Pathology of Renal Neoplasms: Recent Advances
|
|
|
- Constance Barrett
- 5 years ago
- Views:
Transcription


1 Pathology of Renal Neoplasms: Recent Advances Jae Y. Ro, M.D., Ph.D. The Methodist Hospital Weill Medical College of Cornell University, MD Anderson Cancer Center, Houston, Texas Ewha Womans University Hospital Yonsei University Hospital, Seoul, Korea June 7, 2012
2 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States, CA Cancer J Clin 2012;


3 KIDNEY CANCER - CURRENT STATUS UNITED STATES, 2012 Including renal pelvis 64,770 (40,250, males; 24,520, females) New cases in ,570 (8,650, males;4,920, females)
4 Kidney Cancer with other GU Cancers 5-year Relative Survival Rates (%): Kidney Cancer is the Worst of GU Cancers 5-year Relative Survival Rates (%) 1975 to to to 2003 Kidney Bladder Prostate Testis Jemal A. et al. CA Cancer J Clin 2009;59:225-49

5 Male Female Stomach Colon Lung Liver Prostate Thyroid Bladder Pancreas Kidney Biliary tree ttree Thyroid Breast Stomach Colon Lung Uterine Cx Liver Biliary tree Pancreas ovary
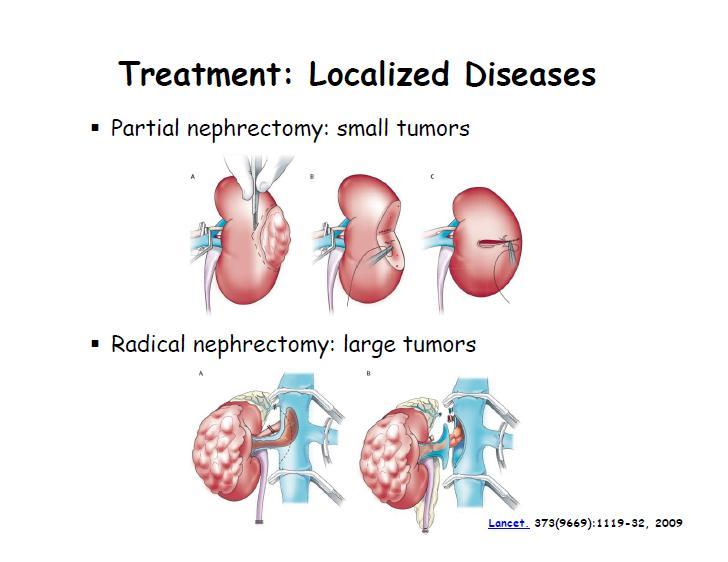
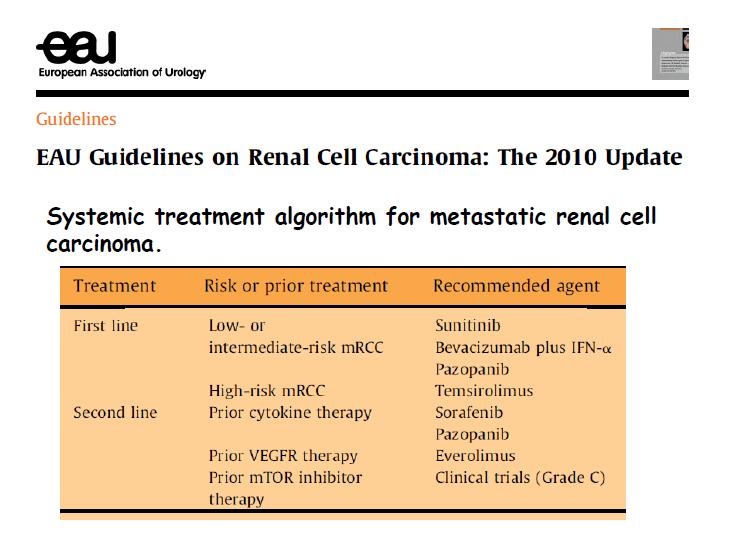
6 Introduction Increased incidence of renal tumors More incidental and small tumors More partial nephrectomy More laparoscopic/robotic surgery Development of molecular targeted therapies (Sunitinib, Sorafenib, Bevacizumab, Temsirolimus )
7 Increasing of Cancers of Kidney /Renal Pelvis USA ( ) Data obtained from Cancer Statistics by American Cancer Society : 64,77 0
8 Surgical Treatment of Renal Tumor More smaller tumors are detected More incidental tumors More benign tumors More partial nephrectomy More laparoscopic/robotic surgery
9
10
11
12
13
14
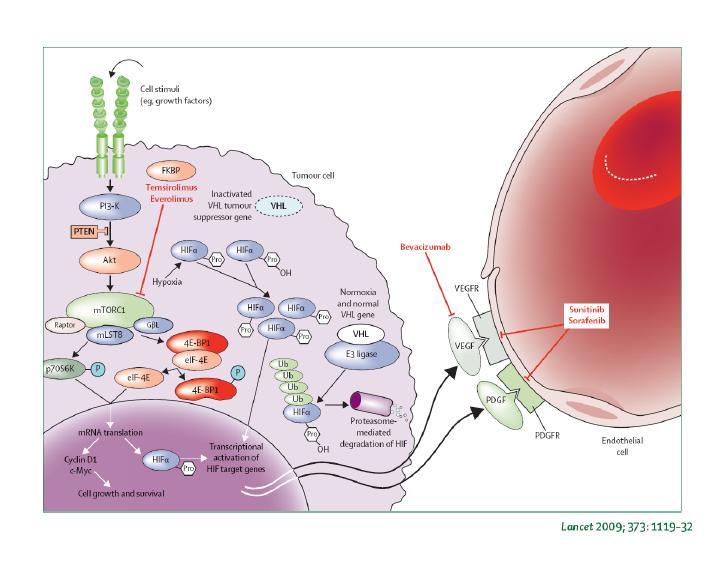
15 RCC Molecular Targeted Therapy No effective adjuvant therapy for RCC Molecular targeted drug approved by FDA All are active in cytokine refractory patients Sunitinib (Sutent) and Sorafenib (Nexavar) VEGF, PDGF Bevacizumab (Avastin) VEGF Temsirolimus (CCI-779) mtor Escudier et al. NEJM 2007;356:124. Motzer et al. NEJM Hudes et al. NEJM 2007
16 Histology and Classification
17 UICC/AJCC Consensus (1997) BENIGN MALIGNANT Oncocytoma Papillary adenoma Metanephric adenoma Clear cell RCC Papillary RCC Chromophobe RCC Collecting duct carcinoma RCC, unclassified
18 WHO Classification (2004) Clear cell RCC Multilocular cystic RCC Papillary RCC Chromophobe RCC Carcinoma of the collecting ducts of Bellini Renal medullary carcinoma Xp11 translocation carcinomas Carcinoma associated with neuroblastoma Mucinous tubular and spindle cell carcinoma RCC, unclassified Papillary adenoma Oncocytoma

19 Kidney Histology


20 RCC marker Kidney specific cadherin

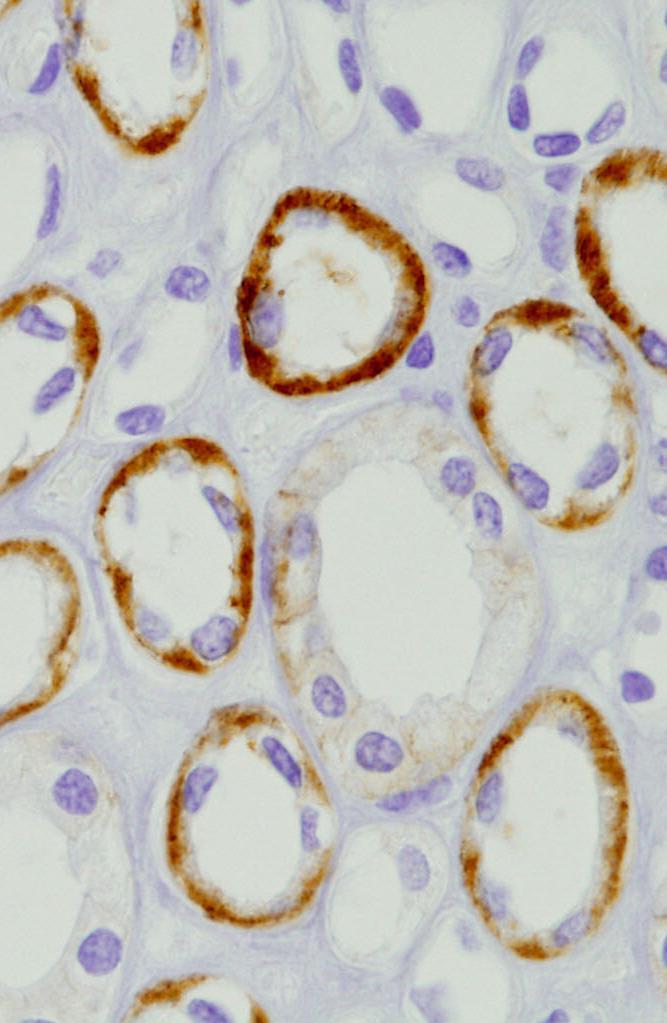
21 Kidney specific cadherin
")
")

 (others -2, -10,")
 (Translocations chr 11)")
 LOH")
22 Proximal tubules (85% -90%) Collecting Ducts (10% -15%) Intercalated cells (cortex) Collecting ducts (medulla) Clear cell RCC (3p-) Papillary RCC (+7, +17, -Y, others) Chromophobe RCC (-1, -Y ) (others -2, -10, -13 etc) Oncocytoma (-1, -Y) (Translocations chr 11) Collecting duct carcinoma (-1, -6, -14, -15, -22) LOH 8p and 13q


23 CRCC4 A B C D a b c d a b c d a b c d a b c d PRCC CHRCC OC

24 RCC Histology and Incidence (Selective large series and TMH data) Histologic Type Incidence (5 studies)* TMH (n=1147) Clear cell 68% % 77.2% Papillary 11% % 15.2% Chromophobe 4.3% - 6.5% 5.6% Collecting duct 0-1% 0.4% Unclassified 1% - 6.1% 1.4% * Ljungberg 1999 (n=186), Moch, 2000 (n=588), Amin 2002 (n=377), Cheville 2003 (n=2385), Kim 2004 (n=795)

25 Histology and Prognosis (Simplistic view ) Oncocytoma Chromophobe RCC Adenoma Type 1 Type 2 Papillary RCC Clear cell RCC Collecting duct Ca Low Malignant potential High
26 Contents 5: 5 types of malignant tumors 4: 4 (+4) newly defined entities 3: 3 benign tumors 2: 2 entities no longer exist 1: 1 (+1) most important prognostic factor
27 5 Malignant



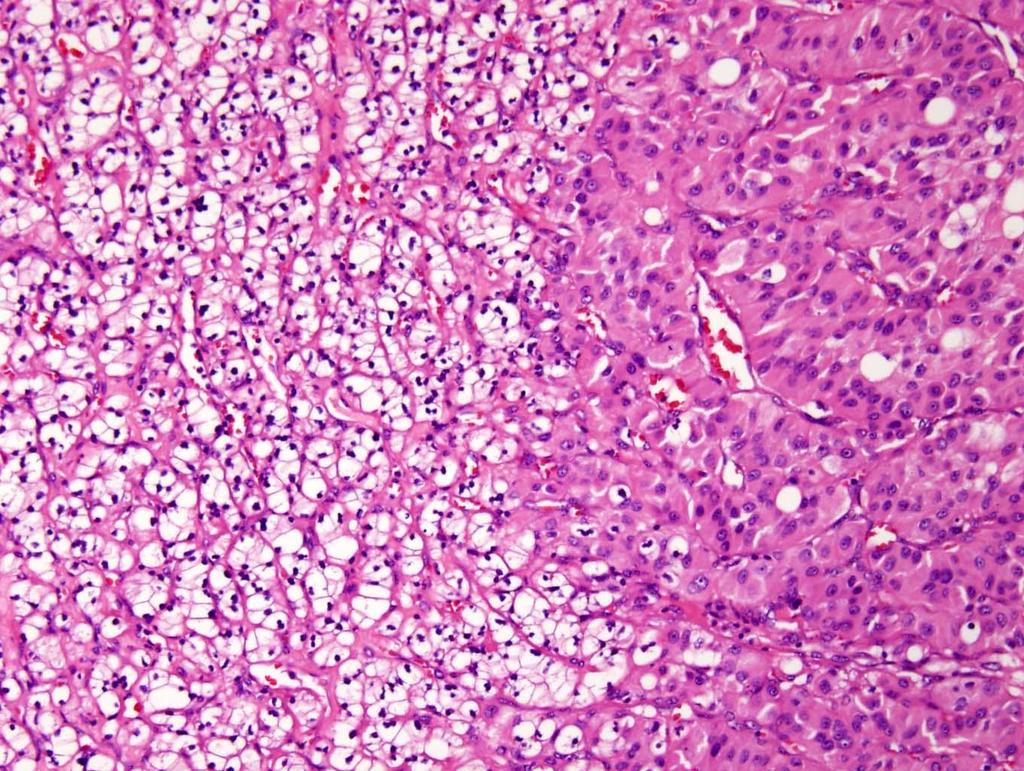
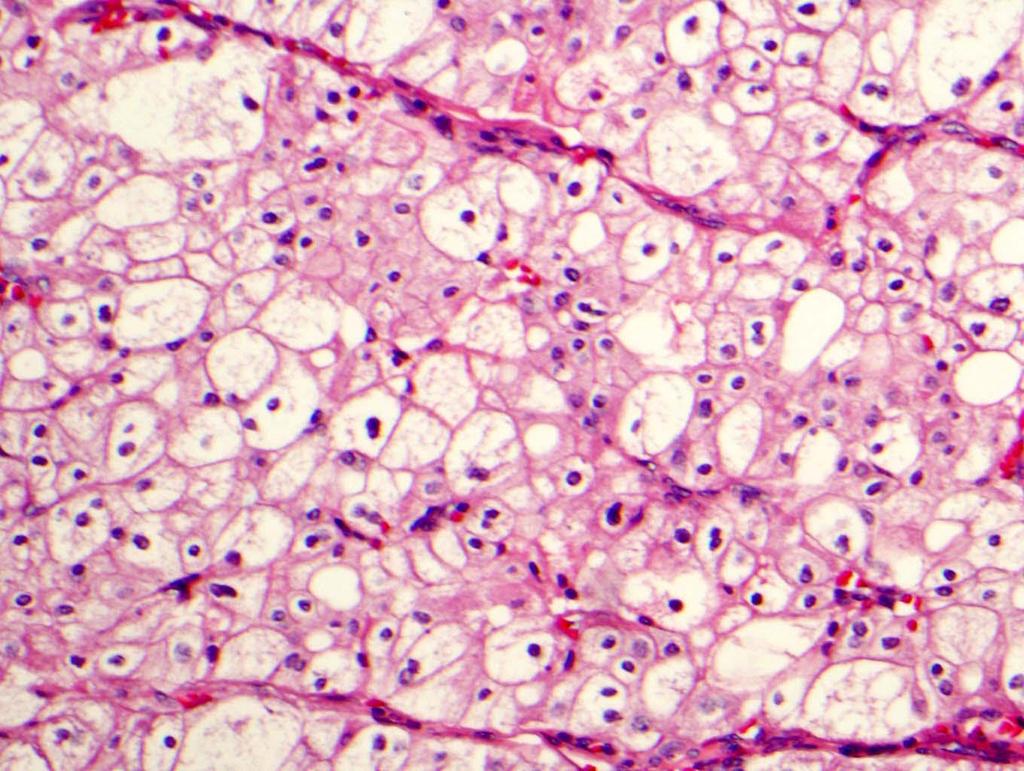
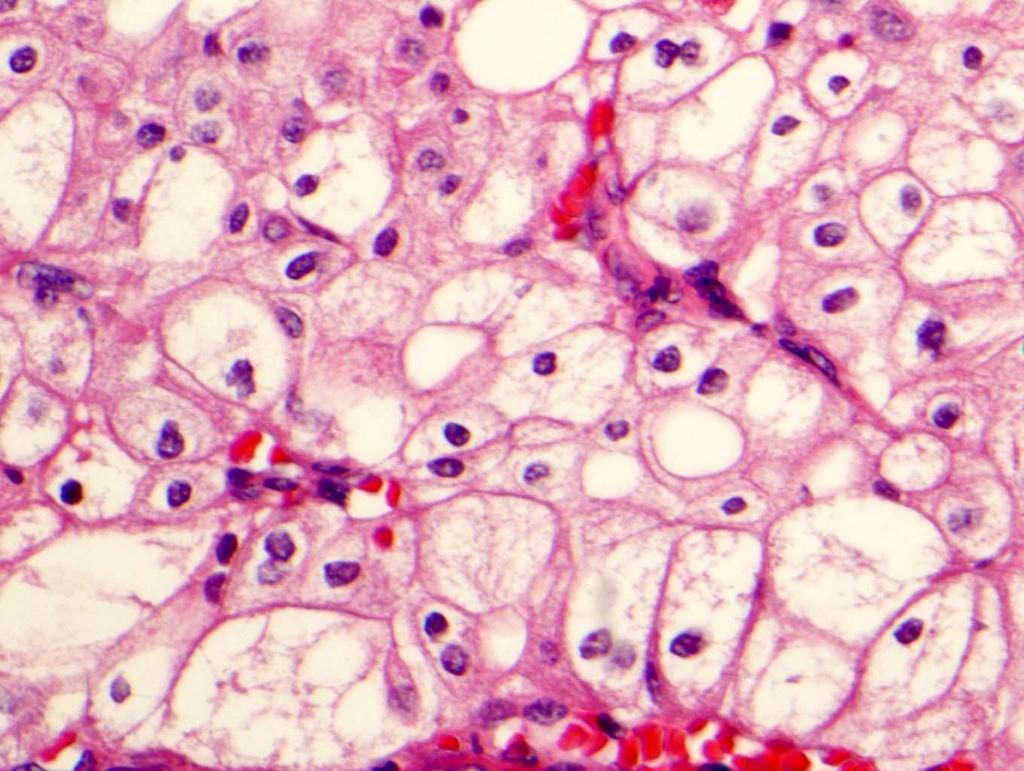
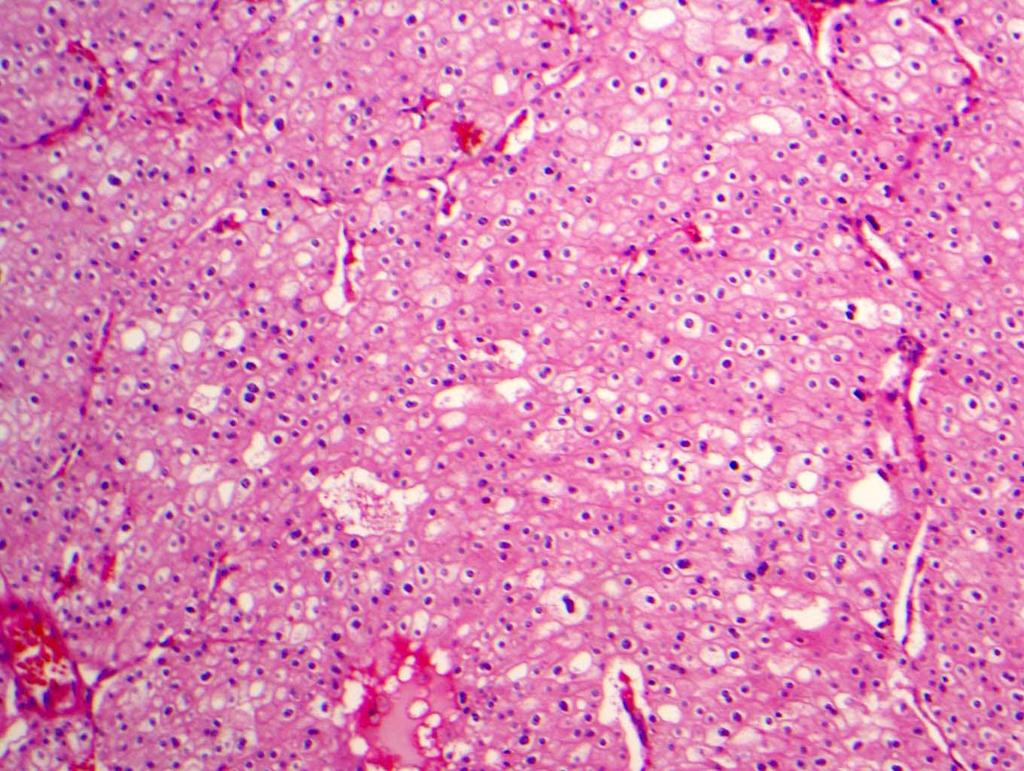
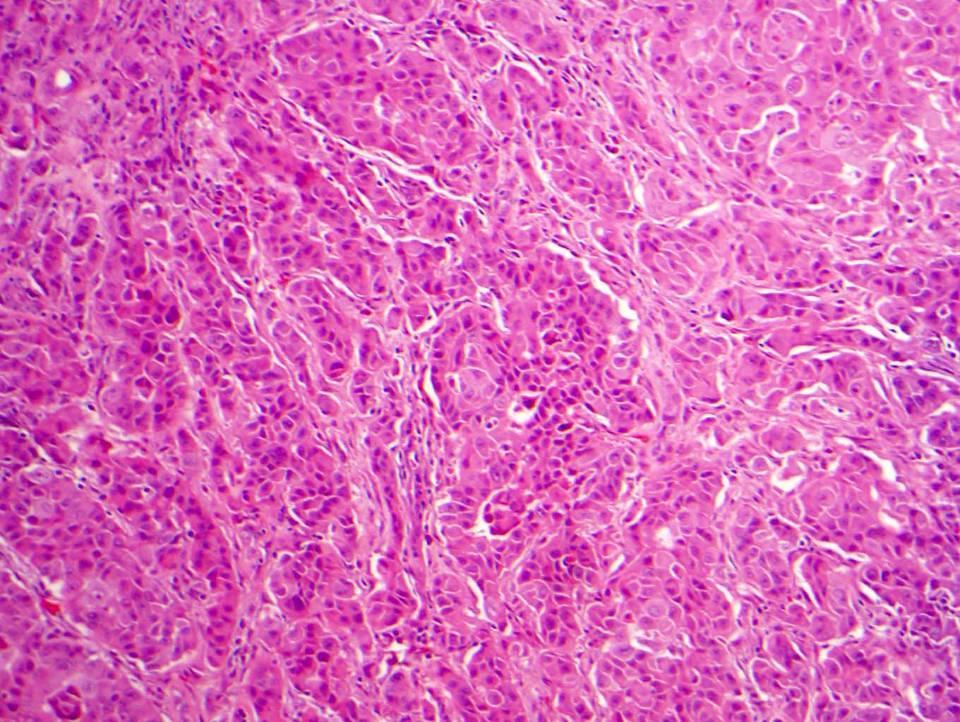
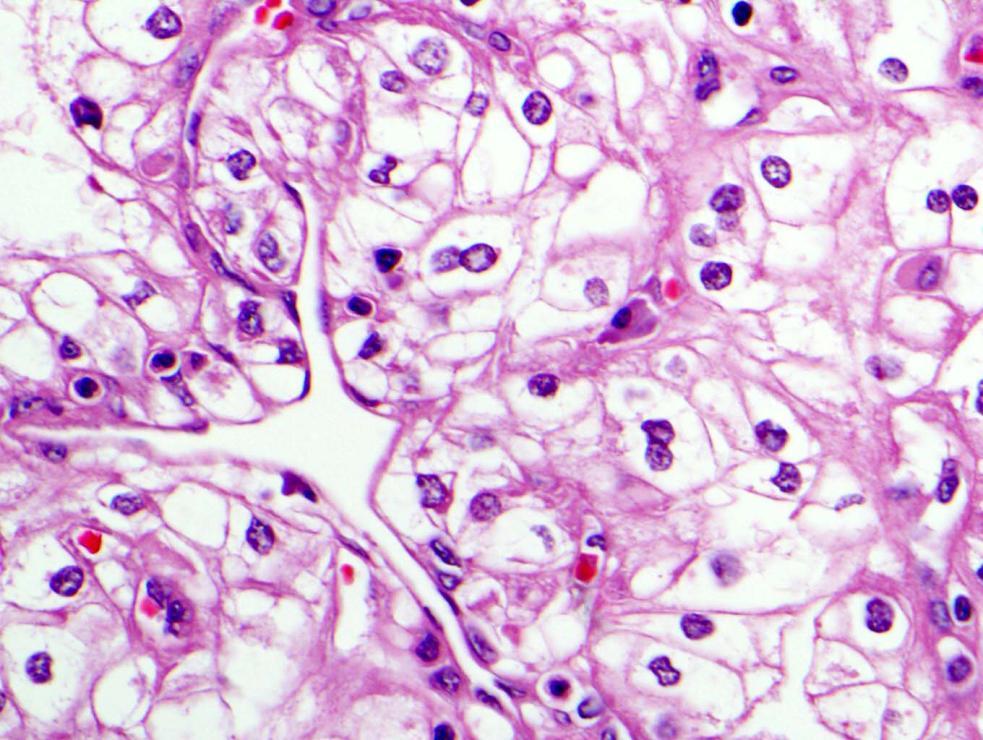
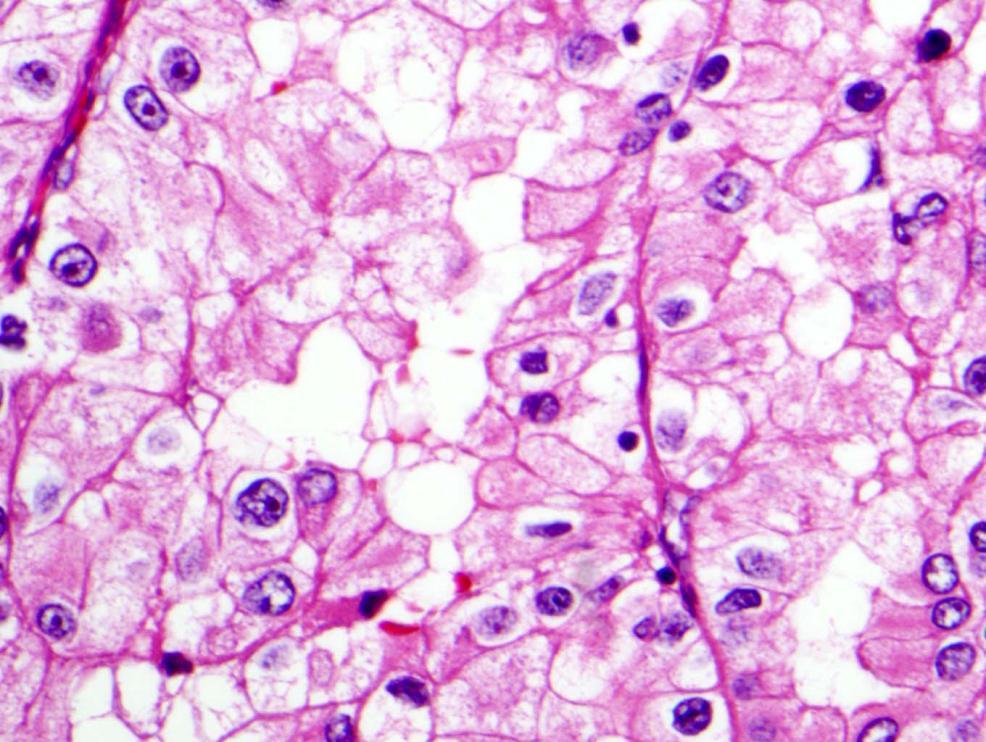
28 Clear Cell RCC


29 Growth Patterns Classic (solid/acinar) Tubular Cystic Pseudopapillary Hemorrhagic Hyalinzed Cytomorphology Classic clear cell Granular Epithelioid Rhabdoid Spindle/sarcomatoid
30
31
32
33

34 Clear Cell RCC Differential Diagnoses Morphologic variation of clear cell RCC Differential diagnosis Chromophobe RCC Papillary RCC type 2 Cellular or epithelioid angiomyolipoma Adrenal cortical carcinoma





