Conceptual basis for active surveillance
|
|
|
- Jasper Ford
- 5 years ago
- Views:
Transcription
1 Conceptual basis for active surveillance 1. Screening results in overdiagnosis 2. Clinically insignificant disease can be identified 3. All treatments have significant side effects and cost. 4. Delayed radical treatment is still curative. 5. The psychological burden is acceptable (less than the effects of overtreatment).
2 The Screening Problem: U.S. Example Welch JNCI 2005:97: Biopsy of all men with PSA > 2.5: Result in 775,000 diagnosed cases, 3 x higher than current incidence This is 25 times the 30,350 Prostate Cancer deaths per year in the US!
3 PSA testing in US men 75% of men and 87% of male MDs have had a PSA 50% tested regularly Lifetime risk of diagnosis 19% (from 10% in pre PSA era) >90% treated radically
4 Overtreatment is common Studies of non-screen detected men Albertsen Johannson SPCGS-4 PSA era studies Cancer registries PCPT ESRPC

5 20-Year Outcomes Following Conservative Management of Clinically Localized Prostate Cancer Albertsen P et al, JAMA. 2005;293: Gleason score shift Lead Time effect Years
6 ESRPC: % of indolent cancer at surgery PSA 1 st screen 2 nd screen < > Total 33 43
7 Estimates of overdiagnosis: Draisma 2007 T1 69% T2 38% T3 30% Gleason < 7 62% 7 40% >7 8%
8 Candidates for active surveillance 60% of new cases are Gleason 5-6 (CapSure) 80% PSA 10 65% T1c, 25% T2a Thus 45-50% of newly diagnosed cases are favorable risk About 50% of these fulfill criteria for insignificant prostate cancer One third of patients (85,000/year in US and Canada)
9 The three challenges of surveillance Identifying the right patient Communicating safety ( cancer hysteria ) Trigger for intervention Timely treatment for patients reclassified as high risk Avoid jumping the gun
10 Surveillance therapy with selective delayed intervention Favorable risk (D Amico): Gleason 6 PSA 10 T1c/T2a In younger patients 1/3 cores positive < 50% involvement of all cores If available, PSA DT > 3 years or PSA velocity < 2.0 ng/ml/year Hypothesis: Most can be observed Delayed treatment effective in those whose disease appears to be higher risk over time

11 Animals in the barnyard and cancer natural history Only the rabbits benefit from early diagnosis and treatment.
12 Identifying the rabbits: the controversies PSA kinetics Reliability (? too late) Interpretation (Velocity vs doubling time) How to calculate Biopsy How often, how many cores Trigger for intervention: extent/volume/grade shift
13 Identifying the rabbits: Toronto approach Rapid PSA doubling time PSA every 3 months x 2 years then every 6 months Usually decision to intervene at 2 years, 8-9 PSAs PSA DT < 3 years (20% of patients) Gleason grade progression Biopsy at 1 year (confirmatory) Then every 4 years (progression) Treat if Gleason 4+3 or worse (5% of patients) Unequivocal clinical progression to T3 (3%) Guidelines, not rules
14 Distribution of PSA doubling times in 331 patients on surveillance. Choo, Klotz J Urol % Median < >100 PSA Doubling time
15 Overall and disease specific survival in Toronto surveillance cohort (adapted from Klotz L, J Clin Oncol Nov 10;23(32):8165-9) Overall Survival (n = 331) Cause Specific Survival (n = 331) Survival distribution function (100 %) P=0.51 Low risk of progression High risk of progression Survival distribution function (100 %) P=0.05 Low risk of progression High risk of progression Time (years) Time (years)
16 The problem of calculating PSA DT FLO: First and last months observation BLF: Best line fit
17 General Linear Mixed Modeling Allows for individual predictors of intercept and slope to be integrated into model Aggregate estimate of variation used to reduce effect of individual PSA variation on PSA DT calculation For high risk line: ln(psa) = ln(baseline PSA) time time2 For low risk line: ln(psa) = 1.03 ln(baseline PSA) Age Gleason time time2 Zhang L, Loblaw DA, Klotz L. J Urol 2006
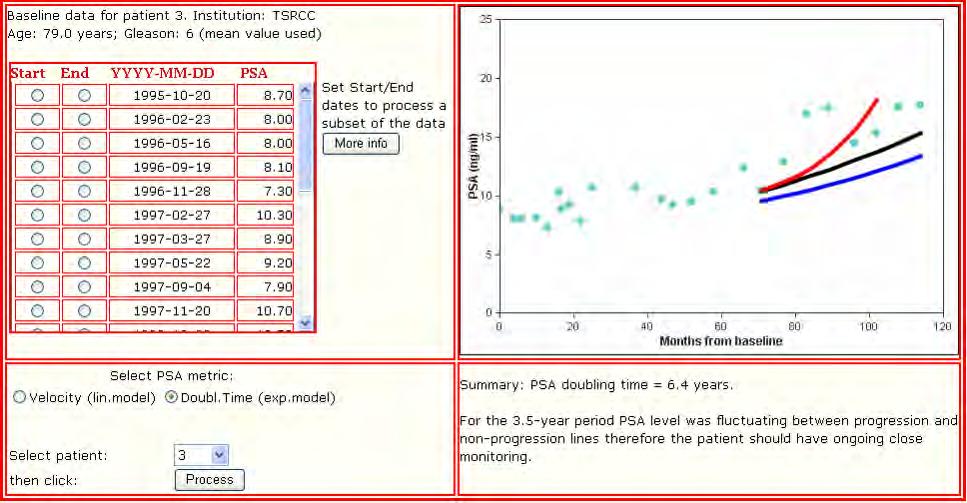
18 High risk Intervene Intermediate: continue close follow up A B 20 High risk 20 PSA (ng/ml) Low risk PSA (ng/ml) High risk 0 0 Low risk Time (years) Time (years) PSA (ng/ml) C High risk Low risk Low risk: relax follow up GLMM approach to PSA DT during active surveillance Time (years)
19
20 Effect of PSA triggers on stable patient cohort General linear mixed model of ln(psa) 0% PSA threshold > 10 15% Linear regression of ln(psa) vs time < 2yr 39% Ln(PSA) vs time < 2 years using first and last PSA 29% Actual PSA velocity > % Calculated PSA velocity > %
21 PSA DT and surveillance: Khatam A, Hugusson Int J Cancer 120, (2006) 270 active surveillance (from Swedish arm of ESRCP) 39% treated 70 RPs 9 (12%) PSA relapse 80% of these had PSA DT < 2 years 0/37 with PSA DT > 4 years relapsed 14 deaths (5%); 0 from PCa No metastatic progression
22 Williams SK, Soloway M AUA 2007 Ab favorable risk patients managed with Toronto approach 99 with > 1 yr f/u, median 4 yrs Mean age 66 Mean PSA 5.7 Intervention 8%: 2 RP, 3 XRT, 3 ADT Mean PSA DT Untreated 13.1 yrs Treated 3.6 yrs 5 year PFS 85% PCa survival 100%
23 Modelling the risk: A number needed to treat analysis
24 The Scandinavian trial Bill-Axelson 2005 Holmberg 2006 Mortality reduction at 10 years NNT All 5% 20 <65 11% % >300
25 A 50% risk reduction may yield little clinical benefit Clinically insignificant Disease Cured by therapy Death from disease
26 Swedish cohort differed from patients diagnosed in 2006 Swedish trial Mean age 64.7 Mean PSA % screen detected 75% T2 40% Gleason 7 or higher Typical screen diagnosed patient Mean age 62 Mean PSA 6 95% screen detected 70% T1c 60% Gleason 6 Volume migration
