Endoscopic techniques for surveillance and treatment of FAP
|
|
|
- Sherman Miles
- 5 years ago
- Views:
Transcription
1 Endoscopic techniques for surveillance and treatment of FAP Evelien Dekker MD PhD Department of Gastroenterology & Hepatology Academic Medical Center Amsterdam The Netherlands
2 FAP: endoscopic surveillance & treatment Colon Duodenum Stomach Small bowel
3 Questions for GE in FAP: Who do we surveil? What age to start Frequency of surveillance Method of surveillance When to intervene Which treatment-options
4 Colon: who do we surveil? Presymptomatic: Persons with familiar risk APC-mutation carriers If no mutation is detected in proband: all 1 st degree family members Symptomatic..

5 Symptomatic 52 yr old man
6 Colon: Age, frequency & method Classic FAP: from 12 yrs 2-yearly sigmoidoscopy Attenuated FAP (AFAP): from 18 yrs 2-yearly colonoscopy
7 Colon: Method Careful non-magnified endoscopy All general quality measures must be taken into account: adequate bowel prep, withdrawal time etc Role for advanced imaging?
8 Chromoendoscopy Contrast stains Indigo-carmine (0,1 0,5%) Absorptive stains Methylene blue (0,1%)

9 Chromoendoscopy Targetted Directly through the workingchannel Segment or full colon With use of a spraycatheter
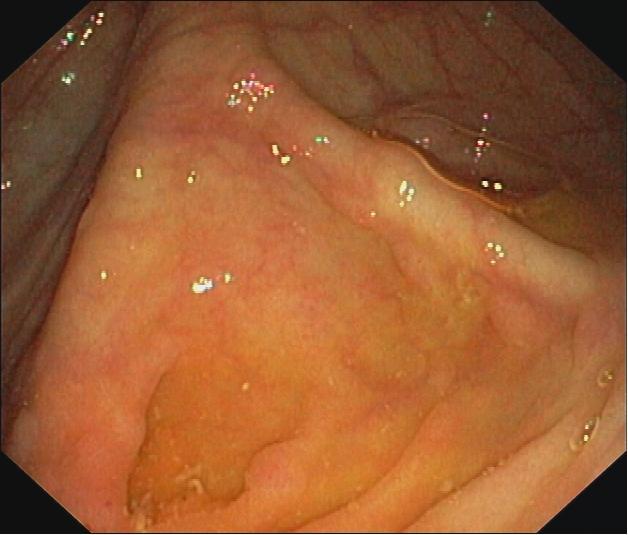

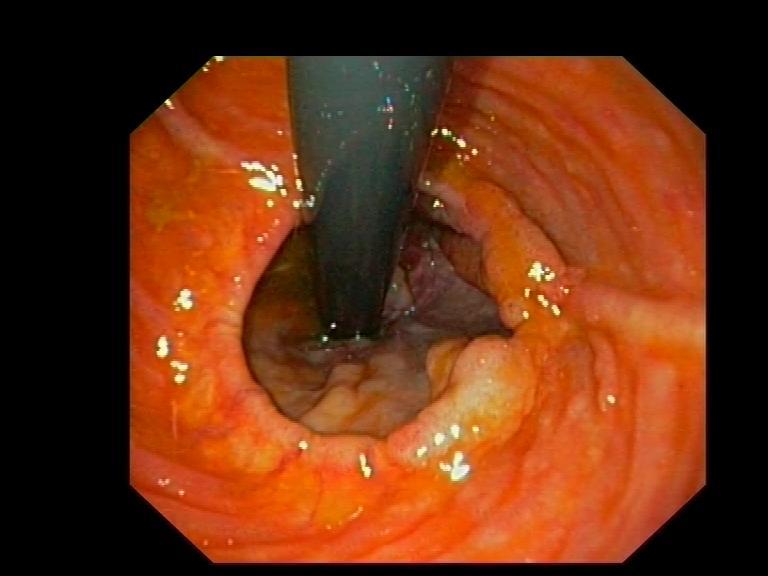
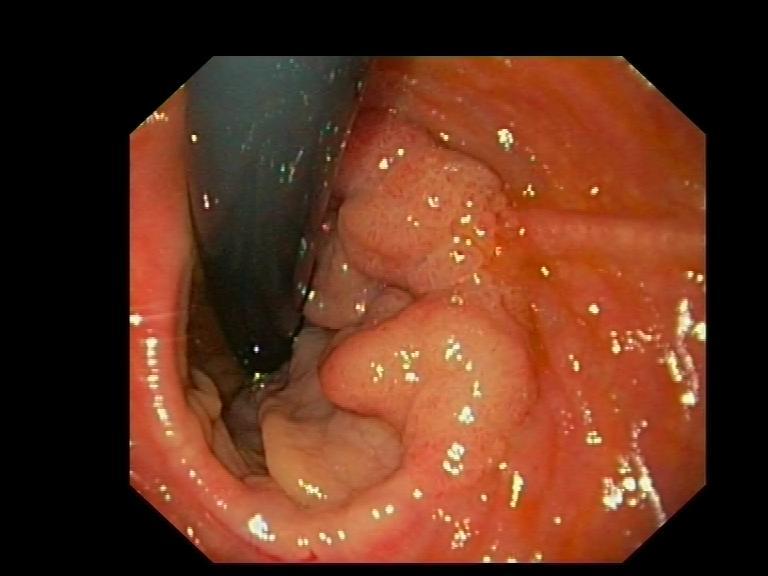
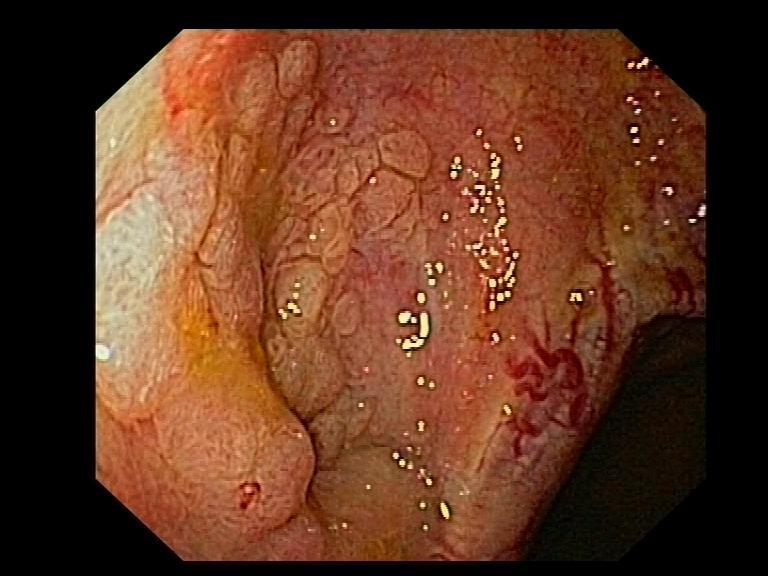
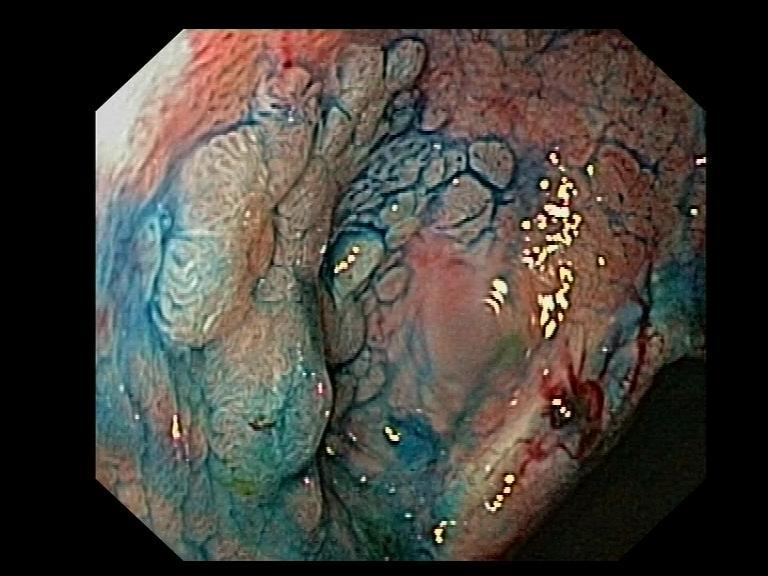
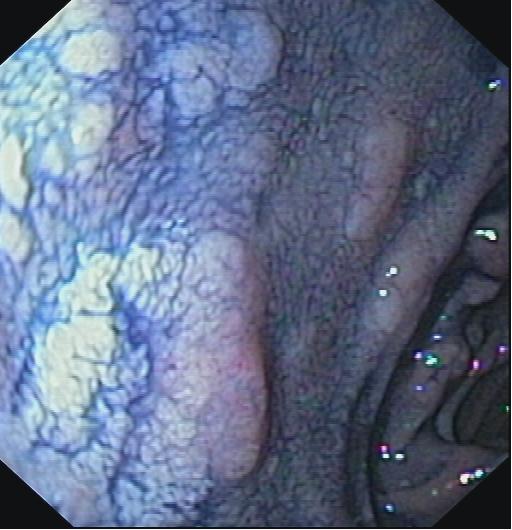
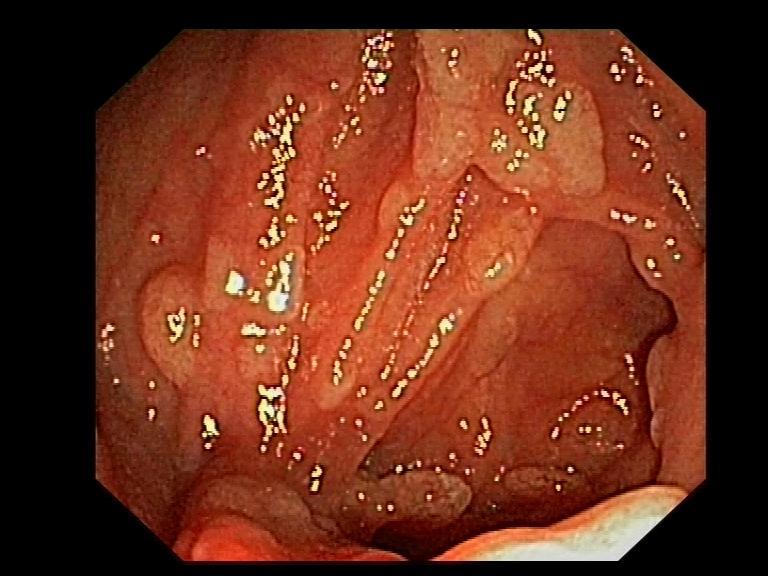
10 Chromoendoscopy in patient with AFAP