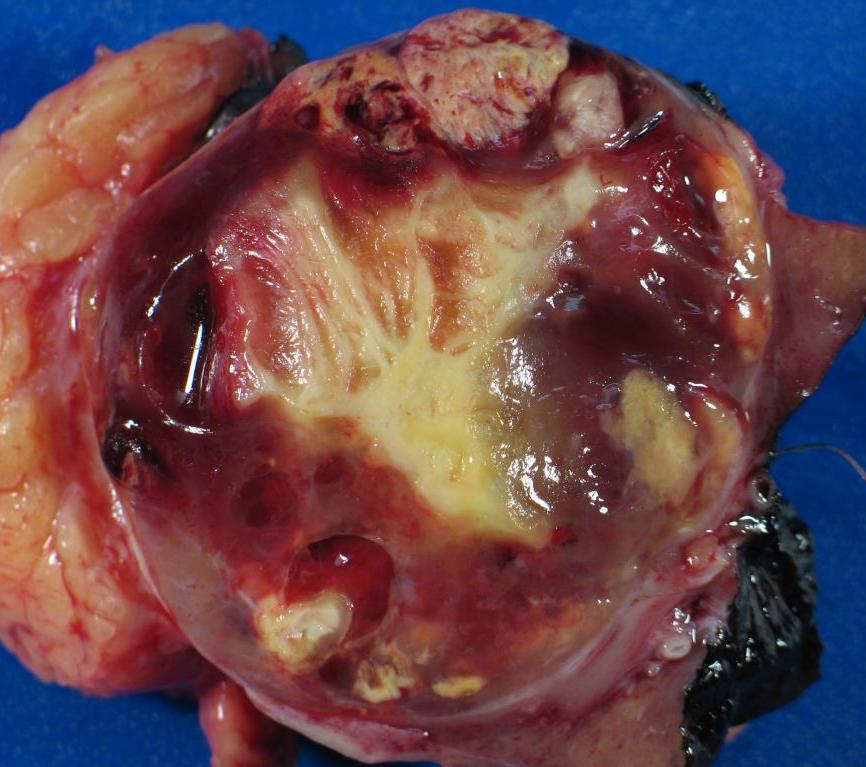
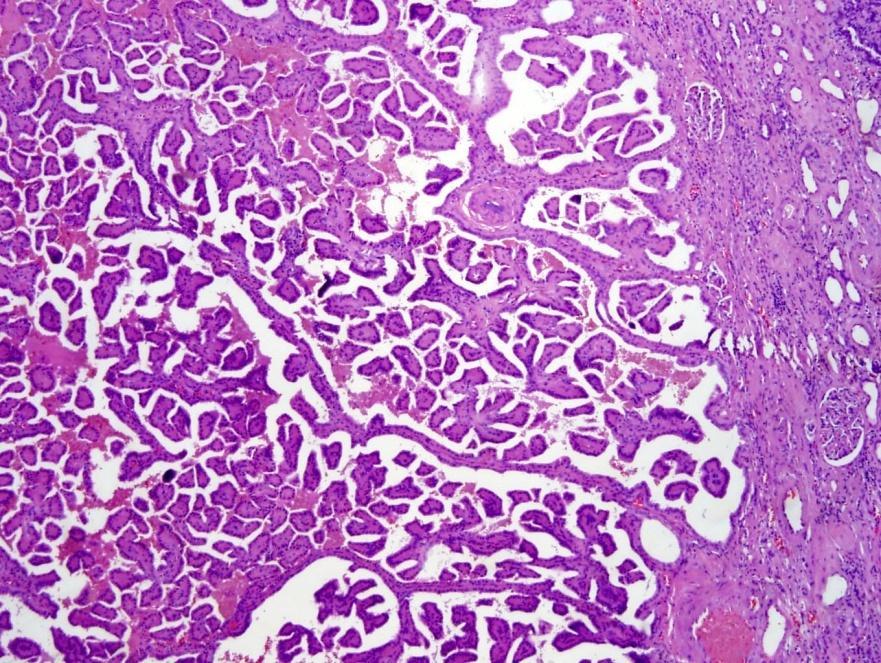
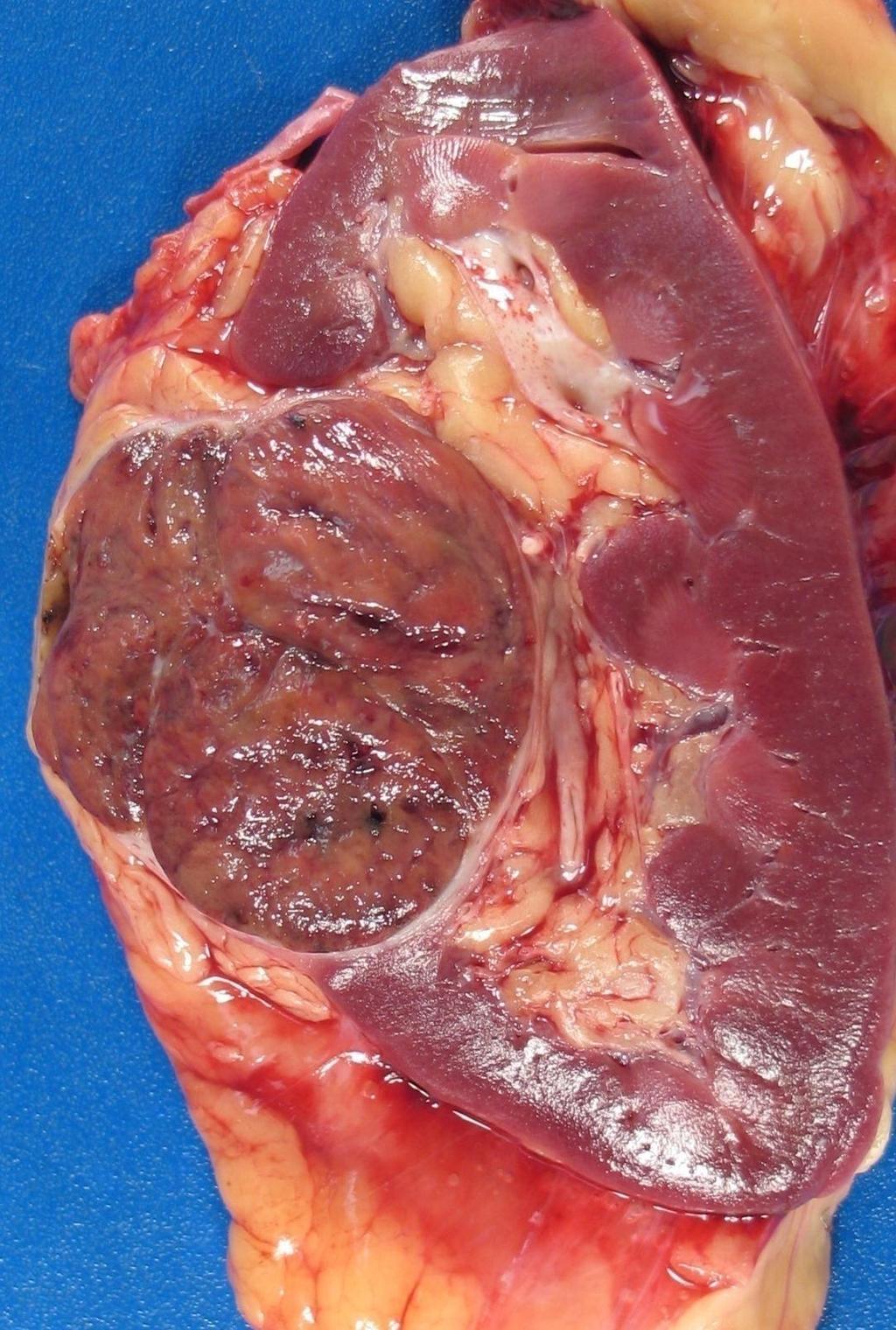
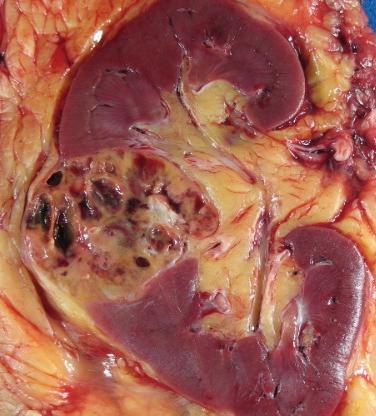
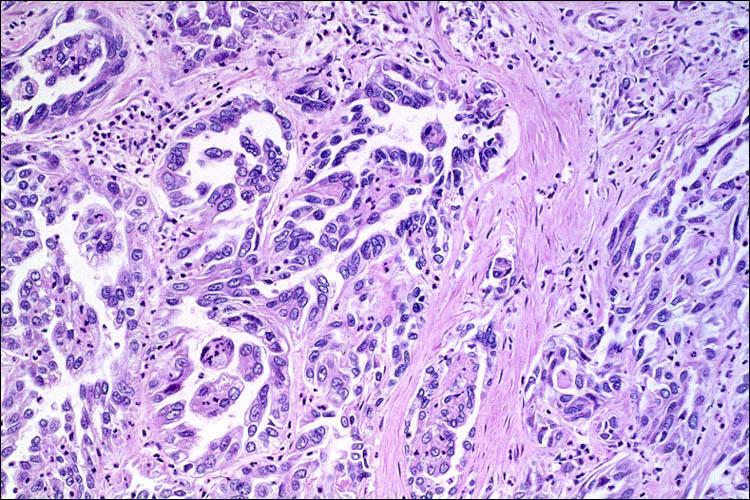
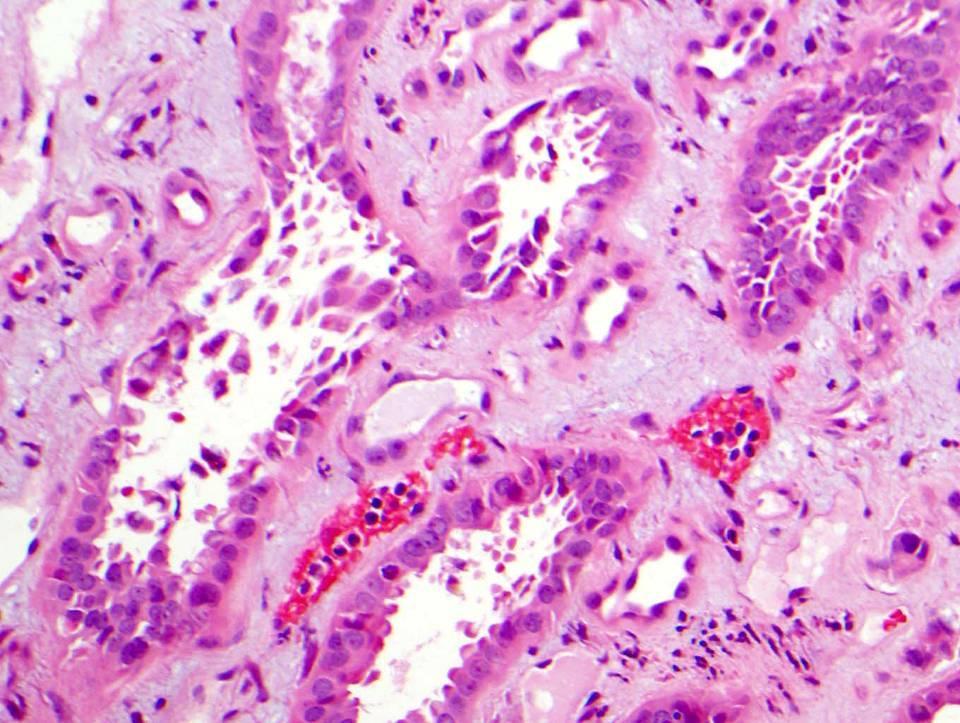
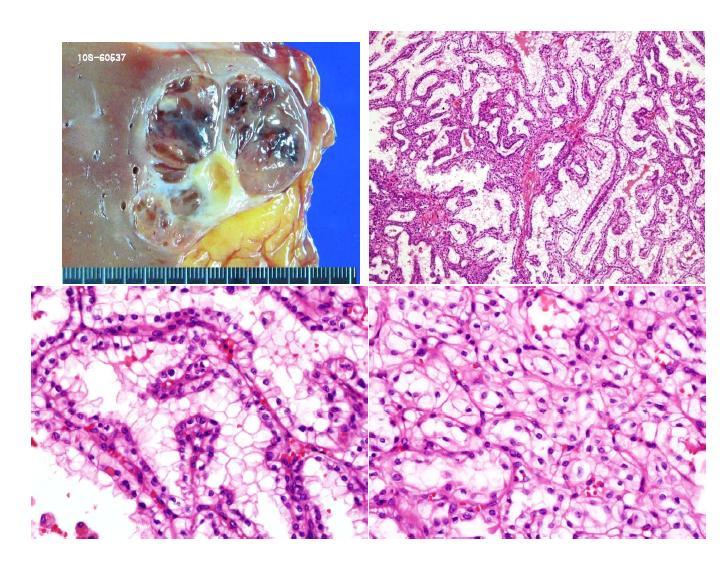
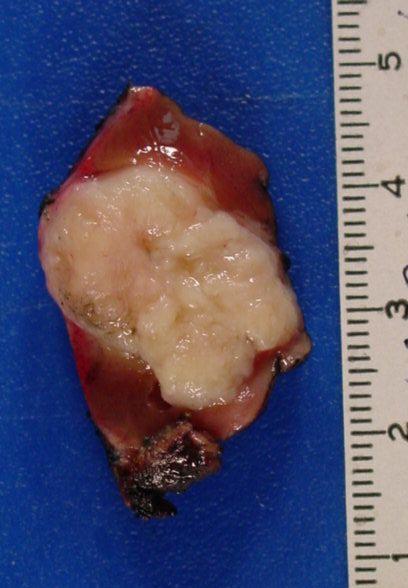
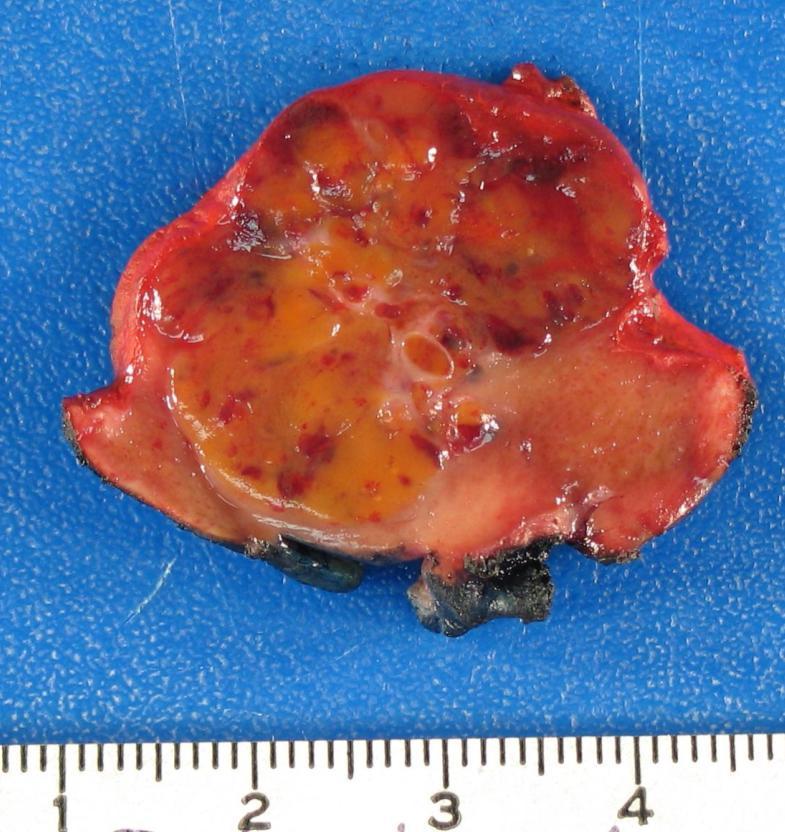
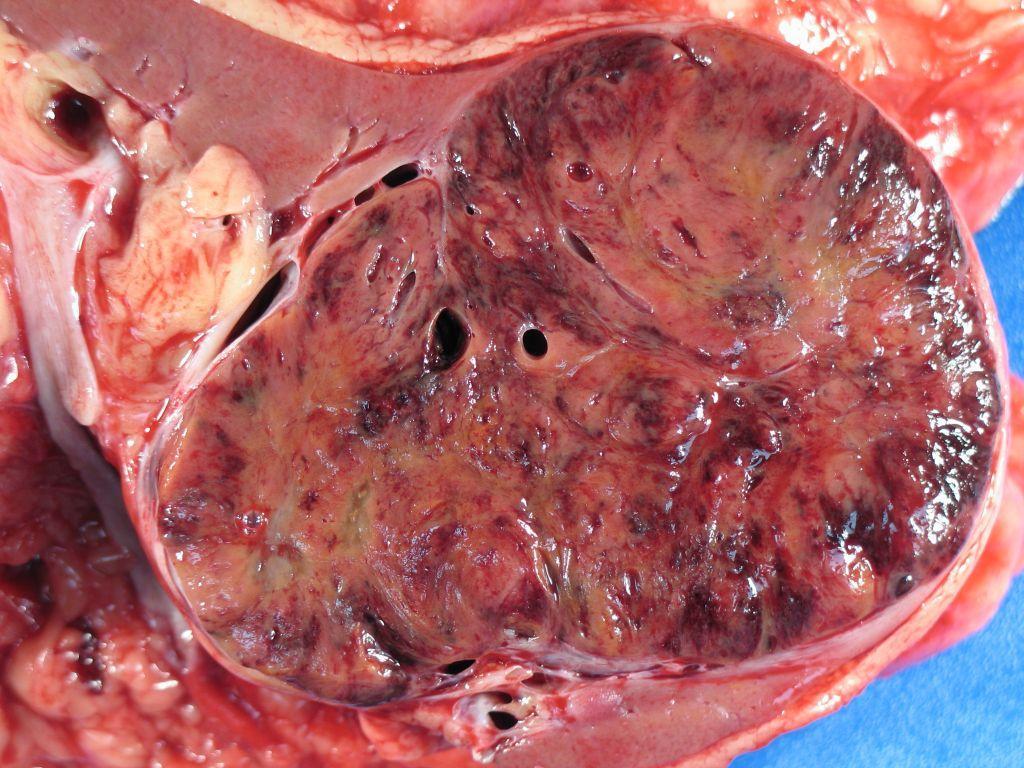
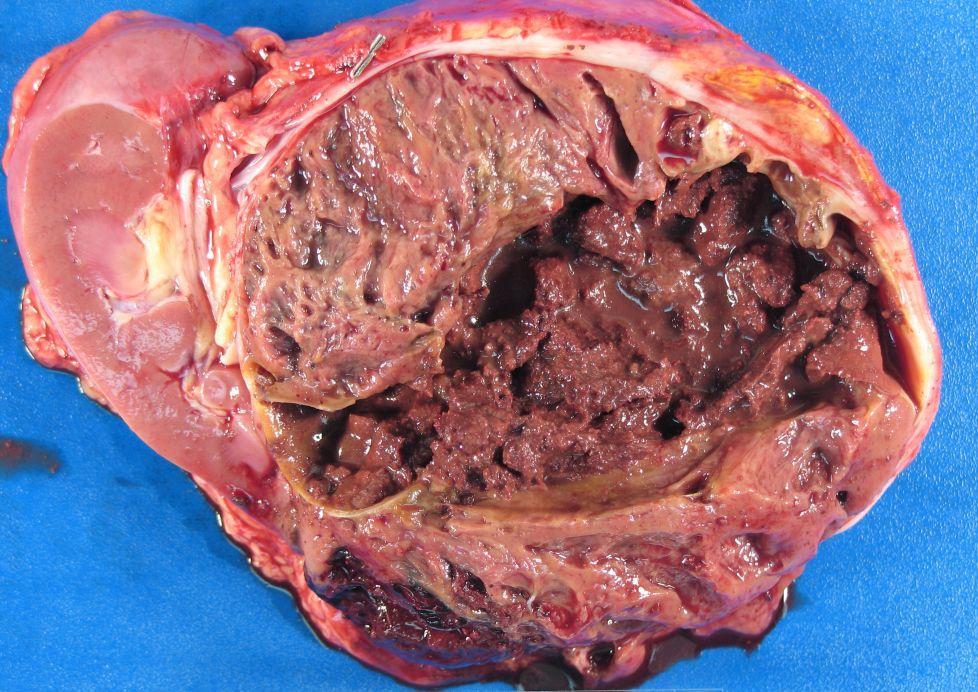
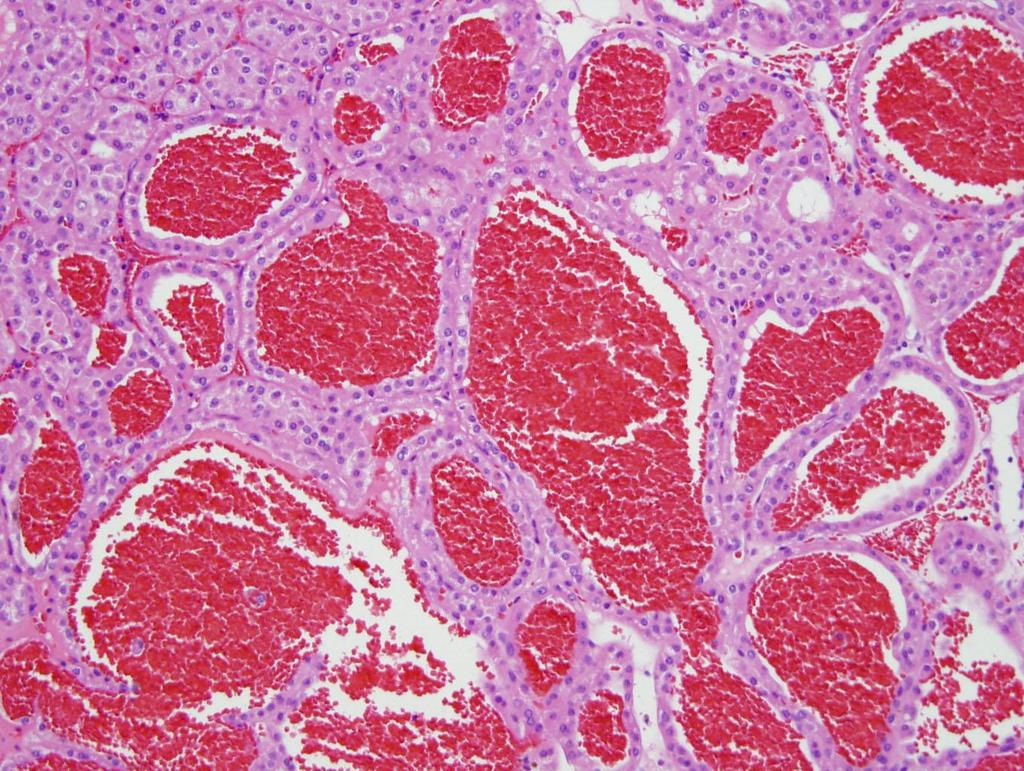
35 Papillary RCC Common Gross Features: 1. More homogeneous 2. White tan 3. Friable, solid/cystic, punctuate chalky area 4. Better circumscription

 Eosinophilic Clear cell")
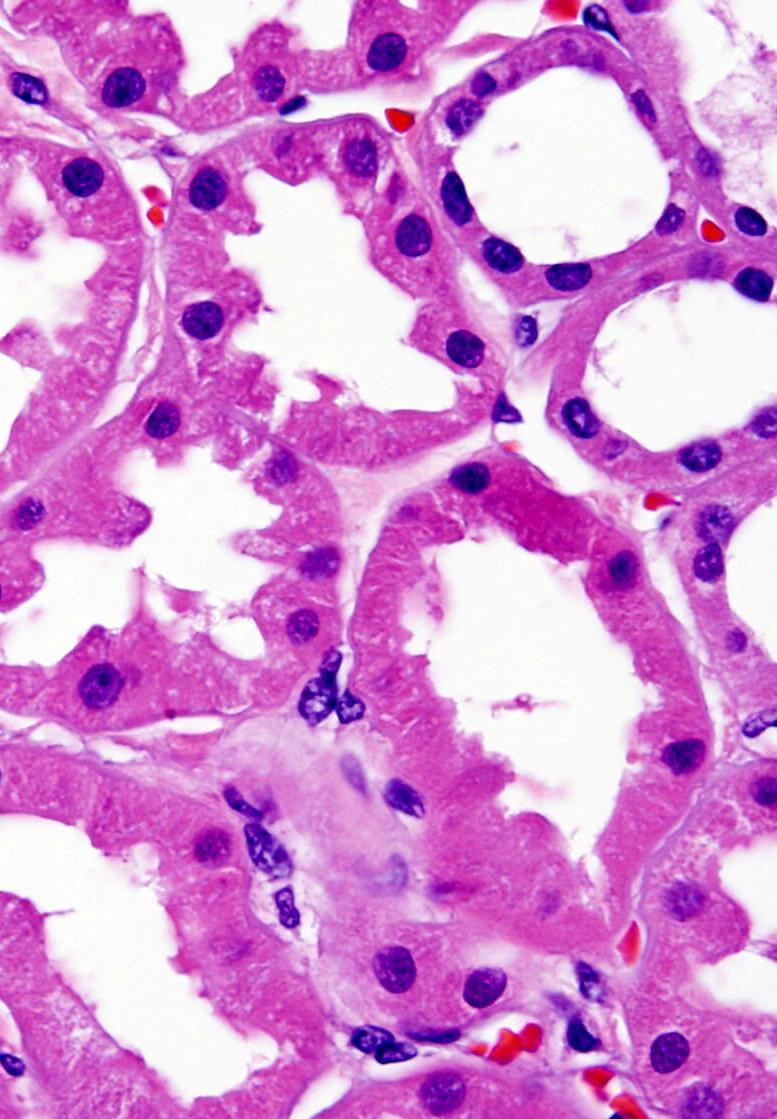
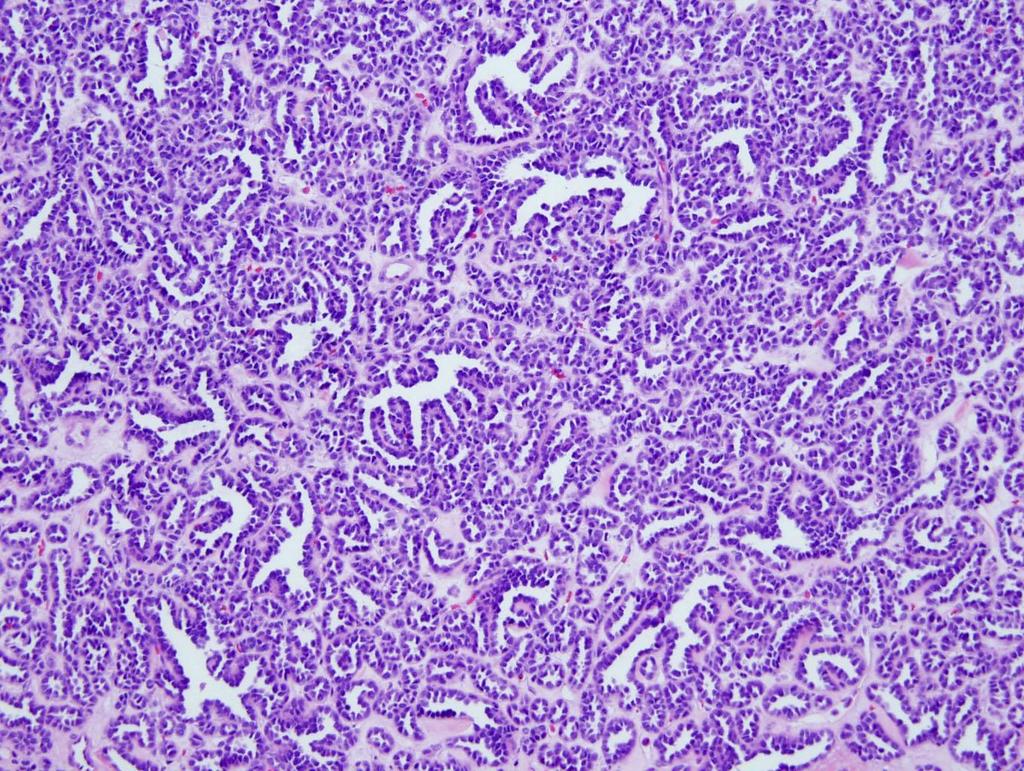
36 Papillary RCC Growth Patterns Papillary Tubular Tubulopapillary Solid Cytomorphology Classic (basophilic) Eosinophilic Clear cell Mixed Sarcomatoid

37 Papillary RCC The second most common type RCC Cytogenetic changes: +7, +17, -Y Met protooncogene More frequent regional nodal metastasis Prognosis variable