27 Unanswered question: NNT for Low grade Small volume Screen detected Option of selective delayed therapy
28 NNT for each cancer death avoided at 20 years for favorable risk prostate cancer: RP vs surveillance Swedish trial Swedish trial Lead time in screened Corrected for 10 years 20 years (estimate) population 20 years grade difference Include salvage opportunity 80
29 Predicted survival - conservative management of screen-detected prostate cancer Parker et al. BJC (2006)



30 Why Men Don t Want to Wait
31 Cancer Hysteria: Who benefits? Fundraising Cancer Societies Cancer Research organizations Physicians Researchers Other health care workers in the cancer field Media Environmental activists
32 Who is Disadvantaged by Cancer Hysteria? The patient
33 Fear is a Danger to Your Health Cancer and sense of doom The dread expands and solidifies into such a major obstacle that I simply can t get past it. Patients may feel so hopeless that they can t absorb the medical facts
34 Communicating Risk The first step in positive thinking is to be able to understand what s actually going on. Positive thinking begins with clear thinking. -a Patient
35 Our challenge I will remember that there is an art to medicine as well as science in that warmth, sympathy and understanding may outweigh the surgeon s knife or the chemist s drug. -Louis Lasagna, Academic Dean of the School of Medicine at Tufts University, 1964
36 The Crucial Question: What do you want from the rest of your life?
37 Our Responsibility Reassure and offer hope Put the risk in perspective De-mystify the word Cancer Provide accurate data (use facts) Help the patient think clearly about the risks and benefits Avoid exploiting the patient s fears Primum non nocere
38 Risk Assessment
39 A Phase III Study of Surveillance Therapy Against Radical Treatment (START) in patients Diagnosed with Favourable Risk Prostate Cancer NCIC CTG Protocol Number: PR.11 SWOG/ECOG/CALGB/RTOG/UKCCR Study to open 2Q 2007 (any day now!)
40 START Trial Schema Randomize (within 6 months of initial diagnosis) ARM 1: Radical intervention (radical prostatectomy or radiotherapy based on patient and physician preference) Prostate cancer death ARM 2: Active surveillance with radical intervention for either Biochemical progression Grade progression Clinical progression


41 Points Biomarker Discovery Preop PSA Gleason Sum Extraprostatic Ext. Surgical Margins Seminal Ves. Invasion Lymph Nodes Total Points Inv.Capsule Established None Focal Pos Neg Yes No Pos Neg Serum Bank 84-Month Rec. Free Prob Serial Biopsy Bank Validation of Nomograms START Trial Natural History Data Base Global Study 2100 pts Correlative Sciences
42 Thank You
J Clin Oncol 28: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 28 NUMBER 1 JANUARY 1 2010 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Clinical Results of Long-Term Follow-Up of a Large, Active Surveillance Cohort With Localized Prostate Cancer
VOLUME 28 NUMBER 1 JANUARY 1 2010 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Clinical Results of Long-Term Follow-Up of a Large, Active Surveillance Cohort With Localized Prostate Cancer
Pre-test. Prostate Cancer The Good News: Prostate Cancer Screening 2012: Putting the PSA Controversy to Rest
 Pre-test Matthew R. Cooperberg, MD, MPH UCSF 40 th Annual Advances in Internal Medicine Prostate Cancer Screening 2012: Putting the PSA Controversy to Rest 1. I do not offer routine PSA screening, and
Pre-test Matthew R. Cooperberg, MD, MPH UCSF 40 th Annual Advances in Internal Medicine Prostate Cancer Screening 2012: Putting the PSA Controversy to Rest 1. I do not offer routine PSA screening, and
Controversies in Prostate Cancer Screening
 Controversies in Prostate Cancer Screening William J Catalona, MD Northwestern University Chicago Disclosure: Beckman Coulter, a manufacturer of PSA assays, provides research support PSA Screening Recommendations
Controversies in Prostate Cancer Screening William J Catalona, MD Northwestern University Chicago Disclosure: Beckman Coulter, a manufacturer of PSA assays, provides research support PSA Screening Recommendations
Urological Society of Australia and New Zealand PSA Testing Policy 2009
 Executive summary Urological Society of Australia and New Zealand PSA Testing Policy 2009 1. Prostate cancer is a major health problem and is the second leading cause of male cancer deaths in Australia
Executive summary Urological Society of Australia and New Zealand PSA Testing Policy 2009 1. Prostate cancer is a major health problem and is the second leading cause of male cancer deaths in Australia
AUA Update Series. Lesson 33 Volume Active Surveillance for Prostate Cancer: Patient Selection and Management
 AUA Update Series Lesson 33 Volume 27 2008 Active Surveillance for Prostate Cancer: Patient Selection and Management Learning Objective: At the conclusion of this continuing medical education activity,
AUA Update Series Lesson 33 Volume 27 2008 Active Surveillance for Prostate Cancer: Patient Selection and Management Learning Objective: At the conclusion of this continuing medical education activity,
PROSTATE CANCER SURVEILLANCE
 PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Long-Term Follow-Up of a Large Active Surveillance Cohort of Patients With Prostate Cancer
 Published Ahead of Print on December 15, 1 as 1.1/JCO.1.55.119 The latest version is at http://jco.ascopubs.org/cgi/doi/1.1/jco.1.55.119 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Long-Term
Published Ahead of Print on December 15, 1 as 1.1/JCO.1.55.119 The latest version is at http://jco.ascopubs.org/cgi/doi/1.1/jco.1.55.119 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Long-Term