11

12
13 Colon: Method Use chromo (targeted or through a spraycatheter) At any discolouration If there is suspicion on genetic or familial basis
14 Colon: when to intervene? No guidelines.. If burden of polyps is severe and cancer cannot be ruled out
15 Colon: when to intervene? Classic FAP: Try to wait until adulthood Attenuated FAP: Possible to manage endoscopically??
16 Which treatment-options? Surgical Subtotal colectomy with ileorectal anastomosis Proctocolectomy with ileoanal pouch-reconstruction with ileostomy
17 Which operation?? Subtotal colectomy Best functional outcome However, chance of need for secondary proctectomy Related to genotype, phenotype & age at surgery Sinha et al, Br J Surg 2010
18 AMC: Proctocolectomy with ileoanal pouchreconstruction, stapeled Final operation Can be performed laparoscopically Functional outcome is good
19 Risks of pouch: 212 pats in Netherlands, 7.9 yrs follow-up Risk of adenomas 45% Risk of advanced pathology 11.8% Risk of cancer 1.9%, 10-year cumulative risk 75.5% However, due to retrospective nature no exact location of lesions possible.. Friederich et al, Clin Gastro Hep 2008

20 Patient 52 yr
21 And: Risk of adenoma formation Pouch In (small) anorectal segment Risk is larger if anastomosis is stapeled and not handsewn (St Marks Polyposis registry, 206 pats with pouch, 10.3 yrs follow-up) Von Roon et al, Ann Surg 2011

22 Patient 64 yr


23 Patient 36 yr

24 Patient 31 yr

25 Patient 20 years
26
27
28

29 Patient 40 years
30
31
32
33

34
35
36

37

38

39

40
41 Now in AMC: All patients undergo colonoscopy before colonic surgery If polyps close to anorectal verge: first polypectomies If in doubt: surgical mucosectomy and inlay with ileal mucosa
42 Surveillance after surgical resection: Ileorectal anastomosis: 6 monthly sigmoidoscopy (yearly??) Ileoanal pouch-reconstruction: Yearly pouch-scopy with gastroscope (NB minute inspection of anorectal segment, also in retroflex!) Ileostomy: No data on endoscopy of stoma

43 Duodenum
44 Questions for duodenum in FAP: Who do we surveil? Method of surveillance Frequency of surveillance When to intervene Which treatment-options
45 Duodenal polyposis in FAP In past: patients died from CRC Genetic testing & awareness of risk surveillance and colectomy better survival Most important causes of death in FAP: desmoïds and duodenal carcinoma
46 Duodenal polyposis Prevalence 60% Life-time cumulative risk 100% Björk et al Gastro 01 Groves et al Gut 02 Bülow et al Gut 04
47 Duodenal polyposis Prevalence 60% Life-time cumulative risk 100% Estimated cumulative risk duodenal carcinoma 4-10% Björk et al Gastro 01 Groves et al Gut 02 Bülow et al Gut 04
48 Duodenal polyposis in FAP How to assess who is at risk for duodenal carcinoma??
49 Spigelman classification # points # Polyps >20 Size (mm) >10 Type adenoma Degree of dysplasia tubulair tubulovillous villous low-grade high-grade Spigelman et al, Lancet 1989
50 Spigelman classification Stage 0: 0 points Stage I: 1-4 points Stage II: 5-6 points Stage III: 7-8 points Stadium IV: 9-12 points
51 Who is most at risk? Correlation between Spigelman stage and chance of getting duodenal cancer highest risk in patients with stage IV Groves Gut 02: 36% vs 2.4% Sp III Bülow Gut 04: 7% vs 0.7% Sp 0-III
52 Duodenum: method, age & frequency Gastroduodenoscopy with assessment of Spigelman stage Start at yrs Interval depending on Spigelman-stage (5 yearly 6 monthly)
53 Duodenum: method Use of advanced imaging techniques? To detect polyps To assess margins To differentiate to target biopsies

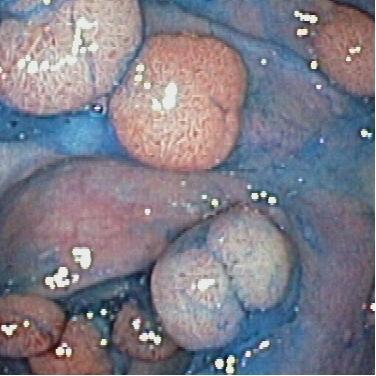
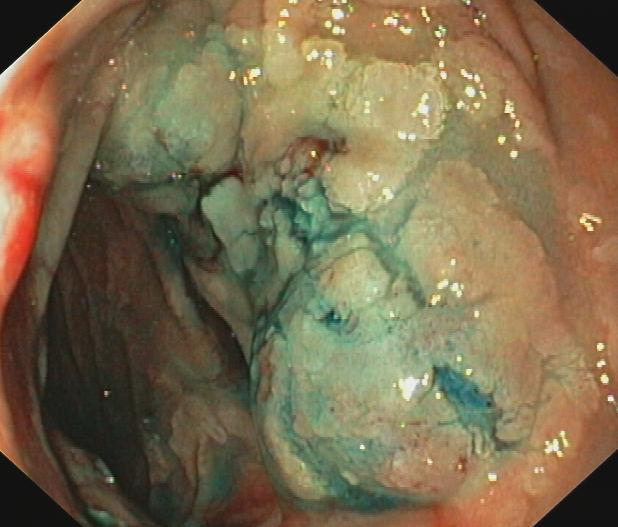
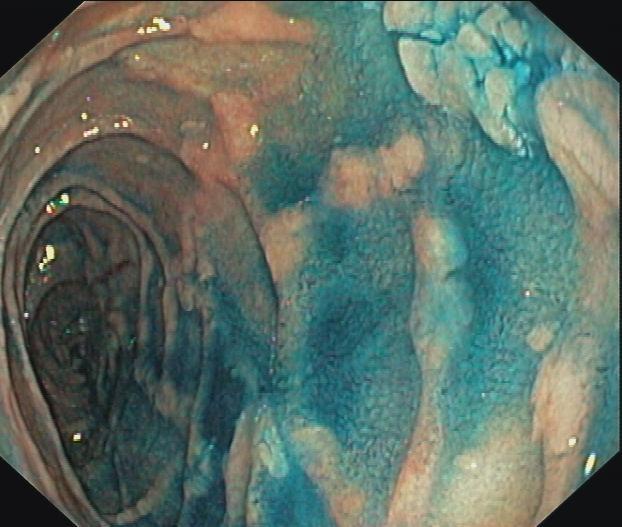
54 Duodenum: chromo