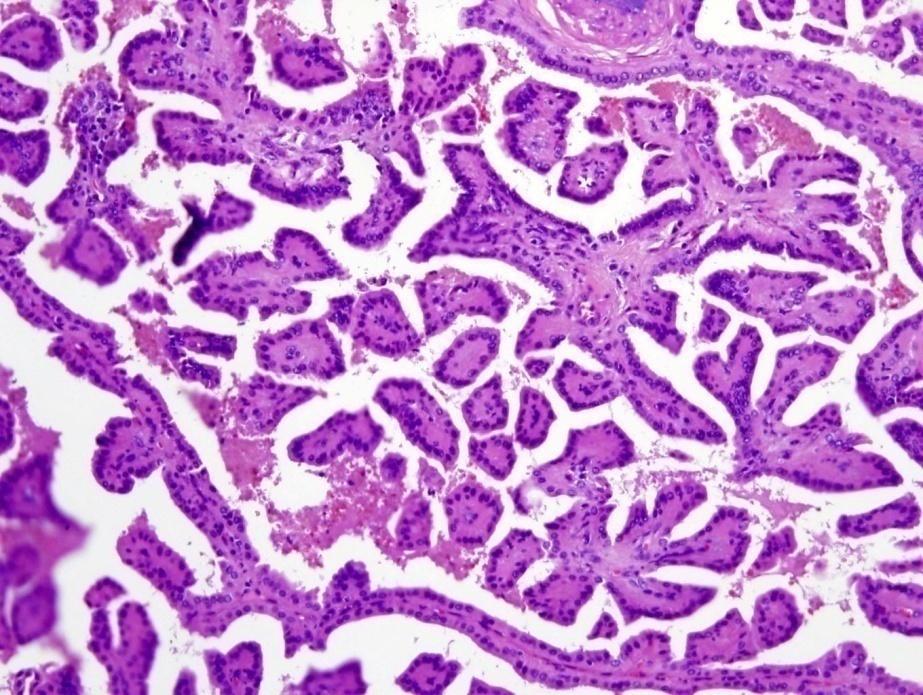
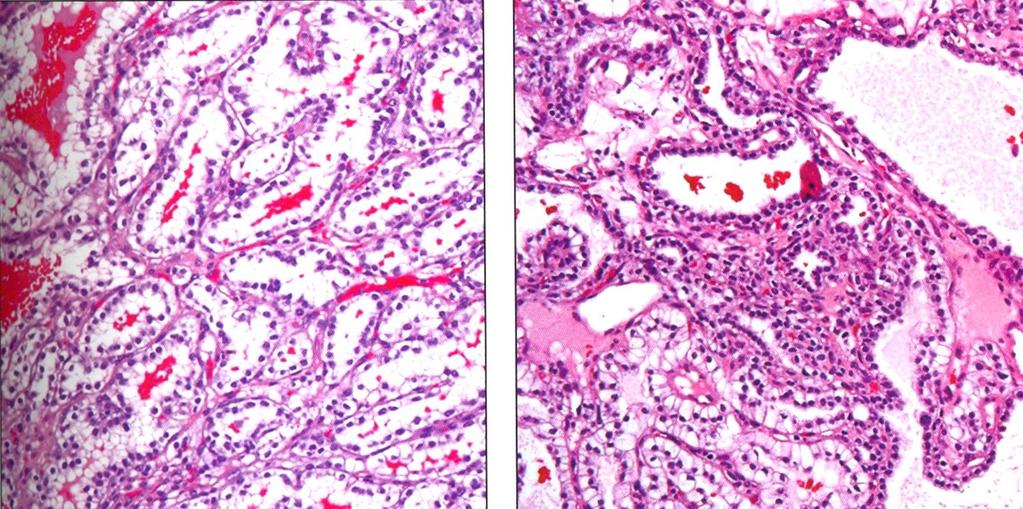
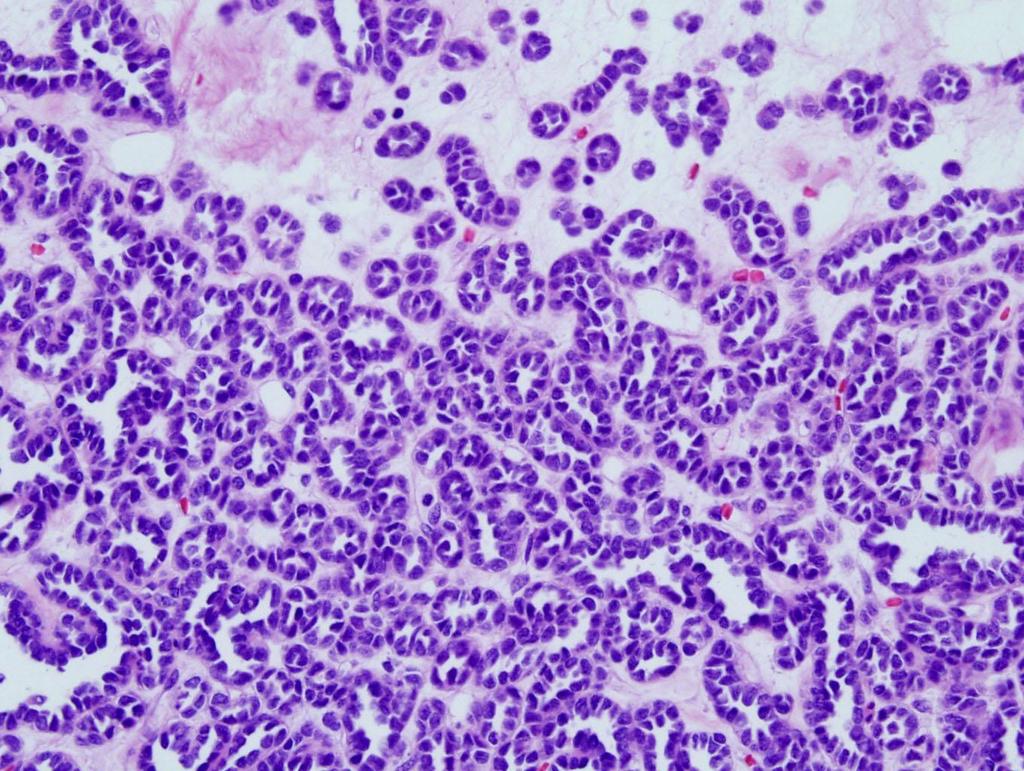
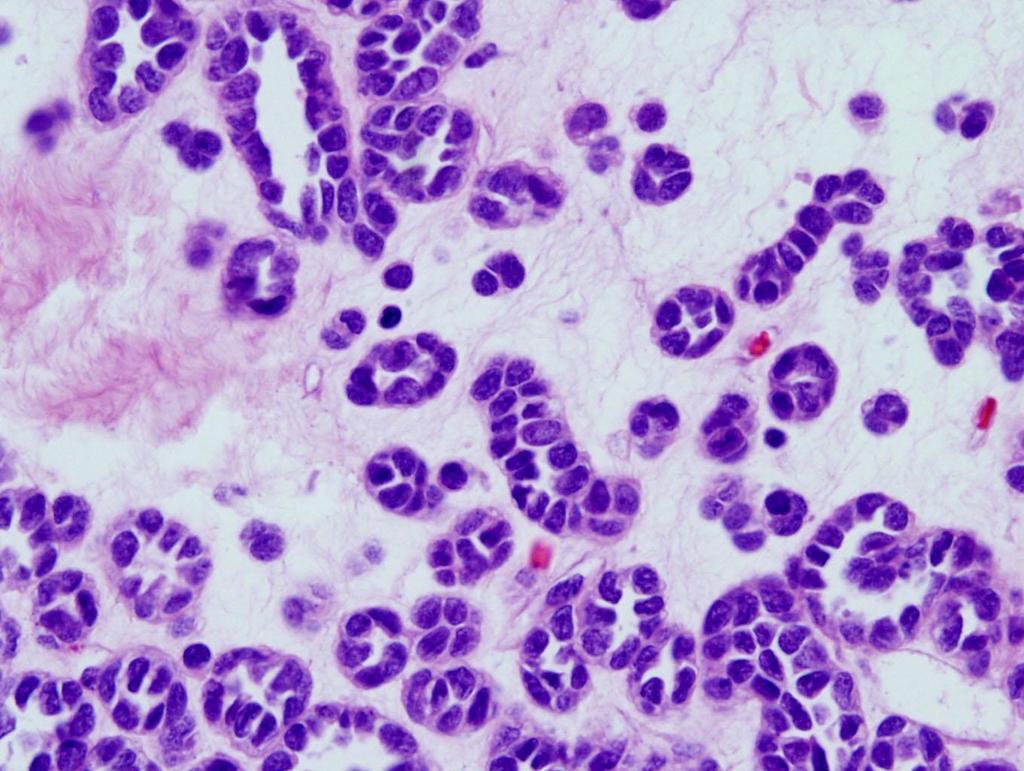
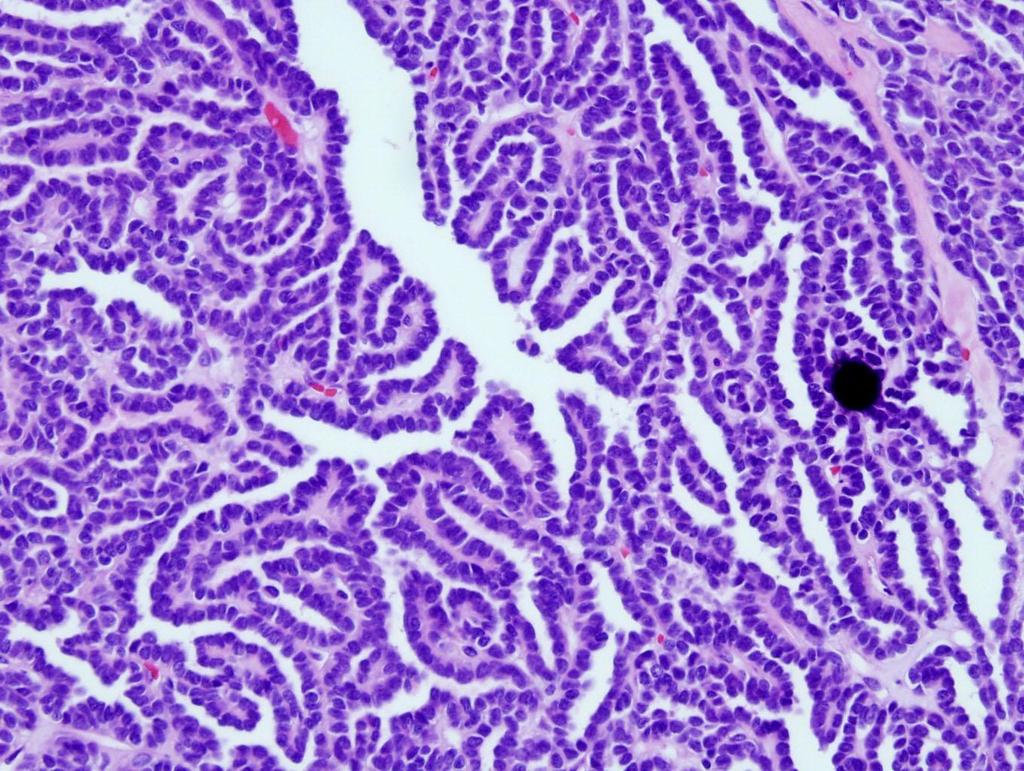
38 Type 1 papillary RCC

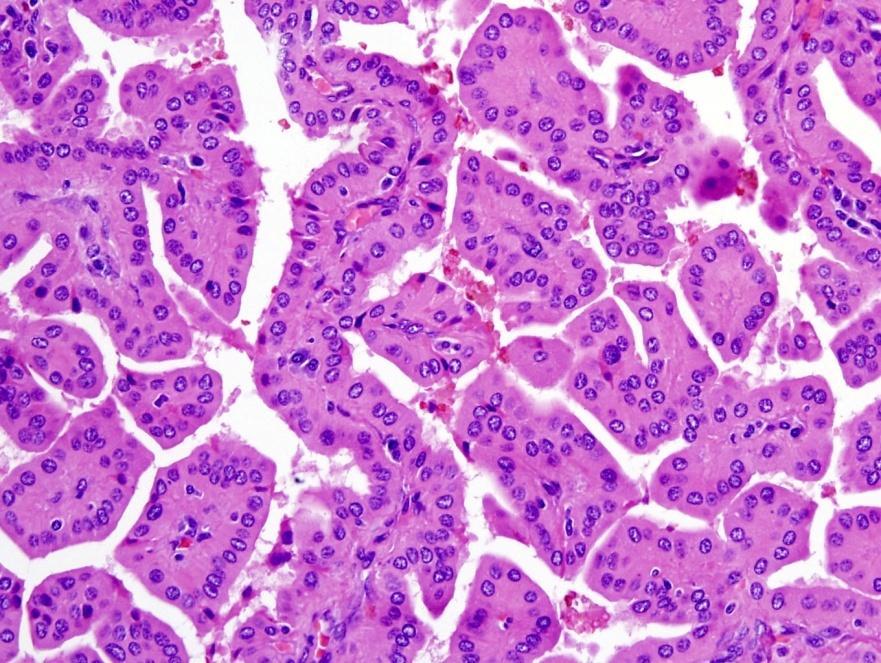
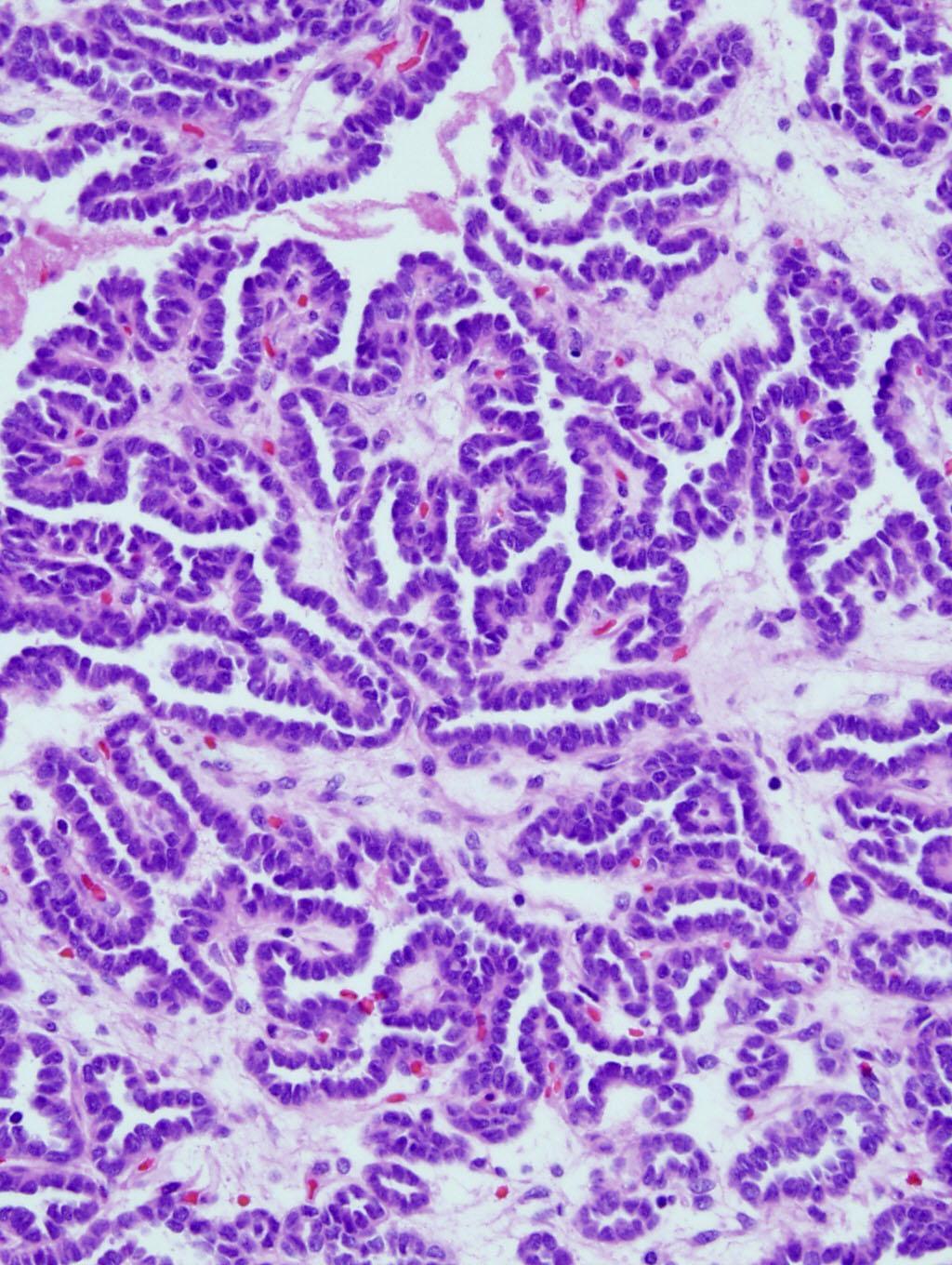
39 Type 2 papillary

40 Type 2 papillary
41 PRCC, type 1 vs. type 2 Type 1 (n=102) 5-yr survival 65% vs. 47% p=0.017 Type 2 (n=48) Shen SS et al. Presented at USCAP 2008, Denver, Colorado

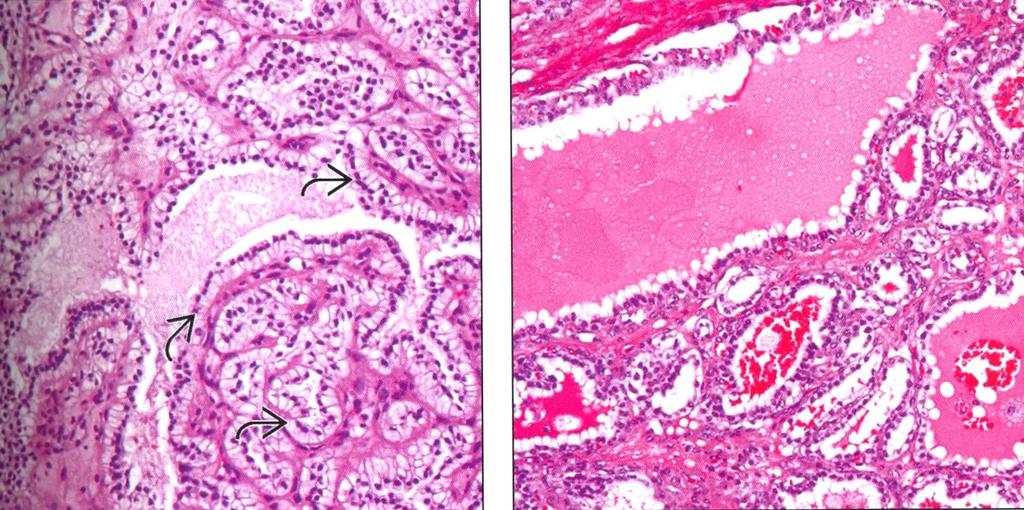
42 Foamy Macrophages

43 Type 2 PRCC macrophages
44 Mucin

45 Solid type

46 Type 1 papillary, solid
 Clear cell papillary RCC specific entity?")
47 Papillary RCC is a Heterogeneous Group of Tumor Clear cell RCC can have pseudopapillary Papillary RCC can have clear cell changes Some papillary RCC can have features of both type 1 and type 2 Type 2 PRCC with low nuclear grade vs. oncocytic papillary RCC (same or different) Clear cell papillary RCC specific entity?
48
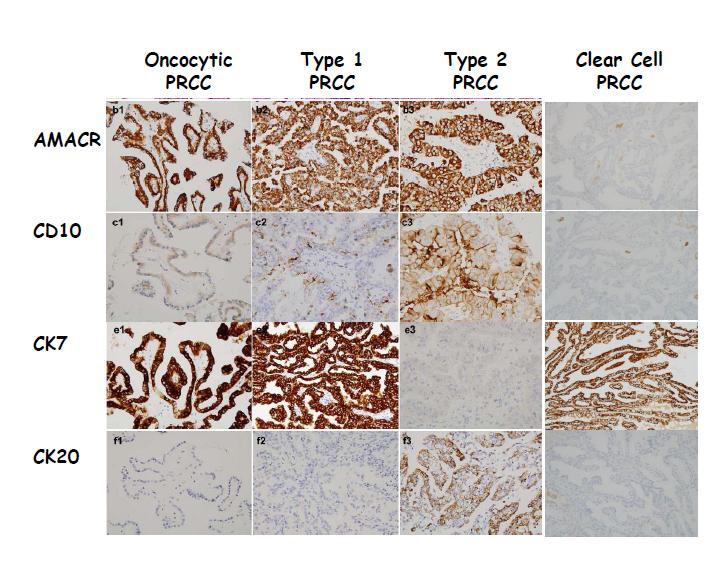
49 Oncocytic Papillary RCC May be a distinct subgroup Kunju et al. (2008) Smaller tumor (mean 2.0 cm) IHC: CK7+ (7/7), CD10+ (7/7), AMACR+ (5/7) FISH: all trisomy 7, 17 No recurrence or metastasis in 22 months Park et al., (2009) Histology: nuclei polarized to surface of papillae IHC: AMACR+ (7/7), CK7+ (7/7), CD15+ (6/7) Cytogenetics: 3p+, 11q+, 17q+, 4q- No recurrence or metastases in 3 years
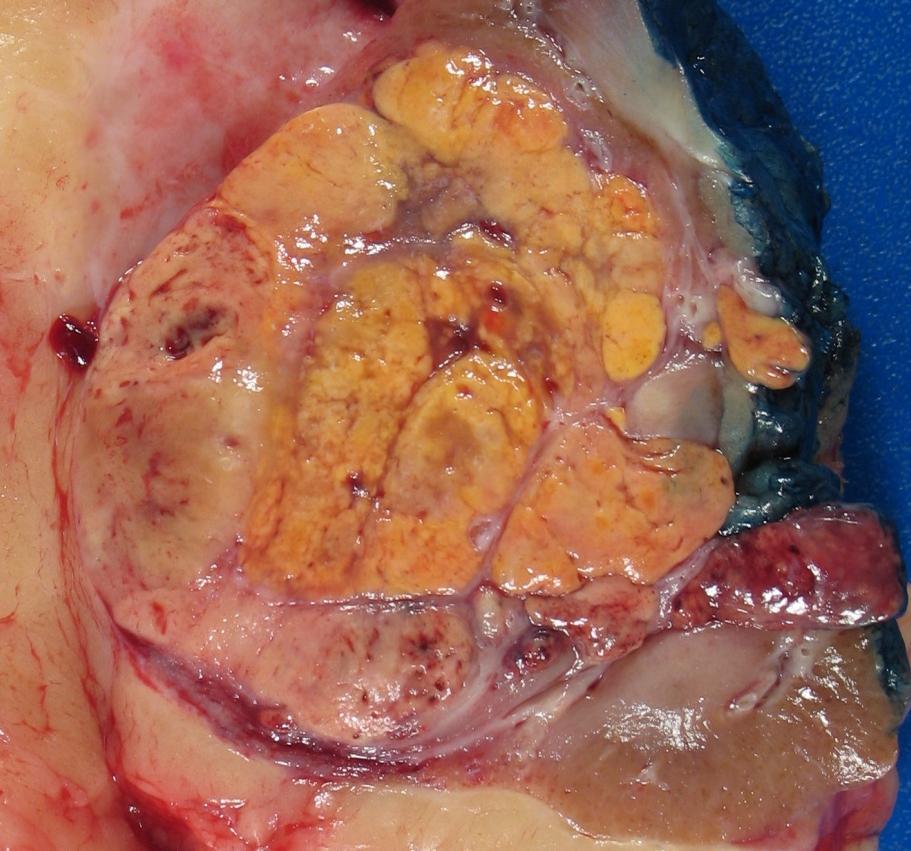
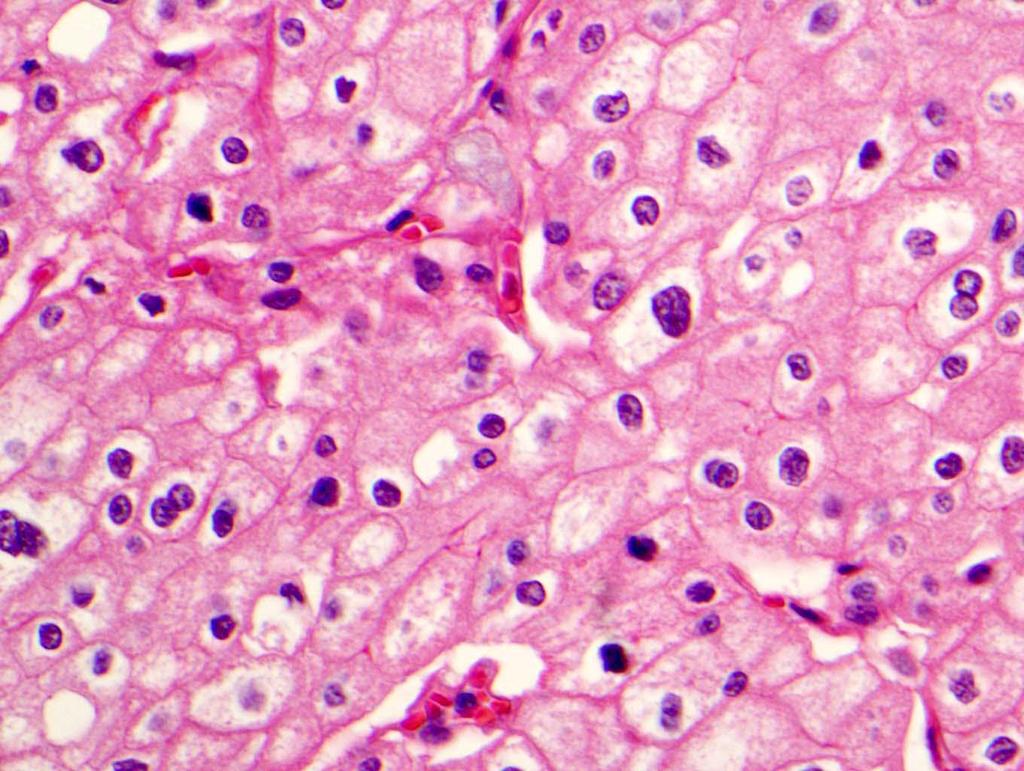
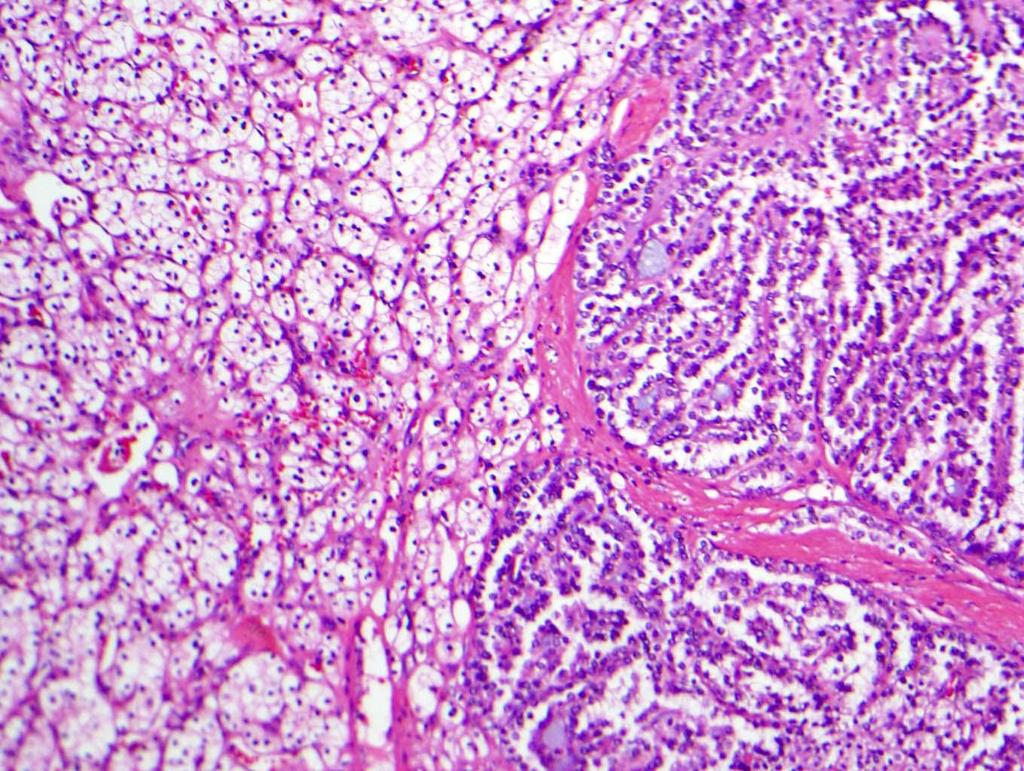
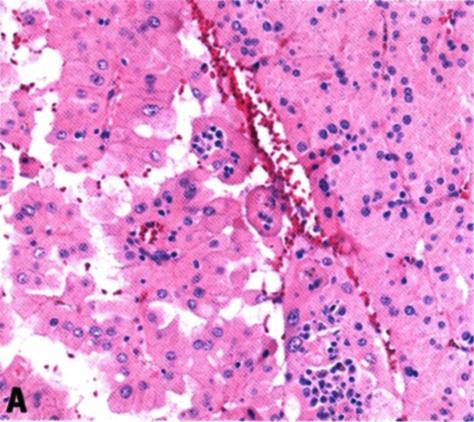
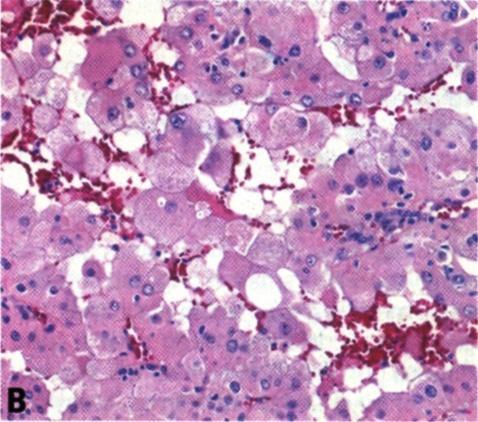
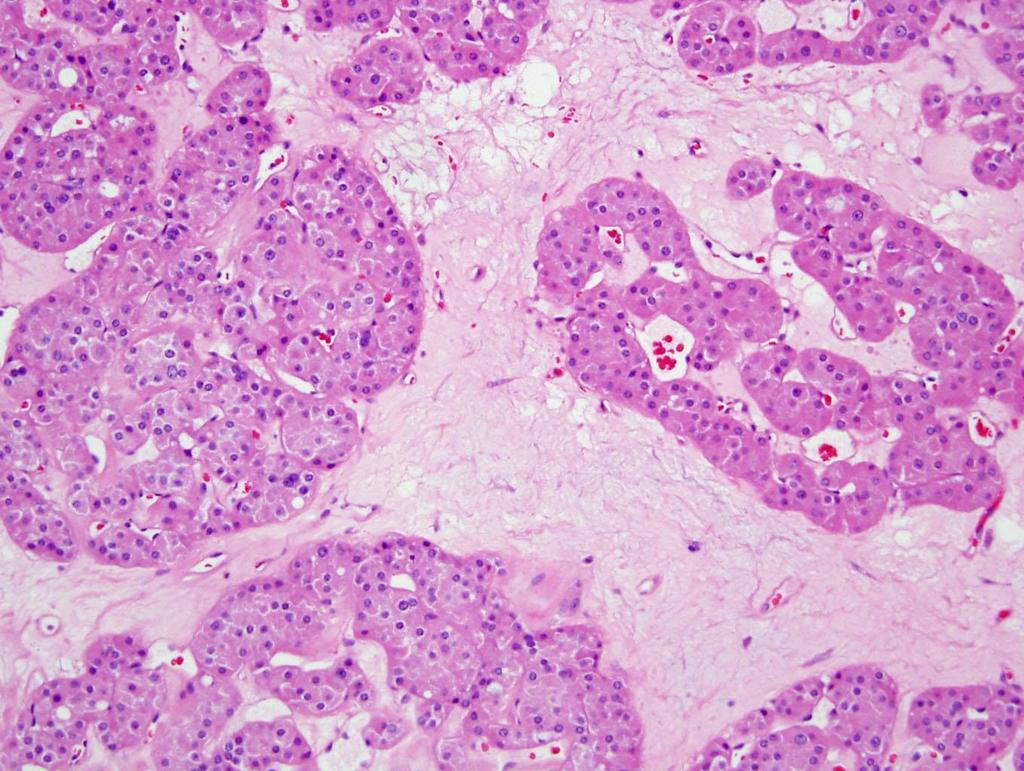
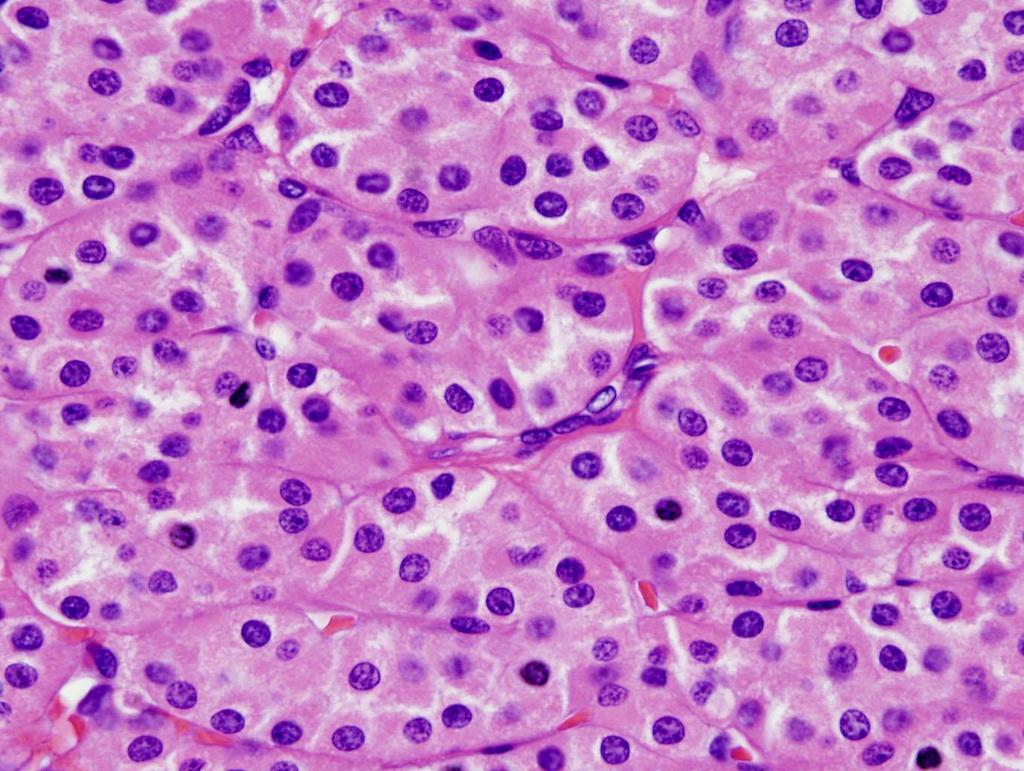
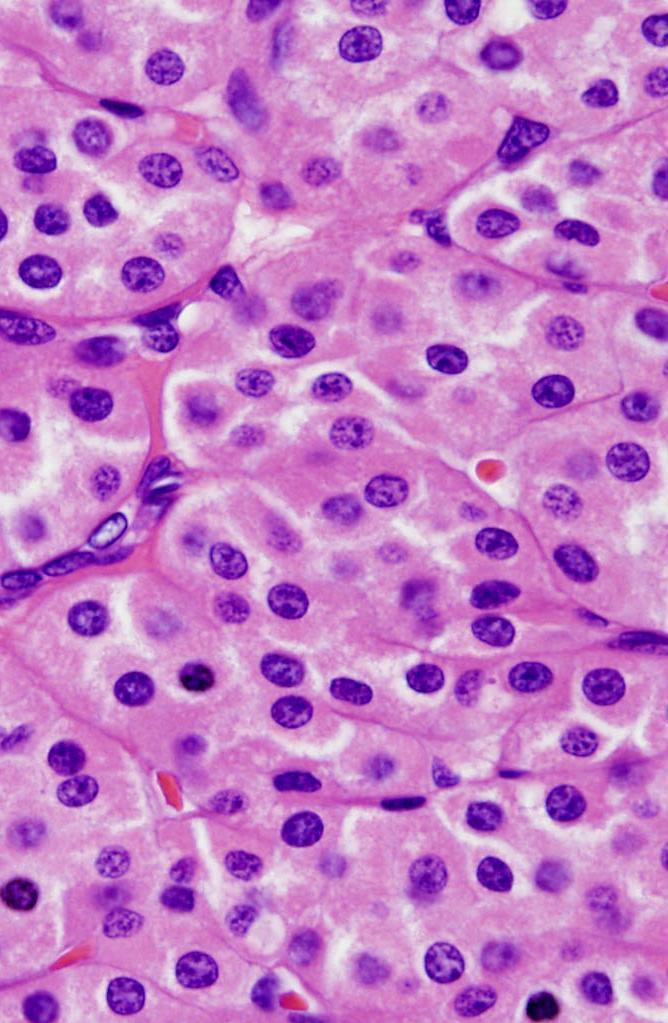
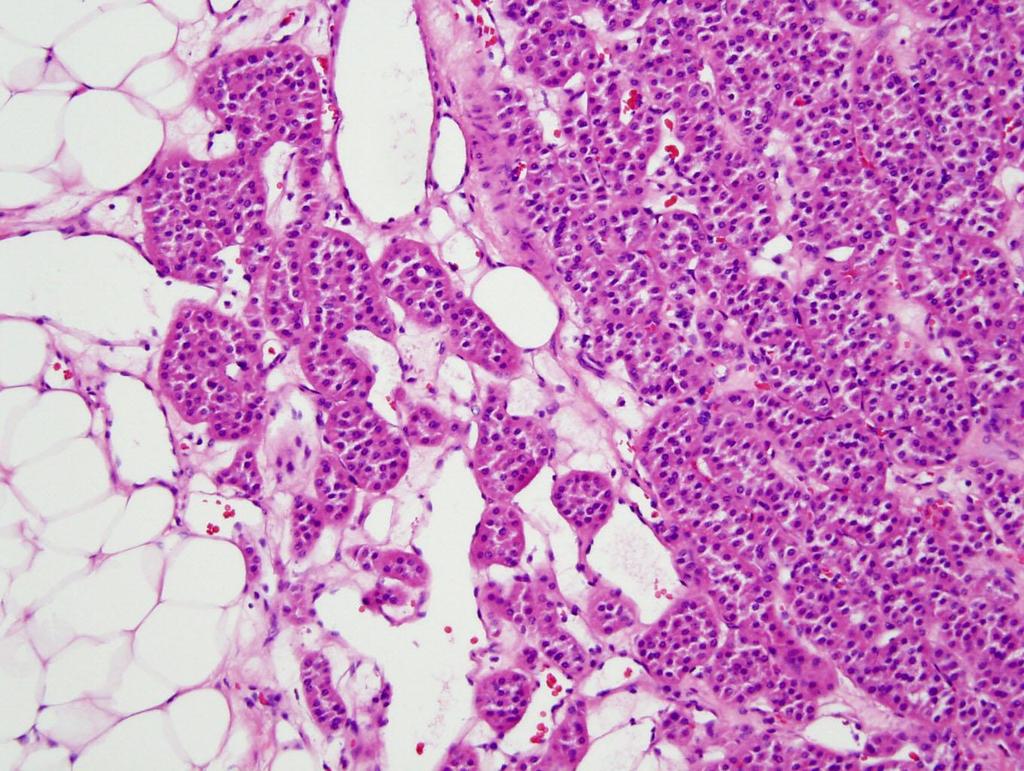
50 Chromophobe RCC Initially described by Thoenes et al in 1985 Two types described in 1988 Loss of multiple chromosomes (-1, -Y -2, -10, -13 etc.) Better prognostic group Association with oncocytoma (hybrid)?




