10/30/2018. Martha K. Terris, MD Witherington Distinguished Professor and Chair Medical College of Georgia Urology November 5, 2018
|
|
|
- Bertram Nicholson
- 5 years ago
- Views:
Transcription




1 Martha K. Terris, MD Witherington Distinguished Professor and Chair Medical College of Georgia Urology November 5, 2018 Elevated PSA and/or nodule on digital rectal examination Prostate biopsies If initial biopsy shows no cancer, a variety of other tests may be performed 1

2 3T Multiparametric MRI of the Prostate Identifies lesions in patients with negative biopsy and persistent concern for cancer Use as an initial evaluation is controversial Biopsies directed at MRI lesions do not replace random systematic biopsies Blood 4Kscore Measures kallikrein proteins: total PSA, free PSA, intact PSA, and human kallikrein related peptidase 2 to assess a patient s risk of having a Gleason score 7 on prostate biopsy. Prostate Health Index (phi) score includes PSA, free PSA, and proenzyme PSA (propsa) to estimate probability of cancer on biopsy Urine Progensa (Gen-Probe, San Diego, CA) prostate cancer antigen-3 (PCA3) urine assay Following a DRE, PCA3 score is calculated from a patient s urine to estimate the risk for prostate cancer on a subsequent biopsy. 2
 from negative prostate biopsy tissue to help")


3 Biopsy Tissue ConfirmMDx Uses the methylation status of three biomarkers (GSTP1, RASSF1, and APC) from negative prostate biopsy tissue to help determine the chance of prostate cancer on a subsequent biopsy. Low Risk PSA level <10 ng/ml Biopsy Gleason score of 6, Clinical stage of T2a Intermediate Risk PSA level of 10.1 to 20 ng/ml Gleason score of 7 and/or a clinical stage of T2b High Risk PSA level >20 ng/ml, Gleason score of 8, and/or a clinical stage of T2c-3a 3
4 Organization Low Risk Intermediate Risk AUA, EAU, D Amico GUROC, NICE CAPSURE NCCN ESMO <T2a, PSA<10, and GS<6 <T2a, PSA<10, and GS<6 <T2a, PSA<10, and GS<6 <T2a, PSA<10, and GS<6 Very Low: <3cores + <50% <T2a, PSA<10, and GS<6 T2b and/or PSA >10-20 and/or GS=7 T1-T2 and/or PSA <20 and/or GS<7 T2b and/or PSA >10-20 and/or GS=7 T2b or T2c and/or PSA >10-20 and/or GS=7 Any between Low and High High Risk >T2c or PSA>20 or GS 8-10 >T3a or PSA>20 or GS 8-10 >T3a or PSA>20 or GS 8-10 Very High T3b-4 T3a or PSA>20 or GS 8-10 Very High T3b-4 >T3a or PSA>20 or GS 8-10 AUA=American Urological Association, EAU=European Association of Urology, D Amico=Harvard, GUROC=GU Radiation Oncologist of Canada, NICE=National Institutes of Health and Clinical Excellence, Capsure=UCSF, ESMO=European Society of Medical Oncology Oncotype Dx/genomic prostate score (GPS) Consists of 12 cancer-related genes and 5 reference genes to evaluate cancer aggressiveness. Prolaris Score Measures RNA expression of 31 genes involved in cell cycle progression compared to 15 house keeping genes to quantify prostate cancer cellular aggression. ProMark Proteomic prognostic test that incorporates eight biomarkers from a prostate biopsy sample to predict an individual s risk of favorable or nonfavorable/aggressive prostate cancer. Considered Experimental Low Risk No Staging Studies necessary If choosing active surveillance may have serial MRI and/or biopsies Intermediate Risk Abdominal/Pelvic imaging (CT or MRI) Bone scan if T2 and PSA >10 High Risk Abdominal/Pelvic imaging (CT or MRI) Bone scan if T2 and PSA >10 *NCCN Guidelines 4
 PSA nadir at <0.")

5 Very healthy 63 year old African American gentleman Prostate Cancer on TRUS bx for elevated PSA 4.3 GS 4+4 in 7/15 cores in 2008 Treated with Brachytherapy (age 54) PSA nadir at <0.01 and was undetectable until 2014 when PSA was found to be 0.2 Repeat PSA in 2/2017 was 4.87 and 3/2017 was ROS: negative PMH: prostate cancer, hypertension, hyperlipidemia PSH: rotator cuff repair, brachytherapy Med: amlodipine, aspirin, lipitor, FH: no hx of PCa SH: non-smoker, social drinker 5

6 IMPRESSION 1. Brachytherapy seeds identified within the prostate gland. The prostate gland is within normal limits of size. 2. A 1.2 x 1.6 cm intermediate density structure is identified adjacent to right external iliac vein, which is highly concerning for pathologically enlarged right pelvic lymph node (i.e. nodal metastatic disease). 6

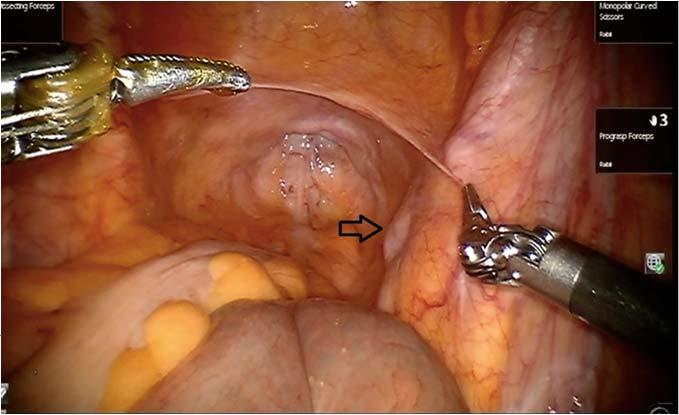
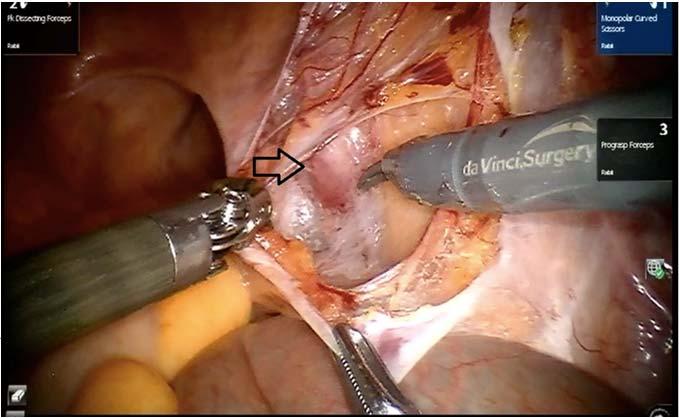