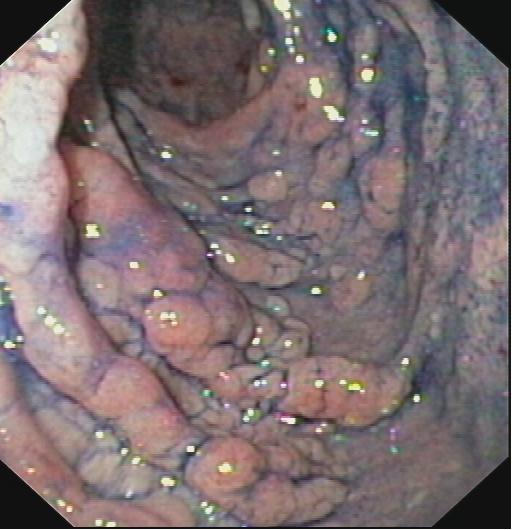
55 Duodenum: chromo
56 Study on chromo in duodenum in 45 pats: Mean Before indigo After indigo p # polyps Size mm Dekker at al, Endoscopy 2009
57 Chromoendoscopy per patient: More duodenal polyps detected in 13 pats Maximum size of the polyps increased in 7 pats Total number of points for the Spigelmanclassification was increased in 8 pats However, this resulted in an increased Spigelman-classification in only 5 pats (11%) Dekker at al, Endoscopy 2009
58 Spigelman classifications: chromoendoscopy Spigelman Before indigo After indigo O 3 (7%) 2 (4%) I 2 (4%) 2 (4%) II 11 (24%) 10 (22%) III 16 (36%) 17 (35%) IV 13 (29%) 14 (31%)
59 Chromoendoscopy duodenal FAP: Extra work No proven additonal benefit Not routinely Dekker at al, Endoscopy 2009
60 NBI in duodenal FAP? No studies published, 1 case-report Prospective study ongoing in AMC (with Spanish help) Yamao et al, Med Sci Monit 2009

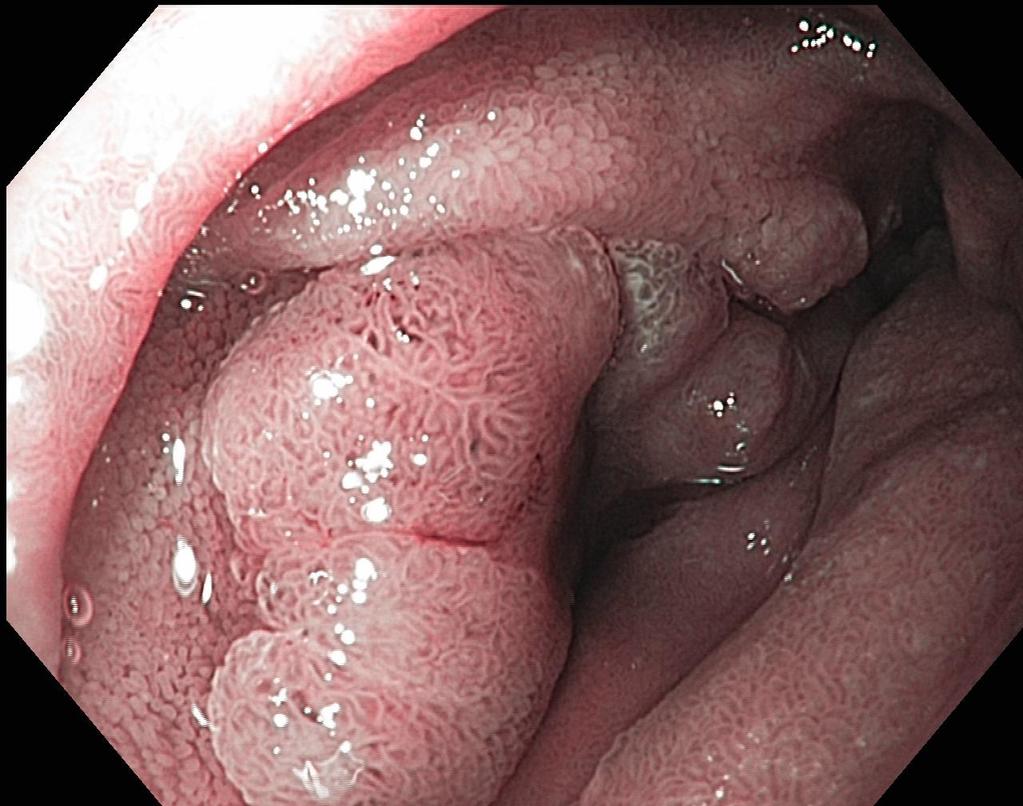
61 TVA with LGD


62 TVA with LGD

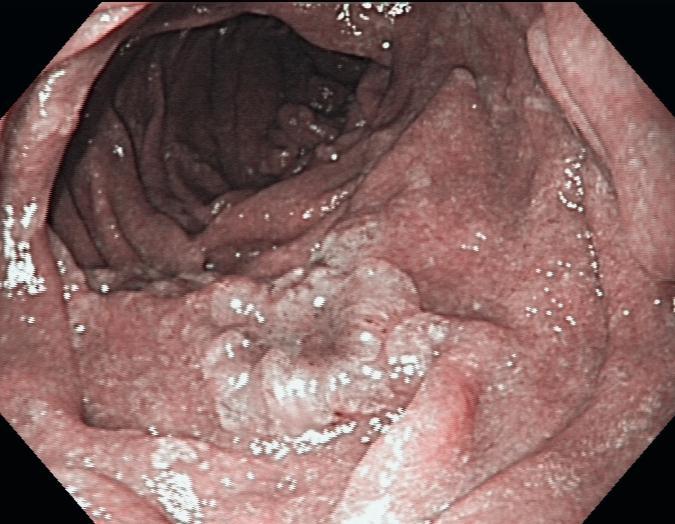
63 TVA with HGD
64 Duodenum: When to intervene?? Correlation between Spigelman stage and chance of getting duodenal cancer highest risk in patients with stage IV However many patients are nowadays in stage IV
65 Netherlands 45 FAP patients (22, median age 47 yrs) Forward and sideward viewing gastroscopy
 27% - 39% III 16 (36%) 17% - 36% IV 13 (29%) 7% - 10% Dekker at al, Endoscopy")
66 Spigelman stages Spigelman This study Historical Bülow Groves 0 3 (7%) 34% - 2% I 2 (4%) 15% - 13% II 11 (24%) 27% - 39% III 16 (36%) 17% - 36% IV 13 (29%) 7% - 10% Dekker at al, Endoscopy 2009
67 Reasons for many stage IV? Age of patients? Better quality of endoscopy?