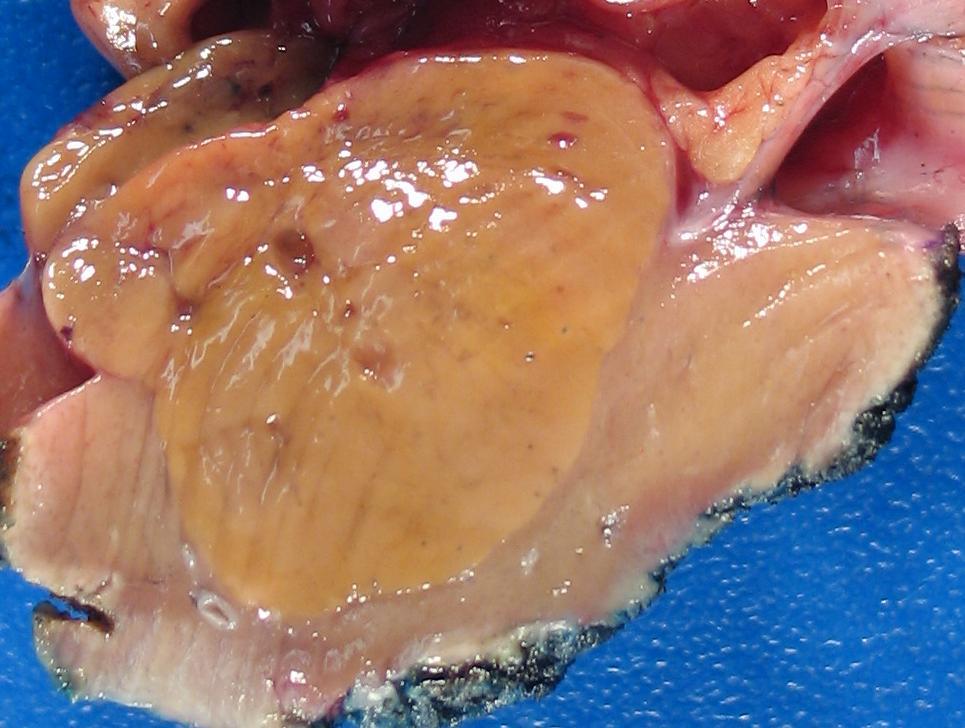
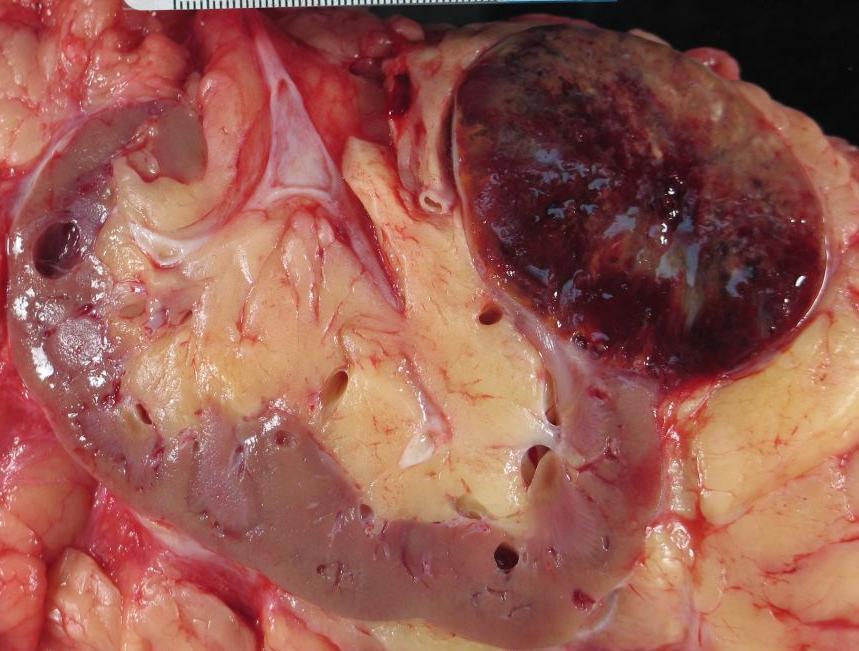
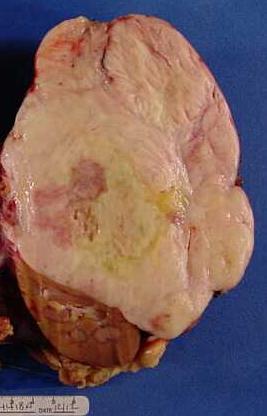
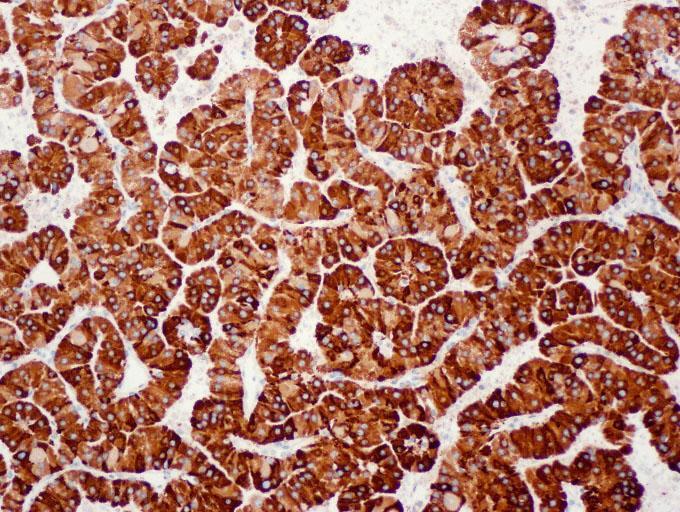
51 Common Gross Features: 1. Homogeneous 2. Mahogany brown Chromophobe RCC 3. Solid 4. Well circumscription
52
 Cytoplasmic quality (halo) Nuclear features (wrinkling, binucleation) Cytoplasmic membrane")
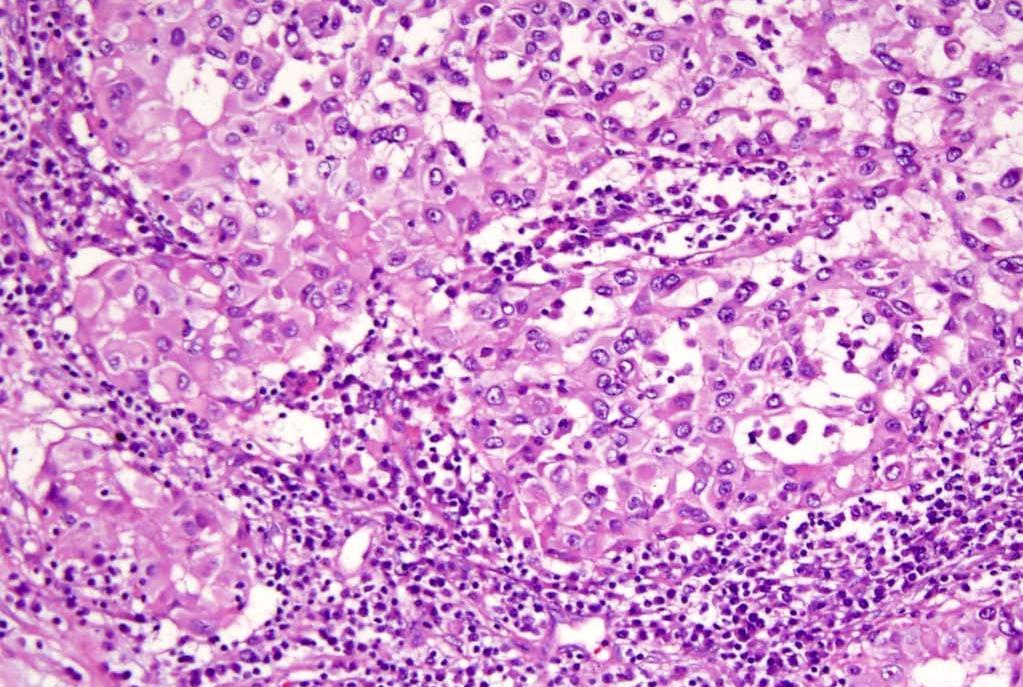
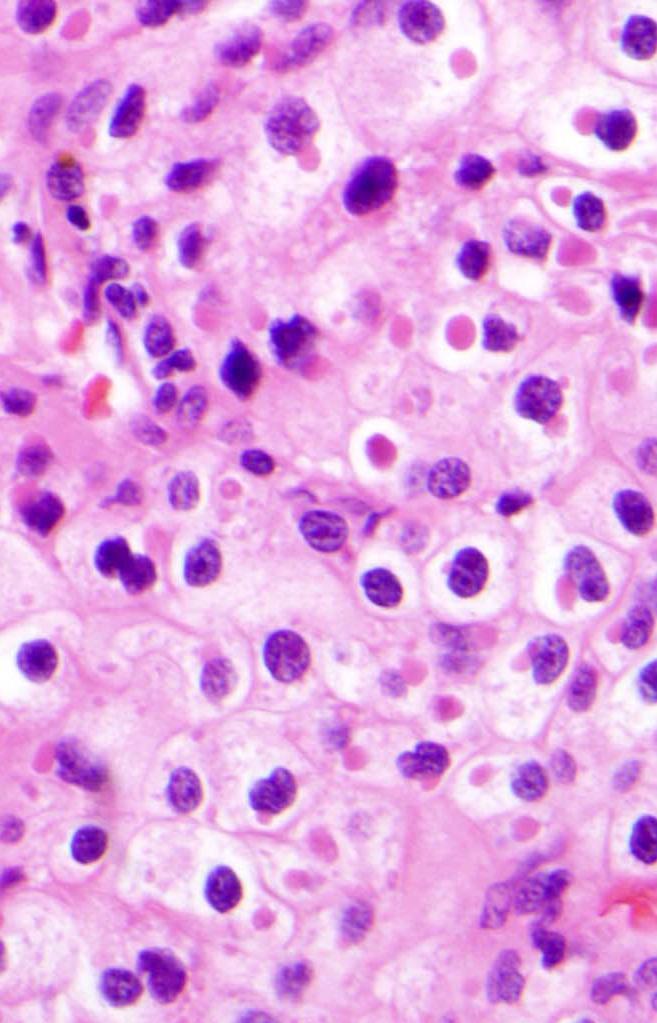
53 Chromophobe RCC Key Diagnostic Features Growth patterns Solid sheets, broad alveoli, tubular Broad fibrotic septae, thick-walled and hyalinized vessels, linear or parallel Cytologic features Cell types (mixed) Cytoplasmic quality (halo) Nuclear features (wrinkling, binucleation) Cytoplasmic membrane (prominent)

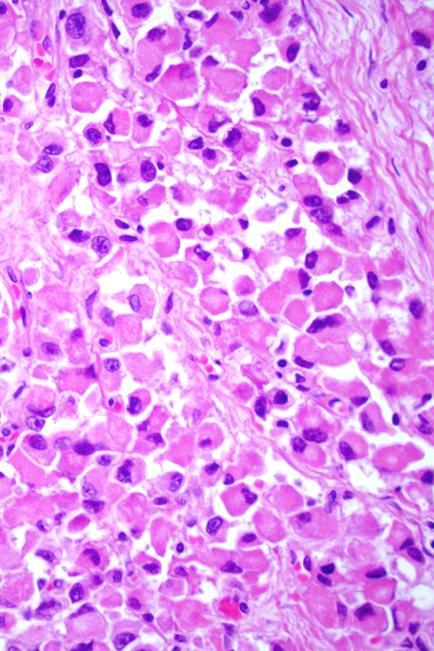
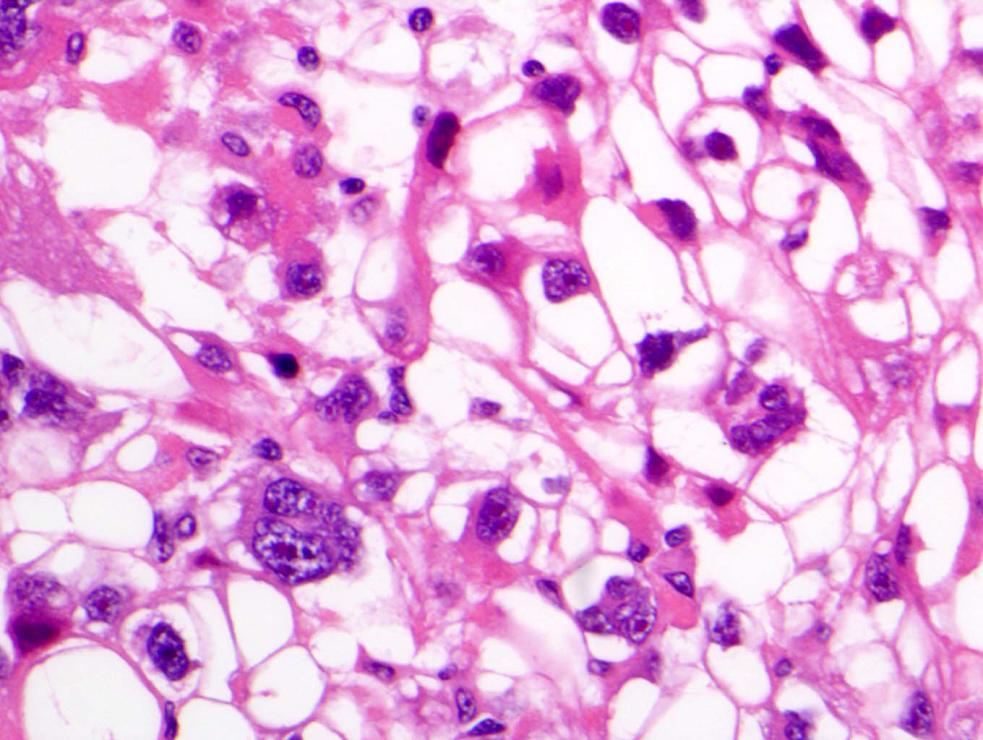
54 Chromophobe RCC Three Types of Cells Type 1: Eosinophilic cell with no perinuclear halo Type 2: Eosinophilic cell with perinuclear halo Type 3: Largest polygonal cells with voluminous, reticulated cytoplasm
55 Chromophobe RCC Morphologic Spectrum Typical: Easy to diagnose May be confused with clear cell RCC + Eosinophilic: + Predominant type 1 or type 2 cells; May be confused with oncocytoma
56
57
58
59
60
61
62 Collecting Duct Carcinoma Rare (less than 1%) Major differential: TCC, metastasis, sarcomatoid RCC Histology: features of a high grade adenoca and TCC, desmoplasia Highly aggressive
63
64
65
66 RCC, Unclassified Definition: tumor that does not fit into any known types by morphology or genetics RCC with mucin production? Composites of recognizable types? Unrecognizable cell types RCC with sarcomatoid change in which the epithelial elements cannot be assigned to one of the known categories

67 RCC with Mucin Production = Unclassified RCC Papillary RCC (20%~30%) Collecting duct carcinoma Invasive urothelial carcinoma Mucinous tubular and spindle cell carcinoma

68 Composite Recognizable Types = Unclassified? If low grade, better to diagnose as mixed subtypes If high grade,? RCC, unclassified
69
70 Renal Cell Carcinoma, Unclassified Reserved for those truly unclassifiable based on adequate sampling of tumor Rule out metastatic tumor Consultation is advisable Immunohistochemical stains may be helpful Cytogenetic analysis?