7 Patient underwent repeat Ultrasound guided prostate biopsy Pathology Report: Benign prostatic tissue showing treatment effect in all cores He was advised by his urologist that Lupron was next step but was opposed to hormone treatment at this point He presented to MCG for a 2 nd opinion AXUMIN PET/CT 7


8 Intensely increased activity in a conglomerate right external iliac lymph node group 1.3 cm short axis x 2.4 cm craniocaudal Numerous brachytherapy seeds throughout the prostate gland. No abnormal focal uptake. IMPRESSION: Intense regional right external iliac tumor lymphadenopathy No other significant active lymphadenopathy or distant metastasis F-18 fluciclovine (AXUMIN) PET/CT F-18 fluciclovine (AXUMIN) PET/CT 8

9 30-40% biochemical recurrence rate after RP and 36-50% for brachytherapy within 10 years Management Options: Androgen deprivation therapy- standard Unfavorable side effect profile Progression to castration-resistant disease Significant toxicity at long term Continuous vs Intermittent Salvage radiation therapy Salvage ablation procedures Salvage lymphadenectomy More favorable outcome than those with mets to bone or other visceral organs Long-term follow-up studies: good cancerspecific survival of patients with limited node-positive disease after RP Even without ADT Removal of node may have beneficial impact on cancer progression Tilki et al. J Urol. 2015; 193: Karnes et al. J Urol. 2015; 193: Suardi et al. Eur Urol : Winter et al. BMC Urol. 2015; 15:10. Rigatti et al

10 Salvage PLND after primary treatment Prolong recurrence-free survival Delay systemic therapies Efficient and precise imaging for identification of suspicious LNs would optimize salvage Traditional CT and MRI low sensitivity Tilki et al. J Urol. 2015; 193: Karnes et al. J Urol. 2015; 193: Suardi et al. Eur Urol : Winter et al. BMC Urol. 2015; 15:10. PET/CT Scan 18-fluorodeoxyglucose 11C-choline 18F-fluoroethylcholine 11C-acetate Sensitivity 58% ; Specificity 69% Small (>5mm) LN metastasis Limitations: 20 min t ½ Requires on-site cyclotron Jadvar H. J Nuc Med.2011;52(1): Almeida et al. Am J Nucl Med Mol Imaging. 2017;7:1-11. PET/CT 18F-fluciclovine (AXUMIN) - amino acid transporter analogue Sensitivity 58% and Specificity 81% min t ½ 68Ga-PSMA - transmembrane protein Prostate-specific membrane antigen (PSMA) 55% detection PSA ng/ml 76% detection PSA ng/ml Pultrone et al. J Urol. 197, 4S, Maurer et al. J Urol. 197, 4S, Maurer et al. Nature Rev Urol 13,


11 Diffusion-weighted MRI combined with ultrasmall particles of iron oxide (USPIO) high sensitivity between benign and malignant lymph nodes even in normal sized nodes. Identified intraoperatively with hand-held magnetometer Intraprostatic injection limits use in salvage setting. Winter et al. Ann. Surg. Oncol. 2014; 21: Harisinghani et al. N. Engl. J. Med. 2003; 348: mTc-labeled colloids Albumin Sulphur Phytate Require intraoperative gamma camera Hybrid ICG and 99m Tc-nanocolloid Intraoperative imaging without gamma camera All require injection into primary tumor Buckle et al. J. Nucl. Med. 2012;53: Near-infrared (NIR) intraoperative molecular imaging with indocyanine green (ICG) Intraoperative, intraprostatic injection of ICG Complexity of lymphatic drainage U Penn: 5 mg/kg IV ICG one day prior to node dissection Xia et al. Urology ,
12 Future imaging with prostate-specific fluorescent compounds Anti-Prostate-Specific Membrane Antigen (PSMA) antibody (J591) linked to ICG YC-27, a near-infrared-emitting fluorophore targeted to PSMA Antibody fragment (cys-diabody, cdb) against prostate stem cell antigen (PSCA) conjugated to farred fluorophore, Cy5 Nakajima et al. Bioconjug Chem : Neuman et al. Clin Cancer Res : Son et al. Clin Cancer Res : Experimental treatment option for PCa patients with nodal recurrence localized on PET/CT after primary treatment failure Lack of current guidelines Two main aims: Delay further cancer recurrence Postpone use of systemic treatments Suardi et al. Eur Urol : Winter et al. BMC Urol. 2015; 15:10. To maximize oncological outcomes, avoid unnecessary morbidity [1,3] Ideal candidate: [3,5,6] Young patients Path stage pt2 Gleason score 7 PSA < 4 ng/ml Castration-sensitive disease Low LN burden limited to pelvis 12
 Significant predictor of cancer progression Rigatti et al: Mean time to clinical progression Persistently elevated PSA: 28.8mo Complete BR: 64.")