68 Also: 44% had papillary adenoma
69 In whom to intervene? Assess during gastroscopy Spigelman-stage (so count, measure and take biopsies) PLUS papilla separately
70 In whom to intervene? Growing papillary adenoma: papillectomy Multiple adenomas with HGD or lage polyp-burden and one with HGD: surgical resection
71 Surgical options: Sparing: Transduodenal polypexcision Partial duodenectomy Definitive, high morbidity & mortality Pancreaticoduodenectomy ( Whipple ) Pancreassparing duodenectomy
72 In whom to intervene? Growing papillary adenoma: papillectomy Multiple adenomas with HGD or lage polyp-burden and one with HGD: surgical resection Relatively low polyp-burden and one adenoma with HGD: EMR??
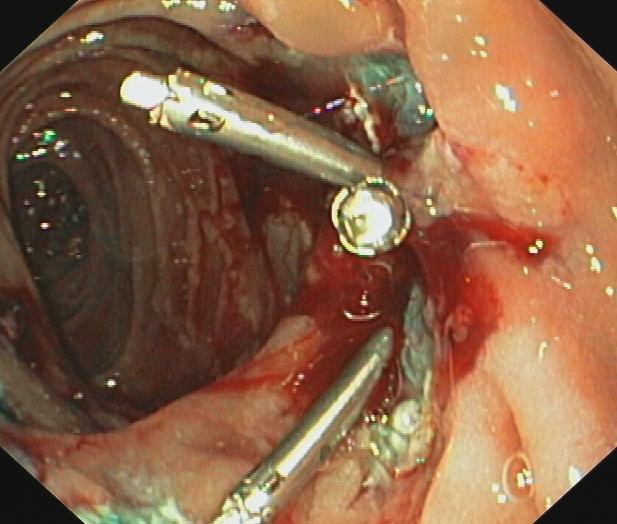
73 Endoscopic ampullectomie Retrospective analysis 59 FAP-pats: Multipele sessions only 34% resulted in normal histology (NB is that required??) Norton et al 2002
74 St Marks All FAP-pats with duodenal polyps >1 cm NO papillary adenoma Endoscopic polypectomy +/- APC Latchford et al, InSight 2007
75 Interim analysis 46 pats 85 therapeutic procedures Median follow-up 24 mo (3-111) 14 downstaged, 3 upstaged, 13 stable, 16 await staging 10 bleedings (4 transfusions), no perforations or deaths Latchford et al, InSight 2007
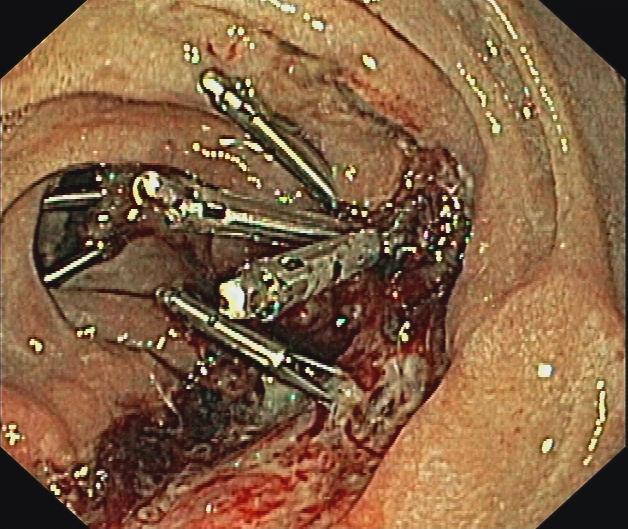
76 AMC Patients with FAP en duodenal polyps with HGD òr papillary adenoma increasing in size Endoscopic treatment of only those polyps: EMR, APC, ampullectomy etc (propofol, 1 night cinical observation) Re-endoscopy after 3 months If necessary re-treatment


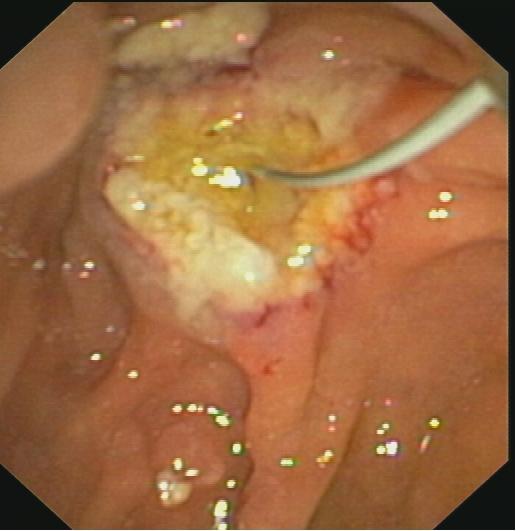

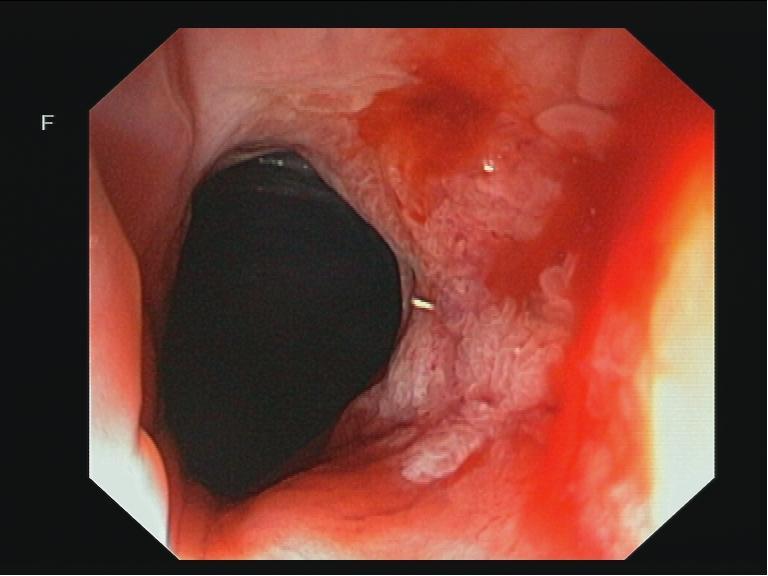
77 Endoscopic ampullectomy Growing TVA with LGD


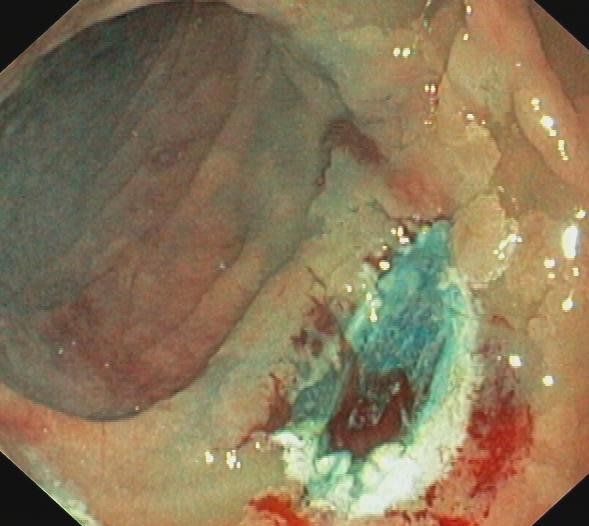
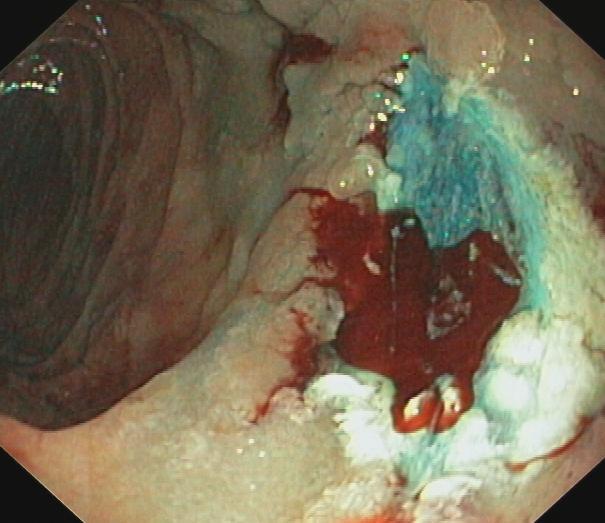
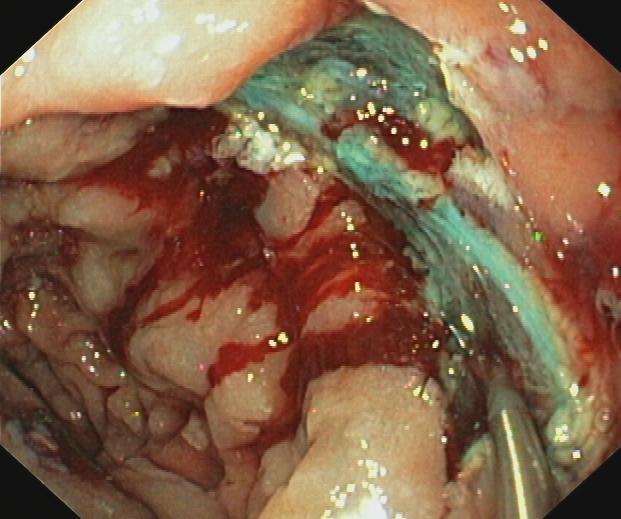
78 Duodenal TVA met HGD


