Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro. Immune checkpoint inhibition in DLBCL
|
|
|
- Roberta Gaines
- 5 years ago
- Views:
Transcription

1 Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL
 Our immune system can also recognize and destroy cancer cells.")
2 Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections by foreign antigens expressed in microorganisms (bacteria, viruses, etc.) Our immune system can also recognize and destroy cancer cells.. However, cancer cells have developed escape mechanisms to avoid their destruction by immune cells put the brakes on Immuno-Oncology: Find ways of unleashing the power of our body s immune system to treat or prevent cancer T-lymphocytes (Tcells)


3 Detectives Dendritic cells Killer T cells Microenvironment antigen (flags)

4 Detectives Dendritic cells Killer T cells Tumor infiltranting T cell recognizable ags Cor e Margin Algorithms Neo-antigens antigen (flags)



5 5


6 Scott DW et al. Nature Rev
7 Strategy approach Effective immune response: barriers microenviroment Activate anti-tumor immune response inhibitory receptors: blocking antibodies Nivo, Pembro, Ipi, (anti PD 1) (CTLA4) combining 2 checkpoint inhibitors combining with chemotherapy activate receptors: agonist Urelumab Utumilumab Varlilumab

8 Strategy approach Effective immune response: barriers microenviroment
9 Inactivated effector T cell angiogenesis metabolism PDL-1 Lymphoma CTLA-4 PDL-1 Strategy approach Effective immune response: barriers PD-1 PDL-1 TIM-3 PDL-1 PDL-1 mtor LAG-3 OXPHOS MHC1 Interferon gamma EB virus T cell activation antigen presenting cells Aerobic glycolysis
10 Strategy approach Effective immune response: barries microenviroment Activate anti-tumor immune response inhibitory receptors: blocking antibodies Nivo, Pembro, Ipi, combining 2 checkpoint inhibitors combining with chemotherapy activate receptors: agonist Urelumab Utumilumab Varlilumab
11 Atezolizumab Inhibitory receptors Durvalumab Ipilimumab Tremelimumab PDL-1 Avelumab Lymphoma CTLA-4 PDL-1 Nivolumab Pembrolizumab Pidilizumab PD-1 PDL-1 TIM-3 PDL-1 PDL-1 LAG-3 Interferon gamma EB virus T cell activation MBG453 TSR-022 IMP321
12 Atezolizumab Inhibitory receptors Durvalumab Avelumab PDL-1 Ipilimumab Tremelimumab Lymphoma PDL-1 CTLA-4 PD-1 Nivolumab Pembrolizumab Pidilizumab PDL-1 PDL-1 TIM-3 MBG453 TSR-022 LAG-3 IMP321 Varlilumab CD27 CD40L 4-1BB Dacetuzumab Utumilumab Activating receptors
13 PD-L1 expression in lymphomas PD-L1 expression was found to be abundant in agressive B- cell lymphoma viral associated, and immunodeficiencyrelated lymphomas Similar to chl, primary mediastinal B cell lymphoma, T- cell/histiocyte rich large B cell lymphoma : 90% PDL1/2 expression NK-T cell lymphoma (80%), primary effusion lymphoma (75%), plasmablastic (44%) and DLCBL NOS: 14%
14 Development of Immune checkpoints Early trials Anti CTLA 4 Ipilimumab Anti PD 1 Pidilizumab Nivolumab Pembrolizumab Combination Ipilimumab + nivolumab Phase II Anti PD 1
15 Development of Immune checkpoints Early trials Anti CTLA 4 Ipilimumab Anti PD 1 Pidilizumab Nivolumab Pembrolizumab Combination Ipilimumab + nivolumab Phase II Anti PD 1