13 Abdollah et al % of patients achieve complete BR after SLND (defined as PSA < 0.2 ng/ml) Significant predictor of cancer progression Rigatti et al: Mean time to clinical progression Persistently elevated PSA: 28.8mo Complete BR: 64.8mo Predictors of BR: PSA <4 ng/ml RP to BCR time <24mo Node-negative at RP Most invariably progress to biochemical recurrence after SLND, despite initial BR [3] Definition: PSA> 0.2 ng/ml and rising Median 18mo 9-31% BCR-free survival rate at 5 yrs Suardi et al: 23% at 8 yrs Winter et al: 3/13 complete remission (PSA<0.01) for 7 yrs Potential for cure Suardi et al. Eur Urol : Winter et al. BMC Urol. 2015; 15:10. 13
![Positive PET/CT after SLND + rising PSA 35%-50% CR-free survival rate at 5 yrs [3,6,7] Suardi et al: 38% CR-free survival at 8 yrs Pre-op predictors of CR: PSA >4 ng/ml at SLND [1,3] Retroperitoneal](/docs-images/89/100111180/images/14-0.jpg "uptake at PET/CT scan Post-op predictors of CR: Pathologic nodes in retroperitoneum Higher # of positive nodes Incomplete PSA response to SLND Most reported complications were mild No post-op")
14 Positive PET/CT after SLND + rising PSA 35%-50% CR-free survival rate at 5 yrs [3,6,7] Suardi et al: 38% CR-free survival at 8 yrs Pre-op predictors of CR: PSA >4 ng/ml at SLND [1,3] Retroperitoneal uptake at PET/CT scan Post-op predictors of CR: Pathologic nodes in retroperitoneum Higher # of positive nodes Incomplete PSA response to SLND Most reported complications were mild No post-op mortality has been reported Suardi et al. Eur Urol : Constraints on sensitivity of current imaging techniques to detect LN recurrence No literature currently on SLND s/p brachytherapy specifically Studies: retrospective, small sample sizes, heterogeneous population, no controls Current randomized prospective trial ongoing Salvage Treatment or Active Clinical Surveillance for Oligometastatic Prostate Cancer: a Randomized Phase II Trial (NCT ) 14
15 15
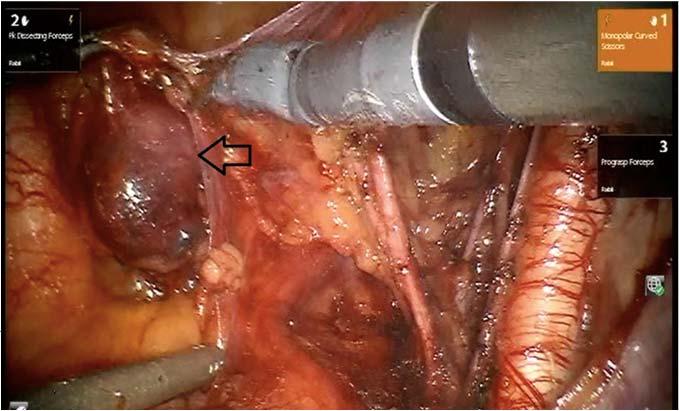
16 A) LYMPH NODES, RIGHT PELVIC (DISSECTION): -Metastatic prostatic adenocarcinoma (2.6cm) involving one of ten lymph nodes (1/10) B) LYMPH NODES, LEFT PELVIC (DISSECTION): -Five lymph nodes, negative for malignancy (0/5) Tolerated procedure without complication Good biochemical response to SLND Pre-op PSA: month post-op PSA: months post-op PSA: months post-op PSA: months post-op PSA: months post-op PSA: 0.02 New imaging techniques help localize disease recurrence after primary prostate cancer treatment. More exact staging in recurrence increases the opportunities for directed treatment and prolonged results to salvage therapy 16

17 17
MEDICAL POLICY Genetic and Protein Biomarkers for Diagnosis and Risk Assessment of
 POLICY: PG0367 ORIGINAL EFFECTIVE: 08/26/16 LAST REVIEW: 09/27/18 MEDICAL POLICY Genetic and Protein Biomarkers for Diagnosis and Risk Assessment of Prostate Cancer GUIDELINES This policy does not certify
POLICY: PG0367 ORIGINAL EFFECTIVE: 08/26/16 LAST REVIEW: 09/27/18 MEDICAL POLICY Genetic and Protein Biomarkers for Diagnosis and Risk Assessment of Prostate Cancer GUIDELINES This policy does not certify
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Consensus and Controversies in Cancer of Prostate BASIS FOR FURHTER STUDIES. Luis A. Linares MD FACRO Medical Director
 BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
Presentation with lymphadenopathy
 Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
#1 cancer. #2 killer. Boulder has higher rate of prostate cancer compared to other areas surrounding Rocky Flats
 Prostate cancer is a VERY COMMON DISEASE BREAKTHROUGHS IN THE DETECTION OF PROSTATE CANCER Carolyn M. Fronczak M.D., M.S.P.H. Urologic Surgery 303-647-9129 #1 cancer #2 killer Ca Cancer J Clin 2018;68:7
Prostate cancer is a VERY COMMON DISEASE BREAKTHROUGHS IN THE DETECTION OF PROSTATE CANCER Carolyn M. Fronczak M.D., M.S.P.H. Urologic Surgery 303-647-9129 #1 cancer #2 killer Ca Cancer J Clin 2018;68:7
Presentation with lymphadenopathy
 Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
MRI in the Enhanced Detection of Prostate Cancer: What Urologists Need to Know
 MRI in the Enhanced Detection of Prostate Cancer: What Urologists Need to Know Michael S. Cookson, MD, FACS Professor and Chair Department of Urology Director of Prostate and Urologic Oncology University
MRI in the Enhanced Detection of Prostate Cancer: What Urologists Need to Know Michael S. Cookson, MD, FACS Professor and Chair Department of Urology Director of Prostate and Urologic Oncology University
L approccio alle stazioni linfonodali in presentazione di malattia ed all eventuale recidiva nodale: il punto di vista dell urologo
 L approccio alle stazioni linfonodali in presentazione di malattia ed all eventuale recidiva nodale: il punto di vista dell urologo Paolo Gontero Division of Urology Città della Salute e della Scienza
L approccio alle stazioni linfonodali in presentazione di malattia ed all eventuale recidiva nodale: il punto di vista dell urologo Paolo Gontero Division of Urology Città della Salute e della Scienza
Newer Aspects of Prostate Cancer Underwriting
 Newer Aspects of Prostate Cancer Underwriting Presented By: Jack Swanson, M.D. Keith Hoffman, NFP Moments Made Possible Objectives To review and discuss Conflicting messages about PSA testing Cautions
Newer Aspects of Prostate Cancer Underwriting Presented By: Jack Swanson, M.D. Keith Hoffman, NFP Moments Made Possible Objectives To review and discuss Conflicting messages about PSA testing Cautions
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Navigating the Stream: Prostate Cancer and Early Detection. Ifeanyi Ani, M.D. TPMG Urology Newport News
 Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostatectomy as salvage therapy. Cases. Paul Cathcart - Guy s & St Thomas NHS Trust, London
 Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps?
 Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps? Michael J Zelefsky, M.D. Professor of Radiation Oncology Chief Brachytherapy Service Department of Radiation Oncology
Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps? Michael J Zelefsky, M.D. Professor of Radiation Oncology Chief Brachytherapy Service Department of Radiation Oncology
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
PET imaging of cancer metabolism is commonly performed with F18
 PCRI Insights, August 2012, Vol. 15: No. 3 Carbon-11-Acetate PET/CT Imaging in Prostate Cancer Fabio Almeida, M.D. Medical Director, Arizona Molecular Imaging Center - Phoenix PET imaging of cancer metabolism
PCRI Insights, August 2012, Vol. 15: No. 3 Carbon-11-Acetate PET/CT Imaging in Prostate Cancer Fabio Almeida, M.D. Medical Director, Arizona Molecular Imaging Center - Phoenix PET imaging of cancer metabolism
AllinaHealthSystems 1
 2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015
 Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate Cancer Local or distant recurrence?
 Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality
 Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality Sanoj Punnen, MD, MAS Assistant Professor of Urologic Oncology University of Miami, Miller School of Medicine and Sylvester
Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality Sanoj Punnen, MD, MAS Assistant Professor of Urologic Oncology University of Miami, Miller School of Medicine and Sylvester
Radioligand imaging & treatment of prostate cancer
 Radioligand imaging & treatment of prostate cancer Christiaan Schiepers, MD, PhD University of California Los Angeles CANM-CAMRT JOINT ANNUAL CONFERENCE MARCH 22-24, 2018 VANCOUVER, B.C. I do not have
Radioligand imaging & treatment of prostate cancer Christiaan Schiepers, MD, PhD University of California Los Angeles CANM-CAMRT JOINT ANNUAL CONFERENCE MARCH 22-24, 2018 VANCOUVER, B.C. I do not have
FOR PATIENTS DIAGNOSED WITH EARLY-STAGE PROSTATE CANCER. Discover a test that can help you on your treatment journey
 FOR PATIENTS DIAGNOSED WITH EARLY-STAGE PROSTATE CANCER Discover a test that can help you on your treatment journey Jim G. Oncotype DX GPS patient navigating prostate cancer since 2014 Not all prostate
FOR PATIENTS DIAGNOSED WITH EARLY-STAGE PROSTATE CANCER Discover a test that can help you on your treatment journey Jim G. Oncotype DX GPS patient navigating prostate cancer since 2014 Not all prostate
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Low risk. Objectives. Case-based question 1. Evidence-based utilization of imaging in prostate cancer
 Evidence-based utilization of imaging in prostate cancer Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Objectives State the modalities,
Evidence-based utilization of imaging in prostate cancer Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Objectives State the modalities,
PROSTATE CANCER SURVEILLANCE
 PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
Prostate Cancer Genomics When To Treat and With What? Ashley E. Ross, M.D., Ph.D. Texas Urology Specialists August 2017
 Prostate Cancer Genomics When To Treat and With What? Ashley E. Ross, M.D., Ph.D. Texas Urology Specialists August 2017 Relevant Disclosures Advisory role, ownership interest, previous unrestricted grant
Prostate Cancer Genomics When To Treat and With What? Ashley E. Ross, M.D., Ph.D. Texas Urology Specialists August 2017 Relevant Disclosures Advisory role, ownership interest, previous unrestricted grant
Does Imaging of Advanced PC change a suggested treatment?
 Does Imaging of Advanced PC change a suggested treatment? Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials and conflict
Does Imaging of Advanced PC change a suggested treatment? Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials and conflict
PSMA PET SCANNING AND THERANOSTICS IN PROSTATE CANCER KEVIN TRACEY, MD, FRCPC PRECISION DIAGNSOTIC IMAGING REGIONAL PET/CT CENTRE
 PSMA PET SCANNING AND THERANOSTICS IN PROSTATE CANCER KEVIN TRACEY, MD, FRCPC PRECISION DIAGNSOTIC IMAGING REGIONAL PET/CT CENTRE DISCLOSURES/CONFLICTS NONE OBJECTIVES Understand current diagnostic role
PSMA PET SCANNING AND THERANOSTICS IN PROSTATE CANCER KEVIN TRACEY, MD, FRCPC PRECISION DIAGNSOTIC IMAGING REGIONAL PET/CT CENTRE DISCLOSURES/CONFLICTS NONE OBJECTIVES Understand current diagnostic role
Focal Therapy is a Fool s Paradise : The whole prostate must be treated!