Prostate Cancer Screening: Risks and Benefits across the Ages
 Prostate Cancer Screening: Risks and Benefits across the Ages 7 th Annual Symposium on Men s Health Continuing Progress: New Gains, New Challenges June 10, 2009 Michael J. Barry, MD General Medicine Unit
Prostate Cancer Screening: Risks and Benefits across the Ages 7 th Annual Symposium on Men s Health Continuing Progress: New Gains, New Challenges June 10, 2009 Michael J. Barry, MD General Medicine Unit
Sommerakademie Munich, June
 Active surveillance: Shrinking the grey zone Sommerakademie Munich, June 30 2016 Active surveillance Overview of 20 year history Laurence Klotz, MD, CM Professor of Surgery Sunnybrook Heatlh Sciences Centre
Active surveillance: Shrinking the grey zone Sommerakademie Munich, June 30 2016 Active surveillance Overview of 20 year history Laurence Klotz, MD, CM Professor of Surgery Sunnybrook Heatlh Sciences Centre
ACTIVE SURVEILLANCE FOR PROSTATE CANCER
 ACTIVE SURVEILLANCE FOR PROSTATE CANCER Dr. Michael J Metcalfe PGY-2 Department of Urological Sciences April 25, 2012 CASE RM 65 year old active Caucasian male, married. PSA= 7.0 T2a Gleason 3+3=6 2/6
ACTIVE SURVEILLANCE FOR PROSTATE CANCER Dr. Michael J Metcalfe PGY-2 Department of Urological Sciences April 25, 2012 CASE RM 65 year old active Caucasian male, married. PSA= 7.0 T2a Gleason 3+3=6 2/6
Prostate Cancer. Axiom. Overdetection Is A Small Issue. Reducing Morbidity and Mortality
 Overdetection Is A Small Issue (in the context of decreasing prostate cancer mortality rates and with appropriate, effective, and high-quality treatment) Prostate Cancer Arises silently Dwells in a curable
Overdetection Is A Small Issue (in the context of decreasing prostate cancer mortality rates and with appropriate, effective, and high-quality treatment) Prostate Cancer Arises silently Dwells in a curable
PROSTATE CANCER Amit Gupta MD MPH
 PROSTATE CANCER Amit Gupta MD MPH Depts. of Urology and Epidemiology Amit-Gupta-1@uiowa.edu dramitgupta@gmail.com Tel: 319-384-5251 OUTLINE PSA screening controversy How to use PSA more effectively Treatment
PROSTATE CANCER Amit Gupta MD MPH Depts. of Urology and Epidemiology Amit-Gupta-1@uiowa.edu dramitgupta@gmail.com Tel: 319-384-5251 OUTLINE PSA screening controversy How to use PSA more effectively Treatment
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Prostate Cancer Screening: Con. Laurence Klotz Professor of Surgery, Sunnybrook HSC University of Toronto
 Prostate Cancer Screening: Con Laurence Klotz Professor of Surgery, Sunnybrook HSC University of Toronto / Why not PSA screening? Overdiagnosis Overtreatment Risk benefit ratio unfavorable Flaws of PSA
Prostate Cancer Screening: Con Laurence Klotz Professor of Surgery, Sunnybrook HSC University of Toronto / Why not PSA screening? Overdiagnosis Overtreatment Risk benefit ratio unfavorable Flaws of PSA
Prostate Cancer Innovations in Surgical Strategies Update 2007!
 Prostate Cancer Innovations in Surgical Strategies Update 2007! Curtis A. Pettaway, M.D. Professor Department of Urology The University of Texas M. D. Anderson Cancer Center Radical Prostatectomy Pathologic
Prostate Cancer Innovations in Surgical Strategies Update 2007! Curtis A. Pettaway, M.D. Professor Department of Urology The University of Texas M. D. Anderson Cancer Center Radical Prostatectomy Pathologic
Sorveglianza Attiva update
 Sorveglianza Attiva update Dr. Sergio Villa Dr. Riccardo Valdagni www.thelancet.com Published online August 7, 2014 http://dx.doi.org/10.1016/s0140-6736(14)60525-0 the main weakness of screening is a high
Sorveglianza Attiva update Dr. Sergio Villa Dr. Riccardo Valdagni www.thelancet.com Published online August 7, 2014 http://dx.doi.org/10.1016/s0140-6736(14)60525-0 the main weakness of screening is a high
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Active Surveillance for Intermediate Risk Prostate Cancer
 Active Surveillance for Intermediate Risk Prostate Cancer Eric Wallen, M.D., FACS Professor Department of Urology The University of North Carolina at Chapel Hill Disclosures: None Objectives Understand
Active Surveillance for Intermediate Risk Prostate Cancer Eric Wallen, M.D., FACS Professor Department of Urology The University of North Carolina at Chapel Hill Disclosures: None Objectives Understand
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
Prostate Cancer Incidence
 Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Risk Migration ( ct2c=high)
") Risk Migration ( ctc=high) Prostate Cancer Over- Detection, but Selective Treatment Active Surveillance Peter R. Carroll, MD, MPH Department of Urology University of California, San Francisco February,
Risk Migration ( ctc=high) Prostate Cancer Over- Detection, but Selective Treatment Active Surveillance Peter R. Carroll, MD, MPH Department of Urology University of California, San Francisco February,
Detection & Risk Stratification for Early Stage Prostate Cancer
 Detection & Risk Stratification for Early Stage Prostate Cancer Andrew J. Stephenson, MD, FRCSC, FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Risk Stratification:
Detection & Risk Stratification for Early Stage Prostate Cancer Andrew J. Stephenson, MD, FRCSC, FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Risk Stratification:
When radical prostatectomy is not enough: The evolving role of postoperative
 When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
To be covered. Screening, early diagnosis, and treatment including Active Surveillance for prostate cancer: where is Europe heading for?