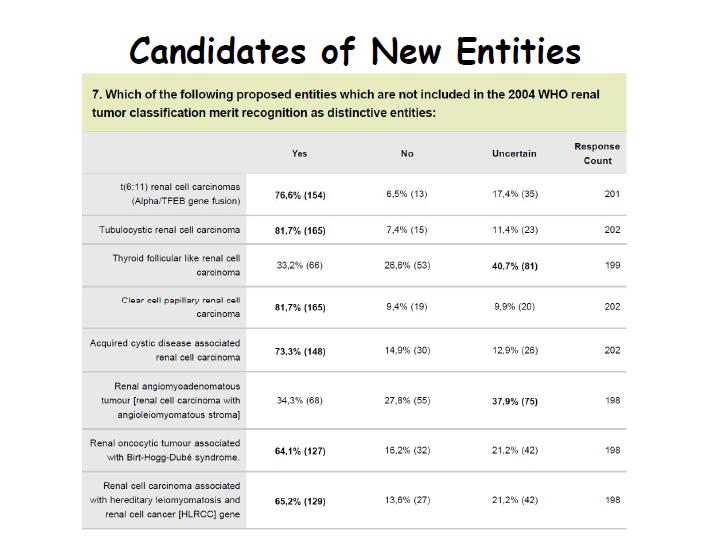
71 4 Newly Defined RCC Entities Xp11 translocation carcinoma Mucinous tubular spindle cell carcinoma Multilocular cystic clear cell RCC Carcinoma associated with neuroblastoma
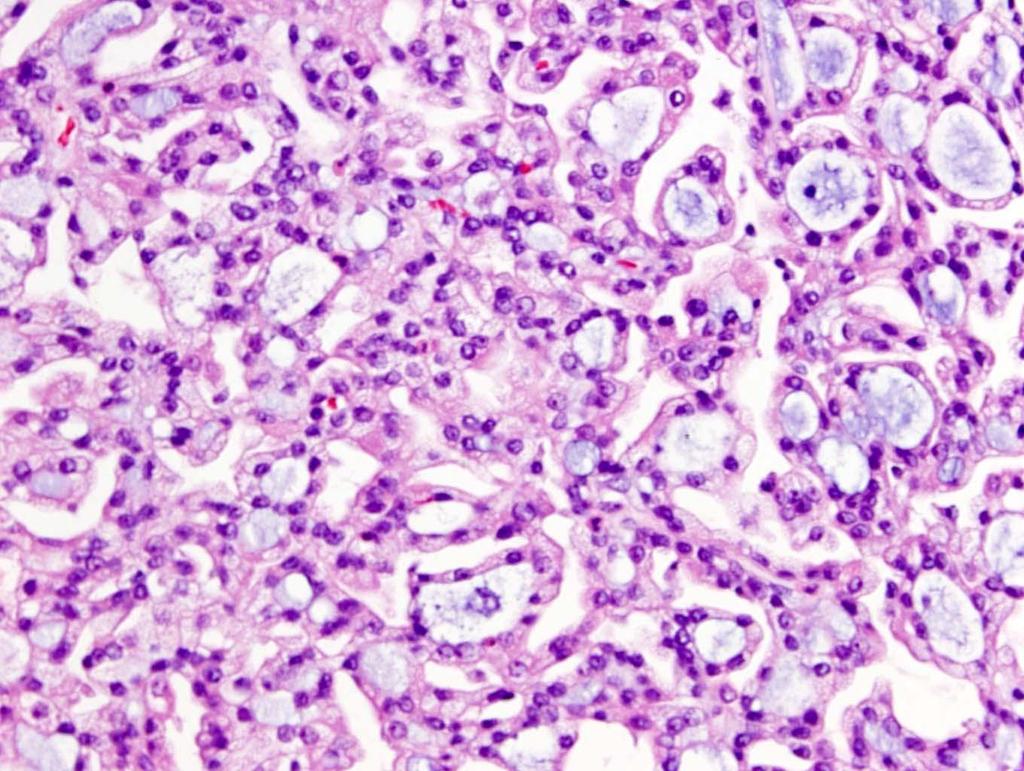
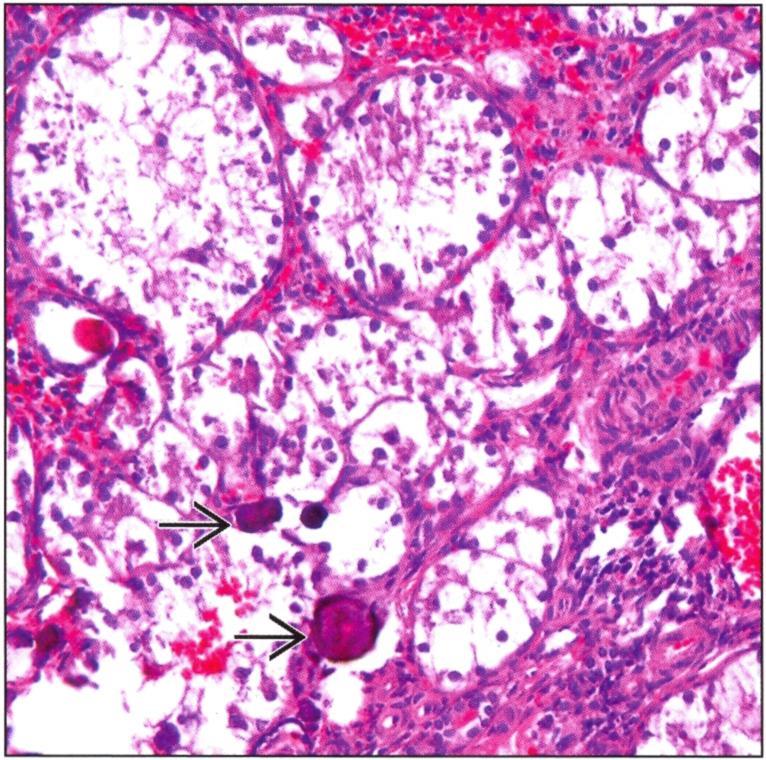
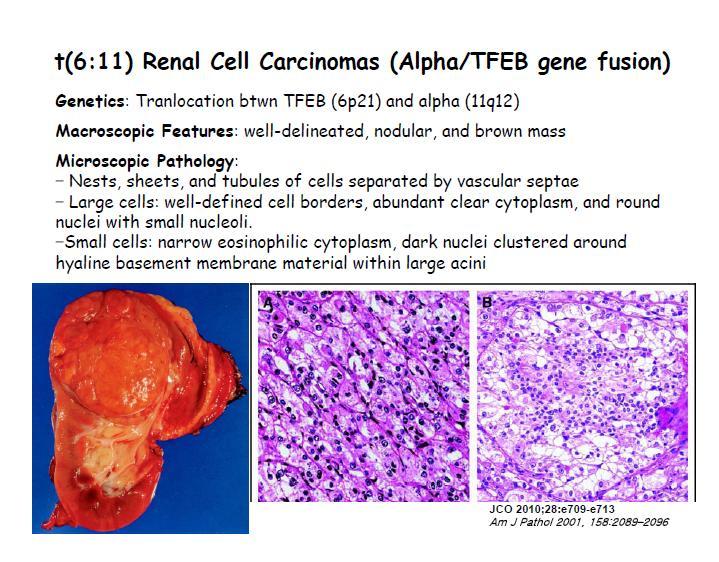
72 Xp11 Translocation Carcinomas A group of RCC with translocation involving Xp11.2, resulting TFE3 genes fusion Occur in children and young adult (~1.5%) Micro: papillary or nested growth with clear cytoplasm, psammoma bodies (common) IHC: TFE3/TFEB+ (nuclear) and RCCm, CD10, Pax-2+ Cytokertain -/weakly + Clinical outcome: may be more aggressive in adult

73 Xp11 Translocation Carcinomas TFE3 TFE3 Shen SS, Truong LD, Ayala AG, and Ro JY. Arch Pathol Lab Med :
74

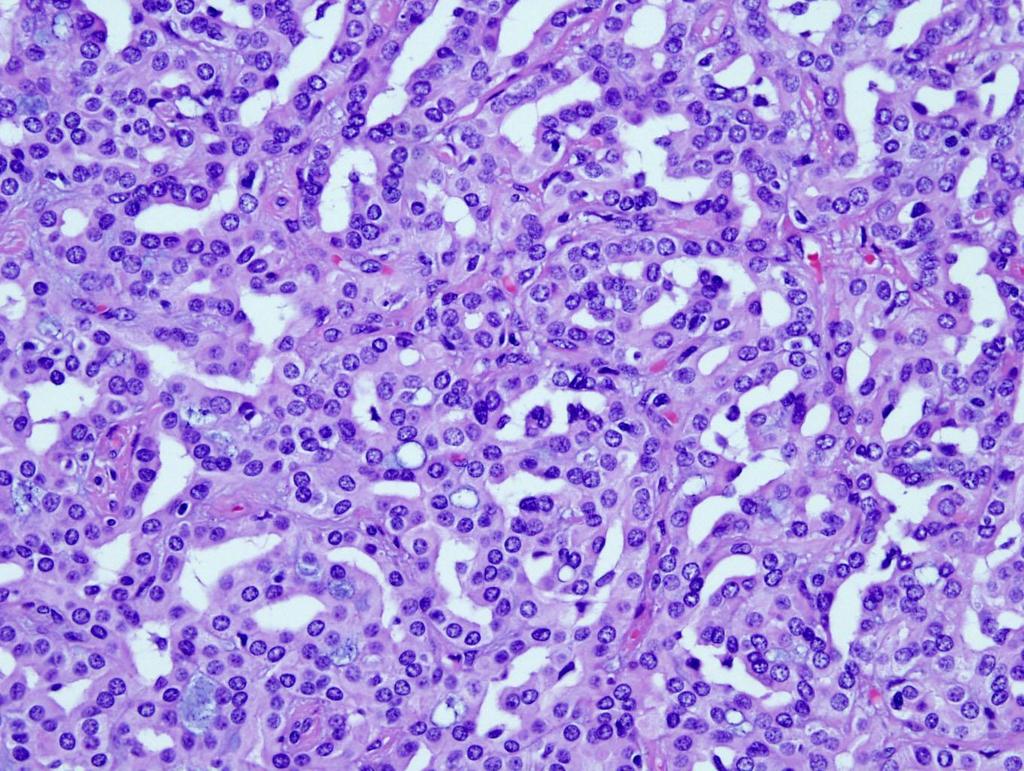
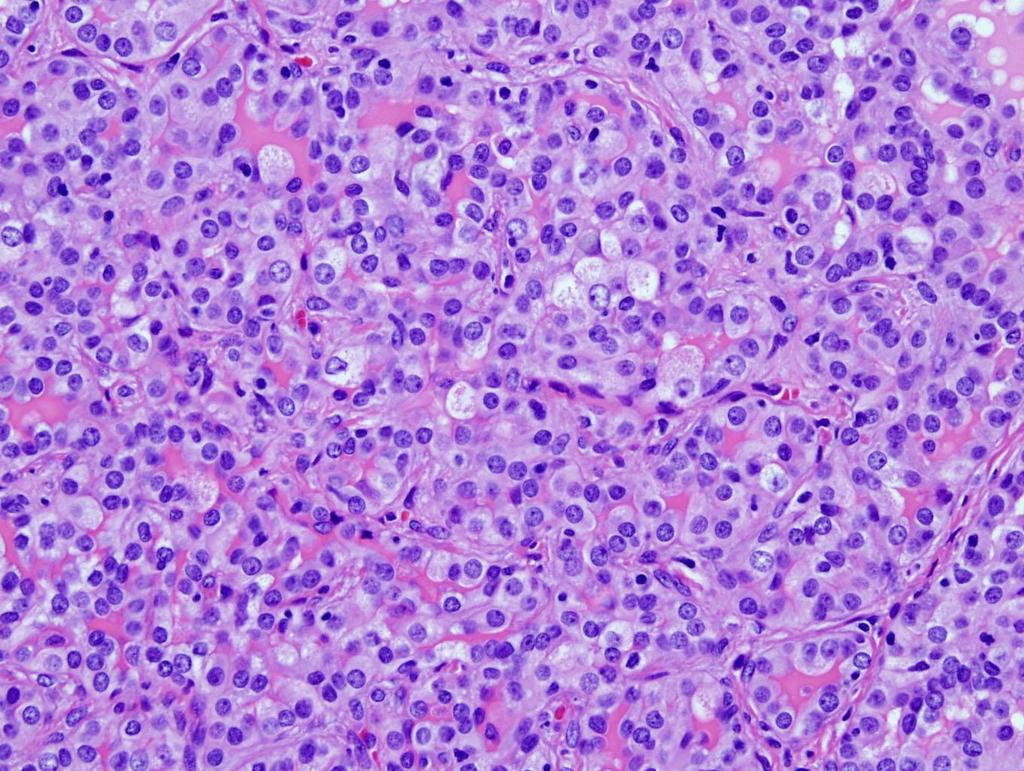
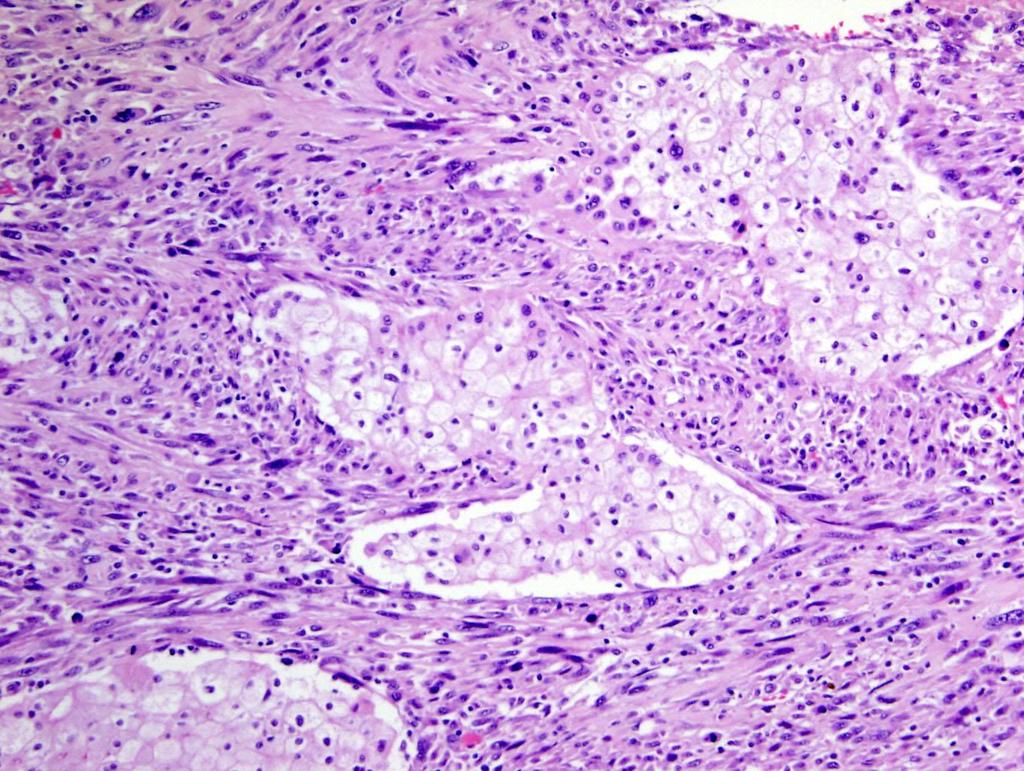
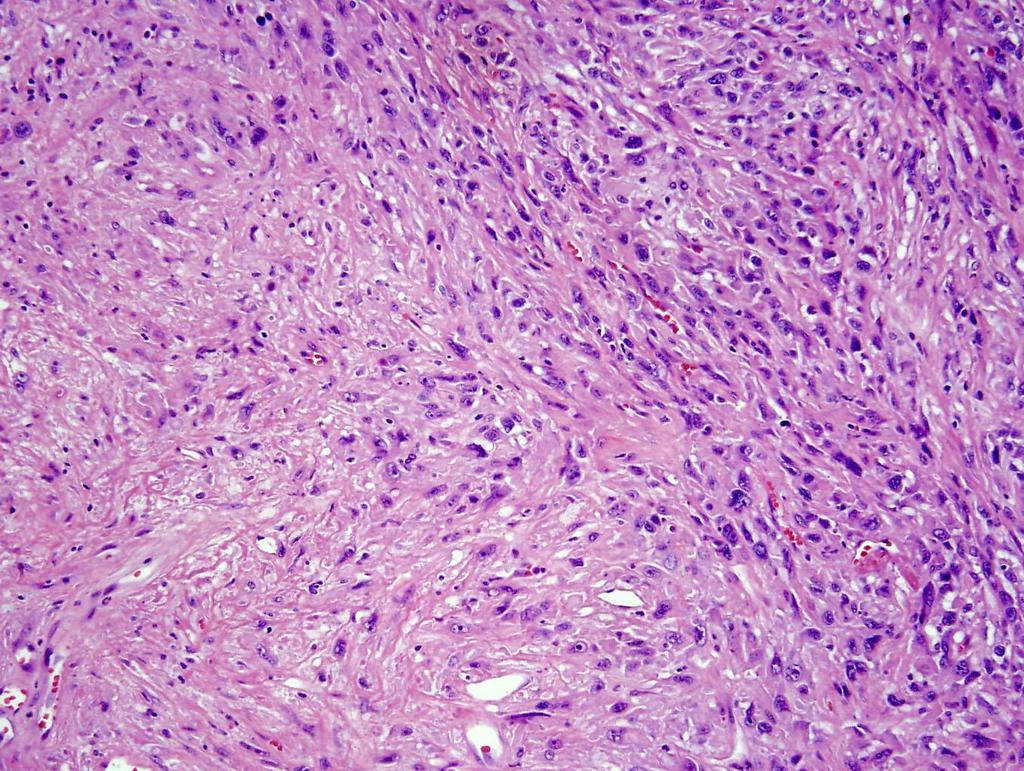
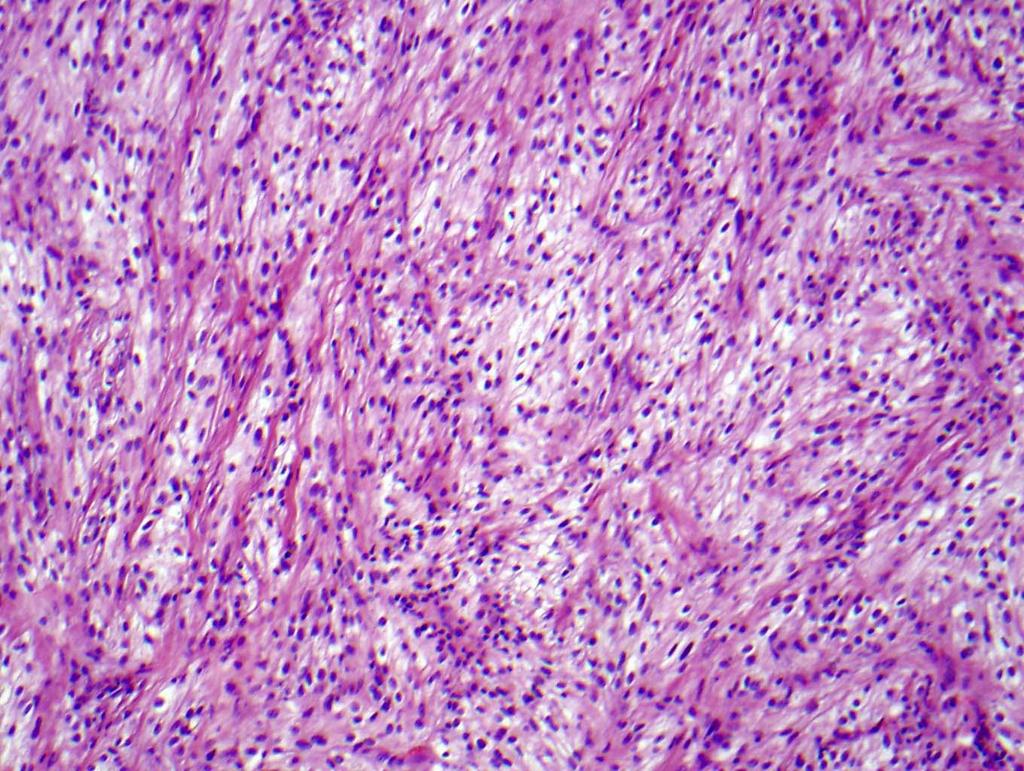
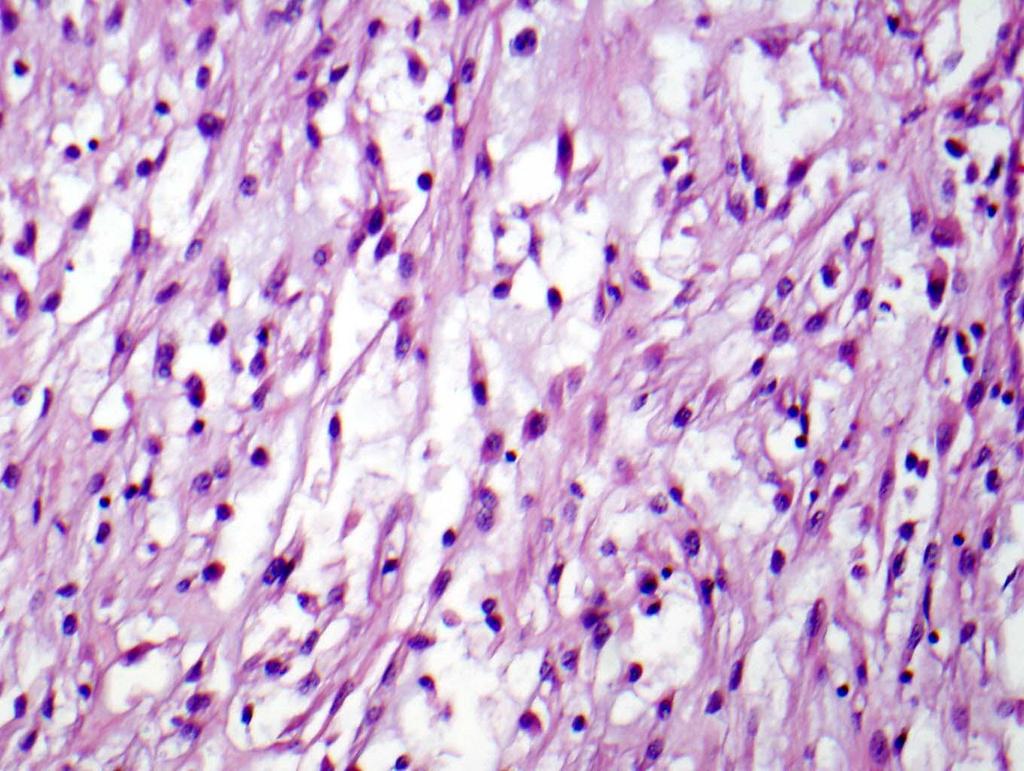
75 Mucinous Tubular and Spindle Cell Carcinomas Female predominance (4:1) Wide age range (17-82 yrs) Low grade indolent behavior? Multiple loss of chromosomes (1, 4, 6, 8, 9, 13, 14, 15, 22), lack of -3p Distinct entity or variant of papillary RCC?


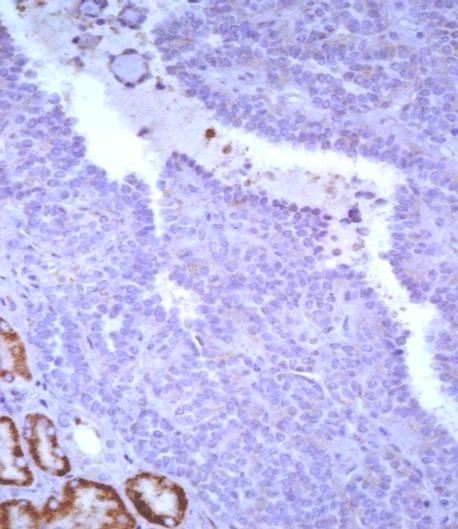
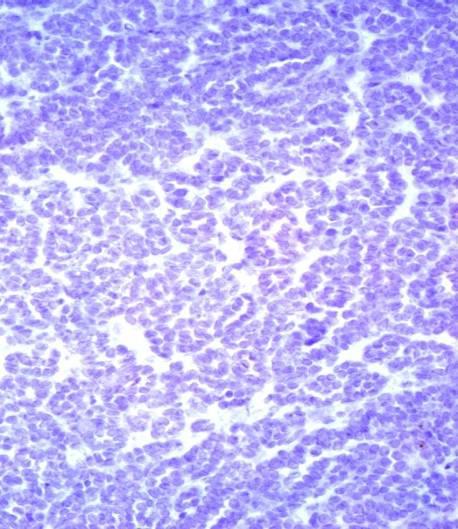
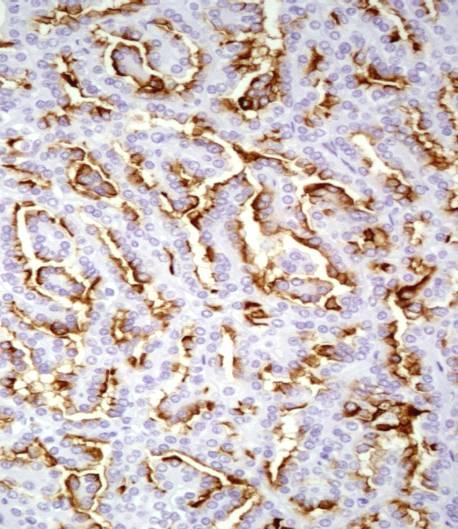
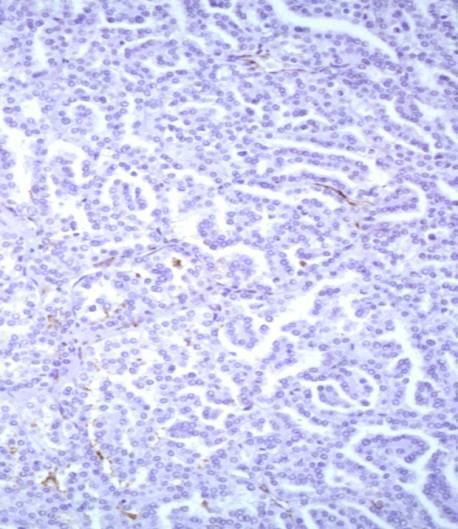
76 Mucinous Tubular and Spindle Cell Carcinoma P504 RCCm CD15 Shen SS, Ro JY et al. Annals of Diag Pathol :13-21.
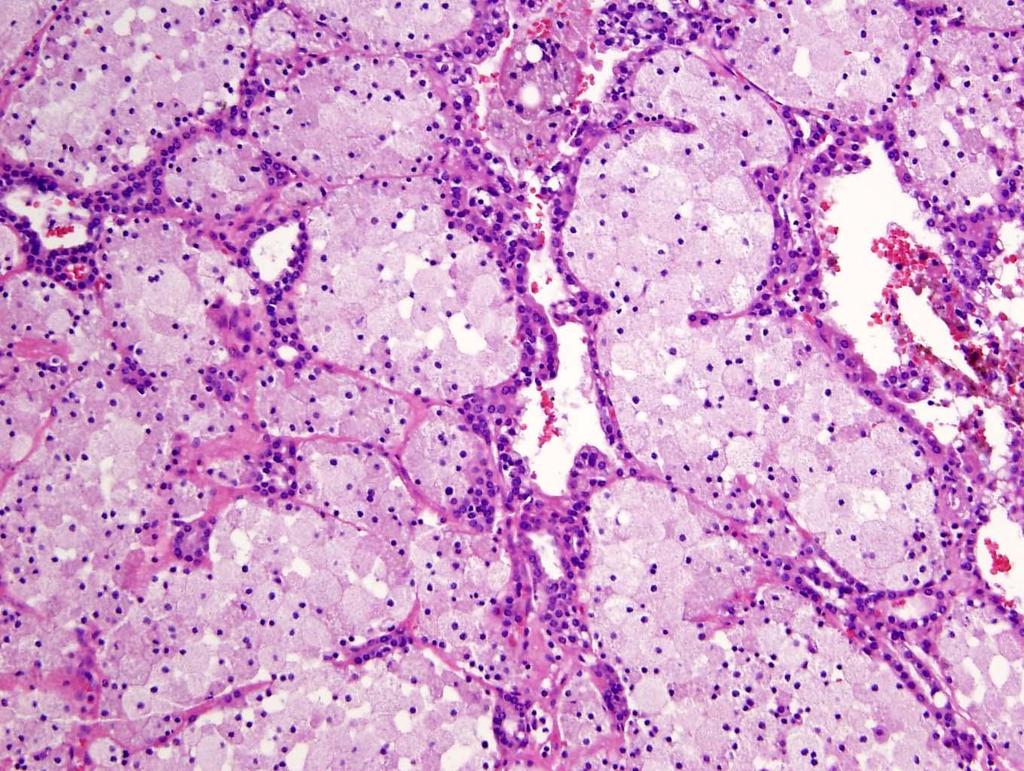
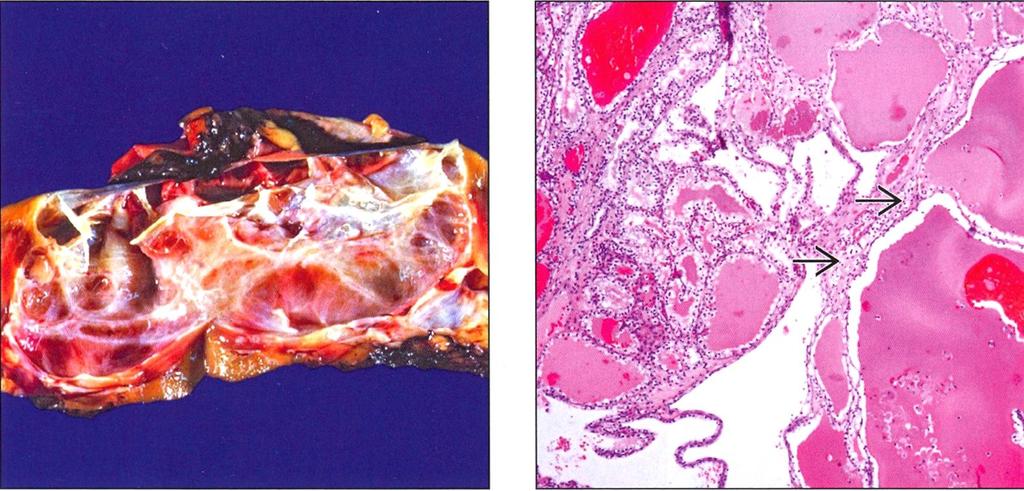
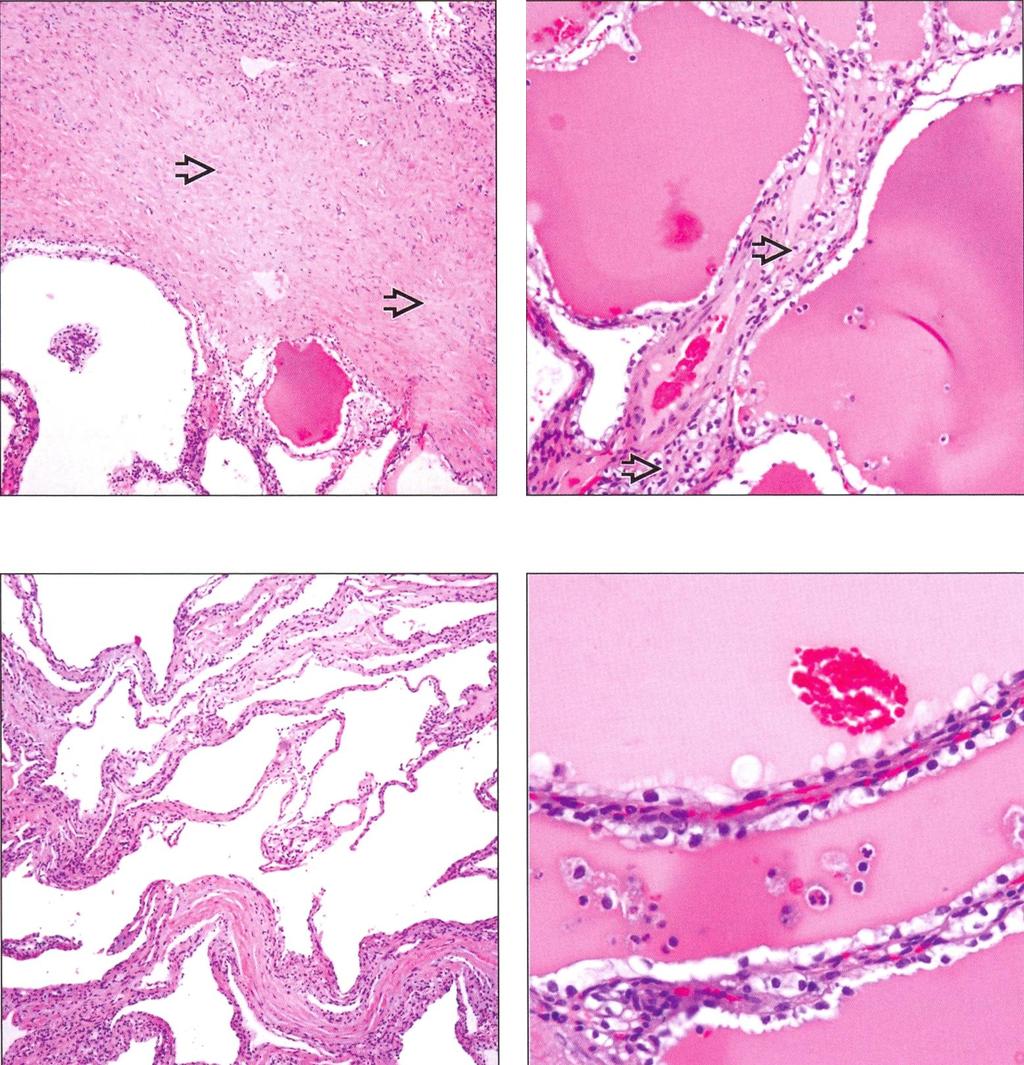
77 Multilocular Cystic Clear Cell RCC Composed of entirely cystic components Lined by layers of clear cells Low nuclear grade (G1 or G2) Lack of nodules of solid area of clear cells Excellent prognosis