16 Ipilimumab CTLA-4 blockade (ipilimumab) APC T-cell interaction Tumor microenvironment MHC DendriticB7 cell B7 TCR +++ Activation (cytokine secretion, lysis, proliferation, migration to tumor) CD T cell CTLA CTLA-4 is expressed on T cells and inhibits T-cell activation Ipilimumab disrupts the CTLA-4 pathway, thus inducing anti-tumor immunity Blockade of CTLA-4 has been shown to enhance T-cell responses and anti-tumor responses
, were durable, lasting over 31 m in")
17 First trial: Ipilimumab in lymphoma 18 patients: 2 responses (11%), were durable, lasting over 31 m in DLCBL
18 Development of Immune checkpoints Early trials Anti CTLA 4 Ipilimumab Anti PD 1 Pidilizumab Nivolumab Combination Ipilimumab + nivolumab Phase II Anti PD 1
 CD28 +++ T cell CTLA-4 --- anti-ctla-4 TCR +++ T cell PD-1 --- PD-1 --- MHC Tumor cell PD-L1 anti-pd-1 PD-L2 CTLA-4 is expressed on T cells and inhibits T-cell")
19 Ipilimumab and PD1 blockade CTLA-4 blockade (ipilimumab) PD-1 blockade APC T-cell interaction Tumor microenvironment MHC DendriticB7 cell B7 TCR +++ Activation (cytokine secretion, lysis, proliferation, migration to tumor) CD T cell CTLA anti-ctla-4 TCR +++ T cell PD PD MHC Tumor cell PD-L1 anti-pd-1 PD-L2 CTLA-4 is expressed on T cells and inhibits T-cell activation5 PD-1 expression on tumor-infiltrating lymphocytes is associated with decreased cytokine production and effector function Ipilimumab disrupts the CTLA-4 pathway, thus inducing anti-tumor immunity Anti PD-1 disrupts PD-1 pathway signaling and restores anti-tumor T-cell function


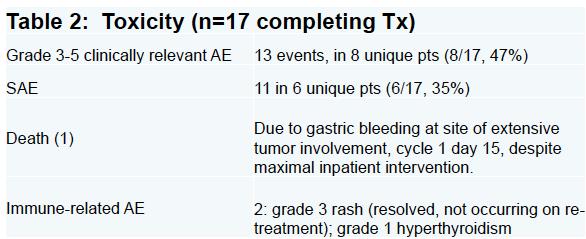
20 Sixty-six eligible patients were treated. At 16 months, PFS was 0.72 (90% CI, 0.60 to 0.82), meeting the primary end point Treatment was associated with an apparent CR rate of 34% and overall response rate of 51% among patients with measurable disease after transplant



21 Nivolumab Efficay results Kinetics response Drug-Related AEs Biomarker assessment IHC for PD-L1 positive >20% of nonmalignant cells and no staining of malignant cells
22

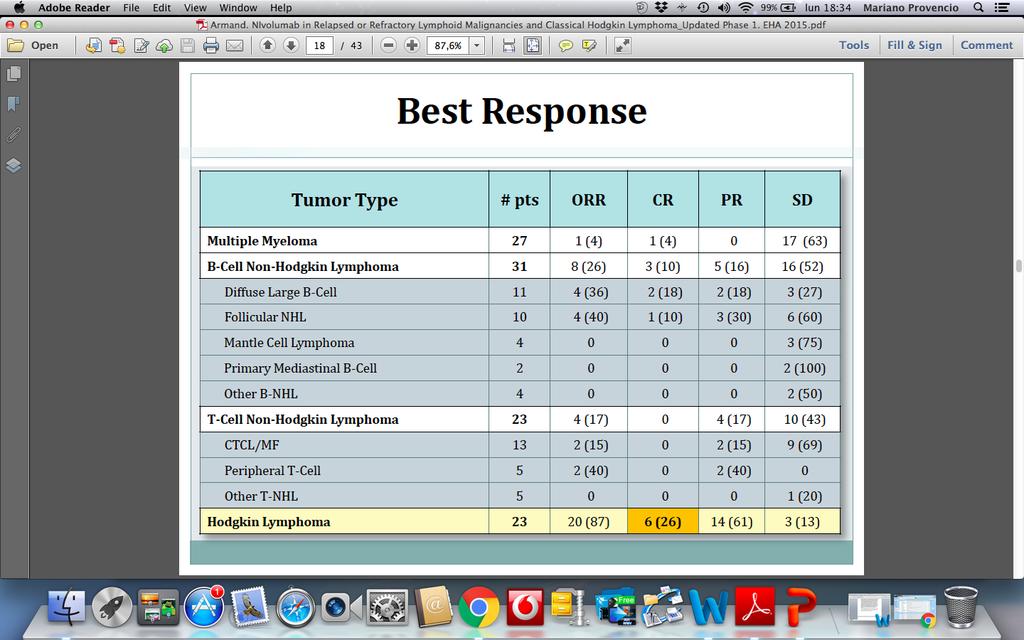
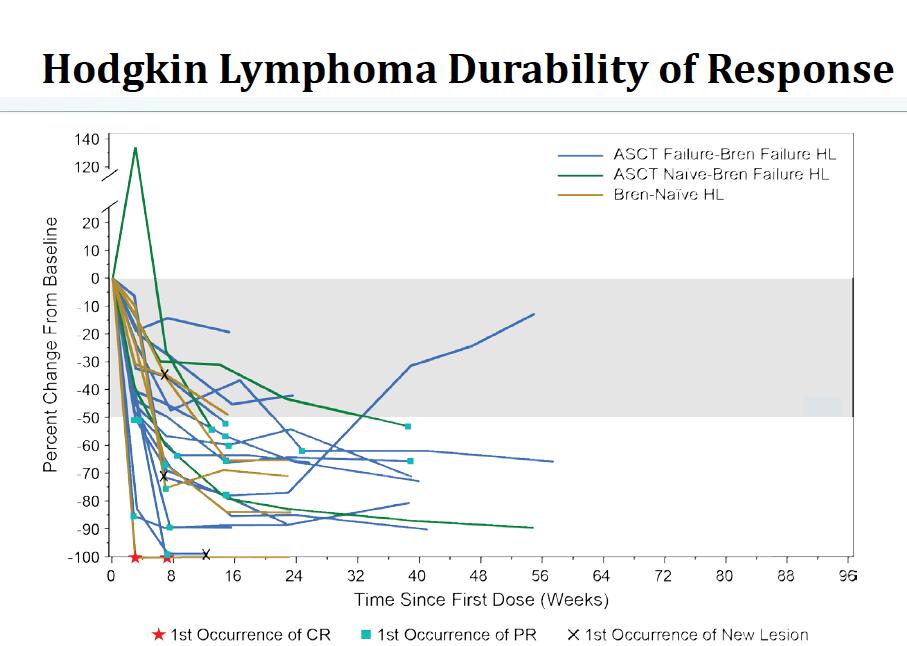
23 Durability of response Armand P EHA 20 th 2015, updated results phase I
24
25 7 lines of treatments including TASPE

26 Post Nivolumab
27 immunotherapy in lymphomas Hodgkin s Lymphomas Copy number of 9p24.2, a genomic region that includes CD274 (encoding PD-L1), PDCD1LG2 (encoding PD- L2), and JAK2 correlates with cell surface PD-L1 protein expression more? Whole-exome sequencing of RS cells from chl revealed a median of only 244 mutations per case But, PD-L1 blockade therapy us extraordinarily effective in chl, suggesting at least in this disease, that antigenic quality is an important as quantity,» in some cases, HRS specific antigens may derived from immunogenic EBV antigens
28 Development of Immune checkpoints Early trials Anti CTLA 4 Ipilimumab Anti PD 1 Pidilizumab Nivolumab Pembrolizumab Combination Ipilimumab + nivolumab Phase II Anti PD 1