 To be covered Screening, early diagnosis, and treatment including Active Surveillance for prostate cancer: where is Europe heading for? Europa Uomo meeting Stockholm 29 Chris H.Bangma Rotterdam, The Netherlands
To be covered Screening, early diagnosis, and treatment including Active Surveillance for prostate cancer: where is Europe heading for? Europa Uomo meeting Stockholm 29 Chris H.Bangma Rotterdam, The Netherlands
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia
 Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Since the beginning of the prostate-specific antigen (PSA) era in the. Characteristics of Insignificant Clinical T1c Prostate Tumors
 era in the. Characteristics of Insignificant Clinical T1c Prostate Tumors") 2001 Characteristics of Insignificant Clinical T1c Prostate Tumors A Contemporary Analysis Patrick J. Bastian, M.D. 1 Leslie A. Mangold, B.A., M.S. 1 Jonathan I. Epstein, M.D. 2 Alan W. Partin, M.D., Ph.D.
2001 Characteristics of Insignificant Clinical T1c Prostate Tumors A Contemporary Analysis Patrick J. Bastian, M.D. 1 Leslie A. Mangold, B.A., M.S. 1 Jonathan I. Epstein, M.D. 2 Alan W. Partin, M.D., Ph.D.
Active Surveillance with High Resolution Color-Doppler Transrectal Ultrasound Monitoring: Is it fool-proof?
 Active Surveillance with High Resolution Color-Doppler Transrectal Ultrasound Monitoring: Is it fool-proof? Duke Bahn MD Prostate Institute of America, Ventura, California INTRODUCTION In the November
Active Surveillance with High Resolution Color-Doppler Transrectal Ultrasound Monitoring: Is it fool-proof? Duke Bahn MD Prostate Institute of America, Ventura, California INTRODUCTION In the November
Prostate Cancer Who needs active surveillance?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller Prostate Cancer Who needs active surveillance? Klinische und molekulare Charakterisierung des Hoch-Risiko-Prostatakarzinoms.
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller Prostate Cancer Who needs active surveillance? Klinische und molekulare Charakterisierung des Hoch-Risiko-Prostatakarzinoms.
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Prostate MRI for local staging and surgical planning in prostate cancer
 Prostate MRI for local staging and surgical planning in prostate cancer 15th Annual Floyd A. Fried Advances in Urology Symposium June 23, 2017 Ray Tan, MD, MSHPM Assistant Professor Disclosures None Objectives
Prostate MRI for local staging and surgical planning in prostate cancer 15th Annual Floyd A. Fried Advances in Urology Symposium June 23, 2017 Ray Tan, MD, MSHPM Assistant Professor Disclosures None Objectives
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Prostate Cancer: from Beginning to End
 Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015
 Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
ACTIVE SURVEILLANCE OR WATCHFUL WAITING
 Prostate Cancer ACTIVE SURVEILLANCE OR WATCHFUL WAITING María Teresa Bourlon, MD MS Head, Urologic Oncology Clinic Hemato-Oncology Department Instituto Nacional de Ciencias Médicas y Nutrición Salvador
Prostate Cancer ACTIVE SURVEILLANCE OR WATCHFUL WAITING María Teresa Bourlon, MD MS Head, Urologic Oncology Clinic Hemato-Oncology Department Instituto Nacional de Ciencias Médicas y Nutrición Salvador
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Active surveillance: Shrinking the grey zone. Sommerakademi e Munich, June rd FOIUS Tel Aviv, July 2016
 Active surveillance: Shrinking the grey zone Active surveillance: 3 rd FOIUS Tel Aviv, July 2016 Shrinking the grey zone Sommerakademi e Munich, June 30 2016 Active Surveillance for low risk PCa What has
Active surveillance: Shrinking the grey zone Active surveillance: 3 rd FOIUS Tel Aviv, July 2016 Shrinking the grey zone Sommerakademi e Munich, June 30 2016 Active Surveillance for low risk PCa What has
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
Active Surveillance (AS) is an expectant management. Health Services Research
 is an expectant management. Health Services Research") Factors Influencing Selection of Active Surveillance for Localized Prostate Cancer Health Services Research Jianyu Liu, Paul R. Womble, Selin Merdan, David C. Miller, James E. Montie, Brian T. Denton on
Factors Influencing Selection of Active Surveillance for Localized Prostate Cancer Health Services Research Jianyu Liu, Paul R. Womble, Selin Merdan, David C. Miller, James E. Montie, Brian T. Denton on
NIH Public Access Author Manuscript World J Urol. Author manuscript; available in PMC 2012 February 1.