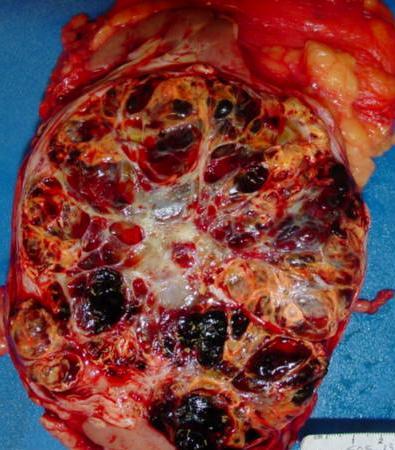
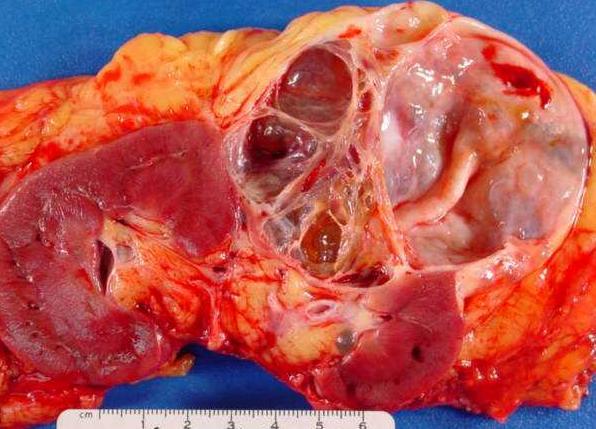
78 Cortical cyst Cystic nephroma/mestk Multilocular cystic clear cell RCC RCC with cystic changes
79
80

81 CA9 CK7 CD10 HMCK
82 RCC associated with neuroblastoma ~18 cases have been reported Male/female equally affected Neuroblastoma diagnosed, Age < 2 yrs RCC detected, 13.5 years (range 2 to 35) Tumor size: 4 cm (1-8cm) 1) solid/papillary with abundant eosinophilic cytoplasm; 2) clear RCC
83
84 4 Newly described entities Tubulocystic carcinoma Thyroid-like follicular carcinoma Acquired cystic disease associated RCC Clear cell papillary RCC


85 Tubulocystic RCC Also known as low grade CDC < 60 cases reported Strong male preponderance 7: (mean 60yo) Closely related to papillary RCC type 1 +CK7, AMACR, CD10, CK19

86 CK7 AMACR H&E RCC, low grade papillary RCC, tubulocystic RCC, high grade papillary Yang XJ, Zhou M, Hes O, Shen SS et al AJSP 32:177;2009, 33:1840
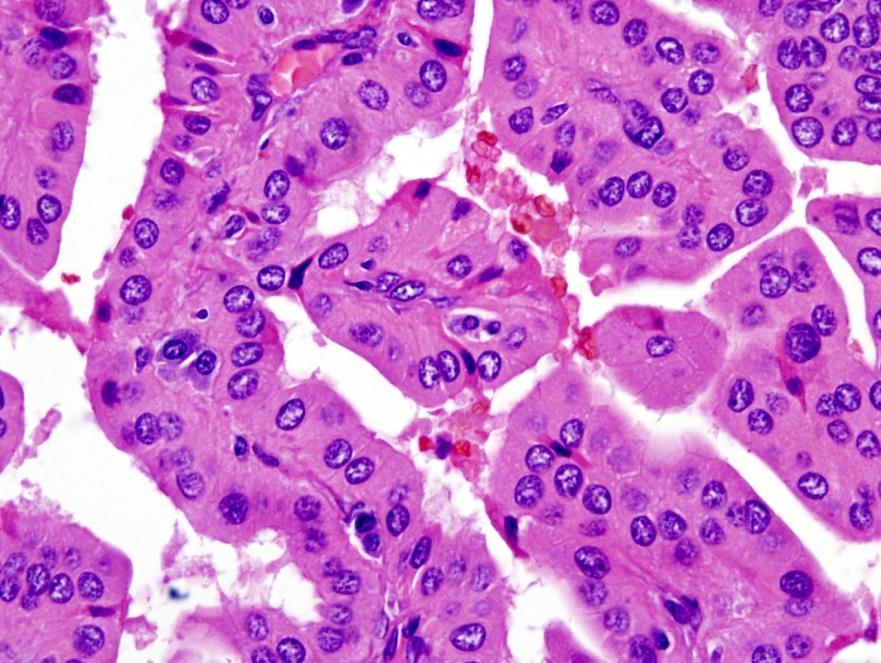
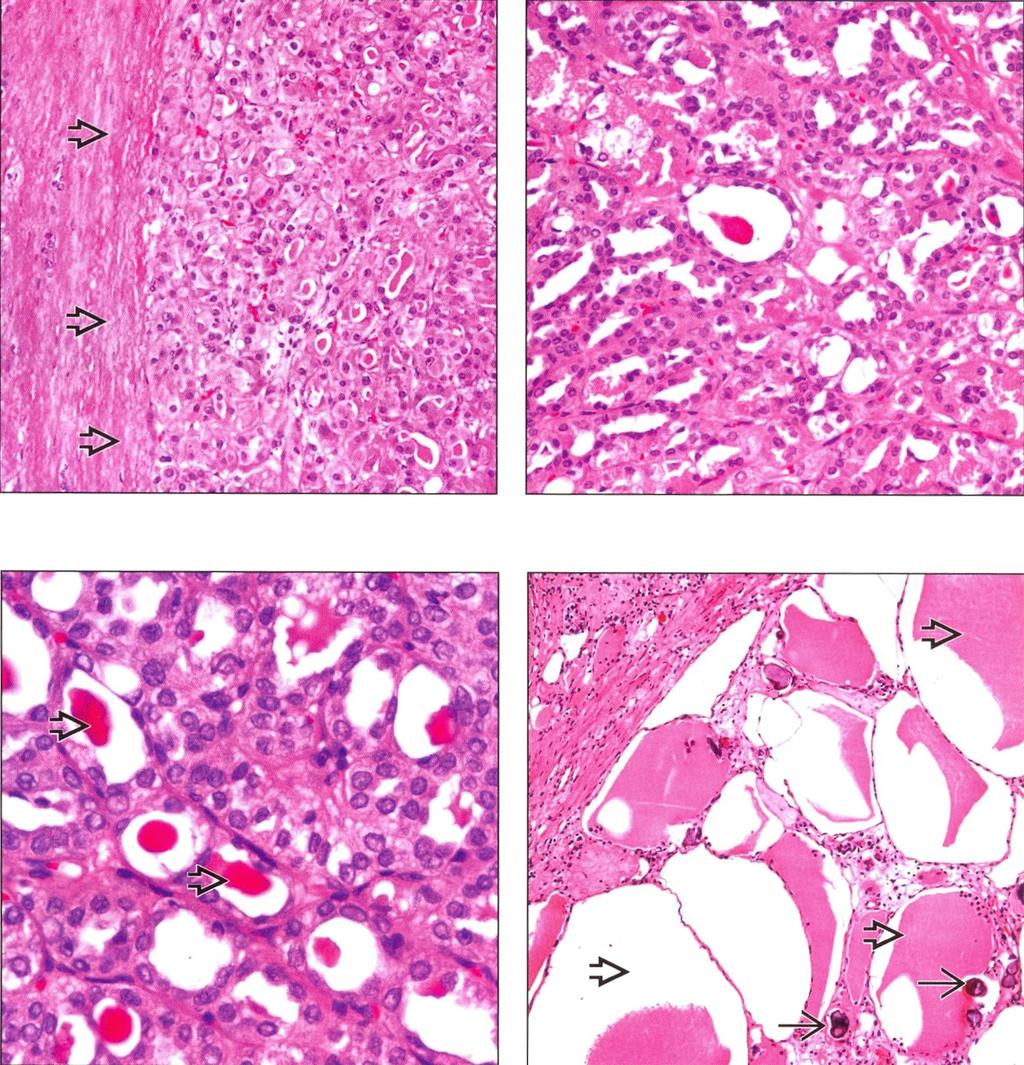
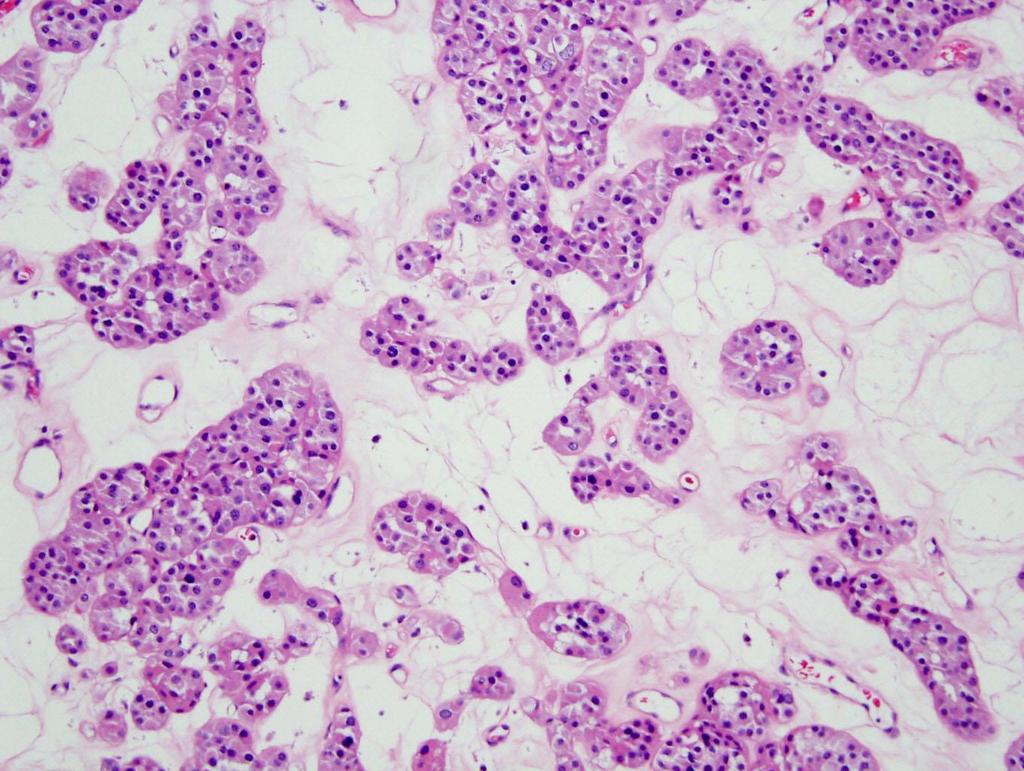
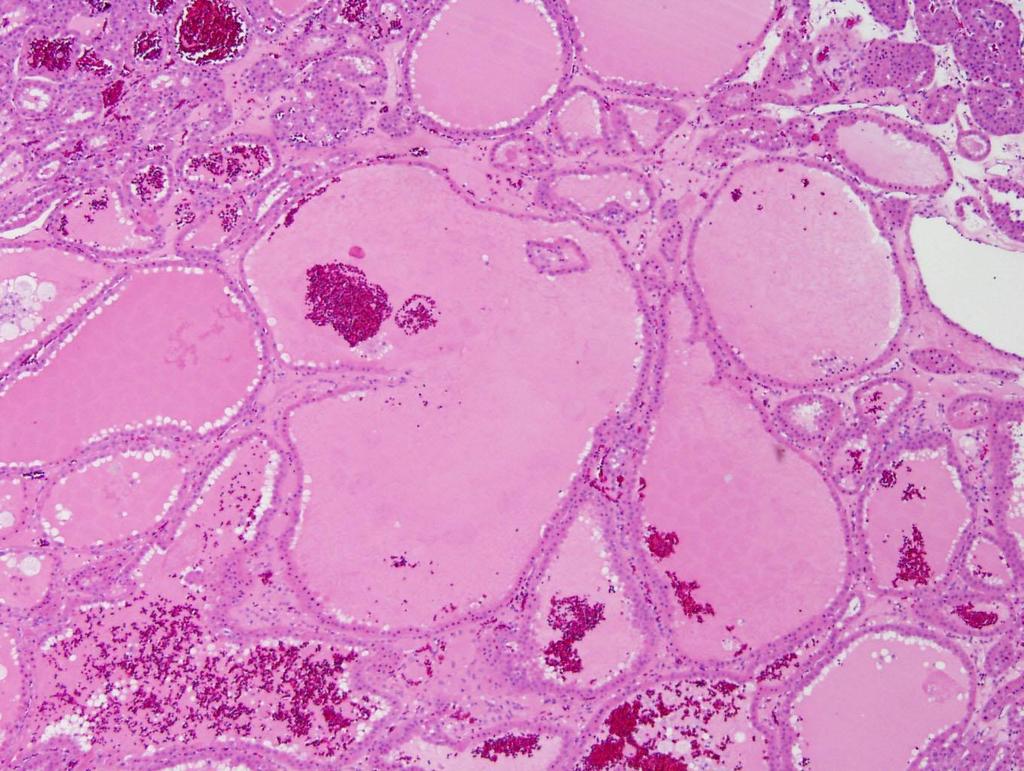
87 Thyroid Follicular Carcinoma-like Tumor of Kidney Jung SJ, Chung JI, Park SH, Ayala AG, and Ro JY. Am J Surg Pathol : The tumor with follicular architectures containing luminal inspissated colloid-like material; no recognizable RCC Strongly positive for CK (AE1/AE3), CD10, Focal cytoplasmic stain for CK35βH11 and vimentin Negative for TTF-1 and thyroglobulin, CK7, CK19, CK20, CK34βE12, CEA, EMA, and CD15. CGH showed gains of 7q36, 8q24, 12, 16, 17p11- q11, 17q24, 19q, 20q13, 21q22.3, and Xp and losses of 1p36, 3, and 9q These findings are dissimilar to previously classified renal neoplasm
88
89 Thyroid Follicular Carcinoma-like Renal Tumor: A Case Report Sterlacci WS et al. Virch Arch. 2008;412:91-5; Amin MB et al, Am J Surg Pathol 2009;33: Follicular structures with abundant eosinophilic colloidal material and focal papillary differentiation by light microscopy. Positive for PAX2, CK-7, CK-20, CAM 5.2 and vimentin. Negative for CD-10, CD-117, TTF-1, and thyroglobulin FISH showed chromosomal losses of 1, 3, 7, 9p21, 12, 17, and X This is an uncommon variant
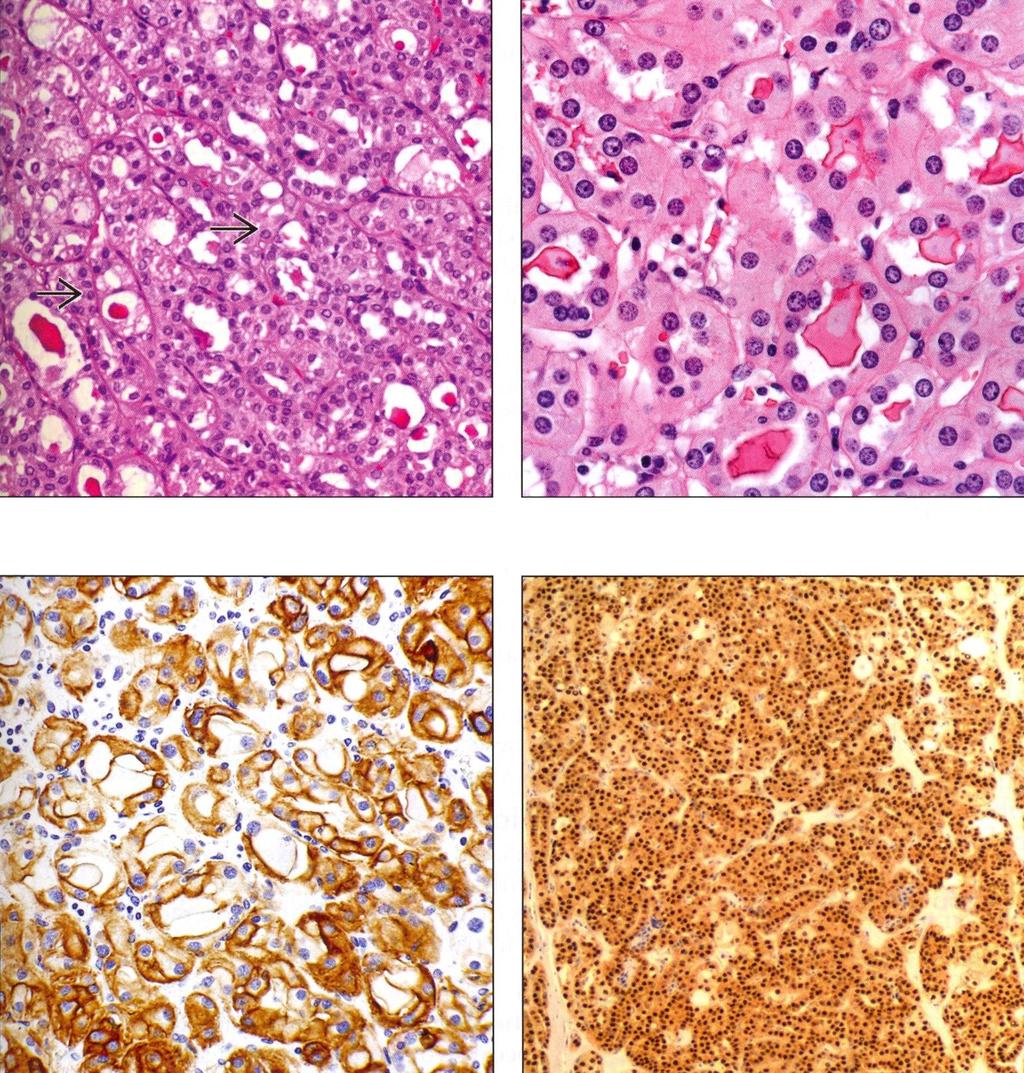
90 CK PAX2

91 Acquired cystic disease associated RCC Most common subtype of RCC in endstage kidneys, especially with acquired cystic disease Incidence of cystic disease (>90% at 10 years or more) RCC: 3-7% in patients with end-stage kidneys Micro: tumor cells with eosinophilic cytoplasm, sieve-like/cribriform appearance and oxalate crystals Clear cell papillary, papillary, clear cell, chromophobe RCC may occur (AMACR+, CD10, RCCm +: CK7- or focal +)
92
93

94 AMACR CK7 focal +

95 AMACR CK7-
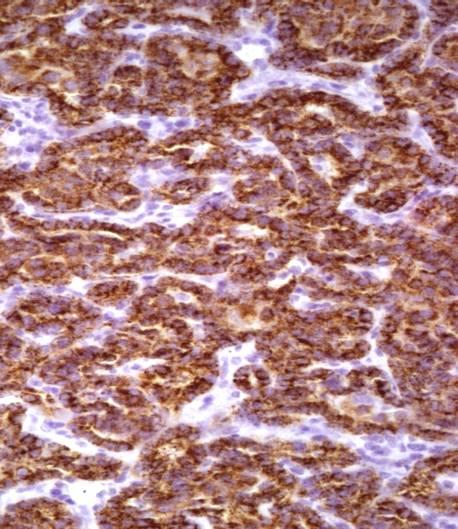
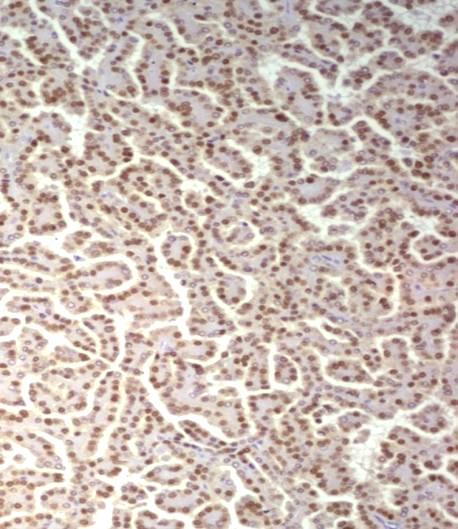
96 Clear cell papillary RCC Both end stage renal disease and also seen in non-endstage setting Unicentric and occasionally multicentric Most are small pt1 with rare pt3 No LN or other sites metastasis Clear cells with low NG; papillary/tubular-acinar; nuclei in linear arrangement away from basal aspect of cells AMACR, RCCM & CD10-; PAX8, CK7, CA9 and HMCK + Cytogenetically, no -3p, no +7, +17
97
98

99 CK7 + in both papillary and tubular areas
100
101
102
103
104
105
106
107
108
109

110 No VHL mutation No HMB45
111
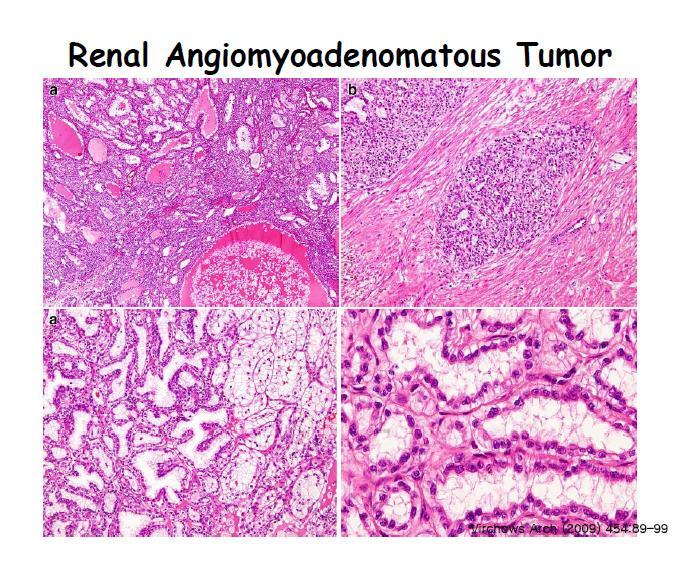
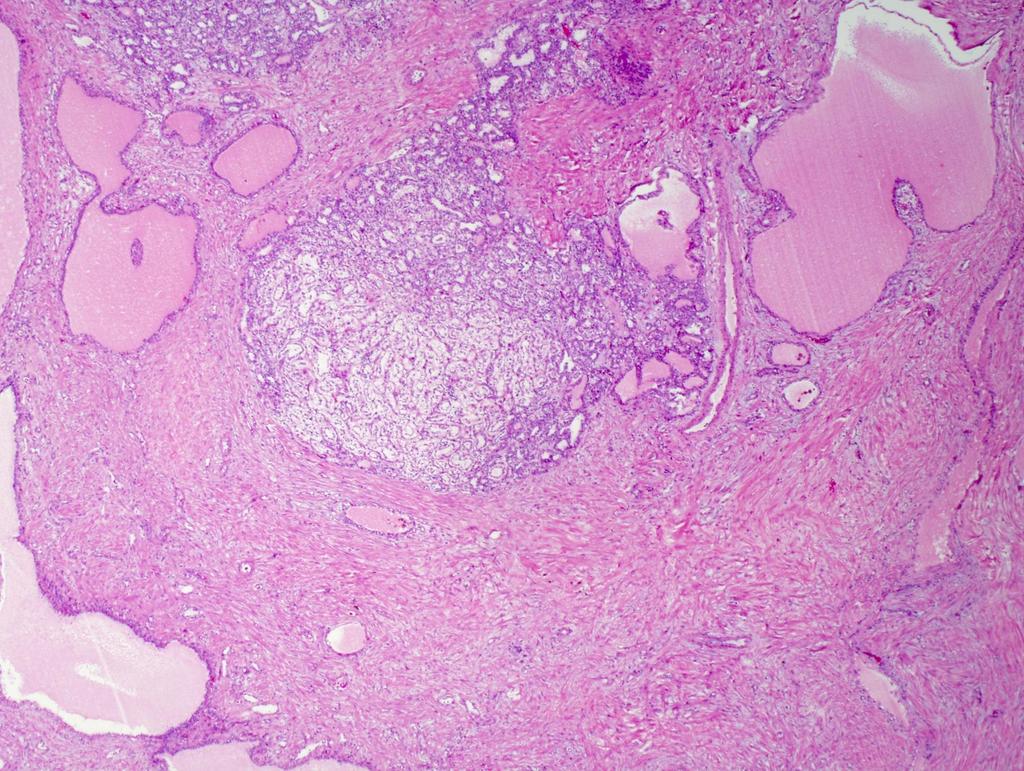
112 ---this neoplasm appears to have both epithelial and mesenchymal components. The epithelial portion has some tubular and solid areas compatible with low grade clear cell RCC and the mesenchymal component reminds me of angiomyoliopma Is it a renal angioadenomyomatous tumor?
113
114 3 Benign

115 Metanephric Adenoma
116 Metanephric Adenoma
117
118
119
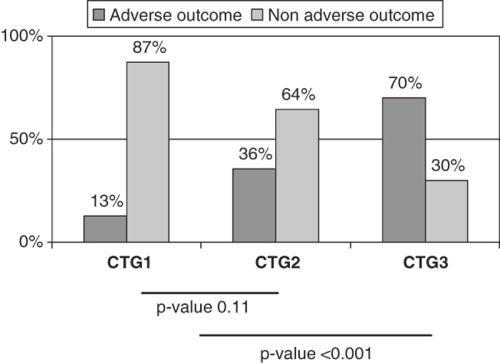
120 Morphologic Overlapping Metanephric Adenoma (MA) and Papillary RCC Papillary Pattern Glomeruloid Pattern Solid Pattern Psammoma Bodies Macrophages MA 6/8 (75%) 4/8 (50%) 8/8 (100%) 6/8 (75%) 1/8 (13%) PRCC 11/11 (100%) 4/11 (36%) 7/11 (64%) 1/11 (9%) 7/11 (64%) Moore B. Dance et al CAP Poster

121 Papillary RCC Metanephric Adenoma
122 Metanephric Adenoma vs. Papillary RCC RCCm AMACR WT-1 PAX2 0% 0% 100% 100% MA 90% 100% 0% 73% prcc Moore B. Dance et al CAP Poster
123 Papillary Adenoma Baby (<0.5 cm) low grade papillary RCC Incidental findings Often associated with end stage renal D Associated with papillary RCC Frequently multiple

