02700-Understanding EMR and ESD Brochure_R3.indd 1 Occasionally, a polyp that infiltrates
Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD) Minimally Invasive Polyp Removal IE-02700-Understanding EMR and ESD Brochure_R3.indd 1 Occasionally, a polyp that infiltrates
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details