 NIH Public Access Author Manuscript Published in final edited form as: World J Urol. 2011 February ; 29(1): 11 14. doi:10.1007/s00345-010-0625-4. Significance of preoperative PSA velocity in men with low
NIH Public Access Author Manuscript Published in final edited form as: World J Urol. 2011 February ; 29(1): 11 14. doi:10.1007/s00345-010-0625-4. Significance of preoperative PSA velocity in men with low
Predictive Models. Michael W. Kattan, Ph.D. Department of Quantitative Health Sciences and Glickman Urologic and Kidney Institute
 Predictive Models Michael W. Kattan, Ph.D. Department of Quantitative Health Sciences and Glickman Urologic and Kidney Institute Treatment for clinically localized prostate cancer Trade off: Substantial
Predictive Models Michael W. Kattan, Ph.D. Department of Quantitative Health Sciences and Glickman Urologic and Kidney Institute Treatment for clinically localized prostate cancer Trade off: Substantial
Prostate Cancer Screening. Eric Shreve, MD Bend Urology Associates
 Prostate Cancer Screening Eric Shreve, MD Bend Urology Associates University of Cincinnati Medical Center University of Iowa Hospitals and Clinics PSA Human kallikrein 3 Semenogelin is substrate Concentration
Prostate Cancer Screening Eric Shreve, MD Bend Urology Associates University of Cincinnati Medical Center University of Iowa Hospitals and Clinics PSA Human kallikrein 3 Semenogelin is substrate Concentration
The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy. Dr. Matt Andrews Supervisor: Dr. David Bowes
 The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy Dr. Matt Andrews Supervisor: Dr. David Bowes Objectives Discuss the evidence for adjuvant radiotherapy (ART) EORTC, SWOG, ARO Current
The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy Dr. Matt Andrews Supervisor: Dr. David Bowes Objectives Discuss the evidence for adjuvant radiotherapy (ART) EORTC, SWOG, ARO Current
PSA testing in New Zealand general practice
 PSA testing in New Zealand general practice Ross Lawrenson, Charis Brown, Fraser Hodgson. On behalf of the Midland Prostate Cancer Study Group Academic Steering Goup: Zuzana Obertova, Helen Conaglen, John
PSA testing in New Zealand general practice Ross Lawrenson, Charis Brown, Fraser Hodgson. On behalf of the Midland Prostate Cancer Study Group Academic Steering Goup: Zuzana Obertova, Helen Conaglen, John
Early outcomes of active surveillance for localized prostate cancer
 Original Article ACTIVE SURVEILLANCE FOR LOCALIZED PROSTATE CANCER HARDIE et al. Early outcomes of active surveillance for localized prostate cancer CLAIRE HARDIE, CHRIS PARKER, ANDREW NORMAN*, ROS EELES,
Original Article ACTIVE SURVEILLANCE FOR LOCALIZED PROSTATE CANCER HARDIE et al. Early outcomes of active surveillance for localized prostate cancer CLAIRE HARDIE, CHRIS PARKER, ANDREW NORMAN*, ROS EELES,
PSA Screening and Prostate Cancer. Rishi Modh, MD
 PSA Screening and Prostate Cancer Rishi Modh, MD ABOUT ME From Tampa Bay Went to Berkeley Prep University of Miami for Undergraduate - 4 years University of Miami for Medical School - 4 Years University
PSA Screening and Prostate Cancer Rishi Modh, MD ABOUT ME From Tampa Bay Went to Berkeley Prep University of Miami for Undergraduate - 4 years University of Miami for Medical School - 4 Years University
Active surveillance for prostate cancer: patient selection and management
 UROLOGIC ONCOLOGY Active surveillance for prostate cancer: patient selection and management L. Klotz md ABSTRACT Screening for prostate cancer using prostate-specific antigen (psa) has been appealing.
UROLOGIC ONCOLOGY Active surveillance for prostate cancer: patient selection and management L. Klotz md ABSTRACT Screening for prostate cancer using prostate-specific antigen (psa) has been appealing.
Active surveillance for low-risk Prostate Cancer Compared with Immediate Treatment: A Canadian cost evaluation
 Active surveillance for low-risk Prostate Cancer Compared with Immediate Treatment: A Canadian cost evaluation Alice Dragomir, PhD Fabio Cury, MD Armen Aprikian, MD Introduction Clinical and economic burden
Active surveillance for low-risk Prostate Cancer Compared with Immediate Treatment: A Canadian cost evaluation Alice Dragomir, PhD Fabio Cury, MD Armen Aprikian, MD Introduction Clinical and economic burden
Appreciating the Natural History of Prostate Cancer in 2005: The Art of Medicine
 Appreciating the Natural History of Prostate Cancer in 2: The Art of Medicine Larry Goldenberg, MD, FRCSC, FACS The Prostate Centre at VGH, University of British Columbia, Vancouver, Canada Prostate Cancer:
Appreciating the Natural History of Prostate Cancer in 2: The Art of Medicine Larry Goldenberg, MD, FRCSC, FACS The Prostate Centre at VGH, University of British Columbia, Vancouver, Canada Prostate Cancer:
Published Ahead of Print on April 4, 2011 as /JCO J Clin Oncol by American Society of Clinical Oncology INTRODUCTION
 Published Ahead of Print on April 4, 2011 as 10.1200/JCO.2010.32.8112 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2010.32.8112 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E
Published Ahead of Print on April 4, 2011 as 10.1200/JCO.2010.32.8112 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2010.32.8112 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E
Untreated Gleason Grade Progression on Serial Biopsies during Prostate Cancer Active Surveillance: Clinical Course and Pathological Outcomes
 Untreated Gleason Grade Progression on Serial Biopsies during Prostate Cancer Active Surveillance: Clinical Course and Pathological Outcomes A. A. Hussein,* C. J. Welty,* N. Ameli,* J. E. Cowan, M. Leapman,*
Untreated Gleason Grade Progression on Serial Biopsies during Prostate Cancer Active Surveillance: Clinical Course and Pathological Outcomes A. A. Hussein,* C. J. Welty,* N. Ameli,* J. E. Cowan, M. Leapman,*
Providing Treatment Information for Prostate Cancer Patients
 Providing Treatment Information for Prostate Cancer Patients For all patients with localized disease on biopsy For all patients with adverse pathology after prostatectomy See what better looks like Contact
Providing Treatment Information for Prostate Cancer Patients For all patients with localized disease on biopsy For all patients with adverse pathology after prostatectomy See what better looks like Contact
Using Markov Models to Estimate the Impact of New Prostate Cancer Biomarkers
 Using Markov Models to Estimate the Impact of New Prostate Cancer Biomarkers Brian Denton, PhD Associate Professor Department of Industrial and Operations Engineering February 23, 2016 Industrial and Operations
Using Markov Models to Estimate the Impact of New Prostate Cancer Biomarkers Brian Denton, PhD Associate Professor Department of Industrial and Operations Engineering February 23, 2016 Industrial and Operations
Prostate Cancer Local or distant recurrence?
 Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Low risk. Objectives. Case-based question 1. Evidence-based utilization of imaging in prostate cancer
 Evidence-based utilization of imaging in prostate cancer Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Objectives State the modalities,
Evidence-based utilization of imaging in prostate cancer Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Objectives State the modalities,
Navigating the Stream: Prostate Cancer and Early Detection. Ifeanyi Ani, M.D. TPMG Urology Newport News
 Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
MATERIALS AND METHODS
 Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline Very Low-/Low-Risk Disease
 Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline Very Low-/Low-Risk Disease Jeffrey A. Cadeddu, MD Professor, Department of Urology UT Southwestern Medical Center Vice-Chair, AUA/ASTRO/SUO
Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline Very Low-/Low-Risk Disease Jeffrey A. Cadeddu, MD Professor, Department of Urology UT Southwestern Medical Center Vice-Chair, AUA/ASTRO/SUO
Reducing overtreatment of prostate cancer by radical prostatectomy in Eastern Ontario: a population-based cohort study
 Reducing overtreatment of prostate cancer by radical prostatectomy in Eastern Ontario: a population-based cohort study Luke Witherspoon MD MSc, Johnathan L. Lau BSc, Rodney H. Breau MD MSc, Christopher
Reducing overtreatment of prostate cancer by radical prostatectomy in Eastern Ontario: a population-based cohort study Luke Witherspoon MD MSc, Johnathan L. Lau BSc, Rodney H. Breau MD MSc, Christopher
Elevated PSA. Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017
 Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
Prostate Cancer Active Surveillance: Rationale, Outcomes and Future Directions
 Prostate Cancer Active Surveillance: Rationale, Outcomes and Future Directions Daniel W. Lin, MD Professor and Chief of Urologic Oncology Bridges Endowed Professorship of Prostate Cancer Research Department
Prostate Cancer Active Surveillance: Rationale, Outcomes and Future Directions Daniel W. Lin, MD Professor and Chief of Urologic Oncology Bridges Endowed Professorship of Prostate Cancer Research Department
BAYESIAN JOINT LONGITUDINAL-DISCRETE TIME SURVIVAL MODELS: EVALUATING BIOPSY PROTOCOLS IN ACTIVE-SURVEILLANCE STUDIES
 BAYESIAN JOINT LONGITUDINAL-DISCRETE TIME SURVIVAL MODELS: EVALUATING BIOPSY PROTOCOLS IN ACTIVE-SURVEILLANCE STUDIES Lurdes Y. T. Inoue, PhD Professor Department of Biostatistics University of Washington
BAYESIAN JOINT LONGITUDINAL-DISCRETE TIME SURVIVAL MODELS: EVALUATING BIOPSY PROTOCOLS IN ACTIVE-SURVEILLANCE STUDIES Lurdes Y. T. Inoue, PhD Professor Department of Biostatistics University of Washington
PCA MORTALITY VS TREATMENTS
 PCA MORTALITY VS TREATMENTS Terrence P McGarty White Paper No 145 July, 2017 In a recent NEJM paper the authors argue that there is no material difference between a prostatectomy and just "observation"
PCA MORTALITY VS TREATMENTS Terrence P McGarty White Paper No 145 July, 2017 In a recent NEJM paper the authors argue that there is no material difference between a prostatectomy and just "observation"
PSA test. PSA testing is not usually recommended for asymptomatic men with < 10 years life expectancy Before having a PSA test men should not have:
 PSA Debate PSA1 PSA2 PSA test PSA testing is not usually recommended for asymptomatic men with < 10 years life expectancy Before having a PSA test men should not have: had a DRE in the previous week. an
PSA Debate PSA1 PSA2 PSA test PSA testing is not usually recommended for asymptomatic men with < 10 years life expectancy Before having a PSA test men should not have: had a DRE in the previous week. an
State-of-the-art: vision on the future. Urology
 State-of-the-art: vision on the future Urology Francesco Montorsi MD FRCS Professor and Chairman Department of Urology San Raffaele Hospital Vita-Salute San Raffaele University Milan, Italy Disclosures
State-of-the-art: vision on the future Urology Francesco Montorsi MD FRCS Professor and Chairman Department of Urology San Raffaele Hospital Vita-Salute San Raffaele University Milan, Italy Disclosures
Contemporary Approaches to Screening for Prostate Cancer
 Contemporary Approaches to Screening for Prostate Cancer Gerald L. Andriole, MD Robert K. Royce Distinguished Professor Chief of Urologic Surgery Siteman Cancer Center Washington University School of Medicine
Contemporary Approaches to Screening for Prostate Cancer Gerald L. Andriole, MD Robert K. Royce Distinguished Professor Chief of Urologic Surgery Siteman Cancer Center Washington University School of Medicine
How do I control (monitor) patients receiving TRT after prostate cancer treatment
 patients receiving TRT after prostate cancer treatment") How do I control (monitor) patients receiving TRT after prostate cancer treatment Anthony J. Bella MD, FRCSC Greta and John Hansen Chair in Men s Health Research Division of Urology, Department of Surgery
How do I control (monitor) patients receiving TRT after prostate cancer treatment Anthony J. Bella MD, FRCSC Greta and John Hansen Chair in Men s Health Research Division of Urology, Department of Surgery
High Intensity Focused Ultrasounds for the treatment of Prostate Cancers Clinical update November D. Maruzzi - L. Ruggera
 High Intensity Focused Ultrasounds for the treatment of Prostate Cancers Clinical update November 2014 D. Maruzzi - L. Ruggera HIFU development Second prototype 1995-2000 Integrated Imaging 2006-2010 1993
High Intensity Focused Ultrasounds for the treatment of Prostate Cancers Clinical update November 2014 D. Maruzzi - L. Ruggera HIFU development Second prototype 1995-2000 Integrated Imaging 2006-2010 1993
Should A PSA threshold of 1.5 ng/ml be the threshold for further diagnostic tests?