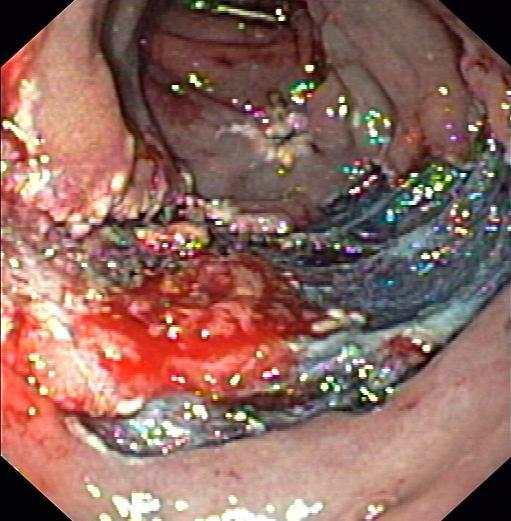
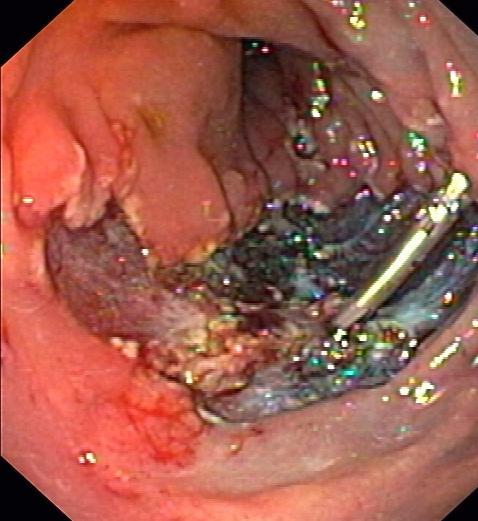
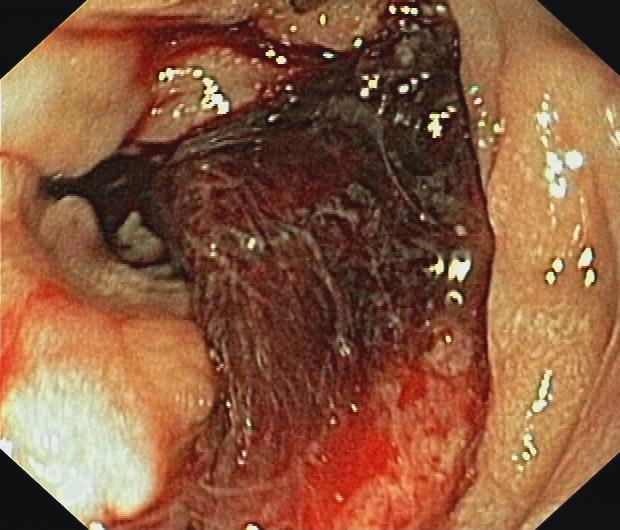


79 Duodenal TVA with HGD
80 After surgical resection: Also surveillance of jejunum, especially area of neopapilla..

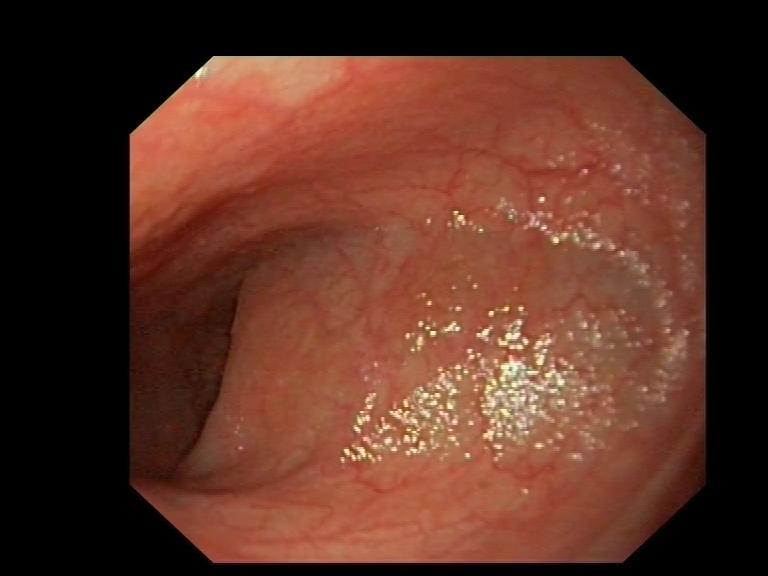
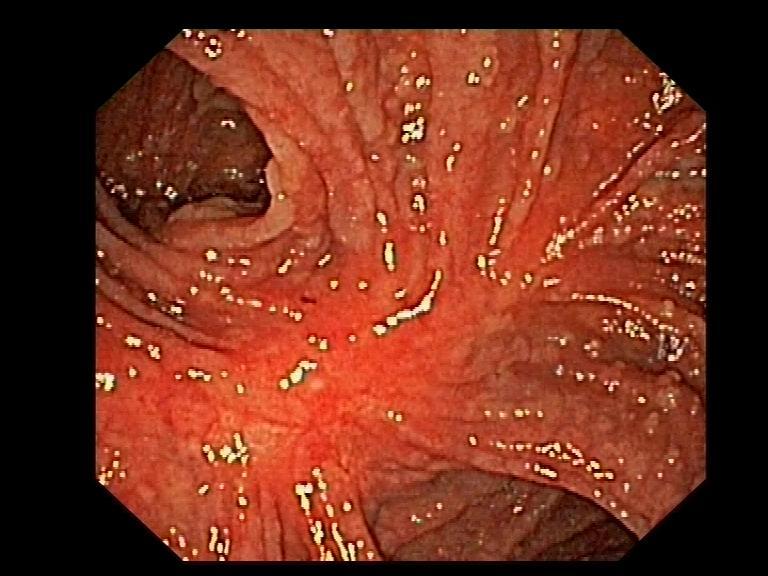
81 Stomach: fundic gland polyps
82 Stomach: fundic gland polyps Benign Literature: one doubtful cancer.. Practice: inspect and biopsy if abnormality

83 Stomach: antral adenomas
84 Stomach: antral adenomas Incidence increased?? Chance of malignant transformation? Practice: inspect antrum and biopsy any abnormalities If proven by histopathology: polypectomy??

85 Patient 40 years

86

87
88 Jejenum & ileum
89 Surveillance jejunum & ileum in FAP? Almost all patients have polyps Several case reports.. However, what is true incidence of cancer?? Ruys et al, Clin Gastro Hep 2010
90 Surveillance jejunum & ileum in FAP? Capsule endoscopy SBE DBE
91 Surveillance jejunum & ileum in FAP? No proven benefit Exceptions: Before duodenal resection After duodenal resection Spigelman IV??