124 Papillary Adenoma

125 Papillary Adenoma
126
127

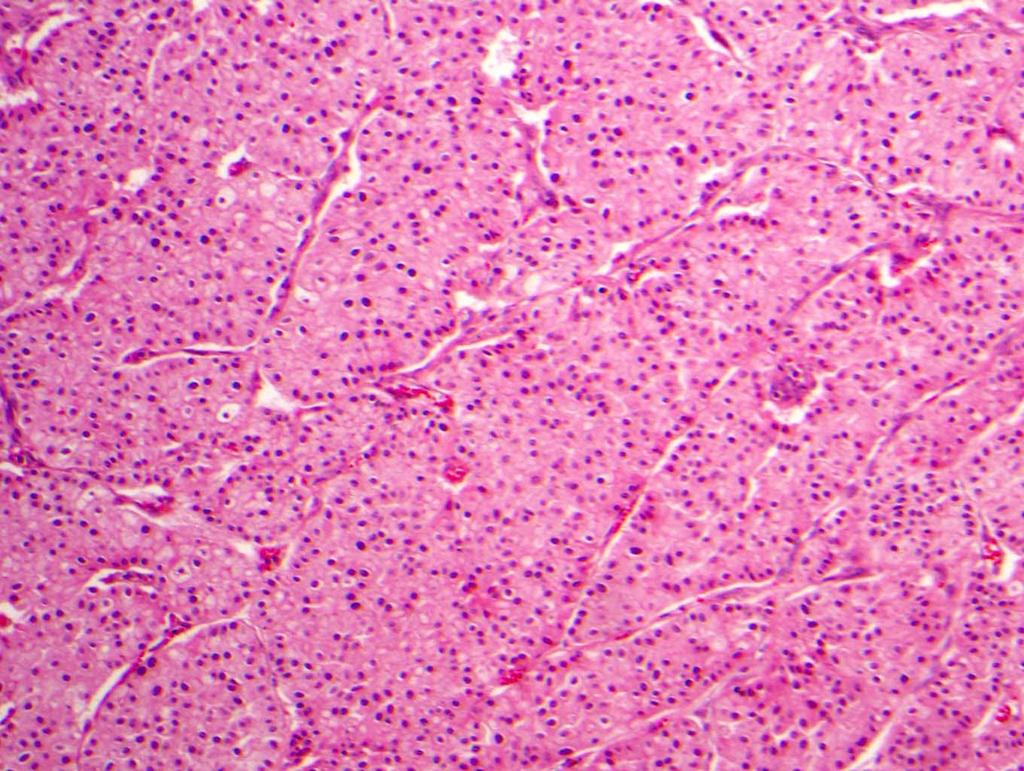
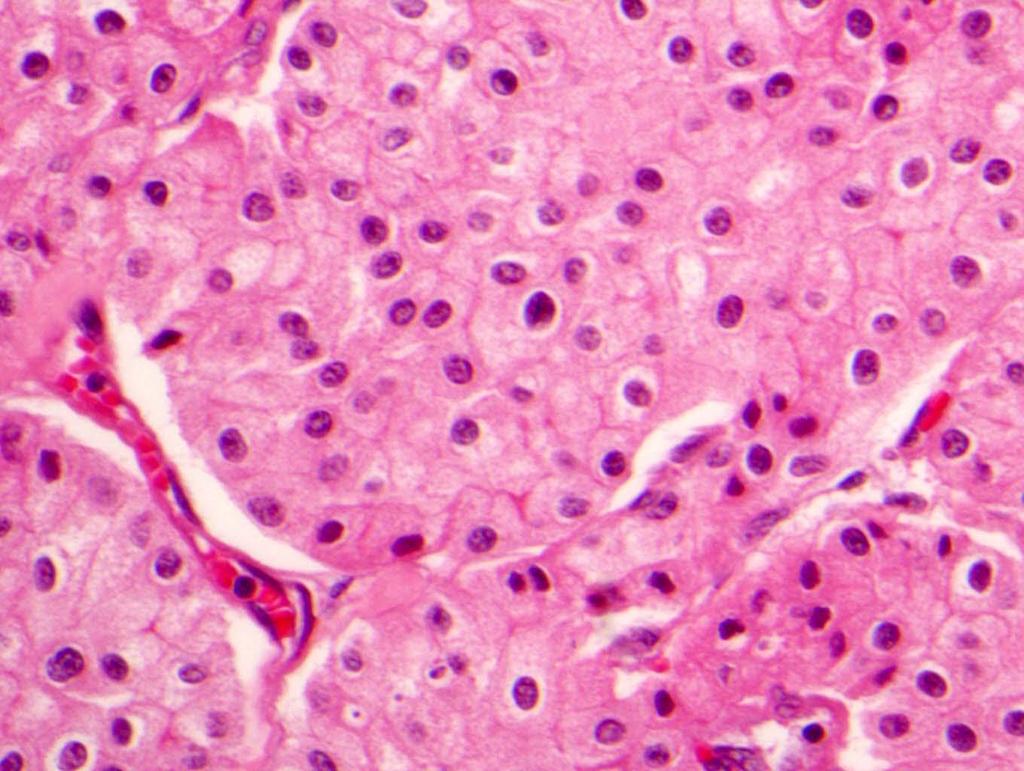
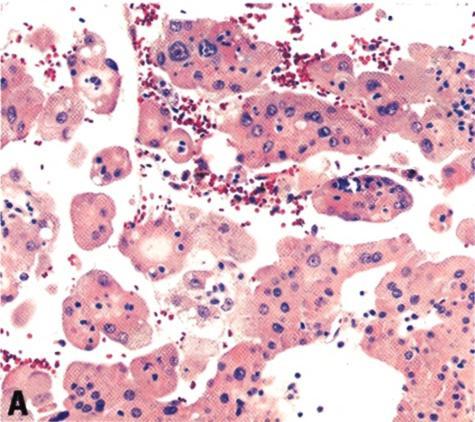
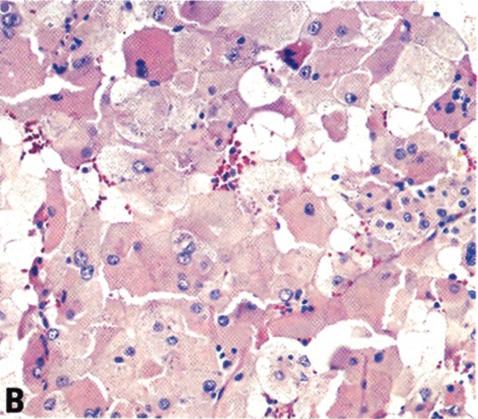
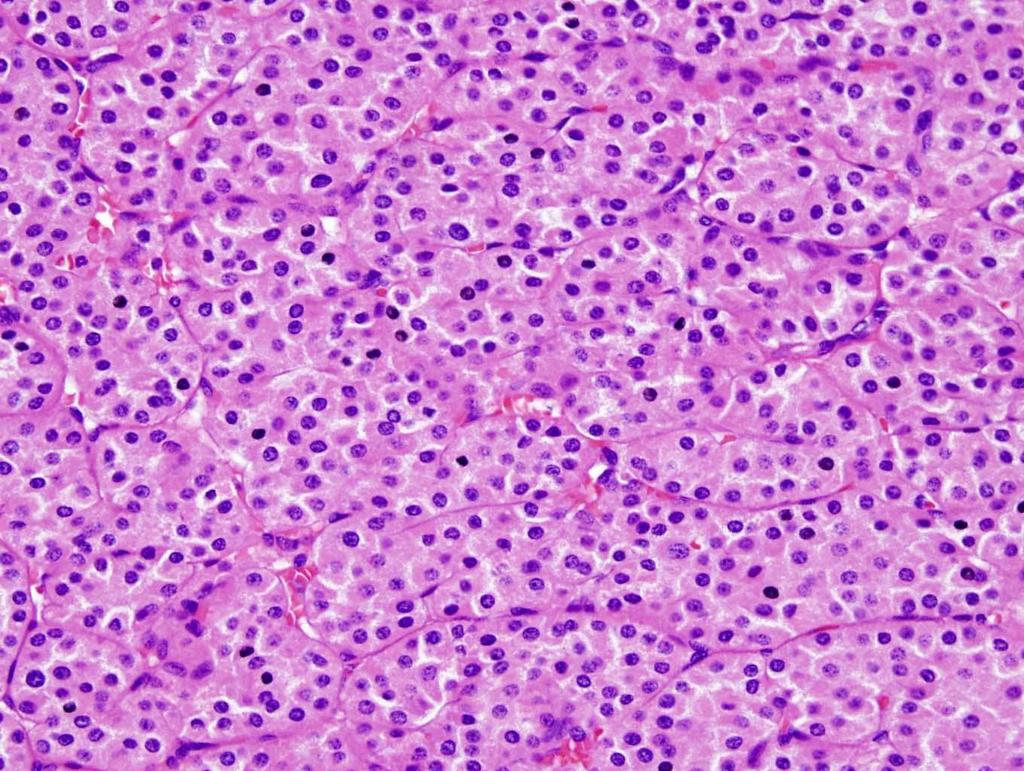
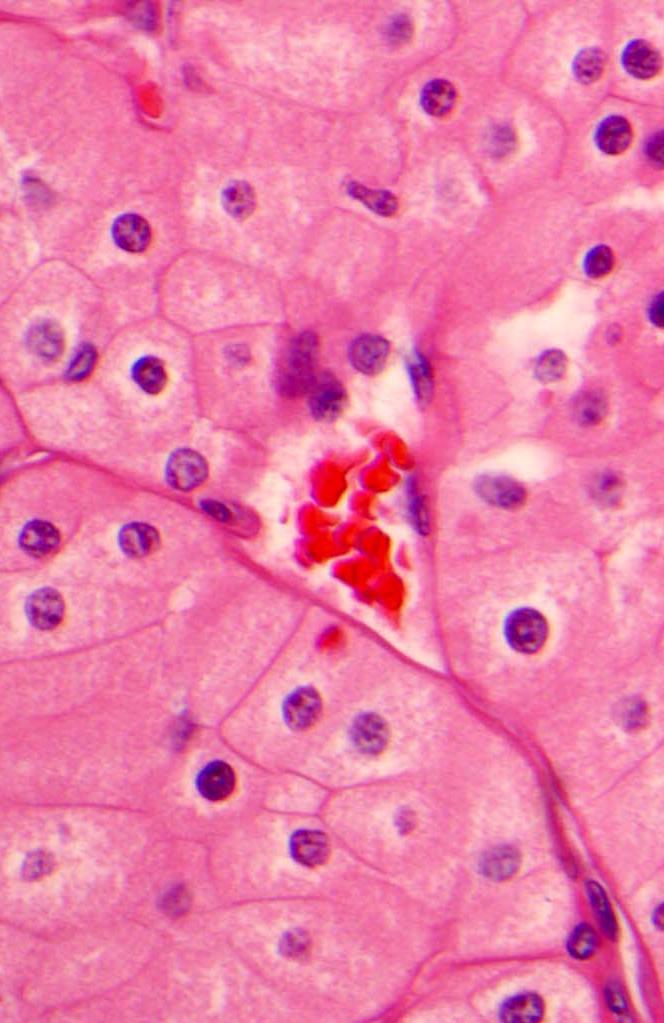
128 Oncocytoma Most frequent benign renal neoplasm Benign behavior Cytogenetic: normal or losses of -1, -Y Close relation with chromophobe RCC

129
130
131
132
133
134
135
136
137
138 Oncocytoma: Atypical Features Focal nuclear atypia (~10%) Hemorrhage Fat invasion (rare) Vascular invasion (rare) Large size
139
140
141

142 2 Entities no longer exist
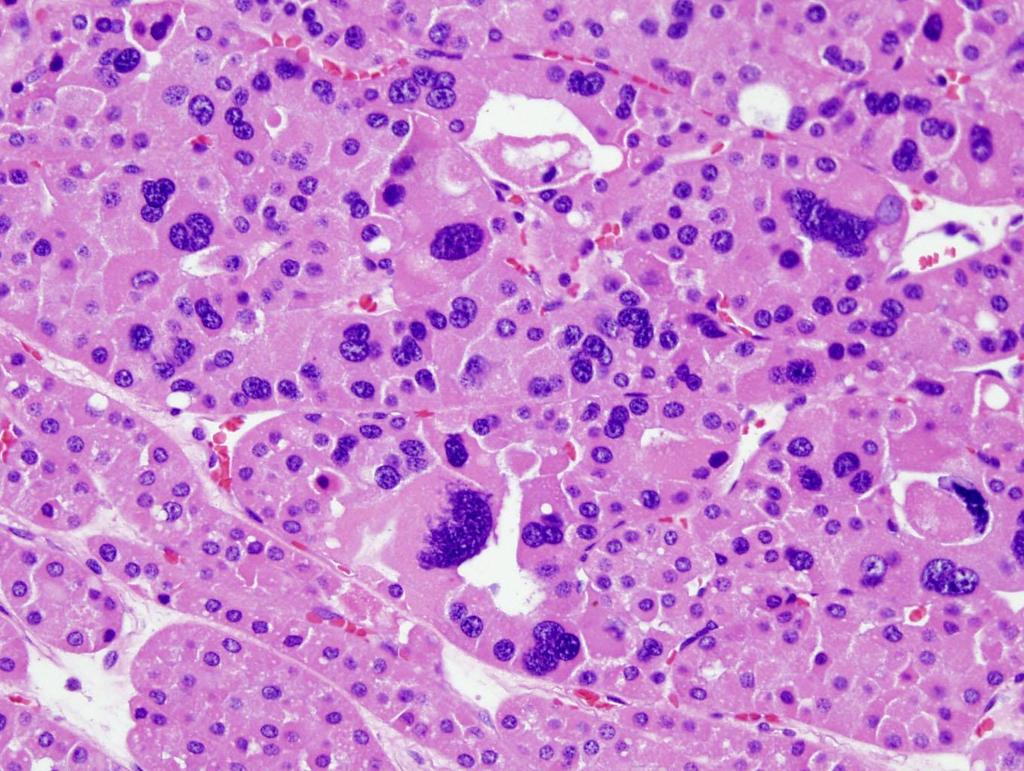
143 Granular RCC
144 Granular Cell RCC Granular cell RCC is not a specific entity Differential diagnoses include: Clear cell RCC Chromophobe RCC, eosinophilic variant Papillary RCC type 2 Oncocytoma Epithelioid angiomyolipoma
145 Clear Cell RCC with Granular Cells Very common Granular cell in clear cell RCC often have higher nuclear grade Keys to the diagnosis of clear cell RCC Component of classic clear cell Typical vascular pattern Exclude other histologic types
146 Clear Cell RCC with Granular Cells All clear cells 12.3% Mixed clear /granular cell 67.1% All granular cell 20.6% Data modified from Victor Reuter s USCAP Long Course 2008
147 Issues of Granular RCC Chromophobe RCC Oncocytoma Angiomyolipoma Clear cell RCC
148 Granular RCC Not a specific entity Think about clear cell RCC first Be familiar with chromophobe RCC Keep angiomyolipoma in mind
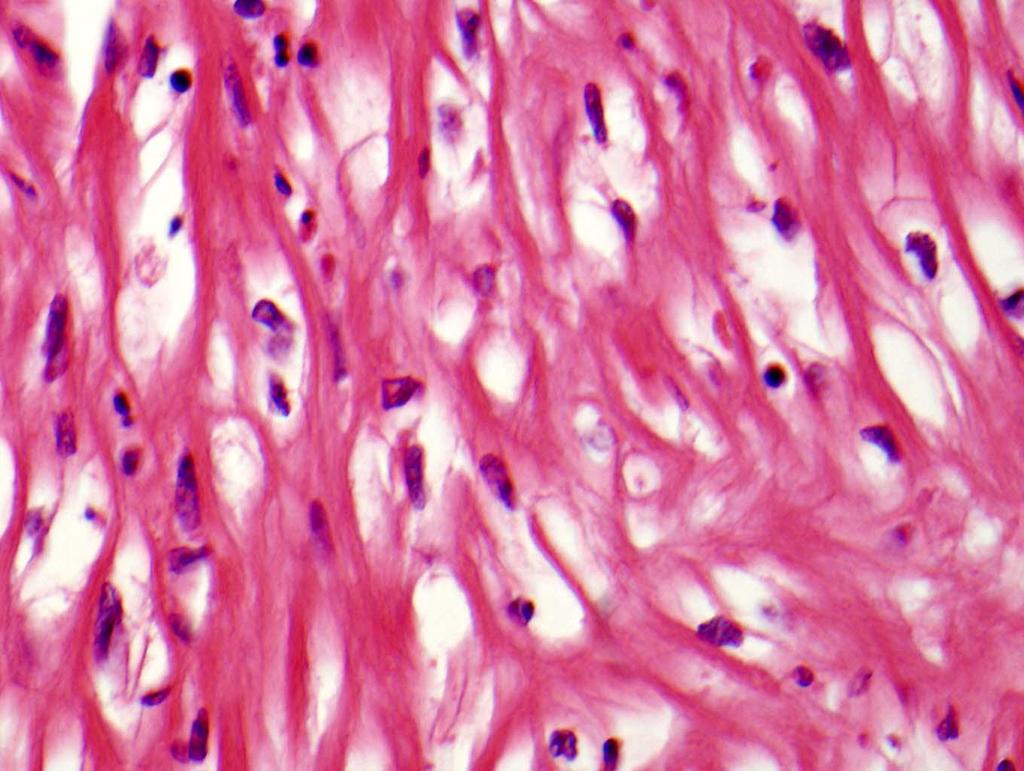
149 Sarcomatoid RCC
 Chromophobe 60 1 (1.7) Collecting duct 6 4 (66.")
150 Sarcomatoid Changes Occur in All Types of RCC # Cases # Sarcomatoid (%) Clear cell (5.4) Papillary (4.5) Chromophobe 60 1 (1.7) Collecting duct 6 4 (66.7) Unclassified 15 6 (40) Total (6) (TMH Unpublished Data)
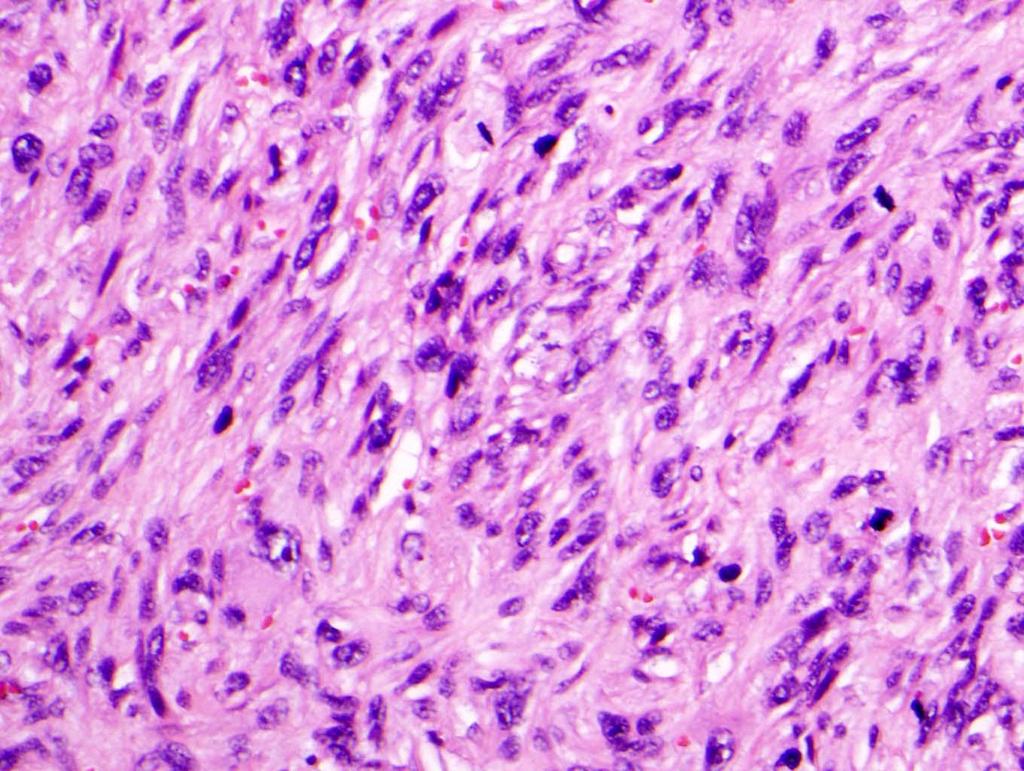
151 Sarcomatoid Changes Spindle cell area with at least moderate cytologic atypia Report the percentages of sarcomatoid and tumor necrosis Attempt to identified RCC histologic type



152 Sampling is important
153
154
155 Is this sarcomatoid?
156 Is this sarcomatoid?
157 Is this sarcomatoid??
158 1 RCC Staging
159 TNM Stage of RCC, 2010 T1 T1a T2 T3 T3a T3b T3c T4 < 7 cm, limited to kidney < 4 cm and T1b > 4 cm > 7 cm, limited to kidney T2a >7- <10 and T2b >10cm invades major veins, perinephric fat, but not beyond Gerota s fascia renal vein, perirenal, renal sinus fat vena cava below diaphragm above diaphragm, invades vena cava wall invades beyond Gerota s fascia, ipsilateral adrenal involvement
160 T stage 1978 AJCC 1987 AJCC 1997 AJCC 2002 AJCC 2009 AJCC pt1 RCC Staging an Evolving Topic pt1a Small tumor <2.5 cm <4 cm pt1b 2.5 to 7 cm 4 to 7 cm pt2 >7 cm >7 cm >7 cm pt2a pt2b pt3 Large tumor 7-10 cm >10 cm pt3a Perirenal/adrenal gland extension pt3b Perirenal spread RV involved RV/VC below diaphragm pt3c VC below diaphragm VC above diaphragm RV inv./ renal fat ext. VC below diaphragm VC above diaphragm or VC wall invasion pt4 pt4a pt4b Adjacent organ or abdominal wall Beyond Gerota s fascia VC above the diaph. Ext. beyond Gerota s fascia Beyond Gerota s fascia and/or ipsilateral adrenal
161 T stage 1978 AJCC 1987 AJCC 1997 AJCC 2002 AJCC 2009 AJCC pt1 RCC Staging an Evolving Topic pt1a Small tumor <2.5 cm <4 cm pt1b 2.5 to 7 cm 4 to 7 cm pt2 >7 cm >7 cm >7 cm pt2a pt2b pt3 Large tumor 7-10 cm >10 cm pt3a Perirenal/adrenal gland extension pt3b Perirenal spread RV involved RV/VC below diaphragm pt3c VC below diaphragm VC above diaphragm RV inv./ renal fat ext. VC below diaphragm VC above diaphragm or VC wall invasion pt4 pt4a pt4b Adjacent organ or abdominal wall Beyond Gerota s fascia VC above the diaph. Ext. beyond Gerota s fascia Beyond Gerota s fascia and/or ipsilateral adrenal
162 T stage 1978 AJCC 1987 AJCC 1997 AJCC 2002 AJCC 2009 AJCC pt1 RCC Staging an Evolving Topic pt1a Small tumor <2.5 cm <4 cm pt1b 2.5 to 7 cm 4 to 7 cm pt2 >7 cm >7 cm >7 cm pt2a pt2b pt3 Large tumor 7-10 cm >10 cm Perirenal/adrenal gland extension pt3a pt3b Perirenal spread RV involved RV/VC below diaphragm pt3c pt4 pt4a pt4b Adjacent organ or abdominal wall VC below diaphragm Beyond Gerota s fascia VC above the diaph. VC above diaphragm Ext. beyond Gerota s fascia RV inv./ renal fat ext. VC below diaphragm VC above diaphragm or VC wall invasion Beyond Gerota s fascia and/or ipsilateral adrenal
163 T stage 1978 AJCC 1987 AJCC 1997 AJCC 2002 AJCC 2009 AJCC pt1 RCC Staging an Evolving Topic pt1a Small tumor <2.5 cm <4 cm pt1b 2.5 to 7 cm 4 to 7 cm pt2 >7 cm >7 cm >7 cm pt2a pt2b pt3 Large tumor 7-10 cm >10 cm pt3a Perirenal spread Perirenal/adrenal gland extension pt3b RV involved RV/VC below diaphragm pt3c VC below diaphragm VC above diaphragm RV inv./ renal fat ext. VC below diaphragm VC above diaphragm or VC wall invasion pt4 pt4a pt4b Adjacent organ or abdominal wall Beyond Gerota s fascia VC above the diaph. Ext. beyond Gerota s fascia Beyond Gerota s fascia and/or ipsilateral adrenal
164 Tumor size T2 tumors T3a tumors RCC Staging Issues Perirenal fat invasion Sinus fat invasion Vascular invasion
 Multiple tumors Cut-off criteria for staging T1a vs.")
165 Size Matters Largest dimension (3 dimension?) Multiple tumors Cut-off criteria for staging T1a vs. T1b (4 cm T1 substage) T2 (>10 cm substage, th AJCC)
166 T2 Tumors Are Uncommon T Stage # Cases % T % T % T % T4 18 2% Total % Form TMH RCC database ( )
167 Fat Invasion and Staging Perirenal fat invasion Sinus fat invasion Extent of fat invasion

168 Renal Sinus Fat Invasion pt3a : directly invades perinephric tissue including sinus fat, direct adrenal invasion (Bonsib et al. AJSP 2000)
169 Renal Sinus vs. Perirenal Fat Invasion Worse 5 yr survival Perirenal fat inv. 51% Sinus fat inv. 26% No difference SF = Sinus fat inv. PF = Perirenal fat inv. (n=70) (n=96) (n=199) Thompson RH et al. J of Urol 2005 Margulis V. et al. J of Urol 2007


170 Extent of perirenal fat invasion (focal vs. extensive) Jung SJ, Ro JY, Truong LD, Ayala AG, and Shen SS. Human Pathol :
171 Extent of Perirenal Fat Invasion Jung SJ, Ro JY, Truong LD, Ayala AG, and Shen SS. Human Pathol :
172 Adrenal Invasion Direct adrenal invasion : pt3a (AJCC, 2002) T4 in th AJCC staging More aggressive behavior than fat invasion (Han et al. J Urol 2003)
173 Adrenal Invasion Group 2-year 5-year Log Rank 1 (n=118) 80% 63% Vs. 2 p< (n=66) 55% 32% Vs. 3 p= (n=14) 31% 21% Vs. 1 p=0.001 Fat inv. Renal vein inv. Adrenal inv. Jung SJ, Ro JY, Truong LD, Ayala AG, and Shen SS. Human Pathol :1689
174 Renal Vein Invasion Combine renal vein invasion with Perirenal fat invasion as T3a (2010)

175 K-M Survival analysis of pt2/pt3 RCC T2 Fat Inv. Groups p value T2 vs Fat Inv Fat vs RV Inv Renal Vein Inv.
176 Grading
177 Fuhrman s Nuclear Grade Nucleolus visible with 10x objectiveyes No G1 or G2 G3 or G4 Nucleolus visible with 40x objective or visible chromatin detains No G1 (Nucleus 10µm) Yes G2 (Nucleus 15µm) Pleomorphis m No Yes G3 G4 (Same nuclear size 20µm)
 G1 (n=73) G3 (n=213) G4 (n=56)")
178 Nuclear Grade and Prognosis (n=721) G2 (n=379) G1 (n=73) G3 (n=213) G4 (n=56)

179 40x Grade 1 40x Grade 2 40x Grade 3 40x Grade 4
180 Fuhrman s Nuclear Grade Two distinct nuclear grades in RCC are not uncommon finding Grading is based on the worst area Take adequate sections of tumor Used for all RCCs Value for chromophobe not clear, most of them are grade 2-3
181 Nucleolar Grade In papillary RCC Only nucleolus change Not considered these factors Nuclear size Nuclear shape
182 Sika-Paotonu, Delahunt, et al AJSP. 2006;30:1091-6
183 Chromophobe RCC, Grade No effective grade for ChRCC Delahunt et al (AJSP 2007:31;957-60) is based on assessment of nuclear crowding & anaplasia: 3-tier (Paner and Amin 2010:34; )

184 Gr 1 Gr 2 Gr 3
185
186 Chromophobe RCC, Grade Univariate associations with CS survival included 2010 TNM stage, sarcomatoid differentiation, coagulative tumor necrosis, chromophobe RCC grade, and nucleolar grade (all P<0.001). (Not FN grade) Nonsarcomatoid TNM stage groupings I and II chromophobe RCC, only stage grouping (I vs. II) was significantly associated with CS survival (P=0.03). Cheville et al AJCP 2012 Feb 24. [Epub ahead of print]
187

188 Ancillary Tests
189 USE of IHC DDX of renal vs. non-renal neoplasms
190 USE of IHC DDX of renal vs. non-renal neoplasms Histologic subtyping of renal cell carcinoma
191 IHC of RCC Clear Cell RCC +: Vimentin, AE1/AE3, CD10, RCCM, PAX2, PAX8, CAIX - : HMWCK, CK7, CK20, CD117, Ksp-cadherin, Parvalbumin Papillary RCC and MTSCC +: Vimentin, AE1/AE3, CK7, AMACR, RCCM, PAX2 and PAX8 - : CD117, Ksp-cadherin, and Parvalbumin. Chromophobe RCC/Oncocytoma +: E-cadherin, Ksp-cadherin, Parvalbumin, CD117, AE1/AE3, CK7 strong/diffuse for chromphobe RCC - : Vim, CK7 (or weak for oncocytoma), CAIX, and AMACR
192 IHC of RCC Collecting Duct Carcinoma +: p63, HMWCK; Some + for PAX2 and PAX8 - : RCCM, CD10, CD117, KSP, and Parvalbumin Xp11.2 Translocation Carcinoma +: CD10, RCCM, TFE3, PAX2 or 8, and Cathepsin-K - : CK (usually or weak) Clear Cell Papillary RCC +: CK7, PAX2 and PAX8 - : AMACR, RCCM, CD10