 Should A PSA threshold of 1.5 ng/ml be the threshold for further diagnostic tests? Hanan Goldberg, MD Princess Margaret Cancer Centre, UHN, Sunnybrook Health science Centre, University of Toronto, Toronto,
Should A PSA threshold of 1.5 ng/ml be the threshold for further diagnostic tests? Hanan Goldberg, MD Princess Margaret Cancer Centre, UHN, Sunnybrook Health science Centre, University of Toronto, Toronto,
Elsevier Editorial System(tm) for European Urology Manuscript Draft
 for European Urology Manuscript Draft") Elsevier Editorial System(tm) for European Urology Manuscript Draft Manuscript Number: EURUROL-D-13-00306 Title: Post-Prostatectomy Incontinence and Pelvic Floor Muscle Training: A Defining Problem Article
Elsevier Editorial System(tm) for European Urology Manuscript Draft Manuscript Number: EURUROL-D-13-00306 Title: Post-Prostatectomy Incontinence and Pelvic Floor Muscle Training: A Defining Problem Article
Personalized Therapy for Prostate Cancer due to Genetic Testings
 Personalized Therapy for Prostate Cancer due to Genetic Testings Stephen J. Freedland, MD Professor of Urology Director, Center for Integrated Research on Cancer and Lifestyle Cedars-Sinai Medical Center
Personalized Therapy for Prostate Cancer due to Genetic Testings Stephen J. Freedland, MD Professor of Urology Director, Center for Integrated Research on Cancer and Lifestyle Cedars-Sinai Medical Center
CONTEMPORARY UPDATE OF PROSTATE CANCER STAGING NOMOGRAMS (PARTIN TABLES) FOR THE NEW MILLENNIUM
 FOR THE NEW MILLENNIUM") RAPID COMMUNICATION CME ARTICLE CONTEMPORARY UPDATE OF PROSTATE CANCER STAGING NOMOGRAMS (PARTIN TABLES) FOR THE NEW MILLENNIUM ALAN W. PARTIN, LESLIE A. MANGOLD, DANA M. LAMM, PATRICK C. WALSH, JONATHAN
RAPID COMMUNICATION CME ARTICLE CONTEMPORARY UPDATE OF PROSTATE CANCER STAGING NOMOGRAMS (PARTIN TABLES) FOR THE NEW MILLENNIUM ALAN W. PARTIN, LESLIE A. MANGOLD, DANA M. LAMM, PATRICK C. WALSH, JONATHAN
european urology 51 (2007)
") european urology 51 (2007) 366 374 available at www.sciencedirect.com journal homepage: www.europeanurology.com Prostate Cancer Overall and Disease-Specific Survival of Patients with Screen-Detected Prostate
european urology 51 (2007) 366 374 available at www.sciencedirect.com journal homepage: www.europeanurology.com Prostate Cancer Overall and Disease-Specific Survival of Patients with Screen-Detected Prostate
Impact of PSA Screening on Prostate Cancer Incidence and Mortality in the US
 Impact of PSA Screening on Prostate Cancer Incidence and Mortality in the US Deaths per 100,000 Ruth Etzioni Fred Hutchinson Cancer Research Center JASP Symposium, Montreal 2006 Prostate Cancer Incidence
Impact of PSA Screening on Prostate Cancer Incidence and Mortality in the US Deaths per 100,000 Ruth Etzioni Fred Hutchinson Cancer Research Center JASP Symposium, Montreal 2006 Prostate Cancer Incidence
Prostate MRI: Who needs it?
 Prostate MRI: Who needs it? Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Abdominal Imaging Magnetic Resonance Science Center
Prostate MRI: Who needs it? Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Abdominal Imaging Magnetic Resonance Science Center
Radical Prostatectomy:
 Overtreatment and undertreatment Radical Prostatectomy: An Emerging Standard of Care for High Risk Prostate Cancer Matthew R. Cooperberg, MD,MPH UCSF Radiation Oncology Update San Francisco, CA April 2,
Overtreatment and undertreatment Radical Prostatectomy: An Emerging Standard of Care for High Risk Prostate Cancer Matthew R. Cooperberg, MD,MPH UCSF Radiation Oncology Update San Francisco, CA April 2,
Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice
 european urology supplements 5 (2006) 362 368 available at www.sciencedirect.com journal homepage: www.europeanurology.com Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice Antonio
european urology supplements 5 (2006) 362 368 available at www.sciencedirect.com journal homepage: www.europeanurology.com Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice Antonio
Information Content of Five Nomograms for Outcomes in Prostate Cancer
 Anatomic Pathology / NOMOGRAMS IN PROSTATE CANCER Information Content of Five Nomograms for Outcomes in Prostate Cancer Tarek A. Bismar, MD, 1 Peter Humphrey, MD, 2 and Robin T. Vollmer, MD 3 Key Words:
Anatomic Pathology / NOMOGRAMS IN PROSTATE CANCER Information Content of Five Nomograms for Outcomes in Prostate Cancer Tarek A. Bismar, MD, 1 Peter Humphrey, MD, 2 and Robin T. Vollmer, MD 3 Key Words:
Otis W. Brawley, MD, MACP, FASCO, FACE
 Otis W. Brawley, MD, MACP, FASCO, FACE Chief Medical and Scientific Officer American Cancer Society Professor of Hematology, Medical Oncology, Medicine and Epidemiology Emory University Atlanta, Georgia
Otis W. Brawley, MD, MACP, FASCO, FACE Chief Medical and Scientific Officer American Cancer Society Professor of Hematology, Medical Oncology, Medicine and Epidemiology Emory University Atlanta, Georgia
ORIGINAL INVESTIGATION
 ORIGINAL INVESTIGATION LESS IS MORE Risk Profiles and Treatment Patterns Among Men Diagnosed as Having Prostate Cancer and a Prostate-Specific Antigen Level Below 4. ng/ml Yu-Hsuan Shao, PhD; Peter C.
ORIGINAL INVESTIGATION LESS IS MORE Risk Profiles and Treatment Patterns Among Men Diagnosed as Having Prostate Cancer and a Prostate-Specific Antigen Level Below 4. ng/ml Yu-Hsuan Shao, PhD; Peter C.