 Focal Therapy is a Fool s Paradise : The whole prostate must be treated! Ofer Yossepowitch, MD Head, Department of Urology Tel Aviv Sourasky Medical Center Preaching against focal therapy in a focal therapy
Focal Therapy is a Fool s Paradise : The whole prostate must be treated! Ofer Yossepowitch, MD Head, Department of Urology Tel Aviv Sourasky Medical Center Preaching against focal therapy in a focal therapy
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Role and extension of lymph node dissection in kidney, bladder and prostate cancer. Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017
 Moderator: Dr A. Noujem 30 th March 2017") Role and extension of lymph node dissection in kidney, bladder and prostate cancer Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017 Bladder Cancer LN dissection in Bladder cancer 25% of patients
Role and extension of lymph node dissection in kidney, bladder and prostate cancer Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017 Bladder Cancer LN dissection in Bladder cancer 25% of patients
Whole Body MRI. Dr. Nina Tunariu. Prostate Cancer recurrence, progression and restaging
 Whole Body MRI Prostate Cancer recurrence, progression and restaging Dr. Nina Tunariu Consultant Radiology Drug Development Unit and Prostate Targeted Therapies Group 12-13 Janeiro 2018 Evolving Treatment
Whole Body MRI Prostate Cancer recurrence, progression and restaging Dr. Nina Tunariu Consultant Radiology Drug Development Unit and Prostate Targeted Therapies Group 12-13 Janeiro 2018 Evolving Treatment
PSA is rising: What to do? After curative intended radiotherapy: More local options?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Case Scenario 1. 4/19/13 Bone Scan: No scintigraphic findings to suggest skeletal metastases.
 Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Molecular Imaging in Prostate Cancer. Carlos Artigas Nuclear Medicine Institut Jules Bordet
 Molecular Imaging in Prostate Cancer Carlos Artigas Nuclear Medicine Institut Jules Bordet Introduction 3 different stages of the disease Local treatment with curative intent Introduction 3 different stages
Molecular Imaging in Prostate Cancer Carlos Artigas Nuclear Medicine Institut Jules Bordet Introduction 3 different stages of the disease Local treatment with curative intent Introduction 3 different stages
PSMA PET in patients with prostate cancer
 PSMA PET in patients with prostate cancer Thomas Hope, MD Assistant Professor of Radiology, UCSF Abdominal Imaging and Nuclear Medicine Co-director, PET/MRI Chief of MRI, San Francisco VA Medical Center
PSMA PET in patients with prostate cancer Thomas Hope, MD Assistant Professor of Radiology, UCSF Abdominal Imaging and Nuclear Medicine Co-director, PET/MRI Chief of MRI, San Francisco VA Medical Center
Joelle Hamilton, M.D.
 Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
10/2/2018 OBJECTIVES PROSTATE HEALTH BACKGROUND THE PROSTATE HEALTH INDEX PHI*: BETTER PROSTATE CANCER DETECTION
 THE PROSTATE HEALTH INDEX PHI*: BETTER PROSTATE CANCER DETECTION Lenette Walters, MS, MT(ASCP) Medical Affairs Manager Beckman Coulter, Inc. *phi is a calculation using the values from PSA, fpsa and p2psa
THE PROSTATE HEALTH INDEX PHI*: BETTER PROSTATE CANCER DETECTION Lenette Walters, MS, MT(ASCP) Medical Affairs Manager Beckman Coulter, Inc. *phi is a calculation using the values from PSA, fpsa and p2psa
State-of-the-art: vision on the future. Urology
 State-of-the-art: vision on the future Urology Francesco Montorsi MD FRCS Professor and Chairman Department of Urology San Raffaele Hospital Vita-Salute San Raffaele University Milan, Italy Disclosures
State-of-the-art: vision on the future Urology Francesco Montorsi MD FRCS Professor and Chairman Department of Urology San Raffaele Hospital Vita-Salute San Raffaele University Milan, Italy Disclosures
MR-US Fusion Guided Biopsy: Is it fulfilling expectations?
 MR-US Fusion Guided Biopsy: Is it fulfilling expectations? Kenneth L. Gage MD, PhD Assistant Member Department of Diagnostic Imaging and Interventional Radiology 4 th Annual New Frontiers in Urologic Oncology
MR-US Fusion Guided Biopsy: Is it fulfilling expectations? Kenneth L. Gage MD, PhD Assistant Member Department of Diagnostic Imaging and Interventional Radiology 4 th Annual New Frontiers in Urologic Oncology
GUIDELINEs ON PROSTATE CANCER
 GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
Active Surveillance for Intermediate Risk Prostate Cancer
 Active Surveillance for Intermediate Risk Prostate Cancer Eric Wallen, M.D., FACS Professor Department of Urology The University of North Carolina at Chapel Hill Disclosures: None Objectives Understand
Active Surveillance for Intermediate Risk Prostate Cancer Eric Wallen, M.D., FACS Professor Department of Urology The University of North Carolina at Chapel Hill Disclosures: None Objectives Understand
Prostate cancer screening: a wobble Balance. Elias NAOUM PGY-4 Urology Hotel-Dieu de France Universite Saint Joseph
 Prostate cancer screening: a wobble Balance Elias NAOUM PGY-4 Urology Hotel-Dieu de France Universite Saint Joseph Epidemiology Most common non skin malignancy in men in developed countries Third leading
Prostate cancer screening: a wobble Balance Elias NAOUM PGY-4 Urology Hotel-Dieu de France Universite Saint Joseph Epidemiology Most common non skin malignancy in men in developed countries Third leading
2/14/09. Why Discuss this topic? Managing Local Recurrences after Radiation Failure. PROSTATE CANCER Second Treatment
 Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Alberto Briganti, M.D., PhD
 Alberto Briganti, M.D., PhD Professore Orinario di Urologia IRCCS San Raffaele Divisione di Oncologia / Unità di Urologia Urological Research Institute (URI) Università Vita-Salute San Raffaele, Milano
Alberto Briganti, M.D., PhD Professore Orinario di Urologia IRCCS San Raffaele Divisione di Oncologia / Unità di Urologia Urological Research Institute (URI) Università Vita-Salute San Raffaele, Milano
Personalizing prostate cancer care: A clinical perspective on imaging and other biomarkers in 2017
 Personalizing prostate cancer care: A clinical perspective on imaging and other biomarkers in 2017 Matthew R. Cooperberg, MD, MPH Departments of Urology and Epidemiology & Biostatistics @dr_coops Osher
Personalizing prostate cancer care: A clinical perspective on imaging and other biomarkers in 2017 Matthew R. Cooperberg, MD, MPH Departments of Urology and Epidemiology & Biostatistics @dr_coops Osher
Using PET/CT in Prostate Cancer
 Using PET/CT in Prostate Cancer Legal Disclaimer These materials were prepared in good faith by MITA as a service to the profession and are believed to be reliable based on current scientific literature.