29 Nivolumab and Ipilimumab CTLA-4 blockade (ipilimumab) PD-1 blockade (nivolumab) APC T-cell interaction Tumor microenvironment MHC DendriticB7 cell B7 TCR +++ Activation (cytokine secretion, lysis, proliferation, migration to tumor) CD T cell CTLA anti-ctla-4 TCR +++ T cell PD PD MHC Tumor cell PD-L1 anti-pd-1 PD-L2 CTLA-4 is expressed on T cells and inhibits T-cell activation5 PD-1 expression on tumor-infiltrating lymphocytes is associated with decreased cytokine production and effector function Ipilimumab disrupts the CTLA-4 pathway, thus inducing anti-tumor immunity Nivolumab disrupts PD-1 pathway signaling and restores anti-tumor T-cell function
30 CheckMate 039 Study Design: Nivolumab and Ipilimumab Combination Cohort Phase 1, non-randomized, non-comparative, sequential cohort pilot study Inclusion Criteria Relapsed/refractory lymphoid malignancies: Hodgkin lymphoma B-cell lymphoma a T-cell lymphoma b Multiple myeloma No prior organ or allogeneic bone marrow transplantation No prior immune checkpoint blockade therapy Combination phase Nivolumab 3 mg/kg IV + Ipilimumab 1 mg/kg IV Q3W x 4 doses Treatment Monotherapy phase Nivolumab 3 mg/kg IV Q2W 2 years Treatment until disease progression, toxicity, or maximum duration of 2 years Primary Endpoints Safety and tolerability Secondary INV-assessed best overall response Duration of response Progression-free survival Biomarker analyses a Includes follicular B-cell lymphoma (FL) and diffuse large B-cell lymphoma (DLBCL). b Includes cutaneous T-cell lymphoma (CTCL) and peripheral T-cell lymphoma (PTCL) INV, investigator; IV, intravenously; Q2W, every 2 weeks; Q3W, every 3 weeks Ansell AHS 2016 ASH
31 Baseline Characteristics Disposition HL (N = 31) B-cell NHL a (N = 15) T-cell NHL b (N = 11) MM (N = 7) (DLBCL + FL) (CTCL + PTCL) Male, % ECOG 1, % Prior systemic therapies, median (range) 4 (2 10) 3 (1 16) 4 (1 11) 5 (2 20) Prior ASCT, % Median time from prior therapy to first nivolumab dose, months (range) 2.2 ( ) 2.0 ( ) 1.4 ( ) 1.0 ( ) a B-cell NHL: DLBCL, n = 10; FL, n = 5; b T-cell NHL: CTCL, n = 7; PTCL, n = 4 ASCT, autologous stem cell transplantation; CTCL, cutaneous T-cell lymphoma; DLBCL, diffuse large B-cell lymphoma; ECOG, Eastern Cooperative Oncology Group; FL, follicular B-cell lymphoma; HL, Hodgkin lymphoma; MM, multiple myeloma; NHL, non-hodgkin lymphoma; PTCL, peripheral T-cell lymphoma For HL cohort, transplant naïve, n = 18 Chemoresistant, n = 13 Ineligible for ASCT, n = 3 Declined procedure, n = 2 ASH
32 Dosage Summary HL (N = 31) B-cell NHL (N = 15) T-cell NHL (N = 11) MM (N = 7) Median number of doses received (range) Nivolumab 12 (2 43) 2 (1 34) 5 (1 24) 2 (1 4) Ipilimumab 4 (2 4) 2 (1 4) 4 (1 4) 2 (1 4) Patients receiving 90% of intended dose, n (%) Nivolumab (combination phase) 21 (68) 14 (93) 9 (82) 5 (71) Ipilimumab (combination phase) 20 (65) 14 (93) 9 (82) 5 (71) Nivolumab (monotherapy phase) a 21 (81) 3 (75) 5 (83) 0 a Total number of patients included in the nivolumab monotherapy for whom dose intensity was reported: HL, n = 26; B-cell NHL, n = 4; T-cell NHL, n = 6; MM, n = 0 HL, Hodgkin lymphoma; MM, multiple myeloma; NHL, non-hodgkin lymphoma The reason for patients receiving <90% of the intended dose was dose delays 32 ASH
33 Safety Overview Drug-related AEs All AEs Grade 3 4 Serious AEs AE leading to discontinuation All patients (N = 65), n (%) a 51 (78) 19 (29) 14 (22) 5 (8) HL (N = 31) 28 (90) 8 (26) 6 (19) 2 (6) B-cell NHL (N = 15) 8 (53) 3 (20) 2 (13) 0 T-cell NHL (N = 11) 11 (100) 5 (45) 4 (36) 2 (18) MM (N = 7) 4 (57) 3 (43) 2 (29) 1 (14) a Total includes 1 patient with primary mediastinal B cell lymphoma HL, Hodgkin lymphoma; MM, multiple myeloma; NHL, non-hodgkin lymphoma Adverse events (AEs) leading to discontinuation: Pneumonitis (grade 1 in a patient with HL; grade 3 in a patient with T-cell NHL; grade 3 in a patient with MM) Pneumonia and pneumonitis (both grade 4, both AEs occurred in a single patient with T-cell NHL) Diabetic ketoacidosis (grade 4 in a patient with HL) No drug-related deaths occurred; most deaths were due to disease progression ASH
34 Drug-Related AEs AEs by preferred term, n (%) Nivolumab + ipilimumab (N = 65) Any grade a Grade 3 4 Fatigue 17 (26) 1 (2) Pyrexia 15 (23) 0 Rash 7 (11) 0 Diarrhea 12 (18) 1 (2) Nausea 9 (14) 1 (2) Pneumonitis 9 (14) 4 (6) Cough 9 (14) 0 Infusion-related reaction 9 (14) 2 (3) Select AEs b by category, n (%) Any grade c Grade 3 4 Gastrointestinal 14 (22) 2 (3) Skin 14 (22) 0 Hypersensitivity/infusion reaction 11 (17) 2 (3) Pulmonary 10 (15) 4 (6) Hepatic 6 (9) 2 (3) Renal 2 (3) 0 a AEs occurring in 10% of patients. b Select AEs = AEs with potential immunologic etiology that require frequent monitoring/intervention that occurred between first nivolumab dose and up to 30 days after last nivolumab dose. c All drug-related select AEs AE, adverse event ASH
35 B-Cell NHL: Best Overall Response B-cell NHL (N = 15) ORR, n (%) a 3 (20) Complete response 0 Partial response 3 (20) Stable disease 1 (7) Relapsed or progressive disease Median duration of PR, months (range) 8 (53) NR (11.0+, 12.7+) a Response was not reported or unable to be determined for 3 (20%) patients with B- cell NHL Change from baseline in target lesions tumor burden (%) Change in tumor burden, B-cell NHL st occurrence of new lesion Off treatment DLBCL responders (n = 2) DLBCL non-responders (n = 8) FL responders (n = 1) FL non-responders (n = 4) Time since first treatment date (weeks) % change truncated to 100 +, censored value; DLBCL, diffuse large B-cell lymphoma; FL, follicular B-cell lymphoma; NHL, non-hodgkin lymphoma; NR, not reached; ORR, overall response rate; PR, partial response ASH
36 Change in Tumor Burden by PD-L1 H-Score Nivolumab and Ipilimumab Combination Non-Hodgkin lymphoma A diverse group of tumors, characterized by variable PD-L1 expression Immune-mediated AEs consistent in frequency and severity with known safety profile of this combination In NHL, activity in a small H proportion H H of DLBCL H H H H H H H H H H H H H Change from baseline in tumor size (%) D F C D D P F P P M C P D D 5 10 Patients PD-L1 H-score quartile: and < and < and 300 ASH
37 Development of Immune checkpoints Early trials Anti CTLA 4 Ipilimumab Anti PD 1 Pidilizumab Nivolumab Pembrolizumab Combination Ipilimumab + nivolumab Phase II Anti PD 1
38 CheckMate 139, phase II, Nivo in DLBCL refractory after ASCT 121 patients were evaluated 87 after ASCT and 34 ASCT ineligible (ASCT-i) ORR. 10.3% (95% CI, 4.8 to 18.7) 3.4% CR in ASCT and 2.9% ASCT-i Duration of response was: 11.4 m PFS: 1.87 m (ASCT) and 1.4m (ASCT-i) This study is ongoing, but not recruiting participants Accessed december, 12, 2017.
39 ASH 2017
40

41 Early combinations
42 Dec 2017
43 Conclusions Anti PD1: Highly tumor-dependent very active in Hodgkin Lymphoma Modest activity in Non-Hodgkin Lymphoma Combinations Modest activity IPI+ Nivo Incorporing promising agentsinto combination approaches Optimizing new terapeutics agents and immune fuction

44 Merci!!
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in lymphoma. Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust
 Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
Nivolumab in Hodgkin Lymphoma
 Nivolumab in Hodgkin Lymphoma Stephen M. Ansell, MD, PhD Professor of Medicine Chair, Lymphoma Group Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers Squibb Celldex Therapeutics Seattle
Nivolumab in Hodgkin Lymphoma Stephen M. Ansell, MD, PhD Professor of Medicine Chair, Lymphoma Group Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers Squibb Celldex Therapeutics Seattle
2018 KSMO Immune Oncology Forum. Immune checkpoint inhibitors in hematologic. malignancies: evidences and perspectives 서울아산병원종양내과 홍정용
 2018 KSMO Immune Oncology Forum Immune checkpoint inhibitors in hematologic malignancies: evidences and perspectives 서울아산병원종양내과 홍정용 2018-07-18 Contents Introduction Immune checkpoint inhibtors in lymphomas
2018 KSMO Immune Oncology Forum Immune checkpoint inhibitors in hematologic malignancies: evidences and perspectives 서울아산병원종양내과 홍정용 2018-07-18 Contents Introduction Immune checkpoint inhibtors in lymphomas
Hodgkin Lymphoma Nivolumab
 New Drugs In Hematology Hodgkin Lymphoma Nivolumab Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center Monday, May 9, 2016 2:10-2:25 p.m immunotherapy modalities CAR T Cells
New Drugs In Hematology Hodgkin Lymphoma Nivolumab Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center Monday, May 9, 2016 2:10-2:25 p.m immunotherapy modalities CAR T Cells
Checkpoint Blockade in Hematology and Stem Cell Transplantation
 Checkpoint Blockade in Hematology and Stem Cell Transplantation Saad S. Kenderian, MD Assistant Professor of Medicine and Oncology Mayo Clinic College of Medicine October 14, 2016 2015 MFMER slide-1 Disclosures
Checkpoint Blockade in Hematology and Stem Cell Transplantation Saad S. Kenderian, MD Assistant Professor of Medicine and Oncology Mayo Clinic College of Medicine October 14, 2016 2015 MFMER slide-1 Disclosures
Linfoma de Hodgkin. Novos medicamentos. Otavio Baiocchi CRM-SP
 Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Challenges in Distinguishing Clinical Signals to Support Development Decisions: Case Studies
 Challenges in Distinguishing Clinical Signals to Support Development Decisions: Case Studies David Feltquate MD, PhD Head of Early Clinical Development, Oncology Bristol-Myers Squibb, Princeton, NJ Challenges
Challenges in Distinguishing Clinical Signals to Support Development Decisions: Case Studies David Feltquate MD, PhD Head of Early Clinical Development, Oncology Bristol-Myers Squibb, Princeton, NJ Challenges
Checkpoint Inhibition in Hodgkin s Lymphoma John Kuruvilla, MD & Rob Laister, PhD
 Checkpoint Inhibition in Hodgkin s Lymphoma John Kuruvilla, MD & Rob Laister, PhD Disclosures for Rob Laister Research Support Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
Checkpoint Inhibition in Hodgkin s Lymphoma John Kuruvilla, MD & Rob Laister, PhD Disclosures for Rob Laister Research Support Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
Role of the Pathologist in Guiding Immuno-oncological Therapies. Scott Rodig MD, PhD
 Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Haemato-Oncology ESMO PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY. Development and clinical experience Monique Minnema, hematologist
 Haemato-Oncology ESMO PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Development and clinical experience Monique Minnema, hematologist Consultancy for disclosures Amgen, Celgene, Jansen Cilag, BMS, Takeda Immune
Haemato-Oncology ESMO PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Development and clinical experience Monique Minnema, hematologist Consultancy for disclosures Amgen, Celgene, Jansen Cilag, BMS, Takeda Immune
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
AACR 2018 Investor Meeting
 AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
Immunotherapy in lung cancer. Saurabh maji
 Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy
: Biomarkers for Immunotherapy") Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA
 Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Immunotherapy Overview, Rationale, and Role in Clinical Practice
 Immunotherapy Overview, Rationale, and Role in Clinical Practice Financial Disclosure Bradi L. Frei, PharmD, BCOP, BCPS has no relevant financial relationships with commercial interests to disclose. OBJECTIVES
Immunotherapy Overview, Rationale, and Role in Clinical Practice Financial Disclosure Bradi L. Frei, PharmD, BCOP, BCPS has no relevant financial relationships with commercial interests to disclose. OBJECTIVES
PD-L1 and Immunotherapy of GI cancers: What do you need to know
 None. PD-L1 and Immunotherapy of GI cancers: What do you need to know Rondell P. Graham September 3, 2017 2017 MFMER slide-2 Disclosure No conflicts of interest to disclose 2017 MFMER slide-3 Objectives
None. PD-L1 and Immunotherapy of GI cancers: What do you need to know Rondell P. Graham September 3, 2017 2017 MFMER slide-2 Disclosure No conflicts of interest to disclose 2017 MFMER slide-3 Objectives
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico
 Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Hodgkin Lymphoma New Combo-Steps
 New Drugs In Hematology Hodgkin Lymphoma New Combo-Steps Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center Monday, May 9, 2016 2:55-3:10 p.m Combinations with Immune Checkpoint
New Drugs In Hematology Hodgkin Lymphoma New Combo-Steps Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center Monday, May 9, 2016 2:55-3:10 p.m Combinations with Immune Checkpoint
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma
 Treating Frail Adults With Common Malignancies: Best Evidence to Personalize Therapy Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma Raul Cordoba, MD, PhD Lymphoma Unit
Treating Frail Adults With Common Malignancies: Best Evidence to Personalize Therapy Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma Raul Cordoba, MD, PhD Lymphoma Unit
Professor Mark Bower Chelsea and Westminster Hospital, London
 Professor Mark Bower Chelsea and Westminster Hospital, London Cancer immunotherapy & HIV Disclosures: None Lessons for oncology from HIV Awareness and advocacy Activism Rational drug design Prescribing
Professor Mark Bower Chelsea and Westminster Hospital, London Cancer immunotherapy & HIV Disclosures: None Lessons for oncology from HIV Awareness and advocacy Activism Rational drug design Prescribing
Immune Checkpoints. PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich
 Immune Checkpoints PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich Activation of T cells requires co-stimulation Science 3
Immune Checkpoints PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich Activation of T cells requires co-stimulation Science 3
AGRESSIVE LYMPHOMAS - FUTURE. Dr Stéphane Doucet CHUM
 AGRESSIVE LYMPHOMAS - FUTURE Dr Stéphane Doucet CHUM What are clinical trials? Clinical trials are carefully planned research studies where the most-promising discoveries and results from laboratory studies
AGRESSIVE LYMPHOMAS - FUTURE Dr Stéphane Doucet CHUM What are clinical trials? Clinical trials are carefully planned research studies where the most-promising discoveries and results from laboratory studies
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento
 tra la prima e la seconda linea di trattamento") Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER. Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia
 IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Distinguishing self from non-self T cells trained in the thymus as
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Distinguishing self from non-self T cells trained in the thymus as
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
Update on the development of immune checkpoint inhibitors
 Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
ONCOS-102 in melanoma Dr. Alexander Shoushtari. 4. ONCOS-102 in mesothelioma 5. Summary & closing
 ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
ASCO 2014 Highlights*
 ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
MMAE disrupts cell division and triggers apoptosis. Pola binds to cell surface antigen CD79b. Pola is internalized; linker cleaves, releasing MMAE
 Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
PD-1 Pathway Inhibitors: Immuno-Oncology Agents for Restoring Antitumor Immune Responses
 PD-1 Pathway Inhibitors: Immuno-Oncology Agents for Restoring Antitumor Immune Responses Patrick J. Medina, 1, * and Val R. Adams, 2 1 Department of Pharmacy: Clinical and Administrative Sciences, The
PD-1 Pathway Inhibitors: Immuno-Oncology Agents for Restoring Antitumor Immune Responses Patrick J. Medina, 1, * and Val R. Adams, 2 1 Department of Pharmacy: Clinical and Administrative Sciences, The
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER. Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium
 THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
A CME-certified Oncology Exchange Program
 A CME-certified Oncology Exchange Program Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Seattle Genetics, Inc. Re-treatment with BV Bartlett
A CME-certified Oncology Exchange Program Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Seattle Genetics, Inc. Re-treatment with BV Bartlett
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for Melanoma. Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France
 Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Relapsed/Refractory Hodgkin Lymphoma
 Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Presentation Number: LBA18_PR. Lecture Time: 09:15-09:27. Speakers: Heinz-Josef J. Lenz (Los Angeles, US) Background
 Background") LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma
 With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma") Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Immunotherapy on the Horizon
 Immunotherapy on the Horizon Andrew L. Coveler Assistant Professor of Medicine, Division of Oncology University of Washington Assistant Member Fred Hutchinson Cancer Research Center Image: NASA.gov 1 2
Immunotherapy on the Horizon Andrew L. Coveler Assistant Professor of Medicine, Division of Oncology University of Washington Assistant Member Fred Hutchinson Cancer Research Center Image: NASA.gov 1 2
ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY
 ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY Lauren Clarine DO, Renil Rodriguez Martinez MD, Matthew Levine MD, Amy Chang MD, and Megan McGarvey MD May 6, 2017 Immune checkpoint inhibitors
ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY Lauren Clarine DO, Renil Rodriguez Martinez MD, Matthew Levine MD, Amy Chang MD, and Megan McGarvey MD May 6, 2017 Immune checkpoint inhibitors
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
Pembrolizumab in Relapsed/Refractory Classical Hodgkin Lymphoma: Phase 2 KEYNOTE-087 Study
 Pembrolizumab in Relapsed/Refractory Classical Hodgkin Lymphoma: Phase 2 KEYNOTE-087 Study Craig H. Moskowitz, 1 Pier Luigi Zinzani, 2 Michelle A. Fanale, 3 Philippe Armand, 4 Nathalie Johnson, 5 John
Pembrolizumab in Relapsed/Refractory Classical Hodgkin Lymphoma: Phase 2 KEYNOTE-087 Study Craig H. Moskowitz, 1 Pier Luigi Zinzani, 2 Michelle A. Fanale, 3 Philippe Armand, 4 Nathalie Johnson, 5 John
PD-1/PD-L1 inhibitors in hematological malignancies, with focus on Lymphoid Malignancies
 PD-1/PD-L1 inhibitors in hematological malignancies, with focus on Lymphoid Malignancies Professor Lim Soon Thye Head, Division of Medical Oncology National Cancer Centre Singapore Head, Singhealth Duke-NUS
PD-1/PD-L1 inhibitors in hematological malignancies, with focus on Lymphoid Malignancies Professor Lim Soon Thye Head, Division of Medical Oncology National Cancer Centre Singapore Head, Singhealth Duke-NUS
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142
 Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142 Abstract #519 Overman MJ, Lonardi S, Leone F, McDermott
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142 Abstract #519 Overman MJ, Lonardi S, Leone F, McDermott
New Agents Beyond Brentuximab vedotin for Hodgkin Lymphoma. Stephen M. Ansell, MD, PhD Professor of Medicine Mayo Clinic
 New Agents Beyond Brentuximab vedotin for Hodgkin Lymphoma Stephen M. Ansell, MD, PhD Professor of Medicine Mayo Clinic Disclosures for Stephen Ansell, MD, PhD In compliance with ACCME policy, Mayo Clinic
New Agents Beyond Brentuximab vedotin for Hodgkin Lymphoma Stephen M. Ansell, MD, PhD Professor of Medicine Mayo Clinic Disclosures for Stephen Ansell, MD, PhD In compliance with ACCME policy, Mayo Clinic
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016
 Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Update: New Treatment Modalities
 ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
CAR-T cell therapy pros and cons
 CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates
 Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates Christopher Turner, MD Vice President, Clinical Science 04 November 2016 Uveal Melanoma Celldex Pipeline CANDIDATE INDICATION Preclinical
Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates Christopher Turner, MD Vice President, Clinical Science 04 November 2016 Uveal Melanoma Celldex Pipeline CANDIDATE INDICATION Preclinical
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
GSK Oncology. Axel Hoos, MD, PhD Senior Vice President, Oncology R&D. March 8, 2017
 GSK Oncology Axel Hoos, MD, PhD Senior Vice President, Oncology R&D March 8, 217 GSK pipeline Oncology R&D Strategy Maximizing survival through transformational medicines and combinations Cancer Epigenetics
GSK Oncology Axel Hoos, MD, PhD Senior Vice President, Oncology R&D March 8, 217 GSK pipeline Oncology R&D Strategy Maximizing survival through transformational medicines and combinations Cancer Epigenetics
Tumor Immunity and Immunotherapy. Andrew Lichtman M.D., Ph.D. Brigham and Women s Hospital Harvard Medical School
 Tumor Immunity and Immunotherapy Andrew Lichtman M.D., Ph.D. Brigham and Women s Hospital Harvard Medical School Lecture Outline Evidence for tumor immunity Types of tumor antigens Generation of anti-tumor
Tumor Immunity and Immunotherapy Andrew Lichtman M.D., Ph.D. Brigham and Women s Hospital Harvard Medical School Lecture Outline Evidence for tumor immunity Types of tumor antigens Generation of anti-tumor
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
Focus on Immunotherapy as a Targeted Therapy. Brad Nelson, PhD BC Cancer, Victoria, Canada FPON, Oct
 Focus on Immunotherapy as a Targeted Therapy Brad Nelson, PhD BC Cancer, Victoria, Canada FPON, Oct 18 2018 Disclosures I have nothing to disclose that is relevant to this presentation. Immunology @ Deeley
Focus on Immunotherapy as a Targeted Therapy Brad Nelson, PhD BC Cancer, Victoria, Canada FPON, Oct 18 2018 Disclosures I have nothing to disclose that is relevant to this presentation. Immunology @ Deeley
PART VI: SUMMARY OF THE RISK MANAGEMENT PLAN BY PRODUCT
 PAGE 175 PART VI: SUMMARY OF THE RISK MANAGEMENT PLAN BY PRODUCT Summary of risk management plan for pembrolizumab This is a summary of the risk management plan (RMP) for pembrolizumab. The RMP details
PAGE 175 PART VI: SUMMARY OF THE RISK MANAGEMENT PLAN BY PRODUCT Summary of risk management plan for pembrolizumab This is a summary of the risk management plan (RMP) for pembrolizumab. The RMP details
IMMUNOTHERAPY FOR CANCER A NEW HORIZON. Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust
 IMMUNOTHERAPY FOR CANCER A NEW HORIZON Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust ASCO Names Advance of the Year: Cancer Immunotherapy No recent
IMMUNOTHERAPY FOR CANCER A NEW HORIZON Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust ASCO Names Advance of the Year: Cancer Immunotherapy No recent
ASCO Annual Meeting 2017 Bart Neyns MD PhD, UZ Brussel. 20th Post-ASCO Meeting, 24th June 2016
 IMMUNOTHERAPY @the ASCO Annual Meeting 2017 Bart Neyns MD PhD, UZ Brussel 20th Post-ASCO Meeting, 24th June 2016 FAS-L Cancer Testis Ag Differentiation Ag Neo-antigens PD-1 CTL CD8+ Tcell CTLA-4 CD28 B7.1/B7.2
IMMUNOTHERAPY @the ASCO Annual Meeting 2017 Bart Neyns MD PhD, UZ Brussel 20th Post-ASCO Meeting, 24th June 2016 FAS-L Cancer Testis Ag Differentiation Ag Neo-antigens PD-1 CTL CD8+ Tcell CTLA-4 CD28 B7.1/B7.2
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Bristol-Myers Squibb, Braine-l Alleud, Belgium; 12 MD Anderson Cancer Center, Houston, TX, USA
 3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
Principles and Application of Immunotherapy for Cancer: Advanced NSCLC
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Histology independent indications in Oncology
 CHMP Oncology Working Party Workshop Histology independent indications in Oncology What have we learnt from the anti PD1- PDL1 story? J Camarero (CHMP alternate ES, OncWP) Disclaimers the views presented
CHMP Oncology Working Party Workshop Histology independent indications in Oncology What have we learnt from the anti PD1- PDL1 story? J Camarero (CHMP alternate ES, OncWP) Disclaimers the views presented
Immuno-Oncology Applications
 Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA
 DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment
 Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
IMMUNE CHECKPOINT THERAPY FOR GENITOURINARY CANCERS: KIDNEY CANCER AND TRANSITIONAL CELL CARCINOMA
 IMMUNE CHECKPOINT THERAPY FOR GENITOURINARY CANCERS: KIDNEY CANCER AND TRANSITIONAL CELL CARCINOMA Kathleen Mahoney, M.D., Ph.D. Instructor of Medicine, Harvard Medical School Attending, Beth Israel Deaconess
IMMUNE CHECKPOINT THERAPY FOR GENITOURINARY CANCERS: KIDNEY CANCER AND TRANSITIONAL CELL CARCINOMA Kathleen Mahoney, M.D., Ph.D. Instructor of Medicine, Harvard Medical School Attending, Beth Israel Deaconess
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma
 Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
Background. Outcomes in refractory large B-cell lymphoma with traditional standard of care are extremely poor 1
 2-Year Follow-Up and High-Risk Subset Analysis of ZUMA-1, the Pivotal Study of Axicabtagene Ciloleucel (Axi-Cel) in Patients with Refractory Large B Cell Lymphoma Abstract 2967 Neelapu SS, Ghobadi A, Jacobson
2-Year Follow-Up and High-Risk Subset Analysis of ZUMA-1, the Pivotal Study of Axicabtagene Ciloleucel (Axi-Cel) in Patients with Refractory Large B Cell Lymphoma Abstract 2967 Neelapu SS, Ghobadi A, Jacobson
CAR T-Cell Therapy for Lymphoma: Assessing Long-Term Durability. Julie M. Vose, MD, MBA
 CAR T-Cell Therapy for Lymphoma: Assessing Long-Term Durability Julie M. Vose, MD, MBA Relevant Disclosures Research Funding: Kite Pharma/Gilead, JUNO/Celgene, Novartis Honorarium/Ad Boards: Novartis,
CAR T-Cell Therapy for Lymphoma: Assessing Long-Term Durability Julie M. Vose, MD, MBA Relevant Disclosures Research Funding: Kite Pharma/Gilead, JUNO/Celgene, Novartis Honorarium/Ad Boards: Novartis,
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies. Eric H. Rubin, MD Merck Research Laboratories
 Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Immunotherapy in non-small cell lung cancer
 Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal. Gabriela Sousa Oncologia Médica IPO Coimbra
 O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal Gabriela Sousa Oncologia Médica IPO Coimbra Incidência aumenta 3% ao ano Envelhecimento populacional
O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal Gabriela Sousa Oncologia Médica IPO Coimbra Incidência aumenta 3% ao ano Envelhecimento populacional
Disclosures WOJCIECH JURCZAK
 Disclosures WOJCIECH JURCZAK ABBVIE (RESEARCH FUNDING), CELGENE (RESEARCH FUNDING); EISAI (RESEARCH FUNDING); GILEAD (RESEARCH FUNDING); JANSEN (RESEARCH FUNDING); MORPHOSYS (RESEARCH FUNDING), MUNDIPHARMA
Disclosures WOJCIECH JURCZAK ABBVIE (RESEARCH FUNDING), CELGENE (RESEARCH FUNDING); EISAI (RESEARCH FUNDING); GILEAD (RESEARCH FUNDING); JANSEN (RESEARCH FUNDING); MORPHOSYS (RESEARCH FUNDING), MUNDIPHARMA