193 Vim RCC Marker AMACR
194 USE of IHC DDX of renal vs. non-renal neoplasms Histologic subtyping of renal cell carcinoma Diagnosis of rare primary renal neoplasm
195 USE of IHC DDX of renal vs. non-renal neoplasms Histologic subtyping of renal cell carcinoma Diagnosis of rare primary renal neoplasm Diagnosis of core biopsy of renal tumor
196 USE of IHC DDX of renal vs. non-renal neoplasms Histologic subtyping of RCC Diagnosis of rare primary renal neoplasm Diagnosis of core biopsy of renal tumor Diagnosis of metastatic RCC
197 Renal tumors with clear/light-staining cytoplasm Antibody Clear Cell RCC Chromophobe RCC MITF/TFE Family XP11.2 Carcinoma Clear Cell Papillary RCC Epithelioid Angiomyolipoma CK7 - + (diffuse, occasionally patchy) - + (diffuse, almost 100% tumor cells) CD10 + (membranous) -/(rarely +) + (but often in TFEB carcinoma) - - Vimentin + -/(rarely +) -/+ + + Ksp-cadherin No Data - CD (diffuse, often peripheral membranous accentuation - No Data - AMACR - (rarely focal +) - + (usually) - - EMA/MUC (rarely focal +) + - PAN-CK(AE1/AE3) (rarely focal +) + - CAIX + (diffuse membranous) - (+ perinecrotic areas) - (+ in some cases) + (diffuse membranous) TFE3/TFEB Parvalbumin Melan-A(MART-1) in TFEB carcinoma, rarely + in TFE3 HMB in TFEB carcinoma, rarely + in TFE3 MiTF in TFEB carcinoma, rarely + in TFE Actin-sm /- - -
198 Renal tumors with papillary or Tubulopapillary Architecture Antibody Papillary RCC Collecting Duct Carcinoma Metanephric Adenoma CK (may be + in branching tubules or papillary structures) CD10 + (often luminal pattern) Mucinous Tubular and Spindle Cell Carcinoma /+ (focal) - RCC Variable -/+ AMACR + - -/+ + - EMA/MUC (may be + in branching tubules or papillary structures) + + WT HMCK(34 E12) - +/- - -/+ + Clear Cell Papillary RCC CD57 - No Data + - No Data INI1 + + (lost in renal medullary carcinoma) Ulex No Data CAIX - (+ perinecrotic areas and papillary tips) -/+ (perinecrotic area) No Data No Data +
199 Antibody Renal tumors with Granular/Eosinophilic Cytoplasm Clear Cell RCC, Eosinophilic Chromophobe RCC, Eosinophilic Oncocytoma MiTF/TFE Family Translocationassociated Carcinoma Vimentin +/- - (rarely +) - -/+ + CD Pax (rarely +) + Variable - RCC + -/+ -/+ + - CK7 - +/ Epithelioid Angiomyolipoma CD10 + -/+ + + in TFE3 carcinoma, often (-) in TFEB - K 네 -cadherin Variable - Parvalbumin No Data - EpCAM/BER-EP4 Variable + - (occasionally focal or patchy +) Variable - TFE3/TFEB Melan-A(MART-1) in TFEB carcinoma, rarely + in TFE3 HMB in TFEB carcinoma, rarely + in TFE3 MiTF in TFEB carcinoma, rarely + in TFE Actin-sm /- HMCK(34 E12) - - (rarely focal +) - - (occasionally focal +) - EMA/MUC1 + + (occasionally only focal +) + (occasionally only focal +) - (occasionally focal +) - CAIX (+ in some cases) -
200 Renal tumors with Spindle Cell Morphology Antibody PAN- CK(AE1/AE3) Spindle Cells in Sarcomatoid RCC Mucinous Tubular and Spindle Cell Carcinoma Sarcoma + (may be focal/rare cells) + - (may be focal + in leiomyosarcoma) Cam5.2 + (may be focal/rare cells) + - (may be focal + in leiomyosarcoma) EMA/MUC1 + (may be focal/rare cells) + - (may be focal + in leiomyosarcoma) Desmin - (may occasionally be +) - + in myosarcomas, occasionally in others Actin-sm - (may occasionally be +) - + in myosarcomas, occasionally in others CD in synovial sarcoma Variable S Variable Variable Melan-A(MART-1) HMB MiTF HMCK(34 E12) -/(rarely focal +) -/+ - - CK7 -/(rarely focal +) CAIX + (usually) - - (+ in perinecrotic areas) - Angiomyolipoma
201 Poorly Differentiated Carcinomas Antibody RCC, Unclassified Collecting Duct Carcinoma CK7 -/+ + + CK (rarely focal +) +/- P HMCK(34 E12) -/+ +/- + Thrombomodulin - - +/- RCC +/- - - Uroplakin /- Vimentin +/- + -/+ CD10 +/- - -/+ CK5/ /- CK /- INI1 + + (loss in medullary) + Ulex /+ Urothelial Carcinoma
202 Small Blue Round Cell Tumors of Kidney Antibody Wilms Tumor Ewing Sarcoma/ PNET Small Cell Carcinoma Lymphoma Desmoplastic Small Round Cell Tumor Synovial Sarcoma, Poorly Differentiated Vimentin /- + + WT S Variable -/+ FLI CD99 +/- + -/+ +/- -/+ -/+ NSE - +/- -/+ - + No Data HMCK(34 E12) - -/+ + (often dot-like) - - -/+ EMA/MUC1 -/+ - -/ /+ CD45(LCA) Chromogranin - - +/- - -/+ - Desmin Pax-2 + No Data No Data No Data No Data No Data PAN- CK(AE1/AE3) + (in tubules) +/- (focal) + (often dot-like) - + -/+
203 Contents 5: 5 types of malignant tumors 4: 4 +4 newly defined entities 3: 3 benign tumors 2: 2 entities no longer exist 1: 1 (+1) most important prognostic factor
204 Take Home Messages Do your BeST! Basic (effort) Study Think Enjoy Pathology of Renal Neoplasms


205 Thank you for your attention!
Unknown Slides Conference
 Unknown Slides Conference Jae Y. Ro, MD, PhD Weill Medical College of Cornell Univ. The Methodist Hospital, and UT MD Anderson Cancer Center Houston, TX November 9, 2013 Amman, Jordan 25 th Congress of
Unknown Slides Conference Jae Y. Ro, MD, PhD Weill Medical College of Cornell Univ. The Methodist Hospital, and UT MD Anderson Cancer Center Houston, TX November 9, 2013 Amman, Jordan 25 th Congress of
IMMUNOPROFILES OF THE MAJOR RENAL NEOPLASMS (%staining)
") Stain Clear Cell Papillary IMMUNOPROFILES OF THE MAJOR RENAL NEOPLASMS (%staining) Chromophobe Collecting Duct Carcinom a Sarcomatoid Xp11 Translocat ion Dr Jon Oxley See also www.jonoxley.com Page 1 MTSCC
Stain Clear Cell Papillary IMMUNOPROFILES OF THE MAJOR RENAL NEOPLASMS (%staining) Chromophobe Collecting Duct Carcinom a Sarcomatoid Xp11 Translocat ion Dr Jon Oxley See also www.jonoxley.com Page 1 MTSCC
Renal tumours: use of immunohistochemistry & molecular pathology. Dr Lisa Browning John Radcliffe Hospital Oxford
 Renal tumours: use of immunohistochemistry & molecular pathology Dr Lisa Browning John Radcliffe Hospital Oxford Renal tumours: the use of immunohistochemistry & molecular pathology Classification of RCC
Renal tumours: use of immunohistochemistry & molecular pathology Dr Lisa Browning John Radcliffe Hospital Oxford Renal tumours: the use of immunohistochemistry & molecular pathology Classification of RCC
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
Various hereditary, acquired and neoplastic conditions can lead to cyst formation in the kidney.
 Dr. Fatima AlAl-Hashimi Hashimi,, MD, FRCPath Salmaniya Medical Complex, Bahrain Various hereditary, acquired and neoplastic conditions can lead to cyst formation in the kidney. The most frequently encountered
Dr. Fatima AlAl-Hashimi Hashimi,, MD, FRCPath Salmaniya Medical Complex, Bahrain Various hereditary, acquired and neoplastic conditions can lead to cyst formation in the kidney. The most frequently encountered
Diagnostic accuracy of percutaneous renal tumor biopsy May 10 th 2018
 Diagnostic accuracy of percutaneous renal tumor biopsy May 10 th 2018 Dr. Tzahi Neuman Dep.Of Pathology Hadassah Medical Center Jerusalem, Israel, (tneuman@hadassah.org.il) Disclosure: 1 no conflicts of
Diagnostic accuracy of percutaneous renal tumor biopsy May 10 th 2018 Dr. Tzahi Neuman Dep.Of Pathology Hadassah Medical Center Jerusalem, Israel, (tneuman@hadassah.org.il) Disclosure: 1 no conflicts of
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Biopsy diagnosis of renal tumors. Current applications Ondřej Hes Department of Pathology Charles University and University Hospital Plzeň Czech Republic Dealing
Enterprise Interest Nothing to declare Biopsy diagnosis of renal tumors. Current applications Ondřej Hes Department of Pathology Charles University and University Hospital Plzeň Czech Republic Dealing
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
04/10/2018. What s new in renal tumor pathology what s important and why. Prognostic factors in RCC
 25th Annual Seminar in Pathology Pittsburgh, PA, April 26-29, 2018 What s new in renal tumor pathology what s important and why Kiril Trpkov, MD FRCPC Department of Pathology and Laboratory Medicine kiril.trpkov@cls.ab.ca
25th Annual Seminar in Pathology Pittsburgh, PA, April 26-29, 2018 What s new in renal tumor pathology what s important and why Kiril Trpkov, MD FRCPC Department of Pathology and Laboratory Medicine kiril.trpkov@cls.ab.ca
RENAL NEOPLASMS: NEW ENTITIES & DIFFICULT DIAGNOSES
 RENAL NEOPLASMS: NEW ENTITIES & DIFFICULT DIAGNOSES Cristina Magi-Galluzzi, MD, PhD Professor of Pathology Director of Anatomic Pathology Kidney Tumors American Cancer Society Cancer Facts and Figures
RENAL NEOPLASMS: NEW ENTITIES & DIFFICULT DIAGNOSES Cristina Magi-Galluzzi, MD, PhD Professor of Pathology Director of Anatomic Pathology Kidney Tumors American Cancer Society Cancer Facts and Figures
RENAL EPITHELIAL NEOPLASMS: IS THERE A ROLE OF IMMUNOSTAINS IN DIAGNOSIS?
 RENAL EPITHELIAL NEOPLASMS: IS THERE A ROLE OF IMMUNOSTAINS IN DIAGNOSIS? John C. Cheville, M.D. Mayo Clinic and Mayo Foundation Rochester, MN The majority of renal epithelial neoplasms are diagnosed on
RENAL EPITHELIAL NEOPLASMS: IS THERE A ROLE OF IMMUNOSTAINS IN DIAGNOSIS? John C. Cheville, M.D. Mayo Clinic and Mayo Foundation Rochester, MN The majority of renal epithelial neoplasms are diagnosed on
ACCME/Disclosures. M31078/07 Ondřej Hes 4/13/2016
 M31078/07 Ondřej Hes Department of Pathology Charles University and University Hospital Plzeň Bioptická laboratoř Plzeň Czech Republic ACCME/Disclosures The USCAP requires that anyone in a position to
M31078/07 Ondřej Hes Department of Pathology Charles University and University Hospital Plzeň Bioptická laboratoř Plzeň Czech Republic ACCME/Disclosures The USCAP requires that anyone in a position to
International Journal of Pharma and Bio Sciences CHROMOPHOBE VARIANT OF RENAL CELL CARCINOMA MASQUARDING AS RENAL ONCOCYTOMA ON CYTOLOGY.
 Case Report Pathology International Journal of Pharma and Bio Sciences ISSN 0975-6299 CHROMOPHOBE VARIANT OF RENAL CELL CARCINOMA MASQUARDING AS RENAL ONCOCYTOMA ON CYTOLOGY. DR.MAMATHA K*, DR. ARAKERI
Case Report Pathology International Journal of Pharma and Bio Sciences ISSN 0975-6299 CHROMOPHOBE VARIANT OF RENAL CELL CARCINOMA MASQUARDING AS RENAL ONCOCYTOMA ON CYTOLOGY. DR.MAMATHA K*, DR. ARAKERI
THE PATHOLOGY OF COMMON RENAL TUMORS. Victor E. Reuter, M.D Memorial Sloan Kettering Cancer Center
 THE PATHOLOGY OF COMMON RENAL TUMORS Victor E. Reuter, M.D Memorial Sloan Kettering Cancer Center A Practical Approach to Genitourinary Pathology Firenze, Italy May, 2016 Disclosures: none 1970 WHO classification:
THE PATHOLOGY OF COMMON RENAL TUMORS Victor E. Reuter, M.D Memorial Sloan Kettering Cancer Center A Practical Approach to Genitourinary Pathology Firenze, Italy May, 2016 Disclosures: none 1970 WHO classification:
Spectrum of Preneoplastic and Neoplastic Cystic Lesions of the Kidney in Adult. by dr. Banan Burhan Mohammed Lecturer in Pathology Department
 Spectrum of Preneoplastic and Neoplastic Cystic Lesions of the Kidney in Adult by dr. Banan Burhan Mohammed Lecturer in Pathology Department Various hereditary, acquired, and neoplastic conditions can
Spectrum of Preneoplastic and Neoplastic Cystic Lesions of the Kidney in Adult by dr. Banan Burhan Mohammed Lecturer in Pathology Department Various hereditary, acquired, and neoplastic conditions can
Pathology Mystery and Surprise
 Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Immunohistochemical Diagnosis of Renal Neoplasms. Luan D. Truong, MD; Steven S. Shen, MD, PhD
 Immunohistochemical Diagnosis of Renal Neoplasms Luan D. Truong, MD; Steven S. Shen, MD, PhD N Context. Histologic diagnosis of renal neoplasm is usually straightforward by routine light microscopy. However,
Immunohistochemical Diagnosis of Renal Neoplasms Luan D. Truong, MD; Steven S. Shen, MD, PhD N Context. Histologic diagnosis of renal neoplasm is usually straightforward by routine light microscopy. However,
the urinary system pathology Dr. Fairoz A Eltorgman
 the urinary system pathology Dr. Fairoz A Eltorgman Tumors of the renal pelvis & kidney Benign tumors of the renal pelvis: Hemangioma Leiomyoma Malignant tumors: Transitional cell carcinoma Squamous cell
the urinary system pathology Dr. Fairoz A Eltorgman Tumors of the renal pelvis & kidney Benign tumors of the renal pelvis: Hemangioma Leiomyoma Malignant tumors: Transitional cell carcinoma Squamous cell
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
6/5/2010. Renal vein invasion & Capsule Penetration (T3a) Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).
 Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).") GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Current insights in renal cell cancer pathology
 Urologic Oncology: Seminars and Original Investigations 26 (2008) 225 238 Review article Current insights in renal cell cancer pathology Vito Mancini, M.D. a, *, Michele Battaglia, M.D. a, Pasquale Ditonno,
Urologic Oncology: Seminars and Original Investigations 26 (2008) 225 238 Review article Current insights in renal cell cancer pathology Vito Mancini, M.D. a, *, Michele Battaglia, M.D. a, Pasquale Ditonno,
What s New in Pathology of Genitourinary Tumors. Jiaoti Huang, MD, PhD Department of Pathology Duke University School of Medicine
 What s New in Pathology of Genitourinary Tumors Jiaoti Huang, MD, PhD Department of Pathology Duke University School of Medicine Kidney Tumors Multilocular cystic renal neoplasm of low malignant potential
What s New in Pathology of Genitourinary Tumors Jiaoti Huang, MD, PhD Department of Pathology Duke University School of Medicine Kidney Tumors Multilocular cystic renal neoplasm of low malignant potential
RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a Pseud
 GENITOURINARY PATHOLOGY Kathleen M. O Toole Toole, M.D. RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a
GENITOURINARY PATHOLOGY Kathleen M. O Toole Toole, M.D. RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a
Prognostic factors of genitourinary tumors: Do we have to care?
 Prognostic factors of genitourinary tumors: Do we have to care? Jae Y. Ro, MD, PhD Professor and Director of Surgical Pathology The Methodist Hospital, Weill Medical College of Cornell University, Houston,
Prognostic factors of genitourinary tumors: Do we have to care? Jae Y. Ro, MD, PhD Professor and Director of Surgical Pathology The Methodist Hospital, Weill Medical College of Cornell University, Houston,
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Case 2. Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset
 Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
ACCME/Disclosures. Diagnosing Mesothelioma in Limited Tissue Samples. Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016
 Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain
 December 2016 59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain Contributed by: Divya Sharma, MD. Fellow, Gastrointestinal Pathology, Department of Pathology
December 2016 59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain Contributed by: Divya Sharma, MD. Fellow, Gastrointestinal Pathology, Department of Pathology
Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency
 Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency World Health Organization Available in Feb 2016 Frame work for reporting Major contributing
Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency World Health Organization Available in Feb 2016 Frame work for reporting Major contributing
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Renal cell carcinoma (RCC)
") Renal cell carcinoma (RCC) Introduction The most common solid renal tumor. Accounts for 2 3% of all adult malignancies. It is the 3 rd most common urological tumor in men and the 2 nd in women. It is th
Renal cell carcinoma (RCC) Introduction The most common solid renal tumor. Accounts for 2 3% of all adult malignancies. It is the 3 rd most common urological tumor in men and the 2 nd in women. It is th
Cutaneous metastases. Thaddeus Mully. University of California, San Francisco Professor, Departments of Pathology and Dermatology
 Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Mesothelioma: diagnostic challenges from a pathological perspective. Naseema Vorajee August 2016
 Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Disclosure of Relevant Financial Relationships
 Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
Tumors of kidney and urinary bladder
 Tumors of kidney and urinary bladder Overview of kidney tumors Benign and malignant Of the benign: papillary adenoma -cortical -small (0.5cm) -in 40% of population -clinically insignificant The most common
Tumors of kidney and urinary bladder Overview of kidney tumors Benign and malignant Of the benign: papillary adenoma -cortical -small (0.5cm) -in 40% of population -clinically insignificant The most common
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
CASE year old male with a PET avid nodule in the left adrenal gland
 CASE 1 55 year old male with a PET avid nodule in the left adrenal gland Case 1 Adrenal gland parenchyma partly replaced by a spindle cell tumour with mild nuclear pleomorphism Atypical mitoses present
CASE 1 55 year old male with a PET avid nodule in the left adrenal gland Case 1 Adrenal gland parenchyma partly replaced by a spindle cell tumour with mild nuclear pleomorphism Atypical mitoses present
Special slide seminar
 Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
NAACCR Webinar Series 1
 NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Kidney 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes 3 NAACCR 2009 2010 Webinar
NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Kidney 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes 3 NAACCR 2009 2010 Webinar
The Panel Approach to Diagnostics. Lauren Hopson International Product Specialist Cell Marque Corporation
 The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
Presenter: Yeh-Han Wang M.D.
 Korea-Taiwan-Japan Joint Meeting for Gynecological Pathology Mini-lecture Female Adnexal Tumor of Probable Wolffian Origin (FATWO) in Taiwan: A Small Case Series and Literature Review Presenter: Yeh-Han
Korea-Taiwan-Japan Joint Meeting for Gynecological Pathology Mini-lecture Female Adnexal Tumor of Probable Wolffian Origin (FATWO) in Taiwan: A Small Case Series and Literature Review Presenter: Yeh-Han
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
ACCME/Disclosures. Case History 4/13/2016. USCAP GU Specialty Conference Case 3. Ann Arbor, MI
 USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
Establishing a definitive pathologic diagnosis in surgical
 SPECIAL ARTICLE Best Practices in the Application of Immunohistochemistry in Urologic Pathology Report From the International Society of Urological Pathology Consensus Conference Mahul B. Amin, MD,* Jonathan
SPECIAL ARTICLE Best Practices in the Application of Immunohistochemistry in Urologic Pathology Report From the International Society of Urological Pathology Consensus Conference Mahul B. Amin, MD,* Jonathan
Kidney-specific cadherin, a specific marker for the distal portion of the nephron and related renal neoplasms
 & 2005 USCAP, Inc All rights reserved 0893-3952/05 $30.00 www.modernpathology.org Kidney-specific cadherin, a specific marker for the distal portion of the nephron and related renal neoplasms Steven S
& 2005 USCAP, Inc All rights reserved 0893-3952/05 $30.00 www.modernpathology.org Kidney-specific cadherin, a specific marker for the distal portion of the nephron and related renal neoplasms Steven S
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
Renal Masses in Patients with Known Extrarenal Primary Primary Cancer Primary Primary n Met Mets s RCC Beni L mphoma Lung Breast Others
 The Importance of Stuart G. Silverman, MD, FACR Professor of Radiology Harvard ard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston, MA The Importance of
The Importance of Stuart G. Silverman, MD, FACR Professor of Radiology Harvard ard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston, MA The Importance of
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04
 Presentation Outline Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 General Information
Presentation Outline Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 General Information
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04
 Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 1 Steven Peace, BS, CTR Susan Smith
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 1 Steven Peace, BS, CTR Susan Smith
Immunohistochemistry in Bone and Soft Tissue Tumors. Sahar Rassi Zankoul, MD
 Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22
 Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a Pseudocapsule
 GENITOURINARY PATHOLOGY Kathleen M. O Toole, M.D. Renal Cell Carcinoma 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow Necrotic Mass Grossly is a Bright
GENITOURINARY PATHOLOGY Kathleen M. O Toole, M.D. Renal Cell Carcinoma 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow Necrotic Mass Grossly is a Bright
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE. Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT
 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE AUTHORS : PROSTATE CHAPTER
2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE AUTHORS : PROSTATE CHAPTER
Pancreatic Cystic Lesions 원자력병원
 Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
Renal Neoplasia: Diagnostic Problems and Recently Recognized Entities
 Renal Neoplasia: Diagnostic Problems and Recently Recognized Entities John N. Eble, M.D. Department Pathology Indiana University, Indianapolis, IN Holger Moch, M.D. Department Pathology University Hospital
Renal Neoplasia: Diagnostic Problems and Recently Recognized Entities John N. Eble, M.D. Department Pathology Indiana University, Indianapolis, IN Holger Moch, M.D. Department Pathology University Hospital
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
Radical Nephrectomy for Renal Cell Carcinoma Its Contemporary Role Related to Histologic Type, Tumor Size, and Nodal Status: A Retrospective Study
 AJCP /ORIGINAL ARTICLE Radical Nephrectomy for Renal Cell Carcinoma Its Contemporary Role Related to Histologic Type, Tumor Size, and Nodal Status: A Retrospective Study Kamran M. Mirza, MD, PhD, Jerome
AJCP /ORIGINAL ARTICLE Radical Nephrectomy for Renal Cell Carcinoma Its Contemporary Role Related to Histologic Type, Tumor Size, and Nodal Status: A Retrospective Study Kamran M. Mirza, MD, PhD, Jerome
Updated Classification of Renal cell carcinoma
 Updated Classification of Renal cell carcinoma Suchin Worawichawong, M.D., FRCPath (Thailand) Department of Pathology, Ramathibodi Hospital, Mahidol University Incidence: Global: 338,000 new cases, 130,000
Updated Classification of Renal cell carcinoma Suchin Worawichawong, M.D., FRCPath (Thailand) Department of Pathology, Ramathibodi Hospital, Mahidol University Incidence: Global: 338,000 new cases, 130,000
3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours
 60 3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours Compilation and editing and of this volume: Prof. Chandu de Silva (Consultant Histopathologist) List of contributors Consultant
60 3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours Compilation and editing and of this volume: Prof. Chandu de Silva (Consultant Histopathologist) List of contributors Consultant
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
GUIDELINES ON RENAL CELL CANCER
 20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia
 Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia Sílvia Bagué Servei de Patologia Hospital de Sant Pau Barcelona Soft tissue sarcomas Heterogeneous group
Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia Sílvia Bagué Servei de Patologia Hospital de Sant Pau Barcelona Soft tissue sarcomas Heterogeneous group
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA
 PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
Renal Parenchymal Neoplasms
 Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
Renal Mass Biopsy: Needed Now More than Ever
 Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Renal tumors of adults
 Renal tumors of adults Urinary Tract Tumors 2%-3% of all cancers in adults. The most common malignant tumor of the kidney is renal cell carcinoma. Tumors of the lower urinary tract are twice as common
Renal tumors of adults Urinary Tract Tumors 2%-3% of all cancers in adults. The most common malignant tumor of the kidney is renal cell carcinoma. Tumors of the lower urinary tract are twice as common
ACCME/Disclosures ALK FUSION-POSITIVE MESENCHYMAL TUMORS. Tumor types with ALK rearrangements. Anaplastic Lymphoma Kinase. Jason L.
 Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Evening Specialty Conference: Cytopathology
 : Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
: Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
BLADDER CANCER EPIDEMIOLOGY
 BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
Sustained Response to Temsirolimus in Chromophobe variant of Metastatic Renal Cell Carcinoma
 JOURNAL OF CASE REPORTS 2015;5(1):280-284 Sustained Response to Temsirolimus in Chromophobe variant of Metastatic Renal Cell Carcinoma Chanchal Goswami, Aditi Mandal B. P. Poddar Hospital & Medical Research
JOURNAL OF CASE REPORTS 2015;5(1):280-284 Sustained Response to Temsirolimus in Chromophobe variant of Metastatic Renal Cell Carcinoma Chanchal Goswami, Aditi Mandal B. P. Poddar Hospital & Medical Research
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Molecular genetics and immunohistochemistry characterization of uncommon and recently described renal cell carcinomas
 Review Article Molecular genetics and immunohistochemistry characterization of uncommon and recently described renal cell carcinomas Qiu Rao 1 *, Qiu-Yuan Xia 1 *, Liang Cheng 2, Xiao-Jun Zhou 1 1 Department
Review Article Molecular genetics and immunohistochemistry characterization of uncommon and recently described renal cell carcinomas Qiu Rao 1 *, Qiu-Yuan Xia 1 *, Liang Cheng 2, Xiao-Jun Zhou 1 1 Department
RENAL EPITHELIAL TUMORS 2009: THE ROLE OF ELECTRON MICROSCOPY IN UNDERSTANDING PATHOGENESIS, DIAGNOSIS, AND CLASSIFICATION.
 RENAL EPITHELIAL TUMORS 2009: THE ROLE OF ELECTRON MICROSCOPY IN UNDERSTANDING PATHOGENESIS, DIAGNOSIS, AND CLASSIFICATION. Guillermo A. Herrera MD Nephrocor, Tempe, Arizona Epithelial renal cell tumors
RENAL EPITHELIAL TUMORS 2009: THE ROLE OF ELECTRON MICROSCOPY IN UNDERSTANDING PATHOGENESIS, DIAGNOSIS, AND CLASSIFICATION. Guillermo A. Herrera MD Nephrocor, Tempe, Arizona Epithelial renal cell tumors
Prognostic and Therapeutic Impact of the Histopathologic Definition of Parenchymal Epithelial Renal Tumors
 EUROPEAN UROLOGY 58 (2010) 655 668 available at www.sciencedirect.com journal homepage: www.europeanurology.com Platinum Priority Collaborative Review Kidney Cancer Editorial by Matthew K. Tollefson and
EUROPEAN UROLOGY 58 (2010) 655 668 available at www.sciencedirect.com journal homepage: www.europeanurology.com Platinum Priority Collaborative Review Kidney Cancer Editorial by Matthew K. Tollefson and
BRAZILIAN PRIMARY RENAL TUMORS: CLINICAL AND PATHOLOGICAL REVIEW OF 137 CASES WITH EMPHASIS ON RENAL CORTICAL EPITHELIAL NEOPLASMS.
 IV CONGRESO VIRTUAL HISPANO AMERICANO DE ANATOMÍA PATOLÓGICA Abstract CONTENIDO PDF Comentarios Título Resumen Introducción Material Resultados Discusión Correspondencia Referencias Imágenes BRAZILIAN
IV CONGRESO VIRTUAL HISPANO AMERICANO DE ANATOMÍA PATOLÓGICA Abstract CONTENIDO PDF Comentarios Título Resumen Introducción Material Resultados Discusión Correspondencia Referencias Imágenes BRAZILIAN
Case 1 PLEASE TURN OFF YOUR CELL PHONES 3/28/2017. Disclosure of Relevant Financial Relationships. Disclosure of Relevant Financial Relationships
 PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose
PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
THE FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA AND NIFTP
 THE FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA AND NIFTP FOLLICULAR VARIANT OF PAPILLARY CARCINOMA HISTORICAL PERSPECTIVE FOLLICULAR VARIANT OF PAPILLARY CARCINOMA 1960 described by Dr. Stuart Lindsay
THE FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA AND NIFTP FOLLICULAR VARIANT OF PAPILLARY CARCINOMA HISTORICAL PERSPECTIVE FOLLICULAR VARIANT OF PAPILLARY CARCINOMA 1960 described by Dr. Stuart Lindsay
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Case: The patient is a 62 year old woman with a history of renal cell carcinoma that was removed years ago. A 2.4 cm liver mass was found on CT
 Case: The patient is a 62 year old woman with a history of renal cell carcinoma that was removed years ago. A 2.4 cm liver mass was found on CT during follow- up. ALT, AST, Alk Phos and bilirubin were
Case: The patient is a 62 year old woman with a history of renal cell carcinoma that was removed years ago. A 2.4 cm liver mass was found on CT during follow- up. ALT, AST, Alk Phos and bilirubin were
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center