Using PET/CT in Prostate Cancer Legal Disclaimer These materials were prepared in good faith by MITA as a service to the profession and are believed to be reliable based on current scientific literature.
GUIDELINES ON PROSTATE CANCER
 10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
Long-term Results of a Comparative PET/CT and PET/MRI Study of 11 C-Acetate and 18 F-Fluorocholine for Restaging of Early Recurrent Prostate Cancer
 ORIGINAL ARTICLE Long-term Results of a Comparative PET/CT and PET/MRI Study of 11 C-Acetate and 18 F-Fluorocholine for Restaging of Early Recurrent Prostate Cancer Giorgio Lamanna, MD,* Claire Tabouret-Viaud,
ORIGINAL ARTICLE Long-term Results of a Comparative PET/CT and PET/MRI Study of 11 C-Acetate and 18 F-Fluorocholine for Restaging of Early Recurrent Prostate Cancer Giorgio Lamanna, MD,* Claire Tabouret-Viaud,
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
Screening and Diagnosis Prostate Cancer
 Screening and Diagnosis Prostate Cancer Daniel Heng MD MPH FRCPC Chair, Genitourinary Tumor Group Tom Baker Cancer Center University of Calgary, Canada @DrDanielHeng Outline Screening Evidence Recommendations
Screening and Diagnosis Prostate Cancer Daniel Heng MD MPH FRCPC Chair, Genitourinary Tumor Group Tom Baker Cancer Center University of Calgary, Canada @DrDanielHeng Outline Screening Evidence Recommendations
Prostate Cancer. David Wilkinson MD Gulfshore Urology
 Prostate Cancer David Wilkinson MD Gulfshore Urology What is the Prostate? Male Sexual Gland Adds nutrients and fluids for sperm This fluid is added to sperm during ejaculation Urethra (urine channel)
Prostate Cancer David Wilkinson MD Gulfshore Urology What is the Prostate? Male Sexual Gland Adds nutrients and fluids for sperm This fluid is added to sperm during ejaculation Urethra (urine channel)
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
 Measure #104 (NQF 0390): Prostate Cancer: Adjuvant Hormonal Therapy for High Risk or Very High Risk Prostate Cancer National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL
Measure #104 (NQF 0390): Prostate Cancer: Adjuvant Hormonal Therapy for High Risk or Very High Risk Prostate Cancer National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL
18-Oct-16. Take home messages. An update for GPs on modern radiation therapy & hormones for prostate cancer. Session plan
 An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
4Kscore. A Precision Test for Risk of Aggressive Prostate Cancer
 4Kscore A Precision Test for Risk of Aggressive Prostate Cancer How to Evaluate Risk for Prostate Cancer? PSA is a good screening tool But abnormal PSA leads to over 1 million prostate biopsies each year
4Kscore A Precision Test for Risk of Aggressive Prostate Cancer How to Evaluate Risk for Prostate Cancer? PSA is a good screening tool But abnormal PSA leads to over 1 million prostate biopsies each year
MRI and metastases of PCa
 MRI and metastases of PCa François CORNUD Céline COUVIDAT David EISS Arnaud LEFEVRE IRM Paris 16, France, Paris, France Université Paris Descartes, Paris, France When imaging should be considered for detection
MRI and metastases of PCa François CORNUD Céline COUVIDAT David EISS Arnaud LEFEVRE IRM Paris 16, France, Paris, France Université Paris Descartes, Paris, France When imaging should be considered for detection
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
Prostate MRI Hamidreza Abdi, MD,FEBU Post Doctoral Fellow Vancouver Prostate Centre UBC Department of Urologic Sciences May-20144
 Prostate MRI Hamidreza Abdi, MD,FEBU Post Doctoral Fellow Vancouver Prostate Centre UBC Department of Urologic Sciences May-20144 Objectives: Detection of prostate cancer the need for better imaging What
Prostate MRI Hamidreza Abdi, MD,FEBU Post Doctoral Fellow Vancouver Prostate Centre UBC Department of Urologic Sciences May-20144 Objectives: Detection of prostate cancer the need for better imaging What
Prostate MRI: Who needs it?