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Fellow GU Lecture Series, Prostate Cancer. Asit Paul, MD, PhD 02/20/2018
 Fellow GU Lecture Series, 2018 Prostate Cancer Asit Paul, MD, PhD 02/20/2018 Disease Burden Screening Risk assessment Treatment Global Burden of Prostate Cancer Prostate cancer ranked 13 th among cancer
Fellow GU Lecture Series, 2018 Prostate Cancer Asit Paul, MD, PhD 02/20/2018 Disease Burden Screening Risk assessment Treatment Global Burden of Prostate Cancer Prostate cancer ranked 13 th among cancer
Newer Aspects of Prostate Cancer Underwriting
 Newer Aspects of Prostate Cancer Underwriting Presented By: Jack Swanson, M.D. Keith Hoffman, NFP Moments Made Possible Objectives To review and discuss Conflicting messages about PSA testing Cautions
Newer Aspects of Prostate Cancer Underwriting Presented By: Jack Swanson, M.D. Keith Hoffman, NFP Moments Made Possible Objectives To review and discuss Conflicting messages about PSA testing Cautions
Testosterone Therapy and the Prostate. Frans M.J. Debruyne Professor of Urology The Netherlands
 Testosterone Therapy and the Prostate Frans M.J. Debruyne Professor of Urology The Netherlands TRT- Risks Prostate ( Cancer, BPH )? Cardiac? Lipids? Polycythemia Sleep apnea Gynecomastia Edema Testosterone
Testosterone Therapy and the Prostate Frans M.J. Debruyne Professor of Urology The Netherlands TRT- Risks Prostate ( Cancer, BPH )? Cardiac? Lipids? Polycythemia Sleep apnea Gynecomastia Edema Testosterone
PORT after RP. Adjuvant. Salvage
 PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
3/22/2014. Goals of this Presentation: in 15 min & 5 min Q & A. Radiotherapy for. Localized Prostate Cancer: What is New in 2014?
 3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
Prostate Biopsy. Prostate Biopsy. We canʼt go backwards: Screening has helped!
 We canʼt go backwards: Screening has helped! Robert E. Donohue M.D. Denver V.A. Medical Center University of Colorado Prostate Biopsy Is cure necessary; when it is possible? Is cure possible; when it is
We canʼt go backwards: Screening has helped! Robert E. Donohue M.D. Denver V.A. Medical Center University of Colorado Prostate Biopsy Is cure necessary; when it is possible? Is cure possible; when it is
Consensus and Controversies in Cancer of Prostate BASIS FOR FURHTER STUDIES. Luis A. Linares MD FACRO Medical Director
 BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
10/2/2018 OBJECTIVES PROSTATE HEALTH BACKGROUND THE PROSTATE HEALTH INDEX PHI*: BETTER PROSTATE CANCER DETECTION
 THE PROSTATE HEALTH INDEX PHI*: BETTER PROSTATE CANCER DETECTION Lenette Walters, MS, MT(ASCP) Medical Affairs Manager Beckman Coulter, Inc. *phi is a calculation using the values from PSA, fpsa and p2psa
THE PROSTATE HEALTH INDEX PHI*: BETTER PROSTATE CANCER DETECTION Lenette Walters, MS, MT(ASCP) Medical Affairs Manager Beckman Coulter, Inc. *phi is a calculation using the values from PSA, fpsa and p2psa
Correspondence should be addressed to Taha Numan Yıkılmaz;
 Advances in Medicine Volume 2016, Article ID 8639041, 5 pages http://dx.doi.org/10.1155/2016/8639041 Research Article External Validation of the Cancer of the Prostate Risk Assessment Postsurgical Score
Advances in Medicine Volume 2016, Article ID 8639041, 5 pages http://dx.doi.org/10.1155/2016/8639041 Research Article External Validation of the Cancer of the Prostate Risk Assessment Postsurgical Score
The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters.
 An Exploration of Risk Stratification for Active Surveillance and Androgen Deprivation Therapy Side Effects for Prostate Cancer Utilizing Data From the Surveillance, Epidemiology, and End Results Database
An Exploration of Risk Stratification for Active Surveillance and Androgen Deprivation Therapy Side Effects for Prostate Cancer Utilizing Data From the Surveillance, Epidemiology, and End Results Database
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #104 (NQF 0390): Prostate Cancer: Combination Androgen Deprivation Therapy for High Risk or Very High Risk Prostate Cancer National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS
Quality ID #104 (NQF 0390): Prostate Cancer: Combination Androgen Deprivation Therapy for High Risk or Very High Risk Prostate Cancer National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS
Dong Hoon Lee, Kyo Chul Koo, Seung Hwan Lee, Koon Ho Rha, Young Deuk Choi, Sung Joon Hong and Byung Ha Chung
 Jpn J Clin Oncol 2013;43(5)553 558 doi:10.1093/jjco/hyt041 Advance Access Publication 11 April 2013 Low-risk Prostate Cancer Patients Without Visible Tumor (T1c) On Multiparametric MRI Could Qualify for
Jpn J Clin Oncol 2013;43(5)553 558 doi:10.1093/jjco/hyt041 Advance Access Publication 11 April 2013 Low-risk Prostate Cancer Patients Without Visible Tumor (T1c) On Multiparametric MRI Could Qualify for
American Urological Association (AUA) Guideline
 Guideline") 1 (AUA) Guideline Approved by the AUA Board of Directors April 2013 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2013 by the American
1 (AUA) Guideline Approved by the AUA Board of Directors April 2013 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2013 by the American
Focal Therapy is a Fool s Paradise : The whole prostate must be treated!
 Focal Therapy is a Fool s Paradise : The whole prostate must be treated! Ofer Yossepowitch, MD Head, Department of Urology Tel Aviv Sourasky Medical Center Preaching against focal therapy in a focal therapy
Focal Therapy is a Fool s Paradise : The whole prostate must be treated! Ofer Yossepowitch, MD Head, Department of Urology Tel Aviv Sourasky Medical Center Preaching against focal therapy in a focal therapy
SIMPOSIO. Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico
 SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
Where are we with PSA screening?
 Where are we with PSA screening? Faculty/Presenter Disclosure Rela%onships with commercial interests: None Disclosure of Commercial Support This program has received no financial support. This program
Where are we with PSA screening? Faculty/Presenter Disclosure Rela%onships with commercial interests: None Disclosure of Commercial Support This program has received no financial support. This program
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10