92
93

94
95
96
97

98
99 Conclusions FAP-patients deserve close endoscopic surveillance and timely surgical (medical??) intervention No evidence-based guidelines for both diagnosis and treatment Uniformly collected, prospective data are difficult to gather but needed!
100
Duodenal adenomas Management. Dr Stratis Alexandridis Consultant Gastroenterologist BRI
 Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
Pathology reports, related operative reports and consult letters must be provided with a request for assessment.
 Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis
 Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right?
 Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Timing of surgery in FAP
 Timing of surgery in FAP Sue Clark Consultant Colorectal Surgeon, The Polyposis Registry, St Mark s Hospital, London, UK. 0-5 5-10 10-15 15-20 20-25 25-30 30-35 35-40 40-45 45-50 50-55 55-60 60-65 65-70
Timing of surgery in FAP Sue Clark Consultant Colorectal Surgeon, The Polyposis Registry, St Mark s Hospital, London, UK. 0-5 5-10 10-15 15-20 20-25 25-30 30-35 35-40 40-45 45-50 50-55 55-60 60-65 65-70
GI Polyp syndromes in children. Screening and surveillance, surgery.
 Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital, UK GI Polyp syndromes in children Screening and surveillance, surgery. No conflict of interests to declare Objectives Understand
Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital, UK GI Polyp syndromes in children Screening and surveillance, surgery. No conflict of interests to declare Objectives Understand
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions. South Island Cancer Nurses Network September 2013
 For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
PENETRANCE ACTIONABILITY SIGNIFICANCE/BURDEN OF DISEASE NEXT STEPS. YES ( 1 of above) YES (Proceed to Stage II)
 YES (Proceed to Stage II)") Stage I: Binning Dashboard GENE/GENE PANEL: APC ACTIONABILITY 1. Is there a qualifying resource, such as a practice guideline or systematic review, for the genetic condition? 2. Does the practice guideline
Stage I: Binning Dashboard GENE/GENE PANEL: APC ACTIONABILITY 1. Is there a qualifying resource, such as a practice guideline or systematic review, for the genetic condition? 2. Does the practice guideline
Familial Adenomatous Polyposis
 Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
YES NO UNKNOWN. Stage I: Rule-Out Dashboard ACTIONABILITY PENETRANCE SIGNIFICANCE/BURDEN OF DISEASE NEXT STEPS. YES ( 1 of above)
") Stage I: Rule-Out Dashboard GENE/GENE PANEL: SMAD4, BMPR1A DISORDER: Juvenile Polyposis Syndrome HGNC ID: 6670, 1076 OMIM ID: 174900, 175050 ACTIONABILITY PENETRANCE 1. Is there a qualifying resource,
Stage I: Rule-Out Dashboard GENE/GENE PANEL: SMAD4, BMPR1A DISORDER: Juvenile Polyposis Syndrome HGNC ID: 6670, 1076 OMIM ID: 174900, 175050 ACTIONABILITY PENETRANCE 1. Is there a qualifying resource,
Familial adenomatous polyposis (FAP) is an autosomal
 is an autosomal") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:1237 1242 Risk of Developing Adenomas and Carcinomas in the Ileal Pouch in Patients With Familial Adenomatous Polyposis PIETER FRIEDERICH,* ANDREA E. DE
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:1237 1242 Risk of Developing Adenomas and Carcinomas in the Ileal Pouch in Patients With Familial Adenomatous Polyposis PIETER FRIEDERICH,* ANDREA E. DE
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS. Family Health Clinical Genetics. Clinical Genetics department
 GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
An Introduction to MUTYH Associated Polyposis (MAP)
") An Introduction to MUTYH Associated Polyposis (MAP) 1 An Introduction to MUTYH Associated Polyposis(MAP) Contents What is MUTYH Associated Polyposis (MAP)? 2 What causes MUTYH Associated Polyposis (MAP)?
An Introduction to MUTYH Associated Polyposis (MAP) 1 An Introduction to MUTYH Associated Polyposis(MAP) Contents What is MUTYH Associated Polyposis (MAP)? 2 What causes MUTYH Associated Polyposis (MAP)?
WEO CRC SC Meeting. Barcelona, Spain October 23, 2015
 WEO CRC SC Meeting Barcelona, Spain October 23, 2015 Identification of serrated polyposis syndrome in the context of population-based CRC screening programs Evelien Dekker Academic Medical Center Amsterdam,
WEO CRC SC Meeting Barcelona, Spain October 23, 2015 Identification of serrated polyposis syndrome in the context of population-based CRC screening programs Evelien Dekker Academic Medical Center Amsterdam,
FAMILIAL ADENOMATOUS POLYPOSIS (COLORECTAL CANCER) PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES
 PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES") FAMILIAL ADENOMATOUS POLYPOSIS (COLORECTAL CANCER) PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES Coordinator: Alex Kartheuser (Colorectal Surgery, Cliniques universitaires St-Luc, UCL) Authors
FAMILIAL ADENOMATOUS POLYPOSIS (COLORECTAL CANCER) PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES Coordinator: Alex Kartheuser (Colorectal Surgery, Cliniques universitaires St-Luc, UCL) Authors
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Rectal EMR: Techniques and Tips
 Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University
 Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University") COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
Content. Diagnostic approach and clinical management of Lynch Syndrome: guidelines. Terminology. Identification of Lynch Syndrome
 of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
2. Describe pros/cons of screening interventions (including colonoscopy, CT colography, fecal tests)
") Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
EXPERT WORKING GROUP Surveillance after neoplasia removal. Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum
 EXPERT WORKING GROUP Surveillance after neoplasia removal Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum AIM To improve the quality of the evidences we have regarding post- polypectomy
EXPERT WORKING GROUP Surveillance after neoplasia removal Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum AIM To improve the quality of the evidences we have regarding post- polypectomy
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
HEREDITARY COLORECTAL CANCER AND POLYPOSIS SYNDROMES
 gastrointestinal tract and abdomen HEREDITARY COLORECTAL CANCER AND POLYPOSIS SYNDROMES Jose G. Guillem, MD, MPH, FACS, and John B. Ammori, MD* The majority of cases of inherited colorectal cancer (CRC)
gastrointestinal tract and abdomen HEREDITARY COLORECTAL CANCER AND POLYPOSIS SYNDROMES Jose G. Guillem, MD, MPH, FACS, and John B. Ammori, MD* The majority of cases of inherited colorectal cancer (CRC)
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes
 ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Syngal, MD, MPH, FACG, 1,2,3 Randall E. Brand, MD, FACG, 4 James M. Church, MD, FACG, 5,6,7
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Syngal, MD, MPH, FACG, 1,2,3 Randall E. Brand, MD, FACG, 4 James M. Church, MD, FACG, 5,6,7
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
B Base excision repair, in MUTYH-associated polyposis and colorectal cancer, BRAF testing, for hereditary colorectal cancer, 696
 Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
University of Groningen
 University of Groningen Incidence of small bowel neoplasia in Lynch syndrome assessed by video capsule endoscopy Haanstra, Jasmijn; Al-Toma, Abdul; Dekker, Evelien; Vanhoutvin, Steven A L W; Nagengast,
University of Groningen Incidence of small bowel neoplasia in Lynch syndrome assessed by video capsule endoscopy Haanstra, Jasmijn; Al-Toma, Abdul; Dekker, Evelien; Vanhoutvin, Steven A L W; Nagengast,
Colorectal Cancer and Hereditary Colon Cancer Syndromes Carol A. Burke, M.D.
 Colorectal Cancer and Hereditary, FACG, FACP Sanford R. Weiss MD Center for Hereditary Colorectal Neoplasia Digestive Disease Institute Cleveland Clinic, Cleveland, Ohio 1 Objectives Review the molecular
Colorectal Cancer and Hereditary, FACG, FACP Sanford R. Weiss MD Center for Hereditary Colorectal Neoplasia Digestive Disease Institute Cleveland Clinic, Cleveland, Ohio 1 Objectives Review the molecular
Adenoma to Carcinoma Pathway
 It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
ORIGINAL ARTICLE. Extracolonic Manifestations of Familial Adenomatous Polyposis After Proctocolectomy