 Prostate MRI: Who needs it? Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Abdominal Imaging Magnetic Resonance Science Center
Prostate MRI: Who needs it? Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Abdominal Imaging Magnetic Resonance Science Center
The 4Kscore A Precision Test for Risk of Aggressive Prostate Cancer. Reduce Unnecessary Invasive Procedures And Healthcare Costs
 The 4Kscore A Precision Test for Risk of Aggressive Prostate Cancer Reduce Unnecessary Invasive Procedures And Healthcare Costs PSA Lacks Specificity for Aggressive Prostate Cancer Abnormal PSA leads to
The 4Kscore A Precision Test for Risk of Aggressive Prostate Cancer Reduce Unnecessary Invasive Procedures And Healthcare Costs PSA Lacks Specificity for Aggressive Prostate Cancer Abnormal PSA leads to
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Adam Raben M.D. Helen F Graham Cancer Center
 Adam Raben M.D. Helen F Graham Cancer Center Is the biopsy sample representative of the extent of the disease in your patient with clinically low-risk prostate cancer? BIOPSY RP registry (n=8095) 3+3=6
Adam Raben M.D. Helen F Graham Cancer Center Is the biopsy sample representative of the extent of the disease in your patient with clinically low-risk prostate cancer? BIOPSY RP registry (n=8095) 3+3=6
στη σταδιοποίηση του καρκίνου του προστάτη Γ. Αρσος, Γ Εργ. Πυρηνικής Ιατρικής ΑΠΘ, ΓΝΘ Παπαγεωργίου
 Η θέση του PET/CT στη σταδιοποίηση του καρκίνου του προστάτη Γ. Αρσος, Γ Εργ. Πυρηνικής Ιατρικής ΑΠΘ, ΓΝΘ Παπαγεωργίου 2014 : the Guidelines year. PRINCIPLES OF IMAGING Imaging is performed for the detection
Η θέση του PET/CT στη σταδιοποίηση του καρκίνου του προστάτη Γ. Αρσος, Γ Εργ. Πυρηνικής Ιατρικής ΑΠΘ, ΓΝΘ Παπαγεωργίου 2014 : the Guidelines year. PRINCIPLES OF IMAGING Imaging is performed for the detection
Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline Very Low-/Low-Risk Disease
 Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline Very Low-/Low-Risk Disease Jeffrey A. Cadeddu, MD Professor, Department of Urology UT Southwestern Medical Center Vice-Chair, AUA/ASTRO/SUO
Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline Very Low-/Low-Risk Disease Jeffrey A. Cadeddu, MD Professor, Department of Urology UT Southwestern Medical Center Vice-Chair, AUA/ASTRO/SUO
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia
 Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
PROSTATE MRI. Dr. Margaret Gallegos Radiologist Santa Fe Imaging
 PROSTATE MRI Dr. Margaret Gallegos Radiologist Santa Fe Imaging Topics of today s talk How does prostate MRI work? Definition of multiparametric (mp) MRI Anatomy of prostate gland and MRI imaging Role
PROSTATE MRI Dr. Margaret Gallegos Radiologist Santa Fe Imaging Topics of today s talk How does prostate MRI work? Definition of multiparametric (mp) MRI Anatomy of prostate gland and MRI imaging Role
Elevated PSA. Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017
 Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
Providing Treatment Information for Prostate Cancer Patients
 Providing Treatment Information for Prostate Cancer Patients For all patients with localized disease on biopsy For all patients with adverse pathology after prostatectomy See what better looks like Contact
Providing Treatment Information for Prostate Cancer Patients For all patients with localized disease on biopsy For all patients with adverse pathology after prostatectomy See what better looks like Contact
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Prostate Cancer: from Beginning to End
 Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Patterns of care for prostate cancer An update
 Patterns of care for prostate cancer An update Daniel Moon Director of Robotic Surgery Epworth Healthcare Honorary Clinical Senior Lecturer University of Melbourne Consultant Urologist Peter MacCallum
Patterns of care for prostate cancer An update Daniel Moon Director of Robotic Surgery Epworth Healthcare Honorary Clinical Senior Lecturer University of Melbourne Consultant Urologist Peter MacCallum
Introduction. Original Article
 bs_bs_banner International Journal of Urology (2015) 22, 363 367 doi: 10.1111/iju.12704 Original Article Prostate-specific antigen level, stage or Gleason score: Which is best for predicting outcomes after
bs_bs_banner International Journal of Urology (2015) 22, 363 367 doi: 10.1111/iju.12704 Original Article Prostate-specific antigen level, stage or Gleason score: Which is best for predicting outcomes after
Controversies in Prostate Cancer Screening
 Controversies in Prostate Cancer Screening William J Catalona, MD Northwestern University Chicago Disclosure: Beckman Coulter, a manufacturer of PSA assays, provides research support PSA Screening Recommendations
Controversies in Prostate Cancer Screening William J Catalona, MD Northwestern University Chicago Disclosure: Beckman Coulter, a manufacturer of PSA assays, provides research support PSA Screening Recommendations
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
[PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK
![[PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK](/thumbs/82/85358853.jpg "[PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK") 06 March, 2018 [PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK Document Filetype: PDF 506.4 KB 0 [PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK See information on benefits and safety. We
06 March, 2018 [PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK Document Filetype: PDF 506.4 KB 0 [PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK See information on benefits and safety. We
Short summary of published results of PET with fluoromethylcholine (18F) in prostate cancer
 in prostate cancer") Short summary of published results of PET with fluoromethylcholine (18F) in prostate cancer JN TALBOT and all the team of Service de Médecine Nucléaire Hôpital Tenon et Université Pierre et Marie Curie,
Short summary of published results of PET with fluoromethylcholine (18F) in prostate cancer JN TALBOT and all the team of Service de Médecine Nucléaire Hôpital Tenon et Université Pierre et Marie Curie,
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Cytoreductive Radical Prostatectomy for de Novo Metastatic Prostate Cancer
 Cytoreductive Radical Prostatectomy for de Novo Metastatic Prostate Cancer Timothy G. Wilson, MD Professor and Chair of Urology John Wayne Cancer Institute Santa Monica, California Disclosures I am on
Cytoreductive Radical Prostatectomy for de Novo Metastatic Prostate Cancer Timothy G. Wilson, MD Professor and Chair of Urology John Wayne Cancer Institute Santa Monica, California Disclosures I am on
BLADDER PROSTATE PENIS TESTICLES BE YO ND YO UR CA NC ER
 BLADDER PROSTATE PENIS TESTICLES THE PROSTATE IS A SMALL, WALNUT-SIZED GLAND THAT IS PART OF THE MALE REPRODUCTIVE SYSTEM. IT RESTS BELOW THE BLADDER, IN FRONT OF THE RECTUM AND SURROUNDS PART OF THE URETHRA.
BLADDER PROSTATE PENIS TESTICLES THE PROSTATE IS A SMALL, WALNUT-SIZED GLAND THAT IS PART OF THE MALE REPRODUCTIVE SYSTEM. IT RESTS BELOW THE BLADDER, IN FRONT OF THE RECTUM AND SURROUNDS PART OF THE URETHRA.
VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE. ELENA CASTRO Spanish National Cancer Research Centre
 VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 17-18 October 2017 Prostate Specific Antigen (PSA) has a role in:
VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 17-18 October 2017 Prostate Specific Antigen (PSA) has a role in:
Overview. What is Cancer? Prostate Cancer 3/2/2014. Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014
 Prostate Cancer Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014 Overview Start with the basics: Definition of cancer Most common cancers in men Prostate, lung, and colon cancers Cancer
Prostate Cancer Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014 Overview Start with the basics: Definition of cancer Most common cancers in men Prostate, lung, and colon cancers Cancer
How will new biomarkers change prostate cancer management
 How will new biomarkers change prostate cancer management Matthew R. Cooperberg, MD, MPH Departments of Urology and Epidemiology & Biostatistics BAUS Section of Oncology Annual Meeting Cardiff, UK 15 November
How will new biomarkers change prostate cancer management Matthew R. Cooperberg, MD, MPH Departments of Urology and Epidemiology & Biostatistics BAUS Section of Oncology Annual Meeting Cardiff, UK 15 November
Financial and Other Disclosures
 Financial and Other Disclosures Off-label use of drugs, devices, or other agents: None Data from IRB-approved human research is not presented I have the following financial interests or relationships to
Financial and Other Disclosures Off-label use of drugs, devices, or other agents: None Data from IRB-approved human research is not presented I have the following financial interests or relationships to
CLINICAL TRIALS Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Prostate Cancer Basics: Background Information for Outreach Activities with Oncologists, Urologists and Surgeons
 Prostate Cancer Basics: Background Information for Outreach Activities with Oncologists, Urologists and Surgeons Legal Disclaimer These materials were prepared in good faith by MITA as a service to the
Prostate Cancer Basics: Background Information for Outreach Activities with Oncologists, Urologists and Surgeons Legal Disclaimer These materials were prepared in good faith by MITA as a service to the
EVIDENCE SUPPORTING TESTOSTERONE THERAPY IN MEN WITH PROSTATE CANCER
 EVIDENCE SUPPORTING TESTOSTERONE THERAPY IN MEN WITH PROSTATE CANCER Abraham Morgentaler, MD Director and Founder Men s Health Boston Associate Clinical Professor Harvard Medical School And the Urology
EVIDENCE SUPPORTING TESTOSTERONE THERAPY IN MEN WITH PROSTATE CANCER Abraham Morgentaler, MD Director and Founder Men s Health Boston Associate Clinical Professor Harvard Medical School And the Urology
Correspondence should be addressed to Taha Numan Yıkılmaz;
 Advances in Medicine Volume 2016, Article ID 8639041, 5 pages http://dx.doi.org/10.1155/2016/8639041 Research Article External Validation of the Cancer of the Prostate Risk Assessment Postsurgical Score
Advances in Medicine Volume 2016, Article ID 8639041, 5 pages http://dx.doi.org/10.1155/2016/8639041 Research Article External Validation of the Cancer of the Prostate Risk Assessment Postsurgical Score
The Selenium and Vitamin E Prevention Trial
 The largest-ever-prostate cancer prevention trial is now underway. The study will include a total of 32,400 men and is sponsored by the National Cancer Institute and a network of researchers known as the
The largest-ever-prostate cancer prevention trial is now underway. The study will include a total of 32,400 men and is sponsored by the National Cancer Institute and a network of researchers known as the
Prostate Cancer: Screening, Treatment, and Survivorship
 Prostate Cancer: Screening, Treatment, and Survivorship Timothy C. Brand, MD, FACS LTC(P), MC, USA Urology Residency Director Associate Professor of Surgery, USUHS Madigan Army Medical Center No Disclosures
Prostate Cancer: Screening, Treatment, and Survivorship Timothy C. Brand, MD, FACS LTC(P), MC, USA Urology Residency Director Associate Professor of Surgery, USUHS Madigan Army Medical Center No Disclosures
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
How to detect and investigate Prostate Cancer before TRT
 How to detect and investigate Prostate Cancer before TRT Frans M.J. Debruyne Professor of Urology Andros Men s Health Institutes, The Netherlands Bruges, 25-26 September 2014 PRISM Recommendations for
How to detect and investigate Prostate Cancer before TRT Frans M.J. Debruyne Professor of Urology Andros Men s Health Institutes, The Netherlands Bruges, 25-26 September 2014 PRISM Recommendations for
2015 myresearch Science Internship Program: Applied Medicine. Civic Education Office of Government and Community Relations
 2015 myresearch Science Internship Program: Applied Medicine Civic Education Office of Government and Community Relations Harguneet Singh Science Internship Program: Applied Medicine Comparisons of Outcomes
2015 myresearch Science Internship Program: Applied Medicine Civic Education Office of Government and Community Relations Harguneet Singh Science Internship Program: Applied Medicine Comparisons of Outcomes
Oligometastasis. Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie?
 Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
PET/CT imaging and RIT of prostate cancer. Kirsten Bouchelouche, MD, DMSc PET & Cyclotron Unit Rigshospitalet, Copenhagen Denmark
 PET/CT imaging and RIT of prostate cancer Kirsten Bouchelouche, MD, DMSc PET & Cyclotron Unit Rigshospitalet, Copenhagen Denmark Prostate cancer Prostate cancer is the most common malignancy in men Imaging
PET/CT imaging and RIT of prostate cancer Kirsten Bouchelouche, MD, DMSc PET & Cyclotron Unit Rigshospitalet, Copenhagen Denmark Prostate cancer Prostate cancer is the most common malignancy in men Imaging