 ORIGINAL ARTICLE Extracolonic Manifestations of Familial Adenomatous Polyposis After Proctocolectomy Hagit Tulchinsky, MD; Andrei Keidar, MD; Hana Strul, MD; Gideon Goldman, MD; Joseph M. Klausner, MD;
ORIGINAL ARTICLE Extracolonic Manifestations of Familial Adenomatous Polyposis After Proctocolectomy Hagit Tulchinsky, MD; Andrei Keidar, MD; Hana Strul, MD; Gideon Goldman, MD; Joseph M. Klausner, MD;
Citation for published version (APA): Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects
: Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects") UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
Classification of polyposis syndromes two major groups. Adenomatous polyposis syndromes. Hamartomatous polyposis syndromes
 Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Understanding Your Genetic Test Result. Positive for a Deleterious Mutation or Suspected Deleterious
 Understanding Your Genetic Test Result Positive for a Deleterious Mutation or Suspected Deleterious This workbook is designed to help you understand the results of your genetic test and is best reviewed
Understanding Your Genetic Test Result Positive for a Deleterious Mutation or Suspected Deleterious This workbook is designed to help you understand the results of your genetic test and is best reviewed
Colorectal Cancer Prevention Quantity and Quality Count
 Colorectal Cancer Prevention Quantity and Quality Count Ernesto Drelichman, MD Gastrointestinal Surgery & Endoscopy Providence Hospital Key Messages Colorectal cancer can be prevented Screening reduces
Colorectal Cancer Prevention Quantity and Quality Count Ernesto Drelichman, MD Gastrointestinal Surgery & Endoscopy Providence Hospital Key Messages Colorectal cancer can be prevented Screening reduces
Journal of Pediatric Gastroenterology and Nutrition, Publish Ahead of Print
 Journal of Pediatric Gastroenterology and Nutrition, Publish Ahead of Print DOI : 10.1097/MPG.0000000000002247 Management of familial adenomatous polyposis in children and adolescents: Position Paper from
Journal of Pediatric Gastroenterology and Nutrition, Publish Ahead of Print DOI : 10.1097/MPG.0000000000002247 Management of familial adenomatous polyposis in children and adolescents: Position Paper from
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool
 When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
Adenomatous Polyposis Syndromes (FAP/AFAP and MAP)
") A Patient s Guide to risk assessment Adenomatous Polyposis Syndromes (FAP/AFAP and MAP) Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer
A Patient s Guide to risk assessment Adenomatous Polyposis Syndromes (FAP/AFAP and MAP) Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer
Mr Chris Wakeman. General Surgeon University of Otago, Christchurch. 12:15-12:40 Management of Colorectal Cancer
 Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Adenomatous Polyposis Syndromes (FAP/AFAP and MAP)
") A Patient s Guide to risk assessment Adenomatous Polyposis Syndromes (FAP/AFAP and MAP) Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer
A Patient s Guide to risk assessment Adenomatous Polyposis Syndromes (FAP/AFAP and MAP) Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer
Chromoendoscopy as an Adjunct to Colonoscopy
 Chromoendoscopy as an Adjunct to Colonoscopy Policy Number: 2.01.84 Last Review: 1/2018 Origination: 7/2017 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide
Chromoendoscopy as an Adjunct to Colonoscopy Policy Number: 2.01.84 Last Review: 1/2018 Origination: 7/2017 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD
 CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
Gastrointestinal polyposis syndromes for the general gastroenterologist
 TRAINING MATTERS CURRICULUM BASED CLINICAL REVIEWS Gastrointestinal polyposis syndromes for the general gastroenterologist Joanna J Hurley, 1,2 Iain Ewing, 3 Julian R Sampson, 2 Sunil Dolwani 1 1 Department
TRAINING MATTERS CURRICULUM BASED CLINICAL REVIEWS Gastrointestinal polyposis syndromes for the general gastroenterologist Joanna J Hurley, 1,2 Iain Ewing, 3 Julian R Sampson, 2 Sunil Dolwani 1 1 Department
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Natural history of adenomas by CT colonography Evelien Dekker Charlotte Tutein Nolthenius, Jaap Stoker
 Natural history of adenomas by CT colonography Charlotte Tutein Nolthenius, Jaap Stoker Academic Medical Center Amsterdam, the Netherlands Possible conflicts of interest None Colonoscopy.. plus polypectomy
Natural history of adenomas by CT colonography Charlotte Tutein Nolthenius, Jaap Stoker Academic Medical Center Amsterdam, the Netherlands Possible conflicts of interest None Colonoscopy.. plus polypectomy
Risk factors for advanced duodenal and ampullary adenomatosis in familial adenomatous polyposis: a prospective, single-center study
 Risk factors for advanced duodenal and ampullary adenomatosis in familial adenomatous polyposis: a prospective, single-center study Authors M. Sulbaran 1,F.G.Campos 2, U. Ribeiro Jr. 2,H.S.Kishi 3,P.Sakai
Risk factors for advanced duodenal and ampullary adenomatosis in familial adenomatous polyposis: a prospective, single-center study Authors M. Sulbaran 1,F.G.Campos 2, U. Ribeiro Jr. 2,H.S.Kishi 3,P.Sakai
Carol A. Burke, MD, FACG
 Updated Guidelines for CRC C Screening and Surveillance Carol A. Burke MD, FACG, FASGE, FACP Cleveland Clinic, Cleveland, OH Gastroenterology t 2012;143:844 143 Gut 2010;59:666 1 Caveat for all Recommendations
Updated Guidelines for CRC C Screening and Surveillance Carol A. Burke MD, FACG, FASGE, FACP Cleveland Clinic, Cleveland, OH Gastroenterology t 2012;143:844 143 Gut 2010;59:666 1 Caveat for all Recommendations
Risk of Colorectal Cancer (CRC) Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE
 Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE") Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Inherited Polyposis Syndromes
 CLINICAL PRACTICE GUIDELINES The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Inherited Polyposis Syndromes Daniel Herzig, M.D. Karin Hardimann, M.D.
CLINICAL PRACTICE GUIDELINES The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Inherited Polyposis Syndromes Daniel Herzig, M.D. Karin Hardimann, M.D.
Cost-effectiveness of adenoma surveillance - the Dutch guidelines -
 Cost-effectiveness of adenoma surveillance - the Dutch guidelines - WEO working group adenoma surveillance 20 May, 2016 Iris Lansdorp-Vogelaar, PhD On behalf of the SAP study-group Introduction Adenoma
Cost-effectiveness of adenoma surveillance - the Dutch guidelines - WEO working group adenoma surveillance 20 May, 2016 Iris Lansdorp-Vogelaar, PhD On behalf of the SAP study-group Introduction Adenoma
The Genetics of Familial Polyposis
 The Genetics of Familial Polyposis Thursday, September 24 th 2015 Kara Semotiuk, MS, (C)CGC & Laura Winter, MSc, CGC Genetic Counsellors at the FGICR Familial Polyposis Familial Can run in the family related
The Genetics of Familial Polyposis Thursday, September 24 th 2015 Kara Semotiuk, MS, (C)CGC & Laura Winter, MSc, CGC Genetic Counsellors at the FGICR Familial Polyposis Familial Can run in the family related
GI Screening/Surveillance in Lynch Syndrome
 GI Screening/Surveillance in Lynch Syndrome M Appleyard Royal Brisbane and Women s Hospital Brisbane, Australia GI Disease and Lynch Syndrome What are risks of GI disease in Lynch? Who do we screen for
GI Screening/Surveillance in Lynch Syndrome M Appleyard Royal Brisbane and Women s Hospital Brisbane, Australia GI Disease and Lynch Syndrome What are risks of GI disease in Lynch? Who do we screen for
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Colorectal Cancer Syndromes. Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago
 Colorectal Cancer Syndromes Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago Outline Colon cancer General Genetics, Risk, Screening Specific Syndromes, when to suspect,
Colorectal Cancer Syndromes Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago Outline Colon cancer General Genetics, Risk, Screening Specific Syndromes, when to suspect,
Finding and Removing Difficult Polyps (safely)
") Finding and Removing Difficult Polyps (safely) David Lieberman MD Chief, Division of Gastroenterology and Hepatology Oregon Health and Science University Colonoscopy Clouds Interval Cancers Interval Cancer:
Finding and Removing Difficult Polyps (safely) David Lieberman MD Chief, Division of Gastroenterology and Hepatology Oregon Health and Science University Colonoscopy Clouds Interval Cancers Interval Cancer:
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
BENEFIT APPLICATION BLUE CARD/NATIONAL ACCOUNT ISSUES
 Medical Policy BCBSA Ref. Policy: 2.01.84 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/Computed
Medical Policy BCBSA Ref. Policy: 2.01.84 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/Computed
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
EMR, ESD and Beyond. Peter Draganov MD. Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida
 EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
Extensive Surgery in LS factoring in gene and gender. Gabriela Möslein
 Extensive Surgery in LS factoring in gene and gender Gabriela Möslein Where we are coming from. Non polyposis colon cancer Recommend subtotal colectomy at the time of the first colon cancer Recommend prophylactic
Extensive Surgery in LS factoring in gene and gender Gabriela Möslein Where we are coming from. Non polyposis colon cancer Recommend subtotal colectomy at the time of the first colon cancer Recommend prophylactic
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
A superficial radiotherapy B single pass curettage C excision with 2 mm margins D excision with 5 mm margins E Mohs micrographic surgery.
 1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
Benchmarking For Colonoscopy. Technology and Technique to Improve Adenoma Detection
 Benchmarking For Colonoscopy Technology and Technique to Improve Adenoma Detection Objectives 1. Review the latest data on performance characteristics and efficacy for colon cancer prevention 2. Highlight
Benchmarking For Colonoscopy Technology and Technique to Improve Adenoma Detection Objectives 1. Review the latest data on performance characteristics and efficacy for colon cancer prevention 2. Highlight
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Precision Cancer Prevention: Hereditary Polyposis Syndromes
 Precision Cancer Prevention: Hereditary Polyposis Syndromes N. Jewel Samadder, MD, MSC, FRCPC HUNTSMAN CANCER INSTITUTE UNIVERSITY OF UTAH Familial Adenomatous Polyposis Familial Adenomatous Polyposis
Precision Cancer Prevention: Hereditary Polyposis Syndromes N. Jewel Samadder, MD, MSC, FRCPC HUNTSMAN CANCER INSTITUTE UNIVERSITY OF UTAH Familial Adenomatous Polyposis Familial Adenomatous Polyposis
Prevention of Bowel Cancer: which patients do I send for colonoscopy?
 Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
27
 26 27 28 29 30 31 32 33 34 35 Diagnosis:? Diagnosis: Juvenile Polyposis with BMPR1A Mutation 36 Juvenile Polyposis Syndrome Rare Autosomal Dominant Disorder with Multiple Juvenile Polyps in GI Tract Juvenile
26 27 28 29 30 31 32 33 34 35 Diagnosis:? Diagnosis: Juvenile Polyposis with BMPR1A Mutation 36 Juvenile Polyposis Syndrome Rare Autosomal Dominant Disorder with Multiple Juvenile Polyps in GI Tract Juvenile
BC CRC Update Malignant Polyp Who Needs Surgery
 BC CRC Update Malignant Polyp Who Needs Surgery Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary
BC CRC Update Malignant Polyp Who Needs Surgery Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary
EARLY DETECTION OF COLORECTAL CANCER. Epidemiology of CRC
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Frameshift Mutations (Deletion at Codon 1309 and Codon 849) in the APC Gene in Iranian FAP Patients: a Case Series and Review of the Literature
 in the APC Gene in Iranian FAP Patients: a Case Series and Review of the Literature") IJMCM Summer 2014, Vol 3, No 3 Case Series Frameshift Mutations (Deletion at Codon 1309 and Codon 849) in the APC Gene in Iranian FAP Patients: a Case Series and Review of the Literature Seyed Mohammad
IJMCM Summer 2014, Vol 3, No 3 Case Series Frameshift Mutations (Deletion at Codon 1309 and Codon 849) in the APC Gene in Iranian FAP Patients: a Case Series and Review of the Literature Seyed Mohammad
Upper gastrointestinal tract polyps in familial
 Upper gastrointestinal tract polyps in familial adenomatosis coli H JARVINEN, M NYBERG, AND P PELTOKALLIO Gut, 1983, 24, 333-339 From the Second Department of Surgery, Helsinki University Central Hospital,
Upper gastrointestinal tract polyps in familial adenomatosis coli H JARVINEN, M NYBERG, AND P PELTOKALLIO Gut, 1983, 24, 333-339 From the Second Department of Surgery, Helsinki University Central Hospital,
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
A Patient s Guide to risk assessment. Hereditary Colorectal Cancer
 A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? Overview of Syndromes This workbook is designed to help you decide if hereditary cancer
A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? Overview of Syndromes This workbook is designed to help you decide if hereditary cancer
Primary Care Approach to Genetic Cancer Syndromes
 Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
The Natural History of Right-Sided Lesions
 The Natural History of Right-Sided Lesions Jasper L.A. Vleugels Dept of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, the Netherlands. None Disclosures Agenda Is there evidence that
The Natural History of Right-Sided Lesions Jasper L.A. Vleugels Dept of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, the Netherlands. None Disclosures Agenda Is there evidence that
HHS Public Access Author manuscript Gastrointest Endosc. Author manuscript; available in PMC 2015 April 29.
 Endoscopic papillectomy: risk factors for incomplete resection and recurrence during long-term follow-up Wiriyaporn Ridtitid, MD 1,2, Damien Tan, MD 1, Suzette E. Schmidt, BSN 1, Evan L. Fogel, MD 1, Lee
Endoscopic papillectomy: risk factors for incomplete resection and recurrence during long-term follow-up Wiriyaporn Ridtitid, MD 1,2, Damien Tan, MD 1, Suzette E. Schmidt, BSN 1, Evan L. Fogel, MD 1, Lee
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Predict, Resect and discard : Yes we can! (at least in some hands)
") Diminutive polyps : Real time endoscopic histology Predict, Resect and discard : Yes we can! (at least in some hands) Robert Benamouzig Hôpital Avicenne AP-HP & Paris 13 University France Why it is important?
Diminutive polyps : Real time endoscopic histology Predict, Resect and discard : Yes we can! (at least in some hands) Robert Benamouzig Hôpital Avicenne AP-HP & Paris 13 University France Why it is important?
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Extracolonic Manifestations in Familial Adenomatous Polyposis
 Govaresh 2003; 8: 178-83 Extracolonic Manifestations in Familial Adenomatous Polyposis Narimantas Evaldas Samalavicius Department of Surgery, Vilnius Center University Hospital, Vilnius, Lithuania ABSTRACT
Govaresh 2003; 8: 178-83 Extracolonic Manifestations in Familial Adenomatous Polyposis Narimantas Evaldas Samalavicius Department of Surgery, Vilnius Center University Hospital, Vilnius, Lithuania ABSTRACT
Cancer Genomics 101. BCCCP 2015 Annual Meeting
 Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes
 PRACTICE GUIDELINES nature publishing group 223 CME ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Sy nga l, MD, M PH, FAC G 1, 2, 3, R and
PRACTICE GUIDELINES nature publishing group 223 CME ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Sy nga l, MD, M PH, FAC G 1, 2, 3, R and
LIST OF ABBREVIATIONS
 Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma?
 17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
COLON: Innovations 3 steps, 3 parts..
 COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
Hereditary GI tumor syndromes ACG guidelines of genetic testing and management. Dr. med. Henrik Csaba Horváth PhD
 Hereditary GI tumor syndromes ACG guidelines of genetic testing and management Dr. med. Henrik Csaba Horváth PhD Genetic testing and management of hereditary GI tumor syndromes June 29, 2016 2 Clinical
Hereditary GI tumor syndromes ACG guidelines of genetic testing and management Dr. med. Henrik Csaba Horváth PhD Genetic testing and management of hereditary GI tumor syndromes June 29, 2016 2 Clinical
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
ACG Clinical Guideline: Colorectal Cancer Screening